
The Continuum of Organ Donation: A Panel … for Transplant •Specialty transplant floors that care...
74
The Continuum of Organ Donation: A Panel Discussion Nebraska Medicine Omaha, Nebraska
Transcript of The Continuum of Organ Donation: A Panel … for Transplant •Specialty transplant floors that care...
The Continuum of
Organ Donation:
A Panel Discussion
Nebraska Medicine
Omaha, Nebraska
Panel Members
• Lisa Butler-Walker, TFC
• Kyle Dorn, RN
• Megan Gregory, BSN, RN
• Leigh Lindner, BSN, RN, CMSRN
• Amber Saltsgaver, BSN, RN
• Amy Schurke, BSN, RN, CCTC
• Karen Townsley, BSN, RN, CCTN
The Process of How a
Patient Gets Listed for
Transplant: Duties of the
Pre-Transplant Team
Leigh Lindner, BSN, RN, CMSRN
Transplant Coordinator
How Patients Get to Nebraska Medicine
• Referral from their local MD
• Self-referral
• Inpatient at Nebraska Medicine
• Providers within the transplant teams
• Insurance Companies
We are a Center of Excellence
• Dialysis Centers
After Referral
• Coordinator calls
Educate them about our program and the evaluation process
Review their PMH
Collect insurance information
o Financial Counselors obtain insurance auth
Request outside records from all providers
**Once Obtained: Clerical Staff Schedules the Evaluation**

Evaluation
• 2-5 Consecutive days of Outpatient testing
Labs - Social Work
Imaging/Procedures - Psychology
o Abd US, Cxray, EKG, ECHO, - Psychiatry (if needed)
DSE, Mammo, PFTs
Cardiology - Financial Counselor
Individual Organ Specialty - H&P
o Hepatology, Nephrology - Pharmacy Financial
Counselor
o Pulmonology, Cardiology - Nutritionist
Transplant Coordinator - Other services and testing
Transplant Surgeon
**Testing is based on each individual person**
Patient Selection Committee
• Every organ team meets weekly
Each member of the team presents the info they gathered
We make a TEAM DECISION
o Further testing
o Too early
o Compliance
– Medical, psychosocial, drug/ETOH
o Does not meet criteria for listing (not approved)
o List for transplant
Listed Patients
• To List:
Transportation needs to be arranged
