Thames Valley Strategic Clinical Networks A Regional ...
162
Thames Valley Strategic Clinical Networks With keynote presentations from National Directors and local leaders in the provision and care of Dementia patients and older people. This will be your opportunity to gain insight into the current provision of services in Thames Valley and beyond, to hear a vision of the future in Dementia care and to participate in shaping how Thames Valley collectively meets the 2014/15 Dementia challenge. Time: 09:30 – 16:30 (registration at 09:00) with networking lunch provided. Representation is encouraged from all health, social and voluntary care sectors. To register CLICK HERE* Please note that places are limited so register soon to ensure your place. For all enquiries please contact [email protected] *or type into your browser. http://www.eventbrite.co.uk/e/thames-valley-scn-dementia-conference-tickets-10077497065 A Regional Dementia Conference Tuesday 25 th February 2014 at the Kassam Stadium, Oxford, OX4 4XP The Thames Valley Strategic Clinical Networks are pleased to announce a regional Dementia conference. This will be a unique opportunity for all those involved in the provision of patient care and the commissioning of Dementia services to hear from leading national thinkers and to discuss local examples of excellence.
Transcript of Thames Valley Strategic Clinical Networks A Regional ...

Thames Valley Strategic Clinical Networks
With keynote presentations from National Directors and local leaders in the provision and care of Dementia patients and
older people. This will be your opportunity to gain insight into the current provision of services in Thames Valley and
beyond, to hear a vision of the future in Dementia care and to participate in shaping how Thames Valley collectively meets
the 2014/15 Dementia challenge. Time: 09:30 – 16:30 (registration at 09:00) with networking lunch provided.
Representation is encouraged from all health, social and voluntary care sectors. To register CLICK HERE* Please note
that places are limited so register soon to ensure your place. For all enquiries please contact [email protected]
*or type into your browser. http://www.eventbrite.co.uk/e/thames-valley-scn-dementia-conference-tickets-10077497065
A Regional Dementia Conference Tuesday 25th February 2014 at the Kassam
Stadium, Oxford, OX4 4XP
The Thames Valley Strategic Clinical Networks are
pleased to announce a regional Dementia conference.
This will be a unique opportunity for all those involved in the provision of
patient care and the commissioning of Dementia services to hear from
leading national thinkers and to discuss local examples of excellence.

________________________________________________________________________________________
alzheimers.org.uk
Thames Valley Strategic Clinical Networks Dementia Conference
Engaging Patients and Carers
Angie Newing Operations Director (South)
Alzheimer’s Society

Dementia: the size of the challenge
________________________________________________________________________________________
alzheimers.org.uk

• Government committed to transforming
participation
• Coordination of care is not meeting people’s
needs.
• Must filter national commitments into local
action and benefit
Integrated and personalised care
is essential for people to live
well with dementia
________________________________________________________________________________________
alzheimers.org.uk

• More than 23,000 people with dementia in the
Thames Valley area
• Stigma, misconception and social isolation
• Want to get involved and make a difference
• Ensures work is focusing on the identified needs and
issues
• Gives everyone’s work credibility – tried and tested
• Organisations will know why and how to improve
their services
________________________________________________________________________________________
alzheimers.org.uk
Involving people with dementia

________________________________________________________________________________________
alzheimers.org.uk
Shaping local health
and social care services
Crawley Forward Thinking Group
Berkshire Empowerment Group

________________________________________________________________________________________
alzheimers.org.uk
The ongoing dialogue ……
•How •Considerations •Resources

Dementia friendly communities - Untapped potential for
local solutions in the
community.
- Join your Dementia
Action Alliance
- Be part of a Dementia
Friendly Community
- Become a dementia
friend.
________________________________________________________________________________________
alzheimers.org.uk

________________________________________________________________________________________
alzheimers.org.uk
Thank you
Any questions?
www.alzheimers.org.uk
Help line number: 0300 222 1122

The Primary Care Diagnosis and Management of Mild Cognitive
Impairment and Dementia
South West Oxfordshire Locality 2013 in collaboration with Older Adult Mental
Health Services
Dr Julie Anderson, GP Berinsfield Health Centre, SWOL

What are we trying to achieve?
• To raise professional awareness & understanding of dementia to ensure its early and timely diagnosis with follow up treatment, advice and support in SWOL
• To raise professional awareness & understanding of dementia to facilitate choice and control over the quality of life of both patients and carers in SWOL

Primary Care Memory Assessment Service
• This is an alternative to the usual secondary care memory clinics in South West Oxfordshire Locality
• The secondary care memory clinics can still be
accessed if required but would not be necessary to make the diagnosis of dementia
• The primary care memory assessment service has been designed to ensure high standards of care for an accurate and timely diagnosis with appropriate condition management

Why should Primary Care Get More Involved?
• Estimated that only about 1/3 of people with dementia receive a formal diagnosis
• Primary Care well placed to identify people with mild cognitive impairment and dementia
• Such people often already have other health problems and managing multiple conditions in the same patient allows for more coordinated and appropriate care
• The assessment and evaluation process to diagnose most people with dementia can be carried out more quickly in primary care
• GP practice is the natural link or hub to liaise the various care needs

