The California School Psychologist - CASPOnlineThe California School Psychologist, 2007, Vol. 12 7...
130
The California School Psychologist 2007, Volume 12 CONTENTS Editorial Shane R. Jimerson The California School Psychologist Provides Valuable 5 Information to Promote School Success Among Students with Emotional or Behavioral Disorders Articles Alberto F. Restori Functional Assessment-Based Interventions for Children 9 Frank M. Gresham At-Risk for Emotional and Behavioral Disorders Tae Chang Howard B. Lee Wilda Laija-Rodriquez Paul Muyskens The Use of Response to Intervention Practices for 31 Doug Marston Behavior: An Examination of the Validity of a Screening Amy L. Reschly Instrument Emily S. Fisher Comprehensive Assessment of Emotional Disturbance: 47 Katie E. Doyon A Cross-Validation Approach Enrique Saldaña Megan Redding Allen Katina M. Lambros Mental Health Intervention Teams: A Collaborative Model 59 Shirley K. Culver to Promote Positive Behavioral Support for Youth with Aidee Angulo Emotional or Behavioral Disorders Pamela Hosmer Stephen E. Brock Diagnosis of Attention-Deficit/Hyperactivity Disorder 73 Amanda Clinton (AD/HD) in Childhood: A Review of the Literature Gail B. Adams Current Educational Practices in Classifying and Serving 93 Thomas J. Smith Students with Obsessive-Compulsive Disorder Sara E. Bolt Patrick Nolten Renée M. Tobin Developing Emotional Competence in Preschoolers: 107 Frank J. Sansosti A Review of Regulation Research and Recommendations Laura Lee McIntyre for Practice Erin Dowdy A Comparison of Classification Methods for Use in 121 Randy W. Kamphaus Predicting School-Based Outcomes
Transcript of The California School Psychologist - CASPOnlineThe California School Psychologist, 2007, Vol. 12 7...

The California School Psychologist2007, Volume 12
CONTENTS
Editorial
Shane R. Jimerson The California School Psychologist Provides Valuable 5 Information to Promote School Success Among Students with Emotional or Behavioral Disorders
Articles
Alberto F. Restori Functional Assessment-Based Interventions for Children 9 Frank M. Gresham At-Risk for Emotional and Behavioral Disorders Tae Chang Howard B. Lee Wilda Laija-Rodriquez
Paul Muyskens The Use of Response to Intervention Practices for 31 Doug Marston Behavior: An Examination of the Validity of a Screening Amy L. Reschly Instrument
Emily S. Fisher Comprehensive Assessment of Emotional Disturbance: 47 Katie E. Doyon A Cross-Validation Approach Enrique Saldaña Megan Redding Allen
Katina M. Lambros Mental Health Intervention Teams: A Collaborative Model 59 Shirley K. Culver to Promote Positive Behavioral Support for Youth with Aidee Angulo Emotional or Behavioral Disorders Pamela Hosmer
Stephen E. Brock Diagnosis of Attention-Deficit/Hyperactivity Disorder 73 Amanda Clinton (AD/HD) in Childhood: A Review of the Literature
Gail B. Adams Current Educational Practices in Classifying and Serving 93 Thomas J. Smith Students with Obsessive-Compulsive Disorder Sara E. Bolt Patrick Nolten
Renée M. Tobin Developing Emotional Competence in Preschoolers: 107 Frank J. Sansosti A Review of Regulation Research and Recommendations Laura Lee McIntyre for Practice
Erin Dowdy A Comparison of Classification Methods for Use in 121 Randy W. Kamphaus Predicting School-Based Outcomes


�
The California School Psychologist Provides Valuable Information to Promote School Success Among Students
with Emotional or Behavioral Disorders Shane R. Jimerson
University of California, Santa Barbara
This volume of The California School Psychologist provides valuable information to promote the success of students with emotional or behavioral disorders, as well as other informative articles. These articles provide valuable information for school psychologists and other professionals working in the schools, and also contribute to the literature and scholarship that aim to promote the educational success of all students. Previous articles published in The California School Psychologist, including the recent volumes addressing a) school engagement, b) strength-based assessment, c) response-to-intervention (RtI), and d) autism are available on-line at www.education.ucsb.edu/school-psychology.
The first article (Restori, Gresham, Chang, Lee, & Laija-Rodriquez, 2007) reports the results of a study using functional assessment-based interventions to support fifth-grade students at-risk for emotional and behavioral disorders. Students whose behavior was found to be functionally related to either task-avoid-ance or attention-seeking were randomly assigned to a treatment strategy that was primarily either ante-cedent or consequent-based. This study reports the results of an ABAB single-case design to examine the effects of treatment strategies. This study also conducted a comparison of treatment strategies that were primarily antecedent or consequent-based. The authors highlight that antecedent-based treatment strate-gies (i.e., self-monitoring and task-modification) were more effective than consequent-based treatment strategies (i.e., differential reinforcement) for increasing academic engagement and reducing disruptive behavior. They also discuss the implications for using functional assessment strategies.
The second article (Muyskens, Marston, & Reschly, 2007) shares the results of a study that examines the validity of a screening instrument to identify students at risk for behavior problems. Within a Response-to-Intervention framework, the authors discuss using a screening measure (a 12-item behavior screener completed by the teacher for each student in the Fall) designed to identify students at risk for behavior difficulties and targeting these students for early intervention. This study included 22,056 kindergarten through 8th grade students from the Minneapolis Public Schools. Results revealed that teacher-completed Fall scores on this measure were significantly correlated with suspensions, achievement scores, and attendance data over the course of the school year. The authors emphasize that providing teachers with a tool which in less than a minute can help them identify students likely to present significant behavioral or academic concerns over the course of the school year warrants further consideration.
The third article (Fisher, Doyon, Saldaña, & Redding-Allen, 2007) discusses a comprehensive assess-ment of emotional disturbance, advocating cross validation procedures, and using the RIOT approach (Review, Interview, Observe, Test). The authors advocate that using all four RIOT processes together allows for comprehensive assessment for emotional disturbance. The authors also encourage school psychologists to consider a student’s strengths, cultural factors, and the interaction between the student and the environment when interpreting the results of assessments. Using the multi-faceted information yielded through a comprehensive assessment, school psychologists may provide recommendations to help remediate areas of weakness and promote social and cognitive competence.
Address correspondence and reprint requests to Shane R. Jimerson; University of California, Santa Barbara; Depart-ment of Counseling, Clinical, and School Psychology; Center for School-Based Youth Development; Phelps Hall; Santa Barbara, CA 93106-9490 or e-mail [email protected]
The California School Psychologist, Vol. 12, pp. 5 – 7, 2007Copyright 2007 California Association of School Psychologists

The California School Psychologist, 2007, Vol. 12�
The fourth article (Lambros, Culver, Angulo, & Hosmer, 2007) describes a collaborative interven-tion model for promoting mental health and positive social adjustment for youth with emotional or behavioral disorders (EBD). The mental health intervention team (MHIT) includes a collaborative part-nership between the Mental Health Resource Center (MHRC) and the Emotional Disturbance Program (ED) and also includes research and evaluation consultation from the Child and Adolescent Services Research Center (CASRC). The MHIT is a collaborative service delivery model using school-based mental health teams to implement evidence-based interventions to promote positive social adjustment for youth with EBD and their families as well as support classroom teachers. The authors advocate that through integrating program components and combining fiscal resources to develop the MHIT, a more efficient use of resources may be possible, resulting in increased services to students and teachers beyond what is offered when mental health and educational programs work in isolation.
The fifth article (Brock & Clinton, 2007) reviews recent literature related to the diagnosis of Atten-tion-Deficit/Hyperactivity Disorder (AD/HD) in childhood. This article discusses diagnostic criteria presented in the Diagnostic and Statistical Manual of Mental Disorders and explores the diagnostic procedures for AD/HD recommended in current publications. The authors highlight that there is no single diagnostic procedure, or set of procedures, has been identified that will diagnose AD/HD with perfect reliability.
Rather, this literature review reveals that rating scales, interviews, laboratory/ psychological testing, and observations are the most frequently recommended AD/HD diagnostic techniques. This information can be valuable for school psychologists and other education professionals and mental health profes-sionals who are responsible for assessing and identifying students with AD/HD.
The sixth article (Adams, Smith, Bolt, & Holten, 2007) describes a study of contemporary educa-tional practices in classifying and serving students with obsessive-compulsive disorder (OCD). This study used a survey to examine current practices for classifying and serving students with a primary diagnosis of OCD. The results indicated that fewer than one percent of the students served by school psychologists had a primary diagnosis of OCD, and that the majority of these students were served under IDEA. Of the students receiving services under IDEA, half were classified under E/BD and one-third under OHI. Approximately two-thirds of the students with OCD were educated in less restrictive settings (e.g., regular classroom with or without resource/part-time special class). The authors conclude that the results suggest a pattern of ambiguity and uncertainty surrounding the appropriateness of IDEA catego-ries for OCD, concerns regarding the stigma of labeling, and problems related to providing appropriate services to these students.
The seventh article (Tobin, Sansoti, & McIntyre, 2007) focuses on the development of emotional competence in preschoolers. This article provides a review of emotional regulation research from the past two decades. Specifically, the developmental literature for both regulation and dysregulation of emotion is reviewed and the implications for both assessment and intervention with preschool children are discussed. Regulation has been implicated in the development of emotional and behavioral disorders in childhood. The literature reveals that emotion dysregulation is one of the most common reasons fami-lies seek psychological services and behavioral supports. The authors emphasize that interventions to support children with regulatory difficulties will be enhanced when they are informed by basic psycho-logical research on the topic. The authors also highlight the role that school psychologists and school-based interventions may play in supporting appropriate regulatory strategies for young children.
The eighth article (Dowdy & Kamphaus, 2007) reports the results of a study comparing three clas-sification methods (categorical, dimensional, person-oriented) in predicting school-based outcomes.

The California School Psychologist, 2007, Vol. 12 7
Elementary school-age children (N=558) were administered the Behavior Assessment System for Chil-dren – Teacher Rating Scale and educational outcome variables were collected seven months later. Results revealed that all three methods for predicting educational outcomes were modest and were best able to predict later grade point averages. The authors emphasize the relative superiority of person-oriented and dimensional methods of classification and also call for further investigations.
This collection of articles provides valuable information that may be used by educational profes-sionals working with children, families, and colleagues to enhance the academic success and promote positive developmental trajectories of students. The authors of the manuscripts in this volume provide valuable information and insights that advance our understanding of numerous important topics. The California School Psychologist contributes important information regarding promoting the social and cognitive competence of all students.
REfEREnCES
Adams, G. B., Smith, T. J., Bolt, S. E., & Holten, P. (2007). Current educational practices in classifying and serving students with Obsessive-Compulsive Disorder. The California School Psychologist, 12, 93 – 105.
Brock, S. E. & Clinton, A. (2007). Diagnosis of Attention-Deficit/Hyperactivity Disorder (AD/HD) in childhood: A review of the literature. The California School Psychologist, 12, 73 – 91.
Dowdy E. & Kamphaus, R. W. (2007). A comparison of classification methods for use in predicting school-based outcomes. The California School Psychologist, 12, 121 – 132.
Fisher, E. S., Doyon, K. E., Saldaña, E., & Redding-Allen, M. (2007). Comprehensive assessment of emotional disturbance: A cross-validation approach. The California School Psychologist, 12, 47 – 58.
Lambros, K. M., Culver, S. K., Angulo, A. & Hosmer, P. (2007). Mental health intervention teams: A collaborative model to promote positive behavioral support for youth with emotional or behavioral disorders. The California School Psychologist, 12, 59 – 71.
Muyskens, P., Marston, D., & Reschly, A. L. (2007). The use of response-to-intervention practices for behavior: An examination of the validity of a screening instrument. The California School Psychologist, 12, 31 – 45.
Restori, A. F., Gresham, F. M., Chang, T., Lee, H. B., & Laija-Rodriquez, W. (2007). Functional assessment-based interventions for children at-risk for emotional and behavioral disorders. The California School Psychologist, 12, 9 – 30.
Tobin, R. M., Sansoti, F. J., & McIntyre, L. L. (2007). Developing emotional competence in preschoolers: A review of regulation research and recommendations for practice. The California School Psychologist, 12, 107 – 120.
The California School Psychologist


9
Please send correspondence to Alberto Restori, PhD, Assistant Professor, Department of Educational Psychology and Counseling, California State University, Northridge, 18111 Nordhoff Street, Northridge, California 91330. Email: [email protected]
The California School Psychologist, Vol. 12, pp. 9 – 30, 2007Copyright 2007 California Association of School Psychologists
functional Assessment-Based Interventions for Children At-Risk for Emotional and Behavioral Disorders
Alberto F. Restori California State University, Northridge
Frank M. Gresham Louisiana State University
Tae Chang, Howard B. Lee &
Wilda Laija-Rodriquez California State University, Northridge
Functional assessments were conducted to identify the variables maintaining disruptive behavior in eight, typically developing fifth-grade students enrolled in general education classrooms. Participants whose behavior was found to be functionally related to either task-avoidance or attention-seeking were randomly assigned to a treatment strategy that was primarily either antecedent- or consequent-based. An ABAB single-case design was employed to analyze the effects of treatment strategies. The current study also conducted a comparison of treatment strategies that were primarily antecedent- or consequent-based. Results showed that antecedent-based treatment strategies (i.e., self-monitoring and task-modification) were more effective than consequent-based treatment strategies (i.e., differential reinforcement) for increasing academic engagement and reducing disruptive behavior. Implications regarding the use of functional assessment with typically developing students at-risk for emotional and behavioral problems enrolled in general education classrooms and the effects of antecedent- and consequent-based treatment strategies as a function of behavior are discussed.
KEYWORDS: Emotional and Behavioral Disorders, Functional Assessment, Behavioral Assessment, Behavioral Interventions, Treatment Strategies.
Students with emotional and behavioral disorders (EBD) are characterized by a number of behav-ioral, social, and academic characteristics that pose challenges to teachers and administrators. When more global intervention efforts such as primary and secondary prevention programs prove insufficient for shaping behaviors, more ideographic efforts, such as functional assessment-based interventions, are invoked (Horner & Sugai, 2000; Lane, Robertson, & Graham-Bailey, 2006).
Functional assessment involves the full range of procedures (e.g., interviews, direct observations, and rating scales) used to identify the antecedent conditions that set the stage for undesirable (target) behaviors to occur and the maintaining consequences (Gresham, Watson, & Skinner, 2001; Horner, 1994). These data are used to develop a hypothesis statement that can then be tested via experimental manipulation of environmental events. Subsequently, an intervention is designed based on the function of the target behavior.
While the original research on function-based interventions originated in analogue conditions (Iwata, Dorsey, Slifer, Bauman, & Richmond, 1982), this ideographic approach to intervention has also proved successful in self-contained (Dunlap et al., 1993), inclusive (Kamps, Wendland, & Culpepper,

The California School Psychologist, 2007, Vol. 1210
2006; Lane, Weisenbach, Little, Phillips, & Wehby, 2006; Lewis & Sugai, 1996; Umbreit & Blair, 1997; Umbreit, Lane, & Dejud, 2004), and preschool (Umbreit, 1996) settings with a wide range of students, including students with and at risk for EBD (Kern, Delaney, Clarke, Dunlap, & Childs, 2001; Kern, Hilt, & Gresham, 2004; Lane, Umbreit, & Beebe-Frankenberger, 1999; Sasso, Conroy, Stichter, & Fox, 2001).
Despite these successful demonstrations of functional assessment-based interventions in applied settings, some argue that the literature base is limited by the absence of functional analyses; the lack of a systematic approach to the process; and questionable reliability and validity of some of the tools employed (Sasso et al., 2001). In addition, other concerns focus on the ability to achieve the appropriate balance between scientific rigor and feasibility when conducting research in applied settings (Scott et al., 2004) and the goal of focusing more primarily on antecedent-based, rather than consequent-based interventions (Restori et al., in review).
Historically, many teachers and researchers have relied heavily on consequent-based interventions in which the target behavior must occur and subsequently be shaped by the consequences that follow (Lewis & Sugai, 1996; Martens, Peterson, Witt, & Cirone, 1986). That is, consequences, often in the form of punitive responses, are applied after the occurrence of an academic or behavioral problem. Research by Newcomer and Lewis (2004) indicates that such a consequent-based approach is not likely to offer the best approach for remediation of academic and behavioral challenges.
One review of the research on behavior disorders indicated that only 11.1% of the individuals treated for maladaptive behavior received treatments that were based primarily upon the manipulation of ante-cedent variables (Lennox, Miltenberger, Spengler, & Erfanian 1988). More recently, increased attention has been placed on the value of antecedent-based interventions in which environmental and curricular modifications are made to prevent the problem behavior from occurring (Clarke et al., 1995; Dunlap, White, Vera, Wilson, & Panacek, 1996; Kern et al., 2001; Kern & Clemens, 2007). While most func-tion-based interventions contain both components (antecedent adjustments and modification of the rein-forcement schedules), one could argue that an intervention could be either primarily antecedent-based or primarily consequent-based. Given the increased emphasis on prevention, one question arises as to the extent to which interventions that are primarily antecedent- or consequent-based are equally effective in producing meaningful, lasting change.
To this end, Restori and colleagues (in review) conducted as series of function-based interven-tions, some primarily antecedent-based and others primarily consequent-based, with eight second grade students with disruptive behavior patterns. Functional assessments were conducted to identify the main-taining variables, which yielded those maintained by task-avoidance or attention-seeking. Results of a series of ABAB withdrawal designs suggested that antecedent-based treatment strategies (i.e., self-moni-toring and task-modification) were as effective and efficient as consequent-based treatment strategies (i.e., differential reinforcement) for increasing academic engagement and reducing disruptive behavior for these general education students. However, questions arise as to the consistency of these findings with older students, who may be less amenable to intervention efforts (Walker, Ramsey, & Gresham, 2004). That is, previous research has demonstrated that disruptive patterns of behavior become more stable as children grow older and are likely to be more resistant to change (e.g., Olweus, 1979; Walker et al., 2004). Therefore, the authors of the current study investigated whether antecedent-based and consequent-based interventions were equally effective for upper elementary students with disruptive behaviors.

The California School Psychologist, 2007, Vol. 12 11
Purpose
This study seeks to extend the Restori and colleagues (in review) investigation by examining the efficacy of function-based interventions that were either primarily antecedent-based or primarily conse-quent-based with fifth-grade students whose patterns of disruptive behavior were similar to that of their second grade sample. We hypothesize that results will be comparable to those in the study of second grade students, but that the magnitude of improvement may be less given that behavior patterns become more resistant to intervention efforts over time (Walker et al., 2004).
METhoD
Participants and Setting
Eight fifth-grade, general education students from two elementary schools in southern California were selected to participate in the study. Written consent to conduct the study was granted by the Director of Special Education of the school district, school principals, and the fifth grade teachers of the two schools included in the study. Parents of the participants gave written permission for their child to be included in the study and had the option to withdraw their child from the study at any time. All of the participants gave their verbal consent to be included in the study and were given the option to withdraw from the study with their parent’s permission. The district serves an urban, ethnically diverse popula-tion with socioeconomic status ranging from lower to upper-middle class. Four of the participants were African American, two Latino, and two Anglo. All eight participants were male and five of the eight participants were enrolled in general education classes for their entire school day. Three of the partici-pants received special education support (i.e., resource specialist program [RSP]) for an hour per day (i.e., homework club). None of the participants had a neurological, psychiatric, or physical disability that could prevent him from behaving appropriately (e.g., autism) or that would interfere with academic performance (e.g., mental retardation). None of the participants in the study was classified as Emotion-ally Disturbed (ED), nor enrolled in a Special Day Class (SDC). Information regarding special education support, disabilities, and/or placement was obtained from parent and teacher interviews, school records, and student observations.
Procedures
Fifth grade teachers from the two elementary schools were asked to nominate his or her three to five most disruptive students. Students nominated for the study had varying degrees of suspensions, referrals to the school principal or counselor, and out-of-class suspensions (OCS), however, school personnel agreed that all of the students nominated for inclusion to the study demonstrated significant behavioral problems and were considered at-risk for emotional and behavioral disorders. A functional assessment consisting of direct student observations employing an A-B-C approach, (i.e., descriptive assessment), interview with the classroom teacher, and completion of the Social Skills Rating System-Teacher form (SSRS-T; Gresham & Elliott, 1990) was conducted with each participant to determine the degree of disruptive, off-task, and on-task behaviors. Preliminary classroom observations were 1� minutes in dura-tion and used for gathering baseline data of the referred students as well as to identify other potential participants for the study. Only students whose disruptive behavior was clearly identified as having a functional relationship to either task-avoidance or attention-seeking were included in the study. Students whose behavior served a dual function (i.e., task-avoidance and attention-seeking), was undifferenti-ated (i.e., not clearly task-avoidance or attention-seeking), or whose behavior was functionally related
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1212
to sensory reinforcement were excluded from the study. Although some students may have multiple or undifferentiated functions of behavior, previously cited research has demonstrated that a comprehensive functional assessment is likely to result in an accurate hypothesis statement regarding a child’s primary function of behavior within a given setting. After completion of the identification process, the eight participants were randomly assigned to receive a treatment strategy that was either primarily antecedent- or consequent-based and matched to their individual function of behavior.
Students selected to participate in the study met the following criteria. First, participants must exhibit disruptive behavior for a minimum of 25% of the intervals observed during four or more of the baseline observations. Second, students must be academically engaged during less than 25% of the intervals observed during four or more of the baseline observations. Classroom observations and teacher reports indicate that the majority of students engaged in disruptive behavior less than 10% of the time and were academically engaged or engaged in task-related activities at least 90% of the time. Third, the overall Social Skills and Academic Competence scores of the SSRS-T was below the 25th percentile and the overall Problem Behaviors score of the SSRS-T was above the 75th percentile. Finally, as previously stated, the function of behavior (i.e., task-avoidance or attention-seeking) must be clearly identified.
Participants’ data were coded and reported by letter and number to maintain their anonymity. The letter referred to the treatment strategy the participant received. Participants receiving an antecedent-based treatment strategy were coded with the letter A and participants receiving a consequent-based treatment strategy were coded with the letter C. Participants 1 and 2 for both the A and C groups desig-nate the participants whose function of behavior was attention-seeking. Likewise, participants 3 and 4 for both the A and C groups designate the participants whose function of behavior was task-avoidance. For example, participant A1 was a participant assigned to an antecedent-based treatment strategy whose disruptive behavior was functionally related to attention-seeking.
Measures
Disruptive behavior. Disruptive behavior was defined employing a modified version of the seven general categories of behavior incompatible with learning described by Becker, Madsen, Arnold, and Thomas (1967). The following four general categories were used to define disruptive behavior for the current study: (a) unauthorized out-of-seat behaviors, (b) disruptive noise, (c) disturbing others, and (d) talking without teacher permission. Out-of-seat behaviors include any unauthorized or non-task related movement within the classroom. Disruptive noise included excessive flipping of pages, pencil tapping, or any non-task related noise (e.g., humming). Disturbing others included physical contact with another student, their desk, any objects on another student’s desk; and aggressive behavior (e.g., hitting another student). Talking without teacher permission included responding to a teacher’s question without being called upon to reply, talking to another student while the teacher is giving a lesson, or talking during a written assignment.
Academic engagement. The current study adopted the definition of Academic Engaged Time (AET) from Walker and Severson’s (1991) Systematic Screening for Behavior Disorders (SSBD). Academic engagement was defined as a student properly working on assigned academic material. An academically engaged student is (a) attending to the material and task, (b) making appropriate motor and/or verbal responses (e.g., writing, computing, answering questions), and (c) asking for assistance (when appro-priate) in an acceptable manner. For example, a student listening to a teacher’s lesson or computing assigned math problems is considered to be academically engaged. A student not actively working on a class assignment, not attending to the teacher’s lesson, and/or breaking classroom rules are examples of

The California School Psychologist, 2007, Vol. 12 13
not exhibiting academically engaged behavior.
Technical Instrumentation
Social Skills Rating System – Teacher (SSRS-T; Gresham & Elliott, 1990). The SSRS-T provides a broad assessment of a student’s social behaviors that can affect teacher-student relations, peer accep-tance, and academic performance. The SSRS-T was standardized on a representative sample of students 3-18 years. The SSRS-T documents the perceived frequency and importance of behaviors influencing students’ development of social competence and adaptive functioning at school. The teacher version contains ratings of three social skill domains (Cooperation, Assertion, and Self-Control) and three problem behavior domains (Internalizing Problems, Externalizing Problems, and Hyperactivity Prob-lems). The SSRS-T also contains a teacher rating of academic competence. Extensive evidence of reli-ability, as well as content, social and criterion-related validity is provided in the SSRS manual.
observation and Recording Procedures
Students selected as participants for the study exhibited high rates of disruptive behavior and low rates of academic engagement as a function of either task-avoidance or attention-seeking. Observations for all participants in all phases of the study were conducted during reading or reading related lessons based on information gathered from teacher interviews. Although teachers reported that the participants demonstrated disruptive behavior throughout the day, they reported that such behaviors appeared to be more frequent during language arts instruction. Participants were observed in 10-second intervals for 15 minutes. A partial-interval, time-sampling procedure was used for recording off-task and disruptive behavior and a whole-interval, time-sampling procedure for recording academic engagement. At the end of each 10-second interval, the participant’s behavior was recorded indicating academic engagement (AE), off-task (OFF), or disruptive behavior (DIS). When a participant exhibited any off-task or disrup-tive behavior during a given interval, DIS or OFF was recorded on the observation form. If a participant displayed both disruptive and off-task behaviors within a given interval, DIS was recorded on the obser-vation form. Participants had to remain academically engaged throughout the entire 10-second interval to be considered academically engaged (AE). The percentages of disruptive behavior, off-task behavior, and academic engagement were calculated for each student after each 15-minute observation. Although there was some risk of over-estimating disruptive behavior and underestimating academic engagement using this observation system, this approach would likely produce more meaningful information when comparing treatment outcomes to baseline levels of each behavior. To calculate the percentage of inter-vals in which disruptive behavior, off-task behavior, or academic engagement occurred, the number of intervals in which each occurred was divided by the total number of intervals and multiplied by 100. Each 1�-minute observation session was considered one data point and a minimum of four data points was required to establish a stable rate of responding in both baseline and treatment phases.
Inter-observer agreement of direct observations was conducted by the first author and a research assistant (RA) by observing the target student at the same time from different places in the classroom employing the previously described observation and recording procedures. A minimum of 20% of all observation sessions included inter-rater reliability probes to ensure adequate levels of reliability. Inter-rater reliability probes were conducted across all phases of the study. The percentage of inter-observer agreement for all reliability probes was 80% or above.
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1214
A1
A2
Students were expected to read silently. Questions pertaining to reading assignment were asked after specified period of time. Classroom points were contingent on all students’ participation.
Students were expected to read silently or complete unfinished work during this time. Students were expected to read or work silently without disturbing other students.
Attention-Seeking
Attention-Seeking
Self-Monitoring
1. Explain self-monitoring procedure to A1.
2. Provide self-monitoring form.
3. Provide 5 verbal/physical prompts.
4. Student and teacher monitor on-task behavior.
5. Compare self-monitoring forms
6. Provide verbal praise for accurate self-monitoring.
7. Provide preferred activity for accurate self-monitoring and on-task-behavior.
Self-Monitoring
1. Explain self-monitoring procedure toA2.
2. Provide self-monitoring form.
3. Provide 5 verbal/physical prompts.
4. Student and teacher monitor on-task behavior.
5. Compare self-monitoring forms.
6. Provide verbal praise for accurate self-monitoring.
7. Provide preferred activity for accurate self-monitoring and on-task-behavior.
TABLE 1. Description of Antecedent-Based Treatment Strategies for Fifth Grade Participants
Student Assignment Hypothesis Modifications

The California School Psychologist, 2007, Vol. 12 1�
Task-Modification
1. Tell A3 to read grade level book for 10 minutes before he can read preferred book.
2. Allow A3 to select a book/story he likes.
3. Pair A3 with a classmate to read with.
4. After 10 minutes, ask A3 questions about story.
�. Provide verbal praise for answering questions and provide time to read preferred story.
Task-Modification
1. Tell A4 to read grade level book for 10 minutes before he can read preferred book.
2. Allow A4 to select a book/story he likes.
3. Pair A4 with a classmate to read with.
4. After 10 minutes, ask A4 questions about story.
�. Provide verbal praise for answering questions and provide time to read preferred story
A3
A4
Students were expected to read silently. Questions pertaining to reading assignment were asked after specified period of time. Classroom points were contingent on all students participation.
Students were expected to read silently from pre-assigned material. Students were expected to complete associated worksheets and not disturb other students.
Task Avoidance
Task Avoidance
Functional Assessment-based Interventions
The California School Psychologist, 2007, Vol. 121�
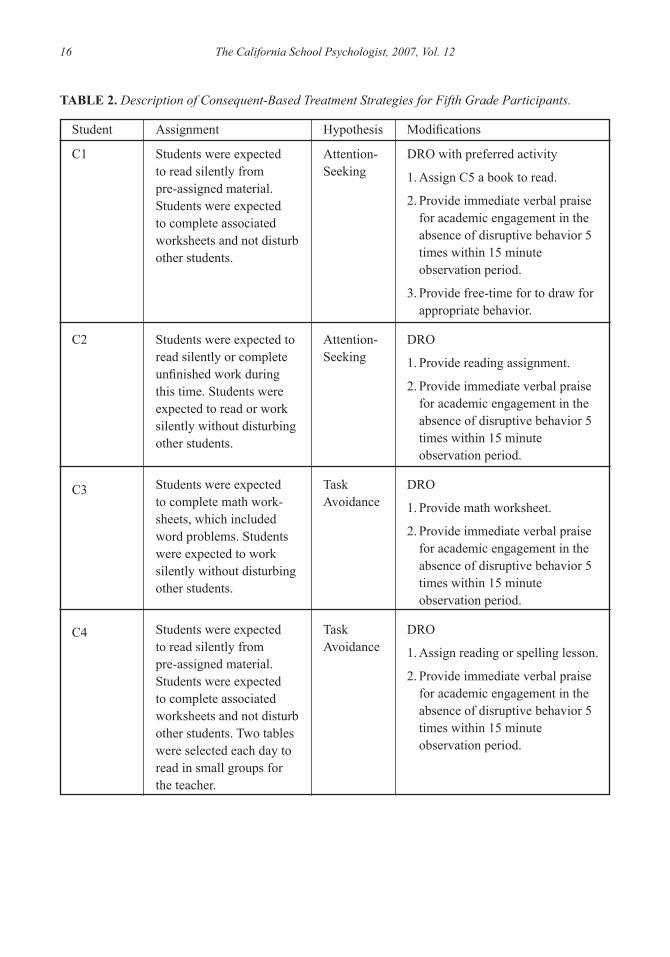
C1
C2
C3
C4
Students were expected to read silently from pre-assigned material. Students were expected to complete associated worksheets and not disturb other students.
Students were expected to read silently or complete unfinished work during this time. Students were expected to read or work silently without disturbing other students.
Students were expected to complete math work-sheets, which included word problems. Students were expected to work silently without disturbing other students.
Students were expected to read silently from pre-assigned material. Students were expected to complete associated worksheets and not disturb other students. Two tables were selected each day to read in small groups for the teacher.
Attention-Seeking
Attention-Seeking
Task Avoidance
Task Avoidance
DRO with preferred activity
1. Assign C5 a book to read.
2. Provide immediate verbal praise for academic engagement in the absence of disruptive behavior � times within 1� minute observation period.
3. Provide free-time for to draw for appropriate behavior.
DRO
1. Provide reading assignment.
2. Provide immediate verbal praise for academic engagement in the absence of disruptive behavior � times within 1� minute observation period.
DRO
1. Provide math worksheet.
2. Provide immediate verbal praise for academic engagement in the absence of disruptive behavior � times within 1� minute observation period.
DRO
1. Assign reading or spelling lesson.
2. Provide immediate verbal praise for academic engagement in the absence of disruptive behavior � times within 1� minute observation period.
TABLE 2. Description of Consequent-Based Treatment Strategies for Fifth Grade Participants.
Student Assignment Hypothesis Modifications

The California School Psychologist, 2007, Vol. 12 17
Interventions
Participants for the current study were assigned to a treatment strategy that was either primarily antecedent- or consequent-based and matched to their function of behavior. Antecedent-based treatment strategies consisted of self-monitoring for the two participants whose disruptive behavior was function-ally related to attention-seeking and task-modification for the two participants whose disruptive behavior was functionally related to task-avoidance. Consequent-based treatment strategies consisted of differen-tial reinforcement of other behaviors (DRO) for three of the participants and DRO with preferred activity for one participant (see Tables 1 and 2 for descriptions of each participant’s treatment plans). Although each participant received his own individual treatment plan, the following is a general overview of the interventions used, by whom and how they were implemented, and other pertinent information related to the intervention strategies used.
Self-monitoring. The current study modified the self-monitoring procedures described by Shapiro and Cole (1992) to fit the general education classroom and curriculum. In the current study, the teacher was trained by the primary investigator to implement the self-monitoring procedure. The classroom teacher was required to tap on the student’s shoulder when it was time to self-monitor their behavior. Self-monitoring was done on a variable-interval 3-minute schedule (VI-3m). At that time, both the teacher and student monitored the student’s behavior. During natural breaks in the school day (e.g., recess and lunch-time), the teacher and student reviewed the student’s self-monitoring forms. Reinforcement in the form of verbal praise and access to preferred activities were dispensed for accurate self-monitoring and on-task behavior.
Task-modification. The current study modified the task-modification procedure described by Dunlap and Kerns (1996) to fit the general education classroom and curriculum. In the current study, the teacher was trained by the primary investigator to implement the task-modification procedure. Participants receiving a task-modification intervention strategy were to select two books to read. One book would be a preferred book, the other, a grade-level book. The participant was to read the grade-level book with a preferred, competent reading peer for 10 minutes. Once the passage was read, the teacher asked ques-tions pertaining to the reading to assess comprehension. After reading the grade-level book, the partici-pant was permitted to read his preferred book and provided with verbal praise.
Differential reinforcement. Differential reinforcement typically involves withholding reinforcement of an undesirable behavior (extinction) and delivering reinforcement contingent on other appropriate behavior (Marcus & Vollmer, 1996). Teachers were trained by the primary investigator to deliver a modi-fied differential reinforcement of other behaviors (DRO). DRO is the delivery of reinforcement imme-diately following the performance of a desired behavior in the absence of the target behavior (Cooper, Herron, & Heward, 2007). Participants were provided with verbal praise for academic engagement in the absence of disruptive behavior.
Experimental Design and Data Analysis
Intervention outcomes were analyzed using a within-series, ABAB reversal design. In this design, each participant serves as his own control, thereby, minimizing the idiosyncratic interactions that have the potential for confounding the interpretations and results when comparing one subject with another. In the current study, baseline and reversal to baseline phase data were collected until a stable trend, with a minimum of four data points per phase was established. In both of these phases, the classroom teacher delivered instruction using his or her own behavior management system without any additional interven-tions for the participants of the current study. Similarly, during both treatment phases, data were collected
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1218
for a minimum of four data points for each treatment phase to determine the effects of the intervention strategies. Two follow-up phases at 15 and 30 days were also conducted to evaluate the maintenance of increased academic engagement and reduced disruptive behavior as a function of treatment. During the follow-up phases, teachers were not required to implement the student’s previously developed individual treatment plans. Graphed data were analyzed using traditional visual inspection (Johnston & Penny-packer, 1993) and mean score comparison techniques to determine the effects of treatment strategies.
Treatment Integrity
Treatment integrity is defined as the degree to which a treatment plan is implemented as intended (Gresham, 1989). Unless an intervention is carried out exactly as planned, results regarding change in the target behavior cannot be attributed to the intervention. Fuchs and Fuchs (1989) recommend the use of a component analysis checklist, wherein, a list of the components of an intervention strategy is provided to the teacher. In the current study, the teacher and researcher checked off each component of the inter-vention strategy as they were implemented during each observation. The component analysis checklist was reviewed by the primary investigator to determine if a particular component of the intervention strategy was consistently ignored. Although the percentage of treatment integrity for a given treatment strategy was not calculated, a visual inspection of the component analysis checklists completed by both the teacher and researcher indicate that the components of each intervention strategy were implemented with high integrity.
RESuLTS
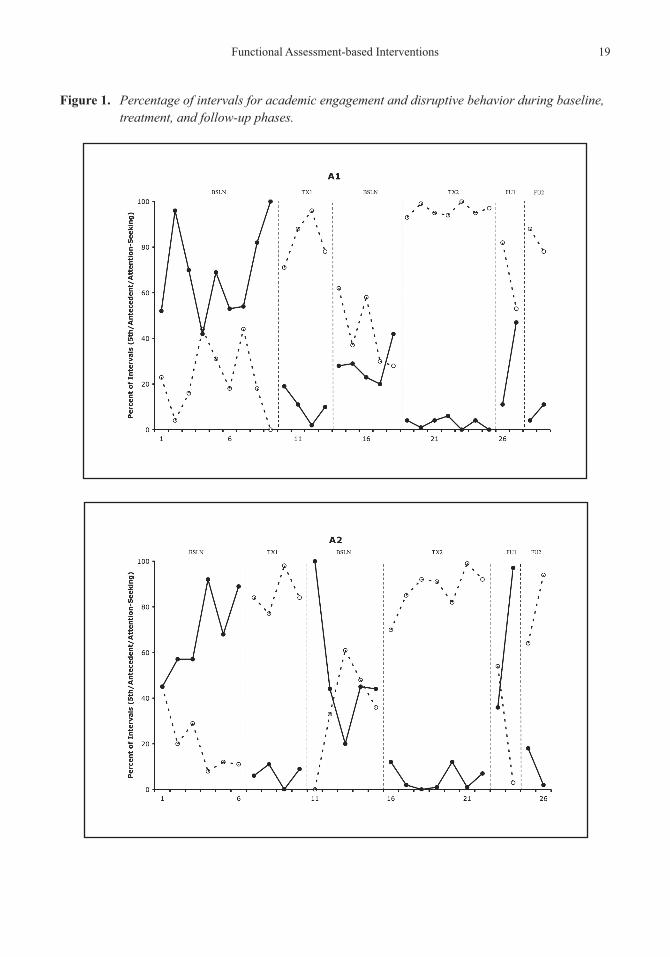
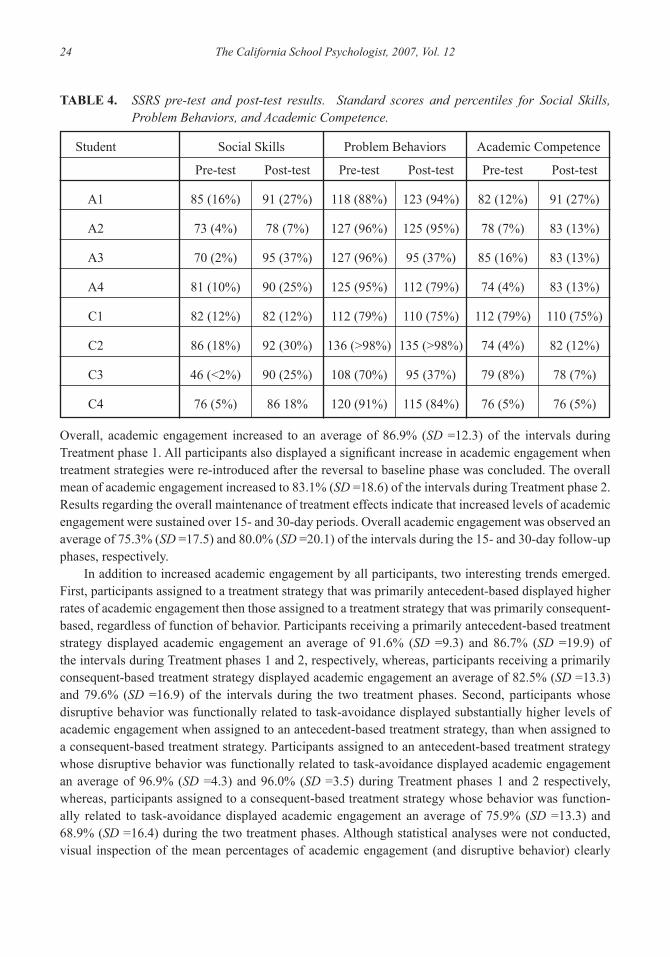
Figures 1 and 2 display the percentage of intervals of academic engagement and disruptive behavior for each participant across baseline, treatment, and follow-up phases. Overall, both antecedent- and consequent-based treatment strategies were effective, regardless of function of behavior. Table 3 provides the means and standard deviations for both academic engagement and disruptive behavior during each phase of the study. Results of the SSRS-T pre and post measures indicate relatively small and inconsis-tent changes on its various scales regardless of treatment strategy or function of behavior (see Table 4). Although results of the SSRS-T pre and post measures were relatively small and inconsistent, teachers reported they observed positive changes in the social skills domains assessed by the SSRS-T in all of their students included in the study. Furthermore, the data from both Figures and Table 3 provide clear evidence of meaningful and substantial change in behavior resulting from both antecedent- and conse-quent-based treatment strategies.
Academic engagement
Most participants displayed stable patterns of low academic engagement during the initial baseline sessions. Although all participants met the pre-established criteria of academic engagement for inclusion into the study, when compared to each other they exhibited considerable variability in academic engage-ment during the initial baseline phase of the study. Overall, participants were academically engaged an average of 22.4% (SD=16.9) of the intervals during the initial baseline phase. A low pattern of academic engagement was not as distinct during the reversal to baseline phase as it was during the initial baseline phase. During the reversal to baseline phase, overall average academic engagement was observed during 37.4% (SD=22.9) of the intervals.
All participants showed a significant increase in academic engagement during both treatment phases.
The California School Psychologist, 2007, Vol. 12 19
figure 1. Percentage of intervals for academic engagement and disruptive behavior during baseline, treatment, and follow-up phases.
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1220

The California School Psychologist, 2007, Vol. 12 21
figure 2. Percentage of intervals for academic engagement and disruptive behavior during baseline, treatment, and follow-up phases..
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1222

The California School Psychologist, 2007, Vol. 12 23
TABLE 3. Means and Standard Deviations for Academic Engagement and Disruptive Behavior of Eight 5th-Grade Students
Academic Engagement Disruptive Behavior
Overall M SD M SD
Baseline 22.35 16.89 59.53 20.44 Treatment 1 86.90 12.26 6.77 7.63Baseline 37.41 22.86 38.31 23.90Treatment 2 83.08 18.57 6.49 8.04Follow Up 1 75.29 25.04 15.62 22.99Follow Up 2 80.00 20.99 10.81 15.98
Attn. Seek / Antecedent M SD M SD
Baseline 21.53 14.45 68.40 19.18 Treatment 1 83.67 9.27 9.33 6.28Baseline 50.11 28.11 35.78 28.52Treatment 2 76.58 25.18 10.42 12.62Follow Up 1 74.78 32.46 22.78 32.47Follow Up 2 81.00 13.11 8.75 7.27
Attn. Seek / Consequent M SD M SD
Baseline 26.93 23.45 53.13 27.07 Treatment 1 89.13 10.13 5.13 4.67Baseline 33.50 26.31 40.40 31.79Treatment 2 88.79 11.16 6.21 6.49Follow Up 1 63.75 24.46 15.25 12.42Follow Up 2 82.00 18.57 12.75 13.65
Task Avoid / Antecedent M SD M SD
Baseline 14.92 14.95 60.17 17.59 Treatment 1 96.89 4.26 0.89 2.32Baseline 34.50 14.55 37.70 11.40Treatment 2 96.00 3.46 0.85 1.21Follow Up 1 85.00 7.35 5.00 6.22Follow Up 2 85.75 6.18 4.25 4.79
Task Avoid / Consequent M SD M SD
Baseline 24.85 10.25 56.08 12.27 Treatment 1 75.88 13.32 13.13 9.70Baseline 32.80 19.70 39.10 23.16Treatment 2 68.92 16.42 9.00 4.63Follow Up 1 78.25 20.07 10.50 13.40Follow Up 2 71.25 38.67 17.50 29.77
Functional Assessment-based Interventions
The California School Psychologist, 2007, Vol. 1224
Overall, academic engagement increased to an average of 86.9% (SD =12.3) of the intervals during Treatment phase 1. All participants also displayed a significant increase in academic engagement when treatment strategies were re-introduced after the reversal to baseline phase was concluded. The overall mean of academic engagement increased to 83.1% (SD =18.6) of the intervals during Treatment phase 2. Results regarding the overall maintenance of treatment effects indicate that increased levels of academic engagement were sustained over 15- and 30-day periods. Overall academic engagement was observed an average of 75.3% (SD =17.5) and 80.0% (SD =20.1) of the intervals during the 15- and 30-day follow-up phases, respectively.
In addition to increased academic engagement by all participants, two interesting trends emerged. First, participants assigned to a treatment strategy that was primarily antecedent-based displayed higher rates of academic engagement then those assigned to a treatment strategy that was primarily consequent-based, regardless of function of behavior. Participants receiving a primarily antecedent-based treatment strategy displayed academic engagement an average of 91.6% (SD =9.3) and 86.7% (SD =19.9) of the intervals during Treatment phases 1 and 2, respectively, whereas, participants receiving a primarily consequent-based treatment strategy displayed academic engagement an average of 82.5% (SD =13.3) and 79.6% (SD =16.9) of the intervals during the two treatment phases. Second, participants whose disruptive behavior was functionally related to task-avoidance displayed substantially higher levels of academic engagement when assigned to an antecedent-based treatment strategy, than when assigned to a consequent-based treatment strategy. Participants assigned to an antecedent-based treatment strategy whose disruptive behavior was functionally related to task-avoidance displayed academic engagement an average of 96.9% (SD =4.3) and 96.0% (SD =3.5) during Treatment phases 1 and 2 respectively, whereas, participants assigned to a consequent-based treatment strategy whose behavior was function-ally related to task-avoidance displayed academic engagement an average of 75.9% (SD =13.3) and 68.9% (SD =16.4) during the two treatment phases. Although statistical analyses were not conducted, visual inspection of the mean percentages of academic engagement (and disruptive behavior) clearly
TABLE 4. SSRS pre-test and post-test results. Standard scores and percentiles for Social Skills, Problem Behaviors, and Academic Competence.
Student Social Skills Problem Behaviors Academic Competence
Pre-test Post-test Pre-test Post-test Pre-test Post-test
A1 85 (16%) 91 (27%) 118 (88%) 123 (94%) 82 (12%) 91 (27%)
A2 73 (4%) 78 (7%) 127 (96%) 125 (95%) 78 (7%) 83 (13%)
A3 70 (2%) 95 (37%) 127 (96%) 95 (37%) 85 (16%) 83 (13%)
A4 81 (10%) 90 (25%) 125 (95%) 112 (79%) 74 (4%) 83 (13%)
C1 82 (12%) 82 (12%) 112 (79%) 110 (75%) 112 (79%) 110 (75%)
C2 86 (18%) 92 (30%) 136 (>98%) 135 (>98%) 74 (4%) 82 (12%)
C3 46 (<2%) 90 (25%) 108 (70%) 95 (37%) 79 (8%) 78 (7%)
C4 76 (5%) 86 18% 120 (91%) 115 (84%) 76 (5%) 76 (5%)

