The current role of photodynamic therapy in oesophageal dysplasia and cancer
9
Photodiagnosis and Photodynamic Therapy (2007) 4, 151—159 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/pdpdt CLINICAL REVIEW The current role of photodynamic therapy in oesophageal dysplasia and cancer Joanna Gray, Grant Fullarton MD, FRCS ∗ Department of Gastrointestinal Surgery, Gartnavel General Hospital, 1053 Great Western Road, Glasgow G12 0YN, UK Available online 16 July 2007 KEYWORDS Photodynamic therapy; Oesophageal cancer; High grade dysplasia; Barrett’s epithelium Summary Over the last 15 years photodynamic therapy (PDT) has become a viable treat- ment for pre-malignant and malignant disease of the oesophagus. Its initial use was in the palliation of oesophageal malignant obstruction bringing improved swallowing hence increas- ing nutritional intake and improving general quality of life. As the therapeutic boundaries of PDT have stretched, current studies look at the role of PDT in the treatment of pre-malignant dysplastic Barrett’s epithelium and early malignancy as a curative mucosal ablative technique. As a curative treatment in early oesophageal cancer, PDT provides an alternative treatment to oesophagectomy for those more elderly or less medically fit patients. This paper reviews the uses of photodynamic therapy in oesophageal cancer with reference to the available publications on its use in the palliation of oesophageal cancer and treatment of early cancer and high grade dysplasia in Barrett’s mucosa. © 2007 Elsevier B.V. All rights reserved. Contents Introduction.............................................................................................................. 152 Photosensitizers .......................................................................................................... 152 Light dosimetry .......................................................................................................... 152 Safety .................................................................................................................... 153 Oesophageal cancer—–incidence and epidemiology ....................................................................... 153 Barrett’s epithelium...................................................................................................... 153 PDT in high grade dysplasia (HGD) in Barrett’s and early oesophageal carcinoma ......................................... 153 High grade dysplasia ..................................................................................................... 154 Early oesophageal cancer ................................................................................................ 155 Palliation of advanced oesophageal carcinoma ........................................................................... 156 Future directions for PDT ................................................................................................ 157 Conclusion ............................................................................................................... 157 References ............................................................................................................. 157 ∗ Corresponding author. E-mail addresses: [email protected] (J. Gray), [email protected] (G. Fullarton). 1572-1000/$ — see front matter © 2007 Elsevier B.V. All rights reserved. doi:10.1016/j.pdpdt.2007.04.003
-
Upload
joanna-gray -
Category
Documents
-
view
217 -
download
1
Transcript of The current role of photodynamic therapy in oesophageal dysplasia and cancer

P
C
To
J
DA
C
1d
hotodiagnosis and Photodynamic Therapy (2007) 4, 151—159
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate /pdpdt
LINICAL REVIEW
he current role of photodynamic therapy inesophageal dysplasia and cancer
oanna Gray, Grant Fullarton MD, FRCS ∗
epartment of Gastrointestinal Surgery, Gartnavel General Hospital, 1053 Great Western Road, Glasgow G12 0YN, UKvailable online 16 July 2007
KEYWORDSPhotodynamictherapy;Oesophageal cancer;High grade dysplasia;Barrett’s epithelium
Summary Over the last 15 years photodynamic therapy (PDT) has become a viable treat-ment for pre-malignant and malignant disease of the oesophagus. Its initial use was in thepalliation of oesophageal malignant obstruction bringing improved swallowing hence increas-ing nutritional intake and improving general quality of life. As the therapeutic boundaries ofPDT have stretched, current studies look at the role of PDT in the treatment of pre-malignantdysplastic Barrett’s epithelium and early malignancy as a curative mucosal ablative technique.As a curative treatment in early oesophageal cancer, PDT provides an alternative treatment tooesophagectomy for those more elderly or less medically fit patients.
This paper reviews the uses of photodynamic therapy in oesophageal cancer with referenceto the available publications on its use in the palliation of oesophageal cancer and treatmentof early cancer and high grade dysplasia in Barrett’s mucosa.© 2007 Elsevier B.V. All rights reserved.
ontents
Introduction.............................................................................................................. 152Photosensitizers.......................................................................................................... 152Light dosimetry .......................................................................................................... 152Safety.................................................................................................................... 153Oesophageal cancer—–incidence and epidemiology ....................................................................... 153Barrett’s epithelium...................................................................................................... 153PDT in high grade dysplasia (HGD) in Barrett’s and early oesophageal carcinoma......................................... 153High grade dysplasia ..................................................................................................... 154Early oesophageal cancer ................................................................................................ 155
Palliation of advanced oesophageal carcinoma ........................................................................... 156Future directions for PDT ................................................................................................ 157Conclusion ............................................................................................................... 157References ............................................................................................................. 157
∗ Corresponding author.E-mail addresses: [email protected] (J. Gray), [email protected] (G. Fullarton).
572-1000/$ — see front matter © 2007 Elsevier B.V. All rights reserved.oi:10.1016/j.pdpdt.2007.04.003

1
I
Pteiioeibiddi
cItattwodtipttmott(o
wntdTphTat
obr[twUtTlmDreaVtccta
P
TcatBegt
L
Ttbpli
52
ntroduction
hotodynamic therapy (PDT) has become an establishedreatment modality over the last 15 years for use in sev-ral different malignant and pre-malignant conditions whichncludes oesophageal, skin, lung, bladder, head and neck andnvasive intracranial tumours. It involves the administrationf a photosensitizing agent which is then activated using anxternal light source in the presence of oxygen. PDT was firstntroduced as a palliative treatment for oesophageal cancerut its role has now been extended as a first line treatmentn patients with early cancer of the oesophagus or high gradeysplasia within a Barrett’s segment not fit enough for stan-ard treatments. We present here an overview of PDT’s rolen the treatment of oesophageal cancer.
PDT has been used in the treatment of oesophageal can-er for the last 10 years as a non-thermal ablative technique.t requires three main non-toxic components: a photosensi-izer, light and oxygen. It is a two stage process whereby
chemical photosensitizer given systemically may selec-ively concentrate in the target tissue. It has been shownhat systemically injected porphyrin (haematoporphyrin)hen activated by red light causes complete eradicationf transplanted experimental tumours [1]. This study alsoemonstrated the preferential accumulation of the pho-osensitizer in malignant tissue [1]. The sensitized tissues then illuminated at a wavelength that will activate thearticular photosensitizer. After activation the photosensi-izer is elevated from ground state to a long lasting excitedriplet state. This excited molecule can then react with cellembranes to form radical ions which interact further with
xygen to produce cytotoxic oxygenated molecules. Alterna-ively the excited molecule can transfer the energy directlyo an oxygen molecule to generate a reactive oxygen speciesROS) which is also highly cytotoxic. Both these reactionsccur simultaneously.
