
The Clinical Course of MS: PttiTh hP iPresentation Through...
56
The Clinical Course of MS: P t ti Th hP i Presentation Through Progression
Transcript of The Clinical Course of MS: PttiTh hP iPresentation Through...
The Clinical Course of MS: P t ti Th h P iPresentation Through Progression

The Clinical Course of MS: Presentation Through Progression
• Clinical Presentation• Clinical Course• Classifications of MS• Disease Progression and DisabilityDisease Progression and Disability
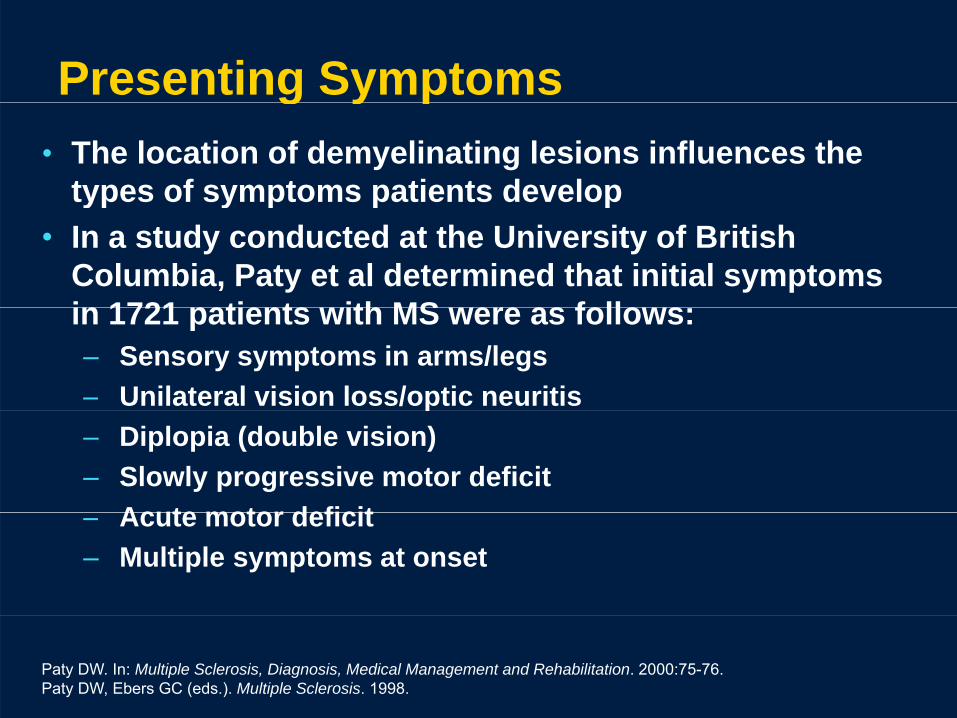
Presenting Symptoms g y p• The location of demyelinating lesions influences the
types of symptoms patients developyp y p p p• In a study conducted at the University of British
Columbia, Paty et al determined that initial symptoms in 1721 patients ith MS ere as follo sin 1721 patients with MS were as follows:– Sensory symptoms in arms/legs – Unilateral vision loss/optic neuritis p– Diplopia (double vision) – Slowly progressive motor deficit
Acute motor deficit– Acute motor deficit– Multiple symptoms at onset
Paty DW. In: Multiple Sclerosis, Diagnosis, Medical Management and Rehabilitation. 2000:75-76. Paty DW, Ebers GC (eds.). Multiple Sclerosis. 1998.
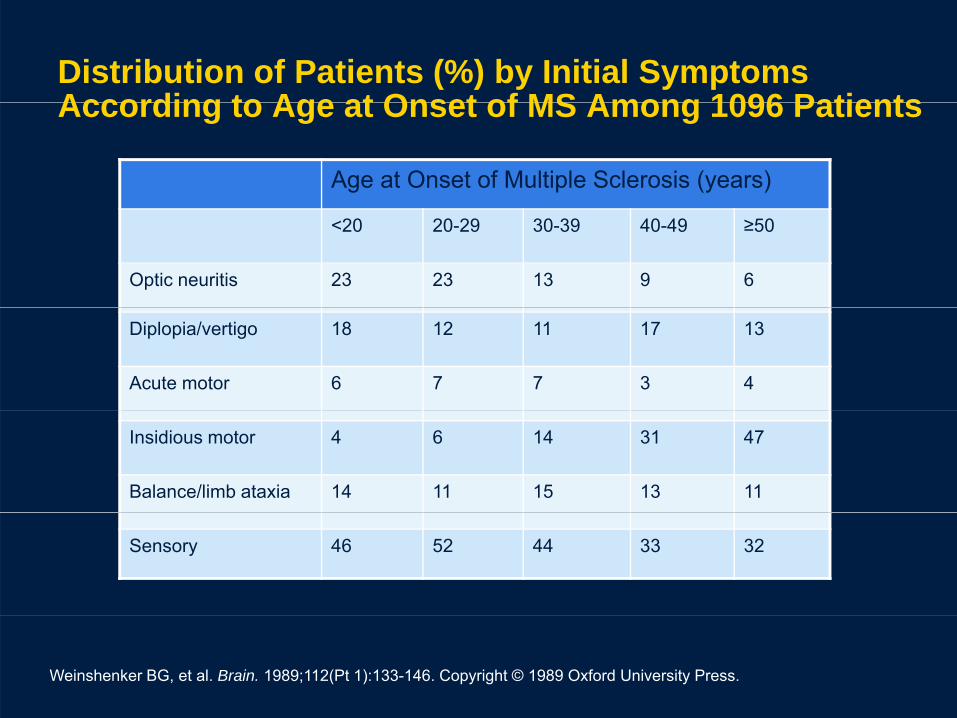
Distribution of Patients (%) by Initial Symptoms According to Age at Onset of MS Among 1096 PatientsAccording to Age at Onset of MS Among 1096 Patients
Age at Onset of Multiple Sclerosis (years)
<20 20-29 30-39 40-49 ≥50
Optic neuritis 23 23 13 9 6
Diplopia/vertigo 18 12 11 17 13
Acute motor 6 7 7 3 4
Insidious motor 4 6 14 31 47
Balance/limb ataxia 14 11 15 13 11
Sensory 46 52 44 33 32
Weinshenker BG, et al. Brain. 1989;112(Pt 1):133-146. Copyright © 1989 Oxford University Press.
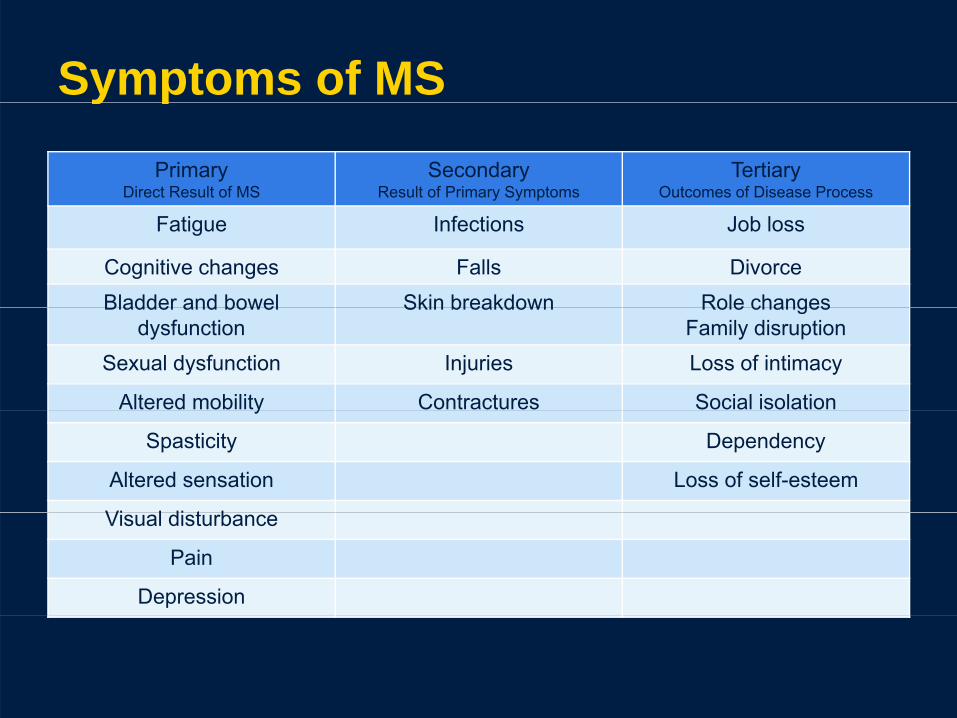
Symptoms of MSPrimary
Direct Result of MSSecondary
Result of Primary SymptomsTertiary
Outcomes of Disease Process
y p
Fatigue Infections Job loss
Cognitive changes Falls DivorceBladder and bowel Skin breakdown Role changesBladder and bowel
dysfunctionSkin breakdown Role changes
Family disruptionSexual dysfunction Injuries Loss of intimacy
Altered mobility Contractures Social isolationy
Spasticity Dependency
Altered sensation Loss of self-esteem
Vi l di t bVisual disturbance
Pain
Depression

