Tbi essentials wsu
264
Traumatic Brain Injury (TBI) Essentials
-
Upload
david-nowell -
Category
Health & Medicine
-
view
488 -
download
2
description
Traumatic Brain Injury (TBI) Essentials: workshop at Worcester State University
Transcript of Tbi essentials wsu

Traumatic Brain Injury (TBI)Essentials

Today’s Schedule• 8-8:30 Registration
• What is Traumatic Brain Injury & Screening for TBI-related deficits
• 10-10:15 Break
• How TBI Impacts Executive Functioning & Populations at Greater Risk for Brain Injury
• 12-1 Lunch
• Locating Community Supports and Services for Head Injured Clients
• 2:15-2:30 Break
• Counseling Brain Injury Survivors and Their Families• 3:45-4:00 Question and Answer

Overview
• Epidemiology• Mechanisms of Injury• Deficits Associated with TBI• Identification• Treatment• Special cases

#tbiwsu

EPIDEMIOLOGY

National prevalence rates of various disabilities
400,000 with Spinal Cord Injuries
500,000 with Cerebral Palsy
2.3 million with Epilepsy
3.0 million with Stroke-related Disabilities
4.0 million with Alzheimer’s Disease5.3 million with Traumatic Brain Injury
5.4 million with persistent Mental Illness
7.2 million with Mental Retardation

In the United States, at least1 million sustain a TBI each year
Incidence

Causes of TBI

Who is at Highest Risk for TBI?
• Males 1.5 times as likely as females to sustain a TBI
• Two age groups most at risk are 0-4 year olds and 15-19 year olds, and
• The elderly, frequently from falls• African Americans have the highest death rate
from TBI

Incidence of TBI x Age and Gender

MECHANISMS OF INJURY

Types of Brain Injuries
Acquired Brain Injuries
Traumatic Brain Injuries Other Brain Injuries:•Strokes•Hydrocephalus•Tumors•Demyelinating disorders•Infections•Toxic encephalopathy•Anoxic/hypoxic injury
Penetrating Closed Head Injury


Causes of TBI

Mechanisms of Injury
• Primary mechanisms of injury– Contusions– Small vessel disruption– Diffuse axonal injury

Coup-Contra Coup




Hematoma



Mechanisms of Injury
• Secondary mechanisms of injury– Edema– Evolving hematoma– Hydrocephalus


Normal ventricles

Managing intracranial pressure

Introduction to Neuroanatomy

Introduction to Neuroanatomy
What’s different about the brain?

Neuron

Synapse

Peripheral and Central Nervous System

Introduction to Neuroanatomy
• Front – back x
• Top – bottom
• Left - right

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
33
what IS…

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
34
…what COULD BE

Introduction to Neuroanatomy
• Front – back
• Top – bottom
• Left – right x


?

Frontal Lobe

Temporal Lobe

Parietal Lobe

Occipital Lobe

Limbic System

Cerebellum

The Ventricles

Normal ventricles

DEFICITS ASSOCIATED WITH TBI

Medical• Physical stamina• Pain• Headaches• Seizures (within 2 years of injury)• Bowel/bladder continence

Motor Functioning
• Paresis or spasticity• Gross motor strength• Fine-motor speed and dexterity• Motor coordination and planning• Spatial-based movement• Oculomotor • Balance

Sensory-Perceptual Abilities
• Tactile, visual, and auditory modalities• Sometimes, olfaction

Attention
• Alertness and arousal.• Selective or focused attention.
– Modality specific• Sustained attention (vigilance).• Span of attention.• Hemi-neglect (ignoring one side of the body).

