THE 2017 RUSH NEUROSCIENCE REVIEW€¦ · 2 /// THE 2017 RUSH NEUROSCIENCE REVIEW Chairpersons’...
67
THE 2017 RUSH NEUROSCIENCE REVIEW
Transcript of THE 2017 RUSH NEUROSCIENCE REVIEW€¦ · 2 /// THE 2017 RUSH NEUROSCIENCE REVIEW Chairpersons’...

T H E 2 017 R U S H
NEUROSCIENCE REVIEW

Forward Progress: Neurologists at Rush, including Dusan Stefoski, MD
(right), and Michael Ko, MD, have played a vital role in advancing
treatment for patients with multiple sclerosis. Learn how on page 59.

T H E 2 0 17 R U S H N E U R O S C I E N C E R E V I E WFaculty editors Sepehr Sani, MD Aimee Szewka, MD
CHAIRPERSONS’ LETTER 2
NEUROSCIENCES AT RUSH: AT A GLANCE 4
PRIMARY AND ASSOCIATED FACULTY
Department of Neurological Sciences 6
Department of Neurological Surgery 7
RESIDENTS AND FELLOWS
Department of Neurological Sciences 8
Department of Neurological Surgery 9
ARTICLES
Preimplantation Modeling of Electrode Lead Implant Sites to Predict the Extent of Cortical Activation 10 During Direct Neurostimulation Therapy Leopoldo Cendejas-Zaragoza; Richard W. Byrne, MD; Marvin A. Rossi, MD, PhD
Improvement of Brain Function by a Lipid-Lowering Factor 18Kalipada Pahan, PhD
Predictors of False-Positive Stroke Thrombectomy Transfers 23Julia Yi, MD; Danielle Zielinski, RN, MSN, AG-ACNP; Bichun Ouyang, PhD; James Conners, MD, MS; Rima Dafer, MD, MPH, FAHA; Michael Chen, MD
Dramatic Reductions in Spine Surgery Infection Rates 29Harel Deutsch, MD
Moving Pictures and Moving Targets in the Care of Patients With Movement Disorders 33Jennifer G. Goldman, MD, MS; Brandon R. Barton, MD, MS; Gian D. Pal, MD, MS
PUBLICATIONS 39
RESEARCH GRANTS 53
VOLUME AND QUALITY DATA
Volumes, neurology and neurological surgery 57
Mortality, neurology and neurological surgery 58
Quality indicators, stroke 58
INTERVIEW: Game-Changers 59Multiple sclerosis specialists Dusan Stefoski, MD, and Michael Ko, MD, discuss Stefoski’s and Rush’s roles in bringing novel therapies to the market to advance care for patients with multiple sclerosis.
2 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Chairpersons’ Letter
Both of us were early in our careers when President George H. W. Bush proclaimed the 1990s the “Decade of the Brain.” In the years between 1990 and 1999, neuroscience research flourished in the US and abroad. The decade also forced a confrontation with an uncomfortable fact: With the steady aging of the nation’s population, the high cost of caring for neurological diseases would only get higher. By the end of the 1990s, the cost to treat neurological diseases in the US was approximately $400 billion a year; by 2014, according to a recent study published in the Annals of Neurology, the country was spending close to $800 billion annually.
Today, the challenge for the neuroscience program at Rush—as for programs throughout the country—is twofold. We must continually innovate to offer high-quality care as efficiently as possible while enhancing the vital relationship between patient and physician. We must also strive to foster a rich intellectual and clinical environment to engage our faculty and nurture the next generation of physicians and researchers.
The following selected highlights from 2016 and early 2017 demonstrate how we’re facing these challenges.
Mobile stroke unit: In October 2016, Rush unveiled its mobile stroke treatment unit—a specially built, state-of-the-art ambulance outfitted with telemedicine technology and a CT scanner to enable brain imaging that is critical to accurate stroke diagnoses and treatment. The unit, one of only a handful of its kind in the US, will serve Chicago’s western suburbs from a base at Rush Oak Park Hospital.
Regenerative research institute: Rush has raised $2 million to fund a regenerative research institute at Rush that will be led by neurosurgeon Richard G. Fessler, MD, PhD, who
has vast experience in research on using stem cells to treat patients with spinal cord injuries. With Fessler’s expertise in the treatment of spinal cord injury as a springboard, the institute will ultimately encompass all areas of regenerative research at Rush, including neurological conditions, cartilage repair, heart disease, and macular degeneration.
Neurology elective in Zambia: Starting in the 2017-2018 academic year, 2 3rd-year residents received a stipend to travel to Zambia’s capital city for a 1-month elective at the University Teaching Hospital in Lusaka. The elective provides a vital service for Zambia, which faces a significant deficit of neurologists—there are only 4 neurologists in the country the size of Texas. And it provides a vital global outlook for Rush residents, who have the opportunity to practice medicine in another country with a significantly different population in a hospital with limited resources.
New neuroimmunology fellowship: Rush has established a 2-year neuroimmunology fellowship that combines training in clinical care and research in the fields of multiple sclerosis and related demyelinated and auto-immune diseases, neurological complications of HIV, and infectious diseases of the nervous system.
Delivering high-quality care in Chicago—and beyond: Over the next 2 years, the Department of Neurological Sciences will be expanding services at Rush offices in the South Loop, River North, Oak Park, and Oakbrook, and at Rush Copley Medical Center in Aurora.
Research highlights
With a growing number of clinical trials in both neurosurgery and neurology, faculty at Rush continue to make substantial contributions to the understanding of neurological disease. Here are just a few examples:
• Hope for patients with spinal cord injuries. Four of 6 people with paralyzing spinal cord injuries who were treated with a new cell therapy have recovered a significant level of movement on at least one side, new study results show. This 67 percent recovery rate is more than double the rates of recovery seen in both matched historical controls and published data in a similar population. Each of the 6 participants in the study had lost all motor function below the location of the spinal injury. They each received a surgical injection of 10 million oligodendrocyte progenitor cells, or AST-OPC1, which potentially can make poorly working nerves function better. Asterias Biotherapeutics, the California-based biotechnology company that manufactures the cell therapy, reported the 12-month results of the study
Igor Koralnik, MD (left), and Richard Byrne, MD.

Chairpersons’ Letter /// 3
in October 2017. Neurosurgeon Richard G. Fessler, MD, PhD, is the principal investigator of the study at Rush, one of 9 clinical sites in the US.
• Disease-modifying therapy for multiple sclerosis. Ocrevus (ocrelizumab), the first and only disease-modifying therapy for both primary progressive and relapsing forms of multiple sclerosis (MS) was approved by the US Food and Drug Administration in late March. Learn how Rush helped pioneer the use of Ocrevus in the interview feature on page 54.
• Clot removal can be effective, even after 6 or more hours. Mechanical thrombectomy, a treatment to remove a stroke-causing blood clot in the brain, is effective in some patients even when performed within 6 to 24 hours after a stroke, according to the results of an international, randomized controlled research study. Neurointerventionalist Michael Chen, MD, the principal investigator of the study at Rush, presented the findings in May 2017 at the European Stroke Organization Conference in Prague. Rush is the only Illinois site, one of 7 sites in the US, and one of only 22 sites in the world to participate in the international study, called the DAWN trial.
Faculty awards and recognition
Each year, many of our faculty members are recognized for their achievements locally, nationally, and internationally. The following are just a few examples:
Department of Neurological Surgery
• Richard W. Byrne, MD, served as co-president at the second annual Chinese and American Neurosurgery Meeting in Harbin, China, and was named president-elect of the Neurosurgical Society of America.
• Among his many honors, Richard G. Fessler, MD, PhD, was listed in the 9th edition of 2000 Outstanding Intellectuals of the 21st Century and was named chairman and president-elect of the International Society for Minimal Intervention in Spinal Surgery.
Department of Neurological Sciences
• Thomas Pritchett Bleck, MD, will be honored with the Lifetime Achievement Award for 2018 from the Society of Critical Care Medicine.
• Kalipada Pahan, PhD, earned the Zenith Fellows Award from the Alzheimer’s Association for researchers who have made a substantial personal commitment to the advancement of Alzheimer’s disease research.
• Christopher Goetz, MD, was elected president of the International Parkinson and Movement Disorder Society
and became a member of the Académie Nationale de Médecine (French National Medical Academy).
• Jeffrey Kordower, PhD, was named vice chairman of the board of directors of the National Association for Biomedical Research.
• Cynthia Comella, MD, was named president-elect of the International Neurotoxin Association and chair-elect of the International Parkinson and Movement Disorders Society, Pan American Section.
• Deborah Hall, MD, received recognition in 2017 for having one of the top 10% of posters at the American Academy of Neurology and an exceptional poster at the Movement Disorder Society International Meeting in Vancouver for her poster titled “Fragile X Gray Zone Alleles Are Associated With Higher Global Motor Function in an Elderly Community Population.”
• Brandon Barton, MD, published a textbook, Non-Parkinsonian Movement Disorders, with Hall.
• Igor Koralnik, MD, was named chair of the international outreach committee of the American Neurological Association.
• The Huntington’s Disease program at Rush, led by Jennifer G. Goldman, MD, MS, was named a Center of Excellence by the Huntington’s Disease Society of America.
• Matthew Meriggioli, MD, was awarded a Muscular Dystrophy Association (MDA) grant, and Rush was designated as an official MDA Care Center.
• James Conners, MD, MS, and the stroke team have been honored with the 2017 Excellence in Telehealth Achievement Award for Improved Care for Underserved Populations.
• Sayona John, MD, was recognized as a Lifesaving Partner by Gift of Hope Organ & Tissue Donor Network for going above and beyond to make donations possible.
• Aimee Szewka, MD, was awarded for outstanding achievement in receiving an A.B. Baker Teacher Recognition Award from the American Academy of Neurology.
We hope you will explore the rest of this publication to learn about our faculty’s many contributions to research and clinical care in the neurosciences.
Richard Byrne, MDChairperson, Department of Neurological SurgeryThe Roger C. Bone, MD, Presidential Chair
Igor Koralnik, MDChairperson, Department of Neurological SciencesThe Jean Schweppe Armour Professor of Neurology

4 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Neurosciences at Rush: At a Glance
32 28 67 54 10 General Neuro Psychiatric Rehabilitation Epilepsy neurology ICU (adult)
Beds
Inpatient Facilities
For additional volume and quality data, see pages 52-53.
Department of Neurological Sciences•Rush Alzheimer’s Disease Center
•Section of Cerebrovascular Disease
•Section of Clinical Neurophysiology and Epilepsy
•Section of Cognitive Neurosciences
•Section of Critical Care Neurology
•Section of General Neurology
•Section of Movement Disorders
•Rush Multiple Sclerosis Center
•Section of Pediatric Neurology
•Section of Neuromuscular Diseases
•Section of Neuro-oncology
•Section of Neuro-ophthalmology
Department of Neurological Surgery•Neuroendovascular Surgery Center
•Skull Base and Pituitary Surgery Center
•Spine and Back Care
Attending physicians
112Residents and fellows
58Advanced practice nursesand physician assistants
33
Neurology outpatient visits29 635
Neurology inpatient discharges2454
Neurological surgery outpatient visits (brain)3958
Neurological surgery outpatient visits (spine)5659
NIA-designated Alzheimer’s Research Center: The Rush Alzheimer’s Disease Center is a designated Alzheimer’s disease research center, funded by the National Institute on Aging of the US National Institutes of Health.
No. 4 in the Nation: In 2017, Rush University Medical Center received Vizient’s (formerly University HealthSystem Consortium’s) Quality Leadership Award, ranking No. 4 among 107 academic medical centers nationwide. It is the 5th consecutive time Rush has been ranked in Vizient’s top 5, and the 9th since 2005.
Comprehensive Stroke Center: Rush’s stroke program received the Get With the Guidelines Gold Plus Award from the American Heart Association and earned a place on the American Stroke Association’s Target: Stroke Elite Plus Honor Roll.
MDA Care Center: In January 2017, the Muscular Dystrophy Association (MDA) named Rush University Medical Center an MDA Care Center, elevating Rush to an elite group of just over 150 providers who have this designation.
Nursing Excellence: Rush University Medical Center has earned Magnet status—the highest recognition for nursing excellence—4 consecutive times from the American Nurses Credentialing Center.
Parkinson’s Foundation Center of Excellence: The Parkinson’s Foundation added Rush University Medical Center to the global network of institutions the foundation has designated as Centers of Excellence. The designation builds upon Rush’s longstanding history and recognition as a Parkinson’s Foundation Research Center.
Neurosciences at Rush: At a Glance /// 5

6 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Faculty (2016)Department of Neurological SciencesChairperson: Igor Koralnik, MD
Aging and neurodegenerative diseasesNeelum Aggarwal, MD
Zoe Arvanitakis, MD, MS
Lisa Barnes, PhD
David Bennett, MD
Katherine Blizinsky, PhD
Aron Buchman, MD
Ana Capuano, PhD
Debra Fleischman, PhD
Chris Gaiteri, PhD
Duke Han, PhD
Namhee Kim, PhD
Sue Leurgans, PhD
Julie A. Schneider, MD
Robert Wilson, PhD
Lei Yu, PhD
Cerebrovascular diseaseLaurel Cherian, MD, MS
James Conners, MD, MS
Rima Dafer, MD, MPH, FAHA
Michael Kelly, MD*
Neha Kramer, MD
Nick Osteraas, MD
Sarah Song, MD, MPH
Alejandro Vargas, MD, MS
Clinical neurophysiology and epilepsyAntoaneta Balabanov, MD
Adriana Bermeo-Ovalle, MD
Lawrence Bernstein, MD
Amar Bhatt, MD
Thomas Bleck, MD
Elia DeSavino, MD*
Thomas Hoeppner, PhD
Maggie McNulty, MD
Rebecca O’Dwyer, MD
Esmeralda Park, MD*
Serge Pierre-Louis, MD*
Lubov Romantseva, MD
Marvin Rossi, MD, PhD
Michael Smith, MD
Travis Stoub, PhD
Critical care neurologyThomas Bleck, MD
Torrey Boland, MD
Michael Chen, MD
Ivan DaSilva, MD
Rajeev Garg, MD, MS
Sayona John, MD
Lauren Koffman, DO
George Lopez, MD, PhD
Sebastian Pollandt, MD
Starane Shepherd, MD
Cognitive neurosciencesChristopher Grote, PhD
Duke Han, PhD
Richard Peach, PhD
Robert Wilson, PhD
General neurologyAmar Bhatt, MD
Richard Brannegan, MD*
Jon Cheponis, MD
James Dorman, MD*
Andrew Dorsch, MD
Katey Ess, MD
Jacob Fox, MD
Laura Goldstein, MD
Christopher Muth, MD
Ligia Rioja, MD
Sava Saeed, MD*
Megan Shanks, MD
Lafayette Singleton, MD*
Milena Stosic, MD
Aimee Szewka, MD
Jordan Topel, MD
Jessica Wilson, MD
Robert Wright, MD
Multiple sclerosisMichael Ko, MD
Danielle Rice, MD*
Fabian Sierra-Morales, MD
Dusan Stefoski, MD

Faculty (2016) /// 7
NeurobiologyYaping Chu, PhD
Malabendu Jana, PhD
Jeffrey Kordower, PhD
Susanta Mondal, PhD
Dan Nicholson, PhD
Kalipada Pahan, PhD
Avik Roy, PhD
Neuroinfectious diseasesIgor Koralnik, MD
Fabian Sierra-Morales, MD
Lakshmi Warrior, MD*
Neuromuscular diseasesReena Ghode, MD*
Rabia Malik, MD
Matthew Meriggioli, MD
Irwin Siegel, MD
Madhu Soni, MD
Neuro-oncologyJoo Yeon Nam, MD
Clement Pillainayagam, MD
Neuro-ophthamologyThomas Mizen, MD
Milena Stosic, MD
Aimee Szewka, MD
Parkinson’s disease and movement disordersSharlet Anderson, PhD
Meagan Bailey, MD
Brandon Barton, MD, MS
Bryan Bernard, PhD
Cynthia Comella, MD
Melany Danehy, MD
Jori Fleisher, MD
Christopher Goetz, MD
Jennifer Goldman, MD, MS
Deborah A. Hall, MD, PhD
Aikaterini Kompoliti, MD
Bichun Ouyang, PhD
Gian Pal, MD, MS
Glenn Stebbins, PhD
Leonard Verhagen Metman, MD, PhD
Pediatric neurologyElizabeth Berry-Kravis, MD
Peter Heydemann, MD
Meryl Lipton, MD
Lubov Romantseva, MD
Department of Neurological SurgeryChairperson: Richard Byrne, MD
Richard Byrne, MD
Michael Chen, MD
R. Webster Crowley, MD
Harel Deutsch, MD
Richard Fessler, MD, PhD
Ricardo Fontes, MD, PhD
Demetrius Lopes, MD
Lorenzo Munoz, MD
John O’Toole, MD, MS
Sepehr Sani, MD
Vincent Traynelis, MD
Research facultyRoberta Glick, MD
Richard Penn, MD
Associated faculty at Rush University Medical CenterPete Batra, MD – Otorhinolaryngology
Aidnag Diaz, MD, MPH – Radiation oncology
Sheila Dugan, MD – Physical medicine and rehabilitation
David Rothenberg, MD – Anesthesiology
Mary Sturaitis, MD – Anesthesiology
R. Mark Wiet, MD – Neurotology
Associated clinical faculty, neurosurgery*Jerry Bauer, MD
Tibor Boco, MD
George Bovis, MD
Martin Herman, MD, PhD
Juan Jimenez, MD
Martin Luken, MD
Patricia Raskin, MD
Szymon Rosenblatt, MD
John Ruge, MD
Andrew Zelby, MD
*Primary appointment is not at Rush University Medical Center
8 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Residents and Fellows (2016)
Department of Neurological Sciences
Residents
Zeeshan Ali, MDMedical school: Indiana University School of Medicine
Bahar Beaver, MDMedical school: University of Oklahoma College of Medicine
Hannah Breit, MDMedical school: Loyola University Chicago Stritch School of
Medicine
Dana Cooper, MDMedical school: Loyola University Chicago Stritch School of
Medicine
Catherine Daley, MDMedical school: University of Toledo College of Medicine and Life
Sciences, Ohio
Gregory Fenton, MDMedical school: Boston University School of Medicine
Rachel Forman, MDMedical school: Chicago Medical School
Edie Graham, MDMedical school: Loyola University Chicago Stritch School of
Medicine
Christopher Green, MDMedical school: Rush Medical College
Emily Grodinsky, MDMedical school: Weill Cornell Medicine, New York
Ryan Hanson, MDMedical school: Rush Medical College
Emily Hill, MDMedical school: Rush Medical College
Teresa Lee, MDMedical school: Georgetown University School of Medicine,
Washington, DC
Stephanie Lyden, MDMedical school: University of Washington School of Medicine,
Seattle
Fiona Lynch, MDMedical school: Rush Medical College
Jacob Manske, MDMedical school: Rush Medical College
Kristin Miller, MDMedical school: George Washington University School of
Medicine and Health Sciences, Washington, DC
Jeremy Pruzin, MDMedical school: Chicago Medical School
Jeffrey Quinn, MDMedical school: Loyola University Chicago Stritch School of Medicine
Daniel Schachter, MDMedical school: New York Medical College
Kathy Slota, MDMedical school: Chicago Medical School
Tammy Smith, MD, PhDMedical school: University of Utah School of Medicine
Maggie Stepien, MDMedical school: Rush Medical College
Jake Torrison, MDMedical school: University of North Dakota School of Medicine
and Health Sciences
Fellows
Fawaz Ahmad, MDMedical school: University of Arkansas College of MedicineResidency: Greater Baltimore Medical Center
Hunan Chaudhry, MDMedical school: Rush Medical CollegeResidency: Rush University Medical Center
Yoon Jae Choi, MDMedical school: Huron Hospital (The Cleveland Clinic)Residency: University of Chicago Medical CenterFellowship (neuro-oncology): University of California, Los Angeles
Christine Chuck, MDMedical school: Indiana University School of MedicineResidency: Rush University Medical Center
Julia Dorneanu, DO, MSMedical school: Chicago College of Osteopathic Medicine,
Midwestern University, Downers Grove, Ill.Residency: University of Illinois at Chicago
Avram Fraint, MDMedical school: Rush Medical CollegeResidency: Rush University Medical Center
Anjali Gera, MDMedical school: University of Illinois at ChicagoResidency: University of Illinois at Chicago
Ajit Indavarapu, MDMedical school: Osmania Medical College, Hyderabad, IndiaResidency: University of Wisconsin - Madison

Residents and Fellows (2016) /// 9
Asma Moussaoui, MDMedical school: V.N. Karazin Kharkiv National University, UkraineResidency: University of Minnesota Medical Center
Benjamin Savage, DOMedical school: Chicago College of Osteopathic Medicine,
Midwestern University, Downers Grove, Ill.Residency: Rush University Medical Center
Arpan Shrivastava, MDMedical school: American University of Antigua, Coolidge, AntiguaResidency: University of Kentucky Medical Center
Ruby Upadhyay, MDMedical school: Rush Medical CollegeResidency: Rush University Medical Center
Rasha Waheed, MDMedical school: Baghdad College of Medicine, IraqResidency: Baghdad Teaching Hospital, IraqFellowship (epilepsy): Detroit Medical Center, Michigan
Natalie Witek, MDMedical school: Boston University School of MedicineResidency: University of California, San Francisco
Amer Zewin, MDMedical school: Damascus University Faculty of Medicine, SyriaResidency: National Hospital, Hamah, Syria
Department of Neurological Surgery
Residents Owoicho Adogwa, MDMedical school: Vanderbilt University School of Medicine,
Nashville, Tenn.
Shahjehan Ahmad, MD Medical school: University of Arizona College of Medicine
Sumeet Ahuja, MDMedical school: Indiana University School of Medicine
Andre Beer Furlan, MD Medical school: University of Sao Paulo Faculty of Medicine, Brazil
Bledi Brahimaj, MDMedical school: University of Cincinnati College of Medicine
Daniel Eddelman, MD, PhD, MBAMedical school: Harvard Medical School
R. David Fessler, MD, PhDMedical school: University of Cincinnati College of Medicine
Mena Kerolus, MDMedical school: University of Missouri - Kansas City School of
Medicine
Ryan Khanna, MDMedical school: Northwestern University Feinberg School of
Medicine, Chicago
Ryan Kochanski, MD Medical school: Wayne State University School of Medicine, Detroit
Joseph Edward Molenda, MDMedical school: Johns Hopkins University School of Medicine,
Baltimore
Stephan Munich, MD Medical school: University at Buffalo Jacobs School of Medicine
and Biomedical Sciences, New York
Ravi Nunna, MDMedical school: University of Cincinnati College of Medicine
Joshua Wewel, MDMedical school: University of Nebraska College of Medicine
Andrew Wong, MD Medical school: University at Buffalo Jacobs School of Medicine
and Biomedical Sciences, New York
Josha Woodward, MDMedical school: Oregon Health and Science University School of
Medicine
Fellows
Krishna Joshi, MD, MBBS, MS, MChMedical school: Govind Ballabh Pant Institute of Postgraduate
Medical Education and Research, Maulana Azad Medical College, New Delhi, India
Residency: Govind Ballabh Pant Hospital, New Delhi
Hani Malone, MDMedical school: Columbia University College of Physicians and
Surgeons, New York Residency: Columbia University Medical Center, New York
Mazda Turel, MDMedical school: Grant Medical College, Mumbai, IndiaResidency: Christian Medical College (CMC), Vellore, India

10 /// THE 2017 RUSH NEUROSCIENCE REVIEW
PREIMPLANTATION MODELING OF ELECTRODE LEAD IMPLANT SITES TO PREDICT THE EXTENT OF CORTICAL ACTIVATION DURING DIRECT NEUROSTIMULATION THERAPY
Leopoldo Cendejas-Zaragoza // Richard W. Byrne, MD // Marvin A. Rossi, MD, PhD
Author Affiliations: Department of Neurological Sciences (Mr Cendejas-Zaragoza and Dr Rossi) and Department of Neurological Surgery (Dr Byrne), Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Marvin A. Rossi, MD, PhD, Rush University Medical Center, Department of Neurological Sciences, 1725 W Harrison St, Suite 885, Chicago, IL 60612 ([email protected]).
Introduction
The RNS System (Responsive Neurostimulation System; NeuroPace) is a neuromodulation technology that was approved in 2013 by the US Food and Drug Administration as an adjunctive therapy for patients with refractory focal-onset epilepsy. This technology is based on delivering direct brain stimulation therapy using a closed-loop on-demand approach to revert a pathological epileptic network to a nonpathophysiological state.
The efficacy of the RNS System has been evaluated and followed in multicenter clinical trials.1-3
Neuromodulation therapy has been shown to demonstrate both acute and chronic efficacy. Proposed mechanisms explaining the acute efficacy of local or direct brain stimulation include conduction blockade,4 synaptic inhibition,5 synaptic depression,6 and overriding of pathophysiological neural network activity.7-10 In addition, chronic exposure to direct neurostimulation has been associated with distant cortical synaptic proliferation.11
Several elements must be considered in the clinical response to stimulation delivered directly to neuronal populations. These variables include stimulation parameter settings,12 the number and interdependence of anatomical targets, electrode number,
B CA
Figure 1. A, A lumped model for an axon oriented in the x direction is presented at the level of a node of Ranvier during bipolar stimulation. Each compartment (red box) is considered to be composed by a membrane capacitance (cM), connected in parallel with the membrane resistance (rM). Compartments are connected to others through resistors in the extracellular space (rE) and intracellular space (ri). The transmembrane voltage (VM) is defined as the potential difference between the extracellular and intracellular fluid (VM = Vi – VE). In the figure, Δx is the length of the compartment. Note that the extracellular potential (VE) is modified by the electric stimulation produced by the electrode (see the isopotential lines produced during a bipolar stimulation of 4.3 mA). Also note how VE changes with the distance. B, The structural MRI was used to create a 3D computational model for the patient. C, Segmentation of the patient’s MRI data set was performed manually by using colored masks (blue, cerebrospinal fluid; gray, gray matter; white, white matter).

Preimplantation Modeling of Electrode Lead Implant Sites /// 11
electrode location and orientation, geometry or shape of the electrode contacts, distribution of the cathode and anode,13,14 and the biophysical properties of the stimulated medium.15
A critical step toward effectively applying direct brain stimulation therapy in patients with focal-onset epilepsy is to effectively interface with epileptogenic neural circuits.15 Therefore, the objective of this study was to predict preoperatively the extent to which direct stimulation therapy, using a limited set of active electrode contacts, can propagate through white matter to influence the maximal extent of an epileptic circuit. A patient-specific preimplant model was generated to calculate the volume of cortical activation (VOCA) in a patient who was a candidate for treatment with the RNS System. This model comprises an iterative, computationally intensive process that calculates regions of hyperpolarization and depolarization in axon bundles immediately surrounding the active electrode contacts, at the gray–white matter interface, using a so-called activation function.
Our center has successfully implanted RNS System depth leads in juxtacortical epileptogenic mesial temporal white matter since 2004. Our goal has been to influence contralateral homotopic mesial temporal regions with a limited set of active electrode contacts. We employed parahippocampal white matter as robust afferent and efferent hippocampal pathways for strategic propagation of direct stimulation therapy.16 Our goal in the present study was to maximize the extent to which preimplant modeling of four cylindrical depth electrode contacts placed in extratemporal basal frontal white matter can enable modulation of distant epileptic tissue in a complex epileptogenic network. Achieving such distant activation can be improved with patient-specific lead placement planning. For this purpose, our model has been incorporated into a preimplant workflow at our institution using novel neuroimaging techniques.15 Postimplant validation of the preimplant
modeling predicting the extent to which distant targeted brain regions would be influenced was performed using subtracted activated SPECT (single-photon emission computed tomography), referred to herein as SAS.15,17
Methods
The preimplantation workflow that was established to predict the extent to which direct stimulation therapy can be strategically guided through white matter was based on an iterative computational model that involved the following 6 steps: (1) description of an activation function derived from the cable equation of axons; (2) calculation of the extracellular electric potential, VE, through the construction of a patient-specific finite element method (FEM) model; (3) identification of axon bundle directionality by means of diffusion tensor imaging (DTI); (4) computation of the activation function using the values of VE and axon directionality, to differentiate among the regions of depolarization and hyperpolarization; (5) generation of regions of interest (ROIs) that were constructed according to the numerical values of the activation function; and (6) identification of influenced tracts by exporting the ROIs as seeds into a tractography algorithm. The model was validated after implantation using SAS. This technique captured transient blood flow changes during delivery of neurostimulation therapy using a relatively high therapeutic charge density delivered through adjacent electrode contacts without generating an afterdischarge.
Patient
The patient was a 19-year-old left-handed woman who experienced a left temporal hemorrhage in utero, secondary to maternal blood incompatibility. Infantile spasms were noted when the patient was 6 months of age, with subsequent frequent
B CA
Figure 2. A, The CAD electrode model consisted of 4 conductive cylinders (1.27 mm diameter × 2 mm height) separated by insulators (10 mm between cylinder midpoints). The numbers in the figure indicate the depth electrode conductors from anterior to posterior. B and C, The +CAD module in Simpleware was used to place the electrodes in white matter.

12 /// THE 2017 RUSH NEUROSCIENCE REVIEW
nocturnal seizures since that time. A left posterior temporal ventriculoperitoneal shunt was placed at the age of 10 months. Seizure semiology included quickly sitting up in bed with right head deviation followed by loud vocalization. Triggers included menstruation and stress. During wakefulness, she reported an aura of sensations that she described as the feeling of “spiders” in her stomach.
Activation Function Definition
The activation function was derived by analyzing a lumped element model of an axon compartment, which is placed within a Cartesian coordinate system in a specific direction, at the level of a node of Ranvier (Figure 1A). A nonhomogenous partial differential equation was derived by applying the Kirchhoff current law. This partial differential equation, known as the cable equation, is as follows:
λ2 – τ – VM = – λ2 ,
where λis the length constant and τis the time constant for the membrane. The solution of this equation describes the transmembrane voltage (VM) as a function of time and geometry. The activation function (the right-hand side of the equation) is proportional to the 2nd derivative of the extracellular voltage (VE) with respect to the x→direction; thus the activation function is proportional to .
In the model depicted in Figure 1A, the axon is oriented in the x direction. However, axons can be oriented in any spatial direction in a 3-dimensional (3D) space. Therefore, the activation function should be computed with respect to the axon direction. The activation function is relevant because previous work has determined that qualitative predictions of neural activation by extracellular sources can be evaluated by direct computation of this parameter.18 It can be assumed that regions of depolarization can be identified where the activation function is positive, whereas regions of hyperpolarization can be identified where the activation function is negative. Also, note that the activation function can be computed if the extracellular potential (VE) and the axon orientation are known.9,18-21
Image Sequences
High-resolution DTI sequences were obtained for the patient with a 3-T magnetic resonance imaging (MRI) scanner using 2-mm-thick oblique axial slices. Diffusion measurements were performed in 60 noncollinear directions with a diffusion weighting factor of 900 s/mm2. Six nondiffusion weights (b values) were used.
In addition, a T1-weighted SPACE MRI sequence and a T2-weighted FLAIR sequence were acquired. The resulting images were used to perform eddy current and distortion corrections for the DTI volumes using TORTOISE version 2.0.1.22 The DTI and T2 images were later resampled and registered to the T1-weighted SPACE image.
Construction of the 3D Model
The structural MRI was used to construct a 3D model of the brain tissue using ScanIP version 6.0 (Simpleware); see Figure 1B. Segmentation of cerebrospinal fluid, gray matter, and white matter was performed manually by creating masks using solid-color filled regions (Figure 1C). This segmentation was later used to compute the solution for VE.
Further resampling of the structural image was performed by means of linear interpolation between neighboring voxels to generate cubic voxels of 0.2 mm. This resolution was necessary to include the depth electrode models. These models were constructed in a computer-aided design (CAD) platform, according to geometric specifications provided by NeuroPace. Specifically, each model had 4 platinum/iridium conductive cylinders (1.27 mm diameter × 2 mm height) separated by insulators (10 mm between the midpoints of the cylinders); see Figure 2A. The CAD electrode lead models were later strategically positioned in the white matter of the segmented MRI data set, within 4-5 mm of the gray–white matter interface, using the +CAD module in Simpleware (Figure 2B and 2C).
The depth electrode placement sites were chosen using 2 functional imaging techniques: subtracted ictal SPECT coregistered to the patient’s MRI (SISCOM), and subtracted postictal DTI (spiDTI). The former was used to identify the ictal onset zones through transient changes in blood perfusion caused during an ictal event. The latter technique, which was developed by researchers at our center to delineate and visualize the epileptic circuit,15 was performed by capitalizing on the transient directionality of water diffusion following a focal-onset seizure. Specifically, acute or transient but evolving postictal changes in fractional anisotropy (FA) could be identified when compared with interictal DTI FA. This technique can be utilized to visualize the subacute remnants of the directionality of an epileptic circuit recruited by focal-onset seizures.23,24 These transient postictal measures are not typically useful in those patients in whom secondarily generalized seizures have occurred. Such widespread propagation pathways may become too complex to analyze. Both SISCOM and spiDTI complemented our standard presurgical scalp video-electroencephalographic monitoring, magnetoencephalography, positron emission tomography, and observed semiology.
The composite model, which included the 3D brain model and the depth leads, was used to construct a variable FEM tetrahedral mesh using ScanIP.
Solving for VE
The FEM mesh was then exported to COMSOL Multiphysics version 4.4 (COMSOL Inc), in which isotropic electric properties were assigned to each segmented tissue and material25 (Table 1). Bipolar stimulation, between two adjacent depth lead contacts, was simulated in the electrodes by applying direct current at

Preimplantation Modeling of Electrode Lead Implant Sites /// 13
4.3 mA. The UMFPACK linear solver was used within COMSOL to compute the extracellular electric potential (VE) by solving a Poisson-like equation derived from electric quasistatic conditions. The solution was performed on a 64-bit dual-processor, 16-core, Windows 7 workstation with 192 GB of accessible RAM.21
Calculation of the Activation Function, Generation of ROIs, and Tractography
The patient’s DTI data set was used to construct an approximation for the 3D axon orientation field. This approximation delivered the orientation of bundles (collection of axons) rather than a specific axon direction. This approximation was necessary because it was not possible to extract directional information of individual axons with the current DTI protocols because of
limited resolution (the size of a voxel is approximately 2 mm). Therefore, a voxel in a DTI data set may contain axons with different directions.
The values of the activation function were computed within the patient’s 3D model using the VE results and the axon directionality field. As discussed previously, regions of depolarization and hyperpolarization were identified where the value of the activation function was positive or negative, respectively. These regions were used to construct 3D ROIs adjacent to the electrode. These ROIs constituted the VOCA solution and were imported as seeds into TrackVis version 0.6 (TrackVis.org).26
Finally, Diffusion Toolkit software26 was used to track DTI fibers using the FACT (Fiber Assignment by Continuous Tracking) algorithm with an angle threshold of 70°. TrackVis was then used to visualize tracts and filter those that entered the imported ROIs.
Postimplant Validation
SAS was used to validate, in vivo, the preoperatively modeled VOCA and white matter propagation circuit. This validation was done 6 months after stereotactic implantation of the depth lead in the patient’s right temporal and left frontal white matter. The stimulation parameters used in the presurgical simulation were delivered during postimplantation testing through contacts 1 and 2 in a bipolar configuration of the left frontal depth electrode. A peripheral intravenous injection of a 5-mL bolus of technetium-99m ethyl cysteinate dimer (99mTc-ECD) was
Table 1. Electrical Values Considered for Segmented Tissue
aRelative permittivity (εR) of all materials is 1.
Materiala Electric Conductivity [S/m]
Cerebrospinal fluid 2.0
Gray matter 0.06
White matter 0.15
Insulator 1 × 10–6
Conductors (platinum/iridium) 1.5 × 107
B C
D
A
Figure 3. A, The solution for VE and its relationship with the E→field streamlines are presented in a 2D sagittal slice that crosses the right temporal region at the
position of the depth electrode. Notice how the E→field is related to the gradient of VE. Also notice how the electric field magnitude decreases as the distance
from the electrode increases (a lower density in streamlines indicates a lower E→field magnitude). B, The diffusion field, obtained from the DTI, is presented in a
2D coronal slice. For simplicity, the y component of the 3D vectors was not considered in the creation of the image. This diffusion field was used to obtain the 3D normal vector field, n. C and D, The activation function was calculated using both n and the solution for VE. The values of the activation function are presented in two cross-sectional 2D sagittal slices at the level of the right temporal depth electrode (C) and depth frontal left electrode (D). Note that areas of depolarization (positive activation function; red) and hyperpolarization (negative activation function; blue) can be identified.

