
Table of Contents - RDL | RDL Reference Laboratory...2 Overview RDL Reference Laboratory (RDL)...
90
Transcript of Table of Contents - RDL | RDL Reference Laboratory...2 Overview RDL Reference Laboratory (RDL)...


1
Table of Contents
Billing Information
Client Billing .......................................... 14
Patient Billing ........................................ 14
Medi-Cal/Medicaid ................................ 14
Medicare & Medicare/Medicaid ............. 14
Insurance Carriers ................................. 15
HMO Billing ........................................... 15
CPT Coding .......................................... 15
Payments .............................................. 15
List of Abbreviations ................................. 16
Alphabetical Listing of Tests
Test Combinations ...........................17-30
Individual Tests .................................31-70
Index of Tests by Test Name
Test Combinations ...........................73-75
Individual Tests ................................76-80
Index of Tests by Test Number
Test Combinations ...........................81-83
Individual Tests ................................84-88
Overview .................................................... 2
Mission Statement ...................................... 2
Support Services
Staff Services .......................................... 3
Technical Services ................................... 3
Client Services ........................................ 3
Patient Services ...................................... 3
Licenses & Certifications ............................. 4
Professional Staff ........................................ 4
Compliance & HIPAA .................................. 5
Ongoing Monitors of Conformance &
Quality Improvement ............................... 5
General Information
Turnaround Time ..................................... 6
Mailing Information & Courier Service ...... 6
ANA Methodology & Reflexive Testing ........ 7
Special Services & Testing Guidelines
Specimen Storage & Add-On Tests ......... 8
Cancellation of Tests ............................... 8
Insufficient Volume .................................. 8
Repeat Testing ........................................ 8
Sendout Tests ......................................... 9
Methodology Changes ............................ 9
Specimen Collection, Transport & Handling
Specimen Collection ............................. 10
Specimen Transport .............................. 10
Specimen Handling .......................... 10,11
Specimen Rejection Criteria .................. 11
Suspected Hepatitis & AIDS .................. 11
Shipping Supplies & Requisition Forms .... 12
Legibility & Current Information ................. 12
Electronic Information Services ................. 13

2
Overview
RDL Reference Laboratory (RDL) provides laboratory services to hospitals, reference laboratories and physicians in the following sub-specialties: Rheumatology, Immunology, Gastroenterology, Hepatology, Infectious Diseases, OB/GYN/Infertility, Nephrology, Neurology, Cardiology and Hematology. RDL also has collaborated with several biotechnology companies interested in developing high quality assays, and has performed testing for a number of research studies.
From its inception, RDL has been dedicated to providing excellence, consistency, innovation, and unique service to our clients in the most cost-effective manner possible.
RDL Reference Laboratory was founded in 1977 by two board certified, UCLA trained Rheumatologists. After three years of rheumatology practice following their fellowships, they found inconsistent performance by local, as well as national commercial laboratories in ANA testing, and an inadequate availability of autoimmune disease testing. These conditions made it apparent that, if they wanted quality testing that could be trusted, they would have to form their own laboratory.
Initially, the menu contained only autoimmune tests, but over the years the menu has expanded. Physicians in most sub-specialties use our services and we have many university teaching centers, hospitals, laboratories, researchers and biomedical companies forwarding specimens daily.
Mission Statement
RDL Reference Laboratory is dedicated to the principles of excellence and consistency in esoteric laboratory testing. We are committed to aiding the clinician in early diagnosis and continued disease management through the design of profiles and panels that provide the ordering physician an array of specialized autoimmune tests. These tests assist in resolving the various clinical problems faced in practice in the most cost-effective manner possible. RDL uses cutting edge technology performed by experienced, licensed professionals.
RDL staff treats our clients, their staff and their patients with the respect they all deserve. RDL client services representatives are geared to do “whatever it takes” to satisfy our clients.

3
Support Services
Staff Services
RDL Reference Laboratory (RDL) provides testing services Monday through Friday, 7 A.M. to 6 P.M. Staff members are available to answer technical questions Monday through Friday. Questions can be addressed to individuals from our client services and billing departments Monday through Friday. All staff members can be reached at (800) 338-1918.
Technical Services
RDL’s technical staff provides support to our clients for all their technical inquiries. Also, RDL’s Laboratory Directors and medical consultants, all Rheumatologists, have broad expertise in the field of autoimmunity. Our Chief Technologist, Lab Manager and Laboratory Directors are available for consultations with clients regarding appropriate testing and for discussion concerning the accurate interpretation of results.
Client Services
RDL’s Client Services representatives provide information regarding test status and results, facilitate special requests, open new accounts and familiarize clients with our procedures, process add-ons and cancellations, manage concerns and dispatch supplies.
Patient Services
Our Patient Services representatives are trained to assist our patients in understanding the billing process and resolving disputes with their insurance companies. For more specific information regarding our billing practices, please see the section entitled “Billing Information”.
4
Licenses and Certifications
CLIA Number 05D0550276
College of American Pathologists 22584-01
HEW CLIA Exempt Number 04-1184
Medicare Number Available Upon Request
Medi-Cal Number Available Upon Request
State of California License CLF3096
State of Florida License 800010357
State of Maryland License 788
State of New York License 4393
State of Pennsylvania License 029006A
State of Rhode Island License LCO00386
Tax ID Number 953053422
National Provider ID # (NPI) 1013900778
Professional StaffLaboratory Directors
Robert I. Morris, M.D. (FACP, FACR) Dmitry Karayev, M.D. (FACP, FACR)
Medical Consultant
Allan L. Metzger, M.D. (FACP, FACR)
Laboratory Manager & Director of Research & Development, Immunodiagnostics Division
Guoqiu Shen, M.D.
Chief Laboratory Technologist
Paula C. Correia, MT (ASCP, CLS)

5
Compliance & HIPAA
RDL complies with all regulatory agencies by which we are certified. They include the College of American Pathologists (CAP), CLIA, Medicare, Medi-Cal, Medicaid, the state of California and the state of New York. Please see the section titled “Licenses & Certifications” for a complete listing.
We anticipate that our clients have complied with regulatory requirements such as CPT coding, ICD-9-CM and/or ICD-10 coding, and patient confidentiality.
RDL has an active quality improvement mechanism in place that complies with HIPAA and HITECH. RDL observes the regulations governing laboratories for patient information confidentiality as stated in the HIPAA regulations and by the State of California. Each patient is entitled to remain completely anonymous throughout the testing and reporting process. Access to confidential information is restricted to authorized personnel and such information may only be provided to persons authorized to receive such information. Also, RDL is very aware of HIPAA concerns regarding standards for electronic transactions and security of those transactions, and has implemented policies and procedures to ensure compliance with HIPAA standards.
Ongoing Monitors of Conformance & Quality Improvement
RDL follows written policies and procedures under our Quality Assurance and Quality Improvement systems to monitor and assess conformance with requirements in these areas:
Human Resources
Facility Design and Resource
Standard Operating Procedures
Pre-examination
Examination
Post-examination
Quality Assessment & Improvement
RDL’s Quality Improvement Plan (QI) is a program for the monitoring and evaluation of the quality and appropriateness of services, for resolving identified problems and for ensuring implementation of the program throughout all lab sections by the directors.
The QI Plan includes procedures and protocols for the organization of personnel, instruments, methodologies and reagents. The components of the QI Plan identify sources of pre-analytic, analytic and post-analytic variations that have an impact on the requirements for high quality patient care. Our QI plan is concerned with outcomes, results, ends and information content.

6
General Information
Turnaround Time
RDL defines turnaround time as the number of days to result a test or panel from the day the specimen is received at RDL in Los Angeles to the day the results are provided to the client by fax, hard copy or electronically (weekend days not included). Turnaround times are specified for each test combination and individual test in alphabetical order following this preface.
Many tests are performed on a daily basis and have a one to two day turnaround time. Several of our more esoteric tests have a longer turnaround time because they are less frequently performed. Many of the tests performed require confirmation in duplicate (CID) if a result is very low, very high or inconclusive. CID testing will be performed on a timely basis but will, of course, increase the standard turnaround time.
A number of tests are identified as being reflexive in the alphabetical listings under the special instructions area. A quick perusal of the test listings reveals a number of reflexive panels and tests that work as algorithms to better manage patient care. Most reflexive panels are resulted within two to five days. All test results are faxed or electronically transmitted nationwide daily.
Mailing Information & Courier Service
Please refer to the schedule of tests to determine the mailing requirements for each individual test requested.
Unless otherwise indicated, serum is stable at room temperature for several days and can be sent by regular mail in a preprinted container supplied to you by RDL. However, it is strongly recommended that overnight express service be used at no charge to clients, guaranteeing next day delivery.
All mailing supplies are shipped to our clients. Please call Client Services at (800) 338-1918 for assistance.
In the greater Los Angeles area, free daily courier service is provided. Please call Client Services to arrange for a personalized pick-up schedule.

