The Clinical Eating Disorders Rating Instrument (CEDRI): A Validation Study
8
Click here to load reader
-
Upload
robert-palmer -
Category
Documents
-
view
218 -
download
1
Transcript of The Clinical Eating Disorders Rating Instrument (CEDRI): A Validation Study

The Clinical Eating Disorders Rating Instrument (CEDRI): A Validation Study
Robert Palmer, David Robertson, Mark Cain and Susanna Black
The study was designed to test the validity of the CEDRI, a semi-structured interview fur the assessment of much of the psychopathology and behuviours associated with the clinical eating disorders. Evidence of its reliability has previously been published. The present study examines the ratings obtained from clinical sampks of subjects with anorexia nervosa (n=39) and bulimia nervosa (n=97) and compares them with a comparison group of women (n=98) who were dieting but not eating disordered. Statistically significant differences were found between the clinical sampks and the comparison group on almost d items. The overall pattern of results provides e d n c e for the validity of the instrument.
INTRODUCTION
Research into the clinical eating disorders, anorexia nervosa and bulimia nervosa, requires the development of instruments to measure their specific psychopathology and the abnormal eating behaviours. Efforts to develop such instruments have tended to yield self-report measures, such as the Eating Attitudes Test (EAT) (Gamer and Garfinkel, 1979), the Eating Disorder Inventory. (EDI) (Gamer et al., 1983) and the Bulimic Investigatory Test- Edinburgh (BITE) (Henderson and Freeman, 1987). However, some features of eating disorders are difficult to elicit reliably using a self-report measure. For instance, the word ‘binge’ may be subject to a wide variety of interpretations. Measures based upon interviews with some standardization of format and definitions are likely to be preferable in much clinical research. A number of such interview based measures have been devised for particular projects or for more general use, for instance the Eating Disorders Examination (Cooper and Fairburn, 1987) and the Structured Interview for Anorexia and Bulimia (SIAB) (Fichter et al., 1989). Similarly, the Clinical Eating Disorders Rating Instrument (CEDRI) is a semi-structured interview which has been developed as a simple and robust measure for use in both clinical work and research (Palmer et al., 1987).
CCC 1072-4 133/96/030 149-08 European Eating Disorders Review 0 1996 by John Wiley & Sons, Ltd. and Eating Disorders Association 4(3), 149-156 (1996)

R. Palmer, D. Robertson, M. Cain and S. Black
Table 1. CEDRI items
CEDRI items: attitudinal Cedri items: behavioural
Reduced appetite Exaggerated food interest Acceptability of normal weight Loss of control fantasy: weight Loss of control fantasy: eating Guilt/self-disgust with weight and/or eating Subjective distortion of body image Preoccupation with body parts and shape
Restrained eating Avoidance of 'fattening' foods Food monitoring Vomiting for weight control Laxative abuse for weight control Use of other drugs for weight control Chewing and spitting out food Exercise for weight control Weighing Self-defined bingeing Defined bingeing Avoidance of social eating Avoidance of certain clothes or activities
The CEDRI is essentially a way of recording in a standard manner clinical judgements about key features of both anorexia nervosa and bulimia nervosa. It can be used by clinicians from various professions with little special training provided they have some experience of people with eating disorders. A manual is available from the author. Previous work has demonstrated it to have an acceptable degree of reliability (Palmer et al., 1987). The aim of this study was to assess the validity of the CEDRI by examining its ability to discriminate between patients with a clinical eating disorder and subjects from a community study who did not meet the diagnostic criteria for an eating disorder but who were nevertheless to a varying degree weight concerned in that they were dieting at the time of assessment. This was considered a more stringent and more appropriate test of validity than comparisons with samples selected at random or indeed for a lack of evident weight concern.
DESCRIPTION OF THE CEDRI
The CEDRI was designed to be a standardized record of the observations of a clinician interviewing an individual thought to have an eating disorder. Subjects are rated on their eating attitudes and behaviour over the preceding month. The current version consists of 21 items, eight concerned with attitudes to eating, weight and shape, and a further 13 which concern eating and related behaviours (Table 1). The original full version also contained items concerned with general psychopathology but these have been omitted from the instrument used in this study as we were interested in its ability to
150

A Validation Study of the CEDRI
Table 2. The study populations
Age BMI
Mean SD Mean SD ~~ ~~~
Clinical Anorexia nervosa (n=39) 24.9 6.4 16.0 2.0 Bulimia nervosa (n=97) 25.7 7.3 23.2 4.6
Dieters (n=98) 35.0 8.4 27.8 5.7 Control
discriminate in terms of eating pathology. Each item has a four-point rating scale. A rating of zero represents either an absence of symptoms or a response judged to be normal for the general population. A rating of one or two represents responses considered to be characteristic of a population of eating disordered patients in either a mild form (one) or a marked form (two). A rating of three represents a response considered to be severe even for a population of eating disordered patients.
