
Thank you for Participating in our SGEC webinar!...
41
Thank you for Participating in our SGEC webinar! We appreciate your participation in our SGEC webinar series. Webinar handouts and instructions are on the following pages. Below is an important announcement and request for all participants : Important Request: When you enter the webinar meeting you will be asked to enter your name. Please enter either: Your Full Name (First and Last as it appears on the Registration) or if you prefer First Initial and Last Name Detailed login instructions are on the following pages. Thank you! Christopher Motola Media Coordinator, Stanford Geriatric Education Center (SGEC) http://sgec.stanford.edu
Transcript of Thank you for Participating in our SGEC webinar!...

Thank you for Participating in our SGEC webinar! We appreciate your participation in our SGEC webinar series. Webinar handouts and instructions are on the following pages. Below is an important announcement and request for all participants:
Important Request: When you enter the webinar meeting you will be asked to enter your name. Please enter either: Your Full Name (First and Last as it appears on the Registration) or if you prefer First Initial and Last Name
Detailed login instructions are on the following pages.
Thank you!
Christopher Motola Media Coordinator, Stanford Geriatric Education Center (SGEC) http://sgec.stanford.edu
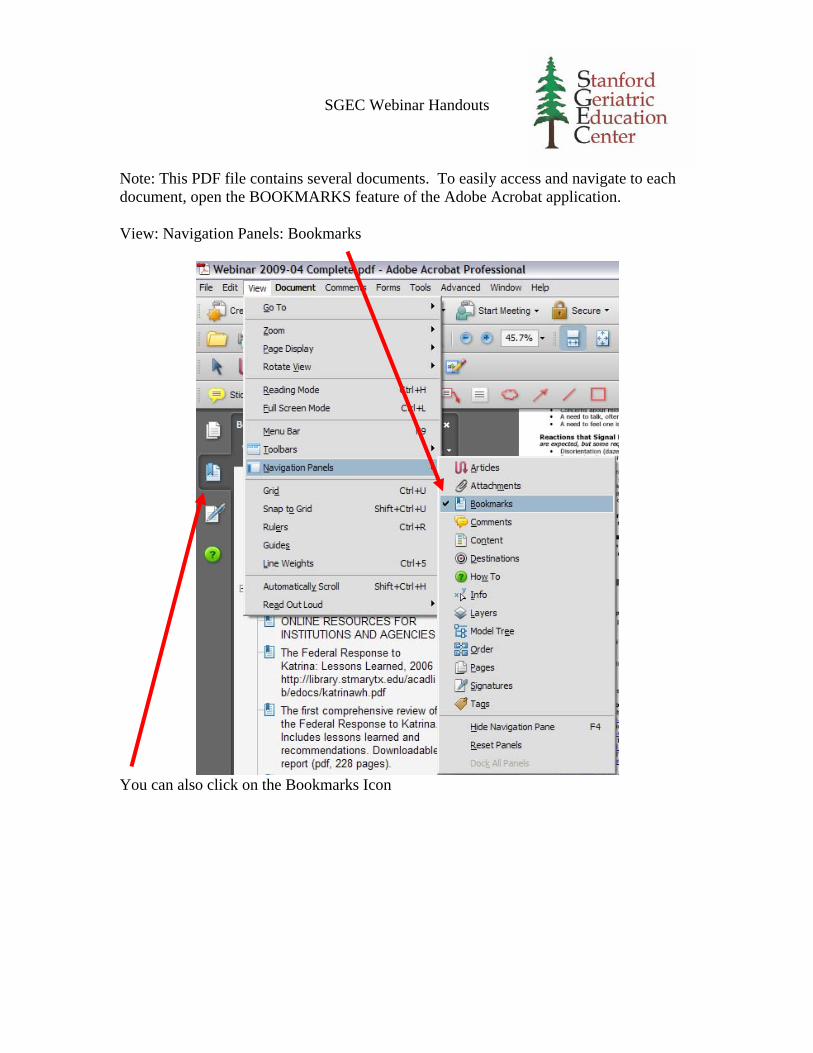
SGEC Webinar Handouts Note: This PDF file contains several documents. To easily access and navigate to each document, open the BOOKMARKS feature of the Adobe Acrobat application. View: Navigation Panels: Bookmarks
You can also click on the Bookmarks Icon

Webinar Technical Quick Reference Guide:
Connect: To Connect to the Webinar: 1. Please visit our web site at: http://connectpro50192156.acrobat.com/sgec/
2. Select "Enter as a Guest," and type your name
IMPORTANT REQUEST: Please enter your
Full Name (First and Last as it appears on the Registration), or if you prefer
First Initial and Last Name. Thank you!
3. Click "Enter Room" and the webinar will start.
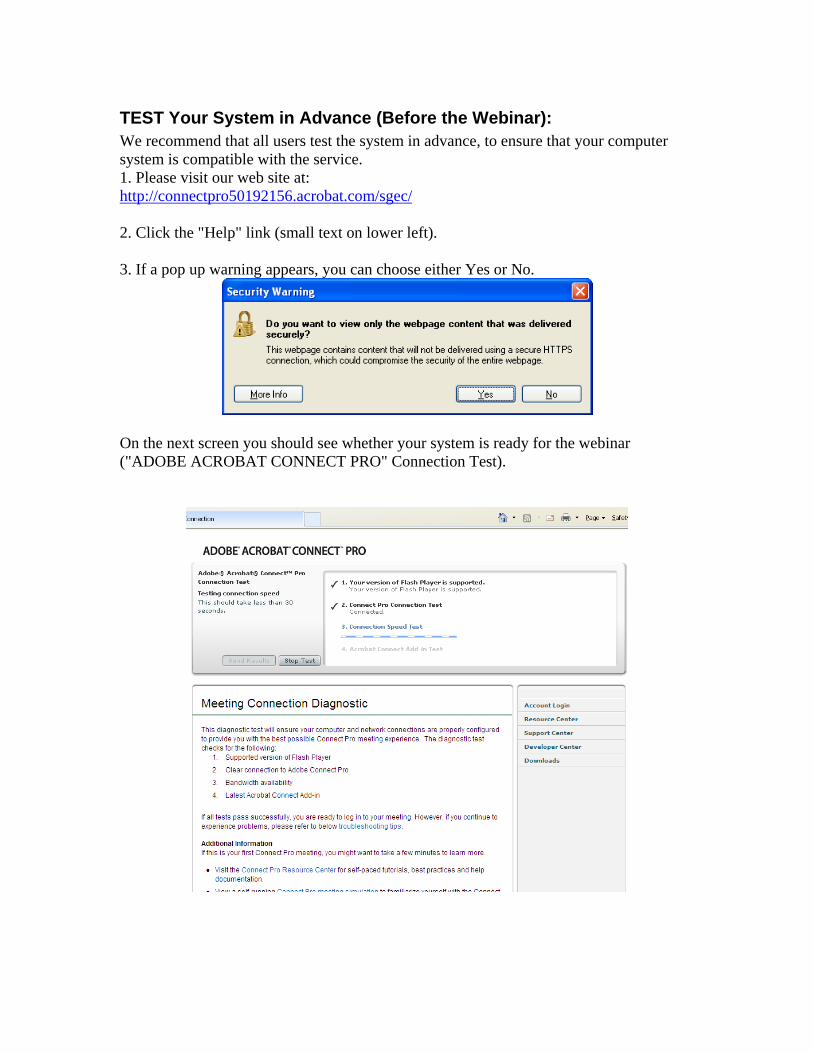
TEST Your System in Advance (Before the Webinar): We recommend that all users test the system in advance, to ensure that your computer system is compatible with the service. 1. Please visit our web site at: http://connectpro50192156.acrobat.com/sgec/ 2. Click the "Help" link (small text on lower left). 3. If a pop up warning appears, you can choose either Yes or No.
On the next screen you should see whether your system is ready for the webinar ("ADOBE ACROBAT CONNECT PRO" Connection Test).