Financial Counselors get clearance from
insurance companies
Each organ submits specific information to Donate
Life Services (DLS)
o DLS submits listing to United Network of Organ
Sharing (UNOS)
Listed Patients
• While patients are Listed:
Monitor/Submit labs to DLS as appropriate
Maintain communication with patients
Schedule/Review any necessary testing – organ
specific
Maintain the requirements of listing
Annual/Bi-annual reviews
What Does This Have to Do With BURNOUT?
• There can be frustration when a patient really needs a transplant evaluation and insurance denies them to come to Nebraska Medicine
• Obtaining records
• Compliance
• Telling people they are not a candidate for transplant
• We get to know some of our patients really well since we follow them closely; it can be hard when they die while waiting for transplant
• We often take on other workload/tasks
• On call
Financial Aspects
of Transplant
Lisa Butler WalkerTransplant Financial Counselor
Transplants
• Necessary
• Important
• Expensive
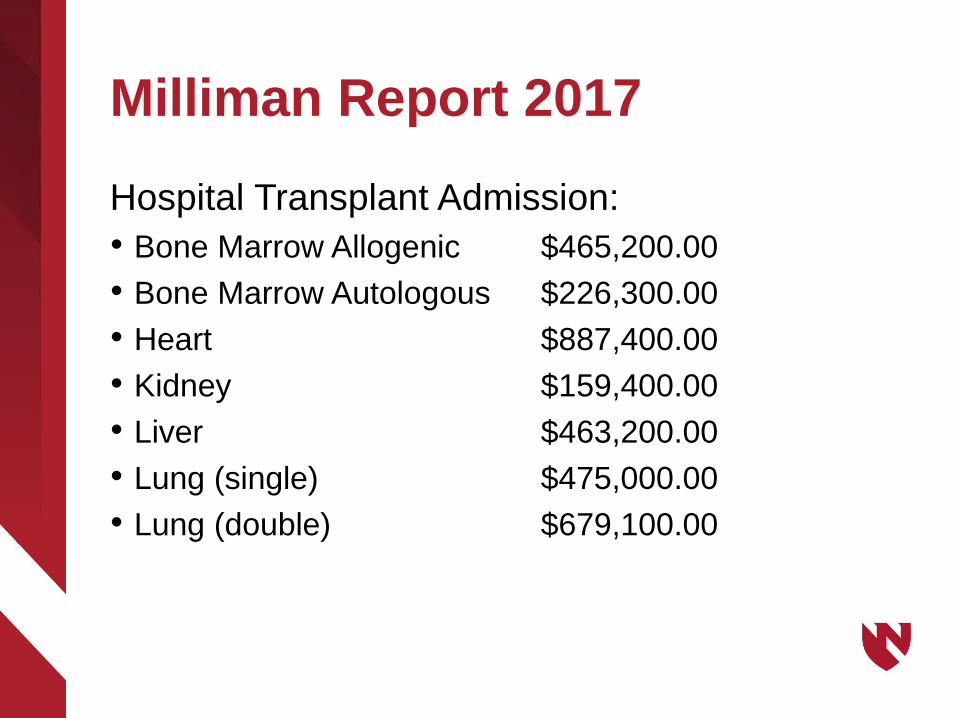
Milliman Report 2017
Hospital Transplant Admission:
• Bone Marrow Allogenic $465,200.00
• Bone Marrow Autologous $226,300.00
• Heart $887,400.00
• Kidney $159,400.00
• Liver $463,200.00
• Lung (single) $475,000.00
• Lung (double) $679,100.00
Transplant Financial Counselors
• Verify patient’s insurance
• Provide financial information to the patient as well as
the patient’s family
• Ensure we provide the correct financial to the
physician as well as the facility we work for
How Patients are Referred
• Current patient
• Referred from another doctor or facility
• Current inpatient referral
• Globally
• Self referral
Candidate Transplant Process
• Consult, inpatient, physician referral
• Verify insurance
• Transplant coordinator / physician discussion
• Authorization for evaluation
• Evaluation
• Patient Selection Committee
Transplant Financial Counselor Burn Out
• Patient’s insurance won’t pay for a transplant at our
facility
• Patient dies before transplant
• Emotional connection with a patient that has passed
away
