TEACHING STRATEGIES USED BY TEACHERS TO ENHANCE …
179
1 TEACHING STRATEGIES USED BY TEACHERS TO ENHANCE LEARNING TO LEARNERS WITH MULTIPLE DISABILITIES IN FOUR SELECTED COUNTIES IN KENYA By WANG’ANG’A ANNE ROSE WANJIKU E83/21627/2010 A RESEARCH THESIS SUBMITTED FOR THE AWARD OF THE DEGREE OF DOCTOR OF PHILOSOPHY (SPECIAL EDUCATION) IN THE SCHOOL OF EDUCATION OF KENYATTA UNIVERSITY AUGUST 2014
Transcript of TEACHING STRATEGIES USED BY TEACHERS TO ENHANCE …

1
TEACHING STRATEGIES USED BY TEACHERS
TO ENHANCE LEARNING TO LEARNERS WITH
MULTIPLE DISABILITIES IN FOUR SELECTED
COUNTIES IN KENYA
By
WANG’ANG’A ANNE ROSE WANJIKU
E83/21627/2010
A RESEARCH THESIS SUBMITTED FOR THE AWARD OF
THE DEGREE OF DOCTOR OF PHILOSOPHY (SPECIAL
EDUCATION) IN THE SCHOOL OF EDUCATION OF
KENYATTA UNIVERSITY
AUGUST 2014

2

3
DEDICATION
This thesis is dedicated to the teachers, parents and caregivers of learners with multiple
disabilities.

4
ACKNOWLEDGEMENT
I am grateful to Kenyatta University for giving me an opportunity to pursue my doctorate degree
programme. My sincere gratitude goes to my supervisors Professor G.K. Karugu and Doctor
Evariste Karangwa who devoted a lot of their time patience and guidance towards the completion
of my study. I wish to acknowledge all the lecturers in the department of Special Needs
Education Kenyatta University for their encouragement. My thanks go to Professor G.K Njoroge
from the University of Rwanda, Dr. Francis N. King‟ori of Freb pharmaceuticals Kiambu and
Professor Gathogo Mukuria from the University of Nairobi for their advice and encouragement.
My deep appreciation goes to my son Morris Mithamo and my daughter Elizabeth Waithera for
their unfailing support. Above all, I wish to thank the Almighty God through whose grace I was
able to realize this long cherished dream.

5
TABLE OF CONTENTS
Title Page…………………………………………………………………………………..1
Declaration………………………………………………………………………………..2
Dedication………………………………………………………………………………...3
Acknowledgment………………………………………………………………………... 4
Table of contents………………………………………………………………………….5
Abbreviations and Acronyms……………………………………………………………11
Abstract………………………………………………………………………………….13
CHAPTER ONE: INTRODUCTION
1.0 Introduction…………………………………………………………………………....14
1.1 Background of the Study……………………………………………………………...14
1.2 Statement of the Problem……………………………………………………………...19
1.3 Purpose of the Study…………………………………………………………………..20
1.4 Objectives to the Study………………………………………………………………..21
1.5 Research Questions……………………………………………………………………21
1.6 Significance of the Study……………………………………………………………...21
1.7 Delimitations and Limitations…………………………………………………………22
1.8 Assumptions of the Study…………………………………………………………….23
1.9 Theoretical and Conceptual Framework………………………………………………24
1.9.1 Theoretical Framework……………………………………………………………...24
1.10 Conceptual Framework……………………………………………………………..26
1.11 Operational Definition of Terms……………………………………………………28
CHAPTER TWO: LITERATURE REVIEW
2.0 Introduction………………………………………………………………………….30
2.1 Instructional Methods for Learners with deaf blindness….........................................30
2.1.1 Curriculum Adaptations for learners with deaf blindness ………………...............43
2.1.2 Teaching Resources and Support Services for Learners with deaf blindness…......46

6
2.1.3 Environmental Adaptations Required for Learners with deafblindness..................49
2.2 Instructional Methods for learners with autism and blindness………………………51
2.2.1 Curriculum Adaptations for learners with autism and blindness ….........................56
2.2.2 Teaching Resources and Support Services for Learners with autism blindness…...57
2.3 Instructional Methods for learners with cerebral palsy intellectual disability……….48
2.3.1Curriculum Adaptations for learners with cerebral palsy intellectual disability…...59
2.3.2 Teaching Resources and Support Services for learners with cerebral palsy
intellectual disability………………………………………………………………69
2.3.3Treatment and Therapy for Learners with cerebral palsy intellectual disability…...75
2.3.4Adaptations for Learners with cerebral palsy intellectual disability ………………79
2.4 Training needs of specialized personnel for learners with multiple disabilities……..82
3.0 CHAPTER THREE: METHODOLOGY
3.0 Introduction………………………………………………………………….............88
3.1 Research Design……………………………………………………………………..88
3.2Variables………………………………………………………………………….......89
3.3 Location of the Study……………………………………………………………….89
3.4 Target Population…………………………………………………………………....90
3.5 Sampling Techniques and Sample Size……………………………………………...91
3.5.1Sampling Techniques………………………………………………………….........91
3.5.2Sample Size…………………………………………………………………………93
3.6 Construction of Research Instruments…………………………………………….....84
3.7 Pilot Study……………………………………………………………………………95
3.7.1Validity……………………………………………………………………………..96
3.7.2Reliability…………………………………………………………………………...96
3.8 Data Collection Techniques……………………………………………………….....97
3.9 Data Analysis………………………………………………………………………...98
3.10 Logistical and Ethical Considerations……………………………………………...99

7
CHAPTER FOUR: DATA PRESENTATION ANALYSIS AND DISCUSSION
4.0 Introduction………………………………………………………………………….101
4.1 Demographic data of the respondents……………………………………………….101
4.2 Instructional Methods for learners with multiple disabilities………………………..103
4.2.1 Teachers Responses on the instructional Methods for learners with multiple
disabilities………………………………………………………………………..109
4.3 Curriculum Adaptations for learners with multiple disabilities ……………………115
4.4 Available teaching resources for learners with multiple disabilities……………….116
4 .4.1 Teachers responses on available teaching resources for learners with multiple
Disabilities…………………………………………………………………….. 116
4.4.2 Headteachers responses on available teaching resources for learners with multiple
disabilities………………………………………………………………………...120
4.5 Support Services for learners with multiple disabilities……………………………121
4.6 Training needs of teachers handling learners with multiple disabilities……………124
4.7 Strategies to improve teaching……………………………………………………...130
4.7.1 Headteachers recommendations………………………………………………….134
CHAPTER FIVE: SUMMARY CONCLUSION AND RECOMMENDATIONS
5.0 Introduction…………………………………………………………………………138
5.1 Summary of Findings……………………………………………………………….138
5.2 Implications of the Findings………………………………………………………..144
5.3 Conclusion………………………………………………………………………….144
5.4 Recommendations…………………………………………………………………..145
5.5 Suggestions for further research……………………………………………………147
REFERENCES……………………………………………………………………….148
APPENDICES………………………………………………………………………. 164

8
LIST OF TABLES
Table 3.1 Study Framework for the Target Population…………………………………91
Table 3.2 Sample Size…………………………………………………………………..92
Table 4.1 Teachers‟ professional qualification across gender………………………….102
Table 4.2 Teachers‟ experience across learners‟ impairments………..…………………103
Table 4.3 Instructional Methods used for Learners with deaf blindness………………..104
Table 4.4 Instructional Methods used by teachers for learners‟ with autism blindness…106
Table 4.5 Instructional Methods used by teachers for learners‟ with cerebral
palsy intellectual disability………………………………………………… 108
Table 4.6 Teachers responses on instructional methods used for learners with
deafblindness……………………………………………………………….109
Table 4.7 Teachers responses on instructional Methods Used for learners with
autism blindness……………………………………………………………111
Table 4.8 Teachers responses on instructional methods used for learners with cerebral
palsy intellectual disability………………......................................................105
Table 4.9 Teachers responses on available teaching resources used for teaching learners
with deafblindness…………………………………………………………113
Table 4.10 Teachers‟ responses on available teaching resources available for teaching
learners with autism blindness……………………………………………..118
Table 4.11 Teachers responses on available teaching resources for educating
learners with cerebral palsy intellectual disability…………………………119
Table 4.12 Teachers‟ responses on support services given to learners with cerebral palsy
intellectual disability………………………………….................................122

9
Table 4.13 Teachers responses on training needs of teachers educating learners with
deafblindness……………………………………………………………..125
Table.4.14 Teachers responses on training needs of teachers educating learners with
autism blindness…………………………………………………………127
Table 4.15 Teachers responses on training needs to teach learners with cerebral palsy
Intellectual disability ………………………………………………………128
Table 4.16 Recommendations from teachers educating learners with deafblindness….130
Table 4.17 Recommendations from teachers educating learners with autism blindness.131
Table 4.18 Recommendations from teachers educating learners with cerebral palsy
intellectual disability………………………………………………………133
Table 4.19 Recommendations from head teachers on ways of improving learning to
Learner‟s with deafblindness………………………………………………..134
Table 4.20 Recommendations from head teachers on ways of improving learning to
Learner‟s with autism blindness…………………………………………...135
Table 4.21 Recommendations from head teachers on ways of improving learning to
Learner‟s with cerebral palsy intellectual disability……………………….136

10
LIST OF FIGURES
Figure1.1. A Diagrammatic Representation of the Conceptual Frame work…………..26

11
ABBREVIATIONS AND ACRONYMS
AB: Autistic blind
AAC: Alternative Augmentative Communication
AFB: American Foundation for the Blind
APA: American Psychiatry Association
ASL: American Sign Language
AAIDD: American Association on Intellectual and Developmental Disabilities
CARS: Childhood Autism Rating Scale
CAI: Computer Assisted Instruction.
CASE: Conceptually Signed English
CPID: Cerebral palsy Intellectual disability.
DFB: Deaf blind
DSM-IV: Diagnostic Statistical Manual for Mental Disorders Fourth Edition.
FLASA: Florida Association of Speech language Pathologists and Audiologists
Convention.
IEP: Individualized Education Programme
KIE: Kenya Institute of Education
KISE: Kenya Institute of Special Education.
KU: Kenyatta University
KNEC: Kenya National Exams Council
MDT: Multidisciplinary team
MOVE: Mobility opportunities via education
MSD: Multi Sensory Deprived.
NCST: National Council of Science and Technology
NIMH: National Institute for the Mentally Handicapped .
SN: Special Needs.
SI: Sensory integration theory

12
SNE: Special Needs Education.
SPSS: Statistical packages for Social Sciences
VAK: Visual Auditory and Kinesthetic Learning Styles.
VI: Visually impaired

13
ABSTRACT
The purpose of this study was to investigate the teaching strategies used by the teachers
educating learners with multiple disabilities in the counties of Baringo, Kiambu, Kisumu and
Nairobi in Kenya. Multiple disabilities are a combination of two or more disabilities. In this
study learners with multiple disabilities include; cerebral palsy intellectual disability, autism
blindness and deaf blindness. The study adopted a triangulation mixed method design. The study
targeted a sample of 9 headteachers and 57 teachers educating learners with multiple disabilities.
Purposive sampling was used to sample the respondents. Piloting the instruments was done in
schools that were not involved in the actual study. The research instruments that were used
included interviews, observation guides and questionnaires with a Likert scale. Reliability of the
instruments was determined by test-retest method. Content related validity was used as a
measure to determine validity. The study used descriptive statistics for the quantative data where
tables of frequencies, mean, standard deviation, and percentages were used to analyze data.
Qualitative data were analyzed using descriptions and thematic text. Results revealed that
majority of the teachers teaching learners with deafblindness used the following instructional
methods; tactile Kenyan sign language, task analysis, Tadoma, sign language among others.
Majority of teachers teaching learners with autistic blind used the following instructional
methods; braille, pre-braille activities, oral methods among others. Majority of teachers teaching
learners with cerebral palsy intellectual disability used the following instructional methods; use
of task analysis, activities of daily living, and real objects among others. The choice of the
instructional method was determined by the needs of learners. Results also revealed that teachers
were inadequately prepared to teach learners with multiple disabilities because their training was
for a specific disability. The curriculum for learners with autism blindness and cerebral palsy
intellectual disability was found to be ineffective. Teachers educating learners with deaf
blindness used the final draft of an adapted curriculum from Kenya institute of Curriculum
Development. Teaching resources and support services were found to be inadequate. The
following were the recommendations that were made following the study findings to improve
teaching; training teachers, provision of a functional curriculum, provision of adequate support
services, provision of enough teaching resources among others.

14
CHAPTER ONE
INTRODUCTION
1.1 Background to the Study
This chapter presents; background to the study, statement of the problem, purpose of the study,
research objectives, research questions, significance of the study, delimitations and limitations,
assumptions, theoretical and conceptual framework and operational definition of terms. Multiple
disabilities means concomitant impairments such as intellectual disability-blindness, intellectual
disability-orthopedic impairment, the combination of which causes such severe educational
needs that they cannot be accommodated in special education programs solely for one of the
impairments (Hallahan, Kauffman & Pullen, 2012). Children with multiple disabilities have a
combination of various disabilities that may include; speech, physical, mobility, learning,
intellectual disability, visual, hearing, brain injury and possibly others. Along with multiple
disabilities, they can also exhibit sensory losses, behavior and social problems. Children with
multiple disabilities will vary in severity and characteristics. These students may have difficulty
attaining and remembering skills or transferring these skills from one situation to another.
Support is usually needed beyond the confines of the classroom. Programming for these children
will be based on the characteristics they display (Watson, 2003; Heller, Forney, Alberto, Best &
Schwartzman, 2009).
According to Hosken (2008), it is difficult to define the term severe and multiple disabilities
precisely because no one definition covers all the conditions that special educators and
psychologists know about. Usually these students have intellectual disability that is accompanied
by other disabilities such as extensive physical disabilities and delayed language skills. Some of
them however have normal intelligence even though their physical and language disabilities may
mask it. There are two major themes in this definition, the extent of the disability is beyond
moderate levels, and there are two or more disabilities occurring simultaneously. Most of the
students served in programmes for severe and multiple disabilities have severe intellectual
disability. Teaching strategies are the methods used to allow learners to access the information
being taught.
15
The teaching strategies determine the approach a teacher may take to achieve learning objectives
(Turnbull, Turnbull &Wilcox 2002). “Instructional methods are the how to” in the delivery of
training. The methods used in any learning situation are primarily dictated by the learning
objectives decided up upon by the course developers. In many cases, combinations of methods
are used to facilitate the learning experiences (Hosken, 2008). The goal of a comprehensive
program for learners with multiple disabilities should be one of increasing their independence.
The functional skills assessment will identify the areas of need and provide structure to address
those areas. The first skills to be taught are those which the learner needs most often in order to
function more independently in a least restrictive environment. Some of the issues to consider
when making skill selections are: Learner‟s health and safety, future programs, level of
independence, age appropriateness and logistics of instruction (Sense International India, 2010).
In developing the learner‟s Individualized Education Plan (IEP), it will be necessary to consider
the need for instruction across several areas of learning, such as sensory development, motor
skills, communication skills, cognition, social development, self care, daily living and
community living activities, recreation or leisure time and vocational skills. For the learner to
benefit from specialized instruction, it may be necessary for some learners to receive appropriate
related services.
In implementing an educational program, attention should be given on the instructional
techniques used, the functionality of the skills taught and the age appropriateness of the
instructional materials and activities used (Best, Heller & Bigge, 2010; Hardman, Drew &Egan,
2005). There are a number of factors affecting choice of teaching strategies for the multiple
disabilities. They include type of disability, level of severity and learner‟s age level among
others. The techniques and materials used to teach learners with one type of disability may be
quite different from those used for another disability. The more serious the disability, the more
likely the learner is to be educated in a special setting (Cartwright, Trudgil & Mansfield, 1995).
There are several components to an effective instructional programme. They include:
Assessment, curriculum, methodology and ongoing evaluation. Assessment is usually seen as the
beginning of instructional models. The teacher needs to know whether there are any medical or
physical factors that will limit performance or affect what should be taught and how it should be
taught. The teacher also needs to know what capabilities the learner possesses as well as deficits

16
and excesses demonstrated and the point at which instruction should begin. Thus there should be
a direct correlation between what is on the test and the curriculum content. The curriculum
should be extensive, ideally consisting of an exhaustive number of items within each curriculum
area. These items should be stated in behavioural terms. Since it is probably impossible to
develop an exhaustive list of behaviours, teachers should always view items as open ended so
that skills can be added or modified as needed for each individual learner. The curriculum for
learners with multiple disabilities includes: the following general skills areas: self care,
socialization, communication, motor, pre-academic and leisure or vocational (Scutta, 2011;
Aslop, 2002; Ellis, 1986).
The history of the education of learners with multiple disabilities can be traced to persons such as
Anne Sullivan Macy (1866-1936) a teacher who used tactile finger spelling to teach Hellen
Keller who was deaf-blind. Hellen Keller became the first learner who was deaf-blind to get a
Bachelors of Arts degree. Laura Bridgman a learner who was also deaf-blind was taught by the
director Perkins Institute of the Blind among others (American Foundation for the Blind (AFB),
2013. According to Deaf blind International (2003), the prevalence of severe and multiple
disabilities is no more than 0.1% to 1.0%. According to the World Bank, the prevalence rate of
multiple disabilities in Kenya is under 1% (Mont, 2007). Globally, research studies have been
carried out on multiple disabilities such as autism blindness; whereby in Norway they found out
that the prevalence of blindness among autistic people was relatively high (National Autism
Programme, 1998).
In Britain, a research project was carried out on the curriculum access for learners with deaf
blindness. The study found out the importance of teaching strategies which were primarily
communicative and which enabled the child to both anticipate and gain a clearer understanding
of what the task demanded. The study also found out the need for teachers to have access to a
wide range of specialist strategies especially where they are working with pupils with the most
complex needs thus teachers need to be able to adapt more generic strategies to meet the specific
needs of an individual. Some of effective strategies identified in the study included; signing,
speech, music prompts and objects of references (Porter, Miller, Pease, 1997). In America, a case
study was carried out on training a learner who was autistic blind to communicate through signs.
17
The child was able to acquire a function sign vocabulary relying primarily on the tactile
kinesthetic and auditory modalities. The newly acquired skill had a beneficial impact on the
child‟s general functioning (Konstanareas, 1982). In Africa, studies were carried out on learners
who are deaf with multiple disabilities in developing countries such as Kenya, Malawi,
Cameroon, Nigeria, Uganda, and Somalia among others. In Kenya, they found out that there
were learners with deaf and multiple disabilities in special schools for the Deaf. For instance, in
Njia special school in Meru North District. They found that no progress had been carried out on
how to deal with the learners who were deaf with multiple disabilities (Shettle, 2004).
A study carried out by the Kenya Institute of Education (KIE) in 1980 on additional disabilities
among 896 children enrolled in special schools for the physically disabled revealed that there
were learners with multiple disabilities(Ndurumo, 1993).The question is whether these learners
with multiple disabilities in our schools are being provided with appropriate instructional
interventions for their diverse needs. The approximate number of learners with multiple
disabilities in the counties of Baringo, Kisumu, Kiambu and Nairobi is about 300. According to
the National Bureau of Statistics (2009), the total population of people in the four counties is
6,286,121. The percentage of people with multiple disabilities is about 0.05 percent. The
Kochung Report (2003) found out that there was lack of reliable statistical data on learners with
Special needs in Kenya. It is most likely that this percentage may be higher due to the following
factors namely, lack of accessibility in certain areas, lack of sensitization regarding learners with
disabilities, among others. This state of affairs is detrimental to learners‟ acquisition of education
and denial of their rights to education. According to the Deaf blind pilot project report (1992-
1996), the population of the deaf-blind in Kenya has not yet been established and an awareness
of the condition among the communities and the authorities concerned. For instance education,
health, administration and social services is still limited, therefore education facilities for these
persons are very few resulting in such learners being placed in either schools for the Deaf or the
visually impaired. The question is whether the learners with deaf-blind are receiving the
appropriate instructional intervention strategies to cater for their diverse needs. In Kenya,
learners with multiple disabilities are found in some of our special schools, special units and in
regular schools (Kochung Report, 2003). Learners with cerebral palsy are categorized under the
physically disabled and are thus educated in schools for learners with physical disabilities and

18
also in schools for learners with intellectual disabilities. Learners with autistic blind may be
found in special schools for the blind and in some special units. In major special schools such as
Thika primary school for the Blind, Likoni school for the Blind among others, a „’special class’’
in the special school has been set aside for learners with multiple disabilities. In Thika primary
school for the blind, the special class is referred to as the „’green class’’. It is not clear what
instructional methods are used to cater for these learners diverse needs in the “special class”. A
special class is a class that is set aside for learners with multiple disabilities. Learners with deaf
blindness are found in some special units and in Kabarnet special school for the Deaf blind.
The Ominde Report (1964) advocated for teacher training to include a component of Special
Education (SE) to meet the needs of learners with Special needs (SN). Kenya is cognizant of the
need to provide specialized training to teachers. This is evidenced by several institutions that
have been set up to offer special education training. These institutions include; Kenyatta
University, Maseno University, Kenya Institute of Special Education (KISE), Moi University,
Pwani University among others. The question is whether and to what extent the curricula used in
these institutions are customized according to the specific educational needs of the learners in
relation to the level and type of disability such as multiple disabilities. The training of special
education teachers in Kenya has been categorical based on the four major areas of disability
namely, hearing, visual, physical and. It is not clear whether teachers are able to differentiate
instructions when faced with learners with more than one disability. In 2006, KISE started
training teachers to teach learners with deaf blindness; however, there are other learners with
multiple disabilities such as autism blindness, cerebral palsy and intellectual disability among
others that require teachers to be retrained to help them cater for these learners‟ instructional
needs. According to Rule 6 of the United Standards Rules on the Equalization of Opportunities
for Persons with Disabilities (1993), education should be provided in an integrated school setting
and in general school setting. It is not clear what is being done in Kenya in order to ensure the
specific education needs of learners with multiple disabilities are mainstreamed, since they are
found in all our school settings. Besides, the Koech Report (1999) reveals that a large number of
teachers in special schools need to be retrained to cope up with knowledge evolution and
teaching techniques in special education. It is not clear whether teachers have been retrained or
updated to cope up with new knowledge and teaching strategies in specific disabilities such as

19
multiple disabilities. The Kochung Report (2003) reveals that learners with multiple disabilities
can follow a specialist curriculum. A specialist curriculum remediates problems of learners such
as communication, mobility among others. It is not clear whether the curriculum for learners
with multiple disabilities has been adapted or modified to cater for the diverse needs of the
learners. Furthermore, the National Policy on Special Needs (2009), a Ministry of Education
policy launched in 2010, shows that the only documented multiple disabilities is deaf-blind it is
not clear why other learners with multiple disabilities such as autism blindness, cerebral palsy
intellectual disabilities among others are not specifically included. The background information
available points out to the deficient efforts to mainstream the needs of learners with multiple
disabilities in all our school settings. In this context, the instructional environment is a factor of
interest. The study sought to investigate the teaching strategies used by teachers for learners with
deaf blindness, autism and blindness and cerebral palsy and intellectual disability in the counties
of Baringo, Kisumu, Kiambu and Nairobi in Kenya.
1.2 Statement of the Problem
Studies carried out by Shettle (2004), Kochung Report (2003), Deaf blind pilot project (1992-
1996) and Kenya Institute of Education (KIE) (1980) revealed that there were learners with
multiple disabilities in schools for learners with single disabilities. However, the studies did not
cover the teaching strategies teachers used for learners with multiple disabilities. Many of the
Kenyan special schools and units combine learners with multiple disabilities into one group
irrespective of the fact that different multiple disabilities will require different instructional
methods, specialized personnel, different teaching resources, different support services and
different curriculum adaptations among others. For instance, some learners with multiple
disabilities are found in programmes for specific disabilities like in Njia special school for the
Deaf in Meru North in Kenya. The learning needs of learners with multiple disabilities are not
adequately addressed because teachers are trained to teach learners with specific disabilities on
the four major areas of disability namely; hearing, visual, physical and Intellectual disability
consequently, if teachers are posted in special schools where learners have multiple disabilities
other than the category in which they have been trained, they are unable to differentiate
instructions accordingly. According to the Kochung report (2003), learners with multiple
disabilities can follow a specialist curriculum. However the Kochung report (2003) found out

20
that many subject areas of the 8-4-4 curriculum were neither adapted nor a specialist curriculum
prepared for the areas where they were required. Consequently, the instructional needs of
learners with multiple disabilities are not adequately met. According to the National Bureau of
Statistics (2009), the total population in the four counties is 6,286,121 Million. The approximate
number of learners with multiple disabilities is about three hundred. The percentage of learners
with multiple disabilities is 0.05 percent. The Kochung report (2003) found out that there was
lack of reliable statistical data on learners with special needs. It is most likely that this percentage
may be higher due to the following factors namely; lack of accessibility in certain areas, lack of
sensitization regarding learners with disabilities, among others. This state of affairs is detrimental
to learners‟ acquisition of education and denial iof their rights to education. In some special
schools for learners who are visually impaired, a “special class” within the special school has
been set aside for learners who are blind with multiple disabilities. In the view of the fact that
learners with multiple disabilities are combined in our educational settings, their special
educational needs may not be taken into consideration and we shall be denying these learners
their right to education which considers each child‟s unique abilities and learning needs as
clearly stipulated in the Salamanca World Conference on Special needs of 1994. If the
instructional methods, human resources, teaching resources, support services and the curriculum
are not customized to their specific educational needs, then opportunities available for these
learners to attain some level of independence as dictated by their diverse needs will be
foreclosed. This in the long run will make it difficult for these learners to lead an independent
life in their homes and communities thus increasing their dependence on their parents which may
have adverse input on national development. This study seemed to merit investigation in the
view of the fact that Basic education is a right to all children regardless of disability, sex, colour,
race or social status as stipulated in the Universal Declaration of Human Rights of 1948. From
the foregoing statement the study sought to investigate the teaching strategies used by teachers
educating learners with deaf blindness, autism and blindness and cerebral palsy and intellectual
disability in Baringo, Kiambu, Kisumu and Nairobi counties in Kenya.
1.3 Purpose of the Study
The study investigated the teaching strategies used by teachers educating learners with multiple
disabilities in the counties of Baringo, Kiambu, Kisumu and Nairobi in Kenya.

21
1.4 Objectives of the Study
The specific objectives of this study were:
1. To investigate the instructional methods used by the teachers educating learners with
multiple disabilities. (deaf-blind, autism blindness, and cerebral palsy intellectual disability).
2. To find out the curriculum adaptations that had been effected for learners with multiple
disabilities. (deaf-blind, autism blindness and cerebral palsy intellectual disability).
3. To find out the available teaching resources for learners with multiple disabilities. (deaf-
blind, autism blindness, and cerebral palsy intellectual disability).
4. To find out available support services for learners with multiple disabilities. (deaf-blind,
autism blindness, and cerebral palsy intellectual disability).
5. To find out the training needs of teachers educating learners with multiple disabilities. (
deaf-blind, autism blindness , and cerebral palsy intellectual disability).
1.5 Research Questions
1. What instructional methods are used for teaching learners with multiple disabilities?
(deaf- blind, autism blindness and cerebral palsy intellectual
disability)?
2. What curriculum adaptations have been effected for learners with multiple disabilities?
(deaf-blind, autism blindness and cerebral palsy intellectual disability).
3. What are the available teaching resources for learners with multiple disabilities?
(deaf-blind, autism blindness and cerebral palsy intellectual disability).
4. What are the available support services for learners with multiple disabilities?
(deaf-blind, autism blindness, and cerebral palsy intellectual disability).
5. What are the training needs of teachers educating learners with multiple disabilities?
(deaf-blind, autistic blind and cerebral palsy intellectual disability).
1.6 Significance of the Study
The findings of the study will hopefully benefit teachers, learners, parents, members of the
society, policy makers and curriculum developers. To the teachers, it will be of benefit to them

22
because they will understand the appropriate instructional methods for the various multiple
disabilities such as cerebral palsy intellectual disabilities, deaf-blind and autism blindness. For
these learners, their diverse needs will be taken into consideration by all education stakeholders.
To the parents, they will understand the various interventions and learning needs for their
children and work as co- therapists with the schools. The study will hopefully make contribution
to the curriculum developers and policy makers to understand the nature of challenges facing
learners with various multiple disabilities and come up with suitable instructional approaches and
suitable curricula for the various multiple disabilities. The study will also help in sealing
knowledge gaps as it will add new knowledge on the instructional methods for learners with
multiple disabilities.
1.7 Delimitations and Limitations
The study focused on nine major special schools and units where learners with multiple
disabilities are found within the counties of Baringo, Kiambu, Kisumu and Nairobi in Kenya.
The four counties were purposively sampled because they have special schools and units having
learners with deaf-blind, autism blindness and cerebral palsy intellectual disability and are also
accessible. One school and two special units for learners with deaf- blind within the four counties
were used. They included: Kabarnet special school, Maseno Deaf blind unit and Kilimani Deaf
blind unit. Two schools and a special unit where learners with autistic blind could be found
within the four counties included; Kibos school for the blind, Thika primary school for the blind
and Kilimani unit for the visually impaired. Three schools where learners with cerebral palsy
intellectual disability could be found within the four counties included: Joyland Special School,
SA Joy Town Special School and Nile Road Special School. The pitfalls the researcher faced
included: Lack of enough time, lack of adequate information on various multiple disabilities and
lack of enough money to facilitate the researcher and the research assistants in transport and
accommodation within the four counties.

23
1.8 Assumptions
1. Teachers educating learners with multiple disabilities may be facing challenges on the choice
of instructional methods to use for learners with multiply disabilities.
2. That teachers may be facing challenges of an appropriate curriculum for learners with multiple
disabilities.
3. The training level of special education teachers educating learners with multiple disabilities
may be posing challenges on the teaching of learners with multiple disabilities.

24
1.9 Theoretical and Conceptual Framework
1.9.1 Theoretical Framework
The study was based on the instructional approaches and learning theories for learners with
multiple disabilities by Dr. Lilli Nielsen and Dr. Jan Van Dijk. Dr. Lilli Nielsen developed the
theory of “Active learning” maintaining that learners who are visually impaired with multiple
disabilities learn best by being actively involved in their environment without direct adult
intervention. She encourages educators and families to design the environment in such a way that
children are motivated to reach out and explore their surroundings using materials such as a little
room and a resonance board (Nielsen, 1998). Dr. Nielsen‟s little room is a core active learning
environment, providing a resonant, warm, rich and a safe place for children to engage. When
properly populated with acoustically responsive toys, it naturally feeds back to the child for
every movement. The resonance board has a thin plywood panel that vibrates every movement a
child makes on it. There is a folding resonance board with a continuous hinge intended for the
itinerant therapist (Nielsen, 1998). Active learning approach enables the child with multiple
disabilities to learn in the same way that very young children without disabilities learn by doing,
rather than being trained or taught. In this approach the child is provided with opportunities to
learn through active exploration and examination of the environment. Teachers and parents set
up developmentally appropriate environments that encourage the child to touch, move and
explore to the child‟s actions and sounds and interact with the child according to his or her level
of interest and development. Active learning works with even the most significantly delayed and
disabled children (Nielsen, 1998).
Dr. Jan Van Dijk in his approach to working with learners who are deaf-blind, also emphasizes
the importance of establishing a relationship and learning to read the child‟s subtle
communication as a first step. Similarly he uses coactive movement following the child in
interaction. He/she develops anticipation through building structured activities and routines, and
then slightly changes something in the routine to introduce novelty and learning. All along his
goal is to build the child‟s self esteem and confidence in his abilities to do for himself and to
interact with others. Specific communication skills are tied to these experiences as concepts are
developed through experiential learning. (Van Dijk, 2001). Routines and turn taking interactions
in the early stages play a critical role in the child‟s development. For instance, all children

25
participate in basic care giving activities such as bathing, diapering and feeding. Through these
care giving activities that occur daily, the child begins to establish a memory and can anticipate
events. Later on, through participation in simple turn taking games that are done in a routine
way, the child is able to cause the adult to do something pleasurable by taking an action of his
own. Still later in his development, the child is able to take part in simple series of actions that
result in some desired outcomes through more structured routines. Finally the child develops
independence in completing the steps of the routine he has spent time “helping‟ the adult to
complete (Van Dijk, 2001). The implications of these theories to the study is that failure to
provide adequate attention to the quality of education given to learners with special needs, by not
availing the necessary teaching resources, skilled personnel, environmental adaptations,
curriculum adaptations and appropriate support services among others many learners with
Special Needs may fail to obtain meaningful schooling. They will therefore reap minimum
benefits in terms of cognitive development and independence.

26
1.10 Conceptual Framework
Fig 1.1 A diagrammatic representation of the conceptual framework
Support services
Source: Researcher‟s own adaptation
Teaching strategies for Learners with Multiple
Disabilities
Independent variables
Instructional methods
Curriculum adaptations
Teaching resources
Support services
Specialized personnel
Dependent variable
Learning
Expected Outcomes
A happy and a productive life
Independence, functional skills, positive self image, confidence,
communication skills among others.

27
Explanation of the conceptual framework
The study was based on the Active learning theory on instructional and learning theories for
learners with multiple disabilities by Dr Lilli Nielsen and Dr Van Dijk. The theory encourages
educators and families to design an enriched environment for learners with multiple disabilities.
An enriched environment enable learners‟ to explore the surroundings using teaching resources
such as the little room and a resonance board thereby enhancing learning among learners with
multiple disabilities. In this study, an attempt was made to find out how the teaching strategies
influence learning. For instance, if the instructional methods are customized to the specific needs
of learners with multiple disabilities in relation to the level and type of disability learners will be
positively motivated to participate in learning. If the curriculum is adapted to suit the individual
needs of learners, the teaching objectives will be achieved thereby enhancing their academic
performance. If the teaching resources and support services are adequate, learners will improve
in their learning. Independent variables are the factors that explain variation in the dependent
variable (Kombo &Tromp, 2006; Orodho, 2005; Creswell & Plano Clark, 2011). The
independent variables are the causes. In figure 1.1 the teaching strategies are the independent
variables. The teaching strategies include; instructional methods, teaching resources, curriculum
adaptations, support services and trained personnel. The effect of teaching strategies to learners
with multiple disabilities is learning which is the dependent variable. The resultant outcomes will
be independence, functional skills, positive self esteem, positive self concept, self determination,
confidence, cognitive development among others.

28
1.11 OPERATIONAL DEFINITION OF TERMS
Disability: It is a restriction in the ability to perform a normal activity of daily living which
someone of the same age can perform.
Functional /Specialist curriculum: This is a curriculum that caters for the diverse needs of
learners with deaf-blind, autism blindness and cerebral palsy and intellectual disability.
Impairment: It is any loss or abnormality of psychological, physiological or anatomical
structure or function.
Learning: This refers to relatively permanent change in behavior as a result of experience or
practice.
Learners’ Diverse Needs: These are variations of abilities and differences found among any
group of learners in a group.
Multiple disabilities: These are a combination of two or more disabilities for Instance, autism
blindness, deaf blindness, and cerebral palsy intellectual disabilities among others.
Regular school: This refers to the mainstream school which follows the curriculum that is
prepared for the average ability learners.
Special educational needs: These are educational needs which vary from one child to another.
Special Needs Education: This is education which provides appropriate modification in the
curricula, teaching methods, education resources or the learning environment.
Specialized personnel: These are individuals who are specially trained in the specific area to
competently handle learners with deaf blindness, autism blindness and Cerebral palsy intellectual
disability.
Special School: This refers to a school that is built and organized to provide educational services
to learners with one type of disability.
Special Unit: This term describes a classroom that is located in a regular school, but is set aside
for educating learners with a specific type of disability.
“Special class”: This is a class set aside in major special schools for learners with
multiple disabilities.

29
Structured teaching: This is how the classroom environment of learners with deaf blindness,
autism blindness and cerebral palsy intellectual disability is organized by developing appropriate
routines, appropriate activities, appropriate instructional strategies and the way the physical
environment is set up to promote successful behaviour and skill acquisition.
Support services: These are special services offered by other professionals apart from teachers
such as speech therapists, sign language interpreters among others and members of the
communities, environmental adaptations, adaptive computers, alternative communication, or
assistive technology given to learners with deaf-blind, autism blindness and cerebral palsy
intellectual disability.
Teaching: This refers to the interaction in which the learner the materials and the environment
participates.
Teaching strategies: These are the personalized instructional approaches or
methodologies that cater for the individual needs of learners with multiple disabilities.
They will also include; support services, structured teaching, a functional curriculum,
teaching resources and specially trained personnel among others.
Multidisciplinary team: This is a team of experts that is involved in the education programming
of an individual learner with special needs.

30
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This chapter reviews literature related to the study under the following sub headings:
Instructional methods for learners with deaf blindness, autism blindness and cerebral palsy
intellectual disability, curriculum adaptations, teaching resources, support services and training
needs of specialized personnel for learners with multiple disabilities.
2.1 Instructional Methods for Learners with Deaf Blindness
Deaf blindness means simultaneous hearing and visual impairments; the combination of which
causes such severe communication and other developmental and educational needs that cannot
be accommodated in special education programs solely for children with deafness or children
with blindness (Hallahan, Kauffman & Pulllen 2012). The term deaf-blind is used to describe a
heterogeneous group of people who may suffer from varying degrees of visual and hearing
impairment, perhaps combined with learning and physical disabilities which can cause severe
communication, developmental and educational needs. A learner with deaf blindness is a Multi
Sensory Deprived child (MSD) who has been denied the effective use of either his or her distant
senses (Mc Innes & Treffrey, 1982). Children who are deaf-blind miss information that would
normally be received by the use of distance senses of vision and hearing. Distance senses allow
individuals to take in information immediately and are the primary channels through which most
people collect information (Prickett & Welch, 1995). Learners who are deaf-blind may receive
distorted or incomplete information from their senses because of their sensory loss. The “near”
senses of touch, smell and taste do provide some information, but they require the learner to be
in close contact with the item, and these senses may not provide adequate information, for
instance, it can be difficult to gain understanding of large items such as a tree or a mountain or
distant objects like a cloud without the use of distant senses (Heller et al., 2009). Due to the loss
of information from distant senses, children who are deaf- blind receive information that usually
results in delays and difficulties in concept development and skill development. The
development of these areas is further hampered by the lack of incidental learning that occurs
from vision loss.