7
ANA Methodology & Reflexive Testing
Anti-Nuclear Ab by IFA
Since 1977, RDL has performed our Anti-Nuclear Ab (ANA) test exclusively by Indirect Immunofluorescence (IFA) which is the preferred methodology officially recommended by the American College of Rheumatology in 2008.
Reflexive ANA Profiles
RDL was the first laboratory in the country offering reflexive ANA profiling and has continued to enhance ANA profile testing by adding new tests after their clinical utility is well established in scientific literature.
If the ANA is positive, all the tests in the ordered profile will be performed. If the ANA is negative, only an Anti-Ro (SS-A) test will be performed to ensure that the ANA is not one of the small percentage of ANAs that are false negative. If the Anti-Ro is positive, all other tests in the profile will be performed.

8
Special Services & Testing Guidelines
Specimen Storage & Add-on Tests
All sera are stored at 4 degrees Centigrade for two months. This allows the physician to conveniently order additional tests. Please call Client Services to order subsequent testing for a recently submitted specimen. We will perform the test(s) in a prompt manner if there is a sufficient amount of available serum.
A phone request by a physician or other authorized person is followed up by a request for signature by RDL Client Services which should be attained within 48 hours of the request. If RDL does not receive the signature within that time period, a call is made to the physician requesting his signature, and another request is sent to him/her to immediately sign and return to RDL.
Cancellation of Tests
Cancellations received before tests are performed will be respected. Requests received after tests have been set up or are resulted will be reported and duly charged.
Insufficient Volume
Each test and each test combination has a specimen requirement. When a specimen is submitted with an insufficient volume for a single test, RDL contacts the client to request more sera. If none can be obtained, the test is deleted and not billed. If an insufficient volume is submitted for a panel or profile and the client cannot supply more sera, RDL performs as many tests as possible, as prioritized by the physician. The client or patient will be billed only for those tests resulted.
Repeat Testing
Any client concerns regarding specific results should be addressed to our Chief Technologist, Paula Correia, Lab Manager, Dr. Guoqiu Shen or Client Services. If necessary, RDL will repeat testing of the result in question at no additional charge.

9
Special Services & Testing Guidelines
Sendout Tests
RDL must comply with California regulations which specify that we charge our clients the exact amount we are charged by the reference laboratories that receive our sendouts. Whenever we are charged a handling fee, we include that charge in our fee to our clients.
Methodology Changes
As laboratory technology advances, RDL may adopt a new methodology for a given assay after extensive in-house validation. Whenever this occurs, RDL promptly informs our clients of these changes, principally due to revised reference ranges. For all tests that have methodology changes, a remark is added to the affected test result specifying the changes on the result form. Also, a “Laboratory Update” is dispatched to all our clients that includes not only methodology changes with new test numbers, but also any new or eliminated tests on our menu. Information regarding special specimen requirements and handling is also included.

10
Specimen Collection, Transport & Handling
Specimen Collection
In order to ensure the best possible specimen for the most accurate test results, please refer to the test combination or individual test listings for specimen requirements before blood collection. Specimen requirements and special instructions are clearly indicated; incorrectly collected specimens and inappropriate specimen volumes or handling can cause erroneous laboratory results and, therefore, will not be processed.
Most determinations are performed on serum. See the instructions under “Specimen Handling” for complete information on collection, labeling and submitting specimens. Please note that for tests requiring anti-coagulated blood, you must mix the tubes immediately after the blood is collected to prevent clotting.
Before drawing the specimen, ask the patient his/her name, birth date and address to ensure you have the correct individual for the requested tests.
Specimen Transport
RDL monitors that samples have been transported to the lab:
• Within a time frame appropriate to the nature of the requested examination and the lab discipline concerned
• Within a temperature range specified in the collection manual and with the designated preservatives to ensure the integrity of samples
• In a manner that ensures safety for the carrier, the general public and RDL and complies with national and local regulatory requirements
Specimen Handling
1. For all tests that require serum, continue to number 2. For all other types of specimens, see the individual test’s requirements and special instructions, and see #’s 3 - 6.
2. Draw one red top tube or SST tube. Let stand for 30 minutes and spin down and separate out the serum into the plastic transfer vial. (1 - 4 mls serum is needed, depending on the number of tests ordered. This information is included in the test combinations listing or the single test listing.)

11
Specimen Collection, Transport & Handling
3. Write the patient’s name and date of draw on the transfer vial. Make certain your name and address appear correctly on the order form (requisition form). Include your phone and fax numbers. Add the patient information including sex and date of birth. If we will be billing the patient or third party, please indicate by placing an “X” in the appropriate box. Include his/her address, telephone number and, if applicable, insurance information, copy of insurance card (both sides) and ICD-9 and/or ICD-10 diagnosis code(s). When applicable, your patient may have to sign the Insurance/HMO/Medicare waiver to avoid payment problems.
4. Specify which tests are to be performed by checking them off in the appropriate boxes on the requisition form. If a sendout test is to be ordered, specify in the “Special Request” area.
5. Place the transfer vial(s) into the mailing container with the order form(s). As many as four vials and requisition forms can fit into each mailing container. This container can be put in any mailbox, but most clients submit specimens by overnight express service. RDL recommends using Fedex, at no charge to your office. Simply place the container(s) in a Fedex clinical pak (as many as three boxes can fit into each pack) and attach the preprinted air bill. Call Fedex customer service at (800) 247-2676 for pick-up.
6. To request additional mailing supplies, you may call Client Services at (800) 338-1918, or e-mail [email protected].
Specimen Rejection Criteria
Criteria for acceptance or rejection of specimens have been developed and documented. Unacceptable specimens do not get tested, and therefore are not reported due to any of the following:
• The apparent condition of the specimen indicates that it is unsatisfactory for testing, or that it is inappropriate for the test requested
• The specimen has been collected, labeled, preserved or otherwise handled in such a manner to make it unsatisfactory or unreliable as a test specimen
• The time between the collection of the specimen and its receipt by RDL is of longer duration than permissible and the findings may no longer be reliable
Whenever a specimen is not tested due to any of the above, the client is promptly notified by phone with the reason.
Suspected Hepatitis & AIDS
All specimens should be handled as if they were infectious. Suspected and/or infectious substances must be sent in a proper I.D. mailer in compliance with ICAO/IATA Packing Instructions 602. These will be provided upon specific request.

12
Shipping Supplies & Requisition Forms
Free, federally-approved long distance mailers with transfer vials and prepaid postage labels are supplied. Preprinted requisition forms are also available. Use of overnight express service is recommended, which RDL offers free of charge through Fedex. See the section on Mailing Information for specifics. Please contact Client Services at (800) 338-1918 for immediate delivery of all shipping materials, including air bills and instructions.
Request Form (Requisition, Accession)
The request form contains sufficient information to identify the patient, the provider requesting processing of the specimen and pertinent clinical data for the patient. The request form allows space for inclusion of:
• Unique identification of patient – two forms of identification should be used (name and date of birth or other identifier, like patient id #)
• Patient information including gender, date of birth and diagnosis
• Name of provider authorized to request examination
• Type of sample and site of origin, where appropriate
• Examinations requested
• Date and time of collection
• Any additional information relevant or necessary for any specific assay to ensure accurate and timely testing and reporting of results
Legibility and Current Information
Problems occur when RDL order entry personnel cannot read what has been written on requisitions. It is important to write legibly. It is also imperative that the tests to be performed are noted on the requisition so that personnel are able to decipher exactly what is being ordered. Because RDL must contact the physician’s office to request information, these problems delay results and cause a longer turnaround time.
RDL also requests that current information regarding the patient and his/her medical insurance be attached to the requisition. Submitting obsolete insurance or patient information will delay results and cause a longer turnaround time.

13
Electronic Information Services
RDL offers several options for electronic data transmissions and regularly updates and explores innovative ways to assist our clients. All of the electronic options have secure internet connections.
For the client who desires his/her test results electronically, RDL offers Webresults. Once an order’s results are complete and a technologist performs the final approval of all the tests in an order, the client is then able to view his/her results over the internet.
RDL also offers an HL7 interface to our clients who meet specified volume criteria. An HL7 interface enables orders to be transmitted from the client’s system to RDL’s Laboratory Information System (LIS) and for RDL to transmit the results from our LIS back to our client’s system. RDL’s technical team works closely with our client’s technical team to enable this type of transmission.
For more information regarding our electronic data transmission, contact Client Services at 800.338.1918 and one of our representatives will discuss what electronic service would most benefit you and your practice.

14
Billing Information
Client Billing
Client accounts are billed monthly for all laboratory tests performed during the previous month. Statements are computer itemized to facilitate reconciliation. Simply place an “X” in the area labeled “Bill Client” on the preprinted requisition form. Payment terms are net 30 days. Due to State and Federal statutes, RDL is prohibited from offering “Professional Courtesy” testing.
Patient Billing
Patients can be billed directly for laboratory tests performed by RDL. Complete all required information on the requisition form, place an “X” in the “Bill Patient” area and provide the patient’s social security number, insurance information and other identifying information. Failure to indicate that patient billing is desired will result in the client being billed.
Please refer to the RDL Support Patient Assistance Program for our affordable Self-Pay Panels.
Medi-Cal/Medicaid
RDL bills for Medi-Cal and Medicaid patients (in those states that allow out-of-state lab work to be performed). Enter the correct numbers on the requisition form with the patient’s address, birth date and issue date. If possible, a copy of the card is appreciated. Place an “X” in the appropriate area. To facilitate billing, please have patients sign the Insurance/HMO/Medicare waiver on the requisition form. Always indicate an ICD-9-CM and/or ICD-10 diagnosis code.
Our referral laboratories do not bill for out-of-state Medicaid patients. Please do not send any sendout tests for your patients with Medicaid to RDL. If you send us any sendout (Medicaid) tests, your client’s account will be billed.
Medicare & Medicare/Medicaid
If a patient has coverage with Medicare or Medicare/Medicaid (Medi-Cal in California), please enter all numbers in the appropriate boxes and attach a copy of the card, if possible. Place an “X” in the “Medicare” area. To facilitate billing, please have patients sign the Insurance/HMO/Medicare waiver on the requisition form. Please verify that the patient’s name, birth date and address indicated on the requisition form are correct. Always indicate an ICD-9-CM and/or ICD-10 diagnosis code.

