The “JaW PrinT” Study: Jaw reconstruction With Printed or ... · presentation than early stage...
25
JaW PrinT Protocol v1.8_22.12.2017 1 The “JaW PrinT” Study: Jaw reconstruction With Printed or flexed Titanium and free tissue transfer. A collaboration between Abertawe Bro Morgannwg University Health Board, University of South Wales and Renishaw PLC.
Transcript of The “JaW PrinT” Study: Jaw reconstruction With Printed or ... · presentation than early stage...

JaWPrinTProtocolv1.8_22.12.2017 1
The“JaWPrinT”Study:
JawreconstructionWithPrintedorflexedTitaniumandfreetissuetransfer.
AcollaborationbetweenAbertaweBroMorgannwgUniversityHealthBoard,UniversityofSouthWalesandRenishawPLC.

JaWPrinTProtocolv1.8_22.12.2017 2
Table of Contents Table of Contents ..................................................................................................... 2
List of Abbreviations ................................................................................................. 3
1.0 Study Team ...................................................................................................... 31.1DetailsofResearchTeam.............................................................................................................................32.0 Literature Review and Study Rationale............................................................ 42.1 Introduction/context...............................................................................................................................42.2 Computeraided3Dplanningandcrudecustomisationofmandibularreconstructionosseosynthesisplates............................................................................................................62.3 3Dprintinginmandibularreconstruction......................................................................................62.4 Summary...........................................................................................................................................................73.0 Study aims and objectives ............................................................................... 73.1 Primaryoutcome..........................................................................................................................................73.2 Secondaryoutcomes...................................................................................................................................74.0 Study design..................................................................................................... 84.1 Inclusioncriteria........................................................................................................................................124.2 Exclusioncriteria.......................................................................................................................................124.3 Recruitment..................................................................................................................................................124.4 Randomization............................................................................................................................................124.5 Studyprocedures.......................................................................................................................................134.5.1 BaselineAssessment..........................................................................................................................134.5.2 Perioperative/inpatientdatacollection..................................................................................134.5.3 6weeksfollowup................................................................................................................................144.5.3 6monthsfollowup.............................................................................................................................144.5.4 1yearfollowup...................................................................................................................................14
5.0 Risk management .......................................................................................... 15
6.0 Statistical analysis .......................................................................................... 16
7.0 Data management and quality control .......................................................... 16
8.0 Ethical considerations .................................................................................... 16
9.0 Funding .......................................................................................................... 17
10.0 Study timeline .............................................................................................. 17
11.0 References ................................................................................................... 18
12.0 Appendices .................................................................................................. 20AppendixA................................................................................................................................................................20AppendixB................................................................................................................................................................23

JaWPrinTProtocolv1.8_22.12.2017 3
List of Abbreviations ABMUHB AbertaweBroMorgannwgHealthBoardCAD-CAM Computeraideddesign–ComputeraidedmanufactureCMF Cranio-maxillo-facial(surgery)CBCT Cone-beamcomputertomography(dental)CT Computertomography(medical)H&N Head&Neck(surgery)HRQOL HealthrelatedqualityoflifeORN Osteoradionecrosis(ofthemandible)PI PrincipalinvestigatorPSI Patient-specificimplantSLM Selectivelasermelting3D Three-dimensional
1.0 Study Team MrAlexanderGoodson Postgraduate(PhD)student
investigatorProfessorMarkWilliams ChiefInvestigator&PhDDirectorof
StudiesMrMadhavKittur PrincipalInvestigatorforABMU
HealthBoardMrPeterEvans Co-investigator,ABMUHealthBoard
1.1 Details of Research Team Name: ProfessorMarkWilliamsRole: ChiefInvestigatorAddress: FacultyofLifeSciencesandEducation UniversityofSouthWales CemeteryRoad
GlyntaffCF374BD
Telephone: 01443654578Email: [email protected]

JaWPrinTProtocolv1.8_22.12.2017 4
Name: MrAlexanderGoodsonRole: PhDStudentInvestigatorAddress: FacultyofLifeSciencesandEducation UniversityofSouthWales GlyntafCampus Pontypridd,CF371DL Telephone: 01443654578Email: [email protected]: MrMadhavKitturRole: PrincipalInvestigatorforABMUHealthBoardAddress: MorristonHospital HeolMaesEglwys
MorristonSwanseaSA66NL
Telephone: 01792703162Email: [email protected]: MrPeterEvansRole: Co-investigatorAddress: MorristonHospital HeolMaesEglwys
MorristonSwanseaSA66NL
Telephone: 01792703162Email: [email protected]
2.0 Literature Review and Study Rationale
2.1 Introduction / context Headandneck(H&N)cancerincludescancersoriginatingfromvarious(andoftenoverlapping)sub-sitesintheheadandneckregion(includingtheoralcavity,pharynx,larynx,noseandparanasalsinuses).H&NcanceristheeighthmostcommoncancerintheUK(2014).IntheUK(mainland)itisfourtimescommonerinmenthanwomen,andgeographicallyEuropeanage-standardised(AS)incidenceratesarehigherinmalesinWalesthanEngland(withrateshighestinScotlandoverallforbothsexes).H&Ncancerincidencehasincreasedinbothsexessincethe1990swithagreaterpercentageincreaseamongstfemales,closingthegenderdifferenceinincidenceovertime.(Cancer_Research_UK)
Forheadandneckcanceringeneral,latestagediseaseisacommonerpresentationthanearlystagedisease(62%arestageIII/IVatpresentation