The photosensitizer accumulates in the mitochondriahere it is synthesized [2] more so in tumour cells thanormal tissue at a ratio of 2:1. This most likely due to theumour tissue’s high vascular permeability, lack of lymphrainage and greater affinity for proliferating endothelium.he photosensitizer aggregates are relatively large and so
revents rapid clearance from tumour interstitial fluid andence uptake in lipophylic components of the cell [3].umour destruction then occurs by direct killing by ROSnd damage to tumour vasculature hence tumour infarc-ion. Studies have also suggested that there is activationoc3rp
Table 1 Photosensitizers
Route ofadministration
Dose(mg/kg)
Porfirmer sodium (Photofrin,Axcan, UK)
IV 2
m-Tetrahydroxyphenylchlorin(mTHPC) (Foscan, BiolitecPharma, Ireland)
IV 0.15
5 Aminolevulinic acid (5ALA)(Medac, Germany)
PO [13] 60
J. Gray, G. Fullarton
f an immune response against tumour cells. This may bey the photosensitizer aggregates causing phagocytosis byeticuloendothelial cells [3]. One study by Gollnick et al.4] examined the immunogenicity of PDT-generated murineumour cell lysates in a preclinical vaccine model comparedith other modes of creating whole tumour vaccines such asV or ionizing radiation. This showed PDT to be more effec-ive, tumour specific and appeared to induce a cytotoxic-cell response. Both the UV and PDT generated tumour cellysates were able to induce phenotypic dendritic cell (DC)aturation, only the PDT generated lysates could activateCs to express IL-12 which is critical to cellular immuneesponse development. This shows that the direct tumourffects of PDT play an important role in enhancing the hostntitumour immune response. A further literature review byan Duijnhoven et al. [5] also concludes that PDT destroyshe structure of the tumour thereby enabling the immuneells in the tumour stroma (that are separated from tumourells by extracellular matrix and cellular membrane struc-ures) to directly interact with the tumour cells resulting insystemic anti-tumour immune response.
hotosensitizers
he photosensitizers that have been used in oesophagealancer are porfimer sodium (Photofrin, Axcan UK),
second generation synthetic photosensitizer meta-etrahydroxyphenylchlorine (mTHPC) (Temoporfin, Foscan,iolitec Pharma, Ireland) and 5 aminolevulinic acid (5ALA) inarly oesophageal cancer [6]. Photofrin and Foscan are bothiven intravenously and 5ALA is given orally. We summariseheir properties and safety profile in Table 1.
ight dosimetry
he light dosimetry required to try to produce adequateumour necrosis with minimal normal tissue damage haseen assessed in previous studies. Hier et al. [16] in 1995erformed a preliminary trial using various doses of 630 nmight on 10 of 32 patients in a randomised trial compar-ng PDT and Nd:YAG for palliative treatment for malignant
bstruction using photofrin. This showed light dosimetryorrelated with depth of tumour necrosis (p < 0.001) with00 J/cm being recommended as the optimal light doseequired for effective and safe range of tumour necrosis foralliation of oesophageal carcinomas.Time to peakconcentration (h)
Lightactivation
Depth ofnecrosis (mm)
48 [7,8] Red 630 nm 6—7 [9]
96 Red 652 nm,Green 514 nm[12]
5—10 [10,11]
6—8 Red 635 nm 2 [14,15]

UiatTcomcip[wmo
B
Bctntasmn(
paodanttotp
rcsa
P
Photodynamic therapy in oesophageal dysplasia and cancer
Ten years later PDT is now being used for early cancerand ablation of high grade dysplasia in Barrett’s epithe-lium [17]. This requires a lesser depth of necrosis otherwisethere is high incidence of stricture formation. Panjeh-pour et al. [18] carried out a non randomised unblendeddose de-escalation study in consecutive patients to deter-mine the lowest dose effective for HGD/T1 cancer ablationwhile reducing stricture incidence. This confirmed thatthe incidence of post-procedure stricture formation wasrelated to the light dose delivered. At 115 J/cm 15.3% ofpatients developed severe strictures (where more than 6dilatations were required) and 17% of patients had resid-ual HGD/T1 disease. At 85 J/cm 5.6% patients had severestrictures but 31.6% patients had residual HGD/T1 disease.This showed that decreasing light dose reduces strictureformation but it also increases the risk of residual dis-ease. The UK clinical PDT study group recommend a totallight dose of 200 J/cm [19]. Clearly further studies arerequired to define the optimum laser light dosimetry fortreatment of both pre-malignant and malignant lesions. Ourunit policy for the treatment of HGD or treatment of earlyT1 tumours with Photofrin involves a light dosimetry of100 J/cm with 300 J/cm for the palliation of oesophagealcarcinoma.
Although photosensitizers are currently activated bylasers it may be possible to achieve this simply by whitelight illumination from the endoscope alone. This would sig-nificantly increase the applicability and cost effectivenessof the treatment and studies are currently assessing thisfurther [20].
Safety
Although PDT is a safe procedure, both early and late compli-cations may be encountered. The early complications afterPDT relate to local effects of tumour necrosis and effecton surrounding non-diseased tissues. Common complicationsimmediately post-procedure can be substernal chest painand odynophagia (in approx. 10% due to oesophagitis [21]),dysphagia due to oedema, fever, leukocytosis, pleural effu-sions (3% [22]) and sometimes pneumonia (1% [23]). Patientsmay also develop cardiovascular complications such as atrialfibrillation and congestive cardiac failure. Late complica-tions relate mainly to photocutaneous reactions, strictureformation and late severe complications such as fistula orperforation. The incidence of this is summarised in Table 2.