Audio During the Webinar: The webinar requires that you use a computer with a sound card in order to hear the participants. A microphone is optional (see below for methods of asking questions). To test your computer sound, please use the Audio Setup Wizard. Select: the “Meeting” menu, then “Manage My Settings” and “Audio Setup Wizard.”
Follow the instructions and guide to test your audio hardware.
If you don’t have a microphone or don’t want to use it you can cancel or skip the microphone tests.
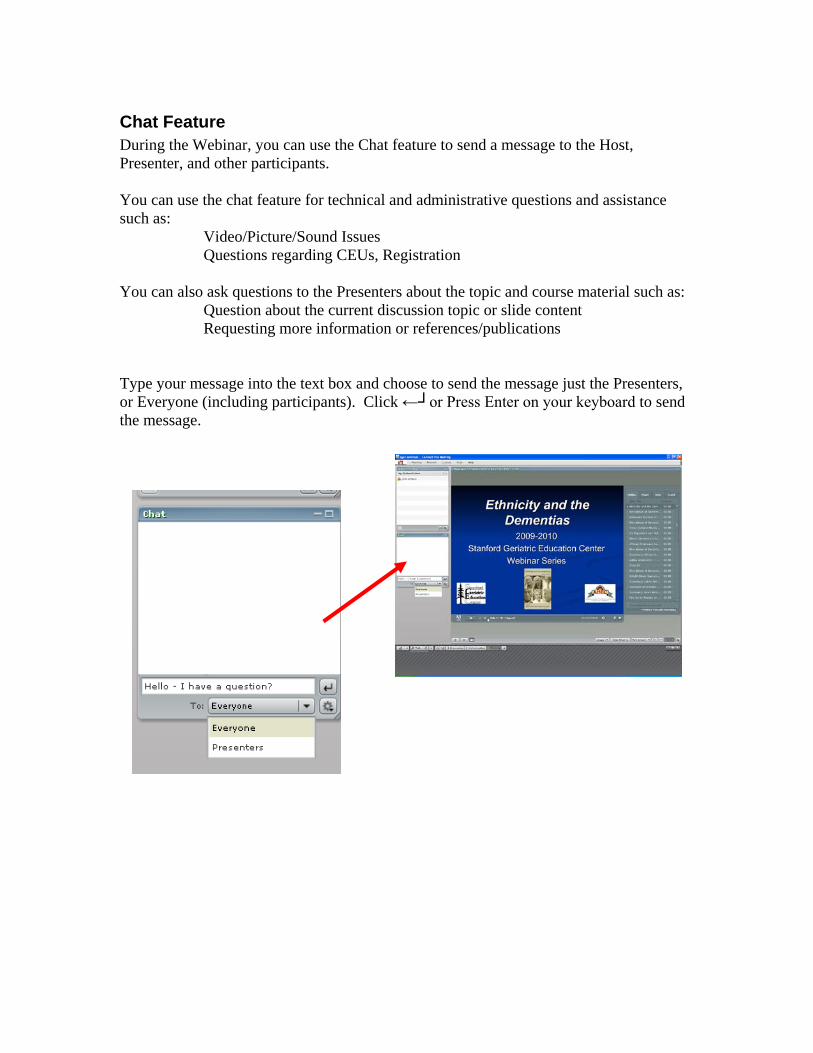
Chat Feature During the Webinar, you can use the Chat feature to send a message to the Host, Presenter, and other participants. You can use the chat feature for technical and administrative questions and assistance such as:
Video/Picture/Sound Issues Questions regarding CEUs, Registration
You can also ask questions to the Presenters about the topic and course material such as:
Question about the current discussion topic or slide content Requesting more information or references/publications
Type your message into the text box and choose to send the message just the Presenters, or Everyone (including participants). Click ←┘or Press Enter on your keyboard to send the message.
10/6/2011
1
• S. Liliana Oakes, MD, CMD
• Melissa A. Talamantes, M.S., PHD
Sponsored by
Stanford Geriatric Education Center
in conjunction with
American Geriatrics Society,
California Area Health Education Centers,
12:30 PM Pacific Time
Dementia Assessment, and Family Caregiving Part 1: Latino
October 6, 2011
This project is/was supported by funds from the Bureau of Health Professions (BHPr), Health Resources and Services Administration (HRSA), Department of Health and Human Services (DHHS) under UB4HP19049, grant title: Geriatric Education Centers, total award amount: $384,525. This information or content and conclusions are those of the author and should not be construed as the official position
or policy of, nor should any endorsements be inferred by the BHPr, HRSA, DHHS or the U.S. Government.
California Area Health ducation Centers,
and
Natividad Medical Center
If you do not hear any audio, please use the audio set up wizard:
Choose the “Meeting” menu (above, left),
Then select “Manage my settings”
and “Audio Setup Wizard”
NatividadMedical Center CME Committee Planner Disclosure Statements:
The following members of the CME Committee have indicated they have no conflicts of interest to disclose
“Dementia Assessment, and Family Caregiving Part 1: Latino”
to the learners: Kathryn Rios, M.D.; Valerie Barnes, M.D.; Anthony Galicia, M.D.; Sandra G. Raff, R.N.; SueLindeman; Janet Bruman; Jane Finney; Tami Robertson; Judy Hyle, CCMEP; Christina Mourad and KevinWilliams.
Stanford Geriatric Education Center Webinar Series Planner Disclosure Statements:
The following members of the Stanford Geriatric Education Center Webinar Series Committee have indicatedthey have no conflicts of interest to disclose to the learners: Gwen Yeo, Ph.D. and John Beleutz, MPH.
Faculty Disclosure Statement:
As part of our commercial guidelines we are required to disclose if faculty have any affiliations or financialAs part of our commercial guidelines, we are required to disclose if faculty have any affiliations or financialarrangements with any corporate organization relating to this presentation. Drs. Talamantes and Oakes haveindicated they have no conflicts of interest to disclose to the learners, relative to this topic.
Drs. Talamantes and Oakes will inform you if they discuss anything off‐label or currently under scientificresearch.

