The Changing Natural History of Tuberculosis and HIV Coinfection ...
7
S208 • CID 2010:50 (Suppl 3) • Bekker and Wood SUPPLEMENT ARTICLE The Changing Natural History of Tuberculosis and HIV Coinfection in an Urban Area of Hyperendemicity Linda-Gail Bekker 1,2 and Robin Wood 1,2 1 The Desmond Tutu HIV Centre, Institute of Infectious Disease and Molecular Medicine, and 2 Department of Medicine, University of Cape Town, Cape Town, South Africa Tuberculosis (TB) has proven to be difficult to control in regions with a high prevalence of human immu- nodeficiency virus (HIV) infection. We previously described high prevalence of HIV infection among adults (23%) and rapidly escalating TB notification rates in a peri-urban township, Site-M in Cape Town, South Africa. The combination of delineated boundaries, a well-characterized population, centralized TB record keeping, and high levels of HIV testing make this population uniquely suited for TB epidemiologic and transmission studies. The driver of the HIV and TB coepidemic appears to be a high annual risk of Myco- bacterium tuberculosis infection in this community. A high annual risk of M. tuberculosis infection may be the result of unrecognized infections coupled with intense social interaction and crowding. New non–facility- based interventions will be required, with emphasis on community-based case finding and contact tracing to decrease the infective TB pool. There is a need for better understanding of the transmission dynamics of TB and the intensity of social interactions, which have exacerbated an HIV and TB epidemic in this community of hyperendemicity. Tuberculosis (TB) remains a challenge to global public health, is a major cause of mortality, and has proven to be particularly difficult to control in regions with a high prevalence of human immunodeficiency virus (HIV) infection. An estimated 1.3 million deaths due to TB occur annually among HIV-uninfected individ- uals, and an additional 0.5 million deaths occur among HIV-infected persons. Of the estimated global burden of 9.3 million new TB cases in 2007, 1.37 million (14.8%) were associated with HIV infection and ac- counted for almost 25% of global AIDS-related mor- tality [1]. Sub-Saharan Africa has borne the brunt of the HIV Reprints or correspondence: Dr Linda-Gail Bekker, The Desmond Tutu HIV Centre, The Institute of Infectious Disease and Molecular Medicine, Wernher Beit Bldg, Health Science Faculty, University of Cape Town, Anzio Rd, Observatory, 7925, Cape Town, South Africa ([email protected]). Clinical Infectious Diseases 2010; 50(S3):S208–S214 2010 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2010/5010S3-0019$15.00 DOI: 10.1086/651493 and TB coepidemics, accounting for 79% of the global burden of HIV infection–associated TB cases in 2007. The 9 countries of the southern African region with hyperendemicity have TB case notification rates that are much higher than those for the rest of the African continent; these 9 countries have generalized HIV ep- idemics and report a prevalence of HIV infection of 50% among persons with newly diagnosed TB (Figure 1). In 2007, the estimated rate of TB case notifications in Africa was 161 cases per 100,000 population; how- ever, in this subregion of hyperendemicity, incidence rates of TB in South Africa and Swaziland increased to 948 cases per 100,000 population and 1198 cases per 100,000 population, respectively, with 73% and 80% of new TB cases, respectively, involving HIV coinfection. The Millennium Development Goals for global TB control are to halt and start to reverse the increasing incidence of TB and to halve the 1990 prevalence and death rates by 2015 [2]. In countries where TB is hy- perendemic, such as South Africa and Swaziland, achievement of Millenium Development Goals for TB Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369 by guest on 13 February 2018
Transcript of The Changing Natural History of Tuberculosis and HIV Coinfection ...

