The development of a conceptual framework for mental handicap nursing practice in the UK
9
The development of a conceptual framework for mental handicap nursing practice in the UK Charlotte Green This article explores a new approach to the development of a conceptual framework for nursing, with special reference to the British post-GrilIiths’ situation and to mental handicap. It then considers the value of this approach for all nursing specialties. INTRODUCTION In a previous article (Green 1985) it was stated that: (a) nursing models and conceptual frame- works provide a wide vista of insight into the nature of nursing and help indiv- idual nurses find meaning in their work; models and conceptual frameworks may also influence how nursing is carried out through influencing what is taught; models and conceptual frameworks are likely to be of limited specific use if they set out to cover nursing in general. (b) Cc) It is considered both that there is a genuine need for applicable nursing models and con- ceptual frameworks and that these may be useful even if unsupported by scientific re- search, as long as no claims are made for more supporting evidence than the situation war- rants. In any case this is likely to be an inevitable stage since models will usually precede the completion of research designed to test them. However, for many, this earlier stage does not truly denote a conceptual model. For this reason, in the rest of this article, the term Charlotte Green MSc MA, Principal Clinical Psychologist, Mental Handicap Services, Paddington Community Hospital, London W9 288 Manuscript accepted January 1987 ‘conceptual framework’ will be used to denote a model without evidence. Finally, it should be noted that in the author’s view: (a) (b) a conceptual framework does not require systematic construction, since how an idea is arrived at is of much less im- portance than its applicability and validity; nursing models should be primarily con- cerned with good nursing practice rather than good nursing values, since where good practice exists, good values are irrelevant, but the converse does not hold. Furthermore, it is pointless for a profession to attempt to dictate its prac- titioners’ values as it is quite impossible for these to be imposed, monitored or controlled. A different, but equally relev- ant line of argument bearing on the priority of practice over attitudes is the psychological truism that measured att- itudes and behaviour rarely correlate highly. The intention is to develop a conceptual frame- work for mental handicap nursing practice to which evidence may or may not be added later, and one which does not spell out the values required for its use. However, it was also stated at the beginning of this article that conceptual frameworks which aimed at too
-
Upload
charlotte-green -
Category
Documents
-
view
212 -
download
0
Transcript of The development of a conceptual framework for mental handicap nursing practice in the UK

The development of a conceptual framework for mental handicap nursing practice in the UK
Charlotte Green
This article explores a new approach to the development of a conceptual framework for nursing, with special reference to the British post-GrilIiths’ situation and to mental handicap. It then considers the value of this approach for all nursing specialties.
INTRODUCTION
In a previous article (Green 1985) it was stated
that:
(a) nursing models and conceptual frame- works provide a wide vista of insight into the nature of nursing and help indiv- idual nurses find meaning in their work; models and conceptual frameworks may also influence how nursing is carried out through influencing what is taught; models and conceptual frameworks are likely to be of limited specific use if they set out to cover nursing in general.
(b)
Cc)
It is considered both that there is a genuine need for applicable nursing models and con- ceptual frameworks and that these may be useful even if unsupported by scientific re- search, as long as no claims are made for more supporting evidence than the situation war- rants. In any case this is likely to be an inevitable stage since models will usually precede the completion of research designed to test them. However, for many, this earlier stage does not truly denote a conceptual model. For this reason, in the rest of this article, the term
Charlotte Green MSc MA, Principal Clinical Psychologist, Mental Handicap Services, Paddington Community Hospital, London W9 288 Manuscript accepted January 1987
‘conceptual framework’ will be used to denote a model without evidence. Finally, it should be noted that in the author’s view:
(a)
(b)
a conceptual framework does not require systematic construction, since how an idea is arrived at is of much less im-
portance than its applicability and
validity; nursing models should be primarily con- cerned with good nursing practice rather than good nursing values, since where good practice exists, good values are irrelevant, but the converse does not hold. Furthermore, it is pointless for a profession to attempt to dictate its prac- titioners’ values as it is quite impossible for these to be imposed, monitored or controlled. A different, but equally relev- ant line of argument bearing on the priority of practice over attitudes is the psychological truism that measured att- itudes and behaviour rarely correlate
highly.
