The contribution of congenital anomalies to infant mortality
13
1 Summary • Congenital anomalies are the second commonest cause of infant deaths in England and Wales; although the vast majority of infants born with a congenital anomaly will survive. There are many different congenital anomalies and the cause of most is not known. In any single year infant deaths due to congenital anomalies are associated with over 150 different causes. Congenital anomalies contribute about one third of the extra infant deaths experienced by the routine and manual socio-economic groups compared with the population as a whole. • The primary prevention of congenital anomalies requires delivery of high quality universal pre-pregnancy and pregnancy care for women in general together with optimisation of management before conception for specific women at higher risk of anomalies, e.g. diabetics. The availability of genetic services is essential for couples with a family history or past history of pregnancies affected by congenital anomalies, particularly due to specific genetic conditions. Some sections of the population are at increased risk of particular genetic conditions and as a consequence infant mortality rates due to congenital anomalies may be higher in some areas compared with England and Wales overall. • Secondary prevention of congenital anomalies is achieved through prenatal screening and diagnosis followed by the offer of termination of pregnancies affected by major anomalies. Because termination of pregnancy is the only option for many congenital anomalies secondary prevention is not universally acceptable. • Infant mortality rates due to congenital anomalies are strongly influenced by prenatal screening and diagnosis, and uptake of termination of pregnancy. However, it is important to note that many of the anomalies subject to primary and secondary prevention would not in any case have resulted in an infant death and thus their prevention, although of great importance because of the associated morbidity and disability, will not necessarily impact on the infant mortality rate. 1 Introduction Congenital anomalies are the second commonest cause of infant deaths in the United Kingdom. This briefing paper is the final in a series of four papers commissioned by the Department of Health as part of a project to evaluate the evidence base of interventions to reduce infant mortality and inequalities in the infant mortality rate. 1,2,3 The aim of this paper is to provide a background to the evidence review process by examining the contribution of congenital anomalies to the infant mortality rate; inequalities in the rate; the role of prevention; and how variations in risk factors and uptake of preventive strategies might affect the infant mortality rate associated with congenital anomalies. Definitions of terms used in this paper are given in the glossary at the end. 2 Congenital anomalies 2.1 Definitions Congenital anomalies, congenital abnormalities, birth defects and congenital malformations are all terms used to describe developmental disorders of the embryo and fetus. There are several hundred separate anomalies which fall under these headings including structural, functional, metabolic and hereditary conditions. However, there is no single universally accepted system of classification of anomalies or indeed a single agreed definition of what constitutes a congenital anomaly. For the purposes of this paper we will use the term congenital anomalies and take this to mean an embryonic or fetal developmental Inequalities in Infant Mortality Project Briefing Paper 4 The contribution of congenital anomalies to infant mortality Jennifer J Kurinczuk, Jennifer Hollowell, Patricia A Boyd, Laura Oakley, Peter Brocklehurst, Ron Gray National Perinatal Epidemiology Unit, University of Oxford June 2010
Transcript of The contribution of congenital anomalies to infant mortality

1
Summary• Congenitalanomaliesarethesecond
commonestcauseofinfantdeathsinEnglandandWales;althoughthevastmajorityofinfantsbornwithacongenitalanomalywillsurvive.Therearemanydifferentcongenitalanomaliesandthecauseofmostisnotknown.Inanysingleyearinfantdeathsduetocongenitalanomaliesareassociatedwithover150differentcauses.Congenitalanomaliescontributeaboutonethirdoftheextrainfantdeathsexperiencedbytheroutineandmanualsocio-economicgroupscomparedwiththepopulationasawhole.
• Theprimary preventionofcongenitalanomaliesrequiresdeliveryofhighqualityuniversalpre-pregnancyandpregnancycareforwomeningeneraltogetherwithoptimisationofmanagementbeforeconceptionforspecificwomenathigherriskofanomalies,e.g.diabetics.Theavailabilityofgeneticservicesisessentialforcoupleswithafamilyhistoryorpasthistoryofpregnanciesaffectedbycongenitalanomalies,particularlyduetospecificgeneticconditions.Somesectionsofthepopulationareatincreasedriskofparticulargeneticconditionsandasaconsequenceinfant mortality ratesduetocongenitalanomaliesmaybehigherinsomeareascomparedwithEnglandandWalesoverall.
• Secondary preventionofcongenitalanomaliesisachievedthroughprenatalscreeninganddiagnosisfollowedbytheofferofterminationofpregnanciesaffectedbymajoranomalies.Becauseterminationofpregnancyistheonlyoptionformanycongenitalanomaliessecondary preventionisnotuniversallyacceptable.
• Infant mortality ratesduetocongenitalanomaliesarestronglyinfluencedbyprenatalscreeninganddiagnosis,anduptakeofterminationofpregnancy.However,itisimportanttonotethatmany
oftheanomaliessubjecttoprimary and secondary preventionwouldnotinanycasehaveresultedinaninfantdeathandthustheirprevention,althoughofgreatimportancebecauseoftheassociatedmorbidityanddisability,willnotnecessarilyimpactontheinfant mortality rate.
1 Introduction
CongenitalanomaliesarethesecondcommonestcauseofinfantdeathsintheUnitedKingdom.ThisbriefingpaperisthefinalinaseriesoffourpaperscommissionedbytheDepartmentofHealthaspartofaprojecttoevaluatetheevidencebaseofinterventionstoreduceinfantmortalityandinequalitiesintheinfant mortality rate.1,2,3Theaimofthispaperistoprovideabackgroundtotheevidencereviewprocessbyexaminingthecontributionofcongenitalanomaliestotheinfant mortality rate;inequalitiesintherate;theroleofprevention;andhowvariationsinriskfactorsanduptakeofpreventivestrategiesmightaffecttheinfant mortality rateassociatedwithcongenitalanomalies.Definitionsoftermsusedinthispaperaregivenintheglossaryattheend.
2 Congenitalanomalies
2.1 DefinitionsCongenitalanomalies,congenitalabnormalities,birthdefectsandcongenitalmalformationsarealltermsusedtodescribedevelopmentaldisordersoftheembryoandfetus.Thereareseveralhundredseparateanomalieswhichfallundertheseheadingsincludingstructural,functional,metabolicandhereditaryconditions.However,thereisnosingleuniversallyacceptedsystemofclassificationofanomaliesorindeedasingleagreeddefinitionofwhatconstitutesacongenitalanomaly.Forthepurposesofthispaperwewillusethetermcongenitalanomaliesandtakethistomeananembryonicorfetaldevelopmental
InequalitiesinInfantMortalityProjectBriefingPaper4
Thecontributionofcongenitalanomaliestoinfantmortality
JenniferJKurinczuk,JenniferHollowell,PatriciaABoyd,LauraOakley,PeterBrocklehurst,RonGray
NationalPerinatalEpidemiologyUnit,UniversityofOxford
June2010

Thecontributionofcongenitalanomaliestoinfantmortality2
abnormalityofanytype,butnotingthatnotallvariationsindevelopmentareanomaliesasanatomicalvariationinhumansiscommon.
Therearefourdistincttypesofanomalieswhichresultfromdifferentsetsofcauses:4
• Malformationsarecausedbyintrinsicallyabnormalprocessesduringthedevelopmentoftheeggorthesperm,orduringfertilisation.Theseincludetheanomaliesthatarecausedbychromosomalabnormalities,forexamplehavinganextrachromosome21inDown’s Syndrome,andsinglegenedefects,forexample,campomelic syndrome.
• Disruptionsrefertodefectsthatarecausedbytheinterferencewithanoriginallynormaldevelopmentalprocess.Disruptionscanbecausedbyteratogenssuchasdrugs,forexamplealcohol,thalidomideandwarfarin;chemicals,forexamplepolychlorinatedbiphenyls(PCBs);viruses,forexamplecytomegalovirus(CMV)andrubella;andionisingradiation,forexampleX-rays.
• Deformationsareabnormalforms,shapesorpositionsofapartofthebodyandresultfrommechanicalforces.Forexample,twinscansufferlimbdeformationsuchasclubbedfootduetothecrowdeduterinespace.
• Dysplasiareferstotheabnormalorganisationofcellsintotissue.Thecausesaregenerallynonspecificandasaconsequenceoftenaffectseveralorganssimultaneously.