Oesophageal cancer—–incidence and
epidemiologyThe incidence of oesophageal cancer, particularly adenocar-cinoma, has been on the increase in the last 30 years in the
a
Ct–
Table 2 Safety of PDT
Photosensitization reactions Stricture/sten
Porfirmer sodium 6—19% [22,25] 2—50% [17,22,mTHPC 8—10% [26] 5—8% [12,26]5ALA 0 [26,27] 0 [26,27]
153
K. Scotland has the highest incidence of adenocarcinoman men in the world [28]. During the period 1971—1998 thege-standardised incidence rates for oesophageal cancer inhe UK rose by 70% for males and 35% for females [29].here are approximately 7500 new cases of oesophagealancer diagnosed each year in the UK, with a M:F ratiof 5:3 [30]. Worldwide it is the eighth commonest form ofalignancy [31] although this increases to being the fourth
ommonest in developing countries [32]. Generally patientsn the UK (and Northern Europe) are elderly [33] with aoor prognosis with average 5-year survival of less than 10%33]. Only one in three patients progress to surgery [34],ith a 5-year survival in operated patients of 10—25% [30]eaning palliation is frequently the only form of treatment
n offer.
arrett’s epithelium
arrett’s epithelium of the oesophagus is a pre-malignantondition in which the stratified squamous epithelium ofhe lower oesophagus is replaced with intestinal-like colum-ar epithelium. Barrett’s is accepted to be primarily relatedo chronic gastroesophageal reflux disease although theetiology is multifactorial. In certain cases for unknown rea-ons Barrett’s epithelium may progress sequentially throughetaplasia, low and high grade dysplasia to adenocarci-
oma. The risk of progression to cancer is similar for short<3 cm) and long (>3 cm) segments [35].
Approximately 1 in 150 of patient’s with Barrett’s meta-lasia will develop a cancer [36] (although conversion ratesre likely to be higher in areas with the highest incidencef adenocarcinoma). The rate of progression from low gradeysplasia to neoplasia is between 10% and 28% [37] wheres the rate of progression from high grade dysplasia toeoplasia has been quoted between 14% and 80% [37]. Fur-hermore when surgical resections for HGD are examined byhe pathologist invasive carcinoma is actually found in 30%f the specimens [38]. This data would therefore suggesthat the target group should be those with HGD to preventrogression to carcinoma.
PDT has been used to treat high grade dysplasia in Bar-ett’s epithelium, and both early and advanced oesophagealarcinomas. With an increase in Barrett’s epithelium andubsequent oesophageal adenocarcinoma then there is alson increase in the target population suitable for PDT.
DT in high grade dysplasia (HGD) in Barrett’s
nd early oesophageal carcinomaurrently oesophagogastrectomy is the gold standardreatment for HGD and early oesophageal malignancy—carcinoma in situ or T1/T2 invasive carcinoma of the
osis requiring dilatation Perforation Fistula formation
24] 1—2% [22,25] 2% [23]5% 10.5% [12]0 [14,26,27] 0%

1
ori(gittccviooiiadbmtee(otitmoOc[
ialaoitttPdtl5sBmatpm(pldgPi
H
EbpeH53amw3wptta[mrbwBcaPcttds5zwo(aPicon(e
lsSneoephm4
54
esophagus. Survival rates with surgery have improved withecent studies quoting >50% 5-year survival rate [39]. Thiss for a number of reasons: the type of tumour is changingadenocarcinoma more than squamous, in distal oesopha-us which is more likely to be completely resected) ands often picked up earlier on Barrett’s surveillance; bet-er patient selection with improved imaging techniques andhe use of neoadjuvent therapies [39]. Surgery, however,an be associated with substantial morbidity (pulmonaryomplications 25%, anastomotic leaks 10—15% [34], cardio-ascular complications 11% [40,41]) and mortality 5—8.8%n large centres in the UK, below the national averagef 10% [40]. Some long-term outcomes of patients havingesophagectomy for HGD shows that although no mortal-ty 29% did have complications [42]. Quality of life scoresn this study were also equal to those of healthy individu-ls however post-operative morbidity included reflux 59%,ysphagia 28% and diarrhoea 55% [42]. It may thereforee suggested that oesophagectomy is not suitable in theore elderly, frail patient or those with significant mul-
iple medical co-morbidity. Oesophagectomy for HGD orarly cancer may also be considered by some, to be anxtremely invasive treatment for what is mucosal diseasethe author does however; recognise that approximately 40%f oesophagectomy specimens removed for HGD do con-ain occult adenocarcinoma [43]). This means a minimallynvasive treatment alternative for HGD and early cancer isherefore clearly needed. PDT is a mucosal ablative treat-ent for such patients which can be used as a sole treatment
r in combination with endoscopic mucosal resection (EMR).ther mucosal ablative treatments include thermal photo-oagulation with standard laser or argon plasma coagulation44].
PDT has several advantages over surgery [45] in thatt is comparatively simple, non invasive, can be targetedccurately, can be used multiple times without the doseimitations of treatments such as radiotherapy and has rel-tively few side effects. Although PDT can occur on anutpatient basis we admit our patients for the admin-stration of the photosensitizer and for up to 2—3 dayshereafter. This in our experience often however relates tohe patient’s age and social circumstances with patients asertiary referrals often travelling long distances from home.DT is less technically challenging than EMR although no ran-omised trial exists comparing the two minimally invasiveechniques. Clinical experience with thermal techniques isimited. A randomised controlled trial in Sheffield [46] ofALA PDT versus argon plasma coagulation in 68 patientshowed them both to be effective for ablating non-dysplasticarrett’s oesophagus. Argon plasma coagulation appearingore effective with 33/34 (97%) patients having complete
blation of Barrett’s mucosa compared to 17/34 (50%) inhe PDT group. A further randomised trial [47] in Liver-ool compared endoscopic ablation of dysplastic Barrett’sucosa using photofrin PDT and argon plasma coagulation
APC). This showed them to be equally effective with allatients having a reduction in the length of Barrett’s epithe-
ium. There were 13 patients in each group and at 4 monthsysplasia eradication was 56% in the APC and 77% in the PDTroups, with follow up at 12 months showing APC 67% andDT 77%. Dysplasia eradication therefore appeared bettern the PDT group.am
uc
J. Gray, G. Fullarton
igh grade dysplasia
ndoscopic treatment of HGD with PDT has been shown toe both safe and effective [48]. The main adverse events arehotosensitivity reactions and stricture formation. Overholtt al. [49] reported long-term follow up of 65 patients withGD treated with Porfimer PDT. The mean follow up was0.65 months. 60/65 (94%) patients had elimination of HGD./65 (4.6%) developed subsquamous adenocarcinoma andfurther 4 (4.9%) developed subsquamous non-dysplasticetaplastic epithelium. The intention to treat success rateas 77.5% for those with HGD although the stricture rate was0%. Wolfsen et al. [50] looked retrospectively at patientsho had had porfimer PDT for HGD and early cancer. 34/48atients had HGD. Of these 19/34 (56%) had complete abla-ion after one treatment and those with residual diseasehen had argon plasma coagulation leading to 34/34 (100%)blation of Barrett’s in the HGD group. A retrospective study51] showed PDT to be effective in ablating HGD in theajority of cases with 80.9% patients having a complete
esponse while 9.5% had a partial response. There has onlyeen one randomised controlled trial [52,53] looking at PDTith porfimer sodium ablation of high-grade dysplasia inarrett’s epithelium in conjunction with acid suppressionompared to acid suppression alone. In this initial 2 year trialblation of HGD was achieved in 77% of patients receivingDT with porfimer sodium and omeprazole 20 mg twice dailyompared to 39% in the group receiving omeprazole 20 mgwice daily alone (p < 0.0001). The trial follow up was con-inued over 5 years to assess the long-term effect on cancerevelopment in HGD. Patients underwent surveillance endo-copies with 2 cm, four quadrant biopsies every 3 months. Atyears PDT was significantly more effective than omepra-
ole alone in preventing progression to cancer (p = 0.027)ith about twice the likelihood of cancer occurring withmeprazole alone (29%) compared to PDT and omeprazole15%). The excellent initial results of this trial maintainedt 2 years led to the regulatory approval of porfimer sodiumDT in Barrett’s HGD in Canada, USA, Japan and Europe. Thiss the first trial to demonstrate a decrease in oesophagealancer development with any therapeutic regime andffers great encouragement for the future. Photofrin hasow also been granted approval in the UK by NICENational Institute of Clinical Excellence) for use in Barrett’spithelium [48].
