Agasiev, A. (2018). Armenia in regional politics on post-soviet space. Orel.
Upload
king-saud-universityCategory
view
1.447download
0
ORIGINAL CONTRIBUTION earthquake; injury, prevention
The 1988 Earthquake in Soviet Armenia: A Case Study
A major earthquake devastated the Armenian Republic of the Soviet Union on December 7, 1988, resulting in thousands of deaths and injuries. In a postearthquake investigation of three towns seriously affected by the earthquake, we studied earthquake-related injury patterns, made obser- vations on rescue and medical efforts, and postulated certain factors asso- ciated with increased morbidity and mortality. Information was obtained from official Soviet documents, interviews with survivors of the earth- quake, and interviews with local, regional, and national government offi- cials. Figures were based on assessments made by these officials in the field in the immediate postearthquake period. Out of a population of 8,500, there were 4,202 (49.4%) deaths and 1,244 (14.6%) injured (casualty rate, 64.0%). Deaths and injuries were 67 and 11 times higher, respectively, among trapped than nontrapped victims. Being outside at the time of the earthquake or having escaped to the outside from the collapsing structure was crucial for survival. Among persons found alive, 89% were rescued during the first 24 hours, mostly without the use of heavy equipment. This observation underscores the importance of swift rescuer response. As with all field surveys after disasters, there were methodological limita- tions to this study due to chaotic postearthquake conditions. Accordingly, results must be approached with caution. Nonetheless, these preliminary observations are striking and have generated several new hypotheses for further investigations using more sophisticated analytic methods. [Noji EK, Kelen GD, Armenian HK, Oganessian A, Jones NP, Sivertson KT: The 1988 earthquake in Soviet Armenia: A case stud~z Ann Emerg Med August 1990;I9:891-897.]
I N T R O D U C T I O N During the past 20 years, earthquakes have caused more than a million
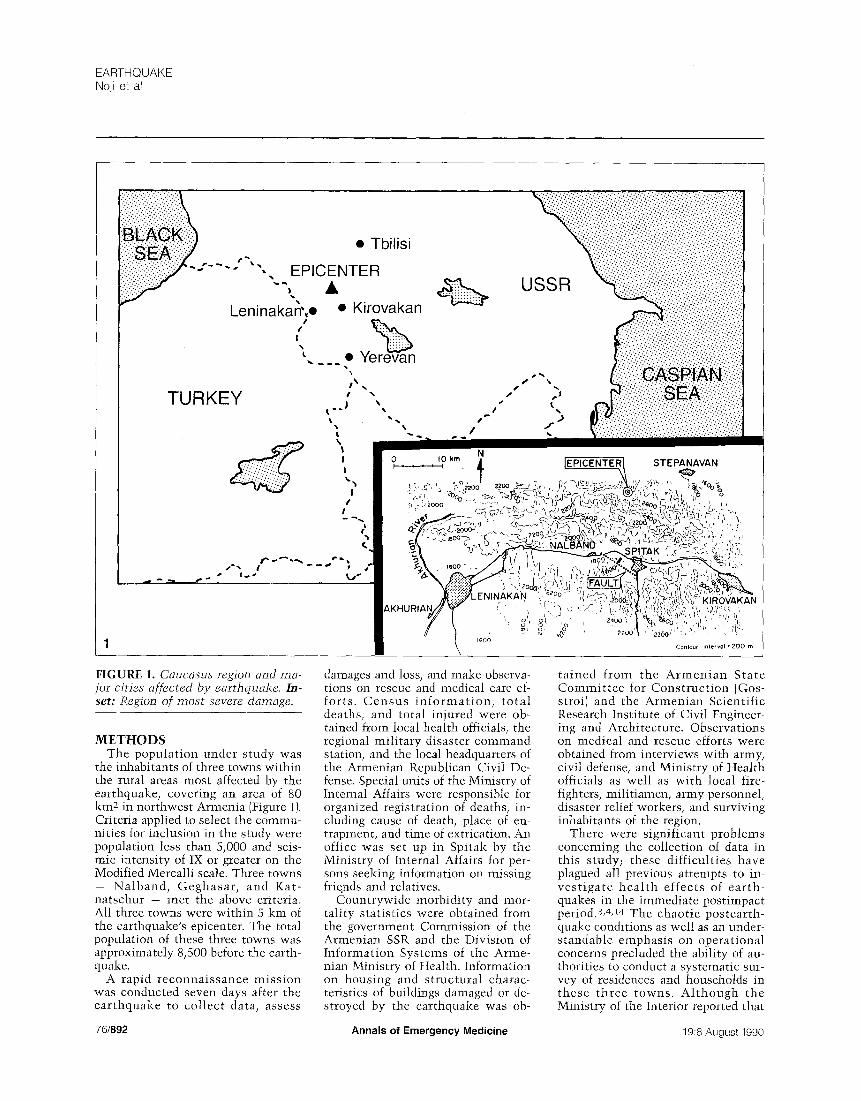
deaths worldwide. Better epidemiological knowledge of the causes of death and the type of injuries and illnesses caused by earthquakes is clearly es- sential for determining appropriate relief supplies, equipment, and person- nel. l-4 On December 7, 1988, an earthquake registering 6.9 on the Richter scale hit the northern part of the Armenian Soviet Socialist Republic, one of the most seismically active regions of the Soviet Union s-s {Figure 1). Caused by movement along a geological fault near the town of Spitak in the northwestern part of the country, the quake affected 40% of the na- tional territory.9,1o Of the 150 villages damaged, 58 were destroyed. A high percentage of Armenia's housing (11%) was destroyed or rendered uninhab- itable, and 500,000 to 700,000 persons were made homeless, t~ Bridges, life- lines (eg, water, power, gas, sewage systems), and industrial facilities were also severely damaged. 1~ The toll in human terms was devastating: approx- imately 40,000 persons were reported trapped in collapsed buildings - 15,000 were successfully rescued, and 25,000 bodies were recovered from the rubble. Another 31,000 were known to be injured, of whom 12,200 required hospitalization. ~ 1,13
