The Cultural Competence Education Resource Toolkit - Springer
88
The Cultural Competence Education Resource Toolkit This toolkit consists of three sets of tools and a total of 21 distinct tools. The three sets of tools are: Resources for Academic Settings; Resources for Health Care Institutions; and Resources for Professional Associations. Taken together, the tools provide a comprehensive set of materials for planning, implementing, and evaluating cultural competence education strategies and programs. These tools may be used alone or in conjunction with other tools and will be of use to a broad range of readers at all levels: nurses, educators, administrators, association leaders, managers, researchers, students, and other health care providers. The tools and this book will enable you to achieve optimal cultural competence. Fees for Use: Any use of the toolkit or portions of the toolkit beyond individual, personal use (such as within an institutional setting and/or in a research study) will require purchase of a license. See below. • Individual Personal use: This toolkit is available for review and individual personal use to all purchasers of the book, Teaching Cultural Competence in Nursing and Health Care, Second Edition, by Marianne R. Jeffreys, EdD, RN. • Educational use: $250 per year • All other uses (Corporate/Institutional/Government): $500 per year (one license per site) To Order the License: Select License type: ❑ Educational use: $250 1-year License ISBN 978-0-8261-1791-5 ❑ All other uses (Corporate/Institutional/Government): $500 1-year License (one license per site) ISBN 978-0-8261-1789-2 Payment may be made with credit card or check. Please complete this form and return either via fax or mail. Usage type: ❑ Educational ❑ Other (Corporate/Institutional/Government) Print Name_______________________________________________ Signature __________________________________________ Institution ____________________________________________________________________________________________________ Street Address: ______________________________________________________________________________________________ City_________________________________________________ State_____________ Country____________ Zip ______________ Fax this form to 212-941-7842. (If you have questions, please call us at 877-687-7476 or 212-431-4370.) or mail to: Attn: Customer Service Springer Publishing Company 11 W. 42nd St., 15th Fl. New York, NY 10036 ANCILLARY FILES FOR: Teaching Cultural Competence in Nursing and Health Care Second Edition Marianne R. Jeffreys, EdD, RN
Transcript of The Cultural Competence Education Resource Toolkit - Springer

The Cultural Competence Education Resource Toolkit
This toolkit consists of three sets of tools and a total of 21 distinct tools. The three sets of tools are: Resources forAcademic Settings; Resources for Health Care Institutions; and Resources for Professional Associations. Takentogether, the tools provide a comprehensive set of materials for planning, implementing, and evaluating culturalcompetence education strategies and programs. These tools may be used alone or in conjunction with other toolsand will be of use to a broad range of readers at all levels: nurses, educators, administrators, association leaders,managers, researchers, students, and other health care providers. The tools and this book will enable you toachieve optimal cultural competence.
Fees for Use:
Any use of the toolkit or portions of the toolkit beyond individual, personal use (such as within an institutional settingand/or in a research study) will require purchase of a license. See below.
• Individual Personal use: This toolkit is available for review and individual personal use to all purchasers of thebook, Teaching Cultural Competence in Nursing and Health Care, Second Edition, by Marianne R. Jeffreys, EdD, RN.
• Educational use: $250 per year
• All other uses (Corporate/Institutional/Government): $500 per year (one license per site)
To Order the License:
Select License type:
� Educational use: $250 1-year LicenseISBN 978-0-8261-1791-5
� All other uses (Corporate/Institutional/Government): $500 1-year License (one license per site)ISBN 978-0-8261-1789-2
Payment may be made with credit card or check. Please complete this form and return either via fax or mail.
Usage type: � Educational � Other (Corporate/Institutional/Government)
Print Name_______________________________________________ Signature __________________________________________
Institution ____________________________________________________________________________________________________
Street Address: ______________________________________________________________________________________________
City_________________________________________________ State_____________ Country____________ Zip ______________
Fax this form to 212-941-7842. (If you have questions, please call us at 877-687-7476 or 212-431-4370.)
or mail to: Attn: Customer ServiceSpringer Publishing Company11 W. 42nd St., 15th Fl.New York, NY 10036
ANCILLARY FILES FOR:
Teaching Cultural Competence in Nursing and Health CareSecond Edition
Marianne R. Jeffreys, EdD, RN

Cultural CompetenceEducation Resource
Toolkit
Marianne R. Jeffreys, EdD, RN
The
S A M
P L
EJeffreys, EdD,ffreys, E

Copyright C©
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying,recording, or otherwise, without the prior permission of Springer Publishing Company, LLC.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY 10036www.springerpub.com
Educational use ISBN 978-0-8261-1791-5All other uses (corporate/institutional/government) ISBN 978-0-8261-1789-2
The author and the publisher of this Work have made every effort to use sources believed to be reliable to provide information that is accurate and compatiblewith the standards generally accepted at the time of publication. Because medical science is continually advancing, our knowledge base continues to expand.Therefore, as new information becomes available, changes in procedures become necessary. We recommend that the reader always consult current research andspecific institutional policies before performing any clinical procedure. The author and publisher shall not be liable for any special, consequential, or exemplarydamages resulting, in whole or in part, from the readers’ use of, or reliance on, the information contained in this book. The publisher has no responsibility forthe persistence or accuracy of URLs for external or third-party Internet Web sites referred to in this publication and does not guarantee that any content on suchWeb sites is, or will remain, accurate or appropriate.
© Springer Publishing Company
201 Springer Publishing Company0
Eook.ook
S A M
P L
Eand does nand d

HOW TO USE THE TOOLKITWelcome to the Cultural Competence Education Resource Toolkit. Used in conjunction with Teaching Cultural Competencein Nursing and Health Care, 2nd Edition, the toolkit contains a wealth of hands-on, user-friendly resources that helps takenurses, educators, administrators, professional association leaders, managers, educators, students, and other healthcare providers from their own starting point toward the pinnacle—optimal cultural competence. Appropriate for alllevels and settings (academic, health care institutions, employee education, professional associations, and continuingeducation), the book and toolkit end the struggle to find ready-to-use materials for planning, implementing, andevaluating cultural competence education strategies and programs. Toolkit items correspond with the seven essentialsteps for optimal cultural competence development: (1) self-assessment; (2) active promotion; (3) systematic inquiry;(4) decisive action; (5) innovation; (6) measurement; and (7) evaluation.
Take the next step. Find your setting and discover the toolkit resources best for you:
Resources* for Academic Settings
Item # Item Name
1. Transcultural Self-Efficacy Tool (TSET)3. Cultural Competence Clinical Evaluation Tool—Student Version (CCCET-SV)4. Cultural Competence Clinical Evaluation Tool—Teacher Version (CCCET-TV)7. Clinical Setting Assessment Tool—Diversity and Disparity (CSAT-DD)8. Demographic Data Sheet—Undergraduate (DDS-U)9. Demographic Data Sheet—Nurses (DDS-N)
10. Self-Assessment Tool—Academic (SAT-A)13. Active Promoter Assessment Tool—Academic (APAT-A)15. Systematic Inquiry: Academic (SI-A)18. Personal Coding Cover Page for Anonymity and Matching Questionnaires19. Sample Permission Letter20. Cultural Competence Documentation Log21. Research Report Template
Resources* for Health Care Institutions
Item # Item Name
1. Transcultural Self-Efficacy Tool (TSET)2. Transcultural Self-Efficacy Tool-Multidisciplinary Health Provider (TSET-MHP)5. Cultural Competence Clinical Evaluation Tool—Employee Version (CCCET-EV)6. Cultural Competence Clinical Evaluation Tool—Agency Evaluator Version (CCCET-AEV)7. Clinical Setting Assessment Tool—Diversity and Disparity (CSAT-DD)9. Demographic Data Sheet—Nurses (DDS-N)
11. Self-Assessment Tool—Health Care Institutions (SAT-HCI)14. Active Promoter Assessment Tool—Health Care Institutions/Professional Associations (APAT-HCIPA)16. Systematic Inquiry: Health Care Institutions (SI-HCI)18. Personal Coding Cover Page for Anonymity and Matching Questionnaires19. Sample Permission Letter20. Cultural Competence Documentation Log21. Research Report Template
*Items may be used alone or in conjunction with other toolkit items for specified settings. See Teaching CulturalCompetence in Nursing and Health Care, 2nd Edition for more details.
© Springer Publishing Company
AM P
L EEersion (CCCET-SV)sion (CCCET-SV)
er Version (CCCET-TV)n (CCCET-TV)sparity (CSAT-DD)DD)
S-U)
demic (APAT-A)-A)
nonymity and Matchingnonymity an
entation Logn Logee
MP
MI
AS A
l Self-Efficacy Tool (TSEEfficacy Tool (Tural Self-Efficacy Tool-Mfficacy Tool-M
al Competence Clinical EClitural Competence Clinictural Competence Clin
Clinical Setting Assessminical Setting AssessmDemographic Data Shemographic Dat
f-Assessment To-AssessmentPromoterPromoter
tic In

Resources* for Professional Associations
Item # Item Name
1. Transcultural Self-Efficacy Tool (TSET)2. Transcultural Self-Efficacy Tool-Multidisciplinary Health Provider (TSET-MHP)5. Cultural Competence Clinical Evaluation Tool—Employee Version (CCCET-EV)6. Cultural Competence Clinical Evaluation Tool—Agency Evaluator Version (CCCET-AEV)9. Demographic Data Sheet—Nurses (DDS-N)
12. Self-Assessment Tool—Professional Associations (SAT-PA)14. Active Promoter Assessment Tool—Health Care Institutions/Professional Associations (APAT-HCIPA)17. Systematic Inquiry: Professional Associations (SI-PA)18. Personal Coding Cover Page for Anonymity and Matching Questionnaires19. Sample Permission Letter20. Cultural Competence Documentation Log21. Research Report Template
*Items may be used alone or in conjunction with other toolkit items for specified settings. See Teaching CulturalCompetence in Nursing and Health Care, 2nd Edition for more details.
TOOLKIT ITEMS OVERVIEW1. Transcultural Self-Efficacy Tool (TSET)
� An 83-item questionnaire designed to measure and evaluate learners’ confidence (transcultural self-efficacy)for performing general transcultural nursing skills among diverse client populations
� Consistently high estimates of validity and reliability for subscales and total� Requested by researchers worldwide in multiple health disciplines for use with students, nurses, and other
health professionals� May be used alone or in conjunction with other toolkit items� EASY SCORING: Self-Efficacy Strength (SEST) refers to the average strength of self-efficacy perceptions within
a particular dimension (subscale) of the construct. Calculate by totaling subscale item responses and dividingby the number of subscale items, resulting in the mean score. For example:
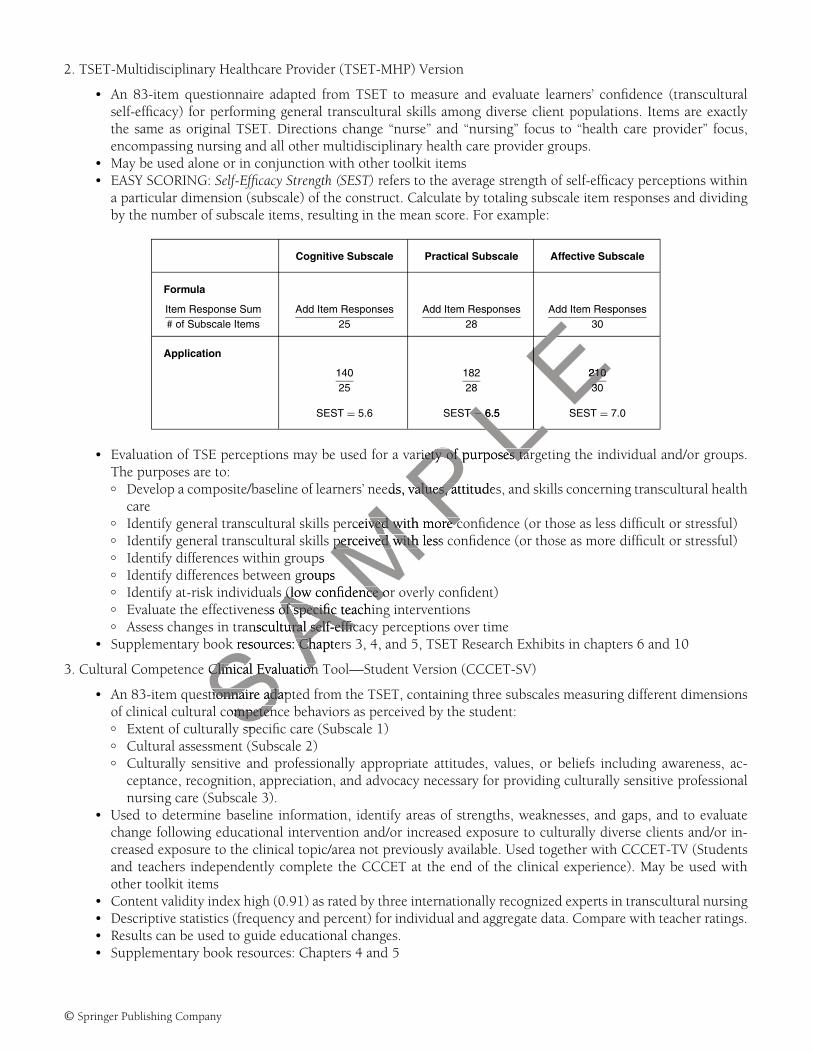
Cognitive Subscale Practical Subscale Affective Subscale
Formula
Item Response Sum# of Subscale Items
Add Item Responses25
Add Item Responses28
Add Item Responses30
Application14025
18228
21030
SEST = 5.6 SEST = 6.5 SEST = 7.0
� Evaluation of TSE perceptions may be used for a variety of purposes targeting the individual and/or groups.The purposes are to:� Develop a composite/baseline of learners’ needs, values, attitudes, and skills concerning transcultural nurs-
ing (or health care)� Identify general transcultural skills perceived with more confidence (or those as less difficult or stressful)� Identify general transcultural skills perceived with less confidence (or those as more difficult or stressful)� Identify differences within groups� Identify differences between groups� Identify at-risk individuals (low confidence or overly confident)� Evaluate the effectiveness of specific teaching interventions� Assess changes in transcultural self-efficacy perceptions over time
� Supplementary book resources: Chapters 3, 4, and 5, and TSET Research Exhibits in chapters 6 and 10.
© Springer Publishing Company
AM P
L E
ifiedified
ate learners’ confidenlearng diverse client popse client po
for subscales and tofor subscales and tohealth disciplines fohealth dis
ther toolkit itemsther toolkit itemEST)T) refers to the avrefers to the a
he construct. Calculahe construct. Cesulting in the meanulting in the mea
AM
SA
SA
S SCognitive SubscalCognitive Subsca
Anse Sum
SAscale Itemsscale Item
Add ItemAddAStionon
2. TSET-Multidisciplinary Healthcare Provider (TSET-MHP) Version
� An 83-item questionnaire adapted from TSET to measure and evaluate learners’ confidence (transculturalself-efficacy) for performing general transcultural skills among diverse client populations. Items are exactlythe same as original TSET. Directions change “nurse” and “nursing” focus to “health care provider” focus,encompassing nursing and all other multidisciplinary health care provider groups.
� May be used alone or in conjunction with other toolkit items� EASY SCORING: Self-Efficacy Strength (SEST) refers to the average strength of self-efficacy perceptions within
a particular dimension (subscale) of the construct. Calculate by totaling subscale item responses and dividingby the number of subscale items, resulting in the mean score. For example:
Cognitive Subscale Practical Subscale Affective Subscale
Formula
Item Response Sum# of Subscale Items
Add Item Responses25
Add Item Responses28
Add Item Responses30
Application
14025
18228
21030
SEST = 5.6 SEST = 6.5 SEST = 7.0
� Evaluation of TSE perceptions may be used for a variety of purposes targeting the individual and/or groups.The purposes are to:� Develop a composite/baseline of learners’ needs, values, attitudes, and skills concerning transcultural health
care� Identify general transcultural skills perceived with more confidence (or those as less difficult or stressful)� Identify general transcultural skills perceived with less confidence (or those as more difficult or stressful)� Identify differences within groups� Identify differences between groups� Identify at-risk individuals (low confidence or overly confident)� Evaluate the effectiveness of specific teaching interventions� Assess changes in transcultural self-efficacy perceptions over time
� Supplementary book resources: Chapters 3, 4, and 5, TSET Research Exhibits in chapters 6 and 10
3. Cultural Competence Clinical Evaluation Tool—Student Version (CCCET-SV)
� An 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensionsof clinical cultural competence behaviors as perceived by the student:� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, ac-
ceptance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professionalnursing care (Subscale 3).
� Used to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available. Used together with CCCET-TV (Studentsand teachers independently complete the CCCET at the end of the clinical experience). May be used withother toolkit items
� Content validity index high (0.91) as rated by three internationally recognized experts in transcultural nursing� Descriptive statistics (frequency and percent) for individual and aggregate data. Compare with teacher ratings.� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4 and 5
© Springer Publishing Company
PL EL EE210210E33
STT == 6.5 S6 L
AM P
riety of purposes tarriety of purposes tar
eds, values, attitudesvalues, a
rceived with more coved with more cperceived with lessperceived with
psgroups
s (low confidence or(low confidence oess of specific teachinof specific
S Aanscultural self-efficaural self-effick resources: ChapterCh
e Clinical EvaluationClinical Evaluation
stionnaire adapttionnaire adaScompetenmpetenspe