The California School Psychologist, 2007, Vol. 12 25
demonstrate that antecedent-based treatment strategies were substantially more effective for participants whose behavior was functionally related to task-avoidance.
When conducting a similar study with second grade students, Restori et al. (in review) found that antecedent-based treatment strategies were significantly more effective with students whose disruptive behavior was functionally related to attention seeking. These results indicate that treatment strategies that are primarily antecedent-based may be more effective for older children whose disruptive behavior is functionally related to task-avoidance, whereas, antecedent-based treatment approaches may be more effective for younger children whose disruptive behavior is functionally related to attention-seeking.
Disruptive behavior
Most participants displayed stable patterns of disruptive behavior during the initial baseline sessions. All participants met the pre-established criteria regarding disruptive behavior for inclusion into the study. Overall, participants displayed disruptive behavior an average of 59.5% (SD=20.4) of the intervals during the initial baseline phase and 38.3% (SD=23.0) during the reversal to baseline phase. Commensurate to the previously reported increases in academic engagement, all participants showed a significant decrease in disruptive behavior during both treatment phases. Overall, the mean of disrup-tive behavior decreased to 6.8% (SD=7.6) of the intervals during Treatment phase 1 and 6.5% (SD=8.0) during Treatment phase 2. Overall disruptive behavior decreased to an average of 15.6% (SD=23.0) and 10.8% (SD=16.0) of the intervals during the 15- and 30-day follow-up phases, respectively.
Similar to academic engagement, all participants demonstrated a significant reduction in disrup-tive behavior. In addition, the two previously described trends pertaining to academic engagement were commensurately observed with disruptive behavior. First, participants assigned to a primarily ante-cedent-based treatment strategy displayed lower levels of disruptive behavior then those assigned to a treatment strategy that was primarily consequent-based regardless of function of behavior. Partici-pants receiving an antecedent-based treatment strategy displayed disruptive behavior an average of 4.3% (SD=6.0) and 5.4% (SD=9.9) of the intervals during Treatment phases 1 and 2, respectively, whereas, participants receiving a consequent-based treatment strategy displayed disruptive behavior an average of 9.1% (SD=8.4) and 7.5% (SD=�.8) of the intervals during the two treatment phases. Second, participants whose disruptive behavior was functionally related to task-avoidance displayed lower levels of disrup-tive behavior when assigned to a primarily antecedent-based treatment strategy, than when assigned to a primarily consequent-based treatment strategy. Participants assigned to an antecedent-based treat-ment strategy whose disruptive behavior was functionally related to task-avoidance displayed disrup-tive behavior an average of 0.89% (SD=2.3) and 0.85% (SD=1.2) during Treatment phases 1 and 2 respectively, whereas, participants assigned to a consequent-based treatment strategy whose behavior was functionally related to task-avoidance displayed disruptive behavior an average of 13.1% (SD=9.7) and 9.0% (SD=4.6) during both treatment phases.
DISCuSSIon
The current study had two primary objectives. First, was to explore the practicality of conducting functional assessments within general education settings with typically developing children who displayed excessive rates of disruptive behavior and poor academic engagement as a function of either attention seeking or task avoidance. If it can be demonstrated that functional assessments can be conducted effec-tively and with minimal intrusion within a general education classroom setting, school psychologists and teachers would be better able to meet the growing demand of students experiencing disruptive patterns
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 122�
of behavior. Second, was to compare treatment strategies that were primarily antecedent-based with treatment strategies that were primarily consequent-based. Since teachers often use consequent-based treatment strategies for addressing the needs of children exhibiting behavioral difficulties, determining the effectiveness and efficiency of antecedent-based treatment strategies would likely have practical implications for teachers working with children demonstrating excessive patterns of disruptive behavior within a general education classroom setting.
Regarding the first objective, teachers and a school psychologist participated in a collabora-tive approach in conducting an FBA and developing and implementing a behavior plan for each of the participants. The school psychologist was primarily responsible for gathering data that would be used to generate a hypothesis statement regarding the function of behavior. As previously stated, this was accomplished via systematic student observations, teacher interviews, and the SSRS-T. The school psychologist and teacher then: (a) analyzed the data, (b) reviewed information obtained from the teacher interview and SSRS-T, (c) generated a hypothesis statement regarding the function of behavior, and (d) developed a behavior plan. Once the behavior plan was developed, teachers and participants were trained in intervention procedures. The teachers were primarily responsible for implementing the behavior plans and completing component analysis checklists. The school psychologist was primarily responsible for gathering student outcome and treatment integrity data. Results of this consultation-based, collaborative approach for conducting FBAs within a general education classroom was successful in identifying the variables maintaining disruptive behavior for students whose behavior was functionally related to either task-avoidance or attention-seeking.
Regarding the second objective, treatment strategies that were primarily antecedent-based were more effective than treatment strategies that were primarily consequent-based for reducing disruptive behavior and increasing academic engagement for all participants. Closer inspection of the data indi-cate that antecedent-based treatment strategies were particularly more effective than consequent-based treatment strategies for reducing disruptive behavior and increasing academic engagement when disrup-tive behavior was functionally related to task avoidance. These results are of particular interest when compared to a similar study conducted by Restori and colleagues (in review) with second grade students, wherein antecedent-based treatment strategies were particularly more effective for students whose disrup-tive behavior was found to be functionally related to attention seeking. Although the conclusions that can be drawn from these two studies are speculative due to the small sample size of each, the age differences of the participants in each study may provide the most plausible explanation for the differences found. That is, an antecedent-based treatment strategy such as self-monitoring may have been more effective with the younger, second grade students whose disruptive behavior was functionally related to attention seeking because self-monitoring provided them with sufficient attention from their teacher’s resulting in the observed increase in academic engagement and reduction in disruptive behavior. Whereas, an antecedent-based intervention such as task-modification may have been more successful with fifth grade students whose disruptive behavior was functionally related to task avoidance where the academic demands were more rigorous because it provided the necessary support, which subsequently produced the observed reduction in disruptive behavior and increase in academic engagement. Results of both studies indicate that treatment strategies that were primarily antecedent-based were more effective than consequent-based treatment strategies for second and fifth grade students whose disruptive behavior was related to either task-avoidance or attention-seeking. Anecdotally, teachers reported that interven-tions that were primarily antecedent-based were easier to implement and monitor, that consequent-based treatment strategies were exhausting, and that students were eager to participate in antecedent-based

The California School Psychologist, 2007, Vol. 12 27
treatment strategies such as self-monitoring and task-modification. This would indicate that antecedent-based treatment strategies were not only as effective as consequent-based treatment strategies, but less labor intensive and efficient.
Limitations of the Current Study
The current study has several important limitations that must be noted. First, due to the small sample of participants used in this study, results regarding external validity should be interpreted cautiously. The issue of external validity was partially addressed by employing two participants (replication) for each of the four possible functions of behavior and intervention strategy combinations. Second, all of the partici-pants in the study were male, therefore, results of treatment outcomes must also be interpreted cautiously regarding their application to females. Although the extent to which these results may apply to females is a limitation of the study, it is important to note that boys are more likely to engage in externalizing behaviors (i.e., disruptive behavior) at a rate of approximately 4:1 (Walker et al., 2004). Third, statements regarding the generalizability of the participants’ behavior are limited, since participants were observed once per day for one 15-minute session and only during a reading or reading related lesson. Although the daily 15-minute observations provide a “snapshot” of behavior, the generalization of behavior across settings (e.g., classrooms, playground, home), lessons (e.g., math, social studies), and situations (e.g., transitions, independent seatwork, lessons) cannot be assumed. Fourth, functional analyses were not conducted therefore, the hypothesized function of disruptive behavior was not experimentally vali-dated. Although functional assessments yield convergent sources of information regarding the function of behavior, a functional analysis is needed to validate the hypothesis regarding function of behavior. Although functional analyses were not conducted and the function of behavior was not validated, use of an ABAB single-case design and the success of the interventions for all participants indicate that the correct function of behavior was identified. Fifth, results regarding function of behavior should be inter-preted cautiously since the participants demonstrated disruptive behavior that was functionally related to either task-avoidance or attention-seeking. It is very likely that some students will engage in disruptive behavior that serves a dual function, is undifferentiated, or is functionally related to some other variable (e.g., sensory reinforcement). Sixth, the distinction between teacher and peer attention was not made. It is probable that students from different age groups will be differentially affected by either teacher and/or peer attention. Seventh, comparing intervention strategies that are primarily antecedent- or consequent-based may reveal which intervention strategies are better, that is, are more effective and/or easier for teachers to implement, however, such a comparison may not demonstrate which approach is best.
Implications for Research and Practice
Results and limitations of the current study indicate that a number of issues will need to be addressed through future research. First, the use of functional assessments in applied settings such as special and general education classrooms with typically developing children and children either at-risk or identified as EBD is of utmost importance. Sasso and his colleagues (2001) raised a number of important issues regarding functional assessment/analysis research that has been conducted in applied settings. Some of these concerns include the use of functional analysis within applied settings, validating the procedures and techniques used when conducting functional assessment research in applied settings, and developing a clear methodology for how each of these techniques and procedures contribute to the development of a hypothesis regarding function of behavior. Each of these concerns must be addressed if a clear, empiri-cally validated science for using applied behavior analysis methodology within applied settings is to
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1228
grow. Second, the field of applied behavior analysis has set a “high bar” regarding how behavior assess-
ment and interventions should be researched and applied. In the context of university research settings where personnel and resources may be more readily available, such standards may be justifiable, attain-able, and practical, however, within public school classroom settings, such standards may not be reason-able. Therefore, those who conduct research in applied behavior analysis and those who apply it in “real world” settings will need to find a common ground from which to build a research base and practice. Johnston, Foxx, Jacobson, Green, and Mulick (2006) have identified two “movements” that have had a significant impact within the behaviorist field. One movement consists of the applied behavior analysts (ABA) who adhere to stringent experimental rigor, high standards with regard to internal validity, and has a well-documented research base. The second and newer movement is comprised of the positive behavior support (PBS) researchers and practitioners that apply variations of applied behavior analysis, usually within school settings. PBS researchers and practitioners are willing to relinquish some of the high research standards set forth by ABA in the interest of using the behavioral technology with children in school settings. Scott and his colleagues (2004) maintain that it is unrealistic to expect practitioners working within public school settings to adhere to the rigorous experimental standards set forth by ABA. Thus, those who research functional assessment in applied settings must continue to build a research base to establish a minimum standard for conducting functional assessment research in applied settings and its use in practice.
Third, future research using functional assessment procedures in applied settings should consider developing assessment procedures that may be employed across a variety of settings, lessons, and situ-ations to further establish their external validity and generalizability. Functional assessment procedures should be modified to be less intrusive and restrictive to ensure success within applied settings. For example, classroom teachers may find a functional assessment observation form to be more practical than a partial-interval, time-sampling procedure for gathering information and data pertaining to the function of behavior. Functional assessment observation forms yield important information regarding the description, frequency, duration, time, and hypothesized function of maladaptive behavior.
Fourth, develop treatment plans that utilize antecedent- and/or consequent-based treatment strate-gies across a variety of settings, lessons, and situations to further establish their external validity and generalizability. Treatment packages should be modified to be less intrusive and restrictive to ensure success within special and general education classrooms. Treatment strategies such as self-monitoring can be modified to be practical for use within classroom settings. For example, the current study modi-fied the self-monitoring procedure described by Shapiro and Cole (1992) to fit the general education curriculum. The previously described observation and self-monitoring procedures can be modified and used across a variety of settings, lessons, and situations within general education settings.
Fifth, future research should classify students whose disruptive behavior is functionally related to attention-seeking, as seeking either teacher or peer attention. The current study did not make the distinc-tion between peer and teacher attention, however, it is likely that some students prefer peer attention, others prefer teacher attention, and others are reinforced by both teacher and peer attention. Consideration of the type of attention-seeking (i.e., peer or teacher attention) among students from different age groups is likely to have a substantial impact on the selection of both assessment and treatment procedures.
Sixth, future research focusing on treatment strategies that are primarily antecedent-based should focus on the following four aspects: (a) modifying established antecedent-based treatment strategies such as self-monitoring and task-modification for use within general education settings, (b) developing

The California School Psychologist, 2007, Vol. 12 29
new and reliable antecedent-based treatment strategies to prevent the occurrence of problem behaviors within general education settings, (c) providing social validation for the use of antecedent-based treat-ment strategies within general education settings, and (d) dissemination of antecedent-based treatment strategies to classroom teachers in order to expand their repertoire for implementing effective classroom management. As previously stated, antecedent-based treatment strategies should be part of a comprehen-sive approach for meeting the challenges posed by students with behavioral disorders.
Conclusion
This investigation provided evidence that functional assessments can be used within a general educa-tion classroom with typically developing students that demonstrate behavior problems. Results of the study indicate that all participants demonstrated decreased disruptive behavior and increased academic engagement. Results of the current study also indicated that antecedent-based treatment strategies were more effective than the more typically used consequent-based treatment strategies. Finally, results of the study indicate that school psychologists and teachers may be able meet the academic and behavioral needs of students in general education classrooms using a collaborative approach.
REfEREnCES
Becker, W., Madsen, C., Arnold, C., & Thomas, D. (1967). The contingent use of teacher attention and praise in reducing classroom behavior problems. The Journal of Special Education, 1, 55-67.
Clarke, S., Dunlap, G., Foster-Johnson, L., Wilson, D., White, R., & Vera, A. (1995). Improving the conduct of students with behavioral disorders by incorporating student interests into curricular activities. Behavioral Disor-ders, 20, 221-237.
Cooper, J. O., Heron, T. E., & Heward, W. L. (2007). Applied Behavior Analysis (2nd ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
Dunlap, G., & Kern, L. (1996). Modifying instructional activities to promote desirable behavior: A conceptual and practical framework. School Psychology Quarterly, 11, 297-312.
Dunlap, G., Kern, L., dePerczel, M., Clarke, S., Wilson, D., Childs, K. E., White, R., & Falk, G. D. (1993). Func-tional analysis of classroom variables for students with emotional and behavioral disorders. Behavioral Disor-ders, 18, 275-291.
Dunlap, G., White, R., Vera, A., Wilson, D., & Panacek, L. (1996). The effects of multi-component, assessment-based curricular modifications of the classroom behavior of children with emotional and behavioral disorders. Journal of Behavior Education, �, 481-500.
Fuchs, D. & Fuchs, L. (1989). Exploring effective and efficient prereferral interventions: A component analysis of behavioral consultation. School Psychology Review, 18, 260-283.
Gresham, F. M. (1989). Assessment of treatment integrity in school consultation and prereferral intervention. School Psychology Review, 18, 37-50.
Gresham, F. M., & Elliott, S. N. (1990). Social Skills Rating System. Circle Pines, MN: American Guidance Service.
Gresham, F. M., Watson, T. S., & Skinner, C. (2001). Functional behavior assessment: Principles, procedures, and future directions. School Psychology Review, 30, 156-172.
Horner, R. D. (1994). Functional assessment contributions and future directions. Journal of Applied Behavior Anal-ysis, 27, 401-404.
Horner, R. H., & Sugai, G. (2000). School-wide behavior support: An emerging initiative (special issue). Journal of Positive Behavioral Interventions, 2, 231-232.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richmond, G. S. (1982). Toward a functional analysis of self-injury. Analysis and Intervention in Development Disabilities, 2, 1-20.
Johnston, J. M., Foxx, R. M., Jacobson, J. W., Green, G., & Mulick, J. A. (2006). Positive behavior support and applied behavior analysis. The Behavior Analyst, 29, 51-74.
Johnston, J. M., & Pennypacker, H. S. (1993). Strategies and tactics of behavioral research (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.
Functional Assessment-based Interventions

The California School Psychologist, 2007, Vol. 1230
Kamps, D., Wendland, M., & Culpepper, M. (2006). Active teacher participation in functional behavior assessment for students with emotional and behavioral disorders risks in general education classrooms. Behavioral Disor-ders, 31, 128-146.
Kern, L., & Clemens, N. H. (2007). Antecedent strategies to promote appropriate classroom behavior. Psychology in the Schools, 44, 65-75.
Kern, L., Delaney, B., Clarke, S., Dunlap, G., & Childs, K. E. (2001). Improving the classroom behavior of students with emotional and behavioral disorders using individualized curricular modifications. Journal of Emotional and Behavioral Disorders, 9, 239-247.
Kern, L., Hilt, A. M., & Gresham, F. M. (2004). An evaluation of the functional behavior assessment process used with students with or at risk for emotional and behavioral disorders. Education and Treatment of Children, 27, 440-452.
Lane, K. L., Robertson, E. J., & Graham-Bailey, M. A. L. (2006). An examination of school-wide interventions with primary level efforts conducted in secondary schools: Methodological considerations. In T. E. Scruggs & M. A. Mastropieri (Eds.), Applications of research methodology: Advances in learning and behavioral disabilities (vol. 19). Oxford, UK: Elsevier.
Lane, K. L., Umbreit, J., & Beebe-Frankenberger, M. (1999). A review of functional assessment research with students with or at-risk for emotional and behavioral disorders. Journal of Positive Behavioral Interventions, 1, 101-111.
Lane, K. L., Weisenbach, J. L., Little, M. A., Phillips, A., & Wehby, J. (2006). Illustrations of function-based inter-ventions implemented by general education teachers: Building capacity at the school site. Education and Treat-ment of Children, 29, 549-671.
Lennox, D. B., Miltenberger, R. G., Spengler, P., & Erfanian, N. (1988). Decelerative treatment practices with persons who have mental retardation: A review of five years of literature. American Journal of Mental Retarda-tion, 92, 492-501.
Lewis, C., & Sugai, G. (1996). Functional assessment of problem behavior: A pilot investigation of the compara-tive and interactive effects of teacher and peer social attention on students in general education settings. School Psychology Quarterly, 11, 1-19.
Marcus, B. A., & Vollmer, T. R. (1996). Combining non-contingent reinforcement and differential reinforcement schedules as treatment for aberrant behavior. Journal of Applied Behavior Analysis, 29, 43-51.
Martens, B. K., Peterson, R. l., Witt, J. C., & Cirone, S. (1986). Teacher perceptions of school-based interventions. Exceptional Children, 53, 213-223.
Newcomer, L. L., & Lewis, T. J. (2004). Functional behavior assessment: An investigation of behavior reliability and effectiveness of function-based interventions. Journal of Emotional and Behavioral Disorders, 12, 168-181.
Olweus, D. (1979). Stability of aggressive reaction patterns in males: A review. Psychological Bulletin, 8�, 852-875.
Restori, A. F., Gresham, F. M., Chang, T., Lee, H. B., Laija-Rodriquez, W. (2007). Functional assessment-based interventions: Outcomes of antecedent- and consequent-based tactics in general education classrooms. Manu-script submitted for publication.
Sasso, G. M., Conroy, M. A., Stichter, J., & Fox, J. J. (2001). Slowing down the bandwagon: The misapplication of functional assessment for students with emotional and behavioral disorders. Behavioral Disorders, 2�, 282-296.
Scott, T. M., Bucalos, A., Liaupsin, C., Nelson, C. M., Jolivette, K., & DeShea, L. (2004). Using functional behavior assessment in general education settings: Making a case for effectiveness and efficiency. Behavioral Disorders, 29, 189-201.
Shapiro, E. S., & Cole, C. L. (1992). Self-monitoring. In T. H. Ollendick & M. Hersen (Eds.). Handbook of child and adolescent assessment (2nd ed). pp. 124-139). New York: Pergmon.
Umbreit, J. (1996). Functional analysis of disruptive behavior in an inclusive classroom. Journal of Early Interven-tion, 20, 18-29.
Umbreit, J., & Blair, K. S. (1997). Using structural analysis to facilitate treatment of aggression and noncompliance in a young child at-risk for behavioral disorders. Behavioral Disorders, 22, 75-86.
Umbreit, J., Lane, K. L., & Dejud, C. (2004). Improving classroom behavior by modifying task difficulty: Effects of increasing the difficulty of too-easy tasks. Journal of Positive Behavior Interventions, �, 13-20.
Walker, H. M., Ramsey, E., & Gresham, F. M. (2004). Antisocial behavior in school: Evidenced-based practices (2nd ed.). Belmont, CA: Wadsworth/Thomson Learning.
Walker, H. M., & Severson, H. H. (1991). Systematic Screening for Behavior Disorders (SSBD): User’s guide and technical manual. Longmont, CO: Sopris West.

The California School Psychologist, 2007, Vol. 12 31
Please send correspondence to Paul Muyskens, at Minneapolis Public Schools; 807 NE Broadway; Minneapolis, MN, USA; 55413-2398 or e-mail [email protected]
The California School Psychologist, Vol. 12, pp. 31 –45, 2007Copyright 2007 California Association of School Psychologists
The use of Response to Intervention Practices for Behavior: An Examination of the Validity of a Screening Instrument
Paul Muyskens & Doug Marston
Minneapolis Public Schools
Amy L. Reschly University of Georgia
Behavioral difficulties of school-aged students are typically dealt with in a reactive, rather than preven-tative manner. This article examines a proactive approach, consistent with the Response-to-Interven-tion model, using a screening measure designed to identify students at risk for behavior difficulties and targeting these students for early intervention. Participants in this study were 22,056 kindergarten through 8th grade students in the Minneapolis Public Schools. Teachers completed a 12-item behavior screener for each student in the fall. The scores on this measure were significantly correlated with suspensions, achievement scores and attendance data over the course of the school year. Potential implications for behavioral planning and interventions are discussed.
KEYWORDS: Behavior, Behavior Screening, Response to Intervention
In a recent report, the National Academy of Sciences Committee on Minority Representation in Special Education noted, “There is substantial evidence with regard to both behavior and achievement that early identification and intervention is more effective than later identification and intervention.” (p. 6, Donovan & Cross, 2002). While the logic of preventing or addressing problems before they become severe is both obvious and compelling, historically, schools have been reactive, rather than proactive institutions (Walker et al., 1996). In terms of addressing academic or behavioral concerns, this reactivity is often referred to as a “wait-to-fail” model. Criticism of this approach is well-documented and there are increasing calls in the literature for screening and/or early intervention for academic and behavior problems (e.g., Donovan & Cross, 2002; O’Shaughnessy, Lane, Gresham, & Beebe-Frankenberger, 2003; Walker et al., 1996; Reschly & Ysseldyke, 2002).
Despite the link between student behavior and academic performance (Alexander, Entwisle, & Dauber, 1993) and the association between behavior and long-term social outcomes for students (Kaplan, Peck, & Kaplan, 1997), the knowledge base for systematic screening and tracking of emotional and behavior problems lags behind that of academics, particularly reading (Donovan & Cross, 2002). In addition to interfering with other students’ learning, problem behaviors can be violent and/or destructive. For example, in 1999-2000, 29% of principals reported that student bullying occurred daily or weekly, while 19% of principals reported acts of disrespect to teachers with the same frequency (DeVoe et al., 2004). Many educators report difficulty managing student behavior on a day-to-day basis and both parents and the general public are concerned about discipline and safety in our schools. For example, when Americans were asked about the biggest problems facing education, concerns over school disci-pline/control were tied for 2nd as the most frequent response (behind school funding and tied with over-crowding; Gallup, 2004); and 1/3 of parents worry about their children’s physical safety at school, a concern that peaks with the parents of middle school-age children (Gallup, 2002).

The California School Psychologist, 2007, Vol. 1232
Although there is evidence for the efficacy of proactive, school-wide behavior support models (e.g., Sugai et al., 2000), schools typically rely on disciplinary action as the primary means of managing student misbehavior. Zero tolerance policies, the elimination of social promotion, and “get tough” rules are the current trends. Unfortunately, there is little evidence for the effectiveness of these approaches for improving school safety or long-term student outcomes (Skiba & Peterson, 1999). In addition, the result of disciplinary policies based upon clear standards or zero tolerance is typically not instructional, but rather exclusionary. Students and schools can ill afford exclusionary policies that result in lost opportunities for instruction, an outcome that is associated with lower student and school-level achievement (Skiba & Rausch, 2004) and may be related to increased dropout rates, or students dropping out at a younger age (Bock, Tapscott, & Savner, 1998; DeRidder, 1990).
Another issue in managing student behavior primarily through disciplinary approaches is that the application of these practices varies by school characteristics, principal attitudes, and even by teachers within the same school (Rausch & Skiba, 2004; Skiba & Rausch, 2006). Whenever there is uneven or inconsistent application of an educational practice or policy, harmful disparities may result. In the case of discipline, there is evidence that the use of harsh disciplinary practices varies by socioeconomic status and race, negatively affecting students of lower socioeconomic backgrounds and African-Amer-ican students. As noted by Skiba and Rausch (2006), “Over thirty years of consistent data concerning African American over-representation in suspension and expulsion indicates that disciplinary school exclusion may carry inherent risks for creating or exacerbating racial and socioeconomic disadvan-tage.” (p. 93).
Concerns over fairness and bias in managing and evaluating student behavior spill over into the special education arena. On a national level, African-American students are disproportionately repre-sented in special education programs for Emotional Disturbance and Mental Retardation, and American-Indian students are disproportionately represented in programs for Learning Disabilities, while Asian Americans, Hispanics, and Whites are underrepresented (Donovan & Cross, 2002; MacMillan & Reschly, 1998). While the causes of over- and under- representation are complex and the debate controversial, there is concern about bias in interpretation of students’ behavior and the seemingly haphazard nature of the referral procedure. The identification and referral process for emotional and behavioral concerns has been described as, “unsystematic, idiosyncratic, and late in the development of a behavioral problem” (Donovan & Cross, 2002, p.296), while the President’s Commission on Excellence in Special Education (U.S. Department of Education, Office of Special Education and Rehabilitative Services, 2002, p. 26) noted that, “Minority children are much more likely to be placed in the emotional disturbance category because of behavioral characteristics associated with the cultural context in which a child is raised. A major factor is the role of teacher referral.”
MInnEAPoLIS PuBLIC SChooLS PRoBLEM-SoLVIng/RESPonSE To InTERVEnTIon MoDEL
A Response-to-Intervention (RtI), or problem-solving, approach has been put forth as a potential alternative to the traditional refer-test-place process for special education (e.g., Gresham, 2002; Grimes, 2002; Marston, 2002; Reschly & Tilly, 1999; Shinn, Good, & Parker, 1999). Problem-solving has been described as, “…a self-correcting methodology to identify, analyze, and intervene with difficulties at the individual, group, and system levels” (Reschly, 2005). As described by Fuchs and Fuchs (2006), the first step in an RtI model is to identify students at-risk for not responding to interventions. This activity should take place early in the school year, and involves screening all students on a tool that is tied to

The California School Psychologist, 2007, Vol. 12 33
subsequent performance. An RtI or problem-solving model is a means of counteracting the wait-to-fail approach because once students are identified as at-risk, their progress is monitored and if progress is not made interventions are provided. Students’ responses, or outcomes to interventions, are then used to determine the need for more intensive interventions and services. When personnel and services are orga-nized around intervention, rather than assessment for placement, the time and resources for screening and early intervention activities become available.
While most recent attention and controversy about RtI concerns the use of this model in identifying students with learning disabilities (e.g., Bradley, Danielson, & Hallahan, 2002; Naglieri, 2005; Reschly, 2005), large-scale applications (Iowa, Minneapolis Public Schools) use this methodology to address both academic and behavioral concerns. In addition, there is some evidence that the utilization of a model like RtI reduces minority overrepresentation in special education (Barbour, 2006), possibly due to the use of direct (e.g., Curriculum-Based Measurement; structured behavioral observation) rather than indi-rect measures (e.g., IQ) of student performance.
Minneapolis Public Schools has used a Problem-Solving Model (PSM) as an alternative to traditional special education eligibility criteria since 1993. The steps in the PSM include defining the problem and establishing the current level of performance, generating possible solutions to the problem, implementing the best solution, and reviewing the results of the intervention (see Deno, 2002). As implemented in Minneapolis, students in need of intervention cycle through this process first within the general educa-tion classroom, then with increasing intensity at the building assistance team level and, if necessary, in the special education evaluation phase. Further information regarding the rationale of the PSM or its implementation in Minneapolis Public Schools may be found in Marston, Muyskens, Lau, and Canter (2003) and Lau, Sieler, Muyskens, Canter, VanKueren and Marston (2006). The expansion of the role of the PSM in the Minneapolis Public Schools was facilitated by a voluntary compliance agreement with the Office of Civil Rights. The purpose of this agreement was to address the disproportionate repre-sentation of some minority groups in special education programs by implementing screening and early interventions for students having difficulty with academics and/or school behavior. Implementation of behavioral screening for kindergarten through 8th grades was a part of this agreement.
Although sites across the country vary in their implementation of the PSM, a hallmark of the Minne-apolis model is the use of both academic and behavioral screening measures. In this model, students go from screening directly into a series of activities or queries related to the design of an interven-tion. More specifically, high scores on the screening measures indicate a need for further investigation, and school staff is subsequently directed to complete the Classroom Intervention Worksheet for these students. Subsequent completion of the Classroom Intervention Worksheet prompts teachers to initiate communications with parents, students, other staff members and a review of records. Further, teachers are asked to describe current levels of performance, identify student strengths, review health informa-tion, and specify potential intervention strategies. This information is used to design a classroom-based intervention that is implemented by the teacher. Students who do not demonstrate improved behaviors in response to this intervention may be referred to the problem-solving team. This team implements a problem-solving process which is used to design a more intensive intervention, along with the collection of more frequent progress-monitoring data. Students who do not respond to these interventions may then be referred for special education evaluation (see Marston et al., 2003).
There is a knowledge base for screening students in core academic areas (Donovan & Cross, 2002). Minneapolis Public Schools utilizes students’ performance on the District-wide achievement test (the Northwest Achievement Levels Test, or NALT), Curriculum-Based Measurement probes, and informal
Behavioral Screening

The California School Psychologist, 2007, Vol. 1234
reading inventories. In many cases, scores on these measures are tied, or benchmarked, to passing scores on the state of Minnesota high-stakes assessment, the Minnesota Comprehensive Assessment – Series II (MCA-IIs). As mentioned previously, however, the methodology to systematically screen and track students with behavioral concerns lags behind that which is available in academic areas. To address the need for behavioral screening in the PSM, staff in the Minneapolis Public Schools developed a new screening measure, the Behavior Screening Checklist (BSC).
The determination that a new behavioral screening measure was needed was largely done through a process of elimination. There were several school-related variables that were plausible indicators of behavioral problems, such as office referral and suspension data, teacher report card ratings, and obser-vations. However, there were problems with using these variables for screening purposes. For example, office referral and suspension data were typically too reactionary for a screening measure (i.e., data are not collected until after a problem is severe), and the data are often not compiled systematically. Report card ratings were quite global in nature (e.g., satisfactory, satisfactory plus) and the use of observations for screening purposes would have been very time-intensive and expensive. In selecting a measure for screening, it was important that the data not only have evidence for technical adequacy and validity but also amenable to quick and systematic collection from all students. Although rating scale reports can be limited by the context or relationship with the child and/or informant and are generally of little utility for determining etiology or intervention planning (McConaughy 1993), rating scales are efficient, rela-tively objective and reliable, allow for a collection of information about a broad range of observations and teacher interactions, and indicate risk status (Feil, Severson, & Walker, 2002). Finally, behavioral rating scale data can be used to estimate symptom severity across times, observers, and settings within a problem-solving model (Busse, 2005).
After a review of the literature and existing instruments, it was determined that existing compre-hensive rating systems such as the Behavior Assessment System for Children (BASC) – Second Edition (Reynolds & Kamphaus, 2004) or Child Behavior Checklist system (Achenbach, 2002) were too long for our purpose of screening all students. For example, the BASC – Second Edition Teacher Rating Scale takes about 10 to 15 minutes to complete. It is recommended that teachers complete it on one occa-sion with minimal distractions (BASC; Reynolds and Kamphaus, 2004). This time commitment does not include scoring, and thus, would be impractical for use as a class- or school-wide screening instrument.
The BSC was developed as a general purpose measure in consultation with district teachers and behavioral experts. A key in the development of our screener was weighing the need for brevity while still tapping a range of important classroom behaviors with adequate psychometric properties. The primary purpose of the BSC is to help teachers identify students early in the year who have behavioral issues who may benefit from general education interventions within the PSM. In this study, we sought to examine the technical adequacy of this measure in terms of, a) the inter-rater and internal consistency reliability and b) the predictive validity of the BSC with subsequent behavioral and academic difficul-ties. Measures of achievement are included in our examination of validity because of the interconnected nature of student behavior and academic performance, and because of the paucity of objective measures of behavior.
METhoD
Participants
The subjects of this study included 22,056 kindergarten through grade 8 students in the Minne-apolis Public Schools (MPS), a large urban district located in Minnesota. Of these students 49.9% were

The California School Psychologist, 2007, Vol. 12 35
female and 51.1% were male. The racial/ethnic distribution of the sample was: 40% African American, 28% White American, 16.6% Hispanic American, 11.8% Asian American, and 3.6% Native American. Approximately 68% of the sample received free or reduced lunch services.
Measures
Behavior Screening Checklist. When first implemented in the District during the 1998-99 academic year, the BSC was comprised of 10 items; items regarding property destruction and out of place behavior were added during the first year based on teacher and staff feedback. The 12 items included in the BSC were grouped into 3 categories: Classroom Behaviors, Externalizing Behaviors, and Socialization (See Appendix A). The Classroom Behaviors section included four items: evaluating student attention, following directions, completing work, and class involvement. The Externalizing Behaviors section included: physical behavior toward others, verbal behavior toward others, physical behavior toward property, and out of place. The last section of the BSC, Socialization, also had four items: adult interac-tions, peer interactions, coping with change, and projected self-image. On each item staff was asked to rate the student on a scale of 1 to �, with 1 representing the most appropriate behavior related to that area and a 5 associated with significant concerns. When introducing the BSC to teachers it was emphasized that this tool is a screening measure, and should be thought of as a prompt to think of all students using the same questions. If questions arose about a particular rating, teachers were encouraged to go with their first impression.
Thirty-six was used as the BSC cut-score for those students in need of additional classroom inter-ventions. This score was initially chosen as the cut score because it was the point in the distribution at which approximately 5% of the student population fell at or above this score. This is similar to the level of students considered to be in need of tertiary prevention or intense individualized interventions in some systems of Positive Behavior Support (Sugai & Horner, 2002) or Response-to-Intervention Models (Batsche, 2005). It was also thought that this targeted a manageable number of students for additional intervention. For these students teachers were directed to begin interventions related to the problem of concern within their classrooms, and to determine their responses to these interventions.
Northwest Achievement Levels Test. The Northwest Achievement Levels Test1, or NALT, is a stan-dardized multiple-choice test that was administered to all students in the district in grades 2 through 7, and 9 in the areas of reading and mathematics. From the item bank, district personnel chose items that corresponded to the district’s curriculum standards, allowing for measurement of students’ knowl-edge and skills with respect to these standards. The NALT is a levels-test with national growth norms and, therefore, student performance may be linked from level-to-level and grade-to-grade. Further, it is possible to measure growth over time at the student, classroom, school, and district levels. The norms are based on a sample of over 1 million students. A student’s performance is based on two factors: the number of correct answers and the difficulty of the questions. Each student’s normal curve equivalent (NCE) score was used in the analysis. NCE scores for reading ranged from 1 to 99 with a mean of 48.7 and a standard deviation of 21.8. For math the NCE scores ranged from 1 to 99 with a mean of 54.6 and a standard deviation of 22.0.
Student behavior: Suspensions and attendance. The total number of suspensions from school during the entire academic year was used as one criterion measure of student behavior. Suspension scores for students in our sample ranged from 0 to 21 with a mean of 0.35 and a standard deviation of 1.24. Student attendance was calculated by dividing the number of days absent from school by the total number of
1 Further information may be found at http://www.nwea.org/
Behavioral Screening

The California School Psychologist, 2007, Vol. 123�
days enrolled (days present and absent). The percentage of days absent in the sample ranged from 0% to 77.4% with a mean of 4.9% and a standard deviation of 5.8%.
PRoCEDuRES
BSC data were collected in the fall. Teachers completed the BSC for all students in their class-rooms by October 1st of the academic year. Data were collected district-wide as part of the PSM process described in the introduction. Teachers were asked to complete screeners for all students, typically all at one time. While they were encouraged to go with their first impression, expanded scoring definitions were available. Other criterion measures were collected from District records.
RESuLTS
Reliability Analyses
Inter-rater reliability. Inter-rater reliability and agreement were used to examine this form of reli-ability. At the time the BSC was first implemented in the District, a collaborative teaching project was in place in which two teachers were assigned to every third grade classroom. These teachers shared instructional responsibilities for their classes, which presented an optimal situation for checking inter-rater agreement of the behavior screener. Research staff recruited six pairs of collaborative teachers to complete a behavior screener with entire classes of students (2 raters for 143 students). These analyses were run with the 10-item version of the BSC. An inter-rater reliability coefficient was calculated for each pair as well as the percent agreement for those below and above the district cut-score1 identifying students in need of additional classroom interventions.
Inter-rater reliability coefficients were calculated for six pairs of 3rd grade teachers who taught 143 students in six classrooms. Sample sizes for those ratings ranged from 17 to 28 students per classroom. All coefficients were significant at or below .01. Coefficients ranged from .659 to .965, with a mean rating of .825 (see Table 1). Inter-rater agreement between teachers for those students below and at or above the cut-score was 91%.
TABLE 1. Inter-rater reliability coefficients for six pairs of teachers
Teacher Group Number of Students Reliability Coefficient
Pair 1 25 .865Pair 2 25 .965Pair 3 27 .847Pair 4 17 .659Pair 5 28 .819Pair 6 21 .796Average Correlation .825
Internal Consistency Reliability
Chronbach’s alpha was used to examine the internal consistency reliability of the BSC. Chronbach’s alpha is reported for the original 10-item version of the BSC (N = 143) and the current 12-item BSC. 1 Thirty-six is the cut score used with the 12-item BSC. A cut score for the 10-item BSC that corresponds with
the same portion of the distribution was 31.

The California School Psychologist, 2007, Vol. 12 37
The distribution of the sample used in analysis of the 12-item BSC by grade may be found in Table 2. The alpha coefficient for the original 10-item BSC was .93. On the more recent 12-item version alpha coefficients ranged from .92 to .95 for grades kindergarten to grade 8 (kindergarten: .93; 1st grade: .92; 2nd grade: .93; 3rd grade; .93, 4th grade; .93, 5th grade: .93; 6th grade: .94; 7th grade: .95; and 8th grade: .94).
Descriptive Analyses
Descriptive data for the entire sample of students are presented in Tables 2 and 3. Scores on the BSC ranged from 12 (which represents a rating of “1” on each item) to 60 (a rating of “5” on each item). The mean total score on the Behavior Screener Checklist was 20.37 with a standard deviation of 8.40. The distribution of scores was positively skewed, with most students earning scores in the low-end of the scale, indicating few behavioral concerns (See Table 2). Approximately 74% of the students scored at or below 24 on the BSC, while 5.2% scored above 36, the cut-off score for initiation of classroom interventions.
TABLE 2. BSC Descriptive Statistics by Grade
Grade Mean N Std. Deviation Minimum Maximum
Kdg 19.68 2607 7.69 12 601 19.29 2623 7.55 12 562 19.84 2710 7.83 12 573 19.53 2431 8.01 12 594 20.17 2443 8.01 12 595 19.43 2521 7.62 12 576 21.87 2192 9.01 12 567 22.33 2197 9.95 12 608 21.82 2332 9.37 12 60Total 20.37 22056 8.40 12 60
Note: Distribution Characteristics of the total Sample Skewness = 1.297 (SE = .016); Kurtosis = 1.711 (SE = .033)
The means, standard deviations and sample sizes at each grade level are presented in Table 2. It is apparent that there is a gradual increase in scores on the BSC as students grow older, with the highest scores recorded for students in the middle school years. Behavior screening scores also vary by gender and ethnicity (Table 3). Male students scored higher than female students. BSC scores are somewhat higher for African-American and Native-American students. Relatively lower scores were obtained for Asian-American and White-American students.
Predictive validity analyses
Predictive criterion validity of the BSC was studied by using separate correlation analyses for students in K to 5 (N = 14,335) and grades 6 to 8 (N = 6,721), corresponding with the change in school level from elementary to middle school. It was anticipated that BSC scores would vary as a function of school level, with more reported difficulties for older students. Fall BSC data were correlated with crite-rion measures (NALT, suspensions, attendance) collected in the spring of the same academic year.
Behavioral Screening

The California School Psychologist, 2007, Vol. 1238
TABLE 3. BSC Descriptive Statistics by Grade
Variable Mean N SD Minimum Maximum
gender Female 18.71 10995 7.32 12 60 Male 22.02 11061 9.06 12 60 Total 20.37 22056 8.40 12 60
Ethnicity Native American 22.58 783 8.82 12 59 African American 23.45 8828 9.29 12 60 Asian American 17.37 2609 6.29 12 60 Hispanic 19.06 3664 7.15 12 58 White 17.73 6172 6.77 12 59 Total 20.37 22056 8.40 12 60
TABLE 4. Correlations between BCS and criterion variables (K-5 sample)
Number of Number of NALT Reading NALT Math Suspensions Absences NCE NCE
Behavior Screener 0.28* 0.19* -0.39* -0.42* N 15335 15335 6135 6117Number of Suspensions 0.18* -0.20* -0.19* N 15335 6135 6117Number of Absences -0.13* -0.18* N 6135 6117 NALT Reading NCE 0.80* N 6092
*p < .001
TABLE 5. Correlation between BSC and Criterion Variables (�-8 sample)
Number of Number of NALT Reading NALT Math Suspensions Absences NCE NCE
Behavior Screener 0.51* 0.36* -0.45* -0.48* N 6721 6721 3657 3357Number of Suspensions 0.46* -0.30* -0.34* N 6721 3657 3357Number of Absences -0.20* -0.26* N 3657 3357 NALT Reading NCE 0.84* N 3320
*p < .001

The California School Psychologist, 2007, Vol. 12 39
Because of the skewed distribution of BSC scores and the ordinal nature of the scale, a Spear-man’s rho correlation was used for the measure of predictive validity for both the K-5 and 6-8 samples. The total score on the BSC administered in the fall was correlated with the end of the year number of suspensions, percentage of days absent from school, and district achievement scores in reading and math from spring test administration. For both groups the correlations between all of these variables were significant at the .01 level (Tables 4 and 5). Correlations between the BSC and criterion variables were higher in all cases for the grade 6-8 group. There were moderate correlations between fall BSC scores and the number of suspensions and reading and math achievement in the spring. The correlation between the BSC and suspensions was higher for the grade 6-8 group (.28 and .51, respectively, K-5 and grades 6-8). Correlations between the achievement measure and the BSC were also better for the grade 6-8 group (an average correlation of -.40 for K to grade 5; -.46 for the upper grade level group).
A visual analysis of the predictive nature of the BSC was also conducted. A cross-tabs procedure was used to display scores on the BSC with the number of suspensions, achievement scores in reading and math, and total days absent from school. This analysis, presented in Figure 1, was conducted because we were interested in examining how higher scores on the fall BSC interacted with the related
Behavioral Screening
80
70
60
50
40
30
20
10
0
GT=
12
GT=
16
GT=
20
GT=
24
GT=
28
GT=
32
GT=
36
GT=
40
GT=
44
GT=
48
GT=
52
BSC3 Rating
Per
cent
ile o
r Sta
ndar
d S
core
% Suspended
% Days Absent
Mean ReadingNALT NCE
Mean MathNALT NCE
figure 1. Percentage of students suspended, median reading and math NALT NCE scores, and average percentage of days absent for groups of students scoring at or above selected BSC total scores.*
* Values on Y-axis represent three different scales associated with suspensions, achievement, and atten-dance.

The California School Psychologist, 2007, Vol. 1240
variables. Note that the vertical axis in Figure 1, which ranges from 0 to 80, represents three scales: percentage of students suspended; mean NCE scores in reading and math for each BSC group, and average percentage of days absent from each BSC group. There appears to be a linear relationship between fall BSC scores and the likelihood of being suspended during the year. While only 13.6% of the total sample was suspended, 60.3% of those students scoring 36 or above on the fall behavior screener were suspended.
The relationship between the BSC scores and achievement scores appears to be greater at the lower end of the scale, but continues in an inverse manner as the behavior scores rise. The student group as a whole achieved over 6 NCE’s higher in reading and math than those scoring 16 or above on the BSC, and 17 to 19 NCE’s higher in reading and math than those scoring 36 or above on the BSC. This differ-ence can be largely accounted for by the average NALT NCE score for reading being above 60 for those students scoring 12 on the BSC (mean score = 61.0 for reading and 67.6 for math (N=2,007 and 1,949, respectively). The mean score for those students scoring 16 on the BSC was 51.1 for reading (N=449) and 57.7 for math (N=485). The relationship between the fall BSC scores and percentage of days absent from school was not strong. There is a gradual increase in percentage of absences as the BSC scores rise, before a plateau around a score of 48.
DISCuSSIon
Student behavior figures prominently in our schools, with links to academic performance and long-term social outcomes for students. The most frequent or common approach to managing student behavior is reactionary, rather than proactive, in nature. The use of harsh disciplinary practices – zero tolerance policies – has increased, despite the absence of evidence for the effectiveness of these approaches for improving student behavior or school climate. Indeed, these practices may negatively affect student achievement and school completion, and there is evidence of socioeconomic and racial disparities in the disciplinary management of students in our nations’ schools. The logic of preventing or intervening early with problems, whether academic or behavioral, before these problems become severe and sometimes intractable, is obvious; however, this requires a major shift in thinking and practice. The knowledge base for screening and tracking emotional and behavioral problems is not well-established. The focus of this study was to examine a classroom behavior screener, the BSC, developed for use in the PSM utilized by the Minneapolis Public Schools. The purpose of the BSC was to identify students with behavior needs to inform general education interventions as part of the PSM.
One of the first questions in the development and use of a new measure relates to the technical adequacy. The inter-rater reliability coefficients examined in this study were technically adequate, as was the inter-rater agreement for teacher ratings of those below and at or above the cut score signaling the need for additional intervention. It should also be noted these coefficients tended to be higher than those often obtained for cross-informant ratings of student behavior. In a meta-analysis of 119 studies, Achenbach, McConaughy, and Howell reported that the average correlation between respondents of similar roles, such as 2 teachers, was .60, while the correlation among respondents of different roles was considerably lower (reported in McConaughy, 1993b). The internal consistency coefficients were extremely high and also documented technical adequacy in the area of reliability.
There are concerns over bias and disparity in both disciplinary actions and special education place-ments. The pattern of scores on the BSC is similar to that found in other research: African American, Native American, middle school, and male students received higher scores on the BSC. Screening with an instrument like the BSC will not address concerns over misinterpretation of student behavior due to

The California School Psychologist, 2007, Vol. 12 41
cultural or racial differences; however, screening with a focus on early intervention is a step in the right direction and may help attenuate some of the poor outcomes associated with harsh disciplinary policies (e.g., loss of instructional time, dropout, special education placements). Donovan and Cross (2002) argued the overall impact of early intervention models will be to reduce the numbers of students who fail, which in turn meets the educational needs of students of color.
BSC predictive validity was evidenced by moderate correlations between fall ratings and behavioral performance over the course of the school year and academic assessments administered in the spring. In addition, the results showed a clear and consistent relationship between scores on the BSC and the likelihood of suspension. Those students scoring 36 or above in the fall have a 50% chance of being suspended over the course of the school year.
This study provided some evidence to support the use of the BSC as an efficient, reliable, and valid screening tool to aid teachers and other school staff in identifying students likely to encounter significant behavioral difficulties, particularly those at-risk for suspensions. As noted by Gersten and Dimino (2006), one of the failures of the prereferral model of the late 1980’s was that, “Student Study Teams typically made intervention recommendations on the basis of the classroom teacher’s description of the student’s academic or behavioral performance. Many of the descriptions were anecdotal; few were data based.” (Gersten & Dimino, 2006, p. 101). The ability to use the BSC to identify students in need of interventions may help teachers to examine their students’ behaviors earlier in the school year, and provides a measure which prompts teachers to rate all students’ behaviors on objective items. This should also lessen the bias introduced by teacher nomination, and will hopefully provide for intervention before a cycle of frustration or failure is created.
In practical terms, the provision of teachers with a tool which in less than a minute can help them identify students likely to present significant behavioral or academic concerns over the course of the school year seems worthy. On average those students scoring at or above 36 on the BSC were over 4 times as likely to be suspended as the total sample, were likely to be absent almost twice as much, and scored around one-half standard deviation lower on measures of achievement. This knowledge can be used to target students, classrooms or programs for intervention programs before these problems arise.
There is a tension between maintaining scientific rigor while conducting research in real-world settings. This study is no exception. The strengths of this study – the design and implementation of a screening measure for use in a PSM and subsequent research with a large, diverse school population – are also weaknesses. There was little time between development and implementation of the BSC as a district-wide K-8 screener; analyses of its adequacy were post-hoc. Future study should address refining the BSC, including examination of individual items, the need for and utility of age-specific versions, and the establishment of norms and cut-scores for screening purposes. In addition, validity studies relating the BSC to other forms of behavioral assessment are needed as further evidence of its validity. Further-more, although behavior rating scales in general are ideal for screening purposes, due to their relative efficiency, objectivity, and reliability (Feil, Severson, & Walker, 2002), these scales do not provide infor-mation regarding etiology or intervention design (McCanaughy, 1993). This is true of the BSC as well. The purpose of this screener was to identify students in need of early intervention; it does not provide information to teachers on how to intervene nor is it a sensitive measure of how a specific behavior changes due to the intervention. Future research must address the critical link between screening and intervention planning and implementation within the PSM.
There are a range of demands on the educational system, including increased accountability, No Child Left Behind, budgeting concerns, and discipline. In the midst of these demands, however, it is
Behavioral Screening

The California School Psychologist, 2007, Vol. 1242
clear that the traditional wait-to-fail model used for academic and behavioral difficulties does not meet the needs of our students or the system as a whole. While wait-to-fail is the past and present, screening and early interventions are the future. In their call for a “paradigm shift,” Reschly and Ysseldyke (2002) argue that data-based problem solving is crucial to system reform. A response-to-intervention model promotes the early identification of students’ academic and behavioral difficulties and provides inter-ventions and monitoring with increasing intensity until effective interventions and environments are found for students. Although further research is needed, the behavior screener described is a model for addressing significant behavioral issues in a proactive way that is linked to problem solving and better outcomes for at risk children and youth.
Appendix A
BEhAVIoR SCREEnIng ChECkLIST III
Student Name: Student ID#: Date:
Rate the student on the following continuum:
I. AREA: CLASSRooM BEhAVIoRS
Attention: 1 2 3 4 �
Consistently attends to Sometimes follows along Rarely follows along classroom activities with classroom activities with classroom activities
follows Directions: 1 2 3 4 �
Consistently follows rules Sometimes follows rules Rarely follows rules
Completing Work: 1 2 3 4 �
Consistently completes Sometimes completes Rarely completes work independently work independently work independently
Class Involvement: 1 2 3 4 �
Participates Well Sometimes participates Rarely participates
II. AREA: ExTERnALIzIng BEhAVIoRS
Physical Behavior Toward others: 1 2 3 4 �
Physically appropriate Occasionally physically Rarely physically appropriate appropriate
Verbal Behavior: 1 2 3 4 �
Uses appropriate Sometimes uses appropriate Rarely uses appropriate verbal behavior verbal behavior verbal behavior

The California School Psychologist, 2007, Vol. 12 43Behavioral Screening
Physical Behavior Toward Materials or Property: 1 2 3 4 �
Is consistently respectful Is sometimes respectful Is rarely respectful of Materials or Property of Materials or Property of Materials or Property
out of Place: 1 2 3 4 �
Remains in assigned area Sometimes remains Rarely is in in assigned area assigned area
III. AREA: SoCIALIzATIon
Coping with Change: 1 2 3 4 �
Handles change Occasionally handles Rarely handles appropriately change appropriately change appropriately
Adult Interactions: 1 2 3 4 �
Seeks positive Sometimes seeks Rarely seeks relationships positive relationships positive relationships
Peer Interactions: 1 2 3 4 �
Seeks positive Sometimes seeks Rarely seeks relationships positive relationships positive relationships
Scores: Classroom Behaviors Externalizing Behaviors Socialization Total
© Special School District #1, 2007 – Minneapolis Public Schools 9/07
REfEREnCES
Achenbach, T. M. (2002). Achenbach System of Empirically Based Assessment. Retrieved June 13, 2005 from ASEBA website, www.aseba.org/index/html.
Alexander, K. L., Entwisle, D. R., & Dauber, S. L. (1993). First-grade classroom behavior: Its short-and long-term consequences for school performance. Child Development, �4(3), 801-813.
Barbour, C. B. (2006). Engaging RTI: Notes from the field. Presentation at the University of Cincinnati, May 12, 2006.
Batsche, G. M. (2005, October 4). Problem-Solving and Response to Intervention: Maximizing Opportunities for Student Progression. Paper presented at the LaGrange Area Department of Special Education. Retrieved May 30, 2006, from http://www.ladse.org/prof%20dev.htm
Bock, S. J., Tapscott, K. E., & Savner, J. L. (1998). Suspension and expulsion: Effective management for students? Intervention in School and Clinic, 34(1), 50-52.
Bradley, R., Danielson, L., & Hallahan, D. P. (2002). (Eds). Identification of learning disabilities: Research to prac-tice. Mahwah, New Jersey: Lawrence Erlbaum
Busse, R. T. (2005). Rating Scale Applications within the Problem-Solving Model. In R. Brown-Chidsey (Ed.) As-sessment for Intervention: A Problem-Solving Approach (pp. 200-218). New York: Guilford.
Casat, C. D., Norton, & Whitsel (1999). Identification of elementary school children at risk for disruptive behav-ioral disturbance: Validation of a combined screening method. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 1246-1253.
Deno, S. L. (2002). Problem solving as “Best Practice.” In A. Thomas & J. Grimes (Eds.), Best Practices in School Psychology IV (pp.37-55). Bethesda, MD: NASP Publications.

