Testicular cancers - shared-d7-royalmarsden-public.s3 ... · The Royal Marsden Question 1 1....
54
The Royal Marsden Testicular cancers Mr Erik Mayer Consultant Urological surgeon, The Royal Marsden
Transcript of Testicular cancers - shared-d7-royalmarsden-public.s3 ... · The Royal Marsden Question 1 1....
The Royal Marsden
Testicular cancers
Mr Erik Mayer Consultant Urological surgeon, The Royal Marsden
The Royal Marsden
Contents
− Referral Guidelines
− Diagnostics
− Common misdiagnosis – Differential Diagnosis
– The newly diagnosed cancer patient
– The awkward Scrotum
2
The Royal Marsden
Referral Guidelines
3
The Royal Marsden
Quiz
The Royal Marsden
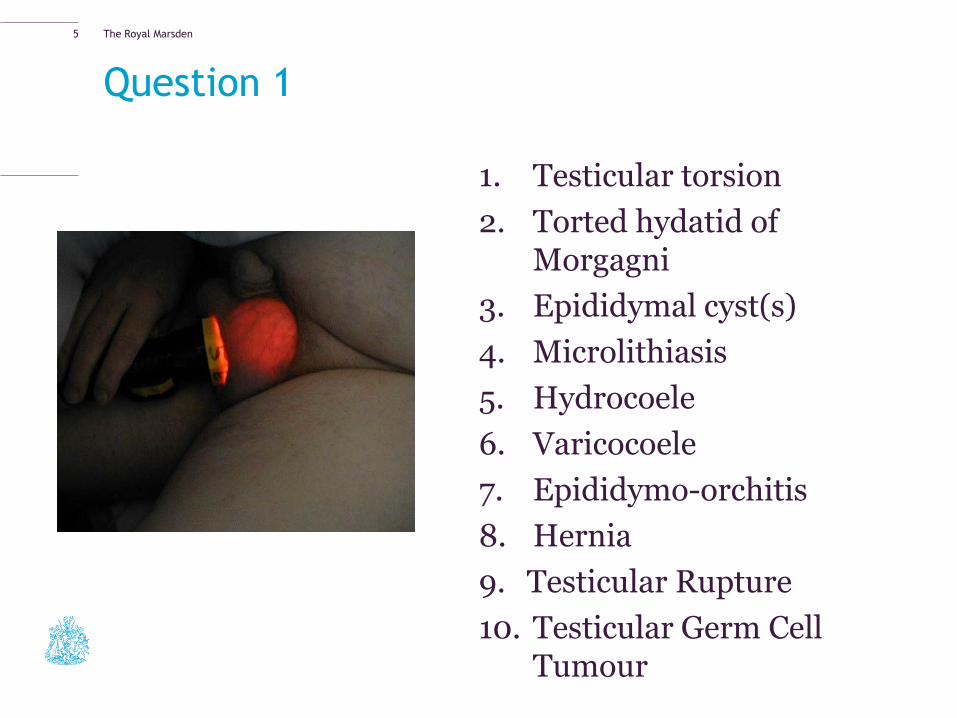
Question 1
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour
5
The Royal Marsden
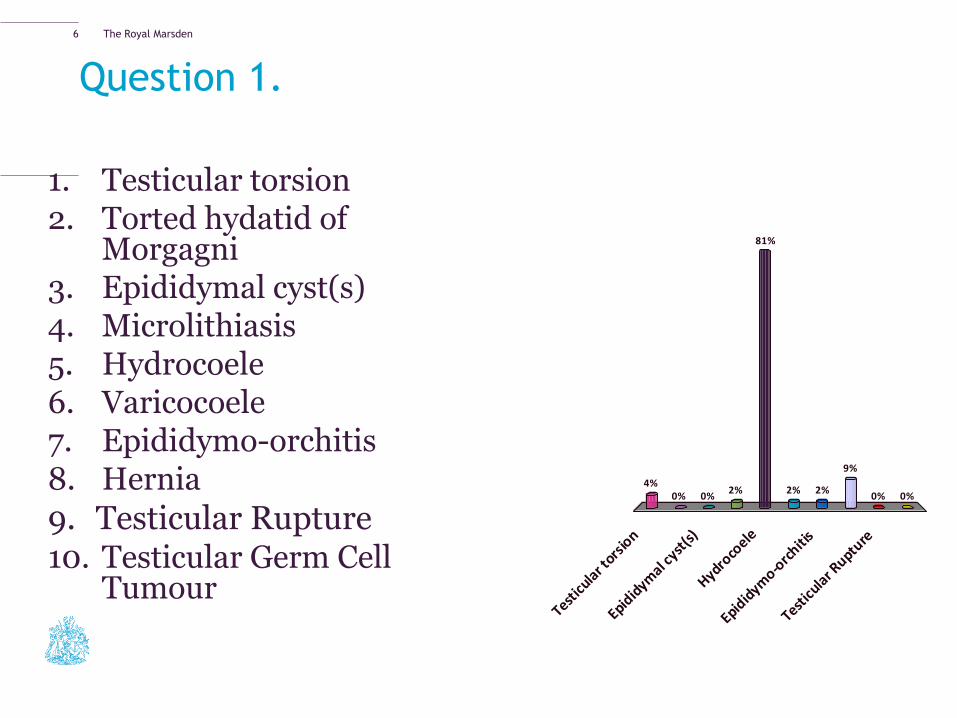
Question 1.
1. Testicular torsion 2. Torted hydatid of
Morgagni 3. Epididymal cyst(s) 4. Microlithiasis 5. Hydrocoele 6. Varicocoele 7. Epididymo-orchitis 8. Hernia
9. Testicular Rupture 10. Testicular Germ Cell
Tumour Test
icula
r tors
ion
Epidid
ymal c
yst(s)
Hydroco
ele
Epidid
ymo-o
rchiti
s
Testicu
lar R
upture
4%0% 0%
2%0%0%
9%
2%2%
81%
6
The Royal Marsden
Question 2
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour
7
The Royal Marsden
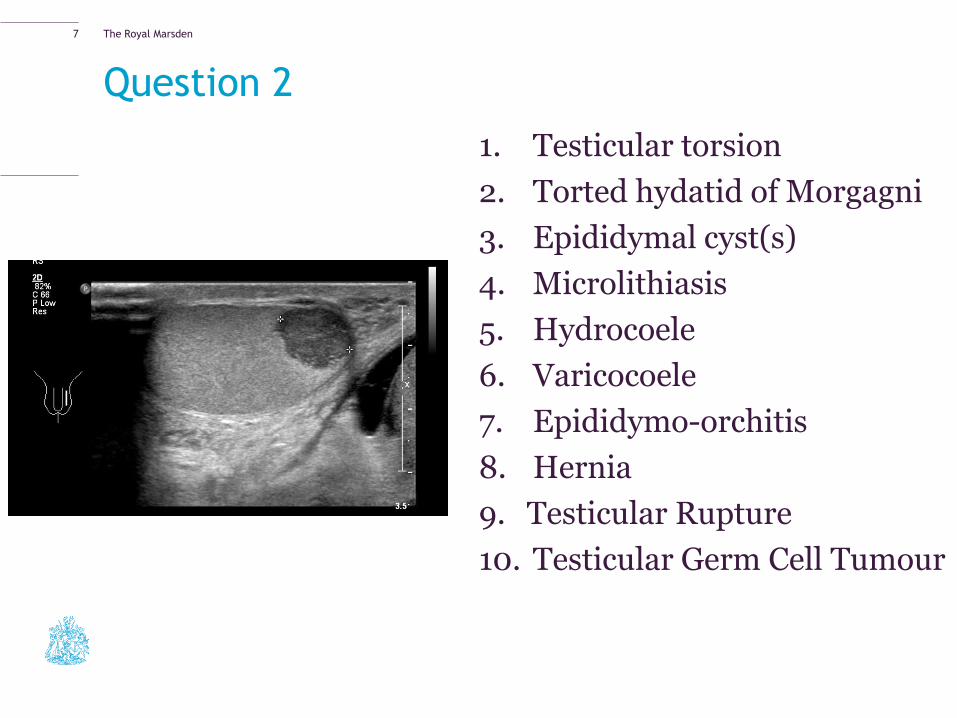
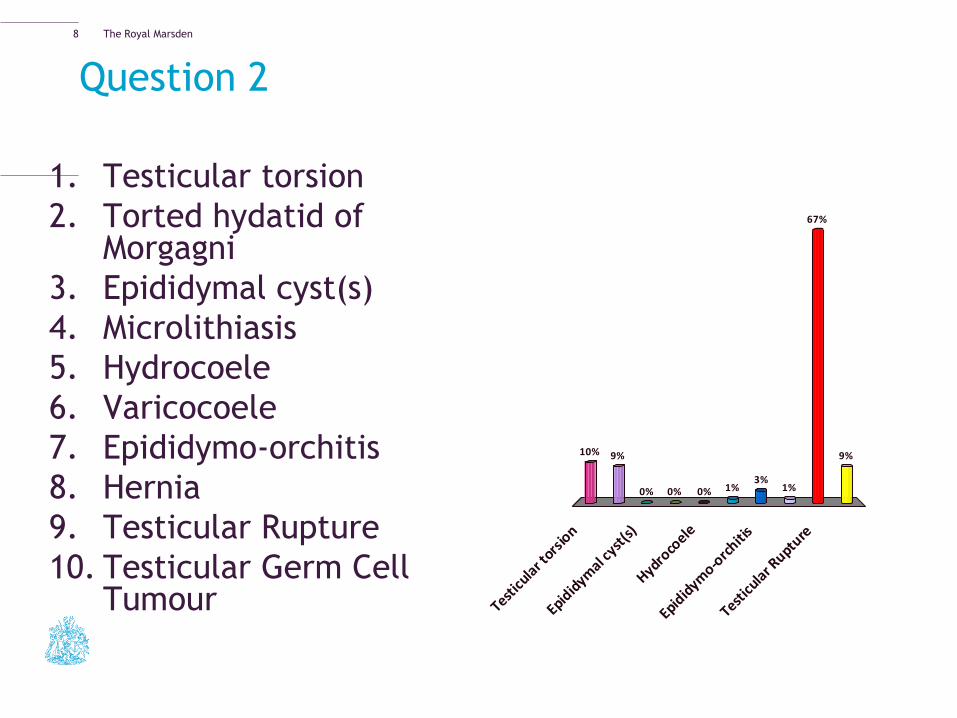
Question 2
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour Test
icula
r tors
ion
Epidid
ymal c
yst(s)
Hydroco
ele
Epidid