S208 • CID 2010:50 (Suppl 3) • Bekker and Wood
S U P P L E M E N T A R T I C L E
The Changing Natural History of Tuberculosisand HIV Coinfection in an Urban Areaof Hyperendemicity
Linda-Gail Bekker1,2 and Robin Wood1,2
1The Desmond Tutu HIV Centre, Institute of Infectious Disease and Molecular Medicine, and 2Department of Medicine, University of Cape Town,Cape Town, South Africa
Tuberculosis (TB) has proven to be difficult to control in regions with a high prevalence of human immu-
nodeficiency virus (HIV) infection. We previously described high prevalence of HIV infection among adults
(23%) and rapidly escalating TB notification rates in a peri-urban township, Site-M in Cape Town, South
Africa. The combination of delineated boundaries, a well-characterized population, centralized TB record
keeping, and high levels of HIV testing make this population uniquely suited for TB epidemiologic and
transmission studies. The driver of the HIV and TB coepidemic appears to be a high annual risk of Myco-
bacterium tuberculosis infection in this community. A high annual risk of M. tuberculosis infection may be
the result of unrecognized infections coupled with intense social interaction and crowding. New non–facility-
based interventions will be required, with emphasis on community-based case finding and contact tracing to
decrease the infective TB pool. There is a need for better understanding of the transmission dynamics of TB
and the intensity of social interactions, which have exacerbated an HIV and TB epidemic in this community
of hyperendemicity.
Tuberculosis (TB) remains a challenge to global public
health, is a major cause of mortality, and has proven
to be particularly difficult to control in regions with a
high prevalence of human immunodeficiency virus
(HIV) infection. An estimated 1.3 million deaths due
to TB occur annually among HIV-uninfected individ-
uals, and an additional 0.5 million deaths occur among
HIV-infected persons. Of the estimated global burden
of 9.3 million new TB cases in 2007, 1.37 million
(14.8%) were associated with HIV infection and ac-
counted for almost 25% of global AIDS-related mor-
tality [1].
Sub-Saharan Africa has borne the brunt of the HIV
Reprints or correspondence: Dr Linda-Gail Bekker, The Desmond Tutu HIV Centre,The Institute of Infectious Disease and Molecular Medicine, Wernher Beit Bldg,Health Science Faculty, University of Cape Town, Anzio Rd, Observatory, 7925,Cape Town, South Africa ([email protected]).
Clinical Infectious Diseases 2010; 50(S3):S208–S214� 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5010S3-0019$15.00DOI: 10.1086/651493
and TB coepidemics, accounting for 79% of the global
burden of HIV infection–associated TB cases in 2007.
The 9 countries of the southern African region with
hyperendemicity have TB case notification rates that
are much higher than those for the rest of the African
continent; these 9 countries have generalized HIV ep-
idemics and report a prevalence of HIV infection of
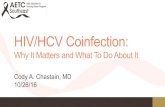
�50% among persons with newly diagnosed TB (Figure
1). In 2007, the estimated rate of TB case notifications
in Africa was 161 cases per 100,000 population; how-
ever, in this subregion of hyperendemicity, incidence
rates of TB in South Africa and Swaziland increased to
948 cases per 100,000 population and 1198 cases per
100,000 population, respectively, with 73% and 80% of
new TB cases, respectively, involving HIV coinfection.
The Millennium Development Goals for global TB
control are to halt and start to reverse the increasing
incidence of TB and to halve the 1990 prevalence and
death rates by 2015 [2]. In countries where TB is hy-
perendemic, such as South Africa and Swaziland,
achievement of Millenium Development Goals for TB
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

TB and HIV in an Area of Hyperendemicity • CID 2010:50 (Suppl 3) • S209
Figure 1. Estimated prevalence of HIV infection among persons with newly diagnosed cases of tuberculosis (TB), 2007. Reprinted with permissionfrom the World Health Organization [1].
is unlikely, because it would require a reversal of present TB
incidence trends and a 6-fold reduction in TB incidence during
the next 6 years.
Since the World Health Organization (WHO) declaration in
1993 that TB was a global emergency, the directly observed
therapy short-course (DOTS) strategy has been the key public
health intervention that has been widely used to affect global
TB control [3]. The strategy focuses on TB case management
of sputum smear–positive cases with use of short-course ri-
fampicin-containing chemotherapy. Case finding is passive and
facility based, with emphasis placed on case retention and the
achievement of a high cure rate. Although DOTS has been
effective in most regions of the world, contributing to the sus-
tained downward trend in global TB prevalence, it has been
comparatively ineffective in countries with a high prevalence
of HIV infection [1, 4–7]. During 2002–2004, the WHO and
the Stop-TB Partnership published guidelines [8], a strategic
framework [9], and an interim policy for TB and HIV infection
[10] to address the specific challenge of HIV infection–asso-
ciated TB. These interventions aim to reduce the burden of TB
in HIV-infected persons through use of TB prevention strat-
egies, including isoniazid preventive therapy (IPT), intensified
case finding, and infection control in conjunction with anti-
retroviral therapy (ART)—the so-called “3 I’s.”