The California School Psychologist, 2007, Vol. 1244
DeRidder, L. M. (1990). The impact of school suspensions and expulsions on dropping out Educational Horizons, �8, 153-157.
DeVoe, J. F., Peter, K., Kaufman, P., Miller, A., Noonan, M., Snyder, T. D., & Baum, K. (2004). Indicators of School Crime and Safety: 2004 (NCES 2005-002/NCJ 205290). U.S. Department of Education and Justice. Wash-ington, DC: U.S. Government Printing Office.
Donovan, M. S., & Cross, C. T. (Eds.). (2002). Minority students in special and gifted education. Washington DC: National Academy Press.
Feil, E. G., Severson, H. H., & Walker, H. M. (2002). Early screening and intervention to prevent the develop-ment of aggressive, destructive behavior patterns among at-risk children. In M. Shinn, H. Walker, & G. Stoner (Eds.), Interventions for Academic and Behavior Problems II: Preventive and Remedial Approaches (pp 143-166. Bethesda, MD: NASP Publications.
Fuchs, D., & Fuchs, L. S. (2006). Introduction to Response to Intervention: What, why, and how valid is it? Reading Research Quarterly 41(1), 93-99.
Gallup Poll News Service (September 17, 2002). Parents concerned about school safety. Available on-line: www.gallup.com
Gallup Poll News Service (October 26, 2004). Americans on local schools: “Show us the money”. Available on-line: www.gallup.com
Gersten, R., & Dimino, J. A. (2006). RTI (Response to Intervention): Rethinking special education for students with reading difficulties (yet again). Reading Research Quarterly 41(1), 99-108.
Ikeda, M. J., Grimes, J., Tilly, W. D., Allison, R., Kurns, S., & Stumme, J. (2002). Implementing an intervention-based approach to service delivery: A case example. In M. Shinn, H. Walker, & G. Stoner (Eds.), Interventions for Academic and Behavior Problems II: Preventive and Remedial Approaches (pp 53-69. Bethesda, MD: NASP Publications.
Kaplan, D. S., Peck, B. M., & Kaplan, H. (1997). Decomposing the academic failure-dropout relationship: A longi-tudinal analysis. Journal of Educational Research, 90(9), 331-343.
Lau, M. Y., Sieler, J. D., Muyskens, P., Canter, A., VanKeuren, B., & Marston, D. (2006). Perspectives on the use of the problem-solving model from the viewpoint of a school psychologist, administrator, and teacher from a large Midwest urban school district. Psychology in the Schools, 43(1), 117-127.
Marston, D., Muyskens, P, Lau, M, & Canter, A. (2003). Problem-solving model for decision making with high-incidence disabilities: The Minneapolis experience. Learning Disabilities Research and Practice, 18(3), 187-200.
Marston, D. (2002). A functional and intervention-based approach to establishing discrepancy for students with learning disabilities. In R. Bradley, D. P. Hallahan, & L. Danielson (Eds.), Identification of learning disabilities: Research to practice. NJ: Lawrence Erlbaum Associates, Inc..
McClelland, M. M., Morrison, F. J., & Holmes, D. (2000). Children at risk for early academic problems: The role of learning-related social skills. Early Childhood Research Quarterly, 15(3), 307-329.
McConoughy, S. H. (1993a). Evaluating behavioral and emotional disorders with the CBLC, TRF, and YSR cross-informant scales. Journal of Emotional and Behavioral Disorders, 1, 40-52.
McConaughy, S. H. (1993b). Advances in empirically based assessment of children’s behavioral and emotional problems. School Psychology Review, 22(2), 285-307.
McEvoy, A., & Welker, R, (2000). Antisocial behavior, academic failure, and school climate: A critical review. Journal of Emotional and Behavioral Disorders, 8, 130-140.
Naglieri, J. (2005). “Current perspectives on behavioral interventions” lacks balance. NASP Communique, 33(�). O’Neil, R., Welsh, M., Parke, R. D., Wang, S., & Strand, C. (1997). A longitude assessment of the academic corre-
lates of early peer acceptance and rejection. Journal of Clinical Child Psychology, 2�, 290-303.O’Shaughnessy, T. E., Lane, K. L., Gresham, F. M., & Beebe-Frankenberger, M. E. (2003). Children placed at-risk
for learning and behavioral difficulties: Implementing a school-wide system of early identification and interven-tion. Remedial and Special Education, 24(1), 27-35.
Rausch, M. K. & Skiba, R. (2004). Unplanned outcomes: Suspensions and expulsions in Indiana. Education Policy Briefs, 2(2). Available On-line: http://ceep.indiana.edu/ChildrenLeftBehind/
Reschly, D. J. (2005). Viewpoint. Child outcomes and school psychology service delivery: Response to Naglieri. NASP Communique, 33(5).
Reschly, D. J., & Tilly, W. D. (1999). Reform trends and system design alternatives. In D. J. Reschly, W. D. Tilly, & J. P. Grimes (Eds). Special Education in Transition: Functional assessment and noncategorial programming. Longmont, CO: Sopris West.

The California School Psychologist, 2007, Vol. 12 45Behavioral Screening
Reschly, D. & Ysseldyke, J. E. (2002). Paradigm shift: The past is not the future. In A. Thomas & J. Grimes (Eds.), Best practices in School psychology IV (pp 3-20). Bethesda, MD: National Association of School Psycholo-gists.
Reynolds, C. R., & Kamphaus, R. W. (2004). Manual: Behavior Assessment System for Children. Circle Pines, MN: American Guidance Service.
Skiba, R. & Peterson, R. (1999). The dark side of zero tolerance: Can punishment lead to safe schools? Phi Delta Kappan, 80(5), 372-382.
Skiba, R., & Rausch, M. K. (2006). School disciplinary systems: Alternatives to suspension and expulsion. In G. Bear & K. Minke (Eds). Children’s Needs III: Understanding and addressing the developmental needs of chil-dren (pp. 87-102). National Association of School Psychologists.
Sugai, G, & Horner, R. H. (2002). Introduction to the special series on Positive Behavior Support in Schools. Journal of Emotional and Behavioral Disorders, 10, 130-135.
Sugai, G., Horner, R. H., Dunlap, G., Hieneman, M., Lewis, T. J., Nelson, C. M., Scott, T., Liaupsin, C., Sailor, W., Turnbull, A. P., Turnbull, H. R. III, Wickham, D., Reuf, M., & Wilcox, B. (2000). Applying positive behavioral support and functional behavioral assessment in the schools. Journal of positive behavioral interventions, 2, 131-143.
U.S. Department of Education, Office of Special Education and Rehabilitative Services (2002). A new era: Revital-izing special education for children and their families. Washington DC, U.S. Department of Education.
Walker, H. M., Horner, R. B., Sugai, G., Bullis, M., Sprague, J.R., Bricker, D., & Kaufman, M. J. (1996). Inte-grated approaches to preventing antisocial behavior patterns among school-age children and youth. Journal of Emotional & Behavioral Disorders, 4(4), 194- 210.
Woodward, L. J., & Fergusson, D. M. (2000). Childhood peer relationship problems and later risks of educational under-achievement and unemployment. Journal of Child Psychology and Psychiatry and Allied Disciplines, 41(2), 191-201.


47
Comprehensive Assessment of Emotional Disturbance: A Cross-Validation Approach
Emily S. Fisher, Katie E. Doyon and
Enrique Saldaña Loyola Marymount University
Megan Redding Allen University of California, Santa Barbara
Assessing a student for emotional disturbance is a serious and complex task given the stigma of the label and the ambiguities of the federal definition. One way that school psychologists can be more confident in their assessment results is to cross validate data from different sources using the RIOT approach (Review, Interview, Observe, Test). Because each data collection process has advantages and limitations, using all four processes together allows for comprehensive assessment for emotional disturbance. Additionally, school psychologists should strongly consider a student’s strengths, cultural factors, and the interaction between the student and the environment in order to interpret assessment findings. This approach serves to tailor interventions regardless of diagnosis.
Assessing a student for emotional disturbance (ED) is a complex task both because of the ambigui-ties of the diagnosis in the educational code and because of the seriousness of assigning this classification to a student. While it is tempting to want to use standardized assessments to make a definitive diagnosis of ED, other forms of data collection are equally important as they allow for the cross-validation of infor-mation from various sources. Leung (1993) first wrote about a method of comprehensive assessment using the acronym of RIOT (Review, Interview, Observe, Test). Leung acknowledged that each tech-nique has flaws and advocated using information from all four data sources to support conclusions about diagnoses. By incorporating information from the cumulative folder, interviews with parents, teachers, and the student, and observations in the classroom and alternative settings along with data from instru-ments and tests, school psychologists can better justify their conclusions and present information in a truly comprehensive manner that allows parents and school personnel to have confidence in the results.
At the beginning of an ED assessment, most often, school personnel have already identified social, emotional, and/or behavioral problems as a primary concern and the reason for referral is to determine the extent to which such problems are contributing to the student’s overall school functioning. While the school psychologist will collect copious amounts of data about the student’s functioning over the course of the assessment, it is imperative that the school psychologist also consider the ecological context in which the student’s behaviors occur (Wright, Gurman, & The California Association of School Psychol-ogists/Diagnostic Center, Southern California Positive Intervention Task Force, 2001). This allows the school psychologist to understand the reciprocal relationship between the student and the environment (Landau & Swerdlik, 2005) and to examine whether adequate interventions were implemented during the pre-referral process. Additionally, by conceptualizing the problems from an ecological perspective, school psychologists are better prepared to make recommendations for interventions at the conclusion of the assessment, regardless of the ultimate diagnosis.
Please send correspondence to Emily S. Fisher, PhD, School of Education, University Hall, Suite 1500, Loyola Mary-mount University, 1 LMU Drive, Los Angeles, California, 90045. Email: [email protected]
The California School Psychologist, Vol. 12, pp. 47 – 58, 2007Copyright 2007 California Association of School Psychologists

The California School Psychologist, 2007, Vol. 1248
REVIEW of RECoRDS
There is virtually no recent research literature on reviewing cumulative records; however, the diag-nosis of emotional and behavioral problems should begin with an understanding of the student’s prior school experience. A review of records provides the school psychologist guidance about what infor-mation needs to be gathered from other assessment procedures and about interventions that have been attempted to help the student be more successful in school. For example, if the school psychologist finds major changes in school functioning of a 10th grade student occurred during 7th grade, he or she will want to elicit perspectives on these changes during the parent and student interviews. Additionally, it would be helpful for the school psychologist to speak with the student’s 7th grade teacher for more information and to find out what interventions, if any, were implemented during that year. Similarly, a review of records can inform the school psychologist about questions to ask during interviews, when and where to observe the student, and which tests and instruments might be most appropriate.
In the case of an ED assessment, a record review is crucial to determine if the student has had emotional, social, and/or behavioral problems “over a long period of time” as required by the federal definition of emotional disturbance (Friend, 2008, p. 203). Because interviews rely on retrospective reports of the onset of problems, the student’s cumulative records provide a less biased report of the student’s prior functioning in school. Report card comments can often provide some evidence of social/emotional functioning over time.
In addition to onset, there is other key information to attend to in the cumulative record, and it is as important to note a lack of findings (i.e., lack of evidence of ED) as it is to note significant findings (i.e., evidence of ED). In addition to examining grades and test scores, school psychologists should look for any early warning signs of emotional problems such as difficult transitions to school and between schools, teacher comments on social skills, discipline records, frequent visits to the nurse’s office, coun-seling referrals, and abnormalities in attendance (e.g., excessive absences or tardiness). It is also impor-tant to note non-normative transitions such as changing schools mid-year. A review of records should also document attempts at intervention and the outcomes of such interventions. Most often, there will have been some type of pre-referral team meeting to discuss the student and develop a plan for action, including interventions. Rather than just documenting the interventions from the pre-referral meeting papers, the school psychologist should investigate whether the interventions were actually implemented with integrity and what worked as well as what did not. The school psychologist might consider exam-ining interventions from a Response-to-Intervention approach, which provides the student with increas-ingly intensive interventions (Fairbanks, Sugai, Guardino, & Lathrop, 2007). A diagnosis of ED should not be considered if appropriate interventions have not been tried.
Leung (1993) highlighted the limitations of information gathered through a review of a student’s records, including “dated materials, incomplete records, [and] skewed opinions” (p. 6). When making inferences about what information records reveal, the school psychologist should cross-validate this information with other assessment procedures before drawing conclusions. So, if it is noted that the student has frequent absences, tardiness, and trips to the nurse’s office, the school psychologist might form the hypothesis that the student may be experiencing significant anxiety or fear about school. In this case, interviews and standardized measures could be used to test if this is a correct hypothesis.

The California School Psychologist, 2007, Vol. 12 49
InTERVIEWS
Interviewing is a commonly used and important tool in the assessment of students for ED. An inter-view can be defined as an interpersonal encounter to obtain information about a person’s symptoms and behaviors, while providing the opportunity for observation of verbal and nonverbal behaviors (Aklin & Turner, 2006). During a comprehensive assessment, interviews should be conducted with the student, his or her parents, and the school staff working directly with the student. Collecting information from these varied perspectives through the interviewing process is important in making eligibility decisions.
The two types of interviews generally used in an assessment are unstructured or open interviews and semi-structured or structured interviews. In an unstructured interview, the school psychologist deter-mines what questions will be asked. School psychologists can collect information on both strengths and challenges the student is having, and tailor questions based on interviewee responses. While this type of interview allows the assessment to fit the individual needs of the interviewee, there are problems with variance and they tend to be unreliable, reflecting more the psychologist’s perception than a reliable and accurate picture of the student’s functioning (Aklin & Turner; 2006; Kamphaus & Frick, 2005).
Semi-structured and structured interviews consist of a set of questions that are asked to the student, parent, or teacher. A stem question is generally provided and then if it is answered affirmatively, follow-up questions are asked based on the response. Structured interviews are more rigid in terms of the questions asked and provide explicit scoring criteria, while semi-structured interviews generally provide sets of questions allowing for some flexibility to ask follow-up questions. Both show better reliability and validity than unstructured interviews, and these types of interviews have been found to increase the accuracy of diagnosis for individuals of diverse backgrounds because they rely more on standardized criteria rather than interpretation (Aklin & Turner, 2006; Kamphaus & Frick, 2005). One example of a semi-structured interview that may be appropriate for use for an ED assessment is the Child Assessment Schedule (CAS; Hodges, Kline, Stern, Cytryn, & McKnew, 1982), which has been shown to have good reliability and validity (Hodges, Cools, & McKnew, 1989; Hodges & Saunders, 1989).
Structured and semi-structured interviews have some limitations that the school psychologist should consider. First, interviews can last for 60-90 minutes, generally longer than an open interview. Addi-tionally, there is some evidence that the student’s self report on diagnostic interviews is unreliable for students younger than 9 years (Hodges & Zeman, 1993).
By using interviews, especially a semi-structured interview supplemented with other important questions, the school psychologist can better understand the parameters of a student’s emotions and behaviors that are not generally assessed by a behavior rating scale or classroom observations. For example, information can be obtained about the duration of the student’s behavioral difficulties, the age at which the problems began to emerge, the level of impairment that is associated with the symptoms, and when symptoms occur (Merrell, 2003). An interview can assess additional psychosocial stressors that may contribute to a student’s emotional difficulties, allowing the symptoms to be understood within the context. Interviewing also allows the school psychologist to establish rapport, trust, and security with the student, family, and teacher, which may be crucial to the eventual implementation of an inter-vention plan.
oBSERVATIonS
Observing a student is “one of the most direct and objective” (Merrell, 2003, p. 51) ways for the school psychologist to see a student’s interactions and behaviors in various naturalistic settings (e.g.,
Comprehensive Assessment of Emotional Disturbance
The California School Psychologist, 2007, Vol. 1250
classroom and playground) across time. There are definite limitations to observations, such as observer bias and observer influence on a student’s behavior (Leung, 1993) and the time commitment that observa-tions require is great, but observations can provide valuable information about a student’s current perfor-mance. Observations also allow the school psychologist to better understand the interaction between the student and the environment, which helps determine the antecedents, consequences, and functions of behaviors and to plan interventions. The school psychologist might want to conduct observations before conducting the student interview or formal testing. This not only reduces the likelihood that the student’s behavior will be influenced by the presence of the observer, but also allows the school psychologist to form hypotheses about the student that should guide the choice of testing instruments.
When conducting an ED assessment, it is important for the school psychologist to conduct both unstructured and structured observations of a student. Unstructured observations typically take the form of a running log of a student’s behaviors during the observation period. The school psychologist might note such things as type of response to teacher directions, on-task behavior, responding to or ignoring other students, level of participation, and response to redirection or discipline. This type of observation should inform the school psychologist about what behaviors are problematic, what type of structured observation should be used to collect data, what type of assessment battery is appropriate, and what types of interventions should be tried.
Structured observations typically take the form of collecting and coding data on certain observ-able behaviors during a defined period of time. Volpe, DiPerna, Hintze, and Shapiro (2005) provide a comprehensive review of structured observation coding systems, including characteristics, psychometric properties, strengths, limitations, and recommendations for each system. Based on this review, the Direct Observation Form (DOF; Achenbach & Rescorla, 2001) is supported for observing both external-izing and internalizing problems across group settings. This system “requires that the observer write a narrative and observe on- and off-task behavior simultaneously” (Volpe et al., 2005, p. 467) and then rate the student’s behavior on items that generally correspond to the Child Behavior Checklist (Achen-bach & Rescorla, 2001). The DOF also allows for social comparison data to be collected, which helps to determine if the student’s behavior is significantly different from the behaviors of peers in the same settings (Merrell, 2003).
It is important for the school psychologist to observe the student in different settings at different times. Based on the cumulative record review and the teacher interview, the school psychologist should identify a classroom time when the student is experiencing more difficulties and a classroom time when the student is experiencing fewer difficulties. This allows the school psychologist to examine the recip-rocal relationship between the student and the classroom environment (Landau & Swerdlik, 2005). The information obtained from these observations can help the school psychologist make recommendations to support a student’s success in the classroom. Additionally, observing a student in a non-academic setting, such as recess or lunch, will provide information on the student’s behavior (e.g., peer interac-tions) in an unstructured setting.
Because observations are time consuming, school psychologists should consider how to make observations serve multiple purposes. One way to do this is to use the structure of a functional behavior assessment (FBA) to interpret qualitative and quantitative observation data collected. FBA requires collecting information on when and where behaviors occur most often, what is happening before the behavior occurs, and what is reinforcing the behavior (Watson & Steege, 2003). By collecting these data, the school psychologist can develop hypotheses about the function of the behavior and environ-mental factors that need to be changed (Wright et al., 2001). If significant external factors are present,

The California School Psychologist, 2007, Vol. 12 �1
then environmental changes should be considered rather than a diagnosis of ED.In addition to observing in the classroom and other school settings, school psychologists should
attend to observational data collected through testing sessions. Because testing sessions are structured and tests are administered in a standardized manner, this environment allows the school psychologist to compare observations of a student to other students with whom the school psychologist has tested, as well as how the student reacts to factors unique to the testing environment, such as one-to-one interactions and few distractions (McConaughy, 2005). If school psychologists want to quantify observational data during testing, the Test Observation Form (McConaughy, 2005) provides a norm-referenced observation system. This system requires that the school psychologist keep a running log of a student’s behavior during testing and then rate the behavior on items that generally correspond to other rating forms in the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2001).
TESTS
“Testing,” in the RIOT model, is loosely defined as the collection of data through various instru-ments, including cognitive assessments, self-report measures of behavior, behavior rating scales, and projective assessments. Most of these provide school psychologists with information about a student’s strengths and challenges as compared to other students of the same age. When using standardized instru-ments, it is important to consider potential sources of bias in administration, scoring, and interpreting test results (Sattler, 2001). For example, Skiba, Knesting and Bush, (2002) found Caucasian teachers, compared to teachers of color, gave Mexican-American and African-American students disproportion-ately higher ratings for problem behaviors on behavior rating scales. Although these ratings do not necessarily indicate bias inherent to the test, they do suggest that behavior rating scales are not immune to informant bias (Skiba et. al., 2002).
Cognitive Assessment
Over 60% of school psychologists use intelligence tests as part of most ED assessments (Shapiro & Heick, 2004). At a very basic level, cognitive assessment allows the school psychologist to determine the extent to which students may be experiencing intellectual or sensory difficulties that impact their ability to learn. In more traditional districts that routinely use cognitive assessments, they may help rule out learning disabilities and mental retardation (Teeter & Korducki, 1998). However, in districts that employ a Response-to-Intervention model, cognitive assessments are not a necessary part of the ED assessment as intervention data, observations, and work samples can provide this information. If cognitive assessments are used, the school psychologist can examine data on cognitive strengths and weaknesses to better understand the interaction of the individual characteristics of the student with the classroom environment (Wright et al., 2001). For example, if a student has average cognitive abilities but slower processing speed, the student might be having inappropriate behaviors in the classroom due to frustration with timed tasks such as tests or embarrassment about being called on before having time to process the question. Thus, adequate academic and behavioral interventions would need to be employed before considering the student for a diagnosis of ED.
Issues of bias in intelligence tests pervade the literature, and perhaps the most significant source of bias concerns the use of these assessments with ethnic minority students. This may be especially true for African American students, who, on average, score one standard deviation below Caucasian students on standardized cognitive measures (Chung-yan & Cronshaw, 2002; Kwate, 2001). Given the overrepre-sentation of minority students labeled as ED, school psychologists should strongly consider using other
Comprehensive Assessment of Emotional Disturbance

The California School Psychologist, 2007, Vol. 1252
sources of data to determine eligibility.
Behavior Rating Scales
Behavior rating scales are the most commonly used assessment modality of childhood psychopa-thology (Achenbach & McConaughy, 1987) due to their many advantages. Rating scales are easy to administer and score, cost-efficient, based on normative data, and organized by grouping problems into larger scales (McConaughy & Ritter, 2002). They also provide information on a large range of problems and allow for systematic comparison across informants (McConaughy & Ritter, 2002).
For an ED assessment, behavior rating scales are typically completed by teachers, parents, and other adults who know the student well (e.g., administrator or day-care provider). Parent reports are especially important as they can provide information about the severity, duration, and frequency of behaviors (Kovacs, 1986). Similarly, teacher reports are beneficial, especially in elementary school, where teachers spend a large part of the day with the student and are able to observe the student over the course of the day (Epkins, 1995).
Two broad social-emotional rating scales that are commonly used are the Behavior Assessment System for Children – Second Edition (BASC-2; Reynolds & Kamphaus, 2004), which has a parent rating form and a teacher rating form, and the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2001), which contains the Child Behavior Checklist (CBCL; to be completed by parents) and the Teacher Report Form (TRF; to be completed by teachers). Both systems have good reliability and validity, and are based on large normative samples of students from back-grounds representative of the population of the United States. Both systems are appropriate for use in an ED assessment, as they provide information in internalizing and externalizing domains. Once the school psychologist determines the areas of most concern based on these broad-based systems, he or she can conduct more targeted assessment of specific problem areas. For example, if both parents and teachers rate the student high for anxiety, the school psychologist may want to explore specific symptoms of anxiety with the student through interviews, self-report measures, or a more narrow-band rating scale, such as the Multidimensional Anxiety Scale for Children (MASC; March, Parker, Sullivan, Stallings, & Conners, 1997).
Despite their many advantages, behavior rating scales have limitations that should be considered by the school psychologist. There may be gender differences in how teachers and parents rate a student’s temperament (Else-Quest, Hyde, Goldsmith, & Van Hulle, 2006). For example, what is considered “cries easily” for boys might be different than for girls. Also, as previously mentioned, characteristics of the rater can impact ratings (Skiba et al., 2002). Additionally, while parents have been found to be good at reporting overt behaviors such as conduct problems (Dollinger, 1992), they tend to underreport depressive symptoms (Angold et al., 1987; Jensen, Rubio-Stipec, & Canino, 1999). Therefore, the school psychologist should use other sources of data, such as observations and interviews, to ensure that their conclusions about a student’s functioning are supported.
Self-Report Measures
Self-report measures share similar advantages with behavior rating scales, and are especially impor-tant in assessing feelings and behaviors that are difficult to observe directly. The two systems previously discussed, the BASC-2 and ASEBA have self-report forms. Reliability of self-reports increases with age (Edelbrock, Costello, Dulcan, Kalas, & Conover, 1985). Consequently, it is important to put more weight on parent and teacher reports for younger students.

The California School Psychologist, 2007, Vol. 12 53
Merrell (2003) identified a number of different response biases that can affect the results of self-report measures. The first, acquiescence, refers to the tendency among children to answer dichotomous questions (those requiring a true/false or yes/no response) consistently in one direction. This can be particularly problematic when test items are unclear. The second, social desirability, refers to either a conscious or unconscious tendency to respond to test items in a manner that makes the student appear favorable to others. The third, faking, refers to deliberate actions taken by the student to create either favorable or negative impressions of him or herself. Because of the errors that occur through response bias, it is important that the school psychologist cross-validate findings with other sources of informa-tion.
Projective Tests
Projective tests, such as sentence completion tasks, storytelling techniques, and drawings, are thought to access information about a student’s internal experience through the use of ambiguous stimuli. In a recent study by Hojnoski, Morrison, Brown, and Matthews (2006), over half of the school psycholo-gists surveyed indicated using projective tests in their practice, including using them to make eligibility decisions. However, since their inception, projective tests have been plagued by controversy, generally due to their lack of adequate reliability and validity (Miller & Nickerson, 2006). Because of the major concerns with the psychometric properties of projective techniques with students, their use in deter-mining ED eligibility is not recommended (Miller & Nickerson, 2006; Smith & Dumont, 1995). Instead, school psychologists should consider using the tests as a way to build rapport and generate hypotheses rather than using them to draw conclusions about a student’s social and emotional functioning (Garb, Wood, Lillienfeld, & Nezworksi, 2002; Miller & Nickerson, 2006).
Sentence completion tasks are the most commonly used projective technique by school psychologists (Hojnoski et al., 2006). They come in a variety of forms that focus on different areas of psychological functioning and have different purposes (Rabin & Zltogorski, 1981) and are generally quick to admin-ister. The open-ended nature of the tests may facilitate students’ ability to express their attitudes and feelings because they allow for a wide variety of responses (Holaday, Smith, & Sherry, 2000). Rogers, Bishop, and Lane (2003) suggest that sentence completion tasks can be used as a quick screening of feelings toward self and others. However, sentence completion tests are often administered in a nonsys-tematic way, are not formally scored, and are rarely individualized based on the presenting problem (Holaday et al., 2000). If school psychologists are going to use them, they should consider administering more specific sentence completion tests, such as the Sentence Completion Test for Depression, for which there is evidence of reliability and validity in assessing depressive thinking (Barton, Morley, Bloxham, Kitson, & Platts, 2005).
Over a quarter of school psychologists who responded to the survey reported using drawing tech-niques in their practice (Hojnoski et al., 2006). Drawing tasks, such as the Draw-A-Person: Screening Procedure for Emotional Disturbance (DAP:SPED; Naglieri, McNeish, & Bardos, 1991), are quick and require little verbal skills, which can help in working with younger students or students with lower verbal abilities (Matto, 2002). The DAP:SPED, which is normed on a large standardization sample, has been found to be able to distinguish students with emotional disturbances from typically developing peers (Matto, Naglieri, & Clausen, 2005) and has been found to be appropriate for use with African-American, Hispanic, and Caucasian students (Matto & Naglieri, 2005). While the DAP:SPED has been shown to be an adequate assessment of internalizing behaviors, it is not as useful for assessing externalizing behav-iors (Matto, 2002). In order to assess externalizing behaviors, observations, behavior rating scales, and
Comprehensive Assessment of Emotional Disturbance

The California School Psychologist, 2007, Vol. 1254
interviews provide more useful data.Storytelling techniques, such as the Roberts-Second Edition (Roberts-2; Roberts & Gruber, 2005)
and the Thematic Apperception Technique (TAT; Murray, 1943) are reported to be used by 16-30% of school psychologists (Hojnoski et al., 2006) and are thought to be non-threatening and fun for children (Kamphaus & Frick, 2005). In general, storytelling techniques can inform the school psychologist about how the student constructs his or her world, the quality of interactions between the student and others, and how the student resolves conflicts. While the TAT is generally interpreted by examining recurrent themes, the Roberts-2 has explicit scoring procedures, resulting in adequate reliability. It should be noted that the developers of the Roberts-2 describe this instrument as a means to assess social cognitive understanding (Roberts & Gruber, 2005). Limitations of storytelling techniques include their heavy reliance on the student’s verbal abilities and questionable reliability and validity resulting from incon-sistent administration, scoring, and interpretation (Kamphaus & Frick, 2005). Like all projective tests, storytelling techniques should not be used as a sole means of determining eligibility and might be better used to build rapport with students.
ConSIDERIng STREngThS
Historically, psychoeducational assessments focus on a student’s deficits (Epstein, 1999), and this seems to be particularly true in the case of ED assessment. It is as if the assessor has to point out that the student is failing in all areas to make the case for ED, but this is unnecessary. The federal definition requires that a student only meet one of the criteria to be considered ED, although a student often meets several criteria. In addition, it is to the benefit of everyone, especially the student and family, to not only include but to highlight a student’s strengths because this provides hope to everyone and aids in the development of interventions (Epstein & Sharma, 1998).
Information about a student’s strengths should be gleaned from all of the aforementioned data-collection processes. From the cumulative record review, the school psychologist might highlight posi-tive comments from teachers and growth in an academic area (e.g., high math ability). During obser-vations, the school psychologist might note a student’s positive attributes such as an ability to persist during a difficult task, offers to help other students, attention to the teacher, or sense of humor. During interviews with the teacher, parents, and student, the school psychologist should ask more than one question about a student’s strengths or interests, and should follow up with other questions to more fully understand the student’s positive attributes. These strengths and interests should inform interventions to ensure success.
There has been a movement to develop strength-based assessments, and research indicates that these are an important component of a comprehensive ED assessment (Reid, Epstein, Pastor, & Ryser, 2000). Specifically, the Behavior and Emotional Rating Scale-Second Edition (BERS-2), which has teacher, parent, and youth rating scales, can be used to quantify a student’s strengths as an overall score (strength index) and in the following domains: interpersonal strength, family involvement, intrapersonal strength, school functioning, affective strength, and career and vocational strengths (Epstein, Mooney, Ryser, & Pierce, 2004). Reid et al. (2000) found that the Behavior and Emotional Rating Scale could discriminate between typical students and those with emotional and behavioral disorders (EBD), with typical students scoring significantly higher in all domains. In addition to the BERS-2, which solely assesses a student’s strengths, the BASC-2 has Adaptive Scales, which measure strengths in addition to the Clinical Scales that measure problem behaviors (Reynolds & Kamphaus, 2004).

The California School Psychologist, 2007, Vol. 12 ��
CuLTuRAL ConSIDERATIonS
Emotions, and thus behaviors and social interactions, vary across cultures, and as such, emotional responses should be evaluated based on the student’s cultural norms (Mesquita and Walker, 2003). School psychologists must balance understanding cultural norms with understanding the degree of influence these norms might have on an individual student. When conducting culturally competent assessment for ED, it is important to consider assessment data with awareness of the societal and historical forces that continue to affect minority students (Skiba et al., 2002). Additionally, because measuring emotions is rather subjective, their assessment is more influenced by cultural differences (Spielberger, 2006).
Given the growing diversity of the United States (as of the year 2000, about one third of the popula-tion was of non-European background; Chen, Downing and Peckham-Hardin, 2002), school psycholo-gists must understand the complexities of conducting culturally competent assessment of ED, especially since there are a disproportionate number of minority students diagnosed as such (U.S. Department of Education, 2003). Engaging in culturally competent assessment does not mean that culture should account for everything, nor should the school psychologist discount its impact altogether (Cartledge, Kea and Simmons-Reed, 2002); rather, culturally competent assessment involves an overall commit-ment to data collection procedures that do not contribute to the over-identification of minority students for special education (Skiba et al., 2002). Culturally competent assessment is much broader than simply examining test bias (Harry & Klingner, 2006; Skiba et al., 2002; Skiba et al., 2006), and at the core of the issue is ensuring that cultural factors and/or lack of educational opportunity are not contributing significantly to the student’s school difficulties. Because overrepresentation is a multi-faceted issue, which includes considering physical facilities, curriculum, expectations, and motivation, to name a few (Skiba et al., 2002), school psychologists need to be well-informed about national and local initiatives to examine overrepresentation. While an in-depth analysis of this topic is beyond the scope of this article, readers are referred to the following sources: “Cultural and Linguistic Competency and Disproportionate Representation” (Osher et al., 2004) and Why are so Many Minority Students in Special Education?: Understanding Race & Disability in Schools (Harry & Klingner, 2006).
ConCLuSIon
While ED assessments are complex, and the methods used to gather data have significant limita-tions, school psychologists can gain confidence in the conclusions they draw if they do not over-rely on any one assessment approach and consistently cross-validate their findings using the RIOT model. In addition to collecting data through the assessment methods described in this article, it is critical that the school psychologist have an appreciation of the student’s strengths and an awareness of the complexity of culturally competent assessment to reduce overrepresentation of minority students classified as ED. By approaching the data collection from an ecological perspective, the school psychologist can present a more complete picture of the student within the school environment and make appropriate recommen-dations for interventions that focus on the environmental contributions to and functions of the student’s behavioral and emotional responses.
The school psychologist should use data gathered from the assessment to make recommendations for interventions and supports to help the student be more successful in school regardless of whether the student qualifies for special education services as ED. Recommendations should go far beyond simply suggesting an appropriate placement. From conducting observations, the school psychologist should be able to make recommendations about environmental and instructional strategies to help the student
Comprehensive Assessment of Emotional Disturbance

The California School Psychologist, 2007, Vol. 125�
experience greater success, as well as suggest ways to support the student’s behavior. From interviews and strength-based approaches, the school psychologist is in a position to recommend strategies to capi-talize on things the student enjoys and build on the student’s strengths. The school psychologist should also recommend ways to help remediate areas of weakness and to build greater academic and social competence.
REfEREnCES
Achenbach, T. M. & McConaughy, S. H. (1987). Empirically based assessment of child and adolescent psychopa-thology: Practical implications. Newbury Park, CA: Sage.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
Aklin, W. M., & Turner, S. M. (2006). Toward understanding ethical and cultural factors in the interviewing process. Psychotherapy: Theory, Research, Practice, and Training, 43, 50-64.
Angold, A., Weissman, M. M., John, K., Merikangas, K. R., Prusoff, B. A. Wickramaratne, P., Gammon, G. D., & Warner, V. (1987). Parent and child reports of depressive symptoms in children at low and high risk of depres-sion. Journal of Child Psychology and Psychiatry, 28, 901–915.
Barton, S., Morley, S., Bloxham, G., Kitson, C., & Platts, S. (2005). Sentence Completion Test for Depression (SCD): An idiographic measure of depressive thinking. British Journal of Clinical Psychology, 44, 29-46.
Cartledge, G., Kea, C., & Simmons-Reed, E. (2002). Serving culturally diverse children with serious emotional disturbance and their families. Journal of Child and Family Studies, 11, 113-126.
Chen, D., Downing J. E., Peckham-Hardin, K.D. (2002). Working with families of diverse cultural and linguistic backgrounds. In J. M. Lucyshyn, R. H. Horner, & G. Dunlap (Eds.), Families and positive behavior support: Addressing problem behavior in family contexts (pp. 133-151). Baltimore, MD: Paul H. Brookes Publishing Co.
Chung-yan, G. A. & Cronshaw, S. F. (2002). A critical re-examination and analysis of cognitive abilities using the Thorndike model of fairness. Journal of Occupational and Organizational Psychology, 75(4), 489-509.
Dollinger, S. J. (1992). Idiographic and nomothetic child assessment: Convergence between the California Child Q-Sort and the Personality Inventory for Children. Personality and Individual Differences, 13, 585–590.
Edelbrock, C, Costello, A. J., Dulcan, M. K., Kalas, R., & Conover, N. C. (1985). Age differences in the reliability of the psychiatric interview of the child. Child Development, 5�, 265-275.
Else-Quest, N. M., Hyde, J. S., Goldsmith, H. H., & Van Hulle, C. A. (2006). Gender differences in temperament: A meta-analysis. Psychological Bulletin, 132, 33-72.
Epkins, C. C. (1995). Teachers’ ratings of inpatient children’s depression, anxiety, and aggression: A preliminary comparison between inpatient-facility and community-based teachers’ ratings and their correspondence with children’s self-report. Journal of Clinical Child Psychology, 24, 63–70.
Epstein, M. H. (1999). The development and validation of a scale to assess the emotional and behavioral strengths of children and adolescents. Remedial and Special Education, 20, 258-262.
Epstein, M. H., Mooney, P., Ryser, G., & Pierce, C. D. (2004). Validity and reliability of the Behavior and Emotional Rating Scale (2nd Edition): Youth Rating Scale. Research on Social Work Practice, 14, 358-367.
Epstein, M. H., & Sharma, H. M. (1998). Behavioral and Emotional Rating Scale: A strength based approach to assessment. Austin, TX: PRO-ED.
Fairbanks, S., Sugai, G., Guardino, D., & Lathrop, M. (2007). Response to intervention: Examining classroom behavior support in second grade. Exceptional Children, 73, 288-310.
Friend, M. (2008). Special education: contemporary perspectives for school professionals. Boston: Pearson.Garb, H. N., Wood, J. M., Lilienfeld, S. O. Nezworski, M. T. (2002). Effective use of projective techniques in
clinical practice: Let the data help with selection and interpretation. Professional Psychology: Research and Practice, 33(5) pp. 454-463.
Harry, B., & Klingner, J. (2006). Why are so many minority students in special education?: Understanding race & disability in schools. New York: Teachers College Press.
Hodges, K., Cools, J., & McKnew (1989). Test-retest reliability of a clinical research interview for children: The Child Assessment Schedule. Psychological Assessment, 1, 317-322.
Hodges, K., Kline, J., Stern, L., Cytryn, L., & McKnew, D. (1982). The development of a child assessment interview for research and clinical use. Journal of Abnormal Child Psychology, 10, 173-189.
Hodges, K., & Saunders, W. (1989). Internal consistency of a diagnostic interview for children: The Child Assess-ment Schedule. Journal of Abnormal Child Psychology, 17, 691-701.

The California School Psychologist, 2007, Vol. 12 57
Hodges, K., & Zeman, J. (1993). Interviewing. In T. H. Ollendick & M. Hersen (Eds.), Handbook of child and adolescent assessment (pp. 65-81). Needham Heights, MA: Allyn & Bacon.
Hojnoski, R. L., Morrison, R., Brown, M., & Matthews, W. J. (2006). Projective test use among school psycholo-gists: A survey and critique. Journal of Psychoeducational Assessment, 24, 145-159.
Holaday, M., Smith, D. A., & Sherry, A. (2000). Sentence Completion Tests: A review of the literature and results of a survey of members of the Society of Personality Assessment. Journal of Personality Assessment, 74, 371–383.
Jensen, P. S., Rubio-Stipec, M., & Canino, G. (1999). Parent and child contributions to diagnosis of mental disorder: Are both informants always necessary? Journal of the American Academy of Child & Adolescent Psychiatry, 38, 1569-1579.
Kamphaus, R. W., & Frick, P. J. (2005). Clinical assessment of child and adolescent personality and behavior (2nd ed.). New York: Springer Science & Business Media, Inc.
Kovacs, M. (1986). A developmental perspective on the methods and measures in the assessment of depressive disorders: The clinical interview. In M. Rutter, C. E. Izard, & P. B. Read (Eds.), Depression in young people: Developmental and clinical perspective (pp. 435-465). New York: Guilford.
Kwate, N. O. A. (2001). Intelligence of misorientation? Eurocentrisim in the WISC-III. Journal of Black Psychology, 27, 221-236.
Landau, S., & Swerdlik (2005). What you see is what you get: A Commentary on school-based direct observation systems. School Psychology Review, 34, 529-536.
Leung, B. P. (1993, November). Back to basics: Assessment is a R.I.O.T.! National Association of School Psycholo-gists Communiqué, 22, 1-6.
March, J. S., Parker, J. D. A., Sullivan, K., Stallings, P., & Conners, C. K. (1997). The Multidimensional Anxiety Scale for Children (MASC): Factor structure, reliability, and validity. Journal of American Academy of Child and Adolescent Psychiatry, 3�, 554-565.
Matto, H. C. (2002). Investigating the validity of the Draw-A-Person: Screening procedure for emotional distur-bance: A measurement validation study with high risk youth. Psychological Assessment, 14, 221-225.
Matto, H. C., & Naglieri, J. A. (2005). Validity of the Draw-A-Person: Screening Procedures for Emotional Distur-bance (DAP:SPED) in strengths-based assessment. Research on Social Work Practice, 15, 41-46.
Matto, H. C., Naglieri, J. A., & Clausen, C. (2005). Validity of the Draw-A-Person: Screening procedure for emotional disturbance (DAP:SPED) in strengths-based assessment. Research on Social Work Practice, 15, 41-46.
McConaughy, S. H. (2005). Direct observational assessment during test sessions and child clinical interviews. School Psychology Review, 34, 490-506.
McConaughy, S. H., & Ritter, D. (2002). Best practices in multidimensional assessment of emotional or behavioral disorders. In A. Thomas & J. Grimes (Eds.), Best practices in school psychology (4th ed., pp. 1303–1336). Bethesda, MD: National Association of School Psychologists.
Merrell, K. W. (2003). Behavioral, social, and emotional assessment of children and adolescents (2nd ed.) Mahwah, NJ: Lawrence Erlbaum Associates.
Mesquita, B., & Walker, R. (2003). Cultural differences in emotions: A context for interpreting emotional experi-ences. Behaviour Research and Therapy, 41, 777-793.
Miller, D. N., & Nickerson A. B. (2006). Projective assessment and school psychology: Contemporary validity issues and implications for practice. The California School Psychologist, 11, 73-84.
Murray, H. A. (1943). Thematic Apperception Test. Cambridge, MA: Harvard University Press.Naglieri, J. A., McNeish, T. J., & Bardos, A. N. (1991). Draw-A-Person: Screening procedure for emotional distur-
bance. Austin, TX: ProEd.Osher, D., Cartledge, G., Oswald, D., Sutherland, K. S., Artiles, A. J., & Coutinho, M. (2004). Cultural and linguistic
competency and disproportionate representation. In R. B. Rutherford, M. M. Quinn, & S. R. Mathur (Eds.), Handbook of research in emotional and behavioral disorders (pp. 54-77). New York: Guilford Press.
Rabin, A. I. & Zltogorski, Z. (1981). Completion methods: Word association, sentence, and story completion. In A. I. Rabin (Ed.), Assessment with projective techniques: A concise introduction (pp. 126-149). New York: Springer.
Reid, R., Epstein, M. H., Pastor, D. A., & Ryser, G. R. (2000). Strengths-based assessment differences across students with LD and EBD. Remedial and Special Education, 21, 346-355.
Reynolds, C.R., & Kamphaus, R.W. (2004). Behavior Assessment System for Children, Second Edition (BASC-2). Circle Pines, MN: AGS.
Roberts, G. E, & Gruber, C. (2005). Roberts-2. Los Angeles, CA: Western Psychological Services.Rogers, K., Bishop, J., & Lane, R. (2003). Considerations for the use of Sentence Completion Tests. Journal of
Contemporary Psychotherapy, 33, 235-242.
Comprehensive Assessment of Emotional Disturbance

The California School Psychologist, 2007, Vol. 1258
Sattler, J. M. (2001). Assessment of children: Cognitive applications (4th ed.). San Diego, CA: Jerome M. Sattler, Publisher.
Shapiro, E. S., & Heick, P. F. (2004). School psychologist assessment practices in the evaluation of students referred for social/behavioral/emotional problems. Psychology in the Schools, 41, 551-561.
Skiba, R., Knesting, K., & Bush, L. (2002). Culturally competent assessment: More than nonbiased tests. Journal of Child and Family Studies, 11, 61-78.
Skiba, R., Simmons, A., Ritter, S., Kohler, K., Henderson, M., & Wu, T. (2006). The context of minority dispropor-tionality: Practitioner perspectives on special education referral. Teacher College Record, 108, 1424-1459.
Smith, D. & Dumont, F. (1995). A cautionary study: Unwarranted interpretations of the Draw-A-Person Test. Profes-sional Psychology: Research and Practice, 2�, 298-303
Spielberger, C. D. (2006). Cross-cultural assessment of emotional states and personality traits. European Psycholo-gist, 11, 297-303.
Teeter, P. A., & Korducki, R. (1998). Assessment of emotionally disturbed children with the WISC-III. In A. Prifitera & D. H. Saklofske (Eds.), WISC-III clinical use and interpretation: Scientist-practitioner perspectives (pp. 119-138). San Diego, CA: Academic Press.
U.S. Department of Education (2003). Twenty-fifth annual report to Congress on the implementation of Individuals with Disabilities Education Act. Washington, DC: Author.
Volpe, R. J., DiPerna, J. C., Hintze, J. M., & Shapiro, E. S. (2005). Observing students in classroom settings: A review of seven coding schemes. School Psychology Review, 34, 454-474.
Watson, T. S. & Steege M. W. (2003). Conducting school-based functional behavioral assessments: A practitioner’s guide. New York: The Guilford Press
Wright, D. B., Gurman, H. B., & The California Association of School Psychologists/Diagnostic Center, Southern California Positive Intervention Task Force (2001). Positive interventions for serious problem behaviors: Best practices in implementing the positive behavioral intervention regulations. Sacramento, CA: California Depart-ment of Education.