15
Billing Information
Insurance Carriers
As a courtesy, RDL will bill insurance companies directly for patients if information is provided with the specimen. However, the patient is responsible for the bill regardless of the filing of any insurance claim. Our laboratory is a contracted provider for Blue Cross and Blue Shield, as well as IPA and PPO plans throughout the country. Please call Client Services at (800) 338-1918 for an up-to-date listing of contracted carriers. Please refer to the RDL Support Patient Assistance Program for our Out-of-Network PPO policy.
Enter the correct numbers on the requisition form with the patient’s address, birth date and issue date. If possible, a copy of the card is appreciated. Place an “X” in the appropriate area. To facilitate billing, please have patients sign the Insurance/HMO/Medicare waiver on the requisition form. Include the patient’s social security number. Always indicate an ICD-9-CM and/or ICD-10 diagnosis code.
HMO Billing
RDL has no contracts with HMOs. Please do not send any requests for service for HMO patients. Due to regulations, if an insurance company is billed and the request is denied because the patient is an HMO member, the charges will be billed to the patient.
CPT Coding
RDL assumes no responsibility for the accuracy of the CPT codes listed in this catalog. It is the client’s responsibility to determine the correct CPT codes to use for billing. The RDL Test Catalog lists CPT codes to provide guidance. They reflect our interpretation of CPT coding and may not be correct due to possible changes. Please consult the CPT coding manual published by the American Medical Association.
Payments
Patients may pay by check, VISA, Mastercard or American Express. Required information for credit card payments: account number or invoice number, name of cardholder, card number, expiration date and amount to be charged. Payment can be made by phone at 800.338.1918 or mailed to RDL Reference Laboratory, P.O. Box 34020, Los Angeles, CA 90034.
Please be advised that specimens for patients residing outside of the United States must be accompanied by cash or the patient’s Credit Card information only. We cannot bill patients, or the insurance companies of patients, who reside outside of the United States. Please call Client Services to request a Credit Card Payment Agreement form.

16
List of Abbreviations
Ab Antibody
CH Chemiluminescence
COAG Coagulation
COL Colorimetric
DHA Direct Hemagglutination
DVVT Dilute Viper Venom Test
EIA ELISA Immunoassay
EL Electrophoresis
ELISPOT Enzyme-Linked Immunospot
ENZ Enzymatic
FC Flow Cytometry
FLOC Floculation
ID Immunodiffusion
IFA Indirect Immunofluorescence
KS Kinetic Spectrophotometry
LMC Lymphocyte Microcytotoxicity
MAC Macroscopic
OSRT One Step Rapid Test
PHA Passive Hemagglutination
PLA Passive Latex Agglutination
RIA Radioimmunoassay
RIPA Radioimmunoprecipitation Assay
TURB Turbidimetry
WB Western Blot
WEST Westergren
ZH Zimmer & Hargraves

17
Test Combinations
In Alphabetical Order

18
1228
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA,TURB, CH
86038, 86039, 86225, 86256, 86160 x 2, 86235 x 6, 86376, 86147 x 3, 86431, 86200
2 - 4 Days
Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), Anti-ENA Abs (Anti-SM & Anti-RNP), Anti-Centromere Ab, C3 & C4 Complements, SS-A Ab (Anti-Ro), SS-B Ab (Anti-La), Anti-SCL-70 Ab, Anticardiolipin Abs (IgG, IgA & IgM), Anti-Thyroid Microsomal Peroxidase Ab (TPO), Anti-Chromatin Ab, Rheumatoid Factor by TURB, Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP)
ANA 12 Plus Profile is reflexive. If ANA is positive, all tests listed are performed. If ANA is negative, an Anti-Ro (SS- A) test is performed to detect the small percentage of ANA false negative results. ANA includes titer & pattern. To order an ANA 12 Plus Profile, Do All, use #1230.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANA 12 Plus Profile
1785
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA,TURB, CH, ID
86038, 86039, 86225, 86256, 86160 x 2, 86235 x 6, 86376, 86147 x 3, 86431, 86200, 86780
2 – 4 Days
Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay by RIA), Anti-ENA Abs (Anti-SM & Anti-RNP), Anti-Centromere Ab, C3 & C4 Complements, SS-A Ab (Anti-Ro), SS-B Ab (Anti-La), Anti-SCL-70 Ab, Anticardiolipin Abs (IgG, IgA & IgM), Anti-Thyroid Microsomal Peroxidase Ab (TPO), Anti-Chromatin Ab, Rheumatoid Factor by TURB, Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP), RPR
ANA 12 Plus Profile with RPR is not reflexive. All tests listed are performed. If RPR is positive, then FTA is also performed. ANA includes titer & pattern. To order an ANA 12 Plus Profile with RPR, Do All, use #1785.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANA 12 Plus Profile with RPR
1201
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA, TURB, CH
86038, 86039, 86225, 86256, 86160 x 2, 86235 x 6, 86376, 86147 x 3
2 - 4 Days
Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), Anti-ENA Abs (Anti-SM & Anti-RNP), Anti-Centromere Ab, C3 & C4 Complements, SS-A Ab (Anti-Ro), SS-B Ab (Anti-La), Anti-SCL-70 Ab, Anticardiolipin Abs (IgG, IgA & IgM), Anti-Thyroid Microsomal Peroxidase Ab (TPO), Anti-Chromatin Ab
ANA 12 Profile is reflexive. If ANA is positive, all tests listed are performed. If ANA is negative, an Anti-Ro (SS-A) test is performed to detect the small percentage of ANA false negative results. ANA includes titer & pattern. To order an ANA 12 Profile, Do All, use #1206.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANA 12 Profile
1100
Requirements: 3 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA, TURB
86038, 86039, 86225, 86256, 86160 x 2, 86235 x 2
2 - 4 Days
Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), Anti-ENA Abs (Anti-SM & Anti-RNP), Anti-Centromere Ab, C3 & C4 Complements
ANA I Profile is reflexive. If ANA is positive, all tests listed are performed. If ANA is negative, an Anti-Ro (SS-A) test is performed to detect the small percentage of ANA false negative results. ANA includes titer & pattern. To order an ANA Profile I, Do All, use #1108.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANA Profile I

19
1020
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA,TURB, FLOC
86038, 86039, 86225, 86256, 86160 x 2, 86235 x 5, 86592
2 - 4 Days
Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), Anti-ENA Abs (Anti-SM & Anti-RNP), Anti-Centromere Ab, C3 & C4 Complements, SS-A Ab(Anti-Ro), SS-B Ab (Anti-La), Anti-SCL-70 Ab, RPR
ANA Profile II is reflexive. If ANA is positive, all tests listed are performed. If ANA is negative, an Anti-Ro (SS-A) test is performed to catch the small percentage of ANA false negative results. ANA includes titer & pattern. To order an ANA Profile II, Do All, use #1022.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANA Profile II
994
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA
86021, 83876, 83520, 86038, 86039
2 - 4 Days
Anti-Neutrophil Cytoplasmic Ab (ANCA), Anti-Myeloperoxidase Ab (MPO), Anti-Proteinase 3 Ab (PR-3), Anti-Nuclear Ab (ANA) if ANCA positive
Please note: C-ANCA & P-ANCA resulted if positive, otherwise reported as ANCA Negative. P-ANCA confirmed on formalin fixed slides. ANA performed if ANCA positive to rule out false positive ANCA due to presence of ANAs.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
ANCA Panel
1811
Requirements: 2 mL serum & 2 frozen plasma vials, 1 mL each from 2 sodium citrated tubes (blue top)
EIA, DRVVT
86147 x 3, 85613, 86146 x 3
2 - 4 Days
Anticardiolipin Abs (IgG, IgA & IgM), Lupus Anticoagulant, Anti-Beta-2-Glycoprotein Abs (IgG, IgA & IgM)
For Lupus Anticoagulant, collect specimen in 2 sodium citrated tubes (blue top). Mix by inverting ten times. Check for fibrin clots using wooden applicator sticks (clotted specimen is unsatisfactory). Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (overnight if out of courier area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Designate on the tubes which is serum and which is plasma.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Antiphospholipid Ab Panel I
1850
Requirements: 3 mL serum & 2 frozen plastic vials plasma, 1 mL each, from 2 sodium citrated tubes (blue top)
EIA, DRVVT, FLOC
86147 x 3, 85613, 86148 x 3, 86146 x 3, 86592
3 - 5 Days
Anticardiolipin Abs (IgG, IgA & IgM), Lupus Anticoagulant, Anti-Phosphatidylserine Abs (IgG, IgA & IgM), Anti-Beta-2-Glycoprotein I Abs (IgG, IgA & IgM), RPR
See Antiphospholipid Ab Panel I for instruction for the Lupus Anticoagulant test. Send plasma frozen on dry ice by overnight express mail. The serum may also be frozen. Designate on the tubes which is serum and which is plasma.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Antiphospholipid Ab Panel II