We undertook this survey during the period immediately after the earth- quake to assess the epidemiologic impact of the disaster and to develop an understanding of the relationships among building characteristics, occu- pant actions, search and rescue, medical care, and patient outcome.
Eric K Noji, MD, MPH, FACEP* Gabor D Kelen, MD, FRCP(C), FACEP* Haroutune K Armenian, MD, DrPHt Baltimore, Maryland Ashot Oganessian, PhD§ Soviet Socialist Republic of Armenia, USSR Nicholas P Jones, PhD~ Keith T Sivertson, MD* Baltimore, Maryland
From the Department of Emergency Medicine, The Johns Hopkins Hospital and School of Medicine;* the Department of Epidemiology, School of Hygiene and Public Health,t and the Department of Civil Engineering]- The Johns Hopkins University, Baltimore, Maryland; and the Computer information Center, Ministry of Health, Soviet Socialist Republic of Armenia, USSR.§
Received for publication December 21, 1989. Accepted for publication March 5, 1990.
Presented at the Society for Academic Emergency Medicine Annual Meeting in San Diego, May 1989.
This study was supported by the National Center for Earthquake Engineering Research (Project No. 884005C), The Armenian Relief Society, and the Office of US Foreign Disaster Assistance/Agency for International Development.
Address for reprints: Eric K Noji, MD, MPH, FACER Department of Emergency Medicine, The Johns Hopkins Hospital, 600 N Wolfe Street, Baltimore, Maryland 212O5.
19:8 August 1990 Annals of Emergency Medicine 891/75
EARTHQUAKE Noji et al
• Tbilisi
. . . . EPICENTER
keninakan',• • Kirovakan
_ __ • Y e r e v a n \
¢ • . TURKEY ,--) ,,
w ! o
¢ l , ~ . , ;
£~-- .a,
USSR
s,•
a,.I
"" t
! •
N : . . . . ,o wm /0. IEPICENTER| STEPANAVAN
• ~ ,,
h: j ,oo I ,.
, o ) o { ~ z40~ ~ - - , ~6 , ' ' ,
/ / ~ , ~ o . 9 / . . . . " " , ' ~, '~' ' l ~ -
\ Conlou¢ 200 m
FIGURE 1. Caucasus region and ma- jor cities affected by earthquake. In- set: Region of most severe damage.
M E T H O D S
The population under study was the inhabitants of three towns within the rural areas most affected by the earthquake, covering an area of 80 km: in northwest Armenia (Figure 1). Criteria applied to select the commu- nities for inclusion in the study were population less than 5,000 and seis- mic intensity of IX or greater on the Modified Mercalli scale. Three towns - Nalband, Geghasar , and Kat- natschur - met the above criteria. All three towns were within 5 km of the earthquake's epicenter. The total population of these three towns was approximately 8,500 before the earth- quake.