Each item consists of a primary question, followed by a list of further probe questions. If necessary the interviewer can ask additional clarifying questions to establish the presence and extent of an item. In case of doubt, the rater is instructed to choose the lower rating.
METHOD The clinical sample comprised 136 consecutive patients presenting to an Eating Disorders Service who fulfilled the DSM-111-R diagnostic criteria (American Psychiatric Association, 1987) for either anorexia nervosa or bulimia nervosa. Where a subject fulfilled criteria for both disorders, that individual was included in the anorexia nervosa series. Of the total sample, 126 were female and 10 were male. The CEDRI ratings were made in the course of routine clinical assessment by one of three raters; a consultant psychiatrist (RLP), a clinical psychologist or a clinical nurse specialist. The numbers and diagnoses of the subjects, and descriptive statistics of their age and body mass index (BMI) are summarized in Table 2.
The comparison group consisted of 98 women who had been interviewed using the CEDRI in a community study. That study involved a two-stage survey in which an initial postal questionnaire screen of 1920 women was followed by the interview of 264. The interview included the CEDRI. The interviewers in this case were two psychiatric registrars, a senior therapist and the clinical nurse specialist who was mentioned above. The subjects who form the comparison group for the present study were those women who, at interview, were found to be actively following a slimming diet (‘dieters’), but without evidence of eating disorder.
151

R. Palmer, D. Robertson, M. Cain and S. Black
Table 3. Comparison of CEDRI scores between the clinical groups and the control group using Mann-Whitney (U) test (Assumption of nonparametric data)
~~~
Mean Anorexia Mean Bulimia Mean CEDRI nervosa CEDRI nervosa CEDRI
scores for (nl=39) versus scores for (nl=97) versus score for anorexics ‘dieters’ ‘dieters’ ‘dieters’ bulimics (n=39) (n2=98) (n=98) (n2=98) (n=97)
CEDRI 1 (Reduced appetite) CEDRI 2 (Restrained eating) CEDRI 3 (Avoid fatty foods) CEDRI 4 (Food monitoring) CEDRI 5 (Exaggerated food interest) CEDRI 6 (Vomiting) CEDRI 7 (Laxatives) CEDRI 8 (Other drugs) CEDRI 9 (Chewing+spitting) CEDRI 10 (weighing) CEDRI 11 (Attitude to normal weight) CEDRI 12 (Loss of control fantasy-weight) CEDRI 13 (Loss of control fantasy-eating) CEDRI 14 (Subjective overeating) CEDRI 15 (DSM-IIIR bingeing) CEDRI 16 (Guildself disgust at eating)
0.18
2.36
2.05
1.33
1 .oo
0.92
0.21
0.00
0.58
1.77
1.62
1.98
1.44
0.97
0.39
1.79
p=0.2505 (nl=38)
p < 0.0001 t
p<0.0001t (nl=37)
p=0.0070t
p=0.0992
p<0.0001~
p=0.0025t
p> 0.9999
p < 0.0001 t
p < 0.0001t
p<0.0001t
p<o.ooolt
p<o.oool~
p=O.O01 It
p < 0.0001 t
p<0.0001t
(nl=38)
(nl=38)
0.08
1.39
1.22
0.91
0.77
0.01
0.03
0.00
0.00
0.88
0.14
0.97
0.26
0.36
0.01
0.89
p=0.0261*
p<0.0001t
p=o.o001 t (nl=95)
(nl=96) p=0.7680
p=0.0713 (n1=96)
p < 0.0001t
p<0.0001~
p=0.0001+
p < 0.0001~
(nl=96)
(nl=96)
(nl=96) p < 0.0323*
(nl=95)
(nl=95) p<0.0001~
p<0.0001t
p < 0.000 1 t
p<0.0001t
p<0.0001~
p<0.0001~
(nl=96)
(nl=96)
(nl=95)
(nl=96)
(nl=96)
0.23
1.91
1.67
0.86
1 .oo
2.00
0.66
0.25
0.36
I .32
0.96
1.82
1.86
2.16
2.10
1.81
(Continued)
152

A Validation Study of the CEDRI
Table 3. (Continued )
Mean Anorexia Mean Bulimia Mean CEDRI nervosa CEDRI nervosa CEDRI
scores for (nl=39) versus scores for (nl=97) versus score for anorexics ‘dieters’ ‘dieters’ ‘dieters’ bulimics (n=39) (n2=98) (n=98) (n2=98) (n=97)
~~
CEDRI 17 1.36 p<0.0001t 0.06 p < 0.0001t 1.10 (Avoidance of social eating) CEDRI 18 0.87 p=0.3851 0.72 p=0.0010t 1.15 (Avoidance of certain clothes/activities) CEDRI 19 1.33 p <0.0001~ 0.37 p<0.0001t 1.34 (Subjective disortion body image) CEDRI 20 1.23 p=0.0001~ 0.55 p < 0.0001t 1.54 (MY p a d CEDRI 21 0.79 p=O.O 1 16* 0.53 p=0.0099? 0.90 (Exercise) (nl=30) (nl=82)
*.Significant difference. ‘Highly significant difference.
RESULTS