4. Cultural Competence Clinical Evaluation Tool—Teacher Version (CCCET-TV)
� An 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensionsof student’s clinical cultural competence behaviors as rated by the teacher or preceptor:� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, ac-
ceptance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professionalnursing care (Subscale 3).
� Used to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available. Used together with CCCET-SV (studentsand teachers independently complete the CCCET at the end of the clinical experience). May be used withother toolkit items
� Content validity index high (0.91) as rated by three internationally recognized experts in transcultural nursing� Descriptive statistics (frequency and percent) for individual and aggregate data. Compare with student
ratings� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4 and 5
5. Cultural Competence Clinical Evaluation Tool—Employee Version (CCCET-EV)� An 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions
of clinical cultural competence behaviors as perceived by the employee:� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3).
� Used to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evalu-ate change following educational intervention and/or increased exposure to culturally diverse clients and/orincreased exposure to the clinical topic/area not previously available. Used together with CCCET-AEV (em-ployees and agency evaluators independently complete the CCCET at the end of the clinical orientation orpreceptor experience). May be used with other toolkit items
� Descriptive statistics (frequency and percent) for individual and aggregate data. Compare with agency evalu-ator ratings.
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4 and 5
6. Cultural Competence Clinical Evaluation Tool—Agency Evaluator Version (CCCET-AEV)� An 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions
of employee’s clinical cultural competence behaviors as rated by the agency evaluator:� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3).
� Used to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available. Used together with CCCET-EV (employeesand agency evaluators independently complete the CCCET at the end of the clinical orientation or preceptorexperience). May be used with other toolkit items
� Descriptive statistics (frequency and percent) for individual and aggregate data. Compare with employeeratings.
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4 and 5
© Springer Publishing Company
ateate
(CCCET-EV)
ing three subscales mg threy the employee:mployee:
priate attitudes, value attitudeacy necessary for proacy necessary f
ion, identify areas oion, identify antervention and/or iervention and/or
al topic/area not prec/area not prs independently cors independently
y be used with othebe used with otherequency and percenncy and perc
ed to guide educatioed to guide educay book resources: Chbook resources: C
Clinical EvaluClinical EvaSnairenaire

7. Clinical Setting Assessment Tool—Diversity and Disparity (CSAT-DD)
� Used to gather demographic information about the clinical setting, diversity, and disparity� Can be used to describe clinical setting characteristics (frequency and percent)� Can be used to create comparison groups based on select demographic categories for comparing scores and
data on the TSET, CCCET, CSAT-DD, and other assessment tools� Results can guide future clinical interventions to eliminate health disparities, student and staff placements,
and educational interventions with students and staff� Supplementary book resources: Chapter 4
8. Demographic Data Sheet—Undergraduate (DDS-U)
� Used to gather demographic information from undergraduate (pre-licensure) students� Can be used to describe sample characteristics (frequency and percent)� Can be used to create comparison groups based on select demographic categories for comparing scores and
data on the TSET, CCCET, CSAT-DD, and other assessment tools� Supplementary book resources: Chapters 4 and 5
9. Demographic Data Sheet—Nurses (DDS-N)
� Used to gather demographic information from nurses working in clinical agencies and/or enrolled in RN-BSand graduate (master’s and doctoral) programs
� May be used to describe sample characteristics (frequency and percent)� May be used to create comparison groups based on select demographic categories for comparing scores and
data on the TSET, CCCET, CSAT-DD, and other assessment tools� Supplementary book resources: Chapters 4 and 5
10. Self-Assessment Tool—Academic (SAT-A)
� Used to help individual faculty member, administrator, and the organization assess various dimensions thatcan impact upon cultural competence in the academic setting
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities.�
11. Self-Assessment Tool—Health Care Institutions (SAT-HCI)
� Used to help individual staff nurse, nurse manager, nurse educator, nurse executive, administrator, and theorganization assess various dimensions that can impact upon cultural competence in the health care setting
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities.� Supplementary book resources: Chapter 10 and 10.2
12. Self-Assessment Tool—Professional Associations (SAT-PA)
� Used to help individual members, elected officers, administrators, association leaders, and the organizationassess various dimensions that can impact upon cultural competence in the professional association
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities.� Supplementary book resources: Chapter 13, 13.2
13. Active Promoter Assessment Tool—Academic (APAT-A)
� Used to help individuals, groups, and organizations� Appraise values, beliefs, and actions concerning cultural competence development
© Springer Publishing Company
Supplementary book resources: Chapter 6, Figure1.2 and 6.2Table
Figure1.2 andTable
Figure1.2 andTable
S A M
P L
Elinical agencies anal agencies an
d percent)pdemographic categomographic ca
ment toolsls
ministrator, and theministrator, anthe academic settinge academic settin
oupsoupn with other toolkitwith other toolki
e with a listing of stlisting ofpriorities.p
alth Care Institutione Institution
vidual staff nurse, nvidual staff nursesess various dimensess various dimensdividually and/oividually and
or in conjr in conjd cod
rces:es: CChapterhapt 6, Ta

� Determine whether or not one is an optimal active role model in cultural competence development within
� Identify factors restricting cultural competence development� Plan and coordinate future active promoter actions toward achieving optimal cultural competence
�
� May be used alone or in conjunction with other toolkit items� Supplementary book resources: Chapter 6 and Table 6.1
14. Active Promoter Assessment Tool—Health Care Institutions/Professional Associations (APAT-HCIPA)
� Used to help individuals, groups, and organizations� Appraise values, beliefs, and actions concerning cultural competence development� Determine whether or not one is an optimal active role model in cultural competence development within
the health care institution or professional association� Identify factors restricting cultural competence development� Plan and coordinate future active promoter actions toward achieving optimal cultural competence
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Supplementary book resources: Chapters 10 and 13, Figure 10.3, Exhibit 13.1
15. Systematic Inquiry: Academic (SI-A)
� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, correspondingactions, notations/reflections, prioritization, and future planning
� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competencydevelopment is actively present:� Overall within the curriculum� Specifically at the individual course level� Via outside connections to supplementary resources.
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the academic setting?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items. (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log.) Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic–prescriptive innovations targeting faculty and student developmentin the overall goal of achieving optimal cultural competence
� Supplementary book resources: Chapter 6 and Figure 6.3
16. Systematic Inquiry: Health Care Institutions (SI-HCI)
� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, correspondingactions, notations/reflections, prioritization, and future planning.
� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competencydevelopment is actively present:� Overall within the institution� Specifically at the individual unit (site) level� Via outside connections to supplementary resources.
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the HCI?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items. (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log.) Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic–prescriptive innovations targeting staff development and improvedpatient care outcomes in the overall goal of achieving optimal cultural competence
� Supplementary book resources: Chapter 10 and Figure 10.4
© Springer Publishing Company
academic setting
May be used individually and/or in groups
s
S A M
P L
Exhibit 13.1ibit 13.1
for systematic appraor splanningng
examine how visibleexamine how visible
ary resources.ry reso additional questioitional
etence an integral coence an integralonents fit together?s fit together
n groupsonjunction with othnjunction with oth
nce Documentation Locumentatioand new diagnostic–diagnostic–
of achievingof ach optimaloptibook resources: Chbook resources: ChSHealth Care InsHealth Care
y quany quan

17. Systematic Inquiry: Professional Associations (SI-PA)
� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, correspondingactions, notations/reflections, prioritization, and future planning.
� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competencydevelopment is actively present:� Overall within the association� Specifically at the membership level� Via outside connections to supplementary resources.
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the professional association?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items. (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log.) Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic–prescriptive innovations targeting staff and membership developmentin the overall goal of achieving optimal cultural competence
� Supplementary book resources: Chapter 13 and Figure 13.3
18. Personal Coding Cover Page for Anonymity and Matching Questionnaires
� Used to match questionnaires and assessment tools while protecting respondent’s anonymity� Attach to front page of questionnaire, questionnaire packet, or assessment tool
19. Sample Permission Letter
� Provides a sample for prospective educators and researchers� Adapt letter according to study purpose and need� Mail one copy to Springer Publishing Company and one copy to Dr. Marianne R. Jeffreys.
20. Cultural Competence Documentation Log
� User-friendly log to assist institutions in documenting cultural competence plans, actions, and evaluations.� Use after Toolkit Systematic Inquiry Assessment Tool.
21. Research Report Template
� User-friendly template to assist individuals and institutions report data generated from assessment tools andquestionnaires in toolkit
� Provides a guide for presentations, publications, future research, and cultural competence interventions� Supplementary book resources: TSET Research Exhibits in chapters 6 and 10
© Springer Publishing Company
affaff
aires
tecting respondent’stecting respondent’st, or assessment toolr assessment
esearchersesearcherseed
any and one copy toany and one co
SA Mns in documenting cin documenting
uiry Assessment Tooessment To
to assist individualsst individualolkit
S Afor presentations, puor presentations, pbook resources: TSbook resources: TS

I T E M 1
Transcultural Self-Efficacy Tool (TSET)
DESCRIPTIONAn 83-item questionnaire designed to measure and evaluate learners’ confidence (transcultural self-efficacy) for per-forming general transcultural nursing skills among diverse client populations. It has been requested by researchersworldwide in multiple health disciplines for use with students, nurses, and other health professionals. The new TSET-Multidisciplinary Healthcare Provider version should be used with multidisciplinary groups (see Toolkit Item 2).
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about TSET, administration, uses, and scoring in Teaching Cultural Competence in Nursing
and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.(4) Send reliability and validity test results and study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGSelf-Efficacy Strength (SEST) refers to the average strength of self-efficacy perceptions within a particular dimension(subscale) of the construct. Calculate by totaling subscale item responses and dividing by the number of subscaleitems, resulting in the mean score. For example:
Cognitive Subscale Practical Subscale Affective Subscale
FormulaItem Response Sum# of Subscale Items
Add Item Responses25
Add Item Responses28
Add Item Responses30
Application14025
18228
21030
SEST = 5.6 SEST = 6.5 SEST = 7.0
Use scores to compare subscale scores within and between groups to determine effectiveness of cultural compe-tence educational intervention(s) as seen by statistically significant differences in scores.
Longitudinal comparison within groups(1) TSET pretest → Cultural Competence Educational Intervention → TSET post-test
Comparison between groups(2) TSET pretest → Cultural Competence Educational Intervention → TSET post-test
TSET pretest (Control Group) → TSET post-test
Cross-sectional comparison between groups(3) TSET administration to novice group (before cultural competence educational intervention)
TSET administration to advanced group (after cultural competence educational intervention)
© Springer Publishing Company
AM P
L E
health pealthlinary groupsinary grou
and administrationrationscoring inorin Teaching C
fore study design anudy design annaire.naire
esults (see Toolkit Itesults (see Toolkit Iof New York CollegNew York
York 10314, USA.314,
average strength of serage strength ofy totaling subscale itng subscale
r example:
S A
S A Cognitive SuCognitive Su
SAsponse Sumponse SumSSSbscale Itemsscale Items
AddddS

PURPOSESEvaluation of transcultural self-efficacy (TSE) perceptions may be used for a variety of purposes targeting the individualand/or groups. The purposes are to:
� Develop a composite/baseline of learners’ needs, values, attitudes, and skills concerning transcultural nursing(or health care)
� Identify general transcultural skills perceived with more confidence (or those as less difficult or stressful)� Identify general transcultural skills perceived with less confidence (or those as more difficult or stressful)� Identify differences within groups� Identify differences between groups� Identify at-risk individuals (low confidence or overly confident)� Evaluate the effectiveness of specific teaching interventions� Assess changes in transcultural self-efficacy perceptions over time
ADDITIONAL INFORMATIONResearchers seeking to group individuals into low efficacy, medium efficacy, and high efficacy groups for the purposeof identifying at-risk individuals and tracking changes should consult standard statistical methods and literature forguidance. The study purpose and sample may guide method selection for group categorization.
Self-Efficacy Level (SEL) refers to the number of items perceived at a specified minimum level of confidence.For example, SEL had been used to identify individuals with “low efficacy” and then track SEL changes followingtreatment interventions. The study purpose and sample may guide the selected definition of the minimum confidencelevel; however this scoring calculation is no longer recommended due to consistently insignificant results with nursingstudents and nurses. (See previously published studies and Chapter 4.)
SUPPLEMENTARY RESOURCESBook Chapters 3, 4, and 5.
TSET Research Exhibits in Chapters 6 and 10.
Jeffreys, M.R. (2000). Development and psychometric evaluation of the Transcultural Self-Efficacy Tool: A synthesis of findings. Journalof Transcultural Nursing, 11(2), 127–136.
Jeffreys, M.R. & Dogan, E. (2010). Factor analysis of the Transcultural Self-Efficacy Tool (TSET). Journal of Nursing Measurement, 18(2),120–139.
Jeffreys, M.R. & Smodlaka, I. (1999). Changes in students’ transcultural self-efficacy perceptions following an integrated approach tocultural care. Journal of Multicultural Nursing and Health, 5(2), 6–12. (Erratum, 2000, 6(1), 20.
Jeffreys, M.R. & Smodlaka, I. (1999). Construct validation of the Transcultural Self-Efficacy Tool. Journal of Nursing Education, 38,222–227.
Jeffreys, M.R. & Smodlaka, I. (1998). Exploring the factorial composition of the Transcultural Self-Efficacy Tool. International Journal ofNursing Studies, 35, 217–225.
Jeffreys, M.R. & Smodlaka, I. (1996). Steps of the instrument-design process: An illustrative approach for nurse educators, Nurse Educa-tor, 21(6), 47–52. (Erratum, 1997, 22(1), 49).
© Springer Publishing Company
SA M
P L
Eigh egh
statisticalstatisticaoup categorizatiop categorizatio
t a specified minimucified minimficacy” and then trahen tra
he selected definitione selected definitiodue to consistently ito consistentl
hapter 4.)hapte
0.0.
metric evaluation of thevaluation o36.
r analysis of the Transcanalysis of the Transc
9). Changes in studennges in studenulticultural Nursing andursin
I. (1999). Construct vI. (1999). Construct
S, I. (1998). ExplorinI. (1998). Exp–225.
996). St996) St19
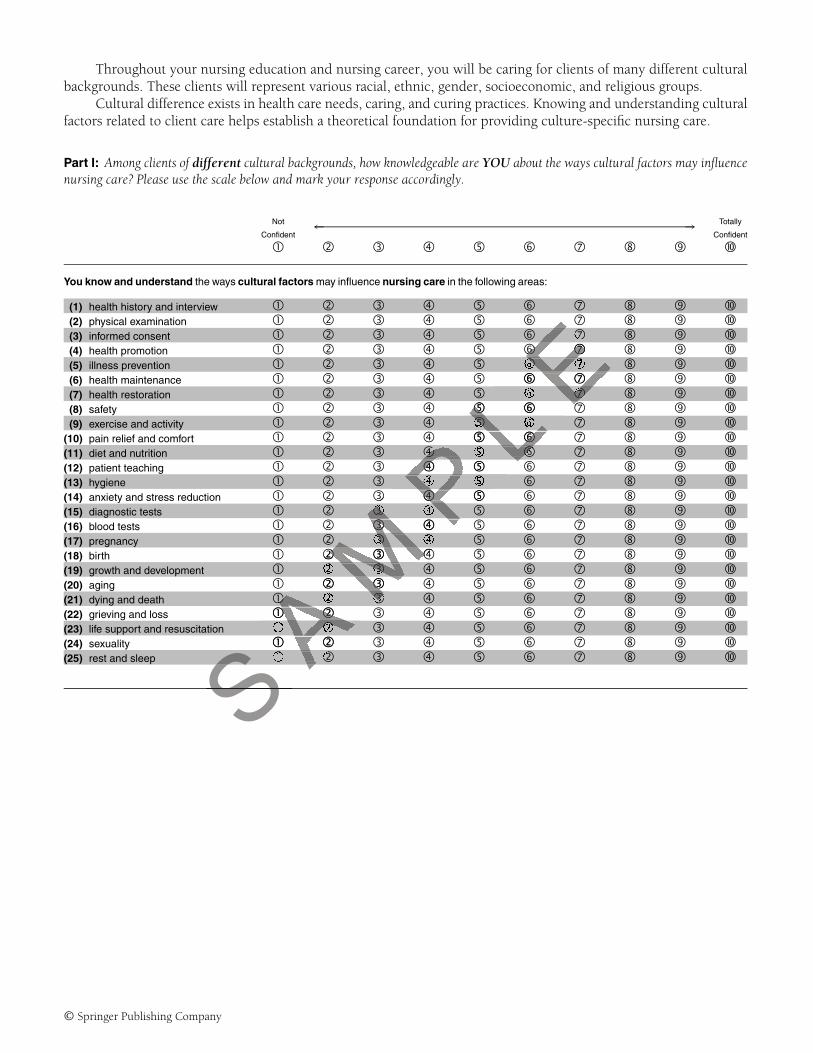
Throughout your nursing education and nursing career, you will be caring for clients of many different culturalbackgrounds. These clients will represent various racial, ethnic, gender, socioeconomic, and religious groups.
Cultural difference exists in health care needs, caring, and curing practices. Knowing and understanding culturalfactors related to client care helps establish a theoretical foundation for providing culture-specific nursing care.
Part I: Among clients of different cultural backgrounds, how knowledgeable are YOU about the ways cultural factors may influencenursing care? Please use the scale below and mark your response accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
You know and understand the ways cultural factors may influence nursing care in the following areas:
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
AM P
L EE� �� �E� �
� ��
L E�� � �� � �L � �� ��
PL� � �
� �� �P �� � ��
MP� �
� �� �
M�� � �� � �
AM�� ��
AM� � �
� �� �
SAA �
� �
SA
SS