Diseases That Mimic MS• Inflammatory/autoimmune
– Sjögren’s syndrome• Demyelinating
– Neuromyelitis optica– Systemic lupus
erythematosus– Wegener’s granulomatosis
S id i
– ADEM– Optic neuritis
• CNS neoplasms– Sarcoidosis– Behçet disease
• InfectiousPML
– CNS lymphoma• Metabolic
– Vitamin B12 deficiency– PML– HIV-related disorders– Lyme’s disease
CNS hili
• Cerebrovascular disease• Migraine• Myasthenia gravis
– CNS syphilis • Genetic/hereditary– Adrenomyeloneuropathy– CADASIL
ADEM=acute disseminated encephalomyelitis; CADASIL=cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; CNS=central nervous system; PML=progressive multifocal leukoencephalopathy
Burks J. Multiple Sclerosis: Diagnosis, Medical Management, and Rehabilitation. 2000.
Lab Studies for Differential Diagnosis
• CBC with differential • Thyroid studies• ESR (sed rate)• Complete metabolic
panel
• VDRL, MHA-TP• Serum B12
H t ipanel• ANA, RA • Lymes titer
• Homocysteine• Methylmalonic acid
S I G• Lymes titer• SSA/SSB• Serum Vitamin D
• Serum IgG: oligoclonal bands in serum• Serum Vitamin D
(25-hydroxyvitamin D)serum
ANA=antinuclear antibody test; RA=rheumatoid arthritis testing; CBC=complete blood cell count; ESR=erythrocyte sedimentation rate; IgG=Immunoglobulin G; SSA/SSB=sicca syndrome A/B; VDRL=venereal disease research laboratory test; MHA-TP=microhemaagglutination assay
The Clinical Course of MS: Presentation Through Progression
• Clinical Presentation• Clinical Course• Classifications of MS• Disease Progression and DisabilityDisease Progression and Disability
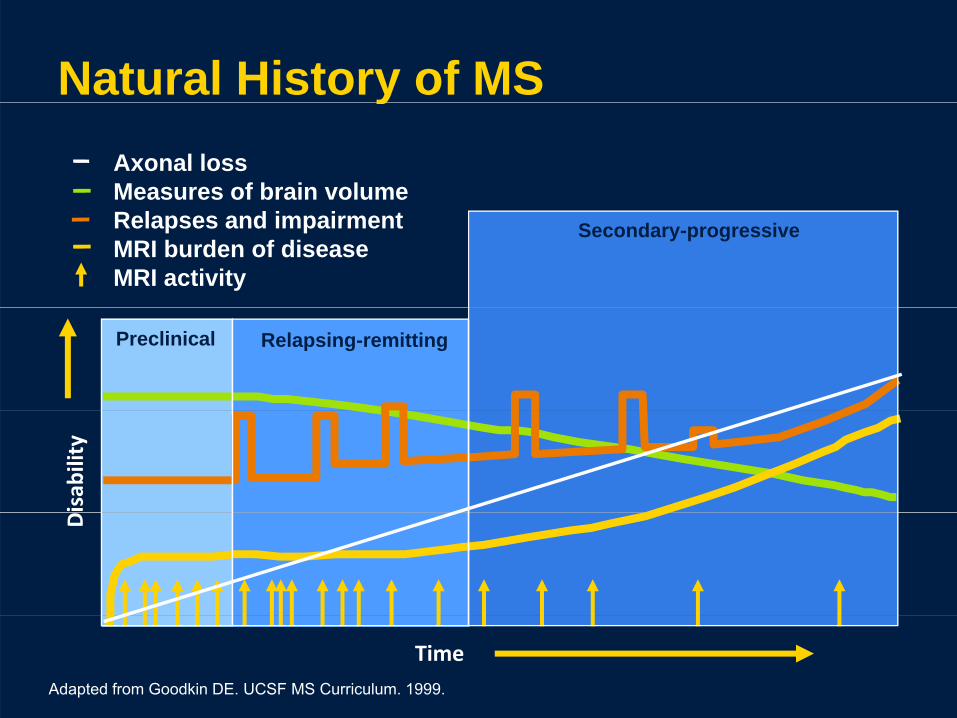
Natural History of MSyAxonal lossMeasures of brain volume
Secondary-progressiveRelapses and impairmentMRI burden of diseaseMRI activity
Relapsing-remittingPreclinical
TimeAdapted from Goodkin DE. UCSF MS Curriculum. 1999.
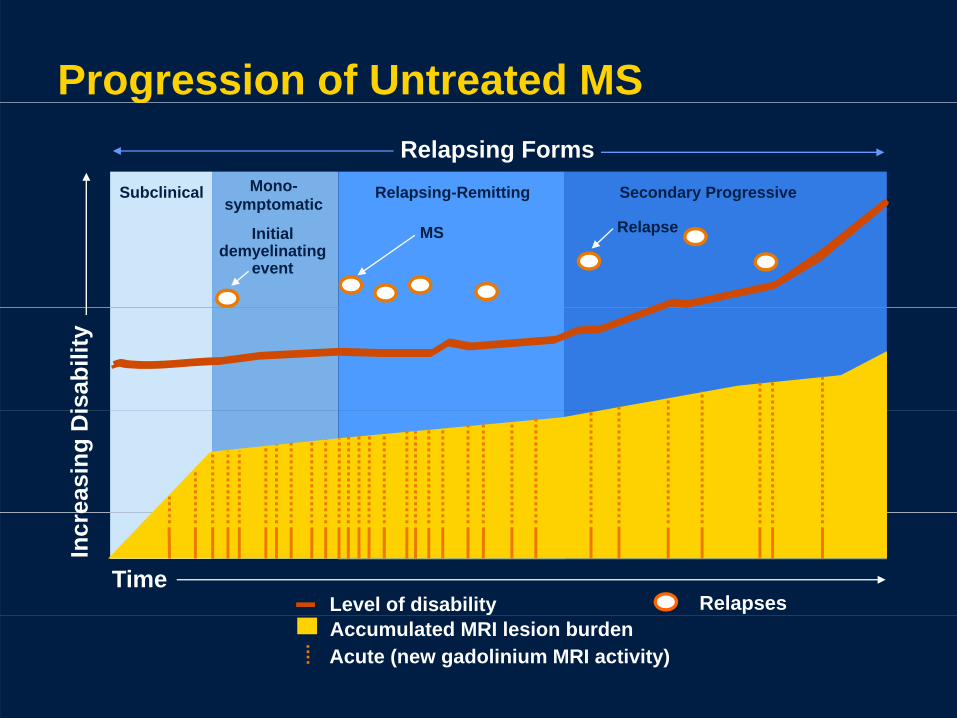
Progression of Untreated MS
Subclinical Mono-symptomatic
Relapsing-Remitting Secondary Progressive
Relapsing Forms
g
symptomatic
Initial demyelinating
event
MS Relapse
isab
ility
ea
sing
Di
Time
Incr
e
Level of disability RelapsesAccumulated MRI lesion burdenAcute (new gadolinium MRI activity)