31
Incidental learning is unplanned learning that results from seeing or engaging in other activities
(Aslop, 2002; Heller et al., 2009). Learners with deaf blindness will need more time to learn
concepts with adults providing ample opportunities and systematic instruction. Learners with
deaf blindness will often have developmental delays in the area of mobility and motor skills. The
loss of vision makes it difficult for young children to monitor their own environment or copy
other people as models. Milestones such as crawling and walking are usually delayed.
Orientation problems can occur due to difficulties in creating a mental map of their surroundings
(Heller et al., 2009; Best et al., 2010). One of the major areas affected by having deaf blindness
is the area of communication. Communication delays and difficulties typically occur usually
resulting in the need for augmentative and alternative communication.
Augmentative and alternative communication can range from the use of gestures and objects to
sign language or electronic communication devices (Heller et al., 2009). When the learner with
deaf blindness has additional impairments such as severe cerebral palsy (CP), the learner‟s
attempts at communication may be easily missed. This difficulty in communication often leads to
secondary behavioural challenges (Holte et al., 2006). The exact characteristics of the learner
who has deaf blindness will depend on the etiology, the severity of the sensory losses and the
individual make up of the child. In addition many learners who are deaf-blind also have
additional disabilities such as cerebral palsy, intellectual disabilities, health impairments and
developmental delays. The teacher will need to learn about the unique characteristic of each
learner with deaf-blind to determine how best to meet his or her needs (Heller et al., 2009;
Mcletchie & Riggio, 1997).
At the University of London Institute of Education in Britain, a research project was carried
out on the curriculum access for learners with deaf-blind by (Porter et al.,1997). The four
objectives of the research project were to gather information on the range of strategies used by
teachers working specifically with pupils who are deaf-blind. To identify how teachers made
decisions about the type of strategy to use with a particular pupil or group of pupils with
reference to modification and adaptations including involvement of pupils and parents in the
process. To examine the effectiveness of different strategies used with the different pupil groups
on the basis of the criteria identified by teachers in their decision making. To collect detailed

32
case study material to illustrate the use of effective strategies with reference to different areas
of the curriculum for each pupil group. The research instrument used was a questionnaire and it
was designed to provide background information to illustrate the context in which they worked
including the nature of setting, levels of staffing, type of curriculum offered, specialist teacher
training, key aspects of the curriculum, how learning was organized and also to identify the
strategies teachers used with learners who were deaf- blind, how they learnt about them and
what influenced their choice (Porter, Miller &Pease,1997).
A total of 82 pupils aged 2 to19 years took part in the study. All had measurable dual sensory
loss. Over half of the participants, 58 % had some useful, functional vision. A fifth of the
pupils, 20%, received no or limited information through the sense of sight and just under a
tenth, 9% received no or limited information through both senses. Only limited information was
provided on the remainder of the samples, 13%. Almost two thirds of the children, 65% attended
schools for children with physical disabilities. Almost a quarter, 23% were in sensory provision
(including specialist Deaf-blind unit and classes). The smallest group, 12% were attending
mainstream schools. All the children were following the national curriculum whereby 11% were
at a key stage commensurate with their age. The rest were working at levels below this, with just
over half the pupils working within or towards key stage one of their curriculums. In total,
teachers identified 145 strategies. Over the course of a week, they used on average thirty
different strategies (Porter et al., 1997). The strategies ranged in specificity and included those
developed with the particular needs of learners with deaf-blind in mind, such as objects of
references, joint action routines and coactive movement, generic strategies adapted to meet the
needs of learners with deaf- blind such as demonstration, speech and role play, strategies
reflecting the culture in which the teacher worked, for example, teachers in sensory settings used
strategies specific to the needs of children with sensory loss, for example signing and auditory
enhancement. Each group of teachers favoured slightly different strategies. Teachers in
mainstream schools generally used demonstration and physical positioning in relation to sound.
They emphasized strategies which focused largely on task presentation and which enabled pupils
to take part in the same curriculum as that provided for the whole class. Teachers in sensory
settings used a mixed approach which combined methods of task presentation, such as imitation,
with the formal system of communication such as signing and speech.

33
Teachers in schools for children with severe learning difficulties or physical disabilities used
strategies which helped the child to succeed through physical intervention. These included
physical prompts, physical positioning in relation to sound and vision, physical contact and in
addition speech. This last group of teachers tended to use fewer strategies Teachers gave a
variety of responses to describe their decision making about the strategy they used. Specialist
training was an indicator. Those with the most specialized training in deaf blindness were best
able to describe what influenced both “within child” factors such as level of sensory impairment,
developmental level, interest and environmental factors including levels of lighting, availability
of space and staffing. A top ten list of effective strategies was identified, four of which included
signing, speech, music prompts and objects of references which were associated with sessions
where teachers met their stated objectives. All effective strategies promoted communication with
the child and provided access at differing levels. The effectiveness of the top ten strategies was
also examined in relation to each group of pupils. For pupils receiving the national curriculum
with access, the most effective strategy was physical positioning being in relation to vision,
sound and speech. For pupils receiving a modified approach to the national curriculum, the most
effective strategies were signing, speech, objects of reference and musical prompts. For pupils
receiving a developmental approach to the national curriculum, the most effective strategies were
choice making, signing and objects of reference. The case studies demonstrated the teachers‟
decision making and how strategies can effectively be used in combination to meet stated
teaching objective or goals (Porter et al., 1997). These case studies reflect the true complexity of
selecting and adapting teaching strategies to meet individual needs. The research findings
highlighted the following: The importance of strategies which were primarily communicative
and which enabled the child to both anticipate an activity and gain a clearer understanding of
what the task demanded. The study found out the need for teachers to have access to a wide
range of specialist strategies especially where they are working with pupils with the most
complex needs whereby there is need for teachers to be able to adapt more generic strategies to
meet the specific needs of an individual pupil. They also found out the need for teachers to have
knowledge of teaching strategies to ensure they are confident in making adaptations in
accordance with the child‟s development and other needs. They also found out the value and
importance for teachers access to information and sharing expertise with others in the field. They

34
also found out the importance of being able to provide intense one to one teaching to maximize
the effectiveness of using strategies for learners with deaf-blind. This study has crucial
information for the present study because the study was looking for the instructional methods for
learners with multiple disabilities. The present study intended to verify whether the same
instructional methods can be applicable in our educational settings.
In America, at the Texas school for the blind and visually impaired a research project was carried
out on the teaching strategies and content modifications for the child with deaf blindness.
Children with deaf blindness have unique educational needs. Although they are deaf the
adaptations needed for their learning style will differ from the child who only has deafness. The
intent of the study was to demonstrate some of the basic differences in educational approaches in
order to address each of these disabilities. To understand what this meant they examined a
variety of issues which were addressed among three different children with disabilities in a
regular pre-schooler class. One born with a severe hearing loss, one born with visual impairment
resulting in activities of 20/600 and one born with a combined severe hearing loss and visual
impairment resulting in activities of 20/600(Moss & Hagood, 1995). A visual acuity of 20/600
means that an eye can see at the distance of 20feet what a normal eye can see at 600feet, or in
other words, an object that a normal eye can see at600 feet away must be brought to within
20feet in order to be discerned by the eye with a visual acuity of 20/600. For the child with
hearing impairment, most of the same teaching strategies used to instruct children who do not
have a disability would be appropriate as the child learns from what he sees and what he does.
Instructions in a large group can be very beneficial for this child because he can prepare for his
response while waiting for his turn. Adaptations for teaching communication and auditory
training goals include small groups or individual instruction. Real experiences should be the
basis of units that are taught, however this child would probably be able to relate storybooks, role
play and discussion to real experience. The teacher may also rely on print, pictures, gestures and
movements to support or give instruction. Issues for the child with hearing impairment include
difficulty with English language structure which can affect the development of reading and
critical thinking skills (Moss & Hagood, 1995).

35
During auditory training the child might try to discriminate between the sound of a pig and cow
makes or point to the appropriate picture of each animal in the old Macdonald song. Speech or
speech reading might focus on the names of farms animals. At the end of the week his class may
visit a working farm for his week long study of farm animals. For the child with visual
impairment the same instruction strategies could be used. However, his learning will take place
primarily through his own actions or experiences and information he receives auditorily. He can
learn many things through group instruction with minimal support (Moss & Hagood, 1995). The
child with deaf blindness requires considerable modifications to teaching content and different
teaching strategies. He cannot learn from what he sees like the deaf child does. He cannot learn
from listening like the blind child does. He learns only by what he does. This means that no
learning is taking place for him while waiting for others to take their turn. For this reason, a
small group or individual instruction becomes more critical. Large group instruction is only
valuable if he or she can be consistently active. This child also may have problems experiencing
new things. Encountering the world without benefit of vision and hearing requires a great deal of
trust. Bonding with the child is critical for the instructor; therefore, it is important to evaluate the
child‟s response to an individual when determining who will be the primary provider of
instruction. He may be withdrawn or passive, content to stay in one place and let the world come
to him. Things often magically appear and disappear before him. Cause and effect are elusive.
People do things to him but not necessarily with him. There is little explanation of events before
they occur. For this reason it is important to make interactions balanced (my turn, your turn) to
encourage him to be responsive. Instruction that is always directive requires no response from
him. Safety is also of critical importance to this child with deaf blindness. Not only must the
environment be made safe for him, but he must feel safe in order to move around on his own. If
he does not, he is likely to stay glued to one spot resisting interaction with his environment and
the people in it. Instruction and support from an orientation and mobility specialist is very
important. She may need to help staff evaluate the environment of hazards and develop travel
routes for the child to use. She may work directly with him to orient him to that environment and
provide training on travel techniques and travel equipment (Moss & Hagood, 1995).
The curriculum focus for the child with deaf blindness will differ from that of the child with only
a single sensory impairment. The deaf education focus may be primarily on using language to

36
code existing concepts. The curriculum focus for a child with visual impairment may be
more oriented towards building concepts and experiences which can provide a firm
cognitive foundation for language. The curriculum focus for a child with deaf blindness should
be on bonding and developing interactions and routines for expanding the frequency and
functions of communication. This child with deaf-blind will not learn about objects or actions
incidentally. He cannot tie together the fragment input he receives without interpretation and
instruction from others. He must be taught to use and accept this instruction. Developing a
communication foundation for learning is a priority. Typically communication is tactile in
nature using signals, objects, gestures and later on sign language or tactile symbols or some
combination of forms. Language for a learner with deafblindness is developed through the use
of routines, calendar systems, and discussion boxes among others. The child with deaf blindness
may first need to be moved co-actively through an activity to know what is expected of him.
After he understands what is expected, this support would be faded to avoid building
prompt dependence because concepts develop so slowly for this child, there should be a
focus on making learning functional (Moss &Hagood,1995). The study has crucial information
for the present study which was investigating on the curriculum adaptations for learners with
deafblindness in the selected counties in Kenya. The present study intended to verify whether the
same curriculum adaptations can be applicable in our educational settings. At the state of
Washington in America a research project was carried out on a new way to set up a program for
the deaf-blind learner. The aim of the study was to come up with a program in order to help
learners with deaf-blind to be fully integrated into the school environment. The programme
would give the students an assortment of communication tools. These tools include American
Sign Language (ASL), English, Braille, touch typing, tactile sign and computer technology. If
the learner with deaf-blind has enough vision to use ASL it may be his first language. He should
also start to learn tactile sign which will become very important if vision loss is progressive. At
the same time he needs to learn English to understand how it relates to and differs from visual
and tactile sign languages (Robinson, 2009). To be fully integrated into our English speaking
society, people with deaf blindness must be able to use English as well as ASL.
The emotional and psychological aspects of learning different modes of communication are as
important as academic training. The learners with deaf blindness should come to view difference

37
as a source of strength rather than a cause of despair. Parents and teachers usually insist that they
should depend solely upon print and visual signing through the first years of school, the child
may fight against learning Braille and tactile sign later on. It is crucial for siblings and parents to
learn ASL and tactile sign so that everyone can communicate with the learner who is deaf-blind.
The earlier the intervention begins, the sooner the child can learn more sophisticated
communication systems (Robinson, 2009). During this phase, a child can be introduced to a
computer that has talking software and a Braille display. Ideally, instruction in ASL, tactile sign
and use of a white cane are well underway by the time the child turns three. He should also be
receiving pre-print, pre- braille and pre-technology training. At this age teaching needs to occur
through real life experiences, just as it does for children with sight and hearing. For example, the
teacher hands the child an object such as a cup of juice. The child drinks the juice. The teacher
signs a sentence, “You drink juice”. Then the teacher presents the same sentence in tactile sign.
Finally, the child types the words on the computer in written English and touches the words on
the Braille display. He also begins to learn the commands for the talking software that eventually
can become his voice. At first, all this instruction is a constant spoon feeding of information, but
the child soon begins to understand him. By age five, a learner who is deaf-blind with this
training will have the same English language skills as his sighted and hearing classmates. He will
use braille, typing and speech output software to communicate. In order for the learner with
deaf-blind to succeed at school, it is vital for the teacher to learn the use of speech access
software, such as Dragon naturally speaking or speech in Microsoft word. When the teacher can
communicate with the child directly, the interpreter eventually can leave the classroom. The
child will be learning on his or her own with the rest of the learners. On the desk in front of him,
the student has a computer with a braille display and talking software. The teacher wears a
microphone. As the teacher speaks, her words appear on the monitor in front of the learner and
on the brailled display. If the student has a question he can raise his hand, type his question on
the computer and have the talking software speak his words. The teacher answers the question by
speaking into microphone which sends her words to the computer. The student reads the
teacher‟s comments on the brailled display and the lesson goes on. To handle classwork the
student reads information in braille. If he has some sight, he uses enlarged print to see pictures or
graphs (Robinson, 2009).

38
He types his work on the computer and e-mails it to the teacher. The teacher uses e-mail to send
her response back to the student. Once the learner with deaf blindness has good touch typing
skills an additional keyboard can be hooked to his computer. The keyboard makes it possible for
the learner with deaf blindness to interact easily with his classmates. This ease of communication
is founded upon the learner‟s knowledge of English. If the learner with deaf blindness knows
only ASL or tactile sign, communication with non- signers is very difficult. Speech software has
little value and the child must depend on an interpreter with him wherever he goes. By learning
all the communication tools (ASL, tactile sign, English, braille, touch typing and technology) the
learner with deaf-blind can enter the world of learning. If every teacher learns to use speech
software, the learner can fully be a part of the school community. To have teachers and others
embrace such learning possibilities calls for a great deal of thought transformation The study
found the importance of teaching learners with deaf-blind all the communication tools and
technology to enable the learner to enter the world of learning. The present study intended to
verify whether the communication tools and technology can be applicable in our educational
settings.
At the California State University in America, a research project named SALUTE (Successful,
Adaptations for Learning to Use Touch Effectively) was carried out on the tactile learning
strategies for children who are deaf- blind. The goal of the project was to identify, develop
and validate tactile instructional strategies for children who have hearing loss and no
functional vision, plus additional cognitive and physical disabilities. Gaps were found on
what was known about tactile methods and also about the use of touch by children who are
deaf-blind. They include, hand over hand guidance which is a common strategy in which an
adult puts his or her hand over a child‟s hand to help the child explore an object, act on an
object or make a gesture or sign. This strategy should be used only when necessary and be
able to keep his or her hand on top of the adult‟s with sensitivity to the child‟s reactions.
Some children dislike having their hands manipulated and feel threatened by the lack of
control. Others can become passive and prompt dependence (Chen, Downing &Rodriguez 2001).
Movement of the hands from one point to another and area of the body ( hand over hand
guidance) may be essential as a strategy for children who have severe physical disabilities
because they often need assistance to manipulate and explore objects. Coactive signing is a

39
type of adapted signing in which an adult physically guides the child to produce signs using
a hand over hand strategy which involves gradually withdrawing the adult‟s hand until the
child‟s fingers touch the surface of the object or texture being explored (Chen et al.,2001).
Body signing is where the signer produces signs on areas of the learner‟s body other than
the hands for instance, the sign of EAT may be placed against the lips. Body signs are based
on manual signs that are symbols or words. Many children who are deaf blind with additional
disabilities have very short attention spans and limited communication play‟‟. The majority of
hearing adults who communicate with them are usually limited in their sign language unless they
have a background of deafness. For these reasons, most children who are deaf- blind who
have additional disabilities are exposed to key word signs rather than to American sign
language or manually coded English . For example, “want play‟‟ are key word signs for “do
you want to play‟‟ Object cues were also used. These are objects or parts of objects used in
activities that are associated with a particular person. They are used to give information, make
requests and provide feedback. Initially object cues should be used during selected activities
so that the child can easily make association between an object and the activity it represents.
For example, a small cardboard container of juice may be used to represent “time for snack”
(Chen et al., 2001).
Touch cues or tactile signals are important communication strategies to use with young children
who are deaf-blind during early stages of communication development. The intended meaning of
a touch cue is derived from the specific context and situation. The use of touch cues should be
consistent. A child will not be able to decipher the meaning of a touch cue if different people
use it for a variety of messages. For example, patting or tapping a child on the shoulder may
express any of the following positive feedback (great job!), a request or directive (sit down),
information ( your turn). The study has crucial information for the present study, because it was
specifically gathering information on the various instructional strategies used by teachers for
learners with deafblindness in special schools and units in four selected counties in Kenya. The
present study intended to verify whether the tactile strategies are applicable in our Kenyan
educational settings.

40
According to Huebner, Nelsen &Bietz (1995), the Deaf blind Manual Alphabet is the best way to
communicate with someone who is deaf-blind. The Deaf blind Manual Alphabet is a method of
spelling out words onto a deaf-blind person's hand. Each letter is denoted by a particular sign or
place on the hand of the learner who is deaf-blind.It is also known as finger-spelling. One can
learn it quickly by doing the following: Stick out your index finger (that's the one next to your
thumb) on your right hand. Fold your other fingers out of the way. Think of this finger as your
pen. You are going to use it to write - not on paper, but on your friends left hand who is deaf-
blind which they will hold out for you. First learn the vowels. They're easy. Just remember the
order A,E,I,O,U. For A, touch the tip of your friend's thumb. For E, Touch the tip of the index
finger. For I, is the middle finger. For O, is the ring finger. For U, is the little finger. For YES,
Just tap twice on your friend's palm. For NO, (or cancelling what you just said) do a rubbing out
movement on your friend's palm. For A, touch the tip of your friend's thumb. For B, bunch the
tips of your fingers and place them on your friend‟s palm. For C, use your index finger to make a
circular movement that starts on the inside of your friend's thumb and ends at the top of his or
her index finger. For D, form a D shape using your thumb and index finger and placing it on
your friend's index finger. For E, touch the tip of the index finger. For F, form an F shape using
your first two fingers together, place across your friend's index finger. For G, clench your fist
and place it on your friend's palm, little finger downside.
For H, lay your open hand across your friend's palm and move it over the fingers and off the
hand. For I, is the middle finger. For J, touch the tip of your friend's middle finger and draw your
finger down to the palm and up the thumb. (Think of this as the letter I with a tail).For K, bend
your index finger and lay the top half of it against your friend's index finger. For L, just lay your
index finger across your friend's palm. For M, lay your first three fingers across your friend's
palm. For N, lay your first two fingers across your friend's palm. For O, is the ring finger. For P,
hold the tip of your friend's index finger between your finger and thumb. For Q, completely
circle the base of your friend's thumb with your thumb and index finger. For R, bend your index
finger and lay it across your friend's palm (Huebner et al., 1995). For S, grasp your friend's little
finger with your index finger. For T, touch the edge of your friend's palm, at the side away from
the thumb. For U, is the little finger. For V, make a V shape with your first two fingers and lay it
on your friend's palm. For W, grasp the upper edge of your friend's fingers, bending your fingers

41
around them. For X, make a cross by laying your index finger over the top of your friend's index
finger. For Y, place your index finger in the joint between your friend's thumb and index finger.
For Z, either: place your finger tips against your friend's palm. Or place the outer edge of your
hand across your friend's palm (Huebner et al., 1995).
An Individualized Education Program (IEP) helps to make short and realistic expectations from
the child. Assessment is the first step. All the IEP‟S teams decision must be based on the
assessment data. The learner must be assessed in all areas of his performance. This is done by
observing the learner across settings carrying out and being involved in various tasks. Interviews
with people associated in the child‟s daily routine also support the assessment process. The
present levels of performance are taken from the child‟s assessment data. It will state clearly
what the child is able to do. This comes from remarks on the child‟s performance in areas such
as brushing, toileting, social interaction, academic areas among others (National Institute of the
Mentally Handicapped (NIMH). The annual goals are then listed in measurable terms. These are
the goals that will be achieved at the end of the academic year. The next step will be developing
short term measurable objectives. It will also explain under what condition the learner will do
what and how long the training period will be.
The role of the teacher is to discuss and formulate goals that are realistic, achievable and
developmentally appropriate for the child. Besides the mother, other professionals are also
involved in the educational process of the child. They include; speech therapist, physiotherapist,
orientation and mobility specialist, vision specialist, orientation and mobility instructor, art and
music therapist, psychologist and a host of others depending upon the needs of the child and the
availability of trained resources in the area. Each member of the multidisciplinary team has a
specific role to play starting with assessment program, evaluation and follow- up action. The
planned and coordinated effort of the entire team helps the learner to move along the educational
program. The teacher remains the main person in contact of the child as well as coordinating the
information between the different professionals involved in the education process. A learner with
deaf blindness will learn best in a real life in the appropriate time, giving the learner the
motivation and reason for learning. The multi sensory approach can be used to teach learners
with deafblindness. This approach makes use of all sensory abilities of the child that is seeing,
touching, smelling and movement. The teacher can also use resourceful persons from the
42
community. They can teach something essential to the learner. Motivation or reward is a very
important part of learning. In designing a task, the teacher will ensure there is appropriate
motivation for the learner. The most successful motivation is to complete the task itself. This is
why many learners are successful at learning to feed themselves. The best rewards are the
learner‟s own pleasure at success, and the teacher‟s pleasure. The teacher will always show
pleasure and the child will gradually learn to recognize this and find it rewarding on its own. A
learner getting dressed may be rewarded with a tickle each time an item is put on (Sense
International, India, 2010; NIMH, 2003; Aslop, 2002& Best et al., 2010). Direct instruction in
daily living areas is often needed for learners who are deaf-blind since incidental learning
cannot occur. Instruction often needs to include eating skills, table etiquette, personal
grooming, clothing care, food preparation, house care, shopping and other areas. Specific
skills may be taught such as judging the amount of food on a spoon by weight,
determining if hair is in place by touch, labeling and storing clothes so that they will match,
labeling cans of food to determine what they are, learning how to fold money to
determine the denominations of the bills for shopping and others (Heller et al.,2009).
Tadoma is tactile lip reading or tactile speech reading. Tadoma is named after the two children to
whom it was taught, Winthrop „Tad‟ Chapman and “Oma” Simpson. Tadoma is a skill used by
the congenitally deaf-blind person. The listener will place his or her hand on the cheek of the
speaker with the thumb resting on the throat, such that he or she feels the vibrations and the
mouth movements so that he or she is able to follow the conversation (NIMH, 2003).
Augmentative communication systems such as objects of reference and pointing are used to
support a learner who is deaf-blind in recalling events. For instance, a teacher can show a real
plate or a model of a plate to indicate lunch time (Chen, 1995,; Aslop, 2002).We use any means
to communicate with a learner who is deaf- blind, adapted to the senses he/she can use. The
different modes of communication reflect the person‟s capacities, and the development of the
learner; that is both cognitive potentials of the learner and the senses he can use in different
situations. With a learner who is deaf-blind one expands from objects to tactile drawings and
sometimes to Braille with learners who are deaf-blind with residual vision. A teacher can move
from objects, to drawings or pictograms and writing. In addition, a teacher often present signs
both tactually and visually depending on the situation and development of the child (Chen, 1995:
Aslop, 2002). Activity based scheduling is another teaching strategy for the learners with deaf-
43
blind that incorporates tasks into the timetable that will actually help the child to learn a set of
skills to perform the particular task (NIMH, 2003). Individuals who are deaf-blind and have a
cognitive disability may not effectively communicate their desires and choices of what to eat
even when provided with the opportunity to do so, because of their frequently limited
communication skills. Choosing what to eat should take place where the learner eats. The
boundary in which the choice making activity takes place should be defined through the use of
appropriate aids and cues. Providing boundaries minimizes the visual motor and cognitive
requirements of orienting and reaching (Campbell, 1987).
In Africa, studies were carried out on learners who are deaf with multiple disabilities in
developing countries such as Kenya, Malawi, Cameroon, Nigeria, Uganda, and Somalia among
others (Shettle, 2004). In Kenya the researcher, found that at the Njia Special School in Maua,
Kenya, which is a school for both special education and deaf education they had some learners
who were 'just Deaf' as well as some who had multiple disabilities. They also found that the
Kaaga School for the Deaf in Meru, Kenya, which is a 'Deaf school‟ also had some learners who
were deaf with multiple disabilities but it is not specifically focused on the education of such
children”. The study found that no progress had been carried out on how to deal with learners
who are deaf with multiple disabilities even though they were found in the various special
schools for deaf children (Shettle, 2004). The study did not show the teaching strategies for
learners who were deaf with multiple disabilities. This study sought to fill the gaps by
investigating the instructional methods used by teachers for learners with deaf blindness in some
selected special schools and units in Baringo, Kiambu, Kisumu and Nairobi in Kenya.
2.1.1 Curriculum Adaptations for Learners with Deaf blindness
Curriculum adaptation refers to the modification of the regular curriculum to suit individual
learners with special needs (Lewis, 1981). Curriculum modification, as described by Koga and
Hall (2004), results in “modified contents, instructions, or learning outcomes for diverse students
needs” (pg.2.) A curriculum for learners who are deaf-blind need to reach the goal of a child
towards personal adequacy, social competence and economic independence and more
significantly make his life a lot happier and healthier. The content of the curriculum is very much
determined by the individual needs of the learner who is deaf-blind. When a curriculum

44
approach takes into account the pupils current individual needs and his future needs and is
designed to meet his needs, it is known as a functional curriculum. The instruction in the
functional curriculum focuses on the individual needs of the child as compared to the
expectations from him in his immediate family and community development. The functional
curriculum uses the learner‟s interest and strengths as the basis for planning intervention
strategies. The curriculum framework begins with the child, family members and other
significant others of the child‟s life who play a role in the intervention programme for the learner
with deaf blindness.
The curriculum addresses the needs of the learner with deaf blindness in the following areas:
Independent living activities; in the early stages the parents and the teacher will do the activities
together coactively, later the learner learns to do it by himself or herself. This area includes:
Training in cooking, washing clothes, brushing teeth, orientation and mobility among others and
maintaining the learner‟s own belongings (Ellis, 1986; Sense International India, 2010& Aslop,
2002). The FIELA Curriculum was designed by Dr. Lilli Nielsen, a pioneer in learning
techniques for teaching learners with multiple disabilities and creator of the learning approach
called Active Learning. FIELA is made from words flexible, individual, enriched, level and
appropriate (Nielsen, 1998).The premise of Active Learning is that all children learn through
their own actions, on their own initiative. According to Nielsen, if given the opportunity to learn
from his own active exploration and examination, the child will achieve skills that become part
of his personality, and so are natural for him to use in interaction with others, and for fulfillment
of his own needs, and will gradually make him ready to develop to be as independent as possible.
The FIELA Curriculum requires: Precise observation of all areas of a child‟s development level
in all areas and the structuring of the child‟s learning activities based on the child‟s own needs
and preferences. The educator‟s role is to provide enriched learning environments, respect the
child‟s need for sufficient time and quietness for learning, and to be ready to share the child‟s
experience when the child is ready to share it (Nielsen, 1998). Kochung report, (2003),
established that the 8-4-4 curriculum does not take care of all learners with Special Educational
Needs (SEN). The curriculum was noted to be rather rigid, demanding and with the same
expectations for all learners. The Kochung Report (2003) noted that this arrangement
disadvantaged learners with SNE since there are some learners such as the gifted and talented

45
who can complete the curriculum in less than the specified time while others may need a long
period to do so.
Koech Report, (1999) posits that the Kenyan school curriculum is inappropriate in that there is
lack of clear policy guidelines and legal status on special needs provisions, inadequate teaching
facilities, equipment and services for learners with disabilities and inadequate teachers who use
rigid teaching approaches which may only benefit the average learners among others. According
to the Policy on Special needs, a document launched by the Ministry of Education in 2010, the
curriculum materials for children with special needs of all categories especially the severely
handicapped, are inadequate at all levels of education. The curriculum also lacks flexibility in
terms of time, learning resources, methodology, and modes of access, presentation and content.
There is lack of sufficient trained personnel for curriculum development. In addition, there are no
clear staffing norms and recommendation on pupil teacher ratios in institutions and programs for
special needs education. According to KIE (1987), learners with multiple disabilities will require
a specialized curriculum. A specialized curriculum refers to the curriculum where the regular
curriculum is exhaustively and significantly modified to suit the target group of children.
Severity of the disability is the primary determinant of whether or not to come up with a
specialized curriculum. The modifications include: a rationale for modification, mode of
presentation of materials, modifications of the teaching methodologies and emphasis on the use
of an Individualized Education Plan. About forty to 60% modifications or adaptations is on the
content of the regular curriculum and the use of specialized materials and equipment.
Modifications of the regular curriculum require collaboration on the part of the special educator,
the regular educator, and other specialists involved in the learner‟s program. Community based
instruction is also an important characteristic of educational programming, particularly as
learners grow older and where increasing time is spent in the community. School to work
transition planning and working towards job placement in integrated competitive setting are
important to a learner‟s success and the long – range of his or her life (Rainforth & Macdonald,
1997). The study sought to investigate the curriculum adaptations that have been effected for
learners with deaf blindness in four selected counties in Kenya.

46
2.1.2 Teaching Resources and Support Services for Learners with Deaf Blindness
For learners with deaf blindness, it is desirable to provide educational services in a traditional
manner. This is a model where skills traditionally taught by one discipline are shared with others
who work directly with the child (Rain forth & York, 1997), According to Campbell (1987),
transdisciplinary teams designate a “primary programmer” who implements the intervention
programmes in collaboration with various specialists who have designed them on the basis of
specialized assessments. The transdisciplinary team model is characterized by sharing
information and skills across discipline-specific boundaries. This approach uses an indirect or
integrative approach where one or two persons (usually the teacher) act as the primary
programme provider, and other team members act as consultants (Snell &Janney, 2000). This
model minimizes the number of people who will work with a child on a daily basis and provide
opportunities for cross-training of staff. It is important to consider programmes and services that
will enhance probabilities for the learner who is deaf-blind to lead a happy and a productive life
(Miles & Riggio, 1999). Related services are of great importance and the appropriate therapists
such as speech and language, occupational, physical, behavioural and recreational therapists
among others need to work closely with the classroom teachers and the parents. Other support
services include: Orientation and mobility, adapted physical education, vocational training,
computer technology training, behavioural consultation, audiology, health services among
others. Orientation and mobility helps deaf-blind learner to know where he is in space and where
he wants to go (Martinez & Moss, 1998). Learners with sensory loss may use several
assistive devices to help with daily living needs. For instance, learners with a hearing loss
may use close captioned television,(Closed captioning allows persons with hearing disabilities to
have access to television programming by displaying the audio portion of a television
programme as text on the television screen), vibrating or flashing alarm clocks or flashing
door bells. Hearing ear dogs are also available. Learners with visual impairment may use
special money readers, special devices that buzz when a beverage is near the top of the
glass among others (Heller et al.,2009).
Wehman & Parent (1997), identified several categories of assistive technology identified and
they include: mobility (wheelchairs, lifts, adaptive driving controls, scooters, laser canes, seating
and positioning (assistance in choosing and using a wheelchair), computers (environmental

47
control units, word processors, software keyboard).Toys and games software and switch operated
toys) activities on daily living feeders, lifts, memory books, watch, alarms, communication
(talking toys, reading systems and talking boards). Learners with severe and multiple disabilities
can benefit from any one or more of these assistive devices or activities. For those who are
unable to use speech and need an additional communication mode, augmentative communication
can be used. It involves adapting existing vocal or gestural abilities into meaningful
communication, teaching manual signing such as American Sign Language (ASL), static
symbols or icons(such as Bliss symbols) using manual or electronic communication devices such
as electric communication boards picture cues or synthetic speech(artificial human speech in a
computer. Orientation and mobility skills are also needed for learners who are deafblind.
Orientation refers to the process of using one‟s senses to determine one‟s position in
relation to other objects in the environment and mobility refers to the ability to move
about in one‟s environment (Emerson & Corn , 2006). Orientation and mobility instructors
teach the learner the skills that will enable them to safely and independently move around
their environments. Mobility aids may be needed such as a specially designed cane, dog
guides, electronic travel devices or a sighted guide. Some learners with additional
physical disabilities will learn mobility techniques using their wheel chair (Emerson & Corn,
2006).
Learners with deafblindness may exhibit stereotypic behaviours such as body rocking &
eye rubbing that occur in excessive quantity, frequency and intensity. A careful assessment is
needed to determine the extent to which these behaviours interfere with learning, inhibiting
social interaction, or cause physical damage to the learner. The teacher may permit
stereotypic behaviours to occur in certain locations (such as rocking in a rocking chair) and
inhibit others ( such as eye rubbing). Stereotypic behaviour may be managed in any number
of ways from simple verbal reminders to the implementation of a behaviour plan that is
agreed on by the educational team to ensure consistent implementation across settings
(Emerson & Corn, 2006). Adapted physical education is a diversified programme of activities
specially designed for an individual who meets eligibility criteria for special education or related
services and is not able to safely participate successfully in the regular physical education

48
programme. The modifications in the adapted physical education include; changing rules,
equipment and time limit (Hardman, Drew & Egan, 2005).
According to the New Hampshire Association of the Blind in the United Kingdom, the services
offered to the learners with deaf blindness include; deaf and hard of hearing services,
counselling, information and referral peer support, personal care attendants, sign language
interpreters services, skills training, transportation services and multisensory interventions
through consultation. There are also consumer advocacy groups that unite people with
disabilities and their allies to work towards better accessibility and quality of life. Other support
services include a support service provider who accompanies the deaf-blind consumer on errands
at community events. Support personnel and service animals provide access to communication
interaction and environmental sights and sounds to a person who is deaf-blind (Archibold, 1994).
Implants are increasingly being used for individuals who cannot benefit from the use of hearing
aids. The success of implantation is very individual. Different types of implants serve different
individual needs and functions: Cochlear implant is a surgically implanted electronic device that
provides a sense of sound to a person who is profoundly deaf or severely hard of hearing. Middle
ear implants are for individuals with conductive or mixed hearing loss; they are microphones that
transmit sound from the middle to the inner ear. Bone-anchored implants are for a variety of
hearing losses; they conduct sound from an implant in the skull behind the ear to the inner ear.
Auditory brain implants are for individuals who don‟t have adequate auditory nerves; they are
electrodes applied to the brain stem that provide electrical signals leading to a sense of hearing
and resulting in support for lip-reading (Vaughn Bos &Schum,2007). A Sensory Room is a place
where children with special needs can explore and develop their senses and skills. The multi-
sensory room can have many different features ranging from soft play areas, padded floors and
walls and interactive equipment which make dramatic changes to the sensory room environment
using sound, lighting and fragrance (Hopcroft, 2010). A multisensory room can engage children
who can learn through play. From following bright lights, shapes and patterns with their eyes to
press buttons to make the sensory room change colour or even change colour to music. Due to
the flexible functionality of the multisensory room, it can also be used to calm and de-stress.
Children become interested in their environment. The overactive can be calmed and the inactive
become interested. The partially sighted can see the vivid moving colours. Those mobile, can

49
chase the slowly moving images. The whole room can change colour by applying pressure to
simple switches or pressure pads. Colours can move or change simply by making a noise and for
those with severe special needs the sensory room can be set to automatically change programme,
giving a constantly changing and interesting environment that is probably the most pleasant
environment they have ever experienced even if all they can do is lay and enjoy. A hydrotherapy
pool may be used to maintain health in children with special needs. Hydrotherapy pools help
children with special needs to relax and in doing so may result in tension being released from
muscles, alleviate pain and calm the nervous system. A Hydrotherapy pool is an ideal concept
for children with special needs. Depending on the level of interaction required, hydrotherapy
pools can contain a number of features to stimulate the senses (Hopcroft, 2010).
2.1.3 Environmental Adaptations required for Learners with Deaf blindness
Several strategies may need to be used to optimize the visual functioning of a learner with a
visual impairment. These include; arranging the environment to optimize the visual characteristic
of objects, teaching the use of optical devices and training the use of
residualvision(Corn,Anderson,Bachofer,Jose&Perez(2003);Wolfe,Sacks,Corn,Erin,Huebner &
Lewis (2002). There are five major environmental dimensions that can be modified to assist the
learner with a visual impairment to access his or her environment through the use of vision:
colour, contrast, time, illumination and space (Corn et al., 2003). Teachers should take into
account the colour of items being used in the classroom. Some learners with low vision may be
able to see bright coloured items with greater ease than other colours while other learners with
low vision may not see bright colours clearly. The use of contrast should be considered when
teaching a learner with visual impairment since contrast can make an item easier to visually
discriminate for instance, black print on white or yellow paper may assist the learner visually.
Some learners with visual impairments will perform better if given time to respond. That is
because learners with visual impairment often need more time to access the item being presented
and explore it in order to identify it (Easter brooks & Baker, 2004).
Learners may benefit from the use of additional light or reduced writing in order to see items for
instance, some learners with retinal detachment (where part of the retina detaches from the back
of the eye) may benefit from increased illumination. Reduced lighting and lighting from behind