JaWPrinTProtocolv1.8_22.12.2017 5
versus38%atstageI/II).(NICR,2016)Consequently,majorresectivesurgery,aimingforcure(withimmediatereconstructionforoptimalfunctionaloutcome)iscommonplace.Inthecaseoforalcancerspecifically,advancedtumoursfrequentlyinvolvethemandible(lowerjawbone),requiringresection/removalofpartofthemandibletoavariableextent,dependingonthenatureofthetumour(with/withoutpostoperativeradiotherapy,dependinguponpatientandtumour-specificfactors).
Radiotherapyiscommonlyusedinheadandneckcancerinisolation(asanalterativetosurgery),mostcommonlyforlaryngealandtonguebasetumoursasithelpstopreservenaturalspeechandswallowing.Howeverforadvancedsquamouscellcarcinomas(SCCs),combinedtreatmentmodalities(surgeryandradiotherapy/chemotherapyandradiotherapy)offerthehighestchanceofcure.(Nutting,2016)Forpatientsinwhomradiotherapyisused,thereisanadditionallifelongriskofdevelopingosteoradionecrosis(ORN)ofthemandibleasaside-effect.Osteoradionecrosisisineffect,“hypovascularityandnecrosisofbonefollowedbytrauma-inducedorspontaneousmucosalbreakdown,leadingtoanon-healingwound.”(Butterworthetal.,2016)Inthelatterstagesofthediseaseprocess,ORNcanresultinpathologicalfractureofthemandibleand/oranorocutaneousfistula,requiringfreetissuetransfertorepairthedefect.(LyonsandBrennan,2014)Consequently,inthecontextofmanagingheadandneckcancer,mandibularreconstructionwithtitaniumplatesandfreetissuetransferiscommonlyperformed;notonlyforimmediatereconstructionaftersurgicalresectionofadvancedtumours,butalsofortreatmentoflate-stageORN.Furthermore,similartechniquescanbeusedforextensiveandprogressive(buthistologicallybenign)jawtumours.
Choiceofreconstructivetechniqueformandibulardefectsdependsontheamountofbonetoberesected.(Brownetal.,2016)However,inlargerdefects,itisfeltbymanysurgeonsthatthegoldstandardformandibularreconstructionisafibulafreeflap(autologousvascularizedboneandsofttissue,transplantedfromthelegandanastomosedtoanarteriovenoussupplyintheneck)supportedwithinanosseosynthesisplatetofacilitateprimarybonyunion/healing.(Kokosisetal.,2016)Otherchoicesofbonyfree-flapscanbeusedsuchasthedeepcircumflexiliacartery(DCIA)flap,favouredoverthefibulafreeflapbysomeauthors.(Chenetal.,2014)Mostosseosynthesisplatesusedforthispurposearecomposedoftitanium,becauseofitsintrinsicbiocompatibilityandhighstrength-to-weightratio.(Parthasarathy,2014).Traditionally,titaniumwasflexedormouldedintraoperativelybyeye(duringsurgery)toreconstructmandibulardefects,withoutthemodernbenefitsofpreoperative3Dcomputer-aidedplanning.Theprocessofflexingarigidosseosynthesisplateformandibularreconstructioninherentlycontributestotheoveralldurationofthesurgery,isdependentupontheexperienceandskillofthesurgeonandcarriestheriskofhumanerrorindimensionalaccuracyofthereconstruction,simplybecauseitisdone‘byhandandbyeye’.Furthermore,manuallydeformingtitaniumimplantsinthismannercreatesintrinsicstresseswithintheimplantedmaterial,potentiallyweakeningtheoverallreconstructioninthelongtermwhilstsubjectedtocyclicalloadingforcesfrommastication/chewingforexample.(Parketal.,2016)

JaWPrinTProtocolv1.8_22.12.2017 6
2.2 Computer aided 3D planning and customisation of mandibular reconstruction osseosynthesis plates Threedimensional(3D)planningandvirtualsurgeryhasevolvedinrecentyearsanditispostulatedthatitimprovesefficiency,accuracy,creativityandreproducibilityinCMFsurgeryinparticular.(Steinbacher,2015)Rapidprototypingisaprocessbywhichastereolithigraphicresinmodelcanbeproducedfollowingcollectionofdatafrom3Dimagingsuchascomputertomography(CT)scanning.Theprocessofvirtualsurgery(followinganalysisof3Dimagingdata)providesthemeanstorapid-prototypeastereolithigraphicresinmodel/moulduponwhichatitaniumimplantcanbeflexed,pressedormouldedpreoperatively(andmostimportantly,checkedagainstthestereolithigraphicmodel)forsubsequentintraoperativeuse.ThistechniquehasbecomecommonplaceinUKmaxillofacialcentres.Whencomparedtotraditionalintraoperativeshapingtechniques,itimprovesaccuracyandefficiencyinmandibularreconstruction(notablyeliminatingthetimetakenduringsurgerytobendtheplatebyeyethatwouldotherwiseberequiredusingthetraditionalapproach,yetallowingasmuchtimeasneededbythetechnicianpreoperativelytoachievethebest‘handmade’resultpossible).(Giletal.,2015)Nevertheless,thistypeof‘customisation’stillremainsopentoconsiderableinaccuracies/humanerrorsofthetechnicianinflexingtheplatebyhand.Furthermoretheriskofintroducingmechanicalweaknessesbyflexingtheplateremains.Besidesproducingpatient-specificimplants(PSIs),3Dplanningandvirtualsurgeryfacilitatestheproductionofintraoperativesurgicalcuttinganddrillingguides/’stents’,whichimproveaccuracyofbonecuts(osteotomies)inmandibularreconstructionwithfibulafreeflapsandaidspreciseplacementofosseointegrateddentalimplants(Wangetal.,2016,Allum,2008).
2.3 3D printing in mandibular reconstruction Itisclearthattodate,3DCAD-CAMhasimprovedtheaccuracyofmandibularreconstructionsinhead&neckoncologysurgery.Withtheadventof“3Dprinting”(morespecificallyselectivelasermelting;SLM),ithasbeenproposedbyoneauthorgroupthatlasersinteredmandibularreconstructionplatesreducethedurationofsurgeryandfrequencyofcomplications,aswellasproducingamoreaccuratereconstructionduetotheeliminationofhumanerrorinthefinalstagesoffabrication(incontrasttothe“pre-flexingtoarapid-prototypedstereolithigraphicmodel”approach).TheauthorssuggestthatfurtherrandomizedstudieswouldbeusefultodeterminewhetherCAD-CAMmandibularreconstructioniseconomicallysustainableinmaxillofacialoncologysurgery(Tarsitanoetal.,2016).CurrentlyateaminHongKongareprospectivelyevaluatingclinicaloutcomesandcomplicationsoflasersinteredmandibularreconstructionplatesinaproposedseriesof48patients(Su,2017).However,todatetherearenorandomizedtrialscomparingclinicaland