10/6/2011
2
S. Liliana Oakes, MD, CMD
S. Liliana Oakes, MD is an Associate Professor in the Department of Family and Community Medicine, at the University of Texas Health Science Center at San A t i T D O k i th G i t i f ll hi di t f GACAAntonio, Texas. Dr. Oakes is the Geriatrics fellowship director, a former GACA awardee (Geriatric Academic Career Award). As a clinician educator she has expertise in curriculum development and evaluation. She is actively involved in leading the first ACE unit (Acute Care of Elderly) in South Texas to improve the care of hospitalized older adults. One of her passions is interdisciplinary teaching around hospital care topics, effective communication, cross‐cultural competence and teaching palliative care to interdisciplinary teams. Her funded research also has focused on caring for patients and families coping with Alzheimer’s disease and on developing culturally competent care for Hispanic elders and theirand on developing culturally competent care for Hispanic elders and their caregivers (Alzheimer’s Association and TARC). Dr. Oakes has a define role as a mentor for fellows, residents and students assisting with curriculum development, and educational faculty development. She is a native of Bogota Colombia.
MELISSA A. TALAMANTES, M.S., PHD
Dr. Talamantes currently is a Palliative Care Psychology Fellow at the South Texas Veterans Health Care Administration (STVHC). She completed her Psychology i t hi i P h l ith i l h i i G h l t th STVHCinternship in Psychology with a special emphasis in Geropsychology at the STVHC. She has Master’s degree in Gerontology and has research and practice expertise working with Mexican American elderly and their caregivers. Her current research project involves developing a dissemination plan for the Cuidando con Respeto Spanish and English language caregiver training program. Prior to internship and postdoctoral training Dr. Talamantes conducted research in the Department of Family and Community Medicine at University of Texas Health Science at San Antonio. Her other research interests include, Palliative Care and End of Life Issues and Intimate Partner Violence with Older Couplesand Intimate Partner Violence with Older Couples.
10/6/2011
3
Thank You for Participating!
2011OCT
Thank You for Participating!
We will send copies of slides by e‐mail.
Please complete this short survey after the webinar.We appreciate your feedback.
NOTE: Continuing Education Participants must complete a final survey in order to receive CEUs
Link to Survey

10/5/2011
1
S Lili O k MD AGSF CMDS. Liliana Oakes MD, AGSF, CMD
Associate Professor, UTHSCSA
Family and Community Medicine‐Internal Medicine
Geriatrics Division
Stanford Geriatric Education Center
October 6,2011
Objectives Define the “Demographic Imperative” for dementia care and delineate the effects of how aging Baby Boomers are stressing the current support systemsupport system
Investigate the specific effects of Alzheimer’s Disease on the Hispanic
Discuss how physicians and caregivers can best cope with increased caseloads
Outline of the session Overview of the prevalence of dementia in Latinos
Review the etiology of dementia and risk factors in Latinos
R i h di ’ i h i Review the disease’s impact on the community
List pearls and challenges: how to diagnose and educate our Latino community, testing limitations
Review programs meeting the Latino need in relation to dementia

10/5/2011
2
The New York Times
More Alzheimer’s Risk for Hispanics, Studies Find ( October 20, 2008)
Jessica Kourkounis for The New York TimesAfter Antonio Vasquez, 63, in North Philadelphia with granddaughter Alexandra Martinez,learned that he had Alzheimer's, he and his wife moved in with a daughter. More Photos >
Latino with DementiaThe Alzheimer’s Association :
Today, 200,000 Latinos in the United States have Al h i ’ Alzheimer’s
By 2050, Alzheimer’s prevalence in Latinos could reach 1.3 million.
By 2050, total number of Alzheimer’s patients will grow from current 5 million to 16 million.
Census Bureau data 2000
Percent of U.S. Population Over 65 by Race & Hispanic Origin
Adapted from U.S. Census Bureau (2001)

10/5/2011
3
Diversity Among Latino Populations in the United States
Mexico Central America
Courtesy of Dr. Dolores Gallagher‐Thompson, Ph.D., ABPPConsuelo Juarez, Health Educator
South AmericaPuerto RicoCuba
Latino Sub Group Variances
Cultural Traditions
Values
Religions
Courtesy of Dr. Dolores Gallagher‐Thompson, Ph.D., ABPPConsuelo Juarez, Health Educator
g
Belief Systems
Dialect
Education
Literacy
Latino Risk Factors
Several factors, many linked to low income or cultural dislocation, may
Hi i put Hispanics at greater risk for dementia, including higher rates of diabetes, obesity, cardiovascular disease, stroke and possibly hypertension.
(NY times, Oct 2008)