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment ofeach client. This is best done by interview.
Right NOW, how confident are YOU about interviewing clients of different cultural backgrounds to learn abouttheir values and beliefs?
Rate your degree of confidence or certainty for each of the following interview topics. Please use the scale below andmark your response accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
Interview clients of different cultural backgrounds about:
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception & orientation � � � � � � � �(32) racial background & identity � � � � � � � �(33) ethnic background & identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background & identity � � � � � � � �(36) educational background & interests � � � � � � � �(37) religious practices & beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health & illness beliefs � � � � � � � �(46) folk medicine tradition & use � � � � � � � �(47) gender role & responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination & bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
A M P
L EE
���
E�� � �� �
L E� �� ��
L E� � �� � �� �
PL �
� � �� � �
PL� � �
� �� P�� � �� �
MP� �
� � �� �M � � �� �� �
AM�� ��
AS
A���S
AS S
ASS

Part III: As a nurse who will care for many different people, knowledge of yourself is very important.
Please rate YOUR degree of confidence or certainty for each of the following items. Use the scale below and mark yourresponse accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
(A) About yourself, you are AWARE OF:
(54) YOUR OWN cultural heritage and belief systems � � � � � � � �(55) YOUR OWN biases and limitations � � � � � � � �(56) differences within YOUR OWN cultural group � � � � � � � �
(B) Among clients of different cultural backgrounds,
You are AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a culturally different world � � � � � � � �(62) interaction between nursing, folk, and professional systems � � � � � � � �
You ACCEPT:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
You APPRECIATE:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) culture-specific health care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
You RECOGNIZE:
(71) inadequacies in the U.S. health care system � � � � � � � �(72) importance of home remedies & folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
You ADVOCATE:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) culture-specific care � � � � � � � �
© Springer Publishing Company
E� �� � �� � �
L E� � �� � ��
L E� � � �� � � �� � �
P�� ��
MP
AM
S Aes A
lth care
SAphy of lif
S

I T E M 2
Transcultural Self-Efficacy Tool—Multidisciplinary HealthcareProvider Version (TSET-MHP)
DESCRIPTIONAn 83-item questionnaire designed to measure and evaluate learners’ confidence (transcultural self-efficacy) for per-forming general transcultural skills among diverse client populations. Items are exactly the same as original TSET.Directions change “nurse” and “nursing” focus to “health care provider” focus, encompassing nursing and all othermultidisciplinary health care provider groups.
The new TSET-Multidisciplinary Healthcare Provider version should be used with multidisciplinary groups. Forlearner groups within the nursing discipline, use the original TSET (Toolkit Item 1).
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about TSET, administration, uses, and scoring in Teaching Cultural Competence in Nursing
and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.(4) Send reliability and validity test results and study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGSelf-Efficacy Strength (SEST) refers to the average strength of self-efficacy perceptions within a particular dimension(subscale) of the construct. Calculate by totaling subscale item responses and dividing by the number of subscaleitems, resulting in the mean score. For example:
Cognitive Subscale Practical Subscale Affective Subscale
FormulaItem Response Sum# of Subscale Items
Add Item Responses25
Add Item Responses28
Add Item Responses30
Application14025
18228
21030
SEST = 5.6 SEST = 6.5 SEST = 7.0
Use scores to compare subscale scores within and between groups to determine effectiveness of cultural compe-tence educational intervention(s) as seen by statistically significant differences in scores.
© Springer Publishing Company
A M P
L E
rananexactlyexac
s, encompassi, encompa
ld be used with multwith mulToolkit Item 1).oo
sting online and admting online and admuses, and scoring inuses, and s
n (2010)0) beforebefo studthe questionnaire.he questionnaire.
and study results (sestudy results (sUniversity of New YUniversity of New
land, New York 103, New York 103
fers to the average stto the averag
S ACalculate by totalingby totalingn score. For examplen score. For exam
S SS

Longitudinal comparison within groups(1) TSET pretest → Cultural Competence Educational Intervention → TSET post-test
Comparison between groups(2) TSET pretest → Cultural Competence Educational Intervention → TSET post-test
TSET pretest (Control Group) → TSET post-test
Cross-sectional comparison between groups(3) TSET administration to novice group (before cultural competence educational intervention)
TSET administration to advanced group (after cultural competence educational intervention)
PURPOSESEvaluation of transcultural self-efficacy (TSE) perceptions may be used for a variety of purposes targeting the individualand/or groups. The purposes are to:
� Develop a composite/baseline of learners’ needs, values, attitudes, and skills concerning transcultural nursing(or health care)
� Identify general transcultural skills perceived with more confidence (or those as less difficult or stressful)� Identify general transcultural skills perceived with less confidence (or those as more difficult or stressful)� Identify differences within groups� Identify differences between groups� Identify at-risk individuals (low confidence or overly confident)� Evaluate the effectiveness of specific teaching interventions� Assess changes in transcultural self-efficacy perceptions over time
ADDITIONAL INFORMATIONResearchers seeking to group individuals into low efficacy, medium efficacy, and high efficacy groups for the purposeof identifying at-risk individuals and tracking changes should consult standard statistical methods and literature forguidance. The study purpose and sample may guide method selection for group categorization.
Self-Efficacy Level (SEL) refers to the number of items perceived at a specified minimum level of confidence.For example, SEL had been used to identify individuals with “low efficacy” and then track SEL changes followingtreatment interventions. The study purpose and sample may guide the selected definition of the minimum confidencelevel; however this scoring calculation is no longer recommended due to consistently insignificant results with nursingstudents and nurses. (See previously published studies and Chapter 4).
SUPPLEMENTARY RESOURCESBook Chapters 3, 4, and 5.
TSET Research Exhibits in Chapters 6 and 10.
Jeffreys, M.R. (2000). Development and psychometric evaluation of the Transcultural Self-Efficacy Tool: A synthesis of findings. Journalof Transcultural Nursing, 11(2), 127–136.
Jeffreys, M.R. & Dogan, E. (2010). Factor analysis of the Transcultural Self-Efficacy Tool (TSET). Journal of Nursing Measurement, 18(2),120–139.
Jeffreys, M.R. & Smodlaka, I. (1999). Changes in students’ transcultural self-efficacy perceptions following an integrated approach toculture care. Journal of Multicultural Nursing and Health, 5(2), 6–12. (Erratum, 2000, 6(1), 20.
Jeffreys, M.R. & Smodlaka, I. (1999). Construct validation of the Transcultural Self-Efficacy Tool. Journal of Nursing Education, 38, 222–227.
Jeffreys, M.R. & Smodlaka, I. (1998). Exploring the factorial composition of the Transcultural Self-Efficacy Tool. International Journal ofNursing Studies, 35, 217–225.
Jeffreys, M.R. & Smodlaka, I. (1996). Steps of the instrument-design process: An illustrative approach for nurse educators, Nurse Educa-tor, 21(6), 47–52. (Erratum, 1997, 22(1), 49).
© Springer Publishing Company
S A M
P L
Es cos co
or those as lessr those as less(or those as more dose as more d
fident)nt)tionst o s
tions over timeions over
w efficacy, medium efficacy, mediumchanges should conchanges shou
may guide method sey guide method sthe number of itemmber of ite
identify individualsividualspurpose and samplurpose and sampl
ulation is no longer rn is no longereviously published sublis
RESOURCESRESOURCE

Throughout your education and career as health care providers, faculty, or students, you will be caring for clientsof many different cultural backgrounds. These clients will represent various racial, ethnic, gender, socioeconomic, andreligious groups.
Cultural difference exists in health care needs, caring, and curing practices. Knowing and understanding culturalfactors related to client care helps establish a theoretical foundation for providing culture-specific health care.
Part I: Among clients of different cultural backgrounds, how knowledgeable are YOU about the ways cultural factors may influencehealth care? Please use the scale below and mark your response accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
You know and understand the ways cultural factors may influence health care in the following areas:
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
A M P
L EE�
E� �� �� �
L E�� � ��
L E�� �� �
PL�� � �� � �
P�� ��
MP�
� �� �
MP� �
� � ��M� � �� ��
AM�� � �� � �
AS A� �� ��
SA� �
SA
�S

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment ofeach client. This is best done by interview.
Right NOW, how confident are YOU about interviewing clients of different cultural backgrounds to learn abouttheir values and beliefs?
Rate your degree of confidence or certainty for each of the following interview topics. Please use the scale below andmark your response accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
Interview clients of different cultural backgrounds about:
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception & orientation � � � � � � � �(32) racial background & identity � � � � � � � �(33) ethnic background & identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background & identity � � � � � � � �(36) educational background & interests � � � � � � � �(37) religious practices & beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health & illness beliefs � � � � � � � �(46) folk medicine tradition & use � � � � � � � �(47) gender role & responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination & bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
A M P
L EE
���
E�� � �� �
L E� �� ��
L E� � �� � �� �
PL �
� � �� � �
PL� � �
� �� P�� � �� �
MP� �
� � �� �M � � �� �� �
AM�� ��
AS
A���S
AS S
ASS

Part III: As a health care provider who will care for many different people, knowledge of yourself is very important.
Please rate YOUR degree of confidence or certainty for each of the following items. Use the scale below and mark yourresponse accordingly.
← →Not Totally
Confident Confident
� � � � � � � �
(A) About yourself, you are AWARE OF:
(54) YOUR OWN cultural heritage and belief systems � � � � � � � �(55) YOUR OWN biases and limitations � � � � � � � �(56) differences within YOUR OWN cultural group � � � � � � � �
(B) Among clients of different cultural backgrounds,
You are AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a culturally different world � � � � � � � �(62) interaction between nursing, folk, and professional systems � � � � � � � �
You ACCEPT:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
You APPRECIATE:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) culture-specific health care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
Among clients of different cultural backgrounds,
You RECOGNIZE:
(71) inadequacies in the U.S. health care system � � � � � � � �(72) importance of home remedies & folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
You ADVOCATE:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) culture-specific care � � � � � � � �
© Springer Publishing Company
E� �� � � �� � �
L E� �� � � ��L�
� � � �� �
P �� ��
MP�
AM
SA Aare
SA
S ultural backgrounds,ltural backgroSSScare

I T E M 3
Cultural Competence Clinical Evaluation Tool—Student Version (CCCET-SV)
DESCRIPTIONAn 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions of clin-ical cultural competence behaviors as perceived by the student:
� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3)
INSTRUCTIONS FOR RESEARCHERS1. Detach this cover sheet before photocopying or posting online and administration to sample.2. Review information about CCCET, administration, uses, and scoring in Teaching Cultural Competence in Nurs-
ing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.3. Please be sure that all respondents return the questionnaire.4. Send study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
Compare with teacher ratings on CCCET-TV.
� Use to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available.
� May be used together with CCCET-TV (students and teachers independently complete the CCCET at the endof the clinical experience).
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
S A M
P L
Ees, or beliefs includbeliefs incluoviding culturally seurally se
sting online and admsting online and admon, uses, and scorin, uses, and
vation (2010)ation (2010) beforebthe questionnaire.he questionnaire.
1) to:University of NewUniversity of New
sland, New York 10New York
y and percent) for inercent) for inratings on CCCET-TCCC
ne baseline informate baseline informang educational intg educationaSto the clinicato the clinic
r withr with

Throughout your career, you will be caring for clients of many different cultural backgrounds. These clients willrepresent various racial, ethnic, gender, socioeconomic, and religious groups. Culturally specific care requires that youknow, understand, and identify cultural factors related to client care and conduct your nursing practice accordingly.
Part I: For clients of different cultural backgrounds, to what extent did you provide culturally specific care during the clinicalpracticum?
Please use the scale below and mark your response accordingly.
If the opportunity to provide care in the listed area was unavailable, please mark A.If the opportunity to provide care in the listed area was available, but diverse clients were unavailable, mark B.
Area Diverse NotNot Clients At ← →
Available Not Available All Totally� � � � � � � �
During this semester’s clinical practicum, you provided culturally specific care in the following areas: (Mark one choice for each item.)
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
SA M
P L
E(Mark oneMark
E� �� � �� �
L E�� � �� � �L�� � �� �
PL� � � �
� � �� � �P� �� � ��
MP� �
� � �� � �
M�
MM� �� �MMM�A
MA
M��A
MA
MA
M�AAAAA AAAAAAAA
SA
SA
SAA
SA
SA
SS ation SSSSSSSS

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment.
How frequently did you assess clients of different cultural backgrounds about each cultural factor during the clinicalpracticum?
Please use the scale below and mark your response accordingly.If the opportunity to conduct an assessment of the listed area was unavailable, please mark A.If the opportunity to conduct an assessment of the listed area was available, but diverse clients were unavailable,mark B.
Area DiverseNot Clients ← →
Available Not Available Never Always� � � � � � � �
During this semester’s clinical practicum, you assessed clients of different backgrounds about: (Mark one choice for each item.)
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception and orientation � � � � � � � �(32) racial background and identity � � � � � � � �(33) ethnic background and identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background and identity � � � � � � � �(36) educational background and interests � � � � � � � �(37) religious practices and beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health and illness beliefs � � � � � � � �(46) folk medicine tradition and use � � � � � � � �(47) gender role and responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination and bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
A M P
L EE�
� ��
E� �� � �� � �
L E� �� � ��
L E�� � �� �
PL� �
� � � �� � �
P� � ��
MP�
MM� ��
MP
MMMM�MMMMMA
MMMMA
MA
MA
MMMA
MA
MMAAAAA
SA
SAAA
S SA
xperiencesSS

Part III: What affective learning outcomes did you gain as a result of your clinical practicum this semester?
Specifically, to what extent did you develop new, culturally sensitive and professionally appropriate attitudes, values,or beliefs OR further develop culturally sensitive and professionally appropriate attitudes, values, and beliefs aboutthe items below?
For Section A, please use the scale below and mark your response accordingly. (Mark one choice for each item.)
Not To aAt ← → Great
All Extent� � � � � � � �
(A) About Yourself: As a result of this semester’s clinical practicum, you developed a greater AWARENESS OF:
(54) YOUR OWN cultural heritage and belief systems � � � � � � � �(55) YOUR OWN biases and limitations � � � � � � � �(56) differences within YOUR OWN cultural group � � � � � � � �
For Section B, please use the scale below and mark your response accordingly. (Mark one choice for each item.)
Diverse Not To aClients At ← → Great
Not Available All Extent� � � � � � � �
(B) Among clients of different cultural backgrounds,
As a result of this semester’s clinical practicum, you became MORE AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a � � � � � � � �
culturally different world(62) interaction between nursing, folk, and professional systems � � � � � � � �
As a result of this semester’s clinical practicum, you became MORE ACCEPTING OF:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
As a result of this semester’s clinical practicum, you became MORE APPRECIATIVE OF:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) cultural-specific nursing care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
© Springer Publishing Company
M P L
EEly. (Mark one cho(Mark one cho
← LAll� � � �� �
PL
WARE OF:E OF:
MP
MP
MP�
MP
MP��
MMMS
A MMMAMprofessional systemsofessio
acticum, you becameyou became MOMO
SA
Sl group
ural groupsral groupsS nt based on beScal practicuml practicumS
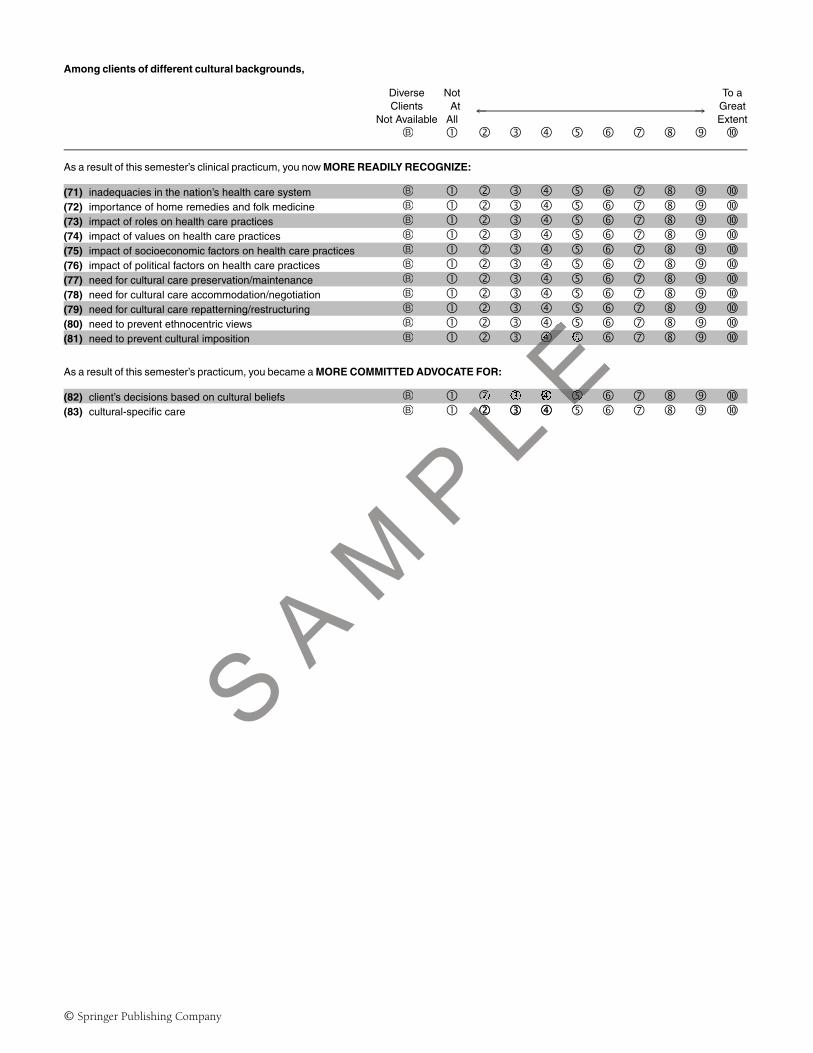
Among clients of different cultural backgrounds,
Diverse Not To aClients At ← → Great
Not Available All Extent� � � � � � � �
As a result of this semester’s clinical practicum, you now MORE READILY RECOGNIZE:
(71) inadequacies in the nation’s health care system � � � � � � � �(72) importance of home remedies and folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
As a result of this semester’s practicum, you became a MORE COMMITTED ADVOCATE FOR:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) cultural-specific care � � � � � � � �
© Springer Publishing Company
L EE�
L EL E�
S A M
P L
� � � ��

I T E M 4
Cultural Competence Clinical Evaluation Tool—Teacher Version (CCCET-TV)
DESCRIPTIONAn 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions of clin-ical cultural competence behaviors as rated by the teacher or preceptor:
� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3).
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about CCCET, administration, uses, and scoring in Teaching Cultural Competence in Nurs-
ing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.(4) Send study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
Compare with student ratings on CCCET-SV.
� Use to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available.
� May be used together with CCCET-SV (Students and teachers independently complete the CCCET at the endof the clinical experience).
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
S A M
P L
Ees, or beliefs includbeliefs incluoviding culturally seurally se
osting online and admsting online and adion, uses, and scorin, uses, and
vation (2010)vation (2010) beforebthe questionnaire.he questionnaire.
1) to:University of NewUniversity of New
Island, New York 10New York
y and percent) for inercent) for int ratings on CCCET-ratings on CCC
ne baseline informae baseline informang educational ing educationa
o the clinicthe cliniwithith

Throughout one’s nursing career, nurses will be caring for clients of many different cultural backgrounds. Theseclients will represent various racial, ethnic, gender, socioeconomic, and religious groups. Culturally specific carerequires that nurses know, understand, and identify cultural factors related to client care and conduct their nursingpractice accordingly.
Part I: For clients of different cultural backgrounds, to what extent did the student provide culturally specific care?
Please use the scale below and mark your response accordingly.
If the opportunity to provide care in the listed area was unavailable, please mark A.If the opportunity to provide care in the listed area was available, but diverse clients were unavailable, mark B.If you are unable to evaluate the student, please leave item blank.
Area Diverse NotNot Clients At ← →
Available Not Available All Totally� � � � � � � �
During this semester’s clinical practicum, student provided culturally specific care in the following areas: (Mark one choice for each item.)
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
SA M
P L
EEng areas: (Mark one careas: (Mark one c
L E�� � ��L�� � �� �
PL� � �
� � �� � �
P� �� � � ��
MP�
� � �� � �
MP�
MM� ��MMM� �
AM
AM��
AM
AM
AM�
AAAM
A �A AAAAAAAAS
AS
AS
AAAS
AS
AS SSSSSSSSSS

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment.
How frequently did the student assess clients of different cultural backgrounds about each cultural factor?
Please use the scale below and mark your response accordingly.If the opportunity to conduct an assessment of the listed area was unavailable, please mark A.If the opportunity to conduct an assessment of the listed area was available, but diverse clients were unavailable,mark B.If you are unable to evaluate the student, please leave item blank.
Area DiverseNot Clients ← →
Available Not Available Never Always� � � � � � � �
During this semester’s clinical practicum, the student assessed clients of different backgrounds about: (Mark one choice for each item.)
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception and orientation � � � � � � � �(32) racial background and identity � � � � � � � �(33) ethnic background and identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background and identity � � � � � � � �(36) educational background and interests � � � � � � � �(37) religious practices and beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health and illness beliefs � � � � � � � �(46) folk medicine tradition and use � � � � � � � �(47) gender role and responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination and bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
A M P
L EE�
� �� �
E� �� � � �� � �
L E� �� � ��L�
� � �� �
PL� �
� � �� � �
P� � ��
MP�
MM� ��
MP
MMMMM�MMMMMA
MA
MMMA
MA
MA
MMMA
MA
MA AA
SAAA
SAAA
S SA
xperiencesSS

Part III: During the clinical practicum experience and/or clinical practicum assignments, to what extent did the student demonstrateor express culturally sensitive and professionally appropriate attitudes, values, or beliefs about the items below?
For Section A, please use the scale below and mark your response accordingly. (Mark one choice for each item.)If you are unable to evaluate the student, please leave item blank.
Not To aAt ← → GreatAll Extent� � � � � � � �
(A) About his/her own culture: As a result of this semester’s clinical practicum, the student developed a greater AWARENESS OF:
(54) HIS/HER OWN cultural heritage and belief systems � � � � � � � �(55) HIS/HER OWN biases and limitations � � � � � � � �(56) differences within HIS/HER OWN cultural group � � � � � � � �
For Section B, please use the scale below and mark your response accordingly. (Mark one choice for each item.)If you are unable to evaluate the student, please leave item blank.
Diverse Not To aClients At ← → Great
Not Available All Extent� � � � � � � �
(B) Among clients of different cultural backgrounds,
As a result of this semester’s clinical practicum, the student became MORE AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a � � � � � � � �
culturally different world(62) interaction between nursing, folk, and professional systems � � � � � � � �
As a result of this semester’s clinical practicum, the student became MORE ACCEPTING OF:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
As a result of this semester’s clinical practicum, the student became MORE APPRECIATIVE OF:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) cultural-specific nursing care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
© Springer Publishing Company
AM P
L E
(Mark one(Mark one
← LAllll� � � �� �
PL
MORE AWARE OF:WARE
MP
MMMMMMMS A
AMg
nd professional systemsfessional syste
al practicum, the studentl practicum, the stu
S ural groupsral groupsal groSSSsed on b
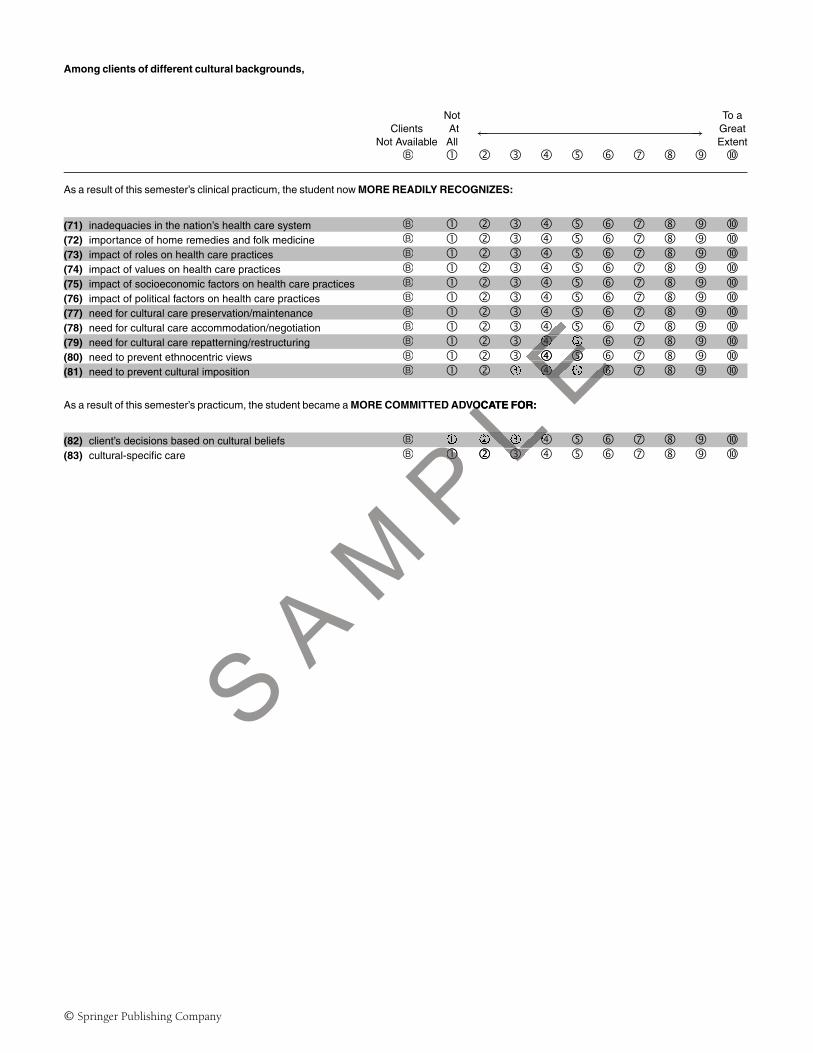
Among clients of different cultural backgrounds,
Not To aClients At ← → Great
Not Available All Extent� � � � � � � �
As a result of this semester’s clinical practicum, the student now MORE READILY RECOGNIZES:
(71) inadequacies in the nation’s health care system � � � � � � � �(72) importance of home remedies and folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
As a result of this semester’s practicum, the student became a MORE COMMITTED ADVOCATE FOR:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) cultural-specific care � � � � � � � �
© Springer Publishing Company
L E� ��
E� �
� � � �� �E� � �
S A M
P L
VOCATE FOR:O
PL� � �
� � �� � �

I T E M 5
Cultural Competence Clinical Evaluation Tool—Employee Version (CCCET-EV)
DESCRIPTIONAn 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions of clin-ical cultural competence behaviors as perceived by the employee:
� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs, including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3).
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about CCCET, administration, uses, and scoring in Teaching Cultural Competence in Nurs-
ing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.(4) Please send study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
Compare with agency evaluator ratings on CCCET-AEV.
� Use to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available.
� May be used together with CCCET-AEV (employees and agency evaluators independently complete theCCCET at the end of the clinical orientation or preceptor experience).
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
S A M
P L
Ees, or beliefs, inclubeliefs, incluoviding culturally seurally se
sting online and admsting online and admon, uses, and scoring, uses, and
vation (2010)ation (2010) beforebthe questionnaire.he questionnaire.
tem 21) to:1) to:University of NewUniversity of New
sland, New York 10New York
y and percent) for inercent) for inevaluator ratings onating
ne baseline informate baseline informang educational intg educationaSto the clinicato the clinic
her witer with

Throughout your career, you will be caring for clients of many different cultural backgrounds. These clients willrepresent various racial, ethnic, gender, socioeconomic, and religious groups. Culturally specific care requires that youknow, understand, and identify cultural factors related to client care and conduct your nursing practice accordingly.
Part I: For clients of different cultural backgrounds, to what extent did you provide culturally specific care?
Please use the scale below and mark your response accordingly.
If the opportunity to provide care in the listed area was unavailable, please mark A.If the opportunity to provide care in the listed area was available, but diverse clients were unavailable, mark B.
Area Diverse NotNot Clients At ← →
Available Not Available All Totally� � � � � � � �
You provided culturally specific care in the following areas: (Mark one choice for each item.)
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
SA M
P L
EE� �� � �� �
L E�� � � �� � �L�� � �� �
PL� � �
� � �� � �P � �� � ��
MP� �
� � �� � �
M�MM� �� �MMM�A
MA
M��A
MA
MA
M�AAAAA AAAA
SAAAA
SA
SA
SA
SA
SA
SS ation SSSSSSS

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment.
How frequently did you assess clients of different cultural backgrounds about each cultural factor?
Please use the scale below and mark your response accordingly.If the opportunity to conduct an assessment of the listed area was unavailable, please mark A.If the opportunity to conduct an assessment of the listed area was available, but diverse clients were unavailable,mark B.
Area DiverseNot Clients
← →Available Not Available Never Always� � � � � � � �
You assessed clients of different backgrounds about: (Mark one choice for each item.)
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception and orientation � � � � � � � �(32) racial background and identity � � � � � � � �(33) ethnic background and identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background and identity � � � � � � � �(36) educational background and interests � � � � � � � �(37) religious practices and beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health and illness beliefs � � � � � � � �(46) folk medicine tradition and use � � � � � � � �(47) gender role and responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination and bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
A M P
L EE�
� �� �
E� �� � �� � �
L E� �� � ��
L�� � �� �
PL� �
� � � �� � �
P� � ��
MP�
MM� ��
MP
MMMM�MMMMMA
MMMMA
MA
MA
MMMA
MA
MMA AA
SAAA
SAAA
S SA
xperiencesSS

Part III: What affective learning outcomes did you gain as a result of the cultural competence education program?
Specifically, to what extent did you develop new, culturally sensitive and professionally appropriate attitudes, values,or beliefs OR further develop culturally sensitive and professionally appropriate attitudes, values and beliefs about theitems below?
For Section A, please use the scale below and mark your response accordingly. (Mark one choice for each item).
Not To aAt
← →Great
All Extent� � � � � � � �
(A) About Yourself: As a result of the cultural competence education program, you developed a greater AWARENESS OF:
(54) YOUR OWN cultural heritage and belief systems � � � � � � � �(55) YOUR OWN biases and limitations � � � � � � � �(56) differences within YOUR OWN cultural group � � � � � � � �
For Section B, please use the scale below and mark your response accordingly. (Mark one choice for each item.)
Diverse Not To aClients At
← →Great
Not Available All Extent� � � � � � � �
(B) Among clients of different cultural backgrounds,
As a result of the cultural competence education program, you became MORE AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a � � � � � � � �
culturally different world(62) interaction between nursing, folk, and professional systems � � � � � � � �
As a result of the cultural competence education program, you became MORE ACCEPTING OF:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
As a result of the cultural competence education program, you became MORE APPRECIATIVE OF:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) cultural-specific nursing care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
© Springer Publishing Company
M P L
EE�
ingly. (Mark one choMark one ch
ttAt
le All ←←� � �� �
Pbecamecame MORE AWAREWARE
M MMS A
MMMAM
A g a
lk, and professional systssion
petence education prograetence education progrSproupsroupsS

Among clients of different cultural backgrounds,
Diverse Not To aClients At
← →Great
Not Available All Extent� � � � � � � �
As a result of the cultural competence education program, you now MORE READILY RECOGNIZE:
(71) inadequacies in the nation’s health care system � � � � � � � �(72) importance of home remedies and folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
As a result of the cultural competence education program, you became a MORE COMMITTED ADVOCATE FOR:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) cultural-specific care � � � � � � � �
© Springer Publishing Company
L E� ��
E� �
� � � �� �E� � �
S A M
P L
TTED ADVOCATE FORTTED ADVOCATE FOR
PL� � �
� � �� � �

I T E M 6
Cultural Competence Clinical Evaluation Tool—Agency Evaluator Version(CCCET-AEV)
DESCRIPTIONAn 83-item questionnaire adapted from the TSET, containing three subscales measuring different dimensions of clin-ical cultural competence behaviors as rated by the agency evaluator:
� Extent of culturally specific care (Subscale 1)� Cultural assessment (Subscale 2)� Culturally sensitive and professionally appropriate attitudes, values, or beliefs including awareness, accep-
tance, recognition, appreciation, and advocacy necessary for providing culturally sensitive professional nurs-ing care (Subscale 3).
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about CCCET, administration, uses, and scoring in Teaching Cultural Competence in Nurs-
ing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.(4) Please send study results (see Toolkit Item 21) to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department,2800 Victory Boulevard, Staten Island, New York 10314, USA.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
Compare with employee ratings on CCCET-EV.
� Use to determine baseline information, identify areas of strengths, weaknesses, and gaps, and to evaluatechange following educational intervention and/or increased exposure to culturally diverse clients and/or in-creased exposure to the clinical topic/area not previously available.
� May be used together with CCCET-EV (employees and agency evaluators independently complete the CCCETat the end of the clinical orientation or preceptor experience).
� Results can be used to guide educational changes.� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
S A M
P L
Erinrin
values, or beliefs iniefs inr providing culturallprov
posting online and aosting onlination, uses, and scoruses, an
ovation (2010)vation (2010) beforbefrn the questionnairee questionnaire
t Item 21) to:Item 21) to:ty University of Newniversity of New
n Island, New York 1New York
y and percent) for inercent) for inee ratings on CCCETn C
ne baseline informae baseline informang educational intg educationaSto the cliniche clinic
r withr with