Problems with diagnosis
Large majority of people with dementia either do not receive a diagnosis at any stage or only late/in crisis when often too late to prevent harm such as breakdown of care and institutionalisation. •Reluctance to pursue diagnosis in early stages •Stigma attached to diagnosis •Reluctance to disclose possible diagnosis of dementia •Culture of “concealment, minimisation or ignoring early symptoms and signs”

Typical patient with dementia journey
• Joan age 84 referred to specialist (elderly CMHT)with memory problem Dec 2011
• Missed appointments, not seen until Oct 2012 and diagnosed with “probably Alzheimer’s”
• Started on donepezil and due to be reviewed in clinic but lost to follow up
• Presented in crisis summer 2013 self-neglecting (sister who was main carer had gone away)
• Admission JR2 chest infection 3 weeks, home 5 hrs after discharge and found on floor, sister called ambulance, readmitted JR2 for 3 months waiting for permanent nursing home

Alternative patient with dementia journey
• Joyce age 85 referred memory difficulty to elderly CMHT Dec 2012-assessed April 2013 and diagnosed “mild memory disturbance”, discharged
• Admitted JR2 after found on floor, abdo pain, diagnosed with constipation and discharged after 1 week
• Carer expressed further concern re ability to function to GP • Seen in GP memory assessment service, diagnosed with
vascular dementia and care plans made including advanced care planning and anticipatory care re hospitalisation
• All documented in medical records and copies in Joyce’s home
• Subsequently found on path outside house with facial injury, carers contacted GP rather than calling ambulance, assessed at Abingdon Emergency Medical Unit and discharged following day after some iv fluids.

Diagnosis of dementia
• Easy in the later stages, hard in the very early stages
• Essentially a clinical diagnosis
• Based on formal cognitive assessment and estimation of functional impairment
• Requires exclusion of other possible causes of cognitive impairment
• Mild memory loss alone is not sufficient to make diagnosis-needs to be some loss of executive function that has no other cause.

Early Diagnosis versus Timely Diagnosis
• Early diagnosis means arranging formal memory assessment when the patient presents with a possible memory problem
• Timely diagnosis allows patient and families to plan ahead and help ensure cognitive function and patient’s independence is preserved for as long as possible

Issues in early stages of dementia
• Clarity about diagnosis
• Helping patient and family plan in advance for loss of capacity (enabling patients to make decisions about hospital care, life-prolonging treatment and financial arrangements while they still have capacity)
• Maximising patient function by treating any co-existing disorders and prolonging independence
• Providing information about advisory and support services
• However, the window of opportunity for patients and their families to plan while the patient still has capacity can be small

The SWOL Primary Care Memory Assessment Service
This based on:
• The GPCOG (GP assessment of cognition)
• A 3 stage assessment process to evaluate memory problems, exclude other conditions and/or identify problems that may be impacting on memory/function
• Recording all the relevant data on a computer template

Types of cognitive assessment
Lots!
•Mini-Mental State Examination-still the usual formal test but takes 8 mins and under copyright
•GP Assessment of Cognition (GPCOG)- takes only a few minutes and widely available www.gpcog.co/au or http://www.patient.co.uk/doctor/general-practitioner-assessment-of-cognition-gpcog-score
•6-item Cognitive Impairment Test (6-CIT) – use limited by complex scoring
•Abbreviated Mental Test (AMT)-used in hospitals but not recommended for diagnostic purposes

What about other tests?
• Other tests commonly done in specialist memory clinic settings include CLOX (Clock Drawing Tests)
• HVLT-R (Hopkins Verbal Learning Test-revised)
• MOCA (Montreal Cognitive Assessment)-available at: www.mocatest.org
• All are validated in dementia to assess memory and/or executive function but none has any greater diagnostic accuracy overall than MMSE, GPCOG or 6-CIT

Impairment in Executive Function
• Whatever cognitive assessment scoring method is chosen, diagnosis of dementia cannot be made safely without some impairment in executive function
• Executive function is umbrella term for distinct, high-level cognitive processes that control everyday thoughts and actions including working memory, attention span, planning, control of behaviour, complex motor tasks and ability to understand concepts.
• Growing evidence that executive impairments present even in early stages of Alzheimer’s Disease

How to assess functional impairment (1)
• Lots of different tests eg the 70-point ADCS-ADLS (Alzheimer’s Disease Collaborative Study-Activities of Daily Living Inventory), Disability Assessment for Dementia, Bristol Activities of Daily Living Scale (BADLS)
• None is proven to be better than another and all have limitations
• There is also no consensus or evidence to link a numerical score to level of functional impairment in practice

How to assess functional impairment(2)
• For the purposes of the PCMAS, the results of the BADLS questionnaire can be used to summarise the level of functional impairment without formally scoring responses.
• Note the GPCOG (IQ) also assesses executive function
• A record of assessment and impairment in activities in everyday life and also in activities of personal care should be made