However, mathematical modeling suggests that a combina-
tion of very high levels of ART coverage and early ART initi-
ation at high CD4 cell counts may be required to significantly
affect population TB control, especially in settings where TB
and HIV infection are hyperendemic [11]. Similarly, IPT is an
intervention that reduces the risk of active TB in already HIV-
infected individuals with latent TB infection rather than a pri-
mary strategy to control the public health burden of TB [12].
Although IPT is effective in decreasing the individual risk of
progression to TB [13], the modeled population impact of IPT
in areas of hyperendemicity is predicted to be small [14]. There-
fore, there is an urgent need to understand the epidemiological
factors driving the coepidemics in regions of hyperendemicity
to inform TB-control strategies.
LESSONS FROM EPIDEMIOLOGIC STUDIES INAN URBAN COMMUNITY WHERE TB ISHYPERENDEMIC
Although the global burden of HIV infection–associated TB is
concentrated in the southern African subregion, there are large
differences in disease burden even in the subregion. Specific
subpopulations, such as South African mine workers, have been
well documented to have a high TB incidence, in part because
of the multiplicative effect of HIV infection and mine work–
associated pulmonary silicosis [15]. In addition, rapid growth
of urban areas is occurring in the context of generally declining
economic performance, and the growth of urban areas includes
huge numbers of persons with low-income status [16, 17]. It
is estimated that ∼61% of South Africans are urbanized, and
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

S210 • CID 2010:50 (Suppl 3) • Bekker and Wood
Figure 2. An aerial photograph of Site-M (in Cape Town, South Africa), with superimposed property boundaries outlined. The figure was createdusing ArcGIS, version 9.2 (ESRI, 380 New York St, Redlands, CA 92373-8100).
57% of these persons live in slum conditions [18] where TB
and HIV burdens are greatest [19].
We previously described an epidemiologic study in South
Africa that found a high prevalence of HIV infection among
adults (23%) [5] and rapidly increasing TB notification rates
[20]. Specifically, annual TB notifications have now reached
2000 cases per 100,000 population in this peri-urban township
in Cape Town, designated by our study as “Site-M” [5, 20].
Regular household censuses have been performed that have
shown that the community has undergone rapid population
growth from 5000 residents in 1996 to 15,000 residents in 2008.
This population growth has occurred within well-circumscribed
boundaries (Figure 2). The community is socially deprived,
living in overcrowded, largely informal dwellings located on
demarcated plots serviced with water and sanitation. There is
a single health care facility that provides primary medical care
to community residents, and there is a primary and secondary
school. Increases in TB notification rate have occurred despite
a well-implemented national TB-control program based on the
WHO DOTS strategy [21] at the single community clinic that
manages all resident TB cases. Routine HIV testing (with con-
sent) of patients with incident TB was introduced in 2002. The
combination of delineated boundaries, a well-characterized
population, centralized TB record keeping, and high levels of
HIV testing make this population uniquely suited for studies
on TB epidemiology and transmission.
IMPACT OF HIV INFECTION ON TB CONTROL
Almost 2 decades ago, before the development of effective com-
bination ART, Styblo [6] reported that existing TB-control
strategies would be significantly undermined by HIV infection,
particularly in Africa. It was postulated that the impact of HIV
infection on the epidemiological situation of TB would depend
primarily on the following parameters: (1) the prevalence of
HIV infection in a community, (2) the prevalence of TB in the
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

TB and HIV in an Area of Hyperendemicity • CID 2010:50 (Suppl 3) • S211
Figure 3. The relationship between tuberculosis (TB) notification rates and seroprevalence of HIV infection in the South African population (diamonds)and the population at Site-M (triangles), with exponential regression lines for South African data during 1990–2005 (R2, 0.8461) and for Site-M dataduring 1996–2005 (R2, 0.9376).
general population aged 15–49 years, (3) the progression from
latent TB to active disease, (4) the level and trend in the annual
risk of (new) TB, and (5) the detection rate of new and relapse
cases of TB and cure rate among persons with smear-positive
cases.