14 /// THE 2017 RUSH NEUROSCIENCE REVIEW
completed during delivery of 20 bursts of high-frequency stimuli (200 Hz) at approximately 2-second intervals (0.5 Hz) for acquisition of an activated SPECT data set. To produce the SAS image, this data set was normalized and subtracted from a baseline SPECT data set obtained 12 hours after the stimulation session. The SAS and the T1 MRI data sets were coregistered using the ITK coregistration algorithm in Analyze version 10 (AnalyzeDirect, Inc).
Results and Validation
The activation function model was used to predict the extent to which direct stimulation therapy can propagate during electrical stimulation for the proposed depth electrode position as follows. The solution for VE was obtained by applying direct current at 4.3 mA between contacts 3 and 4 of the right temporal electrode and between contacts 1 and 2 of the left frontal electrode. This was achieved through construction of a 3D mesh and application of the FEM. The computation in a cross-
sectional 2-dimensional (2D) slice can be observed in Figure 3A, where the maximum value observed for VE was 7.5 V. In addition, this extracellular potential produced a related E
→field (Figure 3A).
The magnitude of the E→field was >1000 mV/mm in areas
within 3-4 mm from the center of the electrodes, as expected.15,27
Following this computation, the DTI was used to create a directionality vector field, n (Figure 3B). Then, the values of both VE and n were used to compute the activation function. Two cross-sectional 2D sagittal slices of the value of the activation function are presented in Figure 3C and Figure 3D, with areas of depolarization and hyperpolarization identified according to the positivity or negativity of the activation function.
Two threshold values were applied to identify the boundaries of the regions of depolarization and hyperpolarization.21 This generated nonspherical 3D ROIs, with a volume that varied from 40 mm3 to 84 mm3, surrounding the active electrode contacts (Figure 4A and 4B). These ROIs were exported to TrackVis as seeds, wherein the influenced tracts were identified
A C D
EB
F
Figure 4. A and B, The calculated ROIs are presented in 2 cross-sectional 2D sagittal slices at the level of the right temporal (RT) electrode position (A) and the left frontal (LF) electrode position (B). The ROIs include regions of depolarization (red) and hyperpolarization (blue) that were obtained by the application of threshold values to the solution of the activation function. Note that the ROIs are nonspherical and vary in shape according to the contact position. C, The anticipated influenced white matter tracts are shown. These results were obtained by exporting the ROIs to a tractography package and filtering the tracts that entered depolarization regions (red and orange tracts) and hyperpolarization regions (dark blue and light blue tracts) at the lead positions (RT and LF). D and E, Stereotactic implantation of the depth leads in both the RT (D) and LF (E) positions is shown. The implantation was guided by our preimplantation model. F, A postimplant CT scan showing the implanted electrodes is presented next to electrocorticography channels (CH) recorded using the implanted RNS System and demonstrating propagation between LF and RT epileptic sources interconnected by white matter (WM). This interconnection is predicted by our tractography model, in which crossing fibers are shown mainly in the genu and the anterior body of the corpus callosum.

Preimplantation Modeling of Electrode Lead Implant Sites /// 15
by filtering those that entered the polarization region. In these tracts, shown in Figure 4C, the ROIs from the left frontal electrode (red and blue) influenced the genu, left forceps minor, and anterior body of the corpus callosum. Importantly, some of the influenced fibers reached the contralateral hemisphere through the splenium of the corpus callosum. Specifically, some of the fibers that crossed the corpus callosum ended at the contralateral temporal lobe. The ROIs from the right temporal lobe (orange and light blue) influenced the ipsilateral uncinate fasciculus, the inferior longitudinal fasciculus (reaching the right occipital lobe), and the fornix tracts.
Stereotactic implantation of two RNS depth leads was guided by our preimplant electrode lead plan. A 4-contact, 1-cm center-to-center depth lead was placed in the right paramesial temporal region using a posterior-to-frontal longitudinal approach in paramesial white matter (Figure 4D). A 4-contact, 2.5-mm center-to-center depth lead was placed using a lateral-to-medial approach in the left frontal lobe targeting the white matter (Figure 4E). The trajectories were guided by our preimplantation model and were facilitated by a Stealth (Medtronic) MRI navigational system. The final positions of the electrode contacts are shown in Figure 4F.
Proof of the principle is demonstrated electrophysiologically in Figure 4F, in which electrocorticography obtained by the implanted RNS System shows propagation between contralateral epileptic sources interconnected by white matter pathways, as predicted by the tractography model. Propagation from the left frontal source to the right temporal source is illustrated.
A SAS study performed during stimulation of distal contacts 1 and 2 of the depth frontal electrode demonstrated transient hyperperfusion and hypoperfusion changes beyond the immediately surrounding tissue. No afterdischarge was recorded by electrocorticography at the site of stimulation. Therefore, these transient hyper- and hypoperfusion-related changes were due to direct stimulation itself and not produced by epileptiform activity. The results of the SAS study are presented next to the preimplant model of the left frontal depth electrode in Figure 5. The gray matter regions of transient hypoperfusion included the contralateral (right) frontal lobe and the ipsilateral (left) parietal cortex, whereas the gray matter regions of transient hyperperfusion included the contralateral (right) anterior temporal region, the ipsilateral (left) head of caudate near the electrode contacts stimulated during the SAS protocol, the contralateral (right) frontal pole, and the contralateral (right) frontal operculum.
Figure 5. A comparison between the preimplant modulated circuit tractography model of the left frontal depth electrode (A) and postimplant SAS (B and C) is presented. The SAS regions of transient hypoperfusion (B) and hyperperfusion (C) coregistered to MRI are displayed separately. Contacts 1 and 2 of the left frontal depth electrode were stimulated without causing a seizure (afterdischarge). The gray matter regions of transient hypoperfusion included the contralateral (right) frontal lobe (1) and the ipsilateral (left) parietal cortex (2), whereas the gray matter regions of transient hyperperfusion included the contralateral (right) temporal region (3), the ipsilateral (left) head of caudate (4), the contralateral (right) frontal pole (5), and the contralateral (right) frontal operculum (6). Note that the tractography in the preimplant plan terminated near or within the regions concordant with the SAS study.
A B
C

16 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Because the stimulation in the left frontal lead produced transient hyperperfusion in the contralateral temporal lobe, these data suggest communication between the epileptic sources that was predicted by the modulated circuit tractography model. This communication was evident in the electrocorticography presented in Figure 4F, which was discussed previously.
Conclusion
This practical application of the activation function model, which is based on the second directional derivative of the extracellular potential, demonstrates the ability to generate a timely preimplant depth electrode planning map for a patient with a refractory epileptogenic circuit. This simulation predicted the white matter tracts that were influenced by direct neurostimulation therapy. That is, the VOCA and modeled modulated circuit tractography map can be visualized before implantation, thereby enabling their inclusion in the final RNS System lead placement plan. Furthermore, the application of the activation function offers an improvement over previously reported activation regions produced by the magnitudes of the E→fields. This model offers the potential for steering the VOCA
to predict the optimal electrode contact implant sites. It considers not only the magnitude of the E
→field, but also
directionality effects in relation to the orientation of the axon bundle.
The electrode placement model, seen as a specialized type of brain–computer interface planning, may improve the probability of modulating the maximal extent of an epileptic network with minimum electrode contacts by targeting white matter, not simply the presumed gray matter focus. Moreover, the demonstration of a mechanistic interplay between cortical and subcortical structures, such as the thalamus, may provide a basis for future clinical trials combining stimulation of both regions. Further development of this strategy will clarify and lead to a better understanding of the individual differences seen when direct cortical stimulation is delivered though white matter pathways to distant epileptogenic neural tissue. The data obtained with this model emphasize the need to recognize localization-related epilepsies as being potentially extensive pathophysiologic neural networks.

Preimplantation Modeling of Electrode Lead Implant Sites /// 17
References1. Morrell MJ, Hirsch LJ, Bergey G, et al. Long-term safety and efficacy of the RNS system in adults with medically intractable partial onset seizures. Epilepsia. 2008;49(s7):480.
2. Morrell MJ; RNS System in Epilepsy Study Group. Responsive cortical stimulation for the treatment of medically intractable partial epilepsy. Neurology. 2011;77(13):1295-1304.
3. Bergey GK, Morrell MJ, Mizrahi EM, et al. Long-term treatment with responsive brain stimulation in adults with refractory partial seizures. Neurology. 2015;84(8):810-817.
4. Beurrier C, Bioulac B, Audin J, Hammond C. High-frequency stimulation produces a transient blockade of voltage-gated currents in subthalamic neurons. J Neurophysiol. 2001;85(4):1351-1356.
5. Dostrovsky JO, Levy R, Wu JP, Hutchison WD, Tasker RR, Lozano AM. Microstimulation induced inhibition of neuronal firing in human globus pallidus. J Neurophysiol. 2000;84(1):570-574.
6. Urbano FJ, Leznik E, Llinás RR. Cortical activation patterns evoked by afferent axons stimuli at different frequencies: an in vivo voltage-sensitive dye imaging study. Thalamus Relat Syst. 2002;1:371-378.
7. Montgomery EB Jr, Baker KB. Mechanisms of deep brain stimulation and future technical developments. Neurol Res. 2000;22(3):259-266.
8. Fukuda M, Mentis MJ, Ma Y, et al. Networks mediating the clinical effects of pallidal brain stimulation for Parkinson’s disease: a PET study of resting-state glucose metabolism. Brain. 2001;124(pt 8):1601-1609.
9. McIntyre CC, Mori S, Sherman DL, Thakor NV, Vitek JL. Electric field and stimulating influence generated by deep brain stimulation of the subthalamic nucleus. Clin Neurophysiol. 2004;115(3):589-595.
10. Zumsteg D, Lozano AM, Wennberg RA. Mesial temporal inhibition in a patient with deep brain stimulation of the anterior thalamus for epilepsy. Epilepsia. 2006;47(11):1958-1662.
11. Keller A, Arissian K, Asanuma H. Synaptic proliferation in the motor cortex of adult cats after thalamic stimulation. J Neurophysiol. 1992;68(1):295-308.
12. Butson CR, Cooper SE, Henderson JM, McIntyre CC. Patient-specific analysis of the volume of tissue activated during deep brain stimulation. Neuroimage. 2007;34(2):661-670.
13. Durand DM, Bikson M. Control of neuronal activity by electric fields: in vitro models of epilepsy. In: Lüders H, ed. Deep Brain Stimulation and Epilepsy. London, England: Martin Dunitz; 2004:67-86.
14. Wagenaar DA, Pine J, Potter SM. Effective parameters for stimulation of dissociated cultures using multi-electrode arrays. J Neurosci Methods. 2004;138(1-2):27-37.
15. Rossi MA, Stebbins G, Murphy C, et al. Predicting white matter targets for direct neurostimulation therapy. Epilepsy Res. 2010;91 (2-3):176-186.
16. Lavenex P, Banta Lavenex P, Amaral DG. Postnatal development of the primate hippocampal formation. Dev Neurosci. 2007;29(1-2):179-192.
17. Rossi MA, Hoeppner TJ, Byrne RW, et al. Subtracted activated SPECT validates depth lead placement in white matter for responsive neurostimulation therapy in refractory partial-onset epilepsy. Epilepsia. 2008;49(suppl 7):355.
18. Rattay F. Analysis of models for external stimulation of axons. IEEE Trans Biomed Eng. 1986;33(10):974-977.
19. Warman EN, Grill WM, Durand D. Modeling the effects of electric fields on nerve fibers: determination of excitation thresholds. IEEE Trans Biomed Eng. 1992;39(12):1244-1254.
20. Rattay F. The basic mechanism for the electrical stimulation of the nervous system. Neuroscience. 1999;89(2):335-346.
21. Cendejas Zaragoza L, Byrne RW, Rossi MA. Pre-implant modeling of depth lead placement in white matter for maximizing the extent of cortical activation during direct neurostimulation therapy. Neurol Res. 2017;39(3):198-211.
22. Pierpaoli C, Walker L, Irfanoglu MO, et al. TORTOISE: an integrated software package for processing of diffusion MRI data. Proc Int Soc Magn Reson Med. 2010;18:1597.
23. Diehl B, Symms MR, Boulby PA, et al. Postictal diffusion tensor imaging. Epilepsy Res. 2005;65(3):137-146.
24. Rossi MA. Regaining white matter integrity and neurocognitive development in rolandic epilepsy after the storm. Epilepsy Curr. 2015;15(1):20-23.
25. Andreuccetti D, Fossi R, Petrucci C. An internet resource for the calculation of the dielectric properties of body tissues in the frequency range 10 Hz - 100 GHz [based on data published by Gabriel C et al in 1996]. Italian National Research Council website. http://niremf.ifac.cnr.it/tissprop. Published 1997. Accessed July 20, 2014.
26. Wang R, Benner T, Sorensen AG, Wedeen VJ. Diffusion toolkit: a software package for diffusion imaging data processing and tractography. Proc Int Soc Magn Reson Med. 2007;15:3720.
27. Aström M, Johansson JD, Hariz MI, Eriksson O, Wårdell K. The effect of cystic cavities on deep brain stimulation in the basal ganglia: a simulation-based study. J Neural Eng. 2006;3(2):132-138. //

18 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Author affiliation: Department of Neurological Sciences, Rush University Medical Center, Chicago, Illinois.
Corresponding author: Kalipada Pahan, PhD, Department of Neurological Sciences, Rush University Medical Center, 1735 W Harrison St, Suite 310, Chicago, IL 60612 ([email protected]).
Introduction
Although brain function decreases with age, in some people the brain functions normally until death. Several risk factors may contribute to decelerated brain function. Among these factors, it has been demonstrated that people with high amounts of abdominal fat in middle age are 3.6 times more likely to develop memory problems later in life than people with less abdominal fat in middle age are.1 Accordingly, a diet rich in saturated long-chain fatty acids decreases memory and learning in mice.2 Although the mechanisms by which abnormal fat metabolism interacts with brain function are not yet fully understood, recent research at our institution has shed some light on a lipid-lowering factor that appears to have various effects on the brain.
This factor, peroxisome proliferator-activated receptor α (PPARα), is a nuclear hormone receptor family transcription factor that controls the metabolism of fatty acids in the liver. Although the brain is not a metabolic organ, we have recently demonstrated that PPARα is constitutively expressed in different parts of the hippocampus.3,4 PPARα is also constitutively present in neurons3,5 and astrocytes.6 Various functions in the brain are controlled and coordinated at the transcriptional level by cAMP response element-binding protein (CREB). We have found that PPARα controls the transcription of CREB and regulates memory and learning.3
The action of PPARα is affected by statins, which are cholesterol-lowering drugs that are widely used throughout the world. Statins have been found to bind to PPARα and protect memory in an animal model of Alzheimer’s disease.6 One of the pathologic hallmarks of Alzheimer’s disease is the presence of
extracellular amyloid plaques (Figure 1) containing amyloid β peptides, which originate from the amyloidogenic proteolytic processing of amyloid precursor protein (APP) through the sequential action of β- and γ-secretases. In contrast, APP can also be cleaved in a nonamyloidogenic pathway by α-secretase, precluding the formation of amyloid β peptides. We have found that activation of PPARα stimulates the transcription of ADAM10 α-secretase and lowers the level of amyloid plaques in an animal model of Alzheimer’s disease.5
Normal and pathologic aging are often linked to reduction in autophagic potential. Moreover, reduced autophagy is also a hallmark of different neurodegenerative disorders. Lysosomes are classically considered to be central to autophagy and the mechanisms of cellular waste management. We have seen that PPARα controls the activity of tripeptidyl peptidase 1 (TPP1) via transcriptional control of the Cln2 gene7 and stimulates lysosomal biogenesis in astrocytes via direct transcriptional
IMPROVEMENT OF BRAIN FUNCTION BY A LIPID-LOWERING FACTOR
Kalipada Pahan, PhD
Figure 1. Neurons with amyloid plaques (right side) compared to healthy neurons (left). Amyloid plaques accumulate outside neurons and are characteristic features of Alzheimer’s disease. They lead to degeneration of the affected neurons, which are destroyed through the activity of microglia cells.
Improvement of Brain Function by a Lipid-Lowering Factor /// 19
regulation of transcription factor EB (TFEB), the master regulator of lysosomal biogenesis,8 thereby contributing to autophagy. Therefore, the activation of PPARα can lower the production of amyloid plaques, stimulate lysosomal clearance mechanisms, and protect memory and learning. Moreover, PPARα may play a role in controlling sleep.
PPARαand Lipid Metabolism
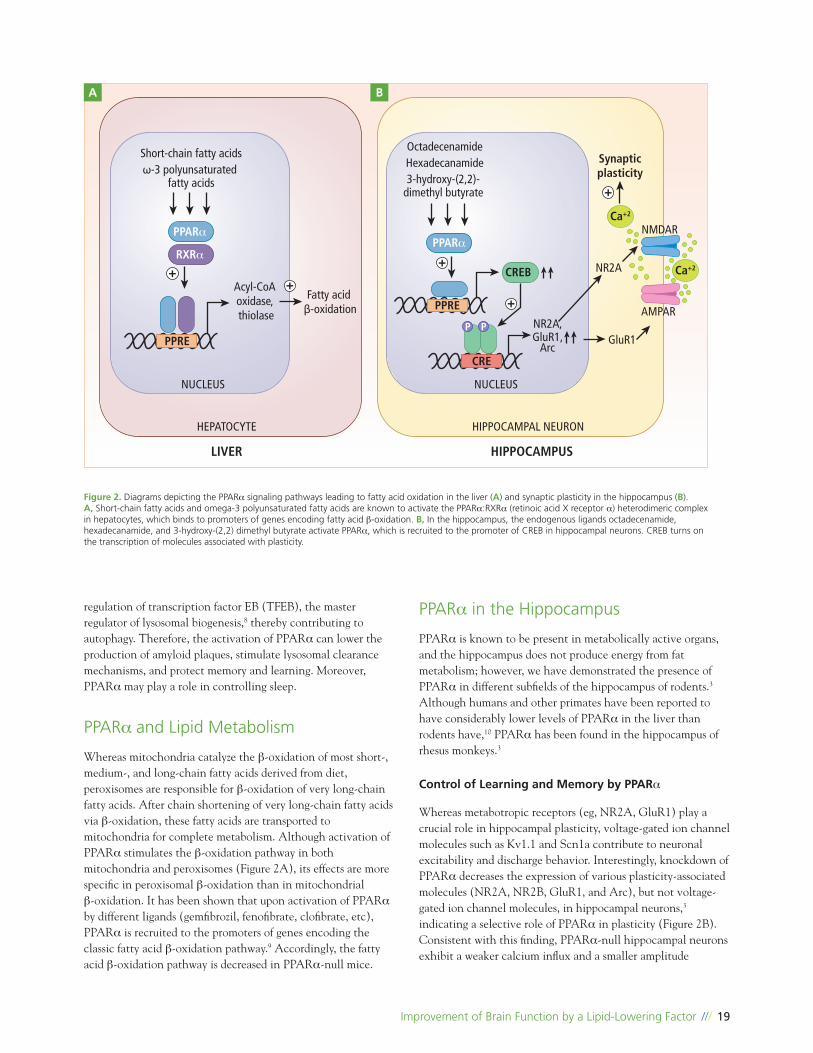
Whereas mitochondria catalyze theβ-oxidation of most short-, medium-, and long-chain fatty acids derived from diet, peroxisomes are responsible for β-oxidation of very long-chain fatty acids. After chain shortening of very long-chain fatty acids viaβ-oxidation, these fatty acids are transported to mitochondria for complete metabolism. Although activation of PPARα stimulates the β-oxidation pathway in both mitochondria and peroxisomes (Figure 2A), its effects are more specific in peroxisomalβ-oxidation than in mitochondrial β-oxidation. It has been shown that upon activation of PPARα by different ligands (gemfibrozil, fenofibrate, clofibrate, etc), PPARα is recruited to the promoters of genes encoding the classic fatty acid β-oxidation pathway.9 Accordingly, the fatty acid β-oxidation pathway is decreased in PPARα-null mice.
PPARα in the Hippocampus
PPARα is known to be present in metabolically active organs, and the hippocampus does not produce energy from fat metabolism; however, we have demonstrated the presence of PPARα in different subfields of the hippocampus of rodents.3 Although humans and other primates have been reported to have considerably lower levels of PPARα in the liver than rodents have,10 PPARα has been found in the hippocampus of rhesus monkeys.3
Control of Learning and Memory by PPARα
Whereas metabotropic receptors (eg, NR2A, GluR1) play a crucial role in hippocampal plasticity, voltage-gated ion channel molecules such as Kv1.1 and Scn1a contribute to neuronal excitability and discharge behavior. Interestingly, knockdown of PPARα decreases the expression of various plasticity-associated molecules (NR2A, NR2B, GluR1, and Arc), but not voltage-gated ion channel molecules, in hippocampal neurons,3 indicating a selective role of PPARα in plasticity (Figure 2B). Consistent with this finding, PPARα-null hippocampal neurons exhibit a weaker calcium influx and a smaller amplitude
Figure 2. Diagrams depicting the PPARα signaling pathways leading to fatty acid oxidation in the liver (A) and synaptic plasticity in the hippocampus (B). A, Short-chain fatty acids and omega-3 polyunsaturated fatty acids are known to activate the PPARα:RXRα (retinoic acid X receptor α) heterodimeric complex in hepatocytes, which binds to promoters of genes encoding fatty acid β-oxidation. B, In the hippocampus, the endogenous ligands octadecenamide, hexadecanamide, and 3-hydroxy-(2,2) dimethyl butyrate activate PPARα, which is recruited to the promoter of CREB in hippocampal neurons. CREB turns on the transcription of molecules associated with plasticity.
++
++
+
Short-chain fatty acids
HEPATOCYTE HIPPOCAMPAL NEURON
NUCLEUS NUCLEUS
LIVER HIPPOCAMPUS
Acyl-CoA oxidase, thiolase
Fatty acid β-oxidation
PPARαPPARα
CREB
Ca+2
Ca+2
PPRE
PPRE
P P
CRE
RXRα
ω-3 polyunsaturated fatty acids
OctadecenamideSynapticplasticity
NR2A,GluR1,
Arc
NR2A
NMDAR
AMPAR
GluR1
Hexadecanamide3-hydroxy-(2,2)-
dimethyl butyrate
A B
20 /// THE 2017 RUSH NEUROSCIENCE REVIEW
oscillation than wild-type neurons in response to both AMPA and NMDA,3 suggesting that PPARα plays a role in controlling the synaptic plasticity in hippocampal neurons. Although there are no significant differences in body weight, general motor behavior, and average food consumption between wild-type and PPARα-null mice, PPARα-null mice have been found to be deficient in spatial learning and memory, compared with wild-type mice.3 This finding is consistent with the involvement of CREB in the generation of long-term memory and spatial learning.11 Upregulation of CREB and restoration of memory and learning in PPARα-null mice by lentiviral delivery of PPARαinto the hippocampus suggests an important role of PPARα in memory and learning.3 Omega-3 fatty acids, such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which are present in fatty fish, have been found to be essential for brain health. Studies have shown that people having more of these fatty acids in their blood or a long-term habit of eating fish every week are less likely to develop Alzheimer’s disease.12,13 Because both DHA and EPA are ligands of PPARα, it is possible that DHA and EPA support hippocampal memory and learning via PPARα.
Hippocampal Memory Not Directly Controlled by Hepatic PPARα
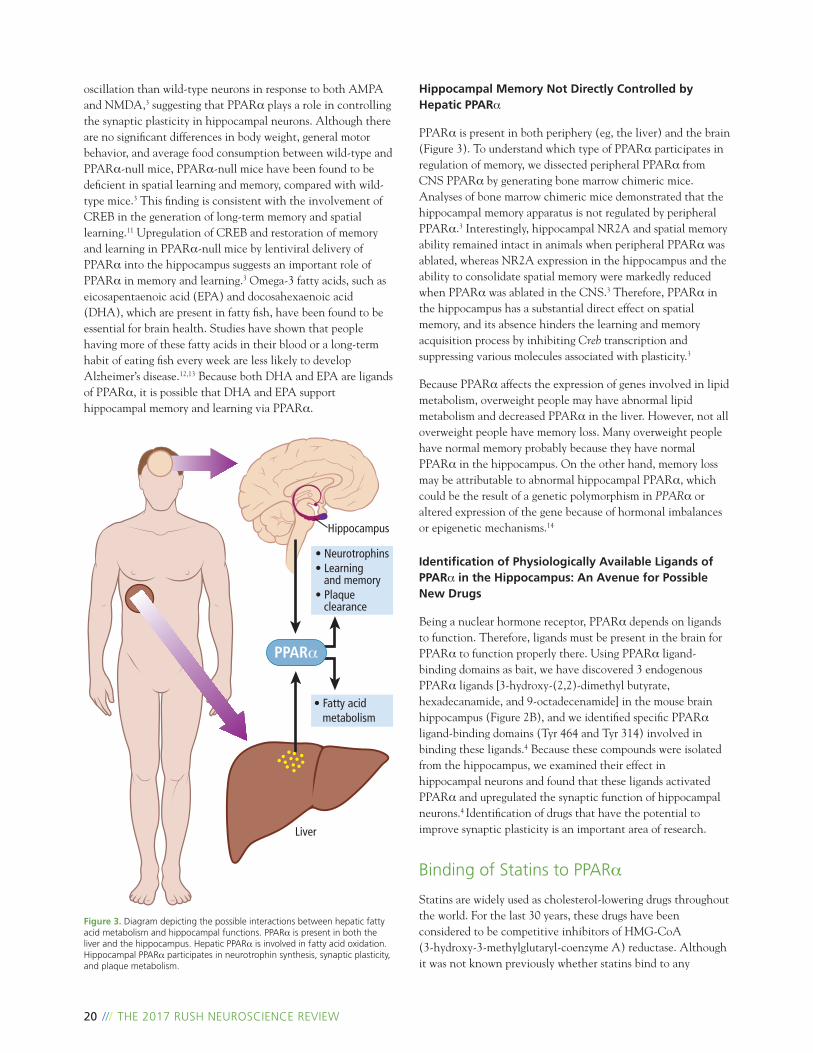
PPARα is present in both periphery (eg, the liver) and the brain (Figure 3). To understand which type of PPARα participates in regulation of memory, we dissected peripheral PPARα from CNS PPARα by generating bone marrow chimeric mice. Analyses of bone marrow chimeric mice demonstrated that the hippocampal memory apparatus is not regulated by peripheral PPARα.3 Interestingly, hippocampal NR2A and spatial memory ability remained intact in animals when peripheral PPARα was ablated, whereas NR2A expression in the hippocampus and the ability to consolidate spatial memory were markedly reduced when PPARα was ablated in the CNS.3 Therefore, PPARα in the hippocampus has a substantial direct effect on spatial memory, and its absence hinders the learning and memory acquisition process by inhibiting Creb transcription and suppressing various molecules associated with plasticity.3
Because PPARα affects the expression of genes involved in lipid metabolism, overweight people may have abnormal lipid metabolism and decreased PPARα in the liver. However, not all overweight people have memory loss. Many overweight people have normal memory probably because they have normal PPARα in the hippocampus. On the other hand, memory loss may be attributable to abnormal hippocampal PPARα, which could be the result of a genetic polymorphism in PPARα or altered expression of the gene because of hormonal imbalances or epigenetic mechanisms.14
Identification of Physiologically Available Ligands of PPARα in the Hippocampus: An Avenue for Possible New Drugs
Being a nuclear hormone receptor, PPARα depends on ligands to function. Therefore, ligands must be present in the brain for PPARα to function properly there. Using PPARα ligand-binding domains as bait, we have discovered 3 endogenous PPARα ligands [3-hydroxy-(2,2)-dimethyl butyrate, hexadecanamide, and 9-octadecenamide] in the mouse brain hippocampus (Figure 2B), and we identified specific PPARα ligand-binding domains (Tyr 464 and Tyr 314) involved in binding these ligands.4 Because these compounds were isolated from the hippocampus, we examined their effect in hippocampal neurons and found that these ligands activated PPARα and upregulated the synaptic function of hippocampal neurons.4 Identification of drugs that have the potential to improve synaptic plasticity is an important area of research.
Binding of Statins to PPARα
Statins are widely used as cholesterol-lowering drugs throughout the world. For the last 30 years, these drugs have been considered to be competitive inhibitors of HMG-CoA (3-hydroxy-3-methylglutaryl-coenzyme A) reductase. Although it was not known previously whether statins bind to any
Figure 3. Diagram depicting the possible interactions between hepatic fatty acid metabolism and hippocampal functions. PPARα is present in both the liver and the hippocampus. Hepatic PPARα is involved in fatty acid oxidation. Hippocampal PPARα participates in neurotrophin synthesis, synaptic plasticity, and plaque metabolism.
Hippocampus
• Neurotrophins• Learning and memory• Plaque clearance
• Fatty acid metabolism
Liver
PPARα

Improvement of Brain Function by a Lipid-Lowering Factor /// 21
receptor protein, we have recently discovered that statins bind to the ligand-binding domain of PPARα and serve as ligands of PPARα.6 Among simvastatin, mevastatin, pravastatin, atorvastatin, and rosuvastatin, simvastatin was found to be the strongest ligand of PPARα, followed by mevastatin. The ligand-binding efficacies of pravastatin, atorvastatin, and rosuvastatin were similar to each other.6 Interestingly, statins upregulate neurotrophins in brain cells via PPARα-mediated transcriptional activation of CREB. Neurotrophins are important for neuronal health and function. Simvastatin treatment also increased BDNF (brain-derived neurotrophic factor) in the hippocampus and cortex and improved memory and learning in an animal model of Alzheimer’s disease via PPARα.6 These findings disclose a new site of action (PPARα) for statins that could offer the potential for therapeutic benefit in patients with Alzheimer’s disease.
PPARα and Plaque Formation
Understanding how plaques are formed is important for the development of effective drugs that lower plaques and stop the progression of Alzheimer’s disease. In the brain of patients with Alzheimer’s disease, pieces of beta-amyloid protein clump together to form hard, insoluble plaques. The beta-amyloid protein pieces come from a parent protein called amyloid precursor protein. In a healthy brain, this precursor protein is broken down by another protein, called ADAM10, in such a way as to preclude the formation of beta-amyloid. We have found that neurons from mice lacking PPARα contain less ADAM10 than is found in neurons from normal mice.5 Our results also indicate that mice lacking PPARα produce more beta-amyloid than normal mice, and in a mouse model of Alzheimer’s disease, the PPARα-deficient mice have more amyloid plaques in their brains and shorter life expectancies than normal mice have. We have seen that a combination of gemfibrozil (a lipid-lowering drug approved by the US Food and Drug Administration) and the vitamin A derivative retinoic acid induces the activation of PPARα, increases ADAM10, and reduces amyloid plaques in the brain in a mouse model of Alzheimer’s disease.5 Replication of these results in human patients with Alzheimer’s disease would open up a promising avenue of treatment for patients with this devastating neurodegenerative disease.
Possible Role of PPARα in Sleep
Despite intense investigation, sleep remains a poorly understood process, and the mechanisms by which it is regulated are unclear. Notably, 9-octadecenamide or oleamide, one of the three hippocampal ligands that we recently isolated,4 is a sleep-inducing supplement. Therefore, it is possible that PPARα plays a role in sleep as well. However, at present, detailed mechanisms are not known. Because 9-octadecenamide and the related compounds 3-hydroxy-(2,2)-dimethyl butyrate and hexadecanamide are constitutively present in the hippocampus as PPARα ligands, an area of future research would be to determine whether these compounds contribute to sleep via PPARα.
Conclusion
These studies illustrate a far-reaching possibility of improving hippocampal functions and preventing memory loss by restoring and/or maintaining normal PPARα activation in the hippocampus. In this respect, our newly discovered physiological ligands of PPARα from the hippocampus may serve as novel brain-derived drugs for maintaining normal brain functions. At present, our lab is involved in investigating this avenue of research.
Acknowledgments: This study was supported by the Zenith Fellows Award (ZEN-17-438829) from the Alzheimer’s Association, grants from the National Institutes of Health (AG050431, NS83054, and NS97426), and merit awards (I01BX002174 and 1I01BX003033) from the US Department of Veterans Affairs.

