Tamás Fenyvesi - Semmelweis Egyetemsemmelweis.hu/belgyogyaszat3/files/2010/12/Acute-abdomen.pdf ·...
69
Acute abdomen Tamás Fenyvesi 1 Tamás Fenyvesi November, 2016
Transcript of Tamás Fenyvesi - Semmelweis Egyetemsemmelweis.hu/belgyogyaszat3/files/2010/12/Acute-abdomen.pdf ·...

Acute abdomen
Tamás Fenyvesi
1
Tamás Fenyvesi November, 2016

2
Acute abdomen is anabdominalemergency no temporizing is ever justifiable.temporizing is ever justifiable.
Patients present more likely in the evening hours
Never wait with your decision for the next
3
Never wait with your decision for the next morning

Characteristics of acute abdomen
�has been present for less than 24 hours�Sudden and unexpected onset of
abdominal painabdominal pain�associated symptoms:
nausea, vomiting, abdominal dystension,diarrhea, constipations, anorexia
The pain may arise from intra-and extra-
4
�The pain may arise from intra-and extra-abdominal structures
acute abdomen not invariable operation

Neural innervation of the gastrointestinal tract
5

History
�allow the patient to give his/her entire allow the patient to give his/her entire current history before asking specific questions�the character and onset of pain are essential
–colicky pain: obstructive processes
6
–colicky pain: obstructive processes–sustained pain :infectious processes
�Referred pain patterns may give a clue

7
Abdominal pain onset patterns
�I. sudden(seconds)I. sudden(seconds)–A. perforation or rupture of a viscus:peptic ulcer, abdominal aortic aneurysm, esophagus, ectopic pregnancy,PTX
8
–B. infarction:gut, heart, lung
P.D. White etc

Abdominal pain onset patterns
II. rapid(minutes)�II. rapid(minutes)–A. colic syndromes: biliary, ureteral, small
bowel obstruction(high)–B. inflammatory processes:
pancreatitis, diverticulitis,
9
pancreatitis, diverticulitis,appendicitis, penetrating ulcer, cholecystitis
–C. ischemic processes: strangulation, torsion

Abdominal pain onset patterns
�III. Gradual(hours)�A. inflammatory :appendicitis, cholec.,
pancreat., divertic., salpingitis, ¤pancreat., divertic., salpingitis, ¤prostatitis, inflamm.bowel dis., intra-abdominal abscess
�B. obstruction:distal small bowel or colon,ectopic pregnancy,urinary retention,
10
colon,ectopic pregnancy,urinary retention,incarcerated hernia
�C. neoplastic:perforating or penetratingtumors (colon, stomach, small intestine)
Physical examination
� Observation of the patients body habitus and facial expressionhabitus and facial expression
–peritonitis :unwillingness to change posture, hip flexion with the knees drawn up, shallow breathing
11
drawn up, shallow breathing–colicky pain: intense movements to alleviate

Physical examination
�Inspection of the abdomen:localized or
generalized dystension, visible peristaltsis, hernial bulges, erythema
�Auscultation of bowel sounds, if nosounds are heard : paralytic ileus
12
sounds are heard : paralytic ileus
� Percussion absence of hepatic dullness (!!) : perforation
13

Physical examination�Palpation : superficial, gentle of all quadrants, first at the least painful areas,
after this deeperafter this deeper�classic rebound tenderness (deep
palpation followed by rapid release) is notspecific
�have the patient laugh, cough, distend ormaximally reduce his/her abdominal girth
14
maximally reduce his/her abdominal girth�A very old and forgotten means to palpate
the abdomen in a bath tub (in only thepatient !!)

•A rectal digital examination is obligatory
15

16
Characteristicscars,Now often laparoscopy

Laboratory evaluation�Complete blood count:WBC differential,
CRP, sed.rate�urinalysis:serum amylase (urine)�serum amylase (urine)
�beta human chorionic gonadotropin infemales
�serum electrolytes,BUN,creatinine andglucose
17
glucose�liver function test in upper abdominal painuse only relevant laboratory
investigationsthe results of which effect therapy !!