Thefrequencyofoccurrenceofcongenitalanomaliesisusuallyquotedasbirth prevalenceratherthanincidence.Thisisbecauseweknowthatmanyfetusesaffectedbyacongenitalanomalywillmiscarry,thatthemiscarriagemayoccurbeforethepregnancyisconfirmedandevenifthemiscarriageislatertheanomalymaynotbediagnosed.Thetermbirth prevalencethereforeacknowledgesthatnotallcasesofcongenitalanomaliescanbediagnosedandcountedinanincidence rate.Thedenominatorforthecalculationofbirth prevalenceisusuallytakenasallbirthswhichexcludesmiscarriagesandterminationsofpregnancy.
2.2 SourcesofinformationaboutcongenitalanomaliesinEngland
The National Congenital Anomalies System (NCAS)wasestablishedin1964inthewakeofthethalidomidedisasterasasurveillancesystemintendedtoidentifyhazardssuchasthalidomidequickly.ThesystemhasoperatedbyissuingmonthlyalertstoDirectorsofPublicHealthwhentherearechangesinthefrequencyofreportedanomaliesasameansofhighlightingpossible
clustersofcasesi.NCASwasnotestablishedasaregisterintendedtoascertainallcasesofcongenitalanomaliesinthepopulation;itspurposewastoconcentrateonidentifyingchangesinthefrequencyofoccurrenceofreportsofanomaliesratherthanestimatingthebirth prevalenceofconditions.ItisonlyinthoseareaswherearegionalcongenitalanomalyregistersuppliesdatatoNCASthatrobustbirth prevalenceestimatescanbederivedfromNCASdata.5
Afurtherlimitationofincreasingimportanceinthecontextofprenatalscreeninganddiagnosisandtheimpactontheinfant mortality rateisthatNCASdoesnotcollectinformationaboutpregnanciesaffectedbyacongenitalanomalythatareterminated.Forconditionswithahighrateofprenataldetectionandtermination,forexampleneural tube defects(NTDs),thisleadstoasubstantialunder-ascertainmentofcasesandmeansthatif,forexample,primary preventionofNTDsthroughfolatefortificationofflourisintroducedintheUK,asithasbeenelsewhere,NCASwillnotbeabletoprovideusefuldatafortheevaluationoftheeffectsoffortification.
TheproblemswithNCASdatamay,however,beoflimitedconcerninthefuturesincethewholeoftheNCASsystemiscurrentlyunderreview(consultationclosedMarch2010)withtheproposalthatdatacollectionwillceaseandafinalreportwillbeissuedin2009/2010.Whilstalegacydatasystemwillberetainedsubsequentdatacollectionwillcease.DiscussionsabouthowtoprovidesurveillancedataandalertsofpotentialclustersintheshortandlongertermareinprogresswiththerelevantmembersoftheBritishIslesNetworkofCongenitalAnomaliesRegisters(BINOCAR).6
Congenital Anomalies Registersarehighlyorganisedsystemsforcollectingdataaboutcongenitalanomalieswiththepurposeofidentifyingallthecasesofcongenitalanomaliesingeographicallydefinedpopulations.MostRegistersintheUKcollectinformationaboutanomaliesdiagnosedprenatally,andthosediagnosedinthenewbornandearlychildhoodinspecificdesignatedgeographicalregions.7IntheUKthenetworkofregionalcongenitalanomaliesregistersisrepresentedbyBINOCAR(Figure1).6Theregionalcongenitalanomaliesregistersarenowtheonlysourceofpopulation-basedcongenitalanomaliesdataintheUKableto:supporton-goingauditandevaluationofthenationalprenatalscreeninganddiagnosisprogramme;provideroutineprevalenceandtrendinformationaboutanomalies;andtheonlymeanstosystematicallyidentifyandinvestigatepotentialclustersofcases.
i NCASceasedissuingalertsinmid-2009andNCAShassubsequentlyclosedcompletely.

Thecontributionofcongenitalanomaliestoinfantmortality 3
GeographicallytheBINOCARregisterscovermuchoftheareaofEngland,however,mainlybecauseoftheconcentrationofbirthsintheEast,LondonandtheSouthEastofEnglandandthelackofregistersinthoseareas,onlyabout50%ofbirthsinEnglandareborninareasservedbyaBINOCARregister.Twooftheregistersarehowever,atriskwithfundinginplaceonlytoMarch2011:CongenitalAnomaliesRegisterforOxfordshire,BerkshireandBuckinghamshire(CAROBB)iandtheNorthernCongenitalAnomaliesSurvey(NorCAS).iiWhereas,anewregisterisproposedforYorkshireandHumber(YHCAR).
Figure 1. BINOCAR Registers Map6*
BINOCAR Register
Proposed BINOCAR Register
No BINOCAR Register coverage
East Midlands & South Yorkshire
Wessex
CARIS Wales
Oxford, Berkshire &
Buckinghamshire
Northern
South West
West Midlands
Glasgow
Cork & Kerry
Dublin
South Eastern
Merseyside& Cheshire
Yorkshire & Humber
Scotland
BINOCAR Register
Proposed BINOCAR Register
No BINOCAR Register coverage
*ABINOCARregisteroperatesinGlasgow;informationaboutcongenitalanomaliesintherestofScotlandiscollectedbyroutinedatasystemsandprovidedbytheInformationServicesDivision,NHSServicesScotland
2.3 Frequencyofoccurrenceofcongenitalanomalies
Thelackofagreementaboutthedefinitionofcongenitalanomaliesmeansthatthecomparisonofthebirth prevalenceofanomaliesisproblematicasinclusionandexclusioncriteriavarybetweendifferentdatasources.Furthermoresomeregistershavehistoricallyconcentratedonprenatallyandneonatallydiagnosedconditions10whereasothersindifferentpartsoftheworldhaveincludedanomaliesdiagnosedfrompregnancyintochildhood,forexampletoage6yearsinWesternAustralia.11Variationsinbirth prevalenceestimatesmayalsoarisedependinguponwhetherornotfiguresrelating
i CAROBBwebsiteavailableat:http://www.npeu.ox.ac.uk/carobb[AccessedApril2010]
iiNorCASwebsiteavailableat:http://www.nepho.org.uk/rmso/surveys/congenital[AccessedApril2010]
topregnanciesterminatedbecauseoffetalcongenitalanomalies(TOPFA)areincluded.Variationsinmethodsofascertainmentarealsoimportant.Passivesystemsofcasenotificationtendtoidentifyfewercasescomparedwithmoreactiveascertainment.7Asaconsequenceofallthesedifferencesestimatesofbirth prevalencevaryfromplacetoplace.However,apartfromasmallnumberofspecificanomalies,anydifferencesinprevalencearethoughtlargelytobeduetomethodologicaldifferencesratherthantruedifferencesinunderlyingpopulationincidence.
About3%offetusesandnewbornsarediagnosedwithacongenitalanomalyintheUKeachyear10,12eitherbeforeorsoonafterbirth;thisincludesfetuseswhichareterminatedbecauseofthepresenceofacongenitalanomaly(TOPFA).Thismeansthatin2008whentherewere712,328live birthsandstillbirthsinEnglandandWalesover21,000wereaffectedbyacongenitalanomalydiagnosedbeforeoraroundbirth.
3 Contributionofcongenitalanomaliestoinfantdeaths
3.1 NationalstatisticsSincetheintroductionofthecurrentstillbirthandneonataldeathcertificatein1986ithasnotbeenpossibletodirectlycomparethecausesofneonataldeathswiththecausesofpostneonataldeaths.1Thisisbecause,incontrasttodeathsingeneral(includingpostneonataldeaths),nosingleunderlyingcauseofdeathisrecordedforneonataldeaths.Asaconsequence,theOfficeforNationalStatistics(ONS)developedahierarchicalclassificationwhichallowsboth neonatal and postneonataldeathstobeassignedtoaspecificcategorybasedonthelikelytimingofthedamageleadingtothedeath(seeglossaryforthedefinitionoftheONS cause of deathclassificationalgorithm).ThecausesofdeathgiveninFigure2areshowninthehierarchicalorderoftheONS causegroups.