ALA has also been assessed in dysplastic Barrett’s epithe-ium. Several studies have shown ALA induced PDT to beafe and effective in the ablation of Barrett’s metaplasia.maller studies have assessed ALA treatment in HGD. Goss-er et al. [54] treated nine patients with HGD in Barrett’spithelium with 5ALA PDT. All nine patients had eradicationf the HGD with a mean follow up of 16.9 months. Pecht al. [55] reported their experience with ALA PDT in 35atients with Barrett’s HGD. Thiry-four out of 35 patientsad a complete response during a median follow up of 37onths. Barr et al. [56] used 5ALA along with omeprazole
0 mg daily in five patients with HGD in Barrett’s epithelium
nd achieved complete ablation and no recurrence by 26—44onths.mTHPC with green light activation at 514 nm has beensed in the ablation of HGD in 12 patients with completelearance of dysplastic tissue [13]. M THPC has also been

Photodynamic therapy in oesophageal dysplasia and cancer
PPsuoh[
tepPpaiPTnstin3rialiorts
peps
bwt1tgihOoui(sipstflow up of 13 months (6—46 months) all three patients were
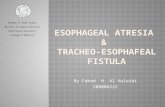
Figure 1 Neosquamous oesophageal epithelium.
used with red light activation to clear three of four patientswith HGD although two serious complications occurred dur-ing this study [12].
Whatever mucosal ablative technique is used in HGD it isimportant to remember that surveillance must continue asthe oesophagus re-epithelialises, however, as the destruc-tion may be incomplete [57] and remaining metaplasticareas may still have oncological potential. The major con-cern with PDT is it involves the potential for cancer cellsto develop beneath the neo-squamous epithelium (Fig. 1).There have been several reports of columnar epithelialremnants persisting beneath the new squamous epitheliumwhichever method of mucosal ablation of Barrett’s epithe-lium is used [58,59]. Van Laethem et al. [60] described acase report where intramucosal adenocarcinoma was foundin squamous re-epithelialisation of Barrett’s oesophagus thathad been ablated with argon plasma coagulation. The ade-nocarcinoma was found 18 months after complete squamousre-epithelialisation and presented as a bulging area cov-ered with squamous epithelium. Such an adenocarcinomamay have originated from residual metaplastic glands buriedunder the neo-squamous epithelium, although it is difficultto exclude a pre-existing tumour. The significance of such‘‘buried columnar glands’’ is yet to be determined there-fore continued surveillance of neo-squamous epithelium isadvised.
There is very little information in the literature lookingat the cost of PDT as a treatment of high grade dysplasiain Barrett’s epithelium. The only study assessing cost of PDTfor use in high grade dysplasia is by Hur et al. [61] comparingPDT, oesophagectomy and intensive endoscopic surveillancefor Barrett’s. This paper shows that there is increased lifeexpectancy and so PDT was cost effective when comparedto endoscopic surveillance and surgical oesophagectomy.
Early oesophageal cancer
Patients require appropriate staging to confirm the diag-nosis of intramucosal carcinoma (CIS or T1) with both alocal assessment by endoscopic ultrasound (EUS) and aCT chest/abdomen. EUS is more accurate in assessing theoesophageal wall in terms of depth and can give evidence of
any regional lymph node involvement giving a more accurateT and N stage [62].We have recently demonstrated the importance ofEUS in the selection of patients who will benefit from
wowd
155
DT for early cancer [17]. This study demonstrated thatDT with sodium porfimer could produce complete endo-copic and histological response in 9/9 patients withp to two treatment sessions at a median follow upf 30 months (range 2—56 months) in patients whoad EUS confirmed early oesophageal cancer (CIS or T1)17].
Sibille et al. [63] retrospectively studied 123 patientso assess the feasibility of PDT as curative treatment inarly oesophageal cancer. Eighty out of 88 patients hadre-operative EUS staging. They were staged as T1 or T2.DT was part of a multimodal therapeutic approach in 67atients, with radiotherapy applied in 58 cases 2 monthsfter PDT and combined chemotherapy and radiotherapyn 18 patients. Nine patients had chemotherapy alone withDT. At 6 months complete response was shown in 91% of the1 group and 78% of the T2 group although this was not sig-ificantly different. Recurrence was not described for thetaged sub groups such as T1, T2, PDT alone or PDT mul-imodal therapy groups but recurrence was more commonn adenocarcinoma (75%) compared to squamous cell carci-oma (28.5%). However overall local tumour recurrence was6% of all patients and patients with local recurrence didespond to repeat PDT. Sixteen were repeated due to initialncomplete response and 28 because of tumour recurrencefter initial complete response. Five-year survival was simi-ar in T1 and T2 groups being 33% and 36%, respectively. Thiss comparable to the overall survival rate in all 123 patientsf 25%. The disease specific survival rate was 74 ± 5%. Theelatively low survival rate reflected the poor clinical sta-us of the patients being treated, with most of them havingevere medical co-morbidities.
Overall current evidence suggests that PDT with sodiumorfimer can be a curative option in patients witharly oesophageal cancer being particularly useful inatients with significant co-morbidities which precludesurgery.