50
the learner may be needed with learners who still have cataracts to reduce glare and promote
maximum visual functioning. Some learners with visual impairment can perform better if there
are changes in space, specifically how they are positioned in the classroom, for instance, a
learner with poor acuity may perform better in the front row of the classroom (Corn et al., 2003).
Learners with a peripheral field loss (tunnel vision) may be better situated if seated in the back of
the room where more of the classroom can be seen. Some learners will also benefit from material
enlarged for instance, large print or large items or using an optical device that enlarges items
when looked through however, enlarging items may be more difficult for learners with reduced
peripheral field of vision since an enlarged item may not fit in the learner‟s visual field (Corn et
al., 2003). A second major adaptation that assists learners to access their environment with their
remaining vision is the use of optical devices such as magnifiers and telescopes that enlarge
normal sized items and print. Some optical devices minimize items in order to better visualize
them. Learners with low vision may be trained to more efficiently use their vision through vision
training programs. These programs are designed to use the systematic presentation of stimuli and
instruction to optimize a learners visual functioning. The vision teacher along with the rest of the
education team will typically teach the learner to use his or her vision to the maximum extent
possible. Learners who are unable to use their vision functionally will need to use their sense of
touch and other senses. Learners will be encouraged to manipulate items and discriminate items
on the basis of various features. Discrimination usually starts with gross, for instance differences
in shape and texture and size and progress to finer discriminations. As the learner gains mastery
over using the sense of touch the teacher will need to modify classroom materials for instance
use of actual items models or tactile graphics to allow the learner to use this sense to enhance his
or her learning (Con et al., 2003). Learners with hearing impairments may benefit from several
environmental and instructional modifications as well as auditory devices.
Environmental and instructional modifications include: Modifications to the auditory
environment and use of listening devices and modifications to the visual environment and
modifications of materials and instruction. Typical classrooms can be very noisy places because
of background noise and poor acoustics. To hear the teachers voice clearly, hearing children
require a signal-to-noise(S/N ratio + 10, where teachers voice is at least 10dB (decibels) louder
than the noise. Children with hearing losses require an S/N of at least +15 (Seep, Glosemeyer,

51
Hulce, Linn & Aytar, 2000). With a personal frequency modulation unit (assistive listening
device), the teacher wears a wireless microphone, and the student wears a wireless receiver
incorporated with a hearing aid. The microphone amplifies the teacher‟s voice 12-15dB above
the classroom noise and is not affected by distance (Vaughn, Bos &Schumm, 2007). To help
improve acoustics, the classroom may be modified with carpets, drapes and other sound
absorbing materials on the walls and floor. The classroom should have lower ceiling with sound
absorbing tiles. Double-pane windows and solid floors reduce reverberation as well. The learner
should be seated away from noisy equipment such as plumbing, air conditioners and over head
projectors, as well as from windows where traffic noise is evident (Seep et al., 2000).
According to Lane, Hoffmeister and Bahan (1996), learners who are deaf and hard of hearing are
visual learners even those who are benefitting from their listening devices. For this reason, it is
important to manage the visual environment as it is to manage the auditory environment. Seating
arrangement should be considered carefully when a learner has a hearing loss to enable learners
to see the teacher as well as classmates. This will allow for speech reading (Stivalet, 1998). The
teacher should be alert for signs of fatigue in the learner since attending to the interpreter, using
residue hearing and attending to the material can be tiring. A very important modification to the
auditory environment is the use of hearing aids, cochlear implants and other listening devices
that amplify sound (Amlani, Rakerd & Punch, 2006). The individual needs of each learner with
deaf blindness will need to be assessed to determine the best way to arrange the environment.
Learners who are deaf-blind will typically need some combination of the visual and hearing
modifications to meet their needs (Heller et al., 2009). The study sought to find out the available
teaching resources and support services for learners with deafblindness in selected special
schools and units in Baringo, Kiambu, Kisumu and Nairobi counties in Kenya.
2.2 Instructional Methods for Learners with Autism and Blindness
A learner who has autism and blindness is a child who has a combination of both autism and
visual impairment. The Diagnostic and Statistical Manual of Mental Disorders (fourth edition)
(DSM- IV) (American Psychiatric Association (APA), 1994) defines autism as a disability
„‟Characterized by severe and pervasive impairment in several areas of development: reciprocal
social interaction skills, communication skills or the presence of stereotyped behaviour, interests

52
and abilities‟‟. Individuals with this disability have considerable disability in interacting with
others socially and in communicating verbally. They also often engage in self stimulating
behaviour and can have a very limited number of routines and interests. Children with visual
impairment are learners with problems in the structure and functioning of the eye. Visual
problems range from total blindness to only slight visual impairment. Children who are visually
impaired are classified into two main categories and they include children who are blind and
children with low vision (Hallahan & Kauffman, 1997). Children who are blind have either
totally lost their sense of vision or those who are only able to perceive light. The second category
includes individuals who are able to tell the difference between darkness and light.
Educationally, children who are blind are those who learn through Braille without the use of
vision, although they may perceive light, which is an advantage and can be used for orientation
and mobility (Hallahan & Kauffman, 1997). Educators give an educational definition and say
that anybody with low vision is still severely visually impaired after correction, but may increase
visual functioning through the use of optical aids, environment modification or low vision
techniques (Corn &Koenig, 2002).
In America, a case study was carried out on a pre-schooler with autism and blindness in
order to unlock the mystery of communication. It was presented as a poster session at the
2003 Florida Association of Speech Language Pathologists and Audiologists Convention
(FLASA). The objective of the study was to describe how Augmentative Alternative
Communication (AAC) strategies were used with this learner. The rationale for teaching both
AAC strategies is provided along with AAC objectives, directions for implementation,
feedback for correct and incorrect responses, list of needed materials, when strategies should
be implemented and by whom. The case study was carried out with a child named Paul who was
4 years old, and non- speaking. He had been diagnosed with autism spectrum disorders and
congenital blindness. Paul began pre- school at 2 years, 5 months of age. His level of autism
was assessed to be in the severely autistic range based on the Childhood Autism Rating
Scale (CARS). He exhibited delays across all developmental milestones and atypical
behaviours such as self stimulatory behaviours (i.e. flopping his wrists or flipping objects for
hours if interrupted ),hypersensitivity to certain textures and lack of initiation of
communication. He screeched in protest and actively resisted when transitioning to non preferred

53
activities. He demonstrated immediate and delayed echolalia of environmental sounds and
speech. He appeared to make no distinction between speech sounds versus non speech sounds.
He walked with stiff legs and small guarded steps at a slow pace due to his blindness. To help
Paul and with the help of a vision specialist and lots of creativity the pre-school educational
team was able to adapt many traditional visual support strategies used with children who
have autism and normal vision into tactile support systems for our student who was blind. The
goal was to teach the child to independently use speech to make requests since the child had
not yet attached meaning to the words he echoed. The child was taught sign language thus he
learned that words had meaning. He was able to attach meaning to words and use single words to
make simple requests. Two treatment methods were used in the study. The first treatment method
was the use of object symbols. The objects were glued to card board squares so the child could
distinguish these objects as tactile communication symbols. It became apparent very quickly that
this system would not be successful due to the child‟s self - stimulating behaviour of flipping
objects with his hand. He was not able to learn to use the communication symbols because his
self stimulating behaviour of flipping objects interfered with his ability to recognize the object
symbols. Individuals with blindness from birth do not understand gestures such as waving or
sign language because they have no concept of sight or that other people have sight to receive the
gesture or sign. It is therefore difficult to teach sign language for this reason and thus the best
way to approach it would be to teach him to use two handed signs (Lilienthal, 2009).
A second treatment method was designed to teach Paul, by the use of two handed sign language.
By using two handed sign language paired with speech the method proved successful. In the two
handed sign language method signs are produced using two hands touching each other and
the child would receive tactile feed back when he produced a sign. Single handed signs
provide little tactile feedback and may require more sophisticated fine motor skills than
two handed signs. Teaching began with hand over hand assistance to produce a modified sign to
request a “goldfish cracker” during snack time (Lilienthal, 2009). Goldfish cracker was chosen
as the first item to request because it was highly motivating for Paul. The sign for “Goldfish
cracker” was actually an approximation of the American Sign Language sign for “fish”. The
sign was modified so Paul would hold the palms of both hands together and move them
forward like a swimming fish. Paul was reinforced immediately after each production of the sign

54
with a goldfish cracker. Once he learned how to produce the sign independently to request gold
fish crackers it was time to teach him to discriminate between two different signs. He now had a
way to communicate when he wanted more goldfish crackers. The American Sign Language sign
for “cookie” was introduced. This was another two handed sign to provide tactile feedback. This
sign was highly motivating for him and was taught during snack time. Paul was immediately
reinforced after each production of the sign with a piece of a cookie and he soon learned to
produce the sign for cookie. Two more words; a push on the swing and listening to music
adapted two handed signs were taught to request highly motivating actions. Paul quickly learned
these signs and was able to independently produce the signs to make requests. To promote
generalization of these skills to the home environment, family members, vision specialist and
baby sitter were trained on the use of the two handed signs. Everyone who worked with Paul at
school and home were given pictures of how to produce the adapted signs so, everyone who
worked with Paul would facilitate the correct production of each sign. Paul began to
independently produce signs to request these four highly desired items or actions.. Paul was
taught to say the word associated with the sign. He had excellent verbal imitation skills so he
was given a phonemic cue ( saying the first sound of the word) in a soft voice and as he
began to imitate the word was completed. As soon as he finished saying the word in imitation
his behaviour was reinforced with the desired item or action. Within two months time, Paul
began to independently and consistently use single words to communicate for these four desired
items and actions and no longer used his signs. The brief use of sign language unlocked the
mystery of communication for Paul and he rapidly learned to generalize this skill to other words.
He was now using single words to communicate his basic wants and he understood that words
had meaning and power (Lilienthal, 2009). The present study intended to verify whether the
same instructional methods can be applicable in our Kenyan educational settings.
In America, as published in the Journal of Autism and Developmental Disorders a case
study was carried out on training a learner with autistic blind to communicate through signs.
The study was done on a 10 year old girl using tactile kinesthetic and auditory modalities. The
visual, auditory and kinesthetic learning styles (VAK) uses the three main sensory receivers:
visual, auditory and kinesthetic (movement) to determine the dominant learning style. According
to VAK one or two of these receiving styles is normally dominant. This dominant style defines

55
the best way for a leaner to learn new information by filtering what is to be learned. The
learner in the study had the auditory and kinesthetic tactile receivers as the most dominant
receivers thus auditory and kinesthetic activities were included in her mode of learning.
The style was integrated into the learning environment by beginning new material with a
brief explanation of what was coming and concluding with a summary of what had been
covered. The Socratic method of teaching whereby learners are questioned to draw as
much information from them was incorporated and then the knowledge gaps were filled by
the teachers expertise (Konstanareas, 1982). Auditory activities such as brain storming among
others were incorporated and also plenty of time was left to debrief activities. Debrief activities
allowed the learner to make connections of what she had learned and how it applied to their
situation. Kinesthetic learning activities were included in the learner‟s style of learning. Since
learners who are kinesthetic learners tend to lose connection if there is little or no external
movement, music was incorporated with the learning activities and also frequent stretch breaks
(brain breaks) were provided (Konstanareas,1982). The present study intended to verify whether
the same instructional methods can be applicable in our Kenyan educational settings.
In America, a research study was carried at the National Federation of the Blind (NFB) Jernigan
Institute in Baltimore on the teaching of skills of blindness to children with additional
disabilities. The researcher found that teachers have to choose appropriate methods for teaching
to meet diverse needs of learners who are autistic blind. Their learning needs should be
supported systematically. She came up with a plan of educating learners with autism and
blindness. In phase one, she provided all the supports commonly found in the classrooms of
sighted learners with autism. Some of the supports include: visual aids, visual schedules, routines
and touch cues among others. She developed a schedule for the class that was consistent as
possible. The schedule was translated into a tactile form. Since the learners could not yet read
their names, each learner was assigned a personal tactile symbol. The symbol appeared on all of
the learners belongings next to their name in braille. Positive behaviour supports was
incorporated as part of the classroom management plan. The classroom was free from clutter and
the learning areas in the room were well, defined so the learners could easily predict the
activities that would take place in each area (Shaheen, 2009). In phase two, everything that
appeared in the classroom in print also appeared in braille. Braille books were put on the shelves

56
in the reading corner. Every surface in the room was adorned with a braille label or a tactile
symbol. Braille writers were brought into the room and placed where the learners could reach
them easily. Braille basic concepts were taught. The stories were brailed and illustrated with
homemade tactile graphics which often included real objects. In order to provide more learning
opportunities, braille was incorporated into other parts of the day. Each of the learners had
reward systems that incorporated a token board. The board had six tactile circles, set up like a
braille cell into two columns of three. Each time the learner earned token for appropriate
behavior she or he placed in one of the circles. The learners counted their tokens according to the
numbering system for the braille dots (Shaheen, 2009).
Other phases of the plan included acquiring orientation and mobility assessments of the students,
teaching appropriate social skills, teaching the beginner abacus and other basic math skills and
teaching simple social studies concepts. Adjustments were made as problems surfaced. They
collaborated with related services providers, administrators thus the plan became more refined
and effective. All learners possess the capacity to learn and learners with multiple disabilities are
no exception. It is the job of the educator to find the proper strategy to teach a learner; it is not
the job of the learner to conform to traditional methodology (Shaheen, 2009). The present study
was crucial to this study because the researcher was finding out the instructional strategies for
learners with autism blindness in four selected counties in Kenya. The present study intended to
verify whether the same instructional methods can be applicable in our educational settings. The
study sought to find out the instructional methods used by teachers educating learners with
autism blindness in selected special schools and units in Baringo, Kiambu, Kisumu and Nairobi
counties in Kenya.
2.2.1 Curriculum Adaptations for Learners with Autism blindness
According to Hatlen (1996), learners with visual impairment including those with multiple
disabilities will require an expanded core curriculum. The core curriculum consists of knowledge
and skills related to academic subjects. The expanded core curriculum incorporates the basic
subjects and adds the following; compensatory or functional academic skills including
communication modes, orientation and mobility social interaction, independent living skills,
recreation and leisure skills, career education, use of assistive technology and visual

57
efficiency skills. Compensatory skills are those needed by the visually impaired learners in order
to access all areas of the core curriculum. Functional skills refers to the skills that the learners
with multiple disabilities learn that provide them with the opportunity to work, play, socialize
and take care of personal needs to the highest level possible. Communication needs will vary,
depending on degree of functional vision, effects of additional disabilities and the task to be
done. Learners may use Braille, large print, print with the use of optical devices, regular
print, tactile symbols, a calendar system, sign language or recorded materials to communicate
(Hatlen,1996).
Orientation and mobility is a vital area of learning. Learners will need to learn about themselves
and the environment in which they move from basic body image to independent travel in rural
areas and busy cities. The existing core curriculum does not include provision for this
instruction. Social skills, career education and leisure skills must be carefully, consciously, and
sequentially taught to the visually impaired learners with multiple disabilities. This is because
they are not incidentally learnt (Hatlen, 1996). A curriculum for learners with autism and
blindness should help the learner to reach levels of performance that are appropriate and planned
for him (Shaheen, 2009). The study sought to find out the curriculum adaptations that have been
effected for learners with autism blindness in the counties of Baringo, Kiambu, Kisumu and
Nairobi in Kenya.
2.2.2 Teaching Resources and Support Services for Learners with
Autism Blindness
According to Boyce & Hammond (1996), learners who are autistic blind who exhibit needs in
the social emotional area must have programmes that address the full range of their cognitive,
emotional and social developments. Learners with social emotional needs must also be
encouraged to become competent and self- confident learners. In terms of early intervention and
the setting of appropriate and positive expectations, these programmes may actually be
preventative in nature. Programmes may include social skills programmes and conflict resolution
programmes. Learners who are autistic blind may have speech impairment and they need early
identification through a systematic approach. The persistent nature of speech impairments (e.g.
articulation or phonological disorder) requires access to services for learners at all grade levels.

58
Some learners with speech impairment have associated difficulties in other areas of development
(reading and writing, learning, intellectual, social emotional, behavioural and sensory. The close
relationships among phonology, language and literacy development are central to the classroom
focus of speech intervention and support services (Boyce & Hammond, 1996).
Learners who are autistic blind also require support due to visual impairment. The level of
support depends on the severity of the eye condition and also the results of a functional vision or
tactile assessment that is conducted by the Vision Program Assessment team. They are taught to
read and write braille and also orientation and mobility by the various specialists. Learners who
are visually impaired rely heavily on adaptive technology to access the curriculum. For example,
a laptop computer with a screen enlargement programme or speech out programme, a braille
embosser (printer), a scanner, a portable braille note taking device and a global position system.
Advances in adaptive technology have helped learners who are visually impaired access the
curriculum independently and quickly (Boyce & Hammond, 1996). Most of the diets used to
treat children with autism were originally constructed for children with attention deficit disorder
and hyperactivity. The diets were adapted for the treatment of autism by some dieticians who
believe that it is a lack of tolerance for certain food substances that lead a child with autism to
food selectivity and idiosyncratic eating habits (Richman, 2005). Four things should be removed
from a child‟s diet who has autism, these include; gluten, casein, monosodium glutamate and
aspartame (Breton, 2001). Learners who are autistic will require auditory training. In auditory
training, an audiogram identifies frequencies to which the child with autism is hypersensitive.
Once these frequencies are determined, they are eliminated from an audio recording that the
child listens to through headphones during therapy sessions. Advocates of auditory training
speculate that hypersensitive hearing causes aggression, hinders children from interacting with
others and impairs their ability to attend to instructional situation (Grandin, 1995). Sensory
integration is usually given by occupational therapists to learners with autism. According to
Grandin (1995), sensory integration is the neurological process that organizes sensation from
ones own body and from the environment and makes it possible to use the body effectively
within the environment. Sensory integration is often recommended for learners who engage in
inappropriate responses to sensory stimuli for instance, tapping and body rocking. According to
Richman (2005), fine arts therapies have been shown to be calming, and have helped learners

59
with motor coordination difficulties and emotional issues. Such therapies can also be effective in
reducing difficult behaviours from autistic learners on a short term basis. Hydrotherapy is also
used with learners who are autistic. For learners with autism, wet heat helps relieve pain,
improves circulation, and promotes relaxation (Richman, 2005; Hopcroft, 2010).
According to Rudy (2010), some children on the autism spectrum may have low muscle tone, or
have a tough time with coordination and sports. These issues can interfere with basic day-to-day
functioning and they're almost certain to interfere with social and physical development. They
will therefore require the services of a physical therapist. Physical therapists may work on with
very young children on basic skills such as sitting, rolling, standing and playing. Occupational
therapists and physiotherapists often work together to assess and develop specific gross and fine
motor skills: major movement skills, like walking or clapping; and more delicate movements,
like holding a spoon or pushing a button. They can help the learners with autism improve their
physical dexterity (Ministry of Education Special Programs Branch, 2000). Speech-Language
therapy is given to learners who are autistic. Speech Language pathologists are professionals
trained to evaluate and develop programmes for individuals with speech or language problems
(Best et al., 2010). The speech-language pathologist will work with the other professionals to
identify communication goals for the child‟s specific needs (Ministry of Education Special
Programs Branch, 2000). The study sought to find out the teaching resources and support
services for learners with autism and blindness in selected special schools and units in Baringo,
Kiambu, Kisumu and Nairobi counties in Kenya.
2.3 Instructional Methods for Learners with Cerebral Palsy Intellectual disability
A learner who has cerebral palsy and intellectual disability has a combination of cerebral palsy
and intellectual disability. Cerebral palsy can be defined as a group of non progressive disorders
characterized by impaired voluntary movement of posture resulting from a brain injury or brain
defect occurring before birth, during birth, or within the first few years of life (Beers, Porter,
Jones, Kaplan & Berkwits, 2006; Miller, 2005). Cerebral palsy is often accompanied by
disorders of sensation, communication, perception, and behavior as well as epilepsy (Bax et al.,
2005). Common to all individuals with cerebral palsy is the difficulty controlling and
coordinating muscles. This makes even very simple movements difficult. Cerebral palsy may

60
involve muscle stiffness (spasticity), poor muscle tone, uncontrolled movement, and problems
with posture, balance, coordination, walking, speech, swallowing and many other functions.
Intellectual disabilities, seizures, breathing problems, learning disabilities and hearing and vision
problems are often linked to cerebral palsy (Ratanawongsa, 2004).
Cerebral palsy has several different etiologies and different types of motor impairments for
example Spastic and Athetoid). Cerebral palsy is non progressive but the symptoms of cerebral
palsy may get worse (Beers et al., 2006; Blair & Stanley, 1997). For instance, movement may
become more inhibited over time because of the development of contractures (shortening of
muscles), or sitting may become difficult because of the development of scoliosis (curvature of
the spine).There are two main types of cerebral palsy that is pyramidal and extra pyramidal. The
pyramidal and extra pyramidal systems are the two principal systems of the brain and spinal cord
that control movement. The pyramidal system is primarily concerned with strength and control
of fine movements of the arms and legs, especially the hands and feet. The extra pyramidal
system is primarily concerned with more basic aspects of movement and exerts greater control
over muscles of the body, shoulders and hips, although it also controls muscles in the arms and
legs (Ratanawongsa, 2004). When there is damage to the pyramidal system of the brain during
gestation or within the first few years of life spastic cerebral palsy occurs. Spastic cerebral palsy
is the most common forms of cerebral palsy, occurring in over 70% of those with cerebral palsy
(Beers et al., 2006) Spastic cerebral palsy uses a topographical classification system to connote
the location and number of limbs affected. The most common types are diplegia, hemiplegia and
quadriplegia. In spastic diplegic cerebral palsy, the legs are primarily affected and there is some
arm involvement. Depending on the severity, the knees may tend to come tightly together, the
legs may tend to cross over each other (Scissoring) and the child may walk awkwardly and on
tiptoe. In spastic hemiplegic cerebral palsy only one side of the body is affected. The arm and the
leg on the affected side have increased muscle tone. The leg muscles are tight, the child is on
tiptoe and the arm may be drawn into a bent position at the elbow (Heller et al., 2009; Best,
Heller& Bigge, 2010). In spastic quadriplegic cerebral palsy, the four limbs are involved, the
legs usually more severely than the arms. The trunk and the face may be involved as well.
Speech is typically affected. There are other types of topographical designations used to describe
spastic cerebral palsy, although they are not as commonly encountered. Some of these include
61
monoplegia (one limb), paraplegia (legs only), triplegia (three limbs) and double hemiplegia
(arms more involved than the legs) (Heller et al., 2009; Best et al., 2010). Damage to the basal
ganglia a part of the extra pyramidal system of the brain can result in abnormal patterns of
movement or very rigid muscle contractions. When they occur during gestation or within the first
few years of life, it is referred to as dyskinetic cerebral palsy, known as Athetoid cerebral palsy
the second most form of cerebral palsy, occurring in about 20% of children with cerebral palsy
(Beers et al., 2006). Athetoid cerebral palsy may present as abnormal, involuntary movements
that may be slow and writhing (athetosis) or rapid, random and jerky (Nehring, 2004)
Abnormal developments or damage to the cerebellum a part of the extra pyramidal system of the
brain during gestation or within the first few years of life can result in ataxic cerebral palsy. In
ataxic cerebral palsy, there is difficulty in the co-ordination of voluntary movement and
problems with the balance. In Dystonic cerebral palsy there are strong muscle contractions with
the recurrent movement patterns. A single area of the body for instance a joint may be affected,
or it may be more generalized and affect most of the body (Miller, 2005). For instance a limb
may involuntarily move into an abnormal position and remain there for a period of time
(Nehring, 2004). No matter which type of cerebral palsy a child has, there will be abnormalities
of movement because normal movement requires a co-ordination of muscles. There is a range of
severity of cerebral palsy and various classification systems that have been used with some
describing the severity as mild, moderate, profound and severe. In addition to abnormal motor
movements, the child with cerebral palsy will have persistent primitive reflexes. Further
difficulties in movements are present when contractures occur. Contractures are permanent
muscular shortenings in which the muscle length is reduced or there is a fixed resistance to
movement (Sankar and Mundkur, 2005). This reduces the child‟s range of motion and ability to
move the limb fully. Contractures can be very debilitating and can result in minimal use of limbs.
The lack of co-ordinated muscle movement and the persistence of primitive reflexes found in
cerebral palsy may affect the oropharyngeal muscles those controlling the mouth and throat.
Speech may be slurred and poorly articulated (dysarthria), making it difficult to understand in
some cases, it can be so severe that no speech may be present (Anarthria) (Sankar and Mundkur,
2005). Cerebral palsy can also affect the non-verbal forms of communication. Facial expressions
may be strained, and difficulty with the head control may impede making eye contact. This may

62
be mistaken for lack of interest. A learner with severe spastic cerebral palsy may want an item
and reach for it but knock it away because of abnormal motor movements. Children with cerebral
palsy may be gifted, have normal intelligence, or have intellectual disabilities overall, there is a
significant incidence of intellectual disability in children with cerebral palsy, with some accounts
of up to 60% of intellectual disabilities (Sankar and Mundkur, 2005).
Certain types of cerebral palsy have been associated with an increased incidence of intellectual
disability. Persons with spastic diplegia and athetoid cerebral palsy may have no intellectual
disabilities. Children with spastic quadriplegia, however have a higher association of intellectual
disabilities or learning disabilities than persons with spastic hemiplegia (Russman & Ashwal,
2004). Approximately 2% of the general population is affected by intellectual disability, whereas
up to 25% of the children with cerebral palsy are affected by intellectual disability. Early
intervention and special education programs can reduce the impact of intellectual disability.
Programs can tailor the curriculum so that learners can learn at a rate that gives them confidence
in their emerging new abilities. Therefore, parents must recognize their child‟s developmental
strengths and weakness so that they can help plan an education program that help achieve their
child‟s potential (Westwood, 2003). According to the American Association on Intellectual and
Developmental Disabilities(AAIDD)(2008) intellectual disability is a disability that is
characterized by significant limitations both in intelligence and adaptive behavior expressed in a
conceptual, social and practical adaptive skill. The disability originates before the age of 18
years. The diagnostic criteria for intellectual disability identifies a learner with intellectual
disability as having a significantly sub average intellectual functioning with an intelligent
quotient (IQ) of approximately 70 or below on an individually administered IQ test (for infants, a
clinical judgment of significantly sub-average intellectual functioning. The intellectual disability
also show concurrent deficits or impairment in present adaptive functioning, that is the person‟s
effectiveness in meeting the standards expected for his or her age or by his or her cultural group;
in at least two of the following areas: communication, self care, home living, social or
interpersonal skills, use of community resources, self direction, functional academic skills, work,
leisure, health and safety. The onset of intellectual disability is before 18 years of age. The code
used to diagnose learners with intellectual disability is based on degree of severity reflecting
level of intellectual impairment. Mild intellectual disabilities have an IQ of 50-55 to

63
approximately 70. The moderately intellectually disabled have an IQ level of 35-40 to 50-55.
The severely intellectually disabled have an IQ level of 20-25 to 35-40 while the profoundly
intellectually disabled have an IQ level of below 20-25. Those with intellectual disability
severity unspecified is when there is a strong presumption of intellectual disability but the person
intelligence is untestable by standard tests (Tasse, 2013). In Kenya an intellectually disabled
child is one with a limited level of intelligence and deficits in adaptive behaviour. This condition
arises between conception and 18 years of age (Ministry of Education, 1995).
Learners with cognitive impairment require special and intensive instruction and this instruction
needs to begin early. When the target of instruction is specifically identified and is taught
directly, and progress is specifically evaluated systematically and consistently, learners with
mental retardation achieve well. School age with mild to moderate intellectual disability tend to
be functioning at what Piaget referred to as the concrete operational stage. According to Piaget,
the concrete operational stage runs from 7-11 years (middle to late childhood). Although a child
at this stage reasons in a logical way the reasoning is limited to things that are physically present
or concrete. The need to see and touch objects during this stage has important implications on
teaching of primary school children (Westwood, 2003). It is expected that learners with moderate
and severe intellectual abilities will progress through the sensory motor stage and have cognitive
understanding and abilities that include the ability to map the environment visually and
auditorily; to reach, grasp, lift, transfer, place and release objects; to understand that an object
exist even if it cannot be seen and will pursue searching until they find it ;and to use attached
tools, for instance, finger feeding, zippers, pumpsoap,wind up toys or faucet and unattached
tools, for instance, pencils, T.V, remote control or keys. Most learners with moderate intellectual
abilities will achieve abilities of the pre-operational stages, including classifications
generalization and seriation (Bukatko & Daehler, 1998).
Many learners with moderate and severe intellectual disabilities are functioning at the pre-
alphabetic stage of reading. At this stage learners do not understand that letters represent the
sounds in words, although they do know that print represents spoken messages. They remember
words such as names of family members and signs by configuration and general visual
appearance and depend on the context in which words occur to recognize them. They have no

64
strategy other than rote memory of visual patterns or recognition of a word in its physical or
environmental context to read it For example, they read “McDonalds” on the sign because of the
golden arches rather than the initial “m” in the name (Ehri,1998;Moats,2000).This is not because
they ignored the letters in the signs but because they did not store the letters in memory as part of
the connections that prompted their reading of the signs (McGee, Lomax & Head,1988). The
most common instructional practice and the majority of reading research conducted with learners
with significant intellectual disabilities focuses on sight-word instruction, where learners go
through repeated practice to recognize and read words on the basis of the configuration of the
letters. A sight word approach is used because of learners‟ articulation difficulties and the
complexity and abstraction of letter sound correspondence in the English language. The words
selected for instruction are functional words that will facilitate access to independence in current
and future environments. Learners are taught words and phrases in the formats they appear in
the natural settings. The words and phrases provide information for instance signs and product
labels, directions for instance, pull, stop and exit. Safety warnings for instance, do not enter and
caution and those that affect job performance (McGee et al., 1988). Learning of learners with
significant intellectual disabilities is a result of systematic, direct instruction. Direct instruction is
teacher directed. It involves the use of behavioral instructional strategies for instance,
reinforcement, response prompting, shaping, fading and task analysis and management of the
learning environment so that it provides opportunities for learners errorless responding,
systematic movement from partial participation in tasks, increasing independent performance
and decision making based on ongoing data collection(Heller et al.,2002). In addition to learning
through direct instruction, these learners benefit from observational learning employing
modeling in which correct imitation of a model by the learner is reinforced. Learning through
observation enables group instruction (Collins, Gast, Ault & Wolery, 1991). Shaping is
reinforcing successive approximations of a behavior until the entire behavior is mastered. For
instance, teaching Tom to say „mmm‟ then „ma‟ then mummy (Ministry of Education Special
Branch Programme, 2000). Antecedent prompts are materials and instructions presented to a
learner to encourage the correct performance of a behavior when the naturally occurring cues are
not sufficient to produce correct behavior (Best et al., 2010). Response prompts provides
guidance assistance in the actual performance of behavior. There are many different types of
response prompts. Some of these are verbal cues (telling the student the step) verbal instructions

65
(providing more directions on how to do the step) gesturing and modeling among others Best et
al., 2010).The use of adults, peers and non- disabled peers as models is effective for social,
motor and some communication and problem solving skills (Mercer & Snell, 1977; Snell &
Brown, 2006 & Westling, 1986). There are several strategies that may be used to increase
attention, memory and retrieval of information. Some of these include using visual imagery,
mnemonic devices, rehearsal strategies( a rehearsal strategy uses repeated practice of information
to learn it) elaboration strategies, advanced organizers, attention cues example, antecedent
prompts, prior knowledge activation strategies and other learning and metacognitive strategies
(Ormrod, 1999; Shiffrin, 1999). In addition to the problems with movement and speech many
learners with cerebral palsy tend to tire easily and have difficulty in attending to tasks for more
than brief periods of time, take a very long time to perform physical actions of pointing at or
picking up an object. Many need to be fed and toileted by a parent or an aide and, require special
physical positioning. In order to make best use of their coordinated movement they require
padded “wedges” or other specially constructed cushions to enable them to be positioned
correctly for work and they rely on the teacher or an aide to lift and move them (Westwood,
2003). Learners with intellectual disabilities require more time to learn to attend to the relevant
dimensions of a task (Mercer & Snell, 1977; Zeaman & House, 1997). Generally, it has been
found that learners with significant intellectual disabilities are less liable than typical learners to
perceive, select and group relevant stimuli and discard irrelevant stimuli (Cha & Merill, 1994).
The teacher must employ behavioural instructional strategies such as antecedent prompting, in
order to focus learners attention for example, a teacher would draw a learners attention to the
first letters of the words “saw and was” by making them larger or different colour in order for the
learner to learn to read them correctly; a teacher would draw a learner‟s attention to the label for
a sweater by attaching a red ribbon in order for the learner to learn front and back for dressing.
Without such prompting, there will be long periods of trial and error by the learner (Best et al.,
2010; Heller et al., 2009). When the curriculum is appropriate, a child is less likely to
experience stress and appropriately appreciate his or her own achievements. Skill development,
not high scores on intelligence tests, should always be the goal. Even though the disabled
learner‟s pace of learning may be slower than other learners, the achievements are just as
meaningful. Parents of learners with cerebral palsy who also have intellectual disability must
remember that they learn new skills more slowly than other learners and find it harder to master

66
advanced skills such as reading, mathematics and complex problem solving. They also may not
be as motivated as other learners to learn new skills, but it does not mean that they cannot learn.
Given a good educational programme and support from family and friends, almost all learners
can make important, steady progress in intellectual abilities (Wheless, 2004). The mathematic
ability of learner‟s with significant intellectual disabilities is circumscribed by their limited
cognitive ability to deal with abstractions. The primary framework for content and process of
mathematics instructions is concrete in a functional curriculum. To meet the needs of these
learner‟s mathematic instruction begins with a foundation of basic skills. The natural occurrence
of mathematics for these learners is with manipulations embedded in functional activities rather
than being able to recite addition and subtraction facts. In an embedded approach to functional
approach to instruction, mathematic skills are taught in the context of daily activities such that
the priority for the instruction increase the learner‟s independence activities.(Ford, Schnorr,
Meyer, Black & Dempsey,1989; Snell & Brown,2006). Research on instructional strategies with
basic skills has demonstrated learner‟s with moderate intellectual disabilities, learning number
identification, rate counting, counting objects; equality and comparison of sets and basic
computation (Butler, Miller, Lee, & Pierce, 2001; Mastropier, Bakken & Scruggs, 1991; Vacc&
Cannon, 1991; Young, Baker & Martin, 1990). Successful use of “dot notation” system, similar
to the published Touch Math materials (Kramer & Krug, 1973) and use of a number line
(Sandknop, Schuster, Wolery & Cross, 1992) have been demonstrated to increase addition and
subtraction performance. However, for many learners, it is more efficient to teach computational
performance by teaching the use of a calculator, which improves efficiency and accuracy of
timed performance (Matson & Long, 1986; Snell & Brown, 2006). Early math skills involve the
use of manipulatives of such things as sorting, counting and computational skills. Learners with
poor fine motor control may need larger manipulatives that are positioned within the learner‟s
range of motion. Software programs also exist that allow learners to move items on a computer
screen with the click of a switch. Several math programs exist that not only assist in practicing
new math skills ranging from counting to Algebra but also provide access to learners requiring
alternative input devices, alternate output and screen modifications. Assistive technology also
exists for functional math skills such as time and money skills. Several software programs
address these areas often with features to make them more accessible. Special money calculators
are available that allow the learner to select dollars or various coins to come up with the total

67
amount (Heller et al., 2009). For learners who have cerebral palsy and intellectual disability, in
order to fully cater for limitations in intellectual functioning teachers need to provide instruction
in a number of skills outside the general curriculum. These skills are more functional in nature
but are absolutely essential for the future independence of the individual. Additional skills areas
include money concepts, time concepts, independent living skills, self care and hygiene,
community access, leisure activities and vocational training. General curriculum areas should not
be neglected, however, and there are some promising practices to help support these learners in a
number of academic areas. One effective early literacy strategy with these learners is pre-
linguistic milieu teaching (Fey, Fitzgerald, Friel &Lapan, 2006). According to Fey et al., (2006),
prelinguistic milieu teaching is a technique that ties instruction to the specific interests and
abilities of the individual learner. This language acquisition instructional strategy also helps
support effective self determination as a key component of the training which is a frequent
required behavior from the learner. Breaking down larger tasks into their specific component
parts is also an effective technique for teaching any number of skills for learners with cerebral
palsy and intellectual disability. More complex concepts and activities can be taught over time
and as the learner master‟s one component of the task, another is added to the routine. This type
of task analysis can be taught using a variety of instructional supports, from physical and verbal
prompting to observational learning. The specific instructional strategies and materials used by
the learner should be aligned to learner‟s own interests and strengths. Useful strategies for
teaching learners with mental handicap and cerebral palsy include the following techniques:
teach one concept or activity component at a time, teach one step at a time to help support
memorization and sequencing, teach learners in a small group, or one on one if possible, always
provide multiple opportunities to practice skills in a number of different settings, use physical
and verbal prompting to guide correct responses and provide specific verbal praise to reinforce
these responses(Fey et al.,2006). The ability of learners with moderate and severe intellectual
disabilities to synthesis information and skills is limited (Westling &Fox, 1995). They have
difficulty perceiving the relationship between parts and whole. The teacher should not teach
isolated skills and expect the learner to organize the information for use. Skills must be taught
within the contexts embedded within the environment and activity in which they will be
performed.