A rapid reconnaissance mission was conducted seven days after the earthquake to collect data, assess
damages and loss, and make observa- tions on rescue and medical care ef- forts. Census i n fo rma t ion , to ta l deaths, and total injured were ob- tained from local health officials, the regional military disaster command station, and the local headquarters of the Armenian Republican Civil De- fense. Special units of the Ministry of Internal Affairs were responsible for organized registration of deaths, in- cluding cause of death, place of en- trapment, and time of extrication. An office was set up in Spitak by the Ministry of Internal Affairs for per- sons seeking information on missing friends and relatives.
Countrywide morbidity and mor- tality statistics were obtained from the government Commission of the Armenian SSR and the Division of Information Systems of the Arme- nian Ministry of Health. Information on housing and structural charac- teristics of buildings damaged or de- stroyed by the earthquake was oh-
tained from the Armen ian State Commit tee for Construct ion (Gos- stroi) and the Armenian Scientific Research Institute of Civil Engineer- ing and Architecture. Observations on medical and rescue efforts were obtained from interviews with army, civil defense, and Ministry of Health officials as well as with local fire- fighters, militiamen, army personnel, disaster relief workers, and surviving inhabitants of the region.
There were significant problems concerning the collection of data in this study; these difficulties have plagued all previous attempts to in- ves t igate heal th effects of earth- quakes in the immediate postimpact period.3,4,14 The chaotic postearth- quake conditions as well as an under- standable emphasis on operational concerns precluded the ability of au- thorities to conduct a systematic sur- vey of residences and households in these three towns. Al though the Ministry of the Interior reported that
76/892 Anna ls of Emergency Medic ine 19:8 August 1990

TABLE 1. Location of individuals and entrapment status: Association w~th death and injury
Location of Individuals
Outside
Inside
Unknown
Total
Nontrapped Persons
q-rapped Persons
CL, confidence interval.
Relative Risk Population Deaths (%) (95% CI) Survivors Injured (%)
651 8.8 1.0 594 1.7
7,120 55.1 6.3 (5.4-7.4) 3,197 36.3
729 30.5 507 14.6
8,500 49.4 4,298 28.9
3,390 1.2 1.0 3,349 8.8
5,110 81.4 67.3 (49.7-91.3) 949 100.0
Relative Risk (95% CI)
1.0
21.6 (15.1-30.9)
1.0
11.4 (10.2-12.7)
a str ict regis t ra t ion of all deaths, in- cluding c i rcumstances of death, had been conduc ted , a l l s t a t i s t i c s pre- sented here should be considered ap- p rox imat ions and, in some cases, an- ecdotal. For example, popula t ion fig- ures for the three towns were taken from a census conducted in i979. It is u n k n o w n w h a t p e r c e n t a g e of households were in terviewed or how sys temat ica l ly the survey was carried out. Unfor tunately , we were not able to de te rmine the number of persons s u c c e s s f u l l y e x t r i c a t e d w h o d i e d later.
The data were ana lyzed w i th the aid of the Stat is t ical Analysis System (SAS Inst i tute , Cary, Nor th Carolina). The ana lyses inc luded re la t ive r i sk ca lcu la t ions and X 2 tes ts of propor- t ion for s imple comparisons. Statist i- cal significance was considered at P < .05.
RESULTS In the three towns, the crude death
r a t e ( the p e r c e n t a g e of r e s i d e n t s f o u n d d e a d on e x t r i c a t i o n ) w a s 49.4%, w i t h a crude in jury rate of 28.9% and an overal l casua l ty ra te (deaths and injuries) of 64.1% (Table 1). At the t ime of the impact , mos t (83.8%) of the people were indoors. The mor ta l i ty rate was s ignif icant ly greater for these individuals (55.1%) than for those who were ou tdoo r s (8.8%) (P < .01) (Table 1). Injury rates were also s i gn i f i c an t l y grea ter for those ins ide (36.3%) than for those outs ide (1.7%)(P < .01)(Table 1).