First assessment
• Patient presents with possible memory problem to GP
• Initial consultation to include GPCOG (patient) and GPCOG(IQ) if needed/possible
• Checklist to include 1. Gradual onset (if not, ensure no acute problem such as UTI) 2. Mood (depression?) Supply PHQ9 if indicated. 3. Review of possible drugs causing cognitive impairment? e.g.
anticholinergic, sedating tricyclics, sedating antihistamines, opiates, benzodiazepines
4. Excess alcohol? 5. PMH of cancer or recent head injury? 6. Recent acute organic illness, e.g. pneumonia, UTI. If so, review at a
suitable interval and do not carry out a GPCOG at this stage • Record on computer dementia diagnostic pathway template

When to consider specialist referral after this initial assessment
Those with cognitive impairment/likely dementia in the following categories: 1.Patients under the age of 65 should be referred to a neurologist 2.Patient with a co-existing serious psychiatric disorder should be considered for referral to an old-age psychiatry service 3.Those in whom there is considerable behavioural disturbance should be referred to the old-age psychiatry service 4.Other factors that make assessment in primary care unreliable or challenging, e.g. learning disability, cerebral palsy The dementia screening blood tests should still be carried out in primary care and results given in referral letter. Anyone else with cognitive impairment based on history and initial GPCOG not in the above categories can be managed in the primary care memory assessment service (PCMAS)-ask patient/carer to book second assessment (20 minute appointment with practice nurse) and third assessment one week later (20 minute appointment with GP)

Second assessment (with practice nurse )
1. Arrange GPCOG (IQ) if not already done but indicated 2. Arrange depression screen if not already done 3. Assessment of any functional impairment eg. by asking by
carer/close relative to complete form, Bristol Activities of Daily Living Scale (BADLS)
4. Repeat GPCOG (patient) 5. Ask if any problems with hearing/eyesight/continence problems 6. Ask if any falls/mobility problems 7. Dementia screening blood tests (as on ICE) 8. Urine dip to exclude UTI 9. BMI (weight loss?), pulse (AF?) and BP 10. Check patient has GP appointment about one week later for third
assessment 11. Enter data from this assessment on computer template

Third assessment ( 20 minute appointment with usual GP)
• With patient and relative/carer • Review results from 1st and 2nd assessments • Obtain more detailed history about the pattern of cognitive
decline if needed: length of history, fluctuations, changes in personality, altered behaviour, other symptoms such as hallucinations
• Examine for any other abnormalities e.g. signs of Parkinson’s • Treat/address any possible factors that could be causing
cognitive impairment especially depression (poor concentration in depression often lowers cognitive scores)
• Consider need for CT scan • Enter data from this third assessment on GP system recording
template

When to consider CT scan brain
The rationale for a CT scan is to exclude other pathology that could be responsible for patient’s decline in cognitive function such as space-occupying lesions. It is not to differentiate types of dementia although the scan may report corroborating features such as cerebral atrophy
Age 65 or less Age 65-79 Age 80+
Not suitable for primary care management-refer secondary care service
Arrange scan unless history of gradual memory decline over 1 yr and no atypical features
Only scan if: • Recent head injury • History of malignancy • Rapid unexplained
deterioration • Unexplained focal
neurological symptoms and signs including early urinary incontinence or gait disturbance

Management of Mild Cognitive Impairment (not bad enough to diagnose dementia)
• Important not to make false positive diagnosis of dementia. Many with MCI will remain stable and not develop dementia but a substantial minority will develop dementia in time
• No suitable Read code for MCI so record on computer as Mild Memory Disturbance
• No evidence that Acetylcholinesterase (AChE) Inhibitors are of any benefit at this stage
• Some evidence that cognitive stimulation is beneficial in MCI
• Offer review and repeat testing in 6-12 months as progressive nature of dementia will become evident with time
• Encourage healthy lifestyle and address any vascular risk factors.

Giving a diagnosis of dementia
• Only once all the relevant information collected and reviewed
• Use principles of breaking bad news • Ensure family member or carer present • Explain that tests seem to show that patient does have a
problem with their memory which is affecting how they manage day to day activities
• Ask patient if they are aware what the diagnosis might be • Would they like you to explain what you think the diagnosis
is? • If so, use the term dementia and explain this is likely to get
worse in time but probably only slowly • Always supply some written patient information Eg: http://www.patient.co.uk/health/memory-loss-and-dementia

Initial management of dementia
• Treat any modifiable conditions-anxiety and depression are common features in early dementia
• Supply contact details Dementia Advisor and make referral
• Advise re DVLA
• Address “thinking ahead issues” eg giving Lasting Power of Attorney to trusted carer for financial matters +/- welfare issues while patient still has capacity
• Consider trial of Acetylcholinesterase (AChE) inhibitors

Actions for patient/carer to consider
• Read the Patient information supplied including one re drug treatment if appropriate
http://www.patient.co.uk/health/memory-loss-and-dementia
http://www.patient.co.uk/health/medicines-for-dementia
• Advise must notify DVLC (see next slide)
• Contact Dementia Advisor