68
The acquisition of skills requires an instructional strategy that breaks down task chains into
component steps and skills so that each can be taught directly (Heller et al., 2009). Other
teaching strategies for learners with intellectual disabilities include a learning strategy and
providing explicit instruction. Learning strategy focuses on how the learners learn, rather than
specific content. This includes any technique that helps a student learn and complete the task
independently (Mercer & Mercer, 2004). Some of these include songs or rhymes, mnemonics,
self instruction and self monitoring. Providing explicit instruction is a teacher- led approach that
typically consists of three main components; demonstration and modeling, guided practice and
independent practice (Dangle & Keel, 2006). In the first component the teacher models the
target behavior. In guided practice, the teacher may use a continuum of assistance, based on
individual student needs (Mercer & Mercer, 2004).In independent practice the learner practices
the skill without assistance but still receives feedback as needed. For example, if the learner is
learning how to use a vending machine, the teacher may first demonstrate use, and then
systematically guide the learner. The student is then allowed to practice the skill independently
providing feedback as needed (Mercer & Mercer, 2004).
In Kenya, in an effort to determine the number of children with multiple disabilities in schools
for the physically disabled children, Kenya Institute of Education found that 34.9 % of the
children who had enrolled in the six major schools in 1980, had multiple disabilities. The
disabilities included; visual problems, hearing problems, learning disabilities and intellectual
disability (Ndurumo, 1993). The study did not show the instructional strategies that teachers
were using in enhancing learning for learners with physical and multiple disabilities. This study
sought to find out the instructional methods used by teachers teaching learners with Cerebral
palsy intellectual disability in some of our special schools and units in Baringo, Kiambu, Kisumu
and Nairobi counties in Kenya.
2.3.1 Curriculum Adaptations for Learners with Cerebral palsy Intellectual
Disability
For curriculum development, skills selected for instructions must be those that occur frequently
in the learners lives so that they have repeated opportunities for practice. For instance, reading
words should be selected from environmental print encountered in the community. Skills that are
used often and in various settings will naturally occur and therefore enhance memory functions

69
(Ellis, 1970; Westling and Fox, 1995). Learners with significant intellectual disabilities learn few
skills within the time available in school, require more instructional (trials) to learn those skills
and therefore more time to learn, and require more time to recoup lost skills (Brown et al.,
1989).These learning characteristics require the careful selection of learning objectives, and
those selected must have a direct effect on the learner‟s life. Context and environment are critical
factors for instruction (Brown et al., 1989). To the extent possible, instruction should take place
in the setting in which skills are to be used with natural materials and with a variety of people.
Learners with cerebral palsy may need adaptations to the classroom and modifications of the
curriculum. These can include changes such as preferential seating for hearing or vision
problems or taping lessons to replay at a later time. He or she may need more time to complete
written assignments or note taking assistance from a peer or a teaching assistant. A learner
might need to take tests orally and take frequent breaks for muscle fatigue. The success of a
student relies on a support team to provide for the learner‟s needs. Regular and special education
teachers are a part of this team as well as occupational and physical therapists, a speech therapist,
the parents and a school administrator. The child might need a personal assistant or teaching
assistant as well (Kartha, 2011; Heller et al., 2009). According to the Kochung Report (2003);
KIE (1987), learners with multiple disabilities can follow a specialist curriculum. Specialist
curriculum remediates the problems such as communication, mobility among others. This study
sought to investigate the curriculum adaptations that had been effected for learners with cerebral
palsy intellectual disability in the counties of Baringo, Kisumu, Kiambu and Nairobi.
2.3.2 Teaching Resources and Support Services for Learners with Cerebral
Palsy Intellectual disability
Depending on the level of the cerebral palsy, special equipment and adaptations are needed to
allow the learner to function optimally in the school setting. Some learners with mild cerebral
palsy may be slower in writing assignment and need more time, while learners with more severe
cerebral palsy may need to use a computer with alternative access to complete assignment
(Heller et al., 2009). Allowance may need to be made for large and poorly coordinated
handwriting. Some may need keyboard to type or word process their assignments. For some,
adapted devices such as pencil grips and page turners may be required. Papers may need to be
taped firmly to the desktop. Computers with adaptations such as switches or touch panels, rather
70
than a keyboard or mouse are useful both for presenting academic work and as a medium of
communication with others (Westwood, 2003). For individuals who have trouble grasping a
pencil, pencil grips or larger writing utensils (fat mechanical pencils or pencils wrapped in pipe
insulation) may provide an easier grasping surface. If a learner has Athetoid movements or
tremors weighted writing utensils may help reduce the extra movements and allow for better
writing control. Hand braces may provide extra stability or eliminate the need to grasp the pencil
while writing. Adapted paper that has darker or larger lines may be needed, papers may also need
to be stabilized by tape, clipboard, slant board (Writing surfaces that change the angle) or a
nonslip material (Example rubber self liner or Dycem) (Heller et al., 2009).
Some learners have difficulty writing by hand. These learners may benefit from small portable
word processors (Example Alpha smart) or laptop computers. The device may also be adapted
with different access features or devices to make it accessible. For example, some devices will be
equipped with talking word processors that give auditory feedback to what is being typed. Some
learner‟s with physical disabilities may benefit from word prediction software that provides a
selection of words as the student types in order to decrease the number of keystrokes and
increase typing speed. For example if the student is trying to type the word difference she begins
by typing “d” and several words that begin with “d” appear in the word prediction list (Example
did, does and don‟t).If her word is not on the list, she types another letter and word prediction
supplies words and so on until the desired word is provided. The learner can select the word or
continue typing (Heller et al., 2009).There is a number of existing software packages designed to
support learners with cerebral palsy and intellectual disability in the classroom. One promising
approach in literacy software utilizes universal design for learning principles. This approach
combines reading for meaning with direct instruction for decoding and understanding. The
resulting software consists of an audio and video based curriculum that can be adjusted by the
teacher to meet the specific academic capacities of the learner. Ultimately, any software that can
tailor content to address the interests of the learner can be useful in supporting learning for an
individual with cerebral palsy and intellectual disability, given that the instruction can be adapted
to meet the needs of the learner (Turnbull et al., 2002). Some learners with fine motor difficulties
have trouble isolating and turning one page at a time. This may be addressed through putting
spaces between the pages by attaching page fluffers (pieces of materials such as sponge or

71
weather stripping) to each page. Some learners may use end of a pencil, a mouth stick or an
electronic page turner to turn pages (Heller et al., 2009). Books can also be accessed
electronically through the teacher scanning them into the computer or using commercially
produced electronic books. Having books on a computer can provide access for learners with
physical disabilities who cannot manipulate a book and help those with reading difficulties
(Heller et al., 2009). The use of real materials or actual tools in a natural environment is an
essential component in the effective instruction of learners with cerebral palsy intellectual
disability. Although these materials would be labeled as “low tech” teaching resources, they
serve to both motivate the learner and facilitate generalization to multiple environments. For
example, the use of manipulative or concrete objects for a math lesson (Turnbull et al.,
2002).There are several assistive devices that may be required for a learner with cerebral palsy to
benefit from his education program. This may include devices for augmentative and alternative
communication among others. Argumentative and alternative communication (AAC) refers to
communication that is used to enhance a learners existing verbal communication (for instance,
Argumentative or Alternative serve as the learners primary form of communication. Sevcik and
Romski (2000) states that, “AAC incorporates the individual full communication abilities and
may include any existing speech or vocalizations, gestures, manual signs and aided
communication. AAC is truly multimodal, permitting individuals to use every mode possible to
communicate.” Individuals with physical and multiple disabilities often use several different
types of communication depending on the setting, need and familiarity of the communication
partner (Patel, 2002). For example, a learner with a severe spastic cerebral palsy who has
dysarthria may use word approximations and gestures with his family members who understand
him well, use an electronic AAC device in the classroom and use pictures on paper on the
playground. AAC enhances a child‟s development of verbal abilities (Romski and Sevcik, 2005).
Even if a learner‟s speech is understandable to those who know him well, AAC should be
considered when native listeners cannot understand the learner‟s speech. For learners who have
severe communications problems, the teacher may need to adapt the presentation of material.
Material may be presented in a multiple choice to allow the learner to choose the answer or the
learner may indicate the response by eye gazing the answer presented by using a scanning device
(Heller et al., 2009). Special pencil holders or grips might be needed or a student may need a
computer for his or her writing. A learner with cerebral palsy might have trouble communicating

72
since speech is controlled by muscles. A speech therapist will work with the classroom to design
the best communication system for the learner. Some schools have an assistive technology team
that specializes in current technology and devices available for classroom use (Heller et al.,
2009; Best et al., 2010). Some learners with cerebral palsy and intellectual disability can use
pictures, and some communication boards which are designed to match the learner‟s cognitive
and receptive language skills and should be continually monitored and evaluated so that it can be
modified with the learner‟s expanding and changing needs. For the learners who cannot use the
computer as a result of physical limitations in their hands or arms, avenues should be explored
for obtaining adaptive access software (including unicorn keyboard, touch pads or foot
controlled mouse), special switches, power pads, eye controlled input systems, touch screens and
foot mice to assist in ensuring communication is possible for the learners with cerebral palsy
intellectual disability (Keller, 2005).The learner should be taught proper transferring techniques
and the personnel be trained in correct lifting and handling techniques. A nurse, physical
therapist or occupational therapist is a good resource for learning proper techniques. If the
learner weighs more than 35% of the adult body weight, the adult should not attempt the lift
alone. For example if an adult weighs 120 pounds, she should not lift a child by herself who
weighs more than 42 pounds. If the adult weighs 185 pounds, the weight limit for a one person
lift would be 65 pounds (Heller, Forney, Alberto, Schwartzman & Goeckel, 2000). The
environment should be arranged to minimize the distance the adult must carry the child. Proper
positioning for learners with physical disabilities is critical to facilitating typical and functional
movement patterns, thereby encouraging child skill development and independence. Sometimes
learners with physical disabilities will need special adaptive positioning equipment or devices in
order to maintain a functional position during typical activities at home or school. Some
equipment includes wedges, a prone stander, and special wheelchairs among others. Parents,
teachers and therapists should work together to determine what positioning devices are needed
for individual children. The physical therapist and occupational therapist work with the
classroom teacher and teaching assistant on positioning ,handling and daily activities (for
instance feeding and toileting) (Heller et al.,2009). The child with cerebral palsy may need to be
positioned in several different types of adaptive equipment, the purpose of this equipment is to
promote good body alignment, prevent contractures and deformities, promote movement and
comfort, lessen effects of abnormal muscle tone and reflexes, improve circulation ,decrease risk

73
of pressure sores (Decubitusulars) decrease fatigue and promote bone growth (Jones and
Gray,2005). Positioning also provides access to the environment and facilitates performance of
certain activities. There is a correspondence between activities and specific positions for
instance, a boy with cerebral palsy positioned in a side lyer (equipments that props the person up
on his side) may have better use of his left arm, allowing him to participate in the group activity
by using a switch (Wheless, 2004). The ability to move about provides learners with opportunity
to interact with their social and physical environment. Learners with physical or multiple
disabilities will need some type of mobility device. This may range from devices to assist with
crawling to those that assist with transportation. Devices can range from a cane for walking,
support to a car that has been especially adapted for an individual with a severe physical
disability. To assist in crawling or creeping, some children can use a scooter board. Scooter
boards are typically small, square pieces of wood covered with plastic and cushioning material
that have four casters in the corners of the board to allow the board to move in all directions.
Scooter boards may support the trunk (allowing the child‟s arms and legs to move) or be
constructed longer to support the entire body (allowing only one arm movement).Children are
typically strapped in, lying on their stomach (Heller et al., 2000; ;Best et al.,2010). To assist with
walking, there are several different mobility devices, including canes, crutches and walkers.
There are two main types of crutches that may be used: Auxiliary crutches (which are full length
crutches that provide support up to the armpit) and Lofstrand or forearm crutches (which are
crutches that extend to the forearm) learners needing more support may use a cane. Individual
with more severe physical impairments may learn to propel themselves using a powered scooter
or a powered wheelchair. Some wheelchairs adjust from a sitting to a standing position (Heller et
al., 2009). Mobility devices are now being introduced early because several positive effects
attributed to the use of powered mobility devices, such as improved head control, trunk stability
and arm hand function; increased motivation in other forms of movement; increase in
communication, exploration, social interactions; and self esteem and no ill effects on motor
development (Judge and Lahm, 1998). Activities of daily living may require adaptations or
assistive technology to allow the learners to participate to the maximum extent possible. (For
instance, tooth brush and tooth paste holders may be used to assist with tooth brushing). A
dressing rack and adapted clothing fasteners may help the learners dress; push pull sticks may
help with putting on socks. Environmental control devices that allow the child activate items

74
with a switch (for instance, turning on lights or television) may be useful (Heller et al., 2009).
Age at which toilet success is achieved is partly dependent on the severity of the(CP) and
cognitive functioning of learners with an intellectual disability ,the teacher will need to use
systematic instructions in toilet use for instance, trip training strategies after determining from
the physicians that there is not any medical reason impending bladder or bowel control.
Learners may have such difficulties as a tongue thrust (causing food to be pushed out of the
mouth) a bite reflex (causing the spoon to be bitten) and chocking (Heller et al., 2009). Children
with arm involvement may be unable to bring the spoon to their mouths or be unable to hold
utensils. Some devices used for feeding such as adapted dishes, cups and utensils may be
necessary.
Some learners will be unable to eat enough orally because of their oral-motor dysfunction and
will need gastrostomy tube feedings (Feeding through a tube directly into the stomach) (Sullivan
et al., 2005). The teacher needs to be alert for any difficulty the learner may have with social
interactions. Learners with cerebral palsy may become socially isolated because of their
appearance and often because of poor social skills. The teacher may need to provide social skills
training. Learners with cerebral palsy may also exhibit frustrations and have behavioral outbursts
when they cannot communicate effectively or are unable to accomplish a task because of their
unintentional movements. Teachers need to be sensitive to the learner‟s needs, provide
augmented forms of communication and provide alternative ways of accomplishing tasks(Heller
et al.,2009; Best et al.,2010). Individuals with cerebral palsy require assistive technology to
perform light management activities such as self care, domestic, prevocational and community
activities. Self care skills that may require assistive technology include activities such as eating,
drinking, dressing, brushing teeth and washing (Heller et al., 2009; Best et al., 2010). Adapted
spoons may be necessary to those with difficult eating. For instance spoons may be fitted with a
strap to fit around the hand for a person who cannot grip, they may be a different shape or they
may be weighted to steady certain types of abnormal motor movements. Adapted bowls and
plates may be necessary for instance, scoop dishes or dishes that adhere to the table, cups may
need handles or part of a side of the cup cut out for the nose to fit when the individual cannot tip
his head back). Individuals who have good head control but are unable to use their arms may
benefit from a switch mechanical feeder (Heller et al., 2009; Best et al., 2010). Adapted clothing

75
may be needed for someone with a physical impairment to promote ease of dressing (for
instance, clothing with Velcro fasteners) people with limited motor abilities may need to use
dressing sticks to help them pull down their pants, shoes with Velcro may be easier for
individuals with cognitive or physical impairments (Best et al.2010; Heller et al., 2009). There
are many adapted items that may be used to maintain proper hygiene for instance; toothbrushes
may have built up handles to hold better or a grip to go around the hand so that the user does not
have to maintain a grip. Hairbrushes with longer handles may assist individuals with limited
movement or shortened limbs. These items are available from companies or can be homemade.
Careful assessment is needed to determine if the technology is appropriate (Best et al., 2010;
Heller et al., 2009). Some individuals with disabilities may use a service animal, such as a
specially trained dog, horse, monkeys, cat or other animal. Service animals may assist learners
with physical disabilities in such tasks as carrying materials, fetching and returning dropped or
needed items, opening doors, turning switches on and off, feeding and pulling wheelchairs up
ramps or across distances (Zapf and Rough, 2002).
2.3.3 Treatment and therapy for learners with Cerebral palsy Intellectual Disability
Treatment of learners with cerebral palsy and intellectual disability varies according to their age,
the severity of their symptoms and type of cerebral palsy. Common steps include: corrective
lenses orthotics (mechanical aid that is used to support or assist movement of a weak part of the
body), braces or corrective surgery for affected limbs, injections of tiny doses of botulin toxin to
relieve spasticity and treat movement disorders, medications that reduce spastic tension in
muscles, speech therapy, physical and occupational therapy, psychological counseling to assist
with adjustment issues, referrals to appropriate resources including a neuropsychologist for the
development of an Individualized Educational Plan (IEP) (Wheless, 2004). The members of a
treatment team for a child with cerebral palsy will most likely include the following: A
physician, such as pediatrician, pediatric neurologist, or pediatric physiatrist, who is trained to
help developmentally disabled children. This doctor, who often acts as the leader of the treatment
team, integrates the professional advice of all team members into a comprehensive treatment
plan, makes sure the plan is implemented properly, and follows the learner‟s progress over a
number of years. An orthopedist is a surgeon who specializes in treating the bones, muscles,

76
tendons and other parts of skeletal system. An orthopedist is often brought in to diagnose and
treat muscle problems associated with cerebral palsy (Heller et al., 2009).
A physical therapist designs and puts into practice special exercise programs to improve strength
and functional mobility. An occupational therapist, teaches the skills necessary for day to day
living, school and work. A speech and language pathologist specializes in diagnosing and
treating disabilities relating to difficulties with swallowing and communication. A social worker
helps individuals and their families locate community assistance and education programs. A
psychologist helps individuals and their families cope with special stresses and demands of
cerebral palsy. An educator may play an especially important role when mental retardation or
learning disabilities present a challenge to education ((Donkervoort, Roebroeck, Weigerin, Van
der Heijden-Maessen& Stam, 2007). The goal of treating cerebral palsy is to develop maximum
independence. The child with cerebral palsy benefits from physical, occupational and speech
therapy‟s positioning devices; orthotic devices; medications and sometimes surgery to improve
motor function. Physical and occupational therapies provide support to children with cerebral
palsy. Most therapy attempts to reduce the abnormal movement patterns and encourage normal,
purposeful movements in an active and functional manner. In addition, speech language therapy
may be able to improve speech production, although augmentative communication will be
needed by many individuals with severe spastic quadriplegic cerebral palsy (Wheless, 2004).
Neurodevelopment treatment approach was developed by Berta Bobath, a physical therapist in
1960. In neurodevelopment approach the therapist uses a “hands- on” approach, placing hands
on specific body parts in order to help align body segments and initiate, guide, or prevent
unwanted movement. The ultimate goal of neurodevelopment treatment is to inhibit a child‟s
atypical patterns of movement and facilitate typical movement patterns, including requisite
postural reactions. Therapy balls are frequently used in treatment sessions to encourage
adaptive postural responses to movement. The aim of treatment is to help the child develop new
patterns of movement. Training and involvement of other team members (family, therapists,
and teachers) is encouraged in the approach in order to plan and execute a well co-
ordinated treatment program. However, good handling techniques on the part of the therapist
are essential to the approach. Their treatment focused on children with cerebral palsy with
atypical muscle tone.

77
Sensory Integration theory and therapy is currently applied to children with a variety of
neurological impairments, such as cerebral palsy for better central nervous system organization.
The approach facilitates the child‟s ability to make adaptive responses to specific sensory
stimulation (including, tactile, vestibular, and proprioceptive stimuli) while engaging in
purposeful activity. Sensory integration is directed towards improving the brains capacity to
perceive remember and plan motor activity. Sensory therapy frequently uses activities that
provide vestibular stimulation to influence balance, muscle tone, ocular-motor responses,
movements against gravity, postural adjustments and arousal or activity level. Suspended
equipment, as well as resistive activities, and weighted objects are often used in Sensory
integration therapy to encourage adaptive postural and movement responses (Effgen, 2005;
Montgomery & Connolly, 2003; Smith, Roley, Blanche, & Schaaf, 2001). The mobility
opportunities via education curriculum was developed in the 1990‟s by Linda Bidabe, an
educator, and John Lollar, a physical therapist to help children systematically develop motor
skills. The program provides naturally occurring practice of functional motor skills while
the learner is engaged in educational or leisure activities. In the programme, activities are
selected for instance, using a public restroom or eating in a restaurant), and they are task
analyzed to determine the physical skills needed to do these tasks for instance, transition
from standing to sitting position or walking backwards. Each of these physical skills is
divided into four levels of success ranging from skills acquisition with independent
mobility to skill acquisition that would improve bone health and functioning (Miller, 2005).
The goal of treatment for individuals with neuromuscular scoliosis(a curvature of spine) is to
correct or prevent progression of the spinal distortion that can cause pain, difficulty sitting,
or compromise in lung volume and affect other body systems (Miller, 2005). The three most
common approaches to treating scoliosis include observation, bracing and Surgery. Very Mild
Curves may only require close observation and x-rays to determine if the curve is progressing.
This is especially the case when the curve is idiopathic and may not be progressive (Heller
et al., 2009). The use of a brace (also known as Orthosis) to prevent further worsening of an
abnormal curvature has shown promising results in some individuals with idiopathic
scoliosis in particular. Bracing is typically used with growing adolescents who have not
reached skeletal maturity and have a moderate curve (Herring, 2002). The most common

78
surgery for scoliosis is a spinal fusion with instrumentation (i.e. rod) and bone graft. In this
surgery prebent (rods) are attached to the spine in certain locations by hooks or screws (or other
means), and the spine is carefully straightened. Small pieces of bone graft for instance, from
the hip, are placed between the vertebrae to fuse them together, keeping the spine straight.
This is referred to as a spinal fusion. The rod(s) keep the spinal column straight while the
bone graph grows and makes the spine solid, preventing a curve. The spine remains flexible
where it has not been fused. Modifications are dictated by the learners needs. They will require a
support team to provide for the learner‟s needs (Donkervoort et al., 2007). The learner with
cerebral palsy may also need to use various braces or splints (Othoses). By applying an orthotic
splint or brace, the muscle group is placed in a more functional position. This helps maintain
proper alignment, improves range of motion and decreases the development of contractures. To
prevent toe walking and the shortening of the Achilles tendon, a short leg splint may be worn.
Specific equipment is prescribed according to the type of motor problem, the child‟s size and
weight and the nature of the activity. Equipment such as side lyers, wedges, special seating
devices and prone standers is commonly used. Other equipment such as scooters, bikes, walkers
and wheelchairs may assist with mobility. Often, modifications are made to those mobility
devices to allow for proper positioning. Wheelchairs for example, may have special inserts to
keep the knees apart (abductor pad) or the body aligned (lateral supports). Head support may be
necessary as well. Some wheelchairs are motorized to allow independent movement for children
with upper arm involvement. A physical therapist should help describe or modify this mobility
equipment, which should help the learner be as independent as possible (Wheless, 2004).To help
improve hand function, a resting hand splint or hand cone may be used. They must be carefully
monitored by therapists for the correct fit as the child grows. Close adherence to the times the
orthosis is supposed to be worn is important if treatment is to be effective (Heller et al., 2009).
Several medications may be taken to control excess muscle tone and promote relaxation of the
muscles. Two commonly prescribed oral medications are Valium (Diazepam) and Dantrium.
Side effects may occur including drowsiness, excessive drooling and changes in memory,
attention and behavior (Verroti, Greco, Spalice, Chiarelli and Iannetti, 2006). Careful monitoring
on the side effects and effectiveness are necessary to make any needed adjustments in dosage or
to try new treatments. Baclofen has been found to be useful in the management of spasticity and
is often delivered by an implantable pump (Verroti et al., 2006). Complications can occur with

79
the pump (example infection or catheter tube breakage) and side effects of the medications
(example hallucinations and Psychosis if the medication is suddenly withdrawn (Miller, 2005).
Another medication that may be used is Botulinum toxin, which reduces excessive muscle tone
in spasticity and dystonia (Pellegrino,2007).Botolinum toxin works best in children requiring one
or two muscles to be injected (Herring, 2002). It can be effective for up to 3 to 4 months (Verroti
et al., 2006). Side effects include muscle weakness and pain during injection. Surgery may be
needed to increase range of motion, decrease discomfort, or increase functional use of a body
part. Individuals with cerebral palsy are especially at risk of developing contractures, which
shorten muscle length and decrease range of motion of a joint. Several different surgical
procedures are designed to treat contractures. One common surgery is used to correct the foot
deformity of the ankle that results in the child being on tip-toe. In this surgery, the Achilles
tendon (heel cord) is lengthened, resulting in the foot being placed flat on the ground. It may
assist in walking (Kreulen, Smeulders, Veeger and Hage, 2006). There are many other surgical
procedures used to improve the range of motion in the arms and legs due to contractures. The
surgical goal of treating children with spasticity in the arms is to release the spastic deformity
and reposition the arm to improve its functional use (Kreulen et al., 2006).The hamstring
muscles in the legs may be released to help with sitting and walking. Surgery to release the
tendons and muscles that result in hip deformities may be needed. These surgeries are aimed at
preventing hip dislocation and allowing the child to assume a sitting position. Neurosurgical
procedures have also been used to treat cerebral palsy. These procedures involve surgery on the
central nervous system. One such procedure known as selective posterior dorsal rhizotomy,
involves cutting a certain percentage of specific spinal roots that cause severe spasticity of the
legs (McLaughlin, Bjornson, Temkin, Wright &Reiner, 2002). Every child with cerebral palsy
may need a different kind of therapy, according to the severity of the disorder. They will require
a support team to provide for the learner‟s needs (Donkervoort et al, 2007; Best et al., 2010).
2.3.4 Adaptations for learners with Cerebral palsy Intellectual Disability
Adaptations are alterations to a task (or material used in the task) that provide access to a task to
facilitate participation in a task for which an individual does not have the requisite abilities
(Bryant & Bryant, 2003). Adaptations include modification and accommodations.
Accommodations refer to changes to the task to accommodate for a disability that does not alter

80
the performance standards, where modifications refer to changes where the content level or
number of skills is altered (Beech, 2006). An adaptation also encompasses assistive technology
and alternative performance strategies that are non typical ways of performing a task, such as a
learner who writes by holding a pencil with his or her teeth. In order to meet the needs of
learners with physical, health or multiple disabilities, it is important that appropriate adaptations
are identified (Heller, Forney, Alberto, Schwartzman & Goeckel, 2000). This begins by
examining the target performance of the task and the learner‟s performance of the task. Any
discrepancy between the target outcome and learner‟s performance is examined in terms of the
reason for the discrepancy (for instance, atypical motor movements and motor abilities resulting
in restricted range of motion, vision loss affecting access to the task, poor physical endurance,
health issues regarding frequent discomfort resulting to inattention to the task, learning
difficulty regarding understanding task requirements, lack of appropriate communication or poor
motivation(Heller et al.,2000). Based on the reason identified for the discrepancy between target
performance of the task and learner‟s performance, appropriate adaptations are selected using a
team approach. The teacher will need to involve the related staff like the occupational and
physical therapists and speech language pathologists, parents and the learner in the selection of
the adaptations as well as the evaluation of their effectiveness. It is important that all individuals
working with the learner understand the adaptations and work together to consistently implement
them. Getting input from all team members while planning adaptations and making sure that
proper training of each adaptation takes place helps to get the right adaption-user match and
helps reduce the possibility that adaptations are unnecessarily abandoned (Bryant & Bryant,
2003).Adaptations must be individualized for the learner to adequately meet the learner‟s unique
characteristics and should aim at promoting effective learner‟s participation and increasing
learner‟s independence. Adaptations cannot be made for a group or category of learners because
in the area of physical disabilities, two learners with the same diagnosis may have significantly
different physical abilities (Heller et al., 2009). Sufficient time must be given to determine if an
adaptation is effective. It is unlikely that an adaptation will be effective after one trial (Baumgart
et al., 1982). The possible adaptations that will be needed in a classroom to assist a learner who
has a physical or multiple disability will fall into several areas: Mobility and seating
arrangement, student positioning to optimize movements, adaptations to work surfaces, special
positioning of materials on the work surface due to restricted range of motions, assistance or

81
adaptations to materials and modifying activities or tasks in the classroom because of fatigue.
Some learners with physical or multiple disabilities will have mobility problems and have
difficulty getting to their desks (or areas in the classroom).To address this issue, aisles may need
to be widened or assistance may be needed (including assisting the learner into transferring into a
chair or moving a chair up to a desk (Wadsworth & Knight, 1999). Cut out desks may be used to
allow the wheelchair to fit under the table and provide additional arm support. Other tables may
need to be lowered for best fit (Heller et al., 2009). The team may need to carefully consider the
layout of the room and how the learner will move to different locations. Seating arrangements
should take into account assistive technology devices used by learners and the ability to access
classroom area. For instance, some learners may need preferential seating and be near the front.
Proper positioning is critical for learners with physical disabilities since good positioning can
maximize movement for instance, better arm movement can occur when proper positioning is in
place for learners with severe cerebral palsy (Wadsworth & Knight, 1999). Good positioning is
also important to decrease health problems for instance; skin breakdown in a learner with severe
scoliosis (a curvature of the spine). Some learners will require an adapted chair or wheelchairs
that provide support and positioning. Once the learner is properly positioned the learner may
have difficulty accessing the work surface because of atypical arm or hand movements. In this
instance the work surface may need to be adapted. Some learners will have improved movements
if the work surface is slanted through use of a slanting table top, slant board or a three-ring
binder. If the material slides all over the surface, it will need to be stabilized using a tape, Dycem
or a rubber shelf liner. It is important to realize that the work surface area includes not only the
desk but also the height, slant and size of the work surface area that learners may access using
other parts of the body, such as their feet (Wadsworth & Knight, 1999). Once the work surface is
correctly adjusted, the best placements of the materials will need to be determined on the basis of
the learner‟s range of motion. This refers to the distance the learner is able to reach with his
hand, foot, mouth stick or other body parts to access materials or by having the learner touch
various areas on the work surfaces or other items such as a keyboard or pictures or an
augmentative or alternative communication(AAC) device (Heller et al.,2009). It should be
specified on the adaptation checklist if a learner will need to have materials handed to him or if
he requires alternative access or if the materials need to be modified to make it easier for the
learner to manipulate them. (For instance, some learners have atypical movements that are

82
uncontrolled or that have extraneous movements. Some learners will experience fatigue or lack
of endurance as they manipulate materials or engage in any activity. For instance a learner with
severe spastic (CP) activating a switch over and over again. Rest breaks should be provided. If
the rest breaks are needed, the teacher should specify on the checklist when they occur and for
how long and what the learner does during the break (Heller et al., 2009). Environmental
adaptations of the classroom should be put in place in order to ensure the teaching process of
learners with cerebral palsy and intellectual disability runs smoothly. By adapting and modifying
the learning room design, is one of the key areas for these learners to ensure effective instruction:
The room should have two doors, one in the front and one near the back. Chalkboards and easels
should not be higher than 24 inches from the floor to enable learners on wheelchairs to see. The
doors should have automatic door checks allowing the door to remain open for wheelchairs and
clutch walkers. Doors should have long grasping bars rather than door knobs. Toilet facilities
should be near the learning environment and floors should be of nonskid type (Donkervoort et
al., 2007). Teachers will need to facilitate toilet training by having appropriate adaptations in
place. Adaptations such as handrails and a properly fitted adapted toilet are important to decrease
fear of falling and allowing the child to relax to allow elimination to occur. The learner will also
need a way to communicate that he needs to use the rest room (Heller et al., 2009; Best et al.,
2010). This study sought to find out the available teaching resources and support services for
learners with cerebral palsy intellectual disabilities in selected special schools and units in
Baringo, Kiambu, Kisumu & Nairobi counties in Kenya.
2.4 Training needs of specialized personnel for Learners with Multiple Disabilities
In America, a research project was carried out under the Perkins National Deaf blind
Training project on the competencies for teachers of learners who are deaf-blind. The aim
of the study was to improve educational practices by ensuring teachers have the basic
competency in all the areas addressed in the knowledge and skill statements in the teaching
of children with deaf blindness. The skills and knowledge areas in the study included the
following areas of deaf blindness: personal identity, relationships and self esteem, concept
development, communication, hearing, vision, orientation and mobility, environment and
materials and professional issues (Reiman,Malley &Klumph, 1998). Children who are deaf-
blind require highly specialized and personalized teaching approaches because of their

83
combined vision and hearing losses . Although children who are deaf-blind have the same
basic needs as all children, the combination of sensory loss accompanied by other
disabilities creates additional highly complex challenges. The extent of vision and hearing
loss varies within the population of children who are deaf-blind. Most have residual use of
either vision or hearing, while others have no usable vision or hearing. Each child is unique but
all share communication challenges and the potential isolating effects of combined vision and
hearing loss (Reiman et al, 1998). Teachers, support personnel and caregivers who are essential
to the lives of infants, children and young adults who are deaf-blind must have excellent training.
There are various competencies that can work as effective tools to identify needs and implement
training in a cohesive way. Communicating with individuals who are deaf-blind is a unique
experience. The language, mode, style, speed, aids and devices used to facilitate communication
are different from person to person (Reiman et al, 1998). The study was crucial for the present
study because it was looking for the competencies required by teachers teaching learners with
deaf-blind. The present study intended to find out whether the same competencies are applicable
in our Kenyan educational settings. Teachers who instruct learners with multiple disabilities
must possess specific competencies that encompass instruction, physical management of
learners, educational environment, and health maintenance, use of assistive technology,
augmentative communication and curricular adaptation (Best, Heller &Bigge, 2005; Council for
Exceptional Children, 1998; Heller, Fredrick, Dykes, Best, & Cohen, 1999; Heller & Swinehart-
Jones, 2003). According to Best et al., (2010), teachers of learners with multiple disabilities must
have more than curricular knowledge and instructional strategies to be effective educators. They
must have knowledge about a variety of disabling conditions and their implications for function.
They must possess the empathy and knowledge required for working with families who may be
coping with highly emotional situations including chronic illness, frequent hospitalizations and
perhaps terminal outcomes. In this process, they become partners with families and collaborate
with them to meet the shared goal of learner‟s success. They must collaborate successfully with
personnel from many disciplines, including therapists, doctors, nurses, speech-language
specialists, and others while they function as a resource for teachers in general education.
Finally, teachers must also be advocates for their learners, and they must always envision the
goal of self-advocacy for learners and their families. To reduce the functional impact of
disability, teachers and others who work with individuals with multiple disabilities must develop

84
knowledge, skills, and abilities that extend beyond standard pedagogy. They must have a
thorough understanding of typical development in motor, sensory/ perception, cognition,
communication, language/social/ emotional and self-care domains. Their knowledge and skills
must include the ability to accommodate and modify the general education curriculum. They
must be able to incorporate essential knowledge and skills for personal self-reliance into the
education program, including domains of functional living skills, physical task performance,
fundamental and assisted communication and individualized preparation for transitions (Best et
al., 2010). The competencies of a teacher who is deaf-blind according to the Council of
Exceptional Children (1995) include; knowledge on deafblindness, personal identity,
relationships and self-esteem, concept development, communication and hearing-vision. On deaf
blindness a teacher should know the critical roles of vision and hearing in all learning (e.g.
communication, concept development, motor development and movement). The complex and
unique effects of combined vision and hearing losses upon all learners who are deaf-blind(e.g.
communication, challenges in accessing information, orientation and mobility, diversity within
the population of learners who are deaf-blind(e.g. differing etiologies; varying ages of onset of
deaf blindness, varying degrees of vision and hearing losses, additional disabilities among others.
On personal identity, relationships and self- esteem, the teacher should have knowledge on the
potential impact of deafblindness upon attachment bonding between learners who are deaf-blind
and their primary care givers among others. On concept development the teacher should have the
knowledge and skills on the potential impact of the combined effects of vision and hearing losses
upon the development of concrete and abstract concepts. On communication, the teacher should
have knowledge and skills on the development of communication partnerships between learners
who are deaf-blind and others for instance, assessing and adapting to learners pace/timing of
communication e.g. (considering physical limitations, vision and hearing losses, processing time,
motor planning and medical conditions) among other skills. On hearing-vision, the teacher
should have knowledge and skills on the structure and functions of auditory and visual systems
and how they interrelate in the learning process. For example, assessing and explaining the
educational implications of visual and auditory impairments‟ upon the learner among other
skills. On orientation and mobility, the teacher should have knowledge and skills on the
influence of vision and hearing in motor development. For example, collaborating with
orientation and mobility specialists and other appropriate specialists (e.g. occupational therapist,

85
physical therapist), in adapting strategies to encourage the learner to move safely and
independently. The teacher should have knowledge on technology to enhance orientation and
mobility skills among others.
On environment and materials the teachers have knowledge on the visual, auditory, tactile and
olfactory information in various environments that influence learning. Some of the skills the
teacher should have include; making appropriate visual adaptations to accommodate for specific
visual impairments‟(e.g., reducing lighting for learners with Colobomas,increased lighting in
dark areas for learners with retinitis pigmentosa, making appropriate adaptations to enhance the
learner‟s auditory functioning in a variety of physical environments(e.g., background noise
reduction, volume modification and adjustment of room acoustics(addition of carpet, draperies
etc]among other skills. On professional issues, the teacher should have knowledge on the history
of practices, people and events that have impacted or impact the lives of people who are deaf-
blind and their possible relevance to current educational practices. The teacher should have
knowledge on resources of support services (e.g., interpreters, counselors, intervenors) for
learners who are deaf-blind and their families; curricula specific to, or adapted for learners who
are deaf-blind(e.g. daily livingskills,vocational,earlyintervention;provide information and
education to team members including families about the uniqueness of the disability of deaf
blindness among others. According to Boyce & Hammond (1996), the competencies of teachers
educating learners with autism blindness should have the opportunity to develop the core skills
that enable them to teach all learners. These core skills include; planning and teaching for
inclusion and access to the curriculum, behavioural management and an awareness of the
emotional and mental health needs of pupils (to build their self-esteem as learners) assessment of
learning skills, and understanding of when professional advice is needed and where to find it,
designing an appropriate learning environment, development of language and designing of
appropriate learning and communication environments. According to Leyser (1985), the
competencies needed by special and general educators for providing an appropriate education for
disabled children include areas such as general competency areas of professional orientation,
knowledge, Curriculum, instructional strategies, learning resources, assessment, evaluation of the
student‟s progress, classroom management and communication. Other competencies often listed

86
are learning styles, motivation, administration, referral, professional values, goal setting, and
classroom climate and acceptance.
According to the National policy on special needs (2009) a ministry of education policy, there is
lack of sufficient trained personnel for curriculum development. In addition, there are no clear
staffing norms and recommendation on pupil teacher ratios in institutions and programmes for
special needs education. There is inadequate provision of trained teachers in SNE and other
personnel. Most of these personnel lack adequate skills and knowledge for effective service
delivery. Most training institutions do not address the SNE learners in their training approaches.
Kochung Report (2003) found that 80% of the teachers working with children with special needs
in education are not trained in SNE. Lack of trained SNE teachers was noted as a critical issue
that is affecting the provision of special needs educational service. The Kochung Report (2003)
found out that only 20% of teachers in special needs educational programmes are trained in SNE.
It was further noted that with the exception of the graduates from Maseno University, most of
these teachers lack the necessary proficiency in Kenyan sign Language and Braille. According to
the Kochung Report on special Needs Education Appraisal Exercise (2003), there was lack of
statistical data on special needs education, hence the need for training and in servicing of
teachers. A survey by Kenya Institute of Special Education (1987), on the training needs of
teachers in special schools and programmes in Kenya to establish the levels of trained; gender
and type of trainings in the special schools revealed that a good number of teachers in the special
institutions have no basic training in special education. Insufficient number of trained teachers
has an effect on teacher-learner ratio in learning institutions. The study sought to find out the
training needs of teachers educating learners with multiple disabilities in the counties of Baringo
Kisumu Kiambu and Nairobi.
Summary of the reviewed studies
In this chapter, relevant literature was reviewed regarding teaching strategies used by teachers to
enhance learning among learners with deaf blindness, autism blindness and cerebral palsy
intellectual disability in four selected counties in Kenya. The chapter has reviewed literature
generally on teaching strategies for learners with multiple disabilities and particularly in Kenya.
Many of the primary sources from other countries were on the teaching strategies for learners
with deaf blindness and autism blindness. The studies were crucial in this study because it was
investigating the instructional methods for learners with multiple disabilities in four selected

87
counties in Kenya. The present study intended to verify whether the same instructional methods
can be applicable in our Kenyan educational settings. The studies done in Kenya by Shettle,
(2004), KIE, (I980), Kochung Report, (2003), Deaf blind Pilot project (1992-1996) established
that there were learners with multiple disabilities in schools for learners with single disabilities.
However the studies did not cover the teaching strategies that were used by teachers to enhance
learning for learners with multiple disabilities in the counties of Nairobi, Kiambu, Baringo and
Kisumu in Kenya. Without empirical research conducted in the area of teaching learners with
multiple disabilities, it may be difficult to understand their instructional methods, their
curriculum adaptations, their teaching resources, support services and the training needs of
teachers educating learners with multiple disabilities. The current study intended to fill the gaps
by investigating on the instructional strategies, curriculum adaptations, teaching resources,
support services and training needs of teachers to facilitate learning for learners with multiple
disabilities in the selected special schools and units in the counties of Nairobi, Kisumu, Baringo
and Kiambu in Kenya.

