The Community Health Protection Programme in … COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR...
12
The Community Health Protection Programme in Dungarpur, Rajasthan
Transcript of The Community Health Protection Programme in … COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR...

The Community Health Protection Programme in Dungarpur, Rajasthan

Save the Children
WE ARE the world’s leading independent organisation for children.
OUR VISION is a world in which every child attains the right to survival, protection, development and
participation.
OUR MISSION is to inspire breakthroughs in the way the world treats children, and to achieve immediate and
lasting change in their lives.
Supported by Official Development Aid, Ministry of Foreign Affairs, Government of Finland
Copyright: Save the Children Finland, 2014
Cover photo credit: People’s Education and Development Organisation (PEDO), Dungarpur
Text: Save the Children, N.R. Management Consultants India Pvt. Ltd
Layout: N.R. Management Consultants India Pvt. Ltd
The names of people have been changed to protect their identity.

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR 3
Family Health Shocks and Vulnerability of ChildrenDungarpur, located in the southernmost tip of Rajasthan, is one of the least developed districts in the state and India at large. A dismal health infrastructure coupled with limited health awareness has resulted in an abysmal health status for the local population. The Infant Mortality Rate of 63 deaths1 and under Five Mortality Rate of 81 deaths2 per 1,000 live births, are both worse than the state average. Communicable and chronic diseases such as tuberculosis, malaria and hIV/AIDS are widespread. Qualified doctors are only consulted as a last resort - if at all.
The profound belief in faith healers, a flourishing local market of quacks and private health clinics3, and the prolonged time involved in seeking appropriate treatment, has led to spiraling medical expenses for poor households. A Save the Children initiated study found that as much as 30 per cent of loans taken by poor households are used for health purposes4.
As parents become ill and are unable to work, medical costs escalate and households adopt various coping strategies that impact children negatively, as well as affect their long-term development opportunities.
1 Annual health Survey Rajasthan Factsheet 2012-13. State IMR is 55.2 Ibid. State u5MR is 74.3 There are limited private medical clinics in Dungarpur. People travel a few hours to the neighboring state of Gujarat or to the district of udaipur in
Rajasthan4 Kaarak, 2010, ultra poor Scoping & Vulnerability study: insights from Dungarpur

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR4
Illness of father leads to children dropping out of school
MEENA, GITA and their younger
brother KANu have dropped out of
school. The two girls have joined their
mother as construction workers in
Gujarat, while Kanu stays at home to
look after his father and a younger
sister, and also manages household
chores. Their father is suffering from
TB and is no longer able to work.
The most common coping strategy is to take children out of school to be at home and help with domestic chores or to send them for labour5.
As a response to the trend observed, Save the Children decided to introduce a community based health protection programme, with the objective of exploring the possibility of social insurance providing an opportunity for mitigating the adverse impact of health stress and shock on children. In the process of outlining the initiative, it became clear that the intervention would only be successful if developed as an integrated package of services, including prevention and consultation, thus focusing on health more widely. As a result of this thought process, the Community health Protection Programme (ChPP) was initiated in 2011.
5 Save the Children, 2012, Child Poverty in Dungarpur

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR 5
Objectives and Key Components of CHPPThe aim of ChPP is to protect low-income households against specific health risks through a package of community based health interventions. The CHPP uses the community based insurance model, which emphasizes the active participation of community members in the insurance process to build community ownership, solidarity and self-management to ensure sustenance of the initiative.
A key actor in the project is the local NGO PEDO (People’s Education and Development Organisation), which has developed an extensive network of Self-help Groups (ShGs) in the district6. Since the ShGs are organized into micro credit federations, they are better experienced at handling finances. With this backdrop, federations provide a well-functioning platform to build ChPP around. uplift, a Pune based organisation experienced in health protection, is providing technical guidance on the modalities of CHPP.
Two feasibility studies were carried out, followed by a scoping study in July 2011 to assess the health care conditions in Dungarpur. The latter also evaluated the problems faced by PEDO ShG members in accessing health care, their health related expenses and capacity and interest to pay a premium. The findings indicated that ChPP would be a viable option for improving health risk management within the project area. Three PEDO federations, i.e Mada, Jhonthri and Genji, covering 550 ShGs across 110 villages, were then selected for the intervention.
6 PEDO has been active in the field of microfinance in all five blocks in Dungarpur for almost 30 years.