Other more recently recognized factors include the obser-
vation that combination ART can significantly decrease TB in-
cidence [22] and the observation that TB incidence is very
dependent on current CD4 cell counts [23]. Taking these factors
into consideration, studies have focused on measuring the fol-
lowing likely drivers of increasing TB incidence in the study
community: prevalence of HIV infection, prevalence of un-
derlying latent TB, rates of progression from latent TB to active
TB, annual risk of TB, and case detection rates.
PREVALENCE OF HIV INFECTION
Since 1990, the South African Department of Health has per-
formed annual national surveys on the prevalence of HIV in-
fection among women attending antenatal services [24]. The
TB notification rates in South Africa from 1990 through 2005
[1] and the national antenatal seroprevalence of HIV infection
are shown in Figure 3 [24]. The corresponding adult TB no-
tification rates and prevalence of HIV infection among adults
at Site-M from 1996 through 2005 are also shown in Figure 3.
During the these periods, the seroprevalence of HIV infection
increased markedly, reaching levels of 30% and 23% among
national antenatal attendees and adults at Site-M, respectively.
TB notification rates have increased logarithmically for linear
increases in prevalence of HIV infection; an even stronger pos-
itive relationship was shown in the high-burden township. Pos-
sible explanations for this nonlinear relationship could include
changes in CD4 cell count distribution in the HIV-infected
population during the rapid-growth phase of the HIV epidemic
or increasing TB transmission between HIV-infected individ-
uals as the HIV epidemic grows rapidly.
AGE-SPECIFIC TB AND HIV INFECTION
Over the past decade the number of TB notifications has in-
creased markedly at Site-M, with the increased burden of TB
disease predominantly affecting persons aged 15–45 years (Fig-
ure 4A). The numbers of TB presentations at any age are a
function of the number of individuals in each age strata and
the TB rate specific to that age group. There have been sig-
nificant changes to age-specific TB rates over the past decade
that have been associated with increasing prevalence of HIV
infection (Figure 4B). TB rates appear to have increased in all
age groups; however, the most marked increases are among
persons aged 15–44 years, the age group most at risk of ac-
quisition of HIV infection.
POPULATION PREVALENCE OF TB
Prevalence of underlying latent TB at any age is influenced by
both the prevailing TB transmission rate and transmission rates
during the preceding years of life; therefore, prevalence of TB
increases with increasing age because of accumulated exposure.
The traditional way to measure latent TB is to measure reaction
to tuberculin antigens by tuberculin skin testing. Population
tuberculin skin testing surveys have been infrequently per-
formed in recent decades; however, a recent tuberculin skin
testing survey at Site-M township primary school reported TB
prevalences that increased from 8% at school entry to 53% by
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

S212 • CID 2010:50 (Suppl 3) • Bekker and Wood
Figure 4. A, Number of tuberculosis (TB) notifications, stratified byage, at Site-M over two 4-year periods: 1996–1999 (diamonds) and 2004–2007 (triangles). B, TB notification rates, stratified by age, at Site-M overtwo 4-year periods: 1996–1999 (diamonds) and 2004–2007 (triangles).
the age of 15 years [25]. Moreover, prevalence of latent TB
appeared to continue to increase throughout adolescence. In
2006, the HIV-uninfected control population at a similar nearby
township in Cape Town had a TB prevalence of 77% by the
age of 28 years [26]. Other similar township populations in
Cape Town have also shown equally high prevalence of adult
TB infection [27].
RATE OF PROGRESSION TO ACTIVE TBDISEASE
The temporal association between infection and risk of pro-
gression to active disease has been well recognized [28]. Pro-
gression to active disease is particularly rapid in children and
has been a marker of ongoing transmission; however, the re-
sultant TB disease is frequently sputum smear negative [29].
Childhood TB is conventionally reported internationally as a
!15 years smear positive rate [1]. In 2007, South Africa reported
a high smear positive childhood rate of 30 cases per 100,000
population. However, the high burden of childhood disease is
not adequately reflected by the !15 years smear positive rate.