10/5/2011
4
Risk FactorsAGE: Prevalence doubles every 5
years 65 + / 47% of persons 85 and older have AD
Hispanics are the fastest growing elderly group in the country
Their life expectancy will increase to age 87 by 2050, surpassing all other ethnic groups in the
United States. Valle, R and Lee. B, Research Priorities in the Evolving Demographic Landscape of Alzheimer’s Disease and Association Dementias. Alzheimer’s Disease and Associated Disorders. 2002. 16(2):S64‐76..
Earlier onset?Earlier Onset of Alzheimer Disease Symptoms in
Latino Individuals Compared
With Anglo Individuals (Clark, Decarli et al)
Latino patients had a mean age at symptom onset 6.8 years earlier (95% confidence interval, 3.5‐10.3 years earlier) than Anglo patients after adjustment for sex, education, or NIA center.
Earlier Onset of Alzheimer Disease Symptoms in Latino Individuals Compared With Anglo IndividualsChristopher M. Clark, MD; Charles DeCarli, MD; Dan Mungas, PhD; Helena I. Chui, MD; Roger Higdon, PhD;Jessica Nuñez; Henrique Fernandez, MD; Mirna Negrón, BSW; Jennifer Manly, PhD; Steven Ferris, PhD;Angelica Perez, PhD; Migdalia Torres, MSW; Douglas Ewbank, PhD; Guila Glosser, PhD; Gerald van Belle, PhDArch Nuero 2005
Risk Factors Education appears to have some protective
effect against Alzheimer’s.
Hispanics have the lowest education levels of any Hispanics have the lowest education levels of any group in the United States.
Approximately one in 10 Hispanic elders has
no formal education.
50% have less than 8 years of educationUS Census Bureau. Educational Attainment in the UnitedStates. March 2000. Detailed Tables.
10/5/2011
5
Risk factorsVascular disease risk factors
Diabetes, Stroke and Hypertension are risk factors for d l i Al h i ' d h d ideveloping Alzheimer's and other dementias
High incidence of DM: 64 % higher than in Non‐Hispanic Whites
Haan, M et al. Prevalence of Dementia in Older Latinos:The Influence of Type 2 Diabetes Mellitus, Stroke andGenetic Factors. JAGS 2003. 51:169‐177. Wu, CC at al.Brain Structure and Cognition in a Community Sample ofElderly Laitnos. Neurology. August 2002. 59(3):383‐391.
Risk Factors DM and HTN contribute more to the dementia in this ethnic group than in European –Americans
% ld i h d i l h DM d HTN i 43% elders with dementia also have DM2 and HTN in this study
APOE allele plays lesser role than in other groups
Haan, M et al. Prevalence of Dementia in Older Latinos:The Influence of Type 2 Diabetes Mellitus, Stroke andGenetic Factors. JAGS 2003. 51:169‐177. Wu, CC at al.Brain Structure and Cognition in a Community Sample ofElderly Laitnos. Neurology. August 2002. 59(3):383‐391.
Research findings on Latinos
Significantly higher incidence of Alzheimer’s in Caribbean Hispanics in Manhattan, independent of co morbidities and education. (Tang X.M,2001)( g , )
Increased incidence of AD in the Latino
population in New York, NY and Houston ,TX compared with Anglo individuals (Gurland, Tang 2000)

10/5/2011
6
Challenges in RecognitionMemory loss seen as part of normal aging
Memory loss seen as mental illness
Memory loss seen as leading to loss of role
Challenges in diagnosis Lack of culturally appropriate diagnostic tools
Not enough professionals with bilingual skills
Academic centers with interest in research, but few opportunities to translate research into practice
Facts…The diagnostic value of common screening instruments is affected by:
Ageg
Education
Language biases
Low sensitivity
Specialized training or equipment

10/5/2011
7
Caution Instruments retain Cultural Bias even when accounting for Age, Education, Gender and SES
Hispanics Tend to Score Lower Than NHW
Translator Use Questionable
Time!
Low vision issues:
small print, fonts with
serif, reverse color text (white on black)
ABC’s: The Key Symptom Domains of Alzheimer’s Disease
Activities of Daily Living
BehaviorCognition
EF Executive Function
ABC’s: The Key Symptom Domains of Alzheimer’s Disease
Activities of Daily Living: ADLs, IADLs
Behavior;
Delusions, paranoia,Halluciantions
Cognition:
MMSE,Mini COG
CLOX
EF Executive Function

10/5/2011
8
MMSE: designInstrument developed in western country
Includes 12 interviewing questions
Covers multiple cognitive domains: orientation, registration, memory, attention, calculation, visual g , y, , ,spatial function, and praxis
Two items are reading and writing dependent (reading and following command‐ “close your eyes”‐ and writing a sentence)
Folstein et al. J Psych Res 12:189, 1975
MMSE
Possible score: 0 to 30
25‐30 for normal
21‐24 for mild AD 4
14‐20 for moderate AD
and less than 13 in severe AD
Folstein 1975, Royall et al,1998
MMSE
What do you think are the limitations of the MMSE?
10/5/2011
9
MMSE
Lack of items that measure Executive Function
Sensitivity 79%
Items dependent in educational level, literacy
CLOX I‐ CLOX II Clock‐drawing tests are relativelysimple / EF
Screening appear less vulnerable to socio‐cultural i flinfluences.
CLOX has been translated into Spanish and validated in multipleelderly populations, including Mexican‐Americans.
Royall DR, Mulroy A, Chiodo LK, et al: Clock drawing is sensitive to executive control: a comparison of six methods. J Gerontol Psychol Sci 1999; 54B:328‐333 Royall DR, Espino DV, Polk MJ, et al: Validation of a Spanish translation of the CLOX for use in Hispanic samples: the Hispanic EPESE study. Int J Geriatr Psychiatry 2003; 18:135–141[
Columbia Center for Active Life of Minority Elders (CALME)