ymo-o
rchiti
s
Testicu
lar R
upture
10% 9%
0% 0%
9%
67%
1%3%
1%0%
8
The Royal Marsden
Question 3
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Adenomatoid Tumour
10. Testicular Germ Cell Tumour
9
The Royal Marsden
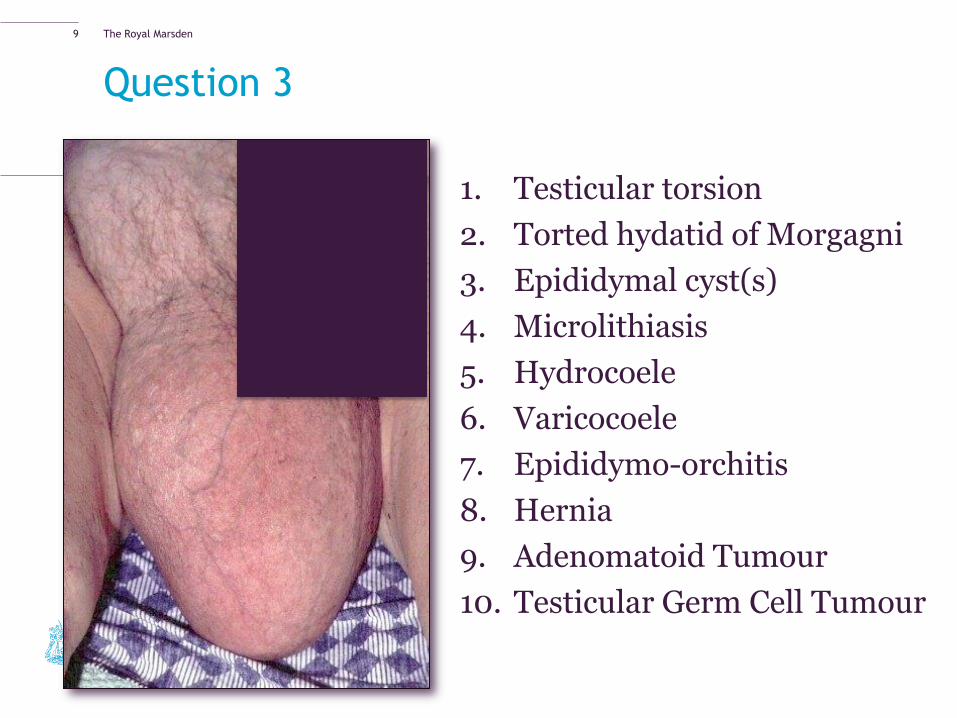
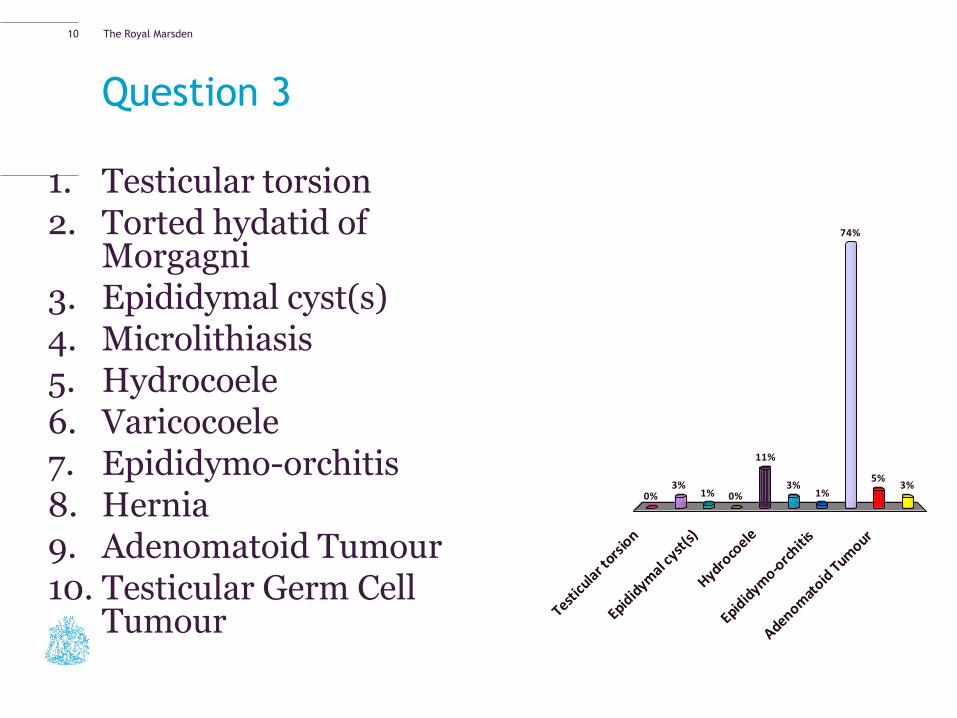
Question 3
1. Testicular torsion 2. Torted hydatid of
Morgagni 3. Epididymal cyst(s) 4. Microlithiasis 5. Hydrocoele 6. Varicocoele 7. Epididymo-orchitis 8. Hernia 9. Adenomatoid Tumour 10. Testicular Germ Cell
Tumour
Testicu
lar t
orsio
n
Epidid
ymal c
yst(s)
Hydroco
ele
Epidid
ymo-o
rchiti
s
Adenomat
oid T
umour
0%3%
1% 0%3%
5%
74%
1%3%
11%
10
The Royal Marsden
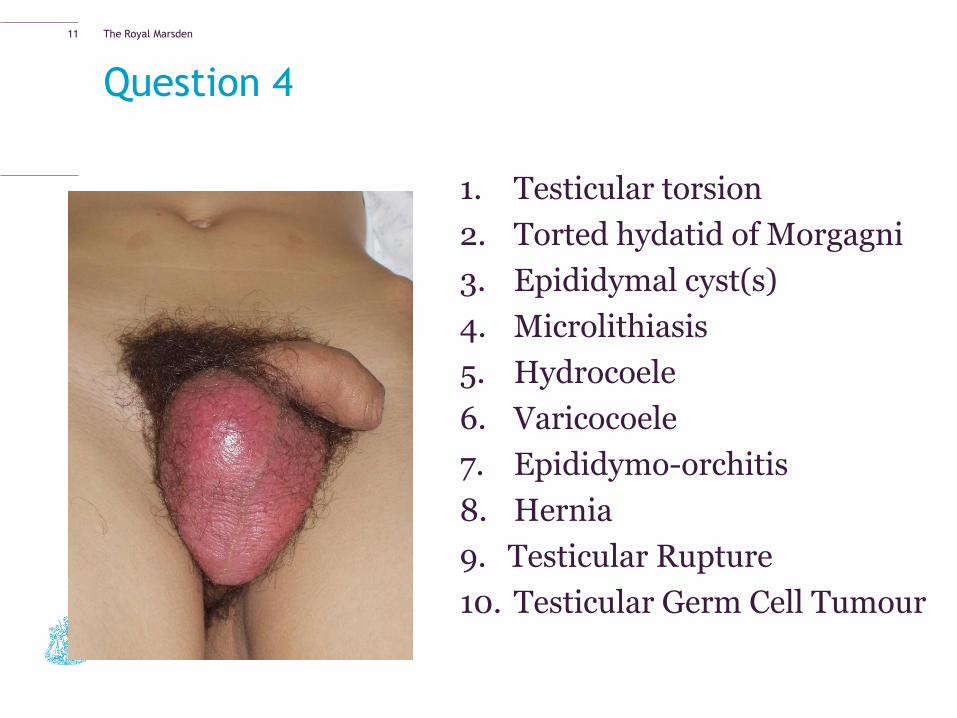
Question 4
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour
11
The Royal Marsden
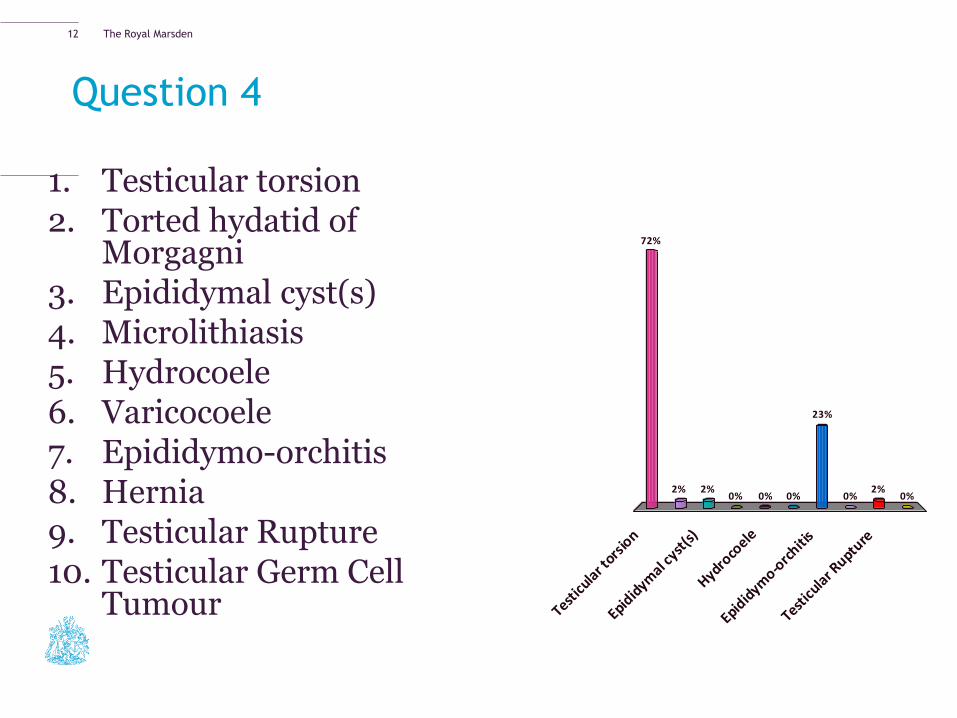
Question 4
1. Testicular torsion 2. Torted hydatid of
Morgagni 3. Epididymal cyst(s) 4. Microlithiasis 5. Hydrocoele 6. Varicocoele 7. Epididymo-orchitis 8. Hernia 9. Testicular Rupture 10. Testicular Germ Cell
Tumour Testicu
lar t
orsio
n
Epidid
ymal c
yst(s)
Hydroco
ele
Epidid
ymo-o
rchiti
s
Testicu
lar R
upture
72%
2% 2%0% 0%
2%0%
23%
0%0%
12
The Royal Marsden
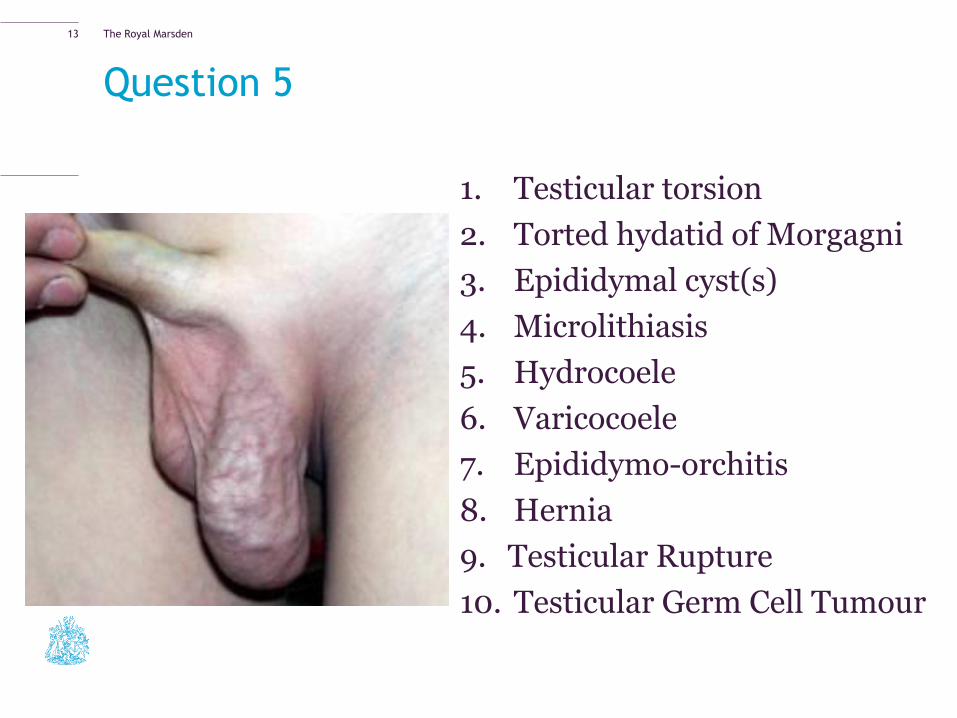
Question 5
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour
13
The Royal Marsden
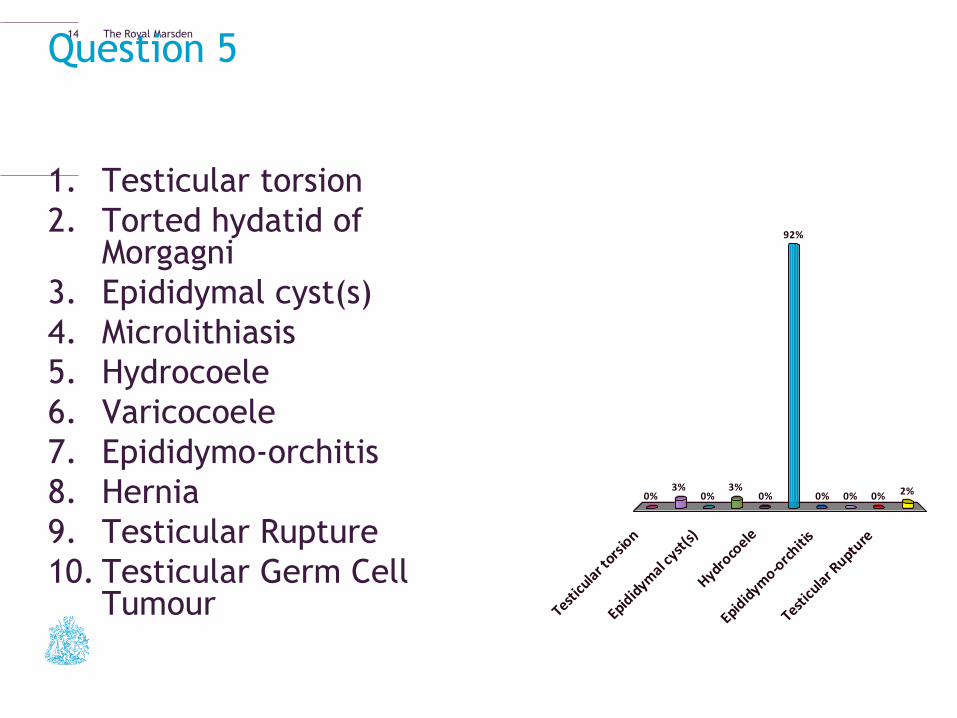
Question 5
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Rupture
10. Testicular Germ Cell Tumour Test