Axonal Transection in MSProposed correlation of MS clinical course, axonal loss, and neurologic disability
RRMS SPMS
ClinicalThreshold
Axonalloss
Irreversibleneurologicdisability
Relapses
Threshold
Neuronal
loss
CNS cannotcompensatefor neuronal
l
Y5 10 15 20
Neuronalloss compensated
by CNS
Axonal Loss Initiatest Di O t
loss
Adapted from Trapp BD, et al. Curr Opin Neurol. 1999;12(3):295-302.
Yearsat Disease Onset
The Clinical Course of MS: Presentation Through Progression
• Clinical Presentation• Clinical Course• Classifications of MS• Disease Progression and DisabilityDisease Progression and Disability
Classifications of MS• Radiologically isolated syndrome (RIS)• Clinically isolated syndrome (CIS)• Clinically isolated syndrome (CIS)• MS • Four established clinical courses differ by the• Four established clinical courses differ by the
time course of relapse and progressionRelapsing remitting MS (RRMS)– Relapsing-remitting MS (RRMS)
– Secondary progressive MS (SPMS) Primary progressive MS (PPMS)– Primary progressive MS (PPMS)
– Progressive relapsing MS (PRMS)
Goodin DS, et al. Neurology. 2002;58(2):169-178. Craig J, et al. J Neurol Neurosurg Psychiatry. 2003;74(9):1225-1230.