JaWPrinTProtocolv1.8_22.12.2017 7
economicoutcomesin3D-printedmandibularreconstructionplatesandcuttingguidesversusmanuallypre-flexedplatetechniques.
2.4 Summary Insummary,3Dprinting(SLM)oftitaniumprovidesanopportunitytonegatetheimpactofhumanerrorincustomisationofmandibularreconstructionosseosynthesisplatesandalignmentofosteotomies,potentiallyimprovinguponthepredictabilityandprecisionofmandibularreconstructioninhead&neckcancerpatients.However,withalackofhigh-levelevidencetodate,thereisnoclearconsensusonwhethertheSLMapproachprovidesabettertreatmentsolutionwhencomparedtoothermoreestablished,butpotentiallymorecrudetechniquesofplatecustomization(pre-flexingtoarapidprototypedmodel).Consequentlyasituationofclinicalequipoiseexistsandinthiscontext,warrantsawell-designedobservationalstudytoevaluateanydifferencesbetweenthetwotreatmentapproaches.
3.0 Study aims and objectives
3.1 Primary outcome Primarily,thestudyaimstoevaluate:
1. Predictabilityandresultantdimensionalaccuracyofmandibularreconstructionsperformedusing:
o Fibularfree-flapreconstructionofthemandiblewithacustomizedpre-flexedmandibularreconstructionplateandcuttingguides(TreatmentpathwayA)
ORo Fibularfree-flapreconstructionofthemandiblewithacustomized
SLMmandibularreconstructionplateandcuttingguides(TreatmentpathwayB)
3.2 Secondary outcomes Secondarily,thestudyaimstocomparetreatmentpathwaysAandBfor:
2. Thedurationofsurgery(inparticularindividualcomponentsofthesurgerysuchasflapwarmischaemiatime,durationofosteotomiesandplatefixationprocedures.

JaWPrinTProtocolv1.8_22.12.2017 8
3. Theoperators’perceptionsoftheoverallintraoperativeusability,confidencewiththetechniqueandimmediatesatisfactionofthesurgicalresult.
4. Theneedtomakeminoradjustmentstoeithertheplate,osteotomyorscrewholesinordertofittheplateduringsurgery.
5. Incidenceofpostoperativecomplications(asrecordedduringinpatientstayaswellasat6weeks,6monthsand1yearoutpatientfollowupvisits),forexample:
a. Localisedinfectionb. Plateextrusion/exposurec. Lengthofhospitalstay(includingdurationofintensivecare/high-
dependency/wardrequirements)d. Mal/non/delayed-unionofthebonycomponentsofthe
mandibularreconstruction(fromobjectiveanalysisofclinicallyroutinepostoperativeCTscanimaging)
e. Platefractures/failures6. Medium-term(upto1year)functionaloutcomes,forexample:
a. Feasibilityofdentalimplantrehabilitation(specificallyinthetechnicalcontextofclinicaland/orradiologicalperspectiveofbonequalityandanatomyaswellasintheholisticcontextofthepatient’ssuitabilityoverall,inordertodeterminetheimportanceofreconstructedbonyanatomyinthedecisionprocessesandplanningofdentalrehabilitation)
b. Objectiveevaluationofchangesindentalocclusion(withtheaidofdentalmodelanalysis).
c. Objectiveassessmentofchangesinfacialaesthetics(facialsymmetrybaseduponbaselineandpostoperative3Dphotography(stereophotogrammetry).
7. Patient-perceivedqualityoflife:a. usingavalidatedqualityoflifeassessmenttools:
i. UniversityofWashingtonQualityofLifeQuestionnairev4ii. Short-formDerrifordappearancescale(DAS24)iii. Liverpooloralrehabilitationquestionnaire
b. bytimetoreturntowork/socialstatusat1year(whereapplicable)
8. Economicimplications(witheconomicanalysistakingtheaboveclinicalandsocialoutcomesintoaccount).
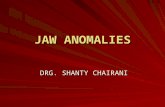
4.0 Study design JaWPrinTisa‘real-world’prospectiveobservationalpilotstudy,evaluatingtheclinicaleffectiveness,usabilityandeconomicsoftwoapproachestomandibularreconstructionsurgery(figure1).Patientparticipantswillberecruitedprospectivelyoveraminimumperiodof18months(withobservationofatleast10participantsineachtreatmentpathway).Thefiguresarebaseduponthehistoricalclinicalpracticeoftheresearchsite,withbothtechniquesinequaluse;