20
1292
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used.
RIPA, EIA
86235, 83516 x 4
10 - 14 Days
Jo-1, PL-7, PL-12, EJ, OJ
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Anti-Synthetase Panel
996
Requirements: 3 mL serum, ambient, refrigerated or frozen TURB, IFA, COL, EIA
86431, 86038, 86039, 84550, 86200
1 - 3 Days
Rheumatoid Factor by TURB, Anti-Nuclear Ab (ANA), Uric Acid, Anti-CCP Ab
Postive ANA includes titer & pattern.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Arthritis Panel
265
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520 x 2
7 Days
Anti-Inner Ear Membrane Ab IgG, Anti-Human Heat Shock Protein 70-kd (HSP-70) Ab IgG
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Autoimmune Inner Ear Disease Panel (AIED Panel)
558
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA, IFA
86038, 86039, 83520 x3, 86235, 86021, 86376
3 - 5 Days
Anti-Nuclear Ab (ANA), Anti-Actin Ab IgG, Anti-Mitochondrial M2 EP Ab, Anti-Liver/Kidney Microsomal Ab, Anti-Soluble Liver Ag Ab, P-ANCA, Anti-Chromatin Ab
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Autoimmune Liver Disease Panel, Comprehensive

21
1044
Requirements: 3 mL serum, ambient, refrigerated or frozen IFA, EIA
83520 x 4, 86256, 82784
3 - 5 Days
Anti-Gliadin II (DGP) Abs IgA & IgG, Anti-Endomysial Ab IgA, Tissue Transglutaminase (tTG) Ab IgA, Immunoglobulin IgA level, Anti-F Actin Ab IgA
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Celiac Disease Ab Panel
1390
Requirements: 10 mL red stoppered tube. Do not use serum separator or gel barrier tube.
MAC,TURB, EL
82595 (If Positive: 82784 x 3, 86334, 86431)
4 -9 Days
If the Cryoglobulin is positive, reflexes to: QIG, IFE & Rheumatoid Factor by TURB
Allow specimen to clot, then place into a water bath at +37 degrees C for 1 hour. Centrifuge and separate immediately, while still warm. After treatment, specimen can be refrigerated. Please mark tube “Treated for Cryo” and note date & time of collection. Send by overnight express mail. Untreated whole blood cannot be sent. Please Note: Cryos have to be read for 6 days to assure positivity. If it turns positive on the 6th day, 3 more days are needed to result it and reflexive tests.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Cryoglobulins Characterization Panel
564
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA
86664, 86665 x 2, 86663
3 - 5 Days
Epstein Barr Nuclear Ag (EBNA) Ab IgG, Epstein Barr Viral Capsid Ag (VCA) Abs IgG & IgM, Epstein Barr Virus - Early Antigen (EA) Ab
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Epstein Barr Viral Panel
1079
Requirements: 4 mL serum, ambient, refrigerated or frozen IFA, EIA, RIA, TURB
86021, 83520 x 2, 83876, 86038, (If ANA Positive: 86039), 86225, 86160 x 2
3 - 5 Days
Anti-Neutrophil Cytoplasmic Ab (ANCA), Anti-Myeloperoxidase Ab (MPO), Anti-Proteinase 3 Ab (PR-3), Anti-Glomerular Basement Membrane Ab (GBM), Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), C3 & C4 Complements
Please note: C-ANCA & P-ANCA resulted if positive. Otherwise reported as ANCA Negative. P-ANCA confirmed on formalin fixed slides. ANA performed if ANCA positive to rule out false positive ANCA due to presence of ANAs.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Glomerulonephritis Panel (GNP)

22
349
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520 x 4
3 - 5 Days
Anti-Gliadin (DGP) Ab IgG & IgA, Tissue Transglutaminase (tTG) Ab IgA, Anti F-Actin Ab IgA
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Gluten Free Dietary Compliance Panel
704
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA, CH
87340, 86705, 86709
3 - 5 Days
Hepatitis B Surface Ag (HBsAg), Hepatitis B Core Ab IgM (HBc), Hepatitis A Virus Ab IgM (HAV)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Hepatitis Panel I – Acute
705
Requirements: 4 mL serum, ambient, refrigerated or frozen EIA, CH
86708, 86709, 87340, 86706, 86704, 86705, 86803
3 - 5 Days
Hepatitis A Virus Abs, IgG & IgM (HAV), Hepatitis B Surface Ag (HBsAg), Hepatitis B Surface Ab (HBsAb), Hepatitis B Core Ab IgG & IgM (HBc), Hepatitis C Virus Ab (HCV)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Hepatitis Panel II
1277
Requirements: 3 mL serum & 2 frozen plastic vials plasma, 1 mL each, from 2 sodium citrated tubes (blue top)
IFA, EIA, DRVVT, CH, TURB
86038, 86309, 86147 x 3, 85613, 86148 x 3, 86146 x 3, 86376, 86800, 86256, 86431
3 - 5 Days
Anti-Nuclear Ab (ANA), Anticardiolipin Abs (IgG, IgA & IgM), Lupus Anticoagulant, Anti-Phosphatidylserine Abs (IgG, IgA & IgM), Anti-Beta-2-Glycoprotein I Abs (IgG, IgA & IgM), Thyroid Microsomal Ab, Thyroglobulin Ab, Anti- Ovary Ab, Rheumatoid Factor by TURB
For Lupus Anticoagulant, collect specimen in 2 sodium citrated tubes (blue top). Mix by inverting ten times. Check for fibrin clots using wooden applicator sticks (clotted specimen is unsatisfactory). Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (overnight if out of courier area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Designate on the tubes which is serum and which is plasma.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Implant Failure Panel

23
1265
Requirements: 2 mL serum, ambient, refrigerated or frozen IFA, EIA
83520 x 2, 86021, 86255
3 - 5 Days
Anti-Saccharomyces Cerevisiae Abs IgG & IgA Isotypes (ASCA), Atypical P-ANCA, Anti-Pancreatic Ab (PAB)
Atypical P-ANCA is confirmed on formalin fixed slides. If the Atypical P-ANCA is positive, an ANA is performed at no further expense.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Inflammatory Bowel Disease Panel
475
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used but should be sent with 2 mL of serum.
RIPA, EIA, IFA, TURB
86235 x 4, 83516 x 7, 86038, 86200, 86431
10 - 14 Days
Jo-1, PL-7, PL-12, EJ, OJ, SRP, PM/Scl, Ku, Anti-SSA 52 kD Ab, ANA, CCP, Scl-70, Rheumatoid Factor by TURB, MDA5
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Interstitial Lung Disease Panel I
354
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used but should be sent with 2 mL of serum.
RIPA, EIA
86235 x 3, 83516 x 6, 83520
10 - 14 Days
Jo-1, PL-7, PL-12, EJ, OJ, SRP, PM/Scl, Ku, Anti-SSA 52 kD Ab, MDA5
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Interstitial Lung Disease Panel II
1065
Requirements: 2 mL serum, ambient, refrigerated or frozen RIA, TURB
86225, 86160 x 2
1 - 3 Days
Anti-dsDNA Ab (Farr Assay), C3 & C4 Complements
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lupus Activity Panel

24
342
Requirements: 2 mL serum, ambient, refrigerated or frozen RIA, TURB, EIA
86225, 86160 x 2, 83520
2 - 5 Days
Anti-dsDNA Ab by Farr, C3 & C4 Complements, C1Q Ab IgG
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lupus Renal Activity Panel
628
Requirements: One 7 or 10 mL EDTA tube (lavender top) whole blood at room temperature
FC
86360, 86359
1 - 3 Days
CD3, CD4, CD8, CD4/CD8 Ratio
EDTA whole blood should be at room temperature. Do not spin or separate. Do not refrigerate. Send by overnight express mail.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lymphocyte Immunophenotyping Panel: Helper/Suppressor Panel
634
Requirements: One 7 or 10 mL EDTA tube (lavender top) whole blood at room temperature
FC
86360, 86359, 86355
1 - 3 Days
CD3, CD4, CD8, CD4/CD8 Ratio, CD19
EDTA whole blood should be at room temperature. Do not spin or separate. Do not refrigerate. Send by overnight express mail.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lymphocyte Immunophenotyping Panel: T & B Cell Panel
629
Requirements: One 7 or 10 mL EDTA tube (lavender top) whole blood at room temperature
FC
86360, 86359, 86355, 86357
1 - 3 Days
CD3, CD4, CD8, CD4/CD8 Ratio, CD19, CD56/16
EDTA whole blood should be at room temperature. Do not spin or separate. Do not refrigerate. Send by overnight express mail.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lymphocyte Immunophenotyping Panel: T, B & NK Cell Panel