22 /// THE 2017 RUSH NEUROSCIENCE REVIEW
References1. Abdominal fat boosts later dementia risk. Harv Ment Health Lett. 2008;25(1):7.
2. Granholm AC, Bimonte-Nelson HA, Moore AB, Nelson ME, Freeman LR, Sambamurti K. Effects of a saturated fat and high cholesterol diet on memory and hippocampal morphology in the middle-aged rat. J Alzheimers Dis. 2008;14(2):133-145.
3. Roy A, Jana M, Corbett GT, et al. Regulation of cyclic AMP response element binding and hippocampal plasticity-related genes by peroxisome proliferator-activated receptor α. Cell Rep. 2013;4(4):724-737.
4. Roy A, Kundu M, Jana M, et al. Identification and characterization of PPARα ligands in the hippocampus. Nat Chem Biol. 2016;12(12):1075-1083.
5. Corbett GT, Gonzalez FJ, Pahan K. Activation of peroxisome proliferator-activated receptor alpha stimulates ADAM10-mediated proteolysis of APP. Proc Natl Acad Sci U S A. 2015;112(27):8445-8450.
6. Roy A, Jana M, Kundu M, et al. HMG-CoA reductase inhibitors bind to PPARα to upregulate neurotrophin expression in the brain and improve memory in mice. Cell Metab. 2015;22(2):253-265.
7. Ghosh A, Corbett GT, Gonzalez FJ, Pahan K. Gemfibrozil and fenofibrate, Food and Drug Administration-approved lipid-lowering drugs, up-regulate tripeptidyl-peptidase 1 in brain cells via peroxisome proliferator-activated receptor α: implications for late infantile Batten disease therapy. J Biol Chem. 2012;287(46):38922-38935.
8. Ghosh A, Jana M, Modi K, et al. Activation of peroxisome proliferator-activated receptor α induces lysosomal biogenesis in brain cells: implications for lysosomal storage disorders. J Biol Chem. 2015;290(16):10309-10324.
9. Reddy JK, Mannaerts GP. Peroxisomal lipid metabolism. Annu Rev Nutr. 1994;14:343-370.
10. Tugwood JD, Holden PR, James NH, Prince RA, Roberts RA. A peroxisome proliferator-activated receptor-alpha (PPARalpha) cDNA cloned from guinea-pig liver encodes a protein with similar properties to the mouse PPARalpha: implications for species differences in responses to peroxisome proliferators. Arch Toxicol. 1998;72(3):169-177.
11. Ghosh A, Ginty DD, Bading H, Greenberg ME. Calcium regulation of gene expression in neuronal cells. J Neurobiol. 1994;25(3):294-303.
12. Cederholm T, Salem N Jr, Palmblad J. α-3 fatty acids in the prevention of cognitive decline in humans. Adv Nutr. 2013;4(6):672-676.
13. Sinn N, Milte CM, Street SJ, et al. Effects of n-3 fatty acids, EPA v. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: a 6-month randomised controlled trial. Br J Nutr. 2012;107(11):1682-1693.
14. Roy A, Pahan K. PPARα signaling in the hippocampus: crosstalk between fat and memory. J Neuroimmune Pharmacol. 2015;10(1):30-34. //

Predictors of False-Positive Stroke Thrombectomy Transfers /// 23
Author Affiliations: University of Illinois at Chicago, Chicago, Illinois (Dr Yi); Department of Neurological Surgery, Rush University Medical Center, Chicago, Illinois (Ms Zielinski and Dr Chen); and Department of Neurological Sciences, Rush University Medical Center, Chicago, Illinois (Drs Ouyang, Conners, and Dafer).
Corresponding Author: Michael Chen, MD, Rush University Medical Center, 1725 W Harrison St, Suite 855, Chicago, IL 60612 ([email protected]).
Introduction
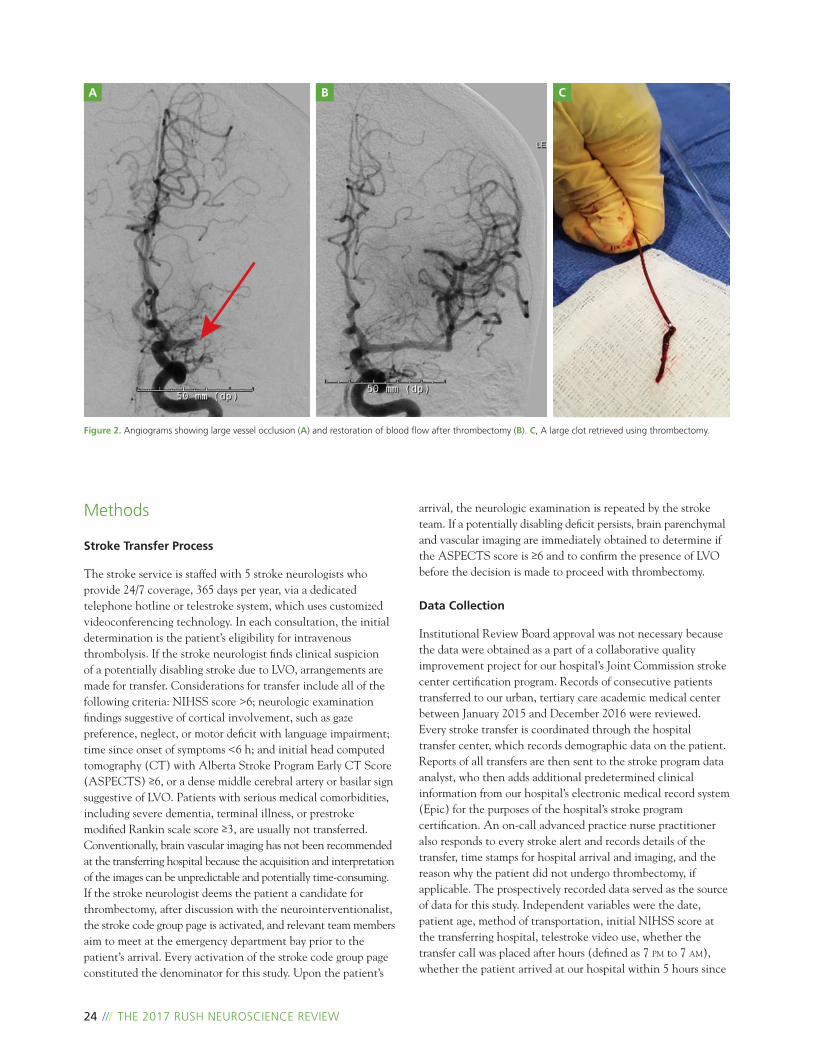
For nearly 20 years, hospitals caring for acute stroke patients have been organized to deliver intravenous thrombolysis. Although robust level 1a evidence demonstrating a clinical benefit of mechanical thrombectomy in patients with acute anterior circulation large vessel occlusions (LVOs)(Figure 2) was published in 2015,1-3 only approximately 10% of the more than 1111 primary stroke centers in the United States are able to reliably provide mechanical thrombectomy. As a result, most patients initially evaluated and deemed to have LVO need to be transferred to a hospital that can provide this treatment.
Over the last 2 years, our stroke team (Figure 1) has noticed a large number of patients transferred for thrombectomy who do not end up undergoing the procedure. To minimize time to recanalization, the decision to transfer a patient for thrombectomy is often based on the severity of the clinical examination rather than on brain vascular imaging. As suggested by American Heart Association/American Stroke Association guidelines, a National Institutes of Health Stroke Scale (NIHSS) score >6 is often used as a surrogate marker for the presence of LVO.4 Turc et al5 evaluated the ability of 13 clinical scores to predict large artery occlusions in more than 1000 patients and found false-negative and false-positive rates that were higher than expected. Furthermore, patient transfers for potential thrombectomy have considerable costs, which include but are not limited to ambulance/helicopter services, call pay for the neuroendovascular and stroke neurology team, repeat imaging, and the cost of the temporary suspension of the team members’ other activity as they await the patient’s arrival.6
Sonig et al7 evaluated 1 311 511 National Inpatient Sample stroke admissions from 2008 to 2010 and found that the mean expenditure for transferred patients undergoing intravenous thrombolysis and thrombectomy was $27 000 more than that of those who were not transferred. Thus, despite the potential to incur substantial unnecessary costs, the decision to transfer is currently based on an oblique measure suggesting the presence of LVO.
In this study, we measured the frequency of nontreatment transfers since the publication of the positive thrombectomy trials in 20151-3 and evaluated the most common reasons why transferred patients did not undergo thrombectomy. The purpose of the study was to find potential predictors of nontreatment transfers based on the limited clinical information available during the initial evaluation at the transferring hospital. Our hope is that identifying these predictors may enable the development of strategies to improve the transfer decision process.
PREDICTORS OF FALSE-POSITIVE STROKE THROMBECTOMY TRANSFERS
Julia Yi, MD // Danielle Zielinski, RN, MSN, AG-ACNP // Bichun Ouyang, PhD // James Conners, MD, MS Rima Dafer, MD, MPH, FAHA // Michael Chen, MD
Figure 1. Neurointerventionalist Michael Chen, MD, is part of a multidisciplinary team at Rush dedicated to rapid, coordinated treatment of stroke patients.
24 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Methods
Stroke Transfer Process
The stroke service is staffed with 5 stroke neurologists who provide 24/7 coverage, 365 days per year, via a dedicated telephone hotline or telestroke system, which uses customized videoconferencing technology. In each consultation, the initial determination is the patient’s eligibility for intravenous thrombolysis. If the stroke neurologist finds clinical suspicion of a potentially disabling stroke due to LVO, arrangements are made for transfer. Considerations for transfer include all of the following criteria: NIHSS score >6; neurologic examination findings suggestive of cortical involvement, such as gaze preference, neglect, or motor deficit with language impairment; time since onset of symptoms <6 h; and initial head computed tomography (CT) with Alberta Stroke Program Early CT Score (ASPECTS) ≥6, or a dense middle cerebral artery or basilar sign suggestive of LVO. Patients with serious medical comorbidities, including severe dementia, terminal illness, or prestroke modified Rankin scale score ≥3, are usually not transferred. Conventionally, brain vascular imaging has not been recommended at the transferring hospital because the acquisition and interpretation of the images can be unpredictable and potentially time-consuming. If the stroke neurologist deems the patient a candidate for thrombectomy, after discussion with the neurointerventionalist, the stroke code group page is activated, and relevant team members aim to meet at the emergency department bay prior to the patient’s arrival. Every activation of the stroke code group page constituted the denominator for this study. Upon the patient’s
arrival, the neurologic examination is repeated by the stroke team. If a potentially disabling deficit persists, brain parenchymal and vascular imaging are immediately obtained to determine if the ASPECTS score is ≥6 and to confirm the presence of LVO before the decision is made to proceed with thrombectomy.
Data Collection
Institutional Review Board approval was not necessary because the data were obtained as a part of a collaborative quality improvement project for our hospital’s Joint Commission stroke center certification program. Records of consecutive patients transferred to our urban, tertiary care academic medical center between January 2015 and December 2016 were reviewed. Every stroke transfer is coordinated through the hospital transfer center, which records demographic data on the patient. Reports of all transfers are then sent to the stroke program data analyst, who then adds additional predetermined clinical information from our hospital’s electronic medical record system (Epic) for the purposes of the hospital’s stroke program certification. An on-call advanced practice nurse practitioner also responds to every stroke alert and records details of the transfer, time stamps for hospital arrival and imaging, and the reason why the patient did not undergo thrombectomy, if applicable. The prospectively recorded data served as the source of data for this study. Independent variables were the date, patient age, method of transportation, initial NIHSS score at the transferring hospital, telestroke video use, whether the transfer call was placed after hours (defined as 7 pm to 7 am), whether the patient arrived at our hospital within 5 hours since
Figure 2. Angiograms showing large vessel occlusion (A) and restoration of blood flow after thrombectomy (B). C, A large clot retrieved using thrombectomy.
A B C

the last known well time, and whether the referring hospital was a Joint Commission–certified primary stroke center. Outcomes included the total number of transfers, the number of nontreatment transfers, and the reasons why those patients were not treated. We used chi-square tests and multivariate logistic regression analysis to compare demographic and clinical variables, including age, NIHSS score, and other variables, between patients with and without thrombectomy. All statistical analyses were performed with SAS 9.3 (SAS Institute). P < .05 was considered statistically significant.
Results
Between January 2015 and December 2016, 106 of the 194 patients transferred for potential thrombectomy (55%) did not undergo thrombectomy. Brain vascular imaging upon arrival—usually computed tomography angiography (CTA)—showing no LVO was by far the most common reason for not undergoing thrombectomy (71 of 106 transfers [67%]). A substantially improved neurologic examination and Alberta Stroke Program Early CT Score (ASPECTS) <6 were the next two most common reasons for nontreatment but were far less common than the first reason (Table 1). Approximately one-third of all transfers were by means of air transport, and approximately one-third occurred during the evening hours. Nearly half of the transferred patients were first evaluated with telestroke video. Most patients received intravenous thrombolysis, most arrived within 5 hours, and most came from a Joint Commission–certified primary stroke center.
The strongest predictor of no treatment was the initial NIHSS score; 14 of 16 patients (88%) with NIHSS score <10 did not undergo thrombectomy, whereas 41 of 78 patients (53%) with NIHSS score >20 underwent thrombectomy (P < .001). Helicopter use was significantly associated with no treatment (P = .003). Arrival within 5 hours was significantly associated with treatment (P < .001); see Table 2. The NIHSS score (as a continuous variable), helicopter use, and arrival within 5 hours were all identified as predictors in multivariate logistic regression analysis (Table 3).
Predictors of False-Positive Stroke Thrombectomy Transfers /// 25
Table 1. Reasons for No Treatment Among Consecutive Patients Transferred for Mechanical Thrombectomy
Abbreviation: ASPECTS, Alberta Stroke Program Early CT Score.
Reason No. (%) (n = 106)
No large vessel occlusion on imaging 71 (67%)
Substantial improvement on examination 19 (18%)
ASPECTS <6 10 (9%)
Premorbid disability discovered 3 (3%)
Patient unstable 3 (3%)
Table 2. Predictors of No Treatment Among Consecutive Patients Transferred for Mechanical Thrombectomy
Abbreviation: NIHSS, National Institutes of Health Stroke Scale.a All values are given as number and percentage except as noted.b Statistically significant at P < .05.
Variablea All Transferred Patients (n = 194)
Not Treated (n = 106)
Treated (n = 88)
P valueb
Age, mean (SD), y 67.3 (14.0) 66.8 (13.9) 67.8 (14.2) .850
Age >80 y 42 (21.9%) 18 (17.3%) 24 (27.3%) .100
Helicopter transfer 67 (34.9%) 46 (44.2%) 21 (23.9%) .003
Intravenous thrombolysis given 140 (72.9%) 73 (70.2%) 67 (76.1%) .360
NIHSS score <10 10-20 >20Mean (SD)
16 (8.3%)98 (51.0%)78 (40.6%)18.8 (6.2)
14 (13.5%)53 (51.0%)37 (35.6%)17.5 (6.8)
2 (2.3%)45 (51.1%)41 (46.6%)20.5 (4.8)
.010 .0005
Telestroke video used 94 (49.0%) 53 (51.0%) 41 (46.6%) .550
Time of transfer call 7 pm to 7 am 69 (35.9%) 33 (31.7%) 36 (40.9%) .190
Arrival within 5 hours 136 (70.8%) 63 (60.6%) 73 (83.0%) <.001
Referred from primary stroke center 154 (80.2%) 81 (77.9%) 73 (83.0%) .380
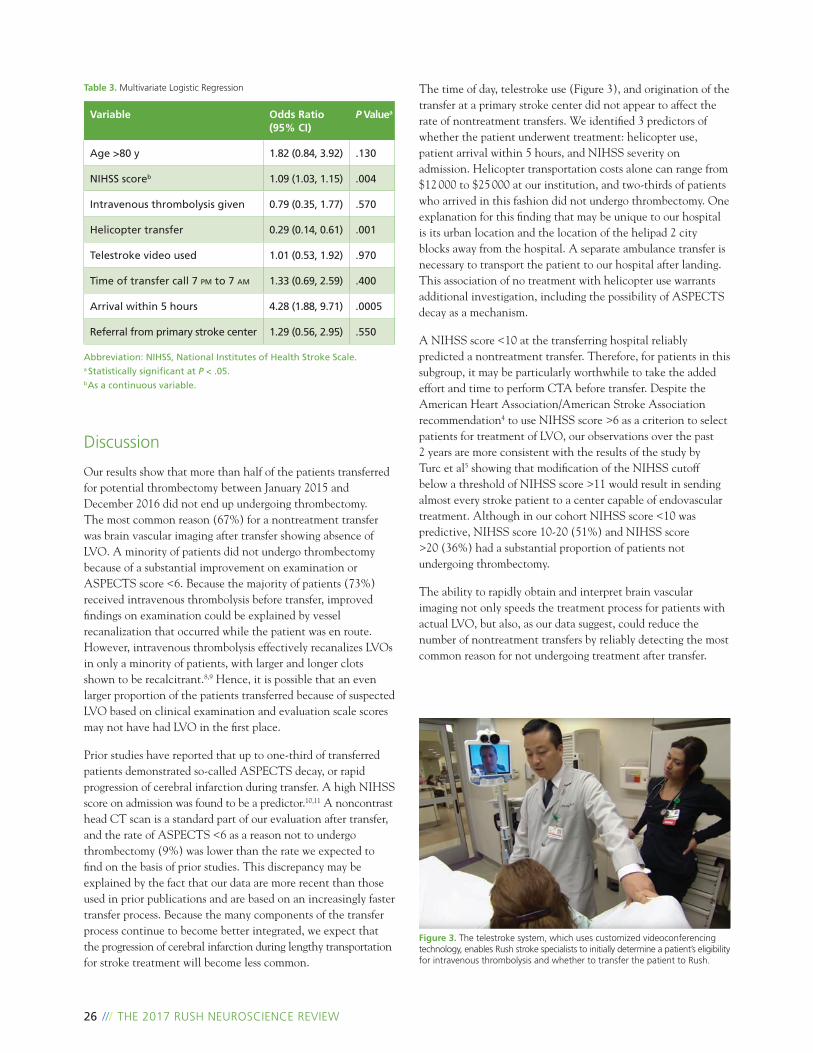
26 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Discussion
Our results show that more than half of the patients transferred for potential thrombectomy between January 2015 and December 2016 did not end up undergoing thrombectomy. The most common reason (67%) for a nontreatment transfer was brain vascular imaging after transfer showing absence of LVO. A minority of patients did not undergo thrombectomy because of a substantial improvement on examination or ASPECTS score <6. Because the majority of patients (73%) received intravenous thrombolysis before transfer, improved findings on examination could be explained by vessel recanalization that occurred while the patient was en route. However, intravenous thrombolysis effectively recanalizes LVOs in only a minority of patients, with larger and longer clots shown to be recalcitrant.8,9 Hence, it is possible that an even larger proportion of the patients transferred because of suspected LVO based on clinical examination and evaluation scale scores may not have had LVO in the first place.
Prior studies have reported that up to one-third of transferred patients demonstrated so-called ASPECTS decay, or rapid progression of cerebral infarction during transfer. A high NIHSS score on admission was found to be a predictor.10,11 A noncontrast head CT scan is a standard part of our evaluation after transfer, and the rate of ASPECTS <6 as a reason not to undergo thrombectomy (9%) was lower than the rate we expected to find on the basis of prior studies. This discrepancy may be explained by the fact that our data are more recent than those used in prior publications and are based on an increasingly faster transfer process. Because the many components of the transfer process continue to become better integrated, we expect that the progression of cerebral infarction during lengthy transportation for stroke treatment will become less common.
The time of day, telestroke use (Figure 3), and origination of the transfer at a primary stroke center did not appear to affect the rate of nontreatment transfers. We identified 3 predictors of whether the patient underwent treatment: helicopter use, patient arrival within 5 hours, and NIHSS severity on admission. Helicopter transportation costs alone can range from $12 000 to $25 000 at our institution, and two-thirds of patients who arrived in this fashion did not undergo thrombectomy. One explanation for this finding that may be unique to our hospital is its urban location and the location of the helipad 2 city blocks away from the hospital. A separate ambulance transfer is necessary to transport the patient to our hospital after landing. This association of no treatment with helicopter use warrants additional investigation, including the possibility of ASPECTS decay as a mechanism.
A NIHSS score <10 at the transferring hospital reliably predicted a nontreatment transfer. Therefore, for patients in this subgroup, it may be particularly worthwhile to take the added effort and time to perform CTA before transfer. Despite the American Heart Association/American Stroke Association recommendation4 to use NIHSS score >6 as a criterion to select patients for treatment of LVO, our observations over the past 2 years are more consistent with the results of the study by Turc et al5 showing that modification of the NIHSS cutoff below a threshold of NIHSS score >11 would result in sending almost every stroke patient to a center capable of endovascular treatment. Although in our cohort NIHSS score <10 was predictive, NIHSS score 10-20 (51%) and NIHSS score >20 (36%) had a substantial proportion of patients not undergoing thrombectomy.
The ability to rapidly obtain and interpret brain vascular imaging not only speeds the treatment process for patients with actual LVO, but also, as our data suggest, could reduce the number of nontreatment transfers by reliably detecting the most common reason for not undergoing treatment after transfer.
Table 3. Multivariate Logistic Regression
Abbreviation: NIHSS, National Institutes of Health Stroke Scale.a Statistically significant at P < .05.b As a continuous variable.
Variable Odds Ratio (95% CI)
P Valuea
Age >80 y 1.82 (0.84, 3.92) .130
NIHSS scoreb 1.09 (1.03, 1.15) .004
Intravenous thrombolysis given 0.79 (0.35, 1.77) .570
Helicopter transfer 0.29 (0.14, 0.61) .001
Telestroke video used 1.01 (0.53, 1.92) .970
Time of transfer call 7 pm to 7 am 1.33 (0.69, 2.59) .400
Arrival within 5 hours 4.28 (1.88, 9.71) .0005
Referral from primary stroke center 1.29 (0.56, 2.95) .550
Figure 3. The telestroke system, which uses customized videoconferencing technology, enables Rush stroke specialists to initially determine a patient’s eligibility for intravenous thrombolysis and whether to transfer the patient to Rush.

Predictors of False-Positive Stroke Thrombectomy Transfers /// 27
One concern related to performing CTA at the transferring hospital is the unpredictability of acquisition and interpretation of the images. Liang et al12 investigated the feasibility of outreach efforts to improve the performance of transferring hospitals in rapidly obtaining CTA prior to transfer. After their efforts, among 57 consecutive transfers, the time from stroke onset to groin puncture was similar regardless of whether CTA was done at the transferring hospital or at the hospital capable of endovascular treatment.
Having the expertise available at the transferring hospital to interpret CTA images immediately after acquisition can be a challenge. Particularly for images that can be automatically and immediately uploaded, the use of telestroke technology may allow for rapid interpretation of CTA images by the receiving hospital before the decision is made to transfer the patient. Anecdotally, to save time, some stroke neurologists at our hospital have asked the physician at the transferring hospital to take HIPAA-compliant mobile phone videos or snapshots of the CTA as the images are being acquired. The ability of stroke neurologists to reliably and accurately interpret CTA images to detect LVO is therefore obviously critical in this time-sensitive process that demands instant availability. A study by Bar et al13 validated this practice by finding strong interrater agreement in CTA evaluation for occlusion in 75 acute stroke patients between stroke neurologists and neuroradiologists. Their study provides data to support practices that are likely already in place to improve triage efficiencies.13
Another consideration related to evaluation of the necessity of transfer is that the transfer of patients with LVOs to a comprehensive stroke center may have benefits for the patient in addition to thrombectomy. Advanced neurocritical and neurosurgical care may not be available at the transferring hospital, potentially justifying the transfer. However, because 67% of transferred patients in our study were found not to have LVO, our data suggest that these patients may in fact be effectively managed without advanced neurocritical and/or neurosurgical care.
A limitation of our study consists of the variability in clinical examination methods to determine stroke severity. Among the 5 stroke neurologists involved in the transfer decision process over the past 2 years, there was no uniform agreement on which clinical scale to use or what cutoff to use as a screen for LVO. It is possible that the use of standardized criteria would have yielded a lower number of nontreatment transfers. However, approximately half of the transfers did not involve the use of telestroke technology, and it may be challenging to achieve an accurate, consistent neurologic assessment in consultation with an emergency physician over the telephone, often in the middle of the night. Additional limitations include the limited perspective from a single center’s experience. The sample size is of course limited, but reflects actual experience over 2 years at an urban tertiary care comprehensive stroke center.
Conclusion
Stroke centers capable of endovascular treatment should reconsider their usual practice of accepting a substantial rate of overdiagnosis in stroke patients considered potential candidates for thrombolysis prior to transfer. Overdiagnosis in this fashion is costly, and our data suggest that the rate of unnecessary transfer may be effectively minimized by obtaining brain CTA before transfer. These findings justify efforts to develop and potentially mandate workflows at the more than 1000 primary stroke centers in the United States that would enable physicians at these facilities to quickly acquire and interpret brain CTA images to efficiently and accurately diagnose LVO as early as possible. If such efforts can be realized, much like other workflow goals that have been mandated for delivery of intravenous thrombolysis, improved diagnostic accuracy could be obtained while minimizing both elapsed time and the costs associated with unnecessary transfers. Our data suggest that the use of clinical scales, particularly the identification of patients with NIHSS score <10, who are likely to undergo unnecessary transfer for thrombectomy, can help to avoid unnecessary transfers that could be obviated by performing CTA prior to transfer.
Acknowledgments: Renata Costa assisted with data collection.
Competing Interests: Michael Chen, MD, is a consultant for General Electric, Genentech, Penumbra, Stryker, and Medtronic. None of the other authors have competing interests.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship Statement: All listed authors (J.Y., D.Z., B.O., J.C., R.D., and M.C.) contributed to the design, data collection, data analysis, and drafting of the manuscript.
Data Sharing: The authors agree to share any data on request.
28 /// THE 2017 RUSH NEUROSCIENCE REVIEW
References1. Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372(1):11-20.
2. Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11):1009-1018.
3. Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019-1030.
4. Powers WJ, Derdeyn CP, Biller J, et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(10):3020-3035.
5. Turc G, Maier B, Naggara O, et al. Clinical scales do not reliably identify acute ischemic stroke patients with large-artery occlusion. Stroke. 2016;47(6):1466-1472.
6. Chen M. Cost-effectiveness of endovascular therapy for acute ischemic stroke. Neurology. 2012;79(13)(suppl 1):S16-S21.
7. Sonig A, Lin N, Krishna C, et al. Impact of transfer status on hospitalization cost and discharge disposition for acute ischemic stroke across the US. J Neurosurg. 2016;124(5):1228-1237.
8. Bhatia R, Hill MD, Shobha N, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action. Stroke. 2010;41(10):2254-2258.
9. Riedel CH, Zimmermann P, Jensen-Kondering U, Stingele R, Deuschl G, Jansen O. The importance of size: successful recanalization by intravenous thrombolysis in acute anterior stroke depends on thrombus length. Stroke. 2011;42(6):1775-1777.
10. Mokin M, Gupta R, Guerrero WR, Rose DZ, Burgin WS, Sivakanthan S. ASPECTS decay during inter-facility transfer in patients with large vessel occlusion strokes. J Neurointerv Surg. 2017;9(5):442-444.
11. Sun CH, Connelly K, Nogueira RG, et al. ASPECTS decay during inter-facility transfer predicts patient outcomes in endovascular reperfusion for ischemic stroke: a unique assessment of dynamic physiologic change over time. J Neurointerv Surg. 2015;7(1):22-26.
12. Liang JW, Stein L, Wilson N, Fifi JT, Tuhrim S, Dhamoon MS. Timing of vessel imaging for suspected large vessel occlusions does not affect groin puncture time in transfer patients with stroke [published online January 24, 2017]. J Neurointerv Surg. doi:10.1136/neurintsurg-2016-012854
13. Bar M, Kral J, Jonszta T, Marcian V, Kuliha M, Mikulik R. Interrater variability for CT angiography evaluation between neurologists and neuroradiologist in acute stroke patients. Br J Radiol. 2017;90(1071):20160670. //

Dramatic Reductions in Spine Surgery Infection Rates /// 29
Author Affiliation: Department of Neurological Surgery, Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Harel Deutsch, MD, Department of Neurological Surgery, Rush University Medical Center, 1725 W Harrison St, Suite 855, Chicago, IL 60612 ([email protected]).
Introduction
Infection remains one of the most common complications related to spine surgery (Figure 1). A postoperative infection may result in substantial increased cost to the procedure and can also result in significant worsening of overall patient outcomes. In a large review of 108 419 spine cases published in 2011, investigators found an overall 2.1% infection rate.1 Factors associated with increased rate of infection were revision surgery (P < .001), spinal fusion (P < .001), and the use of spinal implants (P < .001). Minimally invasive surgery was found to have lower infection rates, with 0.4% for minimally invasive lumbar diskectomies and 2.9% for minimally invasive interbody fusion surgeries.1
Recent introduction of the application of vancomycin powder has been suggested to decrease the incidence of spine infections. Chotai et al showed in 2017 that the use of intraoperative vancomycin was associated with significantly lower infection rates (1.6% [20 of 1215 patients] with vancomycin vs 2.5% [40 of 1587 patients] without vancomycin; P = .02).2 Other investigators have also found a reduction in surgical site infections (SSIs) with the use of vancomycin powder. Ghobrial et al published a review of the literature and found no evidence of adverse effects of vancomycin use in lumbar spine surgery.3 They found mean infection rates among the control patients and vancomycin-treated patients of 7.47% and 1.36%, respectively.3
At Rush University Medical Center, surgeons have adopted the use of vancomycin powder over the past 2 years. Encouraged by early data that showed decreased infection rates with vancomycin powder, more surgeons included the use of vancomycin powder
in their procedures, especially during those that pose a higher risk of postoperative infection. Vancomycin powder was used exclusively in spinal procedures and was not used in cranial procedures. The purpose of the study was to compare the infection rates after cranial procedures and spinal procedures to determine whether the use of vancomycin powder resulted in decreased spine surgery infection rates.
DRAMATIC REDUCTIONS IN SPINE SURGERY INFECTION RATES
Harel Deutsch, MD
Figure 1. Despite the increase in minimally invasive spine procedures in recent years, infection remains the most common complications related to spine surgery.

30 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Methods
This retrospective review examined morbidity and mortality data of all patients who underwent neurological surgery at our institution from 2010 to 2016. Data collected included prior infection, organism, and surgery type. Overall numbers and types of procedures performed in each year were obtained from neurosurgery department records. Endovascular procedures were excluded from cranial procedures in the computation of cranial infection rates. In the review of spinal procedures, lumbar microdiskectomies and anterior cervical diskectomies were excluded because they had extremely low infection rates and their overall numbers skewed the data for spinal procedures. The numbers of gram-negative and gram-positive infections were also tallied for each of the years.
Results
Infection rates after both cranial and spinal procedures have decreased over the years. There has been a notable greater decrease in the infection rates for spinal procedures than for cranial procedures over the period of the study. Figure 2 shows the overall infection rates for cranial and spinal procedures in 2011 to 2016. We were not able to calculate infection rates for 2010 because the numbers and types of cases were not available for that year. The infection rates for spinal procedures and cranial procedures have converged. The number of gram-negative infections has remained essentially unchanged from 2010 to 2016 for both cranial and spinal procedures, albeit at low levels. The number of gram-positive infections decreased by a greater amount for the spinal procedures than for the cranial procedures. Figure 3 shows the number of gram-positive bacterial infections from 2010 to 2016 for both cranial and spinal procedures, and Figure 4 shows the number of gram-negative bacterial infections over the same period.
Discussion
Infections are well-known complications of all surgical interventions. The occurrence of SSIs prolongs hospitalization and increases costs. SSIs can also cause disability and worsened overall outcome for patients (Figure 5). Badia et al4 found in a meta-analysis of European hospitals that the cost of the treatment of a patient with SSI is almost 3 times as high as that of other patients. Hospital stays were 2.3 times greater in patients who had SSIs, compared with other patients. Half of neurosurgery patients who had SSIs required reoperation. Schweizer et al5 found that patients with SSIs in the Veterans
Figure 2. Spine and cranial surgery infection rates over time. Error bars indicate 95% CIs.
0
2
4
6
8
10
2011 2012 2013 2014 2015 2016
Infe
ctio
n r
ate
(%)
Year
Spinal Cranial
Figure 3. Gram-positive bacterial infections in spine and cranial cases over time. Error bars indicate 95% CIs.
2010 2011 2012 2013 2014 2015 20160
2
4
6
8
10
12
14
No
. of
gra
m-p
osi
tive
in
fect
ion
s
Year
Spinal Cranial
Figure 4. Gram-negative bacterial infections in spine and cranial cases over time. Error bars indicate 95% CIs.
2010 2011 2012 2013 2014 2015 20160
1
2
3
No
. of
gra
m-n
egat
ive
infe
ctio
ns
Year
Spinal Cranial

Dramatic Reductions in Spine Surgery Infection Rates /// 31
Affairs hospital system incurred costs up to 1.93 times greater than those of other patients. Patients who had SSIs after undergoing neurosurgery had the greatest cost burden, compared with patients who had SSIs after other types of surgery.
Our data show an overall decrease in SSIs at our institution over time but a greater decrease in the number of SSIs attributable to spine surgery, compared with cranial surgery. The decrease in spine surgery SSIs may be attributable to several general trends in spine surgery. Minimally invasive spine surgery has been correlated with a decreased rate of SSIs after spine surgery.1 Some spinal procedures, such as anterior cervical diskectomies or lateral interbody fusion surgeries, may have a decreased incidence of infection; thus a general shift to those procedures may also be responsible for the decreased rate of infection. On the other hand, the increased use of spine instrumentation (Figure 6) would be expected to result in increased infection rates related to spine surgery.
The utilization of intraoperative vancomycin powder in spine surgeries has been shown recently to decrease the rate of SSIs.6 Surgeons adopted the use of intraoperative vancomycin early, before studies conclusively showed its effectiveness, and subsequent data have shown a substantial decrease in SSIs with the use of vancomycin powder.6 The infection rates in spinal procedures in this study are consistent with the new infection rates documented in other studies of 1%-2%,2 which are an improvement over prior studies showing a 3%-5% infection rate.1 Our data show a substantial decline in gram-positive bacterial infections, while the rate of gram-negative infections has remained relatively constant, which is consistent with the effect we would expect to see with vancomycin powder.
Conclusions
Neurosurgical infection rates have decreased over time, both at our institution and in other studies. The dramatic reduction in the rate of SSI after spine surgery at our institution is likely attributable to the use of intraoperative vancomycin powder in spine surgical procedures.
Disclosures: Dr Deutsch receives consulting royalties from RTI Surgical Inc.
Figure 6. Illustration depicting lumbar spine instrumentation.Figure 5. Photograph of a lumbar wound infection showing localized wound erythema and drainage.
32 /// THE 2017 RUSH NEUROSCIENCE REVIEW
References1. Smith JS, Shaffrey CI, Sansur CA, et al; Scoliosis Research Society Morbidity and Mortality Committee. Rates of infection after spine surgery based on 108,419 procedures: a report from the Scoliosis Research Society Morbidity and Mortality Committee. Spine (Phila Pa 1976). 2011;36(7):556-563.
2. Chotai S, Wright PW, Hale AT, et al. Does intrawound vancomycin application during spine surgery create vancomycin-resistant organism? Neurosurgery. 2017;80(5):746-753.
3. Ghobrial GM, Cadotte DW, Williams K Jr, Fehlings MG, Harrop JS. Complications from the use of intrawound vancomycin in lumbar spinal surgery: a systematic review. Neurosurg Focus. 2015;39(4):E11.
4. Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. 2017;96(1):1-15.
5. Schweizer ML, Cullen JJ, Perencevich EN, Vaughan Sarrazin MS. Costs associated with surgical site infections in Veterans Affairs hospitals. JAMA Surg. 2014;149(6):575-581.
6. Hey HW, Thiam DW, Koh ZS, et al. Is intraoperative local vancomycin powder the answer to surgical site infections in spine surgery? Spine (Phila Pa 1976). 2017;42(4):267-274. //
Moving Pictures and Moving Targets in the Care of Patients With Movement Disorders /// 33
Author Affiliation: Parkinson’s Disease and Movement Disorders Program, Department of Neurological Sciences, Rush University Medical Center, Chicago, Illinois.
Corresponding Author: Jennifer G. Goldman, MD, MS, Rush University Medical Center, 1725 W Harrison St, Suite 755, Chicago, IL 60612 ([email protected]).
Introduction
In the field of movement disorders, many clinical and research advances have been made over the years. These advances include pivotal clinical treatments, such as the use of levodopa, deep brain stimulation, infusion pumps for the management of Parkinson’s disease, and the use of botulinum toxin for the management of dystonia. Other advances include the identification of specific genes linked to Huntington’s disease, Parkinson’s disease, dystonia, spinocerebellar ataxia, and other disorders. However, our quest for a cure for these movement disorders remains unfulfilled, and we are continuing to search for sensitive and specific biomarkers (eg, blood tests, imaging, and other clinical markers) to help clinicians render more accurate diagnoses and provide important prognostic information for patients and families. Thus, a large part of the evaluation of a patient’s movement disorder symptoms continues to be based on the patient’s history and clinical examination, which shows demonstrable, visible signs of involuntary or abnormal movements. Indeed, the keen observation of patients’ symptoms led the
physician James Parkinson to write his famous “Essay on the Shaking Palsy” in 1817, exactly 200 years ago.1 Thus, the recognition of visual cues (or phenomenology) of movement disorders and their documentation by videography play important historical and current roles in the field of movement disorders. In this article, we highlight advances in movement disorder videography, its use in clinical care and education, and video techniques and protocols developed at the Parkinson’s Disease and Movement Disorders Program at Rush University Medical Center (Figure 1).
The ever-growing field of technology has brought not only advances in movement disorder videography, but also novel ways to measure and quantify involuntary or abnormal movements. A wide array of wearable devices, sensors, and monitoring devices is now available, and others are under development. These technologies can offer the clinician a glimpse into the patient’s symptoms outside of the clinic setting
MOVING PICTURES AND MOVING TARGETS IN THE CARE OF PATIENTS WITH MOVEMENT DISORDERS
Jennifer G. Goldman, MD, MS // Brandon R. Barton, MD, MS // Gian D. Pal, MD, MS
Figure 1. The Rush Parkinson’s Disease and Movement Disorders Program has a large staff who work together to fulfill the clinical, research, and educational missions of the group.