• Patient does not qualify for a transplant
• Workload
• Denial


The need for donors
118,000+
waiting list––––––
22 die each day
+ 1 every 10 minutes
––––––
Nebraska Organ Recovery (NORS)
• Established in 1977
• Federally designated Organ Procurement Organization (OPO) serving Nebraska and Pottawattamie County in Iowa
• Non-profit
• Independent of all hospitals and transplant centers
• Cadaveric organ and tissue procurement
Organ Donor Criteria
1. Patient must be ventilated in a hospital2. Patient must have a devastating injury or illness3. Patient must be declared brain dead based on
hospital protocol, or meet Donation after Circulatory Death (DCD) protocol
• Additional criteria• No age restrictions (brain dead only)• Very few medical rule outs• Organ function is important

Medical Management
• 24-72 hours in the ICU• Blood draw
• Hospital labs, serology testing, HLA
• Evaluate and optimize organ function• Echo, EKG, heart cath, bronch, CT
• Organ allocation– Facilitated through UNOS– Recipient list by organ
• Blood type, tissue type, recipient condition, donor condition, size, weight
• Transport to OR

Donate Life
Services:Our Part in the BIG Picture
Megan Gregory, BSN, RN
Nurse Coordinator

The Offer
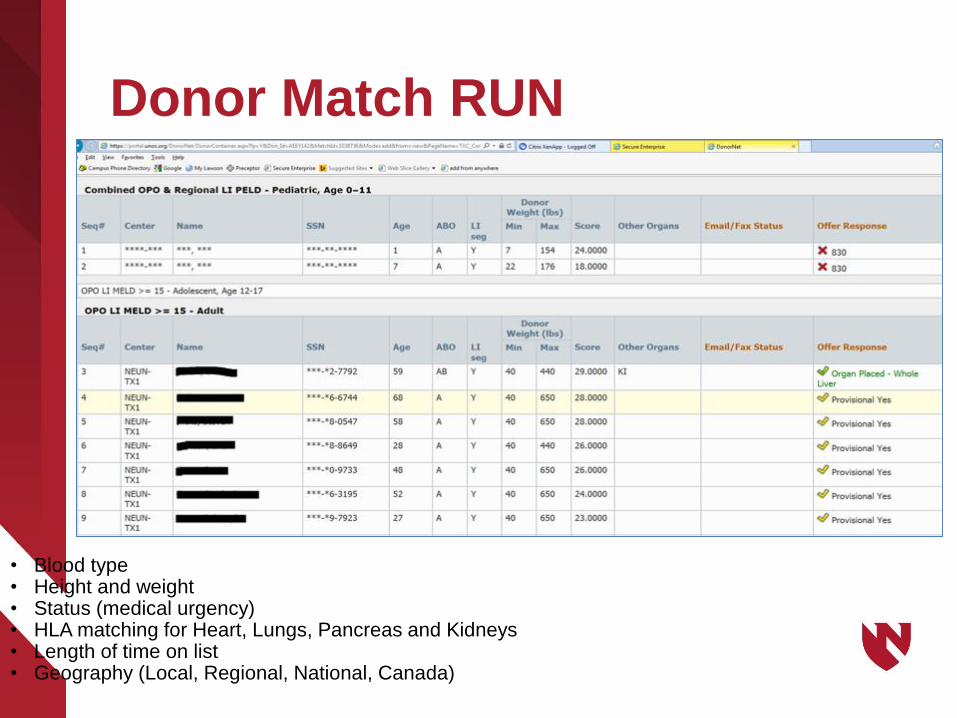
Donor Match RUN
• Blood type• Height and weight• Status (medical urgency)• HLA matching for Heart, Lungs, Pancreas and Kidneys• Length of time on list• Geography (Local, Regional, National, Canada)
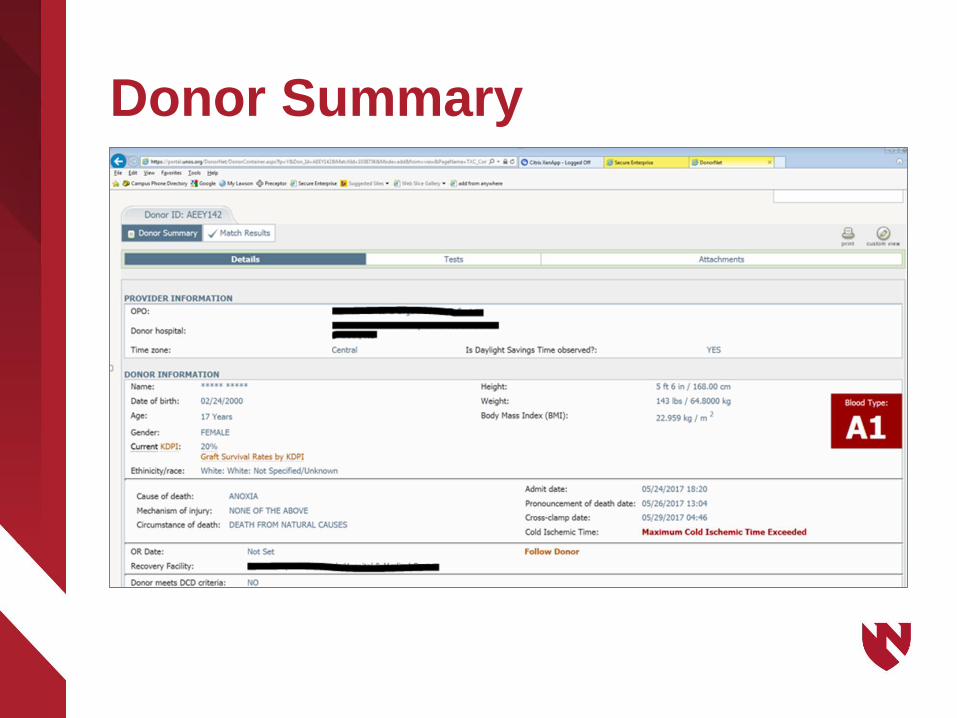
Donor Summary
Accepting an Organ
• Surgeon: Case details
• Organ Coordinator: Get recipient moving
• Transportation: Commercial/Charter
• Recipient OR: Schedule the case
• Pharmacy: Any medication supplies
• OPO: Set up details (OR time, extra
specimens, a ride)

Road Trip
Taking Off
In-Flight Details
Donor Hospital
Packing Up
Optimal Preservation Times
• Heart 4 Hours
• Lung 4-6 Hours
• Pancreas 12-18 Hours
• Liver6-8 Hours
• Kidney 24-48 Hours
• Intestine 6-12 Hours
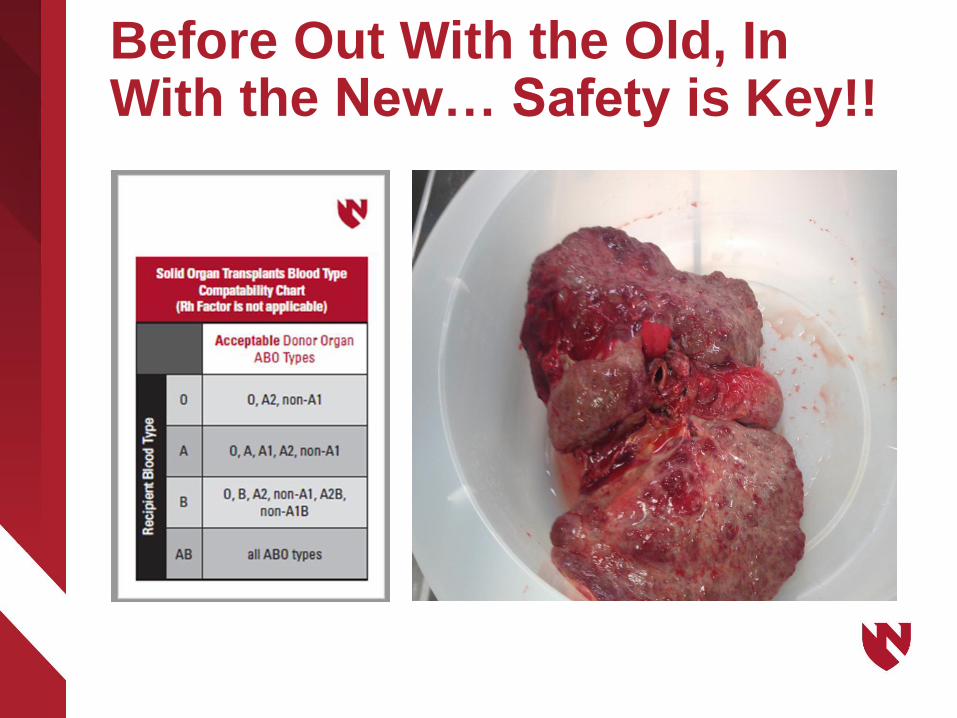
Before Out With the Old, In With the New… Safety is Key!!