In 2007, although the !15 year smear positive rate for Site-M
was 81 cases per 100,000 population, the TB notification rate
was 54 cases per 100,000 population among children !15 years
of age and reached 1390 cases per 100,000 population among
children !5 years of age.
There has been a marked change in the adult age of TB
disease presentation. During 1996–1997, a period of relatively
low prevalence of HIV infection, the incidence of TB increased
progressively with advancing age, with no case notifications for
adolescents (age, 10–19 years); however, TB notification rates
increasing steadily to 1700 cases per 100,000 population in the
fifth decade of life [5]. During 2003–2004, when the prevalence
of HIV infection among adults exceeded 20%, TB notifications
predominantly were for adolescents and young adults.
The estimated incidence of TB among HIV-uninfected and
HIV-infected adult community members in 2005 was 953 cases
per 100,000 population and 5140 cases per 100,000 population,
respectively [20], indicating a 5-fold increased risk among HIV-
infected individuals. As a consequence of these high TB inci-
dence rates, the lifetime cumulative risk of TB is extremely high
for both HIV-uninfected and HIV-infected individuals in this
community. The very high cumulative lifetime TB risk for HIV-
uninfected individuals is also much higher than the conven-
tional estimated lifetime risk of latent infection progressing to
TB disease of 10%–20% [30]. The increased lifetime risk may
result from increased rates of progression because of poor nu-
trition, exogenous reinfection, or exposure to a high initial
amount of infective TB [31]. The majority of individuals who
are coinfected with TB and HIV live in sub-Saharan Africa, an
area where hunger and malnutrition were already pressing con-
cerns before the onset of the HIV and TB epidemics.
LEVEL AND TREND OF ANNUAL RISK OF TB
Population density varies markedly among and within coun-
tries. Both the nature of the dwelling and crowding within the
dwelling will have an impact on the number of individuals
exposed to an infected person. Site-M has had an increasing
population density, reaching 15,700 persons/km2 in 2008. The
annual risk of TB among primary school children in 2008 was
estimated to be 3.8%–4.8% [25], which is unprecedented in
the current TB chemotherapeutic era. The annual risk of TB
is similar to that found in several large scale surveys performed
in western, eastern, and southern Africa from 1995 through
1960 [32]. In the prechemotherapy era, mean annual rates of
infection as high as 13% per annum were reported among
Parisian children in 1910 [33]. Lower rates of infection of 3%
per annum were recorded among children in post–World War
II Denmark [34].
A 77% prevalence of TB infection by age 28 years (during
a period of increasing TB notifications) would indicate a high
and ongoing mean risk of TB infection of 5.5% during an
individual’s preceding years of life. Childhood infection and
TB disease in Site-M have been shown to be strongly associated
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

TB and HIV in an Area of Hyperendemicity • CID 2010:50 (Suppl 3) • S213
with exposure to adult smear-positive TB in combined family
groups that are resident on each serviced plot [35].
In summary, the annual risk of TB in this community is
extremely high and appears to be maintained or to increase
throughout childhood and adolescence. Trends in the annual
risk of TB over time in any specific age group in this community
are less certain; however, there is little evidence for decreasing
transmission.
CASE DETECTION AND TREATMENT
Efficient case management of infective TB is the cornerstone
of the DOTS strategy [3], to which other supplementary control
strategies may be added [8–10]. The single TB facility in Site-
M implements DOTS-based, short-course, rifampicin-contain-
ing chemotherapy, administered in accordance with national
guidelines [36]. TB-associated mortality during 2002–2004, be-
fore availability of ART, among HIV-infected and HIV-unin-
fected persons with TB was 13% and 3%, respectively [20].
Treatment completion rates of persons surviving to 6 months
of age were 84% among HIV-infected persons and 86.6%
among HIV-uninfected persons [20]. In 2005, a cross-sectional
survey of a randomly selected subset of the general population
found that the existing facility-based smear-positive case find-
ing was higher for HIV-uninfected community members than
for HIV-infected community members (rates, 0.67 [95% con-
fidence interval, 0.25–0.53] and 0.37 [95% confidence interval,
0.41–1.0], respectively) [20].