X-ray evaluation
�upright PA and lateral film of the chestupright PA and lateral film of the chest�supine and erect plain film of theabdomen
–the upright film should include thediaphragm
� to detect free intraperitoneal air
18
� to detect free intraperitoneal air� only horizontal beam films detect fluid
levels within the bowel

X-ray evaluation
�contrast study may be required (dangers!)abdominal ultrasound mandatory�abdominal ultrasound mandatory
in some instances endoscopic�CT , MRI, nuclear (PET scan if
cost/benefit !! O K)angiography
19
�angiography� may add to diagnostic accuracy
20

Causes of acute abdomen�Appendicitis �Acute cholecystitisAcute pancreatitis�Acute pancreatitis
�Diverticulitis�Perforated peptic ulcer�Bowel obstructionMesenteric ischemia
21
�Mesenteric ischemia�Ruptured abdominal aortic aneurysm�Gynecologic causes

Appendicitis
History: tipically midabdomonal pain ¤History: tipically midabdomonal pain ¤onset of nausea and vomitingrelocation of pain to the right lower quadrantelevation of temperature
22
elevation of temperature

23ZETA (Sir Zachary Cope)

.Appendicitis : bacterial infection with contributory factors:intraluminal obstruction -fecalith lymphoid obstruction -fecalith lymphoid hyperplasia, parasites, carcinoid tu.
–typical symptoms:midabdominal pain moving to the right lower quadrant- elicited by coughing
24
quadrant- elicited by coughing laughing or bumping, nausea and vomiting, anorexia,fever.
.Appendicitis :
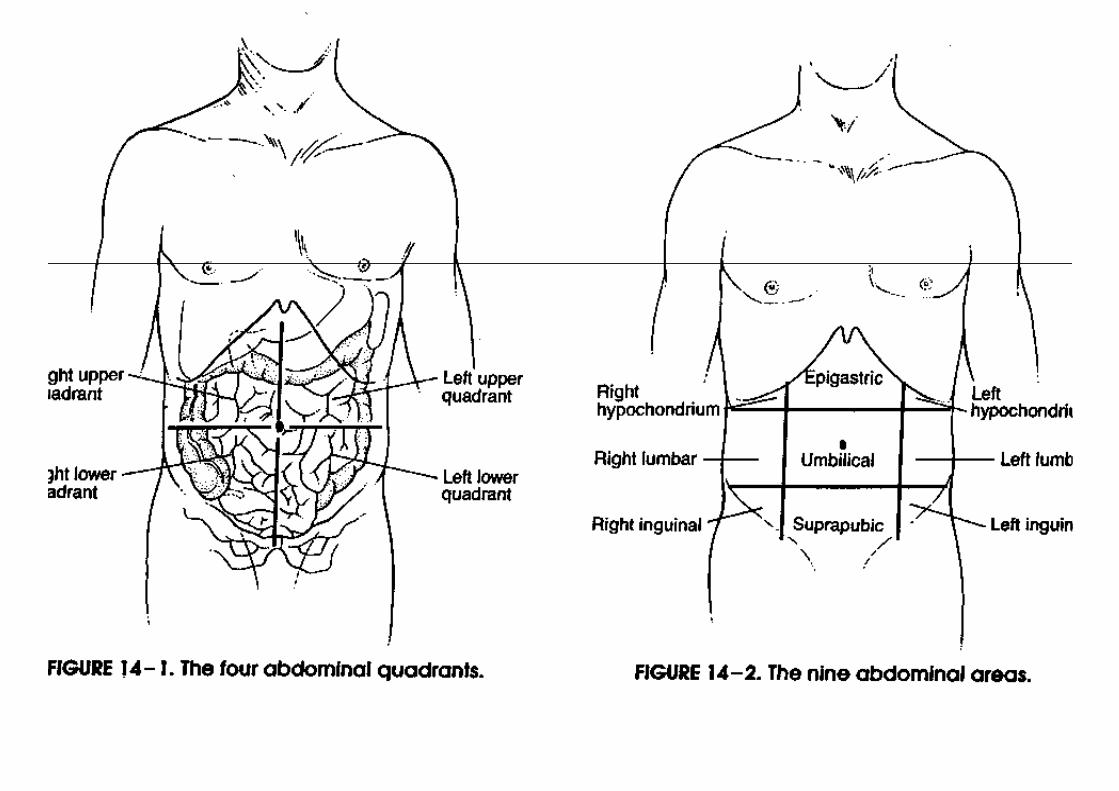
physical : tenderness and guarding over the right lower quadrant (McBurneypoint-1/3 distance superior iliac point-1/3 distance superior iliac spine-umbilicus)
– psoas sign, rebound tendernesslaboratory:WBC,CRP, urinalysis
25