icula
r tors
ion
Epidid
ymal c
yst(s)
Hydroco
ele
Epidid
ymo-o
rchiti
s
Testicu
lar R
upture
0%3%
0%3% 2%0%0%0%
92%
0%
14
The Royal Marsden
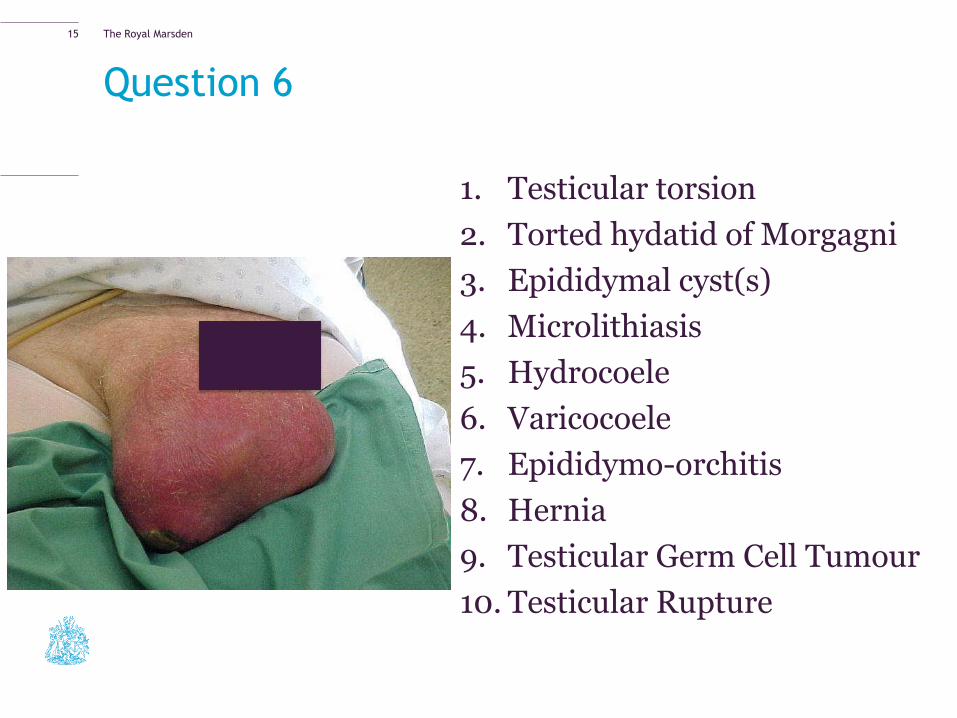
Question 6
1. Testicular torsion
2. Torted hydatid of Morgagni
3. Epididymal cyst(s)
4. Microlithiasis
5. Hydrocoele
6. Varicocoele
7. Epididymo-orchitis
8. Hernia
9. Testicular Germ Cell Tumour
10. Testicular Rupture
15
The Royal Marsden
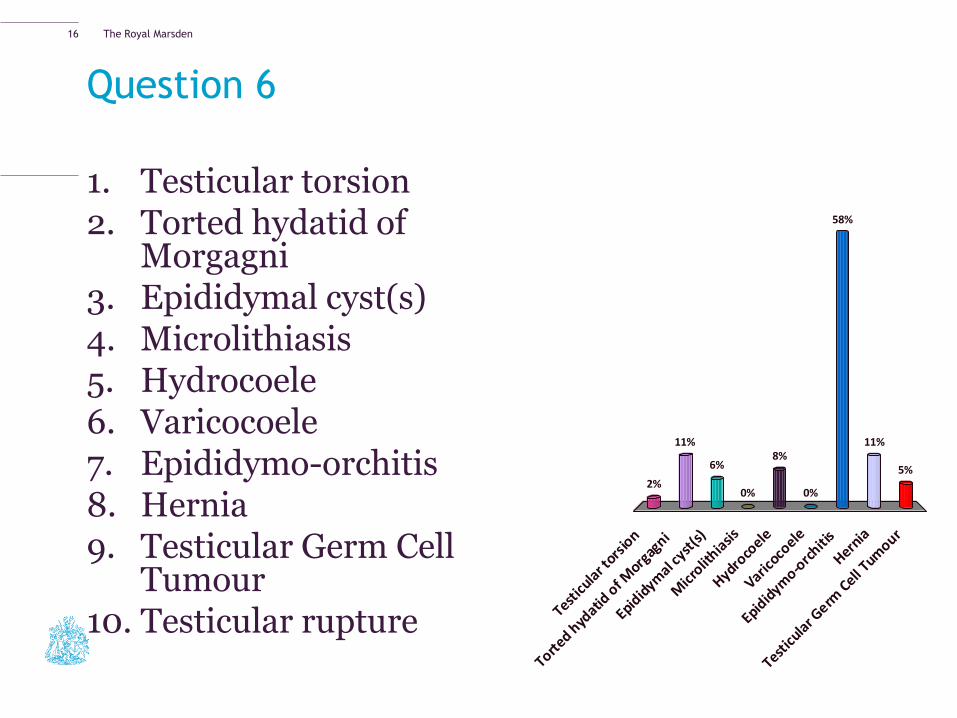
Question 6
1. Testicular torsion 2. Torted hydatid of
Morgagni 3. Epididymal cyst(s) 4. Microlithiasis 5. Hydrocoele 6. Varicocoele 7. Epididymo-orchitis 8. Hernia 9. Testicular Germ Cell
Tumour 10. Testicular rupture Test
icula
r tors
ion
Torted h
ydatid
of M
orgag
ni
Epidid
ymal c
yst(s)
Micr
olithia
sis
Hydroco
ele
Varicoco
ele
Epidid
ymo-o
rchiti
s
Hernia
Testicu
lar G
erm C
ell Tum
our
2%
11%
6%
0%
5%
11%
58%
0%
8%
16
The Royal Marsden
Diagnostics
– History
– Clinical Examination
– Genitals
– Abdomen
– Supraclavicular Lymphadenopathy
– Urine Dipstick & Pregnancy Test
– Tumour Markers
– Ultrasound
17
The Royal Marsden
History
Symptoms
• Hard, painless lump
- Partner detection
• 5-10% scrotal pain
• - Intra-tumoural haemorrhage
- Trauma brings attention to abnormality
• Metastatic
- Weight loss
- Shortness of Breath
- Back/abdominal pain
- Neck lumps
18
The Royal Marsden
Key Points in a Scrotal Mass History
– The Lump
– How was it detected (in the bath etc.)?
– How long has it been there?
– Is it changing in size?