The intention is to develop a conceptual frame- work for mental handicap nursing practice to which evidence may or may not be added later, and one which does not spell out the values required for its use. However, it was also stated at the beginning of this article that conceptual frameworks which aimed at too

10 NURSE EDUCATION TODAY
broad a coverage were paradoxically of limited use. We must therefore set out the parameters for this conceptual framework. The parameters have been chosen to accord with the whole range of mental handicap nursing as it is in the UK today. The conceptual framework must cover:
1. Special factors relating to nursing services in the UK in the post-Grifftths situation;
2. Mental handicap nursing, both in hos- pitals and in the community;
3. All grades of nursing staff within the specialty;
4. Variations in staff ability and preferences.
Throughout, the emphasis will be on develop- ing a framework that reflects what nurses in
mental handicap actually do. Some familiarity with the more popular
nursing models is assumed. These were discus- sed in a previous article (Green 1985) and in the series of papers by Aggleton et al ( 1984 85). The main topic of this section will be addressed by looking at various models in turn.
One of the chief difficulties in choosing a conceptual framework applicable to mental handicap nursing is that the needs of mentally handicapped people vary widely.
METHODS
Now that the boundaries to the coverage of the conceptual framework have been set, the real task, i.e. deciding on the concepts to be in- cluded, and their relation, remains. Some ways of going about this have been suggested by Heath (1986) who suggests as starting points, both choosing one model and adapting it to include aspects of others, and looking at a variety of models and exploring common ground. However, the author has set out a slightly different approach, namely:
1. Looking carefully at a number of models with a view to taking from each the concepts that are applicable to mental handicap nursing.
2. Comnaring mental handicau nursing as it
is with the concepts obtained by above, in order to see the conceptual between what has been obtained what is required.
(1) gap and
3. Filling the conceptual gap through rear- rangement and supplement to evolve a new framework.
Each of these steps will be discussed in turn.
Applicability of some existing nursing models to mental handicap
Some people with a mental hand:cap need physical care due to illness, and for these people restoration-to-equilibrium (Johnson) may be appropriate. However, others need physical care although the concept of restoration-to- equilibrium does not apply as they are not ill. This is also true for mentally handicapped people who have no disturbance, either of a physical or emotional nature, but who may lack skills. Thus Johnson’s concept of the nurse helping the patient back to equilibrium applies only to the needs of some mentally handi- capped people.
A similar argument can be applied to Roy, with the four principal adaptation systems, though if self-potentiation were an alternative to role mastery, Roy’s model would be more widely applicable to mental handicap. This extension of Roy’s model would take care of situations in mental handicap where the ment-
ally handicapped person has no role change to master but needs to develop his or her poten- tial. Much of what has just been said also applies to Riehl’s model, since basically she
sees the need for nursing as arising through bdisturbances. Even if this model might seem more promising for mental handicap nursing as it places less emphasis on physiological dis- turbances, in the writer’s view, Riehl’s em- phasis’ on role play in nursing intervention makes it insufficient for much of mental handi- cap nursing. In fairness however, it should be noted that mental handicap nurses might learn a lot about institutionalisation from role play, and also that role olav can be useful in teach-

NURSE EDUCATION TODAY 11
ing skills, though it is not usually the best
method with the mentally handicapped due to their difftculty in generalising from the role play situation. A further model, (Rogers), cen- tering on disturbance in balance - between human and environmental energy fields - is not seen as wholly applicable to mental handi- cap, even though the need of mentally handi- capped people for appropriate stimulation is recognised.
Models that describe nursing as required for problems of dependency and functional abilities
(Roper, Henderson & Orem) are considered to propose a concept applicable to the broad range of mental handicap. Indeed Roper ex- plicitly mentions disability as associated with a need for nursing care, and Henderson notes that ‘physical and intellectual capacities may affect a person’s ability to carry out basic
activities to satisfy needs’. Roper’s focus on nursing intervention through the patient’s activities of living and normal routines is also highly applicable to mental handicap nursing. So too is Henderson’s focus on funda- mental human needs (rights?) and on showing respect for the patient by negotiating care with him/her. .iVegotiation however, is unlikely to be applicable to the whole range of mental handi- cap. Nevertheless, this concept, together with Henderson’s acknowledgement of the role of the family and of other professionals is to be welcomed. Orem’s model also belongs to this group in so far as it sees nursing intervention as required to increase self-care abilities (skills and knowledge) to match demands on them, thereby promoting independence. Unfortunate- ly though, Orem’s view of patients as moti- vated to achieve self-care does not apply to all
mentally handicapped people.