JaWPrinTProtocolv1.8_22.12.2017 9
choicedependingonresources,surgicaltrainingrequirementsandsurgeon’sclinicalpreference.Asapurelyobservationalstudy,treatmentchoicewillbemadeinthenormalclinicalmannerandwillinnowaybeinfluencedbythestudyitself.Participantswillbefollowedupattheirroutineoutpatientclinics(6weeks,6monthsand1yearpostoperatively)withprospectiveoutcomesdatacollection(figure1).

JaWPrinTProtocolv1.8_22.12.2017 10
PI to prospectively identify potential study participants from weekly maxillofacial and H&N surgery clinics
• Participants to be recruited over a minimum period of 18 months; minimum of 10 patients in each
treatment pathway. • On clinic, potential participants will be asked by the PI if they are interested in taking part in the study. • The PI, after meeting the potential participant, will confirm their eligibility. • Eligible participants meeting inclusion and exclusion criteria will be sent an invitation letter with a
participant information sheet and a consent form (emphasizing the option to either decline or accept the offer of study participation).
Preoperative baseline data collection (CRF01 form). • Medical history and screening of comorbidities (including comorbidity score & performance status), smoking and alcohol status. • Evaluate for history of any previous radiotherapy treatment (date started and completed, regime details). • Physical assessment (BMI, oral hygeine status). • Detailed social history • University of Washington QoL Questionnaire v4. • Short-form Derriford appearance scale (DAS24). • Liverpool oral rehabilitation questionnaire. • 3D Photograph (Stereophotogrammetry) of the head and neck • Baseline clinical blood tests (FBC, U&E, Clotting screen)
Do not enter study
Treatment allocated in normal clinical manner by surgeon to either pathway A (surgery with pre-flexed plate) or pathway B (surgery
with SLM plate).
Participant blinded to treatment allocation at this stage
Pathway A (Customized pre-
flexed plate) n ≥10
Pathway B (Customized SLM
plate) n ≥10
Perioperative / inpatient data collection (CRF02 form). • Prior to commencing surgery, bite registration to be obtained (using viscoelastic silicone impression putty) • At surgery, record of:
o Times at which mandibular osteotomies are first started (cutting guides first placed onto mandible) and completed o Time of knife-to-skin for flap harvest o Time of flap detachment o Time of completing fixation of the plate (with flap) in its final resting position (i.e. when completion of fixation to the residual mandible) o Time of completing arterial anastomosis
• Record of need for any intraoperative adjustment to the plate, osteotomies and/or planned drill hole positions. • Surgeon rating of usability, confidence of use, satisfaction with reconstructive procedure. • Scrub nurse rating of usability, confidence of use, satisfaction with reconstructive procedure. • Record of days-stayed on ITU / HDU and/or Ward, date of discharge. • Record of all complications as inpatient (peri & post operative).
Consent • At the next routine clinical appointment, the potential patient participant’s decision will be noted. • Should the patient wish to participate, the PI will obtain their written informed consent accordingly.

JaWPrinTProtocolv1.8_22.12.2017 11
6 weeks follow up (CRF03 form). • Physicalassessment(BMI,oralhygeinestatus).• UniversityofWashingtonQoLquestionnaire.• Short-formDerrifordappearancescale(DAS24).• Liverpooloralrehabilitationquestionnaire.• Reportoncomplications.• 3D Photograph (Stereophotogrammetry) of the head and neck. • Detailedsocialhistory(e.g.currentoccupation/employment)
6 months follow up (CRF04 form). • Data recorded as per CRF03 form. • Postoperative CT mandible scan (evaluation of actual vs. planned dimensions, quantitative evaluation of bony cortical union at osteotomy sites)
1 year follow up (CRF05 form). • Data recorded as per CRF03 form. • Dental assessment (including routine cone beam CT scan) and restorative dentist rating of technical and practical feasibility of prosthetic rehabilitation
options
End of study Patients informed of treatment type received.
Figure1.TheJaWPrinTstudydesign