88
CHAPTER THREE
METHODOLOGY
3.0 Introduction
This chapter highlights the methodology adopted for the study. This covers; research design,
variables, location of the study, target population, sampling techniques and sample size,
construction of research instruments, pilot study, validity, reliability, data collection techniques,
data analysis, logistical and ethical considerations.
3.1 Research design
The study adopted a triangulation mixed methods design. The use of both qualitative and
quantitative approaches is a triangulation as noted by (Denzin, 1994; Patton, 2002; Creswell &
Plano Clark, 2011). “A mixed method is defined as a research in which the investigator collects
and analyzes data integrates the findings, and draws inferences using both quantative and
qualitative approaches in a single study or a programme of inquiry” (Tashakkori & Creswell,
2007b, p.4). The purpose of a triangulation in this study was to simultaneously collect qualitative
data from the interviews and observations and quantative data from questionnaires, merge the
data and use the results to understand the teaching strategies used by the teachers educating
learners with multiple disabilities (Creswell & Plano Clark, 2011). One data form supplies
strengths to offset the weaknesses of the other form (Denzin, 1994; Creswell & Plano Clark,
2011; Patton, 2002). Morse (1991), States that the purpose of a triangulation mixed method is to
obtain different but complimentary data on the same topic” p.122.
Creswell & Plano Clark (2011), states that the use of mixed methods is “practical” in that the
researcher is free to use all the methods possible to address a research problem. It is also
practical because individuals tend to solve problems using both numbers and words, combine
inductive and deductive thinking and employ skills in observing people as well as recording
behavior. The use of mixed methods also enhances confidence in the validity of the findings
(Somekh & Lewin, 2005). The qualitative data from the interviews and observations and
quantative data from the questionnaires were used side by side to reinforce, enhance, elaborate or
compliment data from the other source (Creswell& Plano Clark, 2007; Rossman &Wilson, 1985;
Greene, Caracelli & Graham, 1989). The use of qualitative methods allowed study participants to
provide responses that reflected their frame of reference, language and provided richer

89
descriptions that complimented the information gleaned by quantative means (Creswell &Plano
Clark, 2011).
3.2 Variables
The independent variables are the instructional methods, curriculum adaptations, support
services, teaching resources, specialized trained personnel among others. The dependent variable
is learning.
3.3 Location of the Study
The study took place in nine selected special schools and units within the counties of Baringo,
Kiambu, Kisumu and Nairobi in Kenya. The schools were purposively selected because they
have learners with multiple disabilities and their long tradition in handling learners with multiple
disabilities. The schools included: Kabarnet special school for the Deaf blind which was
established in 1980 and is located in Baringo County. It is the only special school for learners
with deaf- blind in Kenya. It has 23 learners, 26 teachers and one head teacher. Kilimani Deaf
blind unit was established in 2002 and is located within Kilimani Primary School in Nairobi
County. Kilimani Deaf- blind unit has 14 learners, 6 teachers and one head teacher. Maseno Deaf
blind unit was established in 1995 and is located within Maseno special school for the Deaf in
Kisumu County. Maseno Deaf blind unit has 13 learners and 4 teachers in the Deaf blind unit
and one head teacher. Special schools and units where learners with autism blindness can be
found include: Kibos School for the blind which was established in 1963. It has 12 learners in the
“special class” and 2 teachers of the “special class‟‟ and one head teacher. It is located in
Kisumu County. Thika School for the blind was established in 1962 and is located in Kiambu
County. It has 10 learners in the “special class” and 3 teachers for the “special class”. Kilimani
unit for the visually impaired was established in 1986 and is located within Kilimani primary
school in Nairobi County. It has 13 learners and 2 teachers in the pre- unit for learners who are
visually impaired and one head teacher. Special schools where learners with cerebral palsy
intellectual disability can be found include: Joy land Special school for the physically disabled
located in Kisumu county and which was established in 1974. It has 23 teachers and 12 learners
with Cerebral palsy intellectual disability and one head teacher. Salvation Army Joy town school
for the physically disabled was established in 1967 and is located in Kiambu County. It has 25
teachers and 16 learners with cerebral palsy intellectual disability and one head teacher. Nile
Road special school for the physically disabled was established in 1969. It is located in Nairobi

90
County. It has 25 teachers and 13 learners with cerebral palsy intellectual disability and one head
teacher.
3.4 Target Population
A target population is a group of individuals with some common defining characteristic that the
research can identify and study. It is within the target population a sample is selected (Creswell,
2008; Orodho, 2008). The target population for this study was made up of teachers educating
learners with deaf-blind, autism blindness, cerebral palsy intellectual disability, and head
teachers in the selected special schools and units within the counties of Baringo, Kiambu,
Kisumu and Nairobi in Kenya. The total target population in the four counties representing
learners with deaf-blind was 36 comprising of 33 teachers, and 3 head teachers. The total target
population in the four counties representing learners with autistic blind was 10 comprising of 7
teachers, and 3 head teachers. The total target population in the four counties representing
learners with cerebral palsy intellectual disability was 77 comprising of 74 teachers, and 3 head
teachers. The total target population for learners with multiple disabilities was 123.

91
TABLE 3.1
Study Frame Work for the Target Population
3.5 Sampling Techniques and Sample Size
3.5.1 Sampling Techniques
The study adopted purposive non random sampling to select the sample. Non random sampling
is that sampling procedure which does not afford any basis for estimating the probability that
each item in the population has, of being included in the sample (Krathwol, 2006). Purposive
sampling was used to sample teachers and head teachers.‟ Purposive sampling is handpicking the
cases to be included in the sample on the basis of one‟s judgment of their typicality. In purposive
sampling, the goal is to select cases that are likely to be “information rich” with respect to the
purposes of the study. The intent is to achieve an in-depth understanding of selected individuals
(Creswell, 2008; Orodho, 2005; Kombo & Tromp, 2006 &Mugenda, 2008). In Kabarnet Special
School for the deaf-blind, 6 teachers were sampled on the basis that they had Diploma training
on deaf blindness from Kenya institute of Special Education. Four other teachers were
purposively sampled on the basis of more teaching experience on deaf blindness. In Maseno
Deaf blind unit, all the 4 teachers teaching learners with deaf-blind were purposively sampled. In
Multiple
disabilities.
Teachers
Head
teachers
Target
population
Deaf-
Blind
33 3 36
Autism
Blindness
7 3 10
Cerebral
Palsy
Intellectual
disability
74 3 77
Total 117 9 123

92
Kilimani Deaf blind Unit, all the 6 teachers teaching learners with deaf-blind were sampled. In
Thika school for the Blind, 3 teachers teaching in the „„special class‟‟ for learners with multiple
disabilities were sampled on the basis of teaching experience. At Kibos School for the Blind, the
two teachers teaching learners with autism blindness were selected on the basis of teaching
experience. At Kilimani Unit for the visually impaired, the 2 teachers in the special unit were
selected on the basis of teaching experience. In Joyland special school for the learners with
physical impairment, ten teachers were sampled on the basis of teaching learners with multiple
disabilities who are in the “Special Class” in the school. In Salvation Army Joy town special
school for learners with physical impairment, 10 teachers were selected on the basis of teaching
learners with multiple disabilities in the “Special Class”. In Nile Road special school for learners
with physical impairment, 10 teachers were selected on the basis of teaching learners with
multiple disabilities in the “Special Class”.
Table 3.2 Sample size
Multiple
disabilities
Teachers
Head
Teachers
Sample
size
Deaf Blindness 20 3 23
Autism Blindness 7 3
10
Cerebral palsy
intellectual
disability
30 3 33
Total 57 9 66

93
3.5.2 Sample Size
The number of teachers of deafblindness was 23. The number of teachers of learners with
autism blindness was 10. The number of teachers of cerebral palsy intellectual disability was 33.
The total sample size for the study was 66 comprising of 9 head teachers and 57 teachers.
3.6 Construction of Research Instruments
The study used researcher made interview guides, questionnaires with a Likert scale and an
observation guide. The interviews were constructed using a pre-determined set of questions.
Semi structured, open ended questions were used because they encourage a free response from
the participants (Creswell, 2008). The first question item on the interviews was to provide
information on the instructional methods used by teachers for learners with multiple disabilities
namely, deaf blindness, cerebral palsy intellectual disability and autism blindness. The second
question item was to provide information on curriculum adaptations that had been effected for
learners with deaf blindness, autism blindness and cerebral palsy intellectual disability. The third
question item was to provide information on the teaching resources for learners with deaf
blindness, autism blindness and cerebral palsy intellectual disability. The fourth question item on
the interview schedule was to provide information on the support services offered to learners
with deaf blindness, cerebral palsy intellectual disability and autism blindness.
The fifth question item was to provide information on the training needs of teachers teaching
learners with deaf blindness, autism blindness and cerebral palsy intellectual disability. Follow-
up questions or probes were included in the items. According to Spradley (1980) probes or
follow up questions are important in an interview to clarify the initial questions and to provide an
alternative answer to a question. An observation guide was constructed to guide the researcher
to observe and collect information on the instructional methods used by teachers educating
learners with deaf blindness, cerebral palsy intellectual disability and autism blindness, how the
teachers developed an individualized education programme, the teaching resources, support
services, specialized equipment, classroom organization, the curriculum used, and the physical
environment of the schools serving learners with multiple disabilities. Observations enabled the
researcher to record information as it occurred in schools (Creswell, 2008). Observation is the
process of gathering open-ended, first hand information by observing people and places at a

94
research site. The researcher adopted the role of a participant observer to take part in the
activities in the setting (Spradley 1980). Observations can effectively complement other
approaches and thus enhance the quality of evidence available to the researcher. The
observations may be more valid than questionnaires or interviews (Malhotra, 2006). Interviews
and the observations enabled the researcher to gather qualitative data. A questionnaire with a
Likert scale was constructed to enable the researcher to collect quantative data. A questionnaire
is a formalized set of questions for obtaining information from the respondents. A Likert Scale is
the most popular attitude scale type which measures subjective variables (Kothari, 2004). The
Likert scale was constructed after reviewing the literature. The first step in designing the Likert
Scale was to define the attitude to be measured (Yount, 2006).
In this study the researcher measured the attitude or the opinion of the respondents‟ on the
instructional methods they used for learners with deaf blindness, autism blindness and cerebral
palsy intellectual disability. The response format was a five point Likert type scale and consisted
of 67 items, fifteen of which were demographic questions. Three questionnaires were constructed
for the three multiple disabilities namely; deaf blindness, autism blindness and cerebral palsy
intellectual disability. The Likert Scale for learners with deaf blindness consisted of 19 items and
5 demographic questions while that of learners with autism blindness consisted of 17 items and
5 demographic questions and that of learners with cerebral palsy intellectual disability consisted
of 16 items and 5 demographic questions. The questionnaire with a Likert Scale consisted of a
number of statements followed by several levels of agreement, strongly agree, agree, no opinion,
disagree and strongly disagree. The respondent indicated his or her agreement or disagreement
with each statement in the instrument by ticking an appropriate number. Each response was
given a numerical score, indicating its favorableness, and the scores were totaled to measure the
respondent‟s attitude. A score of 1 denoted strongly disagree, score of 2 denoting disagree, score
of 3 denoting undecided, score of 4 agree and score of 5 strongly agree. Scores above 3 denoted
that teachers engaged in various instructional methods while scores of below 3 denoted that
teachers rarely or never used the various instructional methods. Each of the 3 questionnaires
with a Likert Scale was divided into two sections containing close ended and open ended
question items. The close ended items enabled the researcher to obtain demographic information
such as gender, number of years in the school, teaching experience and professional

95
qualification, while the open ended questions assisted the researcher to gather information
relating to the respondents opinion on the instructional methods they used for learners with
multiple disabilities. Creswell (2008) and Morgan (1985) underscore the importance of using a
variety of interview schedules to collect data from a population for colloborative information.
The questionnaire enabled quantative data to be collected in a standardized way so that data are
internally consistent and coherent for analysis. A questionnaire ensures standardization and
comparability of data across interviewers, increase speed and accuracy of recording and
facilitates data processing (Malhotra, 2006; Creswell, 2008).
3.7 Pilot Study
Prior to the actual data collection, the three research instruments, that is the interview guide,
observation guide and a questionnaire with a Likert scale were subjected to a test on their
validity and reliability through a pilot study. Piloting enabled the researcher to check for
ambiguity and appropriateness of sentence structure of the question items in order to get similar
responses from all respondents (Orodho, 2005; Creswell, 2008; Kothari, 2004). Piloting enabled
the researcher to evaluate the suitability of the instruments especially on the clarity of
instructions contained in the instruments question items and the relevance of the question items.
The responses from the pilot study were analyzed and items with ambiguities addressed
appropriately. Piloting also enabled the researcher to detect any flaws in the administration of the
research instruments (Wiersma, 1986). The purpose of piloting was to discover weaknesses in
the instruments, check for clarity of the questions or items and also elicit comments from
respondents that assisted in the improvement and modification of the instruments.
The researcher piloted the research instruments in three schools with similar characteristics to
the research sample, but not including the special schools and units in the actual study. Piloting
was done at Kitui Deaf blind unit, St. Lucys‟ School for the blind and at Masaku special school
for learners with physical impairments. Five teachers of Kitui Deaf blind unit were asked to
answer research questions from the interview guide, and in the questionnaires with a Likert scale.
The head teacher answered questions from the interview guide. Ten teachers of Masaku Special
School were asked to answer the questions from the interview guide and the questionnaire with a
Likert scale. Two teachers of St. Lucys‟ School for the blind answered the questions from the

96
interview guide and the questionnaire with a Likert scale. The head teacher answered questions
from the interview guide. The researcher did the observations using the observation guide.
3.7.1 Validity
Validity is the extent to which a test measures what it is supposed to measure (Creswell, 2008;
Gay, 2003&Orodho, 2005). Content related validity was used as a measure to determine validity.
Content validity refers to the degree to which the sample of the test represents the content that
the test is designed to measure (Donald, 2003). Given that content validity is examined by expert
judgment (Creswell, 2008), the interviews, observation guide and a questionnaire with a Likert
Scale were scrutinized and approved by expert lecturers in special education. The question items
should measure what they are supposed to measure (Kombo and Tromp, 2006; Orodho, 2005;
Mugenda& Mugenda, 1999; Creswell & Plano Clark, 2011). Content related validity was used to
evaluate the extent to which the question items were clearly understood by the respondents to
enable them give responses to the issues raised in the question items concerning the teaching
strategies used by the teachers for learners with multiple disabilities.
3.7.2 Reliability
Reliability is the degree to which approximately the same results would be obtained if the test
were administered again. It is the consistency with which the test measures what it is supposed to
measure. Unless a test is valid it cannot be reliable (Creswell, 2008; Orodho, 2005). In this study,
reliability was determined by the test- retest method. (The same test was administered to the
same group after a lapse of two weeks). The reliability established when the research instruments
were administered for the first time to the respondents was; Questionnaires 0.61
Interview schedules 0.63
However, when the research instruments were administered to the same respondents a second
time after two weeks the reliability was found to be as follows:
Questionnaires 0.63
Interview schedules 0.65
A comparison of the respondent‟s responses of the two trials was made using Pearson‟s product
moment correlation (r) formula which states that the greater the consistency the higher the

97
reliability of the research instruments (Orodho, 2005; Gay, 2003, Wiersma 1986 &Creswell,
2008). According to Pearson‟s‟ product moment correlation formula shown below, any research
instruments whose co- efficiency range between 0.5 and 1.0 can be considered reliable and can
be used for a research study. Since the research instruments for this study had co-efficiencies
ranging between 0.61 and 0.65 they were considered as reliable and hence used to carry out the
research study. The Pearson correlation was employed to compute the correlation coefficient in
order to establish the extent to which the contents of the interviews and questionnaires were
consistent in eliciting the same responses every time the two instruments were administered.
Pearson product moment correlation formula
3.8 Data Collection Techniques
The researcher used an interview guide, a questionnaire with a Likert scale and an observation
guide to collect data from the respondents. To collect the data, the researcher was assisted by 2
trained research assistants that had previous data collection experience. The researcher and the
two research assistants distributed the questionnaires to the special schools and units. To ensure
efficiency and effectiveness, they agreed on the time and also telephone follow up was done to
remind the respondents. The interview guide was administered by the researcher and the 2
research assistants using an audio-tape and note books for recording the observations. The two
research assistants interviewed teachers in Joyland special school for the physically disabled,
Maseno Deaf blind unit and Kibos School for the Blind. The researcher administered the
interviews at Joy town special school for the physically disabled, Nile Road special school for
the physically disabled, Kilimani special unit for the visually impaired, Karbarnet special school
for the Deaf blind and Kilimani Deaf blind unit. Appointments were set in consultation with the

98
heads of schools and this created consistency in data collection. Care was taken not to interfere
with the normal teaching schedules. The observations were made at the special schools and
special units for learners with multiple disabilities in the following areas: class room
organization, instructional methods, curriculum used, teaching materials, development of an
individualized education programme, physical environment and various support services in use,
among others. The researcher and the research assistants observed the instructional methods
teachers used for educating learners with multiple disabilities during class time in the nine
selected special schools and units for two days a week for every school. The questionnaires with
a Likert scale collected quantative data. The interviews and observations collected qualitative
data.
3.9 Data Analysis
The qualitative data from the interviews and observations were analyzed using descriptions and
thematic text (Creswell & Plano Clark, 2011). Data from the field was organized and transcribed
by typing text from observations and interviews into a word processing document. A preliminary
analysis of the data was conducted by reading through it to obtain a general sense of data. The
data was then coded and codes were used to develop themes in the context of the research
questions. Coding is a major analysis of qualitative data. The process of coding is one of
reducing text database to descriptions and themes. Data was transformed into a simplified form
that could be understood in the context of the research questions (Krathwohl, 1998; Miles &
Huberman, 1994; Flechtling, Sharp & Westat, 1997). The data was grouped into themes using
content analysis and thematic analysis. Content analysis involves coding the data for certain
words or content. Thematic analysis is grouping the data into themes that will help answer
research questions (Taylor-Powell Renner, 2003). After identifying themes the data was
organized in tables. Enumeration was done on the data. Enumeration is the process of
quantifying data. Enumeration was helpful in clarifying words that the researcher used in the
report such as many, some or few. The number helped to clarify what frequency meant. This way
the data helped to identify systematic patterns and interrelationships across themes or content
(Miles & Huberman, 1994; Flechtling et al., 1997).
The findings were reported in narrative discussions or commentary quotes and descriptive
examples from interviews and observations were used to illustrate the points and bring data to

99
life (Asmussen & Creswell, 1995). From the report, the researcher made an interpretation of
meaning of research. Interpretation involves making sense of data or the” lessons learned” as
noted by Lincoln & Guba, (1985). Interpretation was done by making comparisons between the
findings and the literature (Creswell, 2008). The research was then validated through
triangulation as a validation procedure (Creswell & Miller, 2000; Lincoln & Guba, 1985).
Triangulation is a technique for judging the accuracy of data and requires the use of multiple data
sources or multiple data collection (Creswell & Miller, 2000; Lincoln & Guba, 1985). The
collected information from the interviews was used to complement, clarify or colloborate the
quantative data from the questionnaire responses (Patton, 2002; Creswell & Plano Clark, 2007 &
Classen et al., 2007).
The quantative data from the questionnaire with a Likert scale was analyzed using descriptive
statistical analysis. Descriptive statistics involve tabulating graphing and describing data
(Orodho, 2005; Kothari, 2004). Included in the descriptive statistics are frequencies which
showed the number of teachers that responded at each level of the Likert scale, the percentages
of the teachers in each item and the maximum possible score in the form of means and standard
deviation. The researcher using the statistical Packages for Social Sciences (SPSS) computer
programme, standard version 17.0 calculated the mean and standard deviation which were
relevant to the research study so as to compute verifiable findings. According to Kombo &
Tromp (2006) data analysis is complete only when respondents‟ views and opinions have been
incorporated. Data from the observations were analyzed descriptively and interpreted based on
the study objectives. The information from the qualitative and quantative data was then
integrated in the interpretation of the overall results (Creswell, 2009).
3.10 Logistical and Ethical Considerations
The researcher obtained a research permit from the National Council for Science and
Technology (NCST) which was established by the Science and Technology Act.Cap.250 of the
laws of Kenya under the Ministry of Higher Education Science and Technology (MOHEST)
Utalii House, Nairobi through the Dean, Graduate School, and Kenyatta University before
administering the research instruments in the field. The researcher made preliminary visits to the
special schools and special units having learners with multiple disabilities to establish rapport
with the head teachers‟ of the institutions and also to discuss the relevance of the study. Other

100
considerations included, getting informed consent from the respondents before interviewing
them, using information only for disclosed purpose, respecting their right to withdraw at any
time and treating the respondents with dignity.
.

101
CHAPTER FOUR
DATA PRESENTATION ANALYSIS AND DISCUSSION
4.0 Introduction
This chapter presents the demographic data of the respondents and an analysis and interpretation
of data that were collected during the fieldwork. The analysis and interpretation have been done
within the framework of the objectives that this study sought to address. The core objective of
this study was to investigate the teaching strategies used by teachers educating learners with
multiple disabilities in the counties of Baringo, Kiambu, Kisumu and Nairobi in Kenya. The
study findings were presented based on the following study objectives:
i. To investigate the instructional methods used by the teachers educating learners with
multiple disabilities (deaf-blind, autism blindness, and cerebral palsy intellectual
disability).
ii. To find out the curriculum adaptations that had been effected for learners with multiple
disabilities). (deaf-blind, autism blindness, and cerebral palsy intellectual disability).
iii. To find out the available teaching resources for learners with multiple disabilities
(deaf-blind, autism blindness, and cerebral palsy intellectual disability).
iv. To find out available support services for learners with multiple disabilities (deaf-blind,
autism blindness and cerebral palsy intellectual disability).
v. To find out the training needs of teachers educating learners with multiple disabilities).
(deaf-blind, autism blindness, and cerebral palsy intellectual disability).
4.1 Demographic data of the respondents
The study targeted a sample of 9 head teachers and 57 teachers educating learners with multiple
disabilities in the counties of Baringo, Kiambu, Kisumu and Nairobi. Of the 57 teachers, 20
were educating learners with deaf blindness and 3 headteachers, 7 were teaching learners with
autism blindness and 3 were head teachers while 30 teachers were educating learners with
cerebral palsy intellectual disability (CPID) and 3 head teachers.

102
Table 4.1: Teachers’ professional qualification across gender
Professional
qualification
Deaf- blind Autistic blind Cerebral
palsy
intellectual
disability
M F M F M F No. %
Certificate (SNE) 0 0 0 0 0 1 1 1.8
Diploma (SNE) 8 2 0 0 1 7 18 31.5
Degree (SNE) 2 6 1 5 1 15 30 52.6
M.E.D (SNE) 0 2 0 0 0 5 7 12.3
ECDE 0 0 0 1 0 0 1 1.8
Total 10 10 1 6 2 28 57 100.0
As shown in Table 4.1, majority of the teachers, 30 (52.6%) had attained a Degree in Special
Needs Education, followed by 18 (31.5%) who had a Diploma in Special Needs Education.
There were 7 (12.3%) teachers with Masters‟ degrees in Special Needs Education while one
teacher (1.8%) had a Certificate in Special Needs Education and Early Childhood Education
certificate. Teachers‟ professional qualifications have implications on the teaching strategies
used in educating learners with multiple disabilities. The majority of the teachers had Bachelors
or Masters Degrees in Special Needs Education in a specific disability while some few teachers
had a Diploma in deafblindness. Among the 57 teachers, 44 (77.2%) were females while 13
(22.8%) were males. The table further shows that there were an equal proportion of male and
female teachers teaching learners with deaf blindness However, there were more female than
male teachers among those teaching learners with autism blindness and cerebral palsy
intellectual disability. Teachers interrogated said that male teachers perceive teaching as a career
for the female and they don‟t like performing activities such as, bathing, toileting, feeding and
diapering learners with multiple disabilities. The finding that there were more female than male
teachers in the sample is supported by previous research such as Rice & Goessling (2005) and
Wood (2012). Rice and Goessling (2005) found that the percentage of male students who
complete an undergraduate degree in the field of special education continues to be much lower

103
than that of female graduates. They further established that low status, low salaries, the
perception of teaching as women's work, potential complaints of child abuse and sexual
harassment, and a lack of male peer group factor into this low percentage. Rice and Goessling
(2005) argued for the need to train and recruit more male teachers to be positive role models for
all children. Similarly, Wood‟s (2012) study recommended that more male teachers are needed
not only in special education settings but all elementary schools in general.
Table 4.2: Teachers experience across learners’ impairments.
Teaching
Experience
Learners’ impairments
Deaf- blind Autistic blind Cerebral
palsy
intellectual
disability
Total
%
5-10 years 5 2 1 8 14.0
11-15 years 13 3 25 41 72.0
16 years and above 2 2 4 8 14.0
Total 20 7 30 57 100.0
Table 4.2 shows that majority 41 (72%) of the teachers had taught for 11-15 years while 8 (14%)
each had working experience of 5-10 years and 16 years and above. It is therefore clear that
majority of the teachers had over 10 years of teaching experience.
4.2 Instructional Methods used to Educate Learners with Multiple Disabilities
The first objective of the study was to investigate the instructional methods used by the teachers
educating learners with multiple disabilities. (deaf-blind, autism blindness, cerebral palsy
intellectual disability). To address this objective, teachers were asked to indicate on a five-point
Likert scale various instruction methods they engaged in when educating learners with multiple
disabilities. The responses on the scale ranged from Strongly Agree to Strongly Disagree with a
score of 1 denoting strongly disagree, score of 2 denoting disagree, score of 3 denoting
undecided, score of 4 agree and score of 5 strongly agree. The mid-point of the scale was a score
of 3 indicating that one was neutral. Scores above 3 denoted that teachers engaged in various

104
instructional methods while scores below 3 denoted that teachers rarely or never used the various
instructional methods.
Table 4.3: Instructional methods used for Learners with deaf blindness
Instructional methods SA A UN D SD Mean Std
Dev. f % f % f % f % f %
Use of real objects 20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Task analysis 20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Hand over hand guidance, tactual
sign language
20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of speech paired with
Kenyans sign language
20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Tadoma/body language/lip
reading
20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.0 .000
Use of Kenyan sign language 20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of object of reference 20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of Lilli Nielsen resonance
board
20 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of teaching teachable
moments
19 95.0 1 5.0 0 0.0 0 0.0 0 0.0 4.95 .224
Use of speech paired with Braille 18 90.0 2 10.0 0 0.0 0 0.0 0 0.0 4.90 .308
Use of routine, calendar system
and discussion boxes
18 90.0 2 10.0 0 0.0 0 0.0 0 0.0 4.90 .308
Use of experience and picture
board
18 90.0 2 10.0 0 0.0 0 0.0 0 0.0 4.90 .308
Behavior management 2 10.0 14 70.0 4 20.0 0 0.0 0 0.0 3.90 .553
Use of tactile diagrams 3 15.0 11 55.0 3 15.0 3 15.0 0 0.0 3.70 .923
Making a choice 0 0.0 1 5.0 11 55.0 3 15.0 5 25.0 2.40 .940
Use of Deaf blind manual 2 10.0 0 0.0 0 0.0 1 5.0 17 85.0 1.45 1.234
Key: SA-Strongly Agree A-Agree UN-Undecided D-Disagree SD-Strongly Disagree
As shown in Table 4.3, the mean scores obtained by the teachers ranged from 5.00 to 1.45.
Teachers obtained mean scores of 5.00 in ten of the methods listed in the table, meaning that

105
they strongly agreed they used them when educating learners with deaf blindness. These methods
included; use of real objects; task analysis; tactual Kenyan sign language; Tadoma, lip reading,
body language; use of speech paired with Kenyan sign language; use of Kenyan sign language;
use of object of reference; and use of Lilli Nielsen resonance board. Results revealed that
teachers were using a variety of instructional strategies when teaching learners with deaf
blindness. This shows that learners had a diversity of needs. This is supported by Porter et al.,
(1997) whose study on curriculum access to deaf-blind children found the need for teachers to
have access to a wide range of specialist strategies especially where they are working with pupils
with the most complex needs whereby there is need for teachers to be able to adapt more generic
strategies to meet the specific needs of an individual pupil.
Other instructional methods used by majority of the teachers were use of teaching teachable
moments; use of speech paired with braille; use of routine, calendar system, discussion boxes
and use of experience and a communication board. This implies that most of the teachers were
using instructional methods to teach learners with deaf blindness. However, teachers conceded to
not using the deaf blind manual alphabet and teaching learners how to make a choice. The deaf-
blind manual alphabet also known as tactile finger spelling is used in other countries to teach
learners who are deaf-blind to communicate (Huebner, 1995). In Kenya, teachers use the tactile
Kenyan sign language. Teachers also conceded to not teaching learners with deaf-blind how to
make a choice on what they eat. Campbell (1987) emphasizes the need to teach choosing what to
eat where the learner eats. The boundary in which the choice making activity takes place should
be defined through the use of appropriate aids and cues. Providing boundaries minimizes the
visual motor and cognitive requirements of orienting and reaching. The teachers selected certain
modes of teaching and not others because the learner‟s needs dictated the choice of the
instructional methods. For instance, learners who were congenitally deaf-blind without a
cognitive disability and other disabilities could be taught using tactile Kenyan sign language,
Tadoma, use of multi sensory approach, use of object of reference among others. Learners who
were deaf-blind with some residual hearing were taught using braille tactile Kenyan sign
language and speech among others. Learners‟ with deaf-blind with mild intellectual disability
could be taught using tactile Kenyan sign language, task analysis among others. All learners who

106
were deaf-blind regardless of whether they had a cognitive disability or not were taught using the
Lily Nielson resonance board for assessment and stimulation of their senses among others.
Table 4.4: Instructional methods used for learners with autism blindness
Instructional methods SA A UN D SD Mean Std
Dev. f % f % f % f % f %
Use of real objects 7 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of auditory
activities
7 100.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of Braille as a mode
of communication
7 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Orientation and mobility 7 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of supplementary
aids (e.g. slates &stylus,
abacus, cuberithms)
6 85.7 1 14.3 0 0.0 0 0.0 0 0.0 4.86 .378
Use of frequent
stretch breaks
6 85.7 1 14.3 0 0.0 0 0.0 0 0.0 4.86 .378
Use of Kinesthetic
learning activities
6 85.7 1 14.3 0 0.0 0 0.0 0 0.0 4.86 .378
Independent living skills 6 85.7 1 14.3 0 0.0 0 0.0 0 0.0 4.86 .378
Use of tactile
Kinesthetic and auditory
modalities
5 71.4 2 28.6 0 0.0 0 0.0 0 0.0 4.71 .488
Use of consistent
schedules
5 71.4 1 14.3 1 14.3 0 0.0 0 0.0 4.57 .787
Use of large print,
optical devices
3 42.9 3 42.9 1 14.3 0 0.0 0 0.0 4.29 .756
Use of behavior
management strategies
0 0.0 7 100.0 0 0.0 0 0.0 0 0.0 4.00 .000
Use of speech paired
with tactile strategies
3 42.9 1 14.3 1 14.3 2 28.6 0 0.0 3.71 1.380
Use of regular print 1 14.3 1 14.3 0 0.0 3 42.9 2 28.6 2.43 1.512 Use of recorded materials
to communicate 0 0.0 2 28.6 0 0.0 0 0.0 5 71.4 1.86 1.464
Use of two handed sign
language paired with
speech.
0 0.0 0 0.0 0 0.0 0 0.0 7 100.0 1.00 .000
Key: SA-Strongly Agree A-Agree UN-Undecided D-Disagree SD-Strongly Disagree
Table 4.4 above, illustrates that teachers obtained mean scores ranging from 5.00 to 1.00 on the
various methods used to educate learners with autism blindness. Majority of the respondents
obtained scores of above 3, meaning that they applied most of the instructional methods listed in
the table. Methods that were used by all the study respondents were use of real objects,
supplementary aids, and auditory activities, braille as a mode of communication, orientation and
mobility. Other methods used included; use of consistent schedules, use of frequent stretches and

107
use of tactile kinesthetic and auditory modalities. On the other hand, the lowest ranked methods
were; use of two handed sign language paired with speech, behavior management strategies, use
of regular print and use of recorded materials to communicate. Majority of teachers made use of
real objects to teach learners who were autistic blind. The teachers made use of the sense of
touch. It was difficult to teach learners with autism blindness who had communication
difficulties since teachers had only been trained to specifically teach braille.