10/5/2011
10
Montreal Cognitive Assessment (MoCA) The MoCA is a brief cognitive screening tool with high
sensitivity and specificity for detecting Mild Cognitive Impairment
Intended for use by busy clinicians
It is free, and translated versions are available free from It is free, and translated versions are available free from website: http://www.mocatest.org (including Spanish)
Clinical Implications: (1) Useful screening tool for the detection of mild AD and MCI –
thus allowing intervention to begin sooner; (2) Useful predictive tool for the development of dementia in
clients with MCI – again, early intervention is then possible. Limitation: May not be sensitive to change over a 6‐month
period – this is still being researched.
Composite 3 item recall and clock drawing
Developed to be administered in older adults from culturally, linguistically and educationally diverse backgrounds
MINI ‐ COG
backgrounds
Minimal language interpretation and training
The mini-Cog:a cognitive “vital sign "measure for dementia screening in multi –lingual elderly. Borson, S. et al. Int J Geriatr Psychiatry 15,1021-1027.2000
MINI ‐ COG
Scoring ‐ normal vs abnormal
Clock drawing test (CDT) normal ‐ abnormal
Subjects recalling none of the words dementedSubjects recalling none of the words ‐ demented
Subjects recalling all three words ‐ non demented
Subjects recalling 1 or 2 words (intermediate) ‐abnormal

10/5/2011
11
Mini‐Cog scoring algorithmMini‐cog
3 item recall = 0 3 item recall = 1‐2 3 item recall = 3
CDT Abnormal CDT normal
Family Role Drives Care
More Complex than pIt Appears
Needs Time!
Family Structure
Multiple generations often live under one roof
Emphasis on whole family inclusion
Nuclear family with large extended family Nuclear family with large extended family
Compadrazo (Godparents) may play a significant role or take on role of caregiver
Courtesy of Dr. Dolores Gallagher‐Thompson, Ph.D., ABPPConsuelo Juarez, Health Educator
10/5/2011
12
Cultural Beliefs Associated with Memory Loss
Etiology is often attributed to: Locura (craziness) Nervios (nerves) Punishment from god Poor nutrition Poor nutrition Stress earlier in life
Diagnosis of AD is interpreted as a result of: a family tragedy (Ortiz, Simmons, & Hinton, 1999)
lack of social support (Levy, Hillygus, Lui & Levkoff, 2000)
normal aging (Ortiz, Simmons, & Hinton, 1999; Levy et al., 2000)
Diagnosis is difficult: Few distinctions between physical illness, emotional disorders, and social problems
Courtesy of Dr. Dolores Gallagher‐Thompson, Ph.D., ABPPConsuelo Juarez, Health Educator
What is the current and future directions Research and clinical practices
Education and awareness
Professional development
Partnerships
Research opportunities TARC (Texas Alzheimer's Research Consortium)
More academic centers interested in minority interested in minority groups and dementia
More funds to do research in diagnostic tools and treatments
Include more Latinos in research

10/5/2011
13
Clinical practice Aggressive management of the risk factors in mid‐life DM‐ HTN
Addressing health disparities
Screening for dementia? How this looks?
Clinical Practice Offer the current treatments to our Latinos
New treatments :
Targeting the known Start earlier the
Targeting the known neuropathologic hallmarks:
amyloid plaques
tau‐based
neurofi brillary tangles.
treatments when diagnosis is highly suspected vs waiting
An Update on Treatment and Prevention Strategies for Alzheimer’s DiseaseJudith Neugroschl, MD, and Mary Sano, PhD Current Neurology and Neuroscience Reports 2009, 9:368–376
Pathology begin Onset symptoms Loss of ADLs
Death
Mild Cognitive Impairment Mild – moderate AD Severe
55 60 65 70 75 80 85 90
Mild Cognitive Impairment Mild-moderate AD Severe
Normal Prodromic Symptomatic NH
Death
100
Treatment
Courtesy of Dr. Chris Clark

10/5/2011
14
Education and awareness
More media involvement in reaching our community and addressing dementia
For the public
and addressing dementia
More appropriate materials addressing health literacy issues with our Latinos
Empowerment of community partners, caregivers
Education and awarenessHealth Literacy and Cognitive Performance in Older Adults. Sano,M et al. JAGS June 8,2009
Memory and verbal fluency are strongly associated with health literacy independent of education and with health literacy, independent of education and health status, even in those with subtle cognitive
dysfunction.
Reducing the cognitive burden of health information might mitigate the detrimental
effects of limited health literacy in older adults.
Professional Development
More training for health care professionals about dementia and dementia in Latinos
Screening? When ? How? Who?
Establish more partnerships with local networks

10/5/2011
15
Driving retirement or Driving While Demented “DWD” Everyone with dementia must retire from driving, the key is
WHEN
Begin discussion and planning early
Family agreement documents (loss of insight/awareness may interfere))
Observation is key – of driving and car condition
Consider comprehensive on‐road assessment
“The grandchild rule”: If a patient’s children don’t want the grandchildren in the car when the patient is driving, he or she needs to relinquish the keys before hurting someone else’s grandchildren. Gary Kennedy, MD
Sensitivity – giving up the keys is a huge loss
Provide alternatives
The need to plan: legal issues Involve your loved one as much as possible:
KEY Arrangements: Living will (Advance Care Plan) The completion of advanced directives
as an act of family love (minimizing second‐guessing, family conflicts and guilt feelings)
Health Care Agent
Durable Financial Power of attorney
Protection of assets and avoidance of financial losses/ scams/errors
Elder care attorneys may help plan for long term care costs
Participation in research
Consider Hospice

10/5/2011
16
We all need to complete advance directives – for our families’ sake
This is best avoided
“An 80 year old great grandmother makes her wishes absolutely clear”
May 18, 2006© WorldNetDaily.com
PartnershipsAlzheimer's Association:
http://www.alz.org
We Speak Spanish
1.800.272.3900 ‐ Call us anytime for free, confidential guidance and reliable information.
Message Boards‐ Find bilingual support and advice in a caring community.
Partnerships Alzheimer's Association
MedicAlert® + Alzheimer’s Association Safe Return®A 24‐hour emergency response service for wandering and medical emergencies.
Cuidando con Respeto: Dr. Oakes ,Dr. Talamantes et al. UTHSCSA/ AA of California/ AoA grant
Community Centers ; non –profit organizations
Hospices
Home Health Agencies
Multiple reading materials for caregivers