Burn Out
• Long and irregular hours
• Sleep deprivation (24-hour+ shifts)
• On call commitments (24/7/365)
• Poor quality of “off” call time
• Insufficient resources
• Excessive workloads
• Lack of family time
Solid Organ
Transplant Unit –Inpatient Aspect
Karen Townsley, BSN, RN, CCTN
Clinical Education Coordinator for SOTU
Admission for Transplant
• Specialty transplant floors that care for patients pre-transplant, during the transplant phase, and post-transplant:
Solid Organ Transplant Unit (SOTU) for abdominal organs
Cardiac Progressive Care Unit (CPCU) for thoracic organs
• Patient may already be in hospital
• If patient not in hospital, they are admitted preferably to specialized transplant floor or possibly go to Pre-op directly
• Hibiclens (Chlorahexadine – CHG) pre-op:
o Planned surgeries – living donors encouraged to CHG bath/shower at home
o Part of the admission order set to be done prior to pre-op
• Transfer to Pre-op for surgery
After Transplant Surgery
• Kidney and Pancreas transplant recipients return to
SOTU from PACU when stable after being extubated
and discharge from SOTU
• All other transplant recipients transfer to the specialty
ICU for cares post-op up to 24-48 hours then return
to specialty transplant floor (SOTU or CPCU) when
stable after being extubated until discharge:
Surgical Intensive Care Unit (SICU) for abdominal
organs
Cardiovascular Intensive Care Unit (CVICU) for
thoracic organs
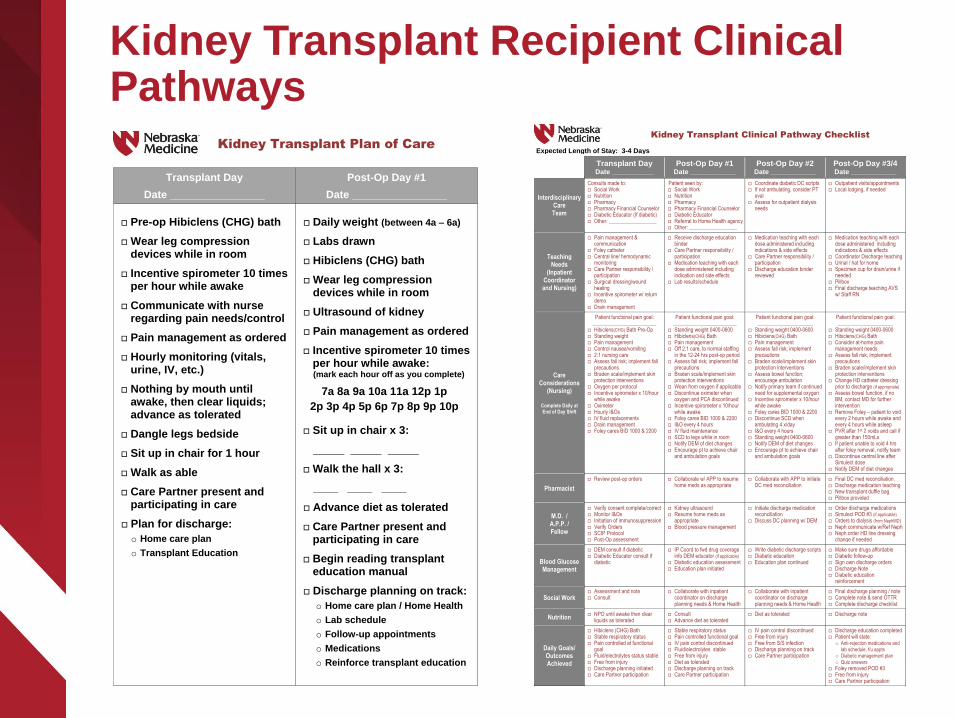
Kidney Transplant Recipient Clinical Pathways
Kidney Transplant Plan of Care
Transplant Day
Date ________________
Post-Op Day #1
Date ________________
Pre-op Hibiclens (CHG) bath
Wear leg compression devices while in room
Incentive spirometer 10 times per hour while awake
Communicate with nurse regarding pain needs/control
Pain management as ordered
Hourly monitoring (vitals, urine, IV, etc.)
Nothing by mouth until awake, then clear liquids; advance as tolerated
Dangle legs bedside
Sit up in chair for 1 hour
Walk as able
Care Partner present and participating in care
Plan for discharge:
o Home care plan
o Transplant Education
Daily weight (between 4a – 6a)
Labs drawn
Hibiclens (CHG) bath
Wear leg compression devices while in room
Ultrasound of kidney
Pain management as ordered
Incentive spirometer 10 times per hour while awake: (mark each hour off as you complete)
7a 8a 9a 10a 11a 12p 1p
2p 3p 4p 5p 6p 7p 8p 9p 10p
Sit up in chair x 3:
_____ _____ _____
Walk the hall x 3:
____ ____ ____
Advance diet as tolerated
Care Partner present and participating in care
Begin reading transplant education manual
Discharge planning on track:
o Home care plan / Home Health
o Lab schedule
o Follow-up appointments
o Medications
o Reinforce transplant education
Kidney Transplant Clinical Pathway Checklist
Expected Length of Stay: 3-4 Days
Transplant Day Date ___________
Post-Op Day #1 Date ____________
Post-Op Day #2 Date ____________
Post-Op Day #3/4 Date ____________
Interdisciplinary Care Team
Consults made to: Social Work Nutrition Pharmacy Pharmacy Financial Counselor Diabetic Educator (If diabetic) Other: __________________
Patient seen by: Social Work Nutrition Pharmacy Pharmacy Financial Counselor Diabetic Educator Referral to Home Health agency Other: __________________
Coordinate diabetic DC scripts If not ambulating, consider PT
eval Assess for outpatient dialysis
needs
Outpatient visits/appointments Local lodging, if needed
Teaching Needs
(Inpatient Coordinator and Nursing)
Pain management & communication
Foley catheter Central line/ hemodynamic
monitoring Care Partner responsibility /
participation Surgical dressing/wound
healing Incentive spirometer w/ return
demo Drain management
Receive discharge education binder
Care Partner responsibility / participation
Medication teaching with each dose administered including indication and side effects
Lab results/schedule
Medication teaching with each dose administered including indications & side effects
Care Partner responsibility / participation
Discharge education binder reviewed
Medication teaching with each dose administered including indications & side effects
Coordinator Discharge teaching Urinal / hat for home Specimen cup for drain/urine if
needed Pillbox Final discharge teaching AVS
w/ Staff RN
Care Considerations
(Nursing)
Complete Daily at End of Day Shift
Patient functional pain goal: ________________________