– Painful or painless
– Sexual history – Any recent STIs
– Any lower urinary tract symptoms
– Any recent testicular trauma
19
The Royal Marsden
Key points continued
− Any abdominal or neck lumps (lymphadenopathy)
− Any SOB or abdominal pain
− PMH
− Previous orchidopexy/maldescent of testicle
− Have they had testicular US scan before/been encouraged to regularly self examine
− FH of testicular Cancer
20
The Royal Marsden
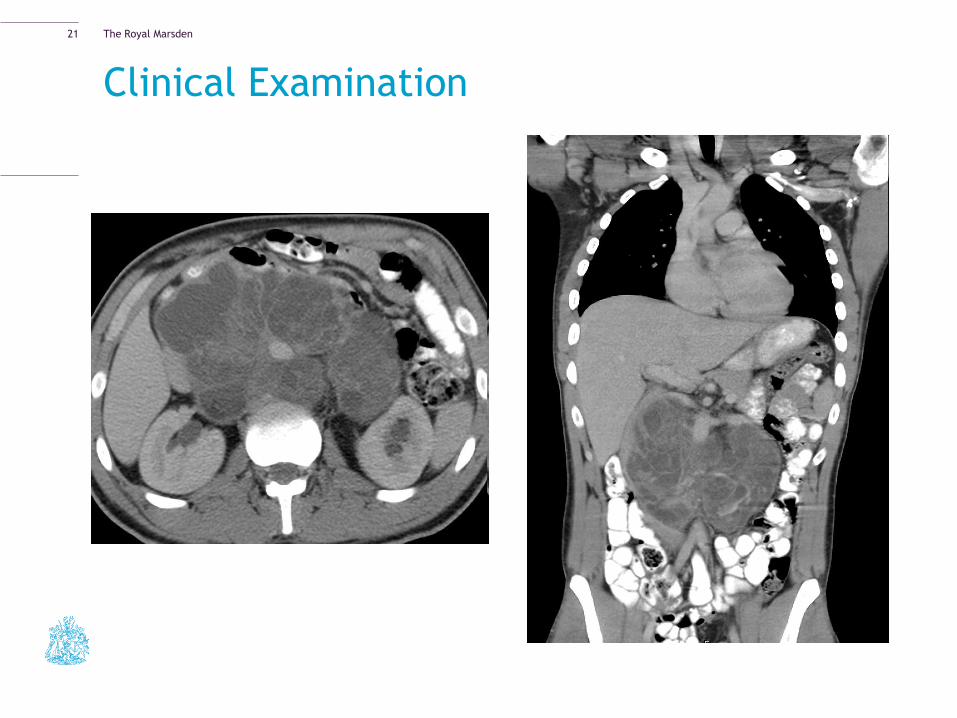
Clinical Examination
21
The Royal Marsden
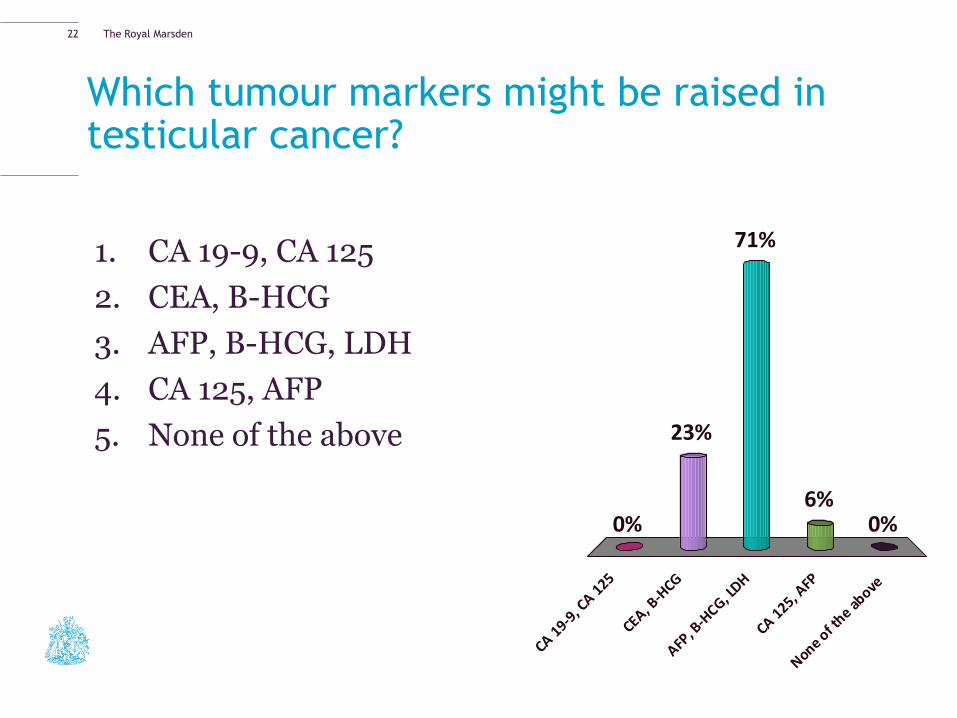
Which tumour markers might be raised in testicular cancer?
1. CA 19-9, CA 125
2. CEA, B-HCG
3. AFP, B-HCG, LDH
4. CA 125, AFP
5. None of the above
CA 19-9
, CA 1
25
CEA, B-H
CG
AFP, B
-HCG, L
DH
CA 125, A
FP
None of t
he above
0%
23%
0%6%
71%
22
The Royal Marsden
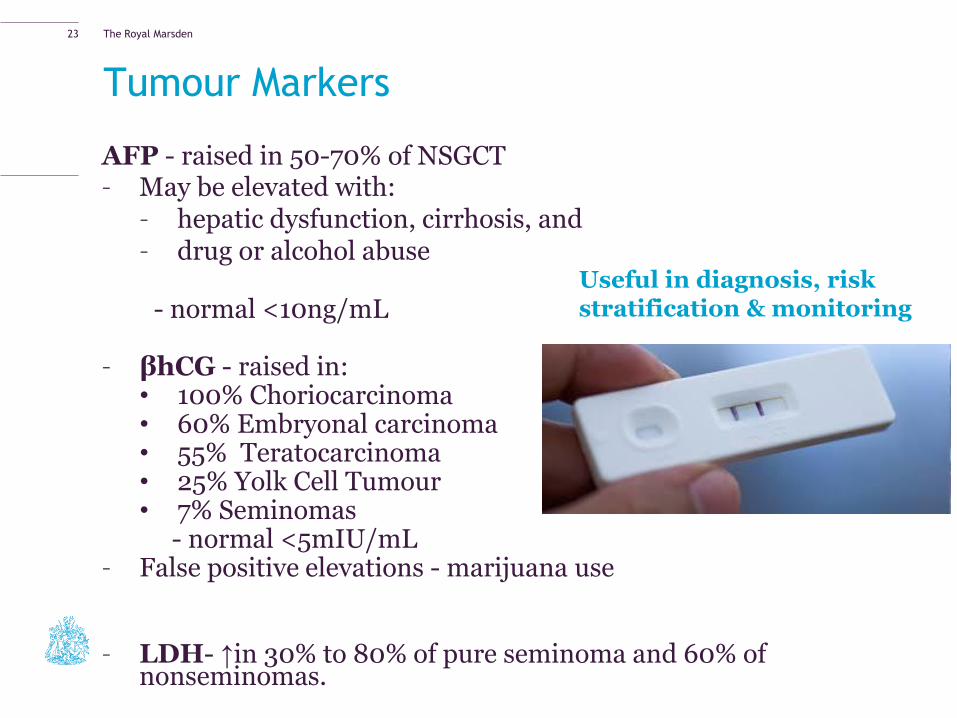
Tumour Markers
AFP - raised in 50-70% of NSGCT – May be elevated with:
– hepatic dysfunction, cirrhosis, and – drug or alcohol abuse
- normal <10ng/mL – βhCG - raised in:
• 100% Choriocarcinoma • 60% Embryonal carcinoma • 55% Teratocarcinoma • 25% Yolk Cell Tumour • 7% Seminomas
- normal <5mIU/mL – False positive elevations - marijuana use – LDH- ↑in 30% to 80% of pure seminoma and 60% of
nonseminomas.
Useful in diagnosis, risk stratification & monitoring
23
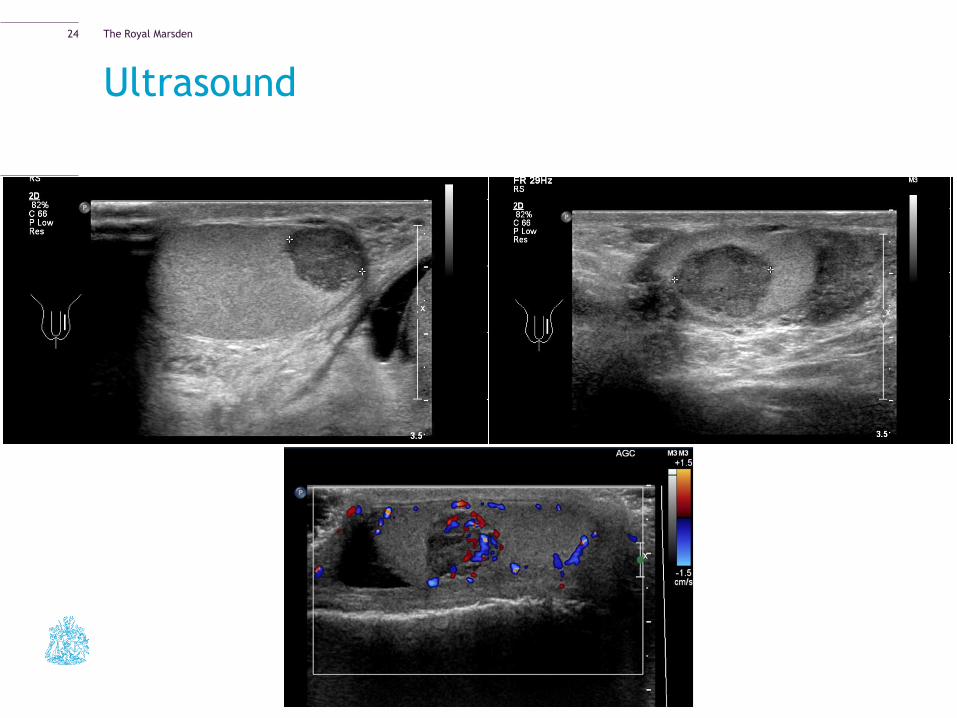
The Royal Marsden
Ultrasound
24
The Royal Marsden
What I discuss with the patient
− Diagnosis
− Prognosis
− CxR/CT scan/tumour markers
− Need for Surgery as first line treatment
− Testicular Prosthesis
− Fertility/Sperm Storage
− Possible further treatment
25
The Royal Marsden
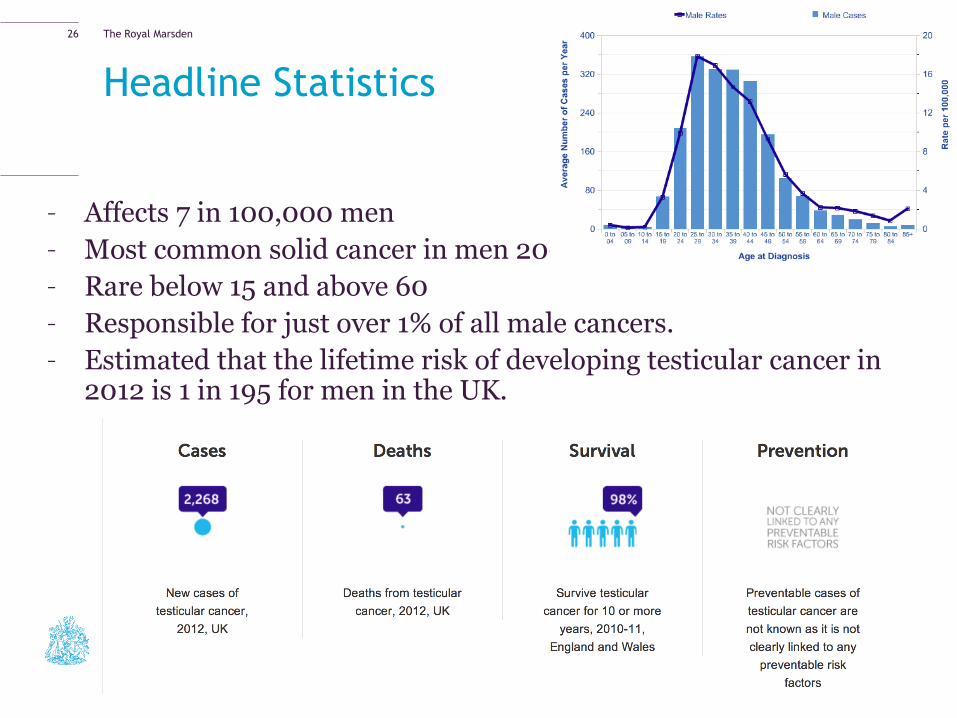
Headline Statistics
– Affects 7 in 100,000 men
– Most common solid cancer in men 20-45
– Rare below 15 and above 60
– Responsible for just over 1% of all male cancers.
