
The Challenge of Consolation: A qualitative study of ... · Kirsten Tornøe The Challenge of...
117
Kirsten Tornøe The Challenge of Consolation: A qualitative study of nurses’ experiences with practicing and teaching spiritual and existential care for the dying PhD Thesis MF Norwegian School of Theology Oslo 2017
Transcript of The Challenge of Consolation: A qualitative study of ... · Kirsten Tornøe The Challenge of...

KirstenTornøe
TheChallengeofConsolation:
Aqualitativestudyofnurses’experienceswithpracticingand
teachingspiritualandexistentialcareforthedying
PhDThesis
MFNorwegianSchoolofTheology
Oslo2017

“Itisinthefearfulmomentsofdesolationwherethereisnomeaningleftthatabravestatementofconsolationpenetratesthedarknessandcreatesnewmeaning.Thishappensontheborderwherenothingispossibleanymore.”(Kierkegaard,citedinNorberg,BergstenandLundman,2001p.545)

I
Contents1.Acknowledgments....................................................................................................................III2.Abstract.........................................................................................................................................V3.Listoforiginalpapers............................................................................................................VII4.Introduction..................................................................................................................................14.1Background..........................................................................................................................................14.1.1Conceptualclarifications............................................................................................................................4
4.2Spiritualandexistentialcare:Thestudy’stheoreticalposition........................................54.3Whyresearchlivedexperience?.................................................................................................10
5.Theaimofthestudy................................................................................................................115.1Thespecificaims..............................................................................................................................115.2Theresearchquestions.................................................................................................................11
6.MethodologicalFrameworkPhenomenologicalHermeneutics..............................126.1EdmundHusserl...............................................................................................................................136.2MartinHeidegger.............................................................................................................................156.3Hans-GeorgGadamer.....................................................................................................................176.4PaulRicoeur......................................................................................................................................206.4.1Textunderstoodashumanaction.......................................................................................................216.4.2Distanciationandappropriation..........................................................................................................216.4.3Explanationandunderstanding...........................................................................................................226.4.4Guessingandvalidation...........................................................................................................................22
7.Themethods..............................................................................................................................247.1Datacollection:Narrativeinterviews.......................................................................................247.1.1Thenarrativefocusgroupinterview..................................................................................................26
7.2Dataanalysis:Interpretingtheinterviewtexts.....................................................................267.2.1Thenaïvereading.......................................................................................................................................277.2.2Thestructuralanalysis.............................................................................................................................277.2.3Comprehensiveunderstanding(Interpretedwhole)..................................................................28
7.3Methodologicalconsiderations...................................................................................................297.3.1Thetrustworthinessofthedatacollection......................................................................................307.3.2Thetrustworthinessofthedataanalysis.........................................................................................327.3.3Rationaleforconductingaphenomenologicalhermeneuticaldataanalysis...................347.3.4Mypreunderstanding................................................................................................................................367.3.5Studylimitations.........................................................................................................................................37
8.Thestudy....................................................................................................................................398.1Thesetting..........................................................................................................................................408.2Recruitmentstrategy......................................................................................................................418.3Thesample.........................................................................................................................................418.4Conductingtheinterviews............................................................................................................428.5Ethicalconsiderations....................................................................................................................43
9.MainresultsinPapersI-III...................................................................................................459.1PaperI.................................................................................................................................................459.2PaperII................................................................................................................................................469.3PaperIII..............................................................................................................................................47
10.Discussion................................................................................................................................4810.1Conveyingconsolation.................................................................................................................48

II
10.1.1Thehermeneuticsofconsolation......................................................................................................5010.1.2Therelationaldimensioninthenurses’consolationnarratives.........................................5210.1.3ConveyingconsolationinrelationtoSpiritual/ExistentialandPsychosocialcare....5510.1.4ConsolationthroughExistentialmeaningmaking.....................................................................5710.1.5ThePowerofConsolingpresence.....................................................................................................6010.1.6Consolationunderstoodasamoralresponsibility....................................................................61
10.2Vulnerabilityandhelplessness................................................................................................6810.2.1Vulnerabilityandembodiedengagement.....................................................................................7010.2.2Compassionfatigue.................................................................................................................................7210.2.3Compassionsatisfaction........................................................................................................................75
10.3CompassionandCourage...........................................................................................................7610.3.1Compassion.................................................................................................................................................7610.3.2Courage.........................................................................................................................................................78
10.4Cancourageandcompassionbetaught?..............................................................................8010.4.1Cancompassionbetaught?..................................................................................................................8110.4.2Cancouragebetaught?..........................................................................................................................84
10.5Pedagogicalimplications............................................................................................................8810.5.1Recommendations...................................................................................................................................91
11.Concludingremarks.............................................................................................................94References......................................................................................................................................95PaperI-III......................................................................................................................................107Appendix.......................................................................................................................................108

III
1.AcknowledgmentsLøgstrup(1997)notesthatwhileeverypersonisanindependentandresponsible
individual,healsopointsoutthatweareinescapablydependentuponeachother,and
thatwebelongtoaworldinwhichweholdsomethingofoneanother’slifeinourhands.
Accordingly,althoughaPhDthesisisanindependentpieceofresearch,itwouldnot
havebeenpossiblewithoutthecontributions,supportandencouragementfrommany
others,forwhichIamextremelygrateful.
Firstly,Iwishtoexpressmygratitudetothenurseswhoparticipatedinthestudy.
Thankyoufortrustingmeandforsharingyourspiritualandexistentialcarestories
whichreverberatewithcourage,compassionandconsolation.
Secondly,IwishtothankmysupervisorsProfessorLarsJohanDanbolt,Professor
VenkeSørlieandProfessorKariKvigne.
IamespeciallygratefultoVenkeSørlieandLarsJohanDanboltwhohelpedmepursue
mydreamofwritingthisPhDthesis.LarsJohanDanbolthasbeenmymainsupervisor.
ThankyouforsharingyourinvaluableinsightsinthefieldofPsychologyofReligionand
forhelpingmetoobtainfundingfromTheInnlandethospitaltrust.Youreffervescent
spiritandoptimisticfaithinmyprojecthasbeencontagious,upliftingandinspiring,
throughouttheentireresearchprocess.
Manythankstomyco-supervisorandcolleagueatLovisenbergDiaconalUniversity
CollegeVenkeSørlie.Venkehasaccompaniedandsupportedmeallthewayfrommy
firsttentativeresearchproposalstillthecompletionofthisthesis.Thankyouforyour
invaluableadviceandguidanceonstudydesign,phenomenologicalhermeneuticaldata
analysis,relationalethicsandforshowingme“theropes”onarticlepublishing.
Manythankstomyco-supervisorKariKvigne,whojoinedthesupervisionteamwhen
weanalyzedthedatafromthefirststudy.Thankyouforyourcontributionstointerpret
theresultsandforcriticalreviewofthemanuscripts.Thankyouforinitiatingthecourse
inphenomenologicalhermeneuticalanalysisatHedmarkUniversityCollege,andfor
givingmetheopportunitytoparticipate.Thankyoualsoforyourwarmhospitality.

IV
SpecialthankstoProfessorValerieDeMariniswhocriticallyexaminedandevaluatedmy
thesisatthefinalPhDseminarinOctober2015.
Ihavebeenfortunatetoparticipateinmonthlymeetingswiththepsychologyofreligion
PhDgroupatMFSchoolofTheology,ledbyProfessorLarsJohanDanbolt.Thisgroup
hasbeenanimportantandinspiringmeetingplace.Thankyoutomyresearchfellows
Torgeir,Liv,SigridHelene,Tor,Hege,Anneandtherestofthegroup.
Iamgratefultomyemployer,LovisenbergDiaconalUniversityCollegeandtothe
InnlandetHospitalTrustforfinancialsupport,whichgavemetheopportunitytopursue
myresearchinafulltimepositionforthreeyears.
AwarmthankyoutomycolleaguesatLovisenbergDiaconalUniversityCollegewho
haveencouragedandcheeredmeonthroughthewritingprocess,andtoourexcellent
libraryandcomputerstaff.
Spendinggruelinglonghourswriting,makesonesusceptibletotheperilsofrepetitive
stressinjuries.IamthereforegratefultomyAlexanderteacherNigelHornbyandthe
Alexandertechnique(Cranz,2000;Hollinghurstetal.,2008)whichhasenabledmeto
improvemyposturalalignmentandtoreleasemusculartensionwhilstworkingatthe
computer.
Lastbutnotleast,Iamthankfulforthesupport,loveandencouragementfrommy
familyandfriends,especiallyRigmor,BørreandAnneBerit,whohadfaithinmyPhD
questthroughoutthemanyyearsof“knockingondoors”,huntingforresearchgrants
andwritingresearchproposalsuntilmywindowofopportunityfinallyflungopen!
(ThankyouLarsandVenke!)
IamespeciallygratefultomymotherJudithTornøe,forproofreadingallthreearticles
andtheentirethesis.
Oslo,December2016

V
2.Abstract
Background:Inwesterncountriesanincreasingproportionofolderpatientswith
incurablecancerorotherchronicconditionswillrequirepalliativecare.Respondingto
thefiscalpressureintheNorwegianhealthcaresystemtheNorwegiangovernment
implementedamajorhealthcarereformin2012.This“CoordinationReform”downsized
specializedhealthcareunitsinthesecondaryhealthcaresectorandtransferredmore
palliativecareresponsibilitiestonursinghomesandhomecarenursingintheprimary
healthcaresector,whichoftenlackadequatenursingexpertise.Asaconsequence,less
qualifiedcareworkersaswellasregisterednursesincreasinglyhavetoprovide
palliativecare,whichincludestheimpeccableassessmentandtreatmentofphysical,
psychosocial,spiritualandexistentialpain.However,researchshowsthatspiritualand
existentialcareforthedyingisfrequentlyoverlookedinmostcaresettingsandthat
nursesandothercareworkersoftenfeelanxiousanduncertainaboutproviding
spiritualandexistentialcarefordyingpatients.Thisindicatesthatthereisawidespread
needforspiritualandexistentialcarecompetencyinpalliativecare.Thereisagapinthe
literatureabouthownursesmayalleviatedyingpatients’spiritualandexistential
sufferingintheireverydaypractice.Thereisalsoagapintheliteratureabouthowto
trainnursingstafftoprovidespiritualandexistentialcareforthedying.
Aim:TheoverallaimofthisPhDthesisistoilluminatethemeaningofregisterednurses’
experienceswithpracticingandteachingspiritualandexistentialcareforthedyingin
differentNorwegianhealthcarecontexts.TheaimsinstudiesI,IIandIIIwere:
I: Todescribethemeaningofhospicenurses’livedexperiencewithalleviatingdyingpatients’spiritualandexistentialsuffering
II: Todescriberegisterednurses’experienceswithspiritualandexistentialcarefordyingpatientsinageneralhospital
III: ToilluminateapioneeringNorwegianmobilehospicenurseteachingteam’sexperiencewithteachingandtrainingcareworkersinspiritualandexistentialcareforthedyinginnursinghomesandhomecaresettings
Methodsanddesign:Thisisaqualitativestudy.StudyIwasbasedoneightindividual
narrativeinterviewswithhospicenurses.StudyIIwasbasedonsixindividualnarrative
VI
interviewswithregisterednursesinamedical-oncologicalwardinageneralhospital.
StudyIIIwasbasedonanarrativefocusgroupinterviewwiththethreehospicenurses
inthemobileteachingteam.Aphenomenologicalhermeneuticalmethodwasusedto
analyzetheinterviewtexts.
Mainresults:Spiritualandexistentialcarewasaboutconsolingthedyingby
unburdeningthemandfacilitatingapeacefuldeath.Thenursesconveyedconsolationby
helpingtheirpatientstosettlepracticalissues,reconcilethemselveswiththeirloved
onesandtofindpeacewithGod,andbysimplybeingpresentwiththeirpatientsto
sharethesuffering.Conveyingconsolationprovedtobeadeeplyrelationalpractice,
whichdemandedcourageandcompassionbecauseitexposedthenursestotheirown
vulnerability,mortalityandhelplessness.Practicaltrainingprogramsproviding
experientiallearningopportunitiesthroughsituatedbedsideteachingmaybeefficient
todevelopcareworkers’courageandcompetencytoprovidespiritualandexistential
careforthedying.However,theresultssuggestthatsuchprogramsshouldalso
introducenursingstafftoreligiousperspectivesonsufferingandreligiousreasoning,
becausetheresultsshowthatthenursesexpresseduncertaintyaboutaddressing
patients’religiousneedsduetoalackofformalknowledge.
Conclusions:Whennothingelsecanbedone,bearingwitnessandsharingthepatients’
sufferingmaybeconsolingactsinthemselves.Nursesandcareworkersinend-of-life
careconfrontintractablesuffering.Hence,theycannotalwaysexpecttobesuccessfulin
theireffortstoalleviateit.Therefore,thestudyresults,whichindicatethatconsolation
maybeconveyedandsustainedthroughpresenceandrelatedness,areextremely
important.Alessqualifiedworkforceincreasinglydominatesnursinghomesand
homecarenursingatatimeofincreasingprevalenceofcomplexhealthconcerns.Mobile
expertnurseteachingteamsinspiritualandexistentialcare,(andothernursingfields)
maybeaneffectivemeanstoredressthewideninggapbetweenworkforcequalityand
thedemandforhighqualitycareintheprimaryhealthsector.
Keywords:consolation,spiritualandexistentialcare,palliativecare,healthcarereform,
phenomenologicalhermeneuticalmethod,narrativeinterviews,primaryandsecondary
healthcaresector

VII
3.ListoforiginalpapersThethesisisbasedonthefollowingpapers,whichwillbereferredtointhetextbytheir
romannumerals:
I.Tornøe,K.A.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2014).Thepowerofconsoling
presence-hospicenurses'livedexperiencewithspiritualandexistentialcareforthedying.BMCNursing,13(1),25.
II.Tornøe,K.A.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2015).Thechallengeof
consolation:nurses’experienceswithspiritualandexistentialcareforthedying-aphenomenologicalhermeneuticalstudy.BMCNursing,14(1),62.
III.Tornøe,K.,Danbolt,L.J.,Kvigne,K.,&Sørlie,V.(2015).Amobilehospicenurse
teachingteam’sexperience:trainingcareworkersinspiritualandexistentialcareforthedying-aqualitativestudy.BMCPalliativeCare,14(1),43.

1
4.IntroductionTheoverallaimofthisPhDthesisistoilluminatethemeaningofregistered
nurses’experienceswithpracticingandteachingspiritualandexistentialcarefor
thedyingindifferentNorwegianhealthcarecontexts.
4.1BackgroundInwesterncountriesanincreasingproportionofpatientsareolderpeoplelivingwith
incurablecancerorotherchronicconditionsthatwillrequirepalliativecareforshorter
orlongerperiodsoftime(Haug,Danbolt,Kvigne,&Demarinis,2014,p.68;Norwegian
DirectorateofHealth,2015;Seale,1999).TheevidenceondeathanddyinginWestern
EuropeandtheUSAsuggeststhatamajorityofpeopledieinhospitals(Costello,2006).
Inlinewiththistrend,Norwegianpalliativecarehasundergonequitedramaticchanges
duringthelastthirty-fiveyears.Movingfromitsidealisticandsocialhospiceorigins,
Norwegianpalliativecarehasbeenintegratedinthepublichealthcaresystemwhichis
wellorganizedwithintwomainsectors:theprimaryhealthandlong-termcaresector
(nursinghomesandhomecarenursing),andthesecondaryhealthcaresector,involving
hospitalandspecialistservices(Romoren,Torjesen,&Landmark,2011).Specialist
palliativecareservices,includinghospices,areorganizedwithinthelevelofsecondary
healthcareinsomatichospitals(Bollig,Rosland,&Husby,2013;Haugetal.,2014;
NorwegianDirectorateofHealth,2015;Strømskag,2012).
However,theNorwegianhealthcaresystemisstrainingunderfiscalpressure,following
theinternationaltrendofcuttinghealthcarecostsanddownsizingspecializedhospital
unitsinsecondaryhealthcare(EuclidNetwork,2012;NorwegianMinistryofHealthand
CareServices,2012;WorldHealthOrganization,2002).Respondingtotheeconomic
challengesinthehealthcaresystem,theNorwegiangovernmentimplementedamajor
healthcarereformin2012:“TheCoordinationreform”(NorwegianMinistryofHealth
andCareServices,2012).Theaimwastoalleviatepressureonthesecondaryhealth
caresectorbyupgradingtheprimaryhealthcaresectorandbytransferringmore
palliativecareresponsibilitiestonursinghomesandhomecarenursing(Bolligetal.,
2013;NorwegianMinistryofHealthandCareServices,2012).Henceforth,nursing

2
homesandhomecaresettingsarebecomingthehospicesofthefuture(Abbey,Froggatt,
Parker,&Abbey,2006).Asaconsequence,lessqualifiedcareworkers(suchas
unregulatednursingassistants)aswellasregisterednurseswillincreasinglyhaveto
providepalliativecareinnursinghomesandhomecarenursing(Annear,Lea,&
Robinson,2014;Colombo,Llena-Nozal,Mercier,&Tjadens,2011;Leclercetal.,2014).
InNorwaynearly50%ofthedyingareresidentsinnursinghomes,withunderpowered
budgetsandoftenlackingadequateexpertise(Bolligetal.,2013).
TheWorldHealthOrganization(WorldHealthOrganization,2002)maintainsthat
palliativecareincludestheimpeccableassessmentandtreatmentofphysical,
psychosocialandspiritualpain.Agrowingbodyofinternationalpalliativecareresearch
indicatesthatspiritualandexistentialcareisanintegralcomponentofholistic,
compassionatecareforthedying(Bachner,O'Rourke,&Carmel,2011;Nolan,2011;
Steinhauseretal.,2000).Oneofthekeygoalsofpalliativecareistoalleviatedying
patients’suffering(Delgado-Guayetal.,2011).EricCassel(1991a)statesthatalthough
sufferingoftenisrelatedtoacutepainorotherbodilysymptoms,itextendsbeyondthe
physical.“Mostgenerally,sufferingcanbedefinedasthestateofseveredistress
associatedwitheventsthatthreatentheintactnessofperson”(Cassell,1991a,p.33).
Dyingpatientsliterallyexperienceathreattotheir“intactnessofperson”,andassuch
arepronetoexperiencesuffering.Existentialandspiritualsufferingareamongthemost
debilitatingconditionsindyingpatients.Henceforth,thereisagreatneedforpalliative
spiritualandexistentialcarecompetencyintheprimaryaswellasthesecondarylevels
oftheNorwegianhealthcaresector(Boston,Bruce,&Schreiber,2011).
Yet,researchrevealsthatspiritualandexistentialcareisfrequentlyoverlookedin
palliativecare.Thereisagrowingawarenessthatmostcaresettingsfailtoprovide
optimalspiritualcaretothosewithseriousillnessandthoseattheendoflife(Puchalski
etal.,2009).Patientswithadvancedillnessesreportthattheirmedicalcaregivers
infrequentlyprovidespiritualcare(Balbonietal.,2013;Sæteren,Lindström,&Nåden,
2011).AccordingtoUdo(2014)severalstudiesrevealthatmanypatientsare
dissatisfiedwiththeemotionalandexistentialsupporttheyaregiven,eveniftheyare
satisfiedwiththeirmedicalandphysicalcare.ThisissupportedbyGroenvold,Pedersen,
Jensen,Faber,andJohnsen(2006)whofoundthatasignificantnumberofdyingpatients

3
longforadequatespiritualorexistentialcareandcounseling.Inspiteofthis,seriouslyill
patientsoftenrefrainfromdiscussingtheirspiritualandexistentialthoughtswith
nursesbecausetheydonotfeelthatnursesacknowledgethisneed(Udo,2014).
Researchshowsthatregisterednursesandcareworkersoftenfeelinadequately
preparedtoprovidespiritualandexistentialcareforthedying,andthatthismakes
themanxiousanduncertain(Christensen,2008;McSherry&Jamieson,2013;Noble&
Jones,2010;Pesut,Fowler,Taylor,Reimer-Kirkham,&Sawatzky,2008;Udo,2014).
Severalstudiesindicatethatalackofskillsinpsychosocialandspiritualcaremayresult
inhighlevelsofmoraldistress,griefandburnout(Back,Bauer-Wu,Rushton,&Halifax,
2009;Bosma,Apland,&Kazanjian,2010;Noble&Jones,2010;Rushtonetal.,2009;
Vivat,2008).Studiesalsoindicatethatthereisawidespreadneedfortraininginall
aspectsofspiritualandexistentialcareforthedying(Balbonietal.,2013;Holloway,
Adamson,McSherry,&Swinton,2011).Accordingtotheliterature,nurses’andcare
workers’discomfortrelatedtoprovidingspiritualandexistentialcareforthedyingmay
leadtounmetspiritualandexistentialneedspossiblyleadingtoincreasedpatient
suffering(Backetal.,2009;Bosmaetal.,2010;Noble&Jones,2010;Rushtonetal.,
2009;Vivat,2008).
Thereisagapintheresearchliteratureabouthowpatients’existentialwellbeingmay
bebestsupportedbynursesandotherhealthcareprovidersineverydaypractice
(Henoch&Danielson,2009).In2014Pesutetal.conductedascopingreviewto
summarizetheavailableevidenceconcerningpalliativecareeducationfornursesand
othernursingcareproviders(Pesutetal.,2014).Noneofthereferencesintheirreview
explicitlymentionedtrainingcareworkersinspiritualandexistentialcareforthedying.
Thissuggeststhatthereisagapintheliteratureconcerningthisissue.Thisthesis,which
isanempiricalstudyofregisterednurses’experienceswithpracticingandteaching
spiritualandexistentialcareforthedying,willhopefullycontributetobridgethese
importantgaps.
NursingresearchinspiritualcarehasuntilrecentlybeendominatedbyAnglo-American
studies.Althoughthisresearchyieldsvaluableinsights,itcannotbedirectlyappliedto
Scandinaviancontexts,duetothedifferencesinspiritualandreligiousclimatesinthese
societies(Lundmark,2006).OnthegroundsofdifferentsurveysSørensen(2012)notes

4
thatreligionisamorepervasiveanddiversephenomenonintheUSA,thaninthe
Scandinaviancountrieswherelargenumbersofthepopulationbelongtothe
protestant/Lutheranmajoritychurches.(Sørensen,2012),InNorwayapproximately73
%ofthepopulationbelongtotheChurchofNorway(StatistiskSentralbyrå(Central
BureauofStatisticsinNorway),2015).However,inspiteofthelargechurch
membership,Scandinaviansocietiesarequitesecularizedandreligiousandspiritual
thoughtsandpracticesarelargelyregardedasprivatematters.However,thisdoesnot
meanthatthemajorityhasturnedawayorishostiletoreligion(DeMarinis,2008;la
Cour,2008;laCour&Hvidt,2010).Althoughtheinterestintraditionalreligionis
declining,Norwayisgraduallybecomingamoremulticulturalandreligiouslydiverse
society(Ulland&DeMarinis,2014),andagrowingnumberofScandinaviansconsider
themselvestobe“spiritualbutnotreligious”.Dismissingdogmatictruths,their
religiosityandreligiousparticipationismainlyrootedinemotionsandhuman
experience,asameanstosearchforandexpress“authenticself-hood”(Botvar&
Schmidt,2010;DeMarinis,2008).Thisformforspiritualityor“worldviewconstruction”
isrelatedto“existentialmeaningmaking”,whichmayormaynotincludeatranscendent
dimension(DeMarinis,2008;Schnell,2009,2010;Schnell&Keenan,2011).
Despitethe“privatizedattitudes”towardsreligionandspiritualityintheScandinavian
countries,recentyearshaveyieldedagrowingnumberofScandinaviannursingstudies
inspiritualandexistentialcare(Ilkjær,2012;Sæterenetal.,2011;Torskenæs&Kalfoss,
2013;Torskenæs,Kalfoss,&Sæteren,2015;Ødbehr,2015)whichdrawontheemerging
bodyofresearchwithinthefieldofpsychologyofreligion,spiritualityandhealth(Haug,
2015;Koenig,King,&Carson,2012;Masters&Hooker,2013;Sørensen,2012;Sørensen,
Lien,Landheim,&Danbolt,2015).ThisPhD.thesisistobeviewedasaNorwegian
contributiontotheemergingfieldofScandinaviannursingresearchinspiritualand
existentialcare.
4.1.1ConceptualclarificationsSpiritualityisaninternationaltermwhichisusedbynurseacademics(Narayanasamy,
2014;Paley,2008;Pesut,2008b;Swinton&Pattison,2010)aswellasbyacademicsin
otherfieldssuchaspracticaltheology(Bueckert&Schipani,2006;Swinton&Mowat,

5
2006)andinpsychologyofreligion(Koenigetal.,2012;Paloutzian&Park,2013).
However,NorthernEuropeanandScandinaviancontextstendtobemorefamiliarwith
termssuchasviewoflife,worldview,religion,meaning-making,existentialityand
existentialquestions(Stifoss-Hanssen,1999;Stifoss-Hanssen&Kallenberg,1998;Ulland
&DeMarinis,2014).(SeeforexampleKarlsson,Friberg,WallengrenandÖhlén’s(2014)
andStrang,Henoch,Danielson,BrowallandMelin-Johansson’s(2014)Swedishstudies
aboutdyingpatients’existentialissues.)Accordingly,“itisnottobeassumedthat
Norwegiansusethetermspiritualityinclinicalpractice”(Ulland&DeMarinis,2014,p.
4).Takingthisintoaccount,thenursesinthisstudywereaskedtonarrateabouttheir
experienceswithpracticingandteachingspiritualandexistentialcareinorderto
captureasmuchin-depthdataaspossible.InlightofUllandandDeMarinis(2014)itis
interestingtonotethatthenursesdidnotdiscernbetweenspiritualandexistentialcare
duringtheinterviews.Consideringthenurses’useoftheterms,andthefactthatthese
termsoftenareusedsynonymouslyinthenursingliterature,(Bostonetal.,2011;
Boston&Mount,2006;Henoch&Danielson,2009)theterm“spiritualandexistential
care”willbeusedthroughoutthisthesis.However,itisimportanttonotethattheuseof
thesetermsvaryintheliterature,whichiscited.Forthesakeofacademicrigourthe
researchers’useofthetermswillbequoted.(SwintonandPattison(2010)forinstance
useonlytheterms“spirituality”,and“spiritualcare”.)
4.2Spiritualandexistentialcare:Thestudy’stheoreticalposition
Spiritualityisahighlydebatedconceptduetothemanyvariationswhichemergefrom
thenursingliterature(Paley,2008;Pesut,2008a).Severalresearcherspointoutthat
sincethereseemstobenosingleagreeddefinitioninthenursingliterature,theterm”
spiritualcare”isopentointerpretation(Kalish,2012;Noble&Jones,2010;Pesutetal.,
2008;Reimer-Kirkham,2009;Swinton&Pattison,2010).Itisthereforeimportantto
clarifythisstudy’stheoreticalstandpoint.
Mypreunderstandingofspiritualandexistentialcareisshapedbyseveralyearsof
experienceasaregisterednurse,caringfordyingpatientsincancerwardsandnursing
homes,mybackgroundasanordaineddeaconintheNorwegianLutheranChurch,a

6
master’sdegreeintheology,(withathesisonspiritualandexistentialend-of-lifecare
basedonnarrativetheology)andmybookaboutspiritualandexistentialcareforthe
dying,basedonmymaster’sthesis(Tornøe,1996).Asanurseeducatorandresearcher,
IfindthatSwintonandPattison’s(2010)pragmaticandfunctionalunderstandingof
spiritualityinnursingcareresonateswithmyownviewpointswhichhaveevolved
throughmyownspiritualandexistentialcareexperiencesinend-of-lifecareandmy
educationalbackground.Ihavethereforechosentogroundthisstudyintheir
understandingofspiritualitybecauseitfitsthestudy’saimwhichistoilluminatethe
meaningofregisterednurses’experienceswithpracticingandteachingspiritualand
existentialcare,ratherthanclarifyingtheontologicalandconceptualquestionsabout
howtodefinespiritualandexistentialcareintheresearchliterature(Reimer-Kirkham,
2009).Thiswillbeelaboratedinthefollowing:
WhilePaley(2008)arguesthatthewiderangeofspiritualitydefinitionsrendersthe
conceptmeaninglessandinsignificant,SwintonandPattison(2010)claimthatthe
concept’sstrengthlaysinitsvagueness,andthatitcannotbedismissedjustbecauseit
doesnotfitwithastrictempiricistviewofreality.Whilehardpositivistsmayarguethat
conceptsinlanguagewhichdonotcorrespondwitheventsorthingsinthematerial
worldshouldnotbeattendedto,SwintonandPattison(2010)statethatnotallconcepts
aresimplyreferentialandtheystillaccordvaluewithinthesocialworld.Drawingon
Wittgenstein,they(2010)pointoutthatwordsareperformativeandexpressiveaswell
asreferential.Accordingly,wordsarenotessentialistintheirmeaning.Ratherthan
deliberatingoverthelexicographicalmeaningsofspirituality,theyadvocatethatitis
moreusefultodevelop“athin,vagueandfunctionalunderstandingofwhatthisword
anditscognatesmightdointheworldofhealthcare”.(Swinton&Pattison,2010,p.227)
Henceforth,theymakeitclearthatdefiningspiritualityforhealthcarepurposesisnot
thesameasclaiminganydirectontologicalstatus(Swinton&Pattison,2010).
AccordingtoSwinton(2014),anydefinitionofspiritualityinhealthcareisapragmatic,
ratherthananontologicdescription,whichmeansthatthefocusisonwhattheconcept
“does”(intermsofitseffectonhealthcarepractice),ratherthanwhatit“is”(intermsof
essentialdefinitions).Thisisillustratedinfigure1.

7
Figure1:SpiritualityinNursing:Twomajortheoreticalpositions(Swinton,2014;Swinton&Pattison,2010)
SwintonandPattison(2010)arguethatspirituality,likeanyotherconcepthasalways
beenandinevitablywillbeasocialconstruction.Butthatisnottosaythatitisnothing
butasocialconstruct.Whilespiritualitymaywellhaveanontologyitisclearthatithas
beeninterpretedinvariouswaysandthatthecontextswheretheseinterpretative
actionstakeplacearesignificant.SwintonandPattison(2010)pointoutthatspirituality
isconstructedindifferentwaysbyvariousreligioustraditions,spiritualmovements,
beliefsystems,culturesandcontext,andnotleastbyparticularindividualsinspecific
circumstances.Accordingly,themeaningofspiritualityisnecessarilyemergentand
dialectical;itisshapedandformedbythecontextwithinwhichspirituallanguageis
expressed(Swinton&Pattison,2010).Sincelife,deathandillnessismessyandchaotic,
itisunreasonabletoexpectthatpracticesandconceptsassociatedwiththeemergent
termofspiritualitywillbeconsistent,coherentanduniversallyvalid.Rather,thevalue
ofthelanguagesthatdeployspiritualityanditspracticalandtheoreticalvalueslayin
theircontingent,evolutionaryandcontextualusage(Swinton&Pattison,2010).
Furthermore,SwintonandPattison(2010)notethatmanyofthekeytermsthatare
usedwithinhealthcare(includinghealthcareitself!)aresimilarlyemergent,
Pragmaticandfunctionalistdefintion:
Ontologicaldefinition"Theessenceofspirituality"
Focuson
whatitdoesFocuson
Whatitmeans
Spirituality

8
constructedandchanging.Theterms“community”,“care”,“love”and“friendship”for
instance,areequallyvague,contestedandmulti-orpolyvalent,asspiritualitybut
nonethelessimportantandnecessary.Thus,thereisnoinherentreasonwhyalackof
clarityshoulddenotealackofsignificance.Rather,multipledefinitionsmaybe
indicativeofthenecessityandtheflexibilityofthetermtomeetparticularneedsthat
wouldotherwisegounmet(Swinton&Pattison,2010).AsSwinton(2014,p.163)points
out:“Spiritualityisunabashedlyafluidanddeeplypragmaticconceptthatshiftsand
changesaccordingtothecontextwithwhichitisconstructedandtheneedsitis
attemptingtomeet.”
AccordingtoSwintonandPattison(2010),inawesternsecularizedhealthcaresystem
anemphasisonspiritualityattemptstocapturesomethingofthephenomenologyof
illness(thelivedexperienceofbeingill)whichhasbeenunderplayedbyhighly
medicalizedmodesofhealthcarestrategyanddelivery.Spiritualityinahighly
secularizedhealthcarecontextseekstorecapturethosedimensionsofthehuman
personthatwereonceexpressedinreligiouslanguageandthatarenotcaptured
effectivelybybiomedicaldiscourse,suchas“theimportanceofmeaning,purpose,hope,
love,Godandrelatedness”(Swinton&Pattison,2010,p.232).SwintonandPattison
(2010)pointoutthatsuchissuesoftencometovitalprominenceduringtheexperience
ofbeingill.Accordingtothem(2010),spiritualcarecannotbeunderstoodasasingle
task,orevenadiscreteseriesoftasks.Rather,itdenotesthemultifarious,disparateand
pluriformskillsandperspectivesthatnursesandcareworkersneedtolearninorderto
caterwellforcertainaspectsoftheexperienceofillnessasitislivedoutwithin
particularhealthcarecontexts.
SwintonandPattison(2010)notethatthetermspiritualityandthediscoursethat
surroundsit,canatitsbest,functionasasensitizingconceptthatdrawsourattentionto
suchissuesasmeaning,purpose,relationality,hope,value,love,Godandtranscendence,
areas,whichwellmaybeoverlookedinhealthcare,withoutthissensitizingfunction.
Accordingtothem(2010),spiritualityisnotperceivableasasinglething,butratherasa
responsetoavarietyofhumanquests,whichoftenareactivatedintimesofillnessand
duress.Thus,ifoneaspectoffunctionalspiritualityisthehumansearchformeaning,
thencarerswillneedtodevelopapproachesandmethodswhichenablethemtodeal

9
withtheexistentialquestsofpeopleintimesofillness.Ifspiritualitydenotesaquestfor
hope,thedesireforrelationshipsortheconstructionofpurpose,variousapproaches
andtechniqueswillberequiredtoenablenursestocarewellforthisaspectofpeople’s
livedexperienceofillness.IfspiritualityisasearchforGodandthetranscendent,then
facilitatingthatquestrequiresaparticularsetofskillsandknowledgeofreligious
traditions,theology,religiouspracticesoratleastanabilitytorecognizetheneedandto
refertoappropriatepersons(Swinton&Pattison,2010).
Forthepurposeofthisstudy,SwintonandPattison’s(2010,p.229)threemost
importantpointsare:
1. Intimesofillness,whatmightlooselybecalledspiritual,meaning,identityand
purposeissuesmaycometothefore,evenwhenreligionandspiritualityformally
definedhavenotpreviouslybeenofsignificanceforthepatient.“Itisinsuch
situationsinthe‘everydayness’oftheirlivesthatpeoplearemostlikelytothink
about‘spiritual’issuesortohave‘spiritualneeds’howeverinchoateorill-
articulated”.(Swinton&Pattison,2010,p.229)
2. Itseemstobethecasethatordinarypeople,patients,carersandprofessional
healthcareworkersseemtofindthelanguageofspiritualitytobefunctional,helpful
andmeaningfulespeciallyduringtimesofillnessandduress(WHO,1998),despite
thelackofcleardefinitionsofwhatspiritualitymightmeaninreferentialterms.
Thereisevidencetosuggestthatthevoices,habitsandperceptionsofordinary
peopleshouldbecloselyattendedtoinanyaspectofhealthcare,andespecially
whenitappearstorelatecloselytoissuesofpurpose,identityandtheself,asthe
languageofspiritualityoftendoes.
3. Ifillpeopleandtheircarersareusingtheconceptofspirituality-“andusingitwith
earnestnessandseriousintent,primafacie,theirviewsshouldbetakenseriouslyby
academicsandhealthcareproviders”.(Swinton&Pattison,2010,p.229)(However,
asnotedinsection4.1.1,itisimportanttobeawarethatinNorthernEuropeanand
Scandinaviancontexts,patientsandnursestendtobemorefamiliarwithtermssuch
10
asviewoflife,worldview,religion,meaning-making,existentialityandexistential
questions.)
InlinewithSwintonandPattison(2010),theobjectiveofthisstudyisnottoquestion
thevalidityofthenurses’languageordefinitionsofspiritualitybuttolistentothemin
ordertoexplorethemeaningoftheirlivedexperienceswithpracticingandteaching
spiritualandexistentialcare.
4.3Whyresearchlivedexperience?Overmanyyearsthescientificmethodhasbecomethemostimportantmeansof
generatingevidenceabouttheworldandhumansociety,andconsiderableefforthas
beendevotedtoimplementevidencebasedpracticeinnursing(EBP)(Avis&
Freshwater,2006).However,Benner(2000a),drawingonMerlau-Ponty(1962)points
outthatscientificlanguagewhichomitsourembodiedexperienceofillness,recovery
andhealthalsoleavesoutperceptualcapacitiesthatenablereasoningandactingas
moralagentsinparticularlifeworlds.SolvollandLindseth(2015)notethat
phenomenologicallyspeaking,weunderstand”experiences”asaseriesofsignificant
eventsthatconstitutetheworldandabodilyself.Thebodyandawarenessfindtheir
placesinthisflowratherthanprecedingit.AccordingtoSolvollandLindseth(2015)
practitioners’professionalknowledgecanbe“observed”throughtheirnarrativesabout
theirexperiences.Whileeachnarrativeisunique,inthesensethatitisbasedonthe
practitioner’spersonalexperience,onepractitioner’sexperiencemayberepresentative
ofotherpractitionerswhoworkinthesamefieldofcare.Accordingly,gleaning
knowledgefromoneexamplemaybeaformofanalogicalreasoning,whichcanbe
transferableandthuscontributetosignificantlearningforotherpractitioners.
Therefore,exploringnurses’livedexperiencewithpracticingandteachingspiritualand
existentialcaremaybeausefulmeanstouncoveressentialembodied,tacitandpractical
knowledge,whichmaybetransferableandusefulforothersinend-oflifecare(Aadland,
1997).