10/5/2011
17
Recommended Readings
The Alzheimer's Action Plan. P Murali Doraiswamy, MD L P G h MSW T Adl MD, L.P. Gwyther MSW, T Adler
The 36 Hour Day (30 years the classic)
Coach Broyles’ Playbook for Alzheimer’s Caregivers: A Practical Tips Guide – offered through www.alz.org
Resources Alzheimer’s Association www.alz.org
1‐800‐356‐5502 Geriatric Mental Health Foundation American Association for Geriatric Psychiatry Alzheimer’s Society Alzheimer s Society ADEAR Alzheimers Disease Education and referral Center of the
National Institute on Aging: www.nia.nih.gov/Alzhimers/ 1‐800‐438‐4380
Family Caregiver Alliance National Center on Elder Abuse National Senior Citizens Law Center United States Administration on Aging TrialMatch (Alzheimer’s Association) http://hartfordauto.the hartford.com

10/5/2011
18
From Frank Broyles My best advice to you is to treasure each day and live it to the fullest. Cherish the time you spend together, and perhaps most important, love each other. I hope you find peace in knowing that it is still possible to live and love when someone you love is living with Alzheimer's disease.
Sincerely,Frank Broyles University of Arkansas, Razorback Athletic Director Emeritus
Questions?
Melissa A. Talamantes, PsyDPalliative Care Psychology Fellow
South Texas Veterans Health Care SystemSan Antonio, TX
.

10/5/2011
19
Acknowledgments
Stanford School of Medicine‐Geriatric Education CenterEducation Center
Dr. Dolores Gallagher & Dr. Gwen Yeo
ObjectivesDescribe Latino Caregiving Characteristics & Relevant Research
Present Core Cultural Concepts
Describe Current Caregiver Interventions for Latinos
Demographics
Over 27% of Latino households provide informal caregiving to family member or friend (NAC, AARP, y1997;AoA, 2003)
Latino caregivers, average age 40 and in sandwich generation (NAC, AARP,
1997;AoA, 2003)

10/5/2011
20
Caregivers
Average age of AD caregivers was 49
80% AD caregivers are working
80% of women are between 25‐54 are 5 54working caregivers
27% of Latino households provide informal caregiving
Latina caregivers begin caregiving at earlier age compared to EA caregivers
(Mausbach, et al., 2004; Aranda & Knight, 1997; Alzheimer’s Association, 2011)
Pt Health and Caregiving Research
Health risks increased risk vascular dementia (Han et al, 2003); Higher rates of diabetes leading to complications (Flores diabetes leading to complications (Flores, 2002)
MA caregivers typically do not utilize formal dementia evaluation or make use of available resource until later stages (Neary & Mahoney, 2005; Morano & Bravo, 2002)
Pt Health and Caregiving Research
Studies from H‐EPESE showed that despite increased disability including physical and emotional impairment, elderly MA’s continue to live in the e de y s co t ue to e t ecommunity (Angel, Angel, Aranda, Miles, 2004)
• MA elderly continue to rely on family for support (Angel & Angel, 1998); other studies show MA elderly identified fewer social support networks (Phillips et al, 2000)

10/5/2011
21
Psychological Impact
Women had higher levels of burden
or strain than men (Yee & Schultz, 2000).
Depression most important potential d f i adverse consequences for caregivers
(Covinsky, Newcomer, Fox, Wood, Sands, Dane, & Yaffe, 2003, p. 1006).
Predictors for institutionalization:
‐Burden, pt deterioration
Predictors for not placing in NH:
‐Race & Ethnicity (Schultz et al., 2004).
Health Literacy
a person’s understanding of a specific health technical language and its language and its accompanying instructions
.
Disparity in Health Literacy• Minority older adults have lower health literacy skills compared to European Americans.
Over half have 8 years of schooling or less & 1 i L i ld h f l d i in 10 Latino elders has no formal education. (Alzheimer’s Association, 2004)
Latinos are not receiving health care information needed to reduce their risk for dementia and/or to reduce associated CG stress
10/5/2011
22
Role of Culture in CaregivingLatino/Hispanic caregivers: higher levels of self‐efficacy compared to EA caregivers
Latina daughters higher self‐efficacy:g g yseeking respiteresponding to disruptive behaviorscontrolling upsetting thoughts about caregiving
(Depp et. al., 2005)
Cultural Competency
The knowledge and interpersonal skills that allows providers to understand, appreciate, and work with individuals from cultures other than their own
It i lIt involves:
acceptance of cultural differences
self‐awareness
knowledge of the patient’s culture
adaptation of skills and changing interventions
Davis BJ, Voegtle KH. Culturally Competent Health Care for Adolescents: A Guide for Primary Health Care Providers.Chicago, IL: American Medical Association, (1994)
Cultural Competence in Service Delivery
Language
Culture
Inclusion of all family not just primary caregiver (e.g. shift care dynamics)
Continuity in Outreach Efforts
Education‐interactive, audiovisual, visual