Throughout one’s nursing career, nurses will be caring for clients of many different cultural backgrounds. Theseclients will represent various racial, ethnic, gender, socioeconomic, and religious groups. Culturally specific carerequires that nurses know, understand, and identify cultural factors related to client care and conduct their nursingpractice accordingly.
Part I: For clients of different cultural backgrounds, to what extent did the nurse provide culturally specific care?
Please use the scale below and mark your response accordingly.
If the opportunity to provide care in the listed area was unavailable, please mark A.If the opportunity to provide care in the listed area was available, but diverse clients were unavailable, mark B.If you are unable to evaluate the nurse, please leave item blank.
Area Diverse NotNot Clients At ← →
Available Not Available All Totally� � � � � � � �
During the designated evaluation period, the nurse provided culturally specific care in the following areas: (Mark one choice per item.)
(1) health history and interview � � � � � � � �(2) physical examination � � � � � � � �(3) informed consent � � � � � � � �(4) health promotion � � � � � � � �(5) illness prevention � � � � � � � �(6) health maintenance � � � � � � � �(7) health restoration � � � � � � � �(8) safety � � � � � � � �(9) exercise and activity � � � � � � � �
(10) pain relief and comfort � � � � � � � �(11) diet and nutrition � � � � � � � �(12) patient teaching � � � � � � � �(13) hygiene � � � � � � � �(14) anxiety and stress reduction � � � � � � � �(15) diagnostic tests � � � � � � � �(16) blood tests � � � � � � � �(17) pregnancy � � � � � � � �(18) birth � � � � � � � �(19) growth and development � � � � � � � �(20) aging � � � � � � � �(21) dying and death � � � � � � � �(22) grieving and loss � � � � � � � �(23) life support and resuscitation � � � � � � � �(24) sexuality � � � � � � � �(25) rest and sleep � � � � � � � �
© Springer Publishing Company
SA M
P L
EEg areas: (Mark og areas: (Mar
L E�� � ��L�� � �� �
PL� �
� � �� � �
P� �� � � ��
MP�
� � �� � �
MP� �
MM� ��MMM� �
AM
AM��
AM
AM
AM�
AAAM
AM��A AAAAAAAA
SA
SA
SAAA
SA
SA
S SA
SSSSSSSSS

Part II: The most effective way to identify specific cultural factors that influence client behavior is to conduct a cultural assessment.
How frequently did the nurse assess clients of different cultural backgrounds about each cultural factor?
Please use the scale below and mark your response accordingly.If the opportunity to conduct an assessment of the listed area was unavailable, please mark A.If the opportunity to conduct an assessment of the listed area was available, but diverse clients were unavailable,mark B.If you are unable to evaluate the nurse, please leave item blank.
Area DiverseNot Clients ← →Available Not Available Never Always
� � � � � � � �
During the designated evaluation period, the nurse assessed clients of different backgrounds about: (Mark one choice per item.)
(26) language preference � � � � � � � �(27) level of English comprehension � � � � � � � �(28) meaning of verbal communication patterns � � � � � � � �(29) meaning of nonverbal behaviors � � � � � � � �(30) meanings of space and touch � � � � � � � �(31) time perception and orientation � � � � � � � �(32) racial background and identity � � � � � � � �(33) ethnic background and identity � � � � � � � �(34) socioeconomic background � � � � � � � �(35) religious background and identity � � � � � � � �(36) educational background and interests � � � � � � � �(37) religious practices and beliefs � � � � � � � �(38) acculturation � � � � � � � �(39) world view (philosophy of life) � � � � � � � �(40) attitudes about health care technology � � � � � � � �(41) ethnic food preferences � � � � � � � �(42) role of elders � � � � � � � �(43) role of children � � � � � � � �(44) financial concerns � � � � � � � �(45) traditional health and illness beliefs � � � � � � � �(46) folk medicine tradition and use � � � � � � � �(47) gender role and responsibility � � � � � � � �(48) acceptable sick role behaviors � � � � � � � �(49) role of family during illness � � � � � � � �(50) discrimination and bias experiences � � � � � � � �(51) home environment � � � � � � � �(52) kinship ties � � � � � � � �(53) aging � � � � � � � �
© Springer Publishing Company
SA M
P L
EE�
� � �� �E� � �� � � �� �
L E�� � � �� � � �L � � �� � � �� �
PL� � � �
� � ��P � ��
MP
MM�
MM�
MMMMMMM�
AMMMMM
AM
AMMM
AM
AM
AMMM
AAA AAS
AAAS
Aors ASesss S xperiencesS
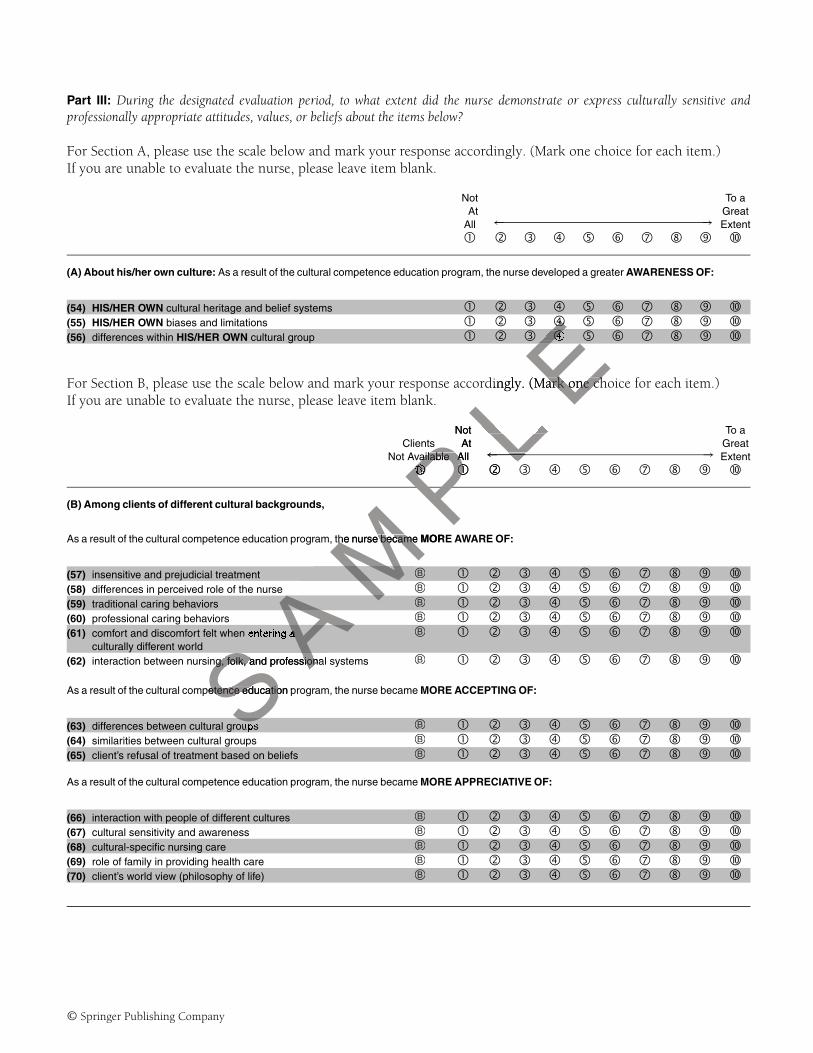
Part III: During the designated evaluation period, to what extent did the nurse demonstrate or express culturally sensitive andprofessionally appropriate attitudes, values, or beliefs about the items below?
For Section A, please use the scale below and mark your response accordingly. (Mark one choice for each item.)If you are unable to evaluate the nurse, please leave item blank.
Not To aAt
← →Great
All Extent� � � � � � � �
(A) About his/her own culture: As a result of the cultural competence education program, the nurse developed a greater AWARENESS OF:
(54) HIS/HER OWN cultural heritage and belief systems � � � � � � � �(55) HIS/HER OWN biases and limitations � � � � � � � �(56) differences within HIS/HER OWN cultural group � � � � � � � �
For Section B, please use the scale below and mark your response accordingly. (Mark one choice for each item.)If you are unable to evaluate the nurse, please leave item blank.
Not To aClients At
← →Great
Not Available All Extent� � � � � � � �
(B) Among clients of different cultural backgrounds,
As a result of the cultural competence education program, the nurse became MORE AWARE OF:
(57) insensitive and prejudicial treatment � � � � � � � �(58) differences in perceived role of the nurse � � � � � � � �(59) traditional caring behaviors � � � � � � � �(60) professional caring behaviors � � � � � � � �(61) comfort and discomfort felt when entering a � � � � � � � �
culturally different world(62) interaction between nursing, folk, and professional systems � � � � � � � �
As a result of the cultural competence education program, the nurse became MORE ACCEPTING OF:
(63) differences between cultural groups � � � � � � � �(64) similarities between cultural groups � � � � � � � �(65) client’s refusal of treatment based on beliefs � � � � � � � �
As a result of the cultural competence education program, the nurse became MORE APPRECIATIVE OF:
(66) interaction with people of different cultures � � � � � � � �(67) cultural sensitivity and awareness � � � � � � � �(68) cultural-specific nursing care � � � � � � � �(69) role of family in providing health care � � � � � � � �(70) client’s world view (philosophy of life) � � � � � � � �
© Springer Publishing Company
P L E
��
E�
dingly. (Mark one chark one ch
Nots At
ailable Allailable All ←
PP
SA M
P� ��P
the nurse becamethe nurse became MORE
AM
AM
SAa
S Ang, folk, and professionang, folk, and profession
petence education petence educatioS

Among clients of different cultural backgrounds,
Not To aClients At
← →Great
Not Available All Extent� � � � � � � �
As a result of the cultural competence education program, the nurse now MORE READILY RECOGNIZES:
(71) inadequacies in the nation’s health care system � � � � � � � �(72) importance of home remedies and folk medicine � � � � � � � �(73) impact of roles on health care practices � � � � � � � �(74) impact of values on health care practices � � � � � � � �(75) impact of socioeconomic factors on health care practices � � � � � � � �(76) impact of political factors on health care practices � � � � � � � �(77) need for cultural care preservation/maintenance � � � � � � � �(78) need for cultural care accommodation/negotiation � � � � � � � �(79) need for cultural care repatterning/restructuring � � � � � � � �(80) need to prevent ethnocentric views � � � � � � � �(81) need to prevent cultural imposition � � � � � � � �
As a result of the cultural competence education program, the nurse became a MORE COMMITTED ADVOCATE FOR:
(82) client’s decisions based on cultural beliefs � � � � � � � �(83) cultural-specific care � � � � � � � �
© Springer Publishing Company
L E� ��
E� �
� � � �� �E� � �
S A M
P L
OMMITTED ADVOCATEOMMITTED ADVOCATE
PL� � �
� � �� � �

I T E M 7
Clinical Setting Assessment Tool—Diversity and Disparity (CSAT-DD)
DESCRIPTIONA demographic tool to collect data about the clinical practicum/agency site, specifically focusing on descriptions ofdiverse client populations (Part I) and clinical problems targeting the 28 focus areas of the Healthy People 2010document (Part II).
The first page gathers information about the type of agency (e.g., private, public, etc.) and whether the instruc-tor/preceptor/agency evaluator completed a college-level course and/or continuing education (CE) units in transcul-tural nursing or cultural competence in health care.
The 15 items in Part I gather information about the demographic makeup of the client population (age, ethnicity,languages spoken, religion, etc.) as well as identifying the most prevalent characteristics represented.
Part II (28 items) identifies the five most frequent focus areas evident in the clinical setting.
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about CSAT-DD, administration, uses, and scoring in Teaching Cultural Competence in
Nursing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) Please be sure that all respondents return the questionnaire.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
This tool is intended for descriptive use but could be used to examine the relationship between select variableson the CSAT-DD and other items or scores on the TSET and/or CCCET. Information can be used to evaluate amountand type of exposure of student/learner/nurse to culturally diverse clients and Healthy People 2010 focus areas.
� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
S A M
P L
Epublic, etc.)public, etctinuing educationuing education
makeup of the clientmakeup of the clienvalent characteristiclent c
eas evident in the client in the cl
or posting online andting onlministration, uses, aninistration, uses
and Innovation (2010Innovation (2010turn the questionnaiturn the questio
d percent) for individpercent) for indiviscriptive use but coptive use but
ms or scores on theores on theudent/learner/nurse tudent/learner/nur
book resources: Chbook resourcSS

Preceptor or Clinical Instructor Name:
Clinical Practicum Information
Site or Agency Name:
Address:
Type of agency (Choose one)© Public © Nonsectarian/nonprofit© Private, for profit © Health service© Religious, nonprofit © School© Government agency © Other
(A) Did preceptor/clinical instructor complete a college-level course in transcultural nursingor cultural competence in health care?
© Yes © No
(B) Did preceptor/clinical instructor complete continuing education (CE) units in transculturalnursing or cultural competence in health care?
© Yes © No
The makeup of the client population:
Included in clientpopulation (select allthat apply)
Was most prevalent inclient population (select1 for each item)
1. SexMaleFemale
©©
©©
2. Age groupsInfantsChildrenAdolescentsYoung adultsMiddle-aged adultsOlder adultsElderlyOlder old
©©©©©©©©
©©©©©©©©
3. LanguageEnglish-speakingNon-English-speakingEnglish as a second (other) languageAmerican sign languageBraille
©©©©©
©©©©©
4. Citizenship StatusU.S.- born citizenNaturalized U.S. citizenImmigrantRefugeeUndocumented individual
©©©©©
©©©©©
5. LiteracyAdults able to read and write EnglishAdults able to read and write a language other than EnglishAdults unable to read and write any language
©©©
©©©
© Springer Publishing Company
PL E
©© No
PL
MPP
Included in clieded in clipopulation (tionthat applyP
S A M
MS

Included in clientpopulation (select allthat apply)
Was most prevalent inclient population (select1 for each item)
6. Highest Education of AdultsNever attended schoolSome elementary schoolElementary school graduate (grade 8)Some high schoolHigh school graduateSome collegeCollege graduate
©©©©©©©
©©©©©©©
7. Employment Status of AdultsEmployed full-timeEmployed part-timeUnemployed
©©©
©©©
8. Health Insurance StatusUninsuredPrivate insuranceMedicaidMedicareOther
©©©©©
©©©©©
9. Ethnicity or RaceAmerican Indian or Alaskan NativeAsian (Chinese, Filipino, Japanese, Korean, Asian Indian, Thai)Other AsianBlack or African AmericanHispanic or LatinoNative Hawaiian or Other Pacific IslanderWhite, non-HispanicMultiracialOther
©©©©©©©©©
©©©©©©©©©
10. ReligionsNone (atheist or agnostic)BuddhistChristianHinduJewishMuslimOther
©©©©©©©
©©©©©©©
11. Marital StatusSingleSingle, living with partnerMarriedDivorced or separatedWidowedOther
©©©©©©
©©©©©©
12. Income StatusPovertyLow incomeMiddle-class incomeHigh income
©©©©
©©©©
13. Residential AreaUrbanSuburbanRural
©©©
©©©
© Springer Publishing Company
L EEE
M P L P
©©
©©©
L©©©©
S A M
©©
MS

Included in clientpopulation (select allthat apply)
Was most prevalent inclient population (select1 for each item)
14. Type of ResidenceApartmentHouseCondominium or co-opFarmSingle-room occupancy housingLow-income subsidized housingTrailerIndian reservationMilitary basePrisonShelterGroup homeDormitoryHomelessOther
©©©©©©©©©©©©©©©
©©©©©©©©©©©©©©©
15. Health StatusHealthyAcutely ill (physical)Acutely ill (mental)Chronically ill (physical)Chronically ill (mental)Other
©©©©©©
©©©©©©
What was the most frequent focus area during this clinical practicum experience?
Number 1most frequent(Mark 1 from the list)
The 4 nextmost frequent(Mark 4 from the list)
1. Access to quality health services2. Arthritis, osteoporosis, and chronic back pain3. Cancer4. Chronic kidney disease5. Diabetes6. Disability and secondary conditions7. Educational and community-based programs8. Environmental health9. Family planning
10. Food safety11. Health communication12. Heart disease and stroke13. HIV14. Immunization and infectious diseases15. Injury and violence prevention16. Maternal, infant, and child health17. Medical product safety18. Mental health and mental disorders19. Nutrition and overweight20. Occupational safety and health21. Oral health22. Physical activity and fitness23. Public health infrastructure24. Respiratory diseases25. Sexually transmitted diseases26. Substance abuse27. Tobacco use28. Vision and hearing
©©©©©©©©©©©©©©©©©©©©©©©©©©©©
©©©©©©©©©©©©©©©©©©©©©©©©©©©©
© Springer Publishing Company
S A M
P L
EP
EE©©©©©©©
Pthis clinical practicuical p
MP
AM
nic back painback pain
ary conditionsary condommunity-based programmunity-based p
h