Hibiclens(CHG) Bath Pre-Op Standing weight Pain management Control nausea/vomiting 2:1 nursing care Assess fall risk; implement fall
precautions Braden scale/implement skin
protection interventions Oxygen per protocol Incentive spirometer x 10/hour
while awake Oximeter Hourly I&Os IV fluid replacements Drain management Foley cares BID 1000 & 2200
Patient functional pain goal: ________________________
Standing weight 0400-0600 Hibiclens(CHG) Bath Pain management Off 2:1 care, to normal staffing
in the 12-24 hrs post-op period Assess fall risk; implement fall
precautions Braden scale/implement skin
protection interventions Wean from oxygen if applicable Discontinue oximeter when
oxygen and PCA discontinued Incentive spirometer x 10/hour
while awake Foley cares BID 1000 & 2200 I&O every 4 hours IV fluid maintenance SCD to legs while in room Notify DEM of diet changes Encourage pt to achieve chair
and ambulation goals
Patient functional pain goal: _____________________
Standing weight 0400-0600 Hibiclens(CHG) Bath Pain management Assess fall risk; implement
precautions Braden scale/implement skin
protection interventions Assess bowel function;
encourage ambulation Notify primary team if continued
need for supplemental oxygen Incentive spirometer x 10/hour
while awake Foley cares BID 1000 & 2200 Discontinue SCD when
ambulating 4 x/day I&O every 4 hours Standing weight 0400-0600 Notify DEM of diet changes Encourage pt to achieve chair
and ambulation goals
Patient functional pain goal: _____________________
Standing weight 0400-0600 Hibiclens(CHG) Bath Consider at-home pain
management needs Assess fall risk; implement
precautions Braden scale/implement skin
protection interventions Change HD catheter dressing
prior to discharge (if appropriate) Assess bowel function, if no
BM, contact MD for further intervention
Remove Foley – patient to void every 2 hours while awake and every 4 hours while asleep
PVR after 1st 2 voids and call if greater than 150mLs
If patient unable to void 4 hrs after foley removal, notify team
Discontinue central line after Simulect dose
Notify DEM of diet changes
Pharmacist
Review post-op orders Collaborate w/ APP to resume home meds as appropriate
Collaborate with APP to initiate DC med reconciliation
Final DC med reconciliation. Discharge medication teaching New transplant duffle bag Pillbox provided
M.D. / A.P.P. / Fellow
Verify consent complete/correct Monitor I&Os Initiation of immunosuppression Verify Orders SCIP Protocol Post-Op assessment
Kidney ultrasound Resume home meds as
appropriate Blood pressure management
Initiate discharge medication reconciliation
Discuss DC planning w/ DEM
Order discharge medications Simulect POD #3 (if applicable)
Orders to dialysis (from NephMD) Neph communicate w/Ref Neph Neph order HD line dressing
change if needed
Blood Glucose Management
DEM consult if diabetic Diabetic Educator consult if
diabetic
IP Coord to fwd drug coverage info DEM educator (if applicable)
Diabetic education assessment Education plan initiated
Write diabetic discharge scripts Diabetic education Education plan continued
Make sure drugs affordable Diabetic follow-up Sign own discharge orders Discharge Note Diabetic education
reinforcement
Social Work Assessment and note Consult
Collaborate with inpatient coordinator on discharge planning needs & Home Health
Collaborate with inpatient coordinator on discharge planning needs & Home Health
Final discharge planning / note Complete note & send OTTR Complete discharge checklist
Nutrition NPO until awake then clear
liquids as tolerated Consult Advance diet as tolerated
Diet as tolerated Discharge note
Daily Goals/ Outcomes Achieved
Hibiclens (CHG) Bath Stable respiratory status Pain controlled at functional
goal Fluid/electrolytes status stable Free from injury Discharge planning initiated Care Partner participation
Stable respiratory status Pain controlled functional goal IV pain control discontinued Fluid/electrolytes stable Free from injury Diet as tolerated Discharge planning on track Care Partner participation
IV pain control discontinued Free from injury Free from S/S infection Discharge planning on track Care Partner participation
Discharge education completed Patient will state:
o Anti-rejection medications and
lab schedule, f/u appts
o Diabetic management plan
o Quiz answers
Foley removed POD #3 Free from injury Care Partner participation
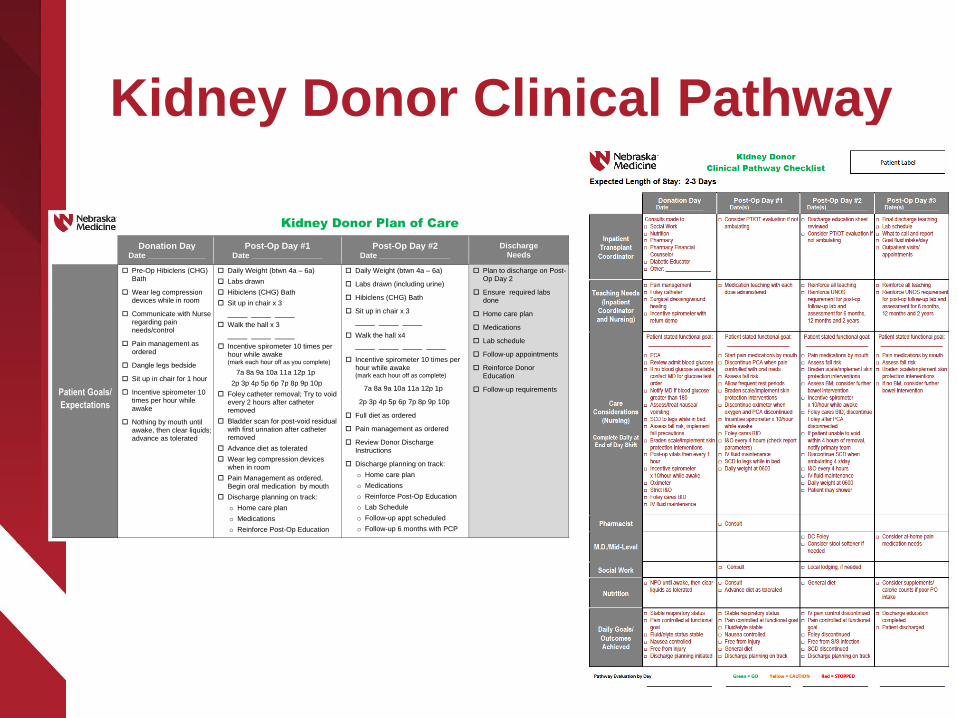
Kidney Donor Clinical Pathway