Radiologically Isolated Syndrome (RIS)
• Absence of MS symptoms• MRI taken for reasons other than MS• MRI taken for reasons other than MS• MRI findings highly suggestive of MS based on location
and morphology in CNS• Okuda study of 44 patients with RIS over 5 years
– 10 patients developed a CIS or MS; 59% showed radiologic progression over timeradiologic progression over time
• Question: When to treat?• Emotional/psychological repercussions for the patient
li i ith di l i l di i b t t li i lliving with a radiological diagnosis but not a clinical diagnosis; risk of patient developing fear of the clinical disease
Okuda DT, et al. Neurology. 2009;72(9):800-805.
Clinically Isolated Syndromey y• First neurologic episode identified using clinical, MRI, laboratory,
and demographic dataMay or may not develop MS• May or may not develop MS
• Features of a CIS that are suggestive of a first MS attack include:– Appropriate age
Ab l b i MRI (di i ti i )– Abnormal brain MRI (dissemination in space)– Characteristic syndrome: monofocal or multifocal lesions
• Optic neuritis: typically unilateral, retrobulbar, and painful; some recovery usualsome recovery usual
• Brainstem/cerebellar dysfunction: most commonly ocular motor syndromes (INO, nystagmus), ataxia, dysarthria, sensory or motor signssensory or motor signs
• Myelitis: partial sensory more common than partial motor, bowel and bladder dysfunction is common, Lhermitte’s, band-like pressure thorax
Frohman EM, et al. Neurology. 2003;61(5):602-611.
INO=internuclear ophthalmoparesis

CIS, continued• The challenge for the physician:
– To determine the likelihood that a patient with a CIS willTo determine the likelihood that a patient with a CIS will experience a second demyelinating event in the future, thereby meeting the criteria for a definite diagnosis of MS
• CIS and MRI findings:– When CIS is accompanied by MRI-detected brain lesions
consistent with MS, there is a high risk of a second neurologic event and diagnosis of MS within several years
– Individuals who experience a CIS with no evidence of MRI-pdetected lesions are at relatively low risk for developing MS
Frohman EM, et al. Neurology. 2003;61(5):602-611.

Clinical Challenges for the MS TeamClinical Challenges for the MS Team
• Implications of disclosure• Need for counselingg• Family and financial planning• Cost of care and cost of treatmentCost of care and cost of treatment• Insurance implications

Implications for the MS TeamImplications for the MS Team
• Disclosure and counseling to patient and family
• Financial planning• Cost of care• Cost of treatment• Insurance implications• Insurance implications

CIS Patients: Risk of MS DiagnosisNumber of MRI lesions at baseline relates to risk of developing MS
g
p g
80
100
(%)
60
80
on to
MS
20
40
onve
rsio
0 2–31 4–10 >100
N b f MRI L i t B li
C
O’Riordan JI, et al. Brain. 1998;121(Pt 3):495-503.Swanton JK, et al. Lancet Neurol. 2007;6(8):677-686.
Number of MRI Lesions at Baseline

MS
MS i di d f ll i CIS i dMS is diagnosed following a CIS episode and presenting with at least 2 neurologic events consistent with demyelinationevents, consistent with demyelination, occurring in separate anatomical locations within the CNS and occurring at differentwithin the CNS and occurring at different times.
Polman CH, et al. Ann Neurol. 2005;58(6):840-846.
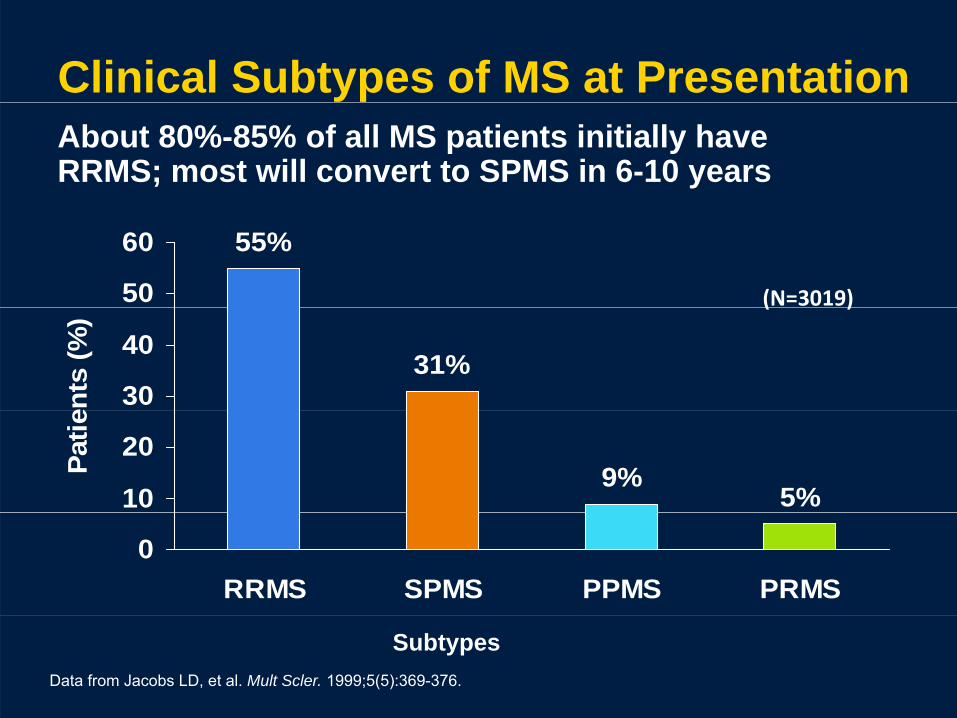
Clinical Subtypes of MS at PresentationAbout 80%-85% of all MS patients initially have RRMS; most will convert to SPMS in 6-10 years
(N=3019)
55%
50
60
( )
31%30
40
ents
(%)
9%5%10
20Patie
0RRMS SPMS PPMS PRMS
Data from Jacobs LD, et al. Mult Scler. 1999;5(5):369-376.
Subtypes

RRMS• Most frequent form of MS: 80%-85% of patients• Female preponderance of about 2:1e a e p epo de a ce o about• Onset usually with a CIS, such as optic neuritis• Characterized by acute episodes of neurologic dysfunction
(relapse) evolving over several days and peaking after 1 2(relapse) evolving over several days and peaking after 1-2 weeks, then stabilizing and improving spontaneously (remission) or in response to corticosteroids over several weeks or even monthsweeks or even months
• Recovery from relapse episodes may be only partial in some patients with residual symptoms persisting indefinitely, especially sensory symptomsespecially sensory symptoms
• In between attacks, the patient is neurologically and symptomatically stable
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911.Goodin DS, et al. Neurology. 2002;58(2):169-178.