– Estimated that the lifetime risk of developing testicular cancer in 2012 is 1 in 195 for men in the UK.
26
The Royal Marsden
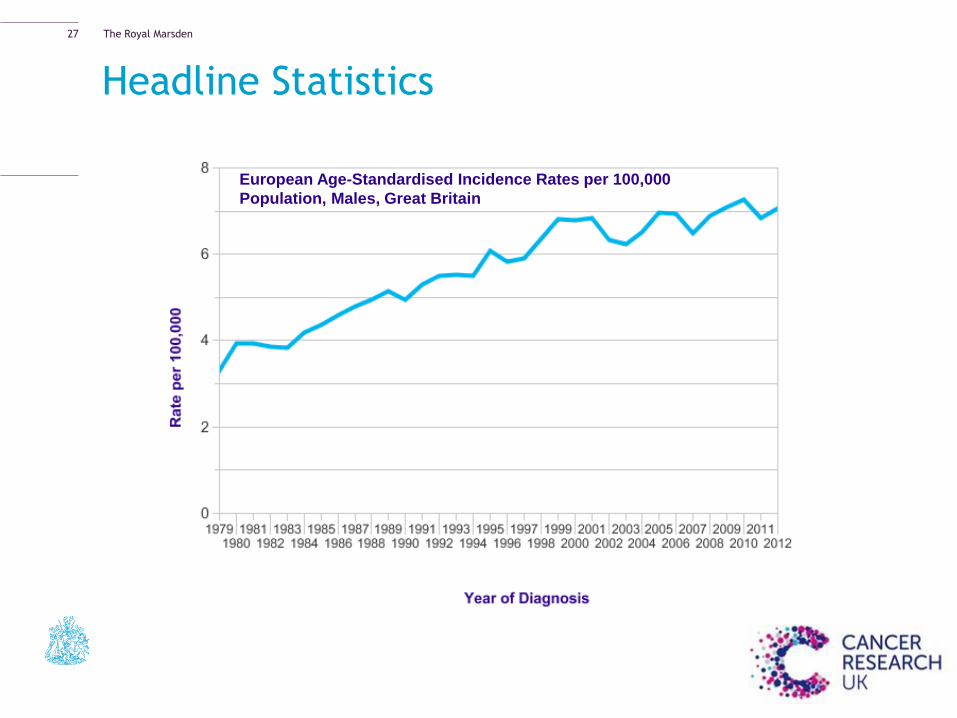
European Age-Standardised Incidence Rates per 100,000
Population, Males, Great Britain
Headline Statistics
27
The Royal Marsden
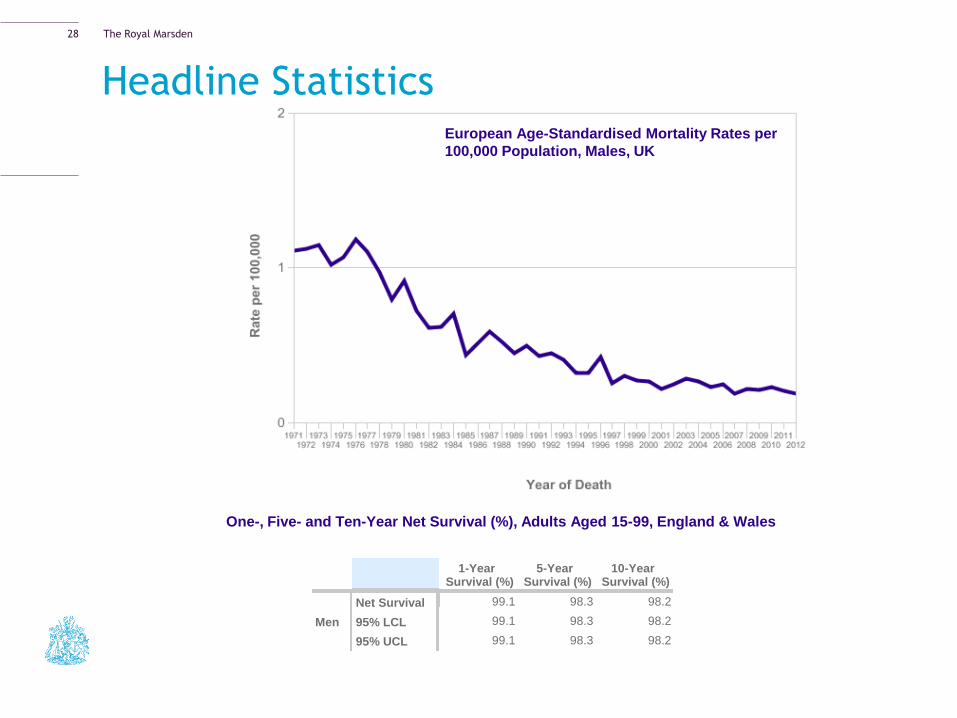
Headline Statistics European Age-Standardised Mortality Rates per
100,000 Population, Males, UK
One-, Five- and Ten-Year Net Survival (%), Adults Aged 15-99, England & Wales
1-Year Survival (%)
5-Year Survival (%)
10-Year Survival (%)
Men
Net Survival 99.1 98.3 98.2
95% LCL 99.1 98.3 98.2
95% UCL 99.1 98.3 98.2
28
The Royal Marsden
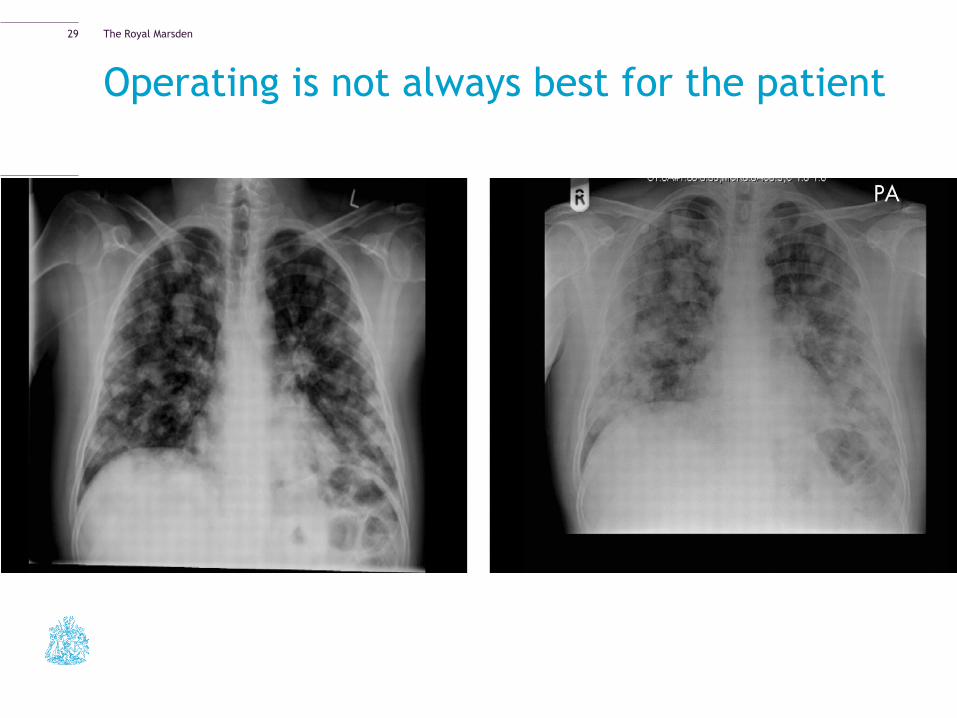
Operating is not always best for the patient
29
The Royal Marsden
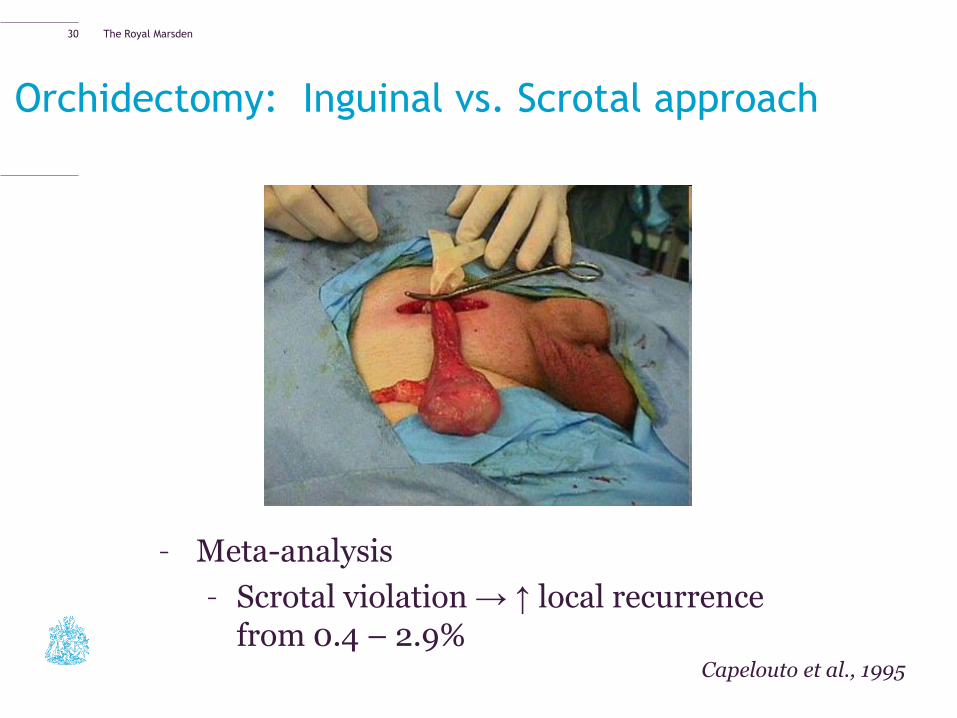
Orchidectomy: Inguinal vs. Scrotal approach
– Meta-analysis
– Scrotal violation → ↑ local recurrence from 0.4 – 2.9%
Capelouto et al., 1995
30
The Royal Marsden
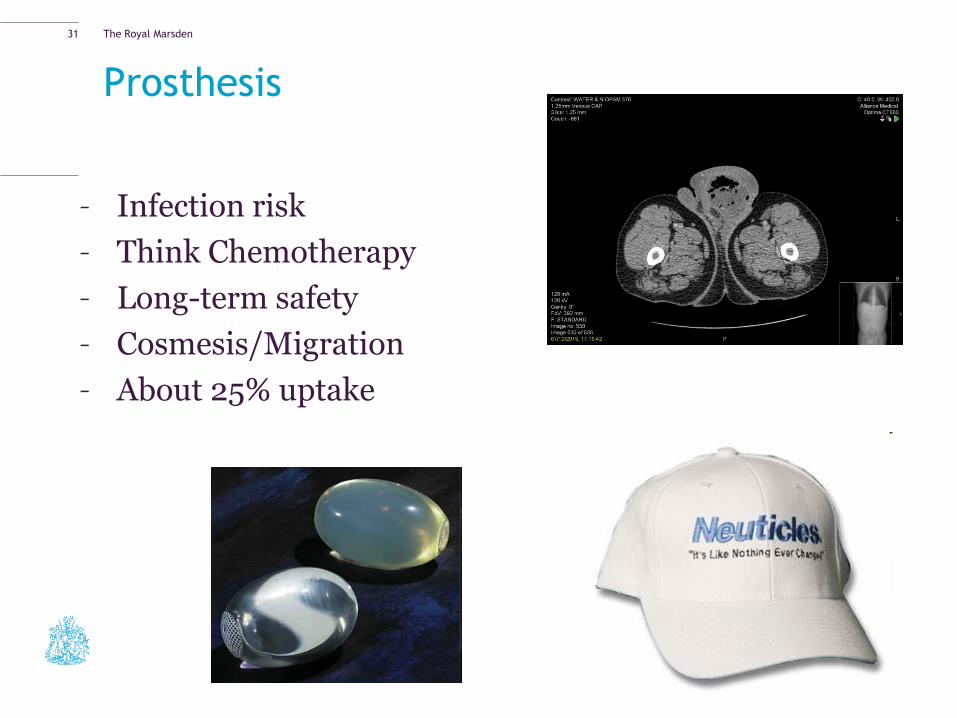
Prosthesis
– Infection risk
– Think Chemotherapy
– Long-term safety
– Cosmesis/Migration
– About 25% uptake
31
The Royal Marsden
Sperm Storage
– Andrology Lab - Hammersmith
– Hep B/C, HIV & CMV screening
– No desperate need to do pre-op although is recommended in
EAU guidelines (3 samples/3 day abstinence)
– Cost associated after year one
– Collecting and freezing the samples can cost between £200
and £400. Then you pay about £300 a year to store them
– Standard storage period 10 years
– Quality of the sperm not guaranteed
32
The Royal Marsden
Further Treatment
– Oncological outcomes – overall survival
– Reducing burden of follow-up