The mean age of the control group was significantly greater than those of the clinical samples. However, correlation of CEDRI item score with age in the control group showed no significant association for all but one of the items. For that item (avoidance of fattening foods) we examined an age-matched group of 34 dieters and found the difference in mean score from anorexics and bulimics to be even greater than for the total control group.
The comparison of CEDRI scores between the groups was analysed using the Mann-Whitney (U) test and is summarized in Table 3. In general, the CEDRI appeared to discriminate well between patients with eating disorders and controls who were actively dieting.
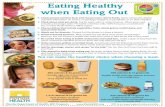
A comparison between the scores of subjects with anorexia nervosa and women who were dieting found significant differences at the p < 0.05 level on 17 of the 21 items, including 13 items with very highly significant differences at the p < 0.0001 level. The mean CEDRI item scores for anorexics and dieters are represented in Figure 1. Whilst the patterns of scoring are broadly similar, the mean scores for the anorexics are almost always higher than for the dieters. The four items which failed to discriminate were ‘reduced appetite’, ‘exaggerated food interest’, ‘use of slimming drugs’ and ‘avoidance of clothes and activities’.
A comparison of those with bulimia nervosa with dieters found significant
153

R. Palmer, D. Robertson, M. Cain and S. Black
2 5
2
1.5 mean cedri score
1
0.5
0 0 5 10 15 20 25
cedri items
Figure I . Comparison of CEDRI scmes of anorexia newosa sample with control sample of ‘dieters’
differences at the p < 0.05 level on 19 of the items, including 16 items with very highly significant differences at the p,<O.OOOl level. The mean CEDRI item scores for bulimics and dieters are represented in Figure 2. The two items which failed to discriminate were ‘food monitoring’ and ‘exaggerated food interest’.
DISCUSSION
It has been suggested that in examining the validity of a rating instrument, it is important to make a comparison between patients with eating disorders and people without such a disorder who nevertheless are concerned about eating, shape, and weight (Cooper et al., 1989). The sample of dieters used in this study would seem to be such a comparison group. The CEDRI was indeed able to discriminate between that group and groups of subjects suffering from each of the major clinical eating disorders. The broad pattern of scores was as expected. In particular, the core symptom items such as those concerned with bingeing, vomiting and loss of control fantasies discriminated to a degree which were highly statistically significant.
The items that did not discriminate are of interest. Reduced appetite does not discriminate between anorexics and dieters (both groups showing low mean scores). Reduced appetite is not typical of anorexia nervosa. Nevertheless, the item may well be of value as part of the evaluation of subjects with pathological weight loss, even if the presence of true loss of appetite may lead to a questioning of the diagnosis of a typical eating disorder. Dieters had a lower mean score for exaggerated food interest although this was not significantly different from anorexics. The item is concerned with interest and preoccupation with nutrition, food theory, cookery and so on, and it is perhaps not surprising that many dieters share such interest with those suffering
154

A Validation Study of the CEDRI
T 2 5 +-did=
4
2
1.5 mean adri scorn
1
0.5
0
Figure 2. COmQarison of CEDRI scum of bulimia nemsa sampk with control sample of ‘dieters’
from anorexia nervosa. Use of drugs other than laxatives for weight control did not discriminate between anorexics and dieters in our study, as both our samples scored zero on this item. Avoidance of wearing certain clothes or taking part in certain activities because of self-consciousness about body size did not discriminate between dieters and anorexics although dieters had slightly lower mean scores. This item is perhaps less well defined than others and was less reliably rated in an earlier study (Palmer et al., 1987).