Receptive Language
• Word and phrase comprehension• Conflictual and comparative statements• Vocal tone and prosody• Speed of processing• Pragmatics (social meaning in language)

Expressive Language
• Fluency• Naming• Word and phrase repetition• Organization of output (e.g., spontaneous versus
confrontational speech)• Vocal tone and prosody• Pragmatics (social use of language)

Memory and Learning

The Executive Functions
X



Places
• San Jose• Aberdeen• Paris• Hattiesburg

Places
• San Jose• Aberdeen
• Paris• Hattiesburg

Boys’ Names
• Dante• Pete• Jordan• Elvis

Boys’ Names
• Dante• Pete
• Jordan• Elvis




“a healthy well-adjusted 26 year old”


The Executive Functions• Inhibition
• Shift
• Regulation
• Initiation
• Working memory
• Planning / organizing
• Self-monitoring

The Executive Functions
• Bridging the now with the past
• Bridging the now with the future

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
68

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
69
1. 1-step errands
2. Chores with cues
3. Basic inhibition
Age-appropriate ExpectationsPreschool

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
70
1. 2-3 step directions
2. Bring papers home
3. 20-30 minute assignments
4. Simple spending decisions
5. Follow rules/inhibit/no grabbing
Age-appropriate ExpectationsKindergarten -2nd Grade

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
71
1. Simple shopping list
2. Keep track of personal items
3. Longer homework assignments
4. Simple project planning
5. Keep track of variable daily schedule
6. Save money
7. Inhibit and regulate even without teacher present
8. Manners
9. Simple delayed gratification (phone)
Age-appropriate Expectations3rd-5th Grade

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
72
1. Complex chores
2. Babysitting
3. Organizing system
4. Complex schedule
5. Longer term projects
6. Time management
7. Self soothe
8. Manage conflict
Age-appropriate Expectations6th – 8th Grade

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
73
1. Independent with assignments
2. Make adjustments based on feedback
3. Longer term goal setting
4. Manage leisure time
5. Inhibit reckless behavior
6. Easily walk away from provocation
7. Say “no” to fun activity if other plans already made
8. Take others’ perspective
Age-appropriate ExpectationsTeenage-mid 20’s

School and Vocational Outcomes• Problems initiating and completing work.• Slowed work pace.• Increased impulsivity.• Trouble navigating physical surroundings.• Decreased productivity.

School and Vocational Outcomes• Confusion and increased stress.• Resistance to change.• Trouble with generalization of new learning.• Distractible.• May resent special assistance.

Social-Behavioral Outcomes
• Loss of friends and social circles.• Decreased affective regulation.• Increased impulsivity.• Increased agitation.

Social-Behavioral Outcomes
• Poor perspective taking.• Comparison to preinjury level of functioning.• Poor understanding of TBI and recovery.• Premature return to school/work.• Unrealistic predictions.

Emotional
• Dependent behaviors / amotivation• Irritability / emotional lability / anger• Depression• Disinhibition• Denial/lack of insight• At risk for substance abuse

Who Gets Better? Predictors of Positive Outcome
x

Preinjury Predictors of Positive Outcome
• History of good academic achievement• Good social relationships• No history of learning, attention, or behavioral
difficulties• No history of substance abuse• No significant family problems

Preinjury Predictors of Positive Outcome
• Strong-willed and determined• Under 21 years of age• No previous neurological history (e.g., a prior
TBI)• Good self regulation skills

Preinjury Predictors of Positive Outcome
• No criminal history• Good relationships with family members• Warm and supportive family• No psychopathology

Behavioral Predictors of Positive Outcome
• Motivated and persistent• Optimistic• Has the capacity to recognize errors and self-
correct• Aware of behavioral deficits• Ambulatory

Behavioral Predictors of Positive Outcome
• Relatively independent with activities of daily living
• Initiates tasks with no/minimal assistance• Preserved perspective-taking capacity• Relatively preserved neurocognitive abilities

Environmental Predictors of Positive Outcome
• Individual treatment plans• Continuity and coordination of treatment
throughout the recovery process• Structure, consistency, and repetition in daily
activities• Good, stable resources (e.g., financial, family,
friends, community, etc.)