Implications for drivers • Must inform DVLA if diagnosis is dementia or if MCI and
concerns re driving
DISORDER GROUP 1 ENTITLEMENT ODL – CAR,
M/CYCLE GROUP 2 ENTITLEMENT VOC – LGV/PCV
(LORRY/BUS)
MILD COGNITIVE IMPAIRMENT (MCI)
If there are no effects on driving then
DVLA does not need to be notified; if
however there are any concerns that
driving may be adversely affected then
DVLA should be notified to allow enquires to take place.
If there are no effects on driving then
DVLA does not need to be notified; if
however there are any concerns that
driving may be adversely affected then
DVLA should be notified to allow enquires to take place.
DEMENTIA OR ANY ORGANIC BRAIN SYNDROME
It is extremely difficult to assess driving
ability in those with dementia. Those
who have poor short-term memory,
disorientation, lack of insight and
judgement are almost certainly not fit to drive. The variable presentations and rates of
progression are acknowledged.
Disorders of attention will also cause
impairment. A decision regarding
fitness to drive is usually based on medical reports. In early dementia when sufficient skills
are retained and progression is slow, a
licence may be issued subject to
annual review. A formal driving
assessment may be necessary (See Appendices 1 & 2).
Refuse or revoke licence

When to consider specialist referral after this
third assessment
• Patient/family/carer wish for second opinion.
• GP concern or uncertainty about the diagnosis
• Significant behavioural or psychiatric problems (consider trial of antidepressants first if possible, including those with sedating or anxiolytic affects if required such as trazodone)
• Atypical dementia features e g. hallucination for Lewy Body dementia, dementia in Parkinson’s Disease, fronto-temporal dementia

Prescribing Protocol for AChE inhibitors
• This has been developed to the diagnosis and management of dementia in primary care and covers the initiation of AChE inhibitors which has been authorised by the Area Prescribing Committee (Oxfordshire) for the purposes of this SWOL initiative.
• It describes how to start treatment, intervals for review and stopping the drugs in those who do not respond or those who progress to severe dementia in time.
• Available on SWOL intranet at: http://opct.oxnet.nhs.uk/OCCG/Pages/Dementia.aspx

Useful resources
• www.alz.org • www.alzheimers.org.uk • www.dementiaweboxfordshire.org.uk (useful resources for
patients/carers about local services and the excellent Guidepost publications)
• Resources for the SWOL PCMAS for professionals all at: • http://nww.oxfordshirepct.nhs.uk/OCCG/Pages/CollaborativeDemen
tiaPilot.aspx Including: • Protocol for the Primary Care Diagnosis and Management of Mild
Cognitive Impairment and Dementia • Computer recording template with appropriate codes for the 3
stages of assessment • Protocol for AChE inhibitor Prescribing in Primary Care • Accessing Dementia Advisors (referral form and leaflet to hand out) • Various forms such as BADLS

How will we know that the project has been a success?
• Increase diagnosis rate of people with dementia
• Increase in the number of patients receiving a memory assessment in primary care
• Increase the number of carers who say they are very satisfied with services to at least the national average, once comparative data is available (currently 39%)

Oxford Academic Health Science Network
Rupert McShane
Consultant Old Age Psychiatry

15 AHSNs nationally Funded by NHS England 5 year Licence – 2013-18 Speed Innovation Improving collaboration NHS – Industry – Research Best Care Clinical Networks - Unwarranted variation Informatics Patient and Public Involvement and Experience
The Oxford Academic Health Science Network

Range of Projects
• Collaboration – webinars
• Information – eSilver Book: Microsoft Health Vault – SMS collection of PROMS and Resource Use: True Colours
• Food industry – Taste of a ‘fuel for thought’
• Devices – Chipped tablets
• Services – Neighbourhood Return – Franchises?

MSc in Evidence Based Medicine Deadline March 16th
• Part time – Usually 3 years – Starts Autumn 2014
• AHSN funds 7 Fellowships • 6 x 1 week taught modules
– Usually in first 2 years – Assignments of up to 4,000 words
• Dissertation project – Up to 10,000 words – Supported by AHSN

Range of Projects
• Collaboration – webinars
• Information – eSilver Book: Microsoft Health Vault – SMS collection of PROMS and Resource Use: True Colours
• Food industry – Taste of a ‘fuel for thought’
• Devices – Chipped tablets
• Services – Neighbourhood Return – Franchises?

Dementia Clinical Network Launch Hedsor House, Nr Marlow
14th May 3.30pm-8pm

Range of Projects
• Collaboration – webinars
• Information – eSilver Book: Microsoft Health Vault – SMS collection of PROMS and Resource Use: True Colours
• Food industry – Taste of a ‘fuel for thought’
• Devices – Chipped tablets
• Services – Neighbourhood Return – Franchises?

Dementia Clinical Network Launch Hedsor House, Nr Marlow
14th May 3.30pm-8pm

Range of Projects
• Collaboration – webinars
• Information – eSilver Book: Microsoft Health Vault – SMS collection of PROMS and Resource Use: True Colours
• Food industry – Taste of a ‘fuel for thought’
• Devices – Chipped tablets
• Services – Neighbourhood Return – Franchises?