There have been a two small studies looking at the com-ination of EMR and PDT. In one study [64] 17 patientsith early adenocarcinoma in Barrett’s epithelium were
reated with EMR and PDT. Seven patients had T0 and0 had T1 disease. Four weeks after EMR, PDT was giveno all patients to remove any occult lesions. The mar-ins had involvement of cancer in three cases and EMRmproved staging in eight patients (47%). Sixteen patientsad no recurrence at a median follow up of 13 months.ne patient developed invasive carcinoma and had anesophagectomy but histology actually revealed no resid-al cancer. Complications included minor bleeding after EMRn one patient (6%), stricture formation in five patients30%), cutaneous phototoxicity in two patients (12%) andupraventricular tachycardia in one patient (6%). Othernteresting findings were eradication of Barrett’s in nineatients and in those with remaining Barrett’s no dyspla-ia was identified. A further retrospective study looked athree patients that had had EMR and PDT 6 weeks lateror early adenocarcinoma (T1N0M0) [65]. At a median fol-
ell, with no evidence of Barrett’s metaplasia, or dysplasian surveillance endoscopies. Post-procedure complicationsere limited to self limiting dysphagia and some chestiscomfort.

156 J. Gray, G. Fullarton
Palliation of advanced oesophageal carcinoma
PDT has become an accepted method of palliation in thepatients with advanced inoperable oesophageal cancer [66]along with other options including laser, argon-plasma coag-ulation, chemically induced tumour necrosis, self expandingstents, radiotherapy and chemotherapy. In addition PDT canbe used alone or in combination with any of the abovetechniques although combination treatment has not beensubject to careful clinical trials.
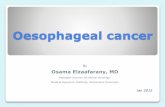
PDT is appropriate for patients with obstructive endo-luminal lesions (Fig. 2) particularly those in the upper(post-cricoid and cervical) oesophagus or in the lowerthird of the oesophagus crossing the gastro-oesophagealjunction, recurrence of tumour after surgical resection orchemoradiotherapy and for tumour overgrowth in stents.Tight fibrotic carcinomas and post-radiotherapy stricturingtumours are not suitable for PDT. Other contraindicationswould be patients with portal hypertension, porphyria orhypersensitivity to porphyrins, hepatic impairment, and theexistence of a tracheo-oesophageal fistula or bleeding fromthe oesophageal tumour [19].
Several uncontrolled trials have documented objec-tive and patient reported response rates of 60% or more[21,22,67]. Other trials comparing Nd:YAG laser to sodiumporfimer PDT have suggested that both methods requireapproximately two treatments to achieve adequate clini-cal response [25,68]. Lightdale [25] compared laser ablationwith sodium porfimer PDT in a multicentred randomisedstudy treating 218 patients. There was no significant dif-ference between the two in terms of dysphagia scores at1 month but PDT was the safer method resulting in fewerperforations and had the better objective tumour response.Hier et al. also published results of a phase 3 trial of sodiumporfimer PDT versus Nd:YAG laser [68] where 22 patientswere randomised to PDT and 20 to Nd:YAG. At 4 weeksPDT treated patients had significant improvement in theirdysphagia grade and performance status (p < 0.006). Theduration of response was also better in the PDT group butsurvival was similar at 145 days for PDT and 128 days forNd:YAG.
In our own unit we have also demonstrated sodiumporfimer PDT’s efficacy in the palliation of advancedoesophageal cancer [69]. In 30 of our patients treatedwith palliative intent for advanced oesophageal cancer withmetastatic disease and previously failed therapies dysphagiascores were measured before and after PDT. The dysphagiascore ranged from 4 to 1 with 4 being inability to swallow.
Figure 2 Endoscopic view of obstructing tumour pre- andpost-PDT.
F
Ts4
lssswiwsovsvPi
saatb53ficfapaepmlpeae5hTvaPaqt
igure 3 Effect of photofrin PDT on dysphagia score.
he median dysphagia score one month after treatment fellignificantly (p < 0.001) (Fig. 3) and the median survival wasmonths (range 1—34 months).It is interesting to compare these results with other pal-
iative methods. We previously assessed in a randomisedtudy of 50 patients the performance of plastic and metallictents in the palliation of oesophageal cancer [70]. Metallictent patients had a median survival of 107 days comparedith 62 days in the plastic stent group. Therefore in a sim-
lar cohort of patients, survival post-PDT appeared somehat improved. In our own last 25 patients treated with
odium porfimer PDT for palliation of oesophageal cancerur median survival is further improved at 197 days. This sur-ival benefit has also been noted after PDT at other tumourites such as cholangiocarcinoma [71]. This improved sur-ival rate may be due to better tumour ablation howeverDT may also induce a systemic effect with an improvedmmune response in these patients.
Another area of combination therapy which requirestudy is PDT and radiotherapy. PDT destroys local diseasend radiotherapy treats loco-regional disease. Sanfillippo etl. [72] retrospectively looked at the cases of three patients,wo oesophageal cancer patients were treated with com-ined chemotherapy and external beam radiation (55.8 and0.4 Gy) followed by intraluminal brachytherapy (12 and5 Gy at 1 cm). These patients then received sodium por-mer PDT for recurrence. A third patient with non-smallell cancer was treated with external beam radiation (60 Gy)ollowed by intraluminal brachytherapy (36.1 Gy at 1 cm)nd then received PDT for recurrence. One oesophagealatient developed a tracheoesophageal fistula requiringstent and the other developed quadriplegia due to an
pidural abscess arising from a fistula within the diseasedortion of the oesophagus. The lung cancer patient had aassive haemoptysis after the procedure and died 2 days
ater—–post-mortem showed necrotising arteritis of the rightulmonary artery. This suggests that patients with PDT andxternal beam radiation are more at risk of complicationslthough this may be related to the radiotherapy dose deliv-red. However a further study by Maier et al. [73] reviewing3 patients after endoluminal palliation, found 15 to havead PDT, brachyradiotherapy and external beam irradiation.he combined multimodal approach showed a median sur-ival of 16.8 months. The severe complication rate was 5.7%
nd mortality was1.9%. This study concluded that the use ofDT combined with irradiation was associated with accept-ble survival rate, low rates of complications and reasonableuality of life. The benefit of combination PDT and radio-herapy may relate to the ability of Photofrin to act as a
lr
art
C
Imlhoti
R
[
[
[
[
Photodynamic therapy in oesophageal dysplasia and cancer
radiosensitizing agent [73—75]. This is an exciting area andfurther studies are required to define the true efficacy andsafety of combined PDT and radiotherapy.
The cost of PDT has always been raised as a concern par-ticularly as the photosensitizer is expensive and specialisedlaser equipment is required. We have recently looked at thecost effectiveness of PDT compared with metallic stents ina retrospective study. This demonstrated that although theoverall cost of palliation of oesophageal cancer was moreexpensive with PDT compared to metallic stents, a pro-longed survival in the PDT group led to a slight cost benefitin terms of cost per day survival in the PDT group [76].