The California School Psychologist, 2007, Vol. 12 59
Mental health Intervention Teams: A Collaborative Model to Promote Positive Behavioral
Support for Youth with Emotional or Behavioral Disorders Katina M. Lambros
Child & Adolescent Services Research Center, Rady Children’s Hospital, San Diego
San Diego State University
Shirley K. Culver & Aidee Angulo
Mental Health Resource Center, San Diego Unified School District
Pamela Hosmer Special Education Programs Division,
San Diego Unified School District
This paper describes an innovative intervention model for promoting mental health and positive social adjustment for youth with emotional or behavioral disorders (EBD) in San Diego. More specifically, it highlights a unique partnership between several program divisions within the San Diego Unified School District (SDUSD), namely, the Mental Health Resource Center (MHRC) and the Emotional Disturbance Program (ED) and also includes research and evaluation consultation from the Child and Adolescent Services Research Center (CASRC). This collaborative service model was developed to expand and standardize evidence-based interventions for students in self-contained special education ED classrooms in order to improve their academic and social outcomes.
Keywords: School-based Services, Mental Health Intervention Emotional or Behavioral Disorders, Evidence-based Practices, Positive Behavioral Support.
The provision of appropriate educational and mental health services for youth with emotional or behavioral disorders (EBD) is a challenging endeavor for school systems (Landrum, Tankersley & Kauffman, 2003). While there has been substantial progress in the school-based services literature outlining positive behavioral support and evidence-based intervention for youth with EBD (Colvin, 2004; Lane, Gresham & O’Shaughnessy, 2002; Sprague & Walker, 2000; Webster-Stratton, Reid & Hammond, 2004), the extent to which these services are available in all classrooms remains unknown (Hunter, Hoagwood, Evans, Weist et al., 2005). Hunter and colleagues identified the following characteristics of effective school-based mental health programs, noting they are difficult to achieve: implementing and sustaining collaboration and training across school staff (i.e., teachers, para-educators, psychologists, etc.) and community providers (i.e., mental health clinicians), overcoming fiscal constraints, home-school collaboration, and progress monitoring program effectiveness.
The California School Psychologist, Vol. 12, pp. 59 – 71, 2007Copyright 2007 California Association of School Psychologists
Please send correspondence to Katina M. Lambros, PhD, Research Scientist, Child and Adolescent Services Research Center (CASRC), Children’s Hospital, San Diego, 3020 Children’s Way MC 5033, San Diego, California, 92123. Email: [email protected]

The California School Psychologist, 2007, Vol. 12�0
Prevalence Rates and Characteristics of Youth with EBD
Prevalence rates of EBD range from 6-10% of school-age youth (Kaufman, 2005), yet federal data indicate that less than 1% of students in the U.S. are identified under the special education handicapping code of Emotionally Disturbed (ED); and in the state of California, even fewer (0.31%) are served under this category (Hallahan & Kauffman, 2006). Inherent problems with the ED definition, lack of cultur-ally appropriate assessment tools, as well as hesitation to negatively label students are potential reasons contributing to the under-identification (Kauffman, 2005). Despite this low identification rate, in 2002, 25,984 students in California alone were classified as needing special education services to address their emotional and behavioral needs (U.S. Department of Education, 2005). Given this sizable number of students, appropriate and accessible mental health supports are warranted.
Youth with EBD often demonstrate complex behaviors and co-occurring disorders (Kauffman, 2005). Youth served in ED special education have higher rates of mental health disorders than youth served by primary care, juvenile justice and mental health sectors (Garland, Hough, McCabe, Yeh, Wood, & Aarons, 2001). Yet national data indicate only 49% of students served as ED received mental health services and 55% had behavior management plans (U.S. DOE, 2005), a statistic revealing that nearly half did not receive necessary support.
Students with EBD often have recurrent contact with juvenile justice, are likely to live in single parent or foster homes, and are frequently economically disadvantaged (Coutinho, Oswald, Best & Forness, 2004; Hallahan & Kaufman, 2006). Males outnumber females within this category by 5 to 1 or more (Kauffman, 2005). ED is also among the five largest disability categories for all racial/ethnic groups except Asian/Pacific Islander, with African American students 2.25 and Native American students 1.30 times more likely than all other racial/ethnic groups combined to receive special education under ED and (U.S. DOE, 2005). Students with EBD also display significant deficits in academic achievement. Due to frequent off-task, disruptive, and defiant behavior, these students spend less time academically engaged and often fail to master basic academic skills (Gunter & Denny, 1998; Hinshaw, 1992). Students with EBD typically perform a year or more below grade level, and compared to students in all other disability categories, fail more courses, have higher absences, more grade retentions (Kauffman, 2005; Wagner, 1995) and unfortunately, have the highest drop-out rates (U.S. DOE, 2005).
Given the serious mental health and academic needs of the EBD population, they are more often educated outside the regular classroom than other students with disabilities. In fact, a large portion (30.7%) of students with EBD is educated outside the regular classroom for more than 60% of the school day (U.S. DOE, 2005).
need for an Integrated Educational and Mental health Treatment Model
There is considerable pressure for schools to address both the mental health and educational needs of youth with EBD. According to a consensus statement by the School Mental Health Alliance (Hunter et al., 2005) “health, and especially mental health, is a fundamental cornerstone for ensuring that all youth have an equal opportunity to succeed at school and that no child is left behind” (p. 8). Along a similar note, the No Child Left Behind Act recommends “student access to quality mental health care by developing innovative programs to link the local school system with the mental health system” (p. 427) (Office of Elementary and Secondary Education, 2002). Lastly, the Individuals with Disabilities Educa-tion Act (IDEA) requires that state and local educational agencies equip school personnel with skills to appropriately address serious behaviors and student mental health (IDEA, 2004).
Because of their daily access to children and families, school personnel are well positioned to

The California School Psychologist, 2007, Vol. 12 61
address significant academic and mental health issues; however, school personnel alone cannot provide all needed services. The EBD population often requires services from multiple community agencies (Farmer & Farmer, 1999) that are ideally, integrated and coordinated with one another as well as with school services (Zanglis, Furlong, & Casas, 2000).
San Diego Unified Schools Mental Health Resource Center
The Mental Health Resource Center (MHRC) as part of the Parent, Community and Student Engage-ment Branch of SDUSD (established in 2001) is funded by county monies and a Safe Schools Healthy Students grant. The MHRC provides mental health prevention and intervention to reduce violence and substance abuse, decrease emotional symptoms, improve behavior, and raise student achievement and attendance. MHRC provides assessment, case management, and treatment for students at all grade levels in both regular and special education. Key components of the MHRC include early screening, acces-sibility of mental health service, coordination with community mental health providers, and parental involvement. Its multi-disciplinary and multicultural staff consists of clinical psychologists, licensed mental health clinicians, social workers, school counselors, behavioral rehabilitation specialists, and psychiatrists. Lastly, the MHRC coordinates, operates and oversees a multitude of programs and uses several evidence-based interventions. A list of MHRC programs is provided on Table 1.
SDuSD Special Education Programs for Youth with EBD and District Demographics
Over 800 SDUSD students require supports and services under the ED category. SDUSD ED classes are located in 45 comprehensive school sites (elementary, middle and high school). Additionally, 40 ED classes are located in more restrictive alternative settings (i.e., non-public day and residential treatment centers). Recommended class size is 10 students for primary classes, and 12 for upper, middle and senior classes. In 2006, the ethnicity of the students classified as having ED was 29% Latino, 34% Caucasian, 3% Asian/Pacific Islander, 33% African American and 1% American Indian. In the same year, 42% of the district students were Latino, 26% Caucasian, 17% Asian/Pacific Islander, 14.5 % African American and .5% American Indian.
It is important to note the diversity of the SDUSD, as it provides the context for all specialized programs. There is a rising culture of economic poverty in San Diego’s inner-city schools, as the city’s border location contributes to drug trafficking and a growing population of migrant workers from Mexico and Central/South America. Influxes of Asian and East African refugees contribute to language barriers, ethnic tensions, and unemployment. Twenty-eight percent of the district students are English learners and 55% receive free/reduced lunch.
MhRC and ED Program Collaboration
A partnership between the MHRC and the ED program was established to address the need for added mental health support in classrooms by restructuring the way district services are delivered. Through a series of planning meetings, a continuum of services was developed. The primary goal was to deliver intensive services to students and their families in their local neighborhoods in order to prevent more restrictive placement (out of neighborhood) of students with EBD. Additional objectives included reducing suspensions and increasing academic achievement among students with EBD, as well as improving teacher retention in ED classrooms. By providing teachers with a larger repertoire of thera-peutic interventions, it was hypothesized that teachers would be better equipped to address the unique
School-Based Services for Youth with EBD
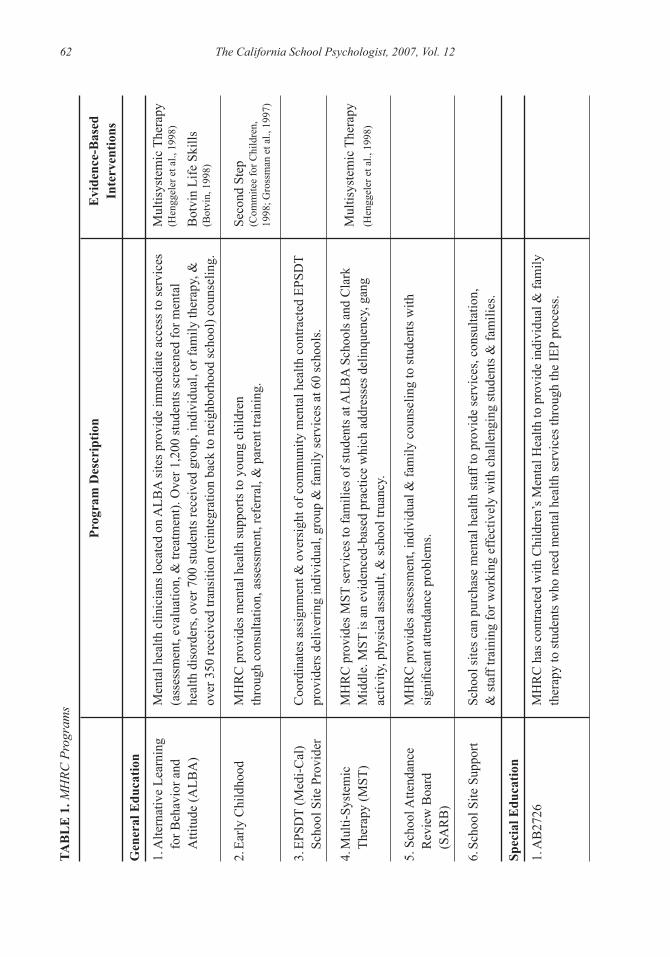
The California School Psychologist, 2007, Vol. 12�2TA
BL
E 1
. MH
RC P
rogr
ams
Prog
ram
Des
crip
tion
gen
eral
Edu
catio
n
1. A
ltern
ativ
e Le
arni
ng
for B
ehav
ior a
nd
Atti
tude
(ALB
A)
2. E
arly
Chi
ldho
od
3. E
PSD
T (M
edi-C
al)
Scho
ol S
ite P
rovi
der
4. M
ulti-
Syst
emic
Th
erap
y (M
ST)
5. S
choo
l Atte
ndan
ce
Rev
iew
Boa
rd
(SA
RB
)
6. S
choo
l Site
Sup
port
Spec
ial E
duca
tion
1. A
B27
26
Men
tal h
ealth
clin
icia
ns lo
cate
d on
ALB
A si
tes p
rovi
de im
med
iate
acc
ess t
o se
rvic
es
(ass
essm
ent,
eval
uatio
n, &
trea
tmen
t). O
ver 1
,200
stud
ents
scre
ened
for m
enta
l he
alth
dis
orde
rs, o
ver 7
00 st
uden
ts re
ceiv
ed g
roup
, ind
ivid
ual,
or fa
mily
ther
apy,
&
over
350
rece
ived
tran
sitio
n (r
eint
egra
tion
back
to n
eigh
borh
ood
scho
ol) c
ouns
elin
g.
MH
RC
pro
vide
s men
tal h
ealth
supp
orts
to y
oung
chi
ldre
n th
roug
h co
nsul
tatio
n, a
sses
smen
t, re
ferr
al, &
par
ent t
rain
ing.
Coo
rdin
ates
ass
ignm
ent &
ove
rsig
ht o
f com
mun
ity m
enta
l hea
lth c
ontra
cted
EPS
DT
prov
ider
s del
iver
ing
indi
vidu
al, g
roup
& fa
mily
serv
ices
at 6
0 sc
hool
s.
MH
RC
pro
vide
s MST
serv
ices
to fa
mili
es o
f stu
dent
s at A
LBA
Sch
ools
and
Cla
rk
Mid
dle.
MST
is a
n ev
iden
ced-
base
d pr
actic
e w
hich
add
ress
es d
elin
quen
cy, g
ang
activ
ity, p
hysi
cal a
ssau
lt, &
scho
ol tr
uanc
y.
MH
RC
pro
vide
s ass
essm
ent,
indi
vidu
al &
fam
ily c
ouns
elin
g to
stud
ents
with
si
gnifi
cant
atte
ndan
ce p
robl
ems.
Scho
ol si
tes c
an p
urch
ase
men
tal h
ealth
staf
f to
prov
ide
serv
ices
, con
sulta
tion,
&
staf
f tra
inin
g fo
r wor
king
effe
ctiv
ely
with
cha
lleng
ing
stud
ents
& fa
mili
es.
MH
RC
has
con
tract
ed w
ith C
hild
ren’
s Men
tal H
ealth
to p
rovi
de in
divi
dual
& fa
mily
th
erap
y to
stud
ents
who
nee
d m
enta
l hea
lth se
rvic
es th
roug
h th
e IE
P pr
oces
s.
Evi
denc
e-B
ased
In
terv
entio
ns
Mul
tisys
tem
ic T
hera
py
(Hen
ggel
er e
t al.,
199
8)
Bot
vin
Life
Ski
lls
(Bot
vin,
199
8)
Seco
nd S
tep
(Com
mite
e fo
r Chi
ldre
n,
1998
; Gro
ssm
an e
t al.,
199
7)
Mul
tisys
tem
ic T
hera
py
(Hen
ggel
er e
t al.,
199
8)

The California School Psychologist, 2007, Vol. 12 632.
Day
Tre
atm
ent
3. In
tens
ive
Out
patie
nt
Prog
ram
(IO
P)
4. D
eaf &
Har
d of
H
earin
g (D
HH
)
5. L
icen
sed
Chi
ldre
ns
Inst
itutio
ns
6. M
enta
l Hea
lth
Inte
rven
tion
team
(M
HIT
)
7. S
peci
al E
duca
tion
Prog
ram
Sup
port
Mar
cy S
choo
l & N
ew D
awn
full-
day
reha
bilit
atio
n pr
ogra
m p
rovi
de
com
preh
ensi
ve tr
eatm
ent s
ervi
ces t
o sp
ecia
l nee
ds e
lem
enta
ry, m
iddl
e,
& h
igh
scho
ol st
uden
ts.
IOP
pilo
t pro
ject
atta
ches
a m
enta
l hea
lth te
am to
one
ED
ele
men
tary
or m
iddl
e sc
hool
cla
ssro
om fo
r an
entir
e se
mes
ter a
nd th
en m
oves
to a
new
cla
ss th
e fo
llow
ing
sem
este
r, le
avin
g be
hind
cas
e m
anag
emen
t ser
vice
s in
first
cla
ssro
om. T
he IO
P te
am
cons
ists
of a
men
tal h
ealth
ther
apis
t, a
reha
bilit
atio
n te
chni
cian
, a c
ase
man
ager
, a
part-
time
psyc
hiat
rist a
nd ta
rget
s thr
ee k
ey e
nviro
nmen
ts/p
eopl
e: a
) cla
ssro
om
teac
her &
supp
ort s
taff,
b) p
aren
t/car
egiv
er, a
nd c
) stu
dent
s. In
terv
entio
n co
mpo
nent
s tea
ch a
ppro
pria
te so
cial
& b
ehav
iora
l ski
lls th
roug
h po
si-
tive
beha
vior
al su
ppor
t.
MH
RC
pro
vide
s tre
atm
ent s
ervi
ces t
o D
HH
st
uden
ts w
/ em
otio
nal/b
ehav
iora
l nee
ds.
LCI s
uppo
rts g
ener
al &
spec
ial e
duca
tion
stud
ents
in sh
elte
rs, f
oste
r you
th
faci
litie
s, ps
ychi
atric
hos
pita
ls &
day
trea
tmen
t pro
gram
s. M
HR
C st
aff
colla
bora
tes w
ith o
utsi
de a
genc
ies p
rovi
ding
trea
tmen
t & e
nsur
es su
cces
s dur
ing
stud
ent t
rans
ition
s.
MH
IT p
rovi
des s
ervi
ces t
o al
l ele
men
tary
& m
iddl
e sc
hool
s tha
t hav
e SD
C-E
D
clas
sroo
ms o
n si
te. M
HIT
Tea
ms h
elp
to st
ruct
ure
clas
sroo
ms,
deve
lop
poin
t sy
stem
s/to
ken
econ
omie
s, as
sist
scho
ol te
ams i
n de
velo
ping
, im
plem
entin
g, a
nd
mon
itorin
g be
havi
or su
ppor
t and
beh
avio
r int
erve
ntio
n pl
ans (
BSP
/BIP
), co
nduc
t gr
oup
ther
apy
for a
nger
man
agem
ent,
soci
al sk
ills,
etc.
(onc
e or
twic
e pe
r wee
k), a
nd
prov
ide
indi
vidu
al th
erap
y (3
0 -6
0 m
inut
es p
er w
eek)
that
is d
epen
dant
upo
n st
uden
t an
d fa
mily
nee
ds.
Ass
ists
with
con
sulta
tion,
hiri
ng m
enta
l hea
lth st
aff &
pro
gram
supe
rvis
ion
(TR
AC
E,D
iagn
ostic
Lea
rnin
g C
ente
r)
Seco
nd S
tep
(Com
mite
e fo
r Chi
ldre
n,
1998
; Gro
ssm
an e
t al.,
199
7)
Stre
ngth
enin
g Fa
mili
es
(Kum
pfer
et a
l., 2
007)
Seco
nd S
tep
(Com
mite
e fo
r Chi
ldre
n,
1998
; Gro
ssm
an e
t al.,
199
7)
Stre
ngth
enin
g Fa
mili
es
(Kum
pfer
et a
l., 2
007)
The
Incr
edib
le Y
ears
(W
ebst
er-S
tratto
n et
al.,
200
4)
Stre
ngth
enin
g Fa
mili
es
(Kum
pfer
et a
l., 2
007)
Pilo
t Pro
ject
:Th
e Pa
rent
Pro
ject
(C
hibn
all &
Abb
ruzz
ese,
20
04)
School-Based Services for Youth with EBD
The California School Psychologist, 2007, Vol. 12�4
challenges of this population, resulting in fewer disciplinary actions that place students outside of the class (i.e., principal’s office, counseling department). A final goal was to improve student achievement and behavior by engaging and empowering parents to be active members of intervention teams.
According to these program objectives, the partnership established a continuum of integrated educa-tional/mental health programs for students classified as ED, which included direct service to students, consultation with teachers on meeting the mental health and behavioral needs of students with EBD, and parent training. This initiative was implemented by the Mental Health Intervention Teams (MHIT).
Mental health Intervention Teams (MhIT)
The MHIT program provides services to all elementary and middle schools on regular school campuses that have self-contained ED classrooms onsite. Program components include classroom behavioral interventions, consultation services, case management, traditional individual and group psychotherapy, and family outreach and parenting groups.
MHIT consists of 6 teams (1 mental health clinician and 1 rehabilitation specialist) to serve ED classrooms. The employment qualifications required for a mental health clinician include: a) a master’s degree in psychology, counseling, social work, or related field; b) licensure as a marriage and family therapist, clinical social worker, or clinical psychologist; and c) four years of post-license experience in counseling and youth/family crisis intervention. For the rehabilitation specialist position, a college degree or license is not essential, however, three years of behavior modification experience (training, experience and/or education) with emotionally disturbed or conduct-disordered youth in a mental health setting, preferably in inpatient hospitalization, intensive day treatment, or residential treatment, is required. A clinical psychologist supports all MHITs and provides neuropsychiatric assessment on complex cases as well as case consultation. Lastly, a psychiatrist is also available to provide medication management and consultation for youth.
Each MHIT has a caseload of 6-8 ED classes (a mix of elementary & middle schools). While these teams support the ED classrooms in a variety of ways, the primary focus is to provide service at three main levels:
Classroom/Teacher: The MHIT provides behavior and classroom management strategies to teachers and para-professionals. Teams help to structure classrooms, develop point systems/token economies, and assist school teams in developing, implementing, and monitoring function-based behavior support and behavior intervention plans (BSP/BIP).
Individual Child/Youth: The MHIT conducts group therapy for anger management, social skills, etc. (once or twice per week), and provides individual therapy (30 -60 minutes per week) for those students and families needing more intensive treatment.
Parent Outreach: The MHIT provides outreach to parents of students with ED. Substantial time each week is spent calling and visiting family homes to build trust and recruit caregivers to attend weekly parenting groups using empirically supported curricula (see Evidence-Based Intervention section below). MHIT staff also provides parent education on various topics and if necessary, refers them to adult mental health resources in the community.
Evidence-Based Intervention Components Implemented by MhIT
The MHIT staff was trained in one or more of the following interventions: a) The Incredible Years, b) Strengthening Families, and c) Parent Project. The MHRC sent several MHIT staff to training in one or more of the above interventions or arranged for trainings to be conducted locally in San Diego. The
MHRC plans to roll-out further training on these interventions as well as “refresher/booster” trainings during Summer 2007 to ensure all MHIT staff are trained in the three programs by the 2007-08 academic year.
The Incredible Years (IY): Elementary Classrooms: The Incredible Years: Parent, Teacher, and Child Training Series is a comprehensive curriculum to promote social competence and prevent, reduce, and treat aggression and related behavior problems in children ages 3-10. The parent intervention is ideally delivered in 2-hour, weekly parent group sessions lasting 20 weeks. The child component is designed as a “pull out” treatment program for small groups of children exhibiting conduct problems, and is to be delivered in 2-hour weekly group sessions lasting 20-22 weeks. The teacher training program is focused on strengthening classroom management strategies, promoting children’s prosocial behavior and school readiness, and reducing aggression and non-compliance. This component can be used to train a variety of school staff (i.e., teacher, aides, psychologists, school counselors).
All IY intervention components have been evaluated and positive findings have been replicated by independent investigators on different ethnic populations and age groups (Webster-Stratton & Hammond, 1997; Webster-Stratton, Reid & Hammond, 2001; Webster-Stratton et al., 2004). Participation in the IY was associated with improvements among culturally diverse, socio-economically disadvantaged popu-lations with mental health problems, including young children diagnosed with Obsessive Compulsive Disorder (ODD), Conduct Disorder (CD) and/or Attention Deficit Hyperactivity Disorder (ADHD). The IY has been modified for Spanish speaking families, which is appropriate for the linguistic diversity present in SDUSD.
The Strengthening Families Program (SFP). Middle School Classrooms: The Strengthening Fami-lies Program is a 14-session parenting and family skills training program designed to increase resilience and reduce risk among youth 10-14 years of age through skill-building, improved parenting practices, and strengthened relationships between children and parents (Kumpfer, Alvarado & Tait, 2007; Molgaard, Kumpfer & Spoth, 1994). This SFP involves groups of 4-12 parents in a Parent Skills Training group conducted during the first hour of each weekly session and a separate Children’s Skills Training group to be held concurrently. In the second hour the families are split into two multifamily Family Skills Training groups that are facilitated by two MHIT group leaders. Families are taught and encouraged to practice observation, monitoring, therapeutic play, communication, and positive discipline skills.
SFP has been associated with improvements in parent competencies, adolescent substance-related risk, and school engagement, as well as long-term academic success (Spoth, Randall & Shin, in press). The SFP has also been adapted for multiethnic populations, including economically disadvantaged and urban youth (Kumpfer, Alvaredo, Smith & Bellamy, 2002).
The Parent Project Pilot: Middle School Classrooms: The Parent Project was created for parents of adolescents, 11-19 years of age, with difficult or unmanageable behaviors. Because several of the EBD students presented significant delinquent and highly destructive behaviors (i.e., substance use, gang involvement, practice of the occult, running away, violence toward others and suicide), the MHIT staff developed lessons that directly tackled these serious behaviors. Using a structured, self-help support group model, parents learn and practice specific prevention and intervention strategies to address each of the above mentioned behaviors. The PP lasts 10-16 weeks and includes two intervention units. Unit I, “Laying the Foundation for Change,” consists of six activity-based instructional units. Typically, each unit is delivered via a weekly three-hour session. Unit II, “Changing Behavior and Rebuilding Family Relationships,” includes 10 topic-focused parent support group sessions, which are delivered via weekly two-hour blocks. Sessions provide parents with emotional support and include an activity-
School-Based Services for Youth with EBD

The California School Psychologist, 2007, Vol. 12 65
challenges of this population, resulting in fewer disciplinary actions that place students outside of the class (i.e., principal’s office, counseling department). A final goal was to improve student achievement and behavior by engaging and empowering parents to be active members of intervention teams.
According to these program objectives, the partnership established a continuum of integrated educa-tional/mental health programs for students classified as ED, which included direct service to students, consultation with teachers on meeting the mental health and behavioral needs of students with EBD, and parent training. This initiative was implemented by the Mental Health Intervention Teams (MHIT).
Mental health Intervention Teams (MhIT)
The MHIT program provides services to all elementary and middle schools on regular school campuses that have self-contained ED classrooms onsite. Program components include classroom behavioral interventions, consultation services, case management, traditional individual and group psychotherapy, and family outreach and parenting groups.
MHIT consists of 6 teams (1 mental health clinician and 1 rehabilitation specialist) to serve ED classrooms. The employment qualifications required for a mental health clinician include: a) a master’s degree in psychology, counseling, social work, or related field; b) licensure as a marriage and family therapist, clinical social worker, or clinical psychologist; and c) four years of post-license experience in counseling and youth/family crisis intervention. For the rehabilitation specialist position, a college degree or license is not essential, however, three years of behavior modification experience (training, experience and/or education) with emotionally disturbed or conduct-disordered youth in a mental health setting, preferably in inpatient hospitalization, intensive day treatment, or residential treatment, is required. A clinical psychologist supports all MHITs and provides neuropsychiatric assessment on complex cases as well as case consultation. Lastly, a psychiatrist is also available to provide medication management and consultation for youth.
Each MHIT has a caseload of 6-8 ED classes (a mix of elementary & middle schools). While these teams support the ED classrooms in a variety of ways, the primary focus is to provide service at three main levels:
Classroom/Teacher: The MHIT provides behavior and classroom management strategies to teachers and para-professionals. Teams help to structure classrooms, develop point systems/token economies, and assist school teams in developing, implementing, and monitoring function-based behavior support and behavior intervention plans (BSP/BIP).
Individual Child/Youth: The MHIT conducts group therapy for anger management, social skills, etc. (once or twice per week), and provides individual therapy (30 -60 minutes per week) for those students and families needing more intensive treatment.
Parent Outreach: The MHIT provides outreach to parents of students with ED. Substantial time each week is spent calling and visiting family homes to build trust and recruit caregivers to attend weekly parenting groups using empirically supported curricula (see Evidence-Based Intervention section below). MHIT staff also provides parent education on various topics and if necessary, refers them to adult mental health resources in the community.
Evidence-Based Intervention Components Implemented by MhIT
The MHIT staff was trained in one or more of the following interventions: a) The Incredible Years, b) Strengthening Families, and c) Parent Project. The MHRC sent several MHIT staff to training in one or more of the above interventions or arranged for trainings to be conducted locally in San Diego. The
MHRC plans to roll-out further training on these interventions as well as “refresher/booster” trainings during Summer 2007 to ensure all MHIT staff are trained in the three programs by the 2007-08 academic year.
The Incredible Years (IY): Elementary Classrooms: The Incredible Years: Parent, Teacher, and Child Training Series is a comprehensive curriculum to promote social competence and prevent, reduce, and treat aggression and related behavior problems in children ages 3-10. The parent intervention is ideally delivered in 2-hour, weekly parent group sessions lasting 20 weeks. The child component is designed as a “pull out” treatment program for small groups of children exhibiting conduct problems, and is to be delivered in 2-hour weekly group sessions lasting 20-22 weeks. The teacher training program is focused on strengthening classroom management strategies, promoting children’s prosocial behavior and school readiness, and reducing aggression and non-compliance. This component can be used to train a variety of school staff (i.e., teacher, aides, psychologists, school counselors).
All IY intervention components have been evaluated and positive findings have been replicated by independent investigators on different ethnic populations and age groups (Webster-Stratton & Hammond, 1997; Webster-Stratton, Reid & Hammond, 2001; Webster-Stratton et al., 2004). Participation in the IY was associated with improvements among culturally diverse, socio-economically disadvantaged popu-lations with mental health problems, including young children diagnosed with Obsessive Compulsive Disorder (ODD), Conduct Disorder (CD) and/or Attention Deficit Hyperactivity Disorder (ADHD). The IY has been modified for Spanish speaking families, which is appropriate for the linguistic diversity present in SDUSD.
The Strengthening Families Program (SFP). Middle School Classrooms: The Strengthening Fami-lies Program is a 14-session parenting and family skills training program designed to increase resilience and reduce risk among youth 10-14 years of age through skill-building, improved parenting practices, and strengthened relationships between children and parents (Kumpfer, Alvarado & Tait, 2007; Molgaard, Kumpfer & Spoth, 1994). This SFP involves groups of 4-12 parents in a Parent Skills Training group conducted during the first hour of each weekly session and a separate Children’s Skills Training group to be held concurrently. In the second hour the families are split into two multifamily Family Skills Training groups that are facilitated by two MHIT group leaders. Families are taught and encouraged to practice observation, monitoring, therapeutic play, communication, and positive discipline skills.
SFP has been associated with improvements in parent competencies, adolescent substance-related risk, and school engagement, as well as long-term academic success (Spoth, Randall & Shin, in press). The SFP has also been adapted for multiethnic populations, including economically disadvantaged and urban youth (Kumpfer, Alvaredo, Smith & Bellamy, 2002).
The Parent Project Pilot: Middle School Classrooms: The Parent Project was created for parents of adolescents, 11-19 years of age, with difficult or unmanageable behaviors. Because several of the EBD students presented significant delinquent and highly destructive behaviors (i.e., substance use, gang involvement, practice of the occult, running away, violence toward others and suicide), the MHIT staff developed lessons that directly tackled these serious behaviors. Using a structured, self-help support group model, parents learn and practice specific prevention and intervention strategies to address each of the above mentioned behaviors. The PP lasts 10-16 weeks and includes two intervention units. Unit I, “Laying the Foundation for Change,” consists of six activity-based instructional units. Typically, each unit is delivered via a weekly three-hour session. Unit II, “Changing Behavior and Rebuilding Family Relationships,” includes 10 topic-focused parent support group sessions, which are delivered via weekly two-hour blocks. Sessions provide parents with emotional support and include an activity-
School-Based Services for Youth with EBD

The California School Psychologist, 2007, Vol. 12��
based parenting skills component. The PP has been featured by the Office of Juvenile Justice and Delinquency Prevention as a promising community and school program to decrease serious delinquent behavior (Chibnall & Abbruzzese, 2004), however; this program has not been sufficiently researched and is presently considered a pilot project.
MhIT and School Staff Interface
At each school with an onsite ED classroom a designated liaison assists the MHIT. More specifi-cally, this liaison can be any school staff member on campus (i.e., school counselor, district resource teacher, vice principal, school psychologist, etc.) who agrees to orient the MHIT with the school, coor-dinate shared office space, and attend weekly/monthly meetings with the MHIT, ED classroom staff, and support personnel.
At the beginning of the school year, the MHIT conducts direct observation and interviews (both semi-structured and informal) with ED teachers and school staff to determine the level of support that is needed and builds relationships in that classroom. MHIT clinicians reported that in some classrooms, ED teachers demonstrated exceptional classroom organization, behavior management skills, and effective instructional practices. These classrooms generally required minimal classroom support, with occa-sional individual child crisis intervention services or consultation for particularly difficult students and moderate (i.e., weekly) concentration on parent/family outreach. Other ED classrooms require signifi-cant and ongoing support in developing classroom reinforcement systems, teaching positive behavioral support strategies, and adjusting instructional practices to be more appropriate for students. Such classes often required intense individual child services and significant parent outreach, resulting in high involve-ment (i.e., daily) of the MHIT with that particular class. In essence, the MHIT developed an individual-ized program of support for each classroom on their caseload.
MHITs adjust support services to accommodate differing levels of student mainstreaming into general education, which varies by school. In the majority of self-contained ED classes, students remain with the same teacher and peer cohort for most of the school day, with some students mainstreaming as appropriate. However, approximately 30% of middle school programs do not have a “core” ED classroom and instead, students are fully mainstreamed into regular classes with itinerant support. In these schools, the MHIT attempted to maintain contact with several general education teachers and the special education teacher regarding student progress and/or behavioral support plans. But it was difficult to provide consultation services to each of the general education teachers and to provide direct services in the individual classrooms. Additionally, as youth are in different general education classes, it was a challenge to find common class periods to conduct group therapy sessions.
MhIT Interface with School Psychologists:
Most of the MHITs communicate several times per week with the school psychologist on site. The MHIT staff provides the school psychologist with assessment and/or treatment information on the students they serve such as, their history of mental health support services, informal and formal behav-ioral observation data, behavioral rating scales results, and group or individual therapy progress updates. MHITs and school psychologists work together to jointly support ED teachers and classroom aides with implementation of behavioral support services (i.e., especially on days where one or the other is not working at the school site), monitor teacher implementation of intervention strategies, make referrals for additional mental health services (i.e., AB3632, etc.), and co-facilitate child therapy groups. The sustained behavioral and mental health support to the ED classes frees the school psychologist to provide
more services to general education students (i.e., Student Study Team, 504 process, prevention efforts, behavioral consultation, etc.), which may prevent ED referrals. Further collaboration occurs regarding parent outreach, as school psychologists and MHIT staff work to engage parents of ED students to become more active in their child’s academic and behavioral interventions. Both MHITs and psycholo-gists attend all Individual Education Plan (IEP) meetings, as well as weekly and monthly meetings with ED teachers and school administration.
The MHITs may also interact with one of four psychologists who are assigned (full-time) to a single school with multiple ED classes. In these instances, the cross-coordination and communication between the MHIT and ED school psychologist occurs several times a day as they work together in multiple ways to support students with ED and their families. The ED program intends to hire four additional ED project school psychologists for the 2007-08 year.
Research and Community Partnership: MhRC/SDuSD and CASRC
The Child and Adolescent Services Research Center (CASRC) at Rady Children’s Hospital-San Diego is a NIMH funded center comprised of a multi-disciplinary consortium of investigators as well as community representatives from the public system of care (i.e., mental health, child welfare, juvenile justice, education, alcohol/drug, primary care). CASRC conducts mental health services research that spans clinical epidemiology studies linked to evidence-based practice, effectiveness and quality of care studies, and implementation studies. CASRC has a long standing relationship with the MHRC and has conducted program evaluation and provided consultation on evidence-based interventions for youth with a range of academic and behavioral needs. Members of CASRC and the MHRC meet monthly to discuss school-based services and research collaborations. This relationship provides a unique and valuable opportunity to study large-scale specialty mental health care taking place in the real world context of schools.
Preliminary Evaluation of MhIT
Process Evaluation: In 2005-06, the MHITs served 37 ED classrooms on comprehensive sites. This start-up year consisted of a) building relationships and integrating with educational and administra-tive staff, b) identifying evidence-based interventions for elementary and middle school populations, c) deciding the appropriate amount of time spent in each class, d) assessing the correct balance of elemen-tary and middle school ED classes on team caseloads, e) determining levels of clinical supervision, f) scheduling formal training for MHIT members on chosen interventions and g) provision of consultation services to classroom teachers.
For 2006-07, the MHIT provided services to students in 38 ED classes on comprehensive school campuses. This second year involved a) provision of direct services to students and parents, b) continuing consultation to classroom teachers, c) hiring additional MHIT staff, d) training new MHIT staff on the IY and SFP, e) training all staff on the new PP intervention, f) working to build relationships at newly assigned schools or with new ED teachers, and g) working with school administrative staff on discipline and suspension policy.
Outcome Evaluation: Members of CASRC, MHRC, and MHIT are trying to secure grant funding for the outcome evaluation component of the MHIT program. Evaluation meetings have focused on how to best capture outcome variables; a process which remains quite challenging as MHIT services vary in intensity within and across the individual stakeholders: students, parents, and teachers. It is important to note, that limited evaluation data have been collected to date (as focus has been on program development
School-Based Services for Youth with EBD

The California School Psychologist, 2007, Vol. 12 67
based parenting skills component. The PP has been featured by the Office of Juvenile Justice and Delinquency Prevention as a promising community and school program to decrease serious delinquent behavior (Chibnall & Abbruzzese, 2004), however; this program has not been sufficiently researched and is presently considered a pilot project.
MhIT and School Staff Interface
At each school with an onsite ED classroom a designated liaison assists the MHIT. More specifi-cally, this liaison can be any school staff member on campus (i.e., school counselor, district resource teacher, vice principal, school psychologist, etc.) who agrees to orient the MHIT with the school, coor-dinate shared office space, and attend weekly/monthly meetings with the MHIT, ED classroom staff, and support personnel.
At the beginning of the school year, the MHIT conducts direct observation and interviews (both semi-structured and informal) with ED teachers and school staff to determine the level of support that is needed and builds relationships in that classroom. MHIT clinicians reported that in some classrooms, ED teachers demonstrated exceptional classroom organization, behavior management skills, and effective instructional practices. These classrooms generally required minimal classroom support, with occa-sional individual child crisis intervention services or consultation for particularly difficult students and moderate (i.e., weekly) concentration on parent/family outreach. Other ED classrooms require signifi-cant and ongoing support in developing classroom reinforcement systems, teaching positive behavioral support strategies, and adjusting instructional practices to be more appropriate for students. Such classes often required intense individual child services and significant parent outreach, resulting in high involve-ment (i.e., daily) of the MHIT with that particular class. In essence, the MHIT developed an individual-ized program of support for each classroom on their caseload.
MHITs adjust support services to accommodate differing levels of student mainstreaming into general education, which varies by school. In the majority of self-contained ED classes, students remain with the same teacher and peer cohort for most of the school day, with some students mainstreaming as appropriate. However, approximately 30% of middle school programs do not have a “core” ED classroom and instead, students are fully mainstreamed into regular classes with itinerant support. In these schools, the MHIT attempted to maintain contact with several general education teachers and the special education teacher regarding student progress and/or behavioral support plans. But it was difficult to provide consultation services to each of the general education teachers and to provide direct services in the individual classrooms. Additionally, as youth are in different general education classes, it was a challenge to find common class periods to conduct group therapy sessions.
MhIT Interface with School Psychologists:
Most of the MHITs communicate several times per week with the school psychologist on site. The MHIT staff provides the school psychologist with assessment and/or treatment information on the students they serve such as, their history of mental health support services, informal and formal behav-ioral observation data, behavioral rating scales results, and group or individual therapy progress updates. MHITs and school psychologists work together to jointly support ED teachers and classroom aides with implementation of behavioral support services (i.e., especially on days where one or the other is not working at the school site), monitor teacher implementation of intervention strategies, make referrals for additional mental health services (i.e., AB3632, etc.), and co-facilitate child therapy groups. The sustained behavioral and mental health support to the ED classes frees the school psychologist to provide
more services to general education students (i.e., Student Study Team, 504 process, prevention efforts, behavioral consultation, etc.), which may prevent ED referrals. Further collaboration occurs regarding parent outreach, as school psychologists and MHIT staff work to engage parents of ED students to become more active in their child’s academic and behavioral interventions. Both MHITs and psycholo-gists attend all Individual Education Plan (IEP) meetings, as well as weekly and monthly meetings with ED teachers and school administration.
The MHITs may also interact with one of four psychologists who are assigned (full-time) to a single school with multiple ED classes. In these instances, the cross-coordination and communication between the MHIT and ED school psychologist occurs several times a day as they work together in multiple ways to support students with ED and their families. The ED program intends to hire four additional ED project school psychologists for the 2007-08 year.
Research and Community Partnership: MhRC/SDuSD and CASRC
The Child and Adolescent Services Research Center (CASRC) at Rady Children’s Hospital-San Diego is a NIMH funded center comprised of a multi-disciplinary consortium of investigators as well as community representatives from the public system of care (i.e., mental health, child welfare, juvenile justice, education, alcohol/drug, primary care). CASRC conducts mental health services research that spans clinical epidemiology studies linked to evidence-based practice, effectiveness and quality of care studies, and implementation studies. CASRC has a long standing relationship with the MHRC and has conducted program evaluation and provided consultation on evidence-based interventions for youth with a range of academic and behavioral needs. Members of CASRC and the MHRC meet monthly to discuss school-based services and research collaborations. This relationship provides a unique and valuable opportunity to study large-scale specialty mental health care taking place in the real world context of schools.
Preliminary Evaluation of MhIT
Process Evaluation: In 2005-06, the MHITs served 37 ED classrooms on comprehensive sites. This start-up year consisted of a) building relationships and integrating with educational and administra-tive staff, b) identifying evidence-based interventions for elementary and middle school populations, c) deciding the appropriate amount of time spent in each class, d) assessing the correct balance of elemen-tary and middle school ED classes on team caseloads, e) determining levels of clinical supervision, f) scheduling formal training for MHIT members on chosen interventions and g) provision of consultation services to classroom teachers.
For 2006-07, the MHIT provided services to students in 38 ED classes on comprehensive school campuses. This second year involved a) provision of direct services to students and parents, b) continuing consultation to classroom teachers, c) hiring additional MHIT staff, d) training new MHIT staff on the IY and SFP, e) training all staff on the new PP intervention, f) working to build relationships at newly assigned schools or with new ED teachers, and g) working with school administrative staff on discipline and suspension policy.
Outcome Evaluation: Members of CASRC, MHRC, and MHIT are trying to secure grant funding for the outcome evaluation component of the MHIT program. Evaluation meetings have focused on how to best capture outcome variables; a process which remains quite challenging as MHIT services vary in intensity within and across the individual stakeholders: students, parents, and teachers. It is important to note, that limited evaluation data have been collected to date (as focus has been on program development
School-Based Services for Youth with EBD

The California School Psychologist, 2007, Vol. 12�8
and implementation), however, an evaluation plan has been drafted. The outcome evaluation is designed to collect information from each stakeholder:
Classroom/Teacher: Classroom teacher acceptability and satisfaction with the MHIT model was assessed with a 15-item survey. Additionally, this survey was administered to school staff who support the ED class (i.e., school counselors, administrators, psychologists). All school staff completed the survey anonymously. A survey response rate of 34% was obtained. The MHIT staff (the clinician and rehabilitation specialist) completed a longer 30-item survey for each assigned ED class. The MHIT survey response rate was substantially higher at 82%. Table 2 contains a portion of the results which addresses the quality of the MHIT and school staff relationship. The overwhelming majority of ED teachers and school staff report having a positive relationship with their MHIT, maintaining effective team communication, and feeling supported by the model. MHIT staff report was also positive, although included more variable responses.
Several open ended survey questions asked “what impact did the MHIT have in your classroom?” Teacher responses included “MHIT helped me a great deal with classroom management, they put a great system in place and I followed it” as well as “the anger management and peer interaction groups the MHIT conducted were great…problem behavior decreased in frequency while learning increased.” Surveys for the 2006-07 year were administered.
ED teacher retention was also tracked. In the year prior to the MHIT program (2004-05), there existed a 50% ED teacher turnover rate, with only 19 of the original 38 elementary and middle school teachers remaining in the program. Following the first year of MHIT, 29 of 37 ED teachers remained (78% retention rate), with 8 teachers leaving for the following reasons: moving out of state, moving to general education or RSP program, or receiving promotions.
Future evaluation efforts will focus on formal implementation of treatment integrity measures incor-porated by the IY and SFP developers for the classroom interventions. This will be a staged process, with independent observers assessing the treatment integrity of the MHIT staff as they train the classroom teachers and school staff and model strategies with students. Subsequently, the school psychologists and MHIT will jointly monitor the treatment fidelity of the classroom teachers as they use intervention strategies. Lastly, informal measures assessing classroom organization, structure, and climate will also be collected.
Individual Child/Youth: Individual student evaluation will consist of educational indicators (i.e., grades, attendance, academic achievement, IEP goal attainment, impairment ratings, educational place-ment maintenance, etc.) and will be downloaded from the Standards, Assessment, and Accountability department in SDUSD at the end of each academic year, beginning with the 2006-07 year. In addition, single subject methodologies will be employed to chart and monitor individual student behavioral prog-ress.
Parent Outreach: During 2006-07, MHITs conducted parenting groups and reported variable atten-dance ranging from 35-65%. Increased attendance was reported for groups that provided childcare and food. Barriers to parent participation included transportation to the school. Future evaluation of parenting groups will include administration of IY and SFP measures (i.e., parenting scale, parent satis-faction questionnaire etc.) to parents/caregivers to assess behavioral support skills and program satisfac-tion. Independent observers will also assess treatment integrity of the MHIT staff as they train parents on intervention strategies.
Lastly, at all service levels, qualitative research methods will be used to answer questions that quan-titative data may be unable to answer. Qualitative methods (i.e., focus groups, key informant inter-

The California School Psychologist, 2007, Vol. 12 69
views) describe complex phenomena such as the experiences and interpretation of events by people with different stakes and roles. Additionally, these approaches can describe complex settings (schools, class-rooms, etc.) and interactions (families, teachers, students) (Sofaer, 1999). It is intended that evaluation results will provide ongoing feedback to the program staff as well as inform the research community on the feasibility and effectiveness of implementing evidence-based interventions within the framework of the MHIT service delivery model.
MhIT Implications and future Directions
The MHIT is a collaborative service delivery model using school-based mental health teams to implement evidence-based interventions to promote positive social adjustment for youth with EBD and their families as well as support classroom teachers. This model is aligned with research suggesting that integrating mental health intervention within schools and classroom settings can improve school climate and attitudes about mental health as well as support teachers who serve children and adolescents with EBD (Bruns, Walrath, Glass-Seigel, & Weist, 2004).
By joining educational staff and clinical providers in the classroom to treat students with EBD, the MHIT has addressed a long standing barrier in the provision of mental health services – lack of infra-structure to support mental health programs (Hunter et al., 2005). MHIT staff does not service youth in isolation, but is integrated into the existing special education class unit and is part of the support staff working closely with school psychologists and other personnel. Thus, mental health services are weaved into the daily classroom curricula rather than fragmented.
TABLE 2. MHIT Program Survey Results
Survey Question School Staff MHIT Staff Surveys (N=17) Surveys* (N=61)
How would you describe the relationship Very Good 15 (88%) 33 (54%) between you and your Teacher or MHIT Good 1 (6%) 23 (37%) team member? Fair 1 (6%) 4 (7%) Poor 0 (0%) 1 (2%)
Do you feel supported by your Teacher or Yes 16 (94%) 42 (69%) MHIT team member? Sometimes 1 (6%) 17 (28%) No 0 (0%) 2 (3%)
Do you feel you communicate/collaborate All the Time 14 (82%) 28 (46%) effectively with your Teacher or MHIT Most of the Time 2 (12%) 20 (32%) team member? Could Improve 0 (0%) 9 (15%) There are Difficulties 1 (6%) 4 (7%) Not at All 0 (0%) 0 (0%)
Do you have established weekly or Yes 13 (76%) 47 (77%) monthly meetings involving the teachers No 4 (24%) 14 (23%) and MHIT team members?* The MHIT staff completed more than one survey
School-Based Services for Youth with EBD

The California School Psychologist, 2007, Vol. 1270
The MHIT model may offer districts a template for combining fiscal and personnel resources from separate departments to provide expanded services. Hunter and colleagues (2005) posit that one of the most salient obstacles to implementing mental health interventions in schools is a lack of funding to support and sustain them. By integrating program components and combining fiscal resources to develop the MHIT, a more efficient use of resources may be possible resulting in increased services to students and teachers beyond what is likely when mental health and educational programs work in isolation.
One strength of the MHIT model is the parenting programs. Parents of children with EBD are typically difficult to engage due to countless negative interactions they have had with school personnel regarding their child’s behavior. Yet, by co-locating mental health services within special education classes, the MHIT model may provide better access to mental health services for students/families who would not otherwise seek individual or family counseling. In addition, the emphasis on devel-oping parenting skills that foster prosocial behavior in youth rather than criticize parenting skills may encourage parental engagement in the groups. Finally, the parent lessons also promote parent-to-parent support systems that can last beyond the class sessions.
Lastly, the integration of clinical mental health providers and school personnel provides a truly multidisciplinary approach, allowing cross-discipline training to occur. School staff learn about psycho-logical symptomotology and diagnoses, while MHITs become familiar with effective instructional prac-tice and IEP goals and objectives. Additionally, the involvement of district administrative staff and school services researchers has enhanced this MHIT model by providing a practitioner-researcher collaborative to working with youth having EBD.
REfEREnCES
Bruns, E.K. Walrath, C., Glass-Siegel, M., & Weist, M.D. (2004). School-based mental health services in Baltimore: Association with school climate and special education referrals. Behavior Modification, 28, 491-512.
Botvin, G. (1998). Life skills training-middle school. White Plains, NY: Princeton Health Press.Chibnall, S. & Abbruzzese, K. (2004). A community approach to reducing risk factors. Journal of the Office of
Juvenile Justice and Delinquency Prevention, IX(1), September, 30-31. Colvin, G. (2004). Managing the cycle of acting-out behavior in the classroom. Eugene, OR: Behavior Associates.Committee for Children. (1998). Second Step Violence Prevention Intervention: Steps for Successful Implementa-
tion. Retrieved May 2004 from http://cfchildren.org/comboimp.odf.Coutinho, M., Oswald, D., Best, A., & Forness, S. (2004). Gender and socio-demographic factors in the dispropor-
tionate identification of minority students as emotionally disturbed. Behavioral Disorders, 27, 109-125. Farmer, E.M., & Farmer, T.W. (1999). The role of schools in outcomes for youth: Implications for children’s mental
health services research. Journal of Child and Family Studies, 8, 377-396. Garland, A.F., Hough, R.L., McCabe, K.M., Yeh, M., Wood, P.A., & Aarons, G.A. (2001). Prevalence of psychi-
atric disorders in youth across five sectors of care. Journal of the American Academy of Child and Adolescent Psychiatry, 40(4), 409-418.
Grossman, D.C., Neckerman, H.J., Koepsell, T.D., Liu, P.Y., Asher, K.N., Beland, K., et al. (1997). Effectiveness of violence prevention curriculum among children in elementary school: A randomized controlled trial. Journal of the American Medical Association, 277(20), 1605-1612.
Gunter, P.L., & Denny, R.K. (1998). Trends and issues in research regarding academic instruction of students with emotional and behavioral disorders. Behavioral Disorders, 24(1), 44-50.
Hallahan, D, & Kauffman, J. (2006). Exceptional learners: Introduction to special education, (10th ed.). Boston: Allyn & Bacon.
Henggeler, S.W., Schoenwald, S.K., Borduin, C.M., Rowland, M.D., & Cunningham, P.B. (1998). Multisystemic treatment of antisocial behavior in children and adolescents. New York, NY: Guilford Press.
Hinshaw, S.P. (1992). Academic underachievement, attention deficits, and aggression: Comorbidity and implica-tions for intervention [Special issue]. Journal of Consulting and Clinical Psychology, �0(6), 893-903.