TB TRANSMISSION PATTERNS
Over a 5-year period from 2001 through 2005, all acid-fast
bacilli–positive sputum samples obtained at the single clinic in
Site-M were cultured, and IS6110-based restriction fragment-
length polymorphism analysis [37] was performed [38]. A
broad diversity of ∼200 distinct circulating M. tuberculosis
strains were estimated to be circulating in this community—a
finding consistent with other studies in sub-Saharan Africa [39,
40]. This study also found an association between W-Beijing
family strains and HIV infection that may reflect ongoing trans-
mission of TB among HIV-infected persons. W-Beijing strains
have been associated with increased virulence [41] and the
development of multidrug resistance [42]. The high degree of
genotypic diversity in certain strains may indicate that they
either are endemic in this population or may be emerging and
diversifying in the community.
Another important finding was the high rate of strain clus-
tering. In this study, approximately half of the strains were
clustered, and there were close temporal associations, especially
among the paired clusters, supporting the likelihood that a
significant proportion of disease in the community is attrib-
utable to recent infections. No association was found between
HIV infection and clustering; therefore, new infections may be
occurring in both HIV-uninfected and HIV-infected patients.
DISCUSSION
This review has focused in detail on a specific, well-demarcated
population that is heavily burdened with the dual epidemics
of HIV infection and TB. Detailed analysis of the HIV and TB
epidemics in this community may reveal insight into the factors
driving the HIV and TB regional emergency in southern Africa.
The incidence of TB has increased logarithmically with growth
of the HIV epidemic and has been associated with a changed
age distribution, resulting in the TB burden transferring from
the elderly to young adults. The HIV epidemic appears to have
unmasked a previously unrecognized high prevalence of TB
and an unprecedented rate of TB in this crowded township.
Modeling studies suggest that a combination of interventions
will be required to regain TB control [12]. The present strategy
for global TB control remains the identification and effective
case management of infectious TB cases [33]. However, al-
though the facility-based program in this community appears
to have achieved standard targets for TB case management for
HIV-uninfected community members, the program has not had
an impact on the extremely high annual risk of TB.
Strategies to decrease progression from prior infection may
include ART and IPT. However, ART will need to be introduced
with high coverage and earlier in the course of HIV infection,
at higher CD4 cell counts, to significantly have an impact on
rates of TB in the population [12]. Although the effect of ART
is greater with continuing length of therapy [34], the benefits
of IPT for HIV-infected patients are time-limited, compared
with those for HIV-uninfected persons [14].
The underlying driver of the explosive HIV and TB coepi-
demic appears to be an extremely high annual risk of TB in
this community. A high annual risk of TB may be the result
of unrecognized infectious cases in the community and intense
social interaction and crowding. New interventions in addition
to the present clinic-based model of TB case management will
be required, with increased emphasis on active community-
based case finding and contact tracing to decrease the infective
TB pool. There is also an urgent need for better understanding
of the transmission dynamics of TB and intensity of social
interactions that have exacerbated the HIV and TB coepidemic
in this community of hyperendemicity.
Acknowledgments
Potential conflicts of interest. L.-G.B. and R.W.: no conflicts.Supplement sponsorship. This article is part of a supplement entitled
“Synergistic Pandemics: Confronting the Global HIV and Tuberculosis Ep-idemics,” which was sponsored by the Center for Global Health Policy, aproject of the Infectious Diseases Society of America and the HIV MedicineAssociation, through a grant from the Bill & Melinda Gates Foundation.
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018

S214 • CID 2010:50 (Suppl 3) • Bekker and Wood
References
1. World Health Organization. Global tuberculosis control 2009. Epide-miology, strategy, financing. Geneva: World Health Organization, 2009.http://www.who.int/tb/publications/global_report/2009/pdf/full_report.pdf. Accessed 25 March 2010.
2. United Nations. The Millenium Development Goals Report 2008. NewYork: United Nations, 2008. http://www.un.org/millenniumgoals/. Ac-cessed 8 June 2009.
3. Frieden TR, Munsiff SS. The DOTS strategy for controlling the globaltuberculosis epidemic. Clin Chest Med 2005;26(2):197–205.