I T E M 8
Demographic Data Sheet—Undergraduate (DDS-U)
DIRECTIONSAdminister along with other questionnaire(s) to gather demographic information from undergraduate (pre-licensure)students.
INSTRUCTIONS FOR RESEARCHERS(1) Detach this cover sheet before photocopying or posting online and administration to sample.(2) Review information about DDS-U, administration, uses, and scoring in Teaching Cultural Competence in Nursing
and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.(3) DDS-U may be adapted to individualize with course numbers, course names, and other desired demographic
data.(4) Please be sure that all respondents return the questionnaire.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
� Can be used to describe sample characteristics (frequency and percent)� Can be used to create comparison groups based on select demographic categories for comparing scores and
data on the TSET, CCCET, CSAT-DD, and other assessment tools� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
MP L
Eadministration to sinistration to sring in Teaching Cultuhing Cultu
study design and dastudy design and dabers, course names,, course name
onnaire.onnaire.
ndividual and aggregdividual and aggr
AM cteristics (frequencycteristics (frequ
groups based on seloups based on seT-DD, and other assnd other a
es: Chapters 4, 5.es: Chapters 4, 5.
S A A
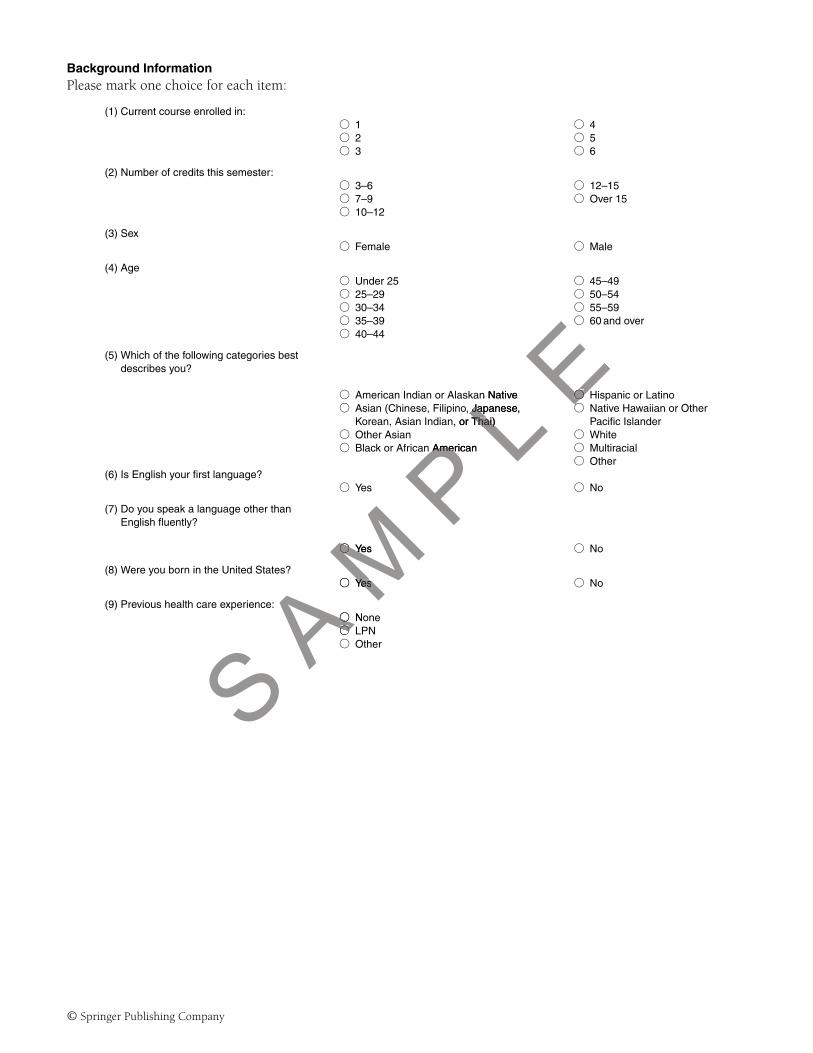
Background InformationPlease mark one choice for each item:
(1) Current course enrolled in:© 1 © 4© 2 © 5© 3 © 6
(2) Number of credits this semester:© 3–6 © 12–15© 7–9 © Over 15© 10–12
(3) Sex© Female © Male
(4) Age© Under 25 © 45–49© 25–29 © 50–54© 30–34 © 55–59© 35–39 © 60 and over© 40–44
(5) Which of the following categories bestdescribes you?
© American Indian or Alaskan Native © Hispanic or Latino© Asian (Chinese, Filipino, Japanese,
Korean, Asian Indian, or Thai)© Native Hawaiian or Other
Pacific Islander© Other Asian © White© Black or African American © Multiracial
© Other(6) Is English your first language?
© Yes © No
(7) Do you speak a language other thanEnglish fluently?
© Yes © No
(8) Were you born in the United States?© Yes © No
(9) Previous health care experience:© None© LPN© Other
© Springer Publishing Company
S A M
P L
En Native ©©, Japanese,Ja
, or Thai)Thai)©©
AmericanAme
©© YesY
© YesYes
e:©© No©©©

I T E M 9
Demographic Data Sheet—Nurses (DDS-N)
DIRECTIONSAdminister along with other questionnaire(s) to gather demographic information from nurses working in clinicalagencies and/or enrolled in RN-BS and graduate (master’s and doctoral) programs.
INSTRUCTIONS FOR RESEARCHERS1. Detach this cover sheet before photocopying or posting online and administration to sample.2. Review information about DDS-N, administration, uses, and scoring in Teaching Cultural Competence in Nurs-
ing and Health Care: Inquiry, Action, and Innovation (2010) before study design and data collection.3. DDS-N may be adapted to individualize with other desired demographic data.4. Please be sure that all respondents return the questionnaire.
EASY SCORINGDescriptive statistics (frequency and percent) for individual and aggregate data.
� Can be used to describe sample characteristics (frequency and percent)� Can be used to create comparison groups based on select demographic categories for comparing scores and
data on the TSET, CCCET, CSAT-DD, and other assessment tools� Supplementary book resources: Chapters 4, 5.
© Springer Publishing Company
P L Eadministration to sinistration to s
oring in Teaching Culching Cuoreore study design andand
d demographic dataemographic dnaire.
AM Pvidual and aggregateand ag
ristics (frequency anics (frequency anoups based on selectups based on
DD, and other assess, and other asses
S A MChapters 4, 5.rs 4, 5.
AM

Please mark one choice for each item:
(1) Sex© Female © Male
(2) Age
© Under 25 © 45–49© 25–29 © 50–54© 30–34 © 55–59© 35–39 © 60 and over© 40–44
(3) Which of the following categories bestdescribes you?
© American Indian or Alaskan Native © Hispanic or Latino© Asian (Chinese, Filipino, Japanese,
Korean, Asian Indian, or Thai)© Native Hawaiian or Other
Pacific Islander© Other Asian © White© Black or African American © Multiracial
© Other
(4) Is English your first language?
© Yes © No
(5) Do you speak a language other than Englishfluently?
© Yes © No
(6) Were you born in the United States?
© Yes © No
(7) Are you employed full-time in nursing?
© Yes © No
(8) Are you employed part-time in nursing?
© Yes © No
(9) Health care setting in which you presently work.(If you work in more than one setting, selectyour primary setting)
© hospital (acute care) © school© hospital (chronic care) © occupational health© clinic © school of nursing© nursing home © hospice© home care © veteran’s administration© public health department © military base© Indian health service © college health service© physician’s office © other
(10) Clinical area in which you presently work.(If you work in more than one area, select yourprimary work area.)
© medical-surgical © geriatric© oncology © rehabilitation© psychiatric © substance abuse© obstetrics, maternity, newborn © HIV and AIDS© pediatrics © community health© emergency © palliative care© intensive care © other
© Springer Publishing Company
©© NN
YesYes
©© Yess
work.elect
©

(11) Nursing position that you currently hold.(If you have more than one position, selectyour primary position.)
© staff RN © nurse entrepreneur© assistant head nurse © research nurse© nurse manager/head nurse © public health nurse© nurse educator © visiting nurse© nurse administrator/supervisor © clinical nurse leader (CNL)© clinical nurse specialist (CNS) © none (unemployed)© nurse practitioner (NP) © other
(12) Nursing position that you would like in thefuture:
© staff RN © nurse entrepreneur© assistant head nurse © research nurse© nurse manager/head nurse © public health nurse© nurse educator © visiting nurse© nurse administrator/supervisor © clinical nurse leader (CNL)© clinical nurse specialist (CNS) © other© nurse practitioner (NP)
(13) How many years have you been licensed as aregistered nurse?
© Under 2 © 20–24© 2–4 © 25–29© 5–9 © 30–34© 10–14 © 35–39© 15–19 © 40 or more
(14) What type of initial nursing program did youcomplete?
© associate degree (university based) © master’s degree© associate degree (hospital based) © other program (foreign)© diploma program (hospital based) © other program (U.S.)© baccalaureate degree
(15) How many years ago did you complete abaccalaureate degree in nursing?
© Currently enrolled in a BS program© Under 5
© Not enrolled in a BS program© 15–19
© 5–9 © 20–25© 10–14 © 25 or more
(16) Did you complete a previous college course intranscultural nursing or cultural competence inhealth care?
© Yes, undergraduate level only © Yes, graduate level only© Yes, undergraduate and graduate level © None
(17) Did you complete continuing educationunits in transcultural nursing or culturalcompetence in health care?
© Yes, inservices at my job only © None© Yes, online or mailed CE only© Yes, conferences only© Yes, 2 or more of the above© All of the above
© Springer Publishing Company
SA M
P L
E©© 22©©
ociate degree (universitygree (ussociate degree (hospitassociate degree (ho
diploma program (hosploma program (hos© baccalaureate degrccalaure
© CurrentCurre© Unded©© 5–
S ©©us college course inus college course in
cultural competence incultural competence in
I T E M 1 0
Self-Assessment Tool—Academic (SAT-A)
USER INFORMATION� Used to help individual faculty members, administrators, and the organization assess various dimensions that
can impact upon cultural competence in the academic setting� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities� Supplementary book resources: Chapter 6, Table 1.2 and Figure 6.2
© Springer Publishing Company
S A M
P L
Eesses, gaps in knows, gaps in kno
ure 6.2L

Self-Assessment Tool—Academic (SAT-A)
Self-Assessment Question Your Response
1. What are your own cultural values and beliefs (CVB)?
2. What do you know about students’ CVB?
3. How did you know about students’ CVB?
4. What values and beliefs do you expect from students?
5. How do you feel when a student’s CVB are different from yours?
6. What actions do you take when a student’s CVB are different from yours?
7. How do/could different CVB affect the student’s relationship with you,other nursing faculty, nurses, and peers?
You:Other nursing faculty:Nurses:Peers:
8. How do/could different CVB affect the student’s cultural competencedevelopment, academic outcomes, satisfaction, stress, persistence, andretention?
Cultural competence development:Academic outcomes:Satisfaction:Stress:Persistence:Retention:
9. How confident are you about your current knowledge, skills, values, andattitudes when interacting with, teaching, and advising culturally differentstudents?
Interacting with:Teaching:Advising:
10. What is your motivation for engaging in the process of becoming culturallycompetent?
11. What is your level of commitment in developing cultural competence inyourself, peers, administrators, and students?
Yourself:Peers:Administrators:Students:
12. What are your strengths, weaknesses, gaps in knowledge, values, goalsand priorities concerning cultural competence development?
Strengths:Weaknesses:Gaps in knowledge:Values:Goals:Priorities:
13. How confident are you about learning new transcultural nursing skillswhen interacting with, teaching, and advising culturally different students?
Interacting with:Teaching:Advising:
14. How confident are you about performing new transcultural nursing skillswhen interacting with, teaching, and advising culturally different students?
Interacting with:Teaching:Advising:
15. How confident are you that you will actively advocate for culturalcompetence development in the academic setting?
© Springer Publishing Company
M P L
EP
Ling faculty:ing faculty
s: ECultural competenceenceAcademic outcomeSatisfaction:Satisfaction:Stress:StresPersistencsistencRetentiotiPkills, values, ands, and
g culturally differentculturally different
MS
A Mprocess of becoming cuocess of becoming cu
AMin developing cultural con developing cultural c
and students?students?
SA
SA
engths, weaknesses, gagths, weaknessSerning cultural compning cultural co

I T E M 1 1
Self-Assessment Tool—Health Care Institutions (SAT-HCI)
USER INFORMATION� Used to help individual staff nurse, nurse manager, nurse educator, nurse executive, administrator, and the
organization assess various dimensions that can impact upon cultural competence in the health care setting� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities� Supplementary book resources: Chapter 10, Table 1.2 and Figure 10.2
© Springer Publishing Company
L Eesses, gaps in knows, gaps in kno
gure 10.2
S A M
P L L

Self-Assessment Tool—Health Care Institutions (SAT-HCI)
Self-Assessment Question Your Response
1. What are your own1 cultural values and beliefs (CVB)?
2. What do you know about the CVB of health care consumers2?
3. What do you know about the CVB of your peers, supervisors, and othermembers of the health care team3?
Your peers:Supervisors:Other members of the health care team:
4. How did you know about the CVB of others?
5. What values and beliefs do you expect from your peers, supervisors, andother members of the health care team?
Your peers:Supervisors:Other members of the health care team:
6. How do you feel when the CVB of health care consumers are differentfrom yours?
7. What actions do you take when a supervisor’s CVB are different fromyours?
8. How do/could different CVB affect a nurse’s relationship with you, peers,and other members of the health care team?
You:Peers:Other members of the health care team:
9. How do/could different CVB affect a nurse’s cultural competencedevelopment, satisfaction, stress, persistence, and retention?
Cultural competence development:Satisfaction:Stress:Persistence:Retention:
10. How confident are you about your current knowledge, skills, values, andattitudes when interacting with, caring for, and advising culturally differentconsumers?
Interacting with:Caring for:Advising:
11. How confident are you about your current knowledge, skills, values, andattitudes when interacting with, collaborating, and performing your worktasks with culturally different members of the health care team?
Interacting with:Collaborating:Performing work tasks:
12. What is your motivation for engaging in the process of becoming culturallycompetent?
13. What is your level of commitment in developing cultural competence inyourself, peers, administrators, and others?
Yourself:Peers:Administrators:Others:
14. What are your strengths, weaknesses, gaps in knowledge, values, goals,and priorities concerning cultural competence development?
Strengths:Weaknesses:Gaps in knowledge:Values:Goals:Priorities:
1Own refers to individual staff nurses, nurse manager, executive, administrator, educator, or organization.2Health care consumers refer to individual patients, families, and communities.3Other members of the health care team include professional and unlicensed health care providers.
© Springer Publishing Company
M P L
EP
L EELers, You:You:Peers:ers:Other mPpetence
tention?entio
SA M
C
Mrent knowledge, skills, ve, skills, ving for, and advising cultng for, and advising cu
About your current knowleentting with, collaborating, ating with, collaboratin
y different members of thdifferent members of thS Son for engagingr engagin
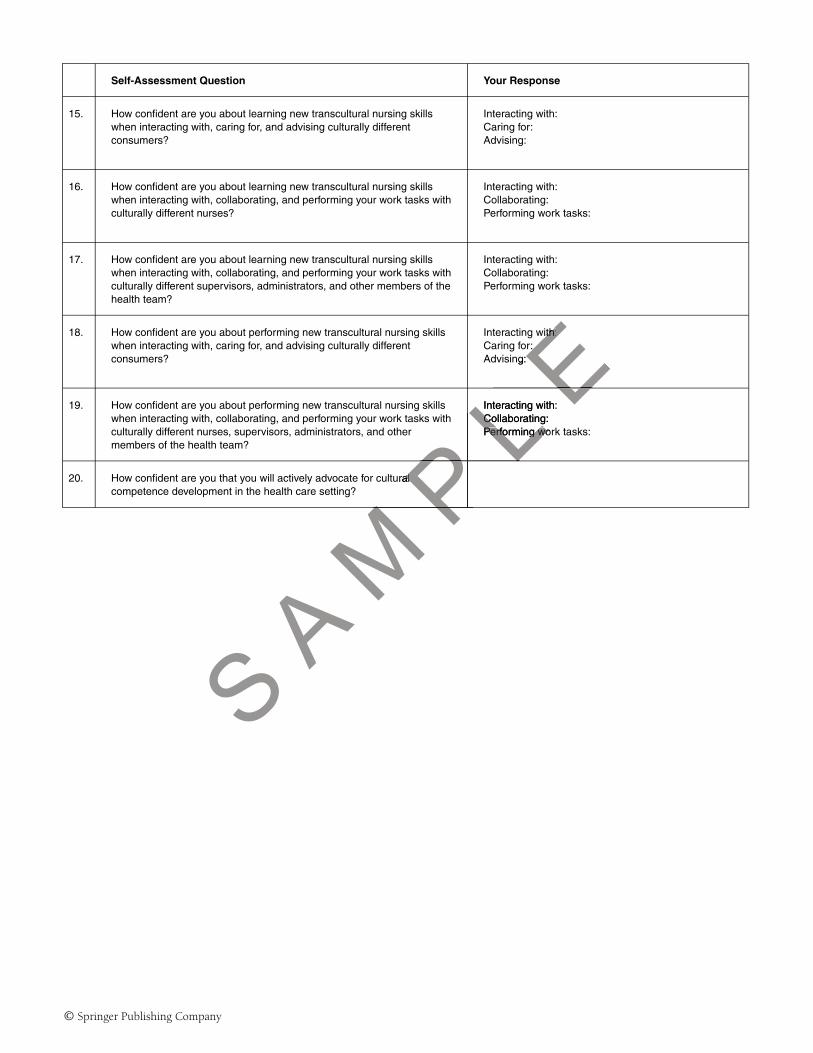
Self-Assessment Question Your Response
15. How confident are you about learning new transcultural nursing skillswhen interacting with, caring for, and advising culturally differentconsumers?
Interacting with:Caring for:Advising:
16. How confident are you about learning new transcultural nursing skillswhen interacting with, collaborating, and performing your work tasks withculturally different nurses?
Interacting with:Collaborating:Performing work tasks:
17. How confident are you about learning new transcultural nursing skillswhen interacting with, collaborating, and performing your work tasks withculturally different supervisors, administrators, and other members of thehealth team?
Interacting with:Collaborating:Performing work tasks:
18. How confident are you about performing new transcultural nursing skillswhen interacting with, caring for, and advising culturally differentconsumers?
Interacting with:Caring for:Advising:
19. How confident are you about performing new transcultural nursing skillswhen interacting with, collaborating, and performing your work tasks withculturally different nurses, supervisors, administrators, and othermembers of the health team?
Interacting with:Collaborating:Performing work tasks:
20. How confident are you that you will actively advocate for culturalcompetence development in the health care setting?
© Springer Publishing Company
PL E
P
with:ith:r:
ng:
L EInteracting with:Collaborating:Co
MP LP
S A M
PPerforming worPerforming wo
PL
uralal
MP