108
Table 4.5: Instructional methods used by teachers to educate learners with
Cerebral palsy intellectual disability
Instructional
methods
SA A UN D SD Mean Std
Dev. f % f % f % f % f %
Breaking down tasks
into simpler activities
30 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of gestures 30 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of observations and
demonstrations
30 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of songs 30 100.0 0 0.0 0 0.0 0 0.0 0 0.0 5.00 .000
Use of pointing 29 96.7 0 0.0 1 3.3 0 0.0 0 0.0 4.93 .365
Use of pictures 28 93.3 2 6.7 0 0.0 0 0.0 0 0.0 4.93 .254
Teachers make use of real
objects
26 86.7 4 13.3 0 0.0 0 0.0 0 0.0 4.87 .346
Use of writing 17 56.7 8 26.7 4 13.3 1 3.3 0 0.0 4.37 .850
Use of group work 7 23.3 7 23.3 9 30.0 6 20.0 1 3.3 3.43 1.165
Use of communication
boards
2 6.7 0 0.0 9 30.0 6 20.0 13 43.3 2.07 1.172
Use of pointers 1 3.3 0 0.0 2 6.7 1 3.3 26 86.7 1.30 .877
Use of the pre-linguistic
milieu teaching
2 6.7 0 0.0 0 0.0 0 0.0 28 93.3 1.27 1.015
Use of pencil grips 1 3.3 0 0.0 0 0.0 1 3.3 28 93.3 1.17 .747
Use of Venn diagrams 1 3.3 0 0.0 0 0.0 0 0.0 29 96.7 1.13 .730
Use of adapted computers 0 0.0 1 3.3 0 0.0 0 0.0 29 96.7 1.10 .548
Use of video and audio
based curriculum
0 0.0 0 0.0 1 3.3 0 0.0 29 96.7 1.07 .365
Use of antecedent
prompting
0 0.0 0 0.0 1 3.3 0 0.0 29 96.7 1.07 .365
Use of page turners 0 0.0 0 0.0 0 0.0 1 3.3 29 96.7 1.03 .183
Use of computer assisted
instruction
0 0.0 0 0.0 0 0.0 0 0.0 30 0.0 1.00 .000
Key: SA-Strongly Agree A-Agree UN-Undecided D-Disagree SD-Strongly Disagree
Mean scores obtained by teachers on instructional methods ranged from 5.00 to 1.00. Teachers
scored above 3 on half of the methods listed in Table 4.5 while on the other half, teachers
obtained mean scores of below 3. The highest ranked methods were; breaking down tasks into
simpler activities, use of gestures, observations and demonstrations, real objects, songs and
pointing. However, the lowest ranked methods were use of; computer assisted instruction, page

109
turners, antecedent prompting, video and audio based curriculum. Task analysis was used by the
teachers to teach learners with mild intellectual disability functional skills and cognitive skills.
Learners with cerebral palsy intellectual disability without communication difficulties could be
taught using rhymes or songs. The cognitive ability of the learners determined the instructional
methods not the motor level.
4.2.1 Teachers’ Views on the instructional methods used for learners with multiple
disabilities.
Instructional strategies enable teachers to build upon knowledge and experience in their areas of
specialization. During the interviews, teachers were asked to indicate methods they used to teach
curriculum based contents to learners with multiple disabilities.
Table 4.6: Teachers’ responses on instructional methods used for learners with
Deafblindness
Instructional methods Frequency(N=20) Percentage
Tactile Kenyan sign language 20 100.0
Use of real objects 19 95.0
Braille paired with speech 19 95.0
Task analysis 19 95.0
Activities of daily living(ADL) 18 90
Nielsen resonance boards 18 90
Tadoma 15 75.0
Calendar boxes/structured boards 15 75.0
Experience books 14 70.0
Kenyan sign language 14 70.0
Total communication/multi sensory approach 14 70.0
Use of prevocational skills e.g. beading 14 70.0
Body language 12 60.0
Use of teachable moments 4 20.0
Use of pointing 2 10.0
Home signs 1 5.0
Table 4.6 above shows that majority of the teachers reported that they used tactile Kenyan sign
language 20 (100.0%). Use of tactile sign language is supported by an attribution made by Aslop
(1993) who stated that communication among learners with deaf-blind can take multiple forms

110
such as gestures, objects, tactile, photos, symbols, sign language and tactile finger spelling. We
use any means to communicate with a learner who is deaf-blind, adapted to the senses he/she can
use. The different modes of communication reflect the person‟s capacities, and the development
of the learner; that is both cognitive potentials of the learner and the senses he can use in
different situations.
Task analysis and Braille paired with speech was cited by 19 (95%) of the respondents when
teaching learners with deaf blindness. Task analysis is supported by Bigge &Best (2005), as
among the most valuable tools available to teachers of individuals with physical, health, or
multiple disabilities and to the learners themselves. The use of the Lily Nielsen Resonance board
was cited by 18 (90%) of the respondents. Nielsen (1998) supports the use of the Lily Nielsen
board as a tool that can help the brain of learners with Deaf-blind integrate motor activity and
listening skills. Activities of daily living were cited by 18 (90%) of the respondents. This study
report is supported by Ellis (1986), who talks about a functional curriculum as an approach that
takes into account the pupils current individual needs and his or her future needs and is designed
to meet his or her needs. It addresses the needs of the learner with Deaf blindness in the
Independent living activities among others.
Tadoma was cited by 15 (75%) of the respondents. The study report is supported Aslop (2002);
NIMH (2003), as a skill used by the congenitally deaf-blind person where the listener places his
or her hand on the cheek of the speaker with the thumb resting on the throat, such that he or she
feels the vibrations and the mouth movements so that he or she is able to follow the conversation.
The use of calendar boxes was also cited by 15 (75%) of the respondents. This is supported by
Moss & Hagood (1995), who said that language among learners with deaf-blind is developed
through the use of routines, calendar systems and discussion boxes. The multisensory approach
and total communication was cited by 14 (70%) of the respondents. The use of Total
Communication is supported by Young (2007); Aslop (1993) & Andreessen et al., (1998) as a
philosophy that advocates for the use of any modes of communication suited to the individual
child in a given situation. The multi sensory approach can be used to teach learners with deaf-
blind. This approach makes use of all sensory abilities of the child that is seeing, touching,
smelling and movement as supported by (Sense International India, 2010). Use of prevocational

111
skills was cited by 14 (70%) of the respondents. Body language was cited by 12 (60%) of the
respondents. The least used instructional methods were use of teachable moments at 4 (20%),
pointing at 2 (10%) and home signs at 1 (5%). Observations that were carried out in schools for
learners with deaf blindness revealed that the instructional methods used by the teachers were
determined by the learner‟s needs. The instructional methods that were commonly used included;
tactile Kenyan sign language, use of real objects, braille paired with speech, task analysis,
activities of daily living, use of Nielsen resonance boards, Tadoma, calendar boxes among
others. The IEP was developed by the teachers without involving the multidisciplinary team as it
is done in other countries; therefore learners were not getting the required support services. In
other countries, an educational team varies according to the educational needs of the individual
learner whom they serve and may change over time as student needs change (Heller et al., 2009).
Table 4.7 Instructional methods used by teachers for learners with autism blindness.
Instructional methods Frequency(N=7) Percentage
Pre Braille activities 7 100.0
Braille 7 100.0
Oral methods 6 85.7
Use of real objects 6 85.7
Singing 4 57.1
Activities of daily living 4 57.1
Prevocational skills 4 57.1
Recitations 3 42.9
Dramatization 3 42.9
From Table 4.7 above, it can be observed that majority 7 (100.0%) teachers reported that they
used, pre-braille and Braille methods to teach learners who are autistic blind. Learners who are
visually impaired will require some preparations as touch readers through the pre-braille
activities as supported by Hatlen (1996). Braille is then taught as a mode of communication. Oral
methods and real objects were also cited as instructional methods to the learners who are autistic
blind at 6 (85%). This is supported by Shaheen (2009), who brailled stories and illustrated with
homemade tactile graphics which often included real objects when teaching a learner who was
autistic blind. Prevocational skills, singing and activities of daily living skills were also cited by

112
4 (57%) of the respondents. Four (57%) of the teachers also said that they were teaching the
activities of daily living to the learners who are autistic blind. Hatlen (1996) supports the
teaching of functional academics skills such as the activities of daily living. Konstanareas (1982)
supports the use of music to learners who are kinesthetic. Kinesthetic learners will tend to lose
connection in class if there is little external movement. The methods that were used by the least
number of teachers were recitations and dramatization at 3 (42.9%). This is due to
communication difficulties among learners with autism blindness. The observations made in
schools for learners with autism blindness confirmed that the majority of teachers used the
following instructional methods namely; use of real objects, pre-braille, braille and activities of
daily living as supported by Shaheen (2009); Hatlen (1996). In two schools prevocational skills
were taught to the learners. Teachers focused on the instructional strategies for learners with
visual impairments‟ because the training they had was specifically on visual impairments.
Teachers were not remediating the problems in the learners brought about by autism such as
communication difficulties, lack of social skills and behaviour disorders among others that were
affecting learning among the learners. In other countries teachers combine teaching methods as
dictated by the learner‟s needs. This finding is supported by Shaheen (2009); Hosken, (2008)
who stated that combination of instructional methods intensifies the learning experiences. The
individualized education programme was developed by the teachers without involving the
multidisciplinary team as it is done in other countries. In other countries, an educational team
will vary according to the educational needs of the individual learner whom they serve and may
change over time as student needs change. Those core team members are those individuals who
are directly involved with the design and daily implementation of the learners educational
programme. For example, core team members for a learner with multiple disabilities could
include the learner, family members, special education teacher, general education teachers,
physical or occupational therapists, speech therapists, classroom teaching assistant, and
community work representative (Heller et al., 2009). The classrooms were partly structured with
minimal use of routines. Some classrooms were small and learning areas were not clearly
defined. A learner with autism blindness requires consistent schedules as supported by Vaughn et
al., (2007); Shaheen, (2009) who have stated that learners with autism may be particularly
challenged when a routine is absent or unpredictable.

113
Table 4.8: Instructional methods used for learners with cerebral palsy Intellectual
disability.
Instructional methods Frequency (N=30) Percentage
Task analysis 29 96.7
Activities of daily living 29 96.7
Real objects(maize, beans and, rice) 29 96.7
Use of songs/rhymes 25 83.3
Oral recitation/rote learning 25 83.3
Prevocational skills 25 83.3
Observation and demonstration 24 80.0
Use of pictures 24 80.0
Use of pointing/gestures 22 73.3
Use of drama 7 23.3
Question and answers 7 23.3
Group work 2 6.7
Home signs 2 6.7
Writing 1 3.3
Discussion 1 3.3
As shown in Table 4.8 above, majority of the teachers educating learners with cerebral palsy
intellectual disability 29 (96.7%) equally reported that they used, task analysis, activities of daily
living and real objects like, maize, beans, stones among others. Task analysis is supported by
Fey et al., (2006) who stated that breaking down larger tasks into their specific component parts
is an effective technique for teaching any number of skills for learners with cerebral palsy
intellectual disability. Activities of daily living were also taught to learners with cerebral palsy
intellectual disability. This is supported by an attribution made by Fey et al., (2006) who says
that in order to fully cater for limitations in intellectual functioning of learners with cerebral
palsy intellectual disability, teachers need to provide instruction in a number of skills outside the
general curriculum. These skills are more functional in nature but are absolutely essential for the
future independence of the individual. The skills areas include money concepts, time concepts,

114
independent living skills, self care and hygiene, community access, leisure activities and
vocational training. Turnbull et al., (2002) supports the use of real materials or actual tools in a
natural environment as an essential component in the effective instruction of learners with
cerebral palsy intellectual disability. Real objects serve to both motivate the learner and facilitate
generalization to multiple environments. Twenty five (83%) of respondents cited the use of
prevocational skills, songs/rhymes, oral recitation and rote learning. Mercer &Mercer (2004)
supports the use of songs or rhymes as a technique that helps a student learn and complete the
task independently. Use of observation demonstration and use of pictures was cited by 24 (80%)
of the respondents. Mercer & Snell (1977); Snell & Brown (2006) & Wrestling (1986) supports
the use of observational learning employing modeling in which correct imitation of a model by
the learner is reinforced and group instruction.
Use of pictures was cited by 24 (80%) of the respondents. Kelly (2005) emphasizes that some
learners with cerebral palsy and intellectual disability can use pictures, and some communication
boards which are designed to match the learner‟s cognitive and receptive language skills and
should be continually monitored and evaluated so that it can be modified with the learner‟s
expanding and changing needs. Twenty two (70%) of respondents cited the use of gestures and
pointing. Kelly (2005) supports the use of gestures and pointing and recommends finding out the
preferred mode of communication for learners with cerebral palsy intellectual disability such as
communicating verbally, using communication boards, gestures, pointing or writing in order for
an education program on communication to be instituted for these learners. The least used
methods were, home signs and group work at 2 (6.7%). discussions and writing at 1 (3.3%). Due
to communication barriers and motor difficulties among learners with cerebral palsy intellectual
disability, discussions, writing and group work may not be possible to many. The observations
made in the schools for learners with cerebral palsy intellectual disability confirmed that the
majority of teachers used the following instructional methods namely; task analysis, real objects,
activities of daily living and prevocational skills among others. Teachers focused more on the
teaching strategies for learners with intellectual impairments‟ without remediating the problems
that were brought about by cerebral palsy that were affecting learning. Learners with cerebral
palsy intellectual disability have communication difficulties, gross motor, behaviour difficulties

115
among others. The learner with cerebral palsy intellectual disability with will require widened
aisles, work surface adaptations, speech therapy, physical therapy among others as supported by
(Pellegrino, 2007;Heller et al.,2009). Individualized education programme was developed by the
teachers alone without involving the multidisciplinary team. This is a cause of concern because
the diverse needs of learners were not met.
4.3 Curriculum adaptations for learners with multiple disabilities
The second study objective sought to find out the curriculum adaptations that had been effected
for learners with multiple disabilities (deaf-blind, autistic blind, and cerebral palsy intellectual
disability). To respond to this objective, teachers and head teachers were asked to indicate
curriculum adaptations that had been implemented in their schools to improve teaching and
learning process of learners with multiple disabilities. In response, 3 (15.0%) of the teachers
educating learners with deaf blindness reported that they had implemented use of drafts while 17
(85.0%) of them did not respond. Drafts are preliminary versions of writing of a curriculum.
Head teachers from the schools of learners with deaf blindness said that they were using the third
draft of an adapted curriculum from KIE. However, all teachers educating learners with autism
blindness and cerebral palsy intellectual disability reported that they had not revised curriculum
programmes in their schools. To confirm teachers‟ responses, head teachers of the schools for
cerebral palsy intellectual disability and autism blindness interviewed reported that their schools
had not revised curriculum used in their respective schools. In one of the schools for learners
with autism blindness, teachers conceded to the use of the syllabus for learners with intellectual
impairments. The observations carried out in schools for learners with autism blindness
confirmed that the curricula used for learners with autism blindness were not adapted to cater for
their diverse needs. The curricula used in two schools was the general curriculum and in one
school, teachers conceded to the use of the curriculum for learners with intellectual impairments.
Observations carried out in schools for learners with deaf blindness confirmed that teachers were
using the final or the third draft of an adapted curriculum from Kenya institute of curriculum
development. Observations carried out in schools for learners with cerebral palsy intellectual
disability confirmed that teachers were using the curriculum for learners with intellectual
disabilities and the general curriculum was used in two schools. Learners with multiple

116
disabilities should follow a specialist curriculum as supported by (KIE, 1987; Kochung Report,
2003).
4.4 Available teaching resources for learners with multiple disabilities
The third objective of the study was to find out the available teaching resources for learners with
multiple handicaps (deaf-blind, autistic blind, and cerebral palsy intellectual disability).
4.4.1 Teachers’ responses on available teaching resources for learners with multiple
Disabilities
Table 4.9: Teachers’ responses on available resources used for teaching learners
with deaf blindness.
Available resources Frequency(N=20) Percentage
Lilly Nielsen box(resonance boards) 17 85.0
Play area 16 80.0.
Calendar boxes/structured boards 16 80.00
Stimulant board 10 50.0
Utensils, basins, soaps,toothbrushes among others 10 50.0
Manila papers 10 50.0
Washrooms 9 45.0
Felt pens 9 45.0
Dining room 9 45.0
Toys (inadequate) 7 35.0
Language room/sensory room 6 30.0
Kitchen 6 30.0
Braillers/braillons 6 30.0
Real objects(maize,beans,rice,stones among others 4 20.0
Experience book 3 15.0
Balls 3 15.0
Workshop 2 10.0
Beadwork 2 10.0
Object of reference 2 10.0
Communication board 1 5.0

117
Table 4.9 above, shows that the most available teaching resources were; Lilly Nielsen box or
Resonance Board 17 (85%), play area and calendar boxes at 16 (80%). Ten (50%) of the
respondents also reported that stimulant boards, utensils, basins, soaps among others and manila
papers were also available. Washrooms, felt pens and dining room were mentioned by 9 (45%)
of the teachers. Other resources mentioned by the teachers included; language room 6 (30%),
sensory room 6 (30%), braillons 6 (30%), real object 4 (20%) experience book and balls 3
(15%), workshop, objects of reference and beadwork were mentioned by 2 (10%) of teachers and
communication boards at 1 (5%). The study found out that some teaching resources were
inadequate. This is supported by Kochung Report (2003) which found out most schools were
operating with barely basic learning aids. For instance, the materials to be used in the workshops
were not there, so learners who were benefitting from the vocational training could not access the
skills so they remained in schools doing nothing. The observations carried out on teaching
resources in schools for learners with deaf-blind revealed that teachers mainly used; real objects,
Lilly Nielsen boards, use of beads, buckets, toothbrushes, braillers among others. In the
classrooms, there were some tables, forms and chairs. Some learners had reading stands. In one
school, there was a workshop but nothing was going on because there were no materials to use.
The teaching resources were inadequate. There were no specialized equipment. Schools for
learners with deaf blindness will require specialized equipment like the adaptive computers with
a Braille display, among others as supported by Moss&Hagood, 1995). These equipment can go
a long way in helping learners‟ access education. In some schools, the physical environment was
barrier free especially in the special schools that were not integrated. The Kochung report (2003)
found that the physical environment in special schools was not barrier free.

118
Table 4.10: Teachers’ responses on available resources used for teaching learners
with autism blindness
.
Available resources Frequency(N=7) Percentage
Braillers 7 100.0
Abacus 7 100.0
Braille papers 6 85.7
Toys 4 57.1
Cubarithims (inadequate) 4 57.1
Peg boards 3 42.9
Real objects 2 28.6
Charts 1 14.3
Talking computers (inadequate) 1 14.3
Talking toys 1 14.3
Blocks 1 14.3
Table 4.10 shows that the most available resources used to teach learners with autism blindness
were; braillers and Abacus at 7 (100%) and braille papers at 6 (85.7%). Other resources
available in most schools were toys and cubarithims at 4 (57%) and peg boards at 3 (42.9%).The
least used teaching resources included; real objects at 2 (28.6%), charts, talking computers,
talking toys and blocks at 1 (14.3%) respectively. Some of the teaching resources like cubarithms
and talking toys were inadequate as supported by the Kochung Report (2003), which found
teachers working barely without teaching resources. The observations carried out in schools for
learners with autism blindness on the teaching resources confirmed that majority of teachers
used real objects,braillers,braille papers,abacus,toys, white canes,buckets,utensils among others.
The teaching resources were inadequate.

119
Table 4.11: Teachers’ responses on available resource used for teaching learners
with cerebral palsy intellectual disability
Available resources Frequency(N=30) Percentage
Real objects(rice,beans,stones and maize) 21 70.0
Beadwork 20 66.7
Manila papers 19 63.3
Felt pens 17 56.7
Abacus 16 53.3
Buckets 11 36.7
Plasticine 9 30.0
Candles 8 26.7
Blocks 7 23.3
Tooth brushes 6 20.0
Mirrors 6 20.0
Mobility aids 5 16.7
Counters 5 16.7
Textured board 4 13.3
Toys 3 10.0
Pictures 2 6.7
Exercise books/ pencils 1 3.3
Dolls 1 3.3
Large printed books 1 3.3
Walking frame 1 3.3
Table 4.11 illustrates real objects 21 (70.0%) were the most available resources used to teach
learners with cerebral palsy intellectual disability followed by bead work 20 (66.7%) and manila
papers 19 (63.3%). Seventeen (56.7%) of the respondents cited the availability of felt pens.
Abacus was mentioned by 16 (53.3%).Other resources used included; buckets 11 (36.7%),
plasticine 9 (30%), candles 8 (26.7%), blocks 7 (23.3%),
tooth brushes and mirrors 6 (20%), mobility aids and counters 5 (16.7%), texture board 4
(13.3%) andtoys3 (10%) However, it emerged that the least available resources were; exercise
books/ pencils, dolls, large printed books and walking frame at 1(3.3%).

120
Observations carried out in schools for learners with cerebral palsy intellectual disability
confirmed that the teaching resources used in the schools included real objects such as rice,
maize beans and blocks. The teaching resources were inadequate as supported by Kochung
Report (2003) which revealed that teachers were working barely without teaching materials.
There were no specialized equipment like adapted computers, prone standers, mechanical lifts,
electronic page turners, shelf liner among others. These equipment can go a long way in
enhancing access to education, mobility and independence among learners with cerebral palsy
intellectual disability. Some schools had a television set and some few computers which were not
used because teachers not computer literate.
4.4.2 Head teachers’ responses on availability of teaching and learning resources
Head teachers from the three sampled schools were asked to indicate available resources in their
schools used to teach learners‟ with multiple disabilities. During the interview 2 (66.7%) out of
the three heads of schools for learners with deaf blindness reported that the most available
resources in their schools were Nielsen box, threading, beadwork, basins of ADL, braillers,
language room, manila papers, real objects felt pens, structured boards, calendar boxes and
stimulant boards and sensory room. Other resources mentioned but were not common in most
schools included; Braille papers, goal balls, toys, and communication boards‟ at1 (33%). All 3
(100.0%) heads of schools for learners with autism blindness interviewed reported that Braillers,
Braille papers and white canes were available. Other resources reported though they were not
common in all the three sampled schools were; peg boards, cubarithms, communication devices
and bead work at 1(33.3%). Observations carried out in schools for learners with autism
blindness confirmed that there were braillers, braillepapers, cubarithms, abacus, real objects and
white canes as teaching resources. During the interview, one of the respondents was asked to say
why the teaching resources were inadequate and this was the response, “The funds we receive
per year is just two thousand shillings per student which is not enough to cater for their needs.
The government should increase the money because some resources such as braillers cost
seventy thousand shillings.” All the three (100%), heads of schools for learners with cerebral
palsy intellectual disability said that, real objects were available for teaching learners with
cerebral palsy intellectual disability. Two out of three heads of schools (66.7%) reported that

121
adapted pens, adapted utensils, Abacus, beadwork and blocks were available in their schools.
Resources that were not available in most schools included; special furniture, special pencils,
exercise books, pictures, plasticine, mirrors and walking frames at 1(33.3%) respectively.
Observations carried out in schools for learners with cerebral palsy intellectual disability on
teaching resources confirmed that the teaching resources that were commonly used by the
teachers included; real objects (maize, beans, rice), pictures and blocks. The teaching resources
were inadequate as supported by Kochung Report (2003) which stated that teachers were
working barely without materials.
4.5 Support services for learners with multiple disabilities.
The fourth objective of the study was to find out available support services for learners with
multiple disabilities (deaf-blind, autism blindness and cerebral palsy intellectual disability
(CPID). To answer this research question, study respondents were asked to indicate support
services offered to learners in their respective schools. Nine (45%) of teachers interviewed
reported that learners with deaf blindness were supported by given services by an occupational
therapist. Four (20%) of teachers reported the services of a physiotherapist. Two (10%) reported
that the physiotherapist services were inadequate. One (5.0%) of teachers reported that
occupational therapy was offered but it was inadequate. Related services such as occupational
and physiotherapy are supported by Martinez & Moss (1998). However the support services
were inadequate as supported by the Kochung Report (2003) which found that the support
services from professionals were lacking in the education system. This is a cause of concern
because there are so many learners who are in dire need of support services but they are
unavailable. In the long run these learners may not access appropriate education. In relation to
this,10 (50%) of the teachers recommended that the school administration should ensure that all
the necessary support services for learners with deaf-blind such as speech therapy, sensory
integration, among others are availed effectively to enhance their academic performance.
The observations carried out in schools for learners with deaf blindness revealed that the support
services that were offered included; the related support services of an occupational therapist who
was only one in one of the schools. The occupational therapist was only one serving learners
with deaf blindness and other learners with other disabilities. In another school the
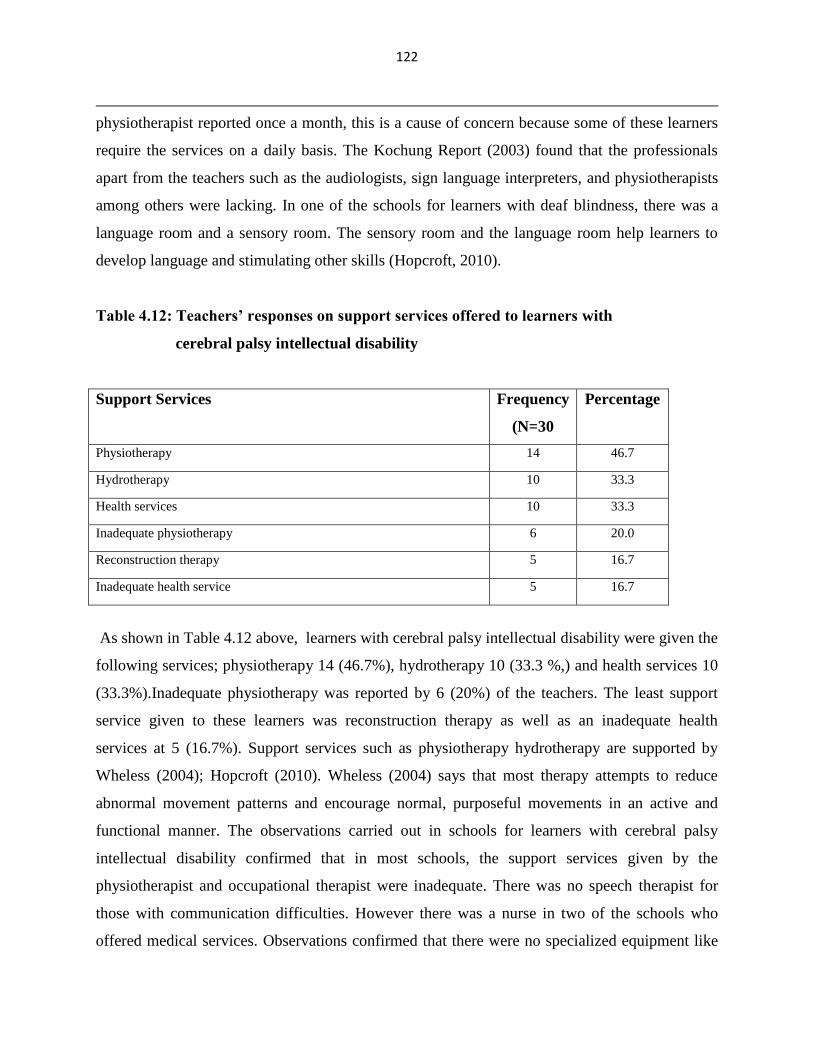
122
physiotherapist reported once a month, this is a cause of concern because some of these learners
require the services on a daily basis. The Kochung Report (2003) found that the professionals
apart from the teachers such as the audiologists, sign language interpreters, and physiotherapists
among others were lacking. In one of the schools for learners with deaf blindness, there was a
language room and a sensory room. The sensory room and the language room help learners to
develop language and stimulating other skills (Hopcroft, 2010).
Table 4.12: Teachers’ responses on support services offered to learners with
cerebral palsy intellectual disability
Support Services Frequency
(N=30
Percentage
Physiotherapy 14 46.7
Hydrotherapy 10 33.3
Health services 10 33.3
Inadequate physiotherapy 6 20.0
Reconstruction therapy 5 16.7
Inadequate health service 5 16.7
As shown in Table 4.12 above, learners with cerebral palsy intellectual disability were given the
following services; physiotherapy 14 (46.7%), hydrotherapy 10 (33.3 %,) and health services 10
(33.3%).Inadequate physiotherapy was reported by 6 (20%) of the teachers. The least support
service given to these learners was reconstruction therapy as well as an inadequate health
services at 5 (16.7%). Support services such as physiotherapy hydrotherapy are supported by
Wheless (2004); Hopcroft (2010). Wheless (2004) says that most therapy attempts to reduce
abnormal movement patterns and encourage normal, purposeful movements in an active and
functional manner. The observations carried out in schools for learners with cerebral palsy
intellectual disability confirmed that in most schools, the support services given by the
physiotherapist and occupational therapist were inadequate. There was no speech therapist for
those with communication difficulties. However there was a nurse in two of the schools who
offered medical services. Observations confirmed that there were no specialized equipment like

123
adapted computers, prone standers, mechanical lifts, electronic page turners, shelf liner among
others. These equipment can go a long way in enhancing access to education, mobility and
independence among learners with cerebral palsy intellectual disability. Some schools had a
television set and some few computers which were not used because teachers were not computer
literate.
Teachers educating learners with cerebral palsy intellectual disability were asked to say their
recommendations on the support services given. Four (13.3%) teachers suggested that learners
should be offered with speech therapy. Four (13.3%) teachers suggested physiotherapy. Four
(13.3%) teachers suggested adequate health services and three (10.0%) teachers suggested
hydrotherapy. Other services that needed to be improved on were, occupational therapy 2
(6.7%) and reconstruction therapy at 1 (3.3%) respectively. One (33.3%) out of the three heads
of schools for learners with deafblindness interviewed, reported that deaf-blind learners were
offered with transport services, another 1(33.3%) head of school reported that they were given
physiotherapy which was inadequate, while the remaining 1(33.3%) head of school indicated that
they were given occupational therapy. Three heads of schools for learners with multiple
disabilities were asked to say the support services that were offered in their schools. Two
(66.7%) heads of schools for learners with autism blindness reported that learners were offered
with medical services while the remaining 1 (33.3 %) head of school confirmed that they were
not given any support service. Three heads of schools for learners with cerebral palsy intellectual
disability were asked to say the support services offered in their schools. Two (66.7%) out of the
three heads of schools indicated that learners with cerebral palsy intellectual disability were
given hydrotherapy, Physiotherapy and prevocational training services respectively. The only
support service given to learners with autism blindness was medical services reported by 4 (57.1)
of the teachers. All other support services were lacking. In relation to this, 2 (28.6%) teachers
recommended that the school administration should ensure that learners were given support
services in order to enhance their academic performances and also have an environment that was
conducive while at school. The observations carried out in schools for learners with autism
blindness confirmed that the only support services offered in two schools were medical services.
They lacked other support services such as auditory training, sensory integration, speech therapy
124
and a special diet, among others. Sensory integration is given to learners with autism blindness
who engages in inappropriate responses to sensory stimuli .In auditory training, an audiogram
identifies frequencies to which the child with autism blindness is hypersensitive (Grandin, 1995).
The diet of learners with autism blindness should be free from casein, gluten, aspartame and
monosodium glutamate (Breton, 2001). A speech language pathologist evaluates and develops
programmes for individuals with speech or language problems (Best et al., 2010). Learners‟ with
autism blindness require the support of speech language pathologists due to their communication
problems (Ministry of Education Special Programs branch, 2000). The observations carried out
in schools for learners with autism blindness confirmed that there were no specialized equipment
such as adapted computers, global positioning devices; note takers among others. The equipment
can go a long way in helping learners‟ access education with ease and also enhance their
independence.
4.6 Training needs of teachers educating learners with multiple disabilities.
The study sought to find out the training needs of teachers educating learners with multiple
disabilities. To address this objective, study respondents (head teachers and teachers) were asked
to indicate whether teachers were competently trained to teach learners with multiple disabilities.
With regard to this, some teachers interviewed confirmed that some teachers were not adequately
trained to teach learners with multiple disabilities and therefore they needed some training.
Research has recently verified that a well-prepared teacher has more influence on a child‟s
learning than any other factor under school control (Darling-Hammond, 2000).

125
Table 4.13: Teachers’ responses on training needs of teachers educating learners with Deaf
blindness
Training Needs Frequency(N=20) Percentage
Interdisciplinary courses to be given in details 18 90
Knowledge on deaf blindness/levels/etiologies 18 90
Communication modes/assistive technology 17 85
Adaptation of curriculum/learning environment 17 85
Orientation and mobility 16 80
Transition skills/functional skills/vocational skills 16 80
Behaviour management/social skills 15 75
Assessment and evaluation 15 75
How to source for funding 14 70
Career choices 13 65
Table 4.13 above shows that majority of the teachers 18 (90%) were of the views that in order to
teach learners with deaf blindness effectively, they required to be trained in details the
interdisciplinary courses and knowledge on deaf blindness. During the interview, one of the
respondents was asked to elaborate on what they meant. This was the reply “I was trained in
braille and sign language to teach learners with deaf-blind at KISE but most of the learners in
this school have deaf-blind and other disabilities such as cerebral palsy, physical disabilities,
autism and intellectual disability and health problems. The interdisciplinary courses that we
learnt were very shallow, teachers should be taught every disability and its implication on
learning in details.” This study report is supported by Best et al., (2010) who stated teachers
must have knowledge about a variety of disabling conditions and their implications for function.
The Council of Exceptional Children (1995) has stated that the competencies of a teacher
teaching learners with deaf blindness should include; knowledge on deaf blindness, types and
various etiologies and their implications to learning. Seventeen teachers (85%) were of the views
that they should be taught skills of communicating with learners who are deaf-blind, assistive
technology and on the modifications of the curricula, instructional strategies and learning
environment as supported by Heller & Swine hart-Jones (2003) who stated that teachers must
possess knowledge and skills on curriculum modifications, instructional techniques, arranging

126
and adapting the learning environment. Sixteen (80%) teachers said that they required training on
vocational, functional skills, transition and orientation and mobility as supported by Best et al.,
(2010) who says that learners will have to be taught functional living skills for maximum
independence in school, home and community and life experiences.
Transition skills should also be taught to teachers to prepare learners for transition. They also
require skills of self reliance. Self reliance means reliance on one‟s own abilities to perform
tasks. Orientation and mobility and training on assistive technology are supported by the Council
of Exceptional children (1995). Fifteen teachers (75%) were of the views that they required
training on behaviour management, how to teach social skills, assessment and evaluation which
are supported by the Council of Exceptional Children (1995). Fourteen(70%) of teachers were of
the views that teachers should be given training on how to source for funds because the money
given by the government is very little to sustain the special unit. During the interview, one of the
respondents said, “We should be taught skills on how to generate income and on how to
collaborate with other stakeholders’‟. Thirteen teachers (65%) were of the views that they
should be taught skills on career choices for learners with deaf-blind.

127
Table 4.14: Teachers’ responses on training needs of teachers educating learners with
Autism blindness
Training Needs Frequency(N=7) Percentage
Knowledge in all areas of disabilities in details
autism blindness
6 85.7
Instructional strategies for the various disabilities 6 85.7
Curriculum adaptations /learning environment 6 85.7
Assessment of autism and other disabilities 6 85.7
Remediation of communication and behayiour 5 71.2
Communication skills/assistive
technology/computers
5 71.2
Support services 5 71.2
Transition/functional/vocational skills 5 71.2
Social skills/special diet 4 57.1
As shown in Table 4.14 above, majority of teachers 6 (85.7%) teaching learners with autism
blindness suggested that they needed training in all areas of disabilities, knowledge on
instructional techniques, curriculum adaptations, assessment and evaluation. Respondents were
asked to explain why they wanted training in all areas. This was the response “Most of the
learners we have in this class are autistic blind with other disabilities such as intellectual
disability, physical, communication difficulties, and cerebral palsy and behaviour challenges.”
This study report is supported by Boyce & Hammond (1996) who have stated that teachers
teaching learners with autism blindness will need core skills that enable them to teach all
learners. Best et al., (2010) also supports the training of teachers dealing with multiple
disabilities on various disabling conditions. Training on autism and blindness is supported by
Shaheen (2009) who trained a learner who was autistic blind. Five (71.2%) teachers suggested to
be given training on remediation of communication and behaviour challenges, use of assistive
technology, use of adaptive computers, support services, transition, functional skills and
vocational training. This study report is supported by Best, Heller,& Bigge (2005);Council for
exceptional children (1998); Heller, Fredrick, Dykes, Best, & Cohen, 1999; Heller & Swinehart-
Jones(2003) who have stated that teachers who instruct learners with multiple disabilities must
possess specific competencies that encompass instruction, physical management of learners,
educational environment, health maintenance, use of assistive technology, communication and

128
curricular adaptation. Koech Report (1999) also emphasized on the retraining of teachers in the
evolvement of new knowledge and technology. Four teachers (57.1%) were of the views that
they required training on how to teach social skills and on the special diet given to learners with
autism blindness.
Table 4.15: Teachers’ responses on training needs required to teach learners with
Cerebral palsy intellectual disability
Training Needs Frequency(N=30) Percentage
Knowledge in all areas of disability/cerebral
palsy
30 100
Instructional strategies for the various disabilities 28 93.3
How to remediate communication and behaviour 28 93.3
Assessment modes of various disabilities and CP 28 93.3
Curriculum adaptations/learning environment 28 93.3
Techniques for lifting and devices/physical
management/personal care
24 80
Transition/functional skills/vocational skills 23 76.6
Use of assistive technology/adaptive computers 23 76.6
Career choices 20 66.6
As shown in Table 4.15, 30 (100 %) of the teachers reported that they required training on all
areas of disabilities in details because learners with cerebral palsy intellectual disability have
other disabilities such as hearing,visual,autism, orthopedic and epilepsy among others. During
the interview one of the respondents was asked to elaborate on the training required, these were
the words “. These learners are not just physically disabled with a cognitive disability they also
have health problems, communication challenges, hearing problems and epilepsy how do I help
and my training was for the physically challenged in general only? I will require detailed
information and knowledge on all other disabilities, their remediation strategies and their
instructional strategies”. This study report is supported by Best et al., (2010) who stated that
teachers must have knowledge about a variety of disabling conditions and their implications for
function. Koech Report (1999) also emphasized on the need for re-training of teachers on the
evolvement of new knowledge and technology. The teachers also needed knowledge on the types

129
of cerebral palsy and their remediation in details. Twenty eight (93.3%) were of the views that
they needed training on all the instructional strategies for the various disabilities, how to
remediate communication and behaviour disorders, assessment modes and curriculum
modifications and the learning environment. Best et al., (2010) supports the study report where
he stated that in order to reduce the functional impact of disability, teachers and others who work
with individuals with multiple disabilities must develop knowledge, skills, and abilities that
extend beyond standard pedagogy. They must have a thorough understanding of typical
development in motor, sensory, perception, cognition, communication, language, social,
emotional and self-care domains. Training on how to remediate communication and behaviour
disorders can help learners with cerebral palsy. For instance, students with severe cerebral palsy
may have speech that is difficult to understand, especially with people unfamiliar to the student.
AAC can be used to augment the existing communication hence the term Alternative
Augmentative Communication (Romski &Sevcik, 1996). Teachers should be trained on how to
use Alternative and Augmentative communication. Twenty four (80%) of teachers suggested that
they required training on techniques for positioning and lifting, and the devices used. Twenty
three (76.6%) were of the views that they should be given training on transition, functional skills
vocational training and assistive technology. Best et al., (2010) supports this study report where
he states that teachers need to prepare learners for life by offering transition skills, vocational
skills and functional skills for maximum independence in school, home, community and life
experiences. They will require skills for self reliance. Career choices were mentioned by twenty
teachers (66.7%).