Of t he t o t a l p o p u l a t i o n , 60.1% were reported to have been trapped. Dea th rates were 81.4% for t rapped individuals as compared wi th a rate of 1.2% for t h o s e w h o w e r e n o t t rapped (P < .01). In jury rates were 100% and 8.8%, respectively, for the
FIGURE 2. Main street in Nnlband showing complete collapse of all buildings. Note complete collapse of precast-concrete frame school build- ing on right side of street.
same groups (Table l). Thus, deaths were 67 t i m e s and in ju ry ra tes 11 t i m e s h i g h e r a m o n g t r a p p e d t h a n n o n t r a p p e d v i c t i m s . The c a s u a l t y rates were repor ted to be 100% for t rapped people as compared wi th a rate of 9.9% for nont rapped individ- uals. For those trapped, the ratio of injuries to deaths was 0.23, whereas for n o n t r a p p e d ind iv idua l s , i t was 7.2.
Al l bu i ld ings in the th ree t owns susta ined severe damage or comple te collapse. Almos t all of the res ident ia l d w e l l i n g s were o n e - s t o r y u n r e i n - forced stone masonry s tructures bu i l t f rom carved b locks of tuff {a l ight - weight, volcanic stone) set in mor ta r to form walls. Most of these dwell- ings p a r t i a l l y or t o t a l l y co l l apsed . There were two types of precast con- crete bu i ld ings in the th ree towns. P recas t concre te e l e m e n t s refer to concrete s t ructural components tha t have been fabricated at a factory and then t ransported to the cons t ruc t ion s i t e fo r e r e c t i o n c o m p a r e d w i t h pou red - in -p l ace conc re t e e l e m e n t s . M o s t i n d u s t r i a l f a c i l i t i e s in t h e towns s tud ied were of the precast - conc re t e f rame type, c o n s i s t i n g of precast concrete co lumns and beams w e l d e d or t i e d t o g e t h e r to f o r m frames (Figure 2); there was a smal ler i nven to ry of p recas t -concre te pane l s t ruc tu res . Of these th ree types of bu i ld ing systems, poor ly re inforced or unreinforced stone masonry build-
19:8 August 1990 Annals of Emergency Medicine 893/77

Building Type
Stone masonry
Precast concrete panel
Precast concrete frame
Total
TABLE 2. Effect of building type on survival m Nalband
Death Buildings Occupants Rate Relative 95% Confidence
(%) (N) Risk Interval
38 415 12.8 (53) 1.0
2 40 47.5 (19) 3.7 2.46 - 5.61
8 577 87.0 (502) 6.8 5.29 - 8.78
48 1,032 55.6 (574)
P
< .01
< .01
!100
50
"0
FIGURE 3. Live rescues as a function of t ime after impact (total numbers and cumulative percentage).
ings performed most poorly in terms of number of complete and partial collapses.
According to statistics collected by the Armenian Minis t ry of Internal Affairs and the State Committee for Construction, most of the fatalities occurred in the collapse of these stone masonry buildings (Table 2). Precast-concrete f rame type build- ings, however, were associated with highest morta l i ty per building. De- tailed stat ist ics were available for eight buildings of this type in Nal- band. Eighty-seven percent of the oc- cupants were killed (Table 2). The risk of death was 6.8 times greater in these eight frame buildings than in stone masonry buildings based on this limited sample (P < .01). In the sample of precast f rame buildings, two of the structures that collapsed resulted in an exceptionally high rate of mortality. One was a sewing fac- tory with 212 workers, of whom 205 (97%) died. The other was a school wi th 302 children, of w h o m 285 (94%) died. The p r eca s t - conc re t e panel buildings were also more lethal than the stone masonry structures (P < .01).
Of 240 pat ients reported by the Ministry of Health to be evacuated from the three towns, 23 (9.6%} de- veloped crash syndrome as a result of limb compression, and 11 {4.6%) de- veloped secondary acute renal failure requiring renal dialysis. All evacu- ated patients were reported to suffer from varying degrees of hypothermia. Pos tmor tem examinat ions of eight vict ims removed from the site of a bu i ld ing co l l apse r evea l ed large amounts of dust in the nasal cavities,
Live Rescues Cumulative %
'°° f 300
200
100
0
EARTHQUAKE Noji et al
0 6 12 18 24 48 72 96 120 144 168
Hours After Impact
Live rescues ~ Cumulative %
*Data from Nalband, Katnatschur, and Geghasar.
3
throat, and respiratory passages of these victims, suggesting that airway obstruct ion and asphyxiat ion from dust were the causes of death. This forensic evidence was corroborated by interviews with local residents of Nalband, who described large and dense dust clouds created by pulver- izat ion of the s tone and concrete walls of falling buildings.