JaWPrinTProtocolv1.8_22.12.2017 12
4.1 Inclusion criteria
• Ageover18years• Abletoprovideinformedconsent• Aplannedfibularfree-flapreconstructionofthemandible• PlannedpostoperativesurveillanceCTscan6monthsfollowingsurgery
4.2 Exclusion criteria
• Clinicallyunfitorinappropriate(baseduponprognosis/lifeexpectancy)forreconstructionusingfreetissuetransfertechniques
• Patientswithplannedsurgicaldefectsinvolvingreconstructionofthecondyle:i.e.BrownclassIc,IIcorIVc.(Clinicaluseofprintedplatesforcondylarreconstructionswouldineffectbe‘off-licence’andnon-standardtreatmentwhichisbeyondtheremitofanobservationalresearchstudy).
• Flapfailurewithinthestudyfollow-upperiod,asthiswouldrequireearlyremovaloftheflapandthereforeprecludecollectionoffollow-upoutcomedata.However,anyflapfailures(andassociatedclinicalcomplications/events)willberecordedandreported.
4.3 Recruitment ParticipantswillberecruitedprospectivelyastheypresentasnewpatientcasestotheABMUMaxillofacialandHead&Neckcancermultidisciplinaryteam(MDT)clinics.Onceapotentialpatientparticipanthasbeengivenhis/herdiagnosisanditisconfirmedbytheprincipalinvestigator(PI)thathe/shemeetstheinclusioncriteria,clinicstaffwillprovidethepotentialparticipantwithaninvitationletterintroducingthestudyaswellasapatientinformationsheetandconsentform(explainingtheavailableoptionsofparticipatingorrefrainingfromthestudy).Patientswillbeallowedupto24hourstodecidewhetherornottoparticipateastoavoidanyimpact/delayontheschedulingoftheirclinicaltreatment.ThePIwillobtainwritteninformedconsentfromwillingparticipants.
4.4 Treatment pathway allocation Uponrecruitment,provisionofinformedconsentandcollectionofbaselinedata,asperstandardclinicalpractice,thepatientparticipant’sCTscandataisusedtoproduceavirtualsurgicalplanforthemandibularresectionandfibularfree-flapreconstruction.Oncetheclinicallyoptimalreconstructivesurgicalplanisestablishedbythesurgeonandtechnician,thechoiceofsurgicalapproachwillbemadeintheroutineclinicalmannerbythesurgeon:PathwayA(pre-flexedcustomizedmandibularreconstructionplateandcuttingguides)ortopathwayB(SLMcustomizedmandibularreconstructionplateandcuttingguides).Both

JaWPrinTProtocolv1.8_22.12.2017 13
treatmentpathwaysarealreadypartofroutine/standardclinicalpracticeatABMUHB.Theexpected/plannedpatientnumbersforthisstudyarebaseduponthehistoricalworkloadoftheOralandMaxillofacialSurgerydepartmentatAbertaweBroMorgannwgUniversityHealthBoard(ABMUHB)of10-20casesannually.Arecruitmentperiodof18monthswithfollow-upfor1yearfitswithinthetimeconstraintsofthepostgraduatestudentinvestigator’sPhDtimeline.
4.5 Study procedures
4.5.1 Baseline Assessment Thiswillbeperformedusinga“baselinecasereportform”(CRF01),whichwillincludepastmedicalhistory(withattentiontoanyhistoryofpreviousradiotherapytotheheadandneckregion);a‘systemsreview’toscreenforundisclosedcomorbiditiesaswellassmokingandalcoholstatus.Thepatientparticipant’scomorbidityandperformancestatusscoreswillalsoberecorded.Thequalitative/subjectiveassessmentoforalhygienestatus(good/fair/poor)byaconsultantoralandmaxillofacialsurgeonwillalsoberecorded.Collectedfromroutineclinicalpreoperativetests,BMIandserumalbuminconcentrationwillberecordedasanindicatorofnutritionalstatus,alongwithafullbloodcount,ureaandelectrolytesandclottingscreen.BaselinequalityoflifeassessmentwillbeperformedusingtheUniversityofWashingtonQoLQuestionnairev4(Rogersetal.,2002)(AppendixA).Abaselineassessmentoftheparticipant’sperceivedappearanceandoralfunctionwillbeevaluatedusingtheshort-formDerrifordappearancescale(DAS24)(Carretal.,2005)whichissuitedasaresearchofappearanceinH&Ncancers(DjanandPenington,2013),andtheLiverpooloralrehabilitationquestionnaire(Pace-Balzanetal.,2006)(AppendixB)respectively.Presurgicalfacialaestheticswillalsobeevaluatedbymeansofassessingfacialsymmetrywithstereophotogrammetry(clinical3Dphotographyinthemedicalillustrationdepartment)oftheheadandneckregion.
4.5.2 Perioperative/inpatient data collection Duringtheinpatientphaseoftheparticipant’smedicaltreatment,alldatawillberecordedonthe“inpatientcasereportform”(CRF02).Toevaluatethepresurgicaldentalocclusion(ifoccludingteethpresent),abiteregistrationwillbetakenwhilstthepatientparticipantisanaesthetised.Thesewillbeobtainedusingaviscoelasticsiliconeimpressionmaterial.Atsurgery,overalltimefromknifetoskin,totransferringthepatientparticipantofftheoperatingtablewillberecorded.Furthermorethetimingsofspecificlandmarksofreconstructivecomponentsofsurgerywillberecorded:
• Timesatwhichmandibularosteotomiesarefirststarted(whenmandibularcuttingguidesfirsttouchesmandible)andcompleted(whenmandibularcuttingguidesremoved)