– Minimising ‘overtreatment’ and treatment related morbidity
33
The Royal Marsden
So it’s NOT Cancer
Most testicular lumps are NOT cancer. At a testicular clinic at the Queen Elizabeth Hospital in Birmingham, only 76 cancers were found out of 2,000 men seen with a testicular lump. This means that fewer than 4 in every
100 testicular lumps (4%) are cancer
The awkward Scrotum
34
The Royal Marsden
Differential Diagnosis
– Any cause of scrotal lump/pain
– Testicular torsion
– Torted hydatid of Morgagni
– Epididymal cyst(s)
– Hydrocoele
– Varicocoele
– Epididymitis (orchitis)
– Hernia
– Adenomatoid Tumour
Other findings on Ultrasound
Microlithiasis
Varicocoele
35
The Royal Marsden
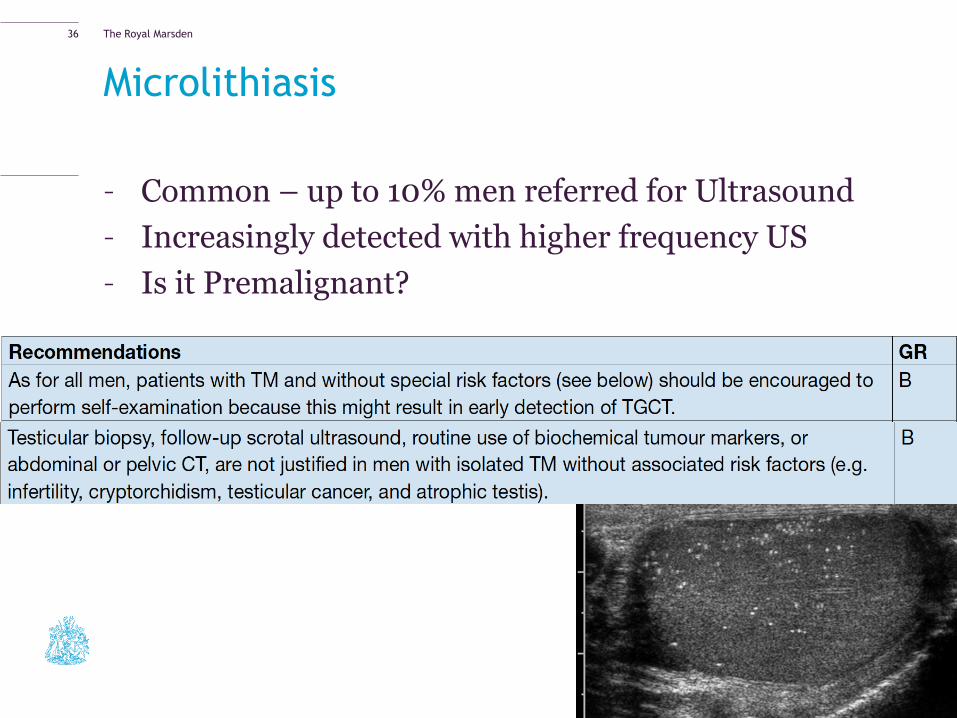
Microlithiasis
– Common – up to 10% men referred for Ultrasound
– Increasingly detected with higher frequency US
– Is it Premalignant?
36
The Royal Marsden
Varicocele – Abnormal dilatation of the testicular
veins in the pampiniform plexus
– 2-22% incidence of normal men, and
25% of infertile men
– Typically pain coming on when standing/
ambulating
– No pain at night
– 90% Left and 10% bilateral
o 10 cms longer and into renal vein.
o ‘nutcracker effect’ left renal vein
between the aorta and SMA.
37
The Royal Marsden
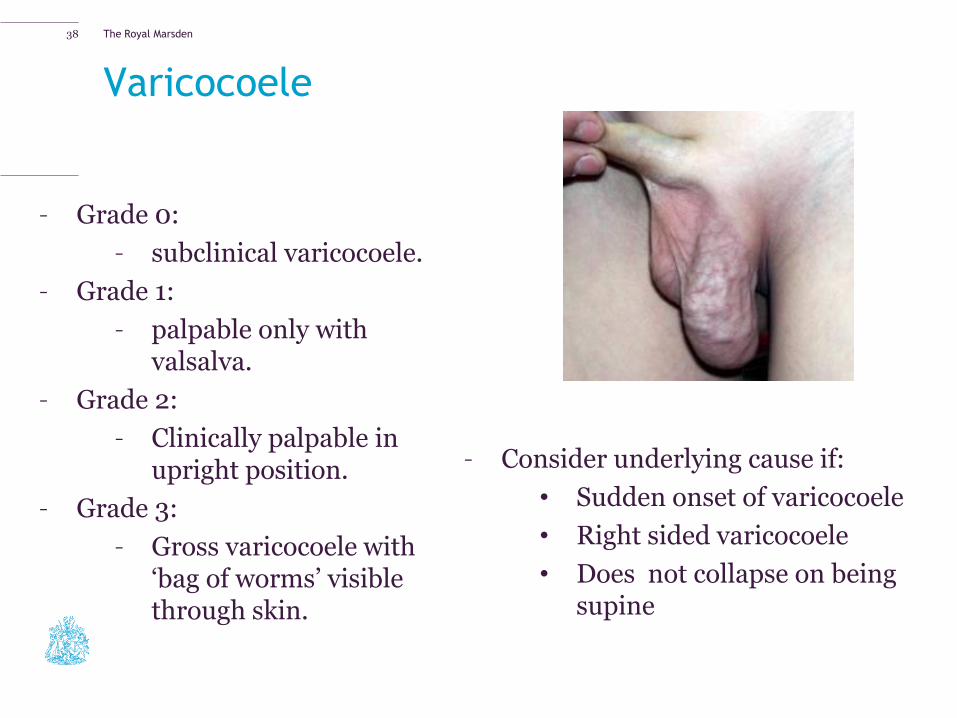
Varicocoele
– Consider underlying cause if:
• Sudden onset of varicocoele
• Right sided varicocoele
• Does not collapse on being supine
38
– Grade 0:
– subclinical varicocoele.
– Grade 1:
– palpable only with valsalva.
– Grade 2:
– Clinically palpable in upright position.
– Grade 3:
– Gross varicocoele with ‘bag of worms’ visible through skin.