4. De Cock KM, Chaisson RE. Will DOTS do it? A reappraisal of tu-berculosis control in countries with high rates of HIV infection. Int JTuberc Lung Dis 1999;3(6):457–465.
5. Lawn SD, Bekker LG, Middelkoop K, Myer L, Wood R. Impact of HIVinfection on the epidemiology of tuberculosis in a peri-urban com-munity in South Africa: the need for age-specific interventions. ClinInfect Dis 2006;42(7):1040–1047.
6. Styblo K. The impact of HIV infection on the tuberculosis problemworldwide. Kekkaku 1990;65:429–438.
7. Arnadottir T. The Styblo Model 20 years later: what holds true? Int JTuberc Lung Dis 2009;13(6):672–690.
8. World Health Organization. Guidelines for implementing collaborativeTB and HIV programme activities. http://www.who.int/tb/publications/2003/en/index1.html. Accessed 20 February 2008.
9. World Health Organization. Strategic framework to decrease the bur-den of TB/HIV. Geneva: World Health Organization, 2002. http://www.who.int/tb/publications/who_cds_tb_2002_296/en/index.html.Accessed 25 March 2010.
10. World Health Organization. Interim policy on collaborative TB/HIVactivities. Geneva: World Health Organization, 2004.http://whqlibdoc.who.int/hq/2004/WHO_HTM_TB_2004.330_eng.pdf. Accessed 25March 2010.
11. Williams BG, Dye C. Antiretroviral drugs for tuberculosis control inthe era of HIV/AIDS. Science 2003;301:1535–1537.
12. World Health Organization.WHO three I’s meeting. Report of a jointWHO HIV/AIDS and TB Department Meeting. Geneva: World HealthOrganization, 2008. http://www.who.int/hiv/pub/meetingreports/WHO_3Is_meeting_report.pdf. Accessed 25 March 2010.
13. Woldehanna S, Volmink J. Treatment of latent tuberculosis infectionin HIV-infected persons. Cochrane Database Syst Rev 2004;(1):CD000171.
14. Guwatudde D, Debanne SM, Diaz M, King C, Whalen CC. A re-examination of the potential impact of preventive therapy on the publichealth problem of tuberculosis in contemporary sub-Saharan Africa.Prev Med 2004;39:1036–1046.
15. Corbett EL, Churchyard GJ, Clayton TC, et al. HIV infection andsilicosis: the impact of two potent risk factors on the incidence ofmycobacterial disease in South African miners. AIDS 2000;14(17):2759–2768.
16. Kok P, Collinson M. 2006: Migration and urbanization in South Africa.Report 03–04-02, Pretoria: Statistics South Africa. http://www.statssa.gov.za/publications/Report-03-04-02/Report-03-04-02.pdf. Accessed24 June 2009.
17. United Nations Population Fund. State of world population 2007:unleashing the potential of urban growth. http://www.unfpa.org/upload/lib_pub_file/695_filename_sowp2007_eng.pdf. Accessed 24June 2009.
18. UN-Habitat (United Nations Human Settlement Programme). Thestate of African Cities 2008. A framework for addressing urban chal-lenges in Africa. http://www.unhabitat.org/pmss/. Accessed 24 June2009.
19. Cape Town TB Control. Progress Report 1997–2003. http://www.hst.org.za/uploads/files/tb_ct.pdf. 25 June 2009.
20. Wood R, Middelkoop K, Myer L, et al. The burden of undiagnosedtuberculosis in an African community with high HIV-prevalence: im-plications for TB control. Am J Resp Crit Care Med 2007;175(1):87–93.
21. World Health Organization. The Global Plan to Stop TB, 2006–2015Stop TB Partnership. Geneva: World Health Organization, 2006.
22. Badri M, Wilson D, Wood R. Effect of highly active antiretroviraltherapy on incidence of tuberculosis in South Africa: a cohort study.Lancet 2002;359:2059–2064.
23. Lawn SL, Myer L, Edwards D, Wood R. Variation in early and long-term risks of tuberculosis associated with CD4 cell response to anti-retroviral therapy in South Africa. AIDS (Epub ahead of print).