25
633
Requirements: One 7 or 10 mL EDTA tube (lavender top) whole blood at room temperature
FC
86359, 86357
1 - 3 Days
CD56/16, CD3
EDTA whole blood should be at room temperature. Do not spin or separate. Do not refrigerate. Send by overnight express mail.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Lymphocyte Immunophenotyping: Natural Killer Cell 56/16
1377
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used.
RIPA
83516 x 8
10 - 14 Days
Mi-2, PL-12, PL-7, EJ, OJ, SRP, Ku, U2 snRNP
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
MyoMarker™ Panel 1
245
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used.
RIPA, EIA
83516 x 8, 86235 x 2
10 - 14 Days
Jo-1, Mi-2, PL-12, PL-7, EJ, OJ, SRP, Ku, U2 snRNP, PM/Scl
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
MyoMarker™ Panel 2
1222
Requirements: 3 mL serum, ambient, refrigerated or frozen. EDTA plasma can be used.
RIPA, EIA
86235 x 4, 83516 x 9, 83520 x 3
10 - 14 Days
Mi-2, Jo-1, PL-12, PL-7, EJ, OJ, SRP, Ku, U2 snRNP, PM/Scl, MDA5, NXP2, TIF-1y, SSA 52 KD Ab IgG, U1 RNP, Fibrillarin U3 RNP
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
MyoMarker™ Panel 3

26
655
Requirements: 3 mL serum, ambient, refrigerated or frozen and 2 Lithium Heparin (green top), 6 mL each at room temperature.
EIA, ELISPOT, CH
86704, 86705, 86706, 87340, 86803, 86481
3 - 5 Days
Hepatitis B Surface Ag, Hepatitis B Surface Ab, Hepatitis B Core Ab Total & IgM, Hepatitis C Ab, T-Spot TB test
Patients can only be drawn Monday – Thursday because of the T-Spot TB test. Please do not draw on Friday (except for clients in the greater Los Angeles area). Before drawing, call RDL for special supplies with gel pack. 1) Draw two lithium heparin [green top] tubes [6 mL each]. Invert ten times to mix. Do not centrifuge. Time of draw must be written on both tubes. Keep them at room temperature. NEVER REFRIGERATE OR FREEZE. 2) Keep the specimen ambient, at room temperature until the RDL courier or FEDEX courier picks it up. The specimen must be picked up same day of draw.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Pre-Biologic Therapy Assessment Panel
822
Requirements: 3 mL serum, ambient, refrigerated or frozen and 2 Lithium Heparin (green top), 6 mL each at room temperature.
EIA, ELISPOT, CH, IFA, RIA
86481, 86706, 87340, 86704, 86705, 86803, 86038, 86039, 86225, 86235
2 - 5 Days
Hepatitis B Surface Ag, Hepatitis B Surface Ab, Hepatitis B Core Ab Total & IgM, Hepatitis C Ab, Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr), Anti-Histone Ab
Patients can only be drawn Monday – Thursday because of the T-Spot TB test. Please do not draw on Friday (except for clients in the greater Los Angeles area). Before drawing, call RDL for special supplies with gel pack. 1) Draw two lithium heparin [green top] tubes [6 mL each]. Invert ten times to mix. Do not centrifuge. Time of draw must be written on both tubes. Keep them at room temperature. NEVER REFRIGERATE OR FREEZE. 2) Keep the specimen ambient, at room temperature until the RDL courier or FEDEX courier picks it up. The specimen must be picked up same day of draw.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Pre-Biologic Therapy Assessment Panel + ANA, dsDNA & Histone
788
Requirements: 3 mL serum, ambient, refrigerated or frozen and 2 Lithium Heparin (green top), 6 mL each at room temperature.
EIA, ELISPOT, ID, CH
86704, 86705, 86706, 87340, 86803, 86481, 86635 x 2
4 - 6 Days
Hepatitis B Surface Ag, Hepatitis B Surface Ab, Hepatitis B Core Ab, Total & IgM, Hepatitis C Ab, T-Spot TB test, Coccidioidomycosis Ab, IgM & IgG
Patients can only be drawn Monday – Thursday because of the T-Spot TB test. Please do not draw on Friday (except for clients in the greater Los Angeles area). Before drawing, call RDL for special supplies with gel pack. 1) Draw two lithium heparin [green top] tubes [6 mL each]. Invert ten times to mix. Do not centrifuge. Time of draw must be written on both tubes. Keep them at room temperature. NEVER REFRIGERATE OR FREEZE. 2) Keep the specimen ambient, at room temperature until the RDL courier or FEDEX courier picks it up. The specimen must be picked up same day of draw.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Pre-Biologic Therapy Assessment Panel with Coccidioidomycosis
1600
Requirements: 3 mL serum, ambient, refrigerated or frozen IFA & EIA
86038, 86256, 83520 x 3
4 - 7 Days
Anti-Nuclear Ab (ANA), Anti-Mitochondrial Ab by IFA, Anti-Mitochondrial M2 EP Ab by EIA, Anti-Gp-210 Ab, Anti-Sp-100 Ab
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Primary Biliary Cirrhosis Panel (PBC)
27
1789
Requirements: 3 mL serum & 2 frozen plasma vials, 1 mL each, from 2 sodium citrated tubes (blue top)
IFA, DVVT, EIA, CH
86038, 86039, 86147 x 3, 85613, 86148 x 3, 86146 x 3, 86376, 86800
3 - 5 Days
Anti-Nuclear Ab (ANA), Anticardiolipin Abs (IgG, IgA & IgM), Lupus Anticoagulant, Anti-Phosphatidylserine Abs (IgG, IgA & IgM), Anti-Beta-2-Glycoprotein I Abs (IgG, IgA & IgM), Anti-Thyroid Microsomal Ab (TPO), Anti-Thyroglobulin Ab
For Lupus Anticoagulant, collect specimen in 2 sodium citrated tubes (blue top). Mix by inverting ten times. Check for fibrin clots using wooden applicator sticks (clotted specimen is unsatisfactory). Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (overnight, if out of courier area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Designate on the tubes which is serum and which is plasma.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Recurrent Pregnancy Loss Panel
1041
Requirements: 4 mL serum, ambient, refrigerated or frozen and 7 mL red stoppered tube (Do not use SST or barrier tube for Cryoglobulins)
EIA, IFA, TURB, RIA, MAC
83876, 83520 x 2, 86431, 87340, 86803, 86038, 86225, 86160 x 2, 82595, 86021
6 - 10 Days if positive
Reflexive from Anti-MPO and Anti-PR-3. If either test is positive, reflexes to an ANCA by IFA. If both tests are negative, reflexes to the following: ANCA by IFA, Rheumatoid Factor by TURB, Hepatitis C Ab, Hepatitis B Surface Ag, Anti-GBM Ab, Cryoglobulins, Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (FARR Assay), Complements C3 & C4
For Cryoglobulin, do not use serum separator or barrier tube. Immediately after collection place into a water bath at +37 degrees C for 1 hour. Centrifuge and separate immediately, while still warm. Please mark tube “Treated for Cryo” and please note date & time of collection. Untreated whole blood cannot be accepted. Send by overnight express mail. For all the other tests, serum can be sent in same package as Cryoglobulins. Please Note: Cryos have to be read for 6 days to assure positivity. If it turns positive on the 6th day, 2 more days are needed to result it.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Reflexive Systemic Vasculitis Panel I (RSVP I)
1085
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA, IFA, RIA, TURB
83876, 83520, 86021, 87340, 86431, 86803, 86038, 86225, 86160 x 2
2 - 6 Days
Reflexive from Anti-MPO and Anti-PR-3. If either test is positive, reflexes to an ANCA by IFA. If both tests are negative, reflexes to the following: ANCA by IFA, Rheumatoid Factor by TURB, Hepatitis C Ab, Hepatitis B Surface Ag, Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (FARR Assay), Complements C3 & C4
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Reflexive Systemic Vasculitis Panel II (RSVP II)
1030
Requirements: 2 mL serum, ambient, refrigerated or frozen TURB, EIA
86431, 86200
1 - 3 Days
Rheumatoid Factor by TURB, Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Rheumatoid Arthritis Ab Panel

28
1836
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA, TURB
86431 x 3, 86200
3 - 5 Days
Rheumatoid Factor IgG & IgA by EIA, Rheumatoid Factor IgM by TURB, Anti-Cyclic Citrullinated Peptide Ab (Anti- CCP)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Rheumatoid Arthritis Autoantibody Panel, Comprehensive
1686
Requirements: 3 mL serum, ambient, refrigerated or frozen EIA, IFA, RIPA
86038, 86039, 86235 x 4, 86256, 83516 x 2
10 - 14 Days
Anti-Nuclear Ab (ANA), Anti-Scl 70 Ab, Anti-RNA Polymerase III Ab, Anti-Centromere Ab, Th/To Ab, Anti-U1 RNP Ab, Fibrillarin U3, Anti-PM/Scl Ab
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Scleroderma Panel, Comprehensive
1257
Requirements: 4 mL serum, ambient, refrigerated or frozen; One EDTA tube (lavender top) whole blood at room temperature
EIA, FC, IFA, WB
86200, 86747 x 2, 86812, 86803, 86038, 86618, 86317 x 2 if Lyme EIA positive
3 - 7 Days
Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP), Parvovirus Ab IgM & IgG, HLA-B27, Hepatitis C Ab (HCV), Anti- Nuclear Ab (ANA), Lyme (EIA) Reflexive to WB
Positive ANA includes titer & pattern.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Seronegative Arthritis Panel I
1438
Requirements: 7 OR 10 mL EDTA tube (lavender top) at room temperature and 3 mL serum, ambient, refrigerated or frozen.
IFA, FC, EIA, COL
86256, 86812, 83520 x 2
3 - 5 Days
Atypical P-ANCA, HLA-B27, ASCA IgA & IgG. If Atypical P-ANCA is positive, an ANA and P-ANCA on ETOH and Formalin will be performed.
EDTA whole blood should be at room temperature. Do not spin or separate. Do not refrigerate. Send by overnight express mail.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Spondyloarthropathy Panel

