Telehealth Alliance of Oregon November 1, 2007
28
Telemedicine Pilot Project Between Sacred Heart Medical Center and Oregon Health & Science University Doernbecher Children’s Hospital Telehealth Alliance of Oregon November 1, 2007
description
Telemedicine Pilot Project Between Sacred Heart Medical Center and Oregon Health & Science University Doernbecher Children’s Hospital. Telehealth Alliance of Oregon November 1, 2007. Presented by. Miles S. Ellenby, M.D., FAAP Associate Professor, Pediatrics & Anesthesiology - PowerPoint PPT Presentation
Transcript of Telehealth Alliance of Oregon November 1, 2007

Telemedicine Pilot ProjectBetween Sacred Heart Medical Center and
Oregon Health & Science University Doernbecher Children’s Hospital
Telehealth Alliance of Oregon
November 1, 2007

Sacred Heart Medical Center 2
Presented by
Miles S. Ellenby, M.D., FAAPAssociate Professor, Pediatrics & Anesthesiology
Division of Critical Care Medicine
Doernbecher Children's Hospital
Oregon Health & Science University
Thomas Roe, M.D.Clinical Professor, Pediatrics, Oregon Health & Science University
Clinical Practice Pediatrics, Eugene, OR
Co-Pediatric Course Director, Oregon Medical Education and Research Collaborative

Sacred Heart Medical Center 3
Disclosure
The Accreditation Council for Continuing Medical Education (ACCME) requires all speakers to make a verbal disclosure of all relevant financial relationships with any commercial interest and the nature of the financial interest pertaining to this lecture.

Sacred Heart Medical Center 4
Sacred Heart Medical Center and Oregon Health & Science University
Sacred Heart Medical Center RiverBend – open August 2008
Sacred Heart Medical Center University District – renovation complete 2010
OHSU tram – opened January 2007

Sacred Heart Medical Center 5
Sacred Heart Medical Center RiverBend

Sacred Heart Medical Center 6
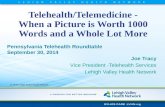
Sacred Heart Medical Center
432 beds
Trauma II
Primary Service Area population: 336,811
Secondary Service Area population: 343,464
100 miles from Oregon Health and Science University
Ground and
Panda Air Transport available • Portland
• Eugene
OREGON
Map Courtesy of KSA

Sacred Heart Medical Center 7
SHMC Current State
• Tele-PICU technology
• Computerized Medical Record
• PAC System (radiology)
• CPOE – Neurology and Rehabilitation units up
• Regionalization of healthcare for medical students
• 32-bed NICU
• No pediatric hospitalists – rollout pending
• Regional hospital with 30-40% admissions from outside Lane County (primary service area)

Sacred Heart Medical Center 8
SHMC Pediatrics Unit
• Pediatric Care Unit opened Spring, 2002− 16 beds, nurse manager, nurse educator
− RNs are PALS certified
• Levels of care: B to E− B – simple
− C – bulk of patients (medical, surgery, trauma)
− D – complex – would be in a PICU at another facility
− E - stabilize and manage for immediate transport
• Patient volume and complexity has increased

Sacred Heart Medical Center 9
SHMC Pediatric Unit Transports
• Current Transports to OHSU and Legacy − Automatic: ventilator, head trauma, heart, new cancer
diagnosis
− Potential: Sepsis, hematologic, neurology (unmanageable seizures)
− Transports are frequently difficult on the family due to loss of work, expenses and lack of local support system.
− CME Children’s Miracle Network Lions Guest House = 14 units

Sacred Heart Medical Center 10
Pediatric Task Force on Regionalization of Pediatric Critical Care
• Pediatric Task Force on Regionalization of Pediatric Critical Care: Consensus report for regionalization of services for critically ill or injured children.
• Crit Care Med 2000;28:236-239.
• Pediatrics Volume 105. 1 January 2000
• Mortality and morbidity of children with serious trauma or illness

Sacred Heart Medical Center 11
A PICU at SHMC?
Question was asked again in 2004: Is a PICU the answer to keep clinically appropriate patients at SHMC?
• Determined not feasible - SHMC does not have enough volume to justify two intensivists and PICU at this time, however …− Acuity level of patients has increased since unit opened in 2002− Many SHMC physicians interested in exploring options for PICU
care− OHSU Critical Care physicians very motivated to start pilot and
are technologically focused and skilled− Telemedicine application proven at UC Davis
• Telemedicine pilot approved Fall 2006• Pilot project started April 2007

Sacred Heart Medical Center 12
Patient Transfer Data
• SHMC transported 58 pediatric patients from January 2004 to Feb 2006 (26 months)− 2/3 of these patients needed a specialist or more
intensive care than was available at SHMC. − 1/3 ended up on OHSU general pediatric ward as PICU
services were not needed
• Cost of transport − Air: $6,378 (fixed wing); $5,486 (rotor wing)
− Ground: $5,832

Sacred Heart Medical Center 13
Background
• OHSU interested in pursuing with SHMC− OHSU Telemedicine champions – Dana Braner, MD; Miles Ellenby, MD
• SHMC Champions− Medical/Nursing
− Manager/Educator Pediatric Unit
− Administrative – Director Marketing and Business Planning
− Physician support
• Meetings held to increase interest− 2005 Telemedicine mini-conference UC Davis
− 2006 first telemedicine colloquium – October 2006
− Grand rounds OHSU - SHMC
− Multiple site visits and meetings