RRMS
No disease progression between relapsesNo disease progression between relapses
crea
sing
isab
ility
crea
sing
isab
ility
Inc D Inc D
Time Time
Acute relapses with full recovery Acute relapses with sequelae and residual deficit upon recovery
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911. Copyright © 1996 The American Academy of Neurology.
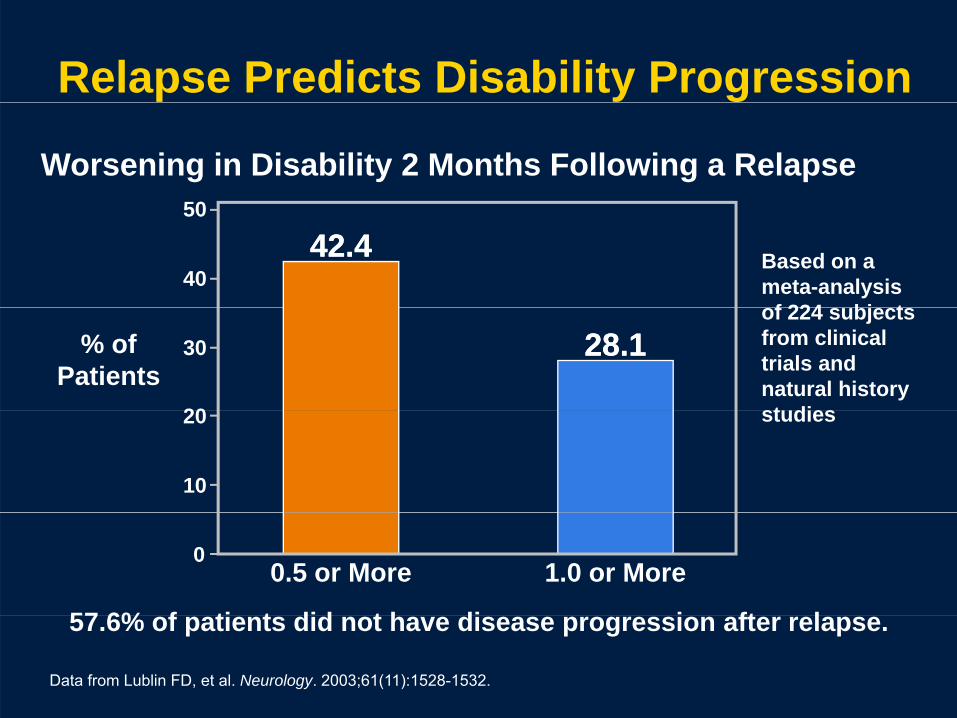
Relapse Predicts Disability Progression
Worsening in Disability 2 Months Following a Relapse50
42.442.440
50
Based on a meta-analysis
f 224 bj t28.128.1
20
30% of Patients
of 224 subjects from clinical trials and natural history t di
10
20 studies
57 6% f ti t did t h di i ft l
00.5 or More 1.0 or More
57.6% of patients did not have disease progression after relapse.
Data from Lublin FD, et al. Neurology. 2003;61(11):1528-1532.

SPMS• Begins as RRMS• Natural history studies show that 50% of untreatedNatural history studies show that 50% of untreated
patients after 10 years will develop SPMS; after 25 years, 90% will have SPMS
f• After 10 or 20 years, the attack rate is reduced and patients transition from RRMS to SPMS
• The course is then a steady deterioration in functionThe course is then a steady deterioration in function unrelated to acute attacks
• Progression of neurologic compromise in SPMS
L bli FD R i ld SC N l 1996 46(4) 907 911
must occur independent of discrete recognized relapses and be evident between clinical attacks
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911.Goodin DS, et al. Neurology. 2002;58(2):169-178.Schwid S. In: Multiple Sclerosis Therapeutics. 1999:443.Weinshenker BG, et al. Brain. 1989;112(Pt 1):133-146.

SPMS
Patients with an initial RRMS course convert to SPMS,
SPMS
Patients with an initial RRMS course convert to SPMS, which is characterized by continuous progression
reas
ing
sabi
lity
reas
ing
sabi
lity
Incr Dis
Incr Dis
Time Time
Without relapses With relapses
Time Time
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911. Copyright © 1996 The American Academy of Neurology.

PPMS
• Occurs in 10%-15% of patientsp• Characterized by steady deterioration of
neurologic function from disease onset in gthe absence of clearly defined relapses
• Patients tend to be older at onset • Frequency of occurrence slightly greater
in men
G di DS t l N l 2002 58(4) 169 178
in men
Goodin DS, et al. Neurology. 2002;58(4):169-178.Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911.Miller DH, Leary SM. Lancet Neurol. 2007;6(10):903-912.Stevenson VL, et al. Neurology. 1999;52(4):839-845.

PPMS
PPMS is characterized by progression of disabilityPPMS is characterized by progression of disability from onset
crea
sing
Dis
abili
ty
crea
sing
isab
ility
In D Inc D
Time Time
Without plateaus or remissions With occasional plateaus and temporary minor improvements
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911. Copyright © 1996 The American Academy of Neurology.
PRMS
• Rarest form of MS• Characterized by steady decline in
neurologic function from the onset, ginterspersed with brief periods of acute exacerbations
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911.

