Targeted Therapy for Melanoma - Dr. Michael Davies
24
Melanoma: From Prevention to Cure Houston, Texas January 31, 2015 Targeted Therapy for Melanoma: A Personalized Approach Michael A. Davies, M.D., Ph.D. Associate Professor, Melanoma Medical Oncology, & Systems Biology, The University of Texas MD Anderson Cancer Center CCR, 2012 Day 1 Day 15 Flaherty NEJM, 2010
-
Upload
the-melanoma-research-foundation -
Category
Education
-
view
1.097 -
download
1
Transcript of Targeted Therapy for Melanoma - Dr. Michael Davies

Melanoma: From Prevention to Cure
Houston, Texas
January 31, 2015
Targeted Therapy for Melanoma:A Personalized Approach
Michael A. Davies, M.D., Ph.D.Associate Professor, Melanoma Medical Oncology, & Systems Biology, The University of Texas MD Anderson Cancer Center
CCR, 2012
Day 1 Day 15
Flaherty NEJM, 2010

Disclosure Information
I have the following financial relationships to disclose:
Consultant for: GSK, Roche/Genentech, Novartis, Sanofi-Aventis
Grant/Research support from: GSK, Roche/Genentech, Astrazeneca, Merck, Myriad,
Oncothyreon, Sanofi-Aventis
I will discuss off-label or investigational use of:Imatinib, TAK-733

New Agents for Stage IV Melanoma
US Approval
Targeted TherapyImmunotherapy
Pre-1998 Approvals w/o (+) randomized trials1998-2011 No approvals
2011-2014 7 new regimens approved
1975 DTIC
1998 HD-IL2
1998-
20112011
Ipilimumab
Vemurafenib
2012 2013
Dabrafenib
Trametinib
2014
Dabrafenib +Trametinib
PembrolizumabNivolumab
Chemotherapy

Targeted Therapy: A Personalized Approach
• What is targeted therapy?
• Why do we use targeted therapy for melanoma?
• What have we learned & what are we working on

A Brief History of Chemotherapy
• WW I: Nitrogen mustards gas
• → 1946 1st successful systemic treatment of cancer with chemotherapy
• 1950s-1980s most standard chemotherapies
• 1977 First report of an oncogene
• 1980s-2000s Oncogenes in most cancers
Dr. Sidney FarberAnd Patient
‘Targeted Therapy’:Treat cancer by targeting the genes activated in cancer cells

Targeted Therapy: Why Melanoma?
• Overall melanomas have more mutations than any other type of cancer
• Targetable mutations can be identified in ~70% of patients with cutaneous melanoma

PET
CT
BRAFi
6 Weeks
The Promise of Targeted Therapy: BRAF

Effective for Brain Metastases
Long et al, Lancet Oncology, 2013
BRAFi
32 Weeks

Clinical Activity of BRAF Inhibitors
Tumor Grew
Tumor Shrank
• 50% of patient achieve a “clinical response”
• 90% achieve disease control, usually very quickly (<1 month)
• KEY: Only work in patients that have a BRAFV600 mutation
• If don’t have a mutation they will make the tumors grow faster
FDA-Approved BRAF Inhibitors• Vemurafenib, 2011• Dabrafenib, 2013
Champman et al, NEJM, 2011
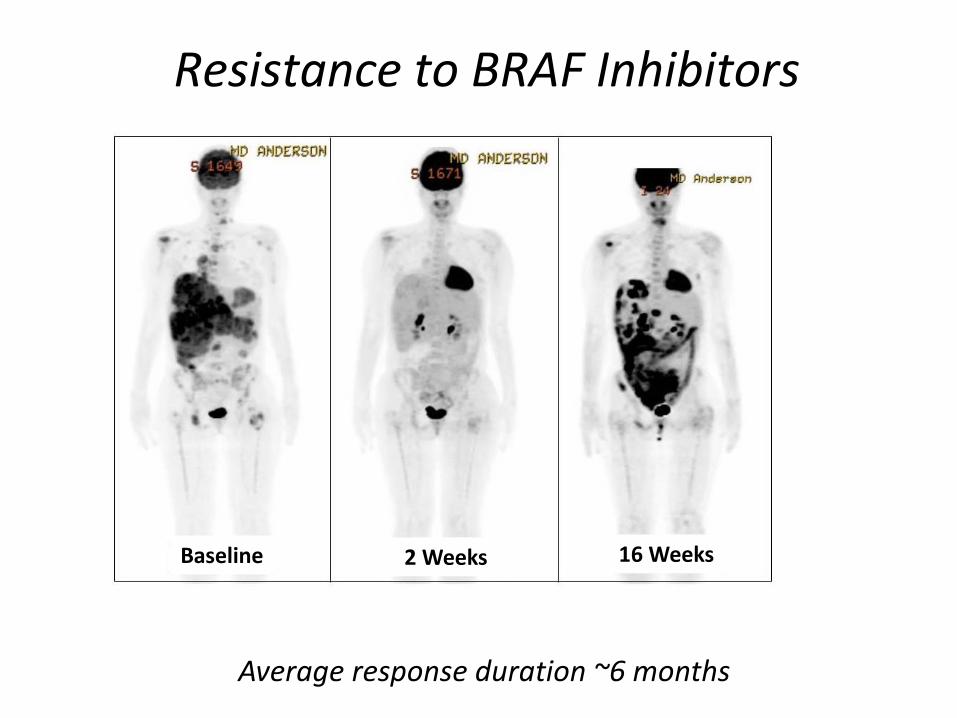
Baseline 2 Weeks 16 Weeks
Resistance to BRAF Inhibitors
Average response duration ~6 months