Only two items did not discriminate between subjects with bulimia nervosa and dieters. The items were exaggerated food interest and food monitoring. The bulimics mean score for exaggerated food interest was higher than the mean score for the dieters but not significantly so. As noted above, it is not surprising that dieters scored highly on this item. Similarly, it might be expected that dieters would score comparatively highly on food monitoring and that their mean scores might not be significantly different from subjects with bulimia nervosa in this respect.
These results suggest that the CEDRI is an instrument which not only shows satisfactory reliability (Palmer et al., 1987) but also has validity in the sense of discriminating between subjects with and without clinical eating disorders. Whilst none of the comparison group in this study suffered from a clinical eating disorder, the subjects were chosen as being likely to be weight concerned in that they were dieting. The ability of the CEDRI to discriminate between a relatively weight concerned comparison group and a sample of subjects with clinical eating disorders could be seen as a particularly exacting test of validity. Moreover, it is just such discriminations that are likely to be required in both research and clinical practice. The CEDRI can be a useful tool for use in both the everyday assessment of patients, and in the measurement of the features of the eating disorders in treatment trials and other studies.
155

R. Palmer, D. Robertson, M. Cain and S. Black
ACKNOWLEDGEMENTS We would like to thank the many people who have been involved in the development and validation of the CEDRI. We are particularly grateful to Pam Marshall and Dr Eric Button for their interview data on the clinical sample, and to Dr Julie Hurley, Dr Fiona McKenzie and Kathy Gadsby for providing data on the community sample of dieters. Dr Robertson was a Woodbourne Research Fellow funded by the Priory Hospitals Group at the time of this study.
REFERENCES AMERICAN PSYCHIATRIC ASSOCIATION (1987). Diagnostic and Statistical Manual of
Mental Disorders, 3rd edn, revised. Washington, DC. COOPER, Z. and Fairburn, C. G. (1987). The Eating Disorder Examination: a semi-structured
interview for the assessment of eating disorders. InternationalJournal of Eating Disurden, 6,143.
COOPER, Z., Cooper, P. J. and Fairbum, C. (3. (1989). The validity of the Eating Disorder Examination and its subscales. British Journal of Psychiatry, 154, 807-812.
FICHTER, M. M., Elton, M., Engel, K., Meyer, A., Poustka, F., Mall H. and von der Heydte, F. (1989). The Structured Interview for Anorexia and Bulimia Nervosa (SIAB): development and characteristics of a semi-standardised instrument. In: Bulimia Nervosa: Basic Research, Diagnosis and Therapy (ed. M. M. Fichter). Chichester: Wiley, pp. 57-70.
GARNER, D. M. and Garfinkel, P. E. (1979). The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychological Medicine, 9, 273-279.
GARNER, D. M., Olmstead, M. P. and Polivy, J. (1983). Development and validation of a multidimensional eating disorders inventory for anorexia nervosa and bulimia. International Journal of Eating Disorders, 2,14-15.
HENDERSON, M. and Freeman, C. P. (1987). A self-rating scale for bulimia. The ‘BITE. British Journal of Psychiatry, 150, 18-24.
PALMER, R., Christie, M., Cordle, C., Davies, D. and Kendrick, J. (1987). The Clinical Eating Disorders Rating Instrument (CEDRI): a preliminary description. International journal of Eating Disorders, 6, 9-16.
Robert Palmer, MB, BS, FRCPsych, DPM (Senior Lecturer)
David Robertson, MB, ChB, MRCPsych (Woodbourne Research Fellow)
Mark Cain, BSc, PhD (Information Systems Assistant)
Susanna Black, BSc (Research Assistant) Department of Psychiatry, University of Leicester Leicester General Hospital, Gwendolen Road Leicester LE5 4PW, U.K.
156