Kidney Donor Plan of Care
Donation Day Date _____________
Post-Op Day #1 Date ________________
Post-Op Day #2 Date ________________
Discharge Needs
Patient Goals/
Expectations
Pre-Op Hibiclens (CHG) Bath
Wear leg compression devices while in room
Communicate with Nurse regarding pain needs/control
Pain management as ordered
Dangle legs bedside
Sit up in chair for 1 hour
Incentive spirometer 10 times per hour while awake
Nothing by mouth until awake, then clear liquids; advance as tolerated
Daily Weight (btwn 4a – 6a)
Labs drawn
Hibiclens (CHG) Bath
Sit up in chair x 3
_____ _____ _____
Walk the hall x 3
_____ _____ _____
Incentive spirometer 10 times per hour while awake (mark each hour off as you complete)
7a 8a 9a 10a 11a 12p 1p
2p 3p 4p 5p 6p 7p 8p 9p 10p
Foley catheter removal; Try to void every 2 hours after catheter removed
Bladder scan for post-void residual with first urination after catheter removed
Advance diet as tolerated
Wear leg compression devices when in room
Pain Management as ordered, Begin oral medication by mouth
Discharge planning on track:
o Home care plan
o Medications
o Reinforce Post-Op Education
Daily Weight (btwn 4a – 6a)
Labs drawn (including urine)
Hibiclens (CHG) Bath
Sit up in chair x 3
_____ _____ _____
Walk the hall x4
_____ _____ _____ _____
Incentive spirometer 10 times per hour while awake (mark each hour off as complete)
7a 8a 9a 10a 11a 12p 1p
2p 3p 4p 5p 6p 7p 8p 9p 10p
Full diet as ordered
Pain management as ordered
Review Donor Discharge Instructions
Discharge planning on track:
o Home care plan
o Medications
o Reinforce Post-Op Education
o Lab Schedule
o Follow-up appt scheduled
o Follow-up 6 months with PCP
Plan to discharge on Post-Op Day 2
Ensure required labs done
Home care plan
Medications
Lab schedule
Follow-up appointments
Reinforce Donor Education
Follow-up requirements

Liver Transplant Recipient Clinical Pathway Liver Transplant Clinical Pathway Checklist
STAFF CHECKLIST
Expected Length of Stay: 7-8 Days
Transplant Day
Date ___________ Post-Op Day #1
Date ____________ Post-Op Day #2
Date ____________ Post-Op Day #3
Date ____________
Interdisciplinary Care Team
Consults made to: Critical Care Surgery Hepatology Social Work Nutrition Pharmacy Pharmacy Financial Counselor Diabetic Educator (if diabetic) PT/OT Other:
Patient seen by: Social Work Nutrition Pharmacy Pharmacy Financial Counselor Diabetic Educator (if diabetic) PT/OT Other:
Teaching Needs (Inpatient
Coordinator and Nursing)
Pain management and communication
Restraints Hemodynamic monitoring/central
line Frequent lab work (every 6 x 24
hours) Care Partner responsibility/
participation Medication teaching with each
dose administered including indication and side effects
Surgical dressing/ wound healing Incentive spirometer w/ return
demo (T, C, DB) Drain management Foley Activity
Receive discharge education binder
SOTU expectations (quiet time, involved in plan of care, infection control)
Pain management and communication
Care Partner responsibility/ participation
Medication teaching with each dose administered including indication and side effects
Infection control Fluid changes (daily standing
weight) Foley – remove Activity
Medication teaching with each dose administered including indications and side effects
Pain management and communication
Care Partner responsibility/ participation
Discharge education binder initiated
Incisional care – staples Infection control Activity Blood glucose management
Medication teaching with each dose administered including indications and side effects
Pain management and communication
Care Partner responsibility/ participation
Rejection Infection control Nutrition Activity Blood glucose management
Care Considerations
(Nursing)
Complete Daily at End-of-Day Shift
Patient functional pain goal: Hibiclens(CHG) treatment pre-op Weight Pain management Control nausea/vomiting Hemodynamic monitoring Remove arterial lines Change over central line Assess fall risk; implement fall
precautions Braden scale/implement skin
protection interventions Oxygen per protocol Incentive spirometer x 10/hour
while awake Turn, cough, deep breathe every
2 hours Continuous pulse-ox Hourly I&Os IV fluid replacements – patient is
NPO Drain management Foley cares per P/P HOB 30 degrees Encourage activity Prepare for SOTU transfer –
discuss staffing ratios
Patient functional pain goal: Hibiclens (CHG) treatment Standing weight 0400-0600 Pain management Central line cares Assess fall risk; implement fall