34 /// THE 2017 RUSH NEUROSCIENCE REVIEW
and on a more continuous and objective basis. In addition, technology has driven changes in our delivery of care services to patients and the education and support that we give them. The Parkinson’s Disease and Movement Disorders Program provides care for several thousand patients with movement disorders each year, with patients coming to Rush University Medical Center from near and far. We continuously strive to offer accessible and efficient services to patients and their families, with programs ranging from comprehensive on-site clinics and in-person support groups to our telemedicine services and virtual education and support groups (Figure 2). Our novel telehealth programs extend our reach well outside of the Rush University Medical Center setting.
Videography: Pictures Are Worth a Thousand Clinic Notes
Movement disorder neurology as a subspecialty focuses on patients with many kinds of abnormal movements, including Parkinson’s disease, other parkinsonian syndromes, choreas, tics, tremors, dystonia, and myoclonus. It is an inherently visual subspecialty wherein the type of movement, its distribution, and its effect on activities or rest are the most important elements
that lead to accurate diagnosis. Since the 19th century, visual documentation has been the technological anchor of movement disorder patient care and research.2
No words in a clinic chart can convey more useful information than that obtained by direct visualization of the patient. Videography or video recordings help to document the type of movements, their anatomic distributions, their effect on standard activities of daily living, and the response to treatment. Video recordings provide a visual document that the clinician can review and discuss with peers. The most important overall effect of careful video recording is improved patient care.
Table 1. Key Elements of Any Video Protocol
Position or Movement Phenomenology to Observe
Seated at rest Parkinsonian rest tremor, hyperkinetic disorders (chorea, ataxia, dystonia)
Standing Parkinsonian posture, ataxic stance, dystonic posturing
Rapid movements of the limbs (finger tapping, hand opening, foot stomping)
Action dystonia, tremors, bradykinesia, ataxia, myoclonus
Speech Dysarthria, hypophonia, tremor, dysphonia
Eye movements Supranuclear ophthalmoplegia, square wave jerks, saccadic pursuit, ataxic saccades
Limbs sustained against gravity Tremor, myoclonus
Gait: forward, backward, tandem Parkinsonism, dystonia, ataxia, gait disorders
Coordination: finger to nose, heel to shin Ataxia, tremor
Figure 2. Neurologist Jennifer G. Goldman, MD, MS, shown here with her neuroimaging research, uses technology to educate patients with Parkinson’s disease and their caregivers about the neuropsychiatric features of the disease.

Moving Pictures and Moving Targets in the Care of Patients With Movement Disorders /// 35
Additionally, video recordings can be used as teaching tools tohelp educate health professionals to properly rate the severity of a given disorder. Unique or informative videos may be published in academic journals or textbooks. Historical videos can help researchers understand disorders that are rare or have become obsolete (such as kuru). Video-recorded case presentations of patients serve as a core of educational presentations at movement disorder teaching conferences and are invaluable for learning the common and rare manifestations of each disorder.
Despite the importance of video recording to the field of movement disorders, no standardized protocols for the video recording of movement disorder patients have been developed. Because patient video recordings enable progress in the study of movement disorders, allowing for better global efforts to diagnose, treat, and research both rare and common conditions, standardization of the approach to video recording should be an essential part of improving this effort. Internal consistency is important when health care providers film a patient at multiple times because inconsistencies in video recording can make it difficult to compare the same examination longitudinally or to compare the outcomes of different treatments.3-5 Although many considerations affect the movements that patients should perform on video, certain common features should be observed in every video (Table 1).
Each type of movement disorder requires a different approach in order to capture the key elements of the disorder. Different scenarios and different patients can also necessitate variation in video-recording techniques. Although the challenges of video
recording are several, the Rush University Medical Center movement disorders group has mastered these techniques over many years of experience in evaluating patients with movement disorders and with the practice of regularly filming patients as part of their office visits. The physicians in our practice have often been asked by local, national, and international colleagues to share our filming strategies. For this reason, the book Video Protocols and Techniques for Movement Disorders, by Brandon R. Barton, MD, MS, and Deborah A. Hall, MD, PhD, shares our experience in movement disorder videography.6 The publication covers technical issues of filming (space, lighting, and equipment), rating scales, and medical decisions regarding
exactly what to film and how to capture the essential features of a given patient’s disorder6 (Figure 3). For each disorder, the publication gives a suggestion on where to focus the camera, followed by specific tasks that can be done when focusing on that body area. It offers examples chosen from our practice that represent the real-world, practical application of video recording in practice. The reader can learn a great deal by observing how experienced videographers efficiently and politely carry out the protocols.
Ultimately, videotaping allows physicians to improve their ability to observe, a critical skill, as Jean-Martin Charcot noted in 1888: “Let someone say of a doctor that he really knows his physiology or anatomy, that he is dynamic—these are not real compliments; but if you say that he is an observer, a man who knows how to see, this perhaps the greatest compliment one can make.”7
Telemedicine: The Future of Patient Interactions
Telemedicine—the delivery of health care using internet-based communication—has been discussed for years, and now technological advances and lower internet costs have made this service a reality.8 Many patients have been willing to travel long distances to be treated by health care providers including specialists, such as in our clinic. However, visits to the clinic may carry a substantial burden for patients and their families. Such factors include travel time, expenses (eg, gas, time off from
Figure 3. The Rush Parkinson’s Disease and Movement Disorders Program has a dedicated video room to create patient-specific video recordings. For every patient, the video recording serves as a visual document to accompany the written chart. The videos can be used for clinical, research, or educational purposes (with appropriate consent).

36 /// THE 2017 RUSH NEUROSCIENCE REVIEW
work, parking), and fatigue of making a long journey, especially for patients with impaired mobility and advanced disease. The availability of telemedicine has had an immediate effect on this burden because telemedicine appointments avoid the need for the patient to travel outside of the home.
Movement disorders are particularly well-suited for telemedicine because the diagnosis and monitoring of the progression of disorders such as Parkinson’s disease is based almost entirely on visual observation. Nearly 10 years ago, Rush University Medical Center’s Christopher G. Goetz, MD, and colleagues helped establish and test the visual criteria used to assess Parkinson’s disease in the home setting.9 Furthermore, the features of Parkinson’s disease and treatment decisions are largely based on visual information about the patient’s function. As discussed above, physicians at Rush have been using videography for decades to track progression of the disease. Therefore, features such as worsening of tremor, changes in gait, or bradykinesia can be accurately assessed via telemedicine from a patient’s home in real time.
In the past year, the movement disorders program at Rush has successfully piloted a telemedicine program that allows clinicians to deliver expert care to patients while they are in the comfort of their own home (Figure 4). More than 20 patients
have enrolled in the pilot project, and both patients and physicians have expressed a high degree of satisfaction. Rather than signing in at the front desk of the clinic, patients sign in to MyChart, a patient portal that provides a secure video feed using a standard webcam. After that, the flow of the appointment mirrors that of the typical appointment. Because insurance companies are not currently covering telemedicine visits, enrollment in this pilot program has been offered free of charge for patients. Patient feedback has been very positive (Figure 5). Though some health care organizations have not yet developed telehealth capabilities, Rush is preparing proactively for the widespread implementation of telemedicine because this technology is readily available and offers a substantial opportunity to deliver expert health care remotely to an expanded patient population. Illinois is expected to join approximately half of the states that currently require private insurers to cover telehealth services the same as in-person services.10,11 When this technology is formally approved for private insurance payment, the movement disorders program at Rush will be ready.
Additionally, Rush is paving the way for the study and use of telemedicine in other movement disorders besides Parkinson’s disease. Avram Fraint, MD, a movement disorders fellow at Rush, received a grant from the Dystonia Medical Research
Figure 4. In the past year, the movement disorders program at Rush has successfully piloted a telemedicine program that gives patients the option of conducting follow-up visits remotely after initially seeing a movement disorders specialist on the Rush campus.

Foundation to study the utility of telemedicine in patients with cervical dystonia under the mentorship of Cynthia L. Comella, MD, and Gian D. Pal, MD, MS. This study will determine the feasibility of using telemedicine to evaluate patients with cervical dystonia, the reliability of a cervical dystonia rating scale in telemedicine visits, and patient and clinician satisfaction with telemedicine compared with standard clinical visits. Such studies will be important in establishing telemedicine as an acceptable alternative to standard clinical care.
Education and Support: Targeting a Wider Audience
Technology-based tools have tremendous potential not only for clinical care, but also for education and research. From an education standpoint, technology-based solutions can support the education and training of health care professionals, patients, and caregivers. To this end, with a grant from the National Parkinson Foundation, Jennifer G. Goldman, MD, MS, is using technology as a platform to deliver education and support group programs virtually to patients with Parkinson’s disease and their caregivers. The program also compares the standard model of live, in-person education and support group sessions to those sessions held online. This program specifically focuses on the neuropsychiatric features of Parkinson’s disease, an area in which there is a great unmet need for education and support for Parkinson’s disease patients and caregivers. Cognitive, behavioral, and emotional features, despite their frequency in patients with Parkinson’s disease, are underreported by patients and caregivers and underrecognized by health care providers. Through this novel program, patients and caregivers have access to educational talks by Parkinson’s disease experts followed by online, virtual support groups and discussions with our nurse,
neuropsychologist, and social worker. These sessions offer patients and caregivers a way to interact with our experts and other attendees in a format that can be conveniently accessed online from one’s home. With this type of technology-based program, we will be able to provide education, support, and resources to a broad community of people with Parkinson’s disease and reach well beyond the walls of our hospital.
Conclusion
Technology holds great promise for the future of patients with movement disorders by providing improved diagnostics and therapeutics as well as enhanced access to care and support. Videography contributes greatly to our patient care and educational efforts, merging the legacy of our field and the importance of acute observational skills with innovative tools that improve accessibility and communication. Telehealth delivery systems will enhance our ability to provide clinical care, research, and educational opportunities to patients who do not have access to a specialist, patients who live far away, and patients who cannot travel to the office setting. In keeping with our center’s three-part mission of excellence in patient care, research, and education, the movement disorders program at Rush University Medical Center is paving the way for crucial improvements in how patients experience health care, research, and education in the near future and beyond.
Moving Pictures and Moving Targets in the Care of Patients With Movement Disorders /// 37
0 2 4 6 8 10
Figure 5. Patient satisfaction with the telemedicine program is high, as is shown in this bar graph depicting results of a patient satisfaction questionnaire, adapted from a study of telemedicine outcomes by Ryan Hansen, MD, and Christopher G. Goetz, MD. Responses are on a Likert scale, with 1 indicating “highly disagree” and 10 indicating “highly agree.” The top bar represents the median of the medians on all satisfaction subdomain items of the questionnaire. The remaining bars show the medians of other selected subdomain items. Response ranges are given in parentheses.
All satisfaction-related items
Favor future telemedicine visits
Pleased with outcome of visit
Prefer future appointments by telemedicine
Median (response range)
9.5 (5-10)
9.0 (7-10)
10.0 (6-10)
8.0 (7-10)
38 /// THE 2017 RUSH NEUROSCIENCE REVIEW
References1. Parkinson J. An Essay on the Shaking Palsy. London: Whittingham and Rowland for Sherwood, Neely, and Jones; 1817.
2. Barboi AC, Goetz CG, Musetoiu R. The origins of scientific cinematography and early medical applications. Neurology. 2004;62(11):2082-2086.
3. de Leon D, Moskowitz CB, Stewart C. Proposed guidelines for videotaping individuals with movement disorders. J Neurosci Nurs. 1991;23(3):191-193.
4. Duker AP. Video recording in movement disorders: practical issues. Continuum (Minneap Minn). 2013;19(5):1401-1405.
5. Jog MS, Grantier L. Methods for digital video recording, storage, and communication of movement disorders. Mov Disord. 2001;16(6):1196-1200.
6. Barton BR, Hall DA. Video Protocols and Techniques for Movement Disorders. New York, NY: Oxford University Press; 2015.
7. Charcot JM. L Leçons du mardi à la Salpêtrière, 1887-1888 [Tuesday lessons at the Salpêtrière, 1887-1888]. Paris: Bureaux du Progrès; 1888:281.
8. Achey M, Aldred JL, Aljehani N, et al. The past, present, and future of telemedicine for Parkinson’s disease. Mov Disord. 2014;29(7):871-883.
9. Goetz CG, Leurgans S, Hinson VK, et al. Evaluating Parkinson’s disease patients at home: utility of self-videotaping for objective motor, dyskinesia, and ON-OFF assessments. Mov Disord. 2008;23(10): 1479-1482.
10. Hermar B. Virtual reality: more insurers are embracing telehealth. Mod Healthc. 2016; 46(8):16-19.
11. US Government Accountability Office. Telehealth and Remote Patient Monitoring Use in Medicare and Selected Federal Programs. GAO-17-365. https://www.gao.gov/assets/690/684115.pdf. Published April 2017. Accessed July 27, 2017. //

Publications (2016) /// 39
Abner EL, Nelson PT, Kryscio RJ, Schmitt FA, Fardo DW, Woltjer RL, Cairns NJ, Yu L, Dodge HH, Xiong C, Masaki K, Tyas SL, Bennett DA, Schneider JA, Arvanitakis Z. Diabetes is associated with cerebrovascular but not Alzheimer’s disease neuropathology. Alzheimers Dement. 2016;12(8):882-889.
Adams HH, Hibar DP, Chouraki V, Stein JL, Nyquist PA, Rentería ME, Trompet S, Arias-Vasquez A, Seshadri S, Desrivières S, Beecham AH, Jahanshad N, Wittfeld K, Van der Lee SJ, Abramovic L, Alhusaini S, Amin N, Andersson M, Arfanakis K, Aribisala BS, Armstrong NJ, Athanasiu L, Axelsson T, Beiser A, Bernard M, Bis JC, Blanken LM, Blanton SH, Bohlken MM, Boks MP, Bralten J, Brickman AM, Carmichael O, Chakravarty MM, Chauhan G, Chen Q, Ching CR, Cuellar-Partida G, Braber AD, Doan NT, Ehrlich S, Filippi I, Ge T, Giddaluru S, Goldman AL, Gottesman RF, Greven CU, Grimm O, Griswold ME, Guadalupe T, Hass J, Haukvik UK, Hilal S, Hofer E, Hoehn D, Holmes AJ, Hoogman M, Janowitz D, Jia T, Kasperaviciute D, Kim S, Klein M, Kraemer B, Lee PH, Liao J, Liewald DC, Lopez LM, Luciano M, Macare C, Marquand A, Matarin M, Mather KA, Mattheisen M, Mazoyer B, McKay DR, McWhirter R, Milaneschi Y, Mirza-Schreiber N, Muetzel RL, Maniega SM, Nho K, Nugent AC, Loohuis LM, Oosterlaan J, Papmeyer M, Pappa I, Pirpamer L, Pudas S, Pütz B, Rajan KB, Ramasamy A, Richards JS, Risacher SL, Roiz-Santiañez R, Rommelse N, Rose EJ, Royle NA, Rundek T, Sämann PG, Satizabal CL, Schmaal L, Schork AJ, Shen L, Shin J, Shumskaya E, Smith AV, Sprooten E, Strike LT, Teumer A, Thomson R, Tordesillas-Gutierrez D, Toro R, Trabzuni D, Vaidya D, Van der Grond J, Van der Meer D, Van Donkelaar MM, Van Eijk KR, Van Erp TG, Van Rooij D, Walton E, Westlye LT, Whelan CD, Windham BG, Winkler AM, Woldehawariat G, Wolf C, Wolfers T, Xu B, Yanek LR, Yang J, Zijdenbos A, Zwiers MP, Agartz I, Aggarwal NT, Almasy L, Ames D, Amouyel P, Andreassen OA, Arepalli S, Assareh AA, Barral S, Bastin ME, Becker DM, Becker JT, Bennett DA, Blangero J, van Bokhoven H, Boomsma DI, Brodaty H, Brouwer RM, Brunner HG, Buckner RL, Buitelaar JK, Bulayeva KB, Cahn W, Calhoun VD, Cannon DM, Cavalleri GL, Chen C, Cheng CY, Cichon S, Cookson MR, Corvin A, Crespo-Facorro B, Curran JE, Czisch M, Dale AM, Davies GE, De Geus EJ, De Jager PL, de Zubicaray GI, Delanty N, Depondt C, DeStefano AL, Dillman A, Djurovic S, Donohoe G, Drevets WC, Duggirala R, Dyer TD, Erk S, Espeseth T, Evans DA, Fedko IO, Fernández G, Ferrucci L, Fisher SE, Fleischman DA, Ford I, Foroud TM, Fox PT, Francks C, Fukunaga M, Gibbs JR, Glahn DC, Gollub RL, Göring HH, Grabe HJ, Green RC, Gruber O, Gudnason V, Guelfi S, Hansell NK, Hardy J, Hartman CA, Hashimoto R, Hegenscheid K, Heinz A, Le Hellard S, Hernandez DG, Heslenfeld DJ, Ho BC, Hoekstra PJ, Hoffmann W, Hofman A, Holsboer F, Homuth G, Hosten N, Hottenga JJ, Pol HE, Ikeda M, Ikram MK, Jack CR Jr, Jenkinson M, Johnson R, Jönsson EG, Jukema JW, Kahn RS, Kanai R, Kloszewska I, Knopman DS, Kochunov P, Kwok JB, Lawrie SM, Lemaître H, Liu X, Longo DL, Longstreth WT Jr, Lopez OL, Lovestone S, Martinez O, Martinot JL, Mattay VS, McDonald C, McIntosh AM, McMahon KL, McMahon FJ, Mecocci P, Melle I, Meyer-Lindenberg A, Mohnke S, Montgomery GW, Morris DW, Mosley TH, Mühleisen TW, Müller-Myhsok B, Nalls MA, Nauck M, Nichols TE, Niessen WJ,
Nöthen MM, Nyberg L, Ohi K, Olvera RL, Ophoff RA, Pandolfo M, Paus T, Pausova Z, Penninx BW, Pike GB, Potkin SG, Psaty BM, Reppermund S, Rietschel M, Roffman JL, Romanczuk-Seiferth N, Rotter JI, Ryten M, Sacco RL, Sachdev PS, Saykin AJ, Schmidt R, Schofield PR, Sigurdsson S, Simmons A, Singleton A, Sisodiya SM, Smith C, Smoller JW, Soininen H, Srikanth V, Steen VM, Stott DJ, Sussmann JE, Thalamuthu A, Tiemeier H, Toga AW, Traynor BJ, Troncoso J, Turner JA, Tzourio C, Uitterlinden AG, Hernández MC, Van der Brug M, Van der Lugt A, Van der Wee NJ, Van Duijn CM, Van Haren NE, Van T Ent D, Van Tol MJ, Vardarajan BN, Veltman DJ, Vernooij MW, Völzke H, Walter H, Wardlaw JM, Wassink TH, Weale ME, Weinberger DR, Weiner MW, Wen W, Westman E, White T, Wong TY, Wright CB, Zielke HR, Zonderman AB, Deary IJ, DeCarli C, Schmidt H, Martin NG, De Craen AJ, Wright MJ, Launer LJ, Schumann G, Fornage M, Franke B, Debette S, Medland SE, Ikram MA, Thompson PM. Novel genetic loci underlying human intracranial volume identified through genome-wide association. Nat Neurosci. 2016;19(12):1569-1582.
Adogwa O, Sure DR, LaBagnara M, Shaffrey CI, Fessler RG. Minimally invasive spine surgery and sagittal correction. Neurosurgery. 2016;63(suppl 1):31-36.
Albers GW, Goyal M, Jahan R, Bonafe A, Diener HC, Levy EI, Pereira VM, Cognard C, Cohen DJ, Hacke W, Jansen O, Jovin TG, Mattle HP, Nogueira RG, Siddiqui AH, Yavagal DR, Baxter BW, Devlin TG, Lopes DK, Reddy VK, de Rochemont Rdu M, Singer OC, Bammer R, Saver JL. Ischemic core and hypoperfusion volumes predict infarct size in SWIFT PRIME. Ann Neurol. 2016;79(1):76-89.
Ali YO, Allen HM, Yu L, Li-Kroeger D, Bakhshizadehmahmoudi D, Hatcher A, McCabe C, Xu J, Bjorklund N, Taglialatela G, Bennett DA, De Jager PL, Shulman JM, Bellen HJ, Lu HC. NMNAT2:HSP90 complex mediates proteostasis in proteinopathies. PLoS Biol. 2016;14(6):e1002472.
Allen GI, Amoroso N, Anghel C, Balagurusamy V, Bare CJ, Beaton D, Bellotti R, Bennett DA, Boehme KL, Boutros PC, Caberlotto L, Caloian C, Campbell F, Chaibub Neto E, Chang YC, Chen B, Chen CY, Chien TY, Clark T, Das S, Davatzikos C, Deng J, Dillenberger D, Dobson RJ, Dong Q, Doshi J, Duma D, Errico R, Erus G, Everett E, Fardo DW, Friend SH, Fröhlich H, Gan J, St George-Hyslop P, Ghosh SS, Glaab E, Green RC, Guan Y, Hong MY, Huang C, Hwang J, Ibrahim J, Inglese P, Iyappan A, Jiang Q, Katsumata Y, Kauwe JS, Klein A, Kong D, Krause R, Lalonde E, Lauria M, Lee E, Lin X, Liu Z, Livingstone J, Logsdon BA, Lovestone S, Ma TW, Malhotra A, Mangravite LM, Maxwell TJ, Merrill E, Nagorski J, Namasivayam A, Narayan M, Naz M, Newhouse SJ, Norman TC, Nurtdinov RN, Oyang YJ, Pawitan Y, Peng S, Peters MA, Piccolo SR, Praveen P, Priami C, Sabelnykova VY, Senger P, Shen X, Simmons A, Sotiras A, Stolovitzky G, Tangaro S, Tateo A, Tung YA, Tustison NJ, Varol E, Vradenburg G, Weiner MW, Xiao G, Xie L, Xie Y, Xu J, Yang H, Zhan X, Zhou Y, Zhu F, Zhu H, Zhu S; Alzheimer’s Disease Neuroimaging Initiative. Crowdsourced estimation of cognitive decline and resilience in Alzheimer’s disease. Alzheimers Dement. 2016;12(6):645-653.
Select Publications (2016)
Departments of Neurological Sciences and Neurological Surgery*
* This is a partial list of published works of the neurosciences faculty at Rush University Medical Center (indicated in bold). The departments gratefully acknowledge the coauthorship of students, nurses, practitioners, therapists, residents, fellows, and other colleagues at Rush.
40 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Almefty RO, Kalani MY, Ducruet AF, Crowley RW, McDougall CG, Albuquerque FC. Middle meningeal arteriovenous fistulas: a rare and potentially high-risk dural arteriovenous fistula. Surg Neurol Int. 2016;7(suppl 9):S219-S222.
Ames C, Traynelis VC, Vaccaro AR. Introduction: dynamic stabilization of the spine. Neurosurg Focus. 2016;40(1):E1.
Amitrano D, Silva IR, Liberato BB, Batistella V, Oliveira J, Nascimento OJ. Simple prediction model for unfavorable outcome in ischemic stroke after intravenous thrombolytic therapy. Arq Neuropsiquiatr. 2016;74(12):986-989.
Arfanakis K, Wilson RS, Barth CM, Capuano AW, Vasireddi A, Zhang S, Fleischman DA, Bennett DA. Cognitive activity, cognitive function, and brain diffusion characteristics in old age. Brain Imaging Behav. 2016;10(2):455-463.
Arvanitakis Z, Capuano AW, Leurgans SE, Bennett DA, Schneider JA. Relation of cerebral vessel disease to Alzheimer’s disease dementia and cognitive function in elderly people: a cross-sectional study. Lancet Neurol. 2016;15(9):934-943.
Arvanitakis Z, Fleischman DA, Arfanakis K, Leurgans SE, Barnes LL, Bennett DA. Association of white matter hyperintensities and gray matter volume with cognition in older individuals without cognitive impairment. Brain Struct Funct. 2016;221(4):2135-2146.
Baharnoori M, Lyons J, Dastagir A, Koralnik I, Stankiewicz JM. Nonfatal PML in a patient with multiple sclerosis treated with dimethyl fumarate. Neurol Neuroimmunol Neuroinflamm. 2016;3(5):e274.
Bailey DB Jr, Berry-Kravis E, Wheeler A, Raspa M, Merrien F, Ricart J, Koumaras B, Rosenkranz G, Tomlinson M, von Raison F, Apostol G. Mavoglurant in adolescents with fragile X syndrome: analysis of Clinical Global Impression-Improvement source data from a double-blind therapeutic study followed by an open-label, long-term extension study. J Neurodev Disord. 2016;8:1.
Bakhsheshian J, Khanna R, Choy W, Lawton CD, Nixon AT, Wong AP, Koski TR, Liu JC, Song JK, Dahdaleh NS, Smith ZA, Fessler RG. Incidence of graft extrusion following minimally invasive transforaminal lumbar interbody fusion. J Clin Neurosci. 2016;24:88-93.
Barban N, Jansen R, de Vlaming R, Vaez A, Mandemakers JJ, Tropf FC, Shen X, Wilson JF, Chasman DI, Nolte IM, Tragante V, van der Laan SW, Perry JR, Kong A; BIOS Consortium, Ahluwalia TS, Albrecht E, Yerges-Armstrong L, Atzmon G, Auro K, Ayers K, Bakshi A, Ben-Avraham D, Berger K, Bergman A, Bertram L, Bielak LF, Bjornsdottir G, Bonder MJ, Broer L, Bui M, Barbieri C, Cavadino A, Chavarro JE, Turman C, Concas MP, Cordell HJ, Davies G, Eibich P, Eriksson N, Esko T, Eriksson J, Falahi F, Felix JF, Fontana MA, Franke L, Gandin I, Gaskins AJ, Gieger C, Gunderson EP, Guo X, Hayward C, He C, Hofer E, Huang H, Joshi PK, Kanoni S, Karlsson R, Kiechl S, Kifley A, Kluttig A, Kraft P, Lagou V, Lecoeur C, Lahti J, Li-Gao R, Lind PA, Liu T, Makalic E, Mamasoula C, Matteson L, Mbarek H, McArdle PF, McMahon G, Meddens SF, Mihailov E, Miller M, Missmer SA, Monnereau C, van der Most PJ, Myhre R, Nalls MA, Nutile T, Kalafati IP, Porcu E, Prokopenko I, Rajan KB, Rich-Edwards J, Rietveld CA, Robino A, Rose LM, Rueedi R, Ryan KA, Saba Y, Schmidt D, Smith JA, Stolk L, Streeten E, Tönjes A, Thorleifsson G, Ulivi S, Wedenoja J, Wellmann J, Willeit P, Yao J, Yengo L, Zhao JH, Zhao W, Zhernakova DV, Amin N, Andrews H, Balkau B, Barzilai N, Bergmann S, Biino G, Bisgaard H, Bønnelykke K, Boomsma DI, Buring JE, Campbell H, Cappellani S, Ciullo M,
Cox SR, Cucca F, Toniolo D, Davey-Smith G, Deary IJ, Dedoussis G, Deloukas P, van Duijn CM, de Geus EJ, Eriksson JG, Evans DA, Faul JD, Sala CF, Froguel P, Gasparini P, Girotto G, Grabe HJ, Greiser KH, Groenen PJ, de Haan HG, Haerting J, Harris TB, Heath AC, Heikkilä K, Hofman A, Homuth G, Holliday EG, Hopper J, Hyppönen E, Jacobsson B, Jaddoe VW, Johannesson M, Jugessur A, Kähönen M, Kajantie E, Kardia SL, Keavney B, Kolcic I, Koponen P, Kovacs P, Kronenberg F, Kutalik Z, La Bianca M, Lachance G, Iacono WG, Lai S, Lehtimäki T, Liewald DC, LifeLines Cohort Study, Lindgren CM, Liu Y, Luben R, Lucht M, Luoto R, Magnus P, Magnusson PK, Martin NG, McGue M, McQuillan R, Medland SE, Meisinger C, Mellström D, Metspalu A, Traglia M, Milani L, Mitchell P, Montgomery GW, Mook-Kanamori D, de Mutsert R, Nohr EA, Ohlsson C, Olsen J, Ong KK, Paternoster L, Pattie A, Penninx BW, Perola M, Peyser PA, Pirastu M, Polasek O, Power C, Kaprio J, Raffel LJ, Räikkönen K, Raitakari O, Ridker PM, Ring SM, Roll K, Rudan I, Ruggiero D, Rujescu D, Salomaa V, Schlessinger D, Schmidt H, Schmidt R, Schupf N, Smit J, Sorice R, Spector TD, Starr JM, Stöckl D, Strauch K, Stumvoll M, Swertz MA, Thorsteinsdottir U, Thurik AR, Timpson NJ, Tung JY, Uitterlinden AG, Vaccargiu S, Viikari J, Vitart V, Völzke H, Vollenweider P, Vuckovic D, Waage J, Wagner GG, Wang JJ, Wareham NJ, Weir DR, Willemsen G, Willeit J, Wright AF, Zondervan KT, Stefansson K, Krueger RF, Lee JJ, Benjamin DJ, Cesarini D, Koellinger PD, den Hoed M, Snieder H, Mills MC. Genome-wide analysis identifies 12 loci influencing human reproductive behavior. Nat Genet. 2016;48(12):1462-1472.
Barclay SF, Rand CM, Gray PA, Gibson WT, Wilson RJ, Berry-Kravis EM, Ize-Ludlow D, Bech-Hansen NT, Weese-Mayer DE. Absence of mutations in HCRT, HCRTR1 and HCRTR2 in patients with ROHHAD. Respir Physiol Neurobiol. 2016;221:59-63.
Barnes LL, Yumoto F, Capuano A, Wilson RS, Bennett DA, Tractenberg RE. Examination of the factor structure of a global cognitive function battery across race and time. J Int Neuropsychol Soc. 2016;22(1):66-75.
Barone FC, Gustafson D, Crystal HA, Moreno H, Adamski MG, Arai K, Baird AE, Balucani C, Brickman AM, Cechetto D, Gorelick P, Biessels GJ, Kiliaan A, Launer L, Schneider J, Sorond FA, Whitmer R, Wright C, Zhang ZG. First translational ‘think tank’ on cerebrovascular disease, cognitive impairment and dementia. J Transl Med. 2016;14:50.
Bartolotti N, Bennett DA, Lazarov O. Reduced pCREB in Alzheimer’s disease prefrontal cortex is reflected in peripheral blood mononuclear cells. Mol Psychiatry. 2016;21(9):1158-1166.
Baslet G, Seshadri A, Bermeo-Ovalle A, Willment K, Myers L. Psychogenic non-epileptic seizures: an updated primer. Psychosomatics. 2016;57(1):1-17.
Beach TG, Corbillé AG, Letournel F, Kordower JH, Kremer T, Munoz DG, Intorcia A, Hentz J, Adler CH, Sue LI, Walker J, Serrano G, Derkinderen P. Multicenter assessment of immunohistochemical methods for pathological alpha-synuclein in sigmoid colon of autopsied Parkinson’s disease and control subjects. J Parkinsons Dis. 2016;6(4):761-770.
Beck JS, Mufson EJ, Counts SE. Evidence for mitochondrial UPR gene activation in familial and sporadic Alzheimer’s disease. Curr Alzheimer Res. 2016;13(6):610-614.
Bera S, Kar RK, Mondal S, Pahan K, Bhunia A. Structural elucidation of the cell-penetrating penetratin peptide in model membranes at the atomic level: probing hydrophobic interactions in the blood-brain barrier. Biochemistry. 2016;55(35):4982-4996.
Berk M, Woods RL, Nelson MR, Shah RC, Reid CM, Storey E, Fitzgerald SM, Lockery JE, Wolfe R, Mohebbi M, Murray AM, Kirpach B, Grimm R, McNeil JJ. ASPREE-D: aspirin for the prevention of depression in the elderly. Int Psychogeriatr. 2016;28(10):1741-1748.
Bermeo-Ovalle A. Dietary treatments for epilepsy: why is this so hard for us to swallow? Epilepsy Curr. 2016;16(5):312-313.
Bermeo-Ovalle A. Do we know what we think we know? reconciling subjective complaints and objective cognitive testing in older adults with epilepsy. Epilepsy Curr. 2016;16(4):230-231.
Bermeo-Ovalle A, Bleck T. Status epilepticus in the intensive care unit. Semin Neurol. 2016;36(6):550-559.
Berry-Kravis E. Cognitive trajectories in rare neurogenetic diseases: minding the gaps and filling the potholes. Dev Med Child Neurol. 2016;58(3):221-222.
Berry-Kravis E, Des Portes V, Hagerman R, Jacquemont S, Charles P, Visootsak J, Brinkman M, Rerat K, Koumaras B, Zhu L, Barth GM, Jaecklin T, Apostol G, von Raison F. Mavoglurant in fragile X syndrome: results of two randomized, double-blind, placebo-controlled trials. Sci Transl Med. 2016;8(321):321ra5.
Besser LM, Alosco ML, Ramirez Gomez L, Zhou XH, McKee AC, Stern RA, Gunstad J, Schneider JA, Chui H, Kukull WA. Late-life vascular risk factors and Alzheimer disease neuropathology in individuals with normal cognition. J Neuropathol Exp Neurol. 2016;75(10):955-962.
Bledsoe IO, Comella CL. Botulinum toxin treatment of cervical dystonia. Semin Neurol. 2016;36(1):47-53.
Bloem BR, Marinus J, Almeida Q, Dibble L, Nieuwboer A, Post B, Ruzicka E, Goetz C, Stebbins G, Martinez-Martin P, Schrag A; Movement Disorders Society Rating Scales Committee. Measurement instruments to assess posture, gait, and balance in Parkinson’s disease: critique and recommendations. Mov Disord. 2016;31(9):1342-1355.
Boeve BF, Dickson DW, Duda JE, Ferman TJ, Galasko DR, Galvin JE, Goldman JG, Growdon JH, Hurtig HI, Kaufer DI, Kantarci K, Leverenz JB, Lippa CF, Lopez OL, McKeith IG, Singleton AB, Taylor A, Tsuang D, Weintraub D, Zabetian CP. Arguing against the proposed definition changes of PD. Mov Disord. 2016;31(11):1619-1622.
Boland T, Henderson GV, Gibbons FK, Brouwers HB, Greenberg SM, Raffeld M, Kourkoulis CE, Rosand J, Christopher KB. Hypernatremia at hospital discharge and out of hospital mortality following primary intracerebral hemorrhage. Neurocrit Care. 2016;25(1):110-116.
Boyle PA, Yu L, Fleischman DA, Leurgans S, Yang J, Wilson RS, Schneider JA, Arvanitakis Z, Arfanakis K, Bennett DA. White matter hyperintensities, incident mild cognitive impairment, and cognitive decline in old age. Ann Clin Transl Neurol. 2016;3(10):791-800.
Breslin RP, Franker L, Sterchi S, Sani S. Implementation of an integrated neuroscience unit. AACN Adv Crit Care. 2016;27(1):40-52.
Brinjikji W, Lanzino G, Cloft HJ, Siddiqui AH, Boccardi E, Cekirge S, Fiorella D, Hanel R, Jabbour P, Levy E, Lopes D, Lylyk P, Szikora I, Kallmes DF. Risk factors for ischemic complications following Pipeline Embolization Device treatment of intracranial aneurysms: results from the IntrePED Study. AJNR Am J Neuroradiol. 2016;37(9):1673-1678.
Brody DM, Litvan I, Warner S, Riley DE, Hall DA, Kluger BM, Shprecher DR, Cunningham CR. Relationship between uric acid levels and progressive supranuclear palsy. Mov Disord. 2016;31(5):663-667.
Brooks NP, Potts E, O’Toole J. The impact of guidelines on clinical practice: survey of the use of methylprednisolone for acute spinal cord injury [letter]. Neurosurgery. 2016;79(3):E516-E520.
Brown BL, Lopes D, Miller DA, Tawk RG, Brasiliense LB, Ringer A, Sauvageau E, Powers CJ, Arthur A, Hoit D, Snyder K, Siddiqui A, Levy E, Hopkins LN, Cuellar H, Rodriguez-Mercado R, Veznedaroglu E, Binning M, Mocco J, Aguilar-Salinas P, Boulos A, Yamamoto J, Hanel RA. The fate of cranial neuropathy after flow diversion for carotid aneurysms. J Neurosurg. 2016;124(4):1107-1113.
Brundin P, Ma J, Kordower JH. How strong is the evidence that Parkinson’s disease is a prion disorder? Curr Opin Neurol. 2016;29(4):459-466.
Buchman AS, Leurgans SE, Yu L, Wilson RS, Lim AS, James BD, Shulman JM, Bennett DA. Incident parkinsonism in older adults without Parkinson disease. Neurology. 2016;87(10):1036-1044.
Buchman AS, Wilson RS, Shulman JM, Leurgans SE, Schneider JA, Bennett DA. Parkinsonism in older adults and its association with adverse health outcomes and neuropathology. J Gerontol A Biol Sci Med Sci. 2016;71(4):549-556.
Buchman AS, Wilson RS, Yu L, Boyle PA, Bennett DA, Barnes LL. Motor function is associated with incident disability in older African Americans. J Gerontol A Biol Sci Med Sci. 2016;71(5):696-702.
Buchman AS, Yu L, Boyle PA, Schneider JA, De Jager PL, Bennett DA. Higher brain BDNF gene expression is associated with slower cognitive decline in older adults. Neurology. 2016;86(8):735-741.
Burns TM, Smith GA, Allen JA, Amato AA, Arnold WD, Barohn R, Benatar M, Bird SJ, Bromberg M, Chahin N, Ciafaloni E, Cohen JA, Corse A, Crum BA, David WS, Dimberg E, Sousa EA, Donofrio PD, Dyck PJ, Engel AG, Ensrud ER, Ferrante M, Freimer M, Gable KL, Gibson S, Gilchrist JM, Goldstein JM, Gooch CL, Goodman BP, Gorelov D, Gospe SM Jr, Goyal NA, Guidon AC, Guptill JT, Gutmann L, Gutmann L, Gwathmey K, Harati Y, Harper CM Jr, Hehir MK, Hobson-Webb LD, Howard JF Jr, Jackson CE, Johnson N, Jones SM, Juel VC, Kaminski HJ, Karam C, Kennelly KD, Khella S, Khoury J, Kincaid JC, Kissel JT, Kolb N, Lacomis D, Ladha S, Larriviere D, Lewis RA, Li Y, Litchy WJ, Logigian E, Lou JS, MacGowen DJ, Maselli R, Massey JM, Mauermann ML, Mathews KD, Meriggioli MN, Miller RG, Moon JS, Mozaffar T, Nations SP, Nowak RJ, Ostrow LW, Pascuzzi RM, Peltier A, Ruzhansky K, Richman DP, Ross MA, Rubin DI, Russell JA, Sachs GM, Salajegheh MK, Saperstein DS, Scelsa S, Selcen D, Shaibani A, Shieh PB, Silvestri NJ, Singleton JR, Smith BE, So YT, Solorzano G, Sorenson EJ, Srinivasen J, Tavee J, Tawil R, Thaisetthawatkul P, Thornton C, Trivedi J, Vernino S, Wang AK, Webb TA, Weiss MD, Windebank AJ, Wolfe GI. Editorial by concerned physicians: unintended effect of the orphan drug act on the potential cost of 3,4-diaminopyridine. Muscle Nerve. 2016;53(2):165-168.
Cade BE, Gottlieb DJ, Lauderdale DS, Bennett DA, Buchman AS, Buxbaum SG, De Jager PL, Evans DS, Fülöp T, Gharib SA, Johnson WC, Kim H, Larkin EK, Lee SK, Lim AS, Punjabi NM, Shin C, Stone KL, Tranah GJ, Weng J, Yaffe K, Zee PC, Patel SR, Zhu X, Redline S, Saxena R. Common variants in DRD2 are associated with sleep duration: the CARe consortium. Hum Mol Genet. 2016;25(1):167-179.
Publications (2016) /// 41