Data collected 14 days after the earthquake on 4,832 patients admit- ted throughout hospitals in Armenia (Table 3) showed that combination injuries constituted 1,918 (39.7%)of the cases. Superficial trauma such as lacerations and contusions were the mos t f requent ly observed (24.9%), fo l lowed by head in jur ies (22%), lower-extremity injuries (19%), crush syndrome (11%), and upper-extremity trauma (10%).
Search and Rescue Rescue work was mos t difficult
during the first night when electric- ity and lights were unavailable; these efforts had to be halted at several lo- cations until the next morning. Oper- at ions in these three towns were compl ica ted by absence of s t ree t markings, maps, and building plans. Destroyed villages and small towns were isolated by numerous landslides and impassable roads, which delayed re l ie f t e a m s and p r e v e n t e d ful l knowledge of the extent of the disas- ter f rom reaching the author i t ies . Most of the initial rescue work and medical relief was carried out en- tirely by local inhabitants. Of the 240 trapped victims who were evacuated for medical care in Yerevan, local Civil Defense workers reported that 228 (95%) were extricated by inhabi-
78/894 Annals of Emergency Medicine 19:8 August 1990

Pat ients
300 I
2OO
0 0 1 2 3 4 5 6 7 8 9 10 11
D a y s 4
TABLE 3. Distribution of hospitalized injuries by site as reported to the Ministry of Health of Armenia after the December 7, 1988, earthquake
Injury
Head or face
Skull, facial fractures
Brain concussion
Other internal head trauma
Open head or facial wounds
Upper extremities
Upper-extermity fractures
Traumatic amputations, arms
Elective amputation, arms
Lower extremities
Lower-extremity fractures
©pen wounds, legs
Traumatic amputations, legs
Elective amputation, legs
Superficial trauma
Crush syndrome
Other
N %
1,040 22.0
130 2.7
417 8.6
173 3.6
320 6.6
475 10.0
265 5.5
197 4.1
13 0.3
915 19.0
584 12.1
102 2.1
170 3.6
59 1.2
1,203 24.9
533 11.0
633 13.1
tants of the three villages them- selves. The m o s t s o p h i s t i c a t e d means of ex t r i ca t ion used were hands, shovels, picks, and farming tools.
External assistance did not arrive in Nalband for the first 24 hours, and Katnatschur and Geghasar did not re- ceive aid until days 3 and 4, respec- t ive ly . The f i rs t ou t s i de re l ief consisted of military and civil de-
fense units stat ioned nearby, fol- lowed a few days later by volunteer teams from less-affected areas. Heavy rescue equipment such as cranes and bulldozers did not arrive in Nalband until day 5. An operations headquar- ters was not established in Nalband until December 18, 11 days after the earthquake.
According to information provided by the local army command center in
FIGURE 4. Patients presenting for emergency care at Erebuni Hospital in Yerevan.
Nalband, the great majority of those rescued alive from collapsed build- ings (89%} were extricated during the first 24 hours (Figure 3). The proba- bility of being extricated alive from the debris declined sharply over time. There were no live rescues af- ter day 6.
Emergency Medical Care Many of the surviving injured vic-
tims (30%) received no on-site medi- cal assistance. No individuals were known to have received any ad- vanced on-site medical care, such as cervical-spine immobilization, ad- ministration of oxygen or IV fluids, or tracheal intubation. Most of the patients were transported in private vehicles with no in-transit advanced medical care. Because all of the hos- pitals in the region were severely damaged and many medical person- nel were either killed or injured (esti- mated to be 80%), 311 of the injured (25%) were transported to hospitals in unaffected parts of Armenia or to neighboring Soviet Georgia (informa- tion provided by Ministry of Health). Unfortunately, winter weather condi- tions hampered aeromedical evacua- tion of the injured. Damage to rail- ways, extraordinary traffic conges- tion, and impassable roads due to mud made ground evacuation diffi- cult. Ground transport times to re- ceiving hospitals in Yerevan, 75 km away, were often as long as five hours.
In Yerevan, several hospitals ad- mitted a large number of casualties in the days immediately following the earthquake. Erebuni Hospital, a 1,000-bed facility in Yerevan, treated 902 patients in the first 11 days after the earthquake, 80% of whom were admitted during the first five days (Figure 4). Only 22 of the 902 pa- tients (2.4%) requiring hospitaliza- tion at Erebuni Hospital as a conse- quence of the earthquake were ad- mitted seven or more days after the impact.