It is important to assess the effect of palliative thera-pies on the quality of life of patients. Prospective studiescomparing PDT with other palliative techniques shouldassess their impact on patient’s quality of life to deter-mine the optimal oesophageal cancer palliation. Currentevidence however suggests that PDT offers good palliationof oesophageal cancer compared to other techniques.
Future directions for PDT
PDT has become an established palliative treatment foradvanced oesophageal cancer and is safe, simple and effec-tive. It leads to an improvement in dysphagia scores, hasbeen shown to increase length of survival and has accept-able side effects for this group of patients with advanceddisease. Photofrin is the only photosensitizer which hasa licence for use in oesophageal disease both for thepalliation of oesophageal cancer and now for the treat-ment of high grade dysplasia in Barrett’s epithelium andearly oesophageal cancer. Safety and efficacy has beenshown for this using porfimer sodium (Photofrin) PDT [25]though continued surveillance is required and more thanone PDT course may need to be applied. Future randomisedstudies comparing PDT with other palliative techniqueswill establish its true place in oesophageal cancerpalliation.
There are several areas of PDT where developments couldlend to future benefit. Photosensitizers which could be takenorally with improved tumour localisation and increasedtumouricidal effects with minimal collateral tissue damagewould be desirable. Photosensitizers with an improved phar-macokinetic profile which would allow it to reach its peakconcentration in several hours but be excreted promptlywould also be an advantage. This in turn would meandecreased side effects such as photosensitivity and stric-ture occurrence. The use of combination photosensitizerswhich target tumour stroma and vascular elements as wellas cellular components may prove beneficial [77].
An improved laser delivery with better assessed lightdosimetry which would provide adequate depth of penetra-tion and tumour destruction in large tumours but superficialmucosal ablation without stricturing in HGD and early cancerwould be helpful. It may be that lasers will not be requiredat all and endoscopic white light activation may be ade-
quate. This would decrease the cost of PDT, improve itssafety profile and greatly increase the applicability of thistreatment.Better light delivery systems with improved laser fibreswith more targeted diffusers such as better balloons would
[
157
ocalise treatment and decrease damage to normal sur-ounding tissue.
The combination of PDT with other modalities suchs EMR (endomucosal resection), local chemotherapy andadiotherapy which may have an additive effect needs fur-her study.
onclusion
n the future PDT will become a more refined treat-ent modality as photosensitizers, light dosimetry and
ight delivery systems are modified. PDT will continue toave a definite clinical role in the palliation of advancedesophageal cancer and will establish its role further in thereatment of pre-malignant disease of the oesophagus andn early oesophageal carcinoma.
eferences
[1] Dougherty TJ. Activated dyes as anti-tumour agent. J Natl Can-cer 1974;52:1333—6.
[2] Barr H, Dix AJ, Kendall C, Stone N. Review article: the poten-tial role for photodynamic therapy in the management ofupper gastrointestinal disease. Aliment Pharmacol Therapeut2001;15:311—21.
[3] Dougherty TJ. Photosensitisation of malignant tumours. SemSurg Oncol 1986;2(1):24—37.
[4] Gollnick S, Vaughan L, Henderson B. Generation of effectiveantitumour vaccines using photodynamic therapy. Cancer Res2002;62:1604—8.
[5] Van Duijnhoven FH, Aalbers RI, Rovers JP, Terpstra OT, Kup-pen PJ. The immunological consequences of photodynamictreatment of cancer, a literature review. Immunobiology2003;207(2):105—13.
[6] Pech O, Gossner L, May A, et al. Long-term results of pho-todynamic therapy with 5 Aminolevulinic acid for superficialBarrett’s cancer and high grade intraepithelial neoplasia. Gas-trointest Endosc 2005;62(1):24—30.
[7] Bruce S. Photodynamic therapy: another option in cancer treat-ment. Clin J Oncol Nurs 2001 Number 3;5:95—9.
[8] Hahn SM, Putt ME, Metz J, et al. Photofrin uptake in the tumourand normal tissues of patients receiving intraperitoneal photo-dynamic therapy. Clin Cancer Res 2006;12(18):5464—70.
[9] Perry Y, Epperly MW, Fernando HC, et al. Photodynamic therapyinduced oesophageal stricture . . . an animal model: from mouseto pig. J Surg Res 2005;123(1):67—74.
10] Cramers P, Ruevekamp M, Oppelaar H, Dalesio O, Baas P, Stew-art FA. Foscan uptake and tissue distribution in relation tophotodynamic efficacy. Br J Cancer 2003;88(2):283—90.
11] Wagnieres G, Hadjur C, Grosjean P, et al. Clinical evaluationof the cutaneous phototoxicity of 5,10,15,20-tetra (m-hydroxyphenyl) chlorine. Photochem Photobiol 1998;68:382—7.
12] Lovat LB, Jamieson NF, Novelli MR, et al. Photodynamic ther-apy with m-tetrahydroxyphenylchlorin for high grade dysplasiaand early cancer in Barrett’s columnar lined oesophagus. Gas-trointest Endosc 2005;62(4):617—23.
13] Etienne J, Dorme N, Bourg-Heckly G, Raimbert P, Flejou JF,Flijou JF. Photodynamic therapy with green light and m-tetrahydroxyphenyl chlorine for intramucosal adenocarcinoma
and high grade dysplasia in Barrett’s oesophagus. GastrointestEndosc 2004;59(7):880—9.14] Barr H, Kendall C, Stone N. Photodynamic therapy foroesophageal cancer: a realistic option. Technol Cancer\ResTreat 2003;2(1):65—75.

1
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
58
15] Brown SG, Rogowska AZ. New photosensitizers for pho-todynamic therapy in gastroenterology. Canadian JournalGastroenterology 1999;13:389—92.
16] Heier SK, Rothman KA, Heier LM, Rosenthal WS. Photodynamictherapy for obstructing oesophageal cancer: light dosimetryand randomised comparison with Nd:YAG laser therapy. Gas-troenterology 1995;109(1):63—72.
17] Craig C, Macpherson M, Hodgson H, Gray J, Zammit M, Fullar-ton G. Photodynamic therapy is of benefit in treatment ofearly oesophageal carcinoma. Gastroenterology 2006;130(4):414.
18] Panjehpour M, Overhalt BF, Phan MN, Haydek JM. Optimisa-tion of light dosimetry for photodynamic therapy of Barrett’soesophagus: efficacy vs. incidence of stricture after treatment.Gastrointest Endosc 2005;61(1):13—8.
19] The UK Clinical PDT Study Group, Clinical guidelines forperforming photodynamic therapy (PDT) on patients with bron-chopulmonary or oesophageal cancer; 2002.