11
5.Theaimofthestudy
TheoverallaimofthisPhDthesisistoilluminatethemeaningofregisterednurses’
experienceswithpracticingandteachingspiritualandexistentialcarefordyingpatients
indifferentNorwegianhealthcarecontexts.
5.1Thespecificaims
PaperI:Todescribethemeaningofhospicenurses’livedexperiencewithalleviating
dyingpatientsspiritualandexistentialsuffering
PaperII:Todescriberegisterednurses’experienceswithspiritualandexistentialcare
fordyingpatientsinageneralhospital
PaperIII:ToilluminateapioneeringNorwegianmobilehospicenurseteachingteam’s
experiencewithteachingandtrainingcareworkersinspiritualandexistentialcarefor
thedyinginnursinghomesandhomecaresettings
5.2Theresearchquestions
PaperI:Whatarethehospicenurses’experienceswithalleviatingdyingpatients’
spiritualandexistentialsuffering?
PaperII:Whataretheregisterednurses’experienceswithalleviatingdyingpatients’
spiritualandexistentialsuffering?
PaperIII:Whatarethemobilehospicenurseteachingteam’sexperienceswithteaching
andtrainingcareworkersinhomecareandnursinghomesinspiritualandexistential
careforthedying?

12
6.MethodologicalFrameworkPhenomenologicalHermeneutics
Whilemethodologyhastodowiththeoverallapproachtoaparticularresearchfield,
implyingafamilyofmethodsthatshareparticularphilosophicalandepistemological
assumptions,methodsarespecifictechniquesthatareusedfordatacollectionand
analysis.Henceforth,thechoiceoftechniques(-ormethods)usedinastudy,mustbe
consistentwithitsmethodologicalframework(Swinton&Mowat,2006).Thestudy’s
methodologicalframeworkwillnowbepresented.
Theoverallaimofthisstudyistoilluminatethemeaningofnurses’experienceswith
practicingandteachingspiritualandexistentialcarefordyingpatientsindifferent
Norwegianhealthcarecontexts.Thisdeterminedthechoicetoanchorthestudyinthe
traditionofphenomenologicalhermeneutics(Gadamer,2004;Heidegger,1962;Ricoeur,
1976,1981,1984,1992,2008)withspecialemphasisonRicoeur’s(1976)interpretation
theory.FollowingRicoeur’s(1976)lineofthought,oneperson’sexperiencecannot
directlybecomeanother’s:
Aneventbelongingtoonestreamofconsciousnesscannotbetransferredassuchintoanotherstreamofconsciousness.Yet,nevertheless,somethingpassesfrommetoyou.Thissomethingisnottheexperienceasexperienced,butitsmeaning.Hereisthemiracle.Theexperienceasexperiencedaslived,remainsprivatebutitssense,itsmeaningbecomespublic.(Ricoeur,1976,pp.15-16)
DrawingonRicoeur,theoverallaimofthisstudyistointerpretand“makepublic”the
meaningofthenurses’spiritualandexistentialcareexperiences.
Phenomenologicalhermeneutics,beingtheprocessofinterpretinganddescribing
humanexperiencetounderstandthemeaningofthatexperienceiswellpositionedasa
suitablemethodologyforhumanscienceresearch.Itisnotaresearchmethodassuch,
butratherbothatheoreticalperspectiveandmethodologythatliesbehindthemethods
employedinaparticularstudy(Tan,Wilson,&Olver,2009;VanManen,2014).
Increasinglyphenomenologicalhermeneuticsisthephilosophicalunderpinningof
choiceinqualitativehealthcareresearchandisfrequentlyusedinnursingresearch

13
(Lindseth&Norberg,2004;Sørlie,2001;Tanetal.,2009;Torjuul,2009;Ødbehr,Kvigne,
Hauge,&Danbolt,2014).
Thetraditionofphenomenologicalhermeneuticswillnowbeoutlined,drawingonthe
worksofHusserl,Heidegger,GadamerandRicoeur.Thiswillbefollowedbyan
explanationofhowRicoeur’s(1976)phenomenologicalhermeneuticalinterpretation
theoryinformedandguidedthechoiceofmethodsthatwereusedinthestudy.
6.1EdmundHusserlEdmundHusserl(1859-1938)isgenerallyregardedastheintellectualfounderof
phenomenologicalphilosophy(VanManen,1990,2014).AccordingtoPorterand
Robinson(2011)Husserl’sphilosophicalresearchisnothermeneutics.Itisnoteven
hermeneuticallyinclinedinitsmethodologybecauseheavoidstakingan“interpretive”
stanceinmanyrespects,focusinginsteadonthings(phenomena)andourconsciousness
orexperienceofthem.Nonetheless,Husserl’sphenomenologyisofinvaluable
significanceforhermeneuticsindirectly,andforthedevelopmentof“phenomenological
hermeneutics”directly.Hisinfluenceisparticularlypronouncedinthehermeneutical
developmentsofMartinHeidegger(1889-1976),Hans-GeorgGadamer(1900-2002)
andPaulRicoeur(1913-2005),allofwhomhavetakenupandexpandedtheirownform
ofphenomenology(Porter&Robinson,2011).Henceforth,thisoutlineof
phenomenologicalhermeneuticalthoughtwillbeginwithabriefdescriptionof
Husserlianphenomenology.
ForHusserlphenomenologyisadisciplinethatendeavorstodescribehowtheworldis
constitutedandexperiencedthroughconsciousacts(VanManen,1990).Husserl’s
phrase“ZudenSachen”(backtothethings)hasbecomeawatchwordin
phenomenology(VanManen,2014,p.92).Generally,“tothethings”seemtomean“to
theissuesthatmatter”.Husserldefinesphenomenologyasadescriptivephilosophyof
theessencesofpureexperiences.Heaimstocaptureexperiencesinitsprimordialorigin
withoutinterpreting,explainingortheorizing.ForHusserl,theessenceswhich
phenomenologyconcernsitselfwithare“Erlebniswesen”,essencesoflivedexperiences.
Onlyknowledgethatisderivedfromimmediateexperientialevidencecanbeaccepted

14
(VanManen,2014,p.89).Inhislastandposthumouslypublishedtext“Thecrisisof
EuropeanSciencesandTranscendentalPhenomenology”(Husserl,1970),citedinVan
Manen(1990,p.182),Husserldevelopedtheideaofthelifeworldanddescribeditas
“alreadythere”,“pregiven”,theworldasexperiencedinthe“naturalprimordialattitude”
thatof“originalnaturallife”(Husserl,1970,pp.103-186)citedinVanManen(1990,p.
182).Husserlreservedthenotionofthe“naturalattitude”tothe“taken-for-
grantedness”ofeverydaythinkingandacting(VanManen,2014).This“naturalattitude”
manifestsitselfinournaturalinclinationtobelievethattheworldexistsoutthere,
independentofourpersonalexistence.Husserlianphenomenologydoesnotdenythe
externalexistenceoftheworld.Butitemphasizestheimportanceofbeingabletoshift
from“anaturaltoaphenomenologicalattitude”inordertoperceivethingsastheygive
themselvesinlivedthroughexperience–notasexternallyrealoreternallyexistent,but
asanopennessthatinvitesustoseethemasifforthefirsttime(VanManen,2014).
Inordertoshiftfromanaturaltoaphenomenologicalattitude,Husserlproposestwo
mainmethods(Porter&Robinson,2011,p.54).Husserl’sfirstmethod,theepoché
reductionistheattempttodescribephenomenaasimmediatelyapparentinexperience.
Thisreductioninvolvesbracketingorsuspendingone’ssubjectiveorprivatefeelings,
preferences,inclinations,orexpectationsthatwouldpreventonefromcomingtoterms
withaphenomenonorexperienceasitislivedthrough(Porter&Robinson,2011,pp.
54-55).Inaddition,onealsoneedstostripawaythetheoriesorscientificconceptions
andthematizationsthatoverlaythephenomenononewishestostudy,andwhich
preventsonefromseeingthephenomenoninanon-abstractingmanner(VanManen,
1990,p.185).
Husserl’ssecondmethodiscalledtheeideticreduction(Porter&Robinson,2011).Inthe
eideticreductiononeneedstoseepastorthroughtheparticularityoflivedexperience
towardstheuniversalessenceoreidosthatliesontheothersideoftheconcretenessof
livedmeaning(VanManen,1990,p.185).Thebracketingprocedureisoftenreferredto
asthetranscendentalreduction.Itiswhatmakestheeideticreductionpossible.
However,theepochéreductionisnotmeanttoreducesomethingtoitsbasicormost
fundamentalprinciplesbuttoallowaccesstothephenomenonintheleastprejudicedor
corruptedway(Porter&Robinson,2011,pp.54-55).

15
6.2MartinHeidegger
Husserlhadhopedforacontinuationofhisphilosophythroughhisformerassistantand
successor,MartinHeidegger(Porter&Robinson,2011).However,Heideggermadea
decisivebreakwithHusserl’stranscendentalphenomenologythroughhisfirstmajor
work“BeingandTime”(Heidegger,1962).ThekeypointsinHeidegger’s
phenomenologywillnowbeoutlined,basedonPorterandRobinson‘s(2011)work.In
contrasttoHusserl,Heideggerisnotinterestedinthestructuresofconsciousness,
essencesorevenknowledgeperse,butinaninvestigationintothemeaningofbeing,
(“Dasein”).Heideggerclaimsthatphenomenologycannotmerelyinvestigatepure
consciousnessbutmusttakeintoaccountthetotalityofthehumansituation,duetothe
factthatweare,eachandeveryoneofus,already“being-intheworld”.
WithHeideggerphenomenologybecomesaradicallyinterpretiveenterprise.Heclaims
thathumanexistencehasahermeneuticalstructurewhichunderliesallour
interpretationsincludingthoseoftheonticornaturalsciences;thatis,bothscientific
andculturalknowledgemustbederivedfromthestructureofbeing(Porter&Robinson,
2011).Accordingly,thereisnoneutralorunbiasedstartingplacefromwhichonemay
begintounderstand.Wearethrownintoaworldinwhichlanguage,cultureand
institutionsoflifealreadyaregiven.Sonomatterwhereorwhenwefindourselves,we
willalwaysbeconditionedbyourownhistoricalsituatedness.Henceforth,Heidegger
arguesthatwecannotpossiblybrackettheworldinordertounderstandourselvesand
thatjudgmentaboutactuallyexistentthingscannotbesuspended.Heideggerstatesthat
themeaningofthingsisknowninthecontextofourrelationshipstothemwithinthe
world.Hearguesthatweunderstandlifefromoutoflifeitself.Understandingbegins
withoursituatednessasbeing-in-theworld.Throughhermeneuticswearemaking
understandingexplicitanddisclosingthenatureofbeing,-orDaseintoourselves.
However,Heideggerpointsoutthatunderstandingmayneverbeself-evidentasifit
werecorrespondingtofactsintheworld,forDaseinhasnosingleobjectorfacttofirst
comprehend.Insteadunderstandingisinherentlycircularorhermeneutical(Porter&
Robinson,2011).

16
Heidegger’shermeneuticalcircleisbestcharacterizedintermsofpreunderstandingand
temporality(Porter&Robinson,2011).Structuresofunderstandinginvolveafore-
structurethatconstantlyprojectsuponthatwhichisalreadyunderstoodandevident.It
isananticipatorystructureorpreliminaryawarenessofmeaning.Ashistoricalbeings,
wehaveanticipationsandexpectationsofthefutureanditspossibilitiesaswellas
conditionedunderstandingfrompreviousunderstanding.Hence,allexistenceis
interpretiveandallmeaningtakesplacewithinacontextofinterpretationmediatedby
cultureandlanguage.Whatremainsininterpretationistoworkout“thethings
themselves”insteadofallowingourpre-understandingtobeguidedbymistaken
assumptionsandillusions(Porter&Robinson,2011,p.68).Evensothisworkingoutis
notatechniqueormethodmeanttoachieveunderstanding.Rather,itismeantasa
descriptionofhowunderstandingemergesasweconstantlyrespondtoourfore-
projectionandprejudgments.Understandinghappenspriortoourreflectionbecausewe
arealreadyparticipating,andthereforeunderstanding,fromaspecificorientationand
awarenessaboutoursituationandcontext(Porter&Robinson,2011).
Accordingly,forHeidegger,Daseinisanevent,anoccurrencewhereinunderstandingis
“tobe”intheworldwhichisalwaystobeunderstoodinterpretively.Heidegger’s
existentialandphenomenologicalanalysisredefineswhatitmeanstounderstand
(Porter&Robinson,2011).WhatisneededHeideggerproposes,isanexistential
analysisthatinquiresintothemeaningof“tobe”thatispresenttous,yetremainstobe
drawnout.Thismeaningwillonlybedisclosedwhenwestopattemptingtograsp
essences,factsandabstractionsandbegintolivelifewithouttryingtomanipulateit.
Knowledgeinthescientificsensemayonlybesupplementaltoourdistinctwayof
existence.Heidegger’sanalysisrestsuponadistinctionbetweentheontologicalandthe
ontic.Theonticoronticalisthefactualworldunderstoodbythesciences,suchas
chemistryandbiology.WhileDaseinhasonticqualities,asananimalinthefactual
world,“Dasein”(he,shewe)isalsounique,forDaseinaloneisconcernedwiththe
questionofbeingandwhatitmeans,“tobe”.Noneoftheotheranimalsinhabitingthe
earthareconcernedwiththemeaningofbeing.ForHeideggerthequestionofbeing
representsourdecisiontoletthequestionbeaquestionforus.Itisaturnoradecision,
aneventofrecognizingawedgebetweenbeingandbeing–anontic-ontological
difference.Wearethebeingswhoaskthequestionsofwhoweare.Wealoneareableto
17
interrogatethenatureofwhatitmeanstobe.Heidegger’sontologicalphenomenology
canbecharacterizedasahermeneuticsoflifeorwhathecalls“hermeneuticsof
facticity”.Hermeneuticsinthissenseisaninterpretationoftheconditionsand
circumstancesthatdetermineorlimitone’spossibilitiesofbeing-in-the-world(Porter&
Robinson,2011).
6.3Hans-GeorgGadamerHans-GeorgGadamerisoneoftheforemostrepresentativesofhermeneutical
phenomenology(VanManen,2014).AsaformerstudentofHeidegger,Hans-Georg
Gadamershareshisnotionthatallunderstandingishermeneuticandthatthe
hermeneuticfunctionisactuallyourbasicmodeofbeing-in-theworld(Porter&
Robinson,2011).Thetaskofhermeneutics,accordingtoHans-GeorgGadamer,isto
clarifytheconditionsinwhichunderstandingandinterpretationtakeplace(Gadamer,
2004).
ThehistoricalstrandsofFriedrichSchleiermacher(1768-1834)andWilhelmDilthey’s
(1833-1911)pioneeringhermeneutics,thephenomenologicaldescriptionofEdmund
Husserl(1859–1938)andtheontologicalanalysisofMartinHeidegger(1889-1976)all
cometogetherinGadamer’sseminalwork“WahrheitundMethode:Gründzügeeiner
philosophischenHermeneutik”(1960)translatedtotheEnglishversionas“Truthand
Method”in1975(Porter&Robinson,2011).
InthismagnumopusGadamer(2004)explicatesinaphenomenologicalmanner,the
hermeneuticmethodasithadbeenoriginallydevelopedbyFriedrichSchleiermacher
andsubsequentlybyWilhelmDiltheyandHeideggerhimself(VanManen,2014).
Schleiermacherappliedhermeneuticstotheinterpretationoftexts,andemphasizedthe
importanceofconsideringthehistoricaltemporalityandrationalityofthetext.For
Schleiermacher,hermeneuticsdealswithreconstructingthepast(VanManen,2014).
WhileGadamer(2004)agreedaboutthenecessityofapproachingtextswithopenness
andsensitivitytotheirhistoricaltraditionsandinterpretivehorizons,healsoargued
thatitwasimpossibletoplaceoneselfintheoriginalreconstructedhistoricalcontext.

18
IncontrasttoSchleiermacher’ssearchfortheauthorialintentofatext,Gadamerargues
thatancienttextsmustbeinterpretedinthecontextofone’sownsocialhistorical
existence(vanManen2014).AccordingtoGadamer(2004)thereexists:
aninsuperabledifferencebetweentheinterpreterandtheauthorthatiscreatedbyhistoricaldistance…..Therealmeaningofatext,asitspeakstotheinterpreter,doesnotdependonthecontingenciesoftheauthorandhisoriginalaudience.Itcertainlyisnotidenticalwiththem,foritisalwaysco-determinedalsobythehistoricalsituationoftheinterpreter,andhencebythetotalityoftheobjectivecourseofhistory.(Gadamer,2004,p.296)
ForGadamer(2004),hermeneuticunderstandingisachievedthroughacircular
interpretationprocess,whereonemovesbackandforthbetweenthetextasawhole
anditsindividualparts.Assuch,construingthemeaningofthewholeinvolvesmaking
senseofthepartsandgraspingthemeaningofthepartsisdependentonhavingsome
senseofthewhole:“Thusthemovementofunderstandingisconstantlyfromthewhole
tothepartandbacktothewhole.Ourtaskistoexpandtheunityoftheunderstood
meaningcentrifugally”.(Gadamer,2004,p.291)
Gadameremphasizesthatthehermeneuticcircleisnota“methodologicalcircle”,rather
itdescribesanelementoftheontologicalstructureofunderstanding(Gadamer,2004,p.
294).ThebasicmodelofunderstandingthatGadamerfinallyarrivesatin1960in“Truth
andMethod”(Gadamer,2004),isconversationanddialogue(Malpas,2015).
ConversationalwaystakesplaceinlanguageandsimilarlyGadamerviews
understandingasalwayslinguisticallymediated.ForGadamer,understandingisa
matterofnegotiationbetweenoneselfandone’spartnerinahermeneuticaldialogue.
Henceforth,theprocessofunderstandingcanbeseenasamatterofcomingtoan
“agreement”aboutthematterathand.ForGadamer(2004),interpretationand
understandingalwaysoccurfromwithinaparticular“horizon”thatisdeterminedby
ourhistoricallydeterminedsituatedness.Accordingly,comingtoanagreement,means
establishingacommonframeworkor“horizon”.Gadamerthustakesunderstandingto
beaprocessthatinvolvesa“fusionofbothparty’shorizons”or“horizontverschmelzung”
(Malpas,2015).
19
Inasmuchasunderstandingistakentoinvolvea“fusionof“horizons”italsoinvolvesthe
formationofanewcontextofmeaningthatenablesintegrationofwhatisotherwise
unfamiliar,strangeoranomalous.Inthisrespectallunderstandinginvolvesaprocessof
mediationanddialoguebetweenwhatisfamiliarandwhatisalien,inwhichneither
remainsunaffected(Malpas,2015).Gadamer(2004)pointsoutthatinthedialogueof
understandingourprejudicescometothefore.Heclaimsthatourprejudicesplaya
crucialroleinopeningupwhatistobeunderstood,inasmuchastheythemselves
becomeevidentinthatprocess.Asourprejudicestherebybecomeapparenttous,they
canalsobecomethefocusofquestioningintheirownreturn:
Theessenceofthequestionistoopenuppossibilitiesandkeepthemopen….Infact,ourownprejudiceisproperlybroughtintoplaybybeingputatrisk.Onlybybeinggivenfullplayisitabletoexperiencetheother’sclaimtotruthandmakeitpossibleforhimtohavefullplayhimself.(Gadamer,2004,pp.298-299)
Notsurprisingly,oneofGadamer’s(2004)mostcontroversialmovesishisdefenseof
theimportanceofprejudiceininterpretation.ForGadamer,understandingrequires
presuppositionsandassumptionsthatenableunderstandingaswellas
misunderstanding(Porter&Robinson,2011).Gadamer(2004)maintainsthatwe
alwaysbringourfiniteandhistoricallyconditionedawarenesswithuswhenwe
encountersomething.Thismeansthatwemustallowourtraditionsandlongheld
assumptionstobechallengedandtested.Theremaybenonewexperienceand
understandingotherwise.Authenticexperienceshakesusawakeandopensoureyesto
thenewandunexpected,thatwhichliesbeyondourpersonalhorizon.Gadamer(2004)
pointsoutthatwithineveryunderstanding,truthispartiallyrelativetotheinterpreter’s
ownhorizonthoughneverentirelyconsumedbyit.Justlikeourlivingrelationshipto
thetruthofatext,ourwholeexperienceoflifereflectsthesameuniversalhermeneutical
dynamics.Gadamer’s(2004)descriptionofhermeneuticsintermsofwhatitmeansto
understandisnotonlyamatterofhowweknowclassicalandphilosophicaltexts,works
ofartandthelike.Rather,Gadamerianhermeneuticsisawayofdisclosingwhatit
meanstohaveanexperienceofunderstandinguniversally(Porter&Robinson,2011).

20
6.4PaulRicoeurPaulRicoeurmorethananyother,cementedtheconnectionandmutualaffinity
betweenhermeneuticsandphenomenology(Ricoeur,1981,2008;Tanetal.,2009).
Inhislandmarkessay“Phenomenologyandhermeneutics”,Ricoeur(1981)confrontsthe
questionofwhatremainsofEdwardHusserl’sphenomenologicalprograminthewake
ofHeideggerandGadamer’sdevastatingcritiqueofphenomenology.Inlinewiththe
hermeneuticsofHeideggerandGadamer,Ricoeurdiscussesourembeddednessinthe
worldoflanguageandsocialrelationshipsandtheinescapablehistoricityofall
understanding(Finlay,2012;Ricoeur,1981).Ricoeurconvincinglydemonstratesthat
whatsuccumbstothehermeneuticalcritiqueisnotphenomenologyassuch,butrather
phenomenologyinitsmostidealisticHusserlianform(Ricoeur,1981).
WhileHusserlarguedthatphenomenologyconsistsofdescribingwhatappearsin
consciousness,Ricoeur(1981,p.137)showsthataccordingtoHusserl’sownaccounts,
whateverappearsinconsciousnessisalreadytheworkoftheconstitutingego.Andin
thisconstitutionprocess,theinterpretiveisalreadyatwork(VanManen,2014).
Ricoeur(1981)pointsoutthatbeyondthesimpleoppositionbetweenphenomenology
andhermeneuticsthereexistsamutualbelongingbetweenthem.Ontheonehand,
hermeneuticsiserectedonthebasisofphenomenology,andthuspreservessomething
ofthephilosophyfromwhichitdiffers.Ontheotherhand,phenomenologycannot
constituteitselfwithoutahermeneuticalpresupposition:
…beyondthecritiqueofHusserlianidealism,phenomenologyremainstheunsurpassablepresuppositionofhermeneutics;andontheotherhand,thatphenomenologycannotcarryoutitsprogrammeofconstitutionwithoutconstitutingitselfintheinterpretationoftheexperienceoftheego.(Ricoeur,1981,p.114)
ThisbringsustothemaintenetsofRicoeur’s(1976)phenomenologicalhermeneutical
interpretationtheory,whichhaveinformedandguidedthisthesis.ForRicoeur(1976),
interpretationisthehingebetweenlanguageandlivedexperience(Geanellos,2000).In
hisfamousinterpretationtheory,Ricoeurattemptedtograftthehermeneuticalproblem
ofinterpretationtocontemporaryinsightsinphenomenology(Ricoeur,1999).

21
6.4.1Textunderstoodashumanaction
AlthoughRicoeur(1976)originallyformulatedhisinterpretationtheorywithrespectto
texts,healsopointsoutthathumanactioncanbeunderstoodasdiscourseand
interpretedastext,whenithasbeenobjectifiedandfixatedthroughwriting.
Accordingly,hisinterpretationtheorycanbeextendedintothesphereofthesocial
sciences(Ricoeur,1981).Inlightofthis,Ricoeur’s(1976)interpretationtheoryis
applicabletointerpretnurses’narrativesabouttheirexperienceswithspiritualand
existentialcare.Thiswillbeelaboratedoninthemethodssection.
6.4.2Distanciationandappropriation
Writingrendersthetextautonomouswithrespecttotheauthor’sintention.When
spokendiscourseiswrittendown,(i.e.liketheresearchinterviewsinthisstudy),the
fixateddiscourseanditsmeaningbecomesdistancedfromthespeechevent.Through
thisdistanciation,thetextbecomes“decontextualized”fromthespeecheventandits
socialandhistoricalconditions,thusopeningitselfuptoanunlimitedseriesofreadings
(Ricoeur,1976,1981,2008).Distanciationcreatesaneedtorecontextualizeand
appropriatethetext,-tofamiliarizeourselveswiththetextandmakeitourown
(Ricoeur,1976).Ricoeur(1976,p.43)pointsoutthat:
readingisthepharmakonthe“remedy”bywhichthemeaningofthetextis“rescued”fromtheestrangementofdistanciationandputinanewproximity,aproximitywhichsuppressesandpreservestheculturaldistanceandincludestheothernesswithintheowness.
Accordingly,thereexistsadialecticrelationshipbetweendistanciationand
appropriationintheinterpretationprocess:“Tomakeone’sownwhatwaspreviously
foreignremainstheultimateaimofallhermeneutics…Thisgoalisachievedinsofaras
interpretationactualizesthemeaningofthetextforthepresentreader”.(Ricoeur,1976,
pp.91-92)

22
Methodologicallydistanciationandappropriationallowresearcherstomovebeyondthe
notionthatonlytheresearchparticipants’understandingismeaningfulandorcorrect.It
alsoallowstheinterpreterstointerpretthesametextfaithfully,yetsomewhat
differentlybecauseitisacknowledgedthattextshavemanymeanings(Geanellos,2000).
6.4.3Explanationandunderstanding
Interpretingatextinvolvesmovingbeyondunderstandingwhatthetextsays(itssense)
tounderstandingwhatittalksabout(itsreference)(Ricoeur,1976,p.88).Assuch,the
text’ssenseanditsreferenceembodiesthetwostagesofRicoeur’sinterpretation
theory:(i)explanation,-orwhatthetextsaysand(ii)understanding,orwhatthetext
talksabout(Geanellos,2000).Whileexplanationisdirectedtowardanalysisofthe
internalrelationsofthetext(theparts)understandingisdirectedtowardgraspingthe
meaningsthetextdiscloses(thewholeinrelationtotheparts)Inthisway,interpretive
understandinggoesforwardinacontinualmovementbetweenthepartsandthewhole
allowingunderstandingtobeenlargedanddeepened(Geanellos,2000).“Ultimatelythe
correlationbetweenexplanationandunderstanding,betweenunderstandingand
explanationis‘thehermeneuticcircle’.”(Ricoeur,2008,p.163)Hence,thesenseofatext
isnotbehindthetext,butinfrontofit.Itisnotsomethinghidden,butsomething
disclosed:
Whathastobeunderstoodisnottheinitialsituationofdiscourse,butwhatpointstoapossibleworld.Thetextspeaksofapossibleworldandofapossiblewayoforientatingoneselfwithinit.Thedimensionsofthisworldareproperlyopenedupanddisclosedbythetext.(Ricoeur,1976,pp.87-88)
6.4.4Guessingandvalidation
Allinterpretiveactivityinvolvesadialecticbetweenguessingandvalidating(Ricoeur,
2008).Wemakeaneducatedguessaboutthemeaningofapartandcheckitagainstthe
wholeandviceversa.Inthesameway,webeginbyguessingaboutthemeaningofthe
wholeasdeterminingtherelativeimportanceofseveralparts.Throughoutthisprocess
ofguessandvalidationwecancometoanendwhenwesaythisishowweunderstand
things.Butthereisnodefiniteoutcome(Dauenhauer&Pellauer,2014,p.154).

23
Itisalwayspossibletorelatesentences,oractionstooneanotherinmorethanone
way:“Thisplurivocityistypicalofthetextconsideredasawhole,opentoseveral
readingsandtoseveralconstructions”(Ricoeur,2008,p.154).Althoughatextmayhave
severalinterpretations,someinterpretationsaremoreprobablethanothers.Itis
thereforenecessarytovalidateourguesses.Validatingguessesisclosertoalogicof
probability,thantoalogicofempiricalverification.Wevalidateaninterpretationby
vindicatingitagainstcompetinginterpretations.Thus,validationisnotverification
(Ricoeur,2008).Rather,itisan“argumentativedisciplinecomparabletothejudicial
proceduresoflegalinterpretation.Itisalogicofuncertaintyandofqualitative
probability.”(Ricoeur,2008,p.155)Guessandvalidationarecircularlyrelatedas
subjectiveandobjectiveapproachestothetext.Althoughthereisalwaysmorethanone
interpretation,allinterpretationsarenotequal.Onemustthereforetrytofindthemost
probableinterpretation.Ricoeurpointsoutthat:
Thetextisalimitedfieldofpossibleconstructions.Thelogicofvalidationallowsustomovebetweenthetwolimitsofdogmatismandskepticism.Itisalwayspossibletoargueagainstaninterpretation,toconfrontinterpretations,toarbitratebetweenthemandtoseekforanagreement,evenifthisagreementremainsbeyondourreach.(Ricoeur,2008,p.155)
Asmentionedinthebeginningofthischapter,theresearcher’schoiceofmethodsto
carryoutastudymustbeconsistentwiththestudy’smethodologicalframework
(Swinton&Mowat,2006).Thelinkbetweenthisstudy’sphilosophicalunderpinnings
andthemethodsusedinthestudy(VanManen,2014)willthereforebeexplicatedinthe
followingchapter.

24
7.ThemethodsDatawerecollectedthroughnarrativeinterviews(Mishler,1986)anda
phenomenologicalhermeneuticalinterpretationmethod(Lindseth&Norberg,2004)
waschosentoanalyzethedata.
7.1Datacollection:NarrativeinterviewsOpen-endednarrativeinterviews(Mishler,1986)wereusedtocollectthedatainall
threestudies.ThenarrativeinterviewsinpaperIandIIwereconductedasindividual
interviews,whilethenarrativeinterviewinpaperIIIwasconductedasafocusgroup
meetingwiththemobilehospicenurseteachingteam.
Ricoeur’s(2008)theoryofnarrativesstatesthatlifehasaprenarrativequalityandthat
actioncanbelookeduponasapotentialnarrative(Vandervelde,2008).Ricoeurnotes
that:
Lifeislived;historyisrecounted….Inremainingboundtotimeandtochange,historyremainstiedtoaction.….Ultimatelyhistorycannotmakeacompletebreakwithnarrativebecauseitcannotbreakwithaction,whichitselfimpliesagents,aimsandcircumstances,interactionsandresultsbothintendedandunintended.(Ricoeur,2008,p.5)
Ricoeurmaintainsthatactionandlifearestructuredororganizedintheirbeingby
narrative-likefeatures,sothattellingthestoryisnotanafter-thefactreorganizationof
whattookplace,butthemakingexplicitofwhatwasalreadyimplicitinactionandin
life.Accordingly,understandingtakestheformofnarrativesandispermeatedbya
culturalworldthatisitselfmadeofnarratives.Aninchoatenarrativestructureliesatthe
heartofpeople,thingsandevents.Narrativesarethusnotmeredescriptionsof
somethingthatwouldbeotherwiseavailableindependentlyofdescription,butare
ontologicallayers,partandparcelofthepastofactionsandexperiences(Ricoeur,2008;
Vandervelde,2008,p.141).
DrawingonRicoeur’sargumentabouttheinterconnectionbetweennarrativeand
humanexperience(Ivic,2009)itseemedreasonabletobelievethatthenarrative

25
interview(Mishler,1986)wouldbeasuitablemethodtogainaccesstotheparticipants’
experienceswithpracticingandteachingspiritualandexistentialcareforthedying.
Thiswasbasedonthepresuppositionthattheinterviewees’perspectiveswouldbebest
revealedinnarrativeswheretheyusetheirspontaneouslanguagetotalkabouttheir
experiences(Mishler,1986;VanManen,1990).AccordingtoMishler(1986,p.68)
“thereisawiderecognitionofthespecialimportanceofnarrativeasamodethrough
whichindividualsexpresstheirunderstandingofeventsandexperiences”.Mishler
(1986)pointsoutthat:“wearemorelikelytofindstoriesreportedinstudies“using
relativelyunstructuredinterviewswhererespondentsareinvitedtospeakintheirown
voices,allowedtocontroltheintroductionandflowoftopics,andencouragedtoextend
theirresponses”.(Mishler,1986,p.69)Thenarrativeinterviewswereconducted,using
oneopen-endedquestion.Clarifyingfollow-upquestionswereusedwhennecessary.
AsdiscussedinChapter4.2,spiritualcareisahighlydebatedconceptduetothemany
variationswhichemergefromthenursingliterature.Theauthorschosenottopresent
anyofthesevariationsduringtheinterviews.Theyalsoavoideddefiningpalliativeand
terminalcare,sincethesetermsareincommonandsometimeinterchangeableuse
(Clark&Seymour,1999)andthemomentwhenapatienttransitionsfrom“palliative”to
“terminal”careisdebatedintheliterature(Clark&Seymour,1999;Harlos,2010).
Accordingly,theauthorschoseanopenapproachtoensurethatthenursesfeltthey
couldnarratefreelyabouttheirexperienceswithspiritualandexistentialcareforthe
dying.Theauthorspresumedthatthiswouldgivethemthebestchancetocollectas
manyrichnarrativesaspossible.
ThehospicenursesinpaperI,andthenursesinpaperIIwereaskedthequestion:“What
areyourexperienceswithprovidingspiritualandexistentialcaretodyingpatients?”
InpaperIIIthemobilespiritualandexistentialcareteachingteamwasaskedthe
question:“Whatareyourexperienceswithteachingandsupervisingcareworkersin
existentialandspiritualcareforthedying?”