MSc in Evidence Based Medicine Deadline March 16th
• Part time – Usually 3 years – Starts Autumn 2014
• AHSN funds 7 Fellowships • 6 x 1 week taught modules
– Usually in first 2 years – Assignments of up to 4,000 words
• Dissertation project – Up to 10,000 words – Supported by AHSN

Range of Projects
• Collaboration – webinars
• Information – eSilver Book: Microsoft Health Vault – SMS collection of PROMS and Resource Use: True Colours
• Food industry – Taste of a ‘fuel for thought’
• Devices – Chipped tablets
• Services – Neighbourhood Return – Franchises?

Next step
• Collaborate…….
• Use webinar to hear about projects
• Decide new projects

EARLY DIAGNOSIS AND SUPPORT
DR KATIE SIMPSON
MENTAL HEALTH GP LEAD BERKSHIRE EAST CCG FEDERATION

DIAGNOSIS

TRAINING
• Protected Learning Time Events all CCGs Berkshire East
• Working with ADS/ Triple A • Dementia CD RoM BHFT to all practices • Continuing Lunch Time sessions on
request • Dementia Challenge Care Homes project • Managing end of life in dementia Jan 14

CODING
• BHFT Contract 2012/13 all practices issued with a list of patients active to the memory clinic
• Coding after consultation with Dr Sube Banerjee
• Annually updated

Detection
• Dementia DES • AT RISK: Offered screen 60YRS: CHD, CVA, PVD 40YRS: Downs Syndrome 50YRS: LD, Long term Neurological conditions
• Referred Memory Services and offered Rx
• Health Checks offered to carers of people with
dementia

MCI

SUPPORT

Understanding dementia courses for carers
• 6 sessions each 2 hours
• 30 per course
• 45% of carers accept
• April 13- Dec 13 164 carers
• Waiting times 4/12
• High satisfaction > 85%

ADS
• Advice & information by phone, email, • Help line • Home visits • Advocacy • Help completing forms • Newsletter • Be-friending service • Interagency referrals • Pilot for Singing for Life music box • Holiday weekends - 3 planned for 2014!!

ADS
• Weekly Drop ins (peer support, advice, friendship)
• Lunch clubs
• Pamper afternoons
• Singing for Pleasure
• Out & About for people with early dementia and mobile
• Moves and Grooves
• Evening Alzheimer’s Cafe
• New Asian speaking dementia adviser in GP surgeries on a roving basis trying to reach these communities
• Dementia awareness training

Dementia Directory
• Provide a single point of information for services in the local area
• Better and quicker access to information on dementia services
• Access for all by producing the directories in other languages, large print and other formats
• Provide information on services that people with dementia and their carers may not have otherwise known about

Dementia Directory
• To support people to have a better quality of life. • Reduce isolation for people living with dementia and
their carers. • An easy to read and straight forward directory. • Provide additional information on benefits, legal
information, support networks, finding the right care home, home care provision and telecare.
• Provide current and reliable information that is regularly updated.

Improving Care Home & Secondary Care Environments

Different types of signage


Memory Clinic and support programme
Ageing Well events
Community Services
MULTIPLE STAKEHOLDER PROJECT -A TAILORED, LOCALISED APPROACH TO INTRODUCING MEMORY TESTING
AS PART OF A “HEALTHY MIND, HEALTHY BODY” CAMPAIGN
PPGs What do
patients need and want?
Practice Nurses
Undertake memory test
as part of regular in-
house clinics
Practice Managers
Devise the plan/
business case &
support PPG ideas
GPs
Regular patient case contact
Review results of 6-CIT scores and make referrals
Collaborative programme for 3 different GP practices led by Patient Participation Groups
WAM Dementia Awareness Project

WHY THIS PROJECT IS IMPORTANT
To enhance quality of life for patients and carers • Enable patients to know, understand and manage their condition at an early stage –
and have better quality of life
• Promote a dignified and compassionate approach to patient needs
• Enables carer education and support to be mobilised more effectively
To create a positive community impact • Reduce the “fear” and stigma of memory testing – reassuring and positive approach,
careful choice of language
• Build on existing relationships between patient and GP practice staff
• Reinforce positive Ageing Well messages for all older patients
• Involve local organisations
• To save money
• To design and deliver an innovative project that would inform future
investment in memory clinic capacity and support services for dementia
patients and carers
Working together locally to deliver sustainable excellence in healthcare
WAM CCG Working together locally to deliver sustainable excellence in healthcare

What happened next?
Intensive 6 month programme alongside 2 days /week in WAM CCG practice – Supported by Oxford Deanery:
Work alongside memory clinic team to review current practices to maximise capacity and enhance quality in the immediacy
Work with multi disciplinary LTC community based teams to include & develop support for dementia patients and carers
Extend 6-CIT training to practice nurses and GPs

What next?
Work with practice managers on integration of dementia screening & dementia awareness for all staff
Develop third sector services & telehealth support
GP education/refresher at GP EPIC & lunch time practice meetings
Review options for increasing capacity and closer working with Social Care teams to offer integrated, outcome based services