Thecontributionofcongenitalanomaliestoinfantmortality4
Figure 2. ONS cause group-specific mortality rates by timing of the death*, England and
Wales, 200713
0
0.5
1
1.5
2
2.5
Infant Neonatal Postneonatal
Timing of the death
Infa
nt m
orta
lity
rate
per
1,0
00 li
ve b
irths
1. Congenital anomalies2. Antepartum infection3. Immaturity4. Intrapartum causes5. External conditions6. Infections7.Other specific causes9.Sudden infant deaths0. Unclassified
*Neonataldeaths–deathsoccurringunder4weeksofagePost-neonataldeaths-deathsoccurringfrom4weekstooneyearofageInfantdeaths–deathsoccurringbeforeoneyearofage
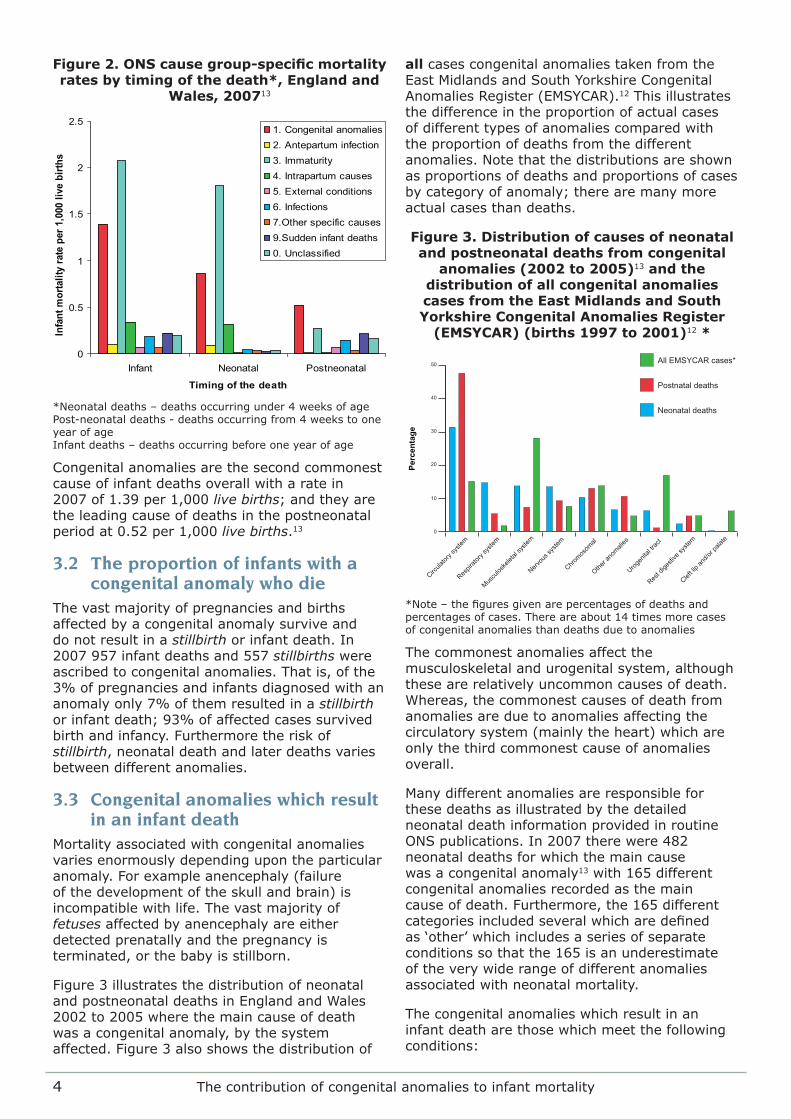
Congenitalanomaliesarethesecondcommonestcauseofinfantdeathsoverallwitharatein2007of1.39per1,000live births;andtheyaretheleadingcauseofdeathsinthepostneonatalperiodat0.52per1,000live births.13
3.2 Theproportionofinfantswithacongenitalanomalywhodie
Thevastmajorityofpregnanciesandbirthsaffectedbyacongenitalanomalysurviveanddonotresultinastillbirthorinfantdeath.In2007957infantdeathsand557stillbirthswereascribedtocongenitalanomalies.Thatis,ofthe3%ofpregnanciesandinfantsdiagnosedwithananomalyonly7%ofthemresultedinastillbirthorinfantdeath;93%ofaffectedcasessurvivedbirthandinfancy.Furthermoretheriskofstillbirth,neonataldeathandlaterdeathsvariesbetweendifferentanomalies.
3.3 Congenitalanomalieswhichresultinaninfantdeath
Mortalityassociatedwithcongenitalanomaliesvariesenormouslydependingupontheparticularanomaly.Forexampleanencephaly(failureofthedevelopmentoftheskullandbrain)isincompatiblewithlife.Thevastmajorityoffetusesaffectedbyanencephalyareeitherdetectedprenatallyandthepregnancyisterminated,orthebabyisstillborn.
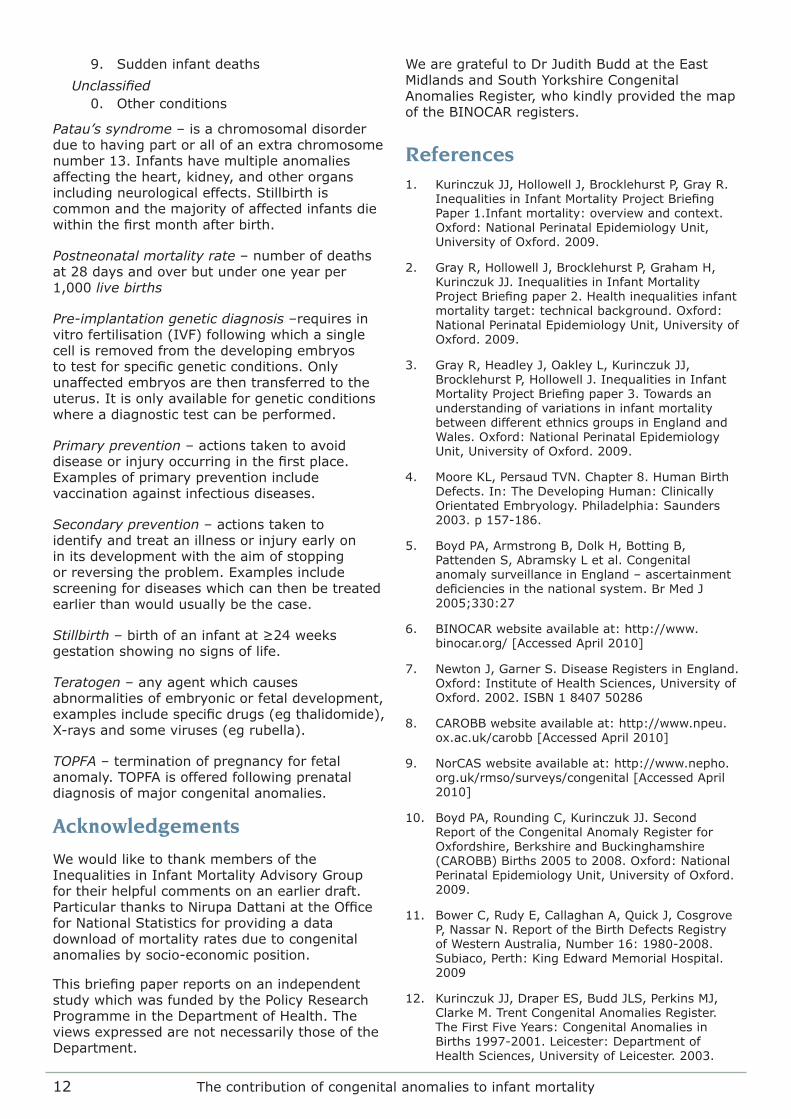
Figure3illustratesthedistributionofneonatalandpostneonataldeathsinEnglandandWales2002to2005wherethemaincauseofdeathwasacongenitalanomaly,bythesystemaffected.Figure3alsoshowsthedistributionof
allcasescongenitalanomaliestakenfromtheEastMidlandsandSouthYorkshireCongenitalAnomaliesRegister(EMSYCAR).12Thisillustratesthedifferenceintheproportionofactualcasesofdifferenttypesofanomaliescomparedwiththeproportionofdeathsfromthedifferentanomalies.Notethatthedistributionsareshownasproportionsofdeathsandproportionsofcasesbycategoryofanomaly;therearemanymoreactualcasesthandeaths.
Figure 3. Distribution of causes of neonatal and postneonatal deaths from congenital
anomalies (2002 to 2005)13 and the distribution of all congenital anomalies cases from the East Midlands and South Yorkshire Congenital Anomalies Register
(EMSYCAR) (births 1997 to 2001)12 *
0
10
20
30
40
50 All EMSYCAR cases*
Postnatal deaths
Neonatal deaths
Cleft li
p and
/or pa
late
Rest d
igesti
ve sy
stem
Urogen
ital tr
act
Other a
nomali
es
Chromos
omal
Nervou
s sys
tem
Muscu
loske
letal
syste
m
Respir
atory
syste
m
Circula
tory s
ystem
Percentage
*Note–thefiguresgivenarepercentagesofdeathsandpercentagesofcases.Thereareabout14timesmorecasesofcongenitalanomaliesthandeathsduetoanomalies
Thecommonestanomaliesaffectthemusculoskeletalandurogenitalsystem,althoughthesearerelativelyuncommoncausesofdeath.Whereas,thecommonestcausesofdeathfromanomaliesareduetoanomaliesaffectingthecirculatorysystem(mainlytheheart)whichareonlythethirdcommonestcauseofanomaliesoverall.