Chan G, White CC, Winn PA, Cimpean M, Replogle JM, Glick LR, Cuerdon NE, Ryan KJ, Johnson KA, Schneider JA, Bennett DA, Chibnik LB, Sperling RA, De Jager PL, Bradshaw EM. Trans-pQTL study identifies immune crosstalk between Parkinson and Alzheimer loci. Neurol Genet. 2016;2(4):e90.
Chandra G, Rangasamy SB, Roy A, Kordower JH, Pahan K. Neutralization of RANTES and eotaxin prevents the loss of dopaminergic neurons in a mouse model of Parkinson disease. J Biol Chem. 2016;291(29):15267-15281.
Charnay AJ, Antisdel-Lomaglio JE, Zelko FA, Rand CM, Le M, Gordon SC, Vitez SF, Tse JW, Brogadir CD, Nelson MN, Berry-Kravis EM, Weese-Mayer DE. Congenital central hypoventilation syndrome: neurocognition already reduced in preschool-aged children. Chest. 2016;149(3):809-815.
Chen CJ, Caruso J, Starke RM, Ding D, Buell T, Crowley RW, Liu KC. Endoport-assisted microsurgical treatment of a ruptured periventricular aneurysm. Case Rep Neurol Med. 2016;2016:8654262.
Chen CJ, Moosa S, Ding D, Raper DM, Burke RM, Lee CC, Chivukula S, Wang TR, Starke RM, Crowley RW, Liu KC. Infundibular dilations of the posterior communicating arteries: pathogenesis, anatomical variants, aneurysm formation, and subarachnoid hemorrhage. J Neurointerv Surg. 2016;8(8):791-795.
Chen M. Level 5. J Neurointerv Surg. 2016;8(7):659-660.
Chen M, Mangubat E, Ouyang B. Patient-reported outcome measures for patients with cerebral aneurysms acquired via social media: data from a large nationwide sample. J Neurointerv Surg. 2016;8(1):42-46.
Chouraki V, Reitz C, Maury F, Bis JC, Bellenguez C, Yu L, Jakobsdottir J, Mukherjee S, Adams HH, Choi SH, Larson EB, Fitzpatrick A, Uitterlinden AG, de Jager PL, Hofman A, Gudnason V, Vardarajan B, Ibrahim-Verbaas C, van der Lee SJ, Lopez O, Dartigues JF, Berr C, Amouyel P, Bennett DA, van Duijn C, DeStefano AL, Launer LJ, Ikram MA, Crane PK, Lambert JC, Mayeux R, Seshadri S; International Genomics of Alzheimer’s Project. Evaluation of a genetic risk score to improve risk prediction for Alzheimer’s disease. J Alzheimers Dis. 2016;53(3):921-932.
Chu Y, Morfini GA, Kordower JH. Alterations in activity-dependent neuroprotective protein in sporadic and experimental Parkinson’s disease. J Parkinsons Dis. 2016;6(1):77-97.
Comella CL, Camba GC, Truong D, Espay AJ, Snyder D, Marchese D, Trosch R. Poster 296: abobotulinumtoxina injection patterns in patients with cervical dystonia from the ANCHOR-CD registry study. PM R. 2016;8(9S):S256-S257.
Comella CL, Perlmutter JS, Jinnah HA, Waliczek TA, Rosen AR, Galpern WR, Adler CA, Barbano RL, Factor SA, Goetz CG, Jankovic J, Reich SG, Rodriguez RL, Severt WL, Zurowski M, Fox SH, Stebbins GT. Clinimetric testing of the comprehensive cervical dystonia rating scale. Mov Disord. 2016;31(4):563-569.
Corbillé AG, Letournel F, Kordower JH, Lee J, Shanes E, Neunlist M, Munoz DG, Derkinderen P, Beach TG. Evaluation of alpha-synuclein immunohistochemical methods for the detection of Lewy-type synucleinopathy in gastrointestinal biopsies. Acta Neuropathol Commun. 2016;4:35.
Costello BT, Silverman ER, Doukky R, Braun LT, Aggarwal NT, Deng Y, Li Y, Lundberg G, Williams KA Sr, Volgman AS. Lipoprotein(a) and increased cardiovascular risk in women. Clin Cardiol. 2016;39(2):96-102.
Cothran FA, Paun O, Farran CJ, Barnes LL. Racial differences in program evaluation of a lifestyle physical activity randomized controlled trial. West J Nurs Res. 2016;38(10):1264-1281.
Counts SE, He B, Prout JG, Michalski B, Farotti L, Fahnestock M, Mufson EJ. Cerebrospinal fluid proNGF: a putative biomarker for early Alzheimer’s disease. Curr Alzheimer Res. 2016;13(7):800-808.
Crane PK, Gibbons LE, Dams-O’Connor K, Trittschuh E, Leverenz JB, Keene CD, Sonnen J, Montine TJ, Bennett DA, Leurgans S, Schneider JA, Larson EB. Association of traumatic brain injury with late-life neurodegenerative conditions and neuropathologic findings. JAMA Neurol. 2016;73(9):1062-1069.
Crossley KM, Agnihotri S, Chaganti J, Rodriguez ML, McNally LP, Venna N, Turbett SE, Gutman M, Morey A, Koralnik IJ, Brew BJ. Recurrence of progressive multifocal leukoencephalopathy despite immune recovery in two HIV seropositive individuals. J Neurovirol. 2016;22(4):541-545.
Crowley RW. Another AVM grading scale … really? World Neurosurg. 2016;92:537-539.
Crystal HA, Holman S, Lui YW, Baird AE, Yu H, Klein R, Rojas-Soto DM, Gustafson DR, Stebbins GT. Association of the fractal dimension of retinal arteries and veins with quantitative brain MRI measures in HIV-infected and uninfected women. PLoS One. 2016;11(5):e0154858.
Cutting S, Regan E, Lee VH, Prabhakaran S. High ABCD2 scores and in-hospital interventions following transient ischemic attack. Cerebrovasc Dis Extra. 2016;6(3):76-83.
Da Silva IR, Gomes JA, Wachsman A, Rodriguez de Freitas G, Provencio JJ. Effect of age on transcranial Doppler velocities in patients with aneurysmal subarachnoid hemorrhage. Eur Neurol. 2016;76(5-6):261-266.
David FJ, Robichaud JA, Vaillancourt DE, Poon C, Kohrt WM, Comella CL, Corcos DM. Progressive resistance exercise restores some properties of the triphasic EMG pattern and improves bradykinesia: the PRET-PD randomized clinical trial. J Neurophysiol. 2016;116(5):2298-2311.
Davis MY, Johnson CO, Leverenz JB, Weintraub D, Trojanowski JQ, Chen-Plotkin A, Van Deerlin VM, Quinn JF, Chung KA, Peterson-Hiller AL, Rosenthal LS, Dawson TM, Albert MS, Goldman JG, Stebbins GT, Bernard B, Wszolek ZK, Ross OA, Dickson DW, Eidelberg D, Mattis PJ, Niethammer M, Yearout D, Hu SC, Cholerton BA, Smith M, Mata IF, Montine TJ, Edwards KL, Zabetian CP. Association of GBA mutations and the E326K polymorphism with motor and cognitive progression in Parkinson disease. JAMA Neurol. 2016;73(10):1217-1224.
Dawe RJ, Yu L, Leurgans SE, Schneider JA, Buchman AS, Arfanakis K, Bennett DA, Boyle PA. Postmortem MRI: a novel window into the neurobiology of late life cognitive decline. Neurobiol Aging. 2016;45:169-177.
Debrey SM, Leehey MA, Klepitskaya O, Filley CM, Shah RC, Kluger B, Berry-Kravis E, Spector E, Tassone F, Hall DA. Clinical phenotype of adult fragile X gray zone allele carriers: a case series. Cerebellum. 2016;15(5):623-631.
Deeb W, Giordano JJ, Rossi PJ, Mogilner AY, Gunduz A, Judy JW, Klassen BT, Butson CR, Van Horne C, Deny D, Dougherty DD, Rowell D, Gerhardt GA, Smith GS, Ponce FA, Walker HC, Bronte-Stewart HM, Mayberg HS, Chizeck HJ, Langevin JP, Volkmann J, Ostrem JL, Shute JB, Jimenez-Shahed J, Foote KD, Wagle Shukla A, Rossi MA, Oh M, Pourfar M, Rosenberg PB, Silburn PA, de Hemptine C, Starr PA, Denison T, Akbar U, Grill WM, Okun MS. Proceedings of the Fourth Annual Deep Brain Stimulation Think
42 /// THE 2017 RUSH NEUROSCIENCE REVIEW

Publications (2016) /// 43
Tank: a review of emerging issues and technologies. Front Integr Neurosci. 2016;10:38.
de Filippis I, Guerra Nunes PC, de Andrade CF, Gonçalves BS, de Araújo ES, Bezerra IO, da Silva IR, Nogueira RM, de Filippis AM. Fatal case of co-infection with dengue virus and Neisseria meningitidis during a dengue epidemic in the state of Rio de Janeiro, Brazil. JMM Case Rep. 2016;3(4):e005055.
Dehay B, Vila M, Bezard E, Brundin P, Kordower JH. Alpha-synuclein propagation: new insights from animal models. Mov Disord. 2016;31(2):161-168.
De Maio F, Shah RC. Community response to a public health advertisement. Am J Public Health. 2016;106(11):1979.
Demirkan A, Lahti J, Direk N, Viktorin A, Lunetta KL, Terracciano A, Nalls MA, Tanaka T, Hek K, Fornage M, Wellmann J, Cornelis MC, Ollila HM, Yu L, Smith JA, Pilling LC, Isaacs A, Palotie A, Zhuang WV, Zonderman A, Faul JD, Sutin A, Meirelles O, Mulas A, Hofman A, Uitterlinden A, Rivadeneira F, Perola M, Zhao W, Salomaa V, Yaffe K, Luik AI; NABEC, Liu Y, Ding J, Lichtenstein P, Landén M, Widen E, Weir DR, Llewellyn DJ, Murray A, Kardia SL, Eriksson JG, Koenen K, Magnusson PK, Ferrucci L, Mosley TH, Cucca F, Oostra BA, Bennett DA, Paunio T, Berger K, Harris TB, Pedersen NL, Murabito JM, Tiemeier H, van Duijn CM, Räikkönen K. Somatic, positive and negative domains of the Center for Epidemiological Studies Depression (CES-D) scale: a meta-analysis of genome-wide association studies. Psychol Med. 2016;46(8):1613-1623.
Deng HX, Shi Y, Yang Y, Ahmeti KB, Miller N, Huang C, Cheng L, Zhai H, Deng S, Nuytemans K, Corbett NJ, Kim MJ, Deng H, Tang B, Yang Z, Xu Y, Chan P, Huang B, Gao XP, Song Z, Liu Z, Fecto F, Siddique N, Foroud T, Jankovic J, Ghetti B, Nicholson DA, Krainc D, Melen O, Vance JM, Pericak-Vance MA, Ma YC, Rajput AH, Siddique T. Identification of TMEM230 mutations in familial Parkinson’s disease. Nat Genet. 2016;48(7):733-739.
Diederich NJ, Goldman JG, Stebbins GT, Goetz CG. Failing as doorman and disc jockey at the same time: amygdalar dysfunction in Parkinson’s disease. Mov Disord. 2016;31(1):11-22.
Do Carmo S, Hanzel CE, Jacobs ML, Machnes Z, Iulita MF, Yang J, Yu L, Ducatenzeiler A, Danik M, Breuillaud LS, Bennett DA, Szyf M, Cuello AC. Rescue of early bace-1 and global DNA demethylation by S-adenosylmethionine reduces amyloid pathology and improves cognition in an Alzheimer’s model. Sci Rep. 2016;6:34051.
Duke Han S, Boyle PA, Yu L, Arfanakis K, James BD, Fleischman DA, Bennett DA. Grey matter correlates of susceptibility to scams in community-dwelling older adults. Brain Imaging Behav. 2016;10(2):524-532.
Durst CR, Hixson HR, Schmitt P, Gingras JM, Crowley RW. Endovascular treatment of a fusiform aneurysm at the M3-M4 junction of the middle cerebral artery using the Pipeline Embolization Device. World Neurosurg. 2016;86:511.e1-4.
Durst CR, Ornan DA, Reardon MA, Mehndiratta P, Mukherjee S, Starke RM, Wintermark M, Evans A, Jensen ME, Crowley RW, Gaughen J, Liu KC. Prevalence of dural venous sinus stenosis and hypoplasia in a generalized population. J Neurointerv Surg. 2016;8(11):1173-1177.
Durst CR, Starke RM, Clopton D, Hixson HR, Schmitt PJ, Gingras JM, Ding D, Liu KC, Crowley RW, Jensen ME, Evans AJ, Gaughen J. Endovascular treatment of ophthalmic artery aneurysms: ophthalmic artery patency following flow diversion versus coil embolization. J Neurointerv Surg. 2016;8(9):919-922.
Ergonul O, Egeli D, Kahyaoglu B, Bahar M, Etienne M, Bleck T. An unexpected tetanus case. Lancet Infect Dis. 2016;16(6):746-752.
Falco-Walter JJ, Bleck T. Treatment of established status epilepticus. J Clin Med. 2016;5(5):E49.
Falco-Walter JJ, Stein M, McNulty M, Romantseva L, Heydemann P. ‘Tickling’ seizures originating in the left frontoparietal region. Epilepsy Behav Case Rep. 2016;6:49-51.
Farfel JM, Yu L, Buchman AS, Schneider JA, De Jager PL, Bennett DA. Relation of genomic variants for Alzheimer disease dementia to common neuropathologies. Neurology. 2016;87(5):489-496.
Farfel JM, Yu L, De Jager PL, Schneider JA, Bennett DA. Association of APOE with tau-tangle pathology with and without β-amyloid. Neurobiol Aging. 2016;37:19-25.
Farran CJ, Etkin CD, Eisenstein A, Paun O, Rajan KB, Sweet CMC, McCann JJ, Barnes LL, Shah RC, Evans DA. Effect of moderate to vigorous physical activity intervention on improving dementia family caregiver physical function: a randomized controlled trial. J Alzheimers Dis Parkinsonism. 2016;6(4):253.
Fehlings MG, Tetreault L, Hsieh PC, Traynelis V, Wang MY. Introduction: degenerative cervical myelopathy: diagnostic, assessment, and management strategies, surgical complications, and outcome prediction. Neurosurg Focus. 2016;40(6):E1.
Felsky D, De Jager PL, Schneider JA, Arfanakis K, Fleischman DA, Arvanitakis Z, Honer WG, Pouget JG, Mizrahi R, Pollock BG, Kennedy JL, Bennett DA, Voineskos AN; authors of the Alzheimer’s Disease Neuroimaging Initiative. Cerebrovascular and microglial states are not altered by functional neuroinflammatory gene variant. J Cereb Blood Flow Metab. 2016;36(4):819-830.
Ferreira da Silva IR, Frontera JA, Moreira do Nascimento OJ. News from the battlefront: Zika virus-associated Guillain-Barré syndrome in Brazil. Neurology. 2016;87(15):e180-e181.
Fontes RB, Wewel JT, O’Toole JE. Perioperative cost analysis of minimally invasive vs open resection of intradural extramedullary spinal cord tumors. Neurosurgery. 2016;78(4):531-539.
Foveau B, Albrecht S, Bennett DA, Correa JA, LeBlanc AC. Increased Caspase-6 activity in the human anterior olfactory nuclei of the olfactory bulb is associated with cognitive impairment. Acta Neuropathol Commun. 2016;4(1):127.
Fraint A, Vittal P, Comella C. Considerations on patient-related outcomes with the use of botulinum toxins: is switching products safe? Ther Clin Risk Manag. 2016;12:147-154.
Friedman JH, Beck JC, Chou KL, Clark G, Fagundes CP, Goetz CG, Herlofson K, Kluger B, Krupp LB, Lang AE, Lou JS, Marsh L, Newbould A, Weintraub D. Fatigue in Parkinson’s disease: report from a mutidisciplinary symposium. NPJ Parkinsons Dis. 2016;2:15025.
Fromer M, Roussos P, Sieberts SK, Johnson JS, Kavanagh DH, Perumal TM, Ruderfer DM, Oh EC, Topol A, Shah HR, Klei LL, Kramer R, Pinto D, Gümüş ZH, Cicek AE, Dang KK, Browne A, Lu C, Xie L, Readhead B, Stahl EA, Xiao J, Parvizi M, Hamamsy T, Fullard JF, Wang YC, Mahajan MC, Derry JM, Dudley JT, Hemby SE, Logsdon BA, Talbot K, Raj T, Bennett DA, De Jager PL, Zhu J, Zhang B, Sullivan PF, Chess A, Purcell SM, Shinobu LA, Mangravite LM, Toyoshiba H, Gur RE, Hahn CG, Lewis DA, Haroutunian V, Peters MA, Lipska BK, Buxbaum JD, Schadt EE, Hirai K, Roeder K, Brennand KJ, Katsanis N, Domenici E, Devlin B, Sklar P. Gene expression elucidates functional impact of polygenic risk for schizophrenia. Nat Neurosci. 2016;19(11):1442-1453.
Publications (2016) /// 43

44 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Frontera JA, da Silva IR. Zika getting on your nerves? the association with the Guillain-Barré syndrome. N Engl J Med. 2016;375(16):1581-1582.
Gaiteri C, Mostafavi S, Honey CJ, De Jager PL, Bennett DA. Genetic variants in Alzheimer disease—molecular and brain network approaches. Nat Rev Neurol. 2016;12(7):413-427.
Gerard CS, Metman LV, Pal G, Karl J, Sani S. Severe, symptomatic, self-limited unilateral DBS lead edema following bilateral subthalamic nucleus implantation: case report and review of the literature. Neurologist. 2016;21(4):58-60.
Ghosh A, Pahan K. PPARα in lysosomal biogenesis: a perspective. Pharmacol Res. 2016;103:144-148.
Ghosh A, Tyson T, George S, Hildebrandt EN, Steiner JA, Madaj Z, Schulz E, Machiela E, McDonald WG, Escobar Galvis ML, Kordower JH, Van Raamsdonk JM, Colca JR, Brundin P. Mitochondrial pyruvate carrier regulates autophagy, inflammation, and neurodegeneration in experimental models of Parkinson’s disease. Sci Transl Med. 2016;8(368):368ra174.
Gillis CC, Kaszuba MC, Traynelis VC. Cervical radiographic parameters in 1- and 2-level anterior cervical discectomy and fusion. J Neurosurg Spine. 2016;25(4):421-429.
Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, Bare M, Bleck T, Dodson WE, Garrity L, Jagoda A, Lowenstein D, Pellock J, Riviello J, Sloan E, Treiman DM. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults: report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48-61.
Goetz CG. Charcot, hysteria, and simulated disorders. Handb Clin Neurol. 2016;139:11-23.
Goetz CG, Liu Y, Stebbins GT, Wang L, Tilley BC, Teresi JA, Merkitch D, Luo S. Gender-, age-, and race/ethnicity-based differential item functioning analysis of the movement disorder society-sponsored revision of the Unified Parkinson’s Disease Rating Scale. Mov Disord. 2016;31(12):1865-1873.
Gold R, Radue EW, Giovannoni G, Selmaj K, Havrdova E, Stefoski D, Sprenger T, Montalban X, Cohan S, Umans K, Greenberg SJ, Ozen G, Elkins J. Safety and efficacy of daclizumab in relapsing-remitting multiple sclerosis: 3-year results from the SELECTED open-label extension study. BMC Neurol. 2016;16:117.
Gold R, Stefoski D, Selmaj K, Havrdova E, Hurst C, Holman J, Tornesi B, Akella S, McCroskery P. Pregnancy experience: nonclinical studies and pregnancy outcomes in the daclizumab clinical study program. Neurol Ther. 2016;5(2):169-182.
Goldman JG. Neuropsychiatric issues in Parkinson disease. Continuum (Minneap Minn). 2016;22(4):1086-1103.
Grigalunas AL, Mizen TR. Myeloid sarcoma of the orbit without systemic recurrence of disease in an adult: a clinicopathological case report. Orbit. 2016;35(2):106-108.
Guella I, Evans DM, Szu-Tu C, Nosova E, Bortnick SF, SNCA Cognition Study Group, Goldman JG, Dalrymple-Alford JC, Geurtsen GJ, Litvan I, Ross OA, Middleton LT, Parkkinen L, Farrer MJ.α-synuclein genetic variability: a biomarker for dementia in Parkinson disease. Ann Neurol. 2016;79(6):991-999.
Guptill JT, Soni M, Meriggioli MN. Current treatment, emerging translational therapies, and new therapeutic targets for autoimmune myasthenia gravis. Neurotherapeutics. 2016;13(1):118-131.
Hadd AG, Filipovic-Sadic S, Zhou L, Williams A, Latham GJ, Berry-Kravis E, Hall DA. A methylation PCR method determines FMR1 activation ratios and differentiates premutation allele mosaicism in carrier siblings. Clin Epigenetics. 2016;8:130.
Hall DA, Robertson-Dick EE, O’Keefe JA, Hadd AG, Zhou L, Berry-Kravis E. X-inactivation in the clinical phenotype of fragile X premutation carrier sisters. Neurol Genet. 2016;2(1):e45.
Hall DA, Robertson E, Shelton AL, Losh MC, Mila M, Moreno EG, Gomez-Anson B, Martínez-Cerdeño V, Grigsby J, Lozano R, Hagerman R, Maria LS, Berry-Kravis E, O’Keefe JA. Update on the clinical, radiographic, and neurobehavioral manifestations in FXTAS and FMR1 premutation carriers. Cerebellum. 2016;15(5):578-586.
Hall D, Todorova-Koteva K, Pandya S, Bernard B, Ouyang B, Walsh M, Pounardjian T, Deburghraeve C, Zhou L, Losh M, Leehey M, Berry-Kravis E. Neurological and endocrine phenotypes of fragile X carrier women. Clin Genet. 2016;89(1):60-67.
Hamilton DK, Kanter AS, Bolinger BD, Mundis GM Jr, Nguyen S, Mummaneni PV, Anand N, Fessler RG, Passias PG, Park P, La Marca F, Uribe JS, Wang MY, Akbarnia BA, Shaffrey CI, Okonkwo DO; International Spine Study Group (ISSG). Reoperation rates in minimally invasive, hybrid and open surgical treatment for adult spinal deformity with minimum 2-year follow-up. Eur Spine J. 2016;25(8):2605-2611.
Hamlett ED, Boger HA, Ledreux A, Kelley CM, Mufson EJ, Falangola MF, Guilfoyle DN, Nixon RA, Patterson D, Duval N, Granholm AC. Cognitive impairment, neuroimaging, and Alzheimer neuropathology in mouse models of Down syndrome. Curr Alzheimer Res. 2016;13(1):35-52.
Han SD, Boyle PA, Arfanakis K, Fleischman D, Yu L, James BD, Bennett DA. Financial literacy is associated with white matter integrity in old age. Neuroimage. 2016;130:223-229.
Han SD, Boyle PA, James BD, Yu L, Barnes LL, Bennett DA. Discrepancies between cognition and decision making in older adults. Aging Clin Exp Res. 2016;28(1):99-108.
Han SD, Boyle PA, James BD, Yu L, Bennett DA. Mild cognitive impairment and susceptibility to scams in old age. J Alzheimers Dis. 2016;49(3):845-851.
Haque RM, Uddin OM, Ahmed Y, El Ahmadieh TY, Hashmi SZ, Shah A, Fessler RG. “Push-through” rod passage technique for the improvement of lumbar lordosis and sagittal balance in minimally invasive adult degenerative scoliosis surgery. Clin Spine Surg. 2016;29(8):323-330.
Heiferman DM, Billingsley JT, Kasliwal MK, Johnson AK, Keigher KM, Frudit ME, Moftakhar R, Lopes DK. Use of flow-diverting stents as salvage treatment following failed stent-assisted embolization of intracranial aneurysms. J Neurointerv Surg. 2016;8(7):692-695.
Hessl D, Sansone SM, Berry-Kravis E, Riley K, Widaman KF, Abbeduto L, Schneider A, Coleman J, Oaklander D, Rhodes KC, Gershon RC. The NIH Toolbox Cognitive Battery for intellectual disabilities: three preliminary studies and future directions. J Neurodev Disord. 2016;8(1):35.
Hindman BJ, Fontes RB, From RP, Traynelis VC, Todd MM, Puttlitz CM, Santoni BG. Intubation biomechanics: laryngoscope force and cervical spine motion during intubation in cadavers—effect of severe distractive-flexion injury on C3-4 motion. J Neurosurg Spine. 2016;25(5):545-555.
44 /// THE 2017 RUSH NEUROSCIENCE REVIEW

Hinrich AJ, Jodelka FM, Chang JL, Brutman D, Bruno AM, Briggs CA, James BD, Stutzmann GE, Bennett DA, Miller SA, Rigo F, Marr RA, Hastings ML. Therapeutic correction of ApoER2 splicing in Alzheimer’s disease mice using antisense oligonucleotides. EMBO Mol Med. 2016;8(4):328-345.
Hock LE, Kontzialis M, Szewka AJ. Linear scleroderma en coup de sabre presenting with positional diplopia and enophthalmos. Neurology. 2016;87(16):1741-1742.
Hohman TJ, Cooke-Bailey JN, Reitz C, Jun G, Naj A, Beecham GW, Liu Z, Carney RM, Vance JM, Cuccaro ML, Rajbhandary R, Vardarajan BN, Wang LS, Valladares O, Lin CF, Larson EB, Graff-Radford NR, Evans D, De Jager PL, Crane PK, Buxbaum JD, Murrell JR, Raj T, Ertekin-Taner N, Logue MW, Baldwin CT, Green RC, Barnes LL, Cantwell LB, Fallin MD, Go RC, Griffith P, Obisesan TO, Manly JJ, Lunetta KL, Kamboh MI, Lopez OL, Bennett DA, Hardy J, Hendrie HC, Hall KS, Goate AM, Lang R, Byrd GS, Kukull WA, Foroud TM, Farrer LA, Martin ER, Pericak-Vance MA, Schellenberg GD, Mayeux R, Haines JL, Thornton-Wells TA; Alzheimer Disease Genetics Consortium. Global and local ancestry in African-Americans: implications for Alzheimer’s disease risk. Alzheimers Dement. 2016;12(3):233-243.
Hong CS, Starke RM, Crowley RW. Endovascular stenting versus carotid endarterectomy for treatment of severe carotid stenosis: recent results from ACT I and the updated CREST studies. World Neurosurg. 2016;92:473-475.
Hopfner F, Haubenberger D, Galpern WR, Gwinn K, Van’t Veer A, White S, Bhatia K, Adler CH, Eidelberg D, Ondo W, Stebbins GT, Tanner CM, Helmich RC, Lenz FA, Sillitoe RV, Vaillancourt D, Vitek JL, Louis ED, Shill HA, Frosch MP, Foroud T, Kuhlenbäumer G, Singleton A, Testa CM, Hallett M, Elble R, Deuschl G. Knowledge gaps and research recommendations for essential tremor. Parkinsonism Relat Disord. 2016;33:27-35.
Huntington Study Group PHAROS Investigators, Biglan KM, Shoulson I, Kieburtz K, Oakes D, Kayson E, Shinaman MA, Zhao H, Romer M, Young A, Hersch S, Penney J, Marder K, Paulsen J, Quaid K, Siemers E, Tanner C, Mallonee W, Suter G, Dubinsky R, Gray C, Nance M, Bundlie S, Radtke D, Kostyk S, Baic C, Caress J, Walker F, Hunt V, O’Neill C, Chouinard S, Factor S, Greenamyre T, Wood-Siverio C, Corey-Bloom J, Song D, Peavy G, Moskowitz C, Wesson M, Samii A, Bird T, Lipe H, Blindauer K, Marshall F, Zimmerman C, Goldstein J, Rosas D, Novak P, Caviness J, Adler C, Duffy A, Wheelock V, Tempkin T, Richman D, Seeberger L, Albin R, Chou KL, Racette B, Perlmutter JS, Perlman S, Bordelon Y, Martin W, Wieler M, Leavitt B, Raymond L, Decolongon J, Clarke L, Jankovic J, Hunter C, Hauser RA, Sanchez-Ramos J, Furtado S, Suchowersky O, Klimek ML, Guttman M, Sethna R, Feigin A, Cox M, Shannon B, Percy A, Dure L, Harrison M, Johnson W, Higgins D, Molho E, Nickerson C, Evans S, Hobson D, Singer C, Galvez-Jimenez N, Shannon K, Comella C, Ross C, Saint-Hilaire MH, Testa C, Rosenblatt A, Hogarth P, Weiner W, Como P, Kumar R, Cotto C, Stout J, Brocht A, Watts A, Eberly S, Weaver C, Foroud T, Gusella J, MacDonald M, Myers R, Fahn S, Shults C. Clinical-genetic associations in the Prospective Huntington at Risk Observational Study (PHAROS): implications for clinical trials. JAMA Neurol. 2016;73(1):102-110.
Ibrahim-Verbaas CA, Bressler J, Debette S, Schuur M, Smith AV, Bis JC, Davies G, Trompet S, Smith JA, Wolf C, Chibnik LB, Liu Y, Vitart V, Kirin M, Petrovic K, Polasek O, Zgaga L, Fawns-Ritchie C, Hoffmann P, Karjalainen J, Lahti J, Llewellyn DJ, Schmidt CO, Mather KA, Chouraki V, Sun Q, Resnick SM, Rose LM, Oldmeadow C, Stewart M, Smith BH, Gudnason V, Yang Q, Mirza SS, Jukema JW, deJager PL, Harris TB, Liewald DC, Amin N, Coker LH, Stegle O, Lopez OL, Schmidt R, Teumer A, Ford I, Karbalai N, Becker JT, Jonsdottir MK, Au R, Fehrmann R, Herms S, Nalls M, Zhao W,
Turner ST, Yaffe K, Lohman K, van Swieten JC, Kardia S, Knopman DS, Meeks WM, Heiss G, Holliday EG, Schofield PW, Tanaka T, Stott DJ, Wang J, Ridker P, Gow AJ, Pattie A, Starr JM, Hocking LJ, Armstrong NJ, McLachlan S, Shulman JM, Pilling LC, Eiriksdottir G, Scott RJ, Kochan NA, Palotie A, Hsieh YC, Eriksson JG, Penman A, Gottesman RF, Oostra BA, Yu L, DeStefano AL, Beiser A, Garcia M, Rotter JI, Nöthen MM, Hofman A, Slagboom PE, Westendorp R, Buckley BM, Wolf PA, Uitterlinden AG, Psaty BM, Grabe HJ, Bandinelli S, Chasman DI, Grodstein F, Räikkönen K, Lambert JC, Porteous DJ; Generation Scotland, Price JF, Sachdev PS, Ferrucci L, Attia JR, Rudan I, Hayward C, Wright AF, Wilson JF, Cichon S, Franke L, Schmidt H, Ding J, de Craen A, Fornage M, Bennett DA, Deary IJ, Ikram MA, Launer LJ, Fitzpatrick AL, Seshadri S, van Duijn CM, Mosley TH. GWAS for executive function and processing speed suggests involvement of the CADM2 gene. Mol Psychiatry. 2016;21(2):189-197.
Jack CR Jr, Bennett DA, Blennow K, Carrillo MC, Feldman HH, Frisoni GB, Hampel H, Jagust WJ, Johnson KA, Knopman DS, Petersen RC, Scheltens P, Sperling RA, Dubois B. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology. 2016;87(5):539-547.
Jalota A, Rossi MA, Pylypyuk V, Stein M, Stoub T, Balabanov A, Bergen D, Bermeo A, Park E, Smith M, Byrne R. Resecting critical nodes from an epileptogenic circuit in refractory focal-onset epilepsy patients using subtraction ictal SPECT coregistered to MRI. J Neurosurg. 2016;125(6):1565-1576.
James BD, Wilson RS, Boyle PA, Trojanowski JQ, Bennett DA, Schneider JA. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain. 2016;139(11):2983-2993.
Jang DK, Stidd DA, Schafer S, Chen M, Moftakhar R, Lopes DK. Monoplane 3D Overlay roadmap versus conventional biplane 2D roadmap technique for neurointervenional procedures. Neurointervention. 2016;11(2):105-113.
Jiang X, Sidhu R, Mydock-McGrane L, Hsu FF, Covey DF, Scherrer DE, Earley B, Gale SE, Farhat NY, Porter FD, Dietzen DJ, Orsini JJ, Berry-Kravis E, Zhang X, Reunert J, Marquardt T, Runz H, Giugliani R, Schaffer JE, Ory DS. Development of a bile acid-based newborn screen for Niemann-Pick disease type C. Sci Transl Med. 2016;8(337):337ra63.
Johnson AK, Tan LA, Lopes DK, Moftakhar R. Progressive deconstruction of a distal posterior cerebral artery aneurysm using competitive flow diversion. Neurointervention. 2016;11(1):46-49.
Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, Hicks M, Puzanov I, Alexander MR, Bloomer TL, Becker JR, Slosky DA, Phillips EJ, Pilkinton MA, Craig-Owens L, Kola N, Plautz G, Reshef DS, Deutsch JS, Deering RP, Olenchock BA, Lichtman AH, Roden DM, Seidman CE, Koralnik IJ, Seidman JG, Hoffman RD, Taube JM, Diaz LA Jr, Anders RA, Sosman JA, Moslehi JJ. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375(18):1749-1755.
Jun G, Ibrahim-Verbaas CA, Vronskaya M, Lambert JC, Chung J, Naj AC, Kunkle BW, Wang LS, Bis JC, Bellenguez C, Harold D, Lunetta KL, Destefano AL, Grenier-Boley B, Sims R, Beecham GW, Smith AV, Chouraki V, Hamilton-Nelson KL, Ikram MA, Fievet N, Denning N, Martin ER, Schmidt H, Kamatani Y, Dunstan ML, Valladares O, Laza AR, Zelenika D, Ramirez A, Foroud TM, Choi SH, Boland A, Becker T, Kukull WA, van der Lee SJ, Pasquier F, Cruchaga C, Beekly D, Fitzpatrick AL, Hanon O, Gill M, Barber R, Gudnason V, Campion D, Love S, Bennett DA, Amin N, Berr C, Tsolaki M, Buxbaum JD, Lopez OL, Deramecourt V, Fox NC, Cantwell LB, Tárraga L, Dufouil C, Hardy J, Crane PK, Eiriksdottir G, Hannequin D, Clarke R, Evans D, Mosley TH Jr, Letenneur L, Brayne C, Maier W, De Jager P, Emilsson V, Dartigues JF,
Publications (2016) /// 45