20] Mordon S, Maunoury V. Using white light during photodynamictherapy: visualization only or treatment? Eur J GastroenterolHepatol 2006;18(7):765—71.
21] Moghissi K, Dixon K, Hudson E, Stringer M. Photodynamic ther-apy of oesophageal cancer. Lasers Med Sci 1995;10:67—71.
22] Litle VR, Luketich JD, Christie NAET-AL>. Photodynamic ther-apy as palliation for oesophageal cancer: experience in 215patients. Ann Thorac Surg 2003;76:1687—92.
23] McCaughan Jr JS. Photodynamic therapy for obstructiveoesophageal malignancies. Diagn Theraput Endosc 1999;5:174.
24] Wolfsen HC, Hemminger LL, Wallace MB, Devault KR. Clini-cal experience of patients undergoing photodynamic therapyfor Barrett’s dysplasia or cancer. Aliment Pharmacol Theraput2004;20:1125—31.
25] Lightdale CJ, Heier SK, Marcon NE, et al. Photodynamic ther-apy with porfirmer sodium versus thermal ablation with NdYAG laser for palliation of oesophageal cancer; a multicentrerandomized trial. Gastrointest Endosc 1996;42:507—12.
26] Etienne J, Dorme N, Bourg-Heckly G, Raimbert P, Flijou J. Pho-todynamic therapy with green light and m-tetrahydroxyphenylchlorine for intramucosal adenocarcinoma and HGD in Barrett’soesophagus. Gastrointest Endosc 2004;59(7):880—9.
27] Gossner L, Stolte M, Sroka R, et al. Photodynamic ablation ofHGD and early cancer in Barrett’s oesophagus by means of 5aminolevulinic acid. Gastroenterology 1998;114(3):448—55.
28] Corley DA, Buffler PA. Oesophageal and gastric cardia ade-nocarcinomas: analysis of regional variation using the cancerincidence in five continents database. Int J Epidemiol2001;30:1415—25.
29] National Statistics. Cancer Atlas of the UK and Ireland1991—2000. Office for National Statistics (ONS); 2006.
30] Cancer Research UK. Information Resource Centre; 2004.Weblink http://info.cancerresearchuk.org.
31] Parkin DM, Bray F, Ferlay J, et al. Estimating the World cancerburden: globocan. Int J Cancer 2000;94:163—6.
32] Parkin DM, Pisani P, Ferlay J. Estimates of the worldwideIncidence of Eighteen major Cancers in 1985. Int J Cancer1993;54:594—606.
33] Phull PS, Salmon CA, Park KGM, Rapson T, Thompson AM, GilbertFJ. Age threshold for endoscopy and risk of missing uppergastrointestinal malignancy—–data from the Scottish Audit ofgastric and oesophageal cancer (SAGOC). Aliment PharmacolTheraput 2006;23(2):229—33.
34] Gilbert FJ, Park K, Thompson AM. Scottish Audit of Gastric andOesophageal Cancer Report 1997—2000. A prospective audit
2002. Scottish Audit of Gastric and Oesophageal Cancer Steer-ing Group, Edinburgh.35] Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segmentlength on risk for neoplastic preogression in patients with Bar-retts oeophaugus. Ann Intern Med 2000;132:612—20.
[
J. Gray, G. Fullarton
36] Van den Bogart, Van Hillergeersberg R, De Bruin RWF, TilanusH. Barrett’s oesophagus: pathophysiology, diagnosis and man-agement. Scand J Gastroenterol 1998;33:449—53.
37] Wolfsen HC. Present status of photodynamic therapy for highgrade dysplasia in Barrett’s oesophagus. J Clin Gastroenterol2005;39(3):189—202.
38] Tseng EE, Wu TT, Yeo CJ, et al. Barrett’s oesophagus withhigh grade dysplasia: surgical results and long term outcome:an update. J Gastrointest Surg 2003;7:164—70, discussion170—171.
39] Portale G, Hagen J, Peters J, et al. Modern 5-yearsurvival of resectable esophageal adenocarcinoma: singleinstitution experience with 263 patients. J Am Coll Surg2006;202(4):588—96.
40] Muller JM, Erasmi H, Stelzner M, Zieren U, PichlmaierH. Surgical therapy of oesophageal carcinoma. Br J Surg1990;77:845—57.
41] Rindani R, Martin CJ, Cox MR. Transhiatal versus Ivor Lewisoesophagectomy: is there a difference? Austr NZ J Surg1999;69:187—94.
42] Chang LC, Oelschlager BK, Quiroga E, et al. Long-term outcomeof esophagectomy for high-grade dysplasia or cancer foundduring surveillance for Barrett’s esophagus. J Gastroint Surg2006;10(3):341—6.
43] Heitmiller RF, Redmond M, Hamilton SR. Barrett’s esopha-gus with high-grade dysplasia. An indication for prophylacticesophagectomy. Ann Surg 1996;224(1):66—71.
44] Thomas T, Richards CJ, De Caestecker J, Robinson RJ. Highgrade dysplasia in Barrett’s oesophagus; natural history andreview of clinical practise. Aliment Pharmacol Theraput2005;21(6):747—55.
45] Brown SB, Walker EA. The present and future role ofphotodynamic therapy in cancer treatment. Lancet Oncol2004;5(8):497—508.
46] Kelty CJ, Ackroyd R, Brown NJ, Stephenson TJ, StoddartCJ, Reed MW. Endoscopic ablation of Barrett’s oesopha-gus: a randomized controlled trial of photodynamic ther-apy vs. argon plasma coagulation. Aliment Pharmacol2004;20(11—12):1289—96.
47] Ragunath K, Krasner N, Raman VS, Haqqani MT, PhillipsCJ, Cheung I. Endoscopic ablation of dysplastic Barrett’soesophagus comparing argon plasma coagulation and photo-dynamic therapy: a randomised prospective trial assessingefficacy and cost-effectiveness. Scand J Gastroenterol 2005July;40(7):750—8.
48] NICE Guidelines 2006. Interventional Procedure Programme.Interventional procedures overview of photodynamic therapyfor high grade dysplasia for Barrett’s oesophagus.
49] Overholt BF, Panjehpour M, Halberg DL. Photodynamic ther-apy for Barrett’s oesophagus with dysplasia and or earlystage carcinoma: long term results. Gastrointest Endosc2003;58(2):183—8.
50] Wolfsen HC, Woodward TA, Raimondo M. Photodynamic ther-apy for dysplastic Barrett’s oesophagus and early oesophagealadenocarcinoma. Mayo Clinic Proc 2002;77(11):1176—81.