Differntial dg of appendicitis
Localization of the appendixascending:
cholec,perf pyonephrduodenal ulc pyelitisduodenal ulc pyelitisperinephr absc nephrolithhydronephr omental torsion
Iliacal penetrating duod ulc Meckel’s diverticulumCrohn diseas!! Psoas absc
26
Crohn diseas!! Psoas abscIleocecal cc. hip !!Tbc muscle rupture uretolith typhlitis

�Appendicitis 2 :�abdominal X-ray rarely useful,
ultrasound(periappendicular fluid,edema,abscess,visualization of fluid,edema,abscess,visualization of the lumen) increasing significance
Peak incidence 15-24 years�choice of treatment ,surgery:10-20%
negative appendectomy
27
�Keep in mind the danger of perforation in the elderly

Acute cholecystitis
obstruction of the bile duct by stone1. bacterial in 50-85% of cases2. Chemical agents : lysolecithin,
other tissue factors3. Inflammation from mechanical
28
3. Inflammation from mechanicalstrech

Acalculous cholecystitis with dilated gallbladder and thickened gallbladder wall
29

Diagnosis of stone disease by ultrasound
shadow
30

Cholesterol stones gall bladder
31

Appearance of gallstones
32
Characteristic symptoms:colic, localized to the right upper
quadrantRUQ tendernessRUQ tendernesspatient suddenly stops inspiration
(Murphy ‘sign) irradiates to the right shoulder or
scapulavomiting , exsiccosis
33
vomiting , exsiccosisfever usually moderate, but also
chills

The„convergence projection” :in thelateral spinothalamictract the fiberin thelateral spinothalamictract the fiber
number is less than the sensory fibers
somatic> visceralis
the brain “learns” that on the given tract
34
the brain “learns” that on the given tract
the somatic signals are transmitted

35

Acute pancreatitis
Increasing incidence: 36 to 44/100 000 adultsin California (1994-2001)
200 000 hospital admission/year in the USA200 000 hospital admission/year in the USA
Bile reflux is the trigger (1856 Claude Bernard)
2 enzymes are released from acinar cells
36
2 enzymes are released from acinar cells amylase and lipase

Causes
gallstones 38%alcohol abuse 36%pancreas divisum ( congenital abnormality ofpancreas divisum ( congenital abnormality of
the pancreatic duct)intraductal papillary tumorsERCP (increase of serum amylase
after the procedure )
37
after the procedure )Serum triglyceride >11mmol/Lsome drugsinfections

Diagnosis Symptoms of acute abdomen•Constant acute pain in the epigastric area or the
right upper quadrant•Nausea , vomiting•Nausea , vomiting•Tenderness in the upper abdomen•Cullen’s sign:
38

39

20% severe (4% die)
Early developmentEarly developmentsequential organ failure
increased capillary permeabilitydecreased intravascular volume hypovolemia renal dysfunction
40
renal dysfunctionpulmonary complication
Pancreatic necrosis a very severe complication