Dr Brian Murray
Consultant Older Adult Psychiatrist and Clinical Director

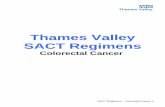
48% diagnosed Aylesbury CCG 38% Chiltern CCG
The MACH clinic project, Bucks
TARGET: 70% diagnosed

Dementia Diagnosis map of UK

Where we are : •Stretched capacity – waiting times
•Inconsistent model
Where we want to be : • Reduced waiting lists • Same day assessment &
diagnosis
• Greater capacity
• Diagnosis closer to home
The MACH clinic project, Bucks

Why is it important?
• Getting an early diagnosis means;
‒ Maximise your quality of life
‒ Gain access to information, resources and support
‒ Benefit from treatments
‒ Plan for the future

New capacity, new service
Our aim? • Improving access • Offering assessment closer to home,
within familiar surroundings • Creating extra capacity, and • Rapid assessment and diagnosis
How will it work? • 4 new memory assessment clinics,
based in GP surgeries • In addition to existing clinics at Aylesbury,
Amersham and High Wycombe
• Aim for assessment and diagnosis same day • In addition to existing clinics

CMHT orders scan
6-8 weeks
Patient offered appointment - Most convenient - Quickest
Memory Advisor
3 month follow-up - Same clinic
GP refers to
Memory Assessment Clinic
Referral appendix to information scan decision
Choose & Book
No scan
1 Clinic Appointment
Assessment & Diagnosis
New clinic model

New referral information for Quicker appointment times
• Other information: - Third Party contact details (for arranging appointment etc): - Blood results: FBC, U&E, Glu, LFTs, Calcium, TFT, B12, Folate (QOF 2013 – 14).
- As indicated: Cholesterol, Syphilis, Serology HBA 1C
Patient < 65 Patient 65 – 79 yrs old Patient > 80
Scan all where there is 3rd party history of memory loss (consider MRI)
Scan all unless Do not scan unless
Hx malignancy (tick)
Rapid unexplained deterioration
History over 1 year (tick)
Unexplained focal neurology signs or symptoms
Typical history
[more detail?]
Recent head injury
Early urinary incontinence or gait disturbance
• Not everyone needs a scan

Suggested timetable Consultant Consultant
recording
Nurse Nurse recording
30
min
s
0850 with family / carer
Background history from family
(+ CADI?)
Rio : Presenting situation
Drug history*
Brief personal history
Alcohol / smoking
Physical history
Mental state examination
Cognitive test: ideally MOCA
RIO: Mental State Exam
Cognitive test score
BP & pulse
Weight if scales
GDI?
10
min
s 0920 Consultant & nurse
Discuss and agree diagnosis / management plan.
Consultant may use time to briefly assess pt if they need to confirm MSE or do brief focussed physical
20
min
s
0930 Consultant with patient and
family / carer
Inform of diagnosis
Discuss medication if applicable
Discuss LPA / AD
Research**
Rio ‘ MCA and information
sharing’
Refer dementia advisor:
Buckingham - ‘in house’
Others - Age Concern- this can be
done by a telephone call at end
of clinic (01296 438415) – even if
only to confirm no referrals. NB
closed PM
Progress note (= ‘1st assessment.
See core’)
Open up care plan***
Risk assessment
Diagnosis / Clustering
Activity
Misc GP letter Take papers for uploading by
admin
Follow up telephone call

Memory Advice Service
• Talk through the implications of being given a diagnosis of
dementia
• Help plan for the future
• Help find out about relevant benefits and other financial matters
• Provide information about services/clubs/support groups that are available and how to access them
• Be available if the situation changes

Evaluation
Decrease the time from GP referral to diagnosis
Increase referrals from GP practices to MAS
Increased knowledge and awareness within practice team
Positive patient experience
Increase in dementia diagnosis rate
Measures
Count of weeks from GP referral to diagnosis
Aims
Referrals by month by practice
GP questionnaire at 6 and 12mths
Patient questionnaire, including added benefit of location
Dementia Register by practice

Thanks to
• Louise Jarvis
• Alison Banks
• Christine Nash

Jacqueline Hussey
Consultant in Old Age Psychiatry

Younger People with dementia, Wokingham

Demographics
• Newens 1993 34.6 per 100,000 45-65 yr old • Harvey 1998 78.2 per 100,000 30-64 yr old male 56.4 per 100,000 30-64 yr female

The problems with YPWD (Patient point of view)
Delays to diagnosis
Delays as people move between
services
Difficult to access / provide age-
appropriate support
Some people never diagnosed / no
support

The problems with YPWD (Service point of view)
Delays in getting to the service
(disenchanted carers)
Small numbers – staff felt un-skilled
Service geared towards older people

The Wokingham service
0
5
10
15
20
25
2005 2006 2007 2008 2009 2010 2011 2012
Chart to show number of confirmed cases of YPWD referrals

Rule 1 – befriend your local neurologist
Services for Younger People With Alzheimers Disease and Other dementias.
Faculty of Old age Psychiatry and Alzheimers Society (2005)
“ joint working between Neurology and
Old Age Psychiatry alone could
significantly improve the person with
dementia’s experience of diagnostic
and follow-on services.”