26
7.1.1Thenarrativefocusgroupinterview
Thenarrativeinterviewinthelastpartofthestudy(paperIII)wasconductedasafocus
groupmeetingbecausetheauthorswantedtocollectnarrativesaboutthegroup’s
experienceasauniquepioneermobilespiritualandexistentialcareteachingteam.
BelzileandÖberg(2012)pointoutthatfocusgroupsareusefultostudytheperceptions,
feelings,meaningsorwaysofthinkingthatareheldbyagroupwhoshareinaparticular
intersubjectivereality.Thefocusgroupisanefficientwaytoobtaindatafrom
participantswhoworktogetherdaily:“…colleaguescanrelatetoeachother’scomments
toincidentsintheirdailysharedlives.Theymayevenchallengeeachotheron
contradictionsbetweenwhattheyprofesstobelieveandhowtheyactuallybehave”.
(Kitzinger,1995,p.300)
7.2Dataanalysis:Interpretingtheinterviewtexts
DrawingontheworksofHeidegger,GadamerandRicoeur,LindsethandNorberg(2004)
underlinethatessentialmeaningissomethingthathumansarefamiliarwithinthe
practicesoflifeandthatthisfamiliarityisexpressedthroughactions,narrativesand
reflections.However,inordertostudytheessentialmeaningofresearchparticipants
livedexperience,theirnarrativesmustbewrittendownandinterpreted.Itisimportant
tonotethatwhenLindsethandNorberg(2004)usethetermessentialmeaning,their
methoddoesnotinvolvea“pure”Husserlian”phenomenologicalsearchformeaning
thatisuncontaminatedbyinterpretation.Nordoesitinvolvea“pure”hermeneutical
textinterpretation,sincetheaimoftheinterpretationistotranscendthemeaningofthe
textinordertorevealessentialtraitsofourlifeworld:“Thusweseethat
phenomenologymustbephenomenologicalhermeneutics.Essentialmeaningmustbe
studiedandrevealedintheinterpretationoftext”(Lindseth&Norberg,2004,p.147).
InLindsethandNorberg’s(2004)interpretationmethod,eachinterviewislookedupon
asatext.Theinterpretationmethodimpliesadialecticmovementbetweenthetextasa
wholeandpartsofthetext.Themethodconsistsofthreepracticalstepsinvolving:
1.Naïvereading,2.Structuralanalysis,3.Comprehensiveunderstanding.

27
7.2.1Thenaïvereading
Theaimofthenaivereadingistograspanoverallimpressionofthetextandtogain
accesstotheparticipants’livedexperience.Duringthenaïvereading,theresearcher
muststrivetoavoidmakingjudgmentsaboutthefactualinthenarratives.Rather,the
researchermustkeepanopenmind,allowingherselftobetouchedandmovedbythe
narratives.Todothis,theresearchermustshiftfroma“natural”toa“phenomenological
attitude”orinotherwords,accomplish“epoché”or“bracketing”(Lindseth&Norberg,
2004,p.147).ItisimportanttonotethatwhenLindsethandNorberg(2004)usethe
Husserlianconceptsof“essentialmeaning”,“epoché”and“bracketing”theydonotmean
thatresearchersshouldgiveuptheirpreunderstandingsinordertoarriveatapureun-
interpretedanduncontaminatedessentialmeaning.Thisisneitherpossiblenor
desirable.Researchersshouldinsteadstrivetobrackettheireagernesstoclassifythe
participants’storiesintocategories,explanationsandmodelsinordertoletthe
participantsleaveanimpressiononthem(Lindseth&Norberg,2004).Byencountering
theparticipantswithopennessandreceptivity,aspaceofattentionopensup.Whenthe
participant’s“expressioncanmakeanimpression,somethingfundamentalhappens...A
spaceofattentionopensup,inwhichwhathasbeensaidcanshowitselfwithgreater
clarity”(Lindseth,2015,p.51).
Strivingtokeepanopenmind,theauthorsrereadtheinterviewtextsseveraltimes.The
processofrereadingdrovetheanalysistowardsaphenomenologicalworld,which
allowedtheauthorstobetouchedbythenarratives.Thenaïveunderstandingofthetext
revealedthedirectionforthestructuralanalyses(Lindseth&Norberg,2004;Ricoeur,
1976,1981,1984).Theresultsfromthenaïvereadingswerediscussedbetweenthe
authors.Thenaïvereadingguidedthestructuralanalysis,whichwasthesecondstepin
theinterpretationprocess.
7.2.2Thestructuralanalysis
Thestructuralanalysisincludesvariousexaminationsofthepartsofthetextinorderto
understandandexplainwhatitsaysandhowitissaid.Thestructuralanalysiscanbe
viewedasastagebetweenanaïveandacomprehensiveinterpretation,orbetweena

28
surfaceandadeepinterpretation.Theobjectiveofthestructuralanalysiswastoexplain
whatthetextwassaying(Lindseth&Norberg,2004;Torjuul,2009).Theauthorsreread
thetranscriptsseveraltimestolookformeaningfulpartsandpatternsthatcouldbe
dividedintonarrativemeaningunits.Ameaningunitcouldconsistofonesentence,
partsofasentenceorawholeparagraphwithrelatedmeaning.Themeaningunitswere
thencondensed,comparedandreflectedupontoidentifythespiritualandexistential
carethemesandsubthemesthatpenetratedthewholeorpartsofthetext.Athememay
beregardedasathreadofmeaningthatpermeatesthetextsasawholeorpartsofit
(Lindseth&Norberg,2004;Torjuul,2009).Themeaningunits,themesandsubthemes
werediscussedandreflecteduponbytheauthors.Theprocessofreading,identifying
anddiscussingthethemesandsubthemeswererepeateduntiltheauthorsreachedan
interpretativeagreement,weretheyfeltthatthethemescorrespondedtotheirtext
interpretations.LindsethandNorberg(2004),theobjectiveofthestructuralanalysisis
toexplainwhatthetextissaying.Hence,thestructuralanalysiscanbeviewedasthe
methodicor“objective”partoftheinterpretationprocess,sincethemeaningunitsare
decontextualizedfromtheindividualaccountsandthetextasawhole(inotherwords:
thepartsandmeaningunitsareconsideredindependentlyfromtheircontextinthe
interviewtexts(Lindseth&Norberg,2004)).Torecontextualizethetext,themeaning
unitsweregroupedtogethertocreatetentativethemesaccordingtotheauthors’naïve
reading.Theauthorsvalidatedthestructuralanalysis,bycheckingtheirinterpretations,
rereadingthetextandcomparingthethemesandmeaningunitswiththeirnaïve
understandingofthetextasawhole.
7.2.3Comprehensiveunderstanding(Interpretedwhole)
Inthethirdandlaststepoftheinterpretationprocess,acomprehensiveunderstanding
wasdeveloped.Thecomprehensiveinterpretationisdevelopedthroughamergingof
theresearchers’pre-understanding,naïvereading,thestructuralanalysis,previous
researchandrelevanttheory(Lindseth&Norberg,2004;Sørlie,2001;Ødbehretal.,
2014).Todevelopacomprehensiveunderstanding,theresearchersmustreflectonthe
themesinrelationtotheresearchquestionandthecontextofthestudy(Lindseth&
Norberg,2004).Theaimofthisstepistogainadeeperunderstandingoftheinterviews
asawhole,-inRicoeur’stermstorecontextualizethetext(Ricoeur,1976).Methodically,

29
interpretationallowsactualizationsofthemeaningsofthetext.ForRicoeur(1976)this
occursthrough“appropriatingthetext”;i.e.tomakeone’sownwhatwaspreviously
foreigninthetext(Ricoeur,1976,pp.91-92).Whentheworldofthetextis
appropriated,thehorizonoftheresearcherisexpanded.Thisopensupthepossibilityof
seeingthingsdifferentlyandorientingoneselfdifferentlyintheworld.Itisthislink
betweenunderstanding,experienceandself-understandingthatgroundsRicoeur’s
theoryinexistence(Geanellos,2000;Ricoeur,1976;Torjuul,2009).Whilethe
structuralanalysisischaracterizedasthemethodicorobjectivepoleofthis
interpretationmethod,LindsethandNorberg(2004)statethatthedevelopmentofa
comprehensiveunderstandingcanbelookeduponasthemethod’snonmethodicpoleof
understandingandtheypointoutthatimaginationisimportantbecauseitisnotpossible
tofollowstrictmethodologicalrulesintheprocessofrecontextualizingthetext.
Accordingly,LindsethandNorbergemphasizethattheirphenomenological
hermeneuticalinterpretationmethodliesbetweenartandscience:“Weuseourartistic
talentstoformulatethenaïveunderstanding,ourscientifictalentstoperformthe
structuralanalysisandourcriticaltalentstoarriveatacomprehensiveunderstanding”
(Lindseth&Norberg,2004,p.152).
Todevelopacomprehensiveunderstanding,thethemesfromthestructuralanalysisin
paperI,II,IIIandthemainresultsinthethesisarediscussedinlightofrelevant
theoreticalperspectivessuchasNorberg,BergstenandLundman’s(2001)modelof
consolation.Thecomprehensiveunderstandingineachindividualstudyispresentedin
thediscussionsectionineachpaper,whilethecomprehensiveunderstandingofthe
mainresultsfromtheentirestudyispresentedinchapter10inthisthesis.
7.3Methodologicalconsiderations
Whatconstitutesqualityinqualitativeresearchandthemeanstodetermineorenhance
ithasbeenasubjectofdebateandcontroversyinrecentyears(Cho&Trent,2006;
Golafshani,2003;Morse,Barrett,Mayan,Olson,&Spiers,2008;Onwuegbuzie&Leech,
2007;Torjuul,2009).Themattersofdisputehaveprimarilyevolvedaroundissues
concerningreliabilityandvalidity.However,tothisdatenoneofthedefinitionsofthese

30
conceptsrepresentahegemonyinqualitativeresearch(Cho&Trent,2006;Golafshani,
2003;Morseetal.,2008;Onwuegbuzie&Leech,2007;Torjuul,2009).Thearrayof
criteriaandterminologyusedmakethisdiscourseproblematicandrathercomplicated.
Moreover,thereexistsnosinglesetofphilosophicalandmethodological
presuppositionsthatcanunderpinaqualitativeparadigm.Inaddition,thereexistsno
uncontestedcollectionofmethodsandstandardsforreportingandevaluating
qualitativeresearchintheliterature(Cho&Trent,2006;Golafshani,2003;Kvale&
Brinkmann,2008;Morseetal.,2008;Onwuegbuzie&Leech,2007;Torjuul,2009).
Nevertheless,qualitativeresearchersagreethatastudy’scredibilityortrustworthiness
hastobewarrantedbyconformingtosomegenerallyacceptedscientificstandards.
Suchstandardsincludemethodologicalcongruence,auditability,orrigourin
documentingandexplainingtheresearchprocess,ethicalrigourandthecredibilityor
fittingnessofthedatainterpretation(Cho&Trent,2006;Golafshani,2003;Morseetal.,
2008;Onwuegbuzie&Leech,2007;Torjuul,2009).
DrawingonLincolnandGuba(1985),Seale(1999)statesthatestablishing
trustworthinessofaresearchreportliesattheheartofissuesconventionallydiscussed
asvalidityandreliability.AccordingtoKvaleandBrinkman(2008)reliabilitypertains
totheconsistencyandtrustworthinessofresearchfindings,whilevaliditypertainsto
thedegreethatamethodinvestigateswhatitisintendedtoinvestigate.Validation
consistsofaconsistentqualitycontrolthroughouteverystageofknowledgeproduction,
ratherthananinspectionattheendoftheproductionline(Kvale&Brinkmann,2008).
FollowingKvaleandBrinkman(2008),anattempttoestablishmethodological
congruencehasalreadybeenconductedinthedescriptionofthestudy’smethodological
frameworkandmethods.Inordertostrengthenthecredibilityofthestudy,therestof
thischapterwilldiscussmethodologicaltrustworthinessrelatedtodatacollection,data
analysis,studylimitationsandthefirstauthor’spreunderstanding.
7.3.1Thetrustworthinessofthedatacollection
Thenarrativeinterviewmethodwasusedtocollectasmanyrichnarrativesaspossible
inordertoachievethestudy’soverallaim,ofilluminatingthenurses’livedexperience.

31
Theauthors’ambitionwastocaptureasmanyfeaturesanddimensionsofthenurses’
experiencesaspossibleinordertoensureauthenticityandtoavoidsuperficialdata
(Lindseth&Norberg,2004;Torjuul,2009).However,asAppleton(1995)andMishler
(1986)emphasize,thequalityofthedatageneratedthroughnarrativeinterviewsis
largelydependentontheskillsandexpertiseoftheinterviewer.
Inordertopromotetrustworthiness,theauthorsstrovetocreateapermissiveandnon-
judgingclimate,encouragingthenursestousetheirownwordsandtonarrateasopenly
andhonestlyaspossibleabouttheirexperiencesduringtheinterviews(Appleton,1995;
Mishler,1986).Nodefinitionsofspiritualandexistentialcarewereintroduced,inorder
toallowthenursestotalkfreelyaboutwhattheyconsideredasspiritualandexistential
care.Carewastakentoavoidinterruptingthenurses’narrativeflowandreflectionin
ordertogivethemenoughtimeandspacetofollowtheirownthoughtsandworkout
theirownstories.Thisrequiredtheabilitytobepatientandenduremomentsofsilence.
Theauthorsfolloweduponthethemesthatthenursesfocusedonduringtheinterview
inordertoobtainthemeaningoftheirnarratives(Gadamer,2004).Thiswasdoneby
tyingquestionsandcommentstothenarrativesandrepeatingthenurses’words
wheneverpossible(Riessman,1993).Occasionallytheauthorswoulduseprobing
questions,suchas“Whathappenedthen?”or“Couldyoupleasetellmemoreabout…?”
toencouragethenurses’narrativeflow.However,itwasnecessarytobesensitiveto
theirresponsesandreactionsinordertoavoidprobingtoomuch(attheriskofinvading
thenurses)andprobingtoolittle(attheriskofmissingoutonimportantstories).In
ordertoincreasetrustworthiness,theauthorsalsostrovetoclarifyunclearquestions
andunclearanswersinordertoreducepotentialmisunderstandingswiththenurses.
Inspiteoftheseprecautions,onecanneveravoidthatsomeresearchparticipantsmight
notbewillingto,ordaretotellstories,whileothersmaynotremember,orfindit
difficulttoexpresstheirthoughtsandfeelings.Thischallengestheresearchertopay
attentiontocuesthatcouldsuggestthatthenursesmighthavemoretosay(Lindseth&
Norberg,2004;Torjuul,2009).
Theactoftellingastorymusttakeplaceaftertheactualeventtookplace:“Lifeislived
historyisrecounted”(Ricoeur,2008,p.5).Assuch,participants’narrativesarestories

32
aboutpastexperiences.Hence,narrativesarenotstoriesconcerningfactualtruths;
rather,theyareasynthesisbetweenaperson’sexperiencedeventsandincidents.
Accordingly,arecountedstoryisalwaysmorethantheactualsumofthesingleevents
(Benzein,1999;Polkinghorne,1988;Ricoeur,2008;Sørlie,2001).Oneoftheproblems
withretrospectiveinterviewsisthatparticipantsmayreconstructthepastwitha
frameworkthattheyhavelearnedlater.Ontheotherhand,narrativeinterviewsgive
participantstheopportunitytospeakaboutwhatisimportantforthemfromtheir
memory(Sørlie,2001).Assuch,thenarrativeinterviewmethodisanimportantwayto
obtaininformationaboutparticipants’experiences.
Nevertheless,theresearchinterviewisalsoasituationwhereparticipantsenacttheir
identitiesthroughtalking,wantingtopresentthemselvesasexperienced,moraland
knowledgeable.Theymaythereforebetemptedtowithholdexperiencesthatmight
proveotherwise(Gullestad,1996;Jordens&Little,2004;Ricoeur,1992;Torjuul,2009).
However,thestudyresultsdidnotgivethisimpression.Inseveraltouchingnarratives,
thenursestoldabouttheiruncertainty;ambiguityandvulnerabilityrelatedto
alleviatingdyingpatients’spiritualandexistentialsuffering.Astheauthorsdidnot
knowthenursespersonally,thismayhavehelpedthemtoexpressthemselvesfreely.
7.3.2Thetrustworthinessofthedataanalysis
Thetrustworthinessofthedataanalysiscanbejudgediftheresearcherisopenabout
howthestepsintheanalysiswerecarriedout(Benzein,1999).Inallthreepapers,care
wastakentodescribethestepsinthephenomenologicalhermeneuticalanalysisto
allowthereadertofollowtheprocessfromthenaïvereading(step1)throughthe
structuralanalysis(step2)towardsthecomprehensiveunderstanding(step3)
(Lindseth&Norberg,2004).
Sincetheaimofthephenomenologicalhermeneuticalanalysisistoobtainthemeaning
thatisopenedupinfrontoftheinterviewtext,-nottosearchfortheparticipants’
meaningsorauthorialintent(Lindseth&Norberg,2004;Ricoeur,1976),the
researchers’interpretationscannotbereturnedtotheparticipantsforvalidationin
ordertoincreasethetrustworthinessoftheinterpretation(Riessman,1993;

33
Sandelowski,1993).Instead,validationisaccomplishedthroughthestructuralanalysis,
wheretheresultsfromthestructuralanalysisarecomparedwiththeinitial
interpretationsstemmingfromthenaïvereadingsinstep1.Thestructuralanalysisis
theobjectivepartoftheinterpretation(Lindseth&Norberg,2004;Ricoeur,1976,pp.
82-88).
Itisimportanttonotethataninterpretiveconstructionreliesoncluescontainedwithin
thetextthatpointtotheirmeaning.Thesecluespermitaninterpretationbecausethe
clueseithermakesenseorinhibitaninterpretationbecausetheydonotfit(Ricoeur,
1976).Ricoeur(1976,2008)emphasizesthatatexthasmultipleinterpretations,and
thatallinterpretationsarenotequal.Becausetherearemultiplepossiblemeanings
withinatext,theinterpretersmustmakechoicesaboutcompetinginterpretationsand
thedifferentpossibilitiesofnamingandframingthem(Torjuul,2009).Following
Ricoeur,researchersneedtoappreciatethatnosingleinterpretationcaneverexhaust
themeaningofatext.Everyinterpretationisthereforeanapproximation.Accordingly,it
istheresearchers’tasktoarguefortheirinterpretation(Benzein,1999;Geanellos,
2000).
Inordertoarriveatthemostplausibleofcompetinginterpretations,alloftheauthors
readtheinterviews,followedthepathsintheanalysisanddiscussedpossible
interpretationsuntilaconsensuswasreached.Thiskindofresearchercooperationis
calledanalysttriangulation(Benzein,1999;Patton,1990).Analysttriangulationis
aimedatreducingthepotentialbias,whichmayoccurwhenasingleresearchercollects
andinterpretsthedata.Analysttriangulationprovidesameansofmoredirectly
assessingthereliabilityandvalidityoftheresults(Benzein,1999).Theauthors’
cooperationandcriticaldiscussionsgavethemawiderframeofreference(horizon)to
interpretthetexts,sinceitenabledthemtoquestioneachother’sinterpretations.
LindsethandNorberg(2004)emphasizethattheresearchermustcheckwhetherthe
resultsfromthestructuralanalysisvalidateorinvalidatetheinitialnaïveunderstanding.
Ifthestructuralanalysisinvalidatesthenaïveunderstanding,thewholetextmustbe
rereadtodevelopanewnaïveunderstanding.Thenewnaïvereadingmustthenbe
checkedbyanewstructuralanalysis.Theresearchermustrepeattheprocessuntils/he
34
experiencesthatthenaïveunderstandingisvalidatedbythestructuralanalysis
(Lindseth&Norberg,2004).Theauthorscheckedthethemesfromthestructural
analysisinrelationtotheirnaïvereadings,whichwerefoundtobeconsistentwiththeir
initialnaïveunderstanding.Thisstrengthenedthetrustworthinessoftheir
interpretations.ThethemesarepresentedintheResultssectioninthethreepapers.
Somenurseresearchersclaimthatusingaphenomenologicalhermeneuticalmethodto
analyzefocusgroupinterviewsisacontroversialchoice.Criticsstatethat
phenomenology’semphasisonindividual,livedexperienceisinconsistentwithgroup
approaches(Webb,2003;Webb&Kevern,2001).Thiscontroversyhasbeenthoroughly
discussedinpaperIwheretheauthorsarguethatthefocusgroupapproachdoesnot
excludeindividualperspectivesandthatsubjectingfocusgroupinterviewsto
phenomenologicalhermeneuticalanalysisisconsistentwithRicoeur’s(1976)
interpretationtheorybecausetheaimofthephenomenologicalhermeneuticalanalysis
istointerpretthemeaningoftheinterviewtext,ratherthantheexperienceofindividual
participants(Lindseth&Norberg,2004;Ricoeur,1976).Thefirstauthor,whoconducted
theinterview,madesurethatalloftheteammemberswereheardandencouragedthe
lessvociferoustotalkabouttheirexperiencesinordertocapturethewholegroup’s
experienceasateachingteam.
7.3.3Rationaleforconductingaphenomenologicalhermeneuticaldataanalysis
Differentepistemologicalperspectivesandpluralismhavecreatedanarrayof
qualitativeapproaches,suchasgroundedtheory,variousformsforphenomenology,
ethnography,actionresearchandqualitativecontentanalysis.Thereisaconsiderable
overlapamongavailableapproachesintermsofmethods,proceduresandtechniques.It
canthereforebechallengingforresearcherstodeterminewhichapproachismost
suitabletoanswertheirresearchquestions(Vaismoradi,Turunen,&Bondas,2013).
Inthisstudywechosetoapplyaphenomenologicalhermeneuticalmethod(Lindseth&
Norberg,2004)toanalyzetheinterviewtexts.Itcouldalsohavebeenpossibletouse
qualitativecontentanalysis(Graneheim&Lundman,2004).Initially,thismethod
focusedonanalyzingthemanifestcontent,-whattheinterviewtextsays,itsvisible,
obviouscomponents(Graneheim&Lundman,2004,p.106).-orinRicoeur’sterms“its
35
sense”(Ricoeur,1976,pp.19-23).However,overtime,qualitativecontentanalysishas
expandedtoincludeinterpretationsofwhatthetexttalksabout,-itslatentcontent
(Graneheim&Lundman,2004,p.106),-orinRicoeur’sterms“thetext’sreference”
(Ricoeur,1976,pp.19-23).Assuch,phenomenologicalhermeneuticalanalysis(Lindseth
&Norberg,2004)andqualitativecontentanalysis(Graneheim&Lundman,2004)seem
toshareacommonaimofanalyzingnarrativematerialsbybreakingthemintorelatively
smallunitsofcontentandsubmittingthemtodescriptiveandinterpretativetreatment.
However,accordingtoSandelowskiandBarroso’s(2003)typologyofqualitative
studies,qualitativecontentanalysisemploysalowerlevelofinterpretationthan
phenomenologicalhermeneuticalapproaches.Theauthorsthereforejudgedthatit
wouldbemoresuitabletoapplyaphenomenologicalhermeneuticalmethodtoanalyze
theinterviewtextsbecausethestudy’soverallaimto“illuminatethemeaningof
registerednurses’experienceswithpracticingandteachingspiritualandexistentialcare
forthedying”demandedamethodwhichemploysahighlevelofinterpretive
complexity.AsvanManen(2014,p.226)notes:”Thephenomenologicalstudyoflivedor
existentialmeaningsattemptstodescribeandinterpretthesemeaningstoacertain
degreeofdepthandrichness.”
UsingLindsethandNorberg’s(2004)phenomenologicalhermeneuticalmethodto
interpretthenarrativeinterviewsprovedtobeagoodchoiceforthisstudy,becauseit
enabledtheauthorstointerpretthenurses’livedexperience.Theinterpretations
providedafruitfuldeparturepointtodevelopacomprehensiveunderstandingaboutthe
meaningofthenurses’experienceswithpracticingandteachingspiritualandexistential
careforthedying.
However,asmentionedearlier,phenomenologicalhermeneuticalresearchersmust
“bracket”theirjudgmentsaboutthefactualinnarrativeinterviewtextsinorderto
disclosethetexts’essentialmeaning.Itisimportanttonotethatbracketingone’s
judgmentisnotthesameasbracketingone’spreunderstanding(Lindseth&Norberg,
2004).DrawingonRicoeur(1976),LindsethandNorberg(2004)pointoutthatevery
humanbeinghasanimplicitpreunderstandingoflifewhichtheycannotfreethemselves
fromandthatresearcherscanonlyunderstandandinterprettheirinformants’
narrativesinrelationtotheirownpreunderstandings.Accordingly,tostrengthena

36
phenomenologicalhermeneuticalstudy’strustworthiness,researchersmustreflect
criticallyanddocumenthowtheirpreunderstandingshaveinfluencedtheresearch
processandthedatainterpretation.Thiswillbepresentedinthefollowing:
7.3.4Mypreunderstanding
AsmentionedinChapter4.2,whenIbeganmyresearch,Ihadapreunderstandingof
spiritualandexistentialcare,whichhadevolvedthroughmyownnursingexperiencein
palliativecareandmytheoreticalframeofreferenceinnursingandnarrativetheology.
Inretrospect,Iseethatthisbackgroundhashaditsadvantagesaswellasdisadvantages.
Ontheonehand,beinganursewithpalliativespiritualandexistentialcareexperience
gavemeanassetasaresearcher,becauseitenabledmetoestablishtrustandrapport
withthenurses.Comingfromthesamebackground,helpedmetocommunicatewith
them.Iexperiencedthatthenursesopenedupandtalkedquitefranklywithmeabout
theirchallengesandstrugglesbecauseIwas“oneofthem”.(Iinformedthembriefly
aboutmybackgroundwhenIpresentedmyselfatthebeginningofeachinterview.)
However,beingviewedas“oneofthem”,alsohaditschallenges.Whenthenursestold
memovingstories,Ioftenfeltthattheyappealedtomeforrecognition,whentheyheld
mygazeandsaidthingslike:“…-youknowwhatImean…!!?”Thiswasespecially
challengingduringmyfirstinterviews,becauseIwasnewtotheroleastheresearcher.I
quicklydiscoveredthatIwastemptedtorespondspontaneouslytotheirappealsasa
fellownurse,andIexperiencedthatIhadtomakeaconsciousefforttoinhibitmy
reactionsinordertomaintainmyroleasaresearcher.Resistingthetemptationto
confirmthatI“absolutelyunderstoodthem”asafellownurse,Imadeanefforttosettle
backandencouragethenursestotellmemoreabouttheirexperiences.Aimingtobe
faithfultoLindsethandNorberg’s(2004)method,Istrovetobracketmythoughtsand
feelingsasmuchaspossible,inordertorefrainfromjudgingorcomparingthenurses’
storieswithmyownnursingbackground(duringtheinterviewsandthroughoutthe
interpretationprocess).Iexperiencedthatthiswasabsolutelynecessaryinorderto
listenactivelyandfocusonthemeaningofthenurses’experiences.Thiscouldbe
especiallychallengingwhentheirstoriesevokedsomeofmyownmemoriesaboutdying
patientswhohadtouchedmedeeply(Tornøe,1996).

37
Duringmyfirstinterpretationattempts,IdiscoveredthatItendedtooverlaythe
interpretationswithmyownnursingexperienceandtheoreticalpreunderstandings.
However,asIgainedproficiencyintheinterpretationmethod,Iwasgraduallyabletolet
goofmynaturalattitude(already“knowing”inlightofmypreunderstanding)to
cultivateamoreopenphenomenologicalattitude(Lindseth,2015;Lindseth&Norberg,
2004).Iexperiencedthatthedialecticalprocessofcomparingmystructuralanalyses
withmyinitialnaïvereadingsexpandedmyinterpretativehorizon.Ibelievethis
reducedtheimpactofmypreunderstandingsandhelpedmetoexploreandinterpretthe
essentialmeaningsintheinterviewtranscripts.
7.3.5Studylimitations
Asthisisaqualitativestudy,itisnotreasonabletodiscusstheconceptsofvalidity,
reliabilityandgeneralizabilityintheirtraditionalsenses.Thenumberofinformantsin
qualitativeresearchprojectsisnotsufficienttoallowforgeneralizedconclusions.
However,theydoinsurestrengthandrepresentativityinrelationtotransferability,as
theypermitanin-depthinsightintothephenomenaunderstudy.Qualitativeprojects
canthereforebestatedtoshowahighcontentvalidity.Thismeansthatthereisahigh
degreeofdetailinthedata(Dehlholm-Lambertsen&Maunsbach,1997).Threetofive
informantsaresufficienttoachieveahighcontentvalidity(Kvale&Brinkmann,2008;
Mishler,1986).Ourdecisionaboutthesamplesizewasguidedbytheneedtoensurea
varietyofin-depthexperiences.Sincequalitativestudiesarenotdesignedtobe
representativeintermsofstatisticalgenerability,theymaygainlittlefromexpanding
samplesizeexceptamorecumbersomedataset,allowingforlessdepthandrichnessto
beextractedfromthematerial(Carlsen&Glenton,2011;Pope,Ziebland,&Mays,2000).
Eventhoughtheresultsinthisstudycannotbegeneralized,theresultsaredeemedas
credibleortrustworthyifpeoplewithsimilarexperiencescanrecognizetheresultsof
thestudy(Benzein,1999;Sandelowski,1993;Sørlie,2001).Inconclusionhowever,one
canargueforandagainsttheinterpretationofthisparticularphenomenological
hermeneuticalstudy,astheresultsthatarepresentedareonlyoneofseveralpossible
interpretations:

38
Aninterpretationmustnotonlybeprobable,butmoreprobablethananotherinterpretation…Itisalwayspossibletoarguefororagainstaninterpretation,toconfrontinterpretations,toarbitratebetweenthemandtoseekagreement,evenifthisagreementremainsbeyondourimmediatereach.(Ricoeur,1976,p.79)
Althoughthehospicenursesinthefirstpapermentionedthattheysometimeshad
Muslimpatientsandthattheyweresensitivetothesepatients’spiritualandexistential
needs,theyhadlimitedexperiencewithspiritualandexistentialcareforpatientsfrom
differentethnicbackgroundsand/orreligioustraditions(paperI).ThestudyinpaperII
wasconductedinasmallruralNorwegiantownwherethemajorityofthepopulation
consistedofethnicNorwegians.NoneoftheparticipantsinpaperIIandIIImentioned
thattheyhadprovidedspiritualandexistentialcaretopatientsfromotherethnic
groupsorreligiousfaiths.TheparticipantsinallthreepaperswereethnicNorwegians.
Duetothestudy’sgeographicalandculturalcontextthestudyislimitedtothe
participants’experienceswithprovidingspiritualandexistentialcaretoethnic
Norwegianpatients.AlthoughNorwayisbecominganincreasinglypluralisticand
multiculturalsociety(Botvar&Schmidt,2010;Aadnanes,2008),approximately73%of
thepopulationhaveanaffiliationtotheChurchofNorway(StatistiskSentralbyrå
(CentralBureauofStatisticsinNorway),2015).Henceforth,theresultsfromthisstudy
arestillrelevantinspiteoftheselimitations.