PRMSPRMS is characterized by disease progression from onset with the occurrence of clear acute relapsesp
ncre
asin
gD
isab
ility
crea
sing
isab
ility
In D Inc D
Time Time
Full recovery following relapse with progression between relapses
Without full recovery following relapse with progression between p p grelapses
Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911. Copyright © 1996 The American Academy of Neurology.
Relapses in MSp• Relapse is a sudden onset of new symptoms that interfere with
function• Synonyms:
– Attack – Exacerbation– Exacerbation – Flare
• Definition:S dd i f MS t th f– Sudden worsening of any MS symptom or the appearance of new symptom
– Last at least 24 hours – Separated from a previous exacerbation by at least 1 month– Occur in absence of environmental, metabolic, or infectious
processes
National MS Society: CIS. http://www.nationalmssociety.org/about-multiple-sclerosis/diagnosing-ms/cis/index.aspx. April 8, 2009.

Relapses in MS, continuedp• Characterized by:
Relatively sudden onset of mobility impairment– Relatively sudden onset of mobility impairment
• May result in:• May result in:– Loss of work– Potential for activity limitationPotential for activity limitation– May require an immediate change in family
member roles (driving, cooking, child care, home ti iti / h )activities/chores)

Relapses in MS, continued p• Etiology:
– Correlate with focal areas of CNS inflammation caused by immune mechanisms, followed by axonal demyelination
– This causes the nerve impulses to be slowed, p ,distorted, or halted, producing the neurological symptoms of MS
– Results in the formation of pathoneumonic MS– Results in the formation of pathoneumonic MS plaques
• Impact on quality of life (QOL):– May be mild or severe interfering with daily life – Usually last from several days to several weeks,
although may extend into months
Compston A, Coles A. Lancet. 2002;359(9313):1221-1231.
a t oug ay e te d to o t s– Occur about once every year in untreated patients
Pseudo Relapsesp
• Last less than 24 hours• Occur in the setting of illness,
overheating, febrile state, heat and humidity, flu-like reactions to interferons, exercise, or infections
• Usually self-limited and rarely require intervention beyond cooling measures and treatment of any underlying infection or inflammation

The Clinical Course of MS: Presentation Through Progression
• Clinical Presentation• Clinical Course • Classifications of MS• Disease Progression and DisabilityDisease Progression and Disability

Relapse vs Disease Progression in MS• Relapses and disease progression are defining clinical features of MS• Relapse: neurological symptoms of MS lasting a minimum of 24 hours
preceded by a period of clinical quiescence and not due to apreceded by a period of clinical quiescence and not due to a metabolic cause, such as a fever
• Disease progression: continued worsening of disease over timeConfavreux et al: “Neurological relapses in MS are the clinical• Confavreux et al: “Neurological relapses in MS are the clinical counterpart of acute focal inflammation of the CNS, whereas neurological progression is that of chronic diffuse neurodegeneration”neurodegeneration
• Controversy – Classic concept: succession of relapses leads to accumulation of
disability; disease progression is caused by subclinical relapsesy; p g y p– New concept: recent data from Lyon MS cohort showed irreversible
disability appeared not to be affected by clinical relapses, and suppressing relapses using disease-modifying therapy did not
i ifi tl i fl th i f i ibl di bilit
Confavreux C, Vukusic S. Clin Neurol Neurosurg. 2006;108(3):327-332.
significantly influence the progression of irreversible disability.

Signs of Disease Progression in MSg g
• Increasing disability without relapses• Increasing relapses without return to
baseline• Decreased cognitive function• Increasing MRI activityg y• Increased use of MS-related medicines to
control symptomscontrol symptoms• Decline in activities of daily living and
quality of lifequality of life
How to Measure Progression of Di i MSDisease in MS• Well-defined methods • Disability Rating Scales
– Expanded Disability Status Scale (EDSS)Multiple Sclerosis Functional Composite (MSFC) (Not– Multiple Sclerosis Functional Composite (MSFC) (Not recognized by the FDA as an outcome measure)
• MRI changes– Gadolinium (Gd)-enhancing lesions (T1 weighted)– Measurement of brain atrophy (using visual analysis of
MRI data to estimate brain atrophy)MRI data to estimate brain atrophy)• Other methods under investigation or being studied
– Optical coherence tomography (a structural biomarker)– Visual evoked potentials – Biologic markers
Measuring Disability: The EDSSMeasuring Disability: The EDSS• Ordinal scale (range 0-10) measuring ( g ) g
disability in increments of 0.5• Divided into stages of increasingDivided into stages of increasing
disability• Most widely accepted measure ofMost widely accepted measure of
disability• Reflects impact on neurological functionReflects impact on neurological function
Kurtzke JF. Neurology. 1983;33(11):1444-1452.
EDSS Functional SystemsEDSS Functional Systems
• Pyramidal• Cerebellar• Brainstem• Mental• Spasticity• Sensory• Visual• Bowel and bladder