The Royal Marsden
Varicocoeles and fertility
– Varicocoeles do not cause infertility
– Routine testing of semen parameters not
required
– Do not require treatment unless associated
with abnormal semen parameters and low
testicular volume in the context of infertility
– Always consider female infertility factors
39
The Royal Marsden
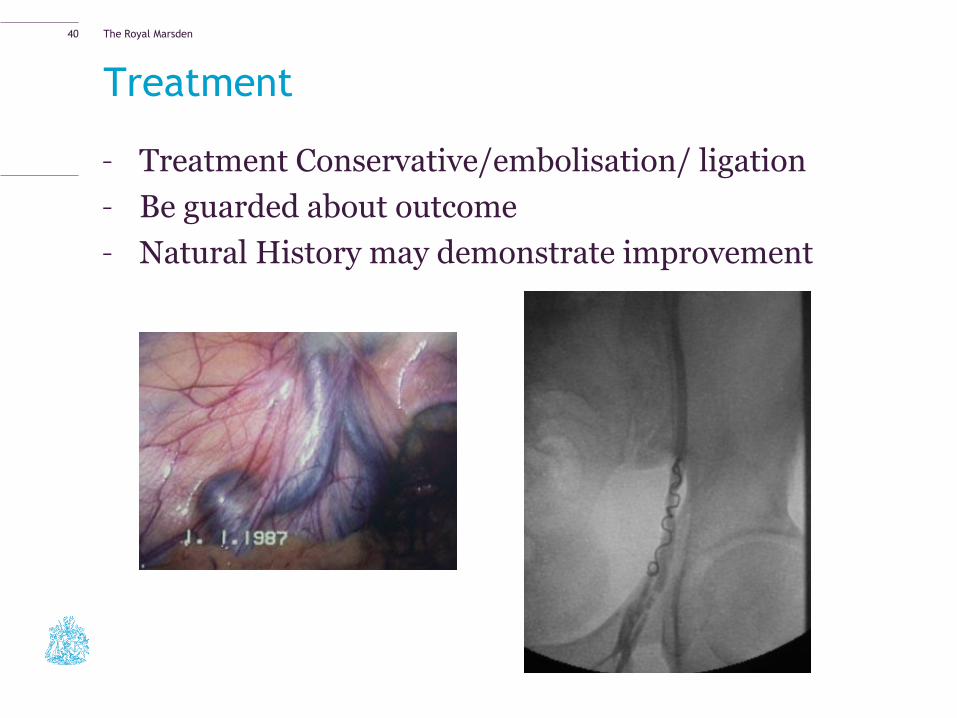
Treatment
– Treatment Conservative/embolisation/ ligation
– Be guarded about outcome
– Natural History may demonstrate improvement
40
The Royal Marsden
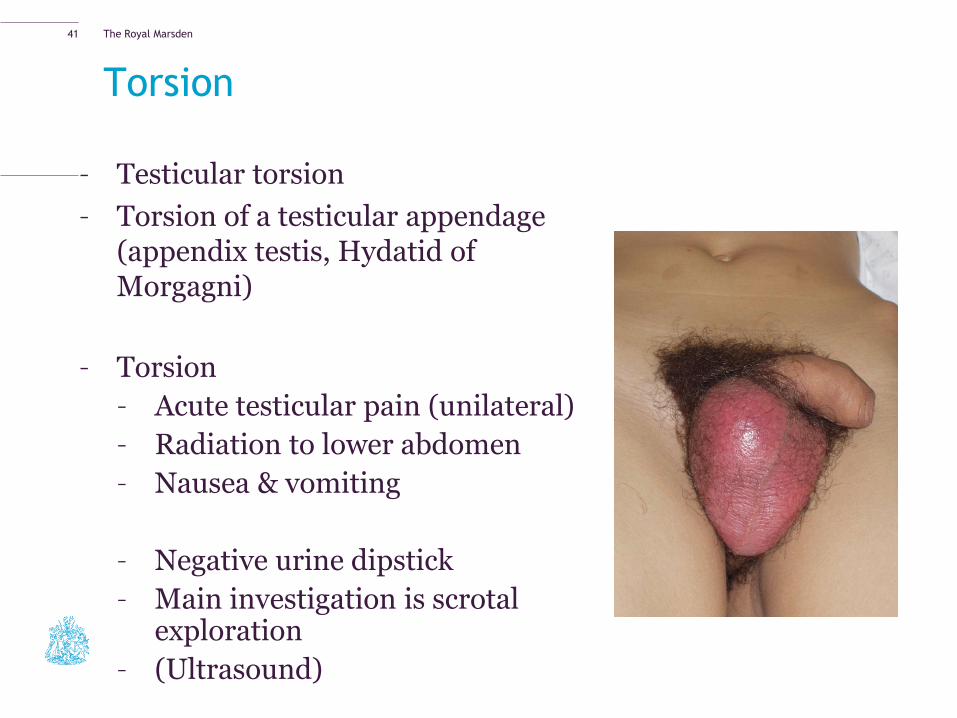
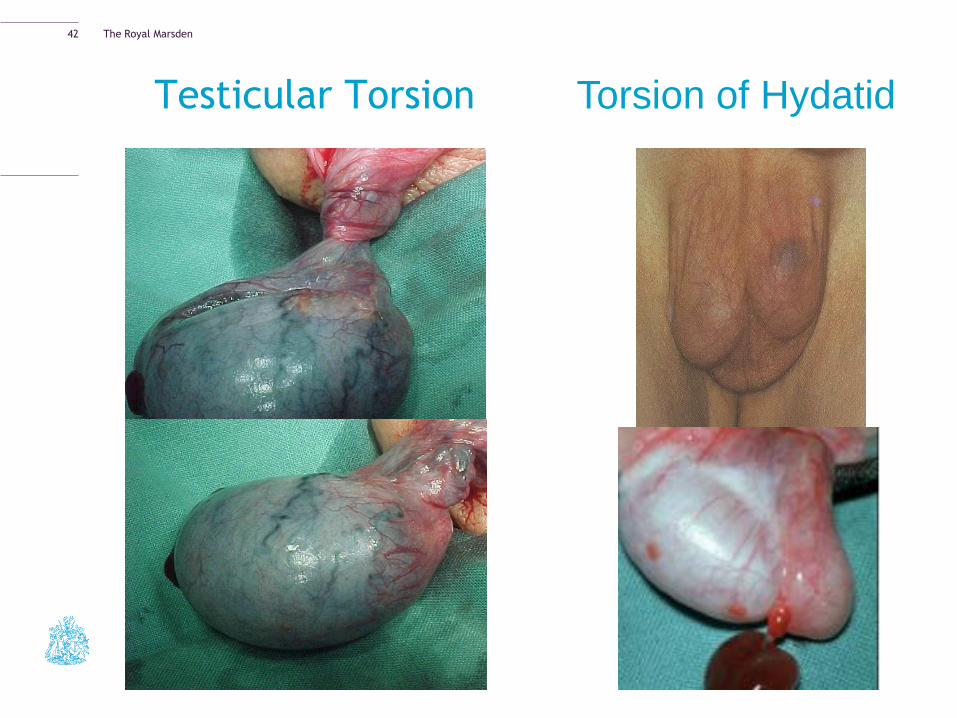
Torsion
– Testicular torsion
– Torsion of a testicular appendage (appendix testis, Hydatid of Morgagni)
– Torsion
– Acute testicular pain (unilateral)
– Radiation to lower abdomen
– Nausea & vomiting
– Negative urine dipstick
– Main investigation is scrotal exploration
– (Ultrasound)
41
The Royal Marsden
Testicular Torsion Torsion of Hydatid
42
The Royal Marsden
Torsion
− Immediate referral to A&E
− No investigation needed
− Scrotal exploration, untwisting of testicle and bilateral 3-point
fixation with non-absorbable sutures in adult, dartos pouch in
children
− Warm ischaemia time 6 hours
− Torted Hydatid of Morgagni – conservative treatment an option
if diagnosis clear
43
The Royal Marsden
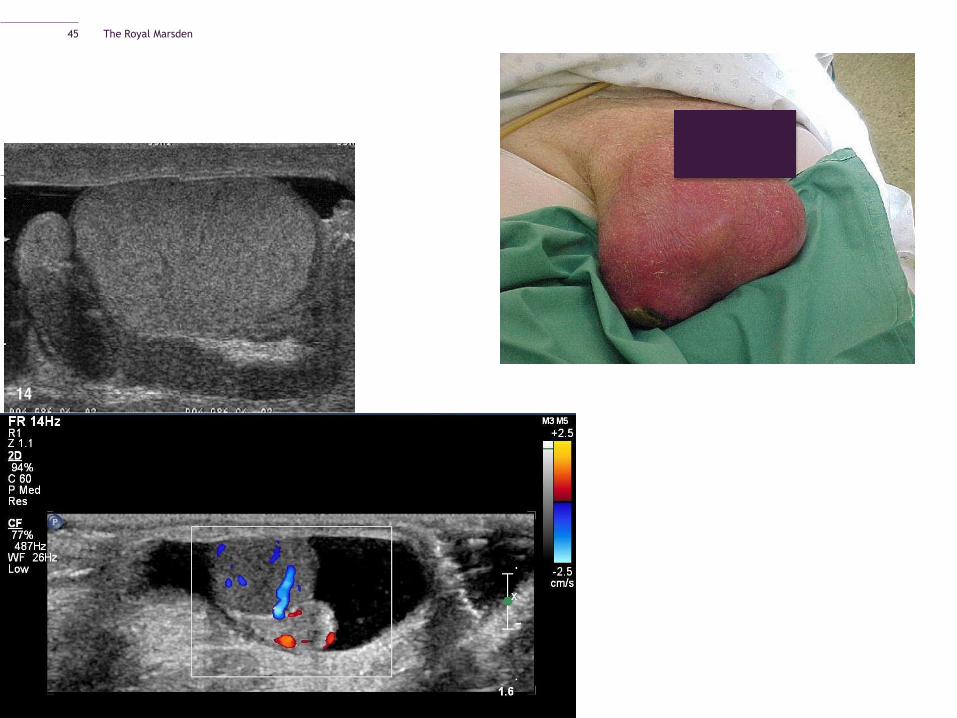
Infection
–Acute epididymitis/Epididymo-orchitis
– Bacterial
– In older men, UTI organisms
– In younger men, Chlamydia and Gonococcus
History
– Examination; tender swelling of epididymis +/- secondary
hydrocoele
– 21 days of appropriate antibiotic but warn patient that swelling
may persist >6 weeks
– Scrotal support