Severity is assessed by CT and contrast enhanced CT
41

Treatment
Correct fluid lossesmonitor respiratory, cardiovascular and monitor respiratory, cardiovascular and
renal function. Multidisciplinary
Stop parenteral nutrition : a rule!??Infection
antibiotic prophylaxis is debated in
42
antibiotic prophylaxis is debated in proven infection: imipenem

43Lancet 2008;371:143¤

44BMJ 2004;328:1407

45

Causes of acute abdomen
Diverticulitis� prevalence 5% , increases with age� the sigmoid colon is most commonly involved� the sigmoid colon is most commonly involved� in 50% the only segment, right sided 0,1-2,5%� signs and symptoms protean� left lower quadrant pain, low grade fever,� leucocytosis,nausea, vomiting, distension� Sigmoidoscopy not indicated(perforation!!),nor
46
� Sigmoidoscopy not indicated(perforation!!),nor� barium enema, not in acute phase ,only later
"elective "� X-ray or CT scanning

Causes of acute abdomen
Mesenteric ischemia: 0,4% of abdominal surgeryMesenteric ischemia: 0,4% of abdominal surgery�vascular disorders-usually catastrophic illness
–embolic occlusion or thrombosis:intestinal infarction--gangrenous bowel–mortality 40-70%
�abdominal pain,vomiting diarrhea, melena , distension,tendernessbowel sounds from hypoactivity to absent
47
�bowel sounds from hypoactivity to absent�Bloody peritoneal transsudate,leucocytosis 20 t hemoconcentration�history of abdominal angina,atrial fibrillation�rapid visceral angiography

Causes of acute abdomen
Perforated peptic ulcer 10% of hospital Perforated peptic ulcer 10% of hospital admission for ulcer 7-10 pts/100000/year�undiagnosed pts die,duodenal 6-8x more often¤�sudden onset epigastric pain"hit with a knife"
–spreading to the entire abdomen:rigidity, diffuse tenderness-hypovolemia, shock
�upright or left lateral decubitus X-ray 55-85%
48
�upright or left lateral decubitus X-ray 55-85% pneumoperitoneum:on physical disappearance of hepatic dullness, X-ray�may heal spontaneously,dudenal anterior wall ¤�surgery,broad spect.antibiot,fluid