The California School Psychologist, 2007, Vol. 12 71
Hunter, L., Hoagwood, K., Evans, S., Weist, M., Smith, C., Paternite, C., Horner, R., Osher, D., Jensen, P., & the School Mental Health Alliance (2005). Working Together to Promote Academic Performance, Social and Emotional Learning, and Mental Health for All Children. New York: Center for the Advancement of Children’s Mental Health at Columbia University.
Individuals with Disabilities Education Improvement Act Amendments of 2004, 20 U.S.C. § 1462 (h) et seq. Kauffman, J.M. (2005). Characteristics of emotional and behavioral disorders of children and youth (8th ed.). Upper
Saddle River, NJ: Merrill Prentice-Hall. Kumpfer C., Alvarado R., Smith, P. & Bellamy, N. (2002). Cultural sensitivity and adaptation in family-based
prevention interventions. Prevention Science, 3(2):241-246.Kumpfer, K.L., Alvarado, R. & Tait, C. (2007). The Strengthening Families Program: An evidence-based, multi-
cultural family skills training program. In: Tolan, P, Szapocznik, J., & Sambrano, S (eds). Preventing youth substance abuse: Science-based programs for children and adolescents. Washington, DC, US: American Psychological Association: 59-181.
Landrum, T.J., Tankersley, M., & Kauffman, J.M. (2003). What’s special about special education for student with emotional and behavioral disorders? The Journal of Special Education, 37, 148-156.
Lane, K.L., Gresham, F.M., & O’Shaughnessy, T. (Eds.). (2002). Interventions for children with or at risk for emotional and behavioral disorders. Needham: Allyn & Bacon.
Molgaard, V., Kumpfer, K. L. & Spoth, R. (1994). The Iowa Strengthening Families Program for Pre and Early Teens. Ames, IA: Iowa State University
Office of Elementary and Secondary Education. (2002). No Child Left Behind: A desktop reference. Washington, DC: U.S. Department of Education.
Sofaer, S. (1999). Qualitative methods: What are they and why use them? Health Services Research, 34(5), 1101-1118.
Spoth, R., Randall, G. K., & Shin, C. (In press). Experimental support for a model of partnership-based family intervention effects on long-term academic success. School Psychology Quarterly .
Sprague, J., & Walker, H. (2000). Early identification and intervention for youth with antisocial and violent behavior. Exceptional Children, ��, 367-379
U.S. Department of Education. (2005). Twenty-sixth annual report to Congress on the implementation of the Indi-viduals with Disabilities Education Act, vol. 2. Washington, DC: Author.
Wagner, M.M. (1995). Outcomes for youths with serious emotional disturbance in secondary school and early adult-hood. The Future of Children, 5(2), 90-112.
Webster-Stratton, C. & Hammond M. (1997). Treating children with early-onset conduct problems: A comparison of child and parent training interventions. Journal of Consulting and Clinical Psychology, 65, 93-109.
Webster-Stratton, C., Reid, M. J., & Hammond, M. (2001). Social skills and problem solving training for children with early-onset conduct problems: who benefits? Journal of Child Psychology and Psychiatry, 42(7), 943-952.
Webster-Stratton, C., & Reid, M. J. & Hammond, M. (2004). Treating children with early-onset conduct prob-lems: Intervention outcomes for Parent, Child, and Teacher Training. Journal of Clinical Child and Adolescent Psychology, 33(1), 105-124.
Zanglis, I., Furlong, M., & Casas, J. (2000). Case study of a community mental health collaborative: Impact on identification of youths with emotional or behavioral disorders. Behavioral Disorders, 25, 359-371.
School-Based Services for Youth with EBD


73
Address correspondence to Stephen E. Brock, Department of Special Education, Rehabilitation, School Psychology, and Deaf Studies; California State University, Sacramento; 6000 J Street; Sacramento, CA 95819-6079. Email: [email protected]
The California School Psychologist, Vol. 12, pp. 73 – 91, 2007Copyright 2007 California Association of School Psychologists
Diagnosis of Attention-Deficit/Hyperactivity Disorder (AD/hD) in Childhood:
A Review of the LiteratureStephen E. Brock &
Amanda Clinton California State University, Sacramento
This article examines recent literature related to the diagnosis of Attention-deficit/Hyperactivity Disorder (AD/HD) in childhood. First, the article discusses diagnostic criteria presented in the Diag-nostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000). Next, it explores the diagnostic procedures for AD/HD recommended in current publications. Results of this comprehensive literature review indicate that rating scales, interviews, laboratory/psychological testing, and observations are the most frequently recommended AD/HD diagnostic techniques. The implications of these findings for school psychologists are discussed.
KEYWORDS: ADHD, Attention Deficit, Diagnosis
Although medical science recognized inattention, impulsivity, and hyperactivity as problematic among children as long as 200 years ago (Anastopoulos & Shelton, 2001), no single method for reli-ably diagnosing Attention-deficit/Hyperactivity Disorder (AD/HD) has yet to be identified. This lack of a specific diagnostic procedure makes AD/HD identification complicated (Brock, 1999; Detweiler, Hicks, & Hicks, 1999). Furthermore, differential diagnosis can be confounded by a variety of other disorders that can co-exist with AD/HD or cause symptoms similar to those observed in AD/HD (Levy, Hay, Bennett, & McStephen, 2004; Power, Costigan, Eiraldi, & Leff, 2004). To address these issues, an accurate diagnosis requires multiple diagnostic procedures, such as obtaining information from different sources (Barkley, 1998; Hoff, Doepke, & Landau, 2002), behavioral observations (Miranda, Presenta-cion, & Soriano, 2002), and psychological assessment (Detwiler et al., 1999).
Before proceeding further, it is important to acknowledge that the role of the school psychologist in the diagnosis of AD/HD is somewhat controversial as this disorder is not a special education eligibility category in either state or federal regulations. Consequently, from the first author’s experiences, it has been observed that some districts do not allow their school psychologists to make AD/HD diagnoses. Such limitations are problematic given that (a) both state and federal regulations clearly specify that students with AD/HD may be eligible for special education services or Section 504 protections (CEC §56339; Davila, Williams, & MacDonald, 1991), and (b) school districts are required to identify special needs and must conduct assessments in all areas of suspected disability (34 C.F.R. §§ 104.32, 104.35, 300.304). Thus, there appear to be important legal reasons for school psychologists at least being well informed about the important elements of the AD/HD diagnosis. Further emphasizing the need for such knowledge is the California Education Code section specifying that all school personnel be trained to develop greater awareness of AD/HD [CEC §56339(d)].
Consistent with the need for school psychologists to be better informed regarding AD/HD, the purpose of this article is to review relevant diagnostic issues and information, beginning with a discus-sion of the American Psychiatric Association’s (APA) diagnostic criteria and, subsequently, presenting the results of a comprehensive literature review that identified the frequently recommended techniques

The California School Psychologist, 2007, Vol. 1274
for diagnosing AD/HD. This latter part of the paper is intended to provide school psychologists with a resource that documents the agreed upon elements of a comprehensive AD/HD diagnostic assessment. While it is clear there is no specific method or set of methods for diagnosing AD/HD, this literature review reveals significant agreement regarding recommended diagnostic practices. In addition to guiding the school psychologist’s practice, from the first author’s applied experiences, this knowledge will be helpful in those instances wherein a school assessment team is presented with an “AD/HD” diagnosis that is judged to be questionable because it fails to meet standard diagnostic practices.
AD/hD DIAgnoSTIC CRITERIA
AD/HD is included in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR; APA, 2000). The diagnosis of AD/HD is found within the section titled, “Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence” (pp. 39-134). Common among all disorders in this section is the presence of symptoms prior to an individual’s 18th birthday. AD/HD is further subsumed within the category of “Attention-Deficit and Disruptive Behavior Disorders” (pp. 85-103). Conduct Disorder, Oppositional Defiant Disorder, and Disruptive Behavior Disorders, Not Otherwise Specified are also included within this broader category.
The primary AD/HD symptoms are a “persistent pattern of inattention and/or hyperactivity-impul-sivity that is more frequently displayed and more severe than is typically observed in individuals at a comparable level of development” (APA, 2000, p. 85). The DSM-IV-TR classifies AD/HD into three subtypes: (a) Predominantly Hyperactive-Impulsive Type; (b) Predominantly Inattentive Type; and (c) Attention-deficit/Hyperactivity Disorder, Combined Type, which includes both hyperactive-impulsive and inattentive symptomology. Although the specific behavioral symptoms presented in the DSM-IV-TR are relatively self-explanatory, other diagnostic requirements appear to require further elaboration and are discussed below.
Although not currently specified in diagnostic criteria, leaders in this field have argued that the Predominantly Inattentive Type of AD/HD can be diagnosed significantly later than AD/HD Hyperac-tive-Impulsive Type and AD/HD Combined Type (e.g., Barkley, 1998). According to the DSM-IV-TR “Academic deficits and school-related problems tend to be most pronounced by the types marked by inattention …, whereas peer rejection and, to a lesser extent, accidental injury are most salient in the types marked by hyperactivity and impulsivity” (APA, 2000, p. 88). Due to differences such as these, Barkley (1997a; 1998) has suggested AD/HD Inattentive Type may be a separate and distinct disorder, rather than a subtype of AD/HD.
Symptom onset
Even though a clinical diagnosis of AD/HD may come later, symptoms of inattention and/or hyper-activity-impulsivity that compromise daily functioning should be observed prior to a child’s 7th birthday. However, this does not mean that a diagnosis must be made prior to the age of 7. In fact, it can be made in adulthood if careful verification of symptom onset prior to 7 years of age is made. To document age of onset, review of records and clinical interviews with parents and teachers may be required.
It is important to note that, since toddlers and preschoolers are typically very active, it is recom-mended that developmentally appropriate behaviors be taken into consideration and diagnosis of AD/HD be made with caution in the preschool years. A diagnosis of AD/HD prior to age 7 should be made only in cases where children are significantly more active than their developmental peers, so as to avoid the tendency to over-diagnose the disorder in preschoolers (Loughran, 2003). Conversely, if symptom onset
The California School Psychologist, 2007, Vol. 12 75
occurs subsequent to 7 years of age (particularly in cases of hyperactivity) the cause may be something other than AD/HD. For example, the cause of “AD/HD-like” behaviors in the older child or adolescent might include substance abuse (Burke, Loeber, & Lahey, 2001), learning disabilities, or physical illness (Root & Resnick, 2003).
Symptom Duration
According to the DSM-IV-TR, the pattern of symptoms for each subtype of AD/HD must be present for a minimum of six months prior to diagnosis. Symptom duration is critical when differentiating AD/HD from other disorders and normative developmental transitions, including school adjustment or temporary family stress. To document duration of symptoms, review of records and clinical interviews with parents and teachers may be required.
Symptom duration of at least six months is particularly important in assessment and diagnosis of AD/HD in preschool children. This is because it has been estimated that from 15% to 29% of this population is rated as inattentive and overactive by their parents at some point prior to age 5 (Gimpel & Kuhn, 1998; Loughran, 2003). However, in the majority of these cases concerns remit within 12 months (Campbell, 1990). In other words, significant inattention and hyperactivity/impulsivity in the 3- to 4-year-old child is not necessarily indicative of a pattern of AD/HD, but may be considered developmen-tally appropriate behavior (Barkley, 1998).
Multiple Settings
According to the DSM-IV-TR, the impairments resulting from the symptoms of hyperactivity/impul-sivity and/or inattention must be observed in at least two distinct settings, such as home, school, work, and social situations (APA, 2000). For example, symptoms could be present at home and school, or at school and after-school programs. The presence of symptomology in only one setting would not be suffi-cient for a diagnosis. Typically, the severity of symptoms varies between settings. For example, inatten-tiveness and hyperactivity/impulsivity are typically more problematic in situations of limited interest or novelty or those that require sustained mental effort. Traditional classroom lectures and lengthy repetitive tasks typically fall into this category. To document that symptoms are problematic in multiple settings, information from direct observations or the use of rating scales by various informants (e.g., parents and teachers) may be appropriate.
Clinical Significance
The DSM-IV-TR specifies that “clear evidence of social, academic, or occupational functioning” (APA, 2000, p. 93) impairments must be considered before a diagnosis of AD/HD is made. Specifically, for a child or adolescent to receive a diagnosis, their symptoms must negatively impact their academic performance, social interactions, and family relationships. For example, if an inattentive and/or hyper-active/impulsive child is able to obtain passing grades, follow classroom and playground rules, and develop appropriate peer relationships, clinically significant impairments may not exist and an AD/HD diagnostic assessment (let alone the diagnosis itself) would not be appropriate. To document clinically significant impairments, review of records and clinical interviews with parents and teachers may be required.
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 127�
Developmental Level
Symptoms of inattentiveness and hyperactivity are often observed among children with low intel-lectual functioning when they are placed in inappropriate educational settings (APA, 2000). Inattentive and hyperactive behavior that results from inappropriate school placement must be distinguished from true AD/HD. In cases of children who have been diagnosed with mental retardation, “an additional diagnosis of AD/HD should be made only if the symptoms of inattention or hyperactivity are excessive for the child’s mental age” (APA, 2000, p. 91). For example, if a 12-year-old with a developmental func-tioning level of 6 years demonstrates behavior typically observed among 6-year-olds, this criterion for a diagnosis of AD/HD would not be met. In this case the behavior is commensurate with developmental level. However, if this same 12-year-old demonstrated inattentiveness and/or hyperactivity similar to that observed among 4-year-olds, a diagnosis of AD/HD may be appropriate.1 To document that symptoms are developmentally inappropriate, norm referenced psycho-educational assessments may be required.
Differential Diagnosis
Finally, AD/HD diagnostic requirements require that other conditions with similar symptoms be ruled out before an AD/HD diagnosis is made (APA, 2000). In addition, the differential diagnosis of this disorder requires that age-appropriate behaviors among younger children (e.g., jumping, running, and yelling among preschoolers), mental retardation, under-stimulating environments, oppositional behavior, learning disorders, and other mental disorders (e.g., Pervasive Developmental Disorders; Psychotic Disorder; and Other Substance-Related Disorder, Not Otherwise Specified) be considered and ruled out as primary causes of the observed behaviors before the diagnosis of AD/HD is made. This requirement highlights the fact that a variety of conditions may generate AD/HD-like behaviors and that the diagnostic evaluation must include evaluation tools designed to consider these alternative explana-tions for AD/HD behaviors (Brock, 1999). Thus, even in those instances where the school psychologist is not making the AD/HD diagnosis, a comprehensive psycho-educational evaluation may be necessary to differentiate AD/HD from other similar disorders.
CoMPonEnTS of ThE AD/hD DIAgnoSIS
To identify frequently recommended components of an AD/HD diagnosis, the authors conducted a comprehensive review of the literature published within the past 1� years. Making use of the PsycINFO database, 48 articles, books, or book chapters, published since 1990 were identified based upon the use of the following words in the publication’s title: “attention deficit” and “diagnose” or “diagnosis” or “assessment.” Next the authors evaluated whether the source was specifically intended to give prac-tical guidance to health and/or mental health care professionals regarding how to diagnose AD/HD in childhood (i.e., did the publication have as one of its goals instructing readers on how to diagnose this disorder). From these selection procedures, 42 sources were identified as being appropriate for this literature review. Analysis of these sources revealed that a variety of different diagnostic procedures are recommended. However, most of these can be classified into one of several specific categories. Table 1 provides a summary of these diagnostic procedure categories and the sources that advocate their use. Table 2 provides an overview of the questions addressed by each procedure and offers examples of
1 Similarly, intellectually gifted children may demonstrate inattentiveness when they are placed in under-stimu-lating academic environments (APA, 2000). In the case of gifted children, obtaining historical information from several informants may help define their ability to regulate behavior across settings and help to determine if behaviors are isolated to the school or if they meet the multiple setting criteria.

The California School Psychologist, 2007, Vol. 12 77
TABLE 1. AD/HD Diagnostic Procedures Recommended in Recent Publications
RS INT L/T DO ME SR PA
1. Am. Acad. of Pediatrics (2000) 3 3 3 3
2. Anastopoulos & Shelton (2001) 3 3 3 3 3
3. Atkins & Pelham (1991) 3 3 3
4. Barkley (1990) 3 3 3 3 3 3
5. Barkley (1991) 3 3 3 3
6. Barkely (1997b) 3 3 3 3 3
7. Barkley (1998) 3 3 3 3 3
8. Barkley (2006) 3 3 3 3 3
9. Brown (2000) 3 3 3 3
10. Burcham & DeMers (1995) 3 3 3 3
11. Casat et al. (2001) 3 3 3 3 3
12. Cipkala-Gaffin (1998) 3 3 3 3 3
13. Detweiler et al. (1999) 3 3 3 3
14. DuPaul et al. (1991) 3 3 3 3
15. DuPaul & Stoner (1994) 3 3 3 3
16. Guevremont & Barkley (1992) 3 3 3 3
17. Guevremont et al. (1990) 3 3 3 3
18. Hardy et al. (2004) 3 3 3
19. Hechtman (2000) 3 3 3 3 3 3
20. Hinshaw (1994) 3 3 3 3
21. Leach & Brewer (2005) 3 3 3 3
22. Learner et al. (1995) 3 3 3 3 3
23. Martin (2003) 3 3 3 3
24. Meyer (1999) 3 3 3 3
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1278
25. Nahlik (2004) 3 3 3 3
26. Oesterheld et al. (2003) 3 3 3
27. Pelham et al. (2005) 3 3 3
28. Quinlan (2000) 3 3 3 3
29. Quinn (1997) 3 3 3 3 3
30. Rapport (1993) 3 3 3 3
31. Robin (1998) 3 3 3 3 3
32. Root & Resnick (2003) 3 3 3 3 3 3
33. Schaughency & Rothlind (1991) 3 3 3 3
34. Searight et al. (1995) 3 3 3
35. Shelton & Barkley (1994) 3 3 3 3
36. Shelton & Barkley (1995) 3 3 3 3
37. Silver (1999) 3 3 3
38. Silver (2004) 3 3 3
39. Slomka (1998) 3 3 3 3
40. Swanson & Smith (1996) 3 3 3 3 3
41. Wolraich et al. (2005) 3 3 3 3
Totals 100% 98% 90% 68% 34% 24% 7%
specific techniques. As can be seen, the four nearly universally recommended procedures are rating scales, interviews, laboratory/psychological assessments, and direct behavioral observations. Thus, these procedures will be discussed first. Subsequently, a discussion of other less frequently recommended procedures, including medical evaluations, school record reviews, and peer ratings is provided.
Rating Scales
Rating scales are the most widely advocated procedure for evaluating children with AD/HD, with 100% of the sources reviewed for this paper endorsing their use. As stated by Hinshaw (1994), “…rating scales are an indispensable element of the assessment of children with suspected attention deficits and hyperactivity” (p. 32). In some cases, rating scales can effectively differentiate children with AD/HD from others without this disorder (Barkley, 1998). In addition, they are time and cost effective (Anasto-poulos & Shelton, 2001). While for the school psychologist many other data sources are readily acces-sible, for the diagnostician not based in a school setting, rating scales are generally the only practical

The California School Psychologist, 2007, Vol. 12 79
TABLE 2. Summary of Recommended AD/HD Diagnostic Procedures
Procedure Diagnostician Sample Techniques Sample Questions
Rating Scales
Parent, Teacher, Child Interviews
Direct Behavioral Observations
Mental Health Professional
Educational Specialist
Mental Health Professional
Medical Professional
Mental Health Professional
Educational Specialist
Conners’ (1997) Rating Scales
Behavior Assessment System for Children 2 (Reynolds & Kamphaus, 2004)
Structured interview techniques (e.g., Diagnostic Interview Schedule for Children [Shaffer et al., 1996])
Unstructured interview techniques
Semi-structured interviews (e.g., developmental & health history)
Observation of test taking behavior
Classroom and play-ground observations
Are AD/HD symptoms present?
How deviant are symptoms for the norm?
Are there comorbid conditions?
Are AD/HD symptoms present?
When was the onset of AD/HD symptoms?
How long have symptoms been present?
Is the environment a factor?
Is there a family history of AD/HD?
Is the developmental/medical history significant?
Are there comorbid conditions?
Does the child display AD/HD behavioral symptoms?
Does the child display AD/HD symptoms?
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1280
Psychological
Pscho-Educational Tests
Medical Evaluation
Neuroimaging
School Records
Mental Health Professional
Educational Specialist
Pediatrician
General Practitioner
Psychiatrist
Medical Specialist
Mental Health Professional
Educational Specialist
Executive functioning tests (e.g., Test of Everyday Attention for children [Manly et al., 1999])
Intelligence testing
Achievement testing
Medical interview
Physical examination
Other medical tests as indicated
PET
MRI
fMRI
SPECT
Cumulative file review
School work sample review
Does the child demonstrate neuro-psychological or processing deficits?
What is the child’s ability level?
What is the child’s academic level?
Are symptoms secondary to a medical condition?
Is there abnormal brain functioning during tasks that require planning, attention, and impulse control?
Is there a history of AD/HD symptoms?
When was the onset of AD/HD symptoms?
way to obtain information from classroom teachers, since more time-consuming clinical interviews and observations may be difficult to arrange (Wender, 2004).
Rating scales provide a structured format for documenting the presence and degree of AD/HD symptoms using a normative frame of reference (Anastopoulos & Shelton, 2001; Burcham & DeMers, 1995; Landau & Burcham, 1995; Nahlik, 2004). Additionally, rating scales also allow the diagnostician to obtain information used in assessment of treatment effectiveness (Landau & Burcham, 1996). In other words, rating scales may be administered during the diagnostic process and again, later, when treatment has been initiated to determine the effect of intervention.
Several rating scales, such as the ADHD Symptoms Rating Scale (ADHD-SRS; Holland, Gimpel, & Merrill, 2003), ADHD Rating Scale-IV (DuPaul, Power, Anastopoulos, & Reid, 1998), and the Conners’ Rating Scales (Conners, 1997), assess symptom severity specific to AD/HD. General purpose rating scales, such as the Behavioral Assessment System for Children-Second Edition (BASC-2; Reynolds & Kamphaus, 2004) and the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001), are also available. These measures are helpful because they provide information about symptoms related to AD/

The California School Psychologist, 2007, Vol. 12 81
HD and other frequently occurring disorders or comorbid conditions (Anastopoulos & Shelton, 2001; Landau & Bircham, 1996). As such, they assist in the consideration of alternative hypotheses for AD/HD-like symptoms. Both types of scales (i.e., symptom-specific and general purpose) are recommended.
Despite their utility, as with all other diagnostic procedures, a rating scale should never be used in isolation to diagnose AD/HD (Nahlik, 2004). According to Rucklidge and Tannock (2002), this is particularly important, since some rating scales, one example being the Brown ADD Scale, may be most useful for screening out AD/HD rather than diagnosing it due to the measure’s low sensitivity (i.e., the probability that a child with AD/HD is accurately identified as having AD/HD is low; Rucklidge & Tannock, 2002).
Different raters, responding to the same rating scale, often provide different results. For example, agreement between parent and teacher ratings on diagnosis and actual symptoms has been shown to be low, possibly due to observations occurring in distinct settings (Wolraich et al., 2004). Yet comparison between raters may show discrepancy related to subtypes, they often correspond at an overall diagnostic level (Mitsis, McKay, Schulz, Newcorn, & Halperin, 2000).
Similar findings have been obtained in relation to self-report and teacher report measures of behavior in the diagnosis of AD/HD. Self-report behavioral ratings have been found to underestimate activity levels as well as attentional problems compared to parent and teacher report (Danckaerts, Heptinstall, Chadwick, & Taylor, 1999; Smith, Pelham, Gnagy, Molina, & Evans, 2000). Finally, use of teacher rating scales for adolescents appears questionable. Possibly due to the large size of many high school classes and the relative brevity of each class meetings, teacher agreement is lower for adolescent behavior (Molina, Pelham, Blumenthal, & Galiszewski, 1998).
Interviews
Another frequently recommended AD/HD diagnostic procedure is the clinical interview, with 98% of the sources reviewed for this paper endorsing their use. Clinical interviews are typically conducted by a mental health professional, such as a psychologist or social worker, or by medical professionals, including pediatricians or family practitioners. Interviews may be conducted with parents, teachers, and/or the student who was referred for assessment. According to Root and Resnick (2003) they are “the most important part of the evaluation process” (p. 36). According to Hinshaw (1994) and Nahlik (2004), clinical interviews address diagnostic issues including: (a) Whether AD/HD symptoms are present and under what conditions are they observed, (b) The onset of the AD/HD symptoms?, (c) The duration of symptom presentation, (d) The presence of environmental factors, (e) Family history of AD/HD, (f) The developmental history relative to AD/HD, (g) The presence of learning difficulties, and (h) The presence of emotional difficulties. Although relatively costly and time consuming, an interview can expand upon the results of behavioral rating scales since it “provides the opportunity to query the informant and make a better judgment about the symptom in question” (Wender, 2004, p. 48).
Formats for clinical interviews include structured, semi-structured, and unstructured procedures. A structured interview is conducted using an interview schedule, or a set of questions that are designed to probe areas of specific concern. Interview questions are read in the order they are written and responses are recorded categorically (Anastopoulos & Shelton, 2001). Structured diagnostic interviews have been defined as the “preferential method of diagnosis because of their exhaustive and direct correspondence to the DSM criteria” (McGrath, Handwerk, Armstrong, Lucas, & Freman, 2004, p. 350). Semi-structured interviews incorporate a specific set of questions while allowing the clinician to engage in open-ended inquiries to obtain further information about relevant points. An unstructured interview is conducted
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1282
through the use of open-ended questioning. Parent interviews. The parent interview is considered an indispensable part of the AD/HD evalu-
ation (Barkley, 1998; Landau & Burcham, 1996). In fact, it has been asserted that the “diagnosis of ADHD and/or other psychiatric comorbidities should be based largely on the information gained in the interviews” (Nahlik, 2004, p. 2). This is because parents are typically able to provide the most detailed and ecologically relevant information to the assessment process (Barkley, 1998). Interview data can effectively guide development of a holistic picture of the child and his or her experiences, filling in the gaps that may remain subsequent to use of other assessment techniques.
In addition to offering information about AD/HD symptoms, semi-structured parent interviews can provide relevant information about a child’s developmental, school, family, and psychiatric history (Barkley, 1998; Hinshaw, 1994). According to the DSM-IV-TR diagnostic criteria, specific data regarding the onset of AD/HD symptoms and family history of AD/HD should be obtained (APA, 2000) and, accordingly, this information can be provided by the child’s parents or caregivers. While the parent interview yields critically important information, it can be subject to bias and therefore not provide a true picture of the student’s functioning (Guevremmont, DuPaul, & Barkley, 1990). Thus, triangulation of data sources is required. In addition, it is important to note that Barkley (1998) asserts that the reliability and validity of parent interviews depends largely on the clinician’s ability to conduct the interview and to ask relevant and specific questions.
Teacher interviews. Of equal importance to the AD/HD assessment and diagnostic process, is the teacher interview. Both accurate diagnosis and evaluation of treatment effects have been reported to be dependent on teacher observation of student behavior. Thus, the teacher interview is critical given the significant amount of time spent at school and the importance of attention in relation to academic success (Molina et al., 1998). As is the case with the parent interview, the teacher interview is an impor-tant complement to teacher behavior rating scales (Molina, Smith, & Pelham, 2001), and for the school psychologist is a readily accessible data source.
Student interviews. The student interview may also be incorporated into the AD/HD diagnostic process. Information obtained directly from children can be helpful, particularly if other psychopatholo-gies, such as depression or psychosis, are suspected. However, regarding externalizing behavior disorders (e.g., AD/HD) it is important to acknowledge that children commonly report fewer symptoms than do adults (Hart, Lahey, Loeber, & Hanson, 1994; Volpe, DuPaul, Loney, & Salisbury, 1999). Nevertheless, at least in the case of adolescents, interviews may be particularly important in obtaining their collabora-tion in acceptance of the AD/HD diagnosis, as well as ensuring treatment compliance (Nahlik, 2004).
Laboratory/Psychological Testing
The use of laboratory and/or psychological tests is also common in the diagnosis of AD/HD, with 90% of the sources reviewed for this paper endorsing their use. According to Anastopoulos and Shelton (2001), standardized, norm-referenced measures are widely used due to “concerns that interviews and rating scales are not objective, are not pure measures of attention, and do not permit a component anal-ysis of the construct of attention” (p. 106). However, Barkley (1998) argues that “the fact that a series of tests is characterized as neuropsychological does not guarantee it actually taps into relevant neuropsy-chological processes” (p. 299). In other words, just because a test is purported to measure attention, does not mean it is a valid and reliable measure of a child’s ability to focus, inhibit and/or sustain responses in natural or clinic settings.
Cognitive assessment. A significant amount of research has been conducted regarding the relevance

The California School Psychologist, 2007, Vol. 12 83
of IQ testing to the AD/HD diagnosis. Findings have been mixed, with some research indicating that chil-dren with AD/HD are likely to perform several points lower than peers on IQ tests (Doyle, Biederman, Seidman, Weber, & Faraone, 2000; Fischer, Barkley, Fletcher, & Smallish, 1990). Others have found that AD/HD and IQ function independent of one another (Shuck & Crinella, 2005). While controversy about the relationship between intelligence test results and AD/HD persists, determining a child’s IQ remains important given the DSM-IV-TR (APA, 2000) diagnostic criterion that rules out the diagnosis if a student’s level of hyperactivity, impulsivity and/or inattention is commensurate with his or her devel-opmental level.
Psycho-educational assessments. Psycho-educational assessment can provide unique information to the diagnostic process as it provides information related to problems that can be either associated with AD/HD or that might serve as alternative explanations for the symptoms. For example, in some cases comorbid learning (Barkley, 1998; Barry, Lyman, & Klinger, 2002), language (Barkley, 1998; Cohen et al., 2000; Riccio & Jemison, 1998) and processing (Bedard, Martinussen, Ickowicz, & Tannock, 2004) disorders may best account for the behaviors often associated with AD/HD. Consequently, some have recommended tests of academic achievement and other measures that assess these abilities be a part of the diagnostic process (Selikowitz, 2004).
Neuropsychological assessments. Some sources reviewed suggested neuropsychological tests to be sensitive to aberrant cognitive processes associated with AD/HD (e.g., inattention and impulsive response patterns; Dige & Wik, 2005; Kaplan & Stevens, 2002). The neuropsychological evaluation may also contribute to understanding children with attentional difficulties who do not meet DSM-IV-TR criterion for a diagnosis of AD/HD (Baron, 2004).
Research has offered some support for the sensitivity of certain neuropsychological tests as measures of attention skills (Roth & Saykin, 2004). For example, measures such as the Wide Range Assessment of Memory and Learning, Second Edition (WRAML 2; Sheslow & Adams, 2003), the California Verbal Learning Test, Children’s Version (CVLT-C; Delis, Kramer, Kaplan, Ober, & Fridlund, 1998), and the Wisconsin Card Sorting Test (WCST; Heaton, Chelune, Talley, Kay, & Curtis, 1993) have been suggested to be sensitive to neuropsychological functions including attention span, sustained attention, both single- and repeated-trial learning, response inhibition, and working memory. In addition, individually adminis-tered assessment batteries designed specifically to measure executive functions related to AD/HD have recently been developed. These include the Delis Kaplan Executive Functioning System (DKEFS; Delis, Kaplan, & Kramer, 2001) and the Test of Everyday Attention for Children (TEA-Ch; Manly, Robertson, Anderson, & Nimmo-Smith, 1999). These tools are designed to measure functions associated with AD/HD, such as sustained attention and vigilance and response inhibition.
Computerized neuropsychological assessments designed to evaluate specific aspects of AD/HD were also recommended by some of the sources reviewed. Among these are the Conners’ Continuous Perfor-mance Test (Conners, 2000), the Test of Variables of Attention (TOVA; Greenberg, Corman, & Kindschi, 2001), and the Gordon Diagnostic System (Gordon, McClure, & Aylward, 1996). These tools purport to evaluate a child’s vigilance and sustained attention using computerized formats and are commonly used in evaluation of suspected AD/HD. These measures of sustained attention typically require a child to listen to or look at a series of numbers or letters and respond (often by pressing a button whenever certain stimuli or pairs of stimuli are presented). Scores are usually calculated according to correct responses, errors of omission (correct answers that were overlooked by the child), and errors of commission (incor-rect answers that were selected by the child).
While neuropsychological testing has been advocated by some to be an important part of the AD/
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1284
HD diagnostic process, it is important to acknowledge that the use of these tests as part of the assessment and diagnostic process is controversial. Because the sensitivity and specificity of neuropsychological measures has been brought into question, they should not be utilized in isolation (Barkley, 1998; Doyle et al., 2000; McGee, Clark, & Symons, 2000). To date researchers suggest that neuropsychological assessment tools cannot accurately differentiate between subtypes of AD/HD (Geurts, Verté, Oosterlaan, Roeyers, & Sergeant, 2005), although they have been reported to effectively distinguish AD/HD children from those with other diagnoses (Dunn & Kronenberger, 2003).
Direct Behavioral observation
As part of the assessment and diagnosis of AD/HD, direct observations are frequently recom-mended, with 68% of the sources reviewed for this paper endorsing their use. Direct observation is typi-cally conducted by either mental health or educational professionals and frequently occurs in the school setting. They are designed to compliment rating scale and clinical interview data (Parker, 1992), as well as to assess interpersonal and social skills (Hinshaw, 1994).
Despite its relatively high cost (when compared to rating scales and interviews), direct observation of behavior is often recommended because of its importance to the differential diagnosis of AD/HD (Anastopoulos & Shelton, 2001). In fact, Barkley (1990) asserted that observations of student behavior is “…likely to prove as useful as (or more useful than) any other sources of information in the evalu-ation, because they directly assess the actual AD/HD symptoms of concern to the child’s teacher” (p. 339). However, in the 2006 edition of his book, Attention Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, Barkley argues that formal behavioral coding is not practical. He states, “Although a number of studies support the benefit of incorporating structured classroom observations into the diagnostic process, they are not enough to justify the considerable cost and effort they involve” (p. 383). However, it is important to acknowledge that Barkley is a clinician and not a school-based professional. Unlike most clinical psychologists, the school psychologist has easy access to this impor-tant data source. Thus, his criticism of the use of direct behavioral observation may not be applicable to the school psychologist.
If a behavioral observation is included in the AD/HD diagnostic process, it may be informal and unsystematic, or formal and systematic. When conducting a behavioral observation in a natural setting, such as the child’s classroom, formal procedures include defining behaviors of concern, observing them at regular intervals (e.g., internal time sampling procedures), calculating the rate of a behavior, and comparing these rates to those of non-referred peers. Formal structured coding systems have been devel-oped. For example, the BASC offers a paper-and-pencil and a Portable Observation Program (Reynolds & Kamphaus, 2004).
Tempering the possible utility of direct behavioral observations is the finding that direct behavioral observation has been shown to be highly correlated with teacher behavior rating scale data. Given this finding, it has been argued by some clinicians that this assessment technique often does not provide unique assessment data (Lett & Kamphaus, 1997), and given its relatively high cost may not be neces-sary in all cases. However, it should be acknowledged that behavioral observations are an important diagnostic strategy for confirming the AD/HD diagnosis and monitoring AD/HD symptoms, and given that they are readily accessible to the school psychologist, they should be employed whenever possible.
The California School Psychologist, 2007, Vol. 12 8�
Medical Evaluations
A medical evaluation was recommended as a component of the AD/HD diagnostic process in 34% of the sources reviewed for this paper. In fact, some authors have argued that the “best person to make a diagnosis is a specialist pediatrician with an interest and expertise” in the area (Selikowitz, 2004, p. 123). Others, however, have noted that a medical evaluation is by itself inadequate to diagnose AD/HD (Barkley, 1990) and that: “Routine physical examinations of children with ADHD frequently indicate no physical problems and are of little help in diagnosing the condition or suggesting its management” (Barkley, 2006, p. 360). Perhaps most importantly, the findings of a medical evaluation can support the diagnostic process, particularly by providing information important to differential diagnosis by ruling out those relatively rare medical conditions that may be the cause of the AD/HD-like symptoms such as pinworms and absence seizures (Anastopoulos & Shelton, 2003; Robin, 1998).
When employed in the diagnostic process, the medical evaluation commonly includes a medical interview and a physical examination. The physician typically assesses for genetic syndromes, neuro-logical abnormalities, gross sensory motor, hearing, vision, and physical impairments (Robin, 1998; Selikowitz, 2004). It has been suggested that the medical examination is especially critical for children with histories of a seizure disorder. Approximately 30% of children with a seizure disorder develop AD/HD, or have its symptoms worsened with anticonvulsants, such as Dilantin or Phenobarbital (Wolf & Forsythe, 1978). Furthermore, research investigations indicate that children with AD/HD demonstrate differential brain wave patterns as compared to control subjects (Clarke et al., 2003; Lazzaro, Gordon, Whitmont, Meares, & Clarke, 2001), and this difference can be detected using electrophysiological assessment procedures. Given these findings and the significant number of children with seizure disor-ders who also have AD/HD, it is not surprising that electrophysiological measures (e.g., EEG) are among the most commonly utilized medical testing procedures in the diagnostic assessment of AD/HD (Loo & Barkley, 2005).
Although a higher rate of AD/HD is not observed among children with asthma (Daly, Biederman, & Bostic, 1996), commonly prescribed asthma medications are reported to affect attention span and may exacerbate a preexisting case of AD/HD (Barkley, 1990; Parker, 1992). Furthermore, Albuterol, a commonly used inhalant medication for asthma, can cause side effects such as increased heart rate, tremor, and nervousness, which may be confused with AD/HD symptoms (Robinson & Geddes, 1996)
Diagnostic imaging. The use of diagnostic imaging (e.g., PET [positron emission tomography] scans, CAT [computed axial tomography] scans, MRIs [magnetic resonance images]) has increased in recent years, although it remains controversial. None of the sources meeting literature review search criteria recommended the use of these techniques as part of the diagnostic evaluation. However, another paper that addressed “executive dysfunction” was located that did identify neuroimaging techniques as a part of their recommended AD/HD diagnostic process (Roth & Saykin, 2004). Some experts, such as Robin (1998), have argued that “there is no evidence for the utility” for PET scans, CAT scans, MRIs, regular or enhanced EEGs in routine clinical assessments (p. 86). Many of the studies using neuroimaging tech-niques in the assessment and diagnosis of AD/HD have utilized very small samples and, therefore, have limited generalizability. However, some researchers have suggested these measures to have the ability to differentiate between AD/HD and non-AD/HD children (Kim, Lee, Shin, Cho, & Lee, D.S., 2002; Kim, Lee, Cho, & Lee, 2001; Rubia et al., 1999).
From the findings mentioned above, it is not surprising that diagnostic imaging techniques, such as MRI, CAT scans, and PET scans, are rarely used in clinical diagnoses. However, they have provided important insights into the brain of the child with AD/HD. For example, MRI studies demonstrate differ-
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 128�
ential activation of the left and right prefrontal cortex, left anterior cingulate, basal ganglia, and cere-bellum on tasks that require selective attention (Roth, & Saykin, 2004; Schulz et al., 2005; Willis & Weiler, 2005). Similarly, PET scans have indicated differential neurotransmitter and receptor binding in the brains of AD/HD children (Jucaite, Fernell, Halldin, Forssberg, & Farde, 2005).
Review of School Records
Examination of school records was also suggested by this literature review to be helpful in the diagnosis of AD/HD, with 24% of the sources reviewed for this paper endorsing their use. Given that the DSM-IV-TR (APA, 2000) diagnostic criteria require symptom onset to occur prior to the age of 7, it is likely the impulse control, hyperactivity, and attention difficulties of children will be documented throughout their school careers. Review of school records, including report cards and disciplinary histo-ries, may yield information regarding when symptoms were first observed and their severity across time (Brock, 1999). Additionally, they can provide information related to a child’s work habits, task comple-tion, and academic functioning.
Peer Assessments
Peer nominations and peer ratings are another set of procedures suggested by three sources (7% of the sources reviewed) to be useful in the diagnosis of AD/HD. The utility of these procedures is based upon the well-documented social difficulties experience by AD/HD children (Whalen & Henker, 1985) and that the severity of these difficulties is an indicator of later adolescent and adult adjustment (Hinshaw, 1994; Weiss & Hechtman, 1986). Peer nominations typically require children to nominate those classmates whom they like the most, and those whom they like the least. Atkins and Pelham (1991) report that AD/HD children are usually rated as less popular and more disliked then children without this disorder. Peer ratings, on the other hand, obtain from classmates information regarding specific behaviors that lead to rejections, neglect, and popularity. Regarding these procedures, Schaughency and Rothlind (1991) suggest that “. . . peers are able to identify attention problems among their classmates who are referred for adjustment difficulties and to differentiate among their classmates who are referred for adjustment difficulties and to differentiate among the externalizing behavior problems of their class-mates” (p. 196).
ConCLuDIng CoMMEnTS: IMPLICATIonS foR ThE SChooL PSYChoLogIST
No one diagnostic procedure, or set of procedures, has been identified that will diagnose AD/HD with perfect reliability. The diagnosis of this disorder is complicated due to the nature of its symp-toms, many of which can be attributed to other psychiatric disorders observed in childhood; and among younger children, to be similar to normative developmental behavior. Given the challenges of making an accurate differential diagnosis of AD/HD, the importance of working with a multidisciplinary team of medical and educational professionals, along with the family, the teacher, and the referred child should be clear.
As discussed at the beginning of this paper there are important legal reasons for the school psycholo-gist being involved in AD/HD diagnoses (i.e., the combination of child find regulations and requirements that children be assessed in all areas of suspected disability). However, from this literature review it should be clear that in addition to these legal motivations, there are also practical reasons for the school

The California School Psychologist, 2007, Vol. 12 87
psychologist being an important part of the AD/HD diagnosis. Specifically, there is no one mental health professional that has more access to the multiple information sources and diagnostic procedures (i.e., rating scales; parent, teacher, and student interviews, psychological testing, and behavioral observations) considered to be required for an AD/HD diagnosis. For example, the classroom observational data that some working in clinical practice (e.g., Barkley, 2006) have come to argue are too costly to include in the standard diagnostic process, are readily accessible to the school psychologist.
While the diagnosis of AD/HD is complicated and perfect diagnostic reliability has yet to be obtained, from this review of the literature it is clear that there is significant consensus among authori-ties in the field regarding what the comprehensive evaluation of the child suspected to have AD/HD should involve. Specifically, it would appear that rating scales, interviews, psychological testing, and behavioral observations are the most commonly recommended procedures. Awareness of this consensus can not only help to guide practice, but can also be used to support the ability of the school psychologist to make this diagnosis. Specifically, it is clear that not only do school psychologists have ready access to the most frequently recommended diagnostic elements, but they also have as a part of their standard pre-service preparation training in the use of these techniques (i.e., how to use rating scales, conduct interviews, administer and interpret psychological tests, and conduct behavioral observations). Thus, given the appropriate supervised practice, it is argued that the school psychologist is well positioned to assist in the AD/HD diagnosis. At the very least, knowledge of the consensus regarding elements of the AD/HD diagnosis will be indispensable when evaluating the adequacy of the many students who present to their school psychologists with AD/HD diagnoses made by other (typically non-school based) health and mental health professionals. It is hoped that this paper has provided information that will assist these school psychologist in critically evaluating these independent AD/HD diagnostic assessments.
REfEREnCES
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VT, University of Vermont, Research Center for Children, Youth, & Families.
American Academy of Pediatrics. (2000). Clinical practice guideline: Diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. Pediatrics, 105, 1158-1170.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Rev.). Washington, DC: Author.
Anastopoulos, A., & Shelton, T. (2001). Assessing attention-deficit/hyperactivity disorder. New York: Kluwer Academic/Plenum Publishers.
Atkins, M. S., & Pelham, W. E. (1991). School-based assessment of attention deficit-hyperactivity disorder. Journal of Learning Disabilities, 24, 197-204.
Barkley, R. A. (1990). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Press.
Barkley, R. A. (1991). Diagnosis and assessment of attention deficit-hyperactivity disorder. Comprehensive Mental Health Care, 1, 27-43.
Barkley, R. A. (1997a). ADHD and the nature of self-control. New York: Guilford Press.Barkley, R. A. (1997b). Attention-deficit/hyperactivity disorder. In E. J. Marsh & L. G. Terdal (Eds.), Assessment of
childhood disorders (3rd ed., pp. 71-129). New York: Guilford Press.Barkley, R. A. (1998). Attention-deficit/hyperactivity disorder: A handbook for diagnosis and treatment (2nd ed.).
New York: Guilford Press. Barkley, R. A. (2006). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (3rd ed.).
New York: Guilford. Baron, I. S. (2004). Neuropsychological evaluation of the child. New York: Oxford University Press. Barry, T., Lyman, R., & Klinger, L. (2002). Academic underachievement and attention deficit/hyperactivity disorder:
The negative impact of symptom severity on school performance. Journal of School Psychology, 40, 259-283.
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1288
Bedard, A. C., Martinussen, R., Ickowicz, A., & Tannock, R. (2004). Methylphenidate improves visual-spatial memory in children with attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 260-268.
Brock, S. E. (1999) Diagnosis of attention-deficit/hyperactivity disorder (ADHD) in childhood. The California School Psychologist, 4, 18-29.
Brown, M. E. (2000). Diagnosis and treatment of children and adolescents with attention-deficit/hyperactivity disorder. Journal of Counseling & Development, 78, 195-203.
Burcham, B., & DeMers, S. T. (1995). Comprehensive assessment of children and youth with ADHD. Intervention in School and Clinic, 30, 211-220.
Burke, J. D., Loeber, R., & Lahey, B. B. (2001). Which aspects of ADHD are associated with tobacco use in early adolescence? Journal of Child Psychology & Psychiatry, 42, 493-502.
Campbell, S. B. (1990). Behavior problems in preschool children. New York: Guilford Press.Casat, C. D., Pearons, D. A., & Casat, J. P. (2001). Attention-deficit/hyperactivity disorder. In V. H. Booney & A.
Pumariega (Eds.), Clinical assessment of child and adolescent behavior (pp. 263-306). Hoboken, NJ: Wiley. Cipkala-Gaffin, J. A. (1998). Diagnosis and treatment of attention-deficit hyperactivity disorder. Perspectives in
Psychiatric Care, 34, 18-25. Clarke, A. R., Barry, R. J., McCarthy, R., Selikowitz, M., Clarke, D. C., & Croft, R. J. (2003). EEG activity in girls
with attention-deficit/hyperactivity disorder. Clinical Neurophysiology, 114, 319-328.Cohen, N. J., Vallance, D. D., Barwick, M., Im, N., Menna, R., Horodezky, N. B., & Isaacson, L. (2000). The
interface between ADHD and language impairment: An examination of language, achievement, and cognitive processing. Journal of Child Psychology & Psychiatry, 41, 353-362.
Conners, K. (1997). Conners’ Rating Scales –Revised. North Tonawanda, NY: Multi Health Systems. Conners, K. (2000). Conners’ Continuous Performance Test II. North Tonawanda, NY: Multi Health Systems.Daly, J. M., Biederman, J., & Bostic, J. Q. (1996). The relationship between childhood asthma and attention deficit
hyperactivity disorder: A review of the literature. Journal of Attention Disorder, 1, 31-40. Danckaerts, M., Heptinstall, E., Chadwick, O., & Taylor, E. (1999). Self report in attention-deficit and hyperactivity
disorder in adolescents. Psychopathology, 32, 81-92.Davila, R. R., Williams, M. L., & MacDonald, J. T. (1991, September 16). Memorandum to chief state school
officers re: Clarification of policy to address the needs of children with attention deficit disorders with general and/or special education. Washington, DC: U.S. Department of Education.
Delis, D., Kaplan, E., & Kramer, J. (2001). The Delis-Kaplan Executive Function System. San Antonio, TX: The Psychological Corporation.
Delis, D., Kramer, J., Kaplan, E., Ober, B., & Fridlund, A. (1998). California Verbal Learning Test, Children’s Version. San Antonio, TX: PsychCorp.
Detweiler, R., Hicks, A., & Hicks, M. (1999). A multi-modal approach to the assessment and management of ADHD. In P. Cooper & K. Bilton (Eds.), ADHD research, practice and opinion. London: Whurr.
Dige, N., & Wick, G. (2005). Adult attention deficit hyperactivity disorder identified by neuropsychological testing. International Journal of Neuroscience, 11, 1�9-183.
Doyle, A. E., Biederman, J., Seidman, L. J., Weber, W., & Faraone, S. V. (2000). Diagnostic efficiency of neuro-psychological test scores for discriminating boys with and without ADHD. Journal of Consulting Clinical Psychology, �8, 477-488.
Dunn, D., & Kronenberger, W. (2003). Attention-deficit/hyperactivity disorder in children and adolescents. Neuro-logic Clinics, 21, 933-940.
DuPaul, G. J., Guevremont, D. C., & Barkley, R. A. (1991). Attention deficit-hyperactivity disorder in adolescence: Critical assessment parameters. Clinical Psychology Review, 11, 231-245.
DuPaul, G. J., & Stoner, G. (1994). ADHD in the schools: Assessment and intervention strategies. New York: Guil-ford Press.
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., & Reid, R. (1998). ADHD rating scale-IV: Checklists, norms, and clinical interpretations. New York: Guilford Press.
Fischer, M., Barkley, R. A., Fletcher, K., & Smallish, L. (2002). The adolescent outcome of hyperactive children diagnosed by research criteria, II: Academic, attentional, and neuropsychological status. Journal of Consulting and Clinical Psychology, 58, 580-588.
Geurts, H. M., Verté, S., Oosterlaan, J., Roeyers, H., & Sergeant, J.A. (2005). ADHD subtypes: Do they differ in their executive functioning profile? Archives of Clinical Neuropsychology, 20, 457-477.
Gimpel, G. A., & Kuhn, B. R. (1998).Maternal report of attention deficit hyperactivity disorder symptoms in preschool children. Child: Care, Health, and Development, 2�, 163-175.