– Patient typically ends up with repeat ultrasound
44
The Royal Marsden
45
The Royal Marsden
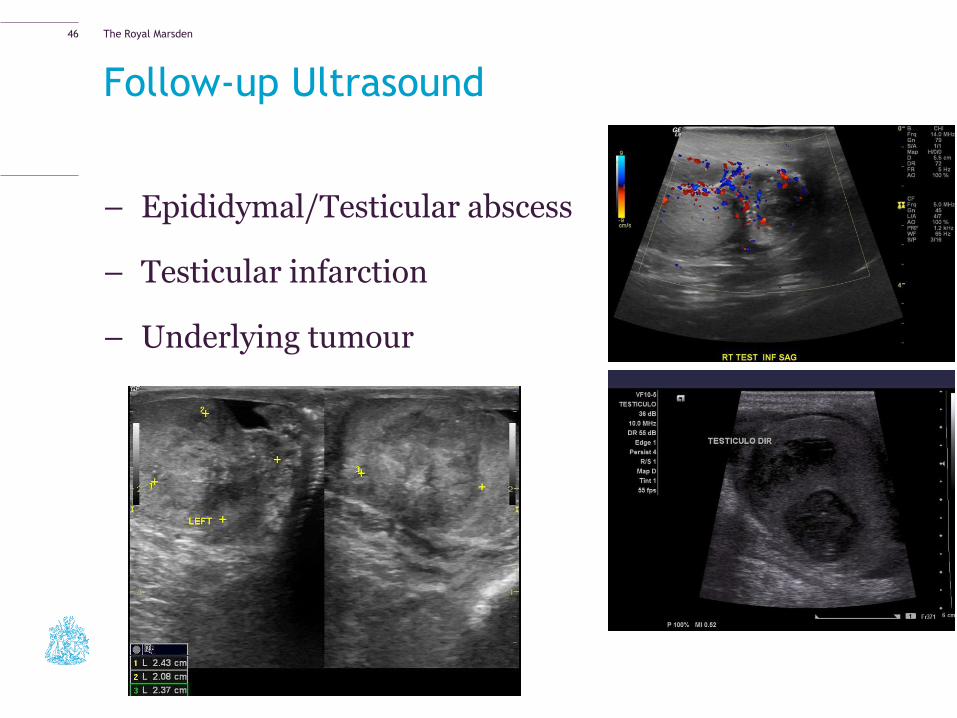
Follow-up Ultrasound
– Epididymal/Testicular abscess
– Testicular infarction
– Underlying tumour
46
The Royal Marsden
Infection
–Orchitis
Can be extension of epididymorchitis
Viral
• Mumps, ?other viruses
• History of parotitis
• Supportive measures – analgesia, bed rest
• Steroids? Tunical incision
If bilateral, mumps orchitis post-puberty may lead to
atrophy and subfertility
47
The Royal Marsden
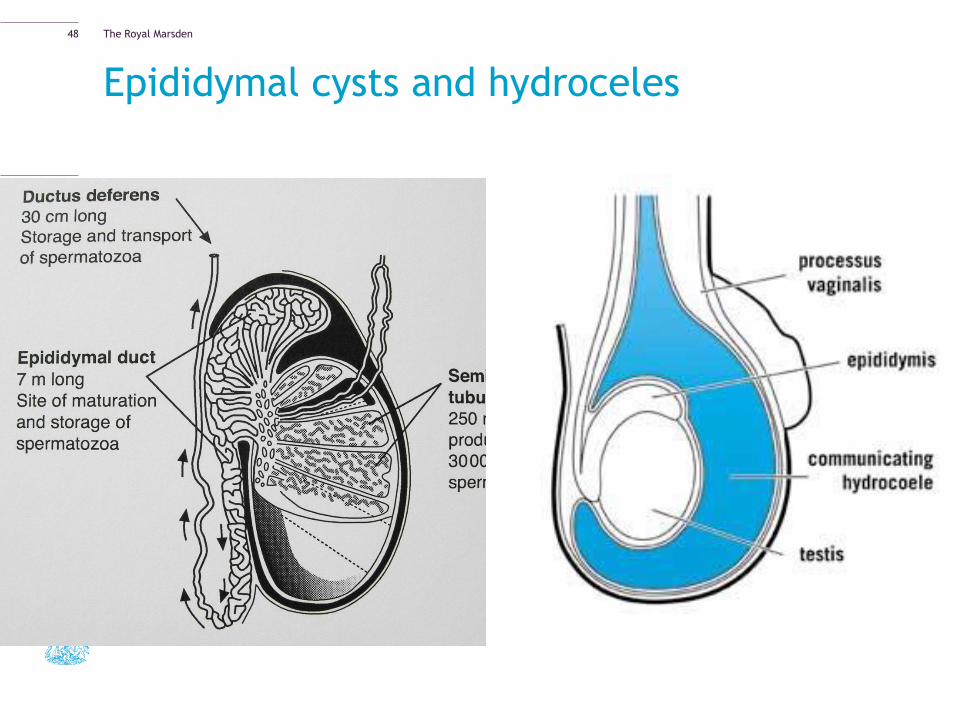
Epididymal cysts and hydroceles
48
The Royal Marsden
Aetiology
Epididymal Cyst
– Possible results from
epididymal tube
obstruction
Hydrocoele
-Excess fluid production
Inflammation
Tumours
-Decreased fluid absorption
Post treatment for varicocoele
-Congenital
Patent Processus Vaginalis
49

The Royal Marsden
Clinical Appearance
50
The Royal Marsden
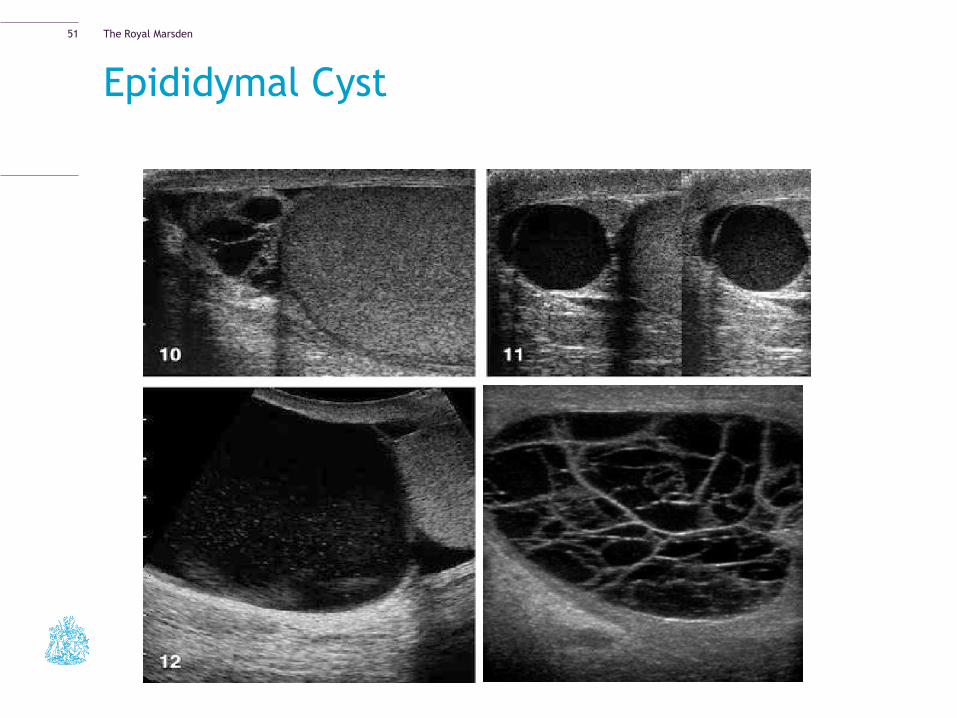
Epididymal Cyst
51
The Royal Marsden
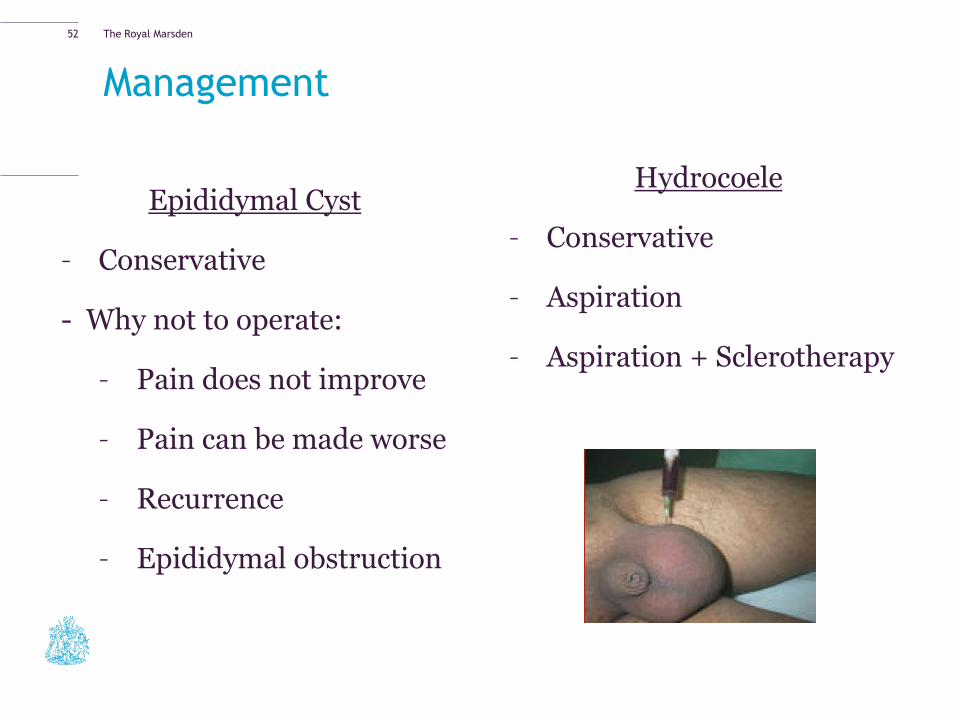
Management
Epididymal Cyst
– Conservative
- Why not to operate:
– Pain does not improve
– Pain can be made worse
– Recurrence
– Epididymal obstruction
Hydrocoele
– Conservative
– Aspiration
– Aspiration + Sclerotherapy
52
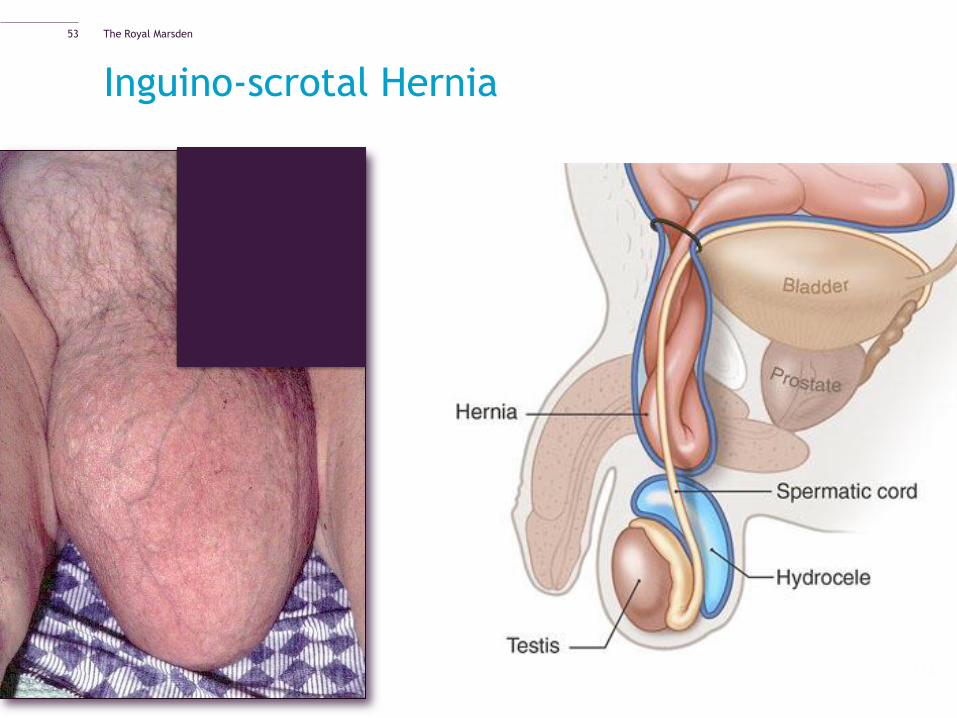
The Royal Marsden
Inguino-scrotal Hernia
53
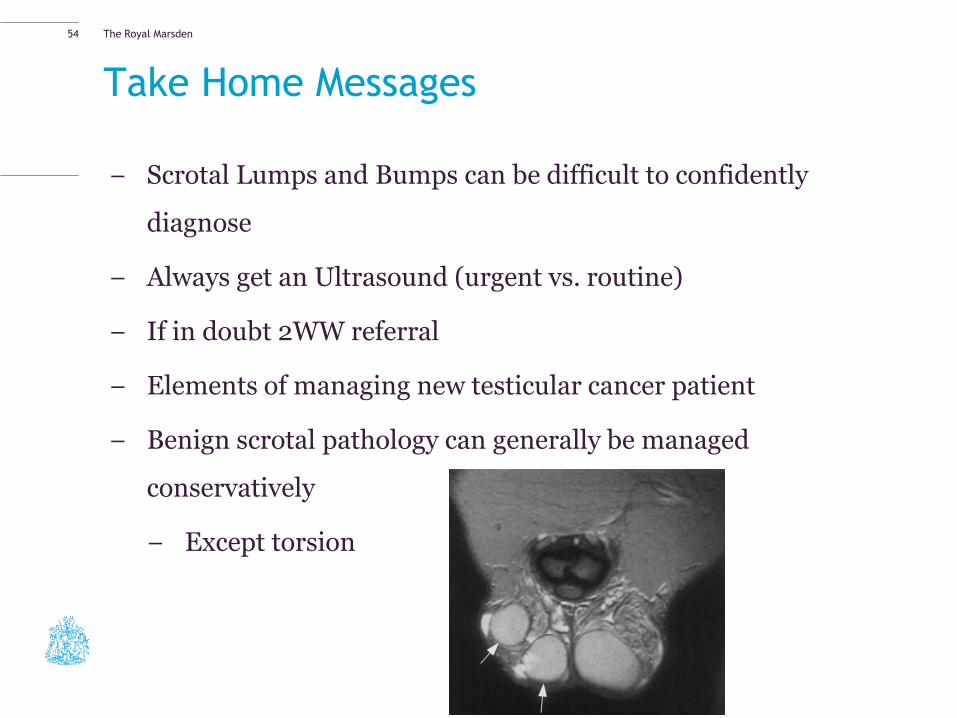
The Royal Marsden
Take Home Messages
− Scrotal Lumps and Bumps can be difficult to confidently
diagnose
− Always get an Ultrasound (urgent vs. routine)
− If in doubt 2WW referral
− Elements of managing new testicular cancer patient
− Benign scrotal pathology can generally be managed
conservatively
− Except torsion
54