JaWPrinTProtocolv1.8_22.12.2017 14
• Timeofknife-to-skinforflapharvest• Timeofflapdetachment• Timeofcompletingfixationoftheplateinitsfinalrestingposition(i.e.
whencompletionoffixationtotheresidualmandible)• Timeofcompletingarterialanastomosis
Toevaluatetheimpactofcuttingguidesonthefitofthebonyflap,thesurgeonwillbeaskedtorecordthenumberofsubsequentadjustmentsneededtothemandibular/fibularosteotomies,drillholesand/ortheplateitself.Tofurtherevaluatetheefficiencyofeithersurgicaltechnique(andanypotential‘learningcurve’effect),thesurgeonandscrubnursewillbeaskedtoprovidea5-pointLikertscaleratingforthefollowingcriteriaattheendoftheoperation:
• Easeofuse• Confidenceinperformingthetechnique• Immediatesatisfactionwithreconstructivecomponentofsurgery
Intheimmediatepostoperative(inpatient)phaseofrecovery,datesofstayintheintensivecareunit(ITU),highdependencyunit(HDU)and/ortheinpatientwardwillberecorded,alongwithafinaldischargedate.Duringthisperiod,anypostoperativecomplicationsaretoberecordedif/astheyoccur.
4.5.3 6 weeks follow up Thiswillincludereportingofanycomplicationssincedischargefromhospital,aswellasrepetitionofsomedatacollectedinthebaselineassessment,usingthe“6weekscasereportform”(CRF03).Specificdatatobecollectedincludes:
• Physicalassessment(BMI,oralhygeinestatus,reportonwoundhealing).• UniversityofWashingtonQoLquestionnaire.• Short-formDerrifordappearancescale(DAS24).• Liverpooloralrehabilitationquestionnaire.• Reportoncomplications.• Stereophotogrammetry(3Dphotography)oftheheadandneck.
4.5.3 6 months follow up The“6monthscasereportform”(CRF04)willbeusedtocollectidenticaldatatothatcollectedat6weeksfollow-up.Thisfollowuppointisselectedasinthecaseofcancersurgery,itisastandardfollow-uppointforassessmentofsignsofearlydiseaserecurrence.Forthisreason,routinemedicalCTscanningtoevaluatefordiseaserecurrenceisperformed.A3DrenderofDICOMdatafromthisclinicalscancanbeusedtodimensionallyandvolumetricallycomparetheactualbonyreconstructionwiththepreoperativeplan,evaluatingoverallaccuracyandprecisionofthereconstructivetechniqueused.Furthermore,CTassessmentofbonyunionwillbeperformedusingaquantitativenumericalratingscore,adaptedfromAkashietal.(Akashietal.,2015)
4.5.4 1 year follow up

JaWPrinTProtocolv1.8_22.12.2017 15
The“1yearcarereportform”(CRF05)willbeusedtocollectidenticaldatatothatcollectedat6weeksfollow-up.Furthermore,insomecasesroutineclinicalandradiographic(conebeamCT)dentalassessmentisperformed1yearpostoperativelywithaviewtofurtherdentalrehabilitation(withdentalimplantsinsomepatients).Fromthisdentalassessment,wewouldaimtoevaluatetheclinician’sopinion(usinga5pointLikertscale)ofthepatientparticipant’soverallsuitabilityfordentalrehabilitation(ifnotalreadyinplace)withavarietyofpossibleprostheticsolutions:
• Simpledentures• Bridge• (Multiple)singletoothimplants• Implantretainedbridge• Implantretaineddentures
Dentalradiology(conebeamCT)ifusedaspartofthisroutinedentalassessmentwillalsobeanalysedtofurtherevaluateanybony(dimensional/volumetric/healing)changesthatoccurovertime.Post-surgicaldentalocclusionwouldclinicallyroutinelybeevaluatedwithabiteregistration.Thiscanbecomparedtothepre-surgicalbiteregistrationtoevaluatetheimpactofthereconstructivesurgeryondentalocclusion.
5.0 Risk management Allclinicaltesting(physical,serologicalandradiological)performedwithinthisstudyiswithintheremitofstandardclinicalcareandthereforethestudyitselfwillnotputtheparticipantatadditionalriskofmedicalcomplicationsorside-effects.Forqualitativedatacollection,validatedscoringtoolswillbeusedwhereverpossible.Bothtreatmentpathways(A&B)observedinthisstudyconstituteroutinesurgicalpractice,withbothtechniquesroutinelyusedatABMUHB.Botharegold-standardtreatmentwithsubtledifferencesintechnique;neitherisexperimentalinanyway.Consequentlyanyclinicalcomplicationscanbedealtwithinthenormalclinicalmanner,regardlessofthestudy.Itwillbemadecleartoparticipantsfromthestartoftheirinvolvementthattheyarefreetowithdrawfromthestudyatanytime,withoutanyreasonandwithoutanyimpactupontheirstandardofcare.Participantswillbegiventhecontactdetailsforthestudyteam,withtheirprimarylinkbeingtheircentre’sPIwhowillsuperviseboththeirclinicalcareanddatacollectionthroughoutthestudyperiod.Shouldclinicalneedrequiredeviationfromthestudyprotocolandsubsequentexclusionastoavoidconfoundingeffectsonstudyresults,thiswillbedisclosedandreportedintheresults.Whereitisfeltthatanydatacollectedwasunaffectedbythisprocess,itwillbeusedwhereverfeasible.