EDSS: Administration and ScoringEDSS: Administration and Scoring
• Administered by a trained professional • Time to complete is 15-45 minutes• Functional systems (FS) quantify the results
of the neurological exam• Rated on a scale 0 to 5 or 6• Rated on a scale 0 to 5 or 6
• EDSS based on a 10-point scale• 0 (no impairment) to 10 (death due to MS)0 (no impairment) to 10 (death due to MS)
• Progression: based on 2-point change in FS and 1-point change on EDSS
Coulthard-Morris L. In: Multiple Sclerosis: Diagnosis, Medical Management, and Rehabilitation. 2000:221-228.
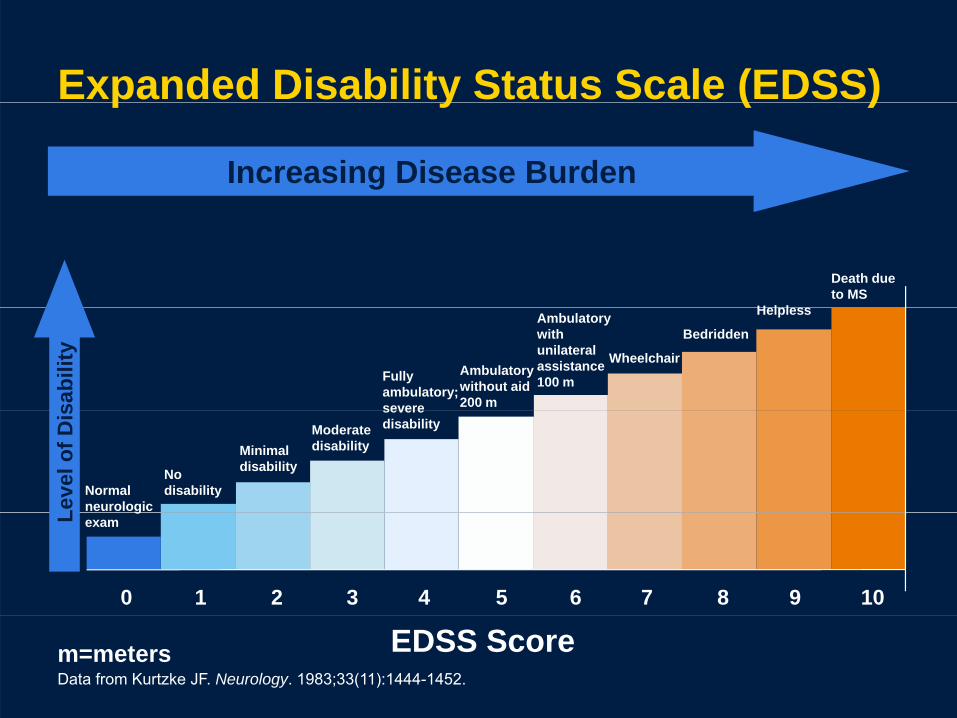
Expanded Disability Status Scale (EDSS)
Increasing Disease Burden
p y ( )
H l l
Death due to MS
Fully ambulatory; severe
Ambulatory without aid 200 m
Ambulatory with unilateral assistance 100 m
Wheelchair
Bedridden
Helpless
sabi
lity
Normalneurologic
No disability
Minimaldisability
Moderate disability
severe disability
Leve
l of D
is
7 8 9 100 1 2 3 4 5 6
gexamL
m=metersData from Kurtzke JF. Neurology. 1983;33(11):1444-1452.
EDSS Score
How to MeasureP i f Di MSFCProgression of Disease: MSFC• Developed by National Multiple Sclerosis Society’s p y p y
Advisory Committee on Clinical Trials of New Agents in Multiple SclerosisMa be s perior to EDSS in terms of sensiti it• May be superior to EDSS in terms of sensitivity, reliability, and statistical validity
• Consists of 3 quantitative tests of neurological q gfunction calculated to provide a single composite scoreU f l f li i l t i l d li i l ti• Useful for clinical trials and clinical practice
• Not recognized by FDA as an outcome measure
Cutter et al. Brain. 1999;122:871‐882.
Rudick RA, et al. J Neurol Sci. 2008.Miller JR. J Manag Care Pharm. 2004;10(3 suppl B);S4-S11.
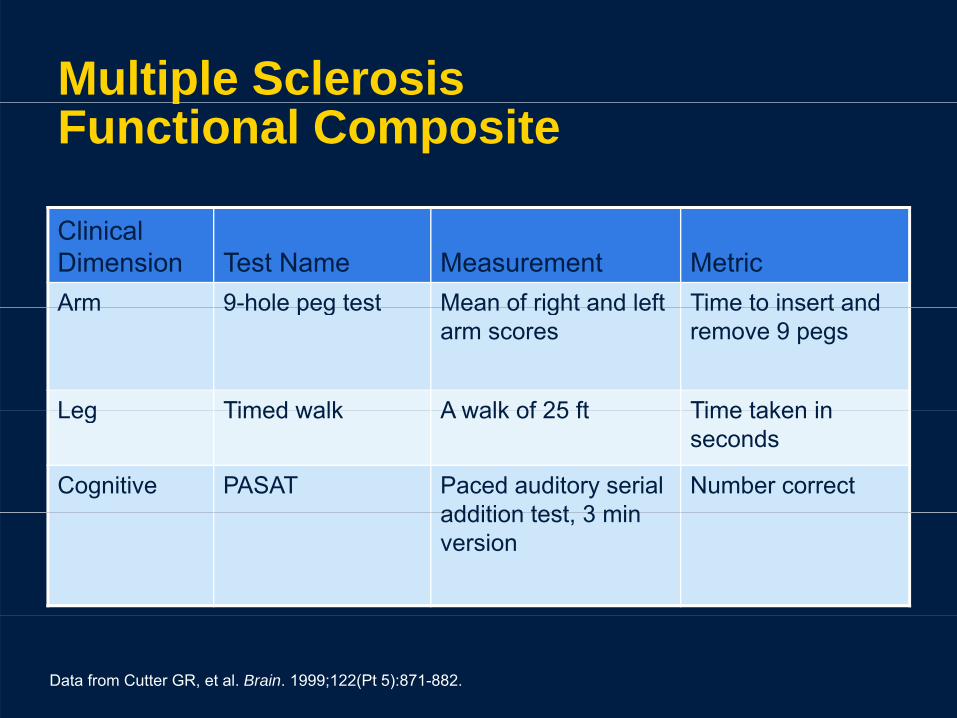
Multiple Sclerosis pFunctional Composite
Clinical Dimension Test Name Measurement MetricArm 9-hole peg test Mean of right and left Time to insert andArm 9 hole peg test Mean of right and left
arm scoresTime to insert and remove 9 pegs
Leg Timed walk A walk of 25 ft Time taken inLeg Timed walk A walk of 25 ft Time taken in seconds
Cognitive PASAT Paced auditory serial addition test 3 min
Number correctaddition test, 3 min version
Data from Cutter GR, et al. Brain. 1999;122(Pt 5):871-882.
Other Methods Under Studyy
• Optical coherence tomography – Noninvasive, noncontact technique– Evaluates qualitative and quantitative changes of the
retinal nerve fiber layer (RNFL)y ( )– Measures axonal pathologic changes
• Visual evoked potentials– In patients diagnosed with optic neuritis but not with
MS multifocal visual evoked potential latency delayMS, multifocal visual evoked potential latency delay may be able to assist in predicting progression to future MS
Sergott RC. Curr Opin Ophthalmol. 2005;16(6):346-350.Fraser C, et al. Arch Neurol. 2006;63(6):847-850.