DISCUSSION Although the risk of catastrophic
earthquakes is widely recognized in parts of California, few people realize that in the past 300 years, the eastern
19:8 August 1990 Annals of Emergency Medicine 895/79

EARTHQUAKE Noji et al
United States has suffered eight earthquakes of similar or greater magni tude than that in Armenia. There is a high probability that a ma- jor earthquake will hit the eastern United States in the next several de- cades. Building damage and life loss in such an event is predicted to be se- rious and widespread due to lack of seismic codes and absence of earth- quake preparedness programs. Other states, such as Utah and Washington, are also at risk from earthquakes, and despite recognition of the threat, mit 2 igation activities in these areas are inadequate.
Past studies have stressed the im- portance of critically analyzing earth- quakes to develop methods of rapidly assessing health-care needs and im- proving disaster relief.15 Epidemio- logic studies on earthquake-related injuries have indicated that a quan- titative relationship may exist be- tween morbidity and mortality.~6, t7 For example, in the Guatemala and Nicaragua earthquakes, the ratio of injured to dead was 3:1. In the area of Armenia studied here, this ratio was reversed, that is, three dead for every person injured. This suggests the ex- traordinary lethality of the Armenian event.
The Armenian earthquake was of lesser magnitude than the 1989 Loma Prieta e a r t hquake in Cal i fornia . However, its consequences were in- comparably greater, primarily be- cause of the design and quality of construction of buildings in the area. The primary cause of death, injury, and destruction was the total col- lapse of buildings that were not ade- quately designed for earthquake re- sistance.
Past studies have shown that fac- tors determining the number of peo- ple killed after a building collapses include entrapment, severity of their injuries, how long they can survive without medical attention, and time to rescue and medical treatment.t8-2o A 1977 s tudy on the Guatemala earthquake concluded that deaths and injuries are critically dependent on housing damage and construction materials used. 21 Results reported in our study carry this concept further by suggesting that different building types and structural systems have different collapse mechanisms and patterns of cavity formation when they fail under the influence of earth- quake ground motion. The limited
survey of three building types in Nalband (eg, stone masonry, precast- concrete panel, and precast-concrete frame) showed death rates of 12%, 46%, and 87%, respectively, suggest- ing that the type of building and col- lapse pat tern affect survival rates (Table 2).
Infill masonry, panels, and bricks often fell off, killing persons both in- side and outside, and the frequent collapse of stairways made it partic- ularly difficult for people to escape because many of these buildings had only one stairway. In all three build- ing types, the collapse of nonstruc- tural e l emen t s such as parapets caused many serious injuries. The to- tal collapse ("disintegration") of the precast-concrete frame buildings was associated with part icularly high mortality rates (more than 90%) be- cause the characteristic failure pat- tern of this type of cons t ruc t ion greatly complicated the search and rescue effort and reduced signifi- cantly the opportunity for occupant survival.
We observed that the fragmenta- tion of the floor system resulted in very tight packing of the rubble with no cavities or "void spaces" for possi- ble survival of victims. The distribu- tion and amount of void space in the collapsed structure and the most likely locations of those voids arc important in locating and rescuing trapped people quickly. Such infor- mat ion may help to guide future search and rescue operat ions by pointing out those collapsed build- ings that have the greatest proba- bility of containing survivors and by indicating the location of likely void spaces.
As might be expected, entrapment appears to be the single most signifi- cant factor associated with death or injury. Death rates were 67-fold and injury rates more than ll-fold those for trapped than nontrapped people. Death rates for those inside greatly exceeded those for persons outside; more than 80% of those trapped died.
This earthquake substantiated that response time for search and rescue is absolutely critical. Our observa- tion that the proportion of people found alive declined with increasing delay in extrication parallels the ob- servations made in Italy after the Campan ia - I rp in i a ea r thquake in 198022`23 and the Tangshan earth- quake in 1976. 24 In the Italian study,
a survey of 3,619 survivors showed that 93% of those who were trapped and survived were extricated within the first 24 hours. As suggested by our data, if any significant reduction in ea r thquake mor t a l i t y is to be achieved, attention should be given to appropriate search and rescue ac- tion within the first two days after the impact.
In the Italian study cited above, 95% of the deaths recorded were among those trapped in rubble who died before extrication. 22 Estimates of survivability among entrapped vic- tims buried under collapsed earthen buildings in Turkey and China indi- cate that within two to six hours, less than 50% of those buried are still alive.22, 2,~ Although it is not pos- sible to determine whether a trapped person died immediately or survived for some time under the debris, it is undoubtedly true that more people might have been saved if they had been extricated sooner. Safar, study- ing the 1980 earthquake in Italy, 2s concluded that 25% to 50% of vic- t ims who were injured and died slowly could have been saved if ini- tial life-saving first aid had been ren- dered immediately.