JaWPrinTProtocolv1.8_22.12.2017 16
6.0 Statistical analysis Datawillbecollatedandanalyzedusingastatisticalsoftwarepackage.Descriptivestatisticswillbeusedforbaselinemeasures,categoricalstatisticsforquestionnaireoutcomedata,andrelationshipswillbeevaluatedusingtestsofcorrelationandcomparison,alongwithregressionalanalysis.
7.0 Data management and quality control DatawillbecollatedandstoredincompliancewiththeDataProtectionAct1998andtheABMUHBdataprotectionpolicy.Alldatausedbeyondtheparticipant’simmediateclinicalenvironmentwillbeanonymizedaccordingly.Thestudyteamwillmeetthroughoutthestudywithquarterlymeetingstodiscussandauditparticipantrecruitment,datacollectionandanyissueswiththestudyprotocolthatmayarise.AllclinicalrecordswillremainwithinABMUHBandstoredwithinthepatient’sclinicalrecordsinthenormalmanner.CaseReportForms(CRFs)willbekeptinthePI’sofficeinalockedcabinet.Tomaintainanonymityfromtheearlieststage,recruitedparticipantswillbeassignedanumericidentitycode(insteadofidentifiableinformationsuchasageordateofbirth)fromthebeginning.Onceanonymised,patientdatawillbestoredelectronicallyonapassword-protectedlaptopcomputerandbacked-uponanexternalharddriveonadailybasis.Asanonymisedrawdata,CRFswillbephysicallystoredfor15yearsbeyondtheterminationofthestudybythePI(asthedatacustodian).ThisstrategyisbasedupontherecommendationsoftheABMUHBresearchanddevelopmentdepartment(wherelocalpolicyadvisesadatastorageperiodof5to15yearsfollowingterminationofthestudy)andtheUKPolicyFrameworkforhealthandsocialcareresearch(Health_Research_Authority,2017).Identifiabledatathatrequiresstorageforclinicalreasonsalone,willonlybestoredintheusualNHSclinicalmanneraccordingtoNHSWalespolicy(The_National_Assembly_For_Wales,2000).
8.0 Ethical considerations Alltreatmentsprovidedtostudyparticipantsarenormal,routineclinicalpracticeatABMUHB.ApartfromHRQOLquestionnairesandgaininginformedwrittenconsentfortheresearchstudy,allinvestigations/testsinthisstudyareroutineclinicalpracticeatABMUHBforpatientsundergoingjawreconstructionsurgery.Withregardstosomespecifictests:

JaWPrinTProtocolv1.8_22.12.2017 17
• Clinical3Dphotography(stereophotogrammetry)isroutinelyavailableandcommonlyusedforABMUHBpatientsundergoingfacialreconstructivesurgery,althoughnotroutinelyinallcases.Inthisstudy,stereophotogrammetry(3Dphotos)willbeobtainedatbaseline(preoperatively),aswellas6weeks,6monthsand1yearpostoperatively.ThishasbeendiscussedwiththeMedicalIllustrationdepartmentatMorristonHospital.
• Dentalbiteregistrationsareroutinelyperformedafterjawreconstructionsurgeryinordertoplanthepatientforrehabilitationwithdentalprostheses.Insome,dentalimpressionsandbiteregistrationsareobtainedpriortothesurgeryaswellbutnotinallcases.Inthisstudy,weplantoobtaindentalimpressions(immediatelybeforesurgerywhilstundergeneralanaesthesia)aswellasseveralmonthslater(asperroutinepractice).Thestudyteamfeltthatcollectingthepreoperativedentalimpressionsatthebeginningoftheparticipant’ssurgeryprovidesanopportunistic,efficient,safeandcontrolledsettinginwhichtodothis.
Theaboveitemsareexplainedfully(inlayterms)inthepatientinformationsheet.
9.0 Funding ThisstudyisfundedexternallythroughKESS,inpartnershipwithRenishawplcandtheUniversityofSouthWalesandincludesthecostofconsumables/equipmentandotherincidentalcostsrelatingtothestudyitself.Knowledge Economy Skills Scholarships (KESS) is a pan-Wales higher level skillsinitiative ledbyBangorUniversityonbehalf of theHE sector inWales. It ispartfunded by the Welsh Government’s European Social Fund (ESF) convergenceprogrammeforWestWalesandtheValleys.
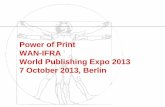
10.0 Study timeline ThestudytimelineisillustratedinthefollowingGanttchart(figure2).

JaWPrinTProtocolv1.8_22.12.2017 18
11.0 References AKASHI,M.,HASHIKAWA,K.,KAKEI,Y.,SAKAKIBARA,A.,HASEGAWA,T.,
MINAMIKAWA,T.&KOMORI,T.2015.Sequentialevaluationforboneunionoftransferredfibulaflapsinreconstructedmandibles:panoramicX-rayversuscomputedtomography.IntJOralMaxillofacSurg,44,942-947.
ALLUM,S.2008.Immediatelyloadedfull-archprovisionalimplantrestorationsusingCAD/CAMandguidedplacement:maxillaryandmandibularcasereports..BrDentJ.,204,377-381.
BROWN,J.,BARRY,C.,HO,M.&SHAW,R.2016.Anewclassificationformandibulardefectsafteroncologicalresection.LancetOncol,17,e23-30.
BUTTERWORTH,C.,MCCAUL,L.&BARCLAY,C.2016.Restorativedentistryandoralrehabilitation:United
KingdomNationalMultidisciplinaryGuidelines.JLO,130,41-44.CANCER_RESEARCH_UKOralcancerincidencestatistics.CARR,T.,MOSS,T.&HARRIS,D.2005.TheDAS24:AshortformoftheDerriford
AppearanceScale(DAS59)tomeasureindividualresponsestolivingwithproblemsofappearance.BritishJournalofHealthPsychology,10,285-298.
CHEN,S.,CHEN,H.,HORNG,S.,TAI,H.,HSIEH,J.,YEONG,E.,CHENG,N.,HSIEH,T.,CHIEN,H.&TANG,Y.2014.Reconstructionforosteoradionecrosisofthemandible:superiorityoffreeiliacboneflaptofibulaflapinpostoperativeinfectionandhealing.AnnPlastSurg,73,18-26.
DJAN,R.&PENINGTON,A.2013.Asystematicreviewofquestionnairestomeasuretheimpactofappearanceonqualityoflifeforheadandneckcancerpatients.JPlastReconstrAesthetSurg,66,647-659.
GIL,R.,ROIG,A.,ARRANZOBISPO,C.,MORLA,A.,MARTIPAGES,C.&LLOPISPEREZ,J.2015.Surgicalplanningandmicrovascularreconstructionofthemandiblewithafibularflapusingcomputer-aideddesignandrapidprototypemodelling,andprecontouredtitaniumreconstructionplates:aprostpectivestudy..BrJOralMaxillofacSurg,53,49-53.
Quarter 1st 2nd 3rd 4th(1yr)
5th 6th 7th 8th(2yrs)
9th 10th EndofStudy
Participantsrecruited
- Unblindingof
studyparticipants
- Disseminationofdata
- Peer-reviewed
publication- Presentation
Participantscompletestudy
Landmarkevents
Studyteammeet
Studyteammeet
Studyteammeet
Studyteammeet
StudyteammeetFirstparticipantcompletesstudy
Studyteammeet
Studyteammeet
Studyteammeet
Studyteammeet
StudyteammeetLastparticipantcompletesstudy
Figure2.Ganttchartillustratingthestudytimeline