Hampel H, Kamboh MI, de Bruijn RF, Tzourio C, Pastor P, Larson EB, Rotter JI, O’Donovan MC, Montine TJ, Nalls MA, Mead S, Reiman EM, Jonsson PV, Holmes C, St George-Hyslop PH, Boada M, Passmore P, Wendland JR, Schmidt R, Morgan K, Winslow AR, Powell JF, Carasquillo M, Younkin SG, Jakobsdóttir J, Kauwe JS, Wilhelmsen KC, Rujescu D, Nöthen MM, Hofman A, Jones L; IGAP Consortium, Haines JL, Psaty BM, Van Broeckhoven C, Holmans P, Launer LJ, Mayeux R, Lathrop M, Goate AM, Escott-Price V, Seshadri S, Pericak-Vance MA, Amouyel P, Williams J, van Duijn CM, Schellenberg GD, Farrer LA. A novel Alzheimer disease locus located near the gene encoding tau protein. Mol Psychiatry. 2016;21(1):108-117.
Kallmes DF, Brinjikji W, Boccardi E, Ciceri E, Diaz O, Tawk R, Woo H, Jabbour P, Albuquerque F, Chapot R, Bonafe A, Dashti SR, Delgado Almandoz JE, Given C II, Kelly ME, Cross DT III, Duckwiler G, Razack N, Powers CJ, Fischer S, Lopes D, Harrigan MR, Huddle D, Turner R IV, Zaidat OO, Defreyne L, Pereira VM, Cekirge S, Fiorella D, Hanel RA, Lylyk P, McDougall C, Siddiqui A, Szikora I, Levy E. Aneurysm study of Pipeline in an observational registry (ASPIRe). Interv Neurol. 2016;5(1-2):89-99.
Kamiya-Matsuoka C, Cachia D, Waguespack SG, Crane CH, Mahajan A, Brown PD, Nam JY , McCutcheon IE, Penas-Prado M. Radiotherapy with concurrent temozolomide for the management of extraneural metastases in pituitary carcinoma. Pituitary. 2016;19(4):415-421.
Kang UJ, Goldman JG, Alcalay RN, Xie T, Tuite P, Henchcliffe C, Hogarth P, Amara AW, Frank S, Rudolph A, Casaceli C, Andrews H, Gwinn K, Sutherland M, Kopil C, Vincent L, Frasier M. The BioFIND study: characteristics of a clinically typical Parkinson’s disease biomarker cohort. Mov Disord. 2016;31(6):924-932.
Kapasi A, Schneider JA. Vascular contributions to cognitive impairment, clinical Alzheimer’s disease, and dementia in older persons. Biochim Biophys Acta. 2016;1862(5):878-886.
Kasliwal MK, Corley JA, Traynelis VC. Posterior cervical fusion using cervical interfacet spacers in patients with symptomatic cervical pseudarthrosis. Neurosurgery. 2016;78(5):661-668.
Kasliwal MK, Fontes RB, Traynelis VC. Occipitocervical dissociation-incidence, evaluation, and treatment. Curr Rev Musculoskelet Med. 2016;9(3):247-254.
Kasliwal MK, Tan LA, Wewel JT, Traynelis VC. Exuberant heterotopic ossification following anterior cervical fusion. Neurol India. 2016;64(3):571-572.
Kasliwal MK, Witiw CD, Traynelis VC. Neck range of motion following cervical spinal fusion: a comparison of patient-centered and objective assessments. Clin Neurol Neurosurg. 2016;151:1-5.
Kaszuba MC, Kasliwal MK, O’Toole JE. Thoracic paraspinal lesion. J Clin Neurosci. 2016;25:116, 169.
Kelley CM, Ash JA, Powers BE, Velazquez R, Alldred MJ, Ikonomovic MD, Ginsberg SD, Strupp BJ, Mufson EJ. Effects of maternal choline supplementation on the septohippocampal cholinergic system in the Ts65Dn mouse model of Down syndrome. Curr Alzheimer Res. 2016;13(1):84-96.
Kelly A, Calamia M, Koval A, Terrera GM, Piccinin AM, Clouston S, Hassing LB, Bennett DA, Johansson B, Hofer SM. Independent and interactive impacts of hypertension and diabetes mellitus on verbal memory: a coordinated analysis of longitudinal data from England, Sweden, and the United States. Psychol Aging. 2016;31(3):262-273.
Kepler CK, Vaccaro AR, Chen E, Patel AA, Ahn H, Nassr A, Shaffrey CI, Harrop J, Schroeder GD, Agarwala A, Dvorak
MF, Fourney DR, Wood KB, Traynelis VC, Yoon ST, Fehlings MG, Aarabi B. Treatment of isolated cervical facet fractures: a systematic review. J Neurosurg Spine. 2016;24(2):347-354.
Kerolus MG, Kellogg RG, Novo J, Arvanitis LD, Byrne RW. Pigmented ganglioglioma in a patient with chronic epilepsy and cortical dysplasia. J Clin Neurosci. 2016;24:17-21.
Kerolus MG, Patil J, Kurian A, Sani S. Intradural cavernous lymphangioma of the thoracic spine: case report, technical considerations, and review of the literature. Spine J. 2016;16(8):e561-e565.
Kerolus M, Turel MK, Tan L, Deutsch H. Stand-alone anterior lumbar interbody fusion: indications, techniques, surgical outcomes and complications. Expert Rev Med Devices. 2016;13(12):1127-1136.
Khanna R, McDevitt JL, Abecassis ZA, Smith ZA, Koski TR, Fessler RG, Dahdaleh NS. An outcome and cost analysis comparing single-level minimally invasive transforaminal lumbar interbody fusion using intraoperative fluoroscopy versus computed tomography-guided navigation. World Neurosurg. 2016;94:255-260.
Klein HU, Bennett DA, De Jager PL. The epigenome in Alzheimer’s disease: current state and approaches for a new path to gene discovery and understanding disease mechanism. Acta Neuropathol. 2016;132(4):503-514.
Kluger BM, Herlofson K, Chou KL, Lou JS, Goetz CG, Lang AE, Weintraub D, Friedman J. Parkinson’s disease-related fatigue: a case definition and recommendations for clinical research. Mov Disord. 2016;31(5):625-631.
Kochanski RB, Byrne N, Arvanitis L, Bhabad S, Byrne RW. A rare intracranial tumor consisting of malignant anaplastic and papillary meningioma subtypes [published correction appears in Surg Neurol Int. 2016;7:58]. Surg Neurol Int. 2016;7:21.
Kochanski RB, Dawe R, Eddelman DB, Kocak M, Sani S. Identification of the stria medullaris thalami using diffusion tensor imaging. Neuroimage Clin. 2016;12:852-857.
Kochanski RB, Kerolus MG, Pal G, Metman LV, Sani S. Use of intraoperative CT to predict the accuracy of microelectrode recording during deep brain stimulation surgery: a proof of concept study. Clin Neurol Neurosurg. 2016;150:164-168.
Koffman L, Prayson R, Manno EM. Malignant cerebral edema related to systemic lupus erythematosus. J Neurol Sci. 2016;364:180-182.
Kompoliti K. Sources of disability in Tourette syndrome: children vs. adults. Tremor Other Hyperkinet Mov (N Y). 2016;5:318.
Kontzialis M, Lee VH, Jhaveri MD. TIA due to cerebral fat embolism following lipid-based sonographic contrast agent injection. Eur Neurol. 2016;75(3-4):169.
Korbakis G, Prabhakaran S, John S, Garg R, Conners JJ, Bleck TP, Lee VH. MRI detection of cerebral infarction in subarachnoid hemorrhage. Neurocrit Care. 2016;24(3):428-435.
Kordower JH. AAV2-neurturin for Parkinson’s disease: what lessons have we learned? Methods Mol Biol. 2016;1382:485-490.
Kordower JH, Brundin P. Mechanisms for cell-to-cell propagation no longer lag behind. Mov Disord. 2016;31(12):1798-1799.
Kordower JH, Olanow CW. Fetal grafts for Parkinson’s disease: decades in the making. Proc Natl Acad Sci U S A. 2016;113(23):6332-6334.
Kovacheva VP, Aglio LS, Boland TA, Mendu ML, Gibbons
46 /// THE 2017 RUSH NEUROSCIENCE REVIEW

FK, Christopher KB. Acute kidney injury after craniotomy is associated with increased mortality: a cohort study. Neurosurgery. 2016;79(3):389-396.
Kovacs GG, Ferrer I, Grinberg LT, Alafuzoff I, Attems J, Budka H, Cairns NJ, Crary JF, Duyckaerts C, Ghetti B, Halliday GM, Ironside JW, Love S, Mackenzie IR, Munoz DG, Murray ME, Nelson PT, Takahashi H, Trojanowski JQ, Ansorge O, Arzberger T, Baborie A, Beach TG, Bieniek KF, Bigio EH, Bodi I, Dugger BN, Feany M, Gelpi E, Gentleman SM, Giaccone G, Hatanpaa KJ, Heale R, Hof PR, Hofer M, Hortobágyi T, Jellinger K, Jicha GA, Ince P, Kofler J, Kövari E, Kril JJ, Mann DM, Matej R, McKee AC, McLean C, Milenkovic I, Montine TJ, Murayama S, Lee EB, Rahimi J, Rodriguez RD, Rozemüller A, Schneider JA, Schultz C, Seeley W, Seilhean D, Smith C, Tagliavini F, Takao M, Thal DR, Toledo JB, Tolnay M, Troncoso JC, Vinters HV, Weis S, Wharton SB, White CL III, Wisniewski T, Woulfe JM, Yamada M, Dickson DW. Aging-related tau astrogliopathy (ARTAG): harmonized evaluation strategy. Acta Neuropathol. 2016;131(1):87-102.
Krishnan B, Scott MT, Pollandt S, Schroeder B, Kurosky A, Shinnick-Gallagher P. Fear potentiated startle increases phospholipase D (PLD) expression/activity and PLD-linked metabotropic glutamate receptor mediated post-tetanic potentiation in rat amygdala. Neurobiol Learn Mem. 2016;128:65-79.
Kryscio RJ, Abner EL, Nelson PT, Bennett D, Schneider J, Yu L, Hemmy LS, Lim KO, Masaki K, Cairns N, Xiong C, Woltjer R, Dodge HH, Tyas S, Fardo DW, Lou W, Wan L, Schmitt FA. The effect of vascular neuropathology on late-life cognition: results from the SMART project. J Prev Alzheimers Dis. 2016;3(2):85-91.
Kundu M, Mondal S, Roy A, Martinson JL, Pahan K. Sodium benzoate, a food additive and a metabolite of cinnamon, enriches regulatory T cells via STAT6-mediated upregulation of TGF-β. J Immunol. 2016;197(8):3099-3110.
Kurowska Z, Kordower JH, Stoessl AJ, Burke RE, Brundin P, Yue Z, Brady ST, Milbrandt J, Trapp BD, Sherer TB, Medicetty S. Is axonal degeneration a key early event in Parkinson’s disease? J Parkinsons Dis. 2016;6(4):703-707.
LaHue SC, Comella CL, Tanner CM. The best medicine? the influence of physical activity and inactivity on Parkinson’s disease. Mov Disord. 2016;31(10):1444-1454.
Leckie S, Yoon ST, Isaacs R, Radcliff K, Fessler R, Haid R Jr, Traynelis V. Perioperative complications of cervical spine surgery: analysis of a prospectively gathered database through the Association for Collaborative Spinal Research. Global Spine J. 2016;6(7):640-649.
LeDoux MS, Vemula SR, Xiao J, Thompson MM, Perlmutter JS, Wright LJ, Jinnah HA, Rosen AR, Hedera P, Comella CL, Weissbach A, Junker J, Jankovic J, Barbano RL, Reich SG, Rodriguez RL, Berman BD, Chouinard S, Severt L, Agarwal P, Stover NP. Clinical and genetic features of cervical dystonia in a large multicenter cohort. Neurol Genet. 2016;2(3):e69.
Lee R, Arfanakis K, Evia AM, Fanning J, Keedy S, Coccaro EF. White matter integrity reductions in intermittent explosive disorder. Neuropsychopharmacology. 2016;41(11):2697-2703.
Lewis SL. AD or not AD? that is just one of the questions. Continuum (Minneap Minn). 2016;22(2):383-384.
Lewis SL. An anthology of epileptology. Continuum (Minneap Minn). 2016;22(1):13-14.
Lewis SL. A kinetic and nonrigid approach to movement disorders. Continuum (Minneap Minn). 2016;22(4):1045-1046.
Lewis SL. Multiple approaches to multiple sclerosis (and other demyelinating diseases). Continuum (Minneap Minn). 2016;22(3):721-722.
Li L, Tan LA, Wewel JT, Kasliwal MK, O’Toole JE. Spinal aneurysmal bone cyst presenting as acute paraparesis during pregnancy. J Clin Neurosci. 2016;28:167-169.
Lim AS, Fleischman DA, Dawe RJ, Yu L, Arfanakis K, Buchman AS, Bennett DA. Regional neocortical gray matter structure and sleep fragmentation in older adults. Sleep. 2016;39(1):227-235.
Lim AS, Yu L, Schneider JA, Bennett DA, Buchman AS. Sleep fragmentation, cerebral arteriolosclerosis, and brain infarct pathology in community-dwelling older people. Stroke. 2016;47(2):516-518.
Lin N, Lanzino G, Lopes DK, Arthur AS, Ogilvy CS, Ecker RD, Dumont TM, Turner RD IV, Gooch MR, Boulos AS, Kan P, Snyder KV, Levy EI, Siddiqui AH. Treatment of distal anterior circulation aneurysms with the Pipeline Embolization Device: a US multicenter experience. Neurosurgery. 2016;79(1):14-22.
Litvan I, Lees PS, Cunningham CR, Rai SN, Cambon AC, Standaert DG, Marras C, Juncos J, Riley D, Reich S, Hall D, Kluger B, Bordelon Y, Shprecher DR; for ENGENE-PSP. Environmental and occupational risk factors for progressive supranuclear palsy: case-control study. Mov Disord. 2016;31(5):644-652.
Liu JA, Hagerman RJ, Miller RM, Craft LT, Finucane B, Tartaglia N, Berry-Kravis EM, Sherman SL, Kidd SA, Cohen J. Clinicians’ experiences with the fragile X clinical and research consortium. Am J Med Genet A. 2016;170(12):3138-3143.
Liu RX, Huang C, Bennett DA, Li H, Wang R. The characteristics of astrocyte on Aβ clearance altered in Alzheimer’s disease were reversed by anti-inflammatory agent (+)-2-(1-hydroxyl-4-oxocyclohexyl) ethyl caffeate. Am J Transl Res. 2016;8(10):4082-4094.
Lopes DK, Moftakhar R, Straus D, Munich SA, Chaus F, Kaszuba MC. Arteriovenous malformation embocure score: AVMES. J Neurointerv Surg. 2016;8(7):685-691.
Lopez GA. Temperature management in the neurointensive care unit. Curr Treat Options Neurol. 2016;18(3):12.
Lu Y, Day FR, Gustafsson S, Buchkovich ML, Na J, Bataille V, Cousminer DL, Dastani Z, Drong AW, Esko T, Evans DM, Falchi M, Feitosa MF, Ferreira T, Hedman ÅK, Haring R, Hysi PG, Iles MM, Justice AE, Kanoni S, Lagou V, Li R, Li X, Locke A, Lu C, Mägi R, Perry JR, Pers TH, Qi Q, Sanna M, Schmidt EM, Scott WR, Shungin D, Teumer A, Vinkhuyzen AA, Walker RW, Westra HJ, Zhang M, Zhang W, Zhao JH, Zhu Z, Afzal U, Ahluwalia TS, Bakker SJ, Bellis C, Bonnefond A, Borodulin K, Buchman AS, Cederholm T, Choh AC, Choi HJ, Curran JE, de Groot LC, De Jager PL, Dhonukshe-Rutten RA, Enneman AW, Eury E, Evans DS, Forsen T, Friedrich N, Fumeron F, Garcia ME, Gärtner S, Han BG, Havulinna AS, Hayward C, Hernandez D, Hillege H, Ittermann T, Kent JW, Kolcic I, Laatikainen T, Lahti J, Mateo Leach I, Lee CG, Lee JY, Liu T, Liu Y, Lobbens S, Loh M, Lyytikäinen LP, Medina-Gomez C, Michaëlsson K, Nalls MA, Nielson CM, Oozageer L, Pascoe L, Paternoster L, Polašek O, Ripatti S, Sarzynski MA, Shin CS, Narancic NS, Spira D, Srikanth P, Steinhagen-Thiessen E, Sung YJ, Swart KM, Taittonen L, Tanaka T, Tikkanen E, van der Velde N, van Schoor NM, Verweij N, Wright AF, Yu L, Zmuda JM, Eklund N, Forrester T, Grarup N, Jackson AU, Kristiansson K, Kuulasmaa T, Kuusisto J, Lichtner P, Luan J, Mahajan A, Männistö S, Palmer CD, Ried JS, Scott RA, Stancáková A, Wagner PJ, Demirkan A, Döring A, Gudnason V, Kiel DP, Kühnel B, Mangino M, Mcknight B, Menni C, O’Connell JR, Oostra BA, Shuldiner AR, Song K, Vandenput L, van Duijn CM, Vollenweider P, White CC, Boehnke M, Boettcher Y, Cooper
Publications (2016) /// 47

48 /// THE 2017 RUSH NEUROSCIENCE REVIEW
RS, Forouhi NG, Gieger C, Grallert H, Hingorani A, Jørgensen T, Jousilahti P, Kivimaki M, Kumari M, Laakso M, Langenberg C, Linneberg A, Luke A, Mckenzie CA, Palotie A, Pedersen O, Peters A, Strauch K, Tayo BO, Wareham NJ, Bennett DA, Bertram L, Blangero J, Blüher M, Bouchard C, Campbell H, Cho NH, Cummings SR, Czerwinski SA, Demuth I, Eckardt R, Eriksson JG, Ferrucci L, Franco OH, Froguel P, Gansevoort RT, Hansen T, Harris TB, Hastie N, Heliövaara M, Hofman A, Jordan JM, Jula A, Kähönen M, Kajantie E, Knekt PB, Koskinen S, Kovacs P, Lehtimäki T, Lind L, Liu Y, Orwoll ES, Osmond C, Perola M, Pérusse L, Raitakari OT, Rankinen T, Rao DC, Rice TK, Rivadeneira F, Rudan I, Salomaa V, Sørensen TI, Stumvoll M, Tönjes A, Towne B, Tranah GJ, Tremblay A, Uitterlinden AG, van der Harst P, Vartiainen E, Viikari JS, Vitart V, Vohl MC, Völzke H, Walker M, Wallaschofski H, Wild S, Wilson JF, Yengo L, Bishop DT, Borecki IB, Chambers JC, Cupples LA, Dehghan A, Deloukas P, Fatemifar G, Fox C, Furey TS, Franke L, Han J, Hunter DJ, Karjalainen J, Karpe F, Kaplan RC, Kooner JS, McCarthy MI, Murabito JM, Morris AP, Bishop JA, North KE, Ohlsson C, Ong KK, Prokopenko I, Richards JB, Schadt EE, Spector TD, Widén E, Willer CJ, Yang J, Ingelsson E, Mohlke KL, Hirschhorn JN, Pospisilik JA, Zillikens MC, Lindgren C, Kilpeläinen TO, Loos RJ. New loci for body fat percentage reveal link between adiposity and cardiometabolic disease risk. Nat Commun. 2016;7:10495.
Majumdar M, Tan LA, Chen M. Critical assessment of the morbidity associated with ruptured cerebral arteriovenous malformations. J Neurointerv Surg. 2016;8(2):163-167.
Malek-Ahmadi M, Perez SE, Chen K, Mufson EJ. Neuritic and diffuse plaque associations with memory in non-cognitively impaired elderly. J Alzheimers Dis. 2016;53(4):1641-1652.
Masoud H, Nguyen TN, Martin CO, Holloway WE, Ambekar S, Yavagal DR, Haussen DC, Nogueira R, Lozano DJ, Puri A, Quateen A, Iancu D, Abraham MG, Chen M, Mehta S, Malisch T, Marden F, Novakovic R, Roy D, Weill A, Norbash AM. Inadvertent stent retriever detachment: a multicenter case series and review of device experience FDA reports [published correction appears in Interv Neurol. 2016;4(3-4):82]. Interv Neurol. 2016;4(3-4):75-82.
Mata IF, Leverenz JB, Weintraub D, Trojanowski JQ, Chen-Plotkin A, Van Deerlin VM, Ritz B, Rausch R, Factor SA, Wood-Siverio C, Quinn JF, Chung KA, Peterson-Hiller AL, Goldman JG, Stebbins GT, Bernard B, Espay AJ, Revilla FJ, Devoto J, Rosenthal LS, Dawson TM, Albert MS, Tsuang D, Huston H, Yearout D, Hu SC, Cholerton BA, Montine TJ, Edwards KL, Zabetian CP. GBA Variants are associated with a distinct pattern of cognitive deficits in Parkinson’s disease. Mov Disord. 2016;31(1):95-102.
Matteini AM, Tanaka T, Karasik D, Atzmon G, Chou WC, Eicher JD, Johnson AD, Arnold AM, Callisaya ML, Davies G, Evans DS, Holtfreter B, Lohman K, Lunetta KL, Mangino M, Smith AV, Smith JA, Teumer A, Yu L, Arking DE, Buchman AS, Chibinik LB, De Jager PL, Evans DA, Faul JD, Garcia ME, Gillham-Nasenya I, Gudnason V, Hofman A, Hsu YH, Ittermann T, Lahousse L, Liewald DC, Liu Y, Lopez L, Rivadeneira F, Rotter JI, Siggeirsdottir K, Starr JM, Thomson R, Tranah GJ, Uitterlinden AG, Völker U, Völzke H, Weir DR, Yaffe K, Zhao W, Zhuang WV, Zmuda JM, Bennett DA, Cummings SR, Deary IJ, Ferrucci L, Harris TB, Kardia SL, Kocher T, Kritchevsky SB, Psaty BM, Seshadri S, Spector TD, Srikanth VK, Windham BG, Zillikens MC, Newman AB, Walston JD, Kiel DP, Murabito JM. GWAS analysis of handgrip and lower body strength in older adults in the CHARGE consortium. Aging Cell. 2016;15(5):792-800.
Matz PG, Meagher RJ, Lamer T, Tontz WL Jr, Annaswamy TM, Cassidy RC, Cho CH, Dougherty P, Easa JE, Enix DE, Gunnoe BA, Jallo J, Julien TD, Maserati MB, Nucci RC, O’Toole JE, Rosolowski
K, Sembrano JN, Villavicencio AT, Witt JP. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2016;16(3):439-448.
Meriggioli MN, Kordower JH. TDP-43 proteinopathy: aggregation and propagation in the pathogenesis of amyotrophic lateral sclerosis. Mov Disord. 2016;31(8):1139.
Mestre TA, van Duijn E, Davis AM, Bachoud-Lévi AC, Busse M, Anderson KE, Ferreira JJ, Mahlknecht P, Tumas V, Sampaio C, Goetz CG, Cubo E, Stebbins GT, Martinez-Martin P; Members of the MDS Committee on Rating Scales Development. Rating scales for behavioral symptoms in Huntington’s disease: critique and recommendations. Mov Disord. 2016;31(10): 1466-1478.
Mi Z, Halfter W, Abrahamson EE, Klunk WE, Mathis CA, Mufson EJ, Ikonomovic MD. Tenascin-C is associated with cored amyloid-β plaques in Alzheimer disease and pathology burdened cognitively normal elderly. J Neuropathol Exp Neurol. 2016;75(9):868-876.
Miskin DP, Chalkias SG, Dang X , Bord E, Batson S, Koralnik IJ. Interleukin-7 treatment of PML in a patient with idiopathic lymphocytopenia. Neurol Neuroimmunol Neuroinflamm. 2016;3(2):e213.
Miskin DP, Herman ST, Ngo LH, Koralnik IJ. Predictors and characteristics of seizures in survivors of progressive multifocal leukoencephalopathy. J Neurovirol. 2016;22(4):464-471.
Miskin DP, Ngo LH, Koralnik IJ. Diagnostic delay in progressive multifocal leukoencephalopathy. Ann Clin Transl Neurol. 2016;3(5):386-391.
Miskin DP, Saadi A, Chikoya L, Sloane JA, Koralnik IJ, Siddiqi OK. Challenges in the diagnosis and treatment of CNS demyelinating disorders in Zambia. Mult Scler J Exp Transl Clin. 2016;2:2055217316657117.
Mocco J, Zaidat OO, von Kummer R, Yoo AJ, Gupta R, Lopes D, Frei D, Shownkeen H, Budzik R, Ajani ZA, Grossman A, Altschul D, McDougall C, Blake L, Fitzsimmons BF, Yavagal D, Terry J, Farkas J, Lee SK, Baxter B, Wiesmann M, Knauth M, Heck D, Hussain S, Chiu D, Alexander MJ, Malisch T, Kirmani J, Miskolczi L, Khatri P; THERAPY Trial Investigators. Aspiration thrombectomy after intravenous alteplase versus intravenous alteplase alone. Stroke. 2016;47(9):2331-2338.
Modi KK, Rangasamy SB, Dasarathi S, Roy A, Pahan K. Cinnamon converts poor learning mice to good learners: implications for memory improvement. J Neuroimmune Pharmacol. 2016;11(4):693-707.
Montine TJ, Monsell SE, Beach TG, Bigio EH, Bu Y, Cairns NJ, Frosch M, Henriksen J, Kofler J, Kukull WA, Lee EB, Nelson PT, Schantz AM, Schneider JA, Sonnen JA, Trojanowski JQ, Vinters HV, Zhou XH, Hyman BT. Multisite assessment of NIA-AA guidelines for the neuropathologic evaluation of Alzheimer’s disease. Alzheimers Dement. 2016;12(2):164-169.
Morris MC, Brockman J, Schneider JA, Wang Y, Bennett DA, Tangney CC, van de Rest O. Association of seafood consumption, brain mercury level, and APOE ε4 status with brain neuropathology in older adults. JAMA. 2016;315(5):489-497.
Mufson EJ, Ikonomovic MD, Counts SE, Perez SE, Malek-Ahmadi M, Scheff SW, Ginsberg SD. Molecular and cellular pathophysiology of preclinical Alzheimer’s disease. Behav Brain Res. 2016;311:54-69.