39
8.Thestudy
AccordingtoHalcomb,Gholizadeh,DiGiacomo,Phillips,andDavidson(2007),itis
importanttoselectpotentialparticipantsthatareabletoprovideinsightintoand
informationabouttheresearchtopicandthattheyareabletoarticulatetheir
perspectiveonrelevantissues.
PaperIandpaperIIexplorehospicenurses’andregisterednurses’spiritualand
existentialcareexperienceswithinthespecializedlevelsofcare,whilepaperIIIexplores
amobilehospicenurseteachingteam’sexperienceswithteachingandsupervisingcare
workersinspiritualandexistentialcarewithintheprimarylevelsofcare.These
healthcarecontextswerechosentocaptureabroadestpossiblerangeofnursing
experiencesrelatedtopracticingandteachingspiritualandexistentialcareforthe
dying.
Forthefirstpartofthestudy(paperI),eightexperiencedhospicenursesfroma
leadingNorwegianhospiceinamajorcitywererecruited.Sincehospicenurseswork
withdyingpatients,itseemedreasonablethatthesenurseswouldbeabletoprovide
richnarrativesabouttheirexperienceswithspiritualandexistentialcareforthedying.
Forthesecondpartofthestudy(paperII)sixregisterednursesfromamedicaland
oncologicalwardinageneralhospitalwererecruited.Incontrasttohospicenurses,
hospitalnursesmustmaintaincurativeresponsibilitiesforpatientswhileatthesame
timecaringforthedyingaspartoftheirdailywork(Costello,2006).Inthisward,eight
bedswereespeciallydesignatedforpatientswithadvancedstagesofcancer.The
authorsassumedthatthesenurseswouldhaveexperiencedthetensionbetween
managingcurativeresponsibilitiesandprovidingspiritualandexistentialcareforthe
dying.
Forthethirdpartofthestudy(paperIII)threehospicenursesinamobilespiritual
andexistentialcareteachingteamwererecruited.Thefourthauthorwasfamiliarwith
themobileteachingteamfrompreviousresearchprojectsatthehospiceandknewthat
theywereableandwillingtoparticipateinresearch.AsNorway’sfirstandonlymobile
spiritualandexistentialcareteachingteam,thesehospicenursespossessedaunique

40
experiencewithtrainingcareworkersinspiritualandexistentialcareforthedyingin
nursinghomesandhomecare.
Anoverviewofthestudy,participantsandpaperscomprisingthisthesisisshownin
table1.
Table1:Overviewofthestudy,participantsandpapersTheStudy Participants Data
collectionInterpretationMethod
Papers Focus
TheHospice Eighthospicenurses
Individualnarrativeinterviews
Phenomenologicalhermeneutical
PaperI Experienceswithpracticingspiritualandexistentialcareforthedying
Medicalandoncologicalwardinageneralhospital
Sixregisterednurses
Individualnarrativeinterviews
Phenomenologicalhermeneutical
PaperII Experienceswithpracticingspiritualandexistentialcareforthedying
Themobilehospicenurseteachingteam
Threehospicenurses
Narrativefocusgroupinterview
Phenomenologicalhermeneutical
PaperIII
Experienceswithtrainingcareworkersinspiritualandexistentialcareforthedying
8.1ThesettingThefirstandthirdpartsofthestudy(paperIandpaperIII)wereconductedwith
hospicenurseswhowereemployedinthesameleadinghospiceinamajorNorwegian
city.Thehospicewasanintegratedunitinasomatichospital.Thehospicenursesin
paperIperformedbedsidenursinginthehospice,whilethehospicenursesinpaperIII,
workedoutsidethehospice,ambulatingbetweenthecity’snursinghomesandhome
caresettingstoteachandtraincareworkersinspiritualandexistentialcare.Thesecond
partofthestudy(paperII)wasconductedwithregisterednurseswhoworkedina
medicalandoncologicalwardinageneralhospital.Thehospitalwassituatedinarural
Norwegiantown.
41
8.2RecruitmentstrategyApurposivesamplingstrategy(Devers&Frankel,2000;Patton,2002)wasappliedto
recruitkeyinformantsfromthechosenhealthcarecontextsinordertofulfilltheoverall
aimofthethesis.Theinclusioncriteriawerethatthenurseswereinterestedinpalliative
careandthattheyhadawidevarietyofexperienceswithspiritualandexistentialcare
fordyingpatients.Inaddition,thenursesinthethirdpartofthestudyalsoneededtobe
experiencedteachersandsupervisorsinspiritualandexistentialcareforthedying.
Forthefirstandthirdpartofthestudy(paperI,andpaperIII),theauthorscontacted
thehospiceleaderandobtainedherpermissiontocarryouttheresearch.Sheassistedin
recruitingparticipantsbyinformingthehospicenursesaboutthestudyandforwarded
theauthors’informationsheetandformalwrittenrequesttoparticipateinthestudy.
Thefirsteighthospicenursesthatsignedupforthestudywereinterviewed.Torecruit
participantsforthelastpartofthestudy(paperIII),thehospiceleaderaskedthethree
hospicenursesinthemobilespiritualandexistentialcareteachingteamiftheywanted
toparticipateinthestudyandsheforwardedtheauthors’informationsheetandformal
writtenrequesttoparticipateinthestudy.Torecruitnursesforthesecondpartofthe
study(paperII),theauthorscontactedtheheadnurseinthemedicalandoncological
hospitalwardandobtainedherpermissiontocarryouttheresearch.Sheassistedin
recruitingparticipantsbytellingthenursesaboutthestudyandsheforwardedthe
authors’writteninformationandformalrequesttoparticipateinthestudy.Thefirstsix
nursesthatsignedupforthestudywereinterviewed.
8.3ThesampleTheeightparticipantsinpaperIwereexperiencedhospicenursesbetweentheages
offorty-oneandsixty-oneyears,witheighttothirty-fiveyearsofnursingexperience.
Everyoneheldnursingdegreesespeciallyrelevantforpalliativecare,suchaspalliative
careandoncologynursing.
ThesixparticipantsinpaperIIwereexperiencedregisterednursesbetweentheages
ofthirty-sevenandsixty-oneyearswithninetotwentyyearsofnursingexperience.
Fourofthemhaddegreesinoncologynursingandpalliativecare.
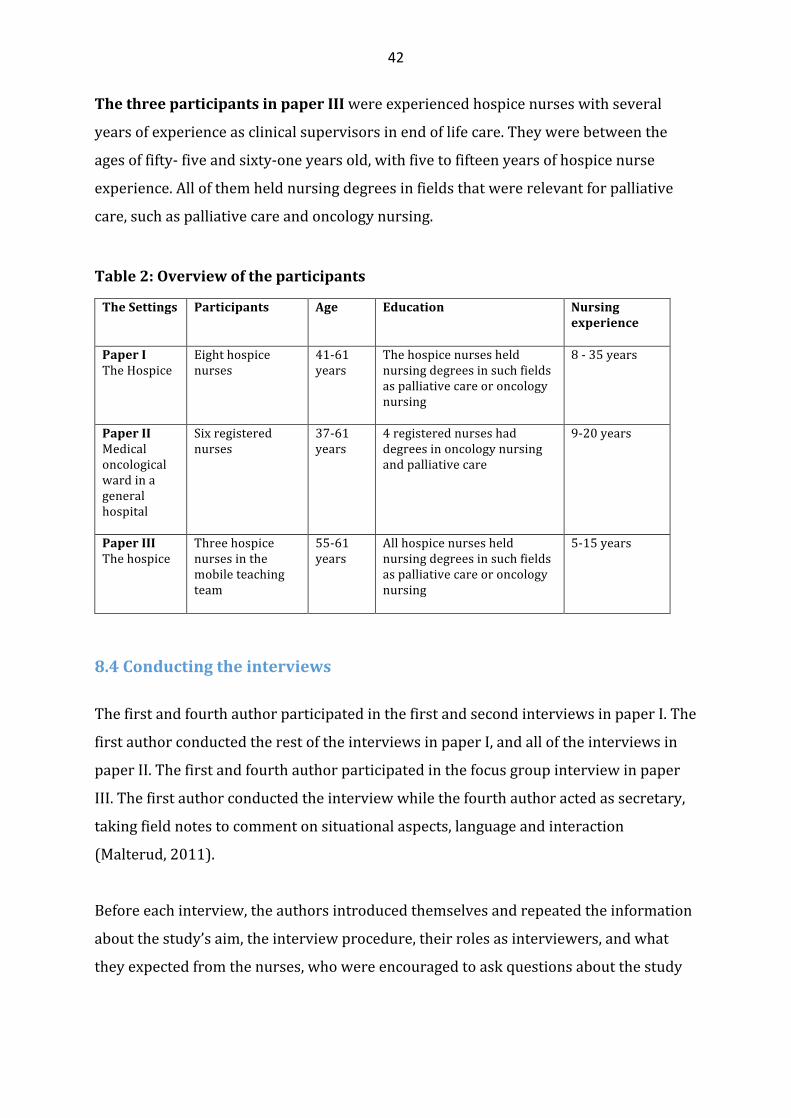
42
ThethreeparticipantsinpaperIIIwereexperiencedhospicenurseswithseveral
yearsofexperienceasclinicalsupervisorsinendoflifecare.Theywerebetweenthe
agesoffifty-fiveandsixty-oneyearsold,withfivetofifteenyearsofhospicenurse
experience.Allofthemheldnursingdegreesinfieldsthatwererelevantforpalliative
care,suchaspalliativecareandoncologynursing.
Table2:Overviewoftheparticipants
TheSettings
Participants Age Education Nursingexperience
PaperITheHospice
Eighthospicenurses
41-61years
Thehospicenursesheldnursingdegreesinsuchfieldsaspalliativecareoroncologynursing
8-35years
PaperIIMedicaloncologicalwardinageneralhospital
Sixregisterednurses
37-61years
4registerednurseshaddegreesinoncologynursingandpalliativecare
9-20years
PaperIIIThehospice
Threehospicenursesinthemobileteachingteam
55-61years
Allhospicenursesheldnursingdegreesinsuchfieldsaspalliativecareoroncologynursing
5-15years
8.4Conductingtheinterviews
ThefirstandfourthauthorparticipatedinthefirstandsecondinterviewsinpaperI.The
firstauthorconductedtherestoftheinterviewsinpaperI,andalloftheinterviewsin
paperII.Thefirstandfourthauthorparticipatedinthefocusgroupinterviewinpaper
III.Thefirstauthorconductedtheinterviewwhilethefourthauthoractedassecretary,
takingfieldnotestocommentonsituationalaspects,languageandinteraction
(Malterud,2011).
Beforeeachinterview,theauthorsintroducedthemselvesandrepeatedtheinformation
aboutthestudy’saim,theinterviewprocedure,theirrolesasinterviewers,andwhat
theyexpectedfromthenurses,whowereencouragedtoaskquestionsaboutthestudy
43
andtheinterviewprocedure.Personalinformationabouteachnursewasobtainedand
writtendown,andthenursesgavetheirwrittenconsent.
TheinterviewswiththehospicenursesinpaperIandpaperIIItookplacein2012and
wereheldinthehospicemeetingroom.Theinterviewswithregisterednursesinpaper
IItookplacein2014andwereheldinameetingroomoutsidethenurses’medical-
oncologicalward.TheindividualinterviewsinpaperIandpaperIIlastedapproximately
onehour.ThefocusgroupinterviewinpaperIIIlasted80minutes.Alloftheinterviews
tookplaceduringthenurses’workinghours.Theinterviewswererecordedand
transcribedverbatimbythefirstauthor.
8.5EthicalconsiderationsThestudywasconductedaccordingtotheHelsinkideclaration(WorldMedical
Association,2001).ApprovalwasobtainedfromtheNorwegianCenterforResearch,
(Norsksamfunnsvitenskapeligdatatjeneste),projectnumber29973.Theethical
considerationsthroughouttheresearchprocesswasinformedbytheHelsinki
declaration(WorldMedicalAssociation,2001)andtheNorwegianCenterforResearch
Data’spolicyandguidelines(NSD,2016).
Theauthorsdistributedaformalwrittenrequestandashortinformationsheetabout
thestudytothenurses.Theinformationsheetdescribedthestudy’saimand
backgroundandexplainedthattheinterviewswouldberecordedandtranscribed
verbatim.Measurestoensureconfidentialityandanonymitywerealsodescribed.The
informationsheetalsostatedthatthenurseswerefreetowithdrawtheirconsentatany
giventime,duringoraftertheinterview.Theinformationwasrepeatedbeforeeach
interviewstarted.Measurestoensureconfidentialityandanonymityrelatedto
publicationwererepeatedandemphasized.Allofthenursesgavetheirwritten,
informedconsenttoparticipateinthestudy.
TheHelsinkideclaration’sethicalguidelinesforhealthcareresearch(WorldMedical
Association,2001)emphasizetheresearcher’sdutytoprotecttheparticipants’life,
health,privacy,dignityandrespect.Italsostressestheimportanceofsafeguarding

44
vulnerableanddisadvantagedindividualsfromthepotentialrisksofthestudyandthe
discomfortitmayentail.Thenursesinthisstudydidnotbelongtoavulnerableor
underprivilegedgroupinsociety,norcantheybesaidtoneedspecialprotectionfrom
theresearcher.However,patientsandtheirlovedonesplayedanimportantroleinthe
nurses’narrativesandwereatriskofbeingexposed.Thisdidnotcauseanyethical
problemsbecausethenursesmadeanefforttopreservepatients’,familymembers’and
colleagues’confidentialityandanonymitywhentheytalkedabouttheirspiritualand
existentialcareexperiences.Thenursesdidnotdiscloseanynamesintheinterviews
andtheyoccasionallyomitteddetailsfromtheirstoriestosafeguardanonymityand
confidentiality.
InScandinaviancountries,spirituality,religionandexistentialissuesareconsideredto
beprivateandsensitivefieldsofenquiry(Botvar&Schmidt,2010;DeMarinis,2008;la
Cour,2008;Aadnanes,2008).Itwasthereforeimportanttobesensitivetothisduring
theinterviewsbecauseoftheasymmetryofpowerintheinterviewee–interviewer
relationship(Mishler,1986).Choosingthenarrativeinterviewmethodwasawayto
rebalancethepowerstructurebetweentheresearcherandthenurses,becausewhena
researcherencouragesintervieweestonarrateabouttheirexperiences,s/heisalso
encouragingthemtofindandspeakintheirownvoice(Mishler,1986).

45
9.MainresultsinPapersI-III
9.1PaperIThenursesdescribedtheirpatients’sufferingasakindof“totalpain”,whichincluded
emotional,spiritualandexistentialdistressandphysicalpain.Theytoldthatthismadeit
difficulttosortoutspiritualandexistentialsuffering.Alleviatingphysicalsymptoms
wasimportant,sinceuncheckedphysicalpainwoulddrainthepatients’energytofocus
onspiritualand/orexistentialconcerns.Thenursessaidthattheyneededagoodsense
oftiming,situationalunderstandingandtheabilityto“senseandtuneinon”patients’
verbalandnon-verbalcuesduringnursingcare,inordertopickupeachpatient’s
existentialand/orspiritualdistressandtorespondadequatelytotheirneeds.
Accordingtothenurses“beingthere”fortheirpatientsliedattheheartoftheirspiritual
andexistentialcarepractice.“Beingthere”wasaboutconveyingconsolationthrough
silentpresencing,companionship,deepexistentialandreligiousconversations,andby
supportingpatients’expressionsoffaithandrituals.Thenursesexpressedthatbuilding
trustingrelationships,easingsuffering,andhelpingpatientsandtheirfamiliestofind
peace,acceptanceofdeathandreconciliation,wasdeeplymeaningfulandrewarding.
Thenursessawthatpatientswhowereunabletoexpresstheirthoughtsandfeelings
aboutdeathcouldbecomestuckinstatesofanxietyanddenial.Itwasthenurses’
impressionthatpatientswhovoicedtheirdistressdiedmorepeacefullythanthosewho
“bottledeverythingup,andtheydescribedanethicaldilemmabetweentheirwishto
helppatientsfindpeaceby“nudgingthemtoopenup”andacceptingthatsomeofthem
wouldnotorcouldnotsharetheirsuffering(p.3).Thenurseswereconcernedaboutthe
riskofviolatingtheirpatients’autonomyandintegrity,andtheystressedthattheywere
boundbytheirprofessionalethicstorespecttheirpatients’choices.Thenurses
expressedthatitwasdeeplypainfulwhentheywereunabletoreachintotheirpatients.
Bearingwitnesstodyingpatients’sufferingandpain,inspiteoftheirconsolationefforts
wasemotionallychallengingbecauseitmadethenursesfeelhelplessandvulnerable.
Theythereforeplacedgreatimportanceondebriefingandsupportfromtheircolleagues
inordertoenduretheemotionaldemandsofbeingwiththedying.

46
9.2PaperII
Thenursesexperiencedthatdyingpatients’spiritualandexistentialsufferingemerged
assubtleandelusiveentanglementsofphysical,emotional,relational,spiritualand
existentialpain.Thenursestoldthatspiritualandexistentialsuffering(whichdidnot
alwaysincludereligiousaspects)couldemergespontaneously,forexampleduring
physicalcare.Theabilitytozoominonfleetingmoments,whenpatientswantedand
neededtotalkwasthereforeviewedasanessentialskill.
Thenursesstrovetoconveyconsolationbyunburdeningtheirpatientstofacilitatea
peacefulandharmoniousdeath.Theytoldthatthiscouldinvolvehelpingpatientsto
resolvepracticalworries,(i.e.completingahomerenovation),aswellashelpingthemto
makepeacewiththeirpast,theirlovedonesandwithGod(p.6).Thenursesfelttheyhad
beenabletoconveyconsolationwhentheysawthattheireffortshadhelpedpatientsto
experienceagood,peacefulandharmoniousdeath.Witnessingthepeacefulpassingofa
patientwasdescribedasaspecialmomentthatfilledthemwithreverenceandawe.This
wasexperiencedasveryrewardingandfulfilling.Thenursesweredeeplymovedand
amazedwhenpatientssharedtheirtrustandopenness:“SometimesI’mreally
astonishedthattheychoosetosharetheirtroublesandworrieswithme!Eventhough
I’mtheirnurse,I’mstillastranger!”(p.7)
Thenursesexpressedthattheyhadanimportantfunctionas“emotionalcontainers”
whentheylistenedandencourageddyingpatientstoventtheirfeelings.“Itdoesn’tdo
anyharmifpeoplestarttocry.Iusuallytellmypatientsthattheydon’thavetofeel
ashamedoftheirtears.Tearsareonlymeltingice!”(p.8).However,thenursesalso
statedthatbearingwitnesstopatients’spiritualandexistentialdistresscouldbe
challengingbecauseitexposedthemtotheirownfeelingsoffinitudeandvulnerability.
Bearingwitnesstounconsolablepatientsprovedtobethenurses’greatestemotional
challenge.Beingunabletohelppatientstowardsapeacefuldeathcouldmakethemfeel
professionallyinadequateandhelplessandtheyfeltthattheyhadnotdoneagood
enoughjob.However,thenursesalsoemphasizedthat,whatpatientsneededmost,were
nurseswhoshowedthattheywerewillingtostandbytheirpatients,andwouldnot
abandonthemintheirtimeofneed.

47
9.3PaperIIIAccordingtothemobilehospicenurseteachingteam,careworkersfrequently
expressedthattheywerereluctanttoaddressdyingpatients’existentialandspiritual
suffering.Theteamexperiencedthatcareworkerscouldbequiteafraidoftalkingwith
patientsabouttheirexistentialandspiritualconcerns.Theteamexpressedthatmanyof
themwereafraidofsilenceand“justbeingwith”thepatient“intheroomofdeath”(p.4-
5).Theteamthereforestressedtheimportanceofhelpingthecareworkersdevelop
theircourageandcompetencytoprovidespiritualandexistentialcare.Theteam
believedthatthecareworkers’fearanduncertaintystemmedfrompersonalinsecurity
aswellasinsufficientcommunicationandlisteningskills.Theythereforeplacedgreat
emphasisontherelationalaspectofspiritualandexistentialcarewhentheytaughtthe
careworkersto“workfromtheheart”.
Theteamtaughtcareworkerstoidentifypatients’spiritualandexistentialsuffering,
initiateexistentialandspiritualconversationsandtoconveyconsolationthroughsilent
presencingandactivelistening.Theteamtransferredtheirpersonalspiritualand
existentialcareknowledgebyparticipatingactivelyinpatientcaretogetherwiththe
careworkers,andbyprovidingsupervisionandfeedbackrelatedtothesesituations.
Thiswascalled“bedsideteaching”,whichcouldtakeplaceduringmanydifferentkinds
ofpatientencounters,suchasgivingphysicalcare,doingnursingprocedures,orjust
takingpartinconversationswithpatients.Theteamemphasizedthatcriticalreflection
wasanimportantpartofbedside“learningbydoing”.Theteamthereforeplacedgreat
weightonconductingreflectivedialogueswiththecareworkersabouttheirchallenges
andexperiencesbeforeandafterthepatientencounter(p.5).
Drawingoncareworkerfeedbackandtheirownobservations,theteamconsideredthat
situated“bed-sideteaching”hadproventobeanimportanttooltodevelopcare
workers’courageandcompetencytoprovidespiritualandexistentialcareforthedying.
Theteamobservedthatcareworkersbecamemoreinvolvedandwillingtoexpose
themselvestotheirpatients’spiritualandexistentialsuffering.Theteamthoughtthis
indicatedthatthecareworkershadbecomemorecourageous:“Iseethattheydareto
involvethemselvesmoreinthesesituations,exposingtheirvulnerability.Iseethatthey
havebecomebraver.”(p.6)

48
10.DiscussionInthisstudythenursesnarratedabouttheirlivedexperiencewithpracticingand
teachingspiritualandexistentialcarefordyingpatientsinthreedifferentNorwegian
healthcarecontexts.
Threethemesemergedthroughthecomprehensiveunderstanding,(discussion)ofthe
resultsinpaperI-III:Conveyingconsolation,Vulnerabilityandhelplessness,Compassion
andcourage.Todevelopthislaststepintheanalysis,thepaperswerereadasawhole,
takingintoaccounttheauthor’spreunderstanding,previousresearchandrelevant
theory.AlthoughconsolationdidnotemergeasanexplicitthemeinpaperIII,themobile
hospiceteachingteam’ssituatedbedsideteaching(p.3)provedtobeconsistentwiththe
consolationtheme,whichemergedinpaperI(p.3-5)andpaperII(p.7-8).
10.1ConveyingconsolationConveyingconsolationprovedtobeanoverarchingthemeinthestudy.Accordingto
Klass(2014),“solace”isunderstoodasasenseofsoothingwhichcaninvolvepleasure,
enjoymentordelightinthemidstofsorrow,hopelessnessanddespair,hencetobe
consoledistobecomforted.Theetymologyofthewordcomfort,carriesthesenseof
intersubjectivitybecauseitisderivedfromtheLatinfortis,whichmeansstrongor
powerfulandtheprefixcom,whichmeanswith(Klass,2014).Accordingly,toconsoleor
comfortanothermeanstostrengthenortofindstrengthtogether(Klass,2014,p.7).
Theresultsshowthatthenursesconveyedconsolationthroughactivepresencingand
relationshipmaintainingactivities,whichcouldinvolvegentlehandorfootmassages,
usingacaringtouchandlisteningandcommunicatingemphaticallywiththeirpatients
duringphysicalcare,orbyjustbeingwiththeminsharedsilence.Thenursesstroveto
createatrustingrelationalhaven,wherethedyingcouldfeelsafeenoughtoopen
themselvesandexpresstheirspiritualandexistentialdistress(paperIp.3-5andpaper
IIp.6-7).

49
ThenursesinpaperIandIIandthemobilehospicenurseteachingteaminpaperIII
emphasizedtheimportanceofseizing“thefleetingmoments”whenpatientsneededand
wantedtotalkabouttheirsuffering.Thenursesstressedthatthisdemandeda“fine
tunedantenna”(paperIIp.5),andthat“Ifyoudothingsproperlyandshowthatyou
care,existentialorspiritualdistresseventuallysurfacesifit’sthere”(paperIp.5).
Strivingto“getitright”thenursestried“totuneinon”theindividualpatient,paying
attentiontotheirenergylevelsandemotionalstates,neitherforcingnoravoiding
spiritualandexistentialconversations(paperIp.3).Themobilehospicenurseteaching
teaminpaperIIIplacedgreatemphasisonshowingthecareworkershowtousenatural
opportunitiesduringphysicalcaretoassessspiritualandexistentialneedsandto
integrateappropriateinterventions.Accordingtotheteachingteam,teachingthecare
workerstoaskpatientsthesimplequestion:“Howareyou?”couldbeenoughto“open
thedoortomeaningfulandsafedialogueswithpatientsabouttheirthoughtsand
feelings”(paperIIIp.5).Theteachingteamtaughtthecareworkerstolistenattentively
andtopayattentiontotheirpatients’facialexpressionsandbodylanguage.(paperIIIp.
5)
Theseresultssuggestthatconsolationcannotbeplanned,prescribedorimposedon
patientsthroughproceduralrulesand/orguidelines.Rather,conveyingconsolation
seemstobeadeeplypersonalandspontaneousactivity,whichdependsonthenurses’
andcareworkers’abilitytoapplytheirrelationalcompetence,creativityand
compassionateperceptivenessinordertotuneintotheparticularpatient’s
circumstances.ThisissupportedbyseveralSwedishconsolationstudies,(Norbergetal.,
2001;Roxberg,Eriksson,Rehnsfeldt,&Fridlund,2008;Söderberg,Gilje,&Norberg,
1999;Talseth,Gilje,&Norberg,2003),whichindicatethatconsolationcanonlybe
conveyedthroughcommunionanddialogueintrustingnurse-patientrelationships.
Whenthesufferingpatientbecomesopenandexpressessuffering,andwhenthenurse
mediatingconsolationbecomesopenandlistensinanemphaticandnon-judgmental
manner,theyareincommunionanddialogue.Duringthesemoments,thenurseandthe
patientmayexperiencemutualconsolation.Thesufferingpatientdrawsconsolation
fromthenurse’spresenceandthenursedrawsconsolationfromobservingthatthe
patient’sdistressedandanguishedstatemovestowardspeaceandtranquility(Norberg
etal.,2001).

50
10.1.1Thehermeneuticsofconsolation
AccordingtoNorbergetal.(2001,p.551),“theimportantprerequisiteforcommunionis
asharedaffectivestate,ratherthanasharedcognitiveinterpretationofthesituation.”
However,drawingontheworksofGadamer(2004)andRicoeur(1976,2008)itcanbe
arguedthatsharingthepatient’ssufferingalsorequiresaninterpretationaldialogue
aboutthemeaningofthepatient’ssuffering.Henceforth,conveyingconsolationthrough
communionanddialoguecanalsobeviewedasahermeneuticalactivity.Thiswillbe
explicatedinthefollowing.
InNorbergetal.’s(2001)consolationmodel,communionanddialogueislinkedtotwo
domains,-thepatient’sexperienceofhisorhersufferingandthenurse’sexperienceof
thepatient’ssuffering.Henceforth,sharingtheirexperienceofthepatient’ssuffering
requiresmorethanjustsharinganaffectivestate,becausethepatient’sexperience
cannotdirectlybecomethenurse’sexperience,andviceversa:
….whatisexperiencedbyonepersoncannotbetransferredwholeassuchandsuchexperiencetosomeoneelse.Myexperiencecannotdirectlybecomeyourexperience.Aneventbelongingtoonestreamofconsciousnesscannotbetransferredassuchintoanotherstreamofconsciousness.(Ricoeur,1976,p.16)
However,Ricoeur(1976)maintainsthatsomethingistransferredfromonesphereof
lifetoanother.“Thatsomething”isnottheexperienceasexperienced,butitsmeaning.
Henceforth,experienceaslived,remainsprivate,butitssense,itsmeaningbecomes
public(Ricoeur,1976).InRicoeur’swords:“….communicationinthiswayisthe
overcomingoftheradicalnon-communicabilityofthelivedexperienceaslived”
(Ricoeur,1976,p.16).Henceforth,thenursecanonlyinterpretthemeaningofthe
patient’ssufferingthroughcommunionanddialogue,inwhichsheexperiencesthe
patientassufferingornot(Kahn&Steeves,1986).AsGadamer(2004,p.292)points
out:“Thetaskofhermeneuticsistoclarifythemiracleofunderstanding,whichisnota
mysteriouscommunionofsouls,butsharingacommonmeaning”.Henceforth,drawing
onGadamer(2004)andRicoeur(1976,2008)conveyingconsolationthrough

51
communionanddialogue(Norbergetal.,2001)canbeunderstoodasakindofclinical
hermeneutics(Kahn&Steeves,1986).Humanactionsarelikeatextwhichawaitsfresh
interpretationsthatdecidetheirmeaning(Ricoeur,2008).Thus,allsignificantevents
anddeedsofhumanactionareopentoakindofpracticalinterpretation,whichisopen
toanybodywhocanread(Ricoeur,2008,p.151).FollowingRicoeur’s(1976,2008)
phenomenologicalhermeneuticallineofthought,theinterpretationofthepatient’s
sufferingdependsonthedialogicinteractionofthreeelements:thetext,thereaderand
thecontext:Thepatient’sexperienceofsufferingcanbeunderstoodasthetextwhich
thereader–nursemustinterpret,andviceversa(Kahn&Steeves,1986).Asthenurse
“reads”thepatient,thestory,andthebody,soalsothepatientalwaysengagesina
reversehermeneuticswherethepatient“reads”andinterpretsthenurse,andjudgeshis
orherinterestandcareforthepatientasauniqueperson(Schei,2006).
Cultural,spiritualandexistentialmeaningsthatthenurseandthepatientshareordo
notshareaboutsufferinginducingeventswillalsoinfluencehowtheyinterpretthe
meaningofthepatient’ssuffering.Inaddition,contextualfactorswithintheparticular
healthcaresetting,suchasphysical,psychologicalandsocioculturalenvironmental
features,alsoimpactonhowthenurseandthepatient“readandinterpret”themeaning
ofthepatient’ssuffering(DeMarinis,Ulland,&Karlsen,2011;Kahn&Steeves,1986;
Ulland&DeMarinis,2014).
Theresultsrevealthatthenurses’ownlifeexperiencesandpersonalbeliefsinfluenced
howtheyfeltaboutprovidingconsolation,especiallyrelatedtothepatients’religious
issues.Althoughthenursesacknowledgedthattheyhadaprofessionalobligationto
supportthepatients’sourcesoffaith,meaningandhope,regardlessoftheirownbeliefs,
someofthemhadmixedfeelingsaboutthisbecausetheywerenot:
veryreligiousor“veryChristian”astheyputit:“Actually,IfeelabituncomfortablewhenpatientstellmethattheyplacetheirlifeinGod’shands.Ithinkit’sprobablybecauseI’mnotabeliever.I’mveryskepticaltowardstheBibleandtheChristianfaith”.(paperIp.4)
Ingeneral,thenursesviewedreligionasaveryprivateandpersonalmatter,which
madethemwaryofimposingthemselvesontheirpatients(paperIIp.5-6).Somealso
saidthattheypreferredtoreferpatientstothehospiceorhospitalchaplainforreligious

52
supportbecausetheyfeltuncertainandinsecureaboutaddressingpatients’religious
concerns(paperIp.4,paperIIp.5,paperIIIp.4-5).TwoofthenursesinpaperIhad
pursuedtheologicalstudiespriortonursing.Theircolleaguesregardedthemasvaluable
resourcesbecausetheywereabletohelppatientswiththeirspiritualandexistential
distressbycombiningtheirpersonalfaithwiththeologicalknowledgeandpastoral
counselingskills.(paperIp.4)However,inspiteoftheirambivalence,thestudyshows
thatthenursesthoughtitwasimportanttoalleviatingtheirdyingpatients’spiritualand
existentialsufferingandtheystrovetoconsolethemasbesttheycouldwithintheir
limitedtimeandresources.(paperIIp.6)
10.1.2Therelationaldimensioninthenurses’consolationnarratives
Schei(2006)pointsoutthatatherapeuticalliancebetweentheclinicianandthepatient
emergesthroughreciprocalinterpretationandprojectionwheregestures,facial
expressions,intonation,pausesandeyemovementstypicallyconveymoreinformation
thanmerewords.Assuch,meaningistransmittedonseverallevelssimultaneously;
compassionandunderstandingmaybeexpressedthroughthelookinthenurse’seyes
orthetimbreofvoice,orthespeedoftalkingwhilefactualbusinessiscarriedoutinthe
explicitverballane.Bothparticipantsinadialoguemonitorthemselves,andtheother,
includingtheother’sapparentinterpretationsofone’sownutterances,incomplex
recursiveinterplay.Thus,thedialoguecontinuallyproducesnewmeanings,basedon
whathasalreadyhappenedintheconversationandinthenurse-patientrelationship.
Importantlessonsmaybegleanedfromtheseconsiderations(Schei,2006).Tothe
extentthatpatientswithorwithoutseriousdisease,alsosuffer,i.e.experiencemental
imbalance,isolation,grief,fearandotherfeelingscommonlyassociatedwithillness,pain
andexistentialloss,theresearchliteraturesuggeststhatbecomingapartofa
therapeuticalliancemayinitselfbeconducivetohealingandadaptation(Eells,1999;
Schei,2006).Moreover,Schei(2006)assertsthatthismaybeespeciallytrue–and
valuablewhenmedicaltechnologyhaslittletoofferinthewayoffurtherdiagnosticor
therapeuticprocedures.Henceforth,receivingconsolationthroughcommunionand
dialoguewiththenurse(Norbergetal.,2001)maybeoftherapeuticvalueforthedying.
Thiswillbediscussedinlightofthreeofthestudy’sconsolationnarratives.

53
1. Breakingtheboil
Inthefirstnarrative,adyingyoungcancerpatient“justwantedtofloatawayinadrug
daze.”(paperIp.4)Thenursedescribedthepatients’spiritualandexistentialpainas“a
largefesteringboil.“I’mnotsurehowwemanagedtopunctureitbecausewehadtrieda
lotofthings.”Oneday,thedoctorspontaneouslyaskedthepatientifshewasbitter
becauseshewasdyingsoyoung.Thedoctor’soutburstseemedtosnapthepatientoutof
herdrugdazebecausesheretortedthatshewasnotbittersinceherillnesshad“helped
hertogrowandmatureinwaysshecouldn’timagineevenifshehadlivedtoaripeold
age”.Accordingtothenurse,thisconversationbrokeopentheboilofsuffering,which
seemedtocreateaturningpointinthepatient’slife,becausesherosefromher
deathbed,reconnectedwithhersisterandmother,andwenthometoherflatonelast
timetosetheraffairsinorder.(paperIp.4)Andthenursethoughttoherself:“Yes!
Exactlythatquestionshiftedsomethingbecausenowwehadagirltakingbackherlife!”
2. Disappearingintoablackhole
Inthesecondnarrative(paperIIp.6),thenursetoldaboutawomanwhowasdyingof
lungcancer.Sensingheranxiety,thenurseaskedwhatshethoughtaboutdeath.The
patientfearedthatshewouldjust“disappearintoabigblackhole”whenshedied.“Isn’t
thereanythingmoreafterwards?”sheaskedthenurse.Thenursewasabletorelievethe
patient’sanxietybysharingherpersonalbeliefthatshewouldbereunitedwithher
lovedoneswhenshepassedaway.Accordingtothenurse,thepatientseemedtodraw
consolationfromthehopeofreunitingwithherdeceasedfather:“Perhapshe’sstanding
therewaitingforme!”sheexclaimed.Althoughthepatientseemedcalmer,shewasstill
worriedaboutnotbeingabletofinishrenovatingherfamily’shome.Toeaseher
worries,thenursecontactedthesocialworkerwhoorganizedherfamilyandfriendsto
completethejob.
3. ApunishmentfromGod
Thethirdandlastnarrative,whichwillbementionedhere,isanarrativeaboutadying
elderlywomanwhorefusedtoreceivemorphinebecauseshebelievedthatGodwas
punishingherthroughherpain.Inthiscasethenursehadtodealwiththepatient’s
religiousissuesbeforeshewaspermittedtorelievethepatient’sphysicalpain.