JaWPrinTProtocolv1.8_22.12.2017 19
HEALTH_RESEARCH_AUTHORITY2017.UKPolicyFrameworkforhealthandsocialcareresearchv3.3.
KOKOSIS,G.,SCHMITZ,R.,POWERS,D.&ERDMANN,D.2016.MandibularReconstructionUsingtheFreeVascularizedFibulaGraft:AnOverviewofDifferentModifications.ArchPlastSurg,43,3-9.
LYONS,A.&BRENNAN,P.2014.Osteoradionecrosisanewclassification.BrJOralMaxillofacSurg,52,e64-e65.
NICR2016.NorthernIrelandCancerRegistry,QueensUniversityBelfast,Incidencebystage2010-2014.
NUTTING,C.2016.Radiotherapyinheadandneckcancermanagement:UnitedKingdomNationalMultidisciplinaryGuidelines.JLO,130,66-67.
PACE-BALZAN,A.,CAWOOD,J.,HOWELL,R.,BUTTERWORTH,C.,LOWE,D.&ROGERS,S.2006.ThefurtherdevelopmentandvalidationoftheLiverpoolOralRehabilitationQuestionnaire:Across-sectionalsurveyofpatientsattendingfororalrehabilitationandgeneraldentalpractice.IntJOralMaxillofacSurg,35,72-78.
PARK,S.,LEE,D.,LEE,J.,KIM,Y.,KIM,L.&NOH,G.2016.Stabilityofthepermanentlybentplatesusedinmandibularreconstructivesurgery.201638thAnnualInternationalConferenceoftheIEEEEngineeringinMedicineandBiologySociety(EMBC).Orlando,FL.
PARTHASARATHY,J.2014.3Dmodeling,cusomimplantsanditsfutureperspectivesincraniofacialsurgery.AnnalsofMaxillofacialSurgery,4,9-18.
ROGERS,S.,GWANNE,S.,LOWE,D.,HUMPRHIS,G.,YUEH,B.&WEYMULLER,E.2002.TheadditionofmoodandanxietydomainstotheUniversityofWashingtonQualityofLifeScale.Head&Neck,24,521-529.
STEINBACHER,D.2015.Three-DimensionalAnalysisandSurgicalPlanninginCraniomaxillofacialSurgery.JOralMaxillofacSurg,73,S40-S56.
SU,Y.2017.Three-DimensionalPrintingofPatient-SpecificTitaniumPlatesinJawSurgery:APilotStudy[Online].https://clinicaltrials.gov/ct2/show/NCT03057223:U.S.NationalInstitutesofHealth.[Accessed2/4/172017].
TARSITANO,A.,BATTAGLIA,S.,CRIMI,S.,CIOCCA,L.,SCOTTI,R.&MARCHETTI,C.2016.Isacomputer-assisteddesignandcomputer-assistedmanufacturingmethodformandibularreconstructioneconomicallyviable?JCraniomaxillofacSurg,44,795-799.
THE_NATIONAL_ASSEMBLY_FOR_WALES2000.Fortherecord-ManagingRecordsinNHSTrustsandHealthAuthorities.WelshHealthCircular.
WANG,Y.,ZHANG,S.,FAN,S.,ZHANG,D.,HUANG,Z.,CHEN,W.,YE,J.&LI,J.2016.Mandibularreconstructionwiththevascularisedfibulaflap:comparisonofvirtualplanningsurgeryandconventionalsurgery..intJOralMaxillofacSurg,45,1400-1405.

JaWPrinTProtocolv1.8_22.12.2017 20
12.0 Appendices
Appendix A

JaWPrinTProtocolv1.8_22.12.2017 21

JaWPrinTProtocolv1.8_22.12.2017 22

JaWPrinTProtocolv1.8_22.12.2017 23
Appendix B

JaWPrinTProtocolv1.8_22.12.2017 24

JaWPrinTProtocolv1.8_22.12.2017 25