Mufson EJ, Malek-Ahmadi M, Perez SE, Chen K. Braak staging, plaque pathology, and APOE status in elderly persons without cognitive impairment. Neurobiol Aging. 2016;37:147-153.
Mufson EJ, Malek-Ahmadi M, Snyder N, Ausdemore J, Chen K, Perez SE. Braak stage and trajectory of cognitive decline in noncognitively impaired elders. Neurobiol Aging. 2016;43:101-110.
Mufson EJ, Perez SE, Nadeem M, Mahady L, Kanaan NM, Abrahamson EE, Ikonomovic MD, Crawford F, Alvarez V, Stein T, McKee AC. Progression of tau pathology within cholinergic nucleus basalis neurons in chronic traumatic encephalopathy: a Chronic Effects of Neurotrauma Consortium study. Brain Inj. 2016;30(12):1399-1413.
Mummaneni PV, Park P, Fu KM, Wang MY, Nguyen S, Lafage V, Uribe JS, Ziewacz J, Terran J, Okonkwo DO, Anand N, Fessler R, Kanter AS, LaMarca F, Deviren V, Bess RS, Schwab FJ, Smith JS, Akbarnia BA, Mundis GM Jr, Shaffrey CI; International Spine Study Group. Does minimally invasive percutaneous posterior instrumentation reduce risk of proximal junctional kyphosis in adult spinal deformity surgery? a propensity-matched cohort analysis. Neurosurgery. 2016;78(1):101-108.
Nadimpalli SB, Cleland CM, Hutchinson MK, Islam N, Barnes LL, Van Devanter N. The association between discrimination and the health of Sikh Asian Indians. Health Psychol. 2016;35(4):351-355.
Nazari P, Kasliwal MK, Wewel JT, Dua SG, Chen M. Delayed intracerebral hemorrhage from a pseudoaneurysm following a depressed skull fracture. Neurointervention. 2016;11(1):42-45.
Nunley PD, Fessler RG, Park P, Zavatsky JM, Mundis GM, Uribe JS, Eastlack R, Nguyen S, Chou D, Wang MY, Anand N, Kanter AS, Shaffrey CI, Mummaneni PV; International Spine Study Group. 371 How do case type, length of stay, and comorbidities affect Medicare diagnosis-related group reimbursement for minimally invasive surgery for deformity? Neurosurgery. 2016;63(suppl 1):210.
Okbay A, Baselmans BM, De Neve JE, Turley P, Nivard MG, Fontana MA, Meddens SF, Linnér RK, Rietveld CA, Derringer J, Gratten J, Lee JJ, Liu JZ, de Vlaming R, Ahluwalia TS, Buchwald J, Cavadino A, Frazier-Wood AC, Furlotte NA, Garfield V, Geisel MH, Gonzalez JR, Haitjema S, Karlsson R, van der Laan SW, Ladwig KH, Lahti J, van der Lee SJ, Lind PA, Liu T, Matteson L, Mihailov E, Miller MB, Minica CC, Nolte IM, Mook-Kanamori D, van der Most PJ, Oldmeadow C, Qian Y, Raitakari O, Rawal R, Realo A, Rueedi R, Schmidt B, Smith AV, Stergiakouli E, Tanaka T, Taylor K, Wedenoja J, Wellmann J, Westra HJ, Willems SM, Zhao W; LifeLines Cohort Study, Amin N, Bakshi A, Boyle PA, Cherney S, Cox SR, Davies G, Davis OS, Ding J, Direk N, Eibich P, Emeny RT, Fatemifar G, Faul JD, Ferrucci L, Forstner A, Gieger C, Gupta R, Harris TB, Harris JM, Holliday EG, Hottenga JJ, De Jager PL, Kaakinen MA, Kajantie E, Karhunen V, Kolcic I, Kumari M, Launer LJ, Franke L, Li-Gao R, Koini M, Loukola A, Marques-Vidal P, Montgomery GW, Mosing MA, Paternoster L, Pattie A, Petrovic KE, Pulkki-Råback L, Quaye L, Räikkönen K, Rudan I, Scott RJ, Smith JA, Sutin AR, Trzaskowski M, Vinkhuyzen AE, Yu L, Zabaneh D, Attia JR, Bennett DA, Berger K, Bertram L, Boomsma DI, Snieder H, Chang SC, Cucca F, Deary IJ, van Duijn CM, Eriksson JG, Bültmann U, de Geus EJ, Groenen PJ, Gudnason V, Hansen T, Hartman CA, Haworth CM, Hayward C, Heath AC, Hinds DA, Hyppönen E, Iacono WG, Järvelin MR, Jöckel KH, Kaprio J, Kardia SL, Keltikangas-Järvinen L, Kraft P, Kubzansky LD, Lehtimäki T, Magnusson PK, Martin NG, McGue M, Metspalu A, Mills M, de Mutsert R, Oldehinkel AJ, Pasterkamp G, Pedersen NL, Plomin R, Polasek O, Power C, Rich SS, Rosendaal FR, den Ruijter HM, Schlessinger D, Schmidt H, Svento R, Schmidt R, Alizadeh BZ, Sørensen TI, Spector TD, Steptoe A, Terracciano A, Thurik AR, Timpson NJ, Tiemeier H,
Uitterlinden AG, Vollenweider P, Wagner GG, Weir DR, Yang J, Conley DC, Smith GD, Hofman A, Johannesson M, Laibson DI, Medland SE, Meyer MN, Pickrell JK, Esko T, Krueger RF, Beauchamp JP, Koellinger PD, Benjamin DJ, Bartels M, Cesarini D. Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet. 2016;48(6):624-633.
Okbay A, Beauchamp JP, Fontana MA, Lee JJ, Pers TH, Rietveld CA, Turley P, Chen GB, Emilsson V, Meddens SF, Oskarsson S, Pickrell JK, Thom K, Timshel P, de Vlaming R, Abdellaoui A, Ahluwalia TS, Bacelis J, Baumbach C, Bjornsdottir G, Brandsma JH, Pina Concas M, Derringer J, Furlotte NA, Galesloot TE, Girotto G, Gupta R, Hall LM, Harris SE, Hofer E, Horikoshi M, Huffman JE, Kaasik K, Kalafati IP, Karlsson R, Kong A, Lahti J, van der Lee SJ, deLeeuw C, Lind PA, Lindgren KO, Liu T, Mangino M, Marten J, Mihailov E, Miller MB, van der Most PJ, Oldmeadow C, Payton A, Pervjakova N, Peyrot WJ, Qian Y, Raitakari O, Rueedi R, Salvi E, Schmidt B, Schraut KE, Shi J, Smith AV, Poot RA, St Pourcain B, Teumer A, Thorleifsson G, Verweij N, Vuckovic D, Wellmann J, Westra HJ, Yang J, Zhao W, Zhu Z, Alizadeh BZ, Amin N, Bakshi A, Baumeister SE, Biino G, Bønnelykke K, Boyle PA, Campbell H, Cappuccio FP, Davies G, De Neve JE, Deloukas P, Demuth I, Ding J, Eibich P, Eisele L, Eklund N, Evans DM, Faul JD, Feitosa MF, Forstner AJ, Gandin I, Gunnarsson B, Halldórsson BV, Harris TB, Heath AC, Hocking LJ, Holliday EG, Homuth G, Horan MA, Hottenga JJ, de Jager PL, Joshi PK, Jugessur A, Kaakinen MA, Kähönen M, Kanoni S, Keltigangas-Järvinen L, Kiemeney LA, Kolcic I, Koskinen S, Kraja AT, Kroh M, Kutalik Z, Latvala A, Launer LJ, Lebreton MP, Levinson DF, Lichtenstein P, Lichtner P, Liewald DC; LifeLines Cohort Study, Loukola A, Madden PA, Mägi R, Mäki-Opas T, Marioni RE, Marques-Vidal P, Meddens GA, McMahon G, Meisinger C, Meitinger T, Milaneschi Y, Milani L, Montgomery GW, Myhre R, Nelson CP, Nyholt DR, Ollier WE, Palotie A, Paternoster L, Pedersen NL, Petrovic KE, Porteous DJ, Räikkönen K, Ring SM, Robino A, Rostapshova O, Rudan I, Rustichini A, Salomaa V, Sanders AR, Sarin AP, Schmidt H, Scott RJ, Smith BH, Smith JA, Staessen JA, Steinhagen-Thiessen E, Strauch K, Terracciano A, Tobin MD, Ulivi S, Vaccargiu S, Quaye L, van Rooij FJ, Venturini C, Vinkhuyzen AA, Völker U, Völzke H, Vonk JM, Vozzi D, Waage J, Ware EB, Willemsen G, Attia JR, Bennett DA, Berger K, Bertram L, Bisgaard H, Boomsma DI, Borecki IB, Bültmann U, Chabris CF, Cucca F, Cusi D, Deary IJ, Dedoussis GV, van Duijn CM, Eriksson JG, Franke B, Franke L, Gasparini P, Gejman PV, Gieger C, Grabe HJ, Gratten J, Groenen PJ, Gudnason V, van der Harst P, Hayward C, Hinds DA, Hoffmann W, Hyppönen E, Iacono WG, Jacobsson B, Järvelin MR, Jöckel KH, Kaprio J, Kardia SL, Lehtimäki T, Lehrer SF, Magnusson PK, Martin NG, McGue M, Metspalu A, Pendleton N, Penninx BW, Perola M, Pirastu N, Pirastu M, Polasek O, Posthuma D, Power C, Province MA, Samani NJ, Schlessinger D, Schmidt R, Sørensen TI, Spector TD, Stefansson K, Thorsteinsdottir U, Thurik AR, Timpson NJ, Tiemeier H, Tung JY, Uitterlinden AG, Vitart V, Vollenweider P, Weir DR, Wilson JF, Wright AF, Conley DC, Krueger RF, Davey Smith G, Hofman A, Laibson DI, Medland SE, Meyer MN, Yang J, Johannesson M, Visscher PM, Esko T, Koellinger PD, Cesarini D, Benjamin DJ. Genome-wide association study identifies 74 loci associated with educational attainment. Nature. 2016;533(7604):539-542.
O’Keefe JA, Robertson-Dick EE, Hall DA, Berry-Kravis E. Gait and functional mobility deficits in fragile X-associated tremor/ataxia syndrome. Cerebellum. 2016;15(4):475-482.
Pal GD, Hall D, Ouyang B, Phelps J, Alcalay R, Pauciulo MW, Nichols WC, Clark L, Mejia-Santana H, Blasucci L, Goetz CG, Comella C, Colcher A, Gan-Or Z, Rouleau GA, Marder K; Consortium on Risk for Early Onset Parkinson’s Disease (CORE-PD) Investigators. Genetic and clinical predictors of deep brain
Publications (2016) /// 49

50 /// THE 2017 RUSH NEUROSCIENCE REVIEW
stimulation in young-onset Parkinson’s disease. Mov Disord Clin Pract. 2016;3(5):465-471.
Pal G, O’Keefe J, Robertson-Dick E, Bernard B, Anderson S, Hall D. Global cognitive function and processing speed are associated with gait and balance dysfunction in Parkinson’s disease. J Neuroeng Rehabil. 2016;13(1):94.
Park P, Okonkwo DO, Nguyen S, Mundis GM Jr, Than KD, Deviren V, La Marca F, Fu KM, Wang MY, Uribe JS, Anand N, Fessler R, Nunley PD, Chou D, Kanter AS, Shaffrey CI, Akbarnia BA, Passias PG, Eastlack RK, Mummaneni PV; International Spine Study Group. Can a minimal clinically important difference be achieved in elderly patients with adult spinal deformity who undergo minimally invasive spinal surgery? World Neurosurg. 2016;86:168-172.
Park P, Wang MY, Nguyen S, Mundis GM Jr, La Marca F, Uribe JS, Anand N, Okonkwo DO, Kanter AS, Fessler R, Eastlack RK, Chou D, Deviren V, Nunley PD, Shaffrey CI, Mummaneni PV; International Spine Study Group. Comparison of complications and clinical and radiographic outcomes between nonobese and obese patients with adult spinal deformity undergoing minimally invasive surgery. World Neurosurg. 2016;87:55-60.
Patel ND, Broderick DF, Burns J, Deshmukh TK, Fries IB, Harvey HB, Holly L, Hunt CH, Jagadeesan BD, Kennedy TA, O’Toole JE, Perlmutter JS, Policeni B, Rosenow JM, Schroeder JW, Whitehead MT, Cornelius RS, Corey AS. ACR Appropriateness Criteria low back pain. J Am Coll Radiol. 2016;13(9):1069-1078.
Perez SE, Sherwood CC, Cranfield MR, Erwin JM, Mudakikwa A, Hof PR, Mufson EJ. Early Alzheimer’s disease-type pathology in the frontal cortex of wild mountain gorillas (Gorilla beringei beringei). Neurobiol Aging. 2016;39:195-201.
Perlman A, Shah RC, Bennett DA, Buchman AS, Matok I. Antihypertensive and statin medication use and motor function in community-dwelling older adults. J Am Med Dir Assoc. 2016;17(3):220-224.
Plonsker J, Tan LA, Munoz LF. Post-operative intracranial hemorrhage related to using t-PA for declotting an occluded hemodialysis catheter: a cautionary tale. J Clin Neurosci. 2016;32:145-147.
Pool LR, Weuve J, Wilson RS, Bültmann U, Evans DA, Mendes de Leon CF. Occupational cognitive requirements and late-life cognitive aging. Neurology. 2016;86(15):1386-1392.
Porto GB, Tan LA, Kasliwal MK, Traynelis VC. Progressive Brown-Séquard syndrome: a rare manifestation of cervical disc herniation. J Clin Neurosci. 2016;29:196-198.
Postuma RB, Berg D, Adler CH, Bloem BR, Chan P, Deuschl G, Gasser T, Goetz CG, Halliday G, Joseph L, Lang AE, Liepelt-Scarfone I, Litvan I, Marek K, Oertel W, Olanow CW, Poewe W, Stern M. The new definition and diagnostic criteria of Parkinson’s disease. Lancet Neurol. 2016;15(6):546-548.
Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G. Abolishing the 1-year rule: how much evidence will be enough? Mov Disord. 2016;31(11):1623-1627.
Powers BE, Velazquez R, Kelley CM, Ash JA, Strawderman MS, Alldred MJ, Ginsberg SD, Mufson EJ, Strupp BJ. Attentional function and basal forebrain cholinergic neuron morphology during aging in the Ts65Dn mouse model of Down syndrome. Brain Struct Funct. 2016;221(9):4337-4352.
Qureshi T, Chaus F, Fogg L, Dasgupta M, Straus D, Byrne RW. Learning curve for the transsphenoidal endoscopic endonasal approach to pituitary tumors. Br J Neurosurg. 2016;30(6):637-642.
Rabie A, Verhagen Metman L, Fakhry M, Eassa AY, Fouad W, Shakal A, Slavin KV. Improvement of advanced Parkinson’s disease manifestations with deep brain stimulation of the subthalamic nucleus: a single institution experience. Brain Sci. 2016;6(4):E58.
Rabie A, Verhagen Metman L, Slavin KV. Using “functional” target coordinates of the subthalamic nucleus to assess the indirect and direct methods of the preoperative planning: do the anatomical and functional targets coincide? Brain Sci. 2016;6(4):E65.
Radue EW, Sprenger T, Vollmer T, Giovannoni G, Gold R, Havrdova E, Selmaj K, Stefoski D, You X, Elkins J. Daclizumab high-yield process reduced the evolution of new gadolinium-enhancing lesions to T1 black holes in patients with relapsing-remitting multiple sclerosis. Eur J Neurol. 2016;23(2):412-415.
Raj T, Chibnik LB, McCabe C, Wong A, Replogle JM, Yu L, Gao S, Unverzagt FW, Stranger B, Murrell J, Barnes L, Hendrie HC, Foroud T, Krichevsky A, Bennett DA, Hall KS, Evans DA, De Jager PL. Genetic architecture of age-related cognitive decline in African Americans. Neurol Genet. 2016;3(1):e125.
Rajan KB, Aggarwal NT, Schneider JA, Wilson RS, Everson-Rose SA, Evans DA. Role of APOE ε4 allele and incident stroke on cognitive decline and mortality. Alzheimer Dis Assoc Disord. 2016;30(4):318-323.
Rajan KB, Arvanitakis Z, Lynch EB, McAninch EA, Wilson RS, Weuve J, Barnes LL, Bianco AC, Evans DA. Cognitive decline following incident and preexisting diabetes mellitus in a population sample. Neurology. 2016;87(16):1681-1687.
Raman J, Ballal A, Hota B, Mirza S, Lai D, Bleck T, Lateef O. Reconstructive valve surgery within 10 days of stroke in endocarditis. Asian Cardiovasc Thorac Ann. 2016;24(6):523-529.
Raper DM, Webster Crowley R, Liu KC, Starke RM. Endovascular techniques and devices for the treatment of intracranial aneurysms: a review of neurointerventional outcomes. J Neurosurg Sci. 2016;60(1):104-115.
Robertson EE, Hall DA, McAsey AR, O’Keefe JA. Fragile X-associated tremor/ataxia syndrome: phenotypic comparisons with other movement disorders. Clin Neuropsychol. 2016;30(6):849-900.
Rossi MA. Planning resective surgery using structural connectivity modeling: the next-generation presurgical evaluation. Epilepsy Curr. 2016;16(3):150-152.
Rossi PJ, Gunduz A, Judy J, Wilson L, Machado A, Giordano JJ, Elias WJ, Rossi MA, Butson CL, Fox MD, McIntyre CC, Pouratian N, Swann NC, de Hemptinne C, Gross RE, Chizeck HJ, Tagliati M, Lozano AM, Goodman W, Langevin JP, Alterman RL, Akbar U, Gerhardt GA, Grill WM, Hallett M, Herrington T, Herron J, van Horne C, Kopell BH, Lang AE, Lungu C, Martinez-Ramirez D, Mogilner AY, Molina R, Opri E, Otto KJ, Oweiss KG, Pathak Y, Shukla A, Shute J, Sheth SA, Shih LC, Steinke GK, Tröster AI, Vanegas N, Zaghloul KA, Cendejas-Zaragoza L, Verhagen L, Foote KD, Okun MS. Proceedings of the Third Annual Deep Brain Stimulation Think Tank: a review of emerging issues and technologies. Front Neurosci. 2016;10:119.
Roth CJ, Angevine PD, Aulino JM, Berger KL, Choudhri AF, Fries IB, Holly LT, Kendi AT, Kessler MM, Kirsch CF, Luttrull MD, Mechtler LL, O’Toole JE, Sharma A, Shetty VS, West OC, Cornelius RS, Bykowski J. ACR Appropriateness Criteria myelopathy. J Am Coll Radiol. 2016;13(1):38-44.
50 /// THE 2017 RUSH NEUROSCIENCE REVIEW

Publications (2016) /// 51
Roy A. Targeting BPOZ-2 in Lewy body disease. Neural Regen Res. 2016;11(6):910-911.
Roy A, Kundu M, Jana M, Mishra RK, Yung Y, Luan CH, Gonzalez FJ, Pahan K. Identification and characterization of PPARα ligands in the hippocampus. Nat Chem Biol. 2016;12(12):1075-1083.
Roy A, Rangasamy SB, Kundu M, Pahan K. BPOZ-2 gene delivery ameliorates alpha-synucleinopathy in A53T transgenic mouse model of Parkinson’s disease. Sci Rep. 2016;6:22067.
Sadleir KR, Kandalepas PC, Buggia-Prévot V, Nicholson DA, Thinakaran G, Vassar R. Presynaptic dystrophic neurites surrounding amyloid plaques are sites of microtubule disruption, BACE1 elevation, and increased Aβ generation in Alzheimer’s disease. Acta Neuropathol. 2016;132(2):235-256.
Sajeev G, Weuve J, Jackson JW, VanderWeele TJ, Bennett DA, Grodstein F, Blacker D. Late-life cognitive activity and dementia: a systematic review and bias analysis. Epidemiology. 2016;27(5):732-742.
Salehi A, Ashford JW, Mufson EJ. The link between Alzheimer’s disease and Down syndrome: a historical perspective. Curr Alzheimer Res. 2016;13(1):2-6.
Samartzis D, Gillis CC, Shih P, O’Toole JE, Fessler RG. Intramedullary spinal cord tumors, II: management options and outcomes. Global Spine J. 2016;6(2):176-185.
Scheff SW, Ansari MA, Mufson EJ. Oxidative stress and hippocampal synaptic protein levels in elderly cognitively intact individuals with Alzheimer’s disease pathology. Neurobiol Aging. 2016;42:1-12.
Schneider JA. The cerebral cortex in cerebral amyloid angiopathy. Lancet Neurol. 2016;15(8):778-779.
Sherman MA, LaCroix M, Amar F, Larson ME, Forster C, Aguzzi A, Bennett DA, Ramsden M, Lesné SE. Soluble conformers of Aβ and tau alter selective proteins governing axonal transport. J Neurosci. 2016;36(37):9647-9658.
Shulman LM, Armstrong M, Ellis T, Gruber-Baldini A, Horak F, Nieuwboer A, Parashos S, Post B, Rogers M, Siderowf A, Goetz CG, Schrag A, Stebbins GT, Martinez-Martin P. Disability rating scales in Parkinson’s disease: critique and recommendations. Mov Disord. 2016;31(10):1455-1465.
Sikazwe I, Elafros MA, Bositis CM, Siddiqi OK, Koralnik IJ, Kalungwana L, Theodore WH, Okulicz JF, Potchen MJ, Birbeck GL. HIV and new onset seizures: slipping through the cracks in HIV care and treatment. HIV Med. 2016;17(2):118-123.
Simpson DM, Hallett M, Ashman EJ, Comella CL, Green MW, Gronseth GS, Armstrong MJ, Gloss D, Potrebic S, Jankovic J, Karp BP, Naumann M, So YT, Yablon SA. Practice guideline update summary: botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016;86(19):1818-1826.
Sivam A, Wroblewski KE, Alkorta-Aranburu G, Barnes LL, Wilson RS, Bennett DA, Pinto JM. Olfactory dysfunction in older adults is associated with feelings of depression and loneliness. Chem Senses. 2016;41(4):293-299.
Song S, Fonarow GC, Olson DM, Liang L, Schulte PJ, Hernandez AF, Peterson ED, Reeves MJ, Smith EE, Schwamm LH, Saver JL. Association of Get With The Guidelines-Stroke program participation and clinical outcomes for Medicare beneficiaries with ischemic stroke. Stroke. 2016;47(5):1294-1302.
Starke RM, Turk A, Ding D, Crowley RW, Liu KC, Chalouhi N, Hasan DM, Dumont AS, Jabbour P, Durst CR, Turner RD. Technology developments in endovascular treatment of intracranial aneurysms. J Neurointerv Surg. 2016;8(2):135-144.
Stoeckel LE, Arvanitakis Z, Gandy S, Small D, Kahn CR, Pascual-Leone A, Pawlyk A, Sherwin R, Smith P. Complex mechanisms linking neurocognitive dysfunction to insulin resistance and other metabolic dysfunction [version 2]. F1000Res. 2016;5:353.
Strupp BJ, Powers BE, Velazquez R, Ash JA, Kelley CM, Alldred MJ, Strawderman M, Caudill MA, Mufson EJ, Ginsberg SD. Maternal choline supplementation: a potential prenatal treatment for Down syndrome and Alzheimer’s disease. Curr Alzheimer Res. 2016;13(1):97-106.
Tan LA, Chen M, Muñoz LF. Utility of dual-energy CT in differentiating contrast extravasation from intracranial hematoma [letter]. J Neurosurg. 2016;124(1):279-280.
Tan LA, Harbhajanka A, Kasliwal MK, Nag S, Munoz LF. Giant trichilemmal cyst of the scalp. Neurol India. 2016;64(2):357-358.
Tan LA, Kasliwal MK, Munoz LF. Ventriculoperitoneal shunt failure presenting as isolated unilateral abducens nerve palsy. J Emerg Med. 2016;50(1):e31-e32.
Tan LA, Lopes DK, Munoz LF, Shah Y, Bhabad S, Jhaveri M, Moftakhar R. Minimally invasive evacuation of intraventricular hemorrhage with the Apollo vibration/suction device. J Clin Neurosci. 2016;27:53-58.
Tan LA, Syed S, Arvanitis LD, Munoz LF. Calcifying pseudoneoplasm of the superior medullary velum: an unusual location for a rare lesion. Neurol India. 2016;64(1):185-186.
Than KD, Park P, Fu KM, Nguyen S, Wang MY, Chou D, Nunley PD, Anand N, Fessler RG, Shaffrey CI, Bess S, Akbarnia BA, Deviren V, Uribe JS, La Marca F, Kanter AS, Okonkwo DO, Mundis GM Jr, Mummaneni PV; International Spine Study Group. Clinical and radiographic parameters associated with best versus worst clinical outcomes in minimally invasive spinal deformity surgery. J Neurosurg Spine. 2016;25(1):21-25.
Tiernan CT, Ginsberg SD, Guillozet-Bongaarts AL, Ward SM, He B, Kanaan NM, Mufson EJ, Binder LI, Counts SE. Protein homeostasis gene dysregulation in pretangle-bearing nucleus basalis neurons during the progression of Alzheimer’s disease. Neurobiol Aging. 2016;42:80-90.
Tison F, Keywood C, Wakefield M, Durif F, Corvol JC, Eggert K, Lew M, Isaacson S, Bezard E, Poli SM, Goetz CG, Trenkwalder C, Rascol O. A phase 2A trial of the novel mGluR5-negative allosteric modulator dipraglurant for levodopa-induced dyskinesia in Parkinson’s disease. Mov Disord. 2016;31(9):1373-1380.
Tosto G, Bird TD, Bennett DA, Boeve BF, Brickman AM, Cruchaga C, Faber K, Foroud TM, Farlow M, Goate AM, Graff-Radford NR, Lantigua R, Manly J, Ottman R, Rosenberg R, Schaid DJ, Schupf N, Stern Y, Sweet RA, Mayeux R; National Institute on Aging Late-Onset Alzheimer Disease/National Cell Repository for Alzheimer Disease (NIA-LOAD/NCRAD) Family Study Group. The role of cardiovascular risk factors and stroke in familial Alzheimer disease. JAMA Neurol. 2016;73(10):1231-1237.
Turk AS, Johnston SC, Hetts S, Mocco J, English J, Murayama Y, Prestigiacomo CJ, Lopes D, Gobin YP, Carroll K, McDougall C. Geographic differences in endovascular treatment and retreatment of cerebral aneurysms. AJNR Am J Neuroradiol. 2016;37(11):2055-2059.
Publications (2016) /// 51

52 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Turner AD, Lim AS, Leurgans SE, Bennett DA, Buchman AS, Barnes LL. Self-reported sleep in older African Americans and white Americans. Ethn Dis. 2016;26(4):521-528.
Upadhyay R, Bleck TP, Busl KM. Hyperammonemia: what urea-lly need to know: case report of severe noncirrhotic hyperammonemic encephalopathy and review of the literature. Case Rep Med. 2016;2016:8512721.
Valenca GT, Srivastava GP, Oliveira-Filho J, White CC, Yu L, Schneider JA, Buchman AS, Shulman JM, Bennett DA, De Jager PL. The role of MAPT haplotype H2 and isoform 1N/4R in parkinsonism of older adults. PLoS One. 2016;11(7):e0157452.
van de Rest O, Wang Y, Barnes LL, Tangney C, Bennett DA, Morris MC. APOE ε4 and the associations of seafood and long-chain omega-3 fatty acids with cognitive decline. Neurology. 2016;86(22):2063-2070.
van Karnebeek CD, Bowden K, Berry-Kravis E. Treatment of neurogenetic developmental conditions: from 2016 into the future. Pediatr Neurol. 2016;65:1-13.
Vargas A, Dixit KS, Quigley JG, Testai FD. Spinal cord and cranial Bing-Neel syndrome complicated by cerebral ischemia: a case report. J Neurol Sci. 2016;366:44-46.
Vargas A, Gorelick PB, Testai FD. Progressive central nervous system vasculopathy in sarcoidosis: a case report. J Neurol Sci. 2016;362:153-154.
Verhagen Metman L, Pal G, Slavin K. Surgical treatment of Parkinson’s disease. Curr Treat Options Neurol. 2016;18(11):49.
Visootsak J, Kidd SA, Anderson T, Bassell JL, Sherman SL, Berry-Kravis EM. Importance of a specialty clinic for individuals with fragile X syndrome. Am J Med Genet A. 2016;170(12):3144-3149.
Weiss A, Baselmans BM, Hofer E, Yang J, Okbay A, Lind PA, Miller MB, Nolte IM, Zhao W, Hagenaars SP, Hottenga JJ, Matteson LK, Snieder H, Faul JD, Hartman CA, Boyle PA, Tiemeier H, Mosing MA, Pattie A, Davies G, Liewald DC, Schmidt R, De Jager PL, Heath AC, Jokela M, Starr JM, Oldehinkel AJ, Johannesson M, Cesarini D, Hofman A, Harris SE, Smith JA, Keltikangas-Järvinen L, Pulkki-Råback L, Schmidt H, Smith J, Iacono WG, McGue M, Bennett DA, Pedersen NL, Magnusson PK, Deary IJ, Martin NG, Boomsma DI, Bartels M, Luciano M. Personality polygenes, positive affect, and life satisfaction. Twin Res Hum Genet. 2016;19(5):407-417.
Weiss A, Mirelman A, Giladi N, Barnes LL, Bennett DA, Buchman AS, Hausdorff JM. Transition between the Timed Up and Go turn to sit subtasks: is timing everything? J Am Med Dir Assoc. 2016;17(9):864.e9-864.e15.
Weuve J, Kaufman JD, Szpiro AA, Curl C, Puett RC, Beck T, Evans DA, Mendes de Leon CF. Exposure to traffic-related air pollution in relation to progression in physical disability among older adults. Environ Health Perspect. 2016;124(7):1000-1008.
Wewel JT, Harbhajanka A, Kasliwal MK, Ahuja SK, Loew JM, Fontes RB. Post-transplant lymphoproliferative disorder of the cervical spine mimicking an epidural abscess. J Clin Neurosci. 2016;29:175-178.
Wewel JT, Kumar V, Kasliwal MK, Fontes RB. Coexistent panspinal subdural abscess and isolated leptomeningeal myeloma relapse presenting as rapid-onset paraparesis. J Emerg Med. 2016;51(6):729-731.
Wewel JT, Mangubat EZ, Patil J, Abraham KP, Sani S. Intradural benign epithelioid schwannoma of the lumbar spine. Neurol India. 2016;64(6):1340-1341.
Wewel JT, Nunna RS, Tan LA, Kasliwal MK, O’Toole JE. Novel reconstruction of the anterior craniocervical junction using an expandable cage with integrated fixation after total C2 spondylectomy for chordoma. J Clin Neurosci. 2016;30:157-160.
Wheeler AC, Sideris J, Hagerman R, Berry-Kravis E, Tassone F, Bailey DB Jr. Developmental profiles of infants with an FMR1 premutation. J Neurodev Disord. 2016;8:40.
Wilson RS, Boyle PA, Capuano AW, Shah RC, Hoganson GM, Nag S, Bennett DA. Late-life depression is not associated with dementia-related pathology. Neuropsychology. 2016;30(2):135-142.
Wilson RS, Capuano AW, Bennett DA, Schneider JA, Boyle PA. Temporal course of neurodegenerative effects on cognition in old age. Neuropsychology. 2016;30(5):591-599.
Wilson RS, Capuano AW, Marquez DX, Amofa P, Barnes LL, Bennett DA. Change in cognitive abilities in older Latinos. J Int Neuropsychol Soc. 2016;22(1):58-65.
Wilson RS, Rajan KB, Barnes LL, Weuve J, Evans DA. Factors related to racial differences in late-life level of cognitive function. Neuropsychology. 2016;30(5):517-524.
Wilson RS, Sytsma J, Barnes LL, Boyle PA. Anosognosia in dementia. Curr Neurol Neurosci Rep. 2016;16(9):77.
Wüthrich C, Batson S, Anderson MP, White LR, Koralnik IJ. JC virus infects neurons and glial cells in the hippocampus. J Neuropathol Exp Neurol. 2016;75(8):712-717.
Xue Y, Ratushny V, Koralnik IJ, Schlaug G, Wu PA. Allergic dermatitis caused by endovascular coiling of brain aneurysm. Dermatitis. 2016;27(3):149-150.
Yi J, Zielinski D, Chen M. Cerebral aneurysm size before and after rupture: case series and literature review. J Stroke Cerebrovasc Dis. 2016;25(5):1244-1248.
Yu L, Chibnik LB, Yang J, McCabe C, Xu J, Schneider JA, De Jager PL, Bennett DA. Methylation profiles in peripheral blood CD4+ lymphocytes versus brain: the relation to Alzheimer’s disease pathology. Alzheimers Dement. 2016;12(9):942-951.
Zhang J, Wang S, Huang W, Bennett DA, Dickson DW, Wang D, Wang R. Tissue transglutaminase and its product isopeptide are increased in Alzheimer’s disease and APPswe/PS1dE9 double transgenic mice brains. Mol Neurobiol. 2016;53(8):5066-5078. //
52 /// THE 2017 RUSH NEUROSCIENCE REVIEW

Research Grants (2016) /// 53
Select Research Grants (2016)
Department of Neurological SciencesAntoaneta Balabanov, MD
• Outcomes and Management of Dietary Treatments of Epilepsy
• Impact of a Low-Carbohydrate, High-Fat Diet on Epileptic Seizures, Gut Milieu, and Metabolic Health
• Epilepsy After the Implantation of a Vagal Nerve Stimulator (VNS)
Brandon Barton, MD
• Impulse Control Disorders in Parkinson’s Disease: Prevalence and Clinical Features in the Rush University Medical Center Movement Disorders Clinic
Adriana Bermeo-Ovalle, MD
• Use of EEG in Patients With Intracerebral Hemorrhage
Bryan Bernard, PhD
• Correlation of MDS-UPDRS Nonmotor Symptoms With Cognitive Functioning in Parkinson’s Disease
Torrey Boland Birch, MD
• Predictors of Outcome in HSV Encephalitis
Cynthia Comella, MD
• Dystonia Coalition Project 1: Natural History and Biospecimen Repository for Dystonia
• Study of Tozadenant as Adjunct Therapy in Levodopa-Treated Patients With PD Experiencing End of Dose “Wearing-Off”
• RTT150 for Injection in Isolated Cervical Dystonia
• ParkinStim: Transcranial Direct Current Stimulation for PD
• Study of Perampanel (E2007) in Subjects With Cervical Dystonia (SAFE-Per CD)
• Diagnostic and Rating Tools for Blepharospasm
• RE-024 for the Treatment of Pantothenate Kinase-Associated Neurodegeneration
• Neuroimaging Biomarkers in Parkinsonism: Differentiating Subtypes and Tracking Disease Progression
James Conners, MD
• Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) Trial
• RESPECT ESUS: Randomized Evaluation in Secondary Stroke Prevention Comparing the Thrombin Inhibitor Dabigatran Etexilate Versus ASA in Embolic Stroke of Undetermined Source
• ARAMIS: Addressing Real World Anticoagulant Management Issues in Stroke
Rima Dafer, MD
• Study to Assess the Safety, Pharmacokinetics, and Pharmacodynamics of DS-1040b in Subjects With Acute Ischemic Stroke
Rajeev Garg, MD
• Prospective Neurosciences Intensive Care Unit Outcomes Research Database
• Assessment of Cerebral Blood Flow by Quantitative Perfusion MRI in Patients With Spontaneous Intracerebral Hemorrhage and Its Effect on DWI Abnormalities
• Retrospective Acute Spontaneous Intracerebral Hemorrhage Data Abstraction
• The Effect of Diffusion Weighted Imaging (DWI) Lesion on Global Cognitive Outcomes in Patients With Primary Spontaneous Intracerebral Hemorrhage
Christopher Goetz, MD
• Topiramate as an Adjunct to Amantadine in the Treatment of Dyskinesia in Parkinson’s Disease
• Study of Urate-Elevating Inosine Treatment to Slow Clinical Decline in Early Parkinson’s Disease
• Validation of the Movement Disorders Society PD Diagnostic Criteria
• APL-130277 in Levodopa Responsive Patients With Parkinson’s Disease Complicated by Motor Fluctuations (“OFF” Episodes)
• Comparing the Efficacy and Safety of Gastric Retentive, Controlled Release Accordion Pill Carbidopa/Levodopa (AP-CD/LD) to Immediate Release CD/LD in Fluctuating PD Patients
• Evaluating the Long-Term Effects of AP-CD/LD in Fluctuating Parkinson’s Disease Subjects Who Completed Study IN 11 004
Jennifer Goldman, MD, MS
• Fox Investigation for New Discovery for Biomarkers (Biofind)
• Clinical and Neuroimaging Predictors of Cognitive Decline in Parkinson’s Disease
• Study of 5-HT6/5-HT2A in the SYNAPSE Parkinson’s Disease Dementia Trial
• Evaluation of the Parkinson’s Disease Psychosis Virtual Reality Simulator Experience
• Study of RVT-101 in Subjects With Dementia With Lewy Bodies (DLB)
• Dementia With Lewy Bodies Consortium
• Mild Cognitive Impairment and Endurance Exercise in Parkinson’s Disease
• Genetic Risk Factors for Cognitive Impairment in Parkinson's Disease
• Validation of the Movement Disorders Society Criteria for Mild Cognitive Impairment in Parkinson’s Disease
• Parkinson’s Disease, Alpha-Synuclein and Cognitive Decline
• Apathy as a Predictor of Executive Function in Parkinson’s Disease Patients
• Psychosis in Parkinson’s Disease Symptom Identification Tool
• Serotonin Gene Polymorphisms (5-HT6 and 5-HT2A) and Parkinson’s Disease Cognitive Impairment
• Gender Differences in Motor and Non-Motor Features and Dopamine Transporter Imaging in Parkinson’s Disease
• Developing T Cell-Based Biomarkers for Autoimmunity in Parkinson’s Disease
• Improving the Detection of Early Parkinson’s Disease
• Cultural Differences in Japanese and American Populations in the Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale
54 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Deborah A. Hall, MD, PhD
• The Role of Antisense FMR1 in the Development of Fragile X-Associated Tremor/Ataxia Syndrome
• Next Generation Sequencing in Parkinson Disease and Aging
• Citicoline for Neurological Signs in Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS)
• Human Blood to Brain Dopamine Neuron Project
• CVT 301 (Levodopa Inhalation Powder) in Parkinson’s Disease Patients With Motor Response Fluctuations (OFF Phenomena)
• Clinical Phenotype of Parkinson’s Disease in African Americans
• Assessment of ABBV-8E12 in Progressive Supranuclear Palsy
• Evaluation of SAGE-217 in the Treatment of Subjects With Essential Tremor (ET)
• Next Generation Sequencing in Parkinson’s Disease and Aging
• Study of ABBV-8E12 in Progressive Supranuclear Palsy
• Genetic Determinants for Age of Parkinson Disease Onset
Michael Ko, MD
• Study of Montelukast on Gastrointestinal Tolerability in Patients With Relapsing Forms of Multiple Sclerosis Receiving Tecfidera (Dimethyl Fumarate) Delayed-Release Capsules
• Intravenous Infusion Study of rHIgM22 in Patients With Multiple Sclerosis Immediately Following a Relapse
• Study of Tysabri in Early RRMS in Anti-JCV Antibody Negative Patients
Aikaterini Kompoliti, MD
• Multidisciplinary Inpatient Rehabilitation for Functional Movement Disorders
• Study of Isradipine as a Disease Modifying Agent in Patients With Early Parkinson’s Disease (STEADY-PD III)
• Study of SD-809 (Deutetrabenazine) for the Treatment of Moderate to Severe Tardive Dyskinesia
• Clinical Study of Patients With Symptomatic Neurogenic Orthostatic Hypotension to Assess Sustained Effects of Droxidopa Therapy
• Study of NBI-98854 for the Treatment of Subjects With Tourette Syndrome
Igor Koralnik, MD
• Virus Detection in Patients With Neurological Disorders and Infections
• Epidemiological Studies in Patients With Neurologic Disorders
• Role of Inflammation in Progressive Multifocal Leukoencephalopathy
• Cohort of HIV-Associated Seizures and Epilepsy in Zambia (CHASE): Scale Up and Expansion Informed by R21 Findings
• Cellular Auto-Immune Mechanisms of Narcolepsy
• JC Virus infection of Choroid Plexi and Meninges of Patients With Progressive Multifocal Leukoencephalopathy, JC Virus Granule Cell Neuronopathy, and JC Virus Encephalopathy, and Control Subjects
• Pathogenesis of a JC Virus Variant in Pyramidal Neurons
Jeffrey Kordower, PhD
• Developing a Human ES Cell-Derived Dopamine Neuron Source for Cell Therapy in Parkinson’s Disease
• Implantable Photo-Stimulation System for the Treatment of Parkinson’s Disease
• Evaluation of Alpha-Synuclein Immunohistochemical Methods for the Detection of Lewy-Type Synucleinopathy in Gastrointestinal Biopsies
• Transplantation of Cryopreserved iPSC-Derived Dopamine Neurons for Parkinson’s Disease
• Nortriptyline-Mediated Attenuation of Alpha-Synuclein Pathology in Parkinson’s Disease
• RNAi Therapy for Spinocerebellar Ataxia Type 1
• Human iPSC-Based Personalized Cell Therapy of PD
George Lopez, MD
• Survey on the Use of Hypothermia for Cardiac Arrest Survivors and Updates After Recent Published Trial Results
• INTREPID: Impact of Fever Prevention in Brain Injured Patients
• ESCAPE: Intravenous NA-1 in Subjects With Acute Ischemic Stroke Undergoing Endovascular Thrombectomy
• ACDC: Assessment of Complications Following Decompressive Craniectomy
• Minimally Invasive Surgery Plus Rt-Pa in the Treatment of Intracerebral Hemorrhage
• iDEF Trial: Futility Study of Deferoxamine Mesylate in Intracerebral Hemorrhage
• Comparing EG-1962 to Standard of Care Oral Nimodipine in Adults With Aneurysmal Subarachnoid Hemorrhage
• ASTROH: Aneurysmal Subarachnoid Hemorrhage Trial Randomizing Heparin
Rabia Malik, MD
• Validation of the CAP-PRI (Chronic Acquired Polyneuropathy-Patient Reported Index)
Daniel Nicholson, PhD
• Computational Neurobiology of Hippocampal Dendrites
Rebecca O’Dwyer, MD
• Study of Brivaracetam Administered Intravenously as Treatment for Increased Seizure Activity in an Epilepsy Monitoring Unit Setting
• A Comparison of Epilepsy Surgery Outcomes in Younger and Older Patients
• Characterization of Epilepsy Patients Through the Use of Enhanced Neuroimaging Analysis
• Investigation of Depression and Anxiety in Older Adults With Epilepsy
Nicholas Osteraas, MD
• Predictors of Follow-Up Post-Stroke
Kalipada Pahan, PhD
• Characterizing Novel Hippocampal Drugs for Alzheimer’s Disease
• Identifying Novel PPAR Ligands From Cerebellum
• Dose Reporting Study of Gemfibrozil and Vitamin A Following Oral Administration to Cin2 (+/-) Mice
• PPAR-alpha in APP Metabolism