The California School Psychologist, 2007, Vol. 12 89
Gordon, M., McClure, F. D., & Aylward, G. P. (1996). The Gordon Diagnostic System. DeWitt, NY: GSI Publica-tions.
Greenberg, L. M., Corman, C. L., Kindschi, C. L. (2001). Test of Variables of Attention. Los Alamitos, CA: Universal Attention Disorders.
Guevremont, D. C., & Barkley, R. A. (1992). Attention deficit-hyperactivity disorder in children. In S. R. Hooper, G. W. Hynd, & R. E. Mattison (Eds.), Child psychopathology: Diagnostic criteria and clinical assessment (pp. 137-177). Hillsdale, NJ: Lawrence Erlbaum.
Guevremont, D. C., DuPaul, G. J., Barkley, R. A. (1990). Diagnosis and assessment of attention-deficit/hyperac-tivity disorder in children. Journal of School Psychology, 28, 51-78.
Hardy, E., Warmbrodt, L., & DeBasio, N. O. (2004). Diagnosis and treatment of children with attention deficit disorder. Clinical Excellence for Nurse Practioners, 8, 126-134.
Hart, E. L., Lahey, B. B., Loeber, R., & Hanson, K. S. (1994). Criterion validity of informants in the diagnosis of disruptive behavior disorders in children: A preliminary study. Journal of Consulting and Clinical Psychology, �2,410-414.
Heaton, R. K., Chelune, G. J., Talley, J. L., Kay, G.C., & Curtis, G. (1993). Wisconsin Card Sorting Test. Odessa, FL: Psychological Assessment Resources.
Hechtman, L. (2000). Assessment and diagnosis of attention-deficit/hyperactivity disorder. Child and Adolescent Psychiatric Clinics of North America, 9, 481-498.
Hinshaw, S. P. (1994). Attention deficits and hyperactivity in children. Thousand Oaks, CA: Sage.Hoff, K. E., Doepke, K., & Landau, S. (2002). Best practices in the assessment of children with attention deficit/
hyperactivity disorder: Linking assessment to intervention. In A. Thomas & J. Grimes (Eds.), Best practices in school psychology IV (pp. 1129-1150). Bethesda, MD: National Association of School Psychologists.
Holland, M. L., Gimpel, G. A., & Merrill, K. W. (2003). ADHD Symptoms Rating Scale. Lutz, FL: Psychological Assessment Resources.
Jucaite, A., Fernell, E., Halldin, C., Forssberg, H., & Farde, L. (2005). Reduced midbrain dopamine transporter binding in male adolescents with attention deficit/hyperactivity disorder: Association between striatal dopamine markers and motor hyperactivity. Biological Psychiatry, 57, 229-238.
Kaplan, R. F., & Stevens, M. C. (2002). A review of adult ADHD: A neuropsychological and neuroimaging perspec-tive, CSN Spectrum, 7, 355-362.
Kim, B. N., Lee, J. S., Cho, S. C., & Lee, D. S. (2001). Methylphenidate increased regional cerebral blood flow in subjects with attention-deficit/hyperactivity disorder. Yonsei Medical Journal, 42, 19-29.
Kim, B. N., Lee, J. S., Shin, M. S., Cho, S. C., & Lee, D. S. (2002). Regional cerebral perfusion abnormalities in attention deficit/hyperactivity disorder: Statistical parametric mapping analysis. European Archives of Psychi-atry and Clinical Neuroscience, 252, 219-225.
Landau, S., & Burcham, B. G. (1995). Best practices in the assessment of children with attention disorders. In A. Thomas & J. Grimes (Eds.), Best practices in school psychology – III (pp. 817-829). Washington, DC: National Association of School Psychologists.
Lazzaro, I., Gordon, E., Whitmont S., Meares, R., & Clarke, S. (2001). The modulation of late component event related potentials by pre-stimulus EEG theta activity in ADHD. International Journal of Neuroscience, 107, 247-264.
Leach, D. J., & Brewer, D. F. (2005). The assessment and diagnosis of attention deficit hyperactivity disorder (ADHD) in children. In R. F. Waugh (Ed.), Frontiers in educational psychology (pp. 281-307). Hauppauge, NY: Nova Science.
Learner, J. W., Lowenthal, B., & Learner, S. R. (1995). Attention deficit disorders: Assessment and teaching. Belmont, CA: Brooks/Cole.
Lett, N. J., & Kamphaus, R. W. (1997). Differential validity of the BASC Student Observation system and the BASC Teacher Rating Scale. Canadian Journal of School Psychology, 13, 1-14.
Levy, F., Hay, D., Bennett, K., & McStephen, M. (2004). Gender differences in ADHD subtype comorbidity. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 369-376.
Loo, S., & Barkley, R. (2005). Clinical utility of EEG in attention deficit hyperactivity disorder. Applied Neuropsy-chology, 12, 64-76.
Loughran, S. B. (2003). Agreement and stability of teacher rating scales for assessing ADHD preschoolers. Early Childhood Education Journal, 30, 247-253.
Manly, T., Robertson, I. H., Anderson, V., & Nimmo-Smith, I. (1999). The Test of Everyday Attention for Children. Bury St. Edmunds, UK: Thames Valley Test Company.
Martin, G. L. (2003). Current developments in the assessment of attention deficit hyperactivity disorder. Marriage & Family: A Christian Journal, �, 171-194.
Diagnosis of AD/HD in Childhood

The California School Psychologist, 2007, Vol. 1290
McGee, R. A., Clark, S. E., & Symons, D. K. (2000). Does the Conners’ Continuous Performance Test aid in ADHD diagnosis? Journal of Abnormal Child Psychology, 28, 415-424.
McGrath, A., Handwerk, M., Armstrong, K., Lucas, P., & Freman, C. (2004). The validity of the ADHD section of the Diagnostic Interview Schedule for Children. Behavior Modification, 28, 349-374.
Meyer, A. (1999). Attention-deficit/hyperactivity disorder: Diagnosis and treatment. In S. N. Madu, P. K. Baguma, & A. Pitz (Eds.), Cross-cultural dialogue on psychotherapy in Africa (pp. 86-98). Sovenga, South Africa: UNIN Press.
Miranda, A., Presentación, M. J., & Soriano, M. (2002). Effectiveness of a school-based multicomponent program for the treatment of children with ADHD. Journal of Learning Disabilities, 35, 546-562.
Mitsis, E., McKay, K., Schulz, K., Newcorn, J., & Halperin, J. (2000). Parent-teacher concordance for DSM-IV attention-deficit/hyperactivity disorder in a clinic-referred sample. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 308-313.
Molina, B. S. G., Pelham, W. E., Blumenthal, J., & Galiszewski, E. (1998). Agreement among teachers’ behavior ratings of adolescents with a history of attention deficit hyperactivity disorder. Journal of Clinical Child Psychology, 27, 330-339.
Molina, B. S., Smith, B. H., & Pelma, W. E. (2001). Factor structure and criterion validity of secondary school teacher ratings of ADHD and ODD. Journal of Abnormal Child Psychology, 29, 71-82.
Nahlik, J. (2004). Issues in the diagnosis of attention-deficit/hyperactivity disorder in adolescents. Clinical Pediat-rics, 43, 1-10.
Oesterheld, J. R., Shader, R. I., & Wender, P. H. (2003). Diagnosis and treatment of attention deficit hyperactivity disorder in youth and adults. In R. I. Shader (Ed.), Manual of psychiatric therapeutics (3rd ed., pp. 346-364). Philadelphia, PA: Lippincott Williams & Wilkins.
Parker, H. C. (1992). The ADD hyperactivity handbook for schools. Plantation, FL: Impact Publications.Pelham, W. E., Fabiano, G. A., & Massetti, G. M. (2005). Evidence-based assessment of attention deficit hyperac-
tivity disorder in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 34, 449-476. Power, T., Costigan, T., Eiraldi, R., & Leff, S. (2004). Variations in anxiety and depression as a function of ADHD
subtypes defined by DSM-IV: Do subtype differences exist or not? Journal of Abnormal Child Psychology, 32, 27-37.
Quinlan, D. M. (2000). Assessment of attention-deficit/hyperactivity disorder and comorbidities. In T. E. Brown (Ed.). Attention-deficit disorders and comorbidities in children, adolescents, and adults (pp. 455-507). Wash-ington, DC: American Psychiatric Publishing.
Quinn, P. O. (1997). Attention deficit disorder: Diagnosis and treatment from infancy to adulthood. New York: Brunner/Mazel.
Rapport, M. D. (1993). Attention deficit hyperactivity disorder. In T. H. Ollendick & M. Hersen (Eds.), Handbook of child and adolescent assessment (pp. 269-291). Needham Heights, MA: Allyn & Bacon.
Reynolds, C., & Kamphaus, R. (2004). Behavior Assessment System for Children (2nd ed.). Circle Pines, MN: Amer-ican Guidance Service.
Robin, A. L. (1998). ADHD in adolescents: Diagnosis and treatment. New York: Guilford Press. Robinson, D. S., & Geddes, D.M. (1996). Inhaled corticosteroids: Benefits and risks. Journal of Asthma, 33, 5-16Root, R., & Resnick, R. (2003). An update on the diagnosis and treatment of attention deficit/hyperactivity disorder
in children. Professional Psychology: Research & Practice, 34, 34-41.Roth, R., & Saykin, A. (2004). Executive dysfunction in attention-deficit/hyperactivity disorder: Cognitive and
neuroimaging findings. Psychiatric Clinics of North America, 27, 83-96. Riccio, C. A., & Jemison, S. J. (1998). ADHD and emergent literacy: Influence of language factors. Reading &
Writing Quarterly, 14, 43-59.Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S.C., Simmons, A., et al. (1999). Hypofrontality in
attention-deficit/hyperactivity disorder during higher-order motor control: A study with functional MRI. Amer-ican Journal of Psychiatry, 15�, 891-896.
Rucklidge, J. J., & Tannock, R. (2002). Validity of the Brown ADD Scales: An investigation in a predominantly inattentive ADHD adolescent sample with and without reading disabilities. Journal of Attention Disorders, 5, 155-164.
Schaughency, E. A., & Rothlind, J. (1991). Assessment and classification of attention deficit hyperactivity disorders. School Psychology Review, 20, 187-202.
Searight, H. R., Nahlik, J. E., & Campbell, D. C. (1995). Attention-deficit/hyperactivity disorder: Assessment, diag-nosis, and management. Journal of Family Practice, 40, 270-279.
Selikowitz, M. (2004). ADHD: The facts. Oxford: Oxford University Press. Shaffer, D., Fisher, P., Dulcan, M., Davies, M., Piacentini, J., Schwab-Stone, M., et al. (1996). The NIMH Diag-

The California School Psychologist, 2007, Vol. 12 91
nostic Interview Schedule for Children Version 2.3 (DISC-2.3): Description, acceptability, prevalence rates, and performance in the MECA Study. Journal of the American Academy of Child Adolescent Psychiatry, 35, 865-877.
Shelton, T. L., & Barkely, R. A. (1994). Critical issues in the assessment of attention deficit disorders in children. Topics in Language Disorder. Special Issue: ADD and its Relationship to Spoken and Written Language, 14, 26-41.
Shelton, T. L., & Barkley, R. A. (1995). The assessment and treatment of attention-deficit/hyperactivity disorder in children. In M. C. Roberts (Ed.), Handbook of pediatric psychology (2nd ed., pp. 633-654). New York: Guilford Press.
Sheslow, D. & Adams, W. (2003). Wide Range Assessment of Memory and Learning (2nd Ed.). Lutz, FL: Psycho-logical Assessment Resources.
Schulz, K., Tang, C., Fan, J., Marks, D., Newcorn, D., Cheung, A., & Halperin, M. (2005). Differential prefrontal cortex activation during inhibitory control in adolescents with and without childhood attention-deficit/hyperac-tivity disorder. Neuropsychology, 19, 390-402.
Shuck, S., & Crinella, F. (2005). Why children with ADHD do not have low IQs. Journal of Learning Disabilities, 38, 262-280.
Sliver, L. B. (1999). Attention-deficit/hyperactivity disorder: A clinical guide to diagnosis and treatment for health and mental health professionals (2nd ed.). Washington, DC: American Psychiatric Publishing.
Sliver, L. B. (2004). Attention-deficit/hyperactivity disorder: A clinical guide to diagnosis and treatment for health and mental health professionals (3rd ed.). Washington, DC: American Psychiatric Publishing.
Slomka, G. (1998). Attention deficit hyperactivity disorder. In P. J. Snyder & P. D. Nussbaum (Eds.), Clinical Neuropsychology: A pocket handbook for assessment (pp. 124-140). Washington, DC: American Psychological Association.
Smith, B. H., Pelham, W. E., Gnagy, E., Molina, B., & Evans, S. (2000). The reliability, validity, and unique contri-butions of self-report by adolescents receiving treatment for attention-deficit hyperactivity disorder. Journal of Consulting and Clinical Psychology, �8, 489-499.
Swanson, M. E., & Smith, T. E. (1996). Attention deficit hyperactivity disorder: Diagnosis and treatment. In D. K. Reid, W. P. Hresko, & H. L. Swanson (Eds.), Cognitive approaches to learning disabilities (3rd ed., pp. 113-151). Austin, TX: PRO-ED.
Volpe, R. J., DuPaul, G. J., Loney, J., & Salisbury, H. (1999). Alternative selection criteria for identifying children with ADHD: Observed behavior and self-reported internalizing symptoms. Journal of Behavioral Disorders, 7, 103-109.
Weiss, G., & Hechtman, L. T. (1986). Hyperactive children grown up. New York: Guilford.Wender, E. (2004). ADHD symptoms and parent-teacher agreement. Developmental and Behavioral Pediatrics, 25,
48-49. Whalen, C. K., & Henker, B. (1985). The social worlds of hyperactive (ADDH) children. Clinical Psychology
Review, 5, 447-478.Willis, W., & Weiler, M. (2005). Neural substrates of childhood attention deficit/hyperactivity disorder: Electroen-
cephalographic and magnetic resonance imaging evidence. Developmental Neuropsychology, 27, 135-182. Wolf, S. M., & Forsythe, A. (1978). Behavior disturbance, Phobarbital, and febrile seizures. Pediatrics, �1, 728-
731.Wolraich, M., Lambert, E. W., Bickman, L., Simmons, T., Doffing, M., & Worley, K., (2004). Assessing the impact
of parent and teacher agreement on diagnosing attention-deficit hyperactivity disorder. Developmental and Behavioral Pediatrics, 25, 41-47.
Wolraich, M. L., Wibbelsman, C. J., Brown, T. E., Evans, S. W., Gotlieb, E. M., Knight, J. R., Ross, E. C., Shubiner, H. H., Wender, E. H., & Wilens, T. (2005). Attention-deficit/hyperactivity disorder among adolescents: A review of the diagnosis, treatment, and clinical implications. Pediatrics, 115, 1734-1746.
Diagnosis of AD/HD in Childhood


93
Current Educational Practices in Classifying and Serving Students with obsessive-Compulsive Disorder
Gail B. Adams & Thomas J. Smith
Northern Illinois University
Sara E. Bolt Michigan State University
Patrick Nolten Illinois Indian Prairie School District 204
Current educational practices for classifying and serving students with mental health disorders such as obsessive-compulsive disorder (OCD) have been associated with specific problems. These include the stigma of labeling, misalignment of school-based categories (e.g., E/BD, OHI) with clinical diagnoses, and concerns regarding the provision of appropriate services to these students. In the present study, Illi-nois school psychologists completed a survey on current practices for classifying and serving students with a primary diagnosis of OCD. The results indicated that 0.7% of the students served by school psychologists had a primary diagnosis of OCD. The majority of these students (74.5%) were served under IDEA. Of the students receiving services under IDEA, 51.4% were classified under E/BD and 31.8% under OHI. Approximately two-thirds of the students with OCD (67.1%) were educated in less restrictive settings (e.g., regular classroom with or without resource/part-time special class). School psychologists’ comments suggested a pattern of ambiguity and uncertainty surrounding the appropri-ateness of IDEA categories for OCD, concerns regarding the stigma of labeling, and problems related to providing appropriate services to these students. Response-to-Intervention (RtI) as an alternative to current evaluation practices is proposed and recommendations for improving traditional categorical service delivery models when RtI is not implemented are provided.
Keywords: obsessive-compulsive disorder, mental disorders, emotional disturbance, behavioral disor-ders, other health impaired, labeling (of persons), school psychologists
Based on recent estimates, approximately one-fifth of all students have diagnosable mental disor-ders (Hoagwood & Johnson, 2003). One mental disorder that recently has appeared on the educational landscape is obsessive-compulsive disorder (OCD), an anxiety disorder characterized by the presence of obsessions and/or compulsions. Obsessions are recurring thoughts, ideas, images, or impulses that are inappropriate, intrusive, and produce considerable distress or anxiety. Compulsions, or rituals, are purposeful, repetitive, behaviors that individuals perform, either overtly or covertly (i.e., mentally), to relieve, prevent, or undo the anxiety or discomfort created by the obsessions, or to avert a feared situa-tion. The obsessions or compulsions are time consuming, cause substantial distress, or disrupt the indi-vidual’s academic, occupational, or social functioning (American Psychiatric Association [APA], 2000). Hence, a person with obsessions related to contamination may engage in washing and cleaning rituals for hours to reduce the anxiety precipitated by contamination fears. (The reader is referred to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision [DSM-IV-TR; APA, 2000] for more detailed information on OCD.)
National and international studies have yielded heterogeneous results with regard to prevalence
The California School Psychologist, Vol. 12, pp. 93 – 105, 2007Copyright 2007 California Association of School Psychologists
Please send correspondence regarding this manuscript to; Gail Adams, Ed.D.; Department of Teaching and Learning; Northern Illinois University; DeKalb, IL 60115 or e-mail [email protected]
The California School Psychologist, 2007, Vol. 1294
estimates of OCD in children and adolescents. Fontenelle, Mendlowicz, and Versiani (2006) reviewed numerous studies of OCD prevalence rates, including 16 studies of childhood OCD conducted between 1987 and 2003. The reviewers reported a wide range of OCD prevalence rates in children and adoles-cents (0.0%-4.0%). Potential explanations for this diversity include such variables as the population studied (e.g., mean age of participants) and methodological decisions (e.g., instrument selected to diag-nose OCD, parent vs. child report) (Fontenelle, et al.; Rapoport, Weissman, Narrow, Jensen, Lahey, & Canino, 2000). In half of these studies, however, reported prevalence rates ranged from 1.9% to 4.0%. Once thought to be rare, OCD now is considered “a common disorder in both adults and the young” (Riddle, 1998, p. 92). The prevalence of OCD and other clinical diagnoses among today’s children demands that school psychologists put into place procedures that promote access to effective mental health services for these students. Moreover, the link between mental health and optimal student learning outcomes is strong (Becker & Luthar, 2002), further highlighting the need for school psychologists to implement measures that enhance mental health among students.
Categorizing Students with Mental health Disorders
Under the current public education system, students with clinical diagnoses must undergo a separate educational evaluation process to determine whether they qualify for special education services due to their disabilities. This process can result in an educational disability category diagnosis that is much broader and less specific than the clinical diagnosis. For example, the DSM-IV-TR clearly articulates OCD as a disability category (APA, 2000); however, a student with OCD may qualify for educational services according to several broader categories such as emotional disorder, behavioral disorder, or other health impairment. Meeting the traditional legal requirements for proper educational identification and categorization of students tends to be a time-intensive process (Hosp & Reschly, 2002) and does not necessarily lead to improved intervention and outcomes among students (Carlburg & Kavale, 1980; Thurlow & Ysseldyke, 1982). Therefore, it remains questionable whether conventional school-based evaluation procedures enhance treatment selection and related outcomes among students with mental health problems. Because maladaptive behavior associated with OCD frequently occurs across a variety of settings (e.g., home, school, community) and involves clinical treatment (Piacentini, Bergman, Keller, & McCracken, 2003), collaboration between school psychologists and clinical psychologists may be particularly helpful in developing effective evaluation and treatment plans.
Another concern associated with categorical diagnoses is labeling, which may lead to a variety of negative outcomes. First, labels can create the perception that students within a given diagnostic category are more alike than different, causing those who work with them to neglect their individual needs and strengths (Bianco, 2005; Smith, 2003). Because students with clinical diagnoses exhibit an array of symptoms, as evidenced by the frequency with which comorbidity is present among these indi-viduals (APA, 2000), they may require a wide variety of treatment options. Second, stigma often is associated with disability labels, which not only may have a negative impact on an individual’s self-concept, but also may alter the responses of individuals who come into contact with a person who has a mental disability (Susman, 1994). Third, labels have been shown to reduce learning expectations for students with disabilities, which may have damaging effects on their actual achievement (Foster & Ysseldyke, 1976). Therefore, it is uncertain whether the perceived benefits of labels (e.g., facilitating efficient communication among individuals, providing services similar to those shown to be effective for students displaying comparable behavior; Gallagher, 1976) outweigh the potential drawbacks.

The California School Psychologist, 2007, Vol. 12 95Classifying And Serving Students With OCD
Categorizing Students with oCD
OCD can be an insidious disorder, interfering with all aspects of a young person’s functioning – social, behavioral, and academic (Adams, 2004; Adams, Waas, March, & Smith, 1994; Clarizio, 1991). In a seminal study that made use of parent and self-report measures to examine the psychosocial func-tioning of children and adolescents with OCD, Piacentini et al. (2003) found that among 151 children and adolescents with a primary diagnosis of OCD, almost 90% reported a significant problem in at least one area of functioning (school/academic, home/family, or social); close to half reported at least one significant problem in each of these three areas. Furthermore, 47% of parents and 44% of children reported that OCD caused significant problems in school/academic functioning. Overall, the two most significant OCD problems reported by parents and children alike were difficulties with concentrating on schoolwork and doing homework. Similarly, Sukhodolsky, do Rosario-Campus, Scahill, Katso-vich, & Pauls (2005) found that children and adolescents with OCD fared significantly more poorly than children in a control group on several measures of adaptive, family, and emotional functioning. In addition, youth with OCD performed significantly worse on the school competence scale of the Child Behavior Checklist than did comparison peers. Children and adolescents with OCD also are at risk for comorbid psychiatric disorders, including tic disorders, major depression, anxiety disorders (e.g., panic disorder), disruptive behavior disorders (attention-deficit/hyperactivity disorder [AD/HD] and opposi-tional defiant disorder), specific developmental disorders, and enuresis (Geller, 2006; Sukhodolsky et al., 2005; Zohar, 1999), further complicating the behavioral and academic functioning of these students. Because of the difficulties they experience in school, many children and adolescents with OCD require school-based accommodations and modifications and/or special education and related services to facilitate their educational functioning. In the past, some students have received accommodations and modifications via Section 504 of the Rehabilitation Act of 1973; others have gone through the traditional educational evaluation process and obtained special education and related services through the Indi-viduals with Disabilities Education Act (IDEA) (Adams, 2004). Students who have received services under IDEA frequently have been classified under the federal category of “Emotional Disturbance” (ED) (Adams, 2004). However, parents of children with OCD and other concerned individuals, including mental health professionals and educational experts in the field of OCD, increasingly have expressed serious reservations about the ED classification and concomitant label. Indeed, a number of researchers have advocated that children and adolescents with OCD be identified under the “Other Health Impaired” (OHI) category (Adams, 2004; Chansky, 2000; Dornbush & Pruitt, 1996).
Several arguments might be offered for such a reclassification. First, many are troubled by the stigma sometimes associated with the ED label (such terms as “Emotional/Behavioral Disorders,” or E/BD, may be used within various state systems; Muller & Markowitz, 2004) and the connotations it may invoke (Tourette Syndrome Association, 2006b). Particularly in cases where the media describe perpetrators of criminal and/or violent behavior as “emotionally disturbed,” parents or guardians of children with OCD may have serious and legitimate concerns when the same label is applied to their child. Second, OCD has a documented neurobiological basis, including a link to the neurotransmitter serotonin (APA, 2000; Blier, Habib, & Flament, 2006), suggesting that OCD has a physiological, rather than a behavioral or emotional, basis. Moreover, AD/HD and Tourette Syndrome (TS), two other neuro-biologically based disorders, are conditions listed under the IDEA “Other Health Impaired” category (34 C.F.R.§ 300.8[c][9][i]). During the reauthorization of IDEA in 1997, many individuals and organiza-tions (e.g., Children and Adults with Attention-Deficit/Hyperactivity Disorder, or CHADD) advocated vigorously that AD/HD be included under the Other Health Impaired category (CHADD of Alachua

The California School Psychologist, 2007, Vol. 129�
County, n.d.). In the final regulations enforcing Part B of IDEA 2004, Tourette Syndrome was listed as a disability under OHI rather than ED. Immediately after the release of the final regulations, the Tourette Syndrome Association (TSA) issued a public announcement entitled Major Victory for Children with Tourette Syndrome: Individuals with Disabilities Education Act to Classify Tourette Syndrome as Other Health Impaired (2006a). In its announcement, the TSA stated that “many educators…erroneously see TS as a behavioral or conduct disorder because of the nature of its symptoms and therefore classify these children under the Emotionally Disturbed (ED) category” (para. 9).
Finally, some individuals may be apprehensive about the ED label for students with OCD because of its potential ramifications for educational placement. As indicated earlier, labeling may create the perception that a particular treatment will be effective for most, if not all, students with a given label, and may lead to inappropriate decisions about how to address their individual needs (Bianco, 2005; Smith, 2003). One psychiatrist known for his work in childhood OCD expressed concern regarding students with OCD who are classified under ED and placed in self-contained classrooms for students with behavioral disorders. He noted that in some cases, the students with behavior disorders who exhibit externalizing, aggressive, acting out behaviors “…have a feeding frenzy at the expense of the kids with OCD. It can result in either withdrawal – sometimes out of school – or lashing back (often futility)” (A. J. Allen, personal communication, September 30, 2002).
Similarly, in its public announcement regarding the inclusion of TS under OHI in IDEA 2004, the Tourette Syndrome Association stated that classifying students with TS under the ED category “frequently results in students being placed in programs that are designed for students with emotional disorders where bullying and teasing generally increase, as does the punishment for their symptoms” (2006a, para. 9). Although a review of the literature yielded no information regarding the extent to which this phenomenon occurs for students with OCD, the potential for its existence raises serious concerns.
In sum, many of the previously cited problems related to educational practices for classifying and labeling students with mental health disorders, in general, have been associated with students who have OCD. These include the stigma linked to attaching the ED label to students with OCD, difficulties aligning a school-based category with a clinical diagnosis, and concerns regarding the provision of services to students with OCD. An understanding of current practices in identifying and classifying students with obsessive-compulsive disorder is essential to inform and advance best practices for serving these students. School psychologists, who play a crucial role in the identification and classification process, represent a key source of information regarding these practices. Yet none of the research that has appeared in the school psychology literature on childhood OCD since 1991 (Adams et al., 1994; Clarizio, 1991; McGough, Speier, & Cantwell, 1993; Sabuncuoglu & Berkem, 2006) has examined school psychologists’ experiences and perceptions related to school-based practices for identifying and categorizing students with a clinical diagnosis of OCD.
The purpose of the present investigation was to conduct descriptive research with school psycholo-gists in the state of Illinois first to determine how commonly childhood OCD is seen in educational settings and current patterns related to serving these students in school (e.g., 504, IDEA). Second, this study explored how students with a primary diagnosis of OCD served under IDEA are identified and categorized as well as school psychologists’ opinions of these practices. Finally, the types of educa-tional placements in which these students receive instruction were examined. To that end, the following research questions were posed:
1. What percentage of students evaluated or served by school psychologists have a primary diag-nosis of OCD?

The California School Psychologist, 2007, Vol. 12 97Classifying And Serving Students With OCD
2. Among students with a primary diagnosis of OCD, how many are served via 504 plans, and how many are served under IDEA?
3. Among students with a primary diagnosis of OCD who are served under IDEA, what is the disability category (e.g., E/BD, OHI) under which they are most frequently classified, and under which disability category do school psychologists believe these students should be classified?
4. Among students with a primary diagnosis of OCD who are served under IDEA, in which educa-tional settings are they placed (e.g., general education class, resource room)?
METhoD
Participants
To facilitate the selection of a suitable sample, a listing of the names and addresses of all school psychologists in the state of Illinois was acquired from the Illinois State Board of Education. From this list, a random sample of 400 names was chosen, using a computer-generated list of random numbers. Of the 400 individuals randomly selected, 123 school psychologists responded, for a response rate of 31%. Participants were recruited in accordance with the Institutional Review Board (IRB) from the first two authors’ institution, which approved the study as exempt from the Code of Federal Regulations for the protection of human subjects. All respondents were entered into a drawing for three U.S. Savings Bonds.
Instrumentation
To gather data relevant to the stated research questions, a survey was constructed that asked respon-dents to provide (1) numerical responses, e.g., “How many students have you evaluated and/or provided services for (including such services as consulting) this school year?”; (2) categorical responses, e.g., “In your opinion, students with a primary diagnosis of OCD should be served under…” (respondents marked one of several categories provided); and (3) short verbal responses, e.g., “If you marked ‘Strongly Disagree’ or ‘Disagree’ above, please explain.” For several items, respondents were asked to indicate the number of students with OCD who fit into each of three different severity categories. The severity levels were defined as follows:
Mild OCD: Slight interference with performance, but overall performance is not impaired Moderate OCD: Definite interference with performance, but still manageable Severe OCD: Substantial impairment in performanceThese definitions were adapted from the Yale-Brown Obsessive-Compulsive Scale (Goodman,
Price, Rasmussen, Mazure, Fleischman, Hill, et al., 1989), a scale that measures the severity of classic OCD symptoms.
Procedures
In April, 2003, a copy of the survey, two copies of the cover letter, and a self-addressed, stamped envelope were sent to the 400 randomly chosen school psychologists. Participants were asked to sign and return one copy of the cover letter along with the completed survey to indicate consent to participate in the study. Follow-up surveys were sent to those psychologists who did not respond after the initial mailing, and follow-up calls were made to individuals who did not respond to either mailing. Data were compiled and then analyzed using descriptive statistics.

The California School Psychologist, 2007, Vol. 1298
RESuLTS AnD DISCuSSIon
Research Question 1
The first research question addressed the percentage of students evaluated or served by school psychologists who had a primary diagnosis of OCD. Of the 12,685 students reported as being evaluated or served, 94 (0.7%) had a primary diagnosis of OCD. While this figure does not necessarily represent the incidence of primary OCD in the population of students at large, it is interesting to note that this statistic is identical to the one-year incidence rate suggested by the APA (0.7%) and relatively close to the 1%, one-year incidence rate established by Flament, Whitaker, Rapoport, Davies, Berg, Kalikow, et al. (1988). The results appear to confirm the assertion by Riddle (1998) that OCD is not a rare disorder among young people.
Research Question 2
Research question two addressed the percentage of students with a primary diagnosis of OCD served via 504 plans and the percentage served under IDEA. School psychologists reported that of the 94 students with a primary diagnosis of OCD, 12 (12.8%) received services under Section 504, 70 (74.5%) were served under IDEA, and the remaining 12 students (12.8%) were receiving no services. Acknowl-edging the role of OCD severity level, some respondents reported that when OCD symptoms were mild or well controlled by medication, no services or modifications were considered necessary.
As a point of interest, the relationship between OCD severity level and the type of services received (i.e., 504 or IDEA) also was examined using a chi-square test of independence. No significant relation-ship between severity level and the type of service received was found (x2 (2, N = 82) = 4.38, p = .11), and the effect size for this relationship was small (Cramer’s V = .23, with a small observed tendency for children with more severe OCD to be served under IDEA rather than 504). It is important to note, however, that because the large majority of students with a primary diagnosis of OCD in the current study were reported as being served under IDEA, it appears that the typical impact of OCD on educa-tional performance was deemed serious enough to warrant special education and related services.
Research Question 3
The first part of research question three addressed the disability category under which students with a primary diagnosis of OCD served under IDEA were classified. The category school psychologists most frequently reported was “E/BD” (51.4%), followed by “Other Health Impaired” (31.8%). The combina-tion category “E/BD or OHI” was less likely to be reported (10.3%), with “Other” and various combina-tion categories comprising only 6.5% of the responses. Thus, E/BD was the IDEA category under which the majority of students with a primary diagnosis of OCD were reported as being classified in the present study (see Table 1).
The second part of research question three was addressed by the survey item, “In your opinion, students with a primary diagnosis of OCD should be identified under the following IDEA category for the OCD…” (five categories were provided: Emotional/Behavioral Disorders, Learning Disabilities, Other Health Impaired, Other, or Need to create a new category under IDEA for these students). The obtained frequencies indicate that there was strong consistency between the category under which students with OCD were reported to be classified (Table 1) and school psychologists’ opinions of the most appropriate IDEA category for these students (Table 2). A small percentage of psychologists believed that fewer students should be classified under E/BD than actually were. Nonetheless, 47.7% of school psycholo-

The California School Psychologist, 2007, Vol. 12 99Classifying And Serving Students With OCD
gists selected E/BD as the most appropriate category for students with a primary diagnosis of OCD. Approximately 5.5% of the respondents reported that a new category is needed to classify students with OCD.
As a follow up to this question, respondents were asked to explain why they chose a particular IDEA category. Overall, two patterns emerged from an analysis of the school psychologists’ comments. First, psychologists expressed considerable disagreement as to which IDEA category was the most appropriate for these students. Those who viewed OCD as a social/emotional or behavior disorder chose the E/BD category for OCD. Others, who perceived OCD as medical/clinical in nature, believed OHI was the best fit. In certain cases, psychologists referred to the IDEA category definition to classify OCD. For example, some chose OHI on the basis of the “limited attention” component of the definition, while others chose E/BD because of the “inappropriate types of feelings or behavior under normal circumstances” clause of the ED definition. Still others referred to the relationship between OCD and the DSM-IV-TR. Ambiguity
TABLE 1. Frequency Distribution of Responses: Reported IDEA Disability Categories for Students with a Primary Diagnosis of OCD
Category Frequency Percent
E/BD 55 51.4%LD 0 0.0OHI 34 31.8Other 2 1.9E/BD or OHI 11 10.3LD and OHI 1 0.9E/BD and LD 3 2.8E/BD, OHI, and Other 1 0.9
Total 107 100.0
Note. E/BD=Emotional/Behavioral Disorder, LD = Learning Disability, OHI = Other Health Impaired
TABLE 2. Frequency Distribution of Responses: Psychologists’ Opinions of Appropriate IDEA Cate-gory for Students with a Primary Diagnosis of OCD
Category Frequency Percent
E/BD 52 47.7%LD 0 0.0OHI 35 32.1Other 2 1.8New category needed 6 5.5E/BD or OHI 12 11.0E/BD, OHI, and Other 1 0.9Other/new category needed 1 0.9
Total 109 100.0Note. E/BD=Emotional/Behavioral Disorder, LD = Learning Disability, OHI = Other Health Impaired

The California School Psychologist, 2007, Vol. 12100
and uncertainty surrounding the appropriate IDEA classification for OCD also appeared in the remarks of several respondents who chose “E/BD or OHI.” One of these psychologists stated, “I do not define it as an emotionally based disorder, and although it may be physiologically based, I have a hard time saying it is a health impairment...”
Overall, the results of the current study indicate that there is a clear lack of agreement among school psychologists with regard to the most appropriate school-based disability category for OCD. It may be that the students with a primary diagnosis of OCD in the present study represented a wide range of difficulties and comorbid disorders. Nonetheless, the psychologists’ varied responses to questions concerning the categorization of students with OCD seem to suggest that current training and guidance for evaluating and classifying OCD are inadequate.
A second pattern inherent in psychologists’ remarks regarding the most suitable educational cate-gory for OCD was concern regarding the stigma that may be associated with the ED label. A number of psychologists specifically alluded to the potentially negative impact of the ED label and parent prefer-ence for the OHI label. These results thus suggest that many of the problems that have been cited in the literature regarding educational practices for classifying and labeling students with mental health disor-ders also apply to students with the specific diagnosis of OCD.
Research Question 4
The final research question addressed the types of educational settings in which students with a primary diagnosis of OCD served under IDEA are placed. In one of the survey items, respondents were presented with a variety of educational placements and asked to indicate the number of students served within each of those settings. As is evident in Table 3, placements for students with OCD represent almost the full continuum of IDEA services. Of the 70 students served under IDEA, 47 (67.1%) were reported as receiving their instruction in less restrictive environments. More specifically, 10.0% were placed in full-time regular classrooms only, 11.4% received instruction in the regular classroom and part-time special classes, and a sizeable percentage (45.7%) received instruction in the regular classroom with part-time resource assistance.
Approximately 29% of the students with a primary diagnosis of OCD served under IDEA were educated in more restrictive settings. Of these students, 4.3%, 7.2%, and 5.7% were placed in LD, ED, and E/BD self-contained classrooms, respectively. An additional 11.4% received instruction in special day schools, and no students were placed in residential settings. Because there was only one residential school in the state of Illinois known to treat students with OCD at the time the survey was administered, this finding was not unexpected. As indicated in Table 3, 4.3% of students were reported as being served in placements designated as “Other.”
The results of this study indicate that the large majority of students with a primary diagnosis of OCD served under IDEA received instruction in regular classrooms, alone or in combination with resource services or part-time special classes. Hence, it appears that the IDEA provision of the least restrictive environment was a guiding principle in decisions related to educational placements for students with OCD.
Study Limitations and future Directions
A limitation of this investigation was that the results were based upon school psychologists’ reports of students on their caseloads who had a primary diagnosis of OCD. Formal clinical evaluations of the presence or absence of primary OCD among students using such standardized instruments as diagnostic

The California School Psychologist, 2007, Vol. 12 101
interviews may have yielded different results. Also, due to the self-selection nature of the sample, it is possible that school psychologists with a greater number of students with OCD on their caseloads were more likely to respond (although the majority of respondents reported having no students with OCD on their current caseloads). Future research could expand upon the results of the present study by obtaining data from a national sample of school psychologists. Future studies also might collect data on students who have OCD as either a primary or secondary diagnosis (only students with a primary diagnosis of OCD were included in the present investigation). It is important to note that, as the first of its kind to be conducted, this study is exploratory in nature. Additional research is necessary not only to confirm or refute the findings of this investigation, but also to gather information in such areas as actual services provided to students with OCD.
ConCLuSIonS/IMPLICATIonS foR SChooL PSYChoLogISTS
The results of this study strongly suggest that the difficulties encountered in current educational prac-tices for classifying and serving students with OCD mirror those associated with classifying and serving students with mental disorders, in general. The traditional educational evaluation process requires the identification of a particular categorical diagnosis for students with OCD – a process that is characterized by ambiguity and lack of agreement. Additionally, concerns exist regarding the stigma of the ED label for children and adolescents with OCD. Furthermore, because comorbidity among students with OCD is very common, these students require many different levels of support.
Although evidence from the present study as well as the existing OCD literature provide support for identifying students with OCD under the IDEA category of OHI (e.g., Adams, 2004), an alternative approach might better ensure that these students receive appropriate services. More specifically, the time
Classifying And Serving Students With OCD
TABLE 3. Frequency Distribution of Responses: Reported Educational Placements for Students with a Primary Diagnosis of OCD Served under IDEA
Placement Frequency Percent
FT regular classroom 7 10.0%Reg. class & PT resource rm 32 45.7Reg. class & PT spec.class 8 11.4
(Total) (47) (67.1)
FT self-contained LD 3 4.3FT self-contained ED 5 7.2FT self-contained BD 0 0.0FT self-contained E/BD 4 5.7FT self-contained OHI 0 0.0Special day school 8 11.4Residential setting 0 0.0
(Total) (20) (28.6)
Other 3 4.3
Grand Total 70 100.0Note. FT = Full time, PT = Part time, E/BD=Emotional/Behavioral Disorder, LD = Learning Disability, OHI = Other Health Impaired

The California School Psychologist, 2007, Vol. 12102
currently spent evaluating students with OCD to meet traditional legal requirements for proper educa-tional identification and categorization might be used more effectively to implement evaluation proce-dures to identify successful services and interventions for these students. Once such interventions are implemented, a heavy emphasis should be placed upon careful monitoring of service effectiveness over time to promote the most positive outcomes possible. Such procedures are beginning to be put into prac-tice for students with learning disabilities as a result of the Response-to-Intervention (RtI) focus within IDEA 2004. A related non-categorical model for service delivery has been developed and implemented in Iowa over the past decade, in which educational services for students with social-emotional problems are provided through a Response-to-Intervention framework within the school setting (see Grimes & Kurns, 2003). Similarly, Gresham (2005) supports RtI as an alternative method for identifying students as having an emotional disturbance, stating that the RtI method is in direct contrast to current practice, which is based on a “refer-test-place model in which students are not exposed to systematic, evidence-based interventions to ameliorate behavior problems” (Gresham, p. 341).
Application of a three-tier RtI model might encourage school systems to conduct universal screening for emotional and behavioral difficulties and implement intervention strategies that show promise for alleviating learning and behavior problems students with OCD frequently experience. Screening tools for detecting emotional and behavioral disorders are available but very infrequently used in school settings (Forness, Serna, Nielsen, Lambros, Hale, & Kavale, 2000). Prevention techniques such as teaching all students strategies for coping with anxiety (Merrell, 2001) and creating a positive and calm classroom environment (Lehr & Christiansen, 2002) might be incorporated as part of a first tier level of service provided to all students.
At the second tier, students with OCD whose symptoms interfere with learning and/or behavior could be brought to the attention of a school psychologist. The psychologist might conduct further assessment and collaborate with families and professionals outside the school to implement such empirically based interventions as teaching more advanced coping strategies, cognitive-behavioral therapy (Freeman et al., 2007), and/or pharmacotherapy treatment (Franklin, March, & Garcia, 2007). A psychologist in a clinical rather than educational setting may play the major role in implementing certain interventions for OCD (e.g., pharmacotherapy). Educational professionals, however, are instrumental in supporting and monitoring the effects of clinical interventions. If these strategies prove ineffective or are highly resource intensive (e.g., additional funding is needed to ensure that the student receives ongoing services to facilitate appropriate progress), an evaluation might be conducted to determine whether the student qualifies for special education services. The evaluation process might be part of a third tier of support provided to students with substantial needs. This evaluation may involve the implementation of interven-tion strategies that are very resource intensive (e.g., frequent therapy sessions, comprehensive behavior intervention plan) to identify the conditions under which the student is successful. If it is determined that the student requires such intervention strategies in order to make sufficient progress, he or she eventually may be provided those strategies on an ongoing basis using funding available through special education. Monitoring of progress over time would be essential to verify the efficacy of these interventions.
Within the three-tiered RtI model described above, interventions that are effective for a given indi-vidual are identified via the evaluation process, placing the focus on instructional needs rather than disability categorization (Grimes and Kurns, 2003). Instead of having to fit a particular disability cate-gory, a student may receive special education services based on the conditions under which he or she was found to be successful.
Although the RtI school psychology service delivery model for students with or at-risk for OCD

The California School Psychologist, 2007, Vol. 12 103Classifying And Serving Students With OCD
may be ideal for some school systems, others may not be capable of facilitating such change in the near future. Therefore, traditional categorical service delivery models may continue in many locations. The clear lack of agreement among school psychologists regarding an appropriate category for students with OCD observed in the present study suggests that there is a need for training and guidance with regard to evaluating and classifying OCD. Such training would help ensure that services provided through categorical service delivery models are tailored to meet individual student needs. By acquiring a basic understanding of conditions that may affect the learning and behavior of students with OCD, school psychologists would be in a position to inform the IEP team about services and settings that would lead to student success.
To ensure that students with OCD receive appropriate services, the potential consequences of cate-gorical diagnoses must be considered carefully. For example, a student with OCD may need substantial structure to avoid being overwhelmed by his or her thoughts and corresponding rituals. Such structure initially might be considered as being most easily facilitated in a self-contained setting. However, other students in that type of setting may engage in behaviors (e.g., teasing, joking) that have the potential to exacerbate the student’s obsessions and compulsions. Additionally, care should be taken to place students with OCD in a setting that optimizes access to services that address their needs. Within the evaluation process, consideration should be given to the students’ specific educational needs and how those can best be met within the existing categorical service delivery system.
In conclusion, the best treatment options and services for students with OCD might result when school psychologists, clinical psychologists, teachers, parents, and the students collaborate in the development of intervention and monitoring plans that can be carried out in clinical, home, and school settings. Additionally, these plans should be informed by research on effective services for students with OCD. To that end, the following recommendations for best practice with regard to OCD interventions are proposed:
(1) Focus on implementing preventative interventions prior to considering 504 or IDEA eligi-bility, which should include a heavy emphasis on educating teachers, psychologists, and other school personnel about OCD. Such strategies as teaching all students techniques for coping with anxiety, holding clear classroom structure and expectations, and creating a generally calm classroom climate may prevent OCD from inhibiting a student’s learning in school (Paige, 2004);
(2) Collaborate with clinical psychologists, parents, teachers and students to design and implement interventions that are aligned across the settings in which a child is engaged;
(3) Collaborate with clinical psychologists to find and implement interventions with empirical support such as cognitive behavior therapy (Freeman et al., 2007) and pharmacotherapy, including selective serotonin reuptake inhibitors (Franklin et al., 2007), to address behaviors that interfere with academic achievement and/or social functioning;
(4) Emphasize program content and relevant goals, i.e., focus on identifying measurable, relevant goals; and
(5) Emphasize progress monitoring and evaluation of student outcomes, which may include assis-tance with monitoring a student’s response to medication (Volpe, Heick, & Guerasko-Moore, 2005).
School psychologists can play a vital role in creating, implementing, and monitoring school-based interventions for children and adolescents with OCD that ultimately will promote mental health and learning outcomes for these students.

The California School Psychologist, 2007, Vol. 12104
REfEREnCES
Adams, G. B. (2004). Identifying, assessing, and treating obsessive-compulsive disorder in school-aged children: The role of school personnel. Teaching Exceptional Children, 37(2), 46-53.
Adams, G. B., Waas, G. A., March, J. S., & Smith, M C. (1994). Obsessive-compulsive disorder in children and adolescents: The role of the school psychologist in identification, assessment, and treatment. School Psychology Quarterly, 9(4), 274-294.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revi-sion). Washington, DC: Author.
Becker, B., & Luthar, S. (2002). Social-emotional factors affecting achievement outcomes among disadvantaged students: Closing the achievement gap. Educational Psychologist, 37, 197-214.
Bianco, M. (2005). The effects of disability label and special education and general education teachers’ referrals for gifted programs. Learning Disability Quarterly, 28, 285-293.
Blier, P., Habib, R., & Flament, M. F. (2006). Pharmacotherapies in the management of obsessive-compulsive disorder. Canadian Journal of Psychiatry, 51(7), 417-430.
Carlburg, C., & Kavale, K. (1980). The efficacy of special versus regular class placement for exceptional children: A meta-analysis. Journal of Special Education, 14, 295-309.
CHADD of Alachua County (n.d.). Welcome to CHADD—Information. Retrieved March 22, 2007, from http://ourworld.cs.com/alachuachadd/
Chansky, T. E. (2000). Freeing your child from Obsessive-Compulsive Disorder. New York: Crown Publishers Crown Publishers.
Clarizio, H. F. (1991). Obsessive-compulsive disorder: The secretive syndrome. Psychology in the Schools, 28(2), 106-115.
Dornbush, M. P., & Pruitt, S. K. (1996). Teaching the tiger. Duarte, CA: Hope Press.Flament, M. F., Whitaker, A., Rapoport, J. L., Davies, M., Berg, C. Z., Kalikow, K. et al. (1988). Obsessive compul-
sive disorder in adolescence: An epidemiological study. Journal of the American Academy of Child and Adoles-cent Psychiatry, 27(6), 764-771.
Fontenelle, L. F., Mendlowicz, M. V., & Versiani, M. (2006). The descriptive epidemiology of obsessive-compulsive disorder. Progress in Neuro-Psychopharmacology & Biological Psychiatry 30, 327-337.
Forness, S., Serna, L., Nielsen, E., Lambros, K., Hale, M., & Kavale, K. (2000). A model for early detection and primary prevention of emotional and behavioral disorders. Education and Treatment of Children, 23, 325-345.
Foster, G., & Ysseldyke, J. (1976). Expectancy and halo effects as a result of artificially induced teacher bias. Contemporary Educational Psychology, 1, 37-45.
Franklin, M. E., March, J. S., & Garcia, A. (2007). Treating obsessive-compulsive disorder in children and adoles-cents. In M. M. Antony, C. Purdon, & L. Summerfeldt (Eds.) Psychological treatment of obsessive-compulsive disorders: Fundamentals and beyond. (pp. 253-266). Washington, DC: American Psychological Association.
Freeman, J. B., Choate-Summer, M. L., Moore, P. S., Garcia, A. M., Sapyta, J. J., Leonard, H.L., et al. (2007). Cognitive-behavioral treatment for young children with obsessive compulsive disorder. Biological Psychiatry, �1, 337-343.
Gallagher, J. J. (1976). The sacred and profane uses of labeling. Mental Retardation, 14, 3-7. Geller, D. A. (2006). Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatric Clinics
of North America, 29, 353-370Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischman, R. L., Hill, C. L., et al. (1989). The Yale-
Brown obsessive-compulsive scale: I. Development, use and reliability. Archives of General Psychiatry, 4�(11), 1006-1011.
Gresham, F. M. (2005). Response to intervention (RTI): An alternative means of identifying students as emotionally disturbed. Education and Treatment of Children, 28, 328-344.
Grimes J., & Kurns, S. (2003, December). An intervention-based system for addressing NCLB and IDEA expecta-tions: A multiple tiered model to ensure every child learns. Paper presented at the National Research Center on Learning Disabilities Responsiveness-to-Intervention Symposium, Kansas City, MO.
Hoagwood, K., & Johnson, J. (2003). School psychology: A public health framework: I. From evidence-based poli-cies. Journal of School Psychology, 41, 3-21.
Hosp, J., & Reschly, D. (2002). Regional differences in school psychology practice. School Psychology Review, 31, 11-29.
Lehr, C., & Christensen, S. (2002). Best practices in promoting a positive school climate. In A. Thomas & J. Grimes (Eds.) Best practices in school psychology IV (pp. 929-948). Bethesda, MD: National Association of School Psychologists.

The California School Psychologist, 2007, Vol. 12 105Classifying And Serving Students With OCD
McGough, J. J., Speier, P. L., & Cantwell, D. P. (1993). Obsessive-compulsive disorder in children and adolescents. School Psychology Review, 22, 243-251.
Merrell, K. (2001). Helping students overcome depression and anxiety: A practical guide. New York: Guilford Publications.
Muller, E., & Markowitz, J. (2004). Disability categories: State terminology, definitions, and eligibility criteria. Alexandria, VA: National Association of State Directors of Special Education. Retrieved on March 17, 2007 from http://www.ecs.org/html/offsite.asp?document=http%3A%2F%2Fwww%2Enasdse%2Eorg%2Fpublications%2Fdisability%5Fcategories%2Epdf +.
Paige, L. Z. (2004). Obsessive-compulsive disorder: Information for parents and educators. In A. Canter, L. Paige, M. Roth, I. Romero, and S. Carroll (Eds.), Helping children at home and school II: Handouts for families and educators. Bethesda, MD: National Association of School Psychologists.
Piacentini, J., Bergman, R. L., Keller, M., & McCracken, J. (2003). Functional impairment in children and adoles-cents with obsessive-compulsive disorder. Journal of Child and Adolescent Psychopharmacology, 13(Suppl. 1), S61-S69.
Rapoport, J. L., Weissman, M. M., Narrow, W. E., Jensen, P. S., Lahey, B. B., & Canino, G. (2000). Childhood obsessive-compulsive disorder in the NIMH MECA study: Parent versus child identification of cases. Journal of Anxiety Disorders, 14(6), 535-548.
Riddle, M. (1998). Obsessive-compulsive disorder in children and adolescents. British Journal of Psychiatry, 173(Suppl. 35), 91-96.
Sabuncuoglu, O., & Berkem, M. (2006). The presentation of childhood obsessive-compulsive disorder across home and school settings: A preliminary report. School Psychology International, 27, 248-256.
Smith, V. (2003). You have to learn who comes with the disability: Students’ reflections on service learning experi-ences with peers labeled with disabilities. Research and Practice for Persons with Severe Disabilities, 28(2), 79-90.
Sukhodolsky, D. G., do Rosario-Campus, M. C., Scahill, L., Katsovich, L., Pauls, D. L., Peterson, B. S., et al. (2005). Adaptive, emotional, and family functioning of children with obsessive-compulsive disorder and comorbid attention deficit hyperactivity disorder. American Journal of Psychiatry, 1�2(6), 1125-1132.
Susman, J. (1994). Disability, stigma and deviance. Social Science and Medicine, 38, 15-22. Thurlow, M. L., & Ysseldyke, J. E. (1982). Instructional planning: Information collected by school psychologists vs.
information considered useful by teachers. Journal of School Psychology, 20, 3-10. Tourette Syndrome Association (2006a, August 3). Major victory for children with Tourette Syndrome: Individuals
with Disabilities Education Act to classify Tourette Syndrome as Other Health Impaired. Retrieved August 31, 2006, from http://www.tsa-usa.org/news/TOURETTEOHI0806.htm.
Tourette Syndrome Association (2006b, Fall). What’s in a name? A lot if the name is a label used by a school. Tourette Syndrome Association, Inc. Newsletter, 34(3), Insert, p. 2.
Volpe, R. J., Heick, P. F., & Guerasko-Moore, D. (2005). An agile behavioral model for monitoring the effects of stimulant medication in school settings. Psychology in the Schools, 42, 509-523.
Zohar, A. H. (1999). The epidemiology of obsessive-compulsive disorder in children and adolescents. Child and Adolescent Psychiatric Clinics of North America, 8(3), 445-460.