49
Succussion splash

Colonic perforation
50

Causes of acute abdomen
Ruptured abdominal aortic aneurysmRuptured abdominal aortic aneurysm
�pain,sudden onset ,midabdominal,paravertebral�pulsatile abdominal mass,hypotension "triad"�risk: atheroscler.diameter and rate of increase
–5,5 cm threshold for elective surgery–Abdominal ultrasound
51
–Abdominal ultrasound�X-ray (contrast iv.deviation of the ureters,aortic � wall,CT,angio time consuming
MR�emergency operation-high mortality
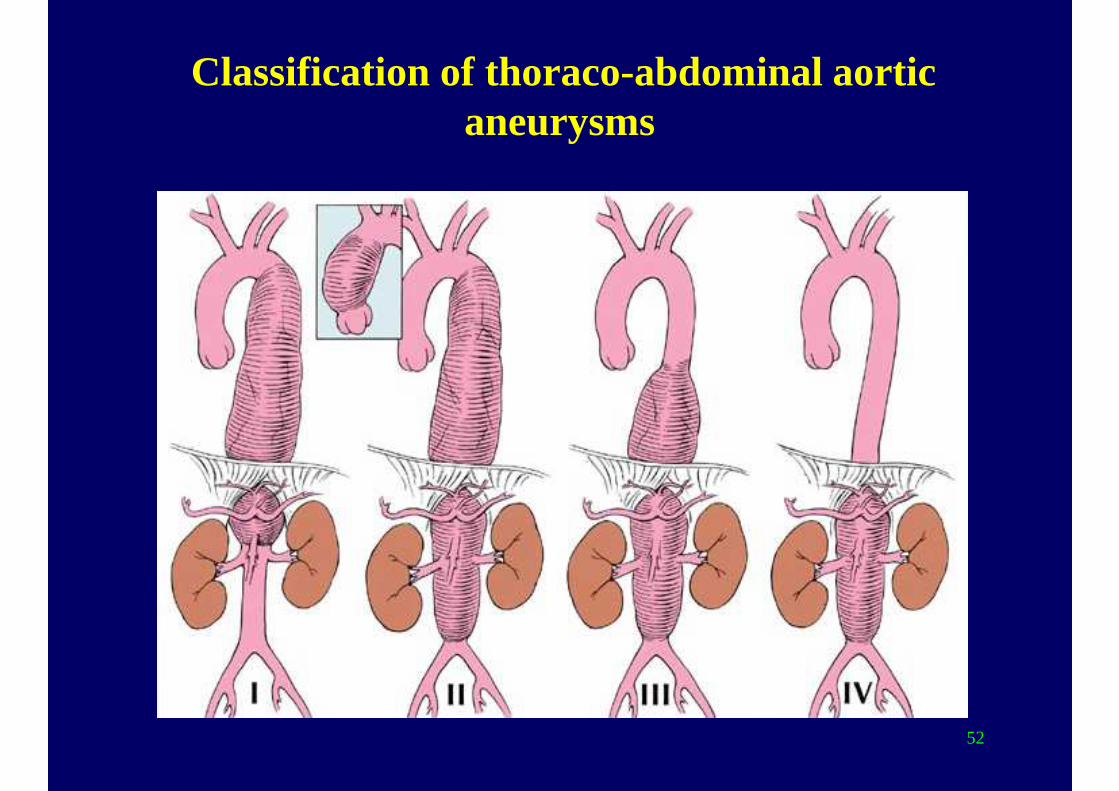
Classification of thoraco-abdominal aortic aneurysms
52

Atherosclerotic abdominal aortic aneurysm after fatal rupture
53

Bowel obstruction: ileus 20% of all acute
Causes of acute abdomen
surgical hospital admissions
causes: mechanical�extrinsic: adhesions,hernias,volvulus,masses
�intraluminal objects: fecal impaction,gallstone,
54
gastric bezoars,foreign bodies
�intrinsic lesions:neoplasms,inflammation,
intussusception,hematoma

55

Causes of acute abdomen
�Ileus 2 : adynamic(paralytic)�reflex inhibition:laparotomy,trauma�reflex inhibition:laparotomy,trauma�inflammation:peritonitis,toxic megacolon,�acute irradiation�infectious process:appendicitis,cholecystitis�ischemic processes:arterial insuff.�retroperitoneal :ureter,kidney
56
�retroperitoneal :ureter,kidney�drug induced:opiates,anticholinergic drugs�metabolic:porphyria ,ketoacidosisX-ray diagnosis: air-fluid levels -small or large bowel
Causes of acute abdomen
�Gynecoligical:in reproductive age�Gynecoligical:in reproductive age� pelvic inflammatory, ectopic pregnancy, ovarian
cyst hemorrhage,adnexal or ovarian torsion�pain,delayed menstrual period,diffuse pelvic�tenderness, acute rupture of blood filled
fallopian tube�SYNCOPE,pelvic examination,pregnancy test
57
�SYNCOPE,pelvic examination,pregnancy test

„A good eater must be a good man,
for a good eater must have good
digestion, and good digestion
depends upon good conscience”
Benjamin Disraeli
58
Benjamin Disraeli1804-1881
Prime minister of Great-Britain: 1868, 1874-80

59

Some reminder of anatomy and Some reminder of anatomy and pathophysiology
60

61

.
The foregut,midgut and hindgut have andThe foregut,midgut and hindgut have andretain their own innervation and bloodsupply
�forgut : oropharynx to the duodenum (bile duct)
�midgut: distal duodenum,jejunum,
62
�midgut: distal duodenum,jejunum,ileum,appendix, ascending colon,proximal 2/3 transverse colon