54
Desperatelysearchingforawaytoreachintothepatientitsuddenlydawnedonthe
nursethatshecoulduseprayer“toturnthesituationaround”assheputit.(paperIIp.
6)Sothenurseaskedthepatientifshewantedtosay“TheLord’sPrayer”withher.
Accordingtothenurse,sharingtheprayerhelpedhertoconnectwiththepatient,which
openedupanaturalopportunitytotalkwithheraboutherpictureofapunishingand
vengefulGod.Althoughthenurseclaimedthatshewasnot“veryreligious”sheshared
herbelieveinatrustingandlovingGod:“TheGodIbelieveinlovesusandwantstohelp
us!AndnowIcanhelpyoutotakeyourpainaway,-atleastsomeofit!–Ifyou’llletme!”
(paperIIp.7)Thenursethoughtthatthepatientseemedtodrawconsolationfromthe
prayerandtheconversation,becausesheacceptedtoreceivemorphineregularlyafter
that,andaccordingtothenurse,thepatientdiedpainfreeandatpeacewithGod.
Inthesenarrativesthepatients’spiritualandexistentialsufferingseemedtoevolve
aroundtheirdisconnectedrelationshipswithself,familymembersandwithGod.The
nursesthereforestrovetohelpthepatientstoreconnectandrestoretheirrelationships
by:
Ø Challengingthepatienttofacehersuffering,insteadofescapinginadrugdaze,
whichstimulatedthepatienttotakechargeofherlife,settleheraffairsand
reconnectwithhersisterandmother(narrative1)
Ø Helpingthepatienttoovercomeherexistentialfearandlonelinessrelatedto
dying,byconveyingahopeofreconnectingwithherlovedonesinthe“here
after”(narrative2)
Ø Helpingthepatienttomaintainherfamilytiesandresponsibilitiesrelatedto
completingtherenovationofherfamilyhome(narrative2)
Ø HelpingthepatienttoconnectwithGodandtoshiftherperceptionofGodfrom
vengefulandpunishingtocaringandloving(narrative3)
InthefollowingtheseresultswillbereflectedoninlightofSulmasy’s(2002)relational
perspectiveonsuffering.AccordingtoSulmasy(2002),illnessdisturbsrelationships
bothinsideandoutsidethebody.Inspiteofthis,contemporaryscientifichealinghas
untilrecentlybeenlimitedtorestoringthephysiologicalhomeostaticrelationships
withinthepatient’sbody,(suchasrestoringadiabetespatient’sbloodsugarbalancein
relationtootherbiochemicalprocesses).Illnesshowever,disturbsmorethanthe
55
relationshipsinsidethehumanorganism.Itcontributestosufferingbecauseitdisrupts
familiesandworkplaces.Itshatterspreexistingpatternsofcoping,anditraises
questionsaboutone’srelationshipwiththetranscendent(Sulmasy,2002).Accordingly,
illnessdisturbstherelationshipbetweentheindividualpatientandhisorher
environment,includingthefamilialandsocialnexusofrelationships,whichsurround
thepatientanditdisturbstherelationshipbetweenthepatientandthetranscendent
(Sulmasy,2002).ThisissupportedbyCassel’s(1991b)work,whichshowsthat
sufferinggeneratesexistentialloneliness,becauseitalienatesthesuffererfromhisor
herrelationshipswithothers,fromtheworldandfromhisorhertranscendentsourceof
meaning.AccordingtoSulmasy(2002)healingimpliesthatgenuineholistichealthcare
attendstoallofthedisturbedrelationshipsoftheillpersonasawhole,restoringthose
thatcanberestored,evenifthepersonisnotcompletelyrestoredtoperfectwholeness.
Thismeansthatattheendoflifewherethepatient’shealthnolongercanberestored,
healingisstillpossible(Sulmasy,2002).FollowingSulmasy(2002)theconsolation
narrativescanbeunderstoodashealingsincetheyinvolverestoringthepatients’
significantrelationshipstoself,othersandthetranscendent.Theresultssuggestthat
appropriateconsolationrequiresattentiontotherestorationofalltheintrapersonaland
extrapersonalrelationshipsthatcanstillbeaddressedevenattheendoflife(Sulmasy,
2002).
10.1.3ConveyingconsolationinrelationtoSpiritual/ExistentialandPsychosocialcare
Giventhenurses’strongfocusonhelpingtheirpatientstorestoredisconnected
relationshipsitcanbediscussedwhethertheconsolationnarrativesprimarilyare
concernedwithpsychosocialcare.Withinthepalliativecarecontext,psychosocialcare
hasbeendefinedasconcernwiththepsychologicalandemotionalwellbeingofthe
patientandtheirfamily/carers,includingissuesofself-esteem,insightintoand
adaptationtoillnessanditsconsequences,communication,socialfunctioningand
relationships(Tan,Wilson,Olver,&Barton,2011).Thereexistsathindividebetween
spiritual/existentialandpsychosocialcareinthepalliativecareliterature,becausethe
importanceofrelationshipsisemphasizedinbothdomains(Sinclair&Chochinov,2012;
Tanetal.,2011).Itisthereforeunderstandablethatpsychosocialandspiritual/
existentialissuestendedtooverlapinthenurses’consolationnarratives:“Shestill

56
worriedaboutherfamilybecauseshewasgoingtodiefromherkids,sointhiscase
unburdeningherwiththepracticalstuffwasanimportantpartofspiritualcare”
(narrative2,paperIIp.6).Thisissupportedbyotherstudies,whichsuggestthatin
clinicalpracticethespiritualdomaincoalesceswithotherdomainsandmaythereforebe
addressedthroughbothpsychologicalandspiritualmodalities(Sinclair&Chochinov,
2012,p.73).Itisthereforeinterestingtonotethattherelationaldimensioninthe
consolationnarrativesalsoresonatewithseveraldefinitionsthatexpressspiritualityin
relationalandtranscendentalterms.Puchalskietal.(2009)forinstance,define
spiritualityas:“theaspectofhumanitythatreferstothewayindividualsseekand
expressmeaningandpurposeandthewaytheyexperiencetheirconnectednesstothe
moment,toself,toothers,tonatureandtothesignificantorsacred”(Puchalskietal.,
2009,p.887).
ThisisinlinewithPargament(2013),whopointsoutthattherelationaldimensionof
spiritualitybecomesespeciallyapparentduringsacredmomentswhichare
characterizedbyadeepsenseofinterconnectednessandcaring.He(2013)maintains
thatsacredmomentsareextraordinarymomentswhennursescanseeintowhotheir
patientsareandtheycanseeintowhothenursesare.Duringthesemoments,thenurse
andthepatienttouchandaretouchedbyeachother.Assuch,sacredmomentsare
momentsofprofoundinterconnectedness(Pargament,2013).Thiscorrespondsto
Norbergetal.’s(2001)pointofview.Accordingtothem,consolationgivesafeelingof
meaning,homecomingandcontactwiththesacreddimension(transcendence).When
thenurseparticipatesinthepatient’spain,communionemerges.Norbergetal.(2001)
maintainthatcommunionisadeepconnectionthattouchesthesacreddimensionwhich
isakintoaconnectionwithsuchphenomenaasbeauty,joyandgoodness.Following
Pargament(2013)andNorbergetal.(2001),thenurses’consolationnarrativescanbe
understoodasdescriptionsofsuchsacredmoments.Itisimportanttonotethat
Pargament(2013)usestheterm“sacred”inapsychologicalratherthanatheological
sense.Accordingtohim(2013)“sacred”referstohumanperceptionsofqualitiesoften
associatedwiththedivineorhigherpowers.Healsopointsoutthattheseperceptions
donotreferonewayortheothertotheontologicalrealityofthesacred,higherpowers
orGod.Rather,theyreflectonhumancharacterandhumanrelationships(Pargament,
2013).Fromthisperspective,itcanbearguedthatnursesmayexperiencesacred

57
momentsintheirworkwhethertheyconsiderthemselvestobereligiousornot.
Henceforthitseemsreasonabletointerpretthenurses’consolationnarrativesas
“sacredmoments”inPargament’spsychologicalsenseoftheterm,althoughsomeofthe
nursesexpressedthattheydidnotexperiencethemselvesasvery“religiousor
Christian”(paperIp.4,paperIIp.6).
Rumbold(2003,p.S12),drawingonLartey(1997),describesspiritualityasthewebof
relationshipsthatgivecoherencetoourlivesandthatreligionmayormaynotbeapart
ofsuchaweb.Rumbold(2003)pointsoutthatoftenpeopleonlybecomeawareof
strandsinthewebwhentheyarestretchedorbroken,whichmayhappenduringlife-
changingeventslikeadiagnosisofseriousillnessinoneselforlovedones.Accordingto
Lartey(1997)citedinRumbold(2003),thiswebofrelationshipsinvolvesrelationships
withplacesandthings,withourselves,withsignificantothers,withgroupsor
communitiesandwithtranscendence.Theserelationshipsformauniquepatternfor
eachofus,andeachofusneedsthatpatterntobelargelyintactinordertofeelwhole.
ThisisconsistentwithSulmasy’s(2002)relationalunderstandingofhealing.Lartey
(1997),citedinRumbold(2003).maintainsthat:“Ourwebofkeyrelationshipsdefines
whoweare,andwhenthoserelationshipsaredisrupted,wefeelvulnerable.”Klass
(1999)citedinRumbold(2003)maintainsthatagoodwaytothinkaboutspirituallifeis
tolookforthosemomentswhenwefeelmostdeeplyconnectedtoourworld.Whenwe
feelleastisolatedinsideourusualegoboundaries,wefeelapartofsomethinglarger
thanourselves,andtherestoftheworldmakessense(Klass,1999).
10.1.4ConsolationthroughExistentialmeaningmaking
DrawingonFrankl(1969),Park(2013)pointsoutthatmeaningiswidelyregardedas
centraltohumanexperience.Iffundamentalrelationsorconditionsinlifearebroken,
sourcesofmeaningareusedtorestorethebalancebetweentheindividual’s
expectationsoflifeandtherealityasitisexperiencedhereandnow.Suchreappraisal
andusageofsourcesofmeaningareessentialwhenoneisconfrontedwithdemanding
lifesituations(Sørensenetal.,2015).Norbergetal.(2001)pointoutthatpeoplewho
suffer,experiencealossofmeaningandintegritybecause“everythingfallsapart”.
InspiredbytheexistentialphilosopherSørenKierkegaard,they(2001)statethatitis“in

58
thefearfulmomentsofdesolationwherethereisnomeaningleftthatabravestatement
ofconsolationpenetratesthedarknessandcreatesnewmeaning.Thishappensonthe
borderwherenothingispossibleanymore”(Norbergetal.,2001,p.545).Henceforth,
assistingpatientsintheirexistentialmeaningmaking,whichaccordingtoSchnell’s
(2009),researchmayormaynotinvolveatranscendentdimension,isalsoanimportant
partofconveyingconsolation.
Schnell(2009)definesmeaningfulnessasafundamentalsenseofmeaning,basedonan
appraisalofone’slifeascoherent,significant,directedandbelonging,andshe(2009)
categorizessourcesofmeaninginthefollowinggroups:Self-transcendence,which
concernsone’scommitmenttoobjectivesbeyondone’simmediateneeds.Verticalself-
transcendence,whichconsistsofreligionandspirituality,thatisorientatedtowardsan
immaterialcosmicpower.Horizontalself-transcendence,whichislinkedtotaking
responsibilityfor(worldly)affairsbeyondone’simmediateconcerns.Self-actualization
referstoemploying,challengingandfosteringone’scapacities.Orderislinkedtoholding
ontovalues,practicality,decencyandthetriedandtested.ThelastofSchnell’s(2009)
sourcesofmeaningiscategorizedaswellbeingandrelatedness,whichinvolves
cultivatingandenjoyinglife’spleasuresinprivacyandcompany.
Schnell’s(2009)researchonexistentialmeaningmakingtakesasecularEuropean
contextintoaccount(laCour,2008;laCour&Hvidt,2010),whichmakesitespecially
relevantforthestudy’sNorwegianhealthcarecontext,whereamajorityofthe
populationeitherdefinethemselvesas“secular”or“spiritualbutnotreligious”(Botvar&
Schmidt,2010;Aadnanes,2008).Inthefollowing,Schnell’s(2009)sourcesofmeaning
willthereforebeappliedtointerprettheconsolationnarratives.
Inthefirstnarrative(paperIp.4),thepatientwishedtowithdrawfromherexistential
sufferinginadazeofMorphineandStesolid.Inherconversationwiththepatient,the
doctoraskedthepatientifshewasbitterbecauseshewasgoingtodiesoyoung.By
confrontingthepatientwithhervulnerability,thedoctorliterally“heldupamirror”
whichchallengedthepatienttoreflectonthemeaningofhersuffering.Accordingtothe
nurse,thepatientlookedthedoctorsquarelyintheeyeandexclaimedthatshewasnot
bitterbecauseheryearsofillnesshadcontributedtogrowthandmaturitybeyondher
59
age(paperIp.4).Thenursebelievedthatthisconversationgeneratedashiftinthe
patient’swayofdealingwithhersituationbecauseshewenthometosetheraffairsin
orderandshereconnectedwithhermotherandsister.Thissuggeststhatthedoctor
stimulatedthepatient’sprocessofexistentialmeaningmakingrelatedtohorizontal
formsofself-transcendence:self-actualization,order,wellbeingandrelatedness
(Schnell,2009).
Inthesecondnarrative(paperIIp.6),thepatient’sneedformeaningseemedtobe
relatedtoorder(wishingtocompletethefamilyhomerenovationbeforeshedied)and
horizontalself-transcendence,sincefixingupthefamilyhomealsoinvolvedthepatient’s
needformeaningbytakingresponsibilityfor(worldly)affairsbeyondherimmediate
concern(Schnell,2009).Thepatient’sneedformeaningwasalsorelatedtowellbeing
andrelatedness(Schnell,2009),becauseshewasafraidthatshewouldceasetoexist
afterdeath,andthatthiswouldcutherofffromherlovedones.Accordingtothenurse,
thepatientseemedtodrawconsolationfromthepossibilityofreunitingwithherloved
onesinthehereafter.
Inthelastnarrative(paperIIp.6-7),thepatient’sneedformeaningwaslinkedto
verticalself-transcendence,wellbeingandrelatedness(Schnell,2009).Thepatient
sufferedfromphysicalandspiritualpain,becauseshethoughtshehadtoendureher
painasGod’spunishmentforhersins.Byprayingwiththepatientandtalkingwithher
aboutwhyshethoughtGodwaspunishingher,thenursewasabletohelpthepatientto
findpeacewithGod.Thisallowedthepatienttoacceptmorphinefromthenurse,which
alleviatedherphysicalsuffering.
TosummarizetheresultsofthisinterpretationinSchnell’s(2009)terms:Conveying
consolationwasaboutassistingpatientsintheirexistentialmeaningmakingrelatedto
thehorizontalrelationaldimension:-helpingpatientstorepairandmaintaintheir
relationshipswithfamilymembers(narrative1and2).Italsoinvolvedassisting
patientsintheirexistentialmeaningmakingrelatedtotheverticalrelationaldimension:
-helpingthepatienttofindpeacewithGod(narrative3).

60
ThisisinlinewithReed’s(1992)understandingofspirituality.Accordingtoher(1992),
spiritualityspecificallyreferstothepropensitytomakemeaningthroughasenseof
relatednesstodimensionsthattranscendtheselfinsuchawaythatempowersanddoes
notdevaluetheindividual.Reed(1992)pointsoutthatthisrelatednessmaybe
experiencedintra-personally(asaconnectednesswithoneself),interpersonally(inthe
contextofothersandthenaturalenvironment),andtrans-personally(referringtoa
senseofrelatednesstotheunseen,Godorpowergreaterthantheselfandordinary
sourceswhichimpliesanexpansionofboundaries,inward,outwardandupward:
“Spiritualitythenismanifestedthroughthesevariouspatternsofconnectedness,in
whichonestepsbeyondthestructuresofeverydayexistencetoendowtheordinary
withextra-ordinarymeaning”.(Reed,1992,p.350)
Thenurses’consolationeffortswhichevolvedaroundenablingtheirpatientstoregain
andmaintaintheirrelatednesstoself,significantothersandtoGodcorrespondwith
Schnell’s(2009)conceptofexistentialmeaningmakingandReed’s(1992)
transcendentalandrelationalunderstandingofspirituality.
10.1.5ThePowerofConsolingpresence
Althoughthenursesexperiencedthattheymanagedtoconsoletheirpatientswhenthey
wereabletohelpthemfindmeaningintheirsuffering,theresultsalsoshowthatthis
wasnotalwayspossible.Thenursesexpressedthat:“Thereissuchathingaspointless
suffering!”andthattheysometimesjusthadtoacceptthat:“Thingsdon’talwayshavea
deepermeaning”(paperIIp.8).Inthesesituations,thenursesfeltthatconveying
consolationby“justbeingthere”tosharethepatient’ssufferingwasmoreimportant
thantryingtoresolvetheirspiritualandexistentialissues.Thenursesexperiencedthat
embracingthesilencetogetherwiththeirpatientscouldhaveapowerfulconsoling
effect,andtheyexpressedthatthisdemandedamentalshiftfromfocusingon“doing
somethingforthepatient”to“beingwiththepatient”(paperIp.3,paperIIp.8,paperIII
p.5).Thenursesexperiencedthattheyhadanimportantfunctionas“emotional
containers”whentheyjuststoodbytheirpatients,listeningandencouragingthemto
venttheirthoughtsandfeelingswhichcouldinvolvetears,griefandsorrowaswellas
angerandfrustration:“Itdoesn’tdoanyharmifpeoplestarttocry.Iusuallytellmy

61
patientsthattheydon’thavetofeelashamedoftheirtears.Tearsareonlymeltingice.”
(paperIIp.8)Thenursesalsopointedoutthatsomepatientscouldbetootiredtotalk
needingthenurse’sconsolingpresence.Eventuallytherewouldcomeapointintime
whenitwastoolateforwords,andinsomecaseswordslostallmeaningduetothe
brevityofthesituation:“Whentheyaresosickthattheyarevomitingtheirownfecal
matter,theonlythingyoucandoistobethere,holdingthem,comfortingthemand
warmingthem”.(paperIp.3)
Accordingtothenurses,whatpatientsneededmost,werenurseswhowerewillingto
endureandstandbytheirpatients,containingthepatients’emotionsandshowingthem
thattheywouldnotbeabandonedintheirtimeofneed(paperIp.3,paperIIp.8)“-just
beingtheresharingthepainandlettingthemtalk,ifthat’swhattheyneed,sometimes
that’sallyoucando”(paperIp.3).ThisissupportedbyRushtonet.al.(2009,p.407),
whodefinepresenceasthecapacityto“befullytherewithaqualityofattentionand
authenticitythatinformsrelationshipsandactions”.Accordingtothem(2009),modern
medicine’semphasison“curing,fixinganddoing”(whichmaynolongerbeappropriate
whenpeoplearedying)mustbebalancedwiththequalityofbeingpresentwiththose
whoaresuffering,andtheypointoutthatbeingpresentwiththedyingandbearing
witnesstotheirsufferingarehealingactsinthemselvesandareoften“enough”
(Rushtonetal.,2009).
10.1.6Consolationunderstoodasamoralresponsibility
AccordingtoNortvedt(1998),“toencounterapatient’spainandunderstandingthat
painassufferingistobestruckbytheother’sagonyasamoralreality”(Nortvedt,1998,
p.387).Hence,Nortvedt(1998)maintainsthatnurseshaveamoralresponsibilitytobe
answerableforthepatients’condition,pain,sufferingandvulnerability.Following
Nortvedt(1998),itcanbearguedthatnurseshavearesponsibilitytoconvey
consolationasameanstoeasetheirpatients’spiritualandexistentialsuffering.
ThiswillbeexplicatedinlightoftheNorwegiannursingphilosopherKariMartinsen’s
philosophyofcare(Martinsen,1993,2000,2006)andtheDanishphilosopherand
theologianK.E.Løgstrup’srelationalethics(Lindseth,1992,pp.102-103),withspecial
62
referenceto“TheEthicalDemand”(Løgstrup,1956,1997)1.Thesethinkerswere
chosen,becausetheirrelationalperspectivesareconsistentwiththenurses’emphasis
ontherelationaldimensionofconsolation.Martinsen(1993,2000,2006)anchorsher
philosophyofcareinLøgstrup’sideasabout“theethicaldemand”(Løgstrup,1997)and
thesovereignexpressionsoflife(Løgstrup,2007)2.Astheseideasaredecisiveto
understandMartinsen’sphilosophyofcare(Delmar,2012)theywillbeoutlinedbriefly
beforeweproceedtoMartinsen’sthoughtsoncare.
“TheEthicalDemand”InTheEthicalDemand,Løgstrup(1997)maintainsthathumanbeingsarealways
alreadyentangledorintertwinedwith,andinthelifeofothers,andthatthisisabasic
ontologicalfactofhumanexistence,whichispriortoourconstitutionasindividuals.For
Løgstrup(1997),toexistashumanbeingsistoexistwithothers.Althoughwemaytend
toviewanotherperson’sworldasseparatefromourown,Løgstruppointsoutthatthis
isnotso.Onthecontrary:“Weareeachother’sworldandeachother’sdestiny”
(Løgstrup,1997,p.16)andLøgstrupisveryclearabouttheconsequencesofthismutual
entanglement.Forhim,theethicaldemandisimplied“bytheveryfactthataperson
belongstotheworldinwhichtheotherpersonholdssomethingofthatperson’slifein
hisorherhands,itisthereforeademandtotakecareofthatperson’slife”(Løgstrup,
1997,p.22).Theethicaldemandissilentinthatitisunspoken,unarticulatedand
merelyimplicit.Moreover,itisnotidenticalwithanydemandthattheotherpersonlays
onyou.Rather,itdemandsthatyou,tothebestofyourknowledge,dowhatwillbenefit
theotherperson.Inaddition,theethicaldemandisradical,unconditionalandabsolute,
whichmeansthatyoumustactexclusivelyandunselfishlyforthesakeoftheother,
regardlessofwhotheotherpersonisoryourrelationshiptothatperson(Løgstrup,
1997,pp.44-46).
1TheEthicalDemand(DenEtiskefordring),(Løgstrup,1956))wastranslatedfromtheoriginalDanishin1997.2Løgstrupelaboratedonhisconceptionof“thesovereignexpressionsoflife”inOpgørmedKierkegaard(Løgstrup,1968)andseverallaterethicalworks(vanKootenNiekerk,2007).MajorexcerptsfromtheseLøgstruptextsweretranslatedfromDanishinBeyondtheEthicalDemand(Løgstrup,2007).

63
Løgstrup(2007)maintainsthatweareboundtotheworldthroughsuchsovereign
expressionsoflifeastrust,opennessofspeech,hopeandmercy.Theseexpressionsbelong
totheverybasicsoflifeandtheyaregivenbylifeitself.Theyarerelationallylivedand
experiencedandtheyappearspontaneouslythroughourengagementswithone
another.Theymakeclaimsonusthroughourembeddednessintheworld,which
accordingtoLøgstrup(2007),subjectsustotheradicaldemandtocareforothers.As
waysoftakingcareofothers,thesovereignexpressionsoflifefulfilltheethicaldemand,
-beforethedemandhasevenmadeitselffelt.However,theethicaldemanddoesnot
makeitselffeltuntilthesovereignexpressionsoflifefail.Løgstrup(2007)statesthatthe
aspectofdutyandmoralitysetsinwhenwearetemptedtopassbyapersonwhoisin
needofourhelp.Whenthedrivetoperformanactofmercystemsfromourmoral
deliberations,ouractisreducedfromaspontaneouslifeexpressiontodutyforduty’s
sake.AsLøgstrup(2007,p.76)pointsout:“DutyenterswhenIamtryingtowriggleout
ofthesituation”.Assoonasopennessofspeech,hopeandmercyareinstrumentalized
theirspontaneityisbroken,whichdestroysthemandturnsthemintotheiropposite.If
mercyforinstance,ismadetoserveoneselforathirdparty,itisnolongermercybut
unmercifulness.Accordingly,thesovereignexpressionsoflifedefybeingmadeameans
toothergoalsthantheirown,whichistheimmediateservicetoone’sneighbor
(Løgstrup,2007).However,Løgstrupdoesnotprovidespecificrulesandguidelines
abouthowtoact.Rather,heassertsthatitisuptoeachindividualtousehisorher
insight,understandingandimaginationtofigureoutwhatthedemandrequires
(Løgstrup,1997,p.22).
DrawingonTheEthicalDemand(Løgstrup,1997),KariMartinsen’scaringphilosophy
(Martinsen,1993,2000,2006)takesonarelationalperspective(Delmar,2012).Using
Løgstrup’sterms(Løgstrup,1997,2007),Martinsen(1993,2000,2006)maintainsthat
thepatientunderstoodas“theother”,makesaphysicalimpressiononthenursethrough
hisorhersenses,whichgeneratesan“appealtolookaftertheother’slife”(Martinsen,
1993,p.19).AccordingtoMartinsen(1993,2000,2006),theappealtocareforthe
patientispoweredbytheethicaldemand(Løgstrup,1997),whichchallengesustoactin
thebestinterestof“theother”and“totakecareofthelifewhichtrusthasplacedinour
hands”(Løgstrup,1997,p.18).Beingmovedandtouchedbytheethicalappealfromthe
patientcompelsthenursetocareforhimorher.Accordingly,somethingaboutthe
64
patientmustappealtothenursetocreateanawarenessofthepatients’plight
(Martinsen,2000,2006).FollowingLøgstrup(Løgstrup,1997,2007)andMartinsen’s
(2000,2006)lineofthought,thenurses’spontaneousandcompassionatereactionsto
theirpatients’sufferingsuggestsanimplicitacceptanceoftheirmoralresponsibilityto
beanswerabletotheethicaldemand.AsMartinsen(2006,p.89)pointsout:“Perceiving
theotherisalreadybeinginanethicalrelationshiptohim.”
“TheMasteryofSeeing”
However,Martinsen(2000,p.17)alsonotesthatpeopleresponddifferentlytothe
sufferingofothers,andthathowtheyrespond,dependsentirelyontheirability“tosee”.
Accordingly,torespondtothepatients’ethicalappeal,Martinsen(2000,2006)asserts
thatnursesmustengagein“amasteryofseeing”.DrawingonLøgstrup’s(1971)
interpretationoftheparableabouttheGoodSamaritan,inTheNewTestament,Luke10:
25-37(Biblegateway,2011),Martinsen(2000,2006)reflectsonwhatitmeans,“tosee”.
IntheparableJesustellsaboutthereactionsofapriest,aLeviteandaSamaritanwhen
theydiscoveredahalfdeadwaylaidman.WhenthepriestandtheLevitesawthevictim,
theparablestatesthattheypassedhimbyontheothersideoftheroad,leavingthe
victimtohisowndevices:“ButaSamaritan,ashetraveled,camewherethemanwas;
andwhenhesawhim,hetookpityonhim”(Luke10:33,Biblegateway,2011).
Martinsen(2000,2006)emphasizesthatitwasthesightofthebatteredandbleeding
manthatgeneratedtheSamaritan’spityforhim.Comingovertothehalfdeadmanthe
Samaritandidnotstandthereanalyzingthesituation.Rather,thesightofthevictim’s
bodilypain,strucktheSamaritanwithagutwrenchingforce,whichpropelledhiminto
action.AsMartinsenpointsout:“TheopenandreceptiveeyesoftheSamaritanwere
struckbytheotherandthesituationhewasin,andwithpityandgreatpainhecoulddo
nothingbutnurseanddressthevictim’swounds”(Martinsen,2006,p.84).Martinsen
(2000,2006)emphasizesthattheSamaritan“sawwithhiswholebody”throughhis
sensesandwastouched.Accordingtoher,theSamaritan“sawwithhis“heart’seye”,
becausehisattentionwasdrawntothesufferingvictiminsteadofhisownpainful
feelingsandself-pity,whichwereinducedbythesightofthebatteredman(Martinsen,
2000,2006).Asthesituationbecamecleartohimheexperiencedanimmediate
65
identificationwiththewoundedman,-that“theother”likehimselfwasafellowhuman
being,whileatthesametime,“theother”wasalsodifferentfromhim,asavictimin
needofhelp.Martinsen(2000,2006)assertsthatliketheSamaritan,nursesmustalso
seethroughtheir“heart’seye”inordertoperceivetheethicalappealfromthepatient.
Thenursemustidentifywiththepatientasafellowhumanbeing,whileatthesametime
beingawareoftheirdifferentness,becausethepatientisinneedofthenurse’shelp.
Thusly,drawingonLøgstrup(1971,1997),Martinsen(2000,2006)assertsthat“Seeing
withtheheart’seye”impliesthattheprofessionalnursemustdaretobeahumanbeing
whoisopentohisorheremotions,whileatthesametimeholdingthembacktoallow
thepatienttoemergeinordertofindoutwhatserveshimbest.Martinsen(2000,2006)
maintainsthatdecidingontherightandbestcarerequiresa“friendlyinteraction”
betweenthenurses’spontaneous,sensory-basedandpre-reflectiveimpressionofthe
patient(wearetouchedandmovedbeforeweunderstand)andherreflective
understandingofthepatient’sillness,(whichisbasedonherprofessionaljudgment).
Whilethenurseisspontaneouslymovedtocareforthepatientbyherimmediate
impression,herreflectiveprofessionaljudgmentenableshertoactinthebestinterestof
thepatient.
Theresultsrevealthatitcouldbechallengingtogetagriponwhatreallytroubledthe
patient.Thenursesexperiencedthatthepatients’spiritualandexistentialsufferingwas
frequentlyembeddedandentangledinawebofpsychosocialandphysicalpain,which
madeitdifficulttosortout(paperIp.5,paperIIp.5,paperIIIp.5).Theytherefore
neededtousetheirclinicaljudgmenttoreflectontheirimmediateemotional
impressionstodecideontherightcourseofactiontoalleviatetheirpatients’suffering.
Thisisillustratedinthefollowingquotes:
Irememberonemanwhowasterriblyrestlessandanxious.Hecouldn’tsleep.NomatterhowIaskedhimhejustsaidthathehurtallover.Butitmusthavebeenmorethanthephysicalpainbecausehewasreceivingstronganalgesicsthroughtwodifferentpumps.Ioftenwonderifwecouldhavedonemoreforhim.Igottheimpressionofaverysadandlonelyman.(paperIp.5)

66
TherewasthisyoungwomanwithCancerofthepancreas.ShewasconstantlycravingMorphineandStesolid.Itseemedlikeshewishedtofloatawayfromallherexistentialpain,butitwasstillthere,underneaththedrugdaze.(paperIp.4)
Inthenurses’experience,such“neverending”requestsforextrapainmedicationor
tranquilizersusuallysuggestedsomekindofunderlyingdistresswhichneededfurther
lookingintoandtheyhadthereforedevelopedakeeneyetopickupimplicitclues,and
toexercisetheirclinicaljudgmenttofindthesourcesforthepatient’ssufferingandto
decideontheappropriateinterventions.
The“EthicalDemand”andthe“seductivepull”ofhelping
Asmentionedearlier,Løgstrup(1997)maintains,theethicaldemandand“thesovereign
expressionsoflifedefybeingmadeameanstoothergoalsthantheirown,whichisthe
immediateservicetoone’sneighbor.Thisimpliesthatanyothermotivationaldriveto
conveyconsolationwhetherovertorcovertcorruptsthesovereignexpressionsoflifein
thenurse-patientrelationship.However,itisimportanttonotethatthefamiliarityand
trustwhichdevelopsbetweenanurseandapatient,coupledwiththeseductivepullof
helping,thecomplexityofthepatient’streatmentneeds,andapotentiallackof
understandingofthepatient’sboundariescanthreatentheintegrityofthenurse’s
relationshipwithherpatients.Thismayultimatelyleadtoaviolationofpatient
autonomy(Peternelj-Taylor&Yonge,2003).Paradoxically,beingdeeplymovedand
touchedbyapatient’ssufferingmayputnursesatriskofoversteppingtheir
professionalboundaries(Peternelj-Taylor&Yonge,2003).Martinsen(2000,2006)
takesthisintoconsiderationinhercrucialdistinctionbetween“emotionality”and
“seeingemotions”.AccordingtoMartinsen(2000,2006)whenanurseisstrickenand
stuckin“emotionality”thenursecirclesaroundherownneedsandemotions,“and
limitstheothertobeingdrawnintoherownhorizon”,whereasintheperceptive,
“seeingemotions”thenursecentersherattentiononthepatient’sexperienceof
sufferingbecausethepatientisperceivedas“theother”whichconcernsandappealsto
thenurse(Martinsen,2006,pp.74-75).Inlightof“theethicaldemand”(Løgstrup,
1997),thisimpliesthatthepatientmustbemetwhereheorsheisspirituallyand
existentiallysituatedatthemoment.