The concept of nursing needs as arising from dependency/disability/deficits in functional abilities is applicable to a wider range of mental handicap than the concept of distur- bance in equilibrium. Also, emphasis on daily living activities, negotiation, the role of the family and of other professionals all form part of mental handicap nursing practice and must therefore be encompassed within the concep- tual framework.
Application of these concepts in nursing
In the absence of data about how mental handi- cap nurses in different areas of the specialty spend their time, this issue must remain a speculation. However, to an outsider it is apparent that there are several very important areas which the models so far referred to - and admittedly there are others - say very little or nothing about. Such areas include managerial responsi- bilities, active concern over physical, social and institutional aspects of the environment, working in the community and with families, liaison with other disciplines and agencies, nurse education and professional development. All these are very important areas which should figure prominently in any conceptual framework which is to be of use to mental handicap nurses.
It should be noted, however, that there will be certain difficulties in including the afore- mentioned areas in a conceptual framework. Firstly, managerial responsibilities: it would seem a truism that the more senior the nurse the greater the managerial responsibility. Yet
this needs qualification: a community mental handicap nurse working at charge nurse/sister level may well have fewer managerial responsi- bilities than his/her equivalent working in a hospital. Also, in certain districts some nurses may have managerial responsibility for non- nursing staff. It will never be possible to repres- ent all the variations on this theme in our framework. However, some indication that they exist should be present.
Secondly, active concern over all aspects of the environment should be considered. Again, how far this does and should figure in the work of a mental handicap nurse may depend on both where he/she is working and on the nurse’s seniority. Whilst there is scope for one interpretation of this approach in the commun- ity, thanks to the problems of institutionalis- ation in hospitals, there is probably greater scope for a rather different interpretation of this approach in hospitals.
The third difficulty is working with families and in the community. While many hospital mental handicap nurses will be involved with

12 NURSE EDUCATION TODAY
the families of their residents, community men-
tal handicap nurses will have a far greater
involvement. Fourthly, liaison with other disci-
plines and agencies. This issue receives little
attention in most nursing models, as one reason
for them is to develop independence from other
disciplines (especially medicine). However -
and this applies particularly to community
mental handicap nurses - nowadays in many
districts, links across disciplines may approach
the importance of links within disciplines. This
statement is made with special reference to
Community Mental Handicap Teams. Fifthly,
nurse education and professional development.
Implementation of the new ENB syllabus for
mental handicap nurses, together with imple-
mentation of the new assessment procedures
and the new requirements for continuing post-
graduate training, is associated with an in-
crease in time spent by many mental handicap
nurses on education and professional develop-
ments. However, again, this will vary accord-
ing to the seniority of the nurse and the
involvement of his/her unit in nurse education.
Although current nursing models have some
relevance to mental handicap nursing, there
are many areas of contemporary practice
which are not adequately represented.
Integration of discussion into a new conceptual framework
Before discussing the new conceptual frame-
work in terms of the key aspects of patient
care, which according to Aggleton and Chal-
mers (1986) all models should cover, certain
features will be noted and presented in dia-
gram. The diagrams will be cumulative in
order to make it easier to understand the final
complex diagram.
The framework has a dual centre represent-
ing the dual minimum requirements of a de-
pendent person and a nurse. The arrows in
both directions indicate mutual influence. The
modes of influence by the nurse are six-fold.
(i) physical care
(ii) psycho-social care
(iii) skill development
(iv) (v)
(4
activities of daily living
removal of constraints/provision of ap-
propriate environment
reduction in undesirable behaviours
This is represented in Figure 1.
The listing does not imply rank order since,
as always, the nurse must use clinical judge-
ment in determining priorities. It should be
noted that all these modes of influence may
potentially be negotiated, though the degree to
which this is possible will vary.