107
Developing Emotional Competence in Preschoolers: A Review of Regulation Research
and Recommendations for PracticeRenée M. Tobin
Illinois State University
Frank J. Sansosti Kent State University
Laura Lee McIntyre Syracuse University
Regulation has been implicated in the development of emotional and behavioral disorders in child-hood. Indeed, emotion dysregulation is one of the most common reasons families seek psychological services and behavioral supports. Interventions to support children with regulatory difficulties may be enhanced if they are informed by basic psychological research on the topic. This paper includes a review of basic regulation research conducted over the last 20 years. This research base about the positive development of regulatory skills is then related to the treatment of emotion regulation deficits, emphasizing the role that school psychologists and school-based interventions may play in supporting appropriate regulatory strategies for young children.
Keywords: emotion regulation, early childhood development, emotional competence, emotional development, emotional control, emotion
One of the most common reasons for seeking childhood psychological services is difficulty with emotion regulation (Linscott & DiGiuseppe, 1994). Katz and Gottman (1995) define emotion regulation as “children’s ability to deal with having a strong negative or positive emotion and organize themselves in the service of an externally imposed goal” (p. 84). That is, the practice of recognizing emotions and developing the skills needed to manage reactions to them. Although emotion regulation deficits are not considered a disorder in their own right, they often are associated with a host of disorders across early ages. When children receive treatment for emotion regulation deficits, it typically is provided within the context of treatment for behavioral disorders (e.g., Oppositional Defiant Disorder, Conduct Disorder), mood disorders (e.g., Major Depressive Disorder), anxiety disorders (e.g., Separation Anxiety Disorder, Generalized Anxiety Disorder), or other disorders of childhood.
Over the last 20 years, basic research on the topic of emotion regulation has increased significantly (Eisenberg, 2002). Despite an overall increase in the amount of research available from various fields of psychology (e.g., clinical, social), there currently is a paucity of applied literature that draws on this basic research base to inform treatment and intervention development for children with emotion regula-tion issues. Thus, a review of basic research may help provide useful information for school psycholo-gists responsible for developing appropriate interventions to support children with disorders related to emotion dysregulation (Eisenberg, Fabes, Guthrie et al., 1996).
According to Thompson (1994), “Emotion regulation consists of the extrinsic and intrinsic processes
Please address all correspondence to Renée M. Tobin, Ph.D., Campus Box 4620, Psychology Department, Illinois State University, Normal, IL 61790-4620.
The California School Psychologist, Vol. 12, pp. 107 – 120, 2007Copyright 2007 California Association of School Psychologists

The California School Psychologist, 2007, Vol. 12108
responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish their goals” (pp. 27-28). A host of psychological systems are thought to be regulated, and a subset of these are assumed to become self-regulating as part of normal development. These systems include control of emotions, reactions to failure and disappointment, and most forms of moral and achievement activities. Indeed, when certain systems fail to demonstrate self-regulation, psychologists often assume that normal development has been disrupted. As such, studying function as well as dysfunction in emotion regulation informs the clinical practice of school psychology. That is, interventionists may benefit from a better understanding of how systems work when they are functioning well, by examining the basic research literature, and when they are disrupted, by examining the applied literature. Here, the developmental literature for both regulation and dysregulation of emotion is reviewed and the implications for both assessment and intervention with preschool children are discussed.
The Development of Emotion Regulation
A review of the empirical studies of regulation from infancy through preschool produces consid-erable material on which to base assessment and intervention practices for preschool children. Basic research on regulation has identified a number of factors that influence the development of these processes at different ages, particularly biobehavioral processes, individual differences in temperament, and interpersonal processes (i.e., modulation of emotion in one person through the activity of another; see Tobin & Graziano, 2006, for a detailed review). Each of these areas are reviewed briefly to provide school psychologists with foundational knowledge related to the development of emotion regulation in children, as well as to provide opportunities to address problems in emotion regulation as it relates to preschool education.
During infancy, regulation focuses on biobehavioral processes such as biological rhythmicity, secu-rity, and synchronicity with a caregiver. In particular, vagal tone, a physiological measure of the inhibi-tory influence of the parasympathetic branch of the autonomic nervous system on the heart (responsible for slowing the heart rate and decreasing blood pressure), has been consistently linked to regulatory processes through its role in soothing and restoring calmness in the body (Katz & Gottman, 1995). For example, Calkins, Smith, Gill, and Johnson (1998) reported that negative control behavior by mothers (e.g., negative control: scolding, anger expressions, derogatory remarks, threats, no’s; physical control: restricting child’s movement, pulling, pushing, picking child up, hand slapping; and verbal control: directing the child’s activity, telling the child what to do) was related to poor child physiological regu-lation (as measured by vagal tone), less adaptive emotional regulation, and noncompliant behavior. It appears that these early infant-mother dyad influences not only shape children’s developing character-istic physiological response style (Bornstein & Suess, 2000), but also may result in the child’s diffi-culty to respond appropriately to a variety of emotion-eliciting stimuli. Lower baseline vagal tone in infants and toddlers is predictive of later difficulties in social interactions that require reciprocal engage-ment (Porges, Doussard-Roosevelt, Portales, & Greenspan, 1996) and the development of anxious and depressed symptoms in preschool and early elementary years (Cole, Zahn-Waxler, Fox, Usher, & Welsh, 1996). Consistent with these findings, Calkins (1997) found that toddlers who had ongoing suppressions in vagal tone during emotionally evocative situations (i.e., the ability to regulate physiological function to meet external demands, referred to as the vagal brake) engaged in more behavioral regulation during emotion-eliciting tasks.
Regulatory differences can also be measured at the hormonal level. The stress response typically involves a cascade of hormones produced by the adrenal cortex. The presence of elevated levels of these

The California School Psychologist, 2007, Vol. 12 109
hormones in the blood (including and especially, cortisol) is usually interpreted as the result of stress. In a study linking basic biological processes to emotion regulation, Gunnar, Mangelsdorf, Larson, and Hertsgaard (1990) found that infants who displayed more distress than their peers during laboratory tests showed greater adrenocortical activity. Similarly, Spangler, Schieche, Ilg, Maier, and Ackermann (1994) found that elevated blood cortisol was more frequently observed among children of highly insensitive mothers, suggesting a role for maternal behavior in infant behavioral regulation. Evidence from human and animal studies clearly shows that in stressful situations, the presence of familiar others, especially if there is close physical contact, reduces the levels of stress hormones in infants.
Related to basic biological factors, the development of self-regulatory processes is largely influ-enced by individual differences in temperament. Stifter and Braungart (1995) suggested a connection to both individual differences in temperament (self-soothing during decreasing negative arousal) and inter-action with caregivers (communicative behavior during increasing distress). Additionally, Goldsmith, Buss, and Lemery (1997) found that toddler and preschool displays of positive emotion share significant environmental influence, whereas emotion regulation was related to both environmental and genetic influence. Blackford and Walden (1998) found that temperament is more closely related to regulation and responsiveness to differences in communication from a parent. “Effortful control,” the ability to ignore a dominant response in favor of a subdominant response (Rothbart & Bates, 1998), has also been linked to young children’s emotion. Researchers found that effortful control in preschoolers is related to regulation of negative affect (Kochanska & Knaack, 2003; Kochanska, Murray, & Harlan, 2000), as well as positive affect (Kieras, Tobin, Graziano, & Rothbart, 2005).
The importance of the relationship with a caregiver in developing emotion regulation skills is also evident as early as infancy. Walden and Baxter (1989) found that older infants demonstrated regulation through social referencing of a parent. Yet another study found that securely attached infants demon-strated greater parent-oriented regulation relative to infants who were less securely attached to one or both parents (Diener, Mengelsdorf, McHale, & Frosch, 2002). Based on a sample of 223 children, Vondra, Shaw, Swearingen, Cohen, and Owens (2001) concluded that attachment classification, though not always stable between infancy and preschool, provides the most valuable information about child functioning.
The influence of both temperament and relationship with caregivers continues to be important as predictors of functioning throughout early childhood. Feldman, Greenbaum, Yirmiya, and Mayes (1996) found that patterns of synchrony between mothers and infants predicted verbal and general IQ at age two. In addition, research demonstrated that preschoolers high in the temperamental dimension of effortful control were unlikely to experience high levels of negative emotional arousal in response to peer inter-actions (Fabes et al., 1999). Moreover, when interactions were of elevated intensity, highly regulated preschoolers were likely to show socially competent responses. Rubin, Coplan, Fox, and Calkins (1995) reported similar links between temperament and peer relations.
Recent research suggests that biobehavioral processes associated with cardiovascular function may relate to basic regulatory processes and contribute to the development of subsequent regulatory processes in other domains. It is unclear whether poor vagal suppression is simply a marker of regulatory dysfunc-tion or dysfunctions in the vagal response system cause emotional dysregulation. Basic biological results also suggest that parent-child relationships play an important role in the development of young children’s physiological systems and may provide an additional target of assessment and intervention modalities. Adding more complexity, the presence of strong biological precursors of regulation does not exclude social and interpersonal influences. Even in infancy, individual differences in temperament and interper-
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12110
sonal relations, especially with caregivers, can influence developing regulatory systems. Thus, it is vital that school psychologists are aware of the bidirectional effects among interpersonal processes, tempera-ment, and basic biological functioning within a developing system. As an interventionist, it is helpful to highlight the important role that adult-child relationships play in the healthy development of biological and temperamental systems.
Taken together, these results suggest that regulation is not a single process or set of processes. Further, basic researchers provide knowledge to inform clinical practice that is within the bounds of current treatment methods. That is, school psychologists have the assessment tools and interventions available to address both within-child and interpersonal processes of emotion regulation. These findings suggest a need for greater communication between the scientific community and practitioners so that the specific findings of basic research may be used to full advantage in treatment.
Measuring Regulation
Basic psychological research has provided multiple methods of measuring regulation in preschool children. These methods vary considerably in their feasibility for practicing school psychologists. For example, physiological measures are frequently used as indicators of regulation in early childhood; however, most school psychologists do not have the time, financial resources, or training to assess chil-dren’s vagal tone, blood chemistry, or electroencephalography (EEG) activity. Fortunately, regulation researchers have developed several other methods to assess regulation processes in early childhood. Of course, no single assessment measure or method is all-encompassing, and it is generally better practice to orient assessment to referral concerns, but these methods are likely to provide valuable information for practicing school psychologists. Table 1 provides examples of regulation measures for preschool aged children. Although this list is not comprehensive, it provides several research-based options for use by school psychologists.
One common assessment method that is used frequently by school psychologists is rating scales completed by knowledgeable adult informants such as parents and teachers. When determining which ratings scales to use, however, most school psychologists tend to rely heavily on established clinical measures such as the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2004) and the Behavior Assessment System for Children (BASC-2; Reynolds & Kamphaus, 2004) without much consideration of the valuable measures available from basic developmental research. Several such measures exist to assess regulation within a preschool population. For example, Rothbart and colleagues (Putnam & Rothbart, 2007; Rothbart, Ahadi, Hershey, & Fisher, 2001) have generated several temperamental measures of regulation in preschoolers including an Effortful Control factor on the Children’s Behavior Questionnaire. Their extensive research has generated instruments that parents use to rate a child’s behavior over the last 6 months using 7-point Likert-type scales.
Building on Rothbart’s work, Eisenberg and Fabes (1995) adapted one of the Rothbart measures to study social competence, regulation, and emotionality. These researchers also developed vignettes to assess children’s emotion regulation based on parents’ reported expectations for their children’s behavior. Similarly, Block and Block (1980) generated yet another parent-report measure of regulation by assessing Ego Control and Ego Resiliency using a Q-sort method.
Emotion regulation in preschoolers has also been measured using observational or behavioral methods. One of the earliest and best known measures of regulation is delay of gratification tasks (Mischel & Baker, 1995; Mischel & Ebbesen, 1970). During these tasks, children’s ability to wait for a

The California School Psychologist, 2007, Vol. 12 111
TABLE 1. Selected List of Research-Based Regulation Measures
Measure Approx. Administration Time Relevant References
Questionnaire Methods
Emotion Regulation subscale 10-20 minutes Achenbach & of the CBCL 1 1/2 – 5 Rescorla (2004)
Emotional Self-Control 10-20 minutes Reynolds & Content Scale of the BASC-2 Kamphaus (2004)
Children’s Behavior Rothbart et al. (2001) Questionnaire Putnam & Rothbart (2007) Standard form (195 items) 60 minutes Short form (94 items) 30-40 minutes Very short form (36 items) 10-15 minutes
observation Methods
Delay of Gratification 15 minutes Mischel & Baker (1995); Mischel & Ebbesen (1970)
Effortful Control 1-3 minutes each; Kochanska & Behavioral Tasks 30-40 minutes for total battery Knaack (2003); Kochanska et al. (1997); Kochanska et al. (2000)
Lack of Control Scale Caspi et al. (1995); Henry et al. (1999)
desirable object (e.g., candy) and their regulation methods (e.g., looking away, distraction) are recorded and coded. According to Metcalfe and Mischel (1999), the ability to shift attention from the tempting object and delay gratification is a measure of emotion regulation. Furthermore, children’s ability to delay gratification in the preschool years may be related to adaptation to kindergarten (McIntyre, Blacher, & Baker, 2006). In a study examining children’s social and behavioral adaptation to kindergarten, McIntyre et al. found that children’s latency to touch a desired toy during a delay of gratification laboratory task at age 36 months predicted teacher reports of behavior problems and quality of student-teacher relation-ships at school entry when children were 5 or 6 years old.
Building on Mischel’s work, Kochanska and colleagues (Kochanska, Coy, & Murray, 2001; Kochanska & Knaack, 2003; Kochanska et al., 2000; Kochanska, Murray, & Coy, 1997) developed a series of activities to assess effortful control in preschoolers. These activities involve a child performing tasks such as moving an animal at various speeds across a game board, whispering, walking a straight line slowly, and resisting the temptation of candy. Children’s behaviors are recorded and coded as indica-tors of effortful control.
Another early observational measure of regulation was developed in 1975. Reported by Caspi, Henry, McGee, Moffitt, and Silva (1995), the Lack of Control observational measure is used to assess
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12112
regulation in preschool children. Henry, Caspi, Moffitt, Harrington, and Silva (1999) found that Lack of Control scores in preschool interacted with school attendance in predicting criminal behavior in males during adolescence. That is, school attendance served as a protective factor from later criminal activity for boys with high Lack of Control scores.
Measures generated by developmentalists are readily available and may be easily integrated into a multi-method, multi-setting, multi-informant assessment, particularly in evaluations of preschool chil-dren. Considering emotion regulation as both a target of assessment and intervention may be particularly important for school psychologists who support young children with or at-risk for behavior disorders. Evidence suggests that self-regulation, specifically effortful control, delay of gratification, and nega-tive emotional responses, may predict externalizing and internalizing disorders (e.g., Eisenberg, Fabes, Guthrie et al., 1996). Furthermore, children who use effective strategies to modulate negative emotional and behavioral responses are more likely to develop social competence (Eisenberg, Fabes, Karbon et al., 1996). Although children’s development is undoubtedly affected by genetic and environmental influences (including parenting), implementing school-based interventions that target the development of prosocial behavior, self-control, and problem solving may foster children’s emotion regulation and decrease the likelihood of developing emotional or behavioral disorders.
IMPLICATIonS foR PRACTICE
From the available research examining the relation of emotion regulation and dysregulation to chil-dren’s behavioral and social developmental trajectories, it is evident that young children who do not develop regulatory control are likely to exhibit emotional and behavioral problems in both school and community settings. These difficulties may emerge as students negotiate the preschool – kindergarten transition. In a recent study, a nationally representative sample of kindergarten teachers reported that over half of their students had a difficult time adjusting to school (Rimm-Kaufman, Pianta, & Cox, 2000). Top concerns included difficulties following directions and working independently (Rimm-Kaufman et al.), both of which may be related to children’s ability to self-regulate.
In light of school entry difficulties, early childhood education programs that equip young children with school readiness skills have been increasingly emphasized. As an example, the National Education Goals Panel Document Ready Schools states that all children should have access to high quality and developmentally appropriate preschool programs in preparation for their transition to formal schooling. The foremost goal is that “all children in America will start school ready to learn” (National Education Goals Panel, 1998, p.1).
The early childhood education and school readiness national trends include frameworks for addressing the social and emotional development of young children in home and school settings (Brooks-Gunn, Berlin, & Fuligini, 2000). Furthermore, there is increasing advocacy and empirical support for implementing preventive and early intervention services for young children with behavioral concerns and poor social-emotional competence using a Positive Behavior Support (PBS) approach (Joseph & Strain, 2003; Lynch, Geller, & Schmidt, 2004; Webster-Stratton & Reid, 2003).
Embedded within national trends and the empirical literature are important contextual factors that must be considered when developing early social-emotional interventions for young children. Critical among those factors are the development of programs based on a resiliency framework that incorpo-rate risk reduction of antisocial behaviors (e.g., noncompliance, defiance, aggression), enhancement of protective factors, and direct teaching of affective and behavioral skills necessary for the development of positive social-emotional well-being (Joseph & Strain, 2003; Miller, Brehm, & Whitehouse, 1998).

The California School Psychologist, 2007, Vol. 12 113
For example, research has demonstrated that the establishment of problem-solving skills, healthy coping mechanisms, and self-discipline (to name a few) during the preschool years, along with the involvement of a caring, competent adult predicts more favorable outcomes for children (e.g., Born, Chevalier, & Humblet, 1997; Cowen, Wyman, Work, & Iker, 1995; Rutter, 1987; Werner, 1993). These findings are consistent with the basic research literature and highlight the importance of both within-child and inter-personal processes in the development of regulatory skills and biological systems.
Although parent-child relationships are often identified in the developmental literature as crucial for children’s socioemotional development, the importance of early student-teacher relationships cannot be underestimated. Evidence suggests that positive student-teacher relationships in kindergarten predict academic and sociobehavioral adjustment across the elementary school years (Hamre & Pianta, 2001). In addition, a large body of research supports the use of PBS techniques for teaching and maintaining appropriate behavior in children (e.g., Eber, Sugai, Smith, & Scott, 2002; Sugai, Horner, & Gresham, 2002) that can be implemented effectively within preschool settings (e.g., Fox & Little, 2001). Closer examination of such research not only suggests that a host of environmental factors may help buffer young children from negative influences, but also emphasizes the positive role that parents and early educational environments have in the development of socially and emotionally competent children. Therefore, it is essential for social-emotional programming during preschool years to incorporate parent support/training that coincides with the establishment of positive early educational environments that utilize PBS strategies.
Parent Support/Training
According to a number of parent surveys, corporal punishment such as spanking, slapping, grab-bing, and shoving is used with more than 90% of children in the United States and is most commonly used with young children (Giles-Sims, Straus, & Sugarman, 1995). Such findings are staggering when considering that early hostile or negative parent interactions are associated with increased defiance and disobedience during later development (Keenan & Shaw, 1995). Consideration of parent support, there-fore, will need to incorporate instruction that targets increased caregiver sensitivity and appropriate behavior management skills.
The basic research reviewed clearly identifies caregiver-child interactions as vital to the develop-ment of children’s emotion regulation. An important aspect of these interactions is parental sensitivity. It includes timely and appropriate responding to a child’s efforts to interact, participating in activities and games that involve turn-taking, and interacting in ways that are equally rewarding for both parent and child. Helping parents learn how to interact may include providing opportunities to engage in play routines (playing games) or other transactions that involve turn-taking in which each partner plays a role that encourages the other in ways that are mutually reinforcing (e.g., peek-a-boo, pat-a-cake). As chil-dren grow older, the context of these interactions, and subsequent training opportunities for parents, may build upon socially mediated conflicts that children encounter. In this regard, the parent may need encour-agement in helping, guiding, and reassuring the child as to the most appropriate method for resolving a particular conflict. Within these situations, it may be effective to offer parenting groups that discuss chil-dren’s ongoing social-emotional problems where information is provided and problems are discussed. Essentially, parents are trained on how to react to their child. From this perspective, parent training involves a contextualized approach (i.e., parent-child interactions). Such parent training programs can be readily incorporated into early childhood education programs (e.g., McIntyre & Phaneuf, (in press) 2007) and include aspects supported by findings from the basic and applied literature.
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12114
In addition to promoting positive parent-child interactions, efforts must be taken to support parents in using discipline effectively (Webster-Stratton, 1990). A complete review of specific strategies is not within the scope of this discussion, rather a collection of themes is provided so readers can develop trainings that coincide with the particular needs of families. First, any discipline trainings should begin with a review of the developmental needs of young children at various age levels. Along with a discus-sion of the developmental needs of children, parents should be oriented to the differences in parenting styles. Second, trainings should incorporate discussions/activities that examine the functions (motives) behind negative behavior(s) observed in young children. Within such discussions, it may be helpful to signal how “punishing” children may serve to maintain problematic behaviors. Such programmatic approaches will begin to elucidate the difference between discipline and punishment. Third, training components should incorporate information on “how to” practice positive discipline in the home by arranging consistent consequences to increase appropriate behavior or decrease inappropriate behavior (e.g., positive reinforcement, differential reinforcement). Finally, trainings should include opportunities for troubleshooting common or specific problems that families encounter.
One example of an evidence-based parent training program that incorporates positive, preven-tive strategies as well as dealing with childhood challenging behavior is the Incredible Years program (Webster-Stratton, 1990; 2001). The Division 12 (clinical psychology) task force of the American Psychological Association deemed Webster-Stratton’s Incredible Years series as one of two well-estab-lished psychosocial treatments for childhood conduct problems (Brestan & Eyberg, 1998) based on effect sizes, sampling, methodology, treatment integrity, and a host of other criteria (Lonigan, Elbert, & Johnson, 1998). Webster-Stratton’s program (www.incredibleyears.com) offers a number of programs targeted at parents, teachers, and children (see Webster-Stratton, 2000, for a review).
Overall, programs that provide families with support/training with regard to sensitivity and disci-pline procedures have demonstrated promising outcomes (e.g., Brooks-Gunn et al., 2000; Yoshikawa, 1995) and are in line with data provided by basic emotion regulation researchers. Moreover, parents who receive support are more emotionally accommodating, less detached, and have more positive interac-tions with their children than control group families (Love et al., 2002). Despite evidence that parent training as a treatment approach is often effective within home settings, similar improvements at school and with peers have been less encouraging (e.g., Webster-Stratton, 1990). More recent efforts at devel-oping social-emotional competence in young children have turned to early educational environments that utilize prevention and early intervention strategies.
Early Education Environments
Although early education environments cannot adjust the basic biological foundations of poor emotion regulation, such environments can provide more opportunities for students to learn the neces-sary skills for developing positive social-emotional health. For example, early education environments can be used as resources to teach young children with regulation difficulties directly how to understand their emotions, as well as adjust their reactions to various environmental stimuli. In order to support early intervention and prevention efforts, many professionals are working to establish systems of PBS within preschool settings. For example, Stormont, Lewis, and Buckner (2005) described how features of PBS could be adapted and implemented with early childhood educational environments (e.g., programs serving children age 3 years to kindergarten). In addition, Fox, Dunlap, and Cushing (2002) outlined the logical extension of PBS systems to a preschool level. Essentially, such extensions have advocated for a three-tiered model of service delivery that incorporates increasing the intensity of instruction to the level
of student need (similar to recent suggestions for the use of Response to Intervention, RtI). Embedded within each tier is a set of instructional practices or evidence-based approaches designed to improve student outcomes, as well as frequent, ongoing assessments of student skills that are collected to monitor systematic efforts.
At the universal level (Tier I), all young children should receive sufficient concentration of positive feedback from teachers and caregivers (Shores, Gunter, & Jack, 1993; Sugai et al., 2002). Therefore, the foundation of an effective early educational program is the time spent building a strong, positive rela-tionship between educators and children, as well as with families. Investing time and attention in getting to know children parallels information presented regarding early parent-child interactions. That is, chil-dren notice responsive, caring adults and are more likely to pay attention to what a teacher says and does. Activities may include organized time to engage in frequent, positive adult-child interactions, as well as opportunities to review basic skills in a fun, interactive manner. Of critical importance at this level is classroom environment. Specifically, early educators will need to maintain a predictable schedule, minimize transitions, provide visual reminders of rules, give time and attention for appropriate behavior, use positive reinforcement to promote appropriate behavior, provide choices where appropriate, and maximize children’s engagement to minimize problem behaviors (see Lawry, Danko, & Strain, 1999, for a complete review). Consistent with findings from both basic and applied research literature, the combination of positive relationships and classroom preventive practices decreases the likelihood of inappropriate behavior.
At the secondary level (Tier II), social-emotional curricula should be adopted and implemented for those children who do not respond positively to universal strategies. In fact, some children may need explicit instruction to ensure they develop competence in emotional literacy, interpersonal problem-solving, and friendship skills (Webster-Stratton & Reid, 2003). Teaching children skills such as how to play with other children, recognizing and expressing feelings, exercising self-control, and negotiating conflict situations may result in fewer displays of inappropriate behavior. Specifically, early educators may want to incorporate lessons that: (a) teach feelings directly through pairing pictures of emotional expressions with a feeling word, (b) provide practice in recognizing emotions through games (e.g., Feeling Face Bingo), and (c) engage in instruction that allows children to observe a model and then role play specific skills related to social problem-solving (e.g., making coping statements, exploring solutions to problems) and friendship making skills (e.g., sharing, turn taking, giving compliments). As is the case with all instruction, effective teaching at the second tier requires careful planning and the adoption of specified curricula. For a complete review of evidenced-based, social-emotional curricula, see Joseph and Strain (2003). Most importantly, early educators should be attentive and offer praise/reinforcement to children when they are engaged in socially competent behavior such as following directions, helping friends, and sharing.
Even when educators are responsive, implement preventive strategies, and explicitly teach skills, a few children may continue to display poor social-emotional competence and/or challenging behavior(s). At this point (tertiary level, Tier III), assessment-based interventions will need to be planned and imple-mented by a team of individuals in home, early education, and community settings. Most important to this level is the completion of a functional behavior assessment (FBA) that identifies factors related to the child’s challenging behavior. When performed by a team of individuals, a complete FBA leads to the development of a behavior support plan that will include: (a) strategies to prevent problematic behavior(s) from occurring, (b) techniques for teaching new skills (e.g., social skills groups), and (c) changes in how family members and/or teachers respond to problematic behavior(s) (Horner, 2000). The
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12 11�
In addition to promoting positive parent-child interactions, efforts must be taken to support parents in using discipline effectively (Webster-Stratton, 1990). A complete review of specific strategies is not within the scope of this discussion, rather a collection of themes is provided so readers can develop trainings that coincide with the particular needs of families. First, any discipline trainings should begin with a review of the developmental needs of young children at various age levels. Along with a discus-sion of the developmental needs of children, parents should be oriented to the differences in parenting styles. Second, trainings should incorporate discussions/activities that examine the functions (motives) behind negative behavior(s) observed in young children. Within such discussions, it may be helpful to signal how “punishing” children may serve to maintain problematic behaviors. Such programmatic approaches will begin to elucidate the difference between discipline and punishment. Third, training components should incorporate information on “how to” practice positive discipline in the home by arranging consistent consequences to increase appropriate behavior or decrease inappropriate behavior (e.g., positive reinforcement, differential reinforcement). Finally, trainings should include opportunities for troubleshooting common or specific problems that families encounter.
One example of an evidence-based parent training program that incorporates positive, preven-tive strategies as well as dealing with childhood challenging behavior is the Incredible Years program (Webster-Stratton, 1990; 2001). The Division 12 (clinical psychology) task force of the American Psychological Association deemed Webster-Stratton’s Incredible Years series as one of two well-estab-lished psychosocial treatments for childhood conduct problems (Brestan & Eyberg, 1998) based on effect sizes, sampling, methodology, treatment integrity, and a host of other criteria (Lonigan, Elbert, & Johnson, 1998). Webster-Stratton’s program (www.incredibleyears.com) offers a number of programs targeted at parents, teachers, and children (see Webster-Stratton, 2000, for a review).
Overall, programs that provide families with support/training with regard to sensitivity and disci-pline procedures have demonstrated promising outcomes (e.g., Brooks-Gunn et al., 2000; Yoshikawa, 1995) and are in line with data provided by basic emotion regulation researchers. Moreover, parents who receive support are more emotionally accommodating, less detached, and have more positive interac-tions with their children than control group families (Love et al., 2002). Despite evidence that parent training as a treatment approach is often effective within home settings, similar improvements at school and with peers have been less encouraging (e.g., Webster-Stratton, 1990). More recent efforts at devel-oping social-emotional competence in young children have turned to early educational environments that utilize prevention and early intervention strategies.
Early Education Environments
Although early education environments cannot adjust the basic biological foundations of poor emotion regulation, such environments can provide more opportunities for students to learn the neces-sary skills for developing positive social-emotional health. For example, early education environments can be used as resources to teach young children with regulation difficulties directly how to understand their emotions, as well as adjust their reactions to various environmental stimuli. In order to support early intervention and prevention efforts, many professionals are working to establish systems of PBS within preschool settings. For example, Stormont, Lewis, and Buckner (2005) described how features of PBS could be adapted and implemented with early childhood educational environments (e.g., programs serving children age 3 years to kindergarten). In addition, Fox, Dunlap, and Cushing (2002) outlined the logical extension of PBS systems to a preschool level. Essentially, such extensions have advocated for a three-tiered model of service delivery that incorporates increasing the intensity of instruction to the level
of student need (similar to recent suggestions for the use of Response to Intervention, RtI). Embedded within each tier is a set of instructional practices or evidence-based approaches designed to improve student outcomes, as well as frequent, ongoing assessments of student skills that are collected to monitor systematic efforts.
At the universal level (Tier I), all young children should receive sufficient concentration of positive feedback from teachers and caregivers (Shores, Gunter, & Jack, 1993; Sugai et al., 2002). Therefore, the foundation of an effective early educational program is the time spent building a strong, positive rela-tionship between educators and children, as well as with families. Investing time and attention in getting to know children parallels information presented regarding early parent-child interactions. That is, chil-dren notice responsive, caring adults and are more likely to pay attention to what a teacher says and does. Activities may include organized time to engage in frequent, positive adult-child interactions, as well as opportunities to review basic skills in a fun, interactive manner. Of critical importance at this level is classroom environment. Specifically, early educators will need to maintain a predictable schedule, minimize transitions, provide visual reminders of rules, give time and attention for appropriate behavior, use positive reinforcement to promote appropriate behavior, provide choices where appropriate, and maximize children’s engagement to minimize problem behaviors (see Lawry, Danko, & Strain, 1999, for a complete review). Consistent with findings from both basic and applied research literature, the combination of positive relationships and classroom preventive practices decreases the likelihood of inappropriate behavior.
At the secondary level (Tier II), social-emotional curricula should be adopted and implemented for those children who do not respond positively to universal strategies. In fact, some children may need explicit instruction to ensure they develop competence in emotional literacy, interpersonal problem-solving, and friendship skills (Webster-Stratton & Reid, 2003). Teaching children skills such as how to play with other children, recognizing and expressing feelings, exercising self-control, and negotiating conflict situations may result in fewer displays of inappropriate behavior. Specifically, early educators may want to incorporate lessons that: (a) teach feelings directly through pairing pictures of emotional expressions with a feeling word, (b) provide practice in recognizing emotions through games (e.g., Feeling Face Bingo), and (c) engage in instruction that allows children to observe a model and then role play specific skills related to social problem-solving (e.g., making coping statements, exploring solutions to problems) and friendship making skills (e.g., sharing, turn taking, giving compliments). As is the case with all instruction, effective teaching at the second tier requires careful planning and the adoption of specified curricula. For a complete review of evidenced-based, social-emotional curricula, see Joseph and Strain (2003). Most importantly, early educators should be attentive and offer praise/reinforcement to children when they are engaged in socially competent behavior such as following directions, helping friends, and sharing.
Even when educators are responsive, implement preventive strategies, and explicitly teach skills, a few children may continue to display poor social-emotional competence and/or challenging behavior(s). At this point (tertiary level, Tier III), assessment-based interventions will need to be planned and imple-mented by a team of individuals in home, early education, and community settings. Most important to this level is the completion of a functional behavior assessment (FBA) that identifies factors related to the child’s challenging behavior. When performed by a team of individuals, a complete FBA leads to the development of a behavior support plan that will include: (a) strategies to prevent problematic behavior(s) from occurring, (b) techniques for teaching new skills (e.g., social skills groups), and (c) changes in how family members and/or teachers respond to problematic behavior(s) (Horner, 2000). The
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 1211�
team then implements this comprehensive plan at home and in preschool settings and monitors changes in the problem behavior, as well as the development of important social skills or other child outcomes.
Role of School Psychologists
Given the critical contexts in the early childhood field (e.g., national focus on school readiness and early intervention services), it may be necessary for many school psychologists to extend their expertise to preschool populations. At the most simplistic level, school psychologists can offer their expertise and knowledge regarding early childhood development by consulting/collaborating with local early childcare agencies/centers. Such support to local agencies/centers could assist with planning of interventions in collaboration with pre-kindergarten and kindergarten teachers, Head Start personnel, child care providers, administrators, parents, and community members. This level of involvement would allow for greater ease in transition for preschool programs to kindergarten classrooms. At a more direct level, school psychologists can organize, develop, and implement parent training programs that focus on positive parent-child interactions, behavior management skills, and child guidance procedures, and offer such programs in conjunction with systems that are already established. Furthermore, school psycholo-gists could be part of a school-based team that helps preschool agencies within or outside of their local school district with the incorporation of PBS principles. Because school psychologists understand the importance of designing interventions with contextual fit in mind, using prevention and early interven-tion approaches, and collecting data for monitoring progress, they stand at the forefront of assisting families and educators with the design, implementation, and evaluation of early care curricula and inter-ventions.
In conclusion, basic research exploring children’s regulation, including emotion displays, delay of gratification, effortful control, and adult-child interactions, may be particularly useful in developing early interventions to promote preschool students’ social competence and to decrease emotional and behav-ioral disorders. Although early childhood populations are not often the emphasis of school psychologists’ efforts, school psychologists may be in a unique position to provide both direct and indirect support to families and early childhood educators. In so doing, school psychologists may assist with the national priority of school readiness for all children.
REfEREnCES
Achenbach, T. M., & Rescorla, L. (2004). Manual for the ASEBA preschool forms and profiles. Burlington, VT: University of Vermont Department of Psychiatry.
Blackford, J. U., & Walden, T. A. (1998). Individual differences in social referencing. Infant Behavior & Develop-ment, 21(1), 89-102.
Block, J. H., & Block, J. (1980). The role of ego-control and ego-resiliency in the organization of behavior. In W. A. Collins (Eds.), Development of cognition, affect, and social relations. The Minnesota symposium on child psychology (Vol. 13, pp. 39-101). Hillsdale, NJ: Erlbaum.
Born, M., Chevalier, V., & Humblet, I. (1997). Resilience, desistance and delinquent career of adolescent offenders. Journal of Adolescence, 20, 679–694.
Bornstein, M. H., & Seuss, P. E. (2000). Child and mother cardiac vagal tone: Continuity, stability, and concordance across the first 5 years. Developmental Psychology, 3�(1), 54-65.
Brestan, E. V., & Eyberg, S. M. (1998). Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5,272 kids. Journal of Clinical Child Psychology, 27(2), 180-189.
Brooks-Gunn, J., Berlin, L., & Fuligni, A. (2000). Early childhood intervention programs: What about the family? In J. Schonkoff & S. Meisels (Eds.), Handbook of early childhood intervention (2nd Ed., pp. 549-589). New York: Cambridge University Press.
Calkins, S. D. (1997). Cardiac vagal tone indices of temperamental reactivity and behavioral regulation in young children. Developmental Psychobiology, 31(2), 125-135.
Calkins, S. D., Smith, C. L., Gill, K. L., & Johnson, M. C. (1998). Maternal interactive style across contexts: Rela-tions to emotional, behavioral, and physiological regulation during toddlerhood. Social Development, 7(3), 350-369.
Caspi, A., Henry, B., McGee, R., Moffitt, T. E., & Silva, P. A. (1995). Temperamental origins of child and adolescent behavior problems: From age three to age fifteen. Child Development, ��, 55-68.
Cole, P. M., Zahn-Waxler, C., Fox, N. A., Usher, B. A., & Welsh, J. D. (1996). Individual differences in emotion regulation and behavior problems in preschool children. Journal of Abnormal Psychology, 105(4), 518-529.
Cowen, E. L., Wyman, P. A., Work, W. C., & Iker, M. R. (1995). A preventive intervention for enhancing resilience among highly stressed urban children. Journal of Primary Prevention, 15, 247–260.
Diener, M. L., Mengelsdorf, S. C., McHale, J. L., & Frosch, C. A. (2002). Infants’ behavioral strategies for emotion regulation with fathers and mothers: Associations with emotional expressions and attachment quality. Infancy, 3(2), 153-174.
Eber, L., Sugai, G., Smith, C. R., & Scott, T. M. (2002). Wraparound and positive behavioral interventions and supports in the schools. Journal of Emotional and Behavioral Disorders, 10, 171-180.
Eisenberg, N. (2002). Emotion-related regulation and its relation to quality of social functioning. In W. Hartup & R. A. Weinberg (Eds.), Child psychology in retrospect and prospect: In celebration of the 75th anniversary of the Institute of Child Development (pp. 133-171). Mahwah, NJ: Erlbaum.
Eisenberg, N., & Fabes, R. A. (1995). The relation of young children’s vicarious emotional responding to social competence, regulation, and emotionality. Cognition & Emotion, 9(2-3), 203-228.
Eisenberg, N., Fabes, R. A., Guthrie, I. K., Murphy, B., Poulin, R., & Shepard, S. (1996). The relations of regula-tion and emotionality to problem behavior in elementary school children. Development & Psychopathology, 8, 141-162.
Eisenberg, N., Fabes, R. A., Karbon, M., Murphy, B. C., Wosinski, M., Polazzi, L., Carlo, G., & Juhnke, C. (1996). The relations of children’s dispositional prosocial behavior to emotionality, regulation, and social functioning. Child Development, �7, 974-992.
Fabes, R. A., Eisenberg, N., Jones, S., Smith, M., Guthrie, I., Poulin, R., Shepard, S., & Friedman, J. (1999). Regula-tion, emotionality, and preschoolers’ socially competent peer interactions. Child Development, 70(2), 432-442.
Feldman, R., Greenbaum, C. W., Yirmiya, N., & Mayes, L. C. (1996). Relations between cyclicity and regulation in mother-infant interaction at 3 and 9 months and cognition at 2 years. Journal of Applied Developmental Psychology, 17(3), 347-365.
Fox, L., Dunlap, G., & Cushing, L. (2002). Early intervention, positive behavior support, and transition to school. Journal of Emotional and Behavioral Disorders, 10, 149-157.
Fox, L., & Little, N. (2001). Starting early: Developing school-wide behavior support in a community preschool. Journal of Positive Behavior Interventions, 3, 251-254.
Giles-Sims, J., Straus, M.A., & Sugarman, D.B. (1995). Child, maternal and family characteristics associated with spanking. Journal of Applied Family and Child Studies, 44, 170-176.
Goldsmith, H. H., Buss, K. A., & Lemery, K. S. (1997). Toddler and childhood temperament: Expanded content, stronger genetic evidence, new evidence for the importance of environment. Developmental Psychology, 33(6), 891-905.
Gunnar, M. R., Mangelsdorf, S., Larson, M., & Hertsgaard, L. (1990). Attachment, temperament, and adrenocortical activity in infancy: A study of psychoendocrine regulation. Developmental Psychology, 25, 355-363.
Henry, B., Caspi, A., Moffitt, T. E., Harrington, H., & Silva, P. A. (1999). Staying in school protects boys with poor self-regulation in childhood from later crime: A longitudinal study. International Journal of Behavioral Devel-opment, 23(4), 1049-1073.
Hamre, B. K., & Pianta, R. C. (2001). Early teacher-child relationships and the trajectory of children’s school outcomes through eighth grade. Child Development, 72, 625-638.
Horner, R. H. (2000). Positive behavior supports. Focus on Autism and Other Developmental Disabilities, 15, 97-105.
Joseph, G. E., & Strain, P. S. (2003). Comprehensive evidence-based social-emotional curricula for young children: An analysis of efficacious adoption potential. Topics in Early Childhood Special Education, 23, 65-76.
Katz, L. F., & Gottman, J. M. (1995). Vagal tone protects children from marital conflict. Development and Psycho-pathology, 7, 83-92.
Keenan, K., & Shaw, D. S. (1995). The development of coercive family processes: The interaction between aversive toddler behavior and parenting factors. In J. McCord (Ed.), Coercion and punishment in long-term perspectives (pp. 165-180). New York: Cambridge University Press.
Kieras, J. E., Tobin, R. M., Graziano, W. G., & Rothbart, M. K. (2005). You can’t always get what you want: Effortful control and young children’s responses to undesirable gifts. Psychological Science, 1�, 391-396.
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12 117
team then implements this comprehensive plan at home and in preschool settings and monitors changes in the problem behavior, as well as the development of important social skills or other child outcomes.
Role of School Psychologists
Given the critical contexts in the early childhood field (e.g., national focus on school readiness and early intervention services), it may be necessary for many school psychologists to extend their expertise to preschool populations. At the most simplistic level, school psychologists can offer their expertise and knowledge regarding early childhood development by consulting/collaborating with local early childcare agencies/centers. Such support to local agencies/centers could assist with planning of interventions in collaboration with pre-kindergarten and kindergarten teachers, Head Start personnel, child care providers, administrators, parents, and community members. This level of involvement would allow for greater ease in transition for preschool programs to kindergarten classrooms. At a more direct level, school psychologists can organize, develop, and implement parent training programs that focus on positive parent-child interactions, behavior management skills, and child guidance procedures, and offer such programs in conjunction with systems that are already established. Furthermore, school psycholo-gists could be part of a school-based team that helps preschool agencies within or outside of their local school district with the incorporation of PBS principles. Because school psychologists understand the importance of designing interventions with contextual fit in mind, using prevention and early interven-tion approaches, and collecting data for monitoring progress, they stand at the forefront of assisting families and educators with the design, implementation, and evaluation of early care curricula and inter-ventions.
In conclusion, basic research exploring children’s regulation, including emotion displays, delay of gratification, effortful control, and adult-child interactions, may be particularly useful in developing early interventions to promote preschool students’ social competence and to decrease emotional and behav-ioral disorders. Although early childhood populations are not often the emphasis of school psychologists’ efforts, school psychologists may be in a unique position to provide both direct and indirect support to families and early childhood educators. In so doing, school psychologists may assist with the national priority of school readiness for all children.
REfEREnCES
Achenbach, T. M., & Rescorla, L. (2004). Manual for the ASEBA preschool forms and profiles. Burlington, VT: University of Vermont Department of Psychiatry.
Blackford, J. U., & Walden, T. A. (1998). Individual differences in social referencing. Infant Behavior & Develop-ment, 21(1), 89-102.
Block, J. H., & Block, J. (1980). The role of ego-control and ego-resiliency in the organization of behavior. In W. A. Collins (Eds.), Development of cognition, affect, and social relations. The Minnesota symposium on child psychology (Vol. 13, pp. 39-101). Hillsdale, NJ: Erlbaum.
Born, M., Chevalier, V., & Humblet, I. (1997). Resilience, desistance and delinquent career of adolescent offenders. Journal of Adolescence, 20, 679–694.
Bornstein, M. H., & Seuss, P. E. (2000). Child and mother cardiac vagal tone: Continuity, stability, and concordance across the first 5 years. Developmental Psychology, 3�(1), 54-65.
Brestan, E. V., & Eyberg, S. M. (1998). Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5,272 kids. Journal of Clinical Child Psychology, 27(2), 180-189.
Brooks-Gunn, J., Berlin, L., & Fuligni, A. (2000). Early childhood intervention programs: What about the family? In J. Schonkoff & S. Meisels (Eds.), Handbook of early childhood intervention (2nd Ed., pp. 549-589). New York: Cambridge University Press.
Calkins, S. D. (1997). Cardiac vagal tone indices of temperamental reactivity and behavioral regulation in young children. Developmental Psychobiology, 31(2), 125-135.
Calkins, S. D., Smith, C. L., Gill, K. L., & Johnson, M. C. (1998). Maternal interactive style across contexts: Rela-tions to emotional, behavioral, and physiological regulation during toddlerhood. Social Development, 7(3), 350-369.
Caspi, A., Henry, B., McGee, R., Moffitt, T. E., & Silva, P. A. (1995). Temperamental origins of child and adolescent behavior problems: From age three to age fifteen. Child Development, ��, 55-68.
Cole, P. M., Zahn-Waxler, C., Fox, N. A., Usher, B. A., & Welsh, J. D. (1996). Individual differences in emotion regulation and behavior problems in preschool children. Journal of Abnormal Psychology, 105(4), 518-529.
Cowen, E. L., Wyman, P. A., Work, W. C., & Iker, M. R. (1995). A preventive intervention for enhancing resilience among highly stressed urban children. Journal of Primary Prevention, 15, 247–260.
Diener, M. L., Mengelsdorf, S. C., McHale, J. L., & Frosch, C. A. (2002). Infants’ behavioral strategies for emotion regulation with fathers and mothers: Associations with emotional expressions and attachment quality. Infancy, 3(2), 153-174.
Eber, L., Sugai, G., Smith, C. R., & Scott, T. M. (2002). Wraparound and positive behavioral interventions and supports in the schools. Journal of Emotional and Behavioral Disorders, 10, 171-180.
Eisenberg, N. (2002). Emotion-related regulation and its relation to quality of social functioning. In W. Hartup & R. A. Weinberg (Eds.), Child psychology in retrospect and prospect: In celebration of the 75th anniversary of the Institute of Child Development (pp. 133-171). Mahwah, NJ: Erlbaum.
Eisenberg, N., & Fabes, R. A. (1995). The relation of young children’s vicarious emotional responding to social competence, regulation, and emotionality. Cognition & Emotion, 9(2-3), 203-228.
Eisenberg, N., Fabes, R. A., Guthrie, I. K., Murphy, B., Poulin, R., & Shepard, S. (1996). The relations of regula-tion and emotionality to problem behavior in elementary school children. Development & Psychopathology, 8, 141-162.
Eisenberg, N., Fabes, R. A., Karbon, M., Murphy, B. C., Wosinski, M., Polazzi, L., Carlo, G., & Juhnke, C. (1996). The relations of children’s dispositional prosocial behavior to emotionality, regulation, and social functioning. Child Development, �7, 974-992.
Fabes, R. A., Eisenberg, N., Jones, S., Smith, M., Guthrie, I., Poulin, R., Shepard, S., & Friedman, J. (1999). Regula-tion, emotionality, and preschoolers’ socially competent peer interactions. Child Development, 70(2), 432-442.
Feldman, R., Greenbaum, C. W., Yirmiya, N., & Mayes, L. C. (1996). Relations between cyclicity and regulation in mother-infant interaction at 3 and 9 months and cognition at 2 years. Journal of Applied Developmental Psychology, 17(3), 347-365.
Fox, L., Dunlap, G., & Cushing, L. (2002). Early intervention, positive behavior support, and transition to school. Journal of Emotional and Behavioral Disorders, 10, 149-157.
Fox, L., & Little, N. (2001). Starting early: Developing school-wide behavior support in a community preschool. Journal of Positive Behavior Interventions, 3, 251-254.
Giles-Sims, J., Straus, M.A., & Sugarman, D.B. (1995). Child, maternal and family characteristics associated with spanking. Journal of Applied Family and Child Studies, 44, 170-176.
Goldsmith, H. H., Buss, K. A., & Lemery, K. S. (1997). Toddler and childhood temperament: Expanded content, stronger genetic evidence, new evidence for the importance of environment. Developmental Psychology, 33(6), 891-905.
Gunnar, M. R., Mangelsdorf, S., Larson, M., & Hertsgaard, L. (1990). Attachment, temperament, and adrenocortical activity in infancy: A study of psychoendocrine regulation. Developmental Psychology, 25, 355-363.
Henry, B., Caspi, A., Moffitt, T. E., Harrington, H., & Silva, P. A. (1999). Staying in school protects boys with poor self-regulation in childhood from later crime: A longitudinal study. International Journal of Behavioral Devel-opment, 23(4), 1049-1073.
Hamre, B. K., & Pianta, R. C. (2001). Early teacher-child relationships and the trajectory of children’s school outcomes through eighth grade. Child Development, 72, 625-638.
Horner, R. H. (2000). Positive behavior supports. Focus on Autism and Other Developmental Disabilities, 15, 97-105.
Joseph, G. E., & Strain, P. S. (2003). Comprehensive evidence-based social-emotional curricula for young children: An analysis of efficacious adoption potential. Topics in Early Childhood Special Education, 23, 65-76.
Katz, L. F., & Gottman, J. M. (1995). Vagal tone protects children from marital conflict. Development and Psycho-pathology, 7, 83-92.
Keenan, K., & Shaw, D. S. (1995). The development of coercive family processes: The interaction between aversive toddler behavior and parenting factors. In J. McCord (Ed.), Coercion and punishment in long-term perspectives (pp. 165-180). New York: Cambridge University Press.
Kieras, J. E., Tobin, R. M., Graziano, W. G., & Rothbart, M. K. (2005). You can’t always get what you want: Effortful control and young children’s responses to undesirable gifts. Psychological Science, 1�, 391-396.
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12118
Kochanska, G., Coy, K. C., & Murray, K. T. (2001). The development of self-regulation in the first four years of life. Child Development, 72(4), 1091-1111.
Kochanska, G., & Knaack, A. (2003). Effortful control as a personality characteristic of young children: Anteced-ents, correlates, and consequences. Journal of Personality, 71(6), 1087-1112.
Kochanska, G., Murray, K. T., & Coy, K. C. (1997). Inhibitory control as a contributor to conscience in childhood: From toddler to early school age. Child Development, �8, 263-277.
Kochanska, G., Murray, K. T., & Harlan, E. T. (2000). Effortful control in early childhood: Continuity and change, antecedents, and implications for social development. Developmental Psychology, 3�(2), 220-232.
Lawry, J., Danko, C., & Strain, P. (1999). Examining the role of the classroom environment in the prevention of problem behaviors. In S. Sandall & M. Ostrosky, (Eds.), Young exceptional children: Practical ideas for addressing challenging behaviors (pp. 49-62). Longmont, CO: Sopris West.
Linscott, J., & DiGiuseppe, R. (1994). Rational emotive therapy with children. In C. W. LeCroy (Ed.), Handbook of child and adolescent treatment manuals (pp. 5-40). New York: Lexington.
Lonigan, C. J., Elbert, J. C., & Johnson, S. B. (1998). Empirically supported psychosocial interventions for children: An overview. Journal of Clinical Child Psychology, 27(2), 138-145.
Love, J. M., Kisker, E. E., Ross, C. M., Schochet, P. Z., Brooks-Gunn, J., Paulsell, D., Boller, K., Constantine, J., Vogel, C., Fuligni, A. S., & Brady-Smith, C. (2002). Making a difference in the lives of infants and toddlers and their families: The impact of early Head Start: Volume 1. Final technical report. Washington, DC: U.S. Depart-ment of Health and Human Services, Administration for Children and Families.
Lynch, K. B., Geller, S. R., & Schmidt, M. G. (2004). Multi-year evaluation of the effectiveness of a resilience-based prevention program for young children. The Journal of Primary Prevention, 24, 335-346.
McIntyre, L. L., Blacher, J., & Baker, B. L. (2006). Transition to school: Adaptation in young children with and without developmental delays. Journal of Intellectual Disability Research, 50, 349-361.
McIntyre, L. L., & Phaneuf, L. (In Press) (2007). A three-tier model of parent education in early childhood: Applying a problem-solving model. Topics in Early Childhood Special Education.
Metcalfe, J., & Mischel, W. (1999). A hot-cool system analysis of delay of gratification: Dynamics of willpower. Psychological Review, 10�(1), 3-19.
Miller, G. E., Brehm, K., & Whitehouse, S. (1998). Reconceptualizing school-based prevention for antisocial behavior within a resiliency framework. School Psychology Review, 27, 364–379.
Mischel, W., & Baker, N. (1995). Cognitive appraisals and transformations in delay behavior. Journal of Personality and Social Psychology, 31, 254-261.
Mischel, W., & Ebbesen, E. B. (1970). Attention in delay of gratification. Journal of Personality and Social Psychology, 1�, 329-337.
National Education Goals Panel (1998). Ready schools. Washington, DC: Author. Porges, S. W., Doussard-Roosevelt, J. A., Portales, A. L., & Greenspan, S. I. (1996). Infant regulation of the vagal
“brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psycho-biology, 29(8), 697-712.
Putnam, S. P., & Rothbart, M. K. (2007). Development of Short and Very Short Forms of the Children’s Behavior Questionnaire. Journal of Personality Assessment, 87, 103-113.
Reynolds, C. R. & Kamphaus, R. W. (2004). BASC-2: Behavior assessment system for children, second edition. Circle Pines: AGS.
Rimm-Kaufman, S., Pianta, R., & Cox, M. (2000). Teachers’ judgments of problems in the transition to kinder-garten. Early Childhood Research Quarterly, 15(2), 147-166.
Rothbart, M. K., Ahadi, S. A., Hershey, K. L., & Fisher, P. (2001). Investigations of temperament at 3-7 years: The Children’s Behavior Questionnaire. Child Development, 72 , 1394-1408.
Rothbart, M. K. & Bates, J.E. (1998). Temperament. In W. Damon (Series Ed.) & N. Eisenberg (Vol. Ed.), Handbook of child psychology: Vol. 3. Social, emotional, personality development (pp. 105-176). New York: Wiley.
Rubin, K. H., Coplan, R. J., Fox, N. A., & Calkins, S. D. (1995). Emotionality, emotion regulation, and preschoolers’ social adaptation. Development & Psychopathology, 7(1), 49-62.
Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57, 316–331.
Shores, R. E., Gunter, P. L., & Jack, S. L. (1993). Classroom management strategies: Are they setting events for coercion? Behavioral Disorders, 18, 92-102.
Spangler, G., Schieche, M., Ilg, U., Maier, U., & Ackermann, C. (1994). Maternal sensitivity as an external organizer for biobehavioral regulation in infancy. Developmental Psychobiology, 27(7), 425-437.
Stifter, C. A., & Braungart, J. M. (1995). The regulation of negative reactivity in infancy: Function and development. Developmental Psychology, 31(3), 448-455.
Stormont, M., Lewis, T. J., & Beckner, R. (2005). Positive behavior support systems: Applying key features in preschool settings. Teaching Exceptional Children, 37, 42-49.
Sugai, G. Horner, R. H., & Gresham, F. M. (2002). Behaviorally effective school environments. In M. R. Shinn, H. M. Walker, & G. Stoner (Eds.), Interventions for academic and behavior problems II: Preventative and remedial approaches (pp. 315-350). Bethesda, MD: National Association of School Psychologists.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. In N. A. Fox (Ed.), Monographs of the Society for Research in Child Development, 59 (2-3, Serial No. 240).
Tobin, R. M., & Graziano, W. G. (2006). Development of regulatory processes through adolescence: A review of recent empirical studies. In D. Mroczek & T. Little (Eds.), Handbook of Personality Development (pp. 263-283). Mahwah, NJ: Erlbaum.
Vondra, J. I., Shaw, D. S., Swearingen, L., Cohen, M., & Owens, E. B. (2001). Attachment stability and emotional and behavioral regulation from infancy to preschool age. Development & Psychopathology, 13(1), 13-33.
Walden, T. A., & Baxter, A. (1989). The effect of context and age on social referencing. Child Development, �0(6), 1�11-1�18.
Webster-Stratton, C. (1990). Long-term follow-up of families with young conduct problem children: From preschool to grade school. Journal of Clinical Child Psychology, 19, 144–149.
Webster-Stratton, C. (2000). The Incredible Years Training series. Office of Juvenile Justice and Delinquency Prevention Bulletin Review, June, 1-24.
Webster-Stratton, C. (2001). The Incredible Years: Parents, teachers, and children training series. Leader’s guide. Seattle, WA: author.
Webster-Stratton, C., & Reid, M. J. (2003). Treating conduct problems and strengthening social and emotional competence in young children: The Dina Dinosaur treatment program. Journal of Emotional and Behavioral Disorders, 11(3), 130-143.
Werner, E. E. (1993). Risk, resilience, and recovery: Perspectives from the Kauai Longitudinal Study. Development & Psychopathology, 5, 503–515.
Yoshikawa, H. (1995). Long-term effects of early childhood programs on social outcomes and delinquency. The Future of Children, 5, 51-75.
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12 119
Kochanska, G., Coy, K. C., & Murray, K. T. (2001). The development of self-regulation in the first four years of life. Child Development, 72(4), 1091-1111.
Kochanska, G., & Knaack, A. (2003). Effortful control as a personality characteristic of young children: Anteced-ents, correlates, and consequences. Journal of Personality, 71(6), 1087-1112.
Kochanska, G., Murray, K. T., & Coy, K. C. (1997). Inhibitory control as a contributor to conscience in childhood: From toddler to early school age. Child Development, �8, 263-277.
Kochanska, G., Murray, K. T., & Harlan, E. T. (2000). Effortful control in early childhood: Continuity and change, antecedents, and implications for social development. Developmental Psychology, 3�(2), 220-232.
Lawry, J., Danko, C., & Strain, P. (1999). Examining the role of the classroom environment in the prevention of problem behaviors. In S. Sandall & M. Ostrosky, (Eds.), Young exceptional children: Practical ideas for addressing challenging behaviors (pp. 49-62). Longmont, CO: Sopris West.
Linscott, J., & DiGiuseppe, R. (1994). Rational emotive therapy with children. In C. W. LeCroy (Ed.), Handbook of child and adolescent treatment manuals (pp. 5-40). New York: Lexington.
Lonigan, C. J., Elbert, J. C., & Johnson, S. B. (1998). Empirically supported psychosocial interventions for children: An overview. Journal of Clinical Child Psychology, 27(2), 138-145.
Love, J. M., Kisker, E. E., Ross, C. M., Schochet, P. Z., Brooks-Gunn, J., Paulsell, D., Boller, K., Constantine, J., Vogel, C., Fuligni, A. S., & Brady-Smith, C. (2002). Making a difference in the lives of infants and toddlers and their families: The impact of early Head Start: Volume 1. Final technical report. Washington, DC: U.S. Depart-ment of Health and Human Services, Administration for Children and Families.
Lynch, K. B., Geller, S. R., & Schmidt, M. G. (2004). Multi-year evaluation of the effectiveness of a resilience-based prevention program for young children. The Journal of Primary Prevention, 24, 335-346.
McIntyre, L. L., Blacher, J., & Baker, B. L. (2006). Transition to school: Adaptation in young children with and without developmental delays. Journal of Intellectual Disability Research, 50, 349-361.
McIntyre, L. L., & Phaneuf, L. (In Press) (2007). A three-tier model of parent education in early childhood: Applying a problem-solving model. Topics in Early Childhood Special Education.
Metcalfe, J., & Mischel, W. (1999). A hot-cool system analysis of delay of gratification: Dynamics of willpower. Psychological Review, 10�(1), 3-19.
Miller, G. E., Brehm, K., & Whitehouse, S. (1998). Reconceptualizing school-based prevention for antisocial behavior within a resiliency framework. School Psychology Review, 27, 364–379.
Mischel, W., & Baker, N. (1995). Cognitive appraisals and transformations in delay behavior. Journal of Personality and Social Psychology, 31, 254-261.
Mischel, W., & Ebbesen, E. B. (1970). Attention in delay of gratification. Journal of Personality and Social Psychology, 1�, 329-337.
National Education Goals Panel (1998). Ready schools. Washington, DC: Author. Porges, S. W., Doussard-Roosevelt, J. A., Portales, A. L., & Greenspan, S. I. (1996). Infant regulation of the vagal
“brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psycho-biology, 29(8), 697-712.
Putnam, S. P., & Rothbart, M. K. (2007). Development of Short and Very Short Forms of the Children’s Behavior Questionnaire. Journal of Personality Assessment, 87, 103-113.
Reynolds, C. R. & Kamphaus, R. W. (2004). BASC-2: Behavior assessment system for children, second edition. Circle Pines: AGS.
Rimm-Kaufman, S., Pianta, R., & Cox, M. (2000). Teachers’ judgments of problems in the transition to kinder-garten. Early Childhood Research Quarterly, 15(2), 147-166.
Rothbart, M. K., Ahadi, S. A., Hershey, K. L., & Fisher, P. (2001). Investigations of temperament at 3-7 years: The Children’s Behavior Questionnaire. Child Development, 72 , 1394-1408.
Rothbart, M. K. & Bates, J.E. (1998). Temperament. In W. Damon (Series Ed.) & N. Eisenberg (Vol. Ed.), Handbook of child psychology: Vol. 3. Social, emotional, personality development (pp. 105-176). New York: Wiley.
Rubin, K. H., Coplan, R. J., Fox, N. A., & Calkins, S. D. (1995). Emotionality, emotion regulation, and preschoolers’ social adaptation. Development & Psychopathology, 7(1), 49-62.
Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57, 316–331.
Shores, R. E., Gunter, P. L., & Jack, S. L. (1993). Classroom management strategies: Are they setting events for coercion? Behavioral Disorders, 18, 92-102.
Spangler, G., Schieche, M., Ilg, U., Maier, U., & Ackermann, C. (1994). Maternal sensitivity as an external organizer for biobehavioral regulation in infancy. Developmental Psychobiology, 27(7), 425-437.
Stifter, C. A., & Braungart, J. M. (1995). The regulation of negative reactivity in infancy: Function and development. Developmental Psychology, 31(3), 448-455.
Stormont, M., Lewis, T. J., & Beckner, R. (2005). Positive behavior support systems: Applying key features in preschool settings. Teaching Exceptional Children, 37, 42-49.
Sugai, G. Horner, R. H., & Gresham, F. M. (2002). Behaviorally effective school environments. In M. R. Shinn, H. M. Walker, & G. Stoner (Eds.), Interventions for academic and behavior problems II: Preventative and remedial approaches (pp. 315-350). Bethesda, MD: National Association of School Psychologists.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. In N. A. Fox (Ed.), Monographs of the Society for Research in Child Development, 59 (2-3, Serial No. 240).
Tobin, R. M., & Graziano, W. G. (2006). Development of regulatory processes through adolescence: A review of recent empirical studies. In D. Mroczek & T. Little (Eds.), Handbook of Personality Development (pp. 263-283). Mahwah, NJ: Erlbaum.
Vondra, J. I., Shaw, D. S., Swearingen, L., Cohen, M., & Owens, E. B. (2001). Attachment stability and emotional and behavioral regulation from infancy to preschool age. Development & Psychopathology, 13(1), 13-33.
Walden, T. A., & Baxter, A. (1989). The effect of context and age on social referencing. Child Development, �0(6), 1�11-1�18.
Webster-Stratton, C. (1990). Long-term follow-up of families with young conduct problem children: From preschool to grade school. Journal of Clinical Child Psychology, 19, 144–149.
Webster-Stratton, C. (2000). The Incredible Years Training series. Office of Juvenile Justice and Delinquency Prevention Bulletin Review, June, 1-24.
Webster-Stratton, C. (2001). The Incredible Years: Parents, teachers, and children training series. Leader’s guide. Seattle, WA: author.
Webster-Stratton, C., & Reid, M. J. (2003). Treating conduct problems and strengthening social and emotional competence in young children: The Dina Dinosaur treatment program. Journal of Emotional and Behavioral Disorders, 11(3), 130-143.
Werner, E. E. (1993). Risk, resilience, and recovery: Perspectives from the Kauai Longitudinal Study. Development & Psychopathology, 5, 503–515.
Yoshikawa, H. (1995). Long-term effects of early childhood programs on social outcomes and delinquency. The Future of Children, 5, 51-75.
Emotional Competence in Preschoolers