29
1717
Requirements: 2 mL serum, ambient, refrigerated or frozen CH
86800, 86376
1 - 3 Days
Anti-Thyroglobulin Ab, Anti-Thyroid Microsomal Peroxidase Ab (TPO)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Thyroid Autoantibody Panel
1661
Requirements: 2 mL serum, ambient, refrigerated or frozen CH
84436, 84479, 84443
1 - 3 Days
T4 Thyroxine,T3 Uptake,T7 Free Thyroxine Index, Thyroid Stimulating Hormone, 3rd Generation (TSH)
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Thyroid Function Panel
1070
Requirements: 4 mL serum, ambient, refrigerated or frozen and 10 mL red stoppered tube
IFA, EIA, RIA, MAC, TURB
86021, 83520 x 2, 83876, 82595, 87340, 86803, 86431, 86038, 86039, 86225, 86160 x 2
4 - 8 Days
Anti-Neutrophil Cytoplasmic Ab (ANCA), Anti-Proteinase 3 Ab (PR-3), Anti-Myeloperoxidase Ab (MPO) , Anti- Glomerular Basement Membrane Ab (GBM), Cryoglobulin, Hepatitis B Surface Ag (HBsAg), Hepatitis C Ab (HCV), Rheumatoid Factor by TURB, Anti-Nuclear Ab (ANA), Anti-dsDNA Ab (Farr Assay), C3 & C4 Complements
For Cryoglobulin, do not use serum separator or barrier tube. Immediately after collection place into a water bath at 37 degrees C for 1 hour. Centrifuge and separate immediately, while still warm. Please mark tube “Treated for Cryo” and please note date & time of collection. Send by overnight express mail. Please Note: Cryos have to be read for 6 days to assure positivity. If it turns positive on the 6th day, 2 more days are needed to result it.
Method:
CPT Codes:
Turnaround Time:
Instructions:
Tests In Profile/Panel:
Vasculitis Panel I

30

31
Individual Tests
In Alphabetical Order
32
272
Requirements: 2 mL serum, ambient, refrigerated or frozen KS
82085
<8.2 U/L
5 Days
Detection of aldolase is a useful tool in the diagnosis and monitoring of many skeletal muscle disorders, myocardial infarction and liver disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Aldolase
465
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
82103
84-218 Mg/dL
1 - 3 Days
Measurement of alpha 1-antitrypsin aids in the diagnosis of juvenile and adult cirrhosis of the liver. Alpha 1-antitrypsin deficiency has been associated with neonatal respiratory distress syndrome, severe protein-losing disorders, and pulmonary emphysema.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Alpha 1-Antitrypsin
147
Requirements: 1 mL serum, ambient, refrigerated or frozen KS
82164
16 - 70 Units
2 - 5 Days
ACE is increased in some cases of active sarcoidosis, with sensitivity of about 75% and specificity about 95%. Elevated ACE levels will return to normal in sarcoidosis as a result of spontaneous or corticosteroid-induced remission. Decreased ACE activity is found in patients having chronic obstructive lung disease, lung cancer, emphysema, and cystic fibrosis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Angiotensin Converting Enzyme (ACE)
105
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20 Units
3 - 5 Days
Anti-actin autoantibodies are the main component of smooth muscle antibodies (SMA). Anti-actin IgG antibodies are found in 52-85% of patients with AIH I and in 22% of patients with primary billiary cirrhosis (PBC). Anti-actin antibodies have been reported, usually in low titers, in 3-18% of sera from the general healthy population. Anti-actin IgG antibody positive patients were more prone to be unresponsive to corticosteroid therapy (16% vs. 4%) and were more prone to suffer liver failure (20% vs. 4%).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Actin Ab, IgG

33
10
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:10
3 - 5 Days
Adrenal antibody (AA) is a marker, particularly in females, for a gonadal dysfunction due to autoimmune oophoritis. AA is detected in about two-thirds of patients with idiopathic Addison disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Adrenal Ab
185
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<10 Units
10 Days
Screening for antibodies directed against alpha-fodrin can be a useful tool in diagnosing early stage Sjogren’s syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Alpha Fodrin Ab, IgA
184
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<10 Units
10 Days
Screening for antibodies directed against alpha-fodrin can be a useful tool in diagnosing early stage Sjogren’s syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Alpha Fodrin Ab, IgG
6
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86146 x 3
<20 EU
1 - 3 Days
The presence of Beta2 GPI IgA, IgG and IgM antibodies can be used in conjunction with clinical findings and other laboratory tests to aid in the diagnosis of certain autoimmune disorders such as antiphospholipid syndrome and systemic lupus erythematosus (SLE).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Beta-2-Glycoprotein I Abs, IgG, IgA & IgM

34
458
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20 Units
5-7 Days
Weak Positive: 20-39 Units, Moderate Positive: 40-80 Units, Strong Positive: >80 Units
Serial testing shows that increasing amounts of anti-C1q IgG predict renal flares in SLE patients. Elevated serum titers of anti-C1q antibodies tend to be associated with proliferative forms of lupus glomerulonephritis and subendothelial deposits of immune complexes.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-C1Q Ab, IgG
9
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86147 x 3
IgG: <15.0 GPL, IgA: <15.0 APL, IgM: <12.5 MPL
1 - 3 Days
Anticardiolipin antibodies (ACA) can be used in conjunction with clinical findings and other laboratory tests to aid in the diagnosis of certain autoimmune disorders such as antiphospholipid syndrome and systemic lupus erythematosus (SLE).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anticardiolipin Abs, IgG, IgA & IgM
12
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:40
1 - 3 Days
The most common setting for finding anti-centromere antibodies is in patients with a limited cutaneous form of scleroderma. Anti-centromere abs are found in 46% of patients with Limited Systemic Sclerosis and 11% in Diffuse Systemic Sclerosis, as well as 12% of patients with primary billiary cirrhosis, and are rarely present in normal individuals.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Centromere Ab
578
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
1 - 3 Days
Chromatin is a native complex of histones and DNA found in the cell nucleus of eukaryotes, and is comprised of approximately 40% DNA, 40% histones and 20% non-histone proteins, RNA and other macromolecules. The presence of chromatin antibodies can be used in conjunction with clinical findings and other laboratory tests to aid in the diagnosis of drug-induced lupus (DIL) and Systemic Lupus Erythematosus (SLE).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Chromatin Ab, IgG

35
165
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86200
<20 Units
1 - 3 Days
Anti-CCP 3.1 has a higher sensitivity (70%) than most commercially available Anti-CCP assays with a specificity of 93-95% for RA. A positive CCP is found in about 40% of RF IgM negative RA patients.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP), IgG
14
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86226
Negative
3 - 5 Days
Single-stranded DNA (ssDNA) autoantibodies aid in the diagnosis of Systemic Lupus Erythematosus (SLE) and related connective tissue diseases. Anti-ssDNA abs are found in 80-90% of SLE patients during the administration of certain drugs (e.g., procainemide or quinidine), but are also present in other autoimmune diseases including rheumatoid arthritis, scleroderma, linear localized scleroderma, polymyositis-dermatomyositis, Sjogren’s syndrome, mixed connective tissue disease (MCTD) and overlap syndromes, myasthenia gravis, chronic active hepatitis, infectious mononucleosis, chronic glomerulonephritis, JIA and billiary cirrhosis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-DNA Ab (Single Stranded)
38
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86225
<1:10
2 - 4 Days
The crithidia IFA method for anti-dsDNA antibodies has a high disease specificity but a low disease sensitivity (as low as 13%). The method detects intermediate to high avidity anti-dsDNA antibodies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-dsDNA Ab (Crithidia)
13
Requirements: 1 mL serum, ambient, refrigerated or frozen RIA
86225
<8.0 IU/mL
1 - 3 Days
The Farr method detects the high avidity anti-dsDNA antibodies. RDL’s Farr has a high sensitivity (72%) with a specificity of 94% for SLE. The Farr assay can be followed to assess SLE disease activity and treatment effectiveness. Anti-dsDNA antibodies correlate with renal involvement.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-dsDNA Ab (Farr Assay, Double Stranded)