Research Grants (2016) /// 55
Gian Pal, MD
• Analysis and Follow-Up on CORE-PD Study
• Technology-Based Tools to Assess Gait After Deep Brain Stimulation in Parkinson’s Disease
• Interest in Genetic Testing in Parkinson’s Disease Patients Receiving Deep Brain Stimulation
• Quantitative Motion Analysis to Characterize the Motor Phenotype of GBA Mutation Carriers With PD
• Comparison of Striatal Dopamine Levels in DBS and Non-DBS Subjects With Parkinson’s Disease
• Parkinson’s Disease and DBS: Cognitive Effects in GBA Mutation Carriers
• Determining the Microbiota Composition of the Middle Meatus in Early Parkinson’s
Clement Pillainayagam, MD
• DCVax-L, Autologous Dendritic Cells Pulsed With Tumor Lysate Antigen for the Treatment of Glioblastoma Multiforme (GBM)
• A071101: Heat Shock Protein-Peptide Complex-96 (HSPPC-96) Vaccine Given With Bevacizumab vs Bevacizumab Alone in the Treatment of Surgically Resectable Recurrent Glioblastoma Multiforme (GBM)
• Veliparib or Placebo in Combination With Adjuvant Temozolomide in Newly Diagnosed Glioblastoma With MGMT Promoter Hypermethylation
Sebastian Pollandt, MD
• Study of SAGE-547 Injection in the Treatment of Subjects With Super-Refractory Status Epilepticus
• Outcomes in Subdural Hematoma: Experience From a Tertiary Referral Center
Lubov Romantseva, MD
• Perampanel as Adjunctive Treatment in Subjects at Least 2 Years of Age With Inadequately Controlled Seizures Associated With Lennox-Gastaut Syndrome
Marvin Rossi, MD, PhD
• Developing an “Activation Function-Dependent” Intra-Operative Depth Lead Guidance System for Direct Neuromodulation Therapy in Patients With Refractory Focal-Onset Epilepsy: A BodyTom CT and O-Arm Comparison
• Interfacing a Mobile Health Delivery Model for Rural Patients With Refractory Epilepsy
• Interfacing a Mobile Health Delivery Model for Pediatric Patients With Refractory Epilepsy
• RNS System Post-Approval Study in Epilepsy
Sarah Song, MD
• The Cardiovascular Health in Asian Elderly Study
• PRISMS Study – Alteplase in Patients With Mild Stroke: Rapidly Improving Symptoms and Minor Neurological Deficits
Glenn Stebbins, PhD
• A New Rating Scale for Focal Task-Specific Dystonia of the Musician’s Hand
• Furst 2.0 Rating Scale
Dusan Stefoski, MD
• Ofatumumab vs Teriflunomide in Patients With Relapsing Multiple Sclerosis
• Siponimod (BAF312) in Patients With Secondary Progressive Multiple Sclerosis
Travis Stoub, PhD
• Prediction of Surgical Outcomes After Epilepsy Surgery Using MEG EEG Source Localization
• Brain Network Activation Analysis in Epilepsy
• Complementary Nature of MEG, EEG and SISCOM in Epilepsy
• Markers for Depression and Anxiety in Epilepsy
Leonard Verhagen Metman, MD, PhD
• Analysis of Stereotactic Accuracy of Deep Brain Stimulation Electrode Implantation Using Leksell Frame and Nexframe
• Effect of Unilateral and Bilateral STN Stimulation on Eye-Hand Coordination
• Product Surveillance Registry Base Protocol
• Study of Apomorphine Administered by Continuous Subcutaneous Infusion in Advanced Parkinson’s Disease Patients With Unsatisfactory Control on Available Therapy
• PF-06649751 in Subjects With Motor Fluctuations Due to Parkinson’s Disease
• Study of Droxidopa in the Treatment of Parkinson’s Disease
• PF-06649751 in Subjects With Early-Stage Parkinson’s Disease
• Post Market Clinical Follow-Up Evaluating the Infinity Deep Brain Stimulation Implantable Pulse Generator System (PROGRESS Study)
56 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Department of Neurological SurgeryRichard Byrne, MD
• A Retrospective Review on Cortical Stimulation Mapping Techniques in Brain Tumor Patients
• A Retrospective Review of Meningioma Surgery Clinical Outcomes
• Evaluation of Cognitive Function From Subdural Electrodes in Patients Considered as Surgical Candidates for Intractable Epilepsy
• Predictors of Surgical Corridors to the Suprasellar Space
• Temporal Lobectomy, Memory, Sleep, and Dreams
Michael Chen, MD
• DAWN Trial: Diffusion Weighted Imaging (DWI) or Computerized Tomography Perfusion (CTP) Assessment With Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention (DAWN)
• Estrogen Therapy as Prevention in the Progression of Aneurysm (EPPA) Trial
• Post-Aneurysm SAH Memory Loss
R. Webster Crowley, MD
• ARTISSE: Aneurysm Treatment Using Intrasaccular Flow Diversion With the Artisse Device
Harel Deutsch, MD
• A Concurrently Controlled Study of the LimiFlex Paraspinous Tension Band in the Treatment of Lumbar Degenerative Spondylolisthesis With Spinal Stenosis
• Activ-L Lumbar Artificial Disc Trial
• LIFT: Lumbar Interbody Fusion Trial
• Safety and Efficacy of Staphylococcus Aureus Vaccine in Adults Undergoing Elective Posterior Instrumented Lumbar Spinal Fusion Procedures
Richard Fessler, MD, PhD
• A Multi-Center, Randomized, Controlled Study to Evaluate the Safety and Effectiveness of AlloStem vs Non-Cellular Allograft Bone in Single and 2-Level Anterior Cervical Discectomy and Fusion
• Asterias Stem Cell Treatment for SCI: Long Term Follow-Up
• Expectations and Outcomes: MIS vs Open
• Minimally Invasive Surgery for the Treatment of Adult Spinal Deformity: A Multicenter Retrospective Study
• Prospective, Multi-Center Minimally Invasive Adult Spinal Deformity Outcomes Database Registry
• Radiographic Findings After Anterior Cervical Discectomy and Fusion With Translational and Rigid Plating System
Demetrius Lopes, MD
• ANSWER: Adjunctive Neurovascular Support for Wide-Neck Aneurysm Embolization and Reconstruction
• ATLAS: Safety and Effectiveness of the Treatment of Wide-Neck, Saccular Intracranial Aneurysms With the Neuroform Atlas Stent System
• BARREL: Study of the Reverse Medical Barrel® Vascular Reconstruction Device (VRD) for Adjunctive Treatment to Embolic Coils for Wide-Neck, Intracranial, Bifurcating/Branching Aneurysms of Middle Cerebral and Basilar Arteries
• FRED - Flow Re-Direction Endoluminal Device: Pivotal Study of the MicroVention Flow Re-Direction Endoluminal Device Stent System in the Treatment of Intracranial Aneurysms
• PREMIER Trial: Prospective Study on Embolization of Intracranial Aneurysms With Pipeline Embolization Device
• SCENT Trial: The Surpass IntraCranial Aneurysm Embolization System Pivotal Trial to Treat Large or Giant Wide-Neck Aneurysms
• WEB-IT: The WEB Intrasaccular Therapy Study
John O’Toole, MD, MS
• MTRON: Metastatic Tumor Research and Outcome Network
Sepehr Sani, MD
• Accuracy of Intraoperative CT in Deep Brain Stimulation and Responsive Neurostimulation Surgeries
• High Order Spectral Analysis of Local Field Potential Data in Parkinson’s Disease
• INTREPID: Implantable Neurostimulator for the Treatment of Parkinson’s Disease
• Reclaim DBS for Obsessive Compulsive Disorder (OCD) Therapy
• The Effect of Vancomycin Powder on Surgical Site Infections in Deep Brain Stimulation Surgery
• TrueBeam for the Treatment of Trigeminal Neuralgia
Vincent Traynelis, MD
• Assessment of Peri-Operative Morbidity and Mortality Following Anterior-Posterior Cervical Spine Decompression and Fusion
• Critical Analysis of Extubation Parameters for Patients Undergoing Combined Anterior-Posterior Cervical Spine Surgery
• Critical Analysis of Tracheoesophageal Bundle Retraction Force Pre- and Post-Section of the Omohyoid Muscle During Anterior Cervical Spine Surgery
• Cervical Radiographic Parameters in 1 and 2 Level Anterior Cervical Discectomy and Fusion
• Hyperlordotic Cornerstone Graft Study
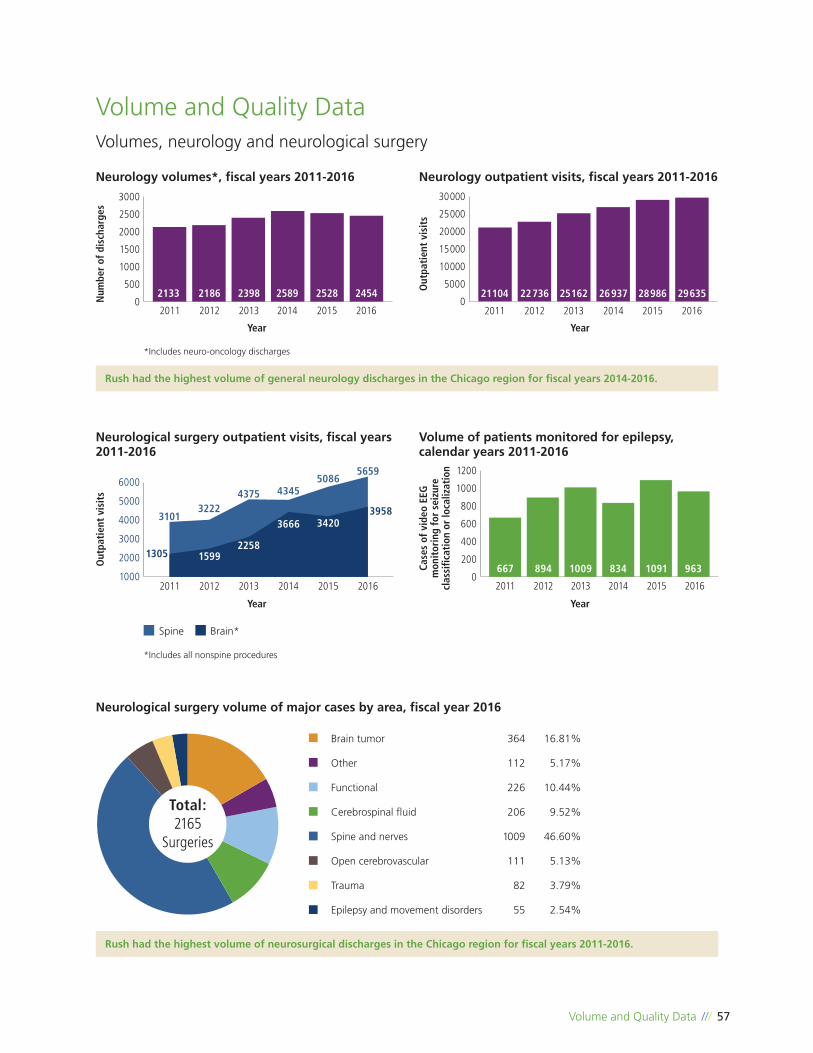
Volume and Quality Data /// 57
0
200
400
600
800
1000
1200
667 894 1009 834 1091 963
2011 2012 2013 2014 2015 2016
Neurological surgery volume of major cases by area, fiscal year 2016
Total:2165
Surgeries
Volume and Quality Data
0
500
1000
1500
2000
2500
3000
2133 2186 2398 2589 2528 2454
2011 2012 2013 2014 2015 2016
Num
ber
of d
isch
arge
s
Out
pati
ent
visi
ts
Year Year
Neurology volumes*, fiscal years 2011-2016 Neurology outpatient visits, fiscal years 2011-2016
Rush had the highest volume of general neurology discharges in the Chicago region for fiscal years 2014-2016.
*Includes neuro-oncology discharges
0
5000
10000
15000
20000
25000
30000
21104 22736 25162 26937 28986 29635
2011 2012 2013 2014 2015 2016
Volumes, neurology and neurological surgery
1000
2000
3000
4000
5000
60005659
3958
1305
32224375 4345
5086
3101
2011 2012 2013 2014 2015 2016
2258
3666 3420
1599
Out
pati
ent
visi
ts
Case
s of
vid
eo E
EG
mon
itor
ing
for
seiz
ure
clas
sific
atio
n or
loca
lizat
ion
Year Year
Neurological surgery outpatient visits, fiscal years 2011-2016
Volume of patients monitored for epilepsy, calendar years 2011-2016
*Includes all nonspine procedures
Spine Brain*
Rush had the highest volume of neurosurgical discharges in the Chicago region for fiscal years 2011-2016.
Brain tumor 364 16.81%
Other 112 5.17%
Functional 226 10.44%
Cerebrospinal fluid 206 9.52%
Spine and nerves 1009 46.60%
Open cerebrovascular 111 5.13%
Trauma 82 3.79%
Epilepsy and movement disorders 55 2.54%
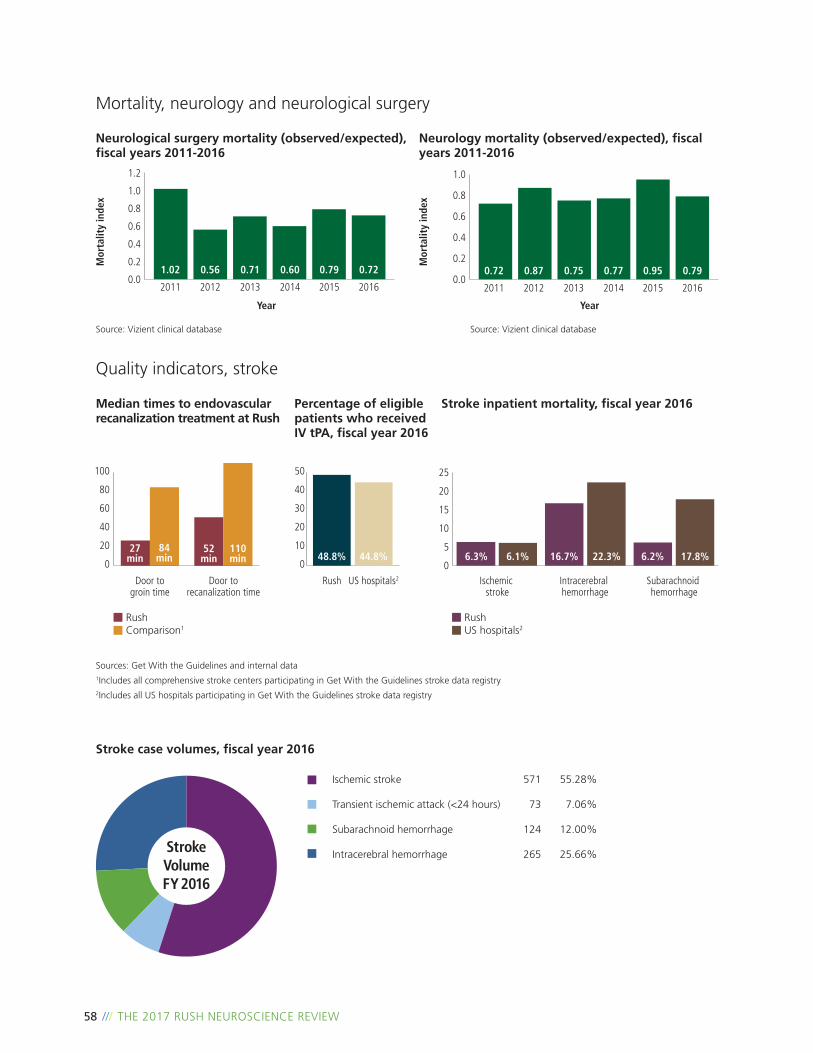
58 /// THE 2017 RUSH NEUROSCIENCE REVIEW
0.0
0.2
0.4
0.6
0.8
1.0
0.72 0.87 0.75 0.77 0.95 0.79
2011 2012 2013 2014 2015 20160.0
0.2
0.4
0.6
0.8
1.0
1.2
1.02 0.56 0.71 0.60 0.79 0.72
2011 2012 2013 2014 2015 2016
Stroke case volumes, fiscal year 2016
StrokeVolumeFY 2016
Ischemic stroke 571 55.28%
Transient ischemic attack (<24 hours) 73 7.06%
Subarachnoid hemorrhage 124 12.00%
Intracerebral hemorrhage 265 25.66%
Year Year
Mor
talit
y in
dex
Mor
talit
y in
dex
Neurological surgery mortality (observed/expected), fiscal years 2011-2016
Source: Vizient clinical database Source: Vizient clinical database
Mortality, neurology and neurological surgery
Neurology mortality (observed/expected), fiscal years 2011-2016
Sources: Get With the Guidelines and internal data1Includes all comprehensive stroke centers participating in Get With the Guidelines stroke data registry2Includes all US hospitals participating in Get With the Guidelines stroke data registry
Median times to endovascular recanalization treatment at Rush
Percentage of eligible patients who received IV tPA, fiscal year 2016
Stroke inpatient mortality, fiscal year 2016
0
5
10
15
20
25
Ischemic stroke
Intracerebral hemorrhage
Subarachnoid hemorrhage
RushUS hospitals2
RushComparison1
6.3% 6.2%
Door torecanalization time
Door to groin time
16.7%6.1% 22.3% 17.8%0
20
40
60
80
100
27 min
84 min
52 min 0
10
20
30
40
50
Rush US hospitals2
44.8%48.8%110 min
Quality indicators, stroke

Game-Changers
The rapid development of new therapies is giving hope to people with multiple sclerosis—and Rush specialists are among those leading the way
As recently as 40 years ago, people diagnosed with multiple sclerosis (MS) were almost entirely at the mercy of
the disease: There were no proven medical interventions that could halt or slow the progression, or even improve
symptoms. People with the most severe forms faced certain debility, often in the prime of their lives.
That was the landscape of MS when Dusan Stefoski, MD, completed his residency at what was then Rush-Presbyterian-
St Luke’s Medical Center and signed on to the Rush Multiple Sclerosis Center. Four decades later, that landscape is
unrecognizable—thanks in large part to the pioneering efforts of Stefoski, now the center’s director, and his Rush
colleagues, past and present.
One of those colleagues is Michael Ko, MD, who also trained at Rush before joining Stefoski in practice. Ko recently
sat down with his mentor to talk about the rapid evolution of MS treatment, and Rush’s vital role in bringing a slew
of promising therapies to the market.
Dusan Stefoski, MD (right), and Michael Ko, MD, are committed to bringing novel therapies and forward-thinking, decisive treatment strategies to their patients at the Rush Multiple Sclerosis Center.
Interview: Game-Changers /// 59

60 /// THE 2017 RUSH NEUROSCIENCE REVIEW
Ko: You first started working with MS patients in 1977. How would you describe the state of MS treatment at that time?
Stefoski: It could best be described as underdeveloped. There was only 1 FDA-approved treatment for MS, adrenocorticotropic hormone (ACTH)—which stimulates the adrenal gland cortex to secrete cortisol and aldosterone, among others, in addition to possibly having a direct ameliorating effect on the immune system. ACTH had some efficacy in terms of speeding up the recovery from acute relapses of MS. But it had no proven efficacy over the long run; it didn’t change the course of the disease.
Ko: There wasn’t another option until Betaseron (interferon beta-1b) was approved in 1993. When you started using it, what was the impact of that medicine?
Stefoski: The impact was relatively modest. People were excited because there was finally a new drug for treatment of MS that held a promise of modest benefit over time. But the availability was initially rather limited, so relatively few people received the drug, and even those who received it often did not experience much in the way of benefit.
But 3 years later, the next interferon, Avonex (interferon beta-1a), was approved. Technically speaking, it showed better long-term efficacy than Betaseron, and Avonex actually began to change the way people felt, meaning they improved some over the long run. We were instrumental in collaborative research to develop Avonex.
Ko: You and your colleagues were also involved in the clinical trials for Tysabri (natalizumab). Was that considered a game-changer when it was approved in 2004?
Stefoski: It was a dramatic game-changer, because that treatment really could halt the disease process in a way that we had not seen before. And it could stop further progression in many people—not all of them, but a large majority of people with MS experienced improvements within the first few months of treatment.
Ko: We’ve treated a lot of people with Tysabri at Rush. Do you think that experience—the high volume of patients—has contributed to a better understanding of how it’s used?
Stefoski: Our initial contribution with Tysabri was collaboratively instrumental in demonstrating its efficacy, because we were part of the phase III trial. But since 2012, we have published a series of pioneering reports on the management of one of the major potential complications of treatment with Tysabri: progressive multifocal leukoencephalopathy (PML), a rare infection of the brain caused by the JC virus. The JC virus is not actually related to MS or to Tysabri. Many healthy people harbor the normally rather innocuous JC virus. However, in people with MS who
have the JC virus, treatment with Tysabri creates a situation that allows the virus to establish itself in the brain and cause PML, which can be severely incapacitating or even fatal.
We were the first in the world—and you were part of that whole process—to develop a novel protocol for early detection and treatment for MS patients who contracted PML in association with Tysabri. We monitor patients both clinically and with brain MRI at 3-4 month intervals, which enables early detection of PML and allows for better management outcomes. Our groundbreaking approach consists of accelerated elimination of the JC virus by stimulating the person’s own immune system with filgrastim (G-CSF, Neupogen). This reduces the damage and fosters a faster recovery. Furthermore, we were the first to also administer maraviroc (Selzentry), an antiretroviral that modulates immune T-cell recruitment, in PML patients.
As reported, there were no fatalities among the PML patients we treated, which is significant in that PML used to be considered a fatal disease.
Ko: There has been recent interest in high-dose chemotherapy and hematopoietic stem cell transplantation, or bone marrow transplantation, at Rush and other institutions. What has been your experience with this approach?
Stefoski: High-dose chemotherapy is a very powerful treatment for MS. It is considered induction therapy, because it has an immediate effect of completely stopping the disease process, which can last for quite a while. Although this approach was conceived elsewhere some time ago, we were among the first in the world to start using it, and to date we’ve treated more than 30 patients with excellent results.
As for stem cell transplantation in MS, the treatment is very high-dose chemotherapy using a powerful anti-cancer medication such as cyclophosphamide (Cytoxan), though other drugs or combinations of drugs have been used at other institutions. Chemotherapy is effective for MS and other autoimmune diseases because it kills the attacking cells, but unfortunately, it also kills healthy cells. The patient’s immune system is nearly destroyed and has to be reconstituted, which is achieved by giving them back their own saved bone marrow stem cells, either autologous (their own marrow) or allogeneic (donor marrow). So the stem cells do not actually treat MS, they just restore the immune system that has been badly damaged by the chemo.
Ko: Do you consider high-dose chemo a cure?
Stefoski: No. Most of these people do well for an extended period, up to 5 years following the initiation of treatments, but 25-30 percent of patients begin to experience recurrence of MS at that point, albeit often in a milder form. And

Interview: Game-Changers /// 61
because it’s so harsh, it’s generally a once-in-a-lifetime therapy; if additional treatments are needed later, standard therapies are applied.
Ko: In March 2017, ocrelizumab (Ocrevus) became the 15th FDA-approved medication for MS, and Rush was the first center in Illinois and one of the first in the country to use it. It’s been receiving a lot of interest in the MS community. What do you expect to see from it?
Stefoski: It’s yet another game-changer for people with MS. It’s the first and only disease-modifying therapy for both primary progressive and relapsing forms of MS, and it has the potential to lead to new avenues of treatment for other diseases as well.
One interesting thing about it is that it treats MS in a way that we never considered would work. The approach is called anti B-cell therapy—Ocrevus is a monoclonal antibody that targets the CD20 molecule on the surface of B cells, allowing for their destruction. The traditional concept of the MS disease process is that T cells are the main culprits, but over the past few years the role of B cells has also emerged.
B cells are best known for their involvement in antibody production through plasma cell formation, but they are also
involved in other functions of the immune system, including directing the actions of their counterpart T cells. Research has shown that B cells can induce T cells to attack myelin though a process known as antigen presentation; that’s why eliminating B cells can be effective for MS. Ocrevus removes B cells that would have been bound for the nervous system to orchestrate inflammation.
What this means is that B cells are perhaps just as important as or even more important than T cells in MS. That’s a huge paradigm shift. Anti T-cell drugs do work in MS—cladribine is one such drug—but the vital role of B cells has now been established.
One of the most appealing and impressive facts about Ocrevus is that it’s administered to patients only twice a year, intravenously, in our offices. That is a tremendous benefit for patients.
Ko: Your research with Floyd Davis, MD, on dalfampridine (originally known as 4-AP) was truly groundbreaking. How did you start pursuing that line of research when there was not a lot of backing?
Stefoski: The initial discovery was really a theoretical one. Some of that work was done here at Rush, when it was realized that blocking the potassium channel on nerves damaged by MS could improve nerve signaling.
Because no two people experience MS in the same way, Dusan Stefoski, MD, and his colleagues at Rush build treatment plans around each patient's needs.

62 /// THE 2017 RUSH NEUROSCIENCE REVIEW
In MS, normal electrical nerve signaling fails because the stripping of myelin that coats the nerves leads to their short-circuiting, slowing and even completely blocking the signals. That’s why people with MS often develop their problems.
Theoretically, in early computer modeling, it was clear that if we could block the potassium channel, it should improve the signaling. But there were no known potassium channel-blocking drugs, or chemicals for that matter. It turns out that researchers at a physiology laboratory at Duke University had discovered, unrelated to MS, that this chemical known then as 4-aminopyridine (4-AP for short) was a potassium channel blocker on nerve fibers. They cataloged it as such, not anticipating any immediate therapeutic usefulness.
Our team at Rush was able to make the connection between our research and the discovery at Duke, and we began studying 4-AP, initially just in nerves and cells. It worked right away, so we quickly shifted into carefully structured human trials in the early 1980s. There was only one other team of researchers doing similar work, at the National Hospital of Neurology and Neurosurgery (aka Queen Square) in London. Their contemporaneous research looked very good in the laboratory, but their clinical results were unsuccessful, and they never pursued it any further. Ours were successful, and we pressed onward with our efforts that ultimately brought dalfampridine to the market as Ampyra.
Most of our research efforts with this project were funded through private philanthropic donations expressly to the Rush MS Center. Without those generous donations, our work would not have been possible because, as you mentioned, there was no backing from other sources.
Ko: What has been the impact of Ampyra in the MS world, and at Rush in general?
Stefoski: It’s the first and only drug in the history of neurology and MS that can help people who have MS walk better and faster, so it falls into the category of function-restoring drugs, not just symptom-relief drugs.
I’m emphasizing that distinction because while its effects are often misconstrued as symptom relief, Ampyra actually restores function. The difference is clear when we analyze the loosening of spastic muscles by the symptom-relief drug baclofen. Baclofen diminishes stiffness, which is beneficial; but it does not actually improve function in the damaged nerves. Ampyra enables patients to walk better and faster, because it restores the nerves’ ability to propagate impulses by making the signals longer and stronger.
Ampyra was the first commercially successful drug ever discovered at Rush, a fairly rare occurrence at any academic institution. Because of its international success, Ampyra has brought significant funds to Rush, which are being
reinvested into various research projects that could generate important discoveries.
Ko: One of the other medications used almost exclusively at Rush for MS is cladribine, a potent chemotherapy drug that’s being investigated as an oral medication. What is your experience with it? Could it eventually get approved in the US for MS?
Stefoski: I reckon that it will be. We have been the early proponents and prescribers of cladribine for MS, and it has proven efficacious in halting the destructive processes of MS and lowering the risk of disability progression. The original work was done at Scripps in California, but we may have been the second center in the world to start using it. We were part of the oral cladribine phase III trial, which almost led to its approval, but the company that created it, EMD Serono, did not pursue approval at that time. They are now rekindling their efforts to bring it to market in the US, and it was recently approved in Europe. I think it will be approved fairly quickly in the US because of the efficacy and safety demonstrated in multiple trials worldwide, which included our team at Rush.
Ko: Nerve regeneration using stem cell therapy is a very hot topic in the MS community. Do you see that coming to fruition anytime soon?
Bringing Ampyra, a drug that can improve walking for many people with MS, to the market in 2010 was a crowning achievement for Dusan Stefoski, MD, and his mentor Floyd Davis, MD.

Interview: Game-Changers /// 63
Stefoski: I do not. The problem with real stem cells is that we don’t know where they go and what they do once they’re put into people’s bodies, at least as far as MS is concerned. Other alleged “stem cell” treatments marketed for MS are actually high-dose chemotherapies, and with those therapies, stem cells serve only to rescue the immune system. The only systematic approach to the treatment of MS with stem cells was done in Israel, with modest benefit. We’re talking about adult mesenchymal stem cells, incidentally, not fetal stem cells. There has been no work with embryonic stem cells for MS.
Unfortunately, since the FDA has relaxed its regulation of adult stem cell treatment centers in the US, they have popped up all over the place. People are going and paying cash up front, but they don’t know what they’re getting. A person with MS is much better off going to a medical facility with a reputable MS center, where they can be properly evaluated and receive a proven treatment that might actually be of benefit.
Ko: What are the benefits of coming to the Rush MS Center specifically?
Stefoski: I think what differentiates Rush from other MS centers is that we have a tradition of and expertise in being proactive with treatments. It’s not unusual for people with MS to be treated with one drug for life even though they’re getting worse, because some centers don’t escalate treatments or think proactively and start with a high-potency treatment. At Rush, we take a proactive approach that is tailored to each person’s type of MS. And we don’t shy away from using a variety of cutting-edge or exclusively experimental treatments, when appropriate, in addition to some very powerful existing drugs that many other major MS centers in the region hardly ever use.
Ko: We are also comprehensive in the sense that we’re the only institution with an independent MS center. We don’t share space with other specialties, such as epilepsy or movement disorders. Our nurses are dedicated MS nurses, and we have dedicated office staff. We are not sharing resources.
Stefoski: That dedicated specialization is very important. Patients are always seeing the same MS center staff members, all of whom have expertise working with this population—from the first administrative contact to the final decision-making health care provider. We used to have a dedicated psychologist, physical therapist, and occupational therapist on our team. Our patients still have access to PT, OT, and psychology, because those disciplines exist within Rush University Medical Center, but the specialists themselves are not dedicated to MS. We hope to eventually return to that level of multidisciplinary care at our center, because that’s the approach preferred by both patients and our staff.
Ko: The Rush MS Center has been around for several decades and has a reputation as a leader in MS treatment and research. What does the future hold?
Stefoski: The biggest task now is expansion, to be able to accommodate the increasing numbers of patients receiving intravenous medications. There are 6 IV medications for MS that can be administered on an outpatient basis, so we recently began to expand our infusion facility as well our professional staff. As for research, we are embarking on testing of a few brand-new drugs, some of which have the potential to repair tissues damaged by MS.
Ko: Treatments have advanced significantly in a relatively short period of time.
Stefoski: About 25 years.
Ko: When you started out, did you think there would be this much progress so quickly?
Stefoski: I did, and that’s actually why I went into the field of MS—the potential for innovation was palpable. In 1977, when I was finishing my residency in neurology here at Rush, I was offered the opportunity to stay on by 3 sections within the Department of Neurological Sciences. The first was neuromuscular neurology, which was too intensely reliant on electromyography (EMG). The second was epilepsy, but back then EEGs (electroencephalograms) were these endless reams of paper that you had to read for hours on end. With MS, it was almost exclusively patient work, which I found very engaging. I also realized that I could learn a lot from Dr Floyd Davis, who was the founding director of the Rush MS Center and the only MS specialist in Chicago at that time. He was doing some really interesting MS-directed research, so I joined his team and our work evolved, leading to the development of Ampyra. It turns out I was correct in anticipating such progress.
Ko: Dr Davis taught you, and you, in turn, have taught me and my peers. When you decide to step away from practicing medicine, what will your legacy be?
Stefoski: I believe a legacy is something best left to objective observers to determine. But from a more subjective point of view, there are several things I’m extremely proud to be cultivating here at Rush and teaching to both current and prospective providers of expert MS care: the strong emphasis on compassionate, comprehensive patient care established by Dr Davis decades ago; a forward-thinking and decisive approach to treatment of people with MS; and a steadfast commitment to translational research, which has led—and will, I am confident, continue to lead—to the development of meaningful novel therapies for MS. //

For a patient consultation or referral to a neurologist at Rush, please
call (312) 942-4500. For a neurosurgeon at Rush, call (312) 942-6644.

PLEASE NOTE: All physicians featured in this publication are on the medical faculty of Rush University Medical Center. Some of the physicians featured are in private practice and,
as independent practitioners, are not agents or employees of Rush University Medical Center.
Rush University Medical Center1653 W. Congress Pkwy.
Chicago, IL 60612 www.rush.edu
M-4925 12/17
Photography by the Rush Photo Group and Kevin Horan
Rush is an academic health system comprising Rush University Medical Center,
Rush Copley Medical Center and Rush Oak Park Hospital.