The Adrenal Glands - Columbia
38
The Adrenal Glands Th J b MD Thomas Jacobs, M.D. Diane Hamele-Bena, M.D.
Transcript of The Adrenal Glands - Columbia

The Adrenal Glands
Th J b M DThomas Jacobs, M.D.Diane Hamele-Bena, M.D.

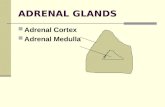
I. Normal adrenal gland: Gross and microscopic features
II. Hypoadrenalism
III. Hyperadrenalism
IV. Adrenal cortical neoplasms
V. Adrenal medulla

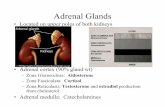
Normal Adrenal Gland
• Normal adult adrenal gland: 3.5 - 4.5 grams

Normal Adrenal Gland
• Normal adult adrenal gland: 3.5 - 4.5 grams

Adrenal Cortex Morphology
• Cortex: 3 zones:– Glomerulosa– Fasciculata– Reticularis

Hypoadrenalismyp

Hypoadrenalism
• Primary Adrenocortical Insufficiency
D t i f il f d l l d–Due to primary failure of adrenal glands
–ACTH is elevated
• Secondary Adrenocortical Insufficiency
–Due to disorder of hypothalamus or pituitaryDue to disorder of hypothalamus or pituitary–ACTH is decreased

HypoadrenalismClinical ManifestationsClinical Manifestations
•Fatigue, weakness, depression
•Anorexia
•Dizziness
•N&V, diarrhea
•Hyponatremia, hyperkalemia
•Hypoglycemia
•HyperpigmentationHyperpigmentation

HypoadrenalismCli i l M if t tiClinical ManifestationsPrimary adrenal insufficiency:y y
Deficiency of glucocorticoids, mineralocorticoids, and androgens
HypoglycemiaF ti
HyponatremiaH k l i
Reduced pubic d illFatigue
AnorexiaWeight loss
HyperkalemiaHypotensionDizziness
and axillaryhair in women
g Dizziness

HypoadrenalismCli i l M if t tiClinical ManifestationsPrimary adrenal insufficiency:y y
Concomitant hypersecretion of ACTH
Hyperpigmentation

HypoadrenalismCli i l M if t tiClinical Manifestations
Secondary adrenal insufficiency:Secondary adrenal insufficiency:Deficiency of ACTH
NO hyperpigmentation

Pathology of Hypoadrenalism
• Primary Adrenocortical Insufficiency– AcuteAcute
•Waterhouse-Friderichsen SyndromeAcute hemorrhagic necrosis, most often due to Meningococci
– Chronic = Addison Disease
• Secondary Adrenocortical Insufficiency• Secondary Adrenocortical Insufficiency

Pathology of Hypoadrenalism
• Primary Adrenocortical Insufficiency– AcuteAcute
•Waterhouse-Friderichsen SyndromeAcute hemorrhagic necrosis, most often due to Meningococci
– Chronic = Addison Disease•Autoimmune adrenalitis•Infections (e g tuberculosis fungi)•Infections (e.g., tuberculosis, fungi)•Metastatic tumors•Other: Amyloidosis, hemochromatosis

Addison DiseaseCli i l fi diClinical findings
Mineralocorticoid deficiency Glucocorticoid deficiencyy•Hypotension•Hyponatremia
•Weakness and fatigue•Weight loss
•Hyperkalemia •Hyponatremia•HypoglycemiaPi t ti
Androgenic deficiencyL f bi d ill
•Pigmentation•Abnormal H2O metabolism•Irritability and mental•Loss of pubic and axillary
hair in women•Irritability and mental sluggishness

Autoimmune AdrenalitisThree settings:
•Autoimmune Polyendocrine Syndrome type 1 (APS1) = Autoimmune Polyendocrinopathy, Candidiasis, and Ectodermal Dysplasia (APECED)
•Autoimmune Polyendocrine Syndrome type 2 (APS2)
•Isolated Autoimmune Addison Disease

Pathologic Changes in Autoimmune Adrenalitis
•Gross:V ll l d (1 1 5 )–Very small glands (1 - 1.5 grams)
–Cortices markedly thinned
•Micro:–Diffuse atrophy of all cortical zones–Lymphoplasmacytic infiltrate–Medulla is unaffected

Pathology of Hypoadrenalism
• Primary Adrenocortical Insufficiency– AcuteAcute
• Waterhouse-Friderichsen Syndrome
– Chronic = Addison Disease• Secondary Adrenocortical Insufficiency
– Any disorder of the hypothalamus or pituitary leading to diminished ACTH; e.g., infection; pituitary tumors, including metastatic carcinoma; irradiation

Hyperadrenalismyp

Hyperadrenalism
Three distinctive clinical syndromes:y
•Excess cortisol: Cushing Syndrome•Excess aldosterone: Conn Syndrome •(Excess androgens: Adrenogenital or Virilizing Syndrome)

Hyperadrenalism
I li i l ti t fIn clinical practice, most cases of Cushing Syndrome are the result of
administration of exogenous glucocorticoidsadministration of exogenous glucocorticoids(“exogenous” or iatrogenic Cushing Syndrome).