BRAFi: Why Does Resistance Happen
MAPK & PI3KPathway
Re-Activated
MAPK Pathway
Re-Activated
UnknownMechanism
of Resistance
Shi,… Lo, Cancer Discovery, 2013
All patients still have the BRAFV600 mutation at the time of resistance
→ Rationale to combine BRAF with other MAPK inhibitors

Combinations to Overcome Resistance:
Targeted Therapy + Targeted Therapy
Testing of other combinations underway
-100
-80
-60
-40
-20
0
20
40
60
80
100
Tumor Shrank
BRAFi + MEKi
• ~100% disease control rate• Average response duration 11 months (~2X BRAFi)• Less skin toxicity than BRAFi alone
Flaherty et al, NEJM, 2012

A New Challenge: Heterogeneity
Shi,… Lo, Cancer Discovery, 2013
Tumor #
Different tumor with different resistance mechanisms
in the same patient

A New Hypothesis:Combining BRAF Inhibitors & Immunotherapy
BRAF Inhibitors
• High rates of responses
• Responses generally < 1 yr
Immunotherapies
• Lower rates of responses
• Responses can → cures
Can BRAF Inhibitors + Immunotherapy → High rate of cures?

Combinations to Overcome Resistance:Targeted Therapy + Immune Therapy
Liu, …Hwu, CCR, 2013 Frederick,…Wargo, CCR, 2013
In Mice In Patients
Challenges:• More side effects• Which agents to combine• How to combine them

Targeted Therapy:
Beyond BRAFV600
‘Wild-type’ BRAF>50% cutaneous MM>80% non-cutaneous
BRAFV600
Mutant
BRAFV600
Wild-Type

Different Types of Melanomas Have Different Mutations
Cutaneousw/o Chronic Sun Damage (C.S.D)
Acral MelanomaMucosal Melanoma Uveal
20-30% mutations in c-KIT
45% BRAF Mutations20% NRAS Mutations
Acral: 20% BRAF 10% NRASMucosal: 3% BRAF 5% NRAS
Virtually No BRAF/NRAS
~80% mutations in GNAQ/GNA11

Targeted Therapy for KIT-Mutant Melanoma
Hodi et al, JCO, 2008
Imatinib
Imatinib• 1% chance of response in unselected melanoma patients• 30-50% chance of response with recurrent KIT mutations

Melanoma TCGA: Initial Results
100 150 215
NRAS mut (28%)
BRAF mut (52%)
NF1 mut (14%)
MITF amp (4%)
BRAF amp (12%)
MDM2 amp(12%)
NOTCH2 amp (5%)
KIT amp (3%)
KIT mut (3%)
PDGFRα amp (3%)
PDGFRα mut (10%)
CCND1 amp (4%)
TERT amp (5%)
PPP6C mut (7%)
PTEN del (12%)
PTEN mut (8%)
CDKN2A del(40%)
CDKN2A mut (13%)
TP53 mut (7%)
50
“Wild-Type”BRAFV600NRAS
Cancer Genome
Atlas Research
Network, 2012

Dahlman, et al Cancer Discovery, 2012
MEKi for Non-V600 BRAF Mutations
Cutaneous & Unknown Primary melanomas WITHOUT
BRAFV600 or NRAS mutations
MDACC, n=113
Siroy, et al, J Inv Derm, 2014
MelanomaBRAF L597V
TAK-733(MEKi)

Targeted Therapy for Melanoma:
What Have We Learned
& What Are We Working On
Targeted Therapy:What We Have Learned
• Virtually all patients with cutaneous melanomas have >100 mutations
• BRAF-Mutant Melanoma (~ 50%)
– Inhibiting driver oncogenes can → benefit
– Right patient, right drug, right dose
– Combinations can be even better!
• Have to identify ways to understand, prevent & overcome resistance

Targeted Therapy:What We Are Working On
• Identify mutations that help us to manage patients across the full continuum of melanoma
• BRAF-Mutant Melanoma
– Benefit of BRAF and MEK inhibitors in earlier stages
– New combinations
• Testing new strategies for other mutations

Thank you for your attentionand to our patients
Michael Davies, M.D., Ph.D.
Departments of Melanoma Medical Oncology and Systems BiologyUniversity of Texas M. D. Anderson Cancer Center
[email protected] SupportNIH/NCICancer Prevention Research Institute of Texas (CPRIT)Melanoma Research AllianceMelanoma Research FoundationAmerican Society for Clinical OncologyMDACC SPORE in MelanomaMDACC Physician-Scientist ProgramDunn Foundation for Chemical Genomics
GlaxoSmithKline
AstraZeneca
Genentech
Merck
Myriad
Oncothyreon
Sanofi-AventisDr. John E. Davies, 1921 - 1999