The California School Psychologist, 2007, Vol. 12120
AUTHOR NOTEThis paper was developed, in part, through the authors’ participation in the 2007 School Psychology Research
Collaboration Conference (SPRCC) co-sponsored by The Society for the Study of School Psychology (SSSP), The National Association of School Psychologists (NASP), Pearson Assessments, Division 16 of the American Psycholog-ical Association (APA), Council of Directors of School Psychology Programs (CDSPP), AIMSweb, Trainers of School Psychologists (TSP), Riverside Publishing, APA Board of Educational Affairs, and Elsevier.

The California School Psychologist, 2007, Vol. 12 121
The California School Psychologist, Vol. 12, pp. 121 – 132, 2007Copyright 2007 California Association of School Psychologists
A Comparison of Classification Methods for use in Predicting School-Based outcomes
Erin Dowdy University of California, Santa Barbara
Randy W. Kamphaus Georgia State University
There is growing evidence that current classification methods are not consistent with current empirical knowledge of childhood psychopathology and the optimal way to classify school-age children remains controversial. The current study investigated three classification methods (categorical, dimensional, person-oriented) for use in predicting school-based outcomes. Children (grades 1-5; N=558) were administered the Behavior Assessment System for Children – Teacher Rating Scale and results were used to form three classification systems. Educational outcome variables were collected seven months later and the predictive validity of the three classification systems was compared using regression analyses. Findings indicated that all three methods for predicting educational outcomes were modest and were best able to predict later grade point averages. Results indicate the relative superiority of person-oriented and dimensional methods of classification; however these classification methods warrant further investigation.
Keywords: classification, diagnosis, person-oriented, psychopathology
The fields of psychiatry and psychology have been grappling with the issue of classification for decades (Achenbach, 1998; 2001). Practitioners, researchers, and educators agree about the importance of classification for a variety of reasons including enhanced communication among professionals, ease of description, and the ability to differentiate individuals (Scotti & Morris, 2000; Blashfield, 1998; Cantwell, 1996). Accurate classification for school-age children is particularly critical considering the fact that the developmental courses or pathways of children are likely to influence subsequent outcomes (Jimerson, Coffino, & Sroufe, 2007; Sroufe, Egeland, Carlson, & Collins, 2005). Insight into children’s adjustment and risk status (Kagan, 1997), tracking developmental pathways (Richters, 1997), differen-tiating individuals by etiology (Cantwell, 1996), and predicting effective treatment approaches (Scotti & Morris, 2000) are among the most salient reasons that accurate classification in school-age children is important. However, children are often classified into groups that receive services only after they exhibit significant impairment. This “wait-to-fail” treatment approach could result from current classification systems that fail to identify subsyndromal psychopathology or current risk status. Classification systems that more accurately identify children for services are thus needed as these systems could effectively aid daily decisions regarding prevention, early intervention, and treatment for children.
There is growing consensus that current diagnostic systems have lagged behind the increase in knowledge about psychopathology and classification (Beutler & Malik, 2002; Houts, 2002). Currently, most school-age children are primarily classified and diagnosed using categorical methods. This approach uses variables to form “all-or-nothing” categories based on the assumption that disorders form discrete categories (Millon, 1991). Specifically, students are placed into categories specified by the DSM (DSM-IV; American Psychiatric Association) or the Individuals with Disabilities Education Act (IDEA). There are several limitations to these methods of classification including that only qualitative differences are
Please send correspondence to Erin Dowdy, at University of California, Santa Barbara; Gevirtz Graduate School of Education; Counseling, Clinical, and School Psychology; Phelps Hall; Santa Barbara,CA, USA; 93106-9490 or e-mail [email protected]

The California School Psychologist, 2007, Vol. 12122
noted. However, throughout the scientific literature evidence exists suggesting that symptoms of hyper-activity/impulsivity, inattention, conduct problems, depression, and anxiety occur along a continuum, or show evidence of quantitative differences (Deater-Deckard, et al., 1997; Fergusson & Horwood, 1995; Hudziak, Wadsworth, Heath, & Achenbach, 1999; Nease, Volk, & Cass, 1999). Other limitations of categorical classification methods include the failure to account for comorbidity (van Lier, Verhulst, van der Ende, & Crijnen, 2003), normally or marginally functional behavioral systems (Jensen, et al., 1996), or subsyndromal psychopathology (Cantwell, 1996). A study by Scahill, et al. (1999) found that children beneath the diagnostic threshold for ADHD still possessed evidence of functional impairment in school, which was nearly identical to the impairment experienced by children above the diagnostic threshold. This study suggests that under a purely categorical model, such as the DSM-IV or IDEA, students who experience functional impairment might not be classified, and thus fail to receive services. Furthermore, there is no differentiation among individuals with lower levels of risk, yielding no useful information for planning prevention or early intervention services.
Considering limitations of categorical methods, dimensional and person-oriented methods have been proposed as alternative approaches to classification. Dimensional approaches to classification assume that behavior does not occur dichotomously, but rather along a continuum. Descriptive variables are collected and combined with other correlated variables to form a dimension, which summarizes information about the descriptive variables into an abstract, higher-order variable (Blashfield, 1998). Dimensional methods of classification improve on categorical methods by accounting for quantitative differences in symptomatology. Namely, this method includes a wider variety of information and has the ability to identify and classify all children, not just the ones with the most severe psychopathology. However, dimensional methods often focus on variables of interest and produce a system that is arguably less parsimonious than a categorical system (Helzer & Hudziak, 2000).
Person-oriented, or multivariate, methods of classification attempt to blend categorical and dimen-sional methods by producing a categorical classification system through the use of dimensional scales. The resulting typology is a different type of categorical classification system that encompasses a full range of dimensionally scaled variables. Person-oriented approaches have been proposed due to their strength in emphasizing the individual as a whole, not just a linear combination of variables (Bergman & Magnusson, 1997), being conducive to a fuller understanding of the complexity and range of child behaviors (Meehl, 1995; Speece & Cooper, 1991), and providing consistency with psychological theo-retical models of psychological systems development (Gottlieb, 2000; Waddington, 1971). Multivariate behavior typologies, derived through cluster analytic techniques, are also gaining wider acceptance as a model of classification due to the evidence supporting the relative superiority of multivariate methods in explaining the complex interactions, correlates, and comorbidities in children (van Lier, et al., 2003; Greenberg, Speltz, DeKlyen, & Jones, 2001).
However, before behavioral typologies are proposed as an alternative classification method, a direct comparison of methods is needed. Few systematic comparisons of classification methods have been conducted. Fergusson and Horwood (1995) examined the relationship between categorical, dimen-sional, and a series of outcome measures and found dimensional methods to result in stronger predic-tions of outcomes. However, findings by Jensen et al. (1996) suggest that categorical and dimensional approaches to classification might produce similar results when similar methods are used, even though highly specific diagnostic categories show fewer relationships with external validators. Furthermore, Mattison and Spitznagel (1999) found prior studies comparing DSM categories to Child Behavior Checklist dimensional scales that suggest that neither system is superior when compared to external validators.
The California School Psychologist, 2007, Vol. 12 123Comparison Of Classification Methods
Theoretically, person-oriented methods of classification are superior to categorical and dimen-sional methods due to their ability to account for the interactional and additive nature among variables (Kamphaus, DiStefano, & Lease, 2003; Dowdy, Hendry, & Kamphaus, 2006). However, it is not known whether person-oriented clusters, derived from such diagnostic tools as teacher rating scales, demon-strate an increased ability to predict future outcomes. The ability of a classification system to predict future outcomes should guide thinking about its utility (Bergman & Magnusson, 1997). Before cluster-analytically derived typologies can be introduced as alternatives, research must examine their ability to predict and generalize based on the attributes of the individual (Lessing, 1982). For example, it is unknown if the additional dimensional scales used to create a person-oriented classification system are more predictive than the single dimensional scale used in a dimensional system.
Initial research by Flanagan, Bierman, and Kam (2003) found cluster membership to be predictive of later outcomes for first grade children, and Toshiaki, et al. (1995) found cluster membership to be predic-tive of outcomes in adults. Additionally, Fergusson and Horwood (1995) found dimensionally scored measures to show better evidence of predictive validity than categorical methods. A study by Greenberg, Speltz, DeKlyen, and Jones (2001) found person-oriented methods to be superior to individual variable approaches in significantly predicting risk factors of conduct problems. However, Haapasalo, Tremblay, Boulerice, and Vitaro (2000) found prediction of problem behavior in kindergartners to be equally accu-rate using either cluster or variable approaches. Blanchard, Morgenstern, Morgan, Labouvie, and Bux (2003) concluded that the utility of clusters to inform clinicians about the future behavior of individuals is unknown.
These discrepant findings suggest that additional research should be conducted on classification methods in an attempt to determine the optimal way to classify school-age children. A direct comparison of methods and information regarding their ability to predict later outcomes is needed. The current study sought to: (1) classify children into categories according to categorical, dimensional, and person-oriented methods and (2) provide a comparison of classification methods for predicting school-based outcomes.
METhoD
Subjects
Data for this study were collected as part of Project ACT Early, funded by Field-Initiated Studies grants (R306F60158, R305T990330) from the Institute for At-Risk Children of the Office of Educational Research and Improvement, United States Department of Education. (Grant principal investigators: Jean A. Baker, Randy W. Kamphaus, and Arthur M. Horne). Project ACT Early was a research grant designed to study the ecological context of risk in elementary schools and was aimed at teacher professional development designed to improve classroom management. The sample consisted of ��8 children (grades 1-5; N=558) and is approximately one half female (N= 298; 53.4%). Approximately 52% of the children were African American (N=295), 30% Caucasian (N=169), 7% Hispanic (N=38), 2% Asian American (N=10), and 2% multiracial (N=13).
Instruments
Children’s behavior problems and adaptive competencies were assessed with the Behavior Assess-ment System for Children - Teacher Rating Scale - Child (BASC-TRS-C; Reynolds & Kamphaus, 1992), designed for students ages 6-11. The BASC-TRS-C is a 148-item, nationally standardized measure that yields ten problem behavior scales and four adaptive behavior scales (Reynolds & Kamphaus, 1992).

The California School Psychologist, 2007, Vol. 12124
The BASC manual provides reliability and validity psychometric information and descriptions of the TRS-C scales. The 148 behavioral items are rated on a 4-point Likert scale (1=never, 2=sometimes, 3=often, 4=almost always).
Procedure
BASC-Teacher Rating Scales were collected in the fall of the academic school year for each partici-pating child. Results from the BASC-TRS were used to form three classification models: a categorical classification model examining symptoms based on DSM-IV criteria (categorical), a dimensional system based on dimensional scales (dimensional), and a categorical system formed by examining the multiple dimensions of symptoms exhibited by individuals (person-oriented, cluster). Each child was concur-rently placed into these three separate classification systems.
Approximately seven months later, educational outcome variables were collected for each child. The predictive validity of the three classification systems was compared using regression techniques.
Categorical Classification Model
To construct a model consistent with DSM-IV criteria (American Psychiatric Association, 1994), the BASC-TRS-C was inspected for items with content similar to diagnostic criteria following the procedure of van Lier, et al., (2003). Based on this analysis, it was determined that a sufficient amount of items existed to account for symptoms of inattention, hyperactivity, impulsivity, oppositional defiance, conduct, and anxiety. However, due to sample sizes needed for regression techniques, diagnostic groups were formed only if 25 individuals from the sample met diagnostic criteria.
The following diagnostic groups were formed based on items consistent with a DSM-IV diag-nosis: (1) Attention-Deficit/Hyperactivity Disorder, Predominantly Inattentive Type; (ADHDI; DSM-IV 314.00) and (2) Oppositional Defiant Disorder (ODD; DSM-IV 313.81). To account for the considerable comorbidity that empirical research has found to occur between behavior disorders (Barkley, 1996), a 3rd diagnostic group was formed that consisted of children with ADHD plus another behavior disorder, specifically (3) ADHD + CD or ODD.
A 4th diagnostic group was formed to account for the comorbidity between Generalized Anxiety Disorder (GAD; DSM-IV 300.02) and ADHDI: (4) GAD and GAD + ADHD, Predominantly Inatten-tive Type. A 5th group, (�) Other, was also formed to capture individuals that met diagnostic criteria for a disorder with symptoms of inattention, hyperactivity, impulsivity, oppositional defiance, conduct, and anxiety but could not be analyzed separately due to small sample sizes. In summary, five psychiatric diagnostic groups were formed: (1) ADHDI, (2) ODD, (3) ADHD + CD or ODD, (4) GAD and GAD + ADHDI, and (5) Other.
To form these diagnostic groups, items that were consistent with diagnostic criteria were dichoto-mized where 0 = never or sometimes, and 1= often or almost always true. Individuals who scored above the diagnostic threshold for one disorder, determined by receiving ratings of often or almost always true on a sufficient number of items consistent with a particular diagnosis, were placed in that particular diagnostic category.
Dimensional Classification Model
Scales from the BASC-TRS were combined to form a dimensional classification model. The BASC-TRS yields 10 problem behavior scales: Aggression, Hyperactivity, Conduct Problems, Anxiety, Depres-

The California School Psychologist, 2007, Vol. 12 125
sion, Somatization, Attention Problems, Learning Problems, Atypicality, and Withdrawal. Two over-arching clinical composite dimensions, which are supported by factorial validity evidence, are formed using these scales: Externalizing and Internalizing Problems. The Externalizing Problems dimension is formed by combining the Hyperactivity, Aggression, and Conduct Problems scales. The Internal-izing Problems dimension consists of the Anxiety, Depression, and Somatization scales (Reynolds & Kamphaus, 1992). Individuals were assigned T scores on both the Externalizing and Internalizing dimensions. These dimensional scores were used as the basis for comparison to the other two classifica-tion systems.
Person-oriented Classification Model
Teacher ratings of children, using the BASC-TRS, have been utilized in multivariate, or person-oriented, methods to develop a classification system for child behavior in school. Kamphaus, et al., (1997) used a two-step cluster analytic technique involving a Ward hierarchical analysis followed by an iterative cluster partitioning via a K-means analysis. A seven-cluster solution was proposed to classify the behavioral adjustment of children in elementary school. The proposed clusters that were found to be adequate for classification were (1) Well Adapted, (2) Average, (3) Disruptive Behavior Problems, (4) Academic Problems, (5) Physical Complaints/Worry, (6) General Problems-Severe, and (7) Mildly Disruptive. This seven-cluster solution was substantially replicated across: samples in the U.S. popula-tion (Kamphaus et al., 1997), a U.S. urban sample (DiStefano, et al., 2003), a U.S. rural sample (DiSte-fano, et al., 2003), and a sample in Medellin, Colombia (Kamphaus & DiStefano, 2001). For the current study children were assigned to one of these seven previously constructed behavioral clusters based on their teachers’ ratings.
Comparison of Classification Models
Once individuals were classified according to categorical, dimensional, and person-oriented methods, the relationship between the classification models and the ability to predict educational outcome vari-ables was assessed. The following educational outcomes were collected for each child: (1) Grade Point Average (GPA), (2) Iowa Test of Basic Skills Reading Composite (ITBS Reading; standardized achieve-ment test), (3) Iowa Test of Basic Skills Mathematics Composite (ITBS Math; standardized achievement test), (4) Number of days absent, (5) Number of days tardy, (6) Number of visits to the Opportunity Room (OR, indicative of a discipline problem), and (7) Number of Suspensions. These educational outcomes were collected through examination of school records.
The predictive validity of the classification systems was examined through regression analyses. Separate regression analyses were computed for each outcome variable. Through regression, unstan-dardized predicted values of each outcome variable using each classification method were obtained and used for comparison. Bivariate correlations were computed for each outcome, correlating the outcome with the unstandardized predicted values obtained using each classification method. Cases were excluded listwise. Then, T tests were used to compare the differential predictive validity of the three classification systems to determine if the differences were statistically significant. Specifically, the correlations of clas-sification systems with outcomes were compared with each method (Glass & Stanley, 1970).
Comparison Of Classification Methods

The California School Psychologist, 2007, Vol. 1212�
RESuLTS
Of the 558 students participating in the cross-sectional study, 166 students met diagnostic criteria and were placed into one of the following categories: (1) ADHDI, N=30 (2) ODD, N=32; (3) ADHD + CD or ODD, N=41; (4) GAD and GAD + ADHDI, N=25; and (5) Other, N= 38. T scores on the external-izing and internalizing dimensions were calculated for all 558 students. Scores ranged from 40 to 95 and 39 to 101 respectively. Additionally, each student was placed into one of the person-oriented clusters: (1) Well Adapted, N= 147 (2) Average, N=87 (3) Disruptive Behavior, N=82 Problems, (4) Academic Problems, N=66, (5) Physical Complaints/Worry, N=60 (6) General Problems-Severe, N=26 and (7) Mildly Disruptive, N=90.
overall Strength of Prediction
Multiple regression techniques were used to predict GPA, ITBS reading and math scores, and number of days absent, days tardy, opportunity room visits, and suspensions using categorical (DSM), dimensional (externalizing, internalizing), and person-oriented (cluster) classification methods. Table 1 lists the overall R squared values for this study.
TABLE 1. Classification Methods Predicting Educational Outcomes
R squared values
Outcomes Categorical Dimensional Cluster
GPA .197 .200 .366ITBS Read .047 .082 .110ITBS Math .074 .086 .100# of Days Absent .030 .048 .060# of Days Tardy .006 .013 .017# of OR visits .320 .416 .294# of Suspensions .107 .138 .079
Note: GPA = Grade Point Average; ITBS Read = Iowa Test of Basic Skills Reading composite; ITBS Math = Iowa Test of Basic Skills Mathematics composite; OR = Opportunity Room
Predicting Academic outcomes
GPA. The ability of the three classification methods to predict GPA and standardized achievement scores was analyzed. Correlations between three academic outcomes (GPA, Iowa Test of Basic Skills Reading and Mathematics composites) and the unstandardized predicted values using the three classifi-cation methods (categorical, dimensional, person-oriented or cluster) were analyzed separately. In order to make inferences about the equality of the population correlation coefficient values that used the same sample, T tests were employed. Overall, results suggest that person-oriented methods predicted GPA significantly better than either dimensional or categorical methods, while there was no significant differ-ence in the prediction of GPA using dimensional or categorical methods. (See Table 2.)

The California School Psychologist, 2007, Vol. 12 127
TABLE 2. Correlations between GPA and Predicted Values of GPA
GPA PGPAC PGPACL PGPAD
GPA 1PGPAC .443PGPACL .605 .650PGPAD .447 .735 .694
Note: GPA = Grade Point Average; PGPAC = Predicted GPA using Categorical method; PGPACL = Predicted GPA using CLuster, person-oriented method; PGPAD = Predicted GPA using Dimensional method
Reading and Math Achievement. The Iowa Test of Basic Skills, Reading (ITBSRead) and Mathe-matics (ITBSMath) Composites were used as indicators of reading and math achievement. T-tests among correlations between ITBSMath and the predicted values using the three classification methods did not yield any significant differences, suggesting that the superiority of any method cannot be established for use in predicting mathematics achievement scores. However, results from T-tests among correlations with ITBSRead, suggest that the person-oriented method and the dimensional method predicted reading scores significantly better than the categorical method. (See Table 3.)
TABLE 3. Correlations between ITBS Reading and Predicted Values
ITBSRead PITBSReadC PITBSReadCL PITBSReadD
ITBSRead 1PITBSReadC .217PITBSReadCL .232 .583PITBSReadD .287 .653 .747
Note: ITBSRead = Iowa Test of Basic Skills Reading composite; PITBSReadC = Predicted ITBSRead using Categorical method; PITBSReadCL = Predicted ITBSRead using CLuster, person-oriented method; PITBSReadD = Predicted ITBSRead using Dimensional method
Predicting Attendance and Behavioral outcomes
The ability of these three classification methods to predict the following outcomes throughout the school year was examined: number of days absent, number of days tardy, number of times a student visited the opportunity room (OR, an indicator of discipline problems), and number of suspensions. Correlations between the outcomes and the predicted values of the outcomes using the three different classification methods were examined separately.
Days Absent/Tardy. Results from T tests indicated that the person-oriented method predicted the number of days absent significantly better than the categorical method. However, no other significant differences were noted for days absent. (See Table 4.) No significant differences were noted between the three possible methods of predicting the number of days a student was tardy.
Opportunity Room Visits. When examining the ability of the classification methods to predict Opportunity Room visits, findings suggest that the dimensional method is superior to the categorical and person-oriented method for predicting the number of OR visits. No significant differences were noted between person-oriented and categorical methods. (See Table �.)
Comparison Of Classification Methods

The California School Psychologist, 2007, Vol. 12128
TABLE 4. Correlations between Days Absent (Absent) and Predicted Values
Absent PAbsentC PAbsentCL PAbsentD
Absent 1PAbsentC .174PAbsentCL .246 .467PAbsentD .219 .429 .734
Note: Absent = Number of school days Absent; PAbsentC = Predicted Absent using Categorical method; PAbsentCL = Predicted Absent using CLuster, person-oriented method; PAbsentD = Predicted Absent using Dimensional method
TABLE 5. Correlations between Number of Visits to OR and Predicted Value
#OR P#ORC P#ORCL P#ORD
#OR 1P#ORC .565P#ORCL .542 .723P#ORD .645 .812 .797
Note: #OR = Number of visits to the Opportunity Room; P#ORP = Predicted #OR using Categorical method; P#ORCL = Predicted #OR using CLuster, person-oriented method; P#ORD = Predicted #OR using Dimensional method
Suspensions. T tests examining the significant differences using the three classification methods indicated that the dimensional method of classification was superior to the person-oriented method when predicting suspensions. No other significant differences were noted. (See Table 6.)
TABLE 6. Correlations between Number of Suspensions and Predicted Values
#Suspend P#SuspendC P#SuspendCL P#SuspendD
#Suspend 1P#SuspendC .327P#SuspendCL .281 .628P#SuspendD .371 .663 .796
Note: Absent = Number of school days Absent; PAbsentC = Predicted Absent using Categorical method; PAbsentCL = Predicted Absent using CLuster, person-oriented method; PAbsentD = Predicted Absent using Dimensional method
DISCuSSIon
The aim of this study was to compare categorical, dimensional, and person-oriented methods of classification for use in predicting school-based outcomes. Through examination of overall R squared values, the value of the categorical, dimensional, and person-oriented methods for predicting educational outcomes was modest. All three classification approaches yielded results suggesting that they were best able to predict later grade point averages (GPA) and number of visits to the opportunity room when compared with other outcome variables. However, the overall ability of these classification models for use in predicting days absent, days tardy, and reading and math achievement is questionable.

The California School Psychologist, 2007, Vol. 12 129
Despite somewhat unfavorable results suggesting that these classification methods were not optimal for predicting educational outcomes, differences among the classification methods were revealed. When examining GPA, person-oriented methods were clearly superior to both dimensional and categorical methods. In schools, GPA is often a global indicator of functioning in the classroom suggesting that person-oriented methods might allow for the prediction of global functioning. Similarly, person-oriented methods were found to be superior to categorical methods for predicting reading achievement scores and days absent.
Dimensional methods of classification were found to be superior to categorical methods for predicting reading achievement scores and number of visits to the opportunity room. Dimensional methods were also found to be better able to predict number of visits to the opportunity room and number of suspen-sions than person-oriented methods of classification. This finding suggests that, for behavioral outcomes, knowledge about a student’s externalizing and internalizing functioning might be sufficient. In other words, the additional dimensional scales used to create a person-oriented classification system were not more predictive than the two dimensional scales used in the dimensional system.
In the current study, categorical classification methods using DSM criteria were not found to be superior for predicting any of the educational outcomes. This knowledge is significant when consid-ering that students in educational systems are currently being classified according to categorical methods (DSM or IDEA). Person-oriented or dimensional methods of classification were found to better predict grade point average, standardized reading achievement measures, number of days absent, number of visits to the opportunity room, and number of suspensions than categorical classification methods.
Similar to results found by Fergusson and Horwood (1995), the current study found the dimensional classification system to show better evidence of predictive validity than a purely categorical system. However, this study did not replicate the findings by Greenberg and colleagues (2001) that indicated the relative superiority of person-oriented methods over individual variable approaches in predicting risk factors of conduct problems. Specifically, the dimensional method utilized in the current study appeared to be superior to person-oriented methods when predicting behavioral outcomes. When predicting many of the educational outcomes, results of the current study were more consistent with findings by Haapasalo et al. (2000), suggesting few differences between the cluster and dimensional approaches. While the ability of person-oriented, dimensional, and categorical classification methods to predict educational outcomes warrants further investigation, the results of this study reveal the relative superi-ority of person-oriented and dimensional methods of classification over the frequently used categorical methods. However, it remains unclear if person-oriented methods are superior to dimensional methods when predicting behavioral outcomes.
There are a number of limitations in this study that should be highlighted. This study was limited in the availability of behavioral outcomes, which would be hypothesized to be more highly correlated with classification systems utilizing teacher ratings of emotional and behavioral functioning. Additionally, the validity of some of the outcome measures, particularly number of suspensions, is questionable due to the fact that they are based on complex teacher and school processes beyond the child’s problems. Another limitation of this study is that the three classification methods were formed based on results of one instrument, the BASC-TRS. Information regarding a student’s categorical classification, such as a current DSM diagnosis, was unavailable. However, it would have been desirable to obtain diagnostic information through a diagnostic semi-structured interview, such as the Diagnostic Interview Schedule for Children (DISC-IV), or another comprehensive measure to assist in forming the categorical clas-sification model.
Comparison Of Classification Methods

The California School Psychologist, 2007, Vol. 12130
Despite limitations, these results are consistent with previous research suggesting the inadequacies of current categorical classification methods. As school psychologists are often called upon to place students into categories, such as determining their eligibility for special education, they should be aware of the limitations of current classification methods used in the schools. The ability of current classifica-tion models to predict later school outcomes is questionable. Additionally, previous research suggests that students, while they might not meet criteria for special education placement, could be experiencing functional impairment or lower levels of risk. This points to the need for prevention and early interven-tion services for students experiencing significant functional impairment or risk, regardless of classifi-cation or placement in special education. Furthermore, school psychologists would benefit from gath-ering comprehensive information regarding students’ functioning, an approach more consistent with dimensional and person-oriented methodologies. Relying solely on information regarding placement eligibility, such as that obtained for categorical classification, might prove insufficient and further the “wait to fail” treatment approach. It should also be emphasized that the present findings point to the need for future research into classification methods for use with school-age children. Particularly, methods utilizing a person-oriented or dimensional approach to classification should be further investigated.
REfEREnCES
Achenbach, T. (1998). Diagnosis, assessment, taxonomy, and case formulations. In T. Ollendick and M. Hersen (Eds.). Handbook of Child Psychopathology (3rd ed.) (pp. 63-87). New York: Plenum Press.
Achenbach, T. (2001). Challenges and benefits of assessment, diagnosis, and taxonomy for clinical practice and research. Australian and New Zealand Journal of Psychiatry, 35 (3), 263–271.
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th ed). Wash-ington, DC: Author.
Barkley, R. A. (1996). Attention-deficit/hyperactivity disorder. In E.J. Mash & R.A. Barkley (Eds.), Child Psychopathology. New York: Guilford Press.Bergman, L. R., & Magnusson, D. (1997). A person-oriented approach in research on developmental psychopa-
thology. Development & Psychopathology, 9(2) 291-319.Beutler, L. E. & Malik, M. L. (2002). Rethinking the DSM: A psychological perspective. Washington, DC: American
Psychological Association. Blanchard, K. A., Morgenstern, J., Morgan, T. J., Labouvie, E. & Bux, D. A. (2003). Motivational subtypes and continuous measures of readiness for change: concurrent and predictive validity.
Psychology of Addictive Behaviors, 17, 1, 56-65.Blashfield, R. K. (1998). Diagnostic models and systems. In A. S. Bellack, M. Hersen, & C. R. Reynolds (Eds.),
Comprehensive clinical psychology: (Vol.4) Assessment. New York: Elsevier Science. Cantwell, D. P. (1996). Classification of child and adolescent psychopathology. Journal of Child Psychology and
Psychiatry, 37, 3-12.Deater-Deckard, K., Reiss, D., Hetherington, E. M., & Plomin, R. (1997). Dimensions and disorders of adolescent
adjustment: A quantitative genetic analysis of unselected samples and selected extremes. Journal of Child Psychology and Psychiatry, 38(5), 515-525.
DiStefano, C., Kamphaus, R. W., Horne, A. M., & Winsor, A. P. (2003). Behavioral Adjustment in the U.S. Elemen-tary School: Cross-validation of a Person-oriented Typology of Risk. Journal of Psychoeducational Assessment, 21, 338-357.
Dowdy, E., Hendry, C., & Kamphaus, R. W. (2006). Clusters of child adjustment. In R.W. Kamphaus & J. M. Camp-bell, (Eds.), Psychodiagnostic Assessment of Children (pp. 437-464). Hoboken, NJ: John Wiley & Sons, Inc.
Fergusson, D. M., & Horwood, J. (1995). Predictive validity of categorically and dimensionally scored measures of disruptive childhood behaviors. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 477-487.
Flanagan, K. S., Bierman, K. L., & Kam, C. M. (2003). Identifying at-risk children at school entry: the usefulness of multibehavioral problem profiles. Journal of Clinical Child and Adolescent Psychology, 32, 396-407).
Glass, G., & Stanley, J. (1970). Statistical methods in education and psychology. Oxford, England: Prentice-Hall.

The California School Psychologist, 2007, Vol. 12 131
Gottlieb, G. (2000). Understanding genetic activity within a holistic framework. In L. R. Bergman, R. B. Cairns, L. G. Nilsson, & L. Nested, (Eds.), Developmental Science and the Holistic Approach (pp. 180-201). Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
Greenberg, M. T., Speltz, M. L., DeKlyen, M. & Jones, K. (2001). Correlates of clinic referral for early conduct problems: variable- and person-oriented approaches. Development and Psychopathology, 13, 255-276.
Haapasalo, J., Tremblay, R. E., Boulerice, B., & Vitaro, F. (2000). Relative advantages of person–and variable-based approaches for predicting problem behaviors from kindergarten assessments. Journal of Quantitative Crimi-nology, 1�, 2, 145-168.
Helzer, J. E. & Hudziak, J. J. (2000). Defining psychopathology in the 21st century: DSM-V and beyond. Wash-ington, DC: American Psychiatric Association.
Houts, A. C. (2002). Discovery, invention, and the expansion of the modern diagnostic and statistical manuals of mental disorders. In Defining psychopathology in the
21st century: DSM-V and beyond. Washington, DC: American Psychiatric Association. Hudziak, J. J., Wadsworth, B. A., Heath, A. C., & Achenbach, T. M. (1999).
Latent class analysis of child behavior checklist attention problems. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 985–991.
Jensen, P. S., Watanabe, H. K., Richters, J. E., Roper, M., Hibbs, E., Salzberg, A., & Liu, S. (1996). Scales, diag-nosis, and child psychopathology: II. Comparing the CBCL and the DISC against external validators. Journal of Abnormal Child Psychology, 24(2), 151-168.
Jimerson, S. R., Coffino, B., & Sroufe, L. A. (2007). Building school-based Interventions on attachment theory and research. Journal of Early Childhood and Infant Psychology, 3, 79-94.
Kagan, J. (1997). Conceptualizing psychopathology: the importance of developmental profiles. Development and Psychopathology, 9, 321-334.
Kamphaus, R. W. & DiStefano, C. (2001). Evaluación multidimensional de la psicopatología infantíl. Revista de Neuropsicología, Neuropsyqiatría y Neurociencias. 3(1), 85-98.
Kamphaus, R. W., DiStefano, C., & Lease, A. M. (2003). A self-report typology of behavioral adjustment for young children. Psychological Assessment, 15(1), 17-28.
Kamphaus, R. W., Huberty, C. J., DiStefano, C., & Petoskey, M. D. (1997). A typology of teacher rated child behavior for a national U. S. sample. Journal of Abnormal Child Psychology, 25, 453-463.
Lessing, E. E., Williams, V., & Gil, E. (1982). A cluster-analytically derived typology: feasible alternative to clinical diagnostic classification of children? Journal of Abnormal Child Psychology, 10, 451-482.
Mattison, R. E. & Spitznagel, E. L. (1999). Long-term stability of child behavior checklist profile types in a child psychiatric clinic population. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 700- 707.
Meehl, P. E. (1995). Bootstraps taxometrics: Solving the classification problem in psychopathology. American Psychologist, 50, 266-275.
Millon, T. (1991). Classification in psychopathology: rationale, alternatives, and standards. Journal of Abnormal Psychology, 100, 245-261.
Nease, D. E., Volk, R. J., & Cass, A. R. (1999). Investigation of a severity-based classification of mood and anxiety symptoms in primary care patients. Journal of the American Board of Family Practice, 12(1), 21-31.
Reynolds, C. R., & Kamphaus, R. W. (1992). Behavior Assessment System for Children. Circle Pines, MN: Amer-ican Guidance Service, Inc.
Richters, J. E. (1997). The Hubble hypothesis and the developmentalists’ dilemma. Development and Psychopa-thology, 9(2), 193-229.
Scahill, L., Schwab-Stone, M., Merikangas, K. R., Leckman, J. F., Zhang, H., & Kasl, S. (1999). Psychosocial and clinical correlates of ADHD in a community sample of school-age children. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 976–984.
Scotti, J. R., & Morris, T. L. (2000). Diagnosis and classification. In M. Hersen & R. T. Ammerman (Eds.) Advanced abnormal child psychology. Mahwah, NJ: Erlbaum.
Speece, D. L., & Cooper, D. H. (1991). Retreat, regroup, or advance? An agenda for empirical classification research in learning disabilities. In L.V. Feagans, E.J. Short, & L.J. Meltzer (Eds.), Subtypes of learning disabilities. Hill-sdale, NJ: Lawrence Erlbaum Associates, Inc.
Sroufe, L. A., Egeland, B., Carlson, E. A., & Collins, W. A. (2005a). The development of the person: The Minnesota study of risk and adaptation from birth to adulthood. New York: Guilford Press.
Toshiaki, F., Awaji, R., Nakazato, H., & Sumita, Y. (1995). Predictive validity of subtypes of chronic affective disor-ders derived by cluster analysis. Acta Psychiatrica Scandinavica, 91, 379-385
Comparison Of Classification Methods

The California School Psychologist, 2007, Vol. 12132
Van Lier, P.A.C., Verhulst, F.C., van der Ende, J., & Crijnen, A.A.M. (2003). Classes of disruptive behaviour in a sample of young elementary school children. Journal of Child Psychology and Psychiatry and Applied Disci-plines, 44, 377-387.
Waddington, C.H. (1971). Concepts of Development. In L.R. Aronson, E. Shaw, & E Tobach, (Eds.), Biopsychology of Development (pp. 17-23). New York: Academic Press.