24. Report National HIV and syphilis antenatal sero-prevalence survey inSouth Africa 2005. National Department of Health. http://www.doh.gov.za/docs/reports/2005/hiv.pdf. Accessed 29 July 2009.
25. Middelkoop K, Wood R, Myer L, Bekker L-G. Tuberculin skin testsurvey in a community with high HIV and tuberculosis prevalence.Clin Infect Dis 2008;47(3):349–355.
26. Lawn SD, Bangani N, Vogt M, et al. Utility of interferon-y ELISPOTassay responses in a highly tuberculosis-exposed patients with advancedHIV-infection in South Africa. BMC Infect Dis 2007;7:99.
27. Rangaka MX, Wilkinson KA, Seldon R, et al. Effect of HIV-1 infectionon T-cell based and skin test detection of tuberculosis infection. AmJ Respir Crit Care Med 2007;175(5):514–520.
28. Walgren A. The time-table of tuberculosis. Tubercle 1948;29:245–251.29. Bloch AB, Snider DE. How much tuberculosis in children must we
accept? Am J Public Health 1986;76:14–15.30. Comstock GW, Livesay VT, Woolpert SF. The prognosis of a positive
tuberculin reaction in childhood and adolescence. Am J Epidemiol1974;99:131–138.
31. Grzybowski S, Barnett GD, Styblo K. Contacts of cases of active pul-monary tuberculosis. Bull Int Union Tuberc 1975;50:107–121.
32. Roelsgaard E, Iversen E, Blocher C. Tuberculosis in tropical Africa: anepidemiological study. Bull World Health Organ 1964;30:459–518.
33. Mantoux C. L’intradermo-reaction a la tuberculine et son interpre-tation. Clinique Presse Med 1910;2:10–13.
34. Groth-Petersen E, Knudsen J, Wilbek E. Epidemiological basis of tu-berculosis eradication in an advanced country. Bull World Health Or-gan 1959;21:5–49.
35. Middelkoop K, Bekker L-G, Morrow C, Zwane E,Wood R. Childhoodtuberculosis infection and disease: a spatial and temporal transmissionanalysis in a South African township. S Afr Med J 2009; 99:738–743.
36. The South African Tuberculosis Control Programmed. Practical guide-lines 2000. Department of Health. http://www.doh.gov.za/tb/index.html. Accessed 27 July 2009.
37. van Embden JD, Cave MD, Crawford JT, et al. Strain identification ofMycobacterium tuberculosis by DNA fingerprinting: recommendationsfor a standardized methodology. J Clin Microbiol 1993;31:406–409.
38. Middelkoop K, Bekker L-G, Mathema B, et al. Molecular epidemiologyof Mycobacterium tuberculosis in a South African community with highHIV prevalence. J Infect Dis 2009; 200:1207–1211.
39. van der Spuy GD, Kremer K, Ndabambi SL, et al. Changing Myco-bacterium tuberculosis population highlights clade-specific pathogeniccharacteristics. Tuberculosis (Edinb) 2009;89:120–125.
40. Lockman S, Sheppard JD, Braden CR, et al. Molecular and conventionalepidemiology of Mycobacterium tuberculosis in Botswana: a population-based prospective study of 301 pulmonary tuberculosis patients. J ClinMicrobiol 2001;39:1042–1047.
41. Hanekom M, van der Spuy GD, Streicher E, et al. A recently evolvedsublineage of the Mycobacterium tuberculosis Beijing strain family isassociated with an increased ability to spread and cause disease. J ClinMicrobiol 2007;45:1483–1490.
42. Drobniewski F, Balabanova Y, Nikolayevsky V, et al. Drug-resistanttuberculosis, clinical virulence, and the dominance of the Beijing strainfamily in Russia. JAMA 2005;293:2726–2731.
Downloaded from https://academic.oup.com/cid/article-abstract/50/Supplement_3/S208/319369by gueston 13 February 2018



![Ooo1tuberculosis-Hiv Coinfection Auto Saved]](https://static.fdocuments.net/doc/165x107/577d281e1a28ab4e1ea53909/ooo1tuberculosis-hiv-coinfection-auto-saved.jpg)