The dependent person and the family are
subject to mutual influence if the link exists.
This also applies to the link between the nurse
and the family. Figure 2 represents this situa-
tion. How the diagram accounts for cases where
the link does not exist is explained at the end
of this section.
The modes of influence between the nurse
and the family are not written in on the
diagram in view of the dual centre nature of
this framework. This is in contrast to triadic
frameworks which regard the f%miIy as a client
itself, thereby postulating three centres, the
nurse, the dependent person and the family.
However, it is the author’s view that in mental
handicap nursing, unlike health visiting for
example, the link between the nurse and the
family does not exist unless there is a depend-
ent person. Modes of influence between the
nurse and the family, while important, are not
therefore represented on this diagram. They
are summarised below:
(i) support and counselling
(ii) information
(iii) skill development, in any or all of the
areas by which the nurse interacts with
the dependent person
The place of other disciplines and agencies in
this framework is pivotal. In the first place,
both in the community and in hospitals, they
are linked directly with nurses. Secondly, they
are, or may be, linked directly with families.
This also applies in the community and in
hospitals. Thirdly, other disciplines and ag-
encies will be linked directly with the depend-
ent person. And fourthly, with regard to the

EDUCATION 'I'ODAY 13
Nurse
Fig 1 Modes of nursing influence
managerial aspects of this framework, other
disciplines and agencies may manage nurses,
but equally nurses may manage other disci-
plines and agencies. Thus it is not uncommon
to find professional mental handicap nurses
working in hostels run by social services. Again,
though it is less common, professional mental
handicap nurses may have responsibility for
other disciplines as unit managers. So far then,
the conceptual framework looks like Figure 3.
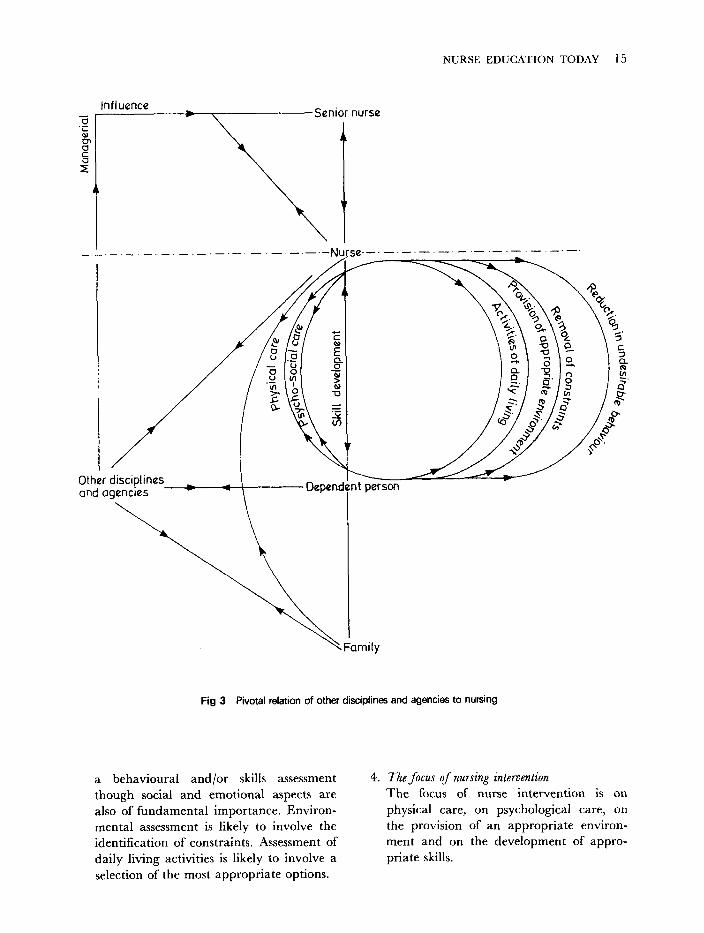
It should be noted that the area above the
line in dots like this -‘-.-.- is for the
representation of managerial and non-clinical
activities such as education and training. With
regard to the managerial links, these may or
may not be routed through a senior nurse.