130
4.7 Strategies to consider in order to improve teaching.
The following were some of the suggestions that were given by the respondents who participated
in the study.
Teachers’ recommendations
Table 4.16: Recommendations from teachers of learners with deaf blindness
Recommendations Frequency(N=20) percentage
Provision of adequate teaching resources/support services 20 100.0
Teacher-pupil ratio should be 1:1 20 100.0
IEP to be done by multidisciplinary team 20 100.0
All teachers should be trained on a variety of disabling
conditions and adaptive technology
20 100.0
Curriculum should be made functional 20 100..0
Frequent refresher courses/exchange programmes 19 95.0
Provision of specialized equipment 15 75.0
Creation of awareness on multiple disabilities 15 75.0
Physical environment should be made barrier free 15 75.0
Proper assessment should be made for proper placement 13 65.0
Heads of institution in integrated and special schools should be
specially trained in the particular category of disabilities
12 60.0
Functional skills to be awarded a certificate 12 60.0
Age of exit of learners should be specified 12 60.0
As shown on Table 4.16 above, 3 (100.0%) teachers recommended that schools should have
enough teaching resources and support services, IEP to be made by a multidisdisciplinary team
and curriculum should be made functional. They also suggested that all teachers be trained on a
variety of disabling conditions and adaptive technology. The respondents further recommended
that teacher‟s work load should be minimized by ensuring that teachers- pupil‟s ratio is 1:1. This
is due to the fact that deaf- blind learner requires considerable modifications to the teaching
content and different teaching strategies. He/she cannot learn from what he/she sees like the deaf
child does. He/she cannot learn from listening like the blind child does. He/she learns only by
what he/she does. This means that no learning is taking place for him/her while waiting for

131
others to take their turn. For this reason, a small group or individual instruction becomes more
critical (Moss & Hagood, 1995). Moreover, 19 (95.0%) teachers suggested that teachers should
be taken for frequent refresher courses and exchange programmes to learn and share experiences.
Other suggestions that were given by 15 (75.0%) of the respondents were; provision of
specialized equipment, physical environment to be made barrier free and creation of awareness
on deaf blindness. Thirteen (65.0%) of respondents suggested that proper assessment be made
for proper placement, heads of special institutions be specially trained, functional skills to be
awarded a certificate to learners with multiple disabilities, and age of exit to be specified.
Table 4.17: Recommendations from teachers of learners with Autism blindness
Recommendations Frequency(N=7) Percentage
Teachers should be given further training in a variety of disabling
conditions/autism blindness/instructional strategies
7 100.0
IEP should be designed by a multidisciplinary team 7 100.0
Provision of adequate teaching resources 7 100.0
Provision of support services 7 100.0
Curriculum should be made functional 7 100.0
Teacher: pupil ratio should be 1:1 6 85.7
Physical environment should be made barrier free 6 85.7
Provision of special diet 5 71.4
Exchange programmes 5 71.4
Creation of awareness on multiple disabilities 4 57.1
Head of institution should be specially trained 4 57.1
Age of exit of learners should be specified 3 42.8
As shown in Table 4.17 above, in order to improve teaching and learning process among learners
with autism blindness all 7 (100.0%) study respondents suggested that teachers should be given
training on a variety of disabling conditions because most of the learners with autism blindness
have more than two disabilities. This would make teachers more effective in content delivery and
hence improving their teaching methodologies as well as learners‟ performances. They further
suggested that IEP should be made by multidisciplinary team and there should be adequate

132
teaching resources. Additionally, all 7 (100.0%) teachers suggested the provision of adequate
support services and curriculum to be made functional. When a curriculum approach takes into
account the pupils current individual needs and his future needs and is designed to meet his
needs it is known as a functional curriculum (Ellis 1986). Six (85.7%) suggested that the teacher
pupil ratio be 1: 1 and the physical environment be made barrier free. Kochung Report (2003)
recommended that teacher learner ratio for learners with multiple disabilities should be 1:1. Five
(71.4%) of the respondents suggested a special diet and exchange programmes from other
countries. Learners who are autistic require a special diet free from gluten, aspartame and casein
found in milk among others as supported by (Breton, 2001). Exchange programmes would help
teachers to share their experiences and learn from other countries on how to teach learners who
are autistic blind.

133
Table 4.18: Recommendations from teachers teaching learners with cerebral palsy
Intellectual disability
Recommendations Frequency
(N=30)
Percentage
Further training on a variety of disabling conditions /instructional
strategies
30 100.0
Provision of adequate teaching resources 30 100.0
IEP to be made by the multidisciplinary team 30 100.0
Provision of adequate support services 30 100.0
curriculum should be made functional 30 100.0
Specialized equipment and adaptive aids 28 93.3
The physical environment should be made disability friendly 28 93.3
Inspection should be made by specialist 28 93.3
Teacher pupil ratio should be 1:1 28 93.3
Acquisition of functional skills be awarded a certificate 28 93.3
Exchange programmes 20 66.6
Creation of awareness 20 66.6
The head of institution should be specially trained 20 66.6
Age of exit of learners should be specified 17 56.6
Provision of special diet 17 56.6
Involve teachers in the making of the curriculum 17 56.6
Mode of assessment to be determined by learners needs 17 56.6
The Joint Admission Board(JAB) should not admit teachers for special
education directly
5 16.6
As shown in Table 4.18 all 30 (100.0%) teachers recommended that teachers should be given
further training on a variety of disabling conditions and their instructional strategies. This would
make them competent in teaching learners with cerebral palsy intellectual disability. The
respondents also suggested that they should be provided with; adequate teaching resources and
support services. Teachers were also of the views that IEP should be developed by the
multidisciplinary team and that the curriculum is made functional. Twenty eight (93.3%) of
teachers suggested the provision of specialized equipment, teacher pupil ratio be made 1:1 and
acquisition of functional skills by learners with multiple disabilities be awarded a certificate.
Twenty (66.6%) suggested the exchange programmes, creation of awareness on disabilities and
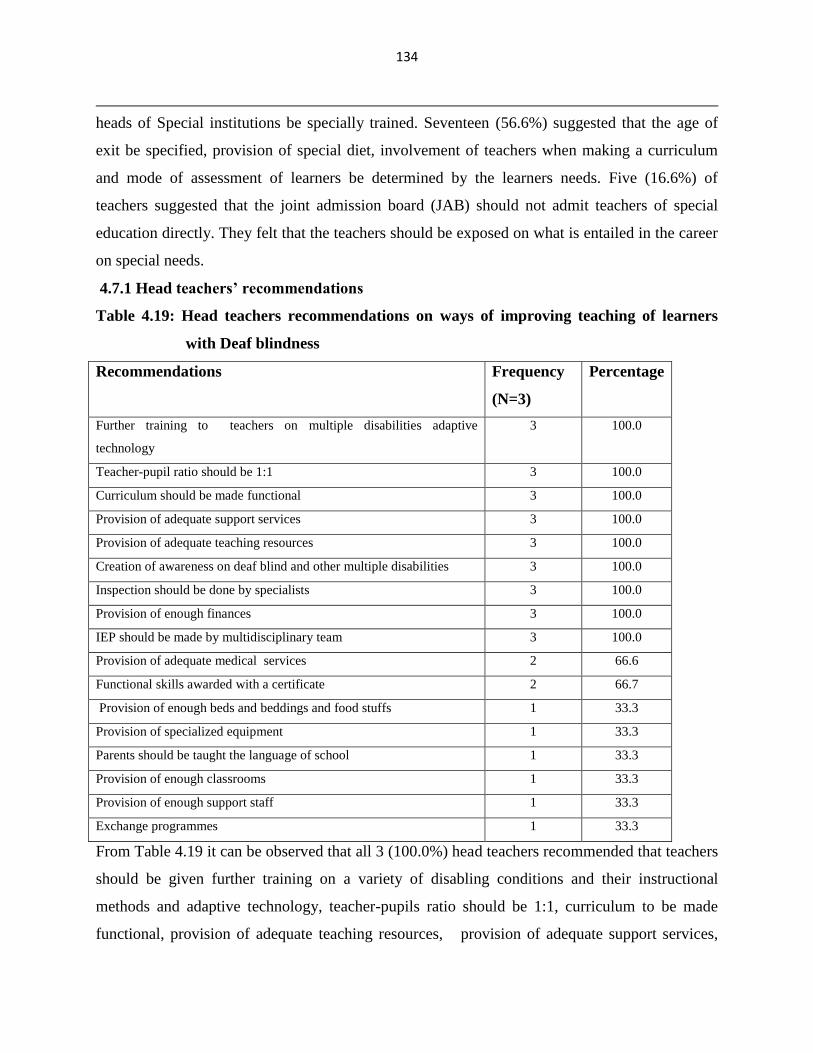
134
heads of Special institutions be specially trained. Seventeen (56.6%) suggested that the age of
exit be specified, provision of special diet, involvement of teachers when making a curriculum
and mode of assessment of learners be determined by the learners needs. Five (16.6%) of
teachers suggested that the joint admission board (JAB) should not admit teachers of special
education directly. They felt that the teachers should be exposed on what is entailed in the career
on special needs.
4.7.1 Head teachers’ recommendations
Table 4.19: Head teachers recommendations on ways of improving teaching of learners
with Deaf blindness
Recommendations Frequency
(N=3)
Percentage
Further training to teachers on multiple disabilities adaptive
technology
3 100.0
Teacher-pupil ratio should be 1:1 3 100.0
Curriculum should be made functional 3 100.0
Provision of adequate support services 3 100.0
Provision of adequate teaching resources 3 100.0
Creation of awareness on deaf blind and other multiple disabilities 3 100.0
Inspection should be done by specialists 3 100.0
Provision of enough finances 3 100.0
IEP should be made by multidisciplinary team 3 100.0
Provision of adequate medical services 2 66.6
Functional skills awarded with a certificate 2 66.7
Provision of enough beds and beddings and food stuffs 1 33.3
Provision of specialized equipment 1 33.3
Parents should be taught the language of school 1 33.3
Provision of enough classrooms 1 33.3
Provision of enough support staff 1 33.3
Exchange programmes 1 33.3
From Table 4.19 it can be observed that all 3 (100.0%) head teachers recommended that teachers
should be given further training on a variety of disabling conditions and their instructional
methods and adaptive technology, teacher-pupils ratio should be 1:1, curriculum to be made
functional, provision of adequate teaching resources, provision of adequate support services,

135
creation of awareness on multiple disabilities, provision of adequate resources, IEP to be
developed by a multidisdisciplinary team and inspections should be done by specialists. Two
head teachers (66.7%) recommended that special schools should be provided with adequate
medical services and those who acquire functional skills are awarded certificates. Functional
skill is supported by Vygotsky (1978), who stated that instead of measuring intelligence by what
a child can do alone, he suggested that intelligence could better be measured by what a child can
do with skilled help. The least recommended strategies were; provision of enough support staff,
provision of enough beddings, exchange programmes, specialized equipment and parents to be
co-therapists with the teachers all at 1(33.3%) respectively.
Table 4.20: Head teachers recommendations on ways of improving teaching of learners
with autism blindness
Recommendations Frequency(N=3) Percentage
Retraining of teachers on a variety of disabling conditions 2 66.7
Train teachers on how to handle multiple disabilities 2 66.7
Provision of enough teaching resources 2 66.7
Provision of support services 2 66.7
IEP to be made by multidisciplinary team 2 66.7
The curriculum should be made functional 2 66.7
Barrier free infrastructure 1 33.3
Specified age of exit 1 33.3
Teacher-pupil ratio should be 1:1 1 33.3
Creation of awareness 1 33.3
Implementation of exchange programmes 1 33.3
As Table 4.20 shows, 2 (66.7%) of the head teachers recommended retraining among teachers on
a variety of disabling conditions because learners with autism blindness have more than two
disabilities and provision of enough teaching resources. This would enhance academic
performance of learners with autism blindness as teachers would be competent enough with the
teaching of the curriculum. Availability of teaching and learning resources would also enhance
smooth teaching and learning process and eventually translate to improved academic
performance among learners and school as a whole. In addition, school heads suggested that
supporting bodies should ensure that learners were provided with the support services they

136
required in order to improve on their learning process. They further suggested that IEP should be
developed by a multidisciplinary team 2 (66.7%) and curriculum should be made functional 2
(66.7%). Other recommendations included; implementation of exchange programmes, teacher
pupil ratio to be 1:1 and learners to have a specified age of exit. This is because the transition of
learners with special needs is unspecified.
Table 4.21: Head teachers’ recommendations on ways of improving teaching of
learners with cerebral palsy intellectual disability
Recommendations Frequency(N=3) Percentage
Training of teachers on a variety conditions and instructional methods 3 100.0
Provision of adequate teaching resources 3 100.0
IEP to be made by the multidisciplinary team 3 100.0
Provision of enough finances 2 66.7
Curriculum should be made functional 2 66.7
Provision of specialized equipment 2 66.7
Inspectors should be specially trained 2 66.7
Creation of awareness on the multiple disabilities 2 66.7
The physical environment should be made barrier free 2 66.7
Exchange programmes 2 66.7
Age of exit of learners to be specified 2 66.7
Teacher pupil ratio should be 1:1 2 66.7
Provision of adequate support services 2 66.7
Mode of assessment should vary accordingly 2 66.7
Functional skills should be certified 2 33.3
Parents should be sensitized on disabilities 2 33.3
As shown in Table 4.21 above, all head teachers 3 (100%) interviewed suggested that teachers
should be offered with training on a variety of disabling conditions and their instructional
strategies and they should be provided with adequate teaching/learning resources and IEP should
be developed by a multidisciplinary team. Two of the three headteachers 2 (66.7%) were also of
the views that special schools should be provided with enough finances, adequate support
services and specialized equipment. Curriculum should also be made functional, functional skills
should be awarded a certificate, mode of assessment should vary and school inspectors should be
specially trained. The physical environment was to be made barrier free, age of exit to be
specified, the teacher pupil ratio be made 1:1 and creation of awareness. Gachathi Report (1976)

137
recommended the creation of awareness on the part of the public on the causes of disabilities
with a view of facilitating the prevention. Individual attention to learners with multiple
disabilities was not possible because learners exceeded the number of teachers in the schools.
Kochung Report (2003) recommended a ratio of 1:1 among the multiply disabled.

138
CHAPTER FIVE
SUMMARY CONCLUSION AND RECOMMENDATIONS
5.0 Introduction
This chapter gives a summary of the study in relations to the objectives of the study. It also
presents the implications of the main findings, conclusions, recommendations and areas for
further research.
5.1 Summary of the Findings.
Majority of the teachers 20 (100%) educating learners with deaf blindness used the following
instructional methods namely; tactile Kenyan sign language, use of real objects, use of sign
language, use of speech paired with braille, task analysis and activities of daily living, among
others. However the teachers conceded to not using the Deaf-blind manual alphabet and on
teaching learners to make a choice. The choice of the instructional methods was determined by
the learner‟s needs. For instance, learners who were deaf-blind without any other disability could
be taught using tactile Kenyan sign language, Tadoma and use of object of reference among
other instructional methods. Most of the instructional methods for learners with deaf blindness
were primarily communicative. The observations carried out in schools for learners with deaf
blindness confirmed that most of the learners with deaf blindness had other disabilities such as,
autism, intellectual disability cerebral palsy, behaviour disorders and physical disabilities.
Teachers educating learners with deaf blindness without other disabilities were able to adapt the
generic teaching strategies to cater for the individual needs of the learner.
Majority of teachers 7 (100%) educating learners with autism blindness used the following
instructional methods namely; pre-braille, braille, oral methods, songs, pre-vocational skills and
real objects. The teachers conceded to not using the following methods namely; the use of two
handed sign language paired with speech, behaviour management strategies, use of tactile
kinesthetic modalities and use of recorded materials. The observations carried out in schools for
learners with autism blindness confirmed that teachers educating learners with autism blindness,
focused on the teaching strategies for learners with visual impairments leaving out the symptoms
of autism affecting learning among the learners. For instance, learners with autism display
communication difficulties, lack of social skills and behaviour disorders among others. Teachers

139
were not able to differentiate instructions because their training was specifically for learners with
visual impairments. The instructional methods used by the majority of teachers 29 (96.7%)
educating learners with cerebral palsy intellectual disability included; task analysis, activities of
daily living and real objects. The teachers conceded to not using the following methods; use of
antecedent prompting, use of computer based instruction, and use of pre-linguistic milieu
teaching. The observations carried out in schools for learners with cerebral palsy intellectual
disability confirmed that teachers were not able to differentiate instructions for learners with
cerebral palsy intellectual disability because their training was specifically for learners with
physical impairments in general without other disabilities. Another observation was that despite
the fact that learners with cerebral palsy intellectual disability have varying levels of cerebral
palsy and cognitive development; teachers were not individualizing their instructions because
they were inadequate.
Teachers focused more on the teaching strategies for learners with intellectual disability without
remediating the symptoms that were brought about by cerebral palsy that were affecting learning
which hindered the achievement of the teaching objectives. For instance, learners with cerebral
palsy have problems in communication, problems in gross and motor skills and other health
conditions that may affect learning. If those problems are not remediated, then their learning will
be affected. Teachers felt inadequately prepared to handle learners with multiple disabilities. All
the teachers who were educating learners with multiple disabilities developed an individualized
education programme without involving the multidisciplinary team as it is done in other
countries therefore learners were not getting all the required support services. Among the schools
for learners with deaf-blind teachers were using the third draft of an adapted curriculum from
KIE. The teachers felt that the functional academics should be included in the final draft. Among
the schools for learners with cerebral palsy intellectual disability, the curriculum used was for
learners with intellectual disability. In schools for learners with autism blindness some teachers
were using the general syllabus while others used the syllabus for learners with intellectual
disability. No curriculum adaptations had been effected for learners with cerebral palsy
intellectual disability and autism blindness. The teachers proposed a functional curriculum or a
specialist curriculum. The primary concern of the specialist curriculum is to remediate

140
fundamental problems in children with special needs. Such problems may include:
communication, speech, mobility and daily living skills among others. Teaching resources that
were available among the schools for the deaf-blind included; Lily Nielsen boards 17 (85%) play
areas and calendar boxes at 16 (80%). Ten (50%) of the respondents also reported that there were
stimulant boards, utensils and manila papers. felt pens, washrooms and dining room. Other
resources mentioned included a language room and a sensory room at 6 (30%) respectively. The
teaching resources were found to be inadequate. In one of the school, there was a workshop but
nothing was going on because there were no materials. In schools for learners with autism
blindness the available resources included braillers and Abacus and real objects 7 (100%), braille
papers at 6 (85.7%), pegboards and cubarithms at 4 (57%) toys among others. Some of the
teaching resources were inadequate. The teaching resources that were most available in schools
for learners with cerebral palsy intellectual disability included; real objects 21 (70%), followed
by beads 20 (66.7%) and manila papers 19(63.3%). Seventeen (56.7%) of the respondents cited
the availability of felt pens. The teaching resources were found to be inadequate.
Among the schools for the learners with deaf blindness, some few teachers had been trained on
braille and sign language to teach learners with deaf blindness from Kenya institute of Special
Education. However, during the interview, the teachers felt that interdisciplinary courses offered
at KISE should be given in details because most of the learners were not just deaf-blind, they had
other additional disabilities. Majority of the teachers 18 (90%) were of the views that in order to
teach learners with deaf blindness effectively, they required to be trained in details the
interdisciplinary courses and knowledge on deaf blindness. Some of the competency areas
teachers suggested included; knowledge on all areas of disabilities in details because learners
with deafblindness have other additional disabilities such as, autism, cerebral palsy, intellectual
disability and physical disabilities. Seventeen teachers (85%) were of the views that they should
be taught skills of communicating with learners who are deaf-blind, assistive technology and on
the modifications of the curricula, instructional strategies and learning environment. Sixteen
(80%) teachers said that they required training on vocational, functional skills, transition skills,
self-reliance, orientation and mobility. Transition and self-reliance skills should also be taught to
teachers to prepare learners for transition and self-reliance. Fifteen teachers (75%) were of the

141
views that they required training on behaviour management, how to teach social skills,
assessment and evaluation. Fourteen (70%) of teachers were of the views that teachers should be
given training on how to source for funds because the money given by the government is very
little to sustain the special schools and units. Thirteen teachers (65%) were of the views that they
should be taught skills on career choices for learners with deafblindness.
Majority of teachers 6 (85.7%) teaching learners with autism blindness suggested that they
needed training in all areas of disabilities including autism and knowledge on instructional
techniques, curriculum adaptations, assessment and evaluation. Respondents explained that they
wanted knowledge on all other disabilities in details because most of the learners they had in
class were autistic blind with other additional disabilities such as intellectual disability, physical,
communication difficulties, cerebral palsy and behaviour challenges. Five (71.2%) teachers
suggested to be given training on remediation of communication and behaviour challenges, use
of assistive technology, use of adaptive computers, support services, transition, functional skills
and vocational training. Four teachers (57.1%) were of the views that they required training on
how to teach social skills and on the special diet given to learners with autism blindness. Thirty
(100 %) of the teachers teaching learners with cerebral palsy intellectual disability reported that
they required training on all areas of disabilities in details because learners with cerebral palsy
intellectual disability have other disabilities such as hearing,visual,autism, epilepsy, orthopedic
among others. Twenty eight (93.3%) teachers‟ were of the views that they needed training on all
the instructional strategies for the various disabilities, how to remediate communication and
behaviour disorders, assessment modes and curriculum modifications and the learning
environment. Twenty four (80%) teachers suggested that they required training on techniques for
positioning and lifting, and the devices used. Twenty three (76.6%) were of the views that they
should be given training on transition, functional skills, use of adaptive computers, vocational
training and assistive technology. Career choices were mentioned by twenty teachers (66.7%).
Teachers required further training on multiple disabilities because the training they had was on
educating learners with physical impairment as a specific disability. Learners with deaf
blindness were supported by being given services such as occupational therapy and
physiotherapy. Nine (45%) teachers interviewed reported that learners with deaf blindness were

142
supported by given services by an occupational therapist. Four (20%) of teachers reported the
services of a physiotherapist.
Two (10%) teachers reported that the physiotherapist services were inadequate. One (5.0%) of
the teachers reported that occupational therapy was offered but it was inadequate. This is a cause
of concern because there are so many learners who are in dire need of support services but they
are unavailable. In the long run these learners may not access appropriate education. In relation
to this,10 (50%) of the teachers recommended that the school administration should ensure that
all the necessary support services for learners with deaf-blind such as speech therapy, sensory
integration, among others are availed effectively to enhance their academic performance.
The observations carried out in schools for learners with deafblindness revealed that the support
services that were offered included; the related support services of an occupational therapist who
was only one in one of the schools. The occupational therapist was only one serving learners
with deafblindness and other learners with other disabilities. In another school the
physiotherapist reported once a month, this is a cause of concern because some of these learners
require the services on a daily basis. In one of the schools for learners with deafblindness, there
was a language room and a sensory room. Learners with cerebral palsy intellectual disability
were given the following services; physiotherapy 14 (46.7%), hydrotherapy 10 (33.3 %,) and
health services 10 (33.3%). Inadequate physiotherapy was reported by 6 (20%) of the teachers.
The least support service given to these learners was reconstruction therapy as well as inadequate
health services at 5 (16.7%). The observations carried out in schools for learners with cerebral
palsy intellectual disability confirmed that in most schools, the support services given by the
physiotherapist and occupational therapist were inadequate. There was no speech therapist for
those with communication difficulties. However there was a nurse in two of the schools who
offered medical services. Observations confirmed that there were no specialized equipment like
adapted computers, prone standers, mechanical lifts, electronic page turners, shelf liner among
others. These equipment if availed, can go a long way in enhancing access to education, mobility
and independence among learners with cerebral palsy intellectual disability. Some schools had a
television set and some few computers which were not used because teachers were not computer
literate. Minimum adaptations had been made in the schools. The only support service given to

143
learners with autism blindness was medical services reported by 4 (57.1) of the teachers. All
other support services were lacking. In relation to this, 2 (28.6%) of teachers recommended that
the school administration should ensure that learners were given support services in order to
enhance their academic performances and also have an environment that was conducive while at
school. The observations carried out in schools for learners with autism blindness confirmed that
the only support services offered in two schools were medical services. They lacked other
support services such as auditory training, sensory integration, speech therapy, occupational
therapy and a special diet, among others. There were no specialized equipment such as adapted
computers, global positioning devices; note takers among others. The equipment if availed can
go a long way in helping learners‟ access education with ease and also enhance their
independence. Teachers did not have consistent schedules for learners with autism blindness and
individual attention of learners was impossible because teachers were inadequate.
To improve teaching for learners with multiple disabilities, learners should be provided with an
adapted or a specialist curriculum, provision of adequate teaching resources, IEP to be designed
by a multidisciplinary team and all teachers to be given further training on how to differentiate
instructions for learners with multiple disabilities. The training should be on a variety of
disabling conditions because most of the learners have more than two disabilities. Teachers
should be trained on how to adapt the curriculum to suit learner‟s needs, adaptations of the
learning materials, learning environment, assessment and evaluation, use of assistive technology
and on the use of adaptive computers among other skills. Teacher pupil ratio should be 1:1,
provision of specialized equipment, age of exit to be specified, creation of awareness on multiple
disabilities, physical environment to be made barrier free, proper assessment for proper
placement and heads of institutions in integrated special schools to be specially trained in a
particular category of disability among others. The government should provide adequate funds,
provision of adequate support services, awarding functional certificate for the functional skills,
age of exit of learners to be specified, provision of enough beddings and foodstuffs, provision of
enough support staff among others.

144
5.2 Implications of the Findings
Teachers were found to be inadequately trained to educate learners with multiple disabilities
because the training they had was for a specific disability therefore teachers were unable to
differentiate instructions. This implies that teachers educating learners with multiple disabilities
should have specialized competencies in order to provide the learners with quality education
opportunities. The teachers should be trained in a variety of disabling conditions and their
instructional strategies because most of the learners have more than two disabilities. Personalized
attention to learners with multiple disabilities was not possible since the teachers were not
enough and they were not adequately trained. This implies the need for more teachers who are
trained to handle diverse needs of learners. Teachers should have access to a wide range of
specialist strategies especially where they work with learners with the most complex needs;
there is the need for teachers to be able to adapt more generic strategies to meet the specific
needs of an individual learner. Teachers should demonstrate understanding of their strategies to
ensure they are confident in making adaptations in accordance with the child‟s development and
other needs. The curriculum was also found to be ineffective because it was not catering for the
diverse needs of learners with multiple disabilities. This implies the need for a functional
curriculum or a specialist curriculum, a curriculum that takes into account the current and future
needs of individual learners. The individualized education programme for learners‟ with multiple
disabilities was made by teachers without involving the multidisciplinary team therefore learners
were not getting the required support services. Most of the learners require related support
services from professionals such as speech therapist, occupational therapist among others who
were not available. Lack of support services was impairing the ability of learners to attend to
instructional situation. Teaching resources were also inadequate. This was found to have adverse
effects on their learning. For instance, some schools had workshops but there were no materials
therefore learners could not learn the prevocational and vocational skills.
5.3 Conclusion
Results revealed that teachers were not adequately trained to teach learners with multiple
disabilities. Most of the teachers had training on a specific disability therefore they had problems
of differentiating instructions for the learners. The teaching resources and support services were

145
also inadequate. The choice of the teaching strategies for learners with multiple disabilities
should be determined by the cognitive ability of the learners. The curricular was found to be
ineffective because it was not catering for learners with cerebral palsy intellectual disability and
autism blindness. The following measures should be taken to improve on their teaching they
include; the provision of a functional curriculum, provision of adequate teaching resources,
provision of adequate support services, and training of teachers on a variety of disabling
conditions because learners with multiple disabilities have more than two or more disabilities.
The study observed that much was needed to be done to make lives of learners with multiple
disabilities bearable in order to achieve success in the curriculum instructions given.
5.4 Recommendations
In this subsection a number of recommendations based on the findings of the study have been
made. It is hoped that the Ministry of Health (MOH), Ministry of Education (MOE) Kenya
Institute of Education (KIE), headteachers, teachers, parents and all the stakeholders in education
including Non-Governmental Organizations (NGOs) will find these recommendations helpful in
trying to improve the education of learners with multiple disabilities in the selected counties. The
government should give teachers further training on a variety of disabling conditions because
learners have more than two disabilities. The competencies required include; knowledge in all
areas of disabilities such as autism, cerebral palsy, intellectual disability, physical disabilities,
health problems, visual, hearing, attention deficit and hyperactivity disorders their instructional
methods, curriculum adaptations, assessment and evaluation, adaptations of the learning
environment, use of assistive technology, physical and positioning devices, transition skills,
vocational skills, functional academics, communication modes among others. The government
should provide adequate teaching resources to the schools. All learners with multiple disabilities
should be provided with a language room and a sensory room. These rooms will ensure
assessment of learners and stimulation of senses among other skills. The government should set
up programmes for people to pursue training as speech therapists, audiologists, dieticians,
physiotherapists and occupational therapists among others to support teachers in related support
services. The government should deploy more teachers to special schools so as to enhance the
teacher pupil ratio. This can improve teacher contact as well as the overall quality of

146
instructional attention. The teacher learner ratio of learners with multiple disabilities should be
one to one.
The government in conjunction with the Ministry of Education should create awareness on
multiple disabilities to all stakeholders in education so that the diverse needs of these learners
may be taken into consideration. This can be done for instance in seminars or in workshops, in
barazas, churches and by the media. The awareness will ensure that all learners regardless of
their disability are taken to school because education is a right to all. The government should
provide specialized facilities to learners with multiple disabilities. Specialized facilities such as
adaptive computers, prone standers, motorized wheelchairs, mechanical lifts among others can
go a long way in enhancing their mobility, independence and access to education. The age of exit
of learners with special needs should be specified to all the stakeholders by the ministry of
education. Most of the learners remain in schools without transition. The government should set
up more vocational training centres to enable learners to make transition from school to
employment. Home based programmes should be funded by the government for learners with
severe disabilities. The ministry of education should ensure that the individualized education
programme is made in consultation with a team of experts so that each learner‟s needs are taken
into consideration. The head teachers in integrated and special schools should be specially
trained. The expertise is needed so as to influence the decisions they make in relation to the
diverse needs of the learners. The Ministry of Education in conjunction with Kenya National
Exams Council (KNEC) should award learners with multiple disabilities with a functional
certificate. Intelligence should not be measured by what a child with multiple disabilities can do
alone, but by what a learner can do as dictated by the cognitive ability with skilled help from a
specially trained teacher. KNEC should be flexible with modes of assessment for learners with
Special needs and should be determined by the learner‟s needs. The physical environment should
be made disability friendly in special schools and in integrated settings. For instance, in some
schools there are no handrails in the toilets for learners who are physically disabled, doors are
not adapted for wheelchairs to go through so learners are forced to leave their wheelchairs
outside and crawl into their class. The government in conjunction with the Teachers Service
Commission should deploy more human resource support staff so as to improve services to
learners with multiple disabilities. The Ministry of Education should ensure that parents are

147
involved in the education of their learners with multiple disabilities. They should be trained on
communication modes such as sign language, braille, use of adaptive computers among other
skills. This will ensure that the learners continue practicing what teachers teach even when out of
school. The Kenya institute of curriculum Development should come up with a functional
curriculum for all learners with multiple disabilities. The adapted curriculum for learners with
deafblindness can be adapted to cater for other multiple disabilities. The National policy on
special needs should be implemented by the government in full to ensure that the needs of all
learners with special needs are mainstreamed.
5.5 Suggestions for further research
The study focused on teaching strategies for three types of multiple disabilities namely deaf
blindness, autism blindness and cerebral palsy intellectual disability. Further research may be
carried out in other types of multiple disabilities such as autism intellectual disability, cerebral
palsy visual impairment, physically disabled hearing impaired, among others. Research may also
be carried out in relation to the challenges facing learners with multiple disabilities such as
health factors, social factors, and emotional factors among others. A study should be carried out
on the impact of wrong placement for learners with multiple disabilities. A study should also be
carried out to establish the prevalence levels of multiple disabilities. This can help establish the
proportion of cases that are not taken to special schools. This is because every child has a right to
education regardless of his or her disability.

148
REFERENCES
Archibold, S. (1994). Monitoring Progress in Children at the Pre Verbal Stage in
McCormick, B. et al., (Eds.) Cochlear Implants for Young Children.
London: Whurr Publishers Limited.
American Psychiatry Association (1994). Diagnosis and Statistical Manual of Mental
Disorders Fourth Edition. Washington D.C:.American
Psychiatry Association.
American Association on Intellectual and Developmental Disabilities (2008). Intellectual
Disability: Understanding its Development, Causes, Classification,
Evaluation and Treatment.
American Foundation for the Blind (2013).History of Hellen Keller. Retrieved from the
Web on June 27th
2013 http://www.google.com/search?q=history
of hellen Keller and how she learnt.
Andreessen, B. E., Rodbroe, F. & Inger, H. (1998). Starting Communication with
Deafblind Children. FSDB/SHIA Publication.
Amulani, A. M., Rackered, B., & Punch, J.L. (2006).Speech-clarity judgments of hearing
aid-processed speech in noise: Differing polar
PatternsandEnvironments.International Journal of Audiology,
45(6), 319-330.
Aslop, L. (2002). Understanding Deaf Blindness Issues Perspectives and Strategies,
Volume1.Utah: Home Oriented Program Essentials dba HOPE
Incorporation.
Aslop, L. (1993). A Resource Manual for Understanding and interacting with Infants,
Toddler and Pre School age children with Deaf Blindness. Utah: Ski-Hi
Institute Utah State University
Asmussen, K .J. & Creswell, J .W. (1995).Education Campus Response to a Student
Gunman. Journal of Higher Education.
Baumgart, D., Brown, L., Pumian, I., Nisbet, J., Seet, M., & Nessina, R. (1982).
Principle of partial participation and individualized
Adaptations in educational programs for severely
Handicapped students. Journal of the association for
Persons with severe Handicaps, 7, 17-27.

149
Bax,M.,Goldstein,M.,Rosenbaum,P.,Leviton,A.,Paneth,N.&Dan,B.(2005).Proposed
Definition and Classification of Cerebral Palsy,
Developmental Medicine and Child Neurology, 47,571-576.
Beech, M. (2002). Accommodations and modification for students with disabilities in
Vocational education and adult education. Retrieved from the web
December24th,2012Fromhttp://ezproxy.gsu.edu.
Beers, M. H., Porter, R.S., Jones, T.V., Kaplan, J.L., &Berkwits, M. (2006).The Merck
manual of diagnosis and therapy(18th
ed.)Whitehouse Station, NJ: Merck &
CO.
Best, S. J., Heller, K.W., & Bigge, J.L. (2005) Teaching individuals with Physical or
Multiple Disabilities (5th
ed.) Upper saddle River, NJ: Merrill / Pearson
Education.
Best, S. J., Heller, K.W., & Bigge, J.L. (2010) Teaching individuals With Physical or
Multiple Disabilities (6th
ed.) Upper saddle Merrill/Pearson
Education.
Bigge, J. L., & Best, S. J. (2001).Task and Situation analysis. In J.L.Bigge, S.J.Best, &
K.W. Heller (Eds.), Teaching individuals with physical, health or
multiple disabilities (4th
ed.,(PP.121-148).Upper Saddle
River, NJ: Merill/Pearson Education.
Blaire, E., & Stanley, F. J. (1997).Issues in the classification of Cerebral palsy. Mental
Retardation and Developmental Disabilities Research Reviews,
3,184-193.
Boyce, F. & Hammond, F. (1996)”.Autism and Visual Impairment MakingSense”.Autism
and Visual Impairment Conference. Scottish Sensory Centre:
Edinburg. Retrieved from the web on 13th
May 2014 at
http:www.ssc.education.ed.ac.uk/resources/vi&multi/boyce.html.
Breton, L.M. (2001). Diet Intervention and Autism: London Jessica Kingsley Publishers.
Brown,L.,Long,E.,Udvari-Solner,A.,Schwartz,P.,Van Deventer,P.&,Ahlgren,C. (1989)
. Should students with severe intellectual disabilities be based In regular
or in special education classrooms in home schools?
Journal of the Association for persons with severe handicaps14, 8-12.
.
Bryant, D. P., & Bryant, B. R. (2003).Assistive technology for people with disabilities.
Boston: Allyn & Bacon.

150
Bukatko, D. & Daehler, M. W.(1998). Child Development a thematic Approach.
Boston: Houghton Mifflin.
Butler, F., Miller, S., Lee, K., & Pierce, T. (2001). Teaching mathematics to students with
mild- to-moderate mental retardation: A review of the
literature. Mental retardation: A review of the literature.
Mental retardation, 39, 20-31.
Campbell, P. H. (1987). Integrated Programming for Students with Multiple Handicaps
In Goetz. et al (Eds) Innovative Program Design for Individuals
with Dual Sensory Impairments (p159-188).Baltimore: Paul H.
Brookes.
Cartwright, A. Trudgil, B.D & Mansfield, C.S. (1995). Educating Special Learners, 4th
Edition. U.S.A.: Wadsworth Publishing Company.
Cha, K., & Merrill, E. (1994). Facilitation and inhibition of visual selective attention
processes of individuals with and without mental retardation.
American Journal on Mental Retardation, 98,594-600.
Chen, D. (1995). Guiding Principles for Instruction and Program Development. In
Chen, D. & Dote-Kwan, J. (Eds).Starting Points: Instructional Practices
for Young Children whose Multiple Disabilities include Visual
Impairment (pp15-28) Los Angeles: Blind Children.
Chen, D., Downing, J., Rodriguez G. G (2001).Tactile Learning Strategies for children
who are Deafblind: Concerns and considerations from
project SALUTE Northridge, California State
University.
Classen, S. Lopez, D. S., Winter, S., Awadz, K. D., Ferre, N. J. & Garvan, C. W. (2007).
Population Based Health Promotion Perspective for Older Driver
Safety: Conceptual Framework to Intervention Plan. Clinical in Aging.
Collins, B., Gast, D., Ault, M., & Wolery, M. (1991).Small group instruction: Guidelines
for Teachers of students with moderate severe handicaps. Education
and training in mental retardation.
Corn, A.L., Bell, J.K., Anderson, E., Bachofer, C., Jose. & Perez, A. (2003). Providing
access to the visual environment: A model of comprehensive
low vision services for children. Journal of Visual
Impairment and Blindness, 97,261-272.