Environmental Predictors of Positive Outcome
• Presence of “key” person in the family• Family involved in the treatment plan• Family realistic about individual’s status• Presence of “key” person on team

Neurological Predictors of Positive Outcome
• Coma < 6 hours• PTA < 24 hours• GCS > 7• Normal EEG and MRI• Normal intracranial pressure• Normal ventricle size• No intracranial hematoma

Indices of Severity of TBI
• Intracranial Pressure• Retrograde Amnesia• Anterograde Amnesia/Post-traumatic Amnesia• Duration of Loss of Consciousness (LOC)• Glasgow Coma Scale score• Rancho Los Amigos Scale (1 to 10)

Indices of Severity of TBI

Mild injury0-30 minute loss of consciousness
Moderate injury
30 minutes to 24 hours LOC
Severe injury> 24 hours LOC

IDENTIFICATION OF TBI

Identification of TBI
• Obtain the medical records if possible• Interview family/friends for collaboration• Arrange for a neuropsychological evaluation• Refer to a neurologist or psychiatrist for medication
and behavioral consultation• Consider referral to a brain injury rehabilitation
program

Inquiry Regarding TBI
• Any history of concussion or head injury?• Ever been knocked out?• Note: this question may lead to discussion of
– Alcohol abuse– Domestic violence
• Postconcussive symptoms?• Return to work/school?

• When did you wake up from the head injury? Do you remember being transported to the hospital? Do you remember being in the trauma unit? Being transferred to the rehab unit?
• PTA: period of time after the CHI for which the patient has no memory
“Getting at” PTA in the clinical interview

Comprehensive Mental Status Examination
• Behavior• Emotion• Cognition

ABC STAMPLICKER

ABC STAMPLICKER• appearance

ABC STAMPLICKER• behavior

ABC STAMPLICKER• cooperation

ABC STAMPLICKER• speech

ABC STAMPLICKER• thought
–Form–Content

ABC STAMPLICKER• affect

ABC STAMPLICKER• mood

ABC STAMPLICKER• perception

TO ORIENT
To understand one’s
relationship to theenvironment

ABC STAMPLICKER• level of arousal

ABC STAMPLICKER• insight

Judgment
• The ability to weigh and compare the relative values of different aspects of an issue.

ABC STAMPLICKER• cognition

ABC STAMPLICKER• knowledge

ABC STAMPLICKER• endings

Risk Assessment Protocol
• Identify predisposing factors• Examine potentiating factors• Conduct a specific suicide inquiry
Ideation?Plan?Intent?
• Determine level of intervention• Documentation

ABC STAMPLICKER• reliability

Diagnostic Issues
• Cognitive Disorder NOS• Dementia Due to Head Trauma

Diagnostic Issues
• Distinguishing psychiatric from TBI-related impairment– Insight/denial/anosagnosia– Explosive behavior disorders– Pseudodementia– “Acquired ADHD”?

TBI TREATMENT

Considerations in TBI Recovery
• What constitutes “recovery”• Will he/she be 100%?• It takes a year?• “Plateaus”• The normal neurological evaluation• Independence and modified independence• No magic bullets
– Meds– Rehab technologies

Medical Management: Acute TBI
• Airway• Close monitoring for edema• Seizure control• Close monitoring for increased intracranial
pressure

Normal ventricles

Increased intracranial pressure

ICP monitor

Pharmacological Treatments
• Amantadine x• Anti-seizure agents• Antipsychotics• Antidepressants • Stimulants


Pharmacological Treatments
• Amantadine x• Anti-seizure agents• Antipsychotics• Antidepressants • Stimulants

Early Rehabilitation Efforts:
• Formal family meetings• Use of an interdisciplinary team approach in
overall treatment• Discharge planning by team members, family,
and community services

Referrals

Referrals
Brain Injury and Statewide SpecializedCommunity Services

Referrals
• Assistive technologies• Independent living skills training• Speech therapy• Occupational therapy• Physical therapy• Neurology • Psychiatry• Physiatry• Substance abuse treatment

Referrals
• Case management• Home modifications• Transportation• Cognitive rehabilitation• Counseling• Financial management• Respite care• Neuropsychological evaluation

Goals of Neuropsychological Assessment
• Determine spared versus impaired abilities.• Understanding impact of injury and/or a
neurodevelopmental problem (e.g., LD).• Assist in localization of function and
dysfunction.