Rule 2 – engage with carers
YPWD FORUM
Across west of Berkshire
Representation from Local authority,
Berkshire Healthcare Trust, a few
voluntary groups
2005 – carers started to attend

Carers Survey
Carers identified need for:
Specialist age-appropriate day
care
Carer support workers
Education

2008 – YPWD education course
Planned to provide mixture of
education, support & social
interaction
Monthly
Evenings
For carers
For patients

Education Course
12- 40 people attended in first year
Range of topics: memory & communication
new behaviours
routes through services
activities
carers’/patients’ perspective
3 socials: summer BBQ, skittles, Xmas meal
Exit strategy
Feedback to modify course

Reflections
Advantages of monitoring
people in non-clinical setting
(sequencing, communication
skills)
Carers found us accessible
Staff confidence & skills
increased
“All in it together”
A catalyst !

Expected numbers of YPWD in
Wokingham
Population 30-64 years
80,150
Expected number YPWD 54
Actual number on case register
53

Diagnoses
0
10
20
30
40
50
60
AD VaD FTD Alc DLBOtherMCI
Harvey
Wokingham

The Wokingham service - 2013
Fortnightly YPWD Memory Clinic
YPWD education course for carers & patients
Designated MHP (part time) OT
Designated Band 3 CSW (0.8 FTE, 0.2 Charity money)

Social care / 3rd sector
Dementia Care Adviser YPWD
3 days day services
Al’s Place

Working alongside a new charity

Charity staffing
6 trustees
2 respite project workers –
1:1 support
workshops
Admiral Nurse (3 days per week)
All employees have honorary contracts with
BHFT

Workshops
• Funded through carers’ grant money
• Meaningful activity
• Exit strategy
• Evidence-based but also patient-led
• Seamless service
• Delays to 24 hour care and admissions


Workshops with RedCape Theatre /
Turtle Key Arts



Orienteering Group


Harmony Choir

Benefits
Seamless service
High patient and carer satisfaction
Joint training for BHFT and charity staff
Joint supervision
Joint care planning

Dementia Friendly Wards
Dr Hannah King
February 2014

February 2014 113
Where it began

February 2014 114

February 2014 115
Empowerment Group
• Corridors are scary and confusing
• Hard for visitors to find a nurse
• Noisy flooring
• Don’t want to just sit staring at the wall.
• Want art work you can lose yourself in.
• Everyone laughing and joking round the nurses station, when you’d like someone to talk to you – makes you feel ignored.

February 2014 116

February 2014 117

February 2014 118

Nurses Station
February 2014 119

February 2014 120

Day Room
February 2014 121

Difficulties
• Reducing the size of nurses station unpopular
• Taking down notice boards
• Taking doors of dayrooms – where to take breaks and have case conferences
February 2014 122

Changing Attitudes
• More Communal Activities
– Staff satisfaction
• Interaction with patients
– One to one care crew
• Wider community
– Links with empowerment group
– Contributors
– Beauty students
February 2014

February 2014 124
Summary •Don‘t need huge amounts of money •De-clutter •More communal spaces

Rowan Ward
• Designing a dementia friendly environment

Rowan Ward
• Context- due to move to a 20 bedded ward by Jan 2014.
• Merging a Reading and a Maidenhead ward.
• A blank canvas
• Opportunity to change environment & practice
• King's Fund dementia design training.


PM's Dementia Challenge
• £50 million available for those to change environment to care for people with dementia.
• First bid submitted by Feb 2013
• I had never written a bid.....
• My dad always used to say- "you don't ask, you don't get".
• So bid was submitted and successful through both sections.
• 42 NHS bids were successful.

Design- focus on:
• Patient friendly
• Lighting
• Colour
• Signage
• Flooring
• Senses
• Family & carer

Before After
Reception area

Before After
Corridors

Before After
Dining Room

Before After
Cinema

Male & Female
sitting areas

Before After

HealWell bedrooms

New Garden Areas


Before
After
After
Family
Room

Before
After
Activity Room

Garden Room

Patient & carer reactions • Patients walked around smiling and
thanking staff.
• The cinema is in regular daily use by patients
• Families have thanked us for having dedicated areas for them to see their relative in.
• People are eating better in the dining room.
• Families are using the dining area in the garden room- so visits remain undisturbed.

Achievements
• First cinema in a hospital in Europe
• LED coloured lighting system- first in Europe to use this
• Described by The King's Fund as 'one of the best wards in Europe ' that they have seen.

"What next ?”