67
Itisthereforeimportanttokeepinmindthatthereexistsapowerdifferentialbetween
thenurseandthepatient,whichcannotbeoverlooked.Byitsverynaturethe
therapeuticnurse-patientrelationshipisasymmetrical.Thepatientbyvirtueofneeding
helpisautomaticallyplacedinapositionofvulnerability;whilethenurseontheother
handassumesapositionofpowerthroughtheroleofthehelper(Martinsen,2000,
2006;Peternelj-Taylor&Yonge,2003).Peternejl-TaylorandYonge(2003)pointout
thatnursesembracemanyrolesintheirpersonalandprofessionallives,andare
involvedin“thedanceofrelationships”.Ifnursesforgetwhich“dancetheyaredancing”
orwhichroletheyareassuming,theirownneedscanbecomemostimportanttothe
relationship.Henceforth,thereisaneedforcautionandethicalawareness,inorderto
avoidintrusivenessandviolationofpatientautonomy(Peternelj-Taylor&Yonge,2003).
Thisisechoedintheresultsofthestudy,whichshowthatthenursesreflectedontheir
ethicalchallengesrelatedtoencouragingpatientstosharetheirsuffering.Whilethe
nursesexperiencedthatpatientswhowereabletoexpresstheirfeelingsoftendied
morepeacefullythanthosewho“bottledeverythingup,”(paperIp.3,paperIIp.7),they
alsostressedthattheyhadtoputasidetheirownviewsandpersonalneedstoreachin
topatientswhowereunwillingorunabletosharetheirsuffering.Thenurses
emphasizedthattheywereprofessionallyandethicallyobligedtorespectthepatients’
choice.“Whoarewetojudgewhatisbestforthem”,theyreflected(paperIp.3)andthey
pointedoutthattherearenoeasyanswersbecauseeverypatientisdifferent(paperIp.
4).Itwasthereforecrucialtosensetheturningpoints,whenpatientsbecamereadyto
sharetheirsufferingandreceiveconsolation.Accordingtothenursesthisdemandeda
goodsenseoftiming,situationalunderstandingandtheabilityto“tuneinon”patients’
verbalandnonverbalcueswhilstperformingnursingcare(paperIp.5,paperIIp.5,
paperIIIp.7).
ThisresonateswithLøgstrup’s(1997,p.15)emphasisontuningintolistento“thenote,
whichisstruck”.AccordingtoLøgstrup(1997)thisisessentialineveryconversation,
becausewedeliverourselvesoverintothehandofanotherinthespeechrelationship,
whichdemandsbasictrust:“Thatallspeechtakesplaceinsuchfundamentaltrustis
evidentinthefactthatthemostcasualcommenttakesonafalsenoteifonebelievesthat

68
itisnotacceptedinthesensethatisintended”.(Løgstrup,1997,p.15)Thusly,ifanurse
ignoresordoesnothearthenoteinwhatthepatientsays,thenthatnurseisatriskof
violatingherpatient’sintegrity,whichinturnwillviolatethepatients’basictrustinher.
InspiredbyLøgstrup(1997),Martinsen(2006,p.60)assertsthat“thetone”3pointstoa
commonworldandprovidesacontextofinterpretationforwhatisgoingoninthe
situation,andsheemphasizesthatthenurseandthepatienttogethermustfind“the
tone”inthesituationwhichenablesbothparties,-nurseandpatient–eachintheir
ownway,todaretocomeforth.
10.2VulnerabilityandhelplessnessWhenthenurseswereaskedtonarrateabouttheirexperienceswithspiritualand
existentialcare,theirconsolationnarrativesevolvedaroundtheireffortstohelptheir
patientstofindpeaceandharmonyduringthefinalstagesofdying(paperIandII).The
resultsshowthatthenursesfelttheyhadbeensuccessfulwhentheywereableto
unburdensomeofthepatients’mostpressingsourcesofanxietyanddistress(paperII
p.12).Thisisillustratedinthethreeconsolationnarratives,insection10.1.2,which
showthatthenursesmanagedtohelptheirpatientstorestoretheirintra,interand
transpersonalrelationships,-theirrelationshipwith,self,lovedonesandwithGod(Reed,
1992).Regainingtheserelationshipsenabledthepatientstotranscendtheisolating
spiritualandexistentiallonelinessofdying.Assuch,theseconsolationnarrativescanbe
characterizedas“successful”consolationnarratives.
However,thenursesalsonarratedabout“unsuccessful”consolationexperiences,which
couldmakethemfeelprofessionallyinadequateandhelpless.Althoughthenurses
acknowledgedthatsufferinganddyingarefactsoflife,whichcannotbecompletely
alleviated,theyfounditdifficulttoacceptthattheycouldnotalleviatetheirdying
patientsdistress(paperIp.6,paperII7-8).Thisishighlightedinthefollowingquote:
Ayoungcancerpatientanxiouslybattleddeathtillthebitterend.Allofusthoughtitwasterriblethewayhedied!Wereallytried,butnobodycouldhelphimfindpeace,becausehesimplyrefusedtodie!Wesatthereholdinghishand,listeningtohim.Buthewascompletelyinconsolable!Itwasvery,very
3(orinLøgstrup’s(1997)terms“thenote”)

69
challengingandfrustratingeventhoughweknowthatweprobablydidallwecould!(paperIIp.7)
Bearingwitnesstopatientswhocontinuedtoradiateanguish,protestanddespairin
spiteofthenurses’consolationeffortswasexperiencedasemotionallychallengingand
draining.The“unconsolablepatients”werelookeduponasproblematic,formingthe
focusofpeersupportanddebriefing(paperIp.6-7,paperIIp.7-8).Inaddition,the
nursesfounditchallengingtobearwitnesstothedyingpatients’sufferingbecauseit
exposedthemtotheirownlatentfearsofmortalityandvulnerability(paperIp.6,paper
IIp.8).Asonenursepointedout:”Youhavetocometotermswithyourownthoughts
andfeelingsaboutyourownvulnerabilitytoendureworkinghereovertime.It’sa
demandingjob!Notallnursesarecutouttocareforthedying”(paperIIp.8).
InpaperIIIthemobilehospicenurseteachingteamstatedthatthecareworkers’main
obstacletoengageinspiritualandexistentialcarewastheirfearanduncertaintyof
facingdyingpatients’suffering(paperIIIp.4-6).Itseemsreasonabletoassumethat
likethenursesinpaperIandII,thecareworkers’reluctancetobewiththedying
stemmedfromtheirfearofrelatingtotheirownmortalityandvulnerability.
Whilevulnerabilityandsufferingareontologicalconditionsoflife,whichare
experiencedbyallhumans(Heidegger,1962;Turner&Dumas,2013),workingonthe
edgebetweenlifeanddeathposesdailypsychosocialchallengeswhichforcenursesand
careworkerstobecomeacutelyawareofthefragilityoflife(Najjar,Davis,Beck-Coon,&
Doebbeling,2009).Researchshowsthattheemotionalstressorsrelatedtocaringfor
patientswhoaresufferingand/ordying,placenursesandcareworkersinaunique
positionofvulnerability(Gjengedaletal.,2013).Recentresearchindicatesthat
emotionsarefeltinthebody(Back,Rushton,Kaszniak,&Halifax,2015).Thisresonates
withtheresultsinthisstudy,whichshowthatthenurses’spontaneousimpressionsof
theirpatients’sufferingcouldbesostrongthattheydescribeditintermsofphysical
sensationsintheirownbodies:
Wefeelthefearanddesperationthemomentweentertheroomeventhoughitisn’tours.IhaveenteredroomsIjusthavetogetoutof.Theatmosphereissoloadedwithsorrow.It’slikeaphysicalsensation.Thegriefjusthitsyoulikeawall!Howdoyoudealwiththat?(paperIp.5)

70
Icanbecomeveryoverwhelmedwhenpatientssharetheirinnermostthoughtsandfeelingsaboutlifeanddeath!Italmostknocksmeoutsometimes!(paperIIp.7)Theiremotionalanguishcanbesostrong.It’softenworsethanthephysicalpain!It’sliketheirheartsarebeingtornout!Howdoyourelievethatkindofpain?(paperIp.3)Youbecomequitefondofthepatients!Sometimestheyjustleapintoyourheart!(paperIp.6)
AccordingtoBenner&Wrubel(1989),citedinRaingruber&Kent(2003),bodily
responsesarestrongerwhenoneisdeeplyinvolvedwithandconcernedabouta
situation.Furthermore,Benner(2000a)pointsoutthattheempiricalresearchof
cognitivescientistsandneurobiologists(Damasio,1999;Lakoff&Johnson,1999;Rosch,
1981)revealsthatemotionsandembodiedfeelings,sensori-motorperceptionsand
skillsshaperationalthoughtandknowingandthatthesocial,sentient,sensori-motor
bodyplaysakeyroleinthoughtandaction.Hence,whenanursefeelsthatherpatientis
sufferingsomuchthat“itseemslikehisheartisbeingtornout”(paperIp.3)”andshe
becomessofondofthepatientthathe“leapsrightintoherheart”(paperIp.6)itseems
reasonablethatthepatients’painwillresonateinthenurse’s“ownheart”.Thiswas
especiallythecasewhenthenursescaredforpatientswhoremindedthemof
themselves:“Oneofmypatientshadalittlebaby.ThatwasreallytoughbecauseIama
mothermyself!”(paperIIp.7).
10.2.1Vulnerabilityandembodiedengagement
AfterabriefreturntoKariMartinsen’scaringphilosophy(Martinsen,2000,2006),
thenurses’physicalreactionstotheirpatients’sufferingwillbediscussedinlightof
Merleau-Ponty’s(1962)conceptofembodiedengagement.Asmentionedinsection
10.1.6,Martinsen(2000,2006)pointsoutthatinordertorespondtotheethicalappeal
fromthepatientthenursemustdareto“seewithherheart’seye”.Thisimpliesthatthe
nurseiswillingtotakeinthepatient’ssufferingthroughheropenandreceptiveeyes
andthatthiscompelshertoalleviatethepatients’suffering.Martinsen(2000,2006)
pointsoutthatfortheSamaritan,thebodilypainofthewaylaidmanstruckhimclose,
withoutdistance:“TheSamaritansawwithhisheart’seye,withhiswholebodywhich

71
waspainfullyopenandreceptive,turnedtowardstheother,attentivelytryingto
understandwiththoughtandwillaswell,whatisatstake”(Martinsen,2006,p.86).
AccordingtoMartinsen(2006,p.89):
Theopennessofperceptioncanbeterrifying.IntheeyesoftheSamaritanthepainoftheotherstruckintohisbody.Hestoodreceptiveandopenbutdidnotknowwhathewaslookingfor.Heonlyfeltit,thatthepainoftheotherconcernedhim.
BoththeSamaritan’sandthenurses’physicalreactionswhichstemmedfrom“seeingthe
sufferer”throughtheir“heart’seye”(Martinsen,2006)canbeunderstoodinlightof
Merleau-Ponty’s(1962)conceptofembodiedengagement.
Merleau-Ponty(1962),citedinRay(2006),conceptualizedthebodyascatching,
comprehendingandspontaneouslyrespondingtothecommunicationsofanother
person,whichhedefinedasembodiedengagement.AccordingtoMerleau-Ponty(1962),
citedinRay(2006),embodimentreflectshowweliveinandexperiencetheworld
throughourbodies,especiallythroughperception,emotion,language,movementin
space,timeandsexuality.Merleau-Ponty(1962),citedinRay(2006),maintainsthat
existencecanonlybeknowninandthroughthebodybecausethephenomenalbodyis
theonlymeansofbeingintheworld.Inthenursingcontextillness,pain,anddisability
areessentiallyconstitutedasembodiedexperiences(McDonald&McIntyre,2001).
Hence,tobeengagedwiththepatient,thenursemustbeengagedwiththepatient’s
existential,subjectiveandembodiedbeing:“Itisthepatient’sbodyasbothobjectand
subjectthatcallsoutforourministerings”(Hess,2003,p.145).
DrawingonLøgstrup(1997),Merleau-Ponty,Dreyfus,andDreyfus(1964)and
Martinsen(1997),Benner(2000a),maintainsthatgoodnursingpracticereliesonthe
humanbackdropofembodimentandourembodiedcapacitiestoexperience“the
spontaneoussovereignexpressionsoflife”(Løgstrup,1997),whichincludetrust,mercy,
opennessofspeech,andourcommonhumanconditionoffinitude,dependencyand
interdependence.InlightofLøgstrup(1997),she(2000a)alsopointsoutthatitisthe
immediateexperienceofembodiment,whichenablesthenursetorespond
spontaneouslywithmercy,withnoadditionalthoughtorcalculation.Nevertheless,
72
bearingwitnesstosufferingcanbeagonizing.AccordingtoMalone(2000),witnessing,-
orinMartinsen’s(2000,2006)termsseeingwith“theheart’seye”isqualitatively
distinctfrommerelooking;witnessingengagesthenurseasabeareroftruththatthe
sufferingpersoncannottell.Malone(2000)maintainsthatthisaspectofnursing
practiceislargelyunacknowledged,andthatthevulnerabilityitrequiresnursesto
experienceisrarelyaddressed.Twonotionsofvulnerabilitydominateinthenursing
literatureaccordingtoMalone(2000).One,whichmightbecalledapublichealthmodel
ofvulnerability,equatesvulnerabilitytothesusceptibilitytoparticularharmfulagents,
conditionsorcircumstances.Assuch,vulnerabilityissomethingtobeavoidedor
resisted.Theotherviewregardsvulnerabilityasthecommonconditionofallsentient
beings.Accordingtothisperspective,vulnerabilityisaconstantconditionofhuman
experience,acommonalitythatwesharebyvirtueofourembodiedexistenceandour
finitude.Assuchvulnerabilitygivesaccesstounderstandingaspectsofthepatients’
experiencesandisregardedpositively(Malone,2000).
Acknowledgingtheirownaswellastheirpatients’vulnerability,sharpensthenurses’
sensitivity,whichenablesthemtoopenthemselvestotheirpatient’ssituation(Norberg,
2001;Sarvimäki&Stenbock-Hult,2014).Asembodiedandvulnerablebeings,nurses
canexperiencetheirpatients’worldandengageintheillpersons’embodiedexperience
(Hess,2003).Thisenablesnursestounderstandmorethanwhatisbeingsaidand
observed,becausetheirimpressionofthepatients’conditionmanifestsitselfas
embodiedsensationsandphysicalresponsesbeforethenursescanunderstandthese
impressionsintellectually(Martinsen,2000,2006;Raingruber&Kent,2003).
10.2.2Compassionfatigue
Researchshowsthatbeingdeeplyengagedinpatients’sufferingoverprolongedperiods
oftimeexposeshealthcareproviderstovariousformsforoccupationalstress.(Backet
al.,2009;Hardiman&Simmonds,2013;Sabo,2008,2011a,2011b;Sandgren,Thulesius,
Fridlund,&Petersson,2006;Smartetal.,2014).Theconceptsofcompassionfatigue,
vicarioustraumatization,secondarytraumaticstressandburnouthavebeencompared
andusedinterchangeablywithintheliterature.Althoughtheseconcepts,have
73
significantsimilaritiestheyalsohavesignificantdifferences(Najjaretal.,2009;Smartet
al.,2014).
Forthepurposeofthisstudyitwillsufficetodiscusstheresultsinlightoftheconceptof
compassionfatiguewhichhasreceivedconsiderableattentionasapotentialformfor
occupationalstressduringrecentyears(Sabo,2011a).Compassionfatiguehasbeen
describedas“thenaturalconsequentbehaviorsandemotionsresultingfromknowing
aboutatraumatizingeventexperiencedbyasignificantother–theresultfromhelping
orwantingtohelpatraumatizedorsufferingperson”(Figley,1995,p.7),citedinSabo
(2011a).
AccordingtoSabo(2011a),severalstudiessuggestthatcompassionfatigueisconnected
tothetherapeuticrelationshipbetweenhealthcareprovidersandpatients,inthatthe
traumaticorsufferingexperienceofthepatienttriggersaresponseonmultiplelevelsin
thehealthcareprovider.Inparticular,anindividual’scapacityforempathyandabilityto
engage,orenterintoatherapeuticrelationshipisconsideredtobecentralto
compassionfatigue.Providingassistancetoindividualsexperiencingpain,sufferingor
trauma,theprofessionalmayexperienceadverseeffectssimilartotheirclients.
CoetzeeandKlopper(2010)claimthatcompassionfatigueisthefinalresultofa
progressiveandcumulativeprocess,whichiscausedbyprolonged,continuous,and
intensecontactwithpatients,theuseoftheselfandexposuretostress.Thephysical
effectsofcompassionfatigueincludeweariness,lossofstrength,reducedoutput,
diminishedperformance,lossofenduranceandincreasedphysicalcomplaint.The
emotionaleffectsincludelessenedenthusiasm,desensitization,diminishedability,
irritabilityandbeingemotionallyoverwhelmed.Thesocialeffectsincludeaninabilityto
aidandshareinthesufferingofpatients.Compassionfatigueissaidtooccurwhen
healthcareproviderscloselyidentifywiththeirpatientsandpersonallyabsorbthe
patients’traumaorpain.Itresultsfromgivinghighlevelsofenergyandcompassion
overaprolongedperiodoftime,particularlywhennursesdonotexperiencethepositive
outcomesofseeingpatientsgetbetter(Najjaretal.,2009).Inlightoftheafore-cited
literature,itseemsreasonablethatthenurseswereatriskofdevelopingcompassion
fatiguebecauseoftheirdeeprelationshipswithpatients,andtheiremotionaland
embodiedreactionstotheirpatients’suffering.

74
However,Sabo’s(2011a)studyoftheHSCTnurses’psychosocialhealth,foundthat
compassionatepresencingandinvolvementinthenurse-patientrelationshipmay
actuallyprovideapotentialbufferingagainsttheadverseeffectsofcaringforthe
seriouslyillanddying,whereasdistancingordisengagementthroughemotionalsurvival
strategiessuchasemotionalshielding,emotionalprocessingandemotionalpostponing
(Sandgrenetal.,2006)mayincreasetheriskofexperiencingcompassionfatigueand
othertypesofoccupationalstress.
AccordingtoSabo(2011a),thereexistsasignificantdifferencebetween“compassionate
presencing”and“emotionalsurvivalstrategies”.Wherecompassionatepresencereflects
thenotionof:“beingwith”,-alivingoutofthecaringnatureofnursingthrough
connectionsandrelationships,emotionalsurvivalgenerallyattendstostrategiesor
methodstoaddressaproblem,“inessenceto“avoidbeingwith”(Sabo,2011a,p.109).
Sabo(2011a)maintainsthatcompassionatepresenceconveysapositivetone,where
connectionorrelationshipscarrybenefits,whileemotionalsurvival(Sandgrenetal.,
2006),suggeststhatcaringmayleadtonegativeeffects,whichnursesmaypostponeby
employingvariousavoidancestrategies.However,Sabo(2011a)doesnotclaimthatthe
potentialriskforpsychological/emotionalpainasaresultofcaringrelationshipsis
non-existentifoneis“compassionatelypresent”rathershepointsoutthatcaringshould
beperceivedasadouble-edgedswordandthatthepotentialforadversepsychosocial
effectssuchascompassionfatiguemaybereducedifnursesareabletobe
compassionatelypresent.AccordingtoSabo’s(2011a)study,theHSCTnursesneededto
remainvigilantaboutwhosepainandsufferingwasbeingshared.Afailuretoestablish
clearboundariesbetweenthepersonalandprofessionalcouldplacethenurseatriskfor
adverseeffects.Sabo’s(2011a)resultsareconsistentwiththeresultsinthisthesis,
whichshowthatthenursesstrovetostrikeabalancebetweendisengagingandover-
engagingintheirpatients’suffering.Thisaspecthasbeenthoroughlydiscussedinpaper
IIp.10.
Sabo(2011a)pointsoutthat“compassionatepresence”isawayofbeingand
connecting,whichrequiresthenursetobeauthentic/genuine,openandavailableto
shareintheethical-moralmomentsoftheirpatientsandfamilies.Compassionate
presenceisareflectionofholisticnursingpracticeembracingthephysical,

75
psychological,emotionalandspiritualdomains.Thisbearscloseresemblancetothe
nurses’emphasisonsharingtheirpatients’sufferingthroughconsolingpresenceand
relationshipmaintainingactivities(paperIp.3-5andpaperIIp.6-7).
10.2.3Compassionsatisfaction
CoetzeeandKlopper’s(2010)distinctionbetween“compassionfatigue”and“compassion
satisfaction”supportsSabo’s(2011a)study.CoetzeeandKlopper(2010)pointoutthat
althoughnursesareexposedtotheexactsameriskfactorsofcontact,useoftheselfand
stress,somenursescontinuetoflourishinthesecircumstances.AccordingtoCoetzee
andKlopper(2010)nurseswhoexperiencecompassionsatisfactionareabletoconnect
withtheirpatientsregardlessofthecircumstances,whichleadstomeaningfuland
purposefulinteractionsbetweennursesandtheirpatients,whilstnurseswho
experiencecompassionfatigue,graduallydistanceandisolatethemselvesfromtheir
patients,whichresultsinthefactthatneitherthenurses’northepatient’sneedsare
fulfilled.
Sabo(2011a)andCoetzeeandKlopper‘s(2010)studiessuggestthatbeingdeeply
involvedinthenurse-patientrelationshipmayprovidemoreprotectionagainst
compassionfatiguethanusingemotionalsurvivalstrategies(Sandgrenetal.,2006)to
avoidthepainfulimpactofwitnessingdyingpatients’suffering.Whiletheprocessof
compassionfatigueiscumulativeandprogressive,movingfromdiscomforttostressand
finallytofatigue,theprocessofcompassionsatisfactionisrestorativeandcircular,
presentingasymbioticrelationshipbetweenthepatientandthenurse,aseachfinds
fulfillmentintheother(Coetzee&Klopper,2010).ItisinterestingtonotethatCoetzee
andKlopper’s(2010)definitionofcompassionsatisfactionresonateswithNorberget
al.’s(2001)claimthatnursesandpatientsmayexperiencemutualconsolationthrough
communionanddialog.
Whiletheresultsinthisstudyshowthatbearingwitnessto“unconsolable”patients’
sufferingcouldbeemotionallydrainingandchallenging(paperIIp.7),theyalsoreveal
thatthenursesfeltthatconveyingconsolationcouldbedeeplymeaningfuland
rewarding(paperIp.6,paperIIp.7).Bearingwitnesstoapatient’speacefulpassing

76
filledthemwithreverenceandawe:“Theroomwasveryquietandthepatientdied
calmlyandpeacefully.Itwasaveryspecialmoment”(paperIIp.7),andthenurses
expressedthattheyfelt“honoredandtouched”whenthepatientssharedtheirtrustand
chosetoconfideinthem(paperIIp.7).
InlightofSabo’s(2011a)andCoetzeeandKlopper’s(2010)studies,itisinterestingto
notethatnoneofthenursesmentionedthattheyhadconsideredchangingtheirlineof
workortakingaleaveofabsence,althoughtheycouldfeelemotionallydrainedand
helplesswhentheywereunabletoconsoletheirpatients.Takingthisintoconsideration
andthefactthatthenurses’workingexperienceinend-of-life-carerangedfromfiveto
thirty-fiveyears,itseemsreasonabletoassumethatthenursesexperiencedsufficient
compassionsatisfactionthroughtheirrelationshipswiththedyingthatitcounter-
balancedpossibleadverseeffectsofcompassionfatigue.Theseresults,togetherwiththe
aforementionedstudiesunderscorethevalueoftherelationaldimensioninconsolation
work(paperIp.3-5andpaperIIp.6-7).
10.3CompassionandCourage
10.3.1Compassion
AccordingtoRushtonetal.,(2013)compassionoptimallyinvolvesaqualityofpresence
thatconveysstabilityandresiliencewithabalancedconcernandheartfeltconnection,
butisnotdepletingoroverwhelmingtoeitherperson.Lazarus(1991)pointsoutthat
compassionimpliesfeelingpersonaldistressatthesufferingofanotherandwantingto
ameliorateit:“Thecorerelationalthemeforcompassion,therefore,isbeingmovedby
another’ssufferingandwantingtohelp”(Lazarus,1991,p.289).Thisresonateswiththe
results,whichshowthatthenursesweredeeplymovedandtouchedbytheirpatients
andyearnedtoconsolethem(paperIp.6,paperIIp.7).However,theresultsalso
indicatethatthenursesinpaperIandII,aswellasthecareworkersinpaperIII,could
beambivalentandreluctanttoaddresstheirpatients’spiritualandexistentialanguish
becauseitconfrontedthemwiththeirownvulnerabilityandlatentfearsofsufferingand
death(paperIp.7,paperIIp.8,paperIIIp.4-5).

77
ThesereactionsareunderstandableaccordingtoSasserandPuchalski(2010,p.3).They
(2010)pointoutthatcaringfordyingpatientsoverthecourseoftheirillnesstrajectory
exposeshealthcareproviderstogut-wrenchingstoriesofhumantragedy,whichovera
periodoftimemayevokeacertainamountof“accompaniphobia”thatmayleadto
avoidancestrategies(Sandgrenetal.,2006).AccordingtoSasserandPuchalski(2010)
thetendencytoavoidaddressingpatients’sufferingmaystemfromapossible
resonancewithunhealedwoundsdeepwithinthehealthcareproviders’ownsoulsthat
needsfurtherworkontheirpart.Thissuggeststhatnursesandcareworkersmust
possesscourageaswellascompassioninordertosuspendtheirpersonalreluctance
andanxietynomatterhowdisquietingthismightbeinordertoaccompanythedying
wheretheywanttogo,whentheywanttogothere,andwhetherthenursesandcare
workerswanttoornot(Sasser&Puchalski,2010).Takingthisintoconsideration,itis
interestingtonotethatthewordcompassionisderivedfromtheLatin“pati”and“cum”
whichliterallymeans,“tosufferwith”(Nouwen,McNeill,&Morrison,2008).Nouwen
et.al.(2008)pointoutthat:
Compassionasksustogowhereithurts,toenterintoplacesofpain,toshareinbrokenness,fear,confusionandanguish.Compassionchallengesustocryoutwiththoseinmisery,tomournwiththosewhoarelonely,toweepwiththoseintears.Compassionrequiresustobeweakwiththeweak,vulnerablewiththevulnerable,andpowerlesswiththepowerless.Compassionmeansfullimmersionintheconditionofbeinghuman.Whenwelookatcompassioninthisway,itbecomesclearthatsomethingmoreisinvolvedthanageneralkindnessortenderheartedness.(Nouwenetal.,2008,pp.3-4)
Nouwenetal.’s(2008)descriptionof“thechallengeofcompassion”resonatesdeeply
withthenurses’andcareworkers’challengesrelatedtoconveyingconsolation.While
Nouwenetal.(2008,p.4)statethat“Compassionmeansfullimmersioninthecondition
ofbeinghuman”,Norbergetal.(2001,p.549)maintainthatconsolationinvolvesbeing
willingto“sinkintosomebodyelse’shellandstaythere”.Beingincommunionwith
patientsinordertosharetheirsuffering(Norbergetal.,2001),-orinNouwenetal.’s
(2008)words:“goingwhereithurts”,demandsopenness,presenceandavailability,
whichcreatestrust.Whentherelationshipistrusting,thereisroomtouncoverthe
wound(thecauseofthesuffering),whichcalmsthesufferingpatientwhodarestolook
athisorherwounds,whilethenursewhomediatesconsolationby“walkingalongside”
showsthepatientthathisorherweakness,griefandexpressionsofpainareaccepted.

78
Intheshortperspective“uncoveringthewound”mayincreasethepainbecausethe
woundbecomesobvious,exposing“allthatisraggedandbroken”(Norbergetal.,2001,
p.548).
Uncertainty
Theresultsshowthatthenursesandcareworkersoftenfeltuncertainabouttheright
andbestthingtosayordotoalleviatetheirpatients’spiritualandexistentialsuffering.
Althoughinthefirstconsolationnarrative(“Breakingtheboil”paperIp.4)thenurse
thoughtthatsomepatientscould“needalittlepush”tohelpthemtranscenda
depressivespiralofexistentiallonelinessandalienation,thenursesexpressedthat
strikingtherightbalancebetweenmildpersuasionandacceptingthepatients’choices
to“bottleuptheirsuffering”couldbedifficult.Choosingtherightapproachwasfraught
withuncertainty,especiallyrelatedtoethicaldilemmasconcerningthepatients’
vulnerability,autonomyandtheasymmetricalpowerstructureinthenurse-patient
relationship.Thenursesexpressedthattheycouldneverbecertainaboutmakingthe
rightchoiceduetounpredictablechangesinthepatients’condition,andtheycouldalso
beuncertainabouthowtheirpatientsmightreacttowardstheirattemptstoconsole
them.Asthenursespointedout:“Eachpatientisdifferentandtherearenoeasy
answers.”(paperIp.4)
10.3.2Courage
Theseresultsindicatethattoconveyconsolationnursesandcareworkersmustbe
willingtoexposethemselvestotheirownaswellastheirpatients’vulnerability,to
accompanytheirpatientsintotheexperienceofuncertainty,andtogiveupcontroland
self-determination.Thisdemandscouragebecauseawindowisopenedtotheunknown
(Thorup,Rundqvist,Roberts,&Delmar,2012).Jordan(2003)definescourageas“the
capacitytoactmeaningfullyandwithintegrityinthefaceofacknowledgedvulnerability
“(Jordan,2003,p.2).AccordingtoJordan(2003),courageandvulnerabilityare
inextricablelinkedtogetherandtherecanbenorealcouragewherevulnerabilityand
feararedenied.Drawingonafeministperspective,Jordan(2003)pointsoutthatthe
traditionalmaleEurocentricmythofthecourageous,loneindividualwhodefies

79
vulnerabilityandfearobscuresthefactthatweallneedencouragementandconnection
throughoutourentirelives,andthathavingthecouragetomovebeyondcertaintyand
invulnerabilityenablesustoentertheworldoflearning,curiosityandlove.From
Jordan’s(2003)pointofview,courageisbuiltthroughvulnerabilityandconnectivity,
whereone’sopennesstobeingaffectedisessentialforconnection.Withoutopenness
peoplerelateinauthentically,adoptingrolesandcomingfromdistancedandprotected
places,whereaswhenwehavethecouragetobevulnerable,wearecapableofbeing
“moved”byourinternalaffectiveexperienceaswellasbeingaffectedbyotherpeople
(Jordan,2003),whichenablesustoexperiencecompassionforthesufferingofothers
(Lazarus,1991).Jordan’s(2003)understandingofcourageresonateswithLøgstrup’s
viewsontheinterdependentnatureofhumanexistenceandtheethicaldemand“totake
careofthelifewhichtrusthasplacedinourhands”(Løgstrup,1997,p.18),as
mentionedinsection10.1.6.AccordingtoDelmar(2004),citedinThorupetal.(2012),
enteringintoseriouspatientrelationshipsdemandscourage,becauseitrequiresa
willingnessfromthenursetoruntheriskofrejection.InlinewithNouwenetal.(2008)
andNorbergetal.(2001),Thorupetal.(2012)pointoutthattheoreticalandempirical
studiesshowthatthenurses’couragelaysinhisorherwillingnesstowalkalongsidethe
patientsontheirjourneytoovercometheirsuffering,nomatterwheretheroadleads.
Thisjourneyishighlyunpredictableandseemstorequirethewillingnessandabilityto
bearwitnesstothepatients’vulnerabilityandsuffering(Thorupetal.,2012).
Thorupetal.’sresearch(2012)revealsthatcouragebecomesevidentinsituations
wherenursesarecapableofcopinginanindeterminatesituation,ofstandingout“inthe
open”ofengagingwithandlisteningtovulnerableandsufferingpatients,insituations
thatexposethemtotheriskofrejection.Couragemanifestsitselfastheabilityand
willingnesstohelppatientstofacetheirownvulnerabilityandsuffering,tobearwitness
topatients’vulnerabilityandsufferingandtohavetheself-confidencetoargueforand
provideforprofessionalcare(Thorupetal.,2012).Thorupetal.’s(2012)work
resonateswiththisstudy,whichshowsthatthenursesandcareworkersneeded
couragetoovercometheirfearandemotionalambivalencetoconsolethedying,because
thisexposedthemtotheirownfearsofmortality,vulnerabilityandprofessional
helplessness.Aspreviouslymentionedcouragewasespeciallyneededinorderto
endurebeingwiththe“unconsolable”patients.(paperIIp.7)
80
AccordingtoThorupetal.(2012),courageisaprerequisiteinnerqualityandafirststep
towardstheexistentialcaringencounter.Thissupportsthestudyresults,whichshow
thathavingthecouragetoovercometheirfearsandreluctancetobewiththedyingwas
aprerequisiteforthenurses’willingnesstoengageincompassionateandconsoling
relationshipswiththeirpatients.Thorupetal.(2012)pointoutthatonthisexistential
level,infacingtheunpredictable,couragecontributestothenurturanceofpersonaland
professionaldevelopment.InlightofThorupetal.’s(2012)study,itisinterestingto
notethatthenursesinpaperIIexperiencedthattheiroldercolleaguesseemedtobe
morewillingtoengagethemselvesinthepatients’spiritualandexistentialsuffering
thantheyoungernurses,andtheyassumedthiswasbecausetheoldernurses’personal
andprofessionallifeexperienceshadmadethemmorematureandrobusttobearthe
weightofthepatients’distressthantheiryoungercolleagues(paperIIp.12).
(Seesection10.4.1,table1)
10.4Cancourageandcompassionbetaught?Thisstudyindicatesthatconsolingthesufferinganddyingisadeeplyrelationaland
compassionateactivity,whichrestsonnurses’andcareworkers’couragetoovercome
theirfearandreluctancetoaddresstheirdyingpatients’spiritualandexistential
distress.Thisraisesimportantpedagogicalquestionsabouthowtoteachandtrain
nursesandcareworkerstoconveyconsolation:
- Cancompassionandcouragebetaught?
- Whatarethepedagogicalimplicationsforteachingandtrainingnursesandcare
workerstoconveyconsolation?
Theseissueswillbediscussedinthefollowing:
81
10.4.1Cancompassionbetaught?Halifax(2012)pointsoutthatthefactorswhichfostercompassionarenotwell
understood.Accordingtoher(2012),whethercompassionisaninherentpersonal
quality,orifitcanbetaughtandlearnedisacentralquestionintheemergingfieldof
compassionresearch(Halifax,2012,2014;Sinclairetal.,2016;StanfordUniversity
SchoolofMedicine,2008).Theanswertothisquestionisimportantbecauseithas
pedagogicalimplicationsforteachingandtrainingcurrentandfuturenursesandcare
workerstoconveyconsolation.
Whiletheconventionaldescriptionofcompassionisbasedontwomaincomponents
fromtheaffectivedomain:theaffectivefeelingofcaringforthesuffererandthe
motivationtorelievesuffering(Lazarus,1991),Halifax(2012,2014)drawingonrecent
neuroscienceresearch,describescompassionasacontingentandemergentprocess,
whicharisesoutoftheinteractionbetweenanumberofinterdependentnon-
compassionelements,whichbelongtothecognitiveandbehavioraldomainsaswellas
theaffectivedomains.AccordingtoHalifax(2012,2014),thesenon-compassion
elements,(whichincludeattentionandaffect(theaffectivedomain),intentionand
insight(thecognitivedomain)andembodimentandengagement(thebehavioral
domain)),interactwitheachotherinacomplexandadaptivesystem.Asaconsequence,
onecannotdirectlytrainincompassionperse,accordingtoHalifax(2012,2014).
However,Halifax(2012,2014)pointsoutthatonecanindirectlysetthefieldforthe
emergenceofcompassionbytrainingtheindividualinsituationsandprocesseswhich
arerelatedtothenon-compassionelementsintheaffective,cognitiveandbehavioral
domains.Theconsolationprocesswhichemergedthroughthestudy,bearsclose
resemblancetothecontingentandemergentprocessbetweentheaffective,cognitive
andbehavioralnon-compassionelementswhicharedescribedinHalifax’s(2012)model
ofenactivecompassion.Assuch,conveyingconsolingcanbeunderstoodasaformfor
enactivecompassion(Halifax,2012).Thisisillustratedinfigure1:

82
Figure1: Conveying consolation through “enactive compassion” based on Halifax (2012)
AccordingtoHalifax’sresearch(2012,2014),itispossibletoindirectlyprimenurses’
andcareworkers’capacityforcompassionbydesigningteachingandtrainingschemes,
aimedatdevelopingnursingcompetencies,whichpertaintothetrainablenon-
compassionelements.Thefollowingtableprovidesasummaryoftheconsolation
challengesandcompetencies,whichwereidentifiedinthethreepapersandtheir
relationshiptoHalifax’s(2012,2014)“non-compassionelements”.
BehavioraldomainConsolingactions:
Respondingappropriatelytopatient'sverbalandnonverbalcues
Consolingthroughpresence,sharedsilenceandphysicaltouch
Consolingthroughspiritual,existentialandreligiousconversations
Alternatingskillfullybetweentalkinglisteningandbeingsilent
Cognitivdomain:Clinicaljudgementand
reflection-assesspatients'needstodecideonthebestcourseofactionandevaluate
outcomes
Affectivedomain:Sensningpatients'suffering
Embodiedreactionstopatients'suffering
Emotionalambivalencetoengageinpatients'sufferingMusteringcouragetobeopen
tothepatients'suffering

83
Table 1. Overview of the nurses’ consolation challenges and competencies Non-compassionelements(Halifax2012,2014)
Consolationchallenges Competenciesneededtoprovideconsolationthrough“enactivecompassion”(Halifax2012,2014)
AffectiveDomainAttentionandaffect
Emotionalchallenges:- Painfulembodiedreactionsto
patients’suffering
- Fearofdeathanddying- Vulnerabilityandhelplessness- Experiencingreluctanceand
ambivalencetosharethepatients’suffering
Couragetoovercomeemotionalchallengesinordertoremainopenandreceptivetothepatients’sufferingCouragetoengageinconsolingactions
- Personalandprofessional
maturityandexperience
- Self-awareness
CognitiveDomainIntentionandinsight
Overcominguncertainty:- Beinguncertainaboutthe
patients’spiritualandexistentialsufferingandneeds
- Beinguncertainaboutthebestcourseofaction
- Beinguncertainabout
addressingdyingpatients’religiousissues
- Risktaking
Clinicaljudgmentandreflection- Assessingpatients’spiritual
andexistentialsufferingandneeds
- Decidingonthebestcourseofaction
- Evaluatingtheoutcomes
BehavioralDomain:Embodimentandengagement
Providingappropriateresponsestopatients’verbalandnonverbalcues:
- Usingnaturalopeningsto
integrateconsolationwhilstperformingnursingcare
- Adoptingbehaviortomatchfluctuationsinthepatients’physical,psycho-socialandspiritual/existentialsuffering
Relationalandpresencingskills:- Beingwiththedying:
Consolingthroughsilentpresencingandphysicaltouch
- Engaginginspiritual,existentialand/orreligiousconversations
- Alternatingskillfullybetweentalking,listeningandsharingthesilence