There were major problems with extr icat ion of trapped vic t ims be- cause of lack of adequate equipment and trained rescue personnel. Pene- trating concrete slabs and cutting through columns and beams of the precas t -concre te frame buildings proved to be major obstacles in the local rescue effort. No cutting tools were available, and the tools that were available proved to be ineffec- tive. The number of people available to help rescue others was greatly re- duced because of the very high per- centage of people trapped and killed. This scarcity of rescue workers may have contributed to the excessively high mortality in the three towns ex- amined. Most of the search and res- cue effort was late and, even at the peak of activity, was seriously inade- quate.
In the three towns visited during our reconnaissance mission, very lit- tle in the way of basic medical care was administered to persons who had been located and were actively being extricated from the debris. The provi- sion of basic supportive care, such as IV fluids, might have gone a tong way toward reducing morbidity and mor- tality, particularly in preventing the
80/896 Annals of Emergency Medicine 19:8 August 1990

development of crush syndrome. 26 z9 As with all field surveys after db
sasters, there were methodological limitations to this study due to chao- tic postearthquake condit ions. Ac- cord ing ly , r e s u l t s m u s t be ap- proached wi th caut ion. The diffi- cult ies encountered in co l lec t ing information in our study point out the great need to develop improved survey sampling methods for imme- diate pos td i sas ter inves t i ga t ions . Much of the data on building dam- age, location of entrapment, details of v ic t im locat ion and extrication process, and on-site medical care are considered "perishable ''3° and thus lost unless collected very early. De- spite the shortcomings of this study, these preliminary observations are striking. Case studies of earthquakes such as described here can suggest hypotheses for future in-depth analy- sis using more sophisticated epide- miologic methods. '31
C O N C L U S I O N The December 7, 1988, Armenian
earthquake was o n e o f the most le- thal in the 20th century. Major medi- cal problems resulted not only from the direct crushing effects of collaps- ing buildings but also from severe cold and exposure, prolonged entrap- ment, delayed medical care, and long transportation times to the nearest u n a f f e c t e d h o s p i t a l s . F o l l o w - u p studies that analyze the complex re- lationship among factors related to survival as detailed here should pro- vide further insights that will lead to the improvement of future rescue ef- forts.
The authors thank Ms Thola Brothers for her help in producing the figures and Dr Deborah McClellan for her assistance in preparing the manuscr ipt . They also ex- press gratitude to the Armenian Relief So- ciety, w i thou t whose support this study would not have been possible. It is hoped that th is project, w h i c h involved close collaboration be tween US and Soviet in- vestigators, will foster scientific coopera- tion be tween the two countr ies in the fu-
' tore and, in a smal l way, con t r ibu te to greater m u t u a l understanding.
REFERENCES 1. Binder S, Sanderson EM: The role of the epi- demiologist in natural disasters. Ann Emerg Med 1987;16:1081-1084.
2. Armenian HK: Methodologic issues in the epidemiologio studies of disasters, in Jones NP, Noji EK, Smith GS, et al (eds): Proceedings of the International Workshop on Earthquake In- jury Epidemiology: Implications for Mitigation and Response. Washington, DC, National Sci- ence Foundation, 1989, p 95-106.
3. Smith GS: Research issues in the epidemiol- ogy of injuries following earthquakes, in Jones NP, Noji EK, Smith GS, et al (eds): Proceedings of the International Workshop on Earthquake Injury EpidemioIogy: Implicntions for Mitiga- tion and Response. Washington, DC, National Science Foundation, 1989, p 61-81.
4. Noji EK: Evaluation of the efficacy of disas- ter response: Research at the Johns Hopkins University. UNDRO News 1987;4:11-13.
5. Filson JR, Agbabian MS, Noji EK: Post-earth- quake investigations of the December 7, 1988, Spitak Earthquake by the United States, in Cid linski K (ed): Proceedings of the International Seminar on the Spitak Earthquake in Yerewm, Armenia. Paris, UNESCO, 1989, p 1-3.