Cushing Syndrome
Endogenous
Complete this diagram during the lecture!
Exogenous
during the lecture!
Exogenous (Iatrogenic)

“Endogenous” Cushing SyndromeEtiology Pathology
hiI. ACTH-dependent:
i i d•Cushing Disease Pituitary adenoma
Adrenal cortical hyperplasia
•Ectopic ACTH production Extra-adrenal ACTH-producing tumor
yp p
II ACTH i d d t
Adrenal cortical hyperplasia
•Hypersecretion of cortisol by adrenal neoplasm
II. ACTH-independent:Adrenal neoplasm

Cushing Syndrome
Pituitary adenoma
Ad l i l
Dorsal fat pad
Ecchymoses
Moon face
Adrenal corticalhyperplasia Thin skin Striae
CO
Thin arms & legs
Pendulousabdomen
RTIACTH-producing tumor
Thin arms & legsSOL
Poor woundhealing
Adapted from Netter
Adrenalcarcinoma
Adrenal adenoma
g

Cushing SyndromeHydrocortisone Excess•Abnormal fat distribution
–Moon face •HirsutismAdrenal Androgen Excess
–Central obesity•Increased protein catabolism
–Thin skin
Hirsutism•Deepened voice in women•Acne•Abnormal menses
–Easy bruisability–Striae–Osteoporosis with
b o a e ses
vertebral fractures–Impaired healing–Muscle wasting •Hypokalemia with alkalosis
Mineralocorticoid Excess
–Suppressed response toinfection
•Diabetes
yp•Usually occurs in cases
of ectopic ACTH production
•Psychiatric symptoms

Pathology of Primary Hyperaldosteronism
• Aldosterone-secreting adenoma
Ad l i l i
– Conn Syndrome
• Adrenal cortical carcinoma– Uncommon cause of hyperaldosteronism

Conn SyndromeConn Syndrome
•Hypertension•Hypertension•Polydipsia•PolyuriaAldosterone
Adrenal
•Hypernatremia•Hypokalemia
adenoma
Adapted from Netter

C i l N lCortical Neoplasms
i i *Adenomas and Carcinomas
Functioning *
N f ti iNon-functioning
* May produce:• Cortisol• Sex steroids
(Cushing Syndrome))Sex steroids
• Aldosterone (Conn Syndrome))

Cortical NeoplasmsCortical Neoplasms
• Adenomas • Carcinomas
• Discrete, but often unencapsulated • Usually unencapsulated
– Gross: – Gross:
• Small (up to 2.5 cm)• Most <30 grams• Yellow-orange, usually without
• Large (many >20 cm)• Frequently > 200-300 grams• Yellow, with hemorrhagic,g , y
necrosis or hemorrhage, g ,
cystic, & necrotic areas
– Micro: – Micro:• Lipid-rich & lipid-poor cells with
little size variation• Ranges from mild atypia to
wildly anaplastic

Adrenal Medulla

Adrenal Medulla
• Specialized neural crest (neuroendocrine) cells• Part of the chromaffin system, which includes the
adrenal medullae & paraganglia• Major source of catecholamines (epi, norepi, &
dopamine)

Tumors of the Adrenal MedullaTumors of the Adrenal Medulla
• Neuroblastoma• Ganglioneuroblastoma• Ganglioneuroma
• Pheochromocytoma

N blNeuroblastoma
• Poorly differentiated malignant neoplasm derived from neural crest cellsfrom neural crest cells
• Usually occurs in infants & small children“S ll d bl ll t ” f hildh d• “Small round blue cell tumor” of childhood
Rhabdomyosarcoma LymphomaRetinoblastoma Wilms tumorEwing sarcoma/PNET Medulloblastoma

Neuroblastoma: Pathology• Gross:
– Large tumor with hemorrhage, necrosis, & calcification
• Micro:• Micro:– Undifferentiated small cells resembling lymphocytes
(“Small round blue cell tumor”)( Small, round, blue cell tumor )– May show areas of differentiation (larger cells with
more cytoplasm and Schwannian stroma)more cytoplasm and Schwannian stroma)

Neuroblastoma: Prognostic Factors• Patient age
g
• Stage• Site of 10 involvement• Histologic grade• DNA ploidy• N-myc oncogene amplification• Others: Chromosome 17q gain, Chromosome 1p loss, Trk-A q g p
expression, Telomerase expression, MRP expression, CD44 expression

Ganglioneuroma
• Differentiated neoplasm of neural crest origin• Benign• Occurs in older age groupOccurs in older age group• Pathology:
G E l t d hit fi– Gross: Encapsulated, white, firm– Micro: Ganglion cells & Schwann cells

Ganglioneuroblastomag
• Composed of malignant neuroblastic elements & ganglioneuromatous elements
• Prognosis depends on % of neuroblasts

PheochromocytomaPheochromocytoma
• Catecholamine secreting neoplasm: HYPERTENSION• Rare, but important: surgically curable form of
hypertension
• Catecholamine-secreting neoplasm: HYPERTENSION
hypertension
• May arise in association with familial syndromes, e.g., MEN2 von Hippel Lindau von Recklinghausen (NF1)MEN2, von Hippel-Lindau, von Recklinghausen (NF1)
• May be “sporadic”: ~24% have germline mutations, including mutations of RET VHL SDH B and SDH D genesincluding mutations of RET, VHL, SDH-B, and SDH-D genes
• Extra-adrenal tumors (e.g., carotid body) are called “paragangliomas”paragangliomas

Ph h P h lPheochromocytoma: Pathology
• Gross:– 1 - 4000 grams (average = 100 grams)
A f h h i & ti d ti– Areas of hemorrhage, necrosis, & cystic degeneration
• Micro:– Balls of cells resembling cells of medulla, with bizarre,
hyperchromatic nuclei; richly vascular stroma
• Benign & malignant tumors are histologically identical; the only absolute criterion for malignancy is metastasis.