ManydifferentanomaliesareresponsibleforthesedeathsasillustratedbythedetailedneonataldeathinformationprovidedinroutineONSpublications.In2007therewere482neonataldeathsforwhichthemaincausewasacongenitalanomaly13with165differentcongenitalanomaliesrecordedasthemaincauseofdeath.Furthermore,the165differentcategoriesincludedseveralwhicharedefinedas‘other’whichincludesaseriesofseparateconditionssothatthe165isanunderestimateoftheverywiderangeofdifferentanomaliesassociatedwithneonatalmortality.
Thecongenitalanomalieswhichresultinaninfantdeatharethosewhichmeetthefollowingconditions:

Thecontributionofcongenitalanomaliestoinfantmortality 5
Theyare:
• Notuniversallylethalduringpregnancyand
• Haveahighriskofearlydeatheitherduetotheanomalyitselforthecomplicationsoftreatmentand○ AreNOTdetectable(orhavealowdetectionrate)throughscreeningduringpregnancyOr
○ Aredetectablethroughprenatalscreeningbutthereispooraccesstoscreening,orlowuptakeofscreening,orterminationofpregnancytendsnottobetaken-up
Thegroupofanomalieswhichbestillustratesthistypologyistheheartanomaliesgroup.Thereareover80individualheartanomaliesdescribedintheICD10 classification system,includingseveralcategoriesof‘other’inwhichmanyindividual,rareranomaliesmaybeclassified.Unlesstheyformpartofasyndrome,heartdefectstendnottoresultinstillbirth.Theoverallprenataldetectionrateforcardiacanomaliesisrelativelylowatabout35-40%10andevenwiththesophisticatedsurgerynowavailablethecomplexcardiacanomaliesgenerallyhavearelativelyhighriskofinfantdeath.
3.4 Variationsininfantmortalityduetocongenitalanomalies
Variationsininfant mortality ratesduetocongenitalanomaliesbetweendifferentgroupsinthepopulationariseunderthetwosetsofconditionsoutlinedinFigure4.
ThetypologyoutlinedinFigure4makesexplicitthepoints(*)atwhichinterventionsmighttheoreticallybeputinplacetoreducevariationsbetweengroupsintherateofinfantdeathsduetocongenitalanomalies.
Thetwomainpointsforinterventiontoreducevariationarefirsttheunderlyingaetiological risk,andsecondintheaccess to screening.Athirdpotentialpointisindifferentialuptake of screeningforwhichtheremaybevariationduetolackofinformation.However,evenassumingthatfullinformationisgiventoallwomen,variationsinchoiceaboutprenatalscreeningbetweendifferentgroupsofwomenarelikelytoremain.15Theseareverypersonalchoicesmainlyrelatingtoterminationofpregnancyforwhichtheremaybestrongcultural,moralandreligiousinfluences,anddifferentviewsofwhatisregardedasa‘good’reproductiveoutcome.
Thereisafourthpotentialinterventionpointifthereisdifferential access to treatmentonceababywithacongenitalanomalyisborn.InthecontextoftheNHSanyvariationsinaccessandqualityoftreatment,wheretheyexist,arelikelytobegeographicalratherthanbased
Figure 4. Conditions under which variations in infant mortality rates due to congenital anomalies might arise between different groups in the population
Conditions 1: • There are NO variations between groups in the underlying risk of the anomalies;
incidence is the same and
• The anomalies are not universally lethal during pregnancy and
• The anomalies have a high risk of early death due to the anomalies or the complications of treatment and
• The anomalies are detectable through prenatal screening BUT there is differential screening access (*), or differential screening uptake, or differential uptake of termination of pregnancy (TOPFA)
Conditions 2:
• There ARE variations between groups in the underlying risk (*) of the anomalies resulting in differences in incidence and
• The anomalies are not universally lethal during pregnancy and
• The anomalies have a high risk of early death due to the anomalies or the complications of treatment and
o The anomalies are NOT detectable (or have a low detection rate) through prenatal screening Or
o The anomalies are detectable through prenatal screening BUT there is differential screening access (*), or differential screening uptake, or uptake of termination of pregnancy (TOPFA)
(*)Pointsatwhichitmaybepossibletointroduceinterventionstoreducevariationsininfantmortalityduetocongenitalanomaliesbetweendifferentgroupsinthepopulation

Thecontributionofcongenitalanomaliestoinfantmortality6
onindividualpatientcharacteristics.However,providinginformationtoparentstoenablethemtomakefullyinformedtreatmentchoicesinrelationtocomplexhighriskproceduresmaybeparticularlydifficultforsomegroups,forexample,whereEnglishisnottheirfirstlanguage.
Tointerveneontheunderlyingriskofanomalies(primary prevention)requiresknowledgeofpotentiallymodifiableriskfactors,themeanstomodifytheriskfactorsandthewidespreaduptakeofthoseinterventions.Riskfactorsforcongenitalanomaliesarediscussedlater.
Tointerveneonaccesstoprenatalscreening(secondary prevention)requiresanunderstandingofvariationsandbarrierstoaccess.However,evenifscreeningaccessisuniversallyequal,andthereissomeevidencethatthisisnotthecase,15theremayneverthelessbegroupsinthepopulationwhochoosenottotakeupprenatalscreeninganddiagnosis15or,wheretheytakeupprenatalscreeninganddiagnosistheymayactona‘positive’resultbychoosingtocontinuewiththeirpregnancyandparenttheirchildasanalternativetochoosingtoterminatethepregnancy.
3.5 Evidenceofvariationsbetweengroupsininfantmortalityratesduetocongenitalanomalies
Theavailablenationaldatarelatingtocongenitalanomalydeathsonlyallowsexaminationofasmallnumberofdifferentgroupsinthepopulation.Figure5illustratesdifferencesintherateofinfantdeathbytheethnicgroupofthemotherandhighlightsthestatisticallysignificantlyfour-foldhigherriskofinfantdeathfromcongenitalanomaliesfacedbybabiesborntomothersofPakistaniorigincomparedwithalltheothergroupslisted.Thishigherriskrepresentsabout90extradeathsperyearintheinfantsborntoPakistanimothersinEnglandandWalesoverthenumberofdeathsthatwouldhavebeenexpectedinthisgrouphadtheyexperiencedthesameinfant mortality rateasWhiteBritishmothers.
Babiesborntomothersfrom‘other’ethnicgroupsarealsoatastatisticallysignificantlyhigherriskofinfantdeathcomparedwithinfantborntoWhiteBritishmothersofabout45%.Thisrepresentsanexcessofabout25deathsperyearcomparedwiththenumberthatwouldhavebeenexpectedhadtheyexperiencedthesameinfant mortality rateasWhiteBritishmothers.
Figure 5. Infant mortality rates due to congenital anomalies with 95% confidence intervals, by ethnic group† per 1,000 live
births for babies born in England and Wales in 200516
0.01.02.03.04.05.06.07.0
Infa
nt m
orta
lity
rate
due
to c
onge
nita
l an
omal
ies
per 1
,000
live
birt
hs
*Statisticallysignificantlyhigherthanalltheothergroups**StatisticallysignificantlyhigherthantheWhiteBritishgroup**Chinese,OtherAsian,OtherBlack,OtherandallMixedgroups†EthnicgroupofmotherderivedfromlinkageofbirthregistrationstatisticstoNHSnumbersforbabies(NN4B)data1,3,16
Figure6illustratesdifferencesintherateofneonataldeathduetocongenitalanomaliesbythesocio-economicpositionoftheneonatebasedonpaternaloccupationcoding.ThishighlightsastatisticallysignificantlydoublingintheriskofneonataldeathduetocongenitalanomaliesinthegroupsofbabiesborntofathersintheNS-SECcategoriesof6and7andthosewhoseoccupationscouldnotbeclassified,comparedwithbabiesborntofathersintheNS-SECgroups1-5.Thishigherriskrepresentsabout88extradeathsperyearingroups6,7andunclassifiedoverthenumberofdeathsthatwouldhavebeenexpectedinthisgrouphadtheyexperiencedthesamemortalityrateastheinfantsborntofathersintheNS-SECgroups1-5.