Goals of Neuropsychological Assessment
• Assist in determining whether to remediate or to compensate.
• Generate suggestions for remediation and compensation.
• Suggestions for monitoring and tracking of progress in school setting.

When to Consider a Referral to Neuropsychology
• Documented brain injury/insult• Suspected brain injury or insult• Neurodevelopmental disorder• Unusual psychological profile• Positive neurological findings• Severe behavior problems• Treatment needs

Cognitive Rehabilitation
• 4 ways our patients “get better”– Brain healing– Brain re-organization / plasticity– Compensatory skills– Restructuring the environment


Cognitive Rehabilitation:Specific Approaches
• Psychometric approach (healing/plasticity)• Stimulus-based approach (restructuring the
environment)• Developmental approach (plasticity and
compensatory)• Behavioral engineering approach
(compensatory skills)










Cognitive Rehabilitation
• Research challenges• Cognitive orthotics and prosthetics



Yoga / read
Staff meeting
Planningsession
Phone calls
billing

Vh: jeff w/ puritan oil
Vc: kate re: brimfield
TC umass dermatology. Spoke w/ cindy 508 8564000





Learn French
Stop smoking
Be a better spouse

Vh: jeff w/ puritan oil
Vc: kate re: brimfield
TC umass dermatology. Spoke w/ cindy 508 8564000

Learn French
Stop smoking
Be a better spouse
Call umass dermatolody - cindy 508 8564000

Yoga / read
Staff meeting
Planningsession
Phone calls
billing

The “Good-Fit” Personal Organizer for the Client with Executive Dysfunction
• 2 pages per day• 7 am to 9 pm• Contains a master to-do list• With the client at all times• Use for work and home• Have only one system

Use of the personal organizer or PDA
• Move it from your head to your calendar• Break long term goals into action items• The organizer is your budget – how you
“spend” your time• Use your organizer for every part of your life

Use of the personal organizer or PDA
• Use your organizer for every part of your life– Your to-do list should contain things you have to do, but
also things you want to do, or to be, or to have.– You make appointments with your doctor or insurance
agent, because they’re important. You can make appointments with yourself as well.
– “Hi Cindy, this is David…..” (win friends and influence people with your amazing phone log)


04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
162
easy hard


“error-free learning”

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
165

Psychotherapy with the brain-injured client
• Mild TBI interventions• Severe TBI interventions

Psychotherapeutic InterventionsIndividual Therapy
• Permitting appropriate expression of emotional reaction to TBI and loss
• Patient education• Social skills training• Family/spouse involvement• Impact of memory problems and decreased
insight

Psychotherapeutic InterventionsIndividual Therapy
• Critical for the therapist to be TBI-savvy• Consider the environment in which the person
functions• “Lieben und arbeiten”

Psychotherapy with the brain-injured client
• Develop routines• Energy conservation


Psychotherapy with the brain-injured client
• Values and motivators

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
172


Psychotherapy with the brain-injured client
• Self-esteem

Self - esteem

Activity Scheduling



Psychotherapy with the brain-injured client
• Substance abuse and dependence

Psychotherapeutic InterventionsGroup Therapy
• Modeling• Problem solving• Peer feedback• Social skills practice

Behavioral Therapies
• Very few people with TBI have fully lost the ability to learn new behaviors
• Structure, consistency, and repetition• Role of cognition in self regulation• External feedback

• This requires a measurable and precise definition of the target behavior– Always get specific examples– Cross check across settings– “Pick your battles”?
• Inquire about the antecedents and consequences
Behavioral Strategies:Defining the Problem

Behavioral Strategies:Identifying the Function
• Everybody’s doing the best he/she can• Every behavior serves a function• Every behavior problem is either
– A skills deficit, or– A contingency problrm

Behavioral Strategies:Identifying Resources
• Personal resources: Memory? Flexibility? Persistence? Motivation?
• Social / family / peer resources• Organizational resources

Behavioral Strategies:Guidelines
• Skills• Safety• Least restrictive• Managing the antecedent: Set me up for
success!