10/5/2011
23
Acculturation Continuum
Retention of values & beliefs from one’s own
culture
Adoption of mainstream values & beliefs
Valle, 1989
Core Cultural Themes Familismo
Personalismo
Jerarquismo
Espiritismo
Presentismo
Respeto
Table 1. Hispanic/Latino Cultural Themes That Can
Influence Beliefs and Practices Concerning Caregiving
DecisionsTheme Meaning Implications for
Practioners
Familismo Emphasis on the well‐
being of the family
over the individual
Include family
members in pt
care decision‐
making
Source: Adapted from Cuellar (1990) & Perkins, Supik & Hazuda, (1993)
Learn about pts
and culture
Providers should
start discussions
about LTC planning
early in diagnosis
10/5/2011
24
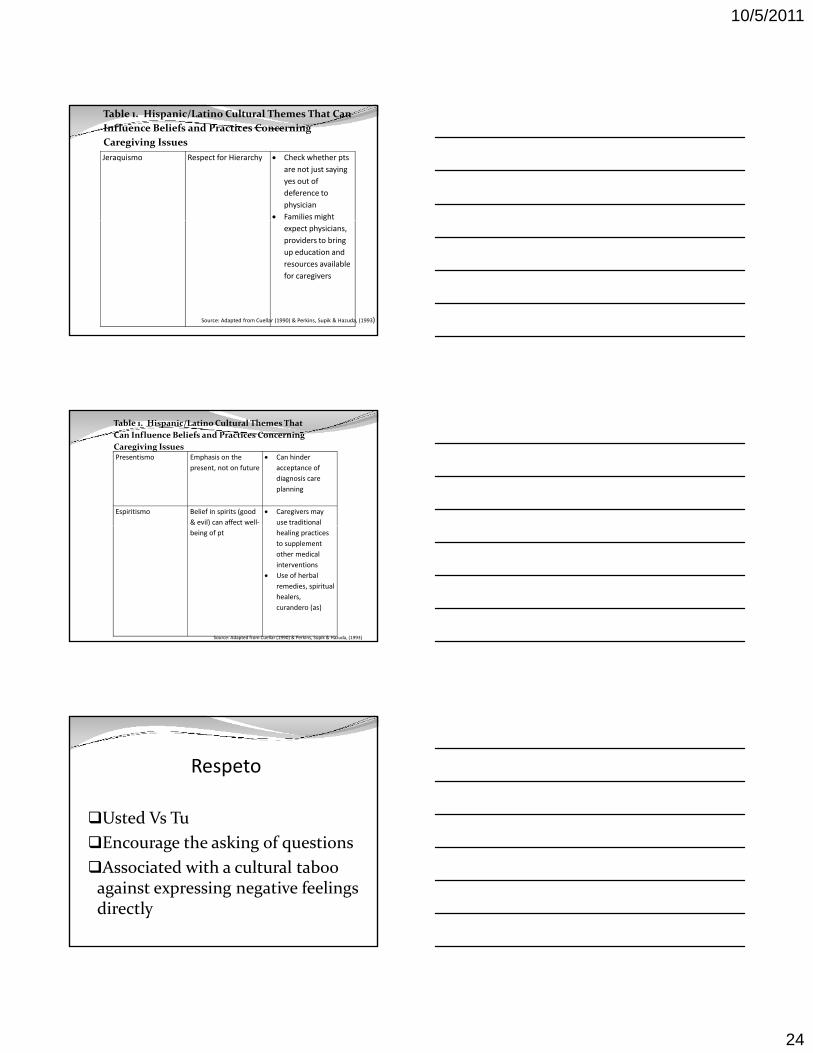
Jeraquismo Respect for Hierarchy Check whether pts
are not just saying
yes out of
deference to
physician
Families might
Table 1. Hispanic/Latino Cultural Themes That Can
Influence Beliefs and Practices Concerning
Caregiving Issues
g
expect physicians,
providers to bring
up education and
resources available
for caregivers
Source: Adapted from Cuellar (1990) & Perkins, Supik & Hazuda, (1993)
Presentismo Emphasis on the
present, not on future
Can hinder
acceptance of
diagnosis care
planning
Espiritismo Belief in spirits (good
& evil) can affect well‐
Caregivers may
use traditional
Table 1. Hispanic/Latino Cultural Themes That
Can Influence Beliefs and Practices Concerning
Caregiving Issues
being of pt healing practices
to supplement
other medical
interventions
Use of herbal
remedies, spiritual
healers,
curandero (as)
Source: Adapted from Cuellar (1990) & Perkins, Supik & Hazuda, (1993)
Respeto
Usted Vs Tu
Encourage the asking of questions
Associated with a cultural taboo against expressing negative feelings directly

10/5/2011
25
Use of alternative medicineHispanic patients may bring quite a broad definition of health to the clinical or diagnostic.
“Botanicas, mal de ojo, empasto, culebrilla”
Different Latinos use different interpretations of language, customs, and beliefs
A Primer for Cultural Proficiency: Towards Quality Health Services for Hispanics. National Alliance for Hispanic Health 2001
Traditional Beliefs on Healing
Curanderas (herbal/traditional healer)
Espiritistas (spiritual healer)
Courtesy of Dr. Dolores Gallagher‐Thompson, Ph.D., ABPPConsuelo Juarez, Health Educator
Six Approaches for Bridging Language Barriers(most to least effective)
(1) Bilingual/Bicultural
Professional Staff
(2) Interpreters
4) Internal Language Banks
(only as a backup)
(5) Phone‐Based Interpreter (3) Language Skills
Training for Existing
Staff
Services
(emergency back‐up)
(6) Written Translations
A Primer for Cultural Proficiency: Towards Quality Health Services for Hispanics. National Alliance for Hispanic Health 2001
10/5/2011
26
Latino Caregiver InterventionsEl Portal
Alzheimer’s Association
REACH I iREACH Interventions
REACH fotonovela
Cuidando con Respeto
Latino Caregiver Interventions
El Portal‐Model Program (Aranda, Villa, Trejo,
Ramirez, Ranney,2003)
Alzheimer’s Association Support ppGroups & Resources (Diversity Tool Kit)
On the Horizon: REACH II Intervention Program
Coping with Caregiving Program
Fotonovela Project 3‐year project (2010‐2012) designed to meet the needs of Latinos with low literacy for health care information
Funded by the national office of the Alzheimer’s Assn‐Collaborators :Dr. Ramon Valle (San Diego State Univ.) and Dr Ladson Hinton (UC Davis)Dr. Ladson Hinton (UC Davis)
Year 1: created the Fotonovela: 20 pages in Spanish & 20 pages English.
Content based on 10 focus groups held with professionals and Latino caregivers in northern and southern CA

10/5/2011
27
Managing Difficult Behaviors Fotonovela
Educational fotonovela is an adaptation of a
popular culture medium used extensively to impart p p y p
health care information
Combines “education” and “entertainment”
Has “vicarious modeling” potential
Specifically targets low‐literacy (6th grade & below)
Hispanics/Latino population
The Jiménez family…
The Storyline… Getting an Alzheimer’s diagnosis
Caregiver in stress, including scenarios like: reacting to a confused grandmother; safety concerns ‐ burning pots and pans; and dealing with a “not quite on board” brother.
Coping StrategiesTh “di t ti ” t h i The “distraction” technique
Seeking support from family, friends, and community resources (i.e. support group, adult day care center
Family meeting mediated by a social worker
Other Information What is dementia?
Tips on taking better care of YOURSELF
Depression checklist
Final Product – new Fotonovela

