TESTS OF LIVER FUNCTION
1
302 Annotations CHICKEN-POX AND HERPES ZOSTER MosT clinicians who work in children’s wards are con- vinced that varicella and zoster are astiologically related. The usual sequence is the occurrence of typical chicken- pox among contacts of a case of zoster but examples are on record of zoster following exposure to chicken-pox. There are, moreover, borderland cases in which a chicken-pox eruption accompanied by consti- tutional disturbance is superimposed on an attack of zoster, Parounagian and Goodman collected records of 29 cases in which these two conditions occurred together and Ferriman found 69 further records in the literature. Laboratory workers have produced valuable evidence that the two diseases are caused by closely related if not identical infective agents. Each virus exists in the form of elementary bodies which can be readily demonstrated in the clear fluid of the early vesicles. In chicken-pox these elementary bodies can also be found in the lesions on the buccal mucosa and even in the expired air. Puri- fied suspensions of varicella and zoster bodies are agglu- tinated by the corresponding convalescent sera and cross- agglutination also takes place, though to a lower titre. Attempts to transmit either disease to laboratory animals have failed except in the hands of certain Japanese workers. Kin 3 claims to have adapted the virus of zoster to proliferation in the rabbit testis, and he says that when infective material from this source is inocu- lated intracutaneously into man it produces a localised vesicular eruption accompanied by mild constitutional symptoms. In convalescents from varicella or zoster there was no response to inoculation, indicating that both diseases give rise to immunity against this modified zoster virus. The difference between the two agents can best be explained in terms of invasiveness and elective localisa- tion in different tissues. In the case of a typical attack of zoster or a mild varicella originating from such the virus proliferates but slightly and the immune response of the host is correspondingly poor on account of the small amount of antigen available for the stimulation of antibody. A normal attack of varicella, on the other hand, provides an adequate amount of antigen for a full immune response and the host is then equipped to deal effectivelv with a subsequent reinfection. This seems a reasonable explanation of the two cases of a second attack of chicken-pox described in Dr. Crisp’s letter which appears elsewhere in this issue. Some of our readers could probably give instances of chicken-pox originating from zoster which resulted in solid immunity to reinfection from another case of varicella. The placing on record of such instances would serve a useful pnrpose. TESTS OF LIVER FUNCTION NO-ONE disputes the great value of tests of kidney function, but few clinicians would say as much of tests which set out to gauge the efficiency of the liver. There are many reasons for this lack of enthusiasm. The liver admittedly is a vexatious organ in that it has numerous functions, many of which may be normally maintained even if the anatomical changes are profound and other functions are completely disorganised. At the same time the clinicians are partly to blame for a lack of sym- pathy with these little foibles of the liver, and for a general failure to grasp the real significance of func- tion tests and the manner in which they should be employed. Within the last year two new tests have been suggested which may turn out to be of more value than many of their predecessors. Both measure general hepatic damage but neither depend on the excretory function of 1. Parounagian, M.B., and Goodman, H. Arch. Derm. Syph., N.Y. 1923, 7, 439. 2. Ferriman, D. G. Lancet, 1939, 1, 930. 3. Kin, O. Jap. J. Derm. Urol. 1939, 46, 133. the liver. Consequently both may be used to differentiate jaundice due to hepatitis and liver injury from jaundice due to extrahepatic mechanical obstruction in, say, the larger bile-passages. The value of such differentiation will be obvious to any practising physician. The first test, described by McArdle, depends on the estimation of the choline esterase in the plasma or serum. This test, while admittedly still rather empirical, is easy to carry out once the technique has been a.cquired; it also puts the patient to the minimum of inconvenience and can be repeated as often as may be required. The second 2 is based on the estimation of the combined cholesterol in the blood-that is, the amount of the sterol present in ester form. It has the same theoretical limitations and practical advantages as the first and it remains to be seen which is the more generally useful. One or other, if not both, look like having a successful future. HORMONE ASSAY AND THE ENDOMETRIUM THERE are to our hand certain lines of investigation which promise to throw light on the functions of the genital tract. Some of these are new and relatively untried; others, by their very survival, have gained a reputation for reliability that may after all be unmerited. Amongst the former may be placed the assay of gonado- tropic substance, aestrin and pregnandiol excreted in the urine as an index of the activity of pituitary and ovary; and among the latter the estimation of the basal meta- bolic rate and the histological examination of the endo- metrium. Randall and ’Wilson have lately investigated the scope as well as the limitations of these laboratory aids to the diagnosis of the functional disorders of the endometrium. The uterus goes through a constantly changing cycle, and a chance reading at the wrong moment of that cycle may provide negative and even misleading results. It is therefore essential to appreciate the physiological before trying to interpret the pathological. If a number of normal women are submitted to serial hormone assays it is possible to plot a rough graph, from which certain facts emerge.’ It is assumed that these women have a 28-day cycle, counting from the first day of bleeding, which should average 5 days; the date of ovulation being computed to occur about the 14th to the 16th day is shown in the figure, modified from Randall and Wilson’s paper. The significance of these curves needs stressing; the assay of the several hormones should be serial and correlated with the menstrual cycle. For example, a reading of nil for gonadotropic hormone on the 20th day does not mean that the pituitary is not acting normally. To pursue the argument to its logical conclusion a normal reading of these hormonal excretion figures should postulate a synchronous normality in the endometrial biopsy and vice versa. For example, an excretion figure for pregnandiol of 5 mg. on the 24th day should mean that a biopsy of the endometrium at that time will show well-marked secretory changes, and again vice versa. Whether this fascinating and simple hypothesis will hold water remains to be fully tested and it is hoped that workers in this country will report on this, the real test of the theory. So much for the physiological; the pathological is not unfortunately so simple. Randall and Wilson investigated fifteen cases of amenorrhoea in women aged between 23 and 35 years who had not bled for periods varying from two months to ten years. In twelve of these the endometrium was atrophic or cestrogenic only in type and the pregnandiol excretion was nil. In the other three that showed some secretory changes in the 1. McArdle, B. Quart. J. Med. 1940, 9, 107. 2. Greene, C. H., Hotz, R. and Leahy, E. Arch. intern. Med. June, 1940, p. 1130. 3. Randall, L. M. and Wilson, R. B. Proc. Mayo Clin. June 26, 1940, p. 401.
Transcript of TESTS OF LIVER FUNCTION

302
Annotations
CHICKEN-POX AND HERPES ZOSTER
MosT clinicians who work in children’s wards are con-vinced that varicella and zoster are astiologically related.The usual sequence is the occurrence of typical chicken-pox among contacts of a case of zoster but examplesare on record of zoster following exposure to
chicken-pox. There are, moreover, borderland cases inwhich a chicken-pox eruption accompanied by consti-tutional disturbance is superimposed on an attack ofzoster, Parounagian and Goodman collected records of29 cases in which these two conditions occurred togetherand Ferriman found 69 further records in the literature.Laboratory workers have produced valuable evidence thatthe two diseases are caused by closely related if notidentical infective agents. Each virus exists in the formof elementary bodies which can be readily demonstratedin the clear fluid of the early vesicles. In chicken-poxthese elementary bodies can also be found in the lesionson the buccal mucosa and even in the expired air. Puri-fied suspensions of varicella and zoster bodies are agglu-tinated by the corresponding convalescent sera and cross-agglutination also takes place, though to a lower titre.Attempts to transmit either disease to laboratory animalshave failed except in the hands of certain Japaneseworkers. Kin 3 claims to have adapted the virus ofzoster to proliferation in the rabbit testis, and he saysthat when infective material from this source is inocu-lated intracutaneously into man it produces a localisedvesicular eruption accompanied by mild constitutionalsymptoms. In convalescents from varicella or zosterthere was no response to inoculation, indicating that bothdiseases give rise to immunity against this modifiedzoster virus.
The difference between the two agents can best beexplained in terms of invasiveness and elective localisa-tion in different tissues. In the case of a typical attackof zoster or a mild varicella originating from such thevirus proliferates but slightly and the immune responseof the host is correspondingly poor on account of thesmall amount of antigen available for the stimulation ofantibody. A normal attack of varicella, on the otherhand, provides an adequate amount of antigen for a fullimmune response and the host is then equipped to dealeffectivelv with a subsequent reinfection. This seems areasonable explanation of the two cases of a secondattack of chicken-pox described in Dr. Crisp’s letter whichappears elsewhere in this issue. Some of our readerscould probably give instances of chicken-pox originatingfrom zoster which resulted in solid immunity toreinfection from another case of varicella. The placingon record of such instances would serve a useful pnrpose.