Examples of Behavioral Strategies• Antecedents
• Does not understand
• Does not begin task
• Unable to do task
• Is not motivated
• Interventions• Provide clear, concrete instructions; notes
• Give prompts; reinforce initiative
• Simplify task; provide skill-based training
• Increase interest or relevance; reward for task completion

Examples of Behavioral Strategies
Consequences• Avoids failure by not
complying• Gets out of work• Receives attention for
not doing task• Gets to assert
independence/control
InterventionsAlternate difficulty
tasks with easy onesPremack principleTime out or ignoring;
reinforce for attentionOffer choices when
appropriate

Behavior Management Strategies:
X

Behavior Management Strategies:Agitation and Irritability

Behavior Management Strategies:Agitation and Irritability
• Redirection• Offer an alternative activity • Relaxation strategies• Recognize antecedent conditions• Speak calmly• Use key familiar phrases

Behavior Management Strategies:Apathy

Behavior Management Strategies:Apathy
• Give choices between doing one thing or another; not between doing and not doing
• Activity scheduling, in advance

Behavior Management Strategies:Denial/Lack of Insight

Behavior Management Strategies:Denial/Lack of Insight
• Have ongoing discussions of “strengths and needs”
• Create discrepancy• This may be the most difficult problem to
address

Behavior Management Strategies:Impulsivity/Disinhibition

Behavior Management Strategies:Impulsivity/Disinhibition
• Structured and organized daily routine• Rewarding/praising impulse control and
inquiring “how exactly did you do that?”• “Talking stick”

Behavior Management Strategies:Depression/Withdrawal

Behavior Management Strategies:Depression/Withdrawal
• Help students identify preserved abilities and strengths - rather than focusing on their deficits
• Keep TBI survivor involved in the present rather than dwelling on the past
• Use active listening techniques, but focus on positive feelings

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
199
AANTECEDENTS
BBEHAVIOR
CCONSEQUENCE
S

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
200
AANTECEDEN
T
BBEHAVIOR
CCONSEQUENC
ES

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
201
AANTECEDEN
T
BBEHAVIOR
CCONSEQUENCES

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
202
AANTECEDENTS
BBEHAVIOR
CCONSEQUENC
ES

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
203

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
204
AANTECEDEN
T
BBEHAVIOR
CCONSEQUENC
ES
metacognition

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
205
Beginning Middle End

04/10/2023 © 2011 David D. Nowell, Ph.D. All rights reserved.
206
AANTECEDEN
T
BBEHAVIOR
CCONSEQUENCES

Treating Sensory Defensiveness

Addressing Visuomotor Problems with Reading

What’s the kid’s deal?
• Greene, Ross. The Explosive Child.

Family Issues and Needs
• Family stress related to severity of TBI• The family’s resilience may be key to a brain
injured child’s successful rehabilitation• Divorce rates range from 15% to 54%

Sources of Family Stress
• Uncertainty about recovery• Cognitive and personality changes• Financial strain• Transitions to “new” settings• Lack of respite care

Family Definition of the Event

Family Issues and Needs• Family’s adaptation may take years• Any change may trigger emotional
response• Watch for signs of grieving

Return to School
• Accommodations and Modifications• IDEA and Section 504

IDEA Definition of TBI:
An acquired injury to the brain caused by an external physical force resulting in functional disability or psychosocial impairment that adversely affects a child’s educational performance.

School Re-Entry Issues
• Educational consultation should begin before return to school
• Continuity of care between school and rehabilitation services
• Prepare for multiple transitions• Re-entry should include interdisciplinary
support

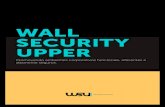
Percentage Referred for Services
23.7
13.2
10.1
2.8
2
1.8
3.6
Physical therapy
Ocupationaltherapy
Speech therapy
Family counseling
Psych. services
Special Ed.
Home Tutor

Basic Criteria for School Re-Entry
• Attends to a task for 10 to 15 minutes– Adjust for age
• Can tolerate 20 to 30 minutes of classroom stimulation
• Can function adequately in a group of 2 or more students
• Engages in meaningful communication• Follows simple directions accurately• Gives some evidence of learning potential