.
hindgut: distal1/3 of transverse colon to�hindgut: distal1/3 of transverse colon toanus
�peritoneum: visceral autonomicinnervation dull,crampy or aching pain
:parietal somatic innervation
63
:parietal somatic innervationsharp, severe and persistent pain

Acute abdomen
�Abdominal pain :visceral, somatic or referred�abdominal wall: anterior and lateral spinal T7-L1�abdominal wall: anterior and lateral spinal T7-L1�Two types of nociceptors
–A-delta fibers rapid : sharp well localized–C-fibers slow:dull, poorly localized
� :posterior L2-L5
64
�pain fibers enter spinal cord ipsilaterally� visceral pain arises in the midline� fibers enter spinal cord bilaterally

“ To study the phenomenon of disease
without books is to sail an uncharted without books is to sail an uncharted
sea,
while to study books without patients
is not to go sea at all”
65
is not to go sea at all”
William Osler

A University should be
a place of light,
of liberty, and of learning.Benjamin DISRAELI, 1873
66
Benjamin DISRAELI, 1873

67

68
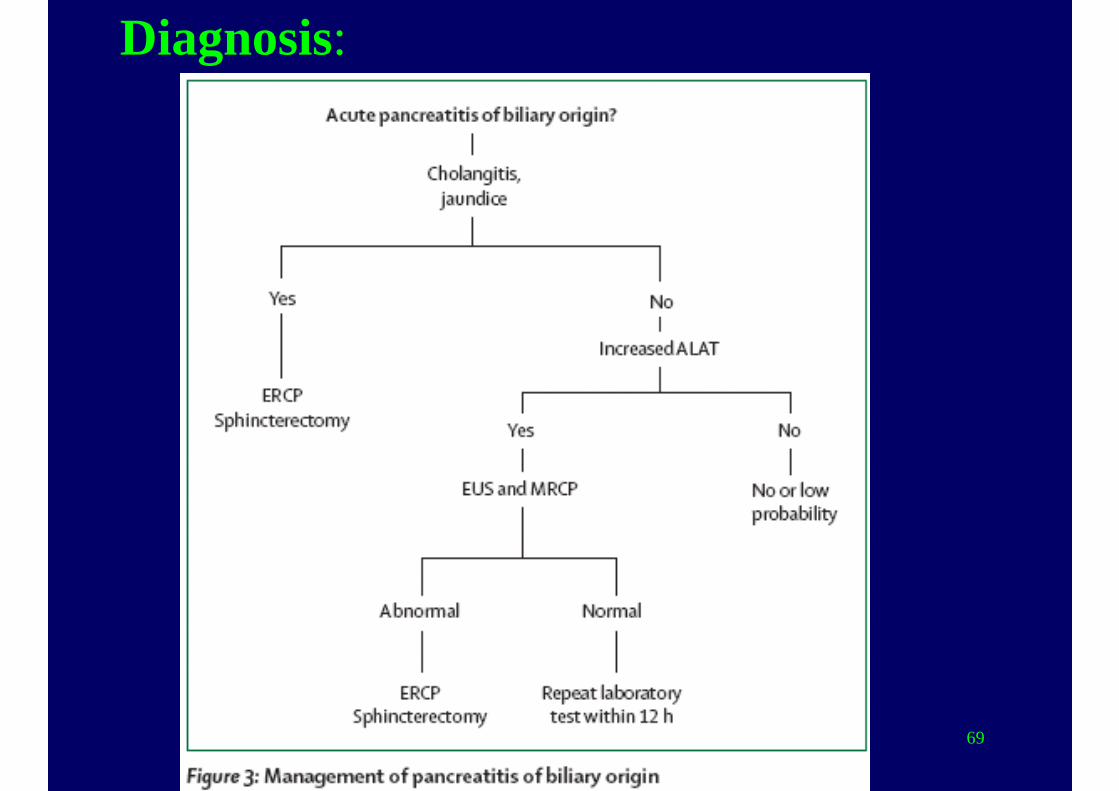
Diagnosis:
69