Deborah Humphrey
Head of Nursing, Older Adult Mental Health

Enhancing Care Home Support
ECHO
Deborah Humphrey
Brian Murray
25th February 2014

Background
• Prime ministers Dementia Challenge Fund • This county faces a major demographic challenge with
the number of people aged 85+ set to double over the next 15 years - a rise in prevalence of Dementia by 31%1,2.
• The current prevalence is 7,086, highest in our rural areas with West Oxfordshire being highest.
• Number of people in care homes with dementia • Challenging Behaviour most likely to be difficult for
staff & other residents, families • Challenging behaviour can result in prescribing of
antipsychotic medication or admission to hospital

Issues
• The majority of people in Oxfordshire’s care homes have dementia.
• Many have co-existing physical or mental health needs.
• Recognition of this full range of complex needs can be difficult for the largely untrained workforce3 in care homes
• Struggle to bring together the physical and the mental aspects of care.

Issues
• Three teams (Care Home Support Service (Falls prevention in-reach), PCT Pharmacy Liaison, and Community Mental Health Teams) provide in-reach services to care homes.
• All operate separately and involve several referral points.
• They also have different training which is not linked.
Consequently there are gaps and inconsistency in quality of the services.

AIMS
• Better dementia awareness amongst paid staff/professionals.
• Develop a competent and sustainable workforce across sectors so that people with dementia can have person-centred and dignified care wherever they are being cared for, including care homes.
• Effective treatment and support that enables people with dementia remain as well as possible in care home without the need for emergency hospital admissions.

What to do
• Development of new roles to provide enhanced mental health expertise within the existing Care Home Support Service team
• Training in the “Newcastle Model” of dementia in the care home support service
• improve homes’ capacity to care for people with dementia closer to their local communities.

Where we are now
• Project group finishes March 2014.
• Recruitment to ECHO MH workers partially completed (final interviews March).
• Training in the model – March 2014
• Protocols completed 2014
• Start date April/May 2014
• Evaluation in 6 & 12 months

Care Home In-Reach Team
Hazelwood
Honey End Lane
Tilehurst
Reading
RG30 4EJ
Tel: 01189 605959
Hours of service:
9am-5pm Monday to Friday
(not including bank or public holidays).
Care Home In-Reach Team

The Team
Carole Jones– Service Manager Jenny Hall -Team Lead
Wokingham, Newbury and Reading
Physical and Mental Health Practitioners. Anne-Marie Adams, Gurudutt Baboolal, Wendy Hunter, Lizzie Harrison
Caroline Bridger and Ralph Chananda
Medical Team Community Geriatricians Consultant Psychiatrists
Care Home In-Reach Team

Vision and Aim
To support the Care Home Staff and raise their knowledge, skills and
confidence.
‘Elderly people with dementia living in care homes should have the same access as everyone else to high standards of service.’
• Prime Ministers challenge on dementia-Objective 11: Living well
with dementia in care homes.
Care Home In-Reach Team

Aims • Assist to deliver care for an improved quality of life for people with dementia living in residential and nursing homes.
• Improve the skills of the care home staff, building their confidence and professionalism.
• Improve communication with people with dementia, and involvement of carers. Including planning for End of Life care.
Care Home In-Reach Team

Service Outcomes….
• Review of the mental and physical health of people with dementia.
• End of Life Care.
• Reduction in number of admissions to hospital.
• Antipsychotic medication reviews.
• Improved quality of life for residents.
Care Home In-Reach Team

Our Criteria:
1. Care homes within the four West of Berkshire CCGs who agree to work with the team
2. Residents in these care homes with a diagnosis of dementia. 3. Residents in these care home where dementia is suspected but not
formally diagnosed
Exclusions:
1. Residents without a diagnosis of dementia, however if dementia is suspected the team will assess and advise accordingly.
2. No individual patient referrals will be accepted
Care Home In-Reach Team

Story so far…. • The team has worked with approximately 12 care homes in the last 7 months each of
which is at a different stage of involvement.
• Actively working with care home managers and staff to address concerns or areas as identified by their CQC report/Business plans.
• Joint working with the discharge team at RBH collating admission data from care homes to the RBH and where appropriate conducting case reviews to check on whether admission was appropriate.
• Met with Commissioning support, Social Services and other Old Age care services looking at ways of working alongside them.
• Forged links with the Berkshire Care Home association to facilitate better relationships and working practices between the care homes and Statutory services (NHS).
Care Home In-Reach Team

Within the homes
• Issues identified vary in individual homes but there we have identified some common themes. • Organisational/management issues.
• Staff Training and Education (including confidence and professionalism).
• Care Home links and relationship with GP practice and Statutory services (NHS and Social services).
• Formal in informal teaching, supervision/modelling with regards to: • Mental Capacity Act
• DOLS
• End Of life Care
• Dementia awareness.
• Challenging behaviours.
• Quality of life and occupation/activity
Care Home In-Reach Team

Challenges…… • Care homes are Private businesses and as a result its not
just with the manager we are attempting to engage but with an organisation.
• As a new service there appears to be some apprehension or reluctance to engage with us.
• It takes time to develop trusting relationships with managers and staff. Effectiveness is very dependent on these relationships. Therefore proving our effectiveness in the short term is difficult.
• Relationships between management and staff has been identified as potential barrier to initiating change
Care Home In-Reach Team

Any Questions???
Care Home In-Reach Team