precautions Braden scale/implement skin
protection interventions Wean from oxygen if applicable Discontinue continuous pulse-ox
when oxygen and PCA discontinued
Incentive spirometer x 10/hour while awake
Remove Foley I&O every 8 hours IV fluid maintenance Drain management SCD to legs while in room Encourage patient to achieve
chair and ambulation goals
Patient functional pain goal: Hibiclens (CHG) treatment Standing weight 0400-0600;
assess fluid status Pain management Central line cares Assess fall risk; implement
precautions Braden scale/implement skin
protection interventions Assess bowel function;
encourage ambulation Notify primary team if continued
need for supplemental oxygen Incentive spirometer x 10/hour
while awake SCD to legs while in room Encourage patient to achieve
chair and ambulation goals
Patient functional pain goal: Hibiclens (CHG) treatment Standing weight 0400-0600 Pain management Central line cares Assess fall risk; implement
precautions Braden scale/implement skin
protection interventions Assess bowel function; if no BM,
contact MD for further intervention
Incentive spirometer x 10/hour while awake
SCD to legs while in room Encourage patient to achieve
chair and ambulation goals
Pharmacist
Review post-op orders Collaborate w/APP to resume
home meds as appropriate
Collaborate w/APP to resume home meds as appropriate
Review transfer orders
MD/APP/Fellow
Verify Transplant, Blood, and Surgical consents are complete/correct
Pre-op assessment Monitor I&Os Initiation of immunosuppression Verify orders Core measure protocols Post-op assessment Liver ultrasound, EKG, CXR
Resume home meds as appropriate
Blood Glucose Management
Glucose checks Glucose management Diabetic Educator consult if
diabetic
Diabetic education assessment Education plan initiated
Diabetic education Diabetic education reinforcement
Social Work
Assessment and note Consult
Collaborate with inpatient coordinator on discharge planning needs and Home Health
Collaborate with inpatient coordinator on discharge planning needs and Home Health
Advanced Transplant Nursing Care Team
• At least 1 year of nursing experience on
specialty transplant floor
• Specialized Cardiology and Transplant
Fellowship classes
• Encourage Transplant Certification within
division:
CEPTC offerings throughout the year to prepare
for and maintain certification (CCTC, CPTC,
CCTN)
Inpatient Nursing Fellowship Classes
CPCU (Cardiology Fellowship)
• Immunosuppression• Surgical procedure and
considerations: Heart• Immediate post-operative care• Nursing care and patient
education• Surgical procedure and
considerations: Lung• Post-operative care and patient
education• LVAD, acute coronary syndrome,
heart failure and electrophysiology
SOTU (Transplant Fellowship)
• Transplant overview• Introduction to kidney and
pancreas transplantation• Transplant pharmacology and
infectious complications• Liver transplantation• Intestinal transplantation• Advanced kidney and pancreas
transplantation• Continuous bladder irrigation,
central venous pressure and arterial lines
Inpatient Hospitalizations
• Pre-Transplant patients can be admitted to
specialized transplant floors prior to evaluation,
during the evaluation process, and while waiting on
the list for transplant for any medical-surgical reason
• Post-Transplant patients can be (and likely are)
admitted to specialized transplant floors for any
reason, but especially anything related to the
transplant surgery or transplanted organ
Transplant Nurse Burnout
According to Progress in Transplantation, “To date,
only a handful of studies have specifically addressed
the experience of organ transplant nurses. Qualitative
data show that transplant nurses are driven by
altruistic motivations and are highly engaged in their
work, even to their own detriment, as they also often
report high levels of stress in their roles.”
Jesse M, Abouljoud Marwan, Hogan K, Eshelman A. Burnout in Transplant Nurses. Progress in Transplantation. 2015; 25(3):196-202
SOTU Bedside RN Struggles
• Bedside nursing is HARD WORK
Managing end-stage organ disease prior to transplant and
continuing with a “Chronic Medical Condition” after transplant
• Transplant patients don’t always have a smooth journey
Medications to manage this “Chronic Condition” makes the
patients susceptible to other disease processes – rejection,
infection, cancer, etc.