51] Christophorus, Foroulis N, Thorpe AC. Photodynamic therapy(PDT) in Barrett’s oesophagus with dysplasia or early cancer.Eur J Cardio-Thorac Surg 2006;29(1):30—4.
52] Overholt BF, Lightdale CJ, Wang K, et al. International multi-centre partially blinded randomised study into the efficacy ofphotodynamic therapy (PDT) using Porfirmer sodium (POR) forthe ablation of high grade dysplasia (HGD) in Barrett’s oesoph-agus (BE):Results of a 24 month follow up. Gastroenterology
2003;124(Suppl 1). A20:151.53] Overholt B, Wang K, Burdick S, et al. A 5 year randomised phase3 trial of efficacy and safety of photodynamic therapy usingporirmer sodium in high grade dysplasia in Barrett’s esophagus.Gastroenterology 2006;130(4).

[
[
[
[
[
[
[
[
[
[
[
Photodynamic therapy in oesophageal dysplasia and cancer
[54] Gossner L, May A, Sroka R, Stolte M, Hahn EG, Ell C. Pho-todynamic destruction of high grade dysplasia and earlycarcinoma of the esophagus after the oral administration of5-aminolevulinic acid. Cancer 1999;86(10):1921—8.
[55] Pech O, Gossner L, May A, et al. Long-term results of pho-todynamic therapy with 5-aminolevulinic acid for superficialBarrett’s cancer and high-grade intraepithelial neoplasia. Gas-trointest Endosc Jul 2005;62(1):24—30.
[56] Barr H, Shepherd NA, Dix A, Roberts DJH, Tan WC, KrasnerN. Eradication of high-grade dysplasia in columnar-lined (Barrett’s) oesophagus by photodynamic therapywith endogenously generated protoporphyrin IX. Lancet1996;348(9027):584—5.
[57] Biddlestone LR, Barham CP, Wilkinson SP, et al. The histologyof treated Barrett’s oesophagus. Am J Pathol 1998;22:239—45.
[58] Barham CP, Jones RL, Biddlestone LR, Hardwick RH, BarrH. Photothermal laser ablation of Barrett’s oesophagus andhistological evidence of squamous re-epithelialisation. Gut1997;41(3):281—4.
[59] Van Laethem JL, Cremner M, Peny MO, et al. Complete erad-ication of Barrett’s mucosa with argon plasma coagulationand acid suppression: immediate and mid term results. Gut1998;43:747—52.
[60] Van Laethem JL, Peny MO, Salmon I, Cremer M, DeviereJ. Intramucosal adenocarcinoma arising under squa-mous re-epithelialisation of Barrett’s oesophagus. Gut2000;46(4):574—7.
[61] Hur C, Nishioka NS, Gazelle GS. Cost-effectiveness of photody-namic therapy for treatment of Barrett’s oesophagus with highgrade dysplasia. Dig Dis bSci 2003;48(7):1273—83.
[62] Zhang X, Watson DI, Lally C, Bessell JR. Endoscopic ultra-sound for pre-operative staging of oesophageal carcinoma. SurgEndosc 2005;19(12):1618—21.
[63] Sibille A, Lambert R, Souquet JC, Sabben G, Descos F. Long termsurvival after photodynamic therapy for oesophageal cancer.Gastroenterology 1995;108(2):337—44.
[64] Buttar NS, Wang KK, Lutzke LS, Krishnadath KK, Anderson MA.Combined endoscopic mucosal resection and photodynamictherapy for oesophageal neoplasia within Barrett’s oesophagus.
Gastrointest Endosc 2001;54(6):682—8.[65] Wolfsen HC, Hemminger LL, Raimomdo M, Woodward TA.Photodynamic therapy and endoscopic mucosal resection forBarrett’s dysplasia and early oesophageal adenocarcinoma.South Med J 2004;97(9):827—30.
[
159
66] Edler DG, Baron TH. Endoscopic palliation of malignant dys-phagia. Mayo Clinic Proc 2001;76(7):731—8.
67] Jin M, Yang B, Zhang W, Wang Y. Photodynamic therapy forupper gastrointestinal tumours over the past 10 years. SemSurg Oncol 1994;10:111—3.
68] Heier SK, Rothman KA, Heier LM, Rosenthal WS. Photodynamictherapy for obstructing oesophageal cancer: light dosimetryand randomized comparison with Nd:YAG laser therapy. Gas-troenterolgy 1995;109:63—73.
69] Fullarton GM. Photodynamic therapy for advanced oesophagealcarcinoma. In: Proceedings of the international congressand symposium (series 255) on photodynamic therapy—–applications in gastroenterology and pulmonology. 2004.
70] O’Donnell CA, Fullarton GM, Watt E, et al. Randomaised clini-cal trial comparing self expanding metallic stents with plasticendoprotheses in the palliation of oesophageal cancer. Br J Surg2002;89:985—92.
71] Zoepf T, Jakobs R, Arnold JC, Apel D, Rosenbaum A, RiemannJF. Photodynamic therapy for palliation of non-resectable bileduct cancer —Preliminary results with a new diode laser sys-tem. Am J Gastroenterol 2001;96(7):2093—7.
72] Sanfilippo NJ, His A, Denittis AS, et al. Toxicity of photody-namic therapy after combined external beam radiotherapy andintra-luminal brachytherapy for carcinoma of the upper aerodi-gestive tract. Lasers Surg Med 2001;28(3):278—81.
73] Maier A, Anegg U, Fell B, et al. Effect of photodynamic ther-apy in a multimodal approach for advanced carcinoma ofthe gastroesophageal junction. Lasers Surg Med 2000;26(5):461—6.
74] Schaffer M, Erti-Wagner, Schaffer PM, et al. The appli-cation of Photofrin 2 as a sensitising agent for ionizingradiation—–a new approach in tumour therapy. Curr Med Chem2005;12(10):1209—15.
75] Schaffer M, Erti-Wagner B, Schaffer PM, et al. Feasibilityof Photofrin 2 as a radiosensitizing agent in solid tumous—–preliminary results. Oncology 2006;29(11):514—9.
76] O’Donnell CA, Gray J, Hodgson H, MacPherson M, Zammit M,Fullarton G. A cost comparison of photodynamic therapy andmetallic stents in the palliation of oesophageal cancer. Photo-
dyn Therapy Photodiagn 2007;4(1):65—70.77] Peng Q, Warloe T, Moan J, et al. Antitumour effect of 5-aminolevulinic acid-mediated photodynamic therapy can beenhanced by the use of a low dose of Photofrin in human tumourxenografts. Cancer Res 2001;61(15):5824—32.