Intryingtounderstandthesedifferencesitisimportanttonotethatthefiguresrelatingtoethnicityandsocio-economicpositionarenotindependentanditislikelythatsomeethnicgroupsaremorelikelytohaveahigherorlowersocio-economicpositionthatis,thesetwofactorsconfoundeachother.ItisnotpossibletountangletheseeffectsinrelationtoinfantmortalityfromONSpublisheddatabecausethedataareonlyavailableinaggregatedform.However,workundertakenbytheBradfordInfantMortalityCommissiondemonstratedthatinBradford88%ofbabiesin1996-2003borntoPakistanimothersand41%ofbabiesborntowhiteBritishmotherswereborninthemostdeprivedtwo-fifthsofneighbourhoods.17ForinfantdeathsoverallafurtheranalysisoftheBradforddatawassuggestiveofanindependentexcessinfantmortalityformothersofPakistanioriginoverandabovetheeffectsofsocio-

Thecontributionofcongenitalanomaliestoinfantmortality 7
economicposition.Theseresultswerenotstatisticallysignificantbutthiswasnotsurprisinggiventhesmallnumbersofdeathsinvolved.
Figure 6. Neonatal mortality rate due to congenital anomalies† with 95% confidence intervals, by socio-economic position (NS-
SEC) per 1,000 live births for babies born in England and Wales 2002 to 2005±
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
1* 2* 3 4 5 6* 7* Not class*
Sole reg*
Overall
Neon
atal
mor
talit
y ra
te d
ue to
con
geni
tal
anom
alie
s pe
r 1,0
00 li
ve b
irths
Socio-economic postion (NS-SEC)
†Formaincauseofdeath±DerivedfromadatadownloadprovidedbyONS*Statisticallysignificantlydifferentthantheoverallrate
3.6 Thecontributionofcongenitalanomaliestothegapininfantmortalitybetweentheroutineandmanualgroupsandthepopulationasawhole
Theaimoftheinfantmortalitypublicserviceagreementtargetforinfantmortalityis:“...toreducebyatleast10%thegapinthemortalitybetweentheroutineandmanualgroupsandthepopulationasawhole....”18UsingthedataprovidedbyONSforEnglandandWalesandillustratedinFigure6wehaveestimatedtheexcessnumberofinfantdeathsperyearfortheroutineandmanualgroupsinthepopulationandhavecalculatedthecontributionofcongenitalanomaliestotheexcess.Fortheperiod2002to2005theroutineandmanualgroupsexperienced,onaverage,160extrainfantdeathsabovethenumberthatwouldhavebeenexpectedhadtheyhadthesameinfant mortality rateastheEnglandandWalespopulationasawhole.Infantdeathsduetocongenitalanomaliescontributedaboutonethirdofthistotalthatis,50oftheseextradeathseachyear.Ofnote,theseareaveragenationalpopulationfiguresandarelikelytovaryacrosslocalitiesduetodifferencesinthepopulationcharacteristics.
4 Causesandpreventionofcongenitalanomalies
4.1 Thecausesofcongenitalanomalies
Thecauseofthemajorityofcongenitalanomaliesisnotknown.4Thereisasmallnumberofveryspecificanomaliesassociatedwithparticularconditions.Theseinclude,theteratogeniceffectsofparticulardrugstakenduringpregnancy,forexample,abnormalorabsentlimbs(phocomelia)associatedwiththalidomide,valproateembryopathyassociatedwithsodiumvalproatetreatmentforepilepsy,andcharacteristicskeletalabnormalitiesassociatedwithwarfariningestionduringpregnancy.19Someinfectiousdiseasesalsocausecharacteristicsanomalies,forexamplerubellainfectioncontractedduringpregnancycanresultintheclassictriadof:eyeandheartanomalieswithsensorineuraldeafness.Somewomenwhohavehadapreviouspregnancyaffectedbyacongenitalanomalyareatanincreasedriskofhavingafurtheraffectedpregnancy,forexampletherecurrenceriskofneural tube defects(spinabifidaandanencephaly)isabout5%.
Somespecificanomaliesareknowntohaveageneticoriginwhereparticulargenemutationsordeletionshavebeenidentified.Forexample,mostcasesofApert’s syndromeareduetoaspontaneousmutationaffectedoneoftwogenes.ThecauseofthemutationsisnotknownbutwhenoneorothermutationispresentApert’s syndromeresults.Apert’s syndromehasanautosomal dominant inheritance,sothatsomeonewith Apert’s syndromehasa1in2chanceofpassingtheconditionontotheirchildren.
Regardlessofthepatternofinheritance,geneticconditionsassociatedwithahighinfant mortality rate,forexample,campomelic syndromegenerallyoccursporadicallybecauseaffectedinfantstendnottosurvive.However,acouplewhohashadachildaffectedbyageneticconditionarelikelyinanysubsequentpregnancytohaveanincreasedriskofhavingafurtheraffectedchildandwillrequiregeneticcounselling.Dependinguponthecondition,insubsequentpregnanciesprenataldiagnosisthroughamniocentesisandtheterminationofanaffectedpregnancy,willbeofferedifanappropriategenetictestisavailable.Pre-implantation genetic diagnosismayalsobeappropriateifcouplesarewillingandabletoundergoinvitrofertilisation(IVF)treatment.Byidentifyingandtransferringonlyunaffectedembryos,pre-implantation genetic diagnosisavoidstheneedforterminationofanaffectedpregnancy.

Thecontributionofcongenitalanomaliestoinfantmortality8
Someconditionsareassociatedwithageneralincreaseintheriskofgroupsofcongenitalanomalies,althoughnotassociatedwithsinglespecificconditionsorsyndromes.Forexample,pregestationalmaternaldiabetesisassociatedwithanincreaseintheriskofcongenitalanomaliesoverall20andthereisevidencethatgestationaldiabetesisassociatedwithasimilartwofoldincreaseintheriskofanomaliesoverall.21Whilecardiac,skeletalandcentralnervoussystemanomaliesarethemostcommon,diabetes-associatedanomaliesusuallyinvolveoneormoreorgans.Whilsttheexactmechanismisunclearhyperglycaemiaisthoughttobetheprimaryteratogencausing,inparticular,cardiacanomalies.20AsaconsequencetheNICEguidancefordiabeticwomenduringpregnancyrecommendsthatwomenwithdiabeteswhoareplanningtobecomepregnantshouldbetoldthat“establishinggoodglycaemiccontrolsbeforeconceptionandcontinuingthisthroughoutthepregnancywillreducetheriskofmiscarriage,congenitalmalformation,stillbirthandneonataldeath.”22
Womenwhoareobesearealsoatanincreasedriskofarangeofcongenitalanomalies,includingcardiovascularanomalies,neuraltubedefects,cleftpalate,hydrocephalyandlimbreductiondefects.23Again,thecausalmechanism(s)underlyingtheseassociationsisunclear.Obesityanddiabetessharecommonmetabolicabnormalitiesincludinghyperglycaemiaandinsulinresistanceandundiagnoseddiabetesandhyperglycaemiaarepossibleexplanationsfortheincreasedriskofcongenitalanomaliesintheoffspringofobesewomen.Nevertheless,whilsttheevidenceisconflictingtheredoesappeartobeanindependentriskofobesityabovethatassociatedwithdiagnoseddiabetes.23Arolefornutritionaldeficienciesassociatedwithobesity,includingreducedfolatelevels,hasalsobeenpostulated.
Furthergenerallynon-specificriskfactorsforcongenitalanomaliesincludematernalage,cigarettesmoking,alcoholanddruguse.Therisksofanomaliesingeneralandchromosomalanomaliesinparticularincreasewithincreasingmaternalage;thereisalsogrowingevidenceoftheeffectsofolderpaternalageontheriskofdominantgenemutations,forexample,Apert’s syndrome.Therearesomespecificexceptionstotheincreaseinriskwithmaternalage,forexampletheriskofgastroschisisisinverselyrelatedtomaternalagewiththepeakbirth prevalenceinwomen<25yrs.Theriskofgastroschisisisalsoincreasedwithuseofrecreationaldrugs,particularlythosewithavasoconstrictiveaction,forexample,cocaine,amphetaminesandecstasy.24
Theroleofconsanguinityasariskfactorforcongenitalanomaliesandinfantdeathiscomplexandstudiesinthepastoftenfailedtoaccountforsocio-economiccircumstancesandotherimportantconfounders.25DatafromPakistan,intheearly1990swhere61%ofmarriageswerebetweenfirst(50%)andsecondcousins(11%),enabledadjustmentforsocio-economicandotherfactors.Againstabackgroundinfant mortality rateof99per1,000live births,infantsoffirstcousinshada42%increasedriskofdeathinthefirstyearandforsecondcousinstheincreasewas24%.25TheoverallcontributionofconsanguinitytoinfantmortalitygenerallyandinfantmortalityduetocongenitalanomaliesintheUKwillinevitablybesmallsincefirstandsecondcousinmarriagesaregenerallyuncommon.26However,aswasfoundinBradford,theburdenwillbedisproportionallybornebygroupsinthepopulationwherecousinmarriagesaremorecommon,forexample,couplesofPakistaniorigin(Figure5).17Ofnoteconsanguinityisparticularlyassociatedwithgeneticconditionswhichhaveanautosomal recessivepatternofinheritance.