Biologic Markersg• In blood
– Uric acid, apoptosis markers, antibodies: (eg, neutralizing , p p , ( g, gantibodies to IFN beta, glatiramer antibodies)
• In CSF – The neurofilament light chain is a promising axonal markerThe neurofilament light chain is a promising axonal marker
for discriminating patients with MS from those with other neurological diseases
– Altered CSF concentrations of tau proteins, actin, tubulin,Altered CSF concentrations of tau proteins, actin, tubulin, and 14-3-3 protein
– Markers reflecting processes in the CNS, those reflecting extra neural processes, and those reflecting whole-bodyextra neural processes, and those reflecting whole body changes
• In urine– Myelin basic protein-like material (MBPLM)
Teunissen CE, et al. Lancet Neurol. 2005;4(1):32-41.Miller A, et al. Clin Neurol Neurosurg. 2004;106(3):249-254.
– Myelin basic protein-like material (MBPLM)

Radiological Progressiong g
• Disease progression is monitored on MRI by:– Number and volume of lesions on T2-
weighted imaging (T2 lesion load of T2 burden of disease [BOD])of disease [BOD])
– Presence, number, and appearance of Gd-enhancing lesionse a c g es o s
– Number and volume of T1-weighted hypointense lesions (T1 BOD)
– Brain atrophy (net tissue loss)
Wolinsky J. In: Multiple Sclerosis Therapeutics. 2007:45-63.

Clinical Case: Angelag• A 21-year-old woman presenting with acute onset of visual loss in
her right eye.• Past medical history: unremarkable • Family history: no neurological or visual problems• Social history: recently graduated from college with a BA in
business• Ophthalmologic examination: decreased visual acuity (20/200 OD),
red desaturation, a relative afferent papillary defect in her right eye• Treatment: methylprednisolone 1 g daily x 3 days; her symptoms
completely resolved• Prior to initiating therapy, a brain MRl with contrast, including
FLAIR MRl h d l i d b i t hFLAIR MRl sequences, showed no lesions and no brain atrophy.• Radiological interpretation: within normal limits• The patient is very anxious and wants to know what is wrong with
h d h t h f t ill bher and what her future will be.• She is planning to start a new career that involves traveling and is
not sure if this is a wise plan.
In light of this history and findings, g y gthis patient:
a. Is at a high risk for MSb. Presented with a CIS and should be
treatedc. Should have a lumbar puncture nowpd. Should be followed clinically and by MRI
If a patient has a CIS and no MRI lesions at b li th 14 i k f d l i MSbaseline, the 14-year risk for developing MS is approximately:
a. 20%b 55%b. 55%c. 65%d 90%d. 90%

Patients with a CIS and 1-3 MRI lesions have approximately ___ risk of developing MS over 14 years?
a. 22%b 55%b. 55%c. 70%d 90%d. 90%
The patient went online and is now convinced h h MS Sh l b li h dshe has MS. She also believes she needs
further studies because she read MS can now be diagnosed using technology. What can you g g gy ydo to help address this concern?
a. Order a lumbar puncturepb. Consider evoked potentialsc Order another MRl using a 3 Teslac. Order another MRl using a 3 Tesla
magnetd Advise the patient that MS is a clinicald. Advise the patient that MS is a clinical
diagnosis supported by paraclinical evidenceevidence
Supportive care for this patient pp pshould include:
a. Reassurance and rescheduling of return visit
b. Counseling about wellness activitiesc. Referral to a support grouppp g pd. Advise the patient to seek a second
opinionop o
Six months later, the patient continues to call regularly for information and has questions and concerns Shefor information and has questions and concerns. She feels depressed and anxious and wants treatment so she will not develop MS. You are concerned about her anxiety and her continual focus on MS She wantsanxiety and her continual focus on MS. She wants another MRI as soon as possible. Your best response would be to:
a. Obtain a brain MRI with contrast and compare it with the previous scanp p
b. Refer her back to her ophthalmologistc Prescribe an anti-anxiety agentc. Prescribe an anti-anxiety agentd. Refer her to a psychiatrist

Angela Conclusionsg• With only one clinical episode and no MRI lesions, this
patient does not meet the diagnostic criteria for MS. However, follow-up over time is important to monitor her possible conversion to MS. In the Optic Neuritis Treatment Trial (388 patients who experienced acute optic neuritis), the 10-year risk of developing MS was 56% for patients with at least one MRI lesion at baseline and 22% for those who had no lesions. Therefore, with this patient, the clinical role is to reassure the patient that her risk for developing MS was negligible and educate her.
• Further testing is usually not performed at this time, although clinicians should use their best judgment.
• However, this patient has been exposed to information on the Internet and is very anxious. It might be prudent to y g prespond to her anxiety and calm her fears now so she will sustain her relationship with you for future follow-up.

References
• Beck RW, et al. Arch Ophthalmol. 2003;121(7):944-949.
• Coyle PK, Johnson KP. J Neurol Sci. 2007;256 Suppl 1:S1-4.


