TESTS OF LIVER FUNCTION
NO-ONE disputes the great value of tests of kidneyfunction, but few clinicians would say as much of testswhich set out to gauge the efficiency of the liver. Thereare many reasons for this lack of enthusiasm. The liveradmittedly is a vexatious organ in that it has numerousfunctions, many of which may be normally maintainedeven if the anatomical changes are profound and otherfunctions are completely disorganised. At the same timethe clinicians are partly to blame for a lack of sym-pathy with these little foibles of the liver, and for ageneral failure to grasp the real significance of func-tion tests and the manner in which they should beemployed. Within the last year two new tests have beensuggested which may turn out to be of more value thanmany of their predecessors. Both measure general hepaticdamage but neither depend on the excretory function of1. Parounagian, M.B., and Goodman, H. Arch. Derm. Syph., N.Y.
1923, 7, 439.2. Ferriman, D. G. Lancet, 1939, 1, 930.3. Kin, O. Jap. J. Derm. Urol. 1939, 46, 133.
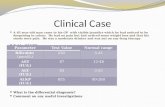
the liver. Consequently both may be used to differentiatejaundice due to hepatitis and liver injury from jaundicedue to extrahepatic mechanical obstruction in, say, thelarger bile-passages. The value of such differentiationwill be obvious to any practising physician. The firsttest, described by McArdle, depends on the estimationof the choline esterase in the plasma or serum. Thistest, while admittedly still rather empirical, is easy to
carry out once the technique has been a.cquired; it alsoputs the patient to the minimum of inconvenience andcan be repeated as often as may be required. The second 2
is based on the estimation of the combined cholesterol inthe blood-that is, the amount of the sterol present inester form. It has the same theoretical limitations andpractical advantages as the first and it remains to beseen which is the more generally useful. One or other, ifnot both, look like having a successful future.
HORMONE ASSAY AND THE ENDOMETRIUM
THERE are to our hand certain lines of investigationwhich promise to throw light on the functions of thegenital tract. Some of these are new and relativelyuntried; others, by their very survival, have gained areputation for reliability that may after all be unmerited.Amongst the former may be placed the assay of gonado-tropic substance, aestrin and pregnandiol excreted in theurine as an index of the activity of pituitary and ovary;and among the latter the estimation of the basal meta-bolic rate and the histological examination of the endo-metrium. Randall and ’Wilson have lately investigatedthe scope as well as the limitations of these laboratoryaids to the diagnosis of the functional disorders of theendometrium.The uterus goes through a constantly changing cycle,
and a chance reading at the wrong moment of that cyclemay provide negative and even misleading results. It istherefore essential to appreciate the physiological beforetrying to interpret the pathological. If a number ofnormal women are submitted to serial hormone assaysit is possible to plot a rough graph, from which certainfacts emerge.’ It is assumed that these women have a28-day cycle, counting from the first day of bleeding,which should average 5 days; the date of ovulationbeing computed to occur about the 14th to the 16thday is shown in the figure, modified from Randall andWilson’s paper. The significance of these curves needsstressing; the assay of the several hormones should beserial and correlated with the menstrual cycle. Forexample, a reading of nil for gonadotropic hormone onthe 20th day does not mean that the pituitary is not
acting normally.To pursue the argument to its logical conclusion a
normal reading of these hormonal excretion figures shouldpostulate a synchronous normality in the endometrialbiopsy and vice versa. For example, an excretion figurefor pregnandiol of 5 mg. on the 24th day should meanthat a biopsy of the endometrium at that time will showwell-marked secretory changes, and again vice versa.
Whether this fascinating and simple hypothesis will holdwater remains to be fully tested and it is hoped thatworkers in this country will report on this, the real testof the theory.
So much for the physiological; the pathological isnot unfortunately so simple. Randall and Wilsoninvestigated fifteen cases of amenorrhoea in women agedbetween 23 and 35 years who had not bled for periodsvarying from two months to ten years. In twelve ofthese the endometrium was atrophic or cestrogenic onlyin type and the pregnandiol excretion was nil. In theother three that showed some secretory changes in the
1. McArdle, B. Quart. J. Med. 1940, 9, 107.2. Greene, C. H., Hotz, R. and Leahy, E. Arch. intern. Med. June,
1940, p. 1130.3. Randall, L. M. and Wilson, R. B. Proc. Mayo Clin. June 26,
1940, p. 401.