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR6
CHPP POLICY
The costs and provisions of the CHPP policy is summarised below:
PremiumRs 120/ person for family if more than 3 people are enrolledRs 360 for single individualRs 480 for couple
Hospitalization reimbursementsGovernment hospitals: 100% of total expenditureNetwork/ Trust hospitals: 70% of total expenditureNon-network/ private hospitals: 50% of total expenditure
ClaimMaximum Rs 12,000 per year per policyDay discharge: Maximum of Rs 2,500General: Maximum of Rs 7,500
Right information for right treatment
� 24X7 help line, handled by General Nurse and Midwife (GNM) � Referrals of beneficiaries to hospital for further treatment and follow up� Follow up with network hospitals to ensure appropriate treatment and discount to CHPP members
Reducing out of pocket expenses
� Community based health insurance policy managed by SHG federations� A panel of network hospitals so that treament can be availed on discounted rates.� Encourage usage of government health serivces, which are of minimal charge or free of cost
Preventive health care services
� Guidance centers with paramedical staff to provide health check ups and referrals� Health check up camps for general or sepcific health ailments, mostly in collaboration with
government health service providers and network hospitals � Health talks on awarness and prevention during SHG meetings
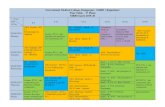
The figure below illustrates the objectives and key components of the ChPP.

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR 7
Level Enrolment Process Preventive Health Care Claim Management
Self help Group
(ShG) level
- a ShG comprises
15-20 women
nClient education of Self Helf
Group members for enrolment
and re- enrollment process by
Field Representatives
nNidhi (membership) Card
Distribution
nhealth Talks by General Nurse
and Midwife (GNM)
nReferrals to hospitals for
primary, secondary and tertiary
care
nOrientation on claim
processes
nClaim processed by
Field Representatives
Cluster level-
20 ShGs form a
cluster
nOrientation of Cluster members
on the product
nGuidance Centre to provide
initial health check up and
referral services
nOrientation on claim
processes
Federation level- 8
clusters make up a
federation
nOrientation of federation
members on the CHPP policy
nCapacity building of federation
leaders on client education,
policy, claim management
nSpecial health camps for general
or specific health ailments
nManagement of 24X7 helpline
through GNMs
nGNMs give 2 hrs at federation
level and then move around
villages for better outreach
nClaim committee
monthly meetings
to decide on claims
received.
nDisbursement of
claim amount to the
member during ShG
meetings
People’s Education
and Development
Organisation
(PEDO)/uPLIFT
nMIS and Back office management
nNidhi Card printing
nIEC Development
nMonitoring and Evaluation
nGuidance to federations
nCapacity building of CHPP team
and federation leaders
nProcess auditing
nLinkages and follow up with
empanelled hospitals
nClaim verification by
Doctors
nProcess auditing by
uPLIFT
The table below gives an overview of how ChPP is organised within the ShG structure:

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR8
Progress of CHPPn Total enrollment: 7,311
household members (October 2012 - October 2014)
68% of household members enrolled against target
66% of target renewed policy
n Access to health care services Steady increase in use of health services
by members n 7,484 members benefited from the
Guidance Centresn Rs 6,81,486 was saved on OPD caren 1523 members benefited from health
camps n 350 members accessed referral
services by General Nurses and Midwives through 24X7 helpline
Note: All figures are applicable to
2014 assessment by PEDO
n Total premium collected: Rs 30,76,000 (October 2012 - October 2014)
Two out of three federations have sufficient money for hospitalization reimbursements of its members
n Total claims received by households: Rs 645,184 till October 2014
Preventing school dropout and child labour
RAJu is a wage labourer and the sole earner in his family. His three sons study in the local school and his wife KAMLESh is an ShG member. The couple is enrolled in the CHPP.
When Raju met with a road accident and landed up with a fractured leg, he was referred to the empaneled hospital Bhagwan Mahavir in Dungarpur where he was hospitalized for four days. he later claimed Rs 12,000 for his complete treatment through CHPP.
Kamlesh is happy that the insurance amount received was timely and very helpful at such a critical time. “If there was no help, we would have had to send the boys to work,” she says.