School Re-Entry Procedures
• Assess needs–Adaptive domain–Cognitive domain –Communication domain–Sensorimotor domain –Social-emotional-behavioral domain–Transportation needs–Family needs

School Re-Entry Procedures• Identify the best setting for intervention
– Outpatient counseling?– Home-based family interventions?– School-based SLP / OT?– Buddy system at school?– In-service for school staff?– Modified school day?– In-school breaks?– “Study halls” with resource teacher?– Pre-vocational training?
• Regular re-evaluation for change over time

Developing IEP Goals
• Focus on 2 or 3 priority issues• Identify metacognitive & organizational strategies• Write measurable goals that incorporate the
strategies• Include specific information about how the
strategy should be taught and implemented across settings
• Write short-term goals that are truly short-term

TBI Impact at School
• Problems initiating and completing work.• Slowed work pace.• Increased impulsivity.• Topographical disorientation• Distractible• Difficulty generalizing new learning

Classroom Management
• Two key factors :– Structure – Motivation
• Explicitly teach rules & expectations• Establish prompts or cues, such as gestures
and reminder cards

Classroom Management
• Can students answer the following questions:– What do I have to do?– How much do I have to do?– When am I finished?– What do I do next?

Classroom Management
• Use repetition & feedback• Avoid multi-step instructions• Supplement verbal instructions with
nonverbal / modeling• Provide additional time for information
processing• Assist with organization of materials and
schedule

Classroom Management
• To be motivating, a task must be interesting• Intersperse difficult or novel tasks with easy or
previously learned ones• Distinguish cognitive factors from other issues
(impact of headache, or depression)

Specific Classroom Strategies:Attentional Processes
• Reward on-task behavior;• Use novel, unusual, relevant or stimulating
activities• Redirect• Remove unneccessary distractors• Explore a variety of cueing systems
– Verbal cues– Physical prompts– Gestural cues

Specific Classroom Strategies:Attentional Processes
• Reduce the number of individual tasks on a printed page
• Reduce the amount of copying from the board• Provide a ruler or EZ-Reader to focus visual
attention• Avoid asking a student to multi-task• Chunking / Pomodoro

Specific Classroom Strategies:Memory and Learning
• Enhance the saliency of material• Regularly summarize information as it is
being taught• Dry-erase board• Use overlapping techniques, such as
repetition and rehearsal

Specific Classroom Strategies:Memory and Learning
• Couple new information with previously learned information
• Identify in advance the key information to be learned
• Make use of over-learning

Specific Classroom Strategies:Language
• Limit length and complexity of communication• Do not use figurative speech• Recognize the student may not understand
humor or sarcasm

Specific Classroom Strategies:Language
• Reminders to start, end, or repair a conversation
• Use question prompts to help the student share more information, especially in groups
• Allow for slowed information processing

Specific Classroom Strategies:Language
• Speak slowly• Reduce background noise

Specific Classroom Strategies:Visual Processing
• Provide longer viewing times or repeat viewings when using visual instructional materials
• Facilitate a systematic approach to reading and math by covering parts of the page
• Provide support for orientation to building and grounds
• Limit visual distractions (web page, handouts, text, desk)

Specific Classroom Strategies:Executive Functions
• Problem Solving Processes• Develop a problem-solving guide to help student through the
stages of problem solving– Identifying the problem– Acquire relevant information– Generate several possible solutions– List pros and cons for each solution– Identify best solution– Create a plan of action– Evaluate the effectiveness of the plan– Encourage generalization

Specific Classroom Strategies:Executive Functions
• Raise questions about alternatives and consequences
• Provide ongoing, non-judgmental feedback• Provide part of a sequence and have the
student finish it• Frequent cues re: main topic vs. supporting
ideas

Specific Classroom Strategies:Executive Functions
• Note impact of fatigue on cognition• Note impact of some medications• Consider reduced workload• Consider note-taker• “How exactly did you do that?”