Sacred Heart Medical Center 14
Barriers
• Capital and operating costs to SHMC
• Capital and operating costs to OHSU
• Billing
• Reimbursement
• Credentialing
• Legal and contract issues
• Resistance from physicians

Sacred Heart Medical Center 15
Capital & Start-up Costs
Hardware and Software: Description Qty Cost
Polycom Practitioner Cart with VSX7000 (encoder unit), NTSC, 20" display with power supply and emergency battery backup; includes 1 yr maint on parts 1 $12,746.25
Network connectivity:
DropsDedicated video connection in each room 11 $3,300
Connection Internet or T1 connectionOne time cost Installation and Equipment $4,350 Monthly cost Circuit expense - T1 $750
Network / Desktop Hours:Network Administration hours 120 $4,200
After hours on-call (use existing network rotation)
noincremental
costCHR Hours:
CHR Analyst support and education 16 $560
Total from Information Technology Budget: $25,906.25

Sacred Heart Medical Center 16
Operating Costs
• Primarily Nursing Staff Education− $30,000 SHMC Foundation Education Endowment
•8 hour critical care core curriculum
•4 hour simulation lab experience OHSU
•4 hour job shadow OHSU PICU
•24 of 27 nurses participated
•Post Anesthesia Care Unit job shadows (use of PALS) at SHMC
•2 hour didactic training on use of TM equipment
•Ongoing teaching with scenarios to encourage MD/Staff use
•Plan to follow-up with 4 hour curriculum in 2008, where staff needs indicate

Sacred Heart Medical Center 17
Effects of Pediatric Telemedicine on SHMC
• Physician shortage
• Transportation costs to the patient and facility
• Decreased revenue
• Safety and quality issues
• Recruitment of medical providers

Sacred Heart Medical Center 18
Benefits of Pediatric Telemedicine
• Increase actual and perceived SHMC quality
• Improve mortality
• Decrease LOS
• Decrease complications
• Improve staff morale and expertise
• Enhance training opportunities
• Economic – increased revenues and margin
• Increase collaboration with ED
• Translation service
• 24/7 PICU resource coverage

Sacred Heart Medical Center 19
Additional Clinical Applications
• Started use in Emergency Department August 2007
• Interpretive Services
• Medical Education
• Intra-campus potential – RiverBend to University District
• Expansion to PHMG physician offices

Sacred Heart Medical Center 20
Metrics and Tracking – Set goals and measure outcomes
• Physician satisfaction
• Patient satisfaction
• Staff satisfaction
• Number of uses relative to number of opportunities
• Number of physicians using transports
• Mortality
• LOS
• Financial issues

Sacred Heart Medical Center 21
Summary of Pilot Project
• Telemedicine consults by Doernbecher intensivists with SHMC pediatricians
• Pilot Spring 2007 – Spring 2008; then evaluate for ongoing implementation− Staff Critical Care Core Educational training at OHSU − Credentialing OHSU pediatric critical care physicians
• Financial Considerations− Contribution margin increase from reduced transports− Expenses – staff training, minimal capital− Payment for consults during trial – 1st 30 patients N/C, $500
each after 30− Senate Bill 519 and State of Oregon reimbursement for
Telemedicine

Sacred Heart Medical Center 22
More Telemedicine Benefits

Sacred Heart Medical Center 23
Impact of Telemedicine on Two PatientsCase Studies
− 8 mo presented with hypotonia, lethargy, “cross-eyed”, loss of head control and visual tracking.
− Workup initiated at SHMC including:•Head CT - normal•Brain MRI - normal•LP - 22 WBC’s, normal glucose, protein
− Telemedicine consult performed•early agreement for transport based on worsening mental status &
concern for potential loss of airway protection.
− OHSU Transport Team dispatched by ground.− Shortly after departure, Transport Team received urgent cell
phone call from SHMC RN’s expressing concern over worsening neuro exam. SHMC MD had departed.
− RN’s were unable to call out as land lines were down.

Sacred Heart Medical Center 24
Impact of Telemedicine on Two PatientsCase Studies
− Transport Team informed PICU attending, questioning need to dispatch helicopter to expedite transport.
− PICU attending was also unable to reach SHMC by phone, but Telemedicine equipment worked.
− Led RN’s through repeat neuro exam including pupillary exam.
− Neuro exam was unchanged from previous.
− What had changed??? The RN’s had changed shift.
− Transport continued by ground and was uneventful.
− Infant was hospitalized x 16 days at OHSU, ultimately had full recovery from meningo-encephalitis (either viral, post-viral, or partially-treated bacterial).

Sacred Heart Medical Center 25
Impact of Telemedicine on Two PatientsCase Studies
− 2 mo hospitalized at SHMC with bronchiolitis.
− By hospital day 5, infant was clinically improving but a CXR demonstrated a large pneumothorax.

Sacred Heart Medical Center 26
Impact of Telemedicine on Two PatientsCase Studies
− OHSU Transport Team urgently dispatched based on size of pneumothorax and possible need of emergent intervention.
− Telemedicine consult performed.− Infant looked “so good” compared to CXR findings that a repeat film was
requested by PICU attending.
− Transport was cancelled with the new finding.

Sacred Heart Medical Center 27
Demonstration of Telemedicine in ICU setting

Sacred Heart Medical Center 28
Telemedicine Parent Testimonial