10/5/2011
28
CUIDANDO CON RESPETOS. Liliana Oakes M.D.
Melissa Talamantes PsyDJeanette Silva Ross M.D
Cindy Alford PhD
Cuidando con Respeto
Adapted from the Savvy Caregiver Program (SCP), a psychoeducational program for caregivers of persons with dementia in Minnesota
Program develops caregiver skill, knowledge, reduces caregiver burden and distress
Telenovela/Fotonovela SiempreViva—Story of Margarita who begins to have memory decline and her families response
Fotovelas/Telenovelaswere derived from Margarita’s character
Fotonovela’s/Telenovelas depict challenging situations and require open discussion by caregivers and active participation in activities
(Aranda, Siempre Viva, 1989; Oakes, Ross, Talamantes, Espino, 2006)

10/5/2011
29
Cuidando con Respeto Adaptation incorporated
relevant language & cultural content processes using Novela teaching approach drawn from approach drawn from Siempre Viva (Aranda, 1989)
3 additional mini novelaepisodes depicting a family struggling with AD
Interaction from participating caregivers regarding CG issues
Goals of Cuidando con Respeto To adapt a successful English language caregiver training program (Savvy caregiver Program) for Spanish Speaking Caregivers
To increase caregiver’s knowledge, improve attitudes, and develop knew skills in caregiving
To evaluate the use of the novela (soap opera) style as an innovative teaching method
(Aranda, Siempre Viva, 1989; Oakes, Ross, Talamantes, Espino, 2006)
Culturally Interactive Program
Telenovela
Fotonovela
GamesGames
Videos
Small group activities

10/5/2011
30
Program Topics
Session 1
Introduction to AD
Effect of AD on Thinking
Effect of AD on Feelings
Session 2
Three Stages of AD (Video)
Strategies for Dealing g
Goal for the Work of Giving Care
Managing Illness Responses
with Daily Care & Complicated Behavior
Self‐Care of caregiver
Partnership with Alzheimer’s Association with funding from Administration on Aging –Evidence Based Latino Caregiver Intervention
Train the Trainer Program
Cuidando con Respeto in California
Train the Trainer Program
Disseminate Training to 300 Caregivers
Formative Evaluations and Qualitative follow up phone contact yielded strongest evidence for effectiveness of the class
Insert Cuidando telenovela
10/5/2011
31
Culturally Responsive Research & Interventions New Paradigm Shifts‐Compared to applying existing caregiving (EU) models to emphasize the cultural constructs and phenomena relevant to Latino caregiverscaregivers
Challenges‐understanding the cultural influences and how MA and other Latino caregivers understand & cope with AD and dementia
Selected References1. Alzheimer’s Association. (2004). Hispanics/Latinos and Alzheimer’s Disease.
Retrieved November 14, 2008, from http://www.alz.org/national/documents/report_hispanic.pdf
2. Centers for Disease Control and Prevention. (2007). The state of aging and health in America 2007. Retrieved November 14, 2008, from http://www.cdc.gov/aging/saha.htm
3. Family Caregiver Alliance. (2004). Cultural competency in working with Latino 3 y g 4 p y gfamily caregivers. Retrieved November 14, 2008, from http://www.caregiver.org/caregiver/jsp/content_node.jsp?nodeid=1095
4. Gallagher‐Thompson, D. & Coon, D.W. (2007). Evidence‐Based Psychological Treatments for Distress in Family Caregivers of Older Adults, Psychology and Aging, 22, 37‐51.
5. Hepburn, K., Lewis, M., Sherman, C.W., Tornatore, J. (2003). The Savvy Caregiver Program: Developing and Testing a Transportable Dementia Family Caregiver Training Program. The Gerontologist, 43 (6), 908‐915.
Selected References
6. Oakes, Hepburn K, Ross J., Talamantes, M., & Espino, D. (2006). Reaching the heart of the caregiver. Clinical Gerontologist, 30(2) 37‐ 49.
7. Pinquart, M., & Sorensen, S. (2005). Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: A meta‐analysis. The Gerontologist, 45, 90‐106.
8 Talamantes M A & Aranda M P (2004) Cultural competency in working with 8. Talamantes, M.A. & Aranda, M.P., (2004). Cultural competency in working with Latino family caregivers. Monograph in Family Caregiver Alliance, National Center on Caregiving. http://caregiver.org
9. Talamantes, M. A., Trejo, L., Jiménez, D., & Gallagher‐Thompson, D. (2006). Working with Mexican American familias. In G. Yeo & D. Gallagher‐Thompson, D. (Eds.), Ethnicity and the dementias (2nd ed.), 327‐340. New York: Routledge Taylor and Francis Group.
10. US Census Bureau. (2005). 65+ in the United States: 2005. Retrieved November 14, 2008, from http://www.census.gov/prod/1/pop/p23‐190/p23‐190.html
11. Valle, R. (1988). Caregiving Across Cultures. Washington, DC: Taylor & Francis

10/5/2011
32
PartnershipsAlzheimer's Association:
http://www.alz.org
We Speak Spanish
1.800.272.3900 ‐ Call us anytime for free, confidential guidance and reliable information.
Message Boards‐ Find bilingual support and advice in a caring community.
For Further Information :
For Cuidando con Respeto information contact Dr. Liliana Oakes by email: [email protected] or Dr. Melissa Talamantes at [email protected]
For Fotonovela Project contact Dr. Dolores Gallagher Thompson by email: [email protected]
The National Office of the Alzheimer’s Assn has a 24‐hour helpline: 1.800.272.390 and excellent website: [email protected]
Questions











![Welcome! []...Welcome! 1 Thank you for participating in our third of three webinars in the Mental Health First Aid First Nations Webinar Series. As you prepare for the webinar, please](https://static.fdocuments.net/doc/165x107/60e62b8522bd56180f76fe01/welcome-welcome-1-thank-you-for-participating-in-our-third-of-three-webinars.jpg)