6. Filson J, Borcherdt RD, Langer C: Seismol- ogy. Earthquake Spectra (suppl) i989;1-12.
7. The December 7, 1988 Armenigl, USSR Earthquake. San Francisco, EQE Engineering, 1989, p 1-48.
8. Ambraseys NN, Adams RD: Long-term seis- micity of north Armenia. EOS: Trans Am Geo- phys Union 1989;70:145-154.
9. Sharp RV: Surface faulting: A preliminary view. Earthquake Spectra (suppl) 1989;13-22.
10. Filson J: Tectonic setting and seismic set- ting for the main shock of December 7, 1988, in Borcherdt RD (ed): Results and Data from Seis- mologic and Geologic Studies Following Earth- quakes of December 7, I988 Near Spitak, Ar- menia, SSR, USGS Open-File Report (89-163A). Reston, Virginia, US Geological Survey, 1989, p 11-20.
11. Report on International Relief Assistance for the Earthquake of 7 December 1988 in the SSR of Armenia, UNDRO/89/6. Geneva, Office of the UN Disaster Relief Coordinator, i989, p 1-35.
12. Schiff A, Yanev P: Performance of lifeline systems. Earthquake Spectra (suppl) 1989; 114-135.
13. Krimgold F: Search and rescue. Earthquake Spectra (suppl) 1989;136-149.
14. Logue JN, Melick ME, Hansen H: Research issues and directions in the epidemiology of health effects of disasters. EpidemioI Rev 1981; 3:140-162.
15. Lechat MF: An epidemiologist's view of earthquakes, in Solnes ] (ed): Engineering Seis- mology and Earthquake Engineering. Leiden, Holland, Noordhoff, 1974, No. 3, p 285-306.
16. de Ville de Goyet C, del Cid E, Romero A, et al: Earthquake in Guatemala: Epidemiologic evaluation of the relief effort. Bull Pan A m Health OrgLm 1976;10:95-109.
17. Alexander DE: Death and injury in earth- quakes. Disasters 1985;9:57-60.
18. Coburn AW, Hughes RE: Fatalities, injury and rescue in earthquakes, in 2nd Conference of the Development Studies Association. Man- chester, England, University, 1987, p 235-243.
19. Durkin ME, Murakami HO: Casualties, sur- vival and entrapment in heavy damaged build- ings, in Proceedings of the 9th World Confer- enee on Earthquake Engineering. Tokyo, Japan Association for Earthquake Disaster Prevention, 1988, vol 8, p 977-982.
20. Coburn AW, Murakami HO, Ohta Y: Fac tots Affecting Fatalities and Injury in Earth- quakes. Internal report, Engineering Seismology and Earthquake Disaster Prevention Planning. Hokkaido, Japan, Hokkaido University, 1987, p 1 80.
21. Glass RI, Urrutia ]J, Sibony S, et al: Earth- quake injuries related to housing in a Gua- temalan village. Science 1977;197:638-643.
22. de Bruycker M, Greco D, Lechat MF: The 1980 earthquake in Southern Italy: Morbidity and mortality. Int J Epidemioi 1985;14:113-117.
23. de Bruycker M, Greco D, Annino I, et al: The 1980 earthquake in Southern Italy: Rescue of trapped victims and mortality. Bull World Health Organ 1983~61:1021-1025.
24. Zhi-Yong S: Medical support in the Tang- shan earthquake: A review of the management of mass casualties and certain major injuries. ] Trauma 1987;27:1130-1135.
25. Safar P: Resuscitation potentials in mass di- sasters. Prehosp Dis~lster Med 1986;2:34-47.
26. Allister C: Cardiac arrest after crush injury. Br Med J 1983;287:531-532.
27. Collins AJ: Kidney dialysis treatment for victims of the Armenian earthquake. N EngI ] Med 1989;320:1291-1292.
28. Richards NT, Tattersall J, McCann M, et ah Dialysis for acute renal failure due to crush in- juries after the Armenian earthquake. Br Med J 1989;298:443-445.
29. Klain M, Ricci E, 8afar P, et al: Disaster re- animatology potentials: A structured interview study in Armenia: I. Methodology and prelimi- nary results. Prehosp Disaster Med 1989;4: 135-154.
30. Le~rning from Earthquakes: i977 Phmning and Field Guides. E1 Cerrito, California, Earth- quake Engineering Research Institute, 1977, p 173-20(/.,
31. Sanchez-Carrillo CI: Morbidity following Mexico City's 1985 earthquakes: Clinical and epidemiologic findings from hospitals and emer- gency units. Public Health Rep 1989;104: 483-488.
19:8 August 1990 Annals of Emergency Medicine 897/81