84
10.4.2Cancouragebetaught?
Asmentionedinsection10.3.2Jordan(2003)describescourageastheabilitytobe
movedandaffectedbyothersandtoembraceandacceptvulnerabilityanduncertainty.
Thisposesanimportantpedagogicalquestion:Isitpossibletoteachandtrainnurses
andcareworkerstoovercometheirfearsandreluctancetowalkwiththedyingtoshare
theirsuffering(Norbergetal.,2001)?
WhileThorupetal.(2012)foundthatcourageisaprerequisiteinnerquality,which
contributestothenurturanceofpersonalandprofessionaldevelopment;theyalsopoint
outthatcourageisnotonlyanisolatedandinherentquality,becauseaspectsofvolition
arealsoinvolvedinnurses’courageousactions.Takingthisintoconsideration,itseems
reasonablethatthevolitionalaspectsofcouragemaybedeveloped.Thissuggeststhatit
ispossibletotrainone’sabilitytoactcourageously.Inthefollowingthiswillbe
discussedinlightofGoud’s(2005)studyconcerningthenatureanddevelopmentof
courage.Drawingonseveralpsychologicalschoolsandtheorists,whichemphasizethat
allorganicandhumanlifehasaninnatedrivetowardsgrowthandself-actualization
(Horney,1950;Jung&VonFranz,1968;Maslow,1968,1972;Maslow,Frager,Fadiman,
McReynolds,&Cox,1970;Rogers,1961,1980).Goud(2005,p.102)definescourageas
the“energizingcatalystforchoosinggrowthoversafetyneeds”.AccordingtoGould
(2005)agapiscreatedwhenevergrowthforcesencounterpowerfulsafetyforces
(fears)andthisgapmustbeleapedinorderforgrowthtoproceed.Gould(2005)points
outthatcourageallowsonetoeffectivelyactunderconditionsofdanger,fear,andrisk.
Withoutcourage,theindividualorgroupremainsstuckinexistingpatternsor
immobilizedinfear.
Inordertopresentaconceptualmodelofcourageandtodescribeguidelinesfor
developingcourageGoud(2005)examinedavarietyofdisciplinesfortheirviewson
courage.Thedisciplinesspannedfrommilitaryhistoryandresearch,variousschoolsof
psychology,literatureandphilosophy.Gould(2005)performedacontentanalysisofthe
divergentsourcesofliterature,whichyieldedthreeprimarydimensionsofcourage,
whichincluded:fear,appropriateactionandahigherpurpose.Gould(2005)foundthat
whiletherearewidevariationsamongstudentsofcourageastothekindsoffears,

85
whichinvolvecourage,allseemtoagree,thatfacingfearsisessentialinacourageous
act.However,inlightofAristotle,Gould(2005)maintainsthatactinginthefaceoffear
isnotenough.Onemusthaveahigherpurposeforacourageousact.Drawingon
Nietzsche,Goud(2005)statesthatthelevelofcommitmenttoacourageousactis
directlyrelatedtoafeltsenseofpurpose.AccordingtoGoud(2005)ahigherpurpose
referstoaffirmingorsecuringavaluebeyondone’sself-interests.Assuch,thenurses’
deeprelationalconnectionwiththeirdyingpatientsandtheirmoralresponsibilityto
consolethem(paperIandII)canbecharacterizedasacourageoushigherpurpose.
(Conveyingconsolationasamoralresponsibilityhasbeendiscussedinsection10.1.6)
Figure 2: Goud’s (2005) three-dimensional model of courage applied to the study
HIGHERPURPOSE:Amoralresponsibilitytoalleviatedying
patients'spiritualandexistentialsuffering
OVERCOMINGFEARS:Embracingand
acceptingvullnerability,
mortality,professionalhelplessnessand
uncertainty
COURAGEAPPROPRIATEACTIONS:Conveyingconsolation

86
Asmentionedearlier,althoughstudies(Halifax,2012,2014;Thorupetal.,2012)
indicatethat,compassionandcourageseemtobeinherentpersonalqualities,these
studiesalsoindicatethatitmaybepossibletocultivatethesequalitiesthroughtraining.
Goud’s(2005)studywhich,drawsonRachman’sresearch(1978)supportsthese
results.AccordingtoRachman(1978),citedinGoud(2005),trainingindangerousjobs
suchasfirefighting,emphasizesgradualandgraduatedpracticeofthedangeroustasks.
Rachman(1978)concludedthat:“Courageousbehaviorisdeterminedpredominantlyby
thecombinationofcompetenceandconfidence,andbothofthesequalitiesare
strengthenedbyrepeatedandsuccessfulpractice.”(Rachman,1978,p.248),citedin
Goud(2005,p.111).Assuch,practicingforcourageisaprocessofmoral,psychological,
andphysical“toughening”accordingtoGoud(2005).Henceforth,“doingtherightthing”
inthefaceoffeardemandsagoodamountofconfidence,fortitudeanddiscipline.
Accordingly,developingtheabilitytotoleraterisksanduncertainty,meansaccepting
fearandanxietyaspartofthisprocess,ratherthansomethingtobeavoided(Goud,
2005).
DrawingonRachman(1978),Gould(2005)statesthatdevelopingconfidenceandself-
efficacy,observingrolemodelsandbolsteringasenseofpurposearepotentforcesfor
developingcourageandcounteractingfears.Developingconfidenceinone’scapabilities
isaprimaryforceincounteringfears,risksandthesafetyimpulse,whereself-efficacy,
whichisaspecificformofself-confidence,isofspecialimport.Self-efficacyisan
estimateofone’scapabilitiestohandlespecificchallengesandtasks.AccordingtoGoud
(2005)self-efficacyisanimportantdeterminantofhowmucheffortpeoplewillexert
andhowlongtheywillpersevereinthefaceofsignificantchallenges.Inlightof
Rachman’s(1978)summaryofstudiesaboutfearandcourage,Goud(2005)
recommendsrisktakingandcomfortzoneexpansionasameansforcourage
development.Theideaistoengagethelearneringradualrisktakingactivities,which
arejustbeyondtheindividual’scomfortzone(inthesamewayaparentcoaxesatoddler
totakeafewsteps).Attemptingtaskstoofarbeyondone’scapabilitiesusuallyresultsin
overwhelmingfailureandfears.Thefearfulpersonwillthen,quitereasonablyretreatto
safetyandbeextremelyhesitanttoriskanynewbehaviors.
87
Inadditiontofacilitatingcouragebuildingopportunitiesthroughactivities,which
involvegradualriskexposure,Goud(2005)recommendsobservationallearningor
modelingasanotherpowerfulmodalitytodevelopcourage.DrawingonBandura
(1986),Goud(2005)statesthatwatchingsomeonesimilartooneselfsucceedinatask
tendstoincreaseone’sconfidenceinperformingthesametasks(whilethereversalso
holdstrue).AccordingtoGoud(2005),beingexposedtodirectmodelsthat
demonstratecourageousbehaviorsincreasesthelikelihoodthatitwillencouragethe
samebehaviorsintheobserver.Goud’s(2005)researchsupportstheresultsinpaperIII
whichshowthatsituated,relationalandexperientialteachingapproachesintheclinical
contextseemtobeanefficientmeanstoteachandtraincareworkerstoprovide
spiritualandexistentialcareforthedying.Thiswillbeexplicatedinthefollowing:
ThemobilehospicenurseteachingteaminpaperIIIfrequentlyexperiencedthatthe
careworkersfeltfearfulandreluctantaboutaddressingtheirdyingpatients’spiritual
andexistentialsuffering.Theteachingteambelievedthatthecareworkers’fearof
exposingthemselvestotheirpatients’spiritualandexistentialsufferingstemmedfrom
personalinsecurityaswellasinsufficientcommunicationandlisteningskills(paperIII
p.5).Tostrengthenthecareworkers’courageandcompetency,themobileteaching
teamtransferredtheirpersonalspiritualandexistentialcareknowledgethrough
situatedbedsideteaching,whichinvolvedparticipatingactivelyinpatientcaretogether
withthecareworkers.Actingasrolemodelsandbyprovidingindividualsupervision
andfeedbackbefore,duringandafterpatientcare,theteamgraduallyencouragedthe
careworkerstoconductthespiritualandexistentialcareconversations,whichthey
wereafraidofinitiating.
Inthebeginning,theteammemberswouldactasrolemodels,(Goud,2005):“Sometimes
theyneedtohearthekindofquestionsIaskandseehowIrelatetothepatient.”(paper
IIIp.5)Theteachingteamgraduallyencouragedthecareworkerstostepoutoftheir
comfortzone(Goud,2005)toconductthepatientconversationsindependentlywhile
theteammemberwouldstayinthebackgroundtoprovidesupport.Astheteaching
teamobservedthatthecareworkersbecamemorecourageousandcompetent,they
graduallywithdrewtheirsupport,transferringtheresponsibilitytothecareworkers:

88
“Manyjustneedalittlepushandencouragementtotalkwiththepatientsalone,using
measaconversationpartnertohelpthemreflectonhowtheyhandledthesituation.”
(paperIIIp.5)Accordingtothemobilehospicenurseteachingteam,supervising,
supportingandencouragingthecareworkersthroughtheirchallengesoveraperiodof
timehadmadethemmorecourageoustobewiththedyingandtotalkwiththemabout
theirspiritualandexistentialsuffering.Drawingoncareworkerfeedbackandtheirown
observations,theteachingteamconsideredthatsituatedbedsideteachinghadprovento
beanimportanttool:”WhenIhaveaccompaniedthesamecareworkertothesame
patientsseveraltimesI’venoticedthattheyhavegraduallybecomebraverbecausethey
actuallydaretoasktheirpatientssomeofthedifficultquestions.”(paperIIIp.6)……”I
seethattheydaretoinvolvethemselvesmoreinthesesituations,exposingtheir
vulnerability.Iseethattheyhavebecomebraver.”(paperIIIp.6)
10.5Pedagogicalimplications
Asmentionedinsection10.4.1and10.4.2,studiesindicatethatitispossibletoprime
nurses’andcareworkers’courageandcompassiontoconveyconsolationthrough
training(Goud,2005;Halifax,2012,2014;Thorupetal.,2012)andthatthismight
increasetheirendurancetobewiththedying.(Seesection10.2.3)
Inthefollowing,thepedagogicalchallengesrelatedtoteachingandtrainingnursesand
careworkerstoconveyconsolationwillbediscussedinlightofeducationalnursing
research,whichdrawsontheAristotelianconceptofphronesis(Benner,1984,2000a,
2000b;Benner,Sutphen,Leonard,&Day,2010;Rowe&Broadie,2002)andsituated
learningtheory(Brown,Collins,&Duguid,1989;Gieselman,Stark,&Farruggia,2000;
Lave&Wenger,1991).
AccordingtoÖhlen(2001),Aristotleviewshumanactionasapracticalskillwhich
involvesthefollowingthreeknowledgeforms:episteme,(theoreticalorformal
knowledge),techne(hands-onskills)andphronesis(thepersonalabilitytotakeactionin
awiseandprudentmanner).Öhlen(2001)pointsoutthatallthreeknowledgeformsare
eachother’sprerequisites.Assuch,noneofthemaresufficientalone.Theabilitytoact
prudentlyandwiselytoalleviatesuffering(phronesis)presumestheoreticalknowledge
89
(episteme)aboutsufferingandalleviatingsufferingaswellashands-onnursingskills
(techne)toalleviatethatsufferingandviceversa(Öhlen,2001)
Thestudyrevealedthatconsolingthedyingwasacomplex,multidimensionaland
deeplypersonalandrelationalnursingchallengewhichdemandingclinicaljudgment
andreflectivepractice.Thisisillustratedinthethreepaperswhichshowthatthenurses
(paperIandII)andthehospicenurseteachingteam(paperIII)strovetointegrateand
mergedtheirtheoreticalandpracticalknowledgeintoaholisticefforttoconsoleand
easethespiritualandexistentialsufferingofthedying.(ThisisillustratedinFigure1
andTable1insection10.4.1.)
TheresultsshowthatboththenursesinpaperIandIIandthehospicenurseteaching
teaminpaperIII,demonstratedaformforspiritualandexistentialcare,whichis
consistentwithSwintonandPattison’s(2010)pragmaticandfunctionalapproachto
spiritualityandspiritualcare,whichhasbeendescribedinchapter4.2.Accordingto
SwintonandPattison(2010)inordertoprovidefunctionalandpragmaticspiritualand
existentialcare,nursesandcareworkersmusthavethecompetencytoidentifyand
respondeffectivelytotheparticularspiritualandexistentialqueststhattheyencounter,
withinwhateversituationtheyfindthemselvesin.SwintonandPattison(2010,p.235)
notethat:
whatiscalledforintermsofnurseeducationisthereforeflexibilityandconsciousnessraising.Thiswillmeanteachingnursesthesignificanceofspiritualityinwaysthatareflexibleandcontextuallyworkableandraisesthenurses’consciousnesstodimensionsoftheircaringpracticesthatareoftenhiddenorforgotten.
Hence,torisetothechallengeofconsolation,nursesandcareworkersareinneedof
phroneticknowledge(Öhlen,2001).Thiswillbeexplicatedinthefollowing:
DrawingonAristotle,Benner(2000a)pointsoutthatlearningtobeagoodpractitioner
requiresdevelopingthemoralimaginationandskillsofbeingagoodpractitioner.
AccordingtoBenner(2000a),Aristotlelabeledthekindofknowingwhichrequires
moralagency,discernmentandrelationshipasphronesis,incontrasttotechne,which
involvesknowledgeaboutmakingthingsorproducingoutcomesandshe(2000a)

90
emphasizesthatnursing,asapracticerequiresbothtechneandphronesisasdescribed
byAristotle.Benner(2000a)emphasizesthatwhiletechne,ortheactivityofproducing
outcomes,isgovernedbyameans-endrationality,phronesisbycontrast,islodgedina
practicewhichcannotrelystrictlyonameans-endrationalitybecauseone’sactsare
governedbyconcernfordoinggoodinparticularcircumstances,wherebeingin
relationshipanddiscerningparticularhumanactionsareatstakeandguideaction.
Benner(2004)emphasizesthatmeansandendsareinextricablyrelatedincaringforthe
ill.
AccordingtoBenner(2000a,2004)thenurseandthepatientbendandrespondtoeach
othersothathorizonsandtheworldareopenedandreconstitutedsothatnew
possibilitiesemerge.Healingandrecoveryofone’sembodiedrelationshiptotheworld
ismysterious.Itislivedratherthanmasteredandrequiresrelationship,opennessand
trust.(Benner’sviewpoints(2000a,2004)resonatewiththerelationalandhealing
dimensionsofconsolation,whichhavebeendiscussedinsections10.1.2and10.1.3.)
Hence,techniquealonecannotaddresstheinterpersonalandrelationalresponsibilities,
discernment,situatedpossibilitiesandchallengesthatnursesandcareworkers
encounterintheireffortstoconsolethevulnerablesufferinganddying.
Benner(2000a)notesthatthephroneticknowledgewhichexperiencednursespossess
canonlybetransferredtothelessexperiencedthroughsituatedexperientiallearningin
communitiesofpractitionerswhoforthesakeofgoodpracticecontinuetoliveoutand
improvepractice.Oneofthefeaturesoflearninginapracticecontextisthatexpertsare
abletoguidenovicesthroughthecomplexitiesofpractice(Benner,1984).Benner
(1984)emphasizesthatmuchclinicalknowhowissituationalandtacitandcanonlybe
demonstratedastheparticularsituationarises.Thevarietyandexceptionsinactual
clinicalpracticeeludetextbookdescriptionsbutgraduallyyieldtotheexperienced
nurse’sfundofpastsimilaranddissimilarsituations.Itisthisdemonstrationthatisso
essentialtothenovice(Benneretal.,2010).Benner(1984,2000a)andBenneretal.’s
(2010)viewpointsaresupportedbysituatedlearningtheorists,whomaintainthat
knowledgeisembeddedwithinthecontextinwhichitisusedandcannotbeseparated
fromtheactivity,contextandcultureofthatsituation(Gieselmanetal.,2000).
AccordingtoLaveandWenger(1991)situatedlearningiscentralforbecoming

91
proficientandtheystatethatlearninginpracticeisamatterofacculturation,ofjoininga
communityofpractice,ratherthantheapplicationofdecontextualizedskillsand
principles.
AccordingtoConeandGiske’s(2013)study,nursingstudentsneedtoseehowspiritual
carecanbepromotedinthefastpacedhospital-environmentaswellasotherclinical
settings,andtheypointoutthatmakingspiritualcareassessmentsandinterventions
morevisibleandexplicitinclinicalstudieswillpromotestudents’maturationandthus
improvetheirprofessionalgrowth.ConeandGiske(2013)foundthatthereisagreat
needfornursingstudentstoseenurseswhorole-modelassessment,spiritualcare
givinganddocumentation,andthey(2013)pointoutthatnursescanplayakeyrolein
providingsupportforstudentstostayindifficultorchallengingsituations.By
promotinganopenatmospherefornursingstudentsitiseasierforthemtoovercome
theirvulnerabilityandtosafeguardethicalissues.ConeandGiske(2013)pointoutthat
althoughtheimportanceofrolemodelingiswidelyreportedintheliteratureitisoften
missinginpractice.Thischallengesnurseeducatorstocollaboratewithnursestohelp
thembemoreexplicitinsharinghowtheyprovidespiritualcare.Ifnurseeducatorsare
notdirectlyinvolvedinclinicalsupervisionofstudentsitiscriticallyimportantforthem
toassistnursesandnursepreceptorstomodelspiritualcareassessmentand
interventionsandtodemonstratehowitisdiscussedanddocumentedasapartof
nursingresponsibilities(Cone&Giske,2013).ConeandGiske(2013)emphasizethat
thisisespeciallyimportantinaNorwegiancontextwerespiritualityandreligionare
regardedasveryprivateandpersonalareas(Botvar&Schmidt,2010;Stifoss-Hanssen,
1999;Stifoss-Hanssen&Kallenberg,1998;Ulland&DeMarinis,2014).
10.5.1Recommendations
Theresultsfromthisstudysuggeststhatnursingleaders(inspecialistcareaswellasin
homecareandnursinghomes)andnurseeducatorsshouldcollaboratetocreate
teachingandtrainingschemesbasedonsituatedexperientialandrelationalteaching
formats,inordertoenablecurrentandfuturenursesandcareworkerstoprovide
competentandcompassionatespiritualandexistentialcareforthedying.Thisis
supportedbysituatedlearningtheory(Brownetal.,1989;Gieselmanetal.,2000;Lave&

92
Wenger,1991),andeducationalnursingresearch(Benner,1984,2000a,2000b,2004;
Benneretal.,2010;Cone&Giske,2013),whichunderpintheimportanceofdeveloping
phroneticspiritualandexistentialcarecompetencybylearningfromexperienced
nursesincommunitiesofclinicalpractice(Lave&Wenger,1991).
Nevertheless,althoughthestudyshowsthatthenurses’maturityaswellastheir
personalbeliefsandprofessionalexperiencewereimportant(asillustratedinthe
consolationnarrativesinsection10.1.2),thestudyalsoshowsthatsometimesthiswas
notenough.Withtheexceptionofthetwonurseswhohadstudiedtheologypriorto
takingupnursingcareers,thenursessaidtheyhadmixedfeelingsabouttheirabilityto
provideexistentialandspiritualcarebecausetheyfeltinsecureanduncertainabout
providingreligiousconsolation(paperIp.4).Accordingtothenurses,theirdiscomfort
anduncertaintystemmedfromtheirownpersonalattitudestowardsreligion(paperI
p.4)astheydidnotconsiderthemselvestobereligiousor“veryChristian”asoneof
themputit(paperIIp.5.)andtheyalsoexpressedthattheydidnothaveenoughformal
knowledgeaboutreligion.(Seesection10.1.1)
Thissuggeststhatspiritualandexistentialcareneedstobe“moved”fromtheprivate
commitmentoftheindividualnurseandcareworkertoapublicunderstanding(Ødbehr,
2015).Practicaltrainingprogramsinspiritualandexistentialcareshould,(inaddition
toprovidingexperientiallearningopportunitiesthroughsituatedbedsideteaching),
introducenursesandcareworkerstothenatureandlexiconoflivedreligion,religious
perspectivesonsufferingandreligiousreasoning(Pesut,2016;Swinton&Pattison,
2010).Practicaltrainingprogramscouldalsoincludeinterdisciplinaryandcross
professionalcollaborationbetweennursingstaffandchaplains.(Ødbehr,2015).This
mightenhancenurses’andcareworkers’couragetorisetothechallengeofconsolation
insituationswherethecomplexitiesofspiritualityandreligioncomeintoplay:AsPesut
pointsout:“Thedegreetowhichpatientscontinuetobringreligiousperspectivesto
careisthedegreetowhichnursingneedstoconsiderthoseperspectives.”(Pesut,2016,
p.7)

93
Baldacchino(2011)constructedastudyunitinspiritualcareforqualifiednursesnamed
“SpiritualCopinginIllnessandcare”.Thestudyunitconsistedof4ECTSandemployeda
varietyofdidacticmethods,whichincludedlectures,patientcasestudies,smallgroup
discussionsandsharingclinicalexperiences,self-reflectiveexercisesonpersonal
spiritualityandnursingpractice.AccordingtoBaldacchino(2011),theevaluation
reportedthatthestudyunithadbeenbeneficialasthelearnershadtimetothink
criticallyabouttheirownspiritualityandtheircurrentclinicalpractice.Theevaluation
suggestedthatthenurses’increasedknowledgeaboutconceptsofspirituality,spiritual
distress,spiritualwellbeing,spiritualcopingandspiritualcareappearedtohelpthemto
seethepossibilityofmeetingpatients’needsthroughtheimplementationofholistic
careandtobecomearesourceofknowledgefortheircolleagues.However,Baldacchino
(2011)alsopointedoutthatinalong-termperspective,mentorshipisneededinorder
toenablenursestoputtheoryintopracticeandtosustaintheminpracticingwhatthey
havelearned.
Alessqualifiedworkforceincreasinglydominatesnursinghomesandhomecarenursing
atatimeofincreasingprevalenceofcomplexheathconcerns(Annearetal.,2014;
Colomboetal.,2011;Leclercetal.,2014;NorwegianMinistryofHealthandCare
Services,2012).Mobileexpertnurseteachingteamsinspiritualandexistentialcare,
(andotherrelevantfieldsofnursing,suchashospice,dementiaandgeriatriccare)may
beapedagogicallyeffectiveandpracticalmeanstoredressthewideninggapbetween
workforcequalityandthedemandforhighqualitycareinprimaryhealthcare(Annear
etal.,2014).However,whilethelevelofindividualnursingcompetencyisimportant,
onemustalsokeepinmindthatthequalityofthecarewhichisdeliveredalsorestson
institutionalvariables,suchasthegeneralworkplaceculture,philosophy,leadership
andorganizationofcare,includingtimeandstaffresources(Caseyetal.,2011).

94
11.Concludingremarks
Thestudyshowsthatconsolationisadeeplyrelationalpractice,andthatenteringinto
relationshipswiththesufferinganddyingdemandscourageandcompassion.Being
willingtoembraceandacceptone’sownaswellasthepatients’vulnerability,mortality
andhelplessnessrequirespersonalmaturityandenduranceaswellasclinical
competencyandprofessionaljudgment(phronesis).Thestudysuggeststhatnursesand
careworkersmayeasesomeofthedyingpatient’sexistentialandspiritualloneliness
throughthepowerofconsolingpresence.Whennothingelsecanbedone,bearing
witnessandsharingthepatients’sufferingmaybeconsolingactsinthemselves.Nurses
andcareworkersinend-of-lifecareconfrontintractablesuffering.Hence,theycannot
alwaysexpecttobesuccessfulintheireffortstoalleviatethespiritualandexistential
sufferingofthedying.Therefore,thestudyresults,whichindicatethatconsolationcan
beconveyedandsustainedthroughpresenceandrelatedness,areextremelyimportant.
Furtherempiricalresearch(qualitativeaswellasquantitative)isneededtouncover
hownursesprovidespiritualandexistentialcarefordyingpatientsineverydaypractice
andtodevisepractical,experientialandrelationaltoolsandcurriculatoteachandtrain
currentandfuturenursingstaff(nursesandcareworkers)toprovidecompetentand
compassionatespiritualandexistentialcareforthedying.Suchresearchisanimportant
andvaluableknowledgesupplementtotheoreticalstudiesinthisfield.

95
ReferencesAbbey,J.,Froggatt,K.A.,Parker,D.,&Abbey,B.(2006).Palliativecareinlong-termcare:
asysteminchange.InternationalJournalofOlderPeopleNursing,1(1),56-63.doi:10.1111/j.1748-3743.2006.00010.x
Annear,M.,Lea,E.,&Robinson,A.(2014).Arecareworkersappropriatementorsfornursingstudentsinresidentialagedcare?BMCNursing,13(1),44.
Appleton,J.V.(1995).Analysingqualitativeinterviewdata:addressingissuesofvalidityandreliability.JournalofAdvancedNursing,22(5),993-997.
Avis,M.,&Freshwater,D.(2006).Evidenceforpractice,epistemology,andcriticalreflection.NursingPhilosophy,7(4),216-224.
Bachner,Y.,O'Rourke,N.,&Carmel,S.(2011).FearofDeath,MortalityCommunication,andPsychologicalDistressAmongSecularandReligiouslyObservantFamilyCaregiversofTerminalCancerPatients.DeathStudies,35(2),163-187.doi:10.1080/07481187.2010.535390
Back,A.L.,Bauer-Wu,S.M.,Rushton,C.H.,&Halifax,J.(2009).Compassionatesilenceinthepatient-clinicianencounter:acontemplativeapproach.JournalofPalliativeMedicine,12(12),1113-1117.doi:10.1089/jpm.2009.0175
Back,A.L.,Rushton,C.H.,Kaszniak,A.W.,&Halifax,J.S.(2015).“WhyAreWeDoingThis?”:ClinicianHelplessnessintheFaceofSuffering.JournalofPalliativeMedicine,18(1),26-30.
Balboni,M.J.,Sullivan,A.,Amobi,A.,Phelps,A.C.,Gorman,D.P.,Zollfrank,A.,...Balboni,T.A.(2013).Whyisspiritualcareinfrequentattheendoflife?Spiritualcareperceptionsamongpatients,nurses,andphysiciansandtheroleoftraining.JournalofClinicalOncology,31(4),461-467.doi:10.1200/jco.2012.44.6443
Baldacchino,D.R.(2011).Teachingonspiritualcare:Theperceivedimpactonqualifiednurses.NurseEducationinPractice,11(1),47-53.
Bandura,A.(1986).Socialfoundationsofthoughtandaction:Asocialcognitivetheory:Prentice-Hall,Inc.
Belzile,J.A.,&Öberg,G.(2012).Wheretobegin?Grapplingwithhowtouseparticipantinteractioninfocusgroupdesign.QualitativeResearch,12(4),459-472.
Benner,P.(1984).Fromnovicetoexpert:excellenceandpowerinclinicalnursingpractice.MenloPark,Calif.:Addison-Wesley.
Benner,P.(2000a).Therolesofembodiment,emotionandlifeworldforrationalityandagencyinnursingpractice.NursingPhilosophy,1(1),5-1915p.
Benner,P.(2000b).Thewisdomofourpractice.AJNTheAmericanJournalofNursing,100(10),99-105.
Benner,P.(2004).UsingtheDreyfusmodelofskillacquisitiontodescribeandinterpretskillacquisitionandclinicaljudgmentinnursingpracticeandeducation.Bulletinofscience,technology&society,24(3),188-199.
Benner,P.,Sutphen,M.,Leonard,V.,&Day,L.(2010).Educatingnurses:acallforradicaltransformation.SanFrancisco,Calif.:Jossey-Bass.
Benner,P.,&Wrubel,J.(1989).Theprimacyofcaring:Stressandcopinginhealthandillness:Addison-Wesley/AddisonWesleyLongman.
Benzein,E.(1999).Tracesofhope.(PhD.thesis),UmeåUniversity,MedicalDissertations,UmeåUniversity(NewSeriesNo.636–ISSN0346-6612)
Biblegateway.(2011).TheNewTestament,NewInternationalVersion.Retrievedfromhttps://www.biblegateway.com/passage/?search=Luke+10%3A25-37

96
Bollig,G.,Rosland,J.H.,&Husby,B.(2013).AchievementandchallengesofpalliativecareinNorway.EuropeanJournalofPalliativeCare,20,256-259.
Bosma,H.,Apland,L.,&Kazanjian,A.(2010).Culturalconceptualizationsofhospicepalliativecare:moresimilaritiesthandifferences.PalliativeMedicine,24(5),510-522.doi:10.1177/0269216309351380
Boston,P.,Bruce,A.,&Schreiber,R.(2011).Existentialsufferinginthepalliativecaresetting:anintegratedliteraturereview.JournalofPainandSymptomManagement,41(3),604-618.
Boston,P.,&Mount,B.M.(2006).Thecaregiver'sperspectiveonexistentialandspiritualdistressinpalliativecare.JournalofPainandSymptomManagement,32(1),13-26.
Botvar,P.K.,&Schmidt,U.(Eds.).(2010).ReligionidagensNorge:mellomsekulariseringogsakralisering(ReligionincontemporaryNorway.Betweensecularizationandsacralization).Oslo:Universitetsforlaget
Brown,J.S.,Collins,A.,&Duguid,P.(1989).Situatedcognitionandthecultureoflearning.Educationalresearcher,18(1),32-42.
Bueckert,L.D.,&Schipani,D.S.(Eds.).(2006).SpiritualcaregivinginthehospitalWindowstochaplaincyministry.Kitchener,Ontario:PandoraPress.
Carlsen,B.,&Glenton,C.(2011).WhataboutN?Amethodologicalstudyofsample-sizereportinginfocusgroupstudies.BMCMedicalResearchMethodology,11(1),26.
Casey,D.,Murphy,K.,NiLeime,A.,Larkin,P.,Payne,S.,Froggatt,K.A.,&O’Shea,E.(2011).Dyingwell:factorsthatinfluencetheprovisionofgoodend-of-lifecareforolderpeopleinacuteandlong-staycaresettingsinIreland.JournalofClinicalNursing,20(13-14),1824-1833.
Cassell,E.J.(1991a).Thenatureofsufferingandthegoalsofmedicine:OxfordUniversityPress.
Cassell,E.J.(1991b).Recognizingsuffering.HastingsCenterReport,21(3),24-24.Cho,J.,&Trent,A.(2006).Validityinqualitativeresearchrevisited.QualitativeResearch,
6(3),319-340.Christensen,K.H.(2008).SpiritualcareperspectivesofDanishregisterednurses.
JournalofHolisticNursing,26(1),7-14.Clark,D.,&Seymour,J.(1999).Reflectionsonpalliativecare.BuckinghamPhiladelphia:
OpenUniversityPress.Coetzee,S.K.,&Klopper,H.C.(2010).Compassionfatiguewithinnursingpractice:A
conceptanalysis.Nursing&HealthSciences,12(2),235-243.Colombo,F.,Llena-Nozal,A.,Mercier,J.,&Tjadens,F.(2011).HelpWanted?:Providing
andPayingforLong-TermCare:OECDPublishing.Cone,P.H.,&Giske,T.(2013).Teachingspiritualcare–agroundedtheorystudyamong
undergraduatenursingeducators.JournalofClinicalNursing,22(13-14),1951-1960.
Costello,J.(2006).Dyingwell:nurses’experiencesof‘goodandbad’deathsinhospital.JournalofAdvancedNursing,54(5),594-601.
Cranz,G.(2000).TheAlexanderTechniqueintheworldofdesign:postureandthecommonchair.JournalofBodyworkandMovementTherapies,4(2),90-98.doi:http://dx.doi.org/10.1054/jbmt.1999.0162
Damasio,A.(1999).TheFeelingofWhatHappens,BodyandEmotionintheMakingofConsciousness.NewYork:Harcourt&BraceCo.
97
Dauenhauer,B.,&Pellauer,D.(2014).PaulRicoeur.TheStanfordEncyclopediaofPhilosophy.Summer2014.Retrievedfromhttp://plato.stanford.edu/archives/sum2014/entries/ricoeur/
Dehlholm-Lambertsen,B.,&Maunsbach,M.(1997).Qualitativemethodsinempiricalhealthresearch.III.Theindividualin-depthinterview.NordiskMedicin,112(3),94-98.
Delgado-Guay,M.O.,Hui,D.,Parsons,H.A.,Govan,K.,DelaCruz,M.,Thorney,S.,&Bruera,E.(2011).Spirituality,religiosity,andspiritualpaininadvancedcancerpatients.JournalofPainandSymptomManagement,41(6),986-994.
Delmar,C.(2004).DevelopmentofEthicalExpertise:AQuestionofCourage.InternationalJournalforHumanCaring,8(3).
Delmar,C.(2012).Theexcessesofcare:amatterofunderstandingtheasymmetryofpower.NursingPhilosophy,13(4),236-243.
DeMarinis,V.(2008).TheimpactofpostmodernizationonexistentialhealthinSweden:psychologyofreligion'sfunctioninexistentialpublichealthanalysis.ArchiveforthePsychologyofReligion/ArchivfürReligionspychologie,30(1),57-74.
DeMarinis,V.,Ulland,D.,&Karlsen,K.E.(2011).Philosophy’sroleforguidingtheoryandpracticeinclinicalcontextsgroundedinaculturalpsychiatryfocus:AcasestudyillustrationfromsouthernNorway.WorldCulturalPsychiatryResearchReview,6(1),47-56.
Devers,K.J.,&Frankel,R.M.(2000).PRACTICALADVICE,Studydesigninqualitativeresearch—2:Samplinganddatacollectionstrategies.Educationforhealth,13(2),263-271.
Eells,T.D.(1999).WhatDoWeKnowAboutMasterTherapists?TheJournalofPsychotherapyPracticeandResearch,8(4),314-317.
EuclidNetwork.(2012).RoundtableoninnovationandvalueinpalliativecareinEurope(Report).Retrievedfromhttp://www.euclidnetwork.eu/projects/current-projects/social-experimentation/roundtable-on-innovation-and-value-in-palliative-care-in-europe.html
Figley,C.R.(1995).Compassionfatigue:Copingwithsecondarytraumaticstressdisorderinthosewhotreatthetraumatized:Routledge.
Finlay,L.(2012).DebatingphenomenologicalmethodsHermeneuticphenomenologyineducation(pp.17-37):Springer.
Frankl,V.(1969).Thewilltomeaning:Principlesandapplicationoflogotherapy.World,NewYork.
Gadamer,H.-G.(2004).TruthandMethod(Second,RevisedEditioned.).LondonNewYork:Continuum.
Geanellos,R.(2000).ExploringRicoeur’shermeneutictheoryofinterpretationasamethodofanalysingresearchtexts.NursingInquiry,7(2),112-119.
Gieselman,J.A.,Stark,N.,&Farruggia,M.J.(2000).Implicationsofthesituatedlearningmodelforteachingandlearningnursingresearch.TheJournalofContinuingEducationinNursing,31(6),263-268.
Gjengedal,E.,Ekra,E.M.,Hol,H.,Kjelsvik,M.,Lykkeslet,E.,Michaelsen,R.,...Wogn-Henriksen,K.(2013).Vulnerabilityinhealthcare–reflectionsonencountersineverydaypractice.NursingPhilosophy,14(2),127-138.doi:10.1111/j.1466-769X.2012.00558.x
Golafshani,N.(2003).Understandingreliabilityandvalidityinqualitativeresearch.Thequalitativereport,8(4),597-606.