151
Corn, A. L., & Koenig, A.J. (2002). Literacy instruction for students with low vision: A
framework for delivery of instruction. Journal of visual
impairment and Blindness, 96, 305-321
Council for Exceptional Children, (2000).Bright Futures for Exceptional Learners: An
Agenda to Achieve Quality Conditions for Teaching and Learning. Reston, VA:
Author
Council for Exceptional Children, (1998). What every special educator should know. The
International standards for the preparation and licensure of special Educators
(3rd
Ed.) Reston, VA: Author.
Council for Exceptional Children, (1995).What every special Educator must know: The
International standards for the preparation certification of special Education.
Teachers 62- 80. Reston. Virginia: Author.
Creswell, J. W., Plano Clark, V. L. (2007). Designing &Conducting Mixed Methods
Research. Thousand Oaks, CA: Sage.
Creswell, J. W. (2008). Educational Research: Planning, Conducting and Evaluating.
Quantative and Qualitative Research.
Creswell, J. W. (2009) Research Design: Qualitative, Quantitative &Mixed Methods
Approaches, (3rd Ed.) Thousand Oaks, CA: Sage Publications Inc.
Creswell, J. W. & Plano Clark, V.L. (2011).Designing and Conducting Mixed Methods
Research. Thousand Oaks, CA: Sage Publications Inc.
Darling-Hammond, L. (2000). Teacher Quality and Student Achievement: A Review of
State Policy Evidence. Education Policy Analysis Archives 5th
Edition. Retrieved on 30th
April 2014 from
http:departments.weber.edu/specialized/Red book.pdf.
Donald, P. (2003).Essential Personality p.37 ISBN 0340761180.
Dangel, H. L., & Keel, M. (2006) Instructional methods of students with mild
disabilities. In R. Colarusso & C.O‟ Rourke (Eds.) Special education for
all teachers 4th
ed. pp.205- 238) Dubuque, 1A: Kendall/ Hunt.

152
Deaf blind International (2003). Deaf Blindness. Retrieved from the web on May 15th
2011. http://www.deafblindinternational.org.
Denzin, N. K. & Lincoln, L.S. (1994). Introduction: Entering the Field of Qualitative
Research. In N.K. Denzin & Y.S. Lincoln (Eds), Handbook of Qualitative
Research. Thousand Oaks: Sage.
Donkervoort, M., Roebroeck, M., Weigerink, D.,Van der Heijden-Maessen H. & Stam,
H. (2007). Determinants of Functioning of Adolescents and Young
Adults with Cerebral palsy: Disability and Rehabilitation, 29.
The Transition Research Group South.
Stam, H. (2007). Determinants of Functioning of Adolescents and Young
Adults with Cerebral palsy: Disability and Rehabilitation, 29.
The Transition Research Group South.
Easter brooks, S. R., & Baker, S. (2004).Language learning in children who are deaf and
hard of hearing: Multiple pathways.Boston:Allyn&Bacon.
Effgen, S. K. (2005). Meeting the physical therapy needs of children. Philadelphia:
F.A.Davis.
Ehri, L. (1998).Grapheme-phoneme knowledge is essential for learning to read words in
English. In J.Metsara & L.Ehri (Eds).Word recognition in
Beginning literacy (pp.3-40).Mahwah, NJ: Lawrence Erlbaum
Associates.
Ellis, N. (1970).Memory process in retardates and normals.In N.Ellis (Ed.).International
Review of research in mental retardation (vol.9, pp.1-32).New York:
Academic press.
Ellis, D. (1986). An Educational Curriculum for Deaf Blind Multihandicapped Persons:
Sensory Impairments in Mentally Handicapped People. London &
Sydney: Croom Helm Publishers.
Emerson, R. S. W. & Corn, A. L. (2006). Orientation and mobility content for children
and youths: A Delphi approach pilot study. Journal of Visual Impairment
and Blindness, 100, 331-342.

153
Fey, M. E., Fitzgerald, Warren, S. F., Brady, N., Finestack, L.H., Bredin-Oja, S.L., Fairchild, M.,
Sokol, S., & Yoder, P. J, (2006). Early Effects of Responsivity Education/
Prelinguistic Milieu Teaching for Children with Developmental
Delays and their Parents Journal of Speech, Language and
Hearing Research. 49,526-547
Ford, A., Schnorr, R., Meyer, L., Black, D. & Dempsey, D. S. (1989). The Syracuse
Community- Referenced Curriculum Guide for students with
Moderate and Severe disabilities: Brookes.
Flechtling, J., Sharp, L. & Westat, L. (1997). User Friendly Handbook for Mixed Method
Evaluations. Division of Research, Evaluation, Communication,
National Science Foundation.
Gachathi Report (1976). The National Committee on Educational Objectives and
Policies (NCEOP) Nairobi: Government printer.
Gay, L. R., (2003).Educational Research. New Jersey: Hearson Education Inc.
Grandin, T. (1995). Thinking in Pictures and Other Reports of My Life with Autism: New
York: Random House Publishers.
Greene, J.W., Caracelli, V.J., & Graham, W.F. (1989). Towards a Conceptual
Framework for Mixed-Method Evaluation Designs.
Hallahan, D. P. & Kaufmann, J. W. (1997). Exceptional Learners Introducing to
Special Education, Seventh Edition. Boston: Allyn & Bacon.
Hallahan, D. P., Kauffmann, J. W. & Pullen, P. C. (2012).Exceptional Learners: An
Introduction to Special Education 12th
Ed. Upper Saddle
River. NJ: Pearson.
Hardman, M. L.; Drew, C. J. & Egan, M. W. (2005). .Human Exceptionality School
Community and Family 8th
edition.U.S.A: Allyn &Bacon.

154
Hatlen, P. (1996). The Core Curriculum for Blind and Visually Impaired Students
Including those with Additional Disabilities. National Agenda Advisory
Board. Retrieved from the web on May 20th
2011.
http://www.tscbvi.edu/Education/corecurric.htm.
Heller, Forney, P. E., Alberto, P. A., Schwartzman, M. N. & Goeckel, T. (2000).
Meeting physical and health needs of children with disabilities: Teaching
students participation and management,Belmont,CA:Wadsworth.
Heller, K. W., Fredrick, L.D., Dykes, M.K., Best, S.J., & Cohen, E.L. (1999).
Competencies in physical/health disabilities. A National perspective.
Exceptional Children, 65, 219-234.
Heller, K. W., & Swine hart- Jones, D. (2003). Supporting the educational needs of
Students with orthopedic impairments .Physical Disabilities:
Education and Related services, 22(1), 3-25.
Heller, W., Forney, P. E., Alberto, P. A., Best,J. S &Schwartzman. N.(2009).
Understanding Physical, Health and Multiple Disabilities (2nd
Ed.).Upper saddle River, New Jersey: Pearson Education inc.
Herring, J. (2002).Tachdijan’sPediatricOrthopedics(3rd
ed.)Philadelphia: W.B.Saunders
Holte,L.,Prickett,J. G.,VanDyke,D. C.,Olson,R. J.,Lubrica,P.& Knutson. L.(2006).
Issues in the management of infants and young children who are
deafblind. Infants &Young Children, 19,323-337.
Hosken, C. (2008). Severe and Multiple Disabilities. Retrieved from the web on
March 8th
2012. http://www.agape biblia.org.
Huebner, K., Nelsen, N. C. & Bietz, E. (1995). Hand in Hand: Essentials of
Communication and Orientation and Mobility for
Your Students who are Deaf Blind. New York: AFB
Press.
Hopcroft, H. (2010). Sensory Room. Retrieved from the web on March 3rd
2013. http://www.premier-solutions.biz.
Huberman, A. M. (1994).Quantitative Data: An Expanded Sourcebook 2nd
Edition.Thousand Oaks,CA:Sage.

155
Jones, M. J., & Gray, J. (2005). Assistive technology: Positioning and Mobility. In
S.K.Eddgen (Ed), Meeting the physical therapy needs of children
(PP.445-474).Philadelphia:F.A.Davis.
Judge, S. L. & Lahm, E. A. (1998).Assistive technology applications for
play,mobility,communication and learning for young children with
disabilities: A guide to family-centered services(pp.16-44)MA
Brookline books.
Kartha, D. (2011) Teaching children with cerebral palsy. Retrieved on the March
12th
2012. http://www.buzzle.com.
Kelly, D. (2005). What is Deafness? U.S.A.: Maryland.
Kenya Institute of Education, (1987). Trends and issues in relation to teacher Education
Curriculum Diploma, 3rd
Unified Draft 1987.
.
Kochung, (2003). A Report on the Task Force on Special Needs Education. Nairobi:
Government Printers.
Koech Report (1999). Totally Integrated Quality Education and Training. Nairobi:
Government Printers.
Koga, N., & Hall, T. (2004).Curriculum modification. Wakefield, MA: National Center
on Accessing the General curriculum.Retrived January 6th
2013
from http://www.cast.org/publications/ncac/_curriculum mod.html
Konstanareas, M. M. (1982). Use of Kinesthetic and Auditory Modalities.
Journal of Autism and Developmental Disorders.
Kombo, D.K. & Tromp, D. L. (2006). Proposal &Thesis Writing: An Introduction.
Nairobi: Pauline Publishers Africa.
Kothari, C. R. (2004).Research Methodology Methods and Techniques, 2nd Edition.
New Age International Limited: New Delhi.
Krathwohl, D. R. (1998). Methods of Educational & Social Science Research: An
Integrated Approach (2nd
Ed).New York: Longman.

156
Kramer, T. & Krug, D. (1973). A rationale and procedure for teaching addition.
Education and training of the mentally retarded, 8,140-144.
Kreulen, M., Smeulders, M. J. C., Veeger, H. E.J., & Hage, J. J. (2006).Movement
patterns of the upper extremity and trunk before and after corrective surgery
of impaired forearm rotation in patients with Cerebral Palsy.
Developmental Medicine and child Neurology, 48,436-441.
Lane, H., Hoffmeister, R. & Bahhan, B. (1996). A journey into the deaf –world.
San Diego: DawnSign Press.
Leyser, Y. (1985). Perspectives of student teachers. The clearing house volume 59 No. 4
Pp.179-181, Taylor & Francis Ltd.
Lewis, S. A. (1981). Curriculum planning for better teaching and learning. Holt,
Newyork: Rinehart and Winston.
Lilienthal, N. (2009). A Preschooler with Autism and Blindness: A Case Study
Unlocking the Mystery of Communication. Retrieved from the Web
on April 20th2011.http://www.speechpathologyguru.com.
Malhotra, N. K. (2004).Marketing Research: An Applied Orientation. 4th
Ed Upper
Saddle River, NJ: Prentice Hall.
Martinez, C. & Moss, K. (1998) .Orientation and Mobility Training: The Way to Go,
Volume3.Retrieved from the web on May 15th
2011.
http://www.498/index
Matson, J. & Long, S. (1986).Teaching computer/shopping skills to mentally retarded
adults. American Journal of Mental Deficiency, 91, 98-101
.
McGee, L., Lomax, R., &Head, M.(1988).Young children’s written language knowledge
What environmental and functional print reading reveals. Journal
Of reading Behaviour, 20, 99-118.
McLaughlin, J., Bjornson, Temkin, N, P., Wright, V. &Reiner, A. (2002). Selective
dorsal Rhizitomy: Meta-analysis of three randomized trials. Developmental
Medicine and Child Neurology, 44, 17-25.
Mc Letchie, A, B. & Riggio, M. (1997).Competencies for Teachers of Learners who are
Deafblind. Reno: Perkins National Deaf Blind Project.
McInnes, J. M. & Treffrey, J. A. (1982).Deaf Blind Infants and Children: A
Developmental Guide .London: University of Toronto Press.

157
Mercer, C. D., & Mercer, A. R. (2004). Teaching students with learning problems
(7 th ed.)Upper saddle River, NJ: Merrill / Pearson Education.
Mercer, C. & Snell, M. (1977).Learning theory research in mental retardation:
Implications for teaching. Columbus, OH: Merrill.
Miles, B. & Riggio, M. (1999) Remarkable conversations: Guide to developing
meaningful communication with children and young adults who
are Deaf blind. Watertown, MA: Perkins School for the blind
Miller, F. (2005). Cerebral Palsy. New York: Springer.
Miles, M. B. & Huberman, A.M. (1994).Quantitative Data: An Expanded Sourcebook
(2nd ed.) Thousand Oaks. CA: Sage.
Ministry of Education Special Programs Branch, (2000) .Teaching Students with Autism:
A Resource Guide in Schools: Victoria: British Columbia.
Ministry of Education, (1995). How to Handle Children with Special
Needs: Guidelines for Teachers, Parents and all
others. Nairobi: Government Printers.
Ministry of Education Science and Technology, (1996). The Deaf Blind Pilot Project
(February1992-1996) Nakuru. Nairobi: Government Publishers.
Ministry of Education, (2009) National Policy on Special Needs Education for Children
with Disabilities. Nairobi: Government Publishers
Ministry of Education Special Programs Branch, (2000) .Teaching Students with Autism:
A Resource Guide in Schools: Victoria: British Columbia.
Ministry of Education Science and Technology, (1996). The Deaf Blind Pilot Project
(February1992-1996) Nakuru. Nairobi: Government Publishers.
Ministry of Education, (2009) National Policy on Special Needs Education for Children
with Disabilities. Nairobi: Government Publishers.
Morgan, D. L. (1998).Practical Strategies for Combining Qualitative& Quantitative Methods:
Applications to Health Research. Qualitative Health Research.
Morse, J. W. (1991). Approaches to Qualitative Quantitative Methodology Triangulation.
Nursing Research.

158
Mont, D. (2007). Measuring Disability Prevalence sponsored by World Bank.
Montgomentry, P. C., & Connolly, B. H. (Eds.) (2003).Clinical applications
For motorcontrol.Thorofare, N, J: SLACK.
Moss, K. & Hagood, L. (1995).Teaching Strategies and Content Modification for the
Child with Deaf Blindness. Texas for the Blind and Visually
Impaired Deaf Blind Project.
Mugenda, G., A. (2008). Social Science Research. Nairobi: Applied Research & Training
Services.
Mugenda, O.M., & Mugenda, A.G. (1999). Research Methods: Quantative & Qualitative
Approaches. Nairobi: Act Press.
National Autism Program, (1998). Autistic Persons with Blindness as an additional
Handicap. Norway: Tambartun National Resource Centre Special for
Education of the Visually Impaired.
National Bureau of Statistics (2009). Population Census Kenya. Retrieved from the web
On March11th
. 2012. http://www.knbs.or.ke/Census%
2520Resultss/KNBS‟
National Institute of the Mentally Handicapped (2003).Voice and Vision
Task Force Hellen Keller Institute for the Deaf and Deaf blind.
Massachusetts: Hilton/Perkins Program of Perkins School for the Blind.
National Research Council, (2001) Educating Children with Autism. Washington, DC:
National Academy Press.
Ndurumo, M. M. (1993) .Exceptional Children Developmental Consequences and
Interventions Nairobi: Longman Kenya Limited.
.
Nehring, W. M. (2004).Cerebral Palsy. In P. J. Allen & J. A.Vessey (Eds.), Primary care
of the child with a chronic condition (4th
ed.,PP.327-
346.) Philadelphia: Mosby.
Nielsen, L. (1998). The Lilli Nielsen FIELA Curriculum in Action: The Sky lands
School Experience. Retrieved from web on
March 8th
2012. http://www.nfb.org/fr/fr9/fro3co14.htm.

159
Ominde Report, (1964). Kenya Education Commission. Nairobi: Government Printers.
Ormrod, J. E. (1999).Human learning (3rd
ed.)Upper saddle River, NJ: Merill Prentice
Hall.
Orodho, J. A. (2005).Techniques of writing Research Proposals &Reports in Education
and Social Sciences 2nd
Ed. Nairobi: Kenzia H.P. Enterprise.
Patel, R. (2002) Phonotary control in adults with Cerebral Palsy and severe
Dysarthria.Augmentative and Alternative communication, 18, 2-10.
Patton, M. Q. (2002).Qualitative Research and Evaluation Methods 3rd
(ed.) Thousand
Oaks, CA: Sage
Pellegrino, L. (2007).Cerebral Palsy. In M.L.Batshaw (Ed.) Children with disabilities
(6th
ed.)PP.387-408).Baltimore: Brookes.
Porter, J., Miller, O., & Pease, L. (1997). Curriculum Access for Deaf Blind Children.
University of London, Institute of Education.
Pricket, J. G., & Welch, R. R. (1995). Deaf-blindness. Implications for learning. In K.M.
Huebner, J.G.Prickett, T.R. Welch, &E.Joffice (Eds.).Hand in hand. Essentials
of communication and orientation and mobility for your students who are deaf-
blind (pp 25-60).New York: AFB Press.
Rain forth, B., York, J. &Macdonald, C. (1997). Collaborative teams for students with
severe disabilities: Integrating therapy and
educational service 2nd
ed. Baltimore: Brookes.
Ratanawongsa, B. (2004). Strategies for teaching learners with Mental Retardation.
Retrieved from the web on May 20th
2011.
http://www.emedicine.medscape.com.
Reiman, J., Malley, J. & Klumph, R. (1998) Research to Practice Focus: Competencies
for Teachers of Learners who are Deaf Blind,
Teaching Research NTAC, Volume6. : Deaf
Blind Perspectives. Massachusetts.
Rice, C. J. and Goessling, D. P. (2005). Recruiting and Retaining Male Special
Education Teachers. Remedial & Special Education, 26(6), 347-356.
Abstract. Accessed from: http://rse.sagepub.com.

160
Richman, S. (2005). .Raising a Child with Autism. London: Jessica Kingsley Publishers.
Robinson, D. M. (2009). A new way to set a Teaching Program for Deaf Blind Students.
Washington: NFB Organization.
Romski, M. A. & Sevcik, R.A. (2005). Augmentative Communication and early
intervention: Myths and Realities ,infants and young chidren,18,174-185.
Rosen, K., &Yampolsky, S. (2000).Automatic speech recognition and
review of its functioning with dysarthric speech. Augmentative and
Alternative communication, 16, 48-60.
Rossman, G. B., & Wilson, B. L. (1985).Numbers and Words. Combining Quantative &
Qualitative Methods in a Single Large Scale Evaluation Study Evaluation
Review.
Rudy, J. L. (2010). Physical therapy and Autism. Retrieved from the web on 26th
June
2013. autism.about.com/od/autismtherapy101 (a (PTbasics.htm
Russman, B. S., & Ashwal, S. (2004).Evaluation of the child with Cerebral
palsy. Seminar in pediatric Neurology, 11, 47-57.
Sankar, C., & Mundkur, N. (2005).Cerebral palsy-definition, classification, etiology and
early diagnosis. Indian journal of Pediatrics, 72,865-868.
Scutta, C. (2011). Competent Learner Model. Retrieved from the web on April 20th
2011 http://www.pattan.net.
Seep,B.,Glosemeyer,R.,Hulce,E.,Linn,M.,&Aytar,P.(2000).Classroom acoustic: A
resource for creating learning environments with desirable
listening conditions. Melville, NY: American Acoustical Society.
.
Sevcik, R. A., & Romski, M. A. (2000).AAC: More than three decades of growth and
development.Asha leader, 5(19),5-6.
Sense International India (2010). Working for Deaf Blind People throughout India.
Retrieved from the web on May 16th
2012.
http://www.senseinternationalindia.org
Shaheen, N. (2009). Without Exception: Teaching the Skills of Blindness to Children
with Additional Disabilities. Baltimore: NFB Jernigan Institute.

161
Shiffrin, R. M. (1999). 30 years of memory. In C.Izawa (Ed.), on the human memory:
Evolution, progress and reflections on the 30th
anniversary of the
Atkinson-Shiffrin model (pp.17-33).Mahwah, NJ: Lawrence
Erlbaum Associates.
Shettle, A. (2004). Deaf children with Additional Disabilities in developing countries.
Retrieved from the web on March11th
2012. http://www.patriot.net/~ashettle/disabilityed.html.
Smith Roley, S., Blanche, E. I., & Schaaf, R. C.(2001).Understanding the nature of
Sensory integration with diverse populations. an Antonio,TX:
Therapy Skill Builders.
Snell, M., & Brown, F. (2006). Instruction of students with severe disabilities (6th
ed.)
Colombus, OH: Merrill/Prentice Hall.
Snell, M. E. J., & Janney, R. (2000).Teachers guides to inclusive practices: Collaborative
teaming.Baltmore: Brookes.
Somekh, B. & Lewin, C. (2005). Research Methods in Social Sciences. London: Sage
Publications Ltd.
Spradley, J. P. (1980). Participant observation. New York: Holt, Rinehart and Winston.
Stivalet, P. (1998).Differences in visual search tasks between congenitally deaf and
normally hearing adults. Cognitive Brain Search, 6, 227-232.
Sullivan. B., Juszcak, E., Bachlet, A., Lambert, B., Vernon-Roberts, A. & Grant, H.W.
(2005).Gastronomy tube feeding in children with cerebral palsy:A
prospective longitudinal study. Developmental Medicine and Child
Neurology, 47, 77-85.
Tashakkori, A., & Creswell, J. W. (2007).The Newa Era of Mixed Methods
(Editorial). Journal of Mixed Methods Research.
Tasse, M. J. (2013). DSM-5: Diagnostic Criteria for Intellectual Disability.
Pittsburgh:PA
Taylor-Powell, E. & Renner M. (2003). .Analyzing Qualitative Data. Madison,
Wisconsin: University of Wisconsin-Extension, Cooperative Extension.

162
Teddlie, C., & Tashakkori, A. (2009).Foundations of Mixed Methods Research.
Thousand Oaks, CA: Sage.
Turnbull, H. R., Turnbull, A.P., & Wilcox, B. L. (2002). Exceptional lives: Special
Education in Today’s Schools (3rd
ed.) Upper Saddle River: Merill-
Prentice Hall .
UNESCO, (1994).The Salamanca Statement and Framework Paris: United Nations,
(1993). Standard Rules on the Equalization of Opportunities for Persons
With Disabilities.Paris:UN.
Universal Declaration of Human Rights (1948). Adopted by the General Assembly
Resolution 2174 (111).
Vacc, N., & Cannon, S. (1991).Cross-age tutoring in mathematics: Sixth graders helping
students who are moderately handicapped. Education and
Training in Mental Retardation, 26, 89-97.
Van Dijk, J. (2001.) Active Learning Theory. Retrieved from the web 11th March, 2012
http://www.tsbvi.edu/materialson-for-educators-becoming-a
good playmate.
Vaughn, S., Bos, C. S. & Schumm, J. S., (2007) Teaching Students who are Exceptional
Diverse, and at Risk (4th
ed.).Boston: Allyn &Bacon.
Verroti, A., Greco, R., Spalice, A., Chiarelli, F., & Iannetti, P. (2006).Pharmacotherapy
of Spasticity in children with Cerebral Palsy. Pediatric Neurology, 34, 1-6.
Vygotsky, L. (1978). Interaction between learning and development. From: Mind and
Society. Cambridge, MA: Harvard University Press.
Wadsworth, D. E., & Knight, D. (1999).Preparing the inclusion classroom for students
with special physical and health needs. Intervention in school and clinic,
24,170-175.
Watson, S. (2003). Definition of multiple disabilities. Retrieved from the web on March
12th
2012 http://specialized about multiple.htm
Wehmann, P. & Parent,W. Ed) (1997). Severe Mental Retardation in Exceptional
Individuals in Schools, Community, (pp145- 173).Texas: PRO-ED.

163
Westling, D. (1986). Introduction to mental retardation. Englewood Cliffs, NJ: Prentice
Hall.
West ling, D., & Fox, L. (1995).Teaching students with severe disabilities. Columbus,
OH: Merrill/Prentice Hall.
Westwood, P. (2003). Common Sense Methods for Children with Special Educational
Needs for the Regular Classroom, 4th Edition
London& New York: Rout ledge Falmer.
Wheless, J. W. (2004). Mental Handicap and Cerebral Palsy. Retrieved from the web
December 29th
2011.http:\\www.epilepsy.com
Wiersma, W. (1986). Research Methods in Education: An Introduction.
Boston: Allyn & Bacon.
Wolff, K. E, Sacks, S. Z., Corn, A. L., Erin, J. N., Huebner, K. M., & Lewis, S. (2002).
Teachers of students with visual impairments’. What are they
teaching? Journal of visual Impairment and Blindness,
96,293-304.
Wood, T. D. (2012). Teacher perceptions of gender-based differences among
elementary school teachers. International Electronic Journal of
Elementary Education, 4(2), 317-345.
Yount, W. R. (2006).Research Design and Statistical Analysis in Christian Ministry, (4th
Edition). Forth worth Texas: School of Education Ministries,
South Baptist Theological Seminary.
Young, M., Baker, J., & Martin, (1990).Teaching basic number skills to students with
moderate intellectual disability. Education and Training
In mental retardation, 25, 83-93.
Young, A. (2007). An Introduction to Total Communication. Retrieved from the web on
June 11th
2011.http://www.helium.com.
Zapf, S. A., & Rough, R. B. (2002).The development of an instrument to match
Individuals with disabilities and service animals. Disability and
Rehabilitation, 24, 47-58.
Zeaman, D., & House, B. (1979). A review of attention theory in N.Ellis (Ed.), Handbook
Of mental deficiency: Psychological theory and research
(2nd
ed., pp.159-223).Hillsdale, NJ: Lawrence Erlbaum
Associates.

164
APPENDIX I
AN INTERVIEW GUIDE FOR THE HEADTEACHERS IN SCHOOLS WITH
LEARNERS WITH DEAFBLINDNESS
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. Are all teachers specially trained to handle learners with deafblindness? If not what are your
recommendations? (Probe on the number of teachers specially trained and their
qualifications).
2. What teaching resources are required for learners with deaf blindness?
(Probe on the availability and effectiveness) if not available or adequate, what are your
recommendations to improve teaching?
3. Do you think the curriculum in use is designed to cater for learners with deafblindness? If not
what are your recommendations to improve teaching? (Probe on the modifications required.)
4. What support services are given to learners with deaf blindness? (Probe for availability and
effectiveness) What are your suggestions on the support services to improve teaching?
165
APPENDIX II
INTERVIEW GUIDE FOR THE HEADTEACHERS IN SCHOOLS WITH
LEARNERS WITH AUTISM BLINDNESS
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. Are all teachers specially trained to handle learners with autism blindness? If not what are
your recommendations?(Probe on number of teachers specially trained and their
qualifications)
2. What teaching resources are required for learners with autism blindness? (Probe for their
availability and effectiveness? If not available what are your recommendations to
improve teaching?
3. Do you think the curriculum in use is designed to cater for learners with autism
blindness? If not what are your recommendations to improve teaching?(Probe on the
modifications required)
4. What support services are given to learners with autism blindness? (Probe on special diet,
auditory training and medical services among others (Probe on the availability and
effectiveness of the support services)

166
APPENDIX III
INTERVIEW GUIDE FOR THE HEADTEACHERS IN SCHOOLS WITH
LEARNERS WHO HAVE CEREBRAL PALSY INTELLECTUAL DISABILITY
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. Are all teachers specially trained to teach learners with multiple disabilities? If not what are
your recommendations? (Probe on number of teachers specially trained and their
qualifications)
2. What teaching resources are required for learners with cerebral palsy intellectual disability?
(Probe for their availability and effectiveness). If not available, what are your
recommendations?
3. Do you think the curriculum you use is designed to cater for the learning needs of
learners with multiple disabilities? If not what are your recommendations? (Probe on the
required adaptations.)
4. What support services are given to learners with cerebral palsy intellectual disability? Are the
support services available? If not what are your recommendations on support
services to improve teaching?

167
APPENDIX IV
INTERVIEW GUIDE FOR THE TEACHERS TEACHING LEARNERS WITH
DEAFBLINDNESS
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. What guides you in the choice of the instructional strategies for learners with deaf-blind?
(Probe on level of severity, age level among others)?
2. What are the various instructional strategies that you use with learners who are deaf-blind?
(Probe for the effectiveness of the stated strategies).
3. Do you think the curriculum you use is designed to cater for learners with multiple
disabilities? If not what are your recommendations to improve teaching?
4. Do you think you are competently trained to teach learners with deaf-blind?
If not, what are the training needs that you require?
5. What teaching resources are available in your school for learners with deaf- blind
(probe on the effectiveness and availability of the stated teaching resources).
6. What support services are given to learners with deaf-blind in your school?
(Probe for the availability and effectiveness and recommendations on the improvement of
stated support services
7. What suggestions would you recommend on the instructional strategies to improve teaching?
(Probe on retraining on new techniques, curriculum adaptations among other s).

168
APPENDIX V
INTERVIEW GUIDE FOR THE TEACHERS TEACHING LEARNERS WITH
AUTISMBLINDNESS.
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. What guides you in the choice of the instructional strategies/methods for learners who are
autistic blind?
2. What are the various instructional methods that you use with the learners who are autistic
blind? (Probe for the effectiveness of the various instructional strategies).
3. Do you think the curriculum you use is designed to cater for learners with multiple
disabilities such as autistic blind? If not what are your recommendations? (Probe on the
required adaptations)
4. Do you think you are competently trained to serve learners with autism blindness? If not,
what are the training needs that you require?
5. What teaching resources are available in your school for learners with autism
blindness? (Probe for their effectiveness and availability of tactile diagrams,
braillers, computers among others).
6. What support services are given to learners with autism blindness in your school?
(Probe for the availability and effectiveness) If not, available what
recommendations would you give for the improvement of the stated support
services.?
7 .What suggestions would you recommend on the instructional strategies to
improve teaching? (Probe on retraining on new techniques, curriculum adaptations).

169
APPENDIX VI
INTERVIEW GUIDE FOR THE TEACHERS TEACHING LEARNERS WITH
CEREBRAL PALSYINTELLECTUAL DISABILITY.
This interview is part of an educational study that is being conducted by the researcher in the
institution. The information will be treated with utmost confidentiality during and even after the
study. The researcher is therefore requesting for your co-operation and assistance. The
information you give will be very important for this study.
1. What guides you in the choice of the instructional strategy that you use for learners with
cerebral palsy intellectual disability? (Probe on age level, level of disability among
others).
2. What are the various instructional strategies for learners with cerebral palsy intellectual
disability? (Probe for the effectiveness of the stated strategies)
3. Do you think the regular curriculum is designed to cater to for learners with multiple
disabilities? If not what are your recommendations? (probe on the required adaptations).
4. Do you think you are competently trained to serve learners with cerebral palsy
intellectual disability? If not, what are the training needs that you require?
5. What available teaching resources do you have for learners with cerebral palsy
intellectual disability? (Probe for mobility aids, page turners, and computer assisted
instructions among others.
6. What support services are given to learners with cerebral palsy intellectual disability?
(Probe for the effectiveness and suggestions on the improvement of the stated support
services?
7. What suggestions would you recommend on the instructional strategies to improve
teaching? (Probe on retraining on the new techniques, curriculum adaptations among
others).

170
APPENDIX VII
QUESTIONAIRES FOR TEACHERS EDUCATING LEARNERS WITH CEREBRAL
PALSYINTELLECTUAL DISABILITY.
Dear respondent,
INSTRUCTIONS
Please tick the column which most represents your views of the following statements. There is
no correct or wrong answer. The best answer is the one that honestly reflects your views. Please,
your name should not appear on your questionnaire.
QUESTONAIRE FOR TEACHERS
Section A: Personal details and general information. Please fill in.
1. Gender Male___________ Female____________
2. Designation Deputy Head ____________
Senior Teacher____________
Teacher__________________
3. Number of years in the school____________________
4. What are your professional qualifications?
Certificate (SNE) _______________ Diploma (SNE) _________________
Degree (SNE) _______________ M.E.D (SNE) _______________
Others (specify) _______________
5. Experience 1-5years___________ 5 years______________ 10-15 years___________
16 years and above___________

171
Key
Strongly agree – SA
Agree – A
Undecided-UN
Disagree-D
Strongly Disagree-SD
Please honestly indicate the extent to which you agree with these statements.
Instructional Methods SA A UN D SD
1. Teachers make use of real objects
2. Breaking down tasks into simpler activities
3. Use of pointers
4. Use of pencil grips
5 Use of page turners
6. Use of computer assisted instruction
7. Use of adapted computers
8. Use of communication boards
9 Use of gestures
10. Use of pointing
11. Use of writing
12. Use of the pre-linguistic milieu teaching
13. Use of pictures
14. Use of observations & demonstrations
15. Use of group work
16. Use of video and audio based curriculum

172
APPENDIX VIII
QUESTIONAIRE FOR THE TEACHERS OF LEARNERS WITH DEAFBLINDNESS
Dear respondent,
INSTRUCTIONS
Please tick the column which most represents your views of the following statements. There is
no correct or wrong answer. The best answer is the one that honestly reflects your views. Please,
your name should not appear on your questionnaire.
QUESTONAIRE FOR TEACHERS
Section A: Personal details and general information. Please fill in.
1. Gender Male___________ Female____________
2. Designation Deputy Head ____________
Senior Teacher____________
Teacher__________________
3. Number of years in the school____________________
4. What are your professional qualifications?
Certificate (SNE) _______________ Diploma (SNE) _________________
Degree (SNE) _______________ M.E.D (SNE) _______________
Others (specify) _______________
5. Experience 1-5years___________ 5 years______________
10-15 years___________ 16 years and above__________
Key

173
Strongly agree – SA
Agree – A
Undecided-UN
Disagree-D
Strongly Disagree-SD
Please honestly indicate the extent to which you agree with these statements
Instructional Methods SA A UN D SD
1. Teachers make use of real objects
2.
Breaking down tasks into simpler activities
3. Allow enough time for task completion
4. Teaching learners how to make a choice
5. Use of behavior management programmes
6. Use of calming or soothing activities
7. Hand over hand guidance, tactual sign
language
8.
Coactive signing
9. Tadoma,Lip reading, body language
10. Use of tactile diagrams
11. Use of speech paired with Braille
12. Use of speech paired with Kenyans sign
language
13. Use of Kenyan sign language
14. Use of routine, calendar system and
discussion boxes
15. Use of the Deafblind manual alphabet
16. Use of objects of reference or pointing
17. Use of experience and picture board
18 Use of Lilli Nielsen resonance board
19 Use of teaching teachable moments

174
APPENDIX IX
QUESTIONAIRE FOR TEACHERS EDUCATING LEARNERS WITH AUTISM
BLINDNESS
Dear respondent,
INSTRUCTIONS
Please tick the column which most represents your views of the following statements. There is
no correct or wrong answer. The best answer is the one that honestly reflects your views. Please,
your name should not appear on your questionnaire.
Section A: Personal details and general information. Please fill in.
1. Gender Male___________ Female____________
2. Designation Deputy Head ____________
Senior Teacher____________
Teacher__________________
3. Number of years in the school____________________
4. Certificate (SNE) _______________ Diploma (SNE) _________________
Degree (SNE) _______________ M.E.D (SNE) _______________
Others (specify) _______________
5. Experience 1-5years___________ 5 years______________
10-15 years___________ 16 years and above____________
Others (specify) _______________

175
Key
Strongly agree – SA
Agree – A
Undecided-UN
Disagree-D
Strongly Disagree-SD
Please indicate honestly the extent to which you agree with these statements
Instructional Methods SA A UN D SD
1. Use of speech paired with tactile strategies
2. Use of real objects(rice,maize,beans among others
3. Use of supplementary aids (e.g. slates & stylus, abacus,
cuberithms)
4. Use of tactile Kinesthetic and auditory modalities
5. Use of frequent stretch breaks
6. Use of auditory activities
7. Use of Kinesthetic learning activities
8 Use of consistent schedules
9. Use of Braille as a mode of communication
10. Use of large print, optical devices
11. Use of regular print
12. Use of recorded materials to communicate
13. Orientation and mobility
14. Independent living skills
15. Use of behavior management strategies.
17. Use of two handed sign language paired with speech.

176
APPENDIX X
OBSERVATION GUIDE FOR USEBY THE RESEARCHER IN SCHOOLS FOR
LEARNERS WITH DEAFBLINDNESS.
ITEM SPECIFIC ITEM CONDITION COMMENTS
Teaching strategies
Developing an IEP
Instructional methods
in use.
Teaching Resources Real objects, use of
experience book
among others
Classroom Adapted desks,
arrangement of the
room among others
Curriculum Specialist curriculum
Support Services Speech therapy,
occupational therapy
among others
Specialized equipment Adapted computers,
Hoyer Hydraulic lifts
among others
Physical environment Barrier free, ramps
among others

177
APPENDIX XI
OBSERVATION GUIDE FORUSE BY THE RESEARCHER IN SCHOOLS WITH
LEARNERS WITH AUTISM BLINDNESS
ITEM SPECIFIC ITEM CONDITION COMMENTS
Teaching strategies
Developing an IEP
Instructional methods
in use
Teaching Resources braillers, white cane
among others
Classroom Arrangement of the
room, use of routines.
Curriculum Adapted curriculum
among others
Special Diet Gluten free, casein
free among others
Support Services Speech therapy,
language pathology
among others
Specialized equipment Adapted computer,
global positioning
device among others
Physical Environment Barrier free among
others

178
APPENDIX XII
OBSERVATION GUIDE FOR USE BY THE RESEARCHER IN SCHOOLS WITH
LEARNERS HAVING CEREBRAL PALSY INTELLECTUAL DISABILITY
ITEM SPECIFIC ITEM CONDITION COMMENTS
Teaching strategies
Developing an IEP
Instructional methods
in use: Antecedent
prompting, , task
analysis among others
Teaching Resources Page turners, paper
grips, AAC devices,
manual signs, adapted
pens, adapted pencils
among others
Classroom
Adapted desks
wedges Prone stander
Mechanical lifts
Curriculum Specialized
curriculum
Mobility devices Braces, splints,
walking frame,
wheelchairs
Support services Physiotherapy, speech
therapy, among
others.
Specialized equipment Adapted computers,
electric wheel chairs
among others

179
AP PENDIX XIII
RESEARCH PERMIT