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR 9
Frequently Asked Questions on CHPP
Is CHPP relevant when there is a government run health insurance scheme?
In Rajasthan, the state government re-launched the Rashtriya Swasthya Bima yojna (RSBy) in 2013, which aims to provide protection to BPL (Below Poverty Line) households as well a few other specific categories of informal workers 7 incurring financial liabilities from health related shocks through cashless insurance. Beneficiaries under RSBy are entitled to hospitalization coverage of up to Rs 30,000 in a year; however, this is restricted to empaneled hospitals and limited to five members per family. The scheme is not fully functional in the state yet, and is also not performing well in many places. Fake claims, corruption, non-functioning of swipe machines installed in hospitals and lack of awareness among the community are the key problems observed.
Even if the performance of RSBy improves, ChPP continues to be relevant for the following reasons: 1) ChPP reaches remote villages and hamlets and members value the comprehensive package that is being offered in areas where health services are scarce. 2) There is follow up with hospitals to ensure that ChPP members are being taken care of properly. 3) ChPP is community owned and over time they can alter the modalities to respond to changing needs of the members if they wish to. 4) ChPP can also be used in conjunction with RSBy so that members can avail of higher insurance coverage if needed. 5) under ChPP, any number of family members can avail services in all hospitals and clinics.
RSBy is just an insurance and does not address the wider problems of health care that people face in remote areas of Dungarpur - ChPP is being valued for its holistic provisions. hence, ChPP appears to be sustainable even with better uptake of RSBy.
7 Street vendors, domestic workers, beedi workers, building and construction workers, people who have worked for more than 15 days in MGNREGS- Rural Employment Guarantee Scheme.

ThE COMMuNITy hEALTh PROTECTION PROGRAMME IN DuNGARPuR10
How does CHPP compete with private health insurance providers?
Cases related to poor health continue to rise in Dungarpur, aggravating the vulnerability of poor households. The objective of ChPP is to provide a fall back mechanism to such families in case of health incidences, and not to make profits. The design of ChPP is different from the conventional health insurance schemes run by private companies. It is a complete package offering preventive health care services for all ages, including health awareness, primary health checkups, treatment and referrals. In addition, it is owned and managed by the community and is a good example of risk pooling and collective decision-making.
Is CHPP for the poorest?
Presently ChPP caters to enrolled ShG members, 67% of which are from the BPL (Below Poverty Line) category. Although the government classification of BPL can be questioned in terms of actual inclusion of the poor, Save the Children has made an assessment of the poverty status of the ShG members and concluded that the groups represent a socio-economic mixture of women. When starting ChPP, it was important to build it around cohesive and existing units, and not to extend it to non-ShG members. however, as the initiative is now firm on the ground, it is being explored as a window for reaching out to additional people, especially among the poorer segments of the population. It is to be noted that in the tribal hinterland of Dungarpur, socio-economic differences are not enormous and majority of the people have limited assets and struggle to make their livelihoods from small-scale farming and unskilled labour.
Does CHPP have an impact on children?
ChPP provides support to the entire family at times of stress and shock induced by poor health. Also, ChPP undertakes focused child sensitive interventions with ShG members and federation leaders to enable them take positive decisions for the benefit of children in times of household stress. however, it is too early to measure the precise impact of ChPP on children.
How can CHPP be sustained?
It was a strategic decision to initiate ChPP with ShG federations as it facilitated the programme to use the huge network and leverage their financial and managerial skills. The ChPP has in place capacity building activities for the federation leaders to better realize various technical aspects of health insurance including finances, claim settlement and collective decision-making. With increase in enrollment, the federations will become financially sustainable, while technical know-how will enable them to independently manage the programme. Therefore, CHPP being community owned and managed is innately sustainable as long as its members value it and there is a functional management system in place.

Phot
o:

CONTACT INFORMATION:
Save the Children, Bal Raksha BharatRajasthan State Programme Office42 Vrindavan Vihar, King’s RoadJaipur 302021Rajasthan, IndiaPhone: +91-141-4035881, 3220881
www.savethechildren.in
Phot
o: H
aris
h C
hand
eriy
a