98
Goud,N.H.(2005).Courage:Itsnatureanddevelopment.TheJournalofHumanisticCounseling,EducationandDevelopment,44(1),102-116.
Graneheim,U.H.,&Lundman,B.(2004).Qualitativecontentanalysisinnursingresearch:concepts,proceduresandmeasurestoachievetrustworthiness.NurseEducationToday,24(2),105-112.
Groenvold,M.,Pedersen,C.,Jensen,C.,Faber,M.,&Johnsen,A.(2006).Kræftpatientensverden-enundersøgelseafhvaddanskekræftpatienterharbrugfor-resultater,vurderingerogforslag(Thecancerpatients'world-astudyofwhatDanishcancerpatientsneed).Retrievedfromhttp://forskningsbasen.deff.dk/Share.external?sp=Sdfb3a4b0-70eb-11dc-bee9-02004c4f4f50&sp=Sku
Gullestad,M.(1996).EverydayLifePhilosophers.Norway:Universitetsforlaget.Halcomb,E.J.,Gholizadeh,L.,DiGiacomo,M.,Phillips,J.,&Davidson,P.M.(2007).
Literaturereview:considerationsinundertakingfocusgroupresearchwithculturallyandlinguisticallydiversegroups.JournalofClinicalNursing,16(6),1000-1011.doi:10.1111/j.1365-2702.2006.01760.x
Halifax,J.(2012).Aheuristicmodelofenactivecompassion.CurrOpinSupportPalliatCare,6(2),228-235.
Halifax,J.(2014).GRACEfornurses:Cultivatingcompassioninnurse/patientinteractions.JournalofNursingEducationandPractice,4(1),121.
Hardiman,P.,&Simmonds,J.G.(2013).Spiritualwell-being,burnoutandtraumaincounsellorsandpsychotherapists.MentalHealth,Religion&Culture,16(10),1044-1055.
Harlos,M.(2010).Theterminalphase.InN.A.Christakis,Cherny,N.I(Ed.),Oxfordtextbookofpalliativemedicine.(Fourtheditioned.,pp.1549-1559).Oxford:OxfordUniversityPress.
Haug,S.H.K.(2015).”Theillnessexperiencesofolderpeoplewithincurablecancerinspecializedpalliativehealthcarecontexts.Aqualitativestudyinclinicalpsychologyofreligionoftheinteractionsbetweendailylivingandexistentialmeaning–making.”.(PhD,MFSchoolofTheology,OsloPhD),MFSchoolofTheology,Oslo,Oslo.
Haug,S.H.K.,Danbolt,L.J.,Kvigne,K.,&Demarinis,V.(2014).Howolderpeoplewithincurablecancerexperiencedailyliving:AqualitativestudyfromNorway.PalliativeandSupportiveCare,1-12.
Heidegger,M.(1962).Beingandtime(JohnMacquarrieandEdwardRobinson,Trans.).Oxford:BasilBlackwell.
Henoch,I.,&Danielson,E.(2009).Existentialconcernsamongpatientswithcancerandinterventionstomeetthem:anintegrativeliteraturereview.Psycho-Oncology,18(3),225-236.
Hess,J.D.(2003).Gadow'srelationalnarrative:anelaboration.NursingPhilosophy,4(2),137-148112p.
Hollinghurst,S.,Sharp,D.,Ballard,K.,Barnett,J.,Beattie,A.,Evans,M.,...Little,P.(2008).RandomisedcontrolledtrialofAlexandertechniquelessons,exercise,andmassage(ATEAM)forchronicandrecurrentbackpain:economicevaluation.BMJ,337.doi:10.1136/bmj.a2656
Holloway,M.,Adamson,S.,McSherry,W.,&Swinton,J.(2011).Spiritualcareattheendoflife:Asystematicreviewoftheliterature.DepartmentofHealth,London.
Horney,K.(1950).TheCollectedWorksofKarenHorney:Selfanalysis.Neurosisandhumangrowth(Vol.2):WWNorton.

99
Husserl,E.(1970).ThecrisisofEuropeansciencesandtranscendentalphenomenology:Anintroductiontophenomenologicalphilosophy(D.Carr,Trans.):Evanston,IL:NorthwesternUniversityPress.
Ilkjær,I.(2012).Ånde-nød:Enundersøgelseafeksistentielleogåndeligefænomenersbetydningforalvorligtsygepatientermedkronisklungelidelse.(Difficultiesinbreathing.Aninvestigationofsignificanceofexistentialandspiritualphenomenaforseriouslyillpatientswithchronicobstructivepulmonarydisease.).(Phd,DetTeologiskeFakultet,UniversitetetiKøbenhavn(UniversityofCopenhagen).).Retrievedfromhttp://curis.ku.dk/ws/files/63613346/Ingeborg_Ilkjaer_Aande_noed_til_CURIS.pdf
Ivic,S.(2009).Ricoeur’snarrativetheoryappliedtoscience.PhilosophicalPapersandReviews,1(3),044-051.
Jordan,J.V.(2003).Valuingvulnerability:Newdefinitionsofcourage.WorkinProgress,paperNo102,1-13.
Jordens,C.F.,&Little,M.(2004).‘Inthisscenario,Idothis,forthesereasons’:narrative,genreandethicalreasoningintheclinic.SocialScienceandMedicine,58(9),1635-1645.
Jung,C.G.,&VonFranz,M.-L.(1968).Manandhissymbols:Laurel.Kahn,D.L.,&Steeves,R.H.(1986).Theexperienceofsuffering:conceptualclarification
andtheoreticaldefinition.JournalofAdvancedNursing,11(6),623-631.Kalish,N.(2012).Evidence-basedspiritualcare:aliteraturereview.CurrOpinSupport
PalliatCare,6(2),242-246.doi:10.1097/SPC.0b013e328353811cKarlsson,M.,Friberg,F.,Wallengren,C.,&Öhlén,J.(2014).Meaningsofexistential
uncertaintyandcertaintyforpeoplediagnosedwithcancerandreceivingpalliativetreatment:alife-worldphenomenologicalstudy.BMCPalliativeCare,13(1),28.
Kitzinger,J.(1995).Qualitativeresearch.Introducingfocusgroups.BMJ,311(7000),299-302.
Klass,D.(1999).Thespirituallivesofbereavedparents:PsychologyPress.Klass,D.(2014).Grief,Consolation,andReligions:AConceptualFramework.OMEGA-
JournalofDeathandDying,69(1),1-18.doi:10.2190/OM.69.1.aKoenig,H.,King,D.,&Carson,V.B.(2012).Handbookofreligionandhealth:Oxford
universitypress.Kvale,S.,&Brinkmann,S.(2008).Interviews:Learningthecraftofqualitativeresearch
interviewing:SagePublications,Incorporated.laCour,P.(2008).Existentialandreligiousissueswhenadmittedtohospitalinasecular
society:Patternsofchange.MentalHealth,Religion&Culture,11(8),769-782.laCour,P.,&Hvidt,N.C.(2010).Researchonmeaning-makingandhealthinsecular
society:Secular,spiritualandreligiousexistentialorientations.SocialScienceandMedicine,71(7),1292-1299.
Lakoff,G.,&Johnson,M.(1999).Philosophyintheflesh:Theembodiedmindanditschallengetowesternthought:Basicbooks.
Lartey,E.Y.(1997).Inlivingcolour:aninterculturalapproachtopastoralcareandcounselling:Cassell.
Lave,J.,&Wenger,E.(1991).Situatedlearning:legitimateperipheralparticipation.Cambridge:CambridgeUniversityPress.
Lazarus,R.S.(1991).Emotionandadaptation.NewYork:OxfordUniversityPress.
100
Leclerc,B.S.,Lessard,S.,Bechennec,C.,LeGal,E.,Benoit,S.,&Bellerose,L.(2014).Attitudestowarddeath,dying,end-of-lifepalliativecare,andinterdisciplinarypracticeinlongtermcareworkers.JournaloftheAmericanMedicalDirectorsAssociation,15(3),207-213.doi:10.1016/j.jamda.2013.11.017
Lincoln,Y.S.,&Guba,E.G.(1985).Naturalisticinquiry.BeverlyHills,Calif.:Sage.Lindseth,A.(1992).Theroleofcaringinnursingethics.InG.Udén(Ed.),Quality
developmentinnursingcare.Frompracticetoscience(1ed.,pp.97-106).LinköpingUniversity,LinköpingSweden:LinköpingCollaborationCentreLCC.
Lindseth,A.(2015).BeingIllasanInevitableLifeTopicPossibilitesofPhilosophicalPracticeinHealthCareandPsychotherapy.InM.N.Weiss(Ed.),TheSocraticHandbook(Vol.Band9,pp.440).Wien,Österreich:LITVerlag.
Lindseth,A.,&Norberg,A.(2004).Aphenomenologicalhermeneuticalmethodforresearchinglivedexperience.ScandinavianJournalofCaringSciences,18(2),145-153.
Lundmark,M.(2006).AttitudestospiritualcareamongnursingstaffinaSwedishoncologyclinic.JournalofClinicalNursing,15(7),863-874.doi:10.1111/j.1365-2702.2006.01189.x
Løgstrup,K.E.(1956).DenEtiskeFordring(TheEthicalDemand)København:Gyldendal.Løgstrup,K.E.(1968).OpgørmedKierkegaard.København:Gyldendal.Løgstrup,K.E.(1971).Etiskebegreberogproblemer(Ethicalconceptsandproblems)
København:GyldendalskeBoghandel,NordiskforlagAS.Løgstrup,K.E.(1997).TheEthicalDemand(T.I.Jensen,Puckering,G.,Watkins,E.,
Trans.).NotreDame,Ill:UniversityofNotreDamePress.Løgstrup,K.E.(2007).BeyondtheEthicalDemand,withintroductionbyKeesvanKooten
Niekerk(SusanDewandHeidiFlegal,Trans.):UniversityofNotreDamePress,NotreDame,Indiana.
Malone,R.E.(2000).Dimensionsofvulnerabilityinemergencynurses'narratives.Advancesinnursingscience,23(1),1-11.
Malpas,J.(2015).Hans-GeorgGadamer.TheStanfordEncyclopediaofPhilosophyRetrievedfrom<http://plato.stanford.edu/archives/sum2015/entries/gadamer/>
Malterud,K.(2011).Kvalitativemetoderimedisinskforskning:eninnføring(Anintroductiontoqualitativemethodsinmedicalresearch).Oslo:Universitetsforl.
Martinsen,K.(1993).FraMarxtilLøgstrup.Ometikkogsanselighetisykepleien(FromMarxtoLøgstrup.Aboutethicsandsensitivityinnursing).TANOAS,Otta.
Martinsen,K.(1997).FromMarxtoLogstrup(Translationinprogress)(2ndedn.ed.).Oslo,Norway:Tano.
Martinsen,K.(2000).Øyetogkallet(TheEyeandtheCalling):Fagboklaget.Martinsen,K.(2006).Careandvulnerability:Akribe.Maslow,A.H.(1968).Towardapsychologyofbeing.NewYork:HarperandRow.Maslow,A.H.(1972).Thefartherreachesofhumannature:MauriceBassett.Maslow,A.H.,Frager,R.,Fadiman,J.,McReynolds,C.,&Cox,R.(1970).Motivationand
personality(Vol.2):Harper&RowNewYork.Masters,K.,&Hooker,S.(2013).Religion,spirituality,andhealth.InR.F.Paloutzian,&
Park.C.L(Ed.),Handbookofthepsychologyofreligionandspirituality(pp.519-539).NewYork,London:TheGuilfordPress.
McDonald,C.,&McIntyre,M.(2001).Reinstatingthemarginalizedbodyinnursingscience:epistemologicalprivilegeandthelivedlife.NursingPhilosophy,2(3),234-239.

101
McSherry,W.,&Jamieson,S.(2013).Thequalitativefindingsfromanonlinesurveyinvestigatingnurses'perceptionsofspiritualityandspiritualcare.JournalofClinicalNursing,22(21-22),3170-3182.doi:10.1111/jocn.12411
Merleau-Ponty,M.(1962).PhenomenologyofPerception[PhénoménologiedelaPerception](C.Smith,Trans.):Routledge&KeganPaul.
Merleau-Ponty,M.,Dreyfus,H.L.,&Dreyfus,P.A.(1964).Senseandnon-sense.Evanston,Ill.:NorthwesternUniversityPress.
Mishler,E.G.(1986).Researchinterviewing:contextandnarrative.Cambridge,Mass.:HarvardUniversityPress.
Morse,J.M.,Barrett,M.,Mayan,M.,Olson,K.,&Spiers,J.(2008).Verificationstrategiesforestablishingreliabilityandvalidityinqualitativeresearch.Internationaljournalofqualitativemethods,1(2),13-22.
Najjar,N.,Davis,L.W.,Beck-Coon,K.,&Doebbeling,C.C.(2009).Compassionfatigueareviewoftheresearchtodateandrelevancetocancer-careproviders.JournalofHealthPsychology,14(2),267-277.
Narayanasamy,A.(2014).TheChallengesofTeachingandLearningSpiritualityinNursing.JournalofNursingCare,3(189),2167-1168.1000189.
Noble,A.,&Jones,C.(2010).Gettingitright:oncologynurses'understandingofspirituality.InternationalJournalofPalliativeNursing,16(11),565-569.
Nolan,S.,Saltmarsh,P.,Leget,C.(2011).Spiritualcareinpalliativecare:workingtowardsanEAPCTaskForce.EJPC,18,86-89.
Norberg,A.(2001).ConsolingCareforPeoplewithAlzheimer'sDiseaseorAnotherDementiaintheAdvancedStage.Alzheimer'sCareToday,2(2),46-52.
Norberg,A.,Bergsten,M.,&Lundman,B.(2001).Amodelofconsolation.NursingEthics,8(6),544-553.
Nortvedt,P.(1998).Sensitivejudgement:aninquiryintothefoundationsofnursingethics.NursingEthics,5(5),385-386.
NorwegianDirectorateofHealth.(2015).Nasjonalthandlingsprogrammedretningslinjerforpalliasjonikreftomsorgen(Nationalactionprogramwithguidelinesforpalliativecancercare)Retrievedfromhttps://helsedirektoratet.no/retningslinjer/nasjonalt-handlingsprogram-med-retningslinjer-for-palliasjon-i-kreftomsorgen
NorwegianMinistryofHealthandCareServices.(2012).ReportNo10(2012-2013)totheStorting(Parliament).Goodquality-safeservicesQualityandpatientsafetyinhealthandcareservices.Oslo:FullversioninNorwegian:Stortingsmeldingnr.10(2012-2013)Godkvalitet-tryggetjenesterKvalitetogpasientsikkerhetihelseogomsorgstjenestenOslo:Helseogomsorgsdepartementet2012.Retrievedfromhttp://www.regjeringen.no/pages/38154897/PDFS/STM201220130010000DDDPDFS.pdf
Nouwen,H.,McNeill,D.,&Morrison,D.(2008).Compassion:areflectionontheChristianlife.London:Darton,LongmanandTodd.
NSD.(2016).DataProtectionOfficialforResearch.Retrievedfromhttp://www.nsd.uib.no/nsd/english/pvo.html
Onwuegbuzie,A.J.,&Leech,N.L.(2007).Validityandqualitativeresearch:Anoxymoron?Quality&Quantity,41(2),233-249.
Paley,J.(2008).Spiritualityandnursing:areductionistapproach.NursingPhilosophy,9(1),3-18.
Paloutzian,R.F.,&Park,C.L.(Eds.).(2013).Handbookofthepsychologyofreligionandspirituality.NewYorkLondon:GuilfordPress.

102
Pargament,K.I.(2013).ConversationswithEeyore:Spiritualityandthegenerationofhopeamongmentalhealthproviders.BulletinoftheMenningerClinic,77(4),395-412.
Park,C.L.(2013).RelgionandMeaning.InR.F.Paloutzian&C.L.Park(Eds.),Handbookofthepsychologyofreligionandspirituality:TheGuildfordPressNewYork.
Patton,M.Q.(1990).Qualitativeevaluationandresearchmethods:SAGEPublications,inc.
Patton,M.Q.(2002).Qualitativeresearch&evaluationmethods.ThousandOaks,Calif.:SagePublications.
Pesut,B.(2008a).Areplyto‘Spiritualityandnursing:areductionistapproach’byJohnPaley.NursingPhilosophy,9(2),131-137.
Pesut,B.(2008b).Spiritualityandspiritualcareinnursingfundamentalstextbooks.JournalofNursingEducation,47(4),167-173.
Pesut,B.(2016).Therebedragons:effectsofunexploredreligiononnurses’competenceinspiritualcare.NursingInquiry.
Pesut,B.,Fowler,M.,Taylor,E.J.,Reimer-Kirkham,S.,&Sawatzky,R.(2008).Conceptualisingspiritualityandreligionforhealthcare.JournalofClinicalNursing,17(21),2803-2810.doi:10.1111/j.1365-2702.2008.02344.x
Pesut,B.,Sawatzky,R.,Stajduhar,K.I.,McLeod,B.,Erbacker,L.,&Chan,E.K.(2014).Educatingnursesforpalliativecare:Ascopingreview.JournalofHospiceandPalliativeNursing,16(1),47-54.
Peternelj-Taylor,C.A.,&Yonge,O.(2003).ExploringBoundariesintheNurse-ClientRelationship:ProfessionalRolesandResponsibilities.PerspectivesinPsychiatricCare,39(2),55-66.
Polkinghorne,D.E.(1988).Narrativeknowingandthehumansciences:SunyPress.Pope,C.,Ziebland,S.,&Mays,N.(2000).Qualitativeresearchinhealthcare:analysing
qualitativedata.BMJ:BritishMedicalJournal,320(7227),114.Porter,S.E.,&Robinson,J.C.(2011).Hermeneutics:Anintroductiontointerpretive
theory:Wm.B.EerdmansPublishing.Puchalski,C.M.,Ferrell,B.,Virani,R.,Otis-Green,S.,Baird,P.,Bull,J.,...Sulmasy,D.
(2009).Improvingthequalityofspiritualcareasadimensionofpalliativecare:thereportoftheConsensusConference.JournalofPalliativeMedicine,12(10),885-904.doi:10.1089/jpm.2009.0142
Rachman,S.J.(1978).Fearandcourage:SanFrancisco:Freeman.Raingruber,B.,&Kent,M.(2003).Attendingtoembodiedresponses:Awaytoidentify
practice-basedandhumanmeaningsassociatedwithsecondarytrauma.QualitativeHealthResearch,13(4),449-468.
Ray,S.L.(2006).Embodimentandembodiedengagement:Centralconcernsforthenursingcareofcontemporarypeacekeeperssufferingfrompsychologicaltrauma.PerspectivesinPsychiatricCare,42(2),106-113.
Reed,P.G.(1992).Anemergingparadigmfortheinvestigationofspiritualityinnursing.ResearchinNursingandHealth,15(5),349-357.
Reimer-Kirkham,S.(2009).Livedreligion:implicationsfornursingethics.NursingEthics,16(4),406-417.doi:10.1177/0969733009104605
Ricoeur,P.(1976).Interpretationtheory:discourseandthesurplusofmeaning.FortWorth,Tex.:TexasChristianUniversityPress.
Ricoeur,P.(1981).Hermeneuticsandthehumansciences:Essaysonlanguage,actionandinterpretation(J.B.Thompson,Trans.J.B.ThompsonEd.):Cambridgeuniversitypress.
103
Ricoeur,P.(1984).Timeandnarrative.Chicago:UniversityofChicagoPress.Ricoeur,P.(1992).Oneselfasanother(Frenchoriginal1990,EditionsduSeuil).(English
translationbyKBlamey):UniversityofChicagoPress,ChicagoandLondon.Ricoeur,P.(1999).Eksistensoghermeneutikk(ExistenceandHermeneutics)(H.H.Ystad
Ed.):Aschehoug.Ricoeur,P.(2008).Fromtexttoaction:essaysinhermeneutics,II(K.Blamey&J.B.
Thompson,Trans.).London:Continuum.Riessman,C.K.(1993).Narrativeanalysis.NewburyPark,Calif.:Sage.Rogers,C.R.(1961).Onbecomingaperson:Atherapist'sviewofpsychology.Boston:
HoughtonMifflin.Rogers,C.R.(1980).Awayofbeing.Boston:HoughtonMifflin.Romoren,T.I.,Torjesen,D.O.,&Landmark,B.(2011).Promotingcoordinationin
Norwegianhealthcare.IntJIntegrCare,11(Spec10thAnniversaryEd),e127.Rosch,E.(1981).Prototypeclassificationandlogicalclassification:Thetwosystems.In
E.Schnolnick(Ed.),NewtrendsinCognitiveRepresentation:ChallengestoPiaget’stheory(pp.73-96):Hillsdale,NJ:Erbaum.
Rowe,C.,&Broadie,S.(2002).Nicomacheanethics:OxfordUniversityPress.Roxberg,Å.,Eriksson,K.,Rehnsfeldt,A.,&Fridlund,B.(2008).Themeaningof
consolationasexperiencedbynursesinahome-caresetting.JournalofClinicalNursing,17(8),1079-1087.
Rumbold,B.D.(2003).Caringforthespirit:lessonsfromworkingwiththedying.MedicalJournalofAustralia,179(6),S11.
Rushton,C.H.,Kaszniak,A.W.,&Halifax,J.(2013).Aframeworkforunderstandingmoraldistressamongpalliativecareclinicians.JournalofPalliativeMedicine,16(9),1074-1079.
Rushton,C.H.,Sellers,D.E.,Heller,K.S.,Spring,B.,Dossey,B.M.,&Halifax,J.(2009).Impactofacontemplativeend-of-lifetrainingprogram:Beingwithdying.PalliativeandSupportiveCare,7(04),405-414.
Sabo,B.M.(2008).Adversepsychosocialconsequences:Compassionfatigue,burnoutandvicarioustraumatization:Arenurseswhoprovidepalliativeandhematologicalcancercarevulnerable?IndianJournalofPalliativeCare,14(1),23.
Sabo,B.M.(2011a).Compassionatepresence:Themeaningofhematopoieticstemcelltransplantnursing.EuropeanJournalofOncologyNursing,15(2),103-111.doi:http://dx.doi.org/10.1016/j.ejon.2010.06.006
Sabo,B.M.(2011b)."ReflectingontheConceptofCompassionFatigue"TheOnlineJournalofIssuesinNursing,Vol.16(No.1).RetrievedfromTheOnlineJournalofIssuesinNursingwebsite:http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Vol-16-2011/No1-Jan-2011/Concept-of-Compassion-Fatigue.html
Sandelowski,M.(1993).Rigororrigormortis:theproblemofrigorinqualitativeresearchrevisited.Advancesinnursingscience,16(2),1-8.
Sandelowski,M.,&Barroso,J.(2003).Classifyingthefindingsinqualitativestudies.QualitativeHealthResearch,13(7),905-923.
Sandgren,A.,Thulesius,H.,Fridlund,B.,&Petersson,K.(2006).Strivingforemotionalsurvivalinpalliativecancernursing.QualitativeHealthResearch,16(1),79-96.
Sarvimäki,A.,&Stenbock-Hult,B.(2014).Themeaningofvulnerabilitytoolderpersons.NursingEthics,0969733014564908.

104
Sasser,C.G.,&Puchalski,C.M.(2010).Thehumanisticclinician:traversingthescienceandartofhealthcare.JournalofPainandSymptomManagement,39(5),936-940.
Schei,E.(2006).Doctoringasleadership:thepowertoheal.PerspectivesinBiologyandMedicine,49(3),393-406.
Schnell,T.(2009).TheSourcesofMeaningandMeaninginLifeQuestionnaire(SoMe):Relationstodemographicsandwell-being.TheJournalofPositivePsychology,4(6),483-499.
Schnell,T.(2010).Existentialindifference:Anotherqualityofmeaninginlife.JournalofHumanisticPsychology,50(3),351-373.
Schnell,T.,&Keenan,W.J.(2011).Meaning-makinginanatheistworld.ArchiveforthePsychologyofReligion,33(1),55-78.
Seale,C.(1999).Qualityinqualitativeresearch.Qualitativeinquiry,5(4),465-478.Sinclair,S.,&Chochinov,H.M.(2012).Communicatingwithpatientsaboutexistential
andspiritualissues:SACR-Dwork.ProgressinPalliativeCare,20(2),72-78.Sinclair,S.,Torres,M.-B.,Raffin-Bouchal,S.,Hack,T.F.,McClement,S.,Hagen,N.A.,&
Chochinov,H.M.(2016).Compassiontraininginhealthcare:whatarepatients’perspectivesontraininghealthcareproviders?BMCMedicalEducation,16(1),1-10.doi:10.1186/s12909-016-0695-0
Smart,D.,English,A.,James,J.,Wilson,M.,Daratha,K.B.,Childers,B.,&Magera,C.(2014).Compassionfatigueandsatisfaction:Across-sectionalsurveyamongUShealthcareworkers.Nursing&HealthSciences,16(1),3-10.
Solvoll,B.-A.,&Lindseth,A.(2015).Theissueofbeingtouched.Medicine,HealthCareandPhilosophy,1-8.
StanfordUniversitySchoolofMedicine.(2008).Thecenterforcompassionandaltruismresearchandeducation.Retrievedfromhttp://ccare.stanford.edu/about/mission-vision/
StatistiskSentralbyrå(CentralBureauofStatisticsinNorway).(2015).Dennorskekirke(TheNorwegianChurch,2015).Retrievedfromhttps://www.ssb.no/kultur-og-fritid/statistikker/kirke_kostra/aar/2016-05-04
Steinhauser,K.E.,Christakis,N.A.,Clipp,E.C.,McNeilly,M.,McIntyre,L.,&Tulsky,J.A.(2000).Factorsconsideredimportantattheendoflifebypatients,family,physicians,andothercareproviders.JAMA,284(19),2476-2482.
Stifoss-Hanssen,H.(1999).Religionandspirituality:WhataEuropeanearhears.TheInternationalJournalforthePsychologyofReligion,9(1),25-33.
Stifoss-Hanssen,H.,&Kallenberg,K.(1998).Livssynoghelse.Teoretiskeogkliniskeperspektiver(ViewofLifeandHealth.Theoreticalandclinicalperspectives.Oslo:AdNotamGyldendal.
Strang,S.,Henoch,I.,Danielson,E.,Browall,M.,&Melin-Johansson,C.(2014).Communicationaboutexistentialissueswithpatientsclosetodeath—nurses'reflectionsoncontent,processandmeaning.Psycho-Oncology,23(5),562-568.
Strømskag,K.(2012).Ognåskaljegdø:HospicebevegelsenogpalliasjonenshistorieiNorge(AndnowIshalldie:ThehistoryofthehospicemovementandpalliativecareinNorway).Oslo,Norway:PaxforlagA/S.
Sulmasy,D.P.(2002).Abiopsychosocial-spiritualmodelforthecareofpatientsattheendoflife.Thegerontologist,42(suppl3),24-33.
Swinton,J.(2014).Spirituality-in-Healthcare:JustBecauseitMayBe‘MadeUp’DoesNotMeanThatitisNotRealandDoesNotMatter(Keynote5).JournalfortheStudyofSpirituality,4(2),162-173.
Swinton,J.,&Mowat,H.(2006).Practicaltheologyandqualitativeresearch:SCM.

105
Swinton,J.,&Pattison,S.(2010).Movingbeyondclarity:towardsathin,vague,andusefulunderstandingofspiritualityinnursingcare.NursingPhilosophy,11(4),226-237.
Sæteren,B.,Lindström,U.Å.,&Nåden,D.(2011).Latchingontolife:livingintheareaoftensionbetweenthepossibilityoflifeandthenecessityofdeath.JournalofClinicalNursing,20(5-6),811-818.
Söderberg,A.,Gilje,F.,&Norberg,A.(1999).Transformingdesolationintoconsolation:themeaningofbeinginsituationsofethicaldifficultyinintensivecare.NursingEthics,6(5),357-373.
Sørensen,T.(2012).EpidemiologicalStudiesofReligiosBehaviorsandHealthintheNord-TrøndelagHealthStudy(HUNT-3),Norway.(PhD,MFSchoolofTheologyPhD),MFSchoolofTheology,Oslo,Oslo.
Sørensen,T.,Lien,L.,Landheim,A.,&Danbolt,L.J.(2015).Meaning-Making,ReligiousnessandSpiritualityinReligiouslyFoundedSubstanceMisuseServices—AQualitativeStudyofStaffandPatients’Experiences.Religions,6(1),92-106.
Sørlie,V.(2001).Beinginethicallydifficultcaresituations:narrativeinterviewswithregisterednursesandphysicianswithininternalmedicine,oncologyandpaediatrics.(PhD,UmeåUniversity),DepartmentofNursing,UmeåUniversity,Umeå
Talseth,A.-G.,Gilje,F.,&Norberg,A.(2003).Strugglingtobecomereadyforconsolation:experiencesofsuicidalpatients.NursingEthics,10(6),614-623.
Tan,H.M.,Wilson,A.,&Olver,I.(2009).Ricoeur’stheoryofinterpretation:Aninstrumentfordatainterpretationinhermeneuticphenomenology.Internationaljournalofqualitativemethods,8(4),1-15.
Tan,H.M.,Wilson,A.,Olver,I.,&Barton,C.(2011).Theexperienceofpalliativepatientsandtheirfamiliesofafamilymeetingutilisedasaninstrumentforspiritualandpsychosocialcare:Aqualitativestudy.(Researcharticle)(Report).BMCPalliativeCare,10,7.
Thorup,C.B.,Rundqvist,E.,Roberts,C.,&Delmar,C.(2012).Careasamatterofcourage:vulnerability,sufferingandethicalformationinnursingcare.ScandinavianJournalofCaringSciences,26(3),427-435.
Torjuul,K.(2009).Livingwithethicaldilemmas:theethicalreasoningofsurgeonsandnursesinsurgicalunits.(PhD,UniversityofTromsøPhd),UIT(UniversityofTromsø),Tromsø,Norway.Retrievedfromhttp://munin.uit.no/bitstream/handle/10037/2468/thesis.pdf?sequence=3&isAllowed=y
Tornøe,K.A.(1996).Kanvitrøstehjertene?Hvordanmøtealvorligsykeogdøendepasientersåndeligebehov?(Canweconsolethehearts?Howtomeetcriticallyillanddyingpatients'spiritualneeds).Oslo:TanoAschehough.
Torskenæs,K.B.,&Kalfoss,M.H.(2013).TranslationandFocusGroupTestingoftheWHOQOLSpirituality,Religiousness,andPersonalBeliefsModuleinNorway.JournalofHolisticNursing,31(1),25-34.
Torskenæs,K.B.,Kalfoss,M.H.,&Sæteren,B.(2015).Meaninggiventospirituality,religiousnessandpersonalbeliefs:exploredbyasampleofaNorwegianpopulation.JournalofClinicalNursing.
Turner,B.S.,&Dumas,A.(2013).Vulnerability,diversityandscarcity:onuniversalrights.Medicine,HealthCare,andPhilosophy,16(4),663-670.doi:http://dx.doi.org/10.1007/s11019-013-9500-6

106
Udo,C.(2014).Theconceptandrelevanceofexistentialissuesinnursing.EuropeanJournalofOncologyNursing,18(4),347-354.doi:10.1016/j.ejon.2014.04.002
Ulland,D.,&DeMarinis,V.(2014).UnderstandingandworkingwithexistentialinformationinaNorwegianadolescentpsychiatrycontext:aneedandachallenge.MentalHealth,Religion&Culture,17(6),582-593.
Vaismoradi,M.,Turunen,H.,&Bondas,T.(2013).Contentanalysisandthematicanalysis:Implicationsforconductingaqualitativedescriptivestudy.Nursing&HealthSciences,15(3),398-405.
vanKootenNiekerk,K.Introduction.InK.E.Løgstrup(2007),BeyondTheEthicalDemand.UniversityofNotreDamePress:NotreDame,Indiana.
VanManen,M.(1990).Researchinglivedexperience:Humanscienceforanactionsensitivepedagogy:SunyPress.
VanManen,M.(2014).Phenomenologyofpractice:Meaning-givingmethodsinphenomenologicalresearchandwriting(Vol.13):LeftCoastPress.
Vandervelde,P.(2008).Thechallengeofthe‘suchasitwas’:Ricoeur’stheoryofnarratives.InD.Kaplan(Ed.),ReadingRicoeur(pp.141-162):SUNYPress.
Vivat,B.(2008).Measuresofspiritualissuesforpalliativecarepatients:aliteraturereview.PalliativeMedicine,22(7),859-868.doi:10.1177/0269216308095990
Webb,C.(2003).Editor'snote:Introductiontoguidelinesonreportingqualitativeresearch.JournalofAdvancedNursing,42(6),544-545.doi:10.1046/j.1365-2648.2003.02716.x
Webb,C.,&Kevern,J.(2001).Focusgroupsasaresearchmethod:acritiqueofsomeaspectsoftheiruseinnursingresearch.JournalofAdvancedNursing,33(6),798-805.
WHO.(1998).WHOQOLandspirituality,religiousnessandpersonalbeliefs(SRPB).WorldHealthOrganization.(2002).InnovativecareforchronicconditionsBuildingblocks
foractionGlobalReport.Retrievedfromhttp://www.who.int/chp/knowledge/publications/icccglobalreport.pdf
WorldMedicalAssociation.(2001).WorldMedicalAssociationDeclarationofHelsinki.Ethicalprinciplesformedicalresearchinvolvinghumansubjects.BulletinoftheWorldHealthOrganization,79(4),373.
Ødbehr,L.S.(2015).Spiritualcareindementianursing-Aqualitative,exploratorystudy.(PhD,FacultyofMedicine,DepartmentofNursingScience),UniversityofOslo,Oslo.
Ødbehr,L.S.,Kvigne,K.,Hauge,S.,&Danbolt,L.J.(2014).Nurses'andcareworkers'experiencesofspiritualneedsinresidentswithdementiainnursinghomes:aqualitativestudy.BMCNursing,13(1),12.
Öhlen,J.(2001).Practicalwisdom:competenciesrequiredinalleviatingsufferinginpalliativecare.JournalofPalliativeCare,18(4),293-299.
Aadland,E.(1997).Ogegserpådeg…Vitenskapsteoriogmetodeihelse-ogsosialfag(AndIlookatyou...PhilosophyofScienceandmethodsforHealthandSocialstudies)(Vol.2):TanoAschehoug.
Aadnanes,P.M.(2008).Gudforkvarmann:Kyrkjaogdennyereligiøsiteten(Godforeveryone:TheChurchandthenewreligiosity).Oslo:Universitetsforlaget.

107
PaperI-III

108
Appendix


