4.2 Primarypreventionofcongenitalanomalies
Theprimary preventionofcongenitalanomaliesisonlypossibleforaverysmallrangeofspecificanomaliesforwhichthereiseitheraknowncause,orevenintheabsenceofaclearunderstandingofthecause,ameansofpreventionhasbeenidentified.Onapopulationleveltheseincludechildhoodrubellaimmunisation,screeningandtreatmentforsyphilisduringpregnancy,periconceptionalfolicacidsupplementationand/orfolatefoodfortificationforthepreventionofneuraltubedefects.Onanindividuallevel,optimisingthemanagementofwomenathigherrisk,forexample,forwomenwhoarediabeticorepileptic,istheidealapproachtominimisingtherisksofanomalies.However,asabout40%ofpregnanciesintheUKareunplanned27thisapproachisnotalwayspossibleeveninthosewomenathigherriskofproblemsintheirpregnancy.Furthermore,sincerelativelyfewoftheanomaliesgivenintheseexampleswouldresultindeathsininfancy,whilstthegoalofreducingtheriskofanomaliesisimportant,itmayhaverelativelylittleimpactontheinfant mortality rate.
4.3 Secondarypreventionofcongenitalanomalies
TherearetwomainmethodsofprenatalscreeningrelatingtocongenitalanomaliesavailableintheUK.ScreeningforDown’s syndrome(trisomy21)whichaffectsabout2.6per1,000pregnanciesisofferedinthefirstorsecondtrimesters.28ScreeningforDown’s

Thecontributionofcongenitalanomaliestoinfantmortality 9
mayalsodetecttheratherrarerconditionsofEdward’s syndrome(trisomy18;0.7per1,000pregnancies)andPatau’s syndrome(trisomy13;0.2per1,000pregnancies).28AlthoughDown’s syndromeisassociatedwithanincreasedriskofmiscarriageorstillbirth,itisararecauseofinfantdeathandwhenadeathdoesoccurisitusuallyduetoacardiacanomalytowhichinfantswithDown’shaveanincreasedrisk.Frommaternalreportitisestimatedthatabout65%ofwomentakeuptheofferofscreeningforDown’s syndrome.15Lackofuniversaluptakeprobablyreflectsfirst,afailureofuniversalofferofscreeningandtheextenttowhichthisoccursandthereasonswhyareunclear;15andsecond,adesirebysomewomennottoterminatetheirpregnancyevenifthefetusisaffectedbyDown’s syndrome.Perceptionsofa‘good’reproductiveoutcomeareverypersonalandinfluencedbymanysocial,culturalandreligiousfactors.
Thesecondmainformofuniversalprenatalscreeningisdetailedsecondtrimesterultrasoundscanningusuallyofferedbetween18to20completedweeksgestationandwhichisdesignedtoassessfetalgrowthandidentifystructuralcongenitalanomaliesincludingsomestructuralanomaliesassociatedwithchromosomaldefects.DespitethefactthattheconsequencesofdetectionofanomaliesthroughthisrouteisthesameasforDown’s syndrome,uptakeofsecondtrimesterultrasoundscanningishigherthantheuptakeofDown’s syndromescreening.Thisispossiblybecausemanywomenmaybeunclearaboutthepurposeofthescanandviewitprimarilyasasourceofreassuranceandofpicturesoftheirbaby.29
Prenataldetectionratesvarybyanomaly(Table1).Itisimportanttonotehowever,thatonlyarelativelysmallproportionofthesecaseswouldcontributetotheinfant mortality rateeveniftheyremainedundetectedprenatally.Themaincontributorstoinfantdeathsfortheseselectedanomalieswouldbeaminorityofthecardiacdefects,themoreseverecasesofcongenital diaphragmatic herniaandaminorityofthechromosomalanomalies.
Table 1. Prenatal detection rates for selected isolated* congenital anomalies,
data from the Congenital Anomalies Register for Oxfordshire, Berkshire and Buckinghamshire (CAROBB)2005-200810
Selected isolated* anomalies
Detection rate (%) 95%CI
Neural tube defects 95% 89%-98%
Cardiacanomalies 35% 30%-42%
Cleftlip+/-palate 65% 53%-75%
Congenital diaphragmatic hernia
64% 41%-83%
Gastroschisis 100% 93%-100%
Exomphalos 90% 68%-99%
Chromosomal 56% 50%-62%
*Isolated–noothercongenitalanomaliespresent
Onanindividualbasiscouplesidentifiedasbeingatincreasedriskofgeneticconditionswillbeofferedgeneticcounsellingandwheresuitabletestsareavailable,theywillbeofferedprenataldiagnosisthroughamniocentesisinasubsequentpregnancy.Asdiscussedabovepre-implantation genetic diagnosismayalsobeanoption.
5 Conclusions
CongenitalanomaliesarethesecondcommonestcauseofinfantdeathsinEnglandandWales,althoughthevastmajorityofinfantsbornwithacongenitalanomalywillsurvivewithanearnormallifeexpectancy.Theunderlyingcauseofmostcongenitalanomaliesisnotknown.TherearemanydifferentcongenitalanomaliesandinanysingleyearinfantdeathsduetocongenitalanomaliesinEnglandandWalesareassociatedwithover150differentcauses.Congenitalanomaliescontributeaboutonethirdoftheextrainfantdeathsexperiencedbytheroutineandmanualgroupscomparedwiththepopulationasawhole.
Theprimary preventionofcongenitalanomaliesrequiresmanydifferentactivitiesandthedeliveryofahighstandardofuniversalpre-pregnancyandpregnancycareforwomeningeneraltogetherwithoptimisationofmanagementbeforeconceptionforspecificwomenathigherriskofanomalies,forexample,womenwithdiabetes,epilepsyandthosetakingotherspecificdrugswithteratogeniceffects.Theavailabilityofgeneticservicesisessentialforcoupleswithafamilyhistoryorpasthistoryofpregnanciesaffectedbycongenitalanomalies,particularlyduetospecificgeneticconditions.Somesectionsofthepopulationareatincreasedriskofparticulargeneticconditionsandasaconsequenceinfant

Thecontributionofcongenitalanomaliestoinfantmortality10
mortality ratesduetocongenitalanomaliesmaybehigherthaninthepopulationingeneral;geneticserviceswillbeofparticularimportanceintheseareas.
Secondary preventionofcongenitalanomaliesisachievedthroughprenatalscreeninganddiagnosisfollowedbytheofferofterminationofpregnanciesaffectedbymajoranomalies.Becauseterminationofpregnancyistheonly‘therapeutic’optionformanycongenitalanomaliessecondary preventionisnotuniversallyacceptable.
Infant mortality ratesduetocongenitalanomaliesarestronglyinfluencedbyprenatalscreeninganddiagnosis,anduptakeofterminationofpregnancy.However,itisimportanttonote,thatmanyoftheanomalieswhichcanbepreventedthroughprimaryorsecondaryactionswouldnotinanycasehaveresultedinaninfantdeathandthustheirprevention,althoughofgreatimportancebecauseoftheassociatedmorbidityanddisability,willnotnecessarilyimpactontheinfant mortality rate.
Glossary
Apert’s syndrome –ararecongenitaldisordercharacterisedbymalformationsoftheskull,face,handsandfeetwhichrequiresextensivesurgery.ItisalmostalwayscausedbyaspontaneousgenemutationofpaternaloriginandtheriskofApert’ssyndromeincreaseswiththeageofthefather.
Autosomal dominant genetic inheritance –thisisthemechanismofinheritanceofgeneticconditionswhicharecausedbyasinglegeneinheritedfromoneparent.Someonewhocarriesthegeneforanautosomaldominantconditionwillalwaysbeaffectedbytheconditionandeachoftheirchildrenwillhavea1in2chanceofinheritingthecondition.