I T E M 1 2
Self-Assessment Tool—Professional Associations (SAT-PA)
USER INFORMATION� Used to help individual members, elected officers, administrators, association leaders, and the organization
assess various dimensions that can impact upon cultural competence in the professional association� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Self-assessment should conclude with a listing of strengths, weaknesses, gaps in knowledge, goals, commit-
ment, desire, motivation, and priorities� Supplementary book resources: Chapter 13, Table 1.2 and Figure 13.2
© Springer Publishing Company
L Epp
esses, gaps in knows, gaps in kno
gure 13.2
S A M
P L L

Self-Assessment Tool—Professional Associations (SAT-PA)
Self-Assessment Question Your Response
1. What are your own1 cultural values and beliefs (CVB)?
2. What do you know about the CVB of the professional associationmembers?
3. What do you know about CVB of your peers, general members, electedofficers, and other members of the professional association’s (PA)leadership team?
Peers:General members:Elected officers:PA leadership team:
4. How did you know about the CVB of others?
5. What values and beliefs do you expect from your peers, generalmembers, elected officers, and other members of the professionalassociation’s leadership team?
Peers:General members:Elected officers:PA leadership team:
6. How do you feel when the CVB of your peers and general members aredifferent from your own?
You:Peers:
7. What actions do you take when elected officers and other members of theprofessional association’s leadership team’s CVB are different fromyours?
8. How do/could different CVB affect a member’s relationship with you,peers, and other members of the professional association?
You:Peers:Other members of the professional association:
9. How do/could different CVB affect a member’s cultural competencedevelopment, satisfaction, stress, participation, and retention?
Cultural competence development:Satisfaction:Stress:Participation:Retention:
10. How confident are you about your current cultural knowledge, skills,values, and attitudes when interacting with, advising, and mentoringculturally different new members?
Interacting with:Advising:Mentoring:
11. How confident are you about your current cultural knowledge, skills,values, and attitudes when interacting with, collaborating, and performingyour association tasks with culturally different members of theprofessional association?
Interacting with:Collaborating:Performing tasks:
12. What is your motivation for engaging in the process of becoming culturallycompetent?
13. What is your level of commitment for facilitating the development ofcultural competence in yourself, peers, general members, electedofficers, and others?
Yourself:Peers:General members:Elected officers:Others:
1Own refers to the individual, nurse manager, executive, administrator, elected officer, educator, or organization/association.
© Springer Publishing Company
AM P
L E
PL
bersberscers:cers
ership team:ership team:EYou:Peers:
Lof theof thomm
Pship with you,ship with you,ciation?tion?
Mber’s cultural competenccultural competenc
S A Mcipation, and retention?d retention?
Aabout your current culturabout your current cwhen interacting with, awhen interacting with,
new members?ew members?Sabout your cbout yourn intern inte

Self-Assessment Question Your Response
14. What are your strengths, weaknesses, gaps in knowledge, values, goals,and priorities concerning cultural competence development?
Strengths:Weaknesses:Gaps in knowledge:Values:Goals:Priorities:
15. How confident are you about learning new transcultural skills wheninteracting with, advising, and mentoring culturally different newmembers?
Interacting with:Advising:Mentoring:
16. How confident are you about learning new transcultural skills wheninteracting with, collaborating, and performing your association tasks withculturally different members, elected officers, administrators, and othermembers of the professional association’s leadership team?
Interacting with:Collaborating:Performing tasks:
17. How confident are you about performing new transcultural skills wheninteracting with, advising, and mentoring culturally different newmembers?
Interacting with:Advising:Mentoring:
18. How confident are you about performing new transcultural skills wheninteracting with, collaborating, and performing your association tasks withculturally different members?
Interacting with:Collaborating:Performing tasks:
19. How confident are you about performing new transcultural skills wheninteracting with, collaborating, and performing your association tasks withculturally different members, elected officers, administrators, and othermembers of the professional association’s leadership team?
Interacting with:Collaborating:Performing tasks:
20. How confident are you that you will actively advocate for culturalcompetence development in the professional association?M P
L E
PEting with:ng wit
ising:Mentoring:
Ls withwithInteracting withInteracting witCollaboratinllaboratinPerforminrmin
P
S A M
ral skills whenral skills whenssociation tasks withociation tasks with
ministrators, and othertors, anership team?ership team?Mvely advocate for culturate for cultura
essional association?essional association?
A
I T E M 1 3
Active Promoter Assessment Tool—Academic (APAT-A)
USER INFORMATION� Used to help individuals, groups, and organizations
� Appraise values, beliefs, and actions concerning cultural competence development� Determine whether or not one is an optimal active role model in cultural competence development within
the academic institution� Identify factors restricting cultural competence development� Plan and coordinate future active promoter actions toward achieving optimal cultural competence
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Supplementary book resources: Chapter 6 and Table 6.1
© Springer Publishing Company
PL E
al comal co
hieving optimaltimal cultucultu
ms
S A M
P LPL

Part 1 Directions1. Check “yes” or “no” for each value, belief, and action.2. Check “yes” or “no” for each active promoter action.3. Review and reflect.4. Proceed to Part 2.
Values, Beliefs, and Actions Active Promoter of Cultural Competence Development
Yes No Yes No
1. Views cultural competence as important inown life
and shares beliefs with students∗
2. Views cultural competence as important instudents’ education, professionaldevelopment, and future practice
and shares view with students
3. Views own nurse educator role to includeactive involvement in promoting culturalcompetence development among students
and shares view with students
4. Routinely updates own knowledge and skillsto enhance cultural competence
and shares relevant information with students
5. Attends professional events concerningcultural competence development
and shares positive and relevant experienceswith students
6. Views professional event participationconcerning cultural competencedevelopment as important in students’education and/or professional development,and future practice
and shares view with students
7. Recognizes the significance of offeringincentives to encourage student participationin professional events
and offers incentives to encourage studentparticipation in professional events
8. Maintains professional partnerships focusedon cultural competence development
and shares positive and relevant experienceswith students
9. Maintains membership(s) in professionalorganizations whose primary mission iscultural competence development
and shares positive and relevant experienceswith students
10. Views student memberships in nursingorganizations/associations (whose primarymission is cultural competence development)as important in students’ education and/orprofessional development, and futurepractice
and shares view with students
11. Recognizes the significance of offeringincentives to encourage student participationin memberships in nursingorganizations/associations committed tocultural competence development
and offers incentives to encourage studentparticipation in memberships in nursingorganizations/associations committed tocultural competence development
∗Active promoter/facilitator actions are indicated by italics.
© Springer Publishing Company
L Estudentsstude
Eres relevant informationmation
LP
LP
M P
MMP
AM
AMM
SA A
and shares positive ans positive anwith studentswith students
Pand shares vand
Micipation
Atnerships focusedocused
S Adevelopment
SA
ership(s) in professionalhip(s) in professe primary missione primary missiSdevelopmentlopmentS

Yes No Yes No
12. Recognizes actual and potential barriershindering students’ development of culturalcompetence
and initiates strategies to remove barriers
13. Recognizes the significance of implementingstrategies to encourage student developmentof cultural competence
and implements strategies to encouragestudent development of cultural competence
14. Recognizes the significance of evaluatingstrategies implemented to encourage studentdevelopment of cultural competence
and evaluates strategies implemented toencourage student development of culturalcompetence
© Springer Publishing Company
S A M
P L
E

Part 2 Directions1. Use black ink, write down active promoter actions implemented for each item. Include how, what, where,
and when.2. Use another color ink, write down FUTURE active promoter actions planned for each item. Include how,
what, where, when.3. Review and reflect.4. Share and discuss with peers. Plan and coordinate strategies throughout the course, curriculum, and program.
Values, Beliefs, and Actions Active Promoter of Cultural Competence Development
How and/or What Where When
1. Views cultural competence as important in own life andshares beliefs with students∗
2. Views cultural competence as important in students’education, professional development, and future practiceand shares view with students
3. Views own nurse educator role to include activeinvolvement in promoting cultural competence developmentamong students and shares view with students
4. Routinely updates own knowledge and skills to enhancecultural competence and shares relevant information withstudents
5. Attends professional events concerning culturalcompetence development and shares positive and relevantexperiences with students
6. Views professional event participation concerning culturalcompetence development as important in students’education and/or professional development, and futurepractice and shares view with students
7. Recognizes the significance of offering incentives toencourage student participation in professional events andoffers incentives to encourage student participation inprofessional events
8. Maintains professional partnerships focused on culturalcompetence development and shares positive and relevantexperiences with students
9. Maintains membership(s) in professional organizationswhose primary mission is cultural competence developmentand shares positive and relevant experiences with students
10. Views student memberships in nursingorganizations/associations (whose primary mission iscultural competence development) as important instudents’ education and/or professional development, andfuture practice and shares view with students
∗Active promoter/facilitator actions are indicated by italics.
© Springer Publishing Company
AM P
L E
M
EELPevantevan
MS
A erning culturalning cultura
students’ts’ment, and futureure
ntsnts
Aof offering incentives tog incentives topation in professional evessio
courage student participacourage student parti
S Sal partnerships fpartnershipsntt and shaand sha

How and/or What Where When
11. Recognizes the significance of offering incentives toencourage student participation in memberships in nursingorganizations/associations committed to culturalcompetence development and offers incentives toencourage student participation in memberships in nursingorganizations/associations committed to culturalcompetence development
12. Recognizes actual and potential barriers hinderingstudents’ development of cultural competence and initiatesstrategies to remove barriers
13. Recognizes the significance of implementing strategies toencourage student development of cultural competenceand implements strategies to encourage studentdevelopment of cultural competence
14. Recognizes the significance of evaluating strategiesimplemented to encourage student development of culturalcompetence and evaluates strategies implemented toencourage student development of cultural competence
© Springer Publishing Company
S A M
P L
EEEL

I T E M 1 4
Active Promoter Assessment Tool—Health Care Institutions/ProfessionalAssociations (APAT-HCIPA)
USER INFORMATION� Used to help individuals, groups, and organizations
� Appraise values, beliefs, and actions concerning cultural competence development� Determine whether or not one is an optimal active role model in cultural competence development within
the health care institution or professional association� Identify factors restricting cultural competence development� Plan and coordinate future active promoter actions toward achieving optimal cultural competence
� May be used individually and/or in groups� May be used alone or in conjunction with other toolkit items� Supplementary book resources: Chapter 10 and 13; Figure 10.3 and Exhibit 13.1
© Springer Publishing Company
PL E
developmeveloltural competetural comp
achievingac optimalal cuc
itemsFigure 10.3 and ExhFigure 10.3 and Exh
S A M
P P

Part 1 Directions
(1) Check “yes” or “no” for each value, belief, and action.(2) Check “yes” or “no” for each active promoter action.(3) Review and reflect.(4) Proceed to Part 2.
Values, Beliefs, and Actions Active Promoter of Cultural Competence Development
Yes No Yes No
1. Views cultural competence as important inown∗1 life
and shares beliefs with others∗2
2. Views cultural competence as important inmembers’∗3 education, professionaldevelopment, and future practice
and shares view with others
3. Views own role to include active involvementin promoting cultural competencedevelopment among members
and shares view with others
4. Routinely updates own knowledge and skillsto enhance cultural competence
and shares relevant information with others
5. Attends professional events concerningcultural competence development
and shares positive and relevant experienceswith others
6. Views professional event participationconcerning cultural competencedevelopment as important in members’ongoing continuing education, professionaldevelopment, and future practice
and shares view with others
7. Recognizes the significance of offeringincentives to encourage members’participation in professional events
and offers incentives to encourage members’participation in professional events
8. Maintains professional partnerships focusedon cultural competence development
and shares positive and relevant experienceswith others
9. Maintains membership(s) in professionalorganizations whose primary mission iscultural competence development
and shares positive and relevant experienceswith others
10. Views memberships in professionalorganizations/associations (whose primarymission is cultural competence development)as important in members’ continuingeducation, professional development, andfuture practice
and shares view with others
11. Recognizes the significance of offeringincentives to encourage members’participation in memberships in professionalorganizations/associations committed tocultural competence development
and offers incentives to encourage members’participation in memberships in nursingorganizations/associations committed tocultural competence development
∗1Own refers to individuals, nurse managers, executive, administrator, elected officer, educator, or organization/association∗2Others refers to unlicensed and licensed members of the health care team & members and elected officers of professional associations∗3Members refers to staff members or association members
© Springer Publishing Company
L Ethersthers
Es relevant information wmation w
LP
LP
M P
MMP
AM
AMM
SA A
and shares positive ands positive andwith otherswith
Pand shares vieand s
MAerships focusedocused
evelopment
S ASA
rship(s) in professionalhip(s) in professse primary mission isprimary missio
developmententSS

Yes No Yes No
12. Recognizes actual and potential barriershindering the development of culturalcompetence
and initiates strategies to remove barriers
13. Recognizes the significance of implementingstrategies to encourage members’development of cultural competence
and implements strategies to encouragemembers’ development of culturalcompetence
14. Recognizes the significance of evaluatingstrategies implemented to encouragemembers’ development of culturalcompetence
and evaluates strategies implemented toencourage members’ development of culturalcompetence
© Springer Publishing Company
S A M
P L
E

Part 2 Directions
(1) Use black ink, write down active promoter actions implemented for each item. Include how, what, where,and when.
(2) Use another color ink, write down FUTURE active promoter actions planned for each item. Include how,what, where, when.
(3) Review and reflect.(4) Share and discuss with peers. Plan and coordinate strategies throughout the employee orientation, ongoing
employee inservice or continuing education programs, HCI and PA.
Values, Beliefs, and Actions Active Promoter of Cultural Competence Development
How and/or What Where When
1. Views cultural competence as important in own life andshares beliefs with others∗
2. Views cultural competence as important in members’education, professional development, and future practiceand shares view with others
3. Views own role to include active involvement in promotingcultural competence development among staff membersand shares view with others
4. Routinely updates own knowledge and skills to enhancecultural competence and shares relevant information withothers
5. Attends professional events concerning culturalcompetence development and shares positive and relevantexperiences with others
6. Views professional event participation concerning culturalcompetence development as important in members’ongoing continuing education, professional development,and future practice and shares view with others
7. Recognizes the significance of offering incentives toencourage members’ participation in professional eventsand offers incentives to encourage members’ participationin professional events
8. Maintains professional partnerships focused on culturalcompetence development and shares positive and relevantexperiences with others
9. Maintains membership(s) in professional organizationswhose primary mission is cultural competence developmentand shares positive and relevant experiences with others
10. Views memberships in nursing organizations/associations(whose primary mission is cultural competencedevelopment) as important in members’ continuingeducation, professional development, and future practiceand shares view with others
∗Active promoter/facilitator actions are indicated by italics.
© Springer Publishing Company
M P L
E
M
EEL EP
LP
nd relevantvant
AMM
SA Mconcerning culturalcultura
ant in members’antofessional development,essional de
s view with otherswith othersAance of offering incentivance of offering inces’ participation in profess’ participation in profes
S ves to encourage membs to encouragentsts Stners

How and/or What Where When
11. Recognizes the significance of offering incentives toencourage members’ participation in memberships inprofessional organizations/associations committed tocultural competence development and offers incentives toencourage members’ participation in memberships inprofessional organizations/associations committed tocultural competence development
12. Recognizes actual and potential barriers hindering thedevelopment of cultural competence and initiates strategiesto remove barriers
13. Recognizes the significance of implementing strategies toencourage members’ development of cultural competenceand implements strategies to encourage members’development of cultural competence
14. Recognizes the significance of evaluating strategiesimplemented to encourage members’ development ofcultural competence and evaluates strategies implementedto encourage members’ development of culturalcompetence
© Springer Publishing Company
S A M
P L
EEEL

I T E M 1 5
Systematic Inquiry: Academic (SI-A)
USER INFORMATION� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, corresponding
actions, notations/reflections, prioritization, and future planning.� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competency
development is actively present:� Overall within the curriculum� Specifically at the individual course level� Via outside connections to supplementary resources
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the academic setting?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log). Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic-prescriptive innovations targeting faculty and student developmentin the overall goal of achieving optimal cultural competence.
� Supplementary book resources: Chapter 6 and Figure 6.3
© Springer Publishing Company
e (or in(or
ns:mponent within thet within the
her toolkit items (Retoolkit iteLog). Results serve aLog). Results se
prescriptive innovatescriptive innova
AM cultural competenccultural comp
apter 6 and Figure 6ter 6 and Figure
S A MAM

Systematic Inquiry: Academic Settings
Directions:1. Reflect on the three inquiry questions below as you appraise each component.2. Using the rating scale below, mark your appraisal decision in the space provided.3. Mark the corresponding action for each appraisal decision in the space provided.4. Write comments and details as needed in the “notes” section.5. Prioritize areas for immediate action by marking the priority rank section.6. Review, discuss, and develop cultural competence plan. (Note: Cultural Competence Documentation Log may
be used for documenting cultural competence plans, actions, and evaluations).
Inquiry Questions� To what degree is cultural competence an integral component within the academic setting?� How visible (invisible) is cultural competence development evident?� How do all the cultural components of the curriculum (course/other) fit/blend together?
Rating Scale
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
© Springer Publishing Company
L Eonn E−→−→− CoEd attachment CC ==
S A M
P L
what integrated Bwhat integrated Bnsistently integratedstent
Predominant themeinant theme
PL

Curriculum
Decision Action PriorityRating Rating Notes Rank
Philosophy
Conceptual framework
Program objectives
Program outcomes
Horizontal threads
Vertical threads
Supplementary Resources
Decision Action PriorityRating Rating Notes Rank
Library resources
Nursing student resourcecenter (NSRC) or NursingNeighborhood
Nursing student lounge
Nursing student club
Sigma Theta Tau chapter
Specialty organizations
Bulletin boards
Web page & discussionboards
Invited guest speakers
Date form completed: Name(s) of evaluator(s):
Date reviewed by curriculum committee: Chairperson, dean, director:
Comments/notes
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
MP L
EEEL EP
LP
MM MA MAA
MS
AS
AAS ASS
AMM
AS
ASSS
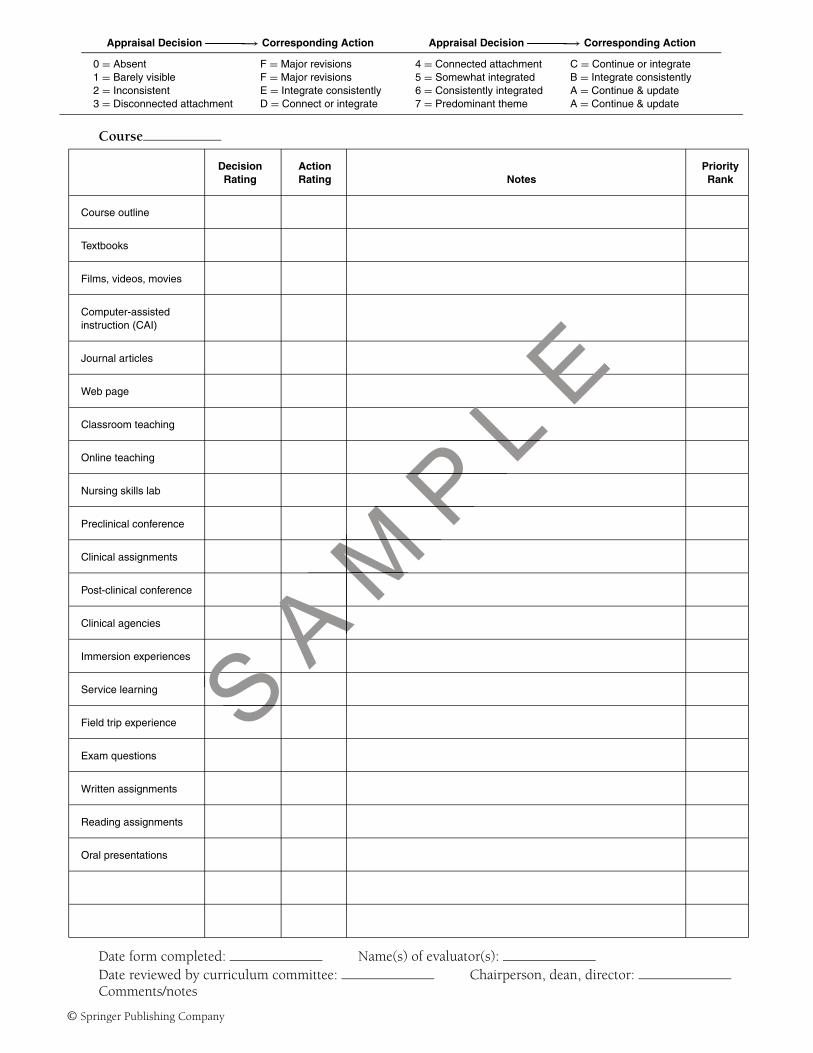
Course
Decision Action PriorityRating Rating Notes Rank
Course outline
Textbooks
Films, videos, movies
Computer-assistedinstruction (CAI)
Journal articles
Web page
Classroom teaching
Online teaching
Nursing skills lab
Preclinical conference
Clinical assignments
Post-clinical conference
Clinical agencies
Immersion experiences
Service learning
Field trip experience
Exam questions
Written assignments
Reading assignments
Oral presentations
Date form completed: Name(s) of evaluator(s):Date reviewed by curriculum committee: Chairperson, dean, director:Comments/notes
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
PL EEEL
PL
MP
MM MA
MAA
MA AA
SA
SA
S SSS
PM
PMM
AASS

I T E M 1 6
Systematic Inquiry: Health Care Institutions (SI-HCI)
USER INFORMATION� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, corresponding
actions, notations/reflections, prioritization, and future planning.� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competency
development is actively present:� Overall within the institution� Specifically at the individual unit (site) level� Via outside connections to supplementary resources.
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the HCI?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log). Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic-prescriptive innovations targeting staff development and improvedpatient care outcomes in the overall goal of achieving optimal cultural competence.
� Supplementary book resources: Chapter 10 and Figure 10.4
© Springer Publishing Company
e (or in(or
ns:mponent within thet within the
her toolkit items (Retoolkit iteLog). Results serve aLog). Results se
prescriptive innovatescriptive innovaoal of achievingal of achieving
AM
optimapter 10 and Figureter 10 and Figur
S A MAM

Systematic Inquiry: Health Care InstitutionsDirections:
1. Reflect on the three inquiry questions below as you appraise each component.2. Using the rating scale below, mark your appraisal decision in the space provided.3. Mark the corresponding action for each appraisal decision in the space provided.4. Write comments and details as needed in the “notes” section.5. Prioritize areas for immediate action by marking the priority rank section.6. Review, discuss, and develop cultural competence plan. (Note: Cultural Competence Documentation Log may
be used for documenting cultural competence plans, actions, And evaluations).
Inquiry Questions� To what degree is cultural competence an integral component within the health care institution?� How visible (invisible) is cultural competence development evident?� How do all the cultural components fit/blend together?
Rating Scale
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
© Springer Publishing Company
L EE−→→ CoEattachment Ct C ==hat integrated BB
PL istently integratedstently integrated
edominant thememina
S A M
P LPL

Institutional Level
Decision Action PriorityRating Rating Notes Rank
Philosophy & mission
New employee orientation
In-service education
Learning strategies
Newsletter & publications
Library
Website
Bulletin boards
Special events
Committees
Supplementary Resources
Decision Action PriorityRating Rating Notes Rank
Local organizations
Local colleges
Continuing education
Guest speakers
Date form completed: Name(s) of evaluator(s):
Date reviewed by committee: Supervisor/administrator:
Comments/notes on back or below.
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
PL EEEL EL
M P L
MA
MA
MA
MAA
MS
A S
AAS
AP
LP
MP
MA
MS
A S ResourcesesourcesS
DecisionSSatingating

Unit/Site Level
Decision Action PriorityRating Rating Notes Rank
In-service education
Learning strategies
Staff meetings
Patient care conferences
Walking rounds and report
Date form completed: Name(s) of evaluator(s):
Date reviewed by committee: Supervisor/administrator:
Comments/notes
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
S A M
P L
E
M
EEL
AM P
L
A N
ittee: A

I T E M 1 7
Systematic Inquiry: Professional Associations (SI-PA)
USER INFORMATION� Offers a user-friendly quantitative and qualitative approach for systematic appraisal decisions, corresponding
actions, notations/reflections, prioritization, and future planning.� Used to help individuals, groups, and organizations examine how visible (or invisible) cultural competency
development is actively present:� Overall within the association� Specifically at the membership level� Via outside connections to supplementary resources.
� The systematic inquiry is guided by two additional questions:� To what degree is cultural competence an integral component within the professional association?� How do all the cultural components fit together?
� May be used individually or in groups� May be used alone or in conjunction with other toolkit items. (Recommended to use prior to Toolkit Item
20—Cultural Competence Documentation Log.) Results serve as a valuable precursor to informed decisions,responsible actions, and new diagnostic-prescriptive innovations targeting staff and membership developmentin the overall goal of achieving optimal cultural competence.
� Supplementary book resources: Chapter 13 and Figure 13.3
© Springer Publishing Company
e (or in(or
ns:mponent within thet within the
er toolkit items. (Reoolkit iteLog.) Results serve aLog.) Results se
rescriptive innovatioscriptive innovat
AM cultural competenccultural comp
apter 13 and Figureter 13 and Figur
S A MAM

Systematic Inquiry: Professional Associations
Directions:1. Reflect on the three inquiry questions below as you appraise each component.2. Using the rating scale below, mark your appraisal decision in the space provided.3. Mark the corresponding action for each appraisal decision in the space provided.4. Write comments and details as needed in the “notes” section.5. Prioritize areas for immediate action by marking the priority rank section.6. Review, discuss, and develop cultural competence plan. (Note: Cultural Competence Documentation Log may
be used for documenting cultural competence plans, actions, and evaluations).
Inquiry Questions� To what degree is cultural competence an integral component within the professional association?� How visible (invisible) is cultural competence development evident?� How do all the cultural components fit/blend together?
Rating Scale
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
© Springer Publishing Company
L EE−→→ CorEd attachment CCwhat integratedwhat integrated
nsistently integratedstent
S A M
P LPredominant themeinant theme
PL

Interpersonal Level
Decision Action PriorityRating Rating Notes Rank
Board or elected officers
Members
Nonmembers or guests
Supplementary Resources
Decision Action PriorityRating Rating Notes Rank
Other professionalassociations
Local colleges
Health care institutions
Guest speakers
Date form completed: Name(s) of evaluator(s):
Date reviewed by committee: Administrator/association leader:
Comments/notes
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
MP L
EL EP
LM PM
AM
AM
AM
AAM
SA
SAA
SA
SSA
S SSSM
PM
AM
AS A

Professional Association LevelChapter or Local Level
Decision Action PriorityRating Rating Notes Rank
Philosophy & mission
Bylaws
Membership criteria
Newsletter andpublications
Library
Web site
Meetings
Workshops
Conferences
Special events
Committees
Learning strategies
Networking
Mentoring
Date form completed: Name(s) of evaluator(s):
Date reviewed by committee: Administrator/association leader:
Comments/notes
© Springer Publishing Company
Appraisal Decision −→ Corresponding Action Appraisal Decision −→ Corresponding Action
0 = Absent F = Major revisions 4 = Connected attachment C = Continue or integrate1 = Barely visible F = Major revisions 5 = Somewhat integrated B = Integrate consistently2 = Inconsistent E = Integrate consistently 6 = Consistently integrated A = Continue & update3 = Disconnected attachment D = Connect or integrate 7 = Predominant theme A = Continue & update
PL EEEL
PL
M P
MA
MA
MA
MAA
MS
A S
AAS
ASS
AS SSS
PM
PM
AM
AS
ASS

I T E M 1 8
Personal Coding Cover Page for Anonymity and Matching Questionnaires
USER INFORMATION� Used to match questionnaires and assessment tools while protecting respondent’s anonymity� Attach to front page of questionnaire, questionnaire packet, or assessment tool.
© Springer Publishing Company
E
S A M
P L
EE

Questionnaire Cover Sheet for Personal Coding System
Purpose: This page will create a unique code that will only be used to match your questionnaires together.Confidentiality: Participants will not be identified using information provided. Respondents will remain anonymous.
Please fill-in the circles below using pen or pencil. Do not use � or on the form.
1. The first 2 letters of your mother’s maiden name (Example: Smith would be SM):2. The month that your mother was born.3. The number of siblings (brothers and sisters) you had when you were 18 years old. (Example: 2 brothers and
1 sister would be 3. If you have 0 siblings, write 0). (If more than 9, please mark 9.)4. The number of brothers who were OLDER than you when you were 18 years old.5. The number of brothers who were YOUNGER than you when you were 18 years old.6. The number of sisters who were OLDER than you when you were 18 years old.7. The number of sisters who were YOUNGER than you when you were 18 years old.
1. 2. 3. 4. 5. 6. 7.
�Jan � � � � �
B B �Feb � � � � �
C C �Mar � � � � �
D D �Apr � � � � �
E E �May � � � � �
F F �Jun � � � � �
G G �Jul � � � � �
H H �Aug � � � � �
I I �Sep
J J �Oct
K K �Nov
L L �Dec
M M
N N
O O
P P
Q Q
R R
S S
T T
U U
V V
W W
X X
Y Y
Z Z
© Springer Publishing Company
PL EE
ol8 years ol8 years o
L E5.
L E�
� ������
S A M
P����� ��� ��

I T E M 1 9
Sample Permission Letter
USER INFORMATION� Provides a sample for prospective educators and researchers� Adapt letter according to study purpose and need� Mail one copy to Springer Publishing Company and one copy to Dr. Marianne R. Jeffreys.
© Springer Publishing Company
Eanne Ranne
S A M
P L
EE

Requester’s Name and CredentialsMailing AddressE-mail AddressDate
Permissions EditorSpringer Publishing Company11 West 42nd StreetFloor 15New York, New York 10036–8002
Dear Publisher:
I am writing to request permission to use the Transcultural Self-Efficacy Tool (TSET) and (list other tools ) in my researchstudy. The study addresses (briefly describe nature of study, purpose, sample, etc.).
I have mailed a copy of this request letter to the author:
Dr. Marianne R. JeffreysThe City University of New York College of Staten IslandNursing Department2800 Victory BoulevardStaten Island, New York 10314
I also agree to send Dr. Jeffreys further reliability and validity test results for the TSET (and list other tools) at the above address.
Sincerely,
Signature
Name, CredentialsTitle
© Springer Publishing Company
S A M
P L
Ee TSET (and list other toSET (and list oth
M
I T E M 2 0
Cultural Competence Documentation Log
USER INFORMATION� User-friendly log to assist institutions in documenting cultural competence plans, actions, and evaluations.� Use after Toolkit Systematic Inquiry Assessment Tool.
© Springer Publishing Company
S A M
P L
EE

Innovation, Measurement, & Evaluation
Person(s) Date to Measurement EvaluationStrategy or Idea Responsible Resources Needed Implement Plan & Date Plan & Date
1
2
3
4
5
Select one strategy or idea from above. Write out a detailed description of steps and timeline for plan/design,implementation, measurement, and evaluation phases.
Repeat for subsequent prioritized strategies
Plan/Design Steps / Date Implementation Steps / Date Measurement Steps / Date Evaluation Steps / Date
1
2
3
4
5
6
7
8
9
10
11
12
© Springer Publishing Company
S A M
P L
EL ELdetailed description oetailed description
MS
ation Steps / Datetion Steps / DateMA
MA
SA
SS

I T E M 2 1
Research Report Template
USER INFORMATION� User-friendly template to assist individuals and institutions report data generated from assessment tools and
questionnaires in toolkit.� Provides a guide for presentations, publications, future research, and cultural competence interventions� Supplementary book resources: TSET Research Exhibits 6.1, 6.2, 6.3, 6.4, 6.5, 10.1, 10.2 and Chapters 4
and 5.
DIRECTIONS FOR TSET AND CCCET USERSComplete Research Report Template to send TSET and CCCET* reliability and validity test results and study results to:
Dr. Marianne R. Jeffreys, The City University of New York College of Staten Island, Nursing Department, 2800Victory Boulevard, Staten Island, New York 10314, USA.
Study Title:
Date (month, year) Study Began:
Date (month, year) Ended:
Purpose:
Research Question(s) or Hypotheses:
Study Design:
Sample:
Size:
Type of learner:
Demographics:
Instrument (TSET or TSET-MHP):
TSET Data Collection (When was data collected?)
Pretest:
Posttest:
*Please note that TSET and CCCET can be used together or separately in research studies. TSET and CCCET can be used in conjunction with other assessmenttools within the toolkit.
© Springer Publishing Company
S A M
P L
Etural comtural com
3, 6.4, 6.5, 10., 6.4, 6.5, 10.
reliability and validy and validYork College of Stateork College of State
or Hypotheseses
SA::

Educational interventions/teaching–learning strategies: (list and describe)
TSET Reliability (Crohnbach’s alpha)
Total TSET:
Cognitive Subscale:
Practical Subscale:
Affective Subscale:
Data Analysis
Results:
Subscale Mean Standard Deviation t-test Significance
CognitivePretestPosttest
PracticalPretestPosttest
AffectivePretestPosttest
(Supplementary [optional] Analyses)If grouping into High, Medium, and Low, describe method used:
Subscale High Medium Low
CognitivePretestPosttest
PracticalPretestPosttest
AffectivePretestPosttest
© Springer Publishing Company
TSE EST scoresS
L EL ELt-testt
PL L
MP
AM
AM
SA M
LP
MA
MS Aonal] Analyses)ses)
gh, Medium, and Logh, Medium, and L
SSS

Other Instruments:
Other Analyses:
Discussion:
Implications:
Dissemination of Results:
Principal Investigator(s) Name, Credentials, and Title:
Principal Investigator(s) Contact Information:
(a) Mailing Address:
(b) Work Address:
(c) E-Mail Address:
(d) Phone:
(e) Fax:
Other Investigator(s) Name, Credentials, and Title:
Other Investigator(s) Contact Information:
(a) Mailing Address:
(b) Work Address:
(c) E-Mail Address:
(d) Phone:
(e) Fax:
Type of study (doctoral dissertation, master’s thesis, postdoctoral, institutional, other)
Abstract:
© Springer Publishing Company
S A M
P L
Ele:
onon M::
toral dissertatiooral disserta