Finally, it is necessary to incorporate the
training activities that the professional nurse
carries out. These have been placed above the
line as they are not clinical in the sense of
relating directly to the dependent person, but
involve links with other nurses. In the main
these will be student nurses, but they might be
qualified nurses undergoing further training,
such as a course of community mental handi-
cap nursing. This brings us to our final dia-
gram, Figure 4.
Advantage of framework
It can be seen that the conceptual frame-
work can allow for variations in district
practice, managerial responsibility, seniority,
area of work (hospital or community) as well
as variations in individual orientation and pre-
ference. This is the case if, except for the nurse
and the dependent person, the reference point
and their lines of influence, are seen as of
variable rather than of fixed salience. Thus
where, for example, a nurse has little or no link
with the family the line joining them can be
thought of as small, faded, or non-existent.
In the author’s view this built-in flexibility
constitutes a major advantage over the rigidity
of models and blueprints in so far as it
provides for the individual nurse adapting the
conceptual framework to his or her own circumstances.

14 NURSE EDUCATION TODAY
Nurse
Dependent person
Fig 2 Family links with modes of nursing influence
Application of the conceptual framework to key aspects of patient care
2.
It remains to be seen how this conceptual
framework applies to key aspects of patient care. These have been delineated by Aggleton and Chalmers ( 1985)
3.
1. The nature of the person receiving nursing care
The person is stated to be mentally handi- capped and dependent.
The cause of problems which are likely to
require intervention
These are likely to be physical, psycholog- ical or environmental in cause.
The nature of the assessment process
Where physical care is required, the nature and care of the physical depen- dency should be assessed. As far as psychological aspects of care are concerned. assessment is likely to take the form of
NURSE EDUCATION TODAY 15
Influence Senior nurse
I
I -.-.
Other disciplines _ and agencies
Depend nt person
1 Family
Fig 3 Pivotal relation of other disciplines and agencies to nursing
a behavioural and/or skills assessment though social and emotional aspects are also of fundamental importance. Environ- mental assessment is likely to involve the identification of constraints. Assessment of daily living activities is likely to involve a selection of the most appropriate options.
4.. The focus of nursing intervention
The focus of nurse intervention is on physical care, on psychological care, on the provision of an appropriate environ- ment and on the development of appro- priate skills.

16 NURSE EDUCAI’ION TODAY
Influence
3 :,
!
li
Senior nurse
A
\
Nurses I mainly students)
lrse._.-._._._.-._.-._.-.-._ .-._
nl t person
’ Family
Fig 4 The full conceptual framework
CONCLUSlONS of contemporary practice in mental handicap
nursing in the UK today will be deemed
While the verdict on the value and usefulness worthwhile. In any case, it is hoped that it has
of a conceptual framework is not for the author been shown that the working method can be
to give, it is hoped that this attempt to develop productive. It is potentially applicable to all
a framework that covers the multifaceted range areas of nursing.

NURSE EDUCATION TODAY 17
References
Aggleton P, Chalmers H 1984a Models and theories: defining the terms. Nursing Times 80 (36): 24-28
Aggleton P, Chalmers H 1984b Models and theories 2: the Roy adaptation model. Nursing Times 80 (40): 45-48
Aggleton P, Chalmers H 1984c Models and theories 3: the Riehl interaction model. Nursing Times 80 (45): 58-61
Aggleton P, Chalmers H 1984d Models and theories 4: Rogers’ unitary field model. Nursing Times 80 (50): 35- 39
Aggleton P, Chalmers H 1984e Models and theories 5: Oran’s self-care model. Nursing Times 81 (I): 36-39
Aggleton P, Chalmers H 1985a Models and theories 6: Roper’s activities of living model. Nursing Times 81 (7): 59-61
Aggfeton F’, Chalmers H 1985b Models and theories 7: Henderson’s model. Nursing Times 81 (10): 33-35
Aggleton P, Chalmers H 1985c Models and theories 8: Critical examination. Nursing Times 81 (14): 38-39
Aggleton P, Chalmers H 1986 Nursing models and the nursing process. Macmillan, London
Green C H 1985 An overview of the value of nursing models in relation to education. Nurse Education Today 5: 267-271
Heath J 1986 More on models: Feedback 1: l--2