Autosomal recessive genetic inheritance –thisisthemechanismofinheritanceofgeneticconditionswhichrequiresasinglegenefrombothparentstobeaffectedinorderfortheirchildtobeaffected.Carriersofrecessivegenesarethemselvesnotaffectedbutiftheyhaveachildwithsomeonewhoisalsoacarriereachchildtheyhavewillhavea1in4chanceofbeingaffectedbythecondition.
BINOCAR –BritishIslesNetworkofCongenitalAnomaliesRegisters.
Birth prevalence –isthemeasureoffrequencyofoccurrenceusuallyusedinrelationtocongenitalanomalies.Thetermincidenceisnotusedinacknowledgementofthefactthatmanyembryos
andfetusesaffectedbyacongenitalanomalyaremiscarriedandthereforenotcountedintheratecalculation.Birthprevalenceisthenumberofnewcasesofcongenitalanomaliesborn(live birthsandstillbirths)dividedbythetotalnumberofbirths.
Campomelic syndrome –araresinglegenedefectwithautosomaldominantinheritancewhichresultsinabnormalitiesofthebonesandthecartilageoftherespiratorytract.Almostwithoutexceptionaffectedbabiesdieintheneonatalperiodfromrespiratorycomplications.Thecharacteristicbonefeaturescanbediagnosedonprenatalultrasound.Thereisnotreatmentavailable,otherthantoproviderespiratorysupporttobabiesbornalive.Itaffectsabout1in500,000pregnancies.
CAROBB –CongenitalAnomaliesRegisterforOxfordshire,BerkshireandBuckinghamshire.
Consanguinity –unionscontractedbetweenpersonsbiologicallyrelatedassecondcousinsorcloser.Thisarbitrarylimithasbeenchosenbecausethegeneticinfluenceinoffspringfrommarriagesbetweencouplesrelatedtoalesserdegreewouldusuallybeexpectedtodifferonlyslightlyfromthatseeninthegeneralpopulation.Globally,themostcommonformofconsanguineousmarriageisbetweenfirstcousins,inwhichthespousesshare1/8oftheirgenesinheritedfromacommonancestor.
Down’s syndrome –isoneofthemorecommonchromosomaldisordersduetohavingpartorallofanextrachromosomenumber21.Itischaracterisedbyaseriesofmajorandminorstructuralabnormalities,forexample,asmallchin,anunusuallyroundface,alargetongueandalmondshaped,widelyspacedeyes.Cognitiveimpairmentisusuallypresent,althoughtheextentisvariable.Healthconcernsincludeahigherriskofcongenitalheartanomalies,recurrentearinfections,obstructivesleepapnoea,thyroiddisease,leukaemiaandearlyonsetAlzheimer’sdisease.
Edward’s syndrome –isachromosomaldisorderduetohavingpartorallofanextrachromosomenumber18.Infantshavemultipleanomaliesaffectingtheheart,kidney,intestines(exomphalos).Themajorityofaffectedinfantsdiewithinthefirstmonthafterbirthandonly10%survivetoageoneyear.Longtermsurvivalisveryuncommon.
Embryo –Inhumansduringpregnancy,anembryoisthedevelopingorganismfromthetimeoffertilisationuntiltheendoftheeighthweekofgestation,followingwhichitiscalledafetus.

Thecontributionofcongenitalanomaliestoinfantmortality 11
Exomphalos –isadefectintheabdominalwallthroughtheumbilicusthroughwhichtheintestinesandotherorgansdevelopoutsidetheabdomen.Itismorecommonlyassociatedwithothercongenitalanomalies,forexampletrisomy 18,thangastroschisisandasaconsequencethelongtermoutcomeislessfavourablethanforgastroschisis;terminationofaffectedpregnanciesismorecommon.
Fetus –Inhumansduringpregnancy,afetusisthedevelopingorganismfromtheendoftheeighthweekofgestationuntilbirth.
Gastroschisis –isadefectintheabdominalwalltoonesideoftheumbilicusthroughwhichtheintestinesandotherorgansdevelopoutsideoftheabdomen.Itisrarelyassociatedwithothercongenitalanomalies.Surgicalrepairofthedefectisrequiredfollowingbirthwiththemajorityoftheinfantstreatedhavingagoodlong-termoutcomealthoughcomplicationscanarise.
ICD10 classification system –TheInternationalStatisticalClassificationofDiseasesandRelatedHealthProblems10thRevision(ICD-10)isacodingofdiseasesandsigns,symptoms,abnormalfindings,complaints,socialcircumstancesandexternalcausesofinjuryordiseases,asclassifiedbytheWorldHealthOrganisation.
Incidence rate –isameasureoftheoccurrenceofnewcasesofadiseaseinapopulation.Thisisincontrasttoprevalencewhichisameasureofbothnewcasesandexistingcasesinthepopulation.Inthefieldofcongenitalanomaliesthetermbirthprevalenceisratherconfusinglyusedtodescribenewcasesofanomalies.Birthprevalenceisusedbecauseweknowthatmanynewcasesofanomaliesdonotsurviveinpregnancylongenoughtobeidentifiedsincetheyaremiscarried.Wethereforecannotknowaboutallnewcasesofaparticularanomaly.
Infant mortality rate –numberofdeathsatagesunderoneyearper1,000live births.
Live birth –birthofaninfantshowinganysignsofliferegardlessofgestationatbirth.
National Statistics Socio-Economic Classification (NS-SEC) –amethodofcodingsocio-economicpositiononthebasisofoccupationintroducedin2002toreplacetheStandardOccupationalClassificationwhichcodedoccupationtotheRegistrarGeneral’sSocialClass.NS-SEChasaseriesofanalyticalclasseswhicharenominalintheextended14operationalcategoriesformandwhichbecomeordinalwhencollapsedintothethree-classversion.Infantmortalitystatisticsarepublishedusingtheeight-classanalyticalversion:
1.1Largeemployersandhighermanagerial1.2Higherprofessional2 Lowermanagerialandprofessional3 Intermediate4 Smallemployerandown-account
workers5 Lowersupervisoryandtechnical6 Semi-routine7 Routine8 Neverworkedandlong-term
unemployedUnclassifiable
NCAS –NationalCongenitalAnomaliesSystemforEnglandandWales.
Neonatal mortality rate –numberofdeathsatagesunderfourweeksper1,000live births.
NorCAS –NothernCongenitalAbnormalitySurvey.
NS-SEC –seeNational Statistics Socio-Economic Classificationabove.
Neural tube defects –agroupofconditionscausedbythefailureofclosureoftheneuraltubeduringembryonicdevelopmentduringthefirst28daysafterfertilisation.Theneuraltubeformsthebrainandspineandthetypeofneuraltubedefectwhichoccursdependsuponwhereonthespineorbrainthefailuretocloseoccurs.Ifitaffectsthebrainaconditioncalledanencephalyresultswherethebrainfailstodevelop;aconditionincompatiblewithlife.Whenitaffectsthespine,spinabifidaresultsanditseffectsdependuponwhereonthespinethedefectoccurs;thehigherupthemoreserioustheeffectandthemorecomplicationsthatresult.
ONS cause (of death) groups hierarchical classification –aclassificationsystemdevelopedtoenablecomparisonofneonatalandpost-neonataldeathsfollowingachangeindeathscertificatesforneonataldeathsandstillbirthswherebyasingleunderlyingcauseofdeathwasnolongerassigned.Thissystemallowsthedeathtobeassignedhierarchicallytoaspecificcategorybasedonthelikelytimingofthedamageleadingtothedeath:
Before the onset of labour11.Congenitalanomalies12.Antepartuminfections13.Immaturityrelatedconditions
In or shortly after labour14.Asphyxia,anoxiaortrauma
Postnatal15.Externalconditions16.Infections17.Otherspecificconditions
Thecontributionofcongenitalanomaliestoinfantmortality12
9. Suddeninfantdeaths
Unclassified0. Otherconditions
Patau’s syndrome –isachromosomaldisorderduetohavingpartorallofanextrachromosomenumber13.Infantshavemultipleanomaliesaffectingtheheart,kidney,andotherorgansincludingneurologicaleffects.Stillbirthiscommonandthemajorityofaffectedinfantsdiewithinthefirstmonthafterbirth.
Postneonatal mortality rate –numberofdeathsat28daysandoverbutunderoneyearper1,000live births
Pre-implantation genetic diagnosis –requiresinvitrofertilisation(IVF)followingwhichasinglecellisremovedfromthedevelopingembryostotestforspecificgeneticconditions.Onlyunaffectedembryosarethentransferredtotheuterus.Itisonlyavailableforgeneticconditionswhereadiagnostictestcanbeperformed.