• SOTU RNs often form close relationships with the patients that
have frequent inpatient hospitalizations
• Bedside nurses experience the joy and frustration of the transplant
journey with their patients and the families
• SOTU is a hard floor – sick patients, emotional variability with
patients and care givers, huge learning curve and high
expectations
RNs take their knowledge and skills learned to other areas
(ICUs, ED, Float Pool) when they are ready to move on
Nebraska Medicine
Center of Excellence
Amber Saltsgaver, BSN, RN
Staff Lead RN, Quality Champion for
SOTU
Quality Champion
• An RN on each specific unit is designated to lead
quality change to increase patient safety
• Leads monthly performance unit meeting to discuss
areas of performance improvement in regards to
Nursing Quality Indicators and unit initiatives
• Member of the Quality and Innovation Council
within Nebraska Medicine that meets monthly to
discuss quality and safety initiatives and outcomes
throughout the organization
Nursing Quality Indicators
• CAUTI (Catheter Associated Urinary Tract Infection)
• CLABSI (Central Line-Associated Blood Stream
Infection)
• HAPU (Hospital-Acquired Pressure Ulcers)
• Falls – both Injury and Non-injury falls
• VAP (Ventilator-Associated Pneumonia) in the ICU
Settings
Quality Initiatives
• House-wide education and competencies for CAUTI reduction
• House-wide education and competencies for CLABSI reduction:
CVICU Unit Based Council initiative was shared house-wide for
Second Nurse observation for all central line dressing changes
Collaboration with the PICC team on central line dressing
changes on SOTU (pilot starting to expand to other units)
• Collaboration with the PICC team on central line cares on
SOTU
• Purposeful hourly rounding to aid with fall reduction
• Collaboration with wound nurse to reduce pressure
injuries within unit
Patient Satisfaction and Experience
Information is shared with the staff on the inpatient units
and at the Transplant Quality Assessment Performance
Improvement meeting for continuous improvement
ideas/opportunities:
• HCAHPS -
Nurses listen carefully to you
Nurses explain in a way you understand
Nurses treat you with courtesy and respect
Nurse Call Light responsiveness
Hospital rating (0-10)
• Press Ganey
• Patient rounding and discharge follow-up phone calls
High Expectations at all Times
• With the immunocompromised status of our patients, we have to be perfect all of the time
• Sometimes you can do everything correctly and have every intervention in place and still have problems
Patients may be weaker than they anticipate
Central line placement – IJs dressings stick to hair or beards instead of occlusive on the skin
Patients need extra encouragement to eat, bathe, be active
• Surveys are subjective based upon patient’s perception:
One negative experience in one moment of time – not happy with food, test took to long, pain level not at zero, etc., is what the patient remembers and responds to survey with that in mind

Post Transplant
Amy Schurke, BSN, RN, CCTC
Transplant Coordinator
Compliance
• Medications:
Antirejection meds need to be taken 12 hours apart -
o Timing of meds is very important
• Labs:
Timing importance -
o Needs to be 30-45 minutes before IS meds taken
o Should be at same time with each draw; patients should be consistent with what they do before each draw
o Should be fasting
Follow-up
• All team members of the multidisciplinary
team are involved in the patient’s care
• Clinic visits are in their organ specific clinic:
Pretty frequent visits right after transplant
Further out the less they are seen
• In general patients are followed by the
transplant team indefinitely (or the lifetime of
their transplant)
Lifetime Follow-up
• Once a patient is a transplant patient, they will
always be the transplant team’s patient
• The transplant team is available to follow any
medical needs:
Rejection
Graft loss
Hernia repair
Any other concerns
After Hours
• There is a nurse coordinator on call 24/7 for
emergencies:
Call the main office number to reach on call
coordinator after hours
• Transplant Physician and Transplant Surgeon are
also on call for MD-to-MD phone calls
Outcomes
• All outcomes for each transplant center for all
organs is public:
Website: www.srtr.org
Updated outcomes twice a year, usually
December and June

Post-transplant Coordinator Burnout
• Follow same patients through the entirety:
Patients are not always fully honest
Work short staffed due to vacations or illness
Patient load 180-200 patients each
Cumbersome/difficult patients
• On call demands
• Ever changing processes within the transplant realm:
CMS requirements
UNOS requirements
Other Governing bodies
o HIPPA requirements
Post-transplant Coordinator Burnout
• Completing non-nurse tasks:
Takes away from patient care
• Coordinators work Monday-Friday:
May not be as flexible as staff nurses’ 12-hour/
3 days a week schedule
• Patient follow-up:
Non-compliant patients
Compliant patients with bad outcomes
Graft failure, rejection, or infection
• Care partner burnout
Coping with Burnout
• Employee Assistance Programs
• Friends with coworkers
Food days at work
o Past patients send goodies over the holidays
Gatherings outside of work
o Celebrating wine/beer/margarita days responsibly
• Time away from work
Vacations, days off
• Remembering patients
Donor ceremony
Celebrating successes either in media or when patient’s visit
Coping with Burnout
• Self-Care
Exercise, massage, pedicure
• Getting away from desk
Lunch
Walking breaks
• We are a TEAM and it takes a TEAM to get through it
all
Heart Lung Transplant
• https://www.youtube.com/watch?v=WbemBjviJ7I


