SPECIAL CASES

SPECIAL CASES
• Domestic violence• Shaken baby syndrome• Combat trauma• Alcohol abuse/dependence• Mild TBI

SPECIAL CASES
• Domestic violence

In women reporting to ERs for injuries associated with DV:
• 30% of battered women reported a loss of consciousness at least once.
• 67% reported residual problems that were potentially head-injury related.
(Corrigan 2003)

Domestic Violence…
Greater than 90% of all injuries secondary to domestic violence occur to the head, neck or face region.
(Monahan & O’Leary 1999)

SPECIAL CASES
• Shaken baby syndrome

American Academy of Pediatrics-Committee on Child Abuse and Neglect Pediatrics 2001
“ …95% of serious intercranial injuries and 64% of all head injuries in infants younger than 1 year were
attributable to child abuse”
Pediatrics, 2001

Shaken Baby Syndrome

Shaken Baby Syndrome
• Rotational, acceleration, deceleration forces• There may or may not be impact trauma• Brain rotates inside the skull• Bridging veins in the brain may be stretched or
torn• Subdural hematoma may develop

Shaken Baby Syndrome
Kirschner & Wilson’s “dirty dozen”• 1. Child fell from a low height • 2. Child fell and struck head on floor or
furniture, or hard object fell on child• 3. Child unexpectedly found dead (age and/or
circumstances not appropriate for SIDS)• 4. Child choked while eating and was
therefore shaken or struck on back

Shaken Baby Syndrome
Kirschner & Wilson’s “dirty dozen”• 5. Child suddenly turned blue or stopped
breathing, and was then shaken• 6.Sudden seizure activity• 7. Aggressive or inexperienced resuscitation• 8. Alleged traumatic event one day or morebefore death

Shaken Baby Syndrome
Kirschner & Wilson’s “dirty dozen”• 9. Caretaker tripped or slipped while carrying
child• 10. Injury inflicted by sibling• 11. Child left in dangerous situation (e.g.
bathtub) for just a few moments• 12. Child fell down stairs

Shaken Baby Syndrome
Symptoms• Apnea • Listlessness• Lethargy• Poor feeding• Irritability• Vomiting• Seizures

SPECIAL CASES
• Combat trauma

Combat Trauma
• TBI as “signature wound” of Iraqi conflict• USA Today 9/07

Combat Trauma
• Iraq characterized by different kind of weaponry: explosive munitions.
• 15% of soldiers returning from Iraq may have sustained at least mild TBI (Hoge et al 2008)
• 36% may have been exposed to blasts (Maguen et al 2012)

Combat Trauma
• Comorbid PTSD • Headache• Sensory impairment• Alcohol use

SPECIAL CASES
• Alcohol abuse/dependency

Alcohol Abuse
• May increase morbidity of MVA-related TBI (Cunningham et al 2002)
• Although low amounts may be protective• Chronic alcohol abuse associated with falls,
assaults, multiple head injuries• Overlay of alcohol-related impairment


SPECIAL CASES
• Mild TBI

TBI Severity: Mild TBI (mTBI)
• Concussion signs and symptoms include ANY changes in behavior such as:– Cognitive impairments – Physical symptoms (e.g., headaches, blurry vision,
diplopia, dizziness)– Emotional symptoms (e.g., irritability, volatility)– Sleep difficulties – Not “feeling like themselves.”

TBI Severity: Mild TBI (mTBI)
• Persistent symptoms following the concussion is often referred to as Post-Concussive Syndrome.
• Cumulative effect

TBI Severity: Mild TBI (mTBI)
• Chronic traumatic encephalopathy

Psychotherapy with the persistent post-concussive client
• Perfectionistic tendencies• Somatic focus• Poignancy• Secondary gain• “old me / new me”• Check to see whether you are working at
cross-purposes

The “Big 5” (plus 1)
• The “Big 5”– Daily planner– Daily organization time– Movement– Nutrition– Connection– Sleep

Let’s stay in touch!
Join my e-newsletter list:
Fill out a card today and drop it in the box.
Text to join: text DNSEMINARS to 22828
Sign up on my web site or Facebook page
Visit us on the web: www.DrNowell.com
davidnowell David Nowell Seminars