Primary prevention –actionstakentoavoiddiseaseorinjuryoccurringinthefirstplace.Examplesofprimarypreventionincludevaccinationagainstinfectiousdiseases.
Secondary prevention –actionstakentoidentifyandtreatanillnessorinjuryearlyoninitsdevelopmentwiththeaimofstoppingorreversingtheproblem.Examplesincludescreeningfordiseaseswhichcanthenbetreatedearlierthanwouldusuallybethecase.
Stillbirth –birthofaninfantat≥24weeksgestationshowingnosignsoflife.
Teratogen –anyagentwhichcausesabnormalitiesofembryonicorfetaldevelopment,examplesincludespecificdrugs(egthalidomide),X-raysandsomeviruses(egrubella).
TOPFA –terminationofpregnancyforfetalanomaly.TOPFAisofferedfollowingprenataldiagnosisofmajorcongenitalanomalies.
Acknowledgements
WewouldliketothankmembersoftheInequalitiesinInfantMortalityAdvisoryGroupfortheirhelpfulcommentsonanearlierdraft.ParticularthankstoNirupaDattaniattheOfficeforNationalStatisticsforprovidingadatadownloadofmortalityratesduetocongenitalanomaliesbysocio-economicposition.
ThisbriefingpaperreportsonanindependentstudywhichwasfundedbythePolicyResearchProgrammeintheDepartmentofHealth.TheviewsexpressedarenotnecessarilythoseoftheDepartment.
WearegratefultoDrJudithBuddattheEastMidlandsandSouthYorkshireCongenitalAnomaliesRegister,whokindlyprovidedthemapoftheBINOCARregisters.
References1. KurinczukJJ,HollowellJ,BrocklehurstP,GrayR.
InequalitiesinInfantMortalityProjectBriefingPaper1.Infantmortality:overviewandcontext.Oxford:NationalPerinatalEpidemiologyUnit,UniversityofOxford.2009.
2. GrayR,HollowellJ,BrocklehurstP,GrahamH,KurinczukJJ.InequalitiesinInfantMortalityProjectBriefingpaper2.Healthinequalitiesinfantmortalitytarget:technicalbackground.Oxford:NationalPerinatalEpidemiologyUnit,UniversityofOxford.2009.
3. GrayR,HeadleyJ,OakleyL,KurinczukJJ,BrocklehurstP,HollowellJ.InequalitiesinInfantMortalityProjectBriefingpaper3.TowardsanunderstandingofvariationsininfantmortalitybetweendifferentethnicsgroupsinEnglandandWales.Oxford:NationalPerinatalEpidemiologyUnit,UniversityofOxford.2009.
4. MooreKL,PersaudTVN.Chapter8.HumanBirthDefects.In:TheDevelopingHuman:ClinicallyOrientatedEmbryology.Philadelphia:Saunders2003.p157-186.
5. BoydPA,ArmstrongB,DolkH,BottingB,PattendenS,AbramskyLetal.CongenitalanomalysurveillanceinEngland–ascertainmentdeficienciesinthenationalsystem.BrMedJ2005;330:27
6. BINOCARwebsiteavailableat:http://www.binocar.org/[AccessedApril2010]
7. NewtonJ,GarnerS.DiseaseRegistersinEngland.Oxford:InstituteofHealthSciences,UniversityofOxford.2002.ISBN1840750286
8. CAROBBwebsiteavailableat:http://www.npeu.ox.ac.uk/carobb[AccessedApril2010]
9. NorCASwebsiteavailableat:http://www.nepho.org.uk/rmso/surveys/congenital[AccessedApril2010]
10. BoydPA,RoundingC,KurinczukJJ.SecondReportoftheCongenitalAnomalyRegisterforOxfordshire,BerkshireandBuckinghamshire(CAROBB)Births2005to2008.Oxford:NationalPerinatalEpidemiologyUnit,UniversityofOxford.2009.
11. BowerC,RudyE,CallaghanA,QuickJ,CosgroveP,NassarN.ReportoftheBirthDefectsRegistryofWesternAustralia,Number16:1980-2008.Subiaco,Perth:KingEdwardMemorialHospital.2009
12. KurinczukJJ,DraperES,BuddJLS,PerkinsMJ,ClarkeM.TrentCongenitalAnomaliesRegister.TheFirstFiveYears:CongenitalAnomaliesinBirths1997-2001.Leicester:DepartmentofHealthSciences,UniversityofLeicester.2003.
Thecontributionofcongenitalanomaliestoinfantmortality 13
Pleasecitethisdocumentas:
JenniferJKurinczuk,JenniferHollowell,PatriciaABoyd,LauraOakley,PeterBrocklehurst,RonGray.Inequalitiesininfantmortalityprojectbriefingpaper4.Thecontributionofcongenitalanomaliestoinfantmortality.Oxford:NationalPerinatalEpidemiologyUnit,2010
ThisbriefingpaperandotherInequalitiesinInfantMortalityProjectreportsareavailableat:
www.npeu.ox.ac.uk/infant-mortality
13. OfficeforNationalStatistics.MortalityStatistics,Childhood,InfantandPerinatal.ReviewoftheNationalStatisticianondeathsinEnglandandWales,2007.SeriesDH3number40.London:OfficeforNationalStatistics.2009.
14. TennantPW,PearceMS,BythellM,RankinJ.20-yearsurvivalofchildrenbornwithcongenitalanomalies:apopulation-basedstudy.Lancet2010;375:649-56.
15. RoweR,PuddicombeD,HockleyC,RedshawM.OfferanduptakeofprenatalscreeningforDownsyndromeinwomenfromdifferentsocialandethnicbackgrounds.PrenatDiag2008;28:1245-50.
16. MoserK,StanfieldKM,LeonDA.Birthweightandgestationalagebyethnicgroup,EnglandandWales2005:introducingnewdataonbirths.HealthStatisticsQuarterlyAutumn2008;39:22-31.
17. HelenBrownandtheBradfordHealthInformaticsServiceteam.BradfordInfantMortalityCommission:Analysisandinterpretationofinfantmortalitydata.Bradford2006.Availableat:http://www.bradford.nhs.uk/ebm/BDIMC/Pages/TheReport.aspx[AccessedApril2010].
18. HealthInequalitiesUnit,DepartmentofHealth.ReviewoftheHealthInequalitiesInfantMortalityPSATarget.London:DepartmentofHealth.2007.
19. HolmesLB.Teratogen-inducedlimbdefects.AmJMedGenet2002;112:297-303.
20. CorriganN,BrazilDP,McAuliffeF.Fetalcardiaceffectsofmaternalhyperglycemiaduringpregnancy.BirthDefectsResAClinMolTeratol2009;85:523-30.
21. MacintoshMCM,FlemingKM,BaileyJA,DoyleP,ModderJ,AcoletDetal.Perinatalmortalityandcongenitalanomaliesinbabiesofwomenwithtype1ortype2diabetesinEngland,WalesandNorthernIreland:populationbasedstudy.BrMedJ2006;333:177
22. NationalCollaboratingCentreforWomen’sandChildren’sHealth.NICEguideline:Diabetesinpregnancy.London:RoyalCollegeofObstetriciansandGynacologists.2008
23. StothardKJ,TennantPW,BellR,RankinJ.Maternaloverweightandobesityandtheriskofcongenitalanomalies:asystematicreviewandmeta-analysis.JAMA2009;301:636-50.
24. DraperES,RankinJ,TonksAM,AbramsKR,FieldDJ,ClarkeM,KurinczukJJ.Recreationaldruguse:amajorriskfactorforgastroschisis?AmJEpidemiol2008;167:485-91
25. GrantJC,BittlesAH.ThecomparativeroleofconsanguinityininfantandchildhoodmortalityinPakistan.AnnHumGenet1997;61:143-9.
26. http://www.consang.net/index.php/Global_prevalence[AccessedApril2010]
27. JayaweeraH,JoshiH,MacfarlaneA,HawkesD,ButlerN,PregnancyandChildBirth.In:DexS&JoshiH(Eds)Childrenofthe21stCentury:FromBirthto9months.TheUKMillenniumCohortStudySeries.PolicyPress:Bristol.2005
28. MorrisJK,DeSouzaE.TheNationalDownSyndromeCytogeneticRegisterforEnglandandWales:2008/09annualreport.London:WolfsonInstituteofPreventiveMedicine,QueenMarchUniversityofLondon.2009
29. GarciaJ,BrickerL,HendersonJ,MartinMA,MugfordM,NielsonJ,RobertsT.Women’sviewofpregnancyultrasound:asystematicreview.Birth2002;29:225-50.