36
136
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86225
<92.6 WHO u/mL
3 - 5 Days
Aids in the diagnosis of systemic lupus erythematosus (SLE) and related connective tissue diseases. The EIA method can detect low to high avidity anti-dsDNA antibodies. The specificity of the EIA assay is not as good as other anti-dsDNA detection methods. It can be positive in other autoimmune diseases such as Scleroderma, autoimmune hepatitis, Sjogren’s syndrome, Myasthenia gravis and others.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-dsDNA Ab by ELISA
914
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235 x 2
<20 Units
1 - 3 Days
Aid in the diagnosis of Systemic Lupus Erythematosus (SLE), and related connective tissue diseases such as Sjogren’s Syndrome. Anti-Sm is highly specific for SLE. Anti-RNP, especially in high titers, is highly specific for MCTD, although it may also be found is other autoimmune disorders such as Scleroderma.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-ENA Abs (Anti-SM & Anti-RNP)
52
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:10
1 - 3 Days
The sensitivity of Endomysial IgA antibodies in untreated celiac disease (CD) is 80-97% with a specificity of over 97%. They are found in at least 70-80% of patients with dermatitis herpetiformis (DH) on a gluten-containing diet and 100% of patients with gluten-sensitive enteropathy with severe villous atrophy.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Endomysial Ab, IgA
575
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20 Units
3 - 5 Days
Anti-actin autoantibodies are the main component of smooth muscle antibodies (SMA). Anti-F-Actin IgA antibodies are 86-93% sensitive and 81-90% specific for celiac disease. IgA antibodies to F-Actin show a strong correlation with the degree of intestinal villus atrophy present in celiac disease patients. Anti-F-Actin IgA antibodies decrease following institution of a gluten-free diet and measurement of these antibodies may have a role in monitoring gluten free diet compliance.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-F Actin Ab, IgA

37
452
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520 x 2
<20 Units
3 - 5 Days
IgG and IgA AGA-DGP (Anti-Gliadin Ab-Deaminated Gliadin Peptides) are useful in screening for celiac disease and monitoring compliance with a gluten-free diet. IgG AGA-DGP are 82% sensitive and 90% specific and can be positive in patients with an IgA deficiency. IgA AGA-DGP have a sensitivity of 86-93% and a specificity of 81-90%.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Gliadin II (DGP) Ab, IgG & IgA
956
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20 Units
3 - 5 Days
Anti-GBM autoantibodies are recognized as being important in the pathogenesis of the rapidly progressive glomerulonephritis of Goodpasture’s syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Glomerular Basement Membrane Ab (Anti-GBM)
1601
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520
<=20.0 Units
4 - 7 Days
Primary Biliary Cirrhosis (PBC) is an organ-specific autoimmune disease characterized by chronic progressive destruction of intrahepatic bile ducts with portal inflammation resulting in chronic cholestasis and ultimately fibrosis. Serologic assays are important tools for the recognition and diagnosis of PBC, since many antibodies associated with PBC can be present years before symptoms become evident. Gp210 has a sensitivity of 16-32% and a specificity of 99% for PBC. Gp210, along with Sp100 can detect up to 70% of AMA negative PBC patients.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Gp-210 Ab
15
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<1.0 Units
3 - 5 Days
Anti-Histone Abs may help in confirming a suspicion of Drug Induced LE, but cannot distinguish Drug Induced ANA from Drug Induced LE which typically targets H2A-H2B-DNA (Anti-Chromatin), particularly in Procainamide Induced LE. Found in 67-100% of Drug Induced LE and 24-95% of SLE. Can be seen occasionally in SSc, RA, Sjogren’s, JIA, Felty’s Syndrome, MCTD, Vasculitis, Neoplasms and Liver Disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Histone Ab

38
1809
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20
Anti-HMGCR IgG antibodies are highly associated with necrotizing myositis; appearing in 42% of all necrotizing myositis cases and about 5% of DM/PM. 73% of positive patients have been exposed to statin medications. They are rarely found in statin-naive adults and children.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-HMGCR IgG Ab
260
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520
<25 Units/mL
7 Days
Autoimmune inner ear disease (AIED) is a heterogeneous group of diseases with regard to clinical presentation and immunoreactivity to inner ear components. They include rapidly progressive sensorineural hearing loss (SNHL), Ménière’s disease (MD) and sudden deafness (SD). Anti-HSP-70 antibodies have a sensitivity of 50-84% and a specificity of >90% for AIED.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Human Heat Shock Protein 70-kd Ab, IgG (HSP-70), EIA
559
Requirements: 1 mL serum, ambient for 2 days, refrigerated for 2 weeks or frozen for 6 months
WB
84181
Negative
7 Days
Autoimmune inner ear disease (AIED) is a heterogeneous group of diseases with regard to clinical presentation and immunoreactivity to inner ear components. They include rapidly progressive sensorineural hearing loss (SNHL), Ménière’s disease (MD) and sudden deafness (SD). Anti-HSP-70 antibodies have a sensitivity of 50-84% and a specificity of >90% for AIED.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Human Heat Shock Protein 70-kd Ab, IgG (HSP-70), WB
259
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520
<25 Units/mL
7 Days
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Inner Ear Membrane Ab, IgG
Autoimmune inner ear disease (AIED) is a heterogeneous group of diseases with regard to clinical presentation and immuno-reactivity to inner ear components. They include rapidly progressive sensorineural hearing loss (SNHL), Ménière’s disease (MD), and sudden deafness (SD). The search for a diagnostic test led to the finding that most AIED patients had antibodies that react with 130-kd, 68-kd, 58-kd, 42-kd and 30-kd (P0) proteins from human and bovine ears. The presence of antibodies to a 68-kd antigen, identified by Western blot, has been the best candidate to date as a diagnostic test for AIED and may be useful in predicting steroid responsiveness. Moreover, reactivity with the 68-kd protein was present in serum samples from 89% of 47 patients with active disease compared to none of 25 patients with inactive disease. Of the 36 patients with a positive test result on Western blot assay for antibodies to the 68-kd protein, 27 (75%) responded to steroid therapy. Only four (18%) of the 22 patients with a negative test result responded to steroid therapy. Another study showed a positive reaction to P0 (from guinea pig inner ear extraction) in all bilateral MD and bilateral sudden hearing loss patients and indicates these pathologies are the result of an ongoing autoimmune process directed against specific inner ear antigens. The 68-kd inner ear antigen identified by Ramakrishnam is not HSP-70.

39
53
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86341
<1:2
3 - 5 Days
Multiple antibodies are detected in the Islet Cell IgG autoantibodies assay (ICA), including GAD (Glutamic Acid Decarboxylase) autoantibodies. Sensitivity in new insulin-dependent diabetes mellitus is usually over 80%. Specificity is greatly improved if subjects have both ICA and other autoantibodies such as GAD and anti-insulin antibodies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Islet Cell Ab
434
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
Negative
4 - 6 Days
Jo-1 antibodies are found in approximately 20% of adult patients with Idiopathic Inflammatory Myopathy, which can include polymyositis, dermatomyositis or overlap syndromes. This antibody is highly associated with non-erosive arthritis, interstitial lung disease, fever, mechanic’s hands and Raynaud’s.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-JO 1 Ab
576
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
1 - 3 Days
Autoantibodies to SS-B/La antigen are detected by EIA in 60% of primary Sjogren’s syndrome (SS), 15% of SLE and 80% of subacute cutaneous lupus. Circulating SS-B or SS-A antibodies in the mother can cause neonatal congenital heart block.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-LA Ab (SS-B)
129
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86376
<=20 Units
3 - 5 Days
Anti-LKM antibody positivity is a defining characteristic of Autoimmune Hepatitis Type 2. This antibody is found in approximately 4% of all autoimmune hepatitis patients. LKM-1 antibodies have been reported in up to 8% of patients with chronic HCV infection.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Liver/Kidney Microsomal Ab

40
173
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
EIA
83520
<20
10 - 14 Days
Anti-MDA5 antibodies are present in 7-35% of adult DM. Clinical features consist of absent or mild muscle symptoms (CADM), rapidly progressive ILD, specific mucocutaneous features of skin ulcerations and papules, oral ulcerations and arthritis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-MDA5 (part of P140 kD) AKA CADM-140
18
Requirements: 2 mL serum, ambient, refrigerated or frozen IFA
86256
<1:20
2 - 4 Days
Anti-mitochondrial antibodies (AMA) have been reported in up to 95% of patients with primary billiary cirrhosis (PBC) with a specificity of 93%. AMA are also occasionally found in patients with other liver conditions, including chronic active hepatitis, cryptogenic cirrhosis and in patients with no clinical or biochemical evidence of liver disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Mitochondrial Ab by IFA
428
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<=20 Units
3 - 5 Days
Anti-Mitochondrial M2 EP antibodies by ELISA (EIA) add additional sensitivity and specificity to the IFA method. These antibodies react against major M2 components that may be missed on IFA.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Mitochondrial M2 EP Ab
230
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
EIA
83520
<20 Units
10 - 14 Days
These antibodies have a good specificity for sporadic inclusion body myositis (sIBM). This is the first commercially available antibody to aid in the diagnosis of sIBM.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Mup44 (cN1A) Ab

41
88
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83876
0 - 20 Units
1 - 3 Days
Anti-MPO autoantibodies aid in assessment of certain autoimmune vasculitides such as microscopic polyarteritis (MPA), and crescentic glomerulonephritis. MPO is the main target antigen for the antineutrophil cytoplasmic autoantibodies (ANCA) which give a perinuclear (P- ANCA) immunofluorescence pattern. The presence of both P-ANCA and MPO yields a sensitivity of 67% and a specificity of 99% for MPA.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Myeloperoxidase Ab (Anti-MPO)
19
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:10
3 - 5 Days
Myocardial autoantibodies are found in a variety of clinical conditions including Dressler syndrome. The titer also rises in about 66% of patients with coronary artery bypass and need not be related to post cardiotomy syndrome. The antibodies are found in most patients with acute rheumatic fever.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Myocardial Ab
156
Requirements: 1 mL serum or CSF, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
FC
88182
Negative
14 Days
Neurologic and/or psychiatric manifestations occur in up to two thirds of patients with Systemic Lupus Erythematosus (SLE). The cerebral manifestations are extremely diverse, ranging from mild depression to severe, life-threatening presentations. Studies have shown that anti-neuronal antibodies are more frequently found in the blood and CSF of neuropsychiatric lupus erythematosus (NPLE) patients compared to SLE patients without NPLE. Serial testing of of anti-neuronal antibodies appear to correlate well with clinical response to SLE therapy.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Neuronal Ab, IgG
990
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86021
<1:10
1 - 2 Days
C-ANCA & P-ANCA resulted if positive, otherwise, reported as ANCA Negative. P-ANCA confirmed on formalin fixed slides. ANA performed if ANCA is positive to rule out false positive ANCA due to presence of ANAs.
C-ANCA is primarily due to the presence of PR-3 antibodies, while P-ANCA is typically due to the presence of MPO antibodies. C-ANCA is present in up to 90% of active generalized GPA (Granulomatosis with Polyangiitis; previously known as Wegener’s granulomatosis). P-ANCA is a useful marker for MPA (Microscopic Polyangiitis) and Pauciimune Crescentic GN. P-ANCA can also be seen in other connective tissue diseases (SLE, RA, ReA, AS, UC) but it is directed against different intracellular neutrophil cytoplasmic antigens. There are several drugs that have been implicated in ANCA-associated Vasculitis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Neutrophil Cytoplasmic Ab (ANCA)

42
20
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86038 (If Positive, Add 86039)
<1:40, No pattern
1 - 2 Days
Positive ANA includes titer and pattern. This test can also be performed on synovial fluid - please specifiy on the order form, requesting test #205.
ANA are commonly found in a variety of autoimmune diseases. They can also be detected in first degree relatives of patient’s with autoimmune disorders and found in smaller frequency in healthy controls. Antibody frequency can increase with age. ANA patterns on Hep-2 slides provide only general clues about particles (chromatin, nucleosomes, and spliceosomes). ANA patterns (other than centromere pattern) are not reliably correlated with the presence of specific antibodies and must be further evaluated by EIA using individual ENA antigens.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Nuclear Ab (ANA)
205
Requirements: 1 mL body fluid, ambient, refrigerated or frozen IFA
86038 (If Positive, Add 86039)
<1:10, No pattern
1 - 2 Days
Positive ANA includes titer and pattern.
ANA are commonly found in a variety of autoimmune diseases. They can also be detected in first degree relatives of patient’s with autoimmune disorders and found in smaller frequency in healthy controls. Antibody frequency can increase with age. ANA patterns on Hep-2 slides provide only general clues about particles (chromatin, nucleosomes, and spliceosomes). ANA patterns (other than centromere pattern) are not reliably correlated with the presence of specific antibodies and must be further evaluated by EIA using individual ENA antigens.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Nuclear Ab (ANA), Body Fluid
287
Requirements: 2 mL serum, ambient, refrigerated or frozen IFA
86038 (If Positive, Add 86039)
<1:1, No Pattern
1 - 2 Days
ANA are commonly found in a variety of autoimmune diseases. They can also be detected in first degree relatives of patient’s with autoimmune disorders and found in smaller frequency in healthy controls. Antibody frequency can increase with age. ANA patterns on Hep-2 slides provide only general clues about particles (chromatin, nucleosomes, and spliceosomes). ANA patterns (other than centromere pattern) are not reliably correlated with the presence of specific antibodies and must be further evaluated by EIA using individual ENA antigens.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Nuclear Ab, CSF
174
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
EIA
83520
<20
10 - 14 Days
Anti-NXP-2 antibodies are present in 2-30% of adult DM and 18-25% of JDM. In JDM they are associated with cutaneous calcinosis cutis. In adult DM they are significantly associated with the presence of cancer (cancer was found in 13.6% of Anti-NXP-2 positive DM patients).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-NXP-2 (MJ) (part of P140 kD)

43
55
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:4
2 - 4 Days
Anti-ovary antibodies are present in 78% of patients with premature ovarian failure and Addisons disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Ovary Ab
645
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86255
Negative
3 - 5 Days
PAB has 90% specificity and 30% sensitivity for Crohn’s Disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Pancreatic Ab
21
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:20
2 - 4 Days
Studies show a high frequency (90-100%) of parietal cell antibodies (PCA) in pernicious anemia (PA), although the frequency decreases (55%) in younger patients. Explanations for the seronegative cases in pernicious anemia patients include: A) juvenile PC prior to the development of autoantibodies, B) an immunological reaction restricted to a cellular response rather than antibody response, C) exhaustion of autoimmune response as the parietal cell antibodies are developed, D) incorrect diagnosis, E) unrecognized antibodies directed towards highly sensitive epitomes.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Parietal Cell Ab
1888
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86148 x 3
IgG: <11 GPS, IgA: <20 APS, IgM: <25 MPS U/mL
2 - 4 Days
Anti-phosphatidylserine (aPS) antibodies IgG and IgM are associated with both arterial and venous thrombosis, as well as obstetric complications. The combination of aPS and anti-B2GPI is a very strong predictor for secondary APS in SLE. IgA aPS antibodies correlate with migraine headaches in SLE. These antibodies can be found in 5-10% of “Seronegative APS.”
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Phosphatidylserine Abs, IgG, IgA & IgM
44
531
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<30 Units
5-7 Days
aPS/PT antibodies have a stronger correlation with LAC activity than aCL and B2GPI antibodies and can therefore serve as a confirmatory test for the presence of true LAC, even while on anticoagulation therapy. However, they should not be viewed as a complete replacement for LAC (48%-92% of LAC patients will be positive for aPS/PT IgM and/or IgG). Studies confirm that IgG/IgM aPS/PT antibodies are independent risk factors for venous thromboses, arterial thrombosis and obstetric abnormalities. The presence of both IgG aPS/PT and/or IgM aPS/PT has a sensitivity of 52% and specificity of 86% to 92% for APS. These antibodies can be found in 5-10% of “Seronegative APS”.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-phosphatidylserine/prothrombin antibodies (aPS/PT) Abs, IgG & IgM
69
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
3 - 5 Days
Found in 10% of idiopathic inflammatory myopathy, 25% of Scleroderma/myositis overlap and 2% of Scleroderma. The antibodies are associated with myositis, arthritis, Raynaud’s, Scleroderma cutaneous changes and ILD.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-PM/Scl Ab
73
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86255
Negative
3 - 5 Days
Anti-proliferating cell nuclear antibodies (PCNA) are found in <10% of SLE patients. The presence of PCNA is associated with renal, CNS involvement and thrombocytopenia in SLE; PCNA titers are elevated prior to development of proteinuria and decrease following corticosteroid treatment.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Proliferating Cell Nuclear Ab (Anti-PCNA)
89
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
0 - 20 Units
1 - 3 Days
PR-3 antibodies aid in the assessment of certain autoimmune vasculitides such as microscopic polyarteritis and crescentic glomerulonephritis. PR-3 is the major target antigen of antineutrophil cytoplasmic autoantibodies (ANCA) that give a cytoplasmic (C-ANCA) immunofluorescence pattern. The presence of both C-ANCA and PR3 antibodies yields a sensitivity of 73% and a specificity of 99% for GPA (Granulomatosis with Polyangiitis; previously known as Wegener’s granulomatosis).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Proteinase 3 Ab (PR-3)

45
572
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<20 Units
3 - 5 Days
Ribosomal P antibodies are highly specific for SLE (99%) occurring in 6-46% of SLE patients depending on ethnicity. They are associated with renal and hepatic involvement in SLE and are more prevalent in juvenile-onset SLE. Some studies show that up to 90% of patients with lupus psychosis test positive for Ribosomal P antibodies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Ribosomal P Protein Ab
449
Requirements: 1 mL serum, ambient for 2 days, refrigerated or frozen EIA
83520
<20 Units
2 - 5 Days
The detection of anti-RNAP III antibodies is useful in the diagnosis of SSc and for the identification of patients at risk for developing progressive skin thickening, cancer and renal crisis. The prevalence of IgG RNAP III antibodies is from 9-35% in SSc patients.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-RNA Polymerase III IgG Ab
574
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
1 - 3 Days
Anti-U1snRNP antibodies typically appear in both SLE and MCTD. In MCTD, the presence of high titer U1snRNP without other antibodies is required for diagnosis, whereas, anti-snRNP antibodies occur in only 30% of SLE. Anti-RNP antibody activity in SLE often accompanies anti-Sm antibodies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-RNP Ab (U1 snRNP)
570
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
1 - 3 Days
Anti-Ro (SS-A) antibodies occur in 30% of SLE, 60-75% of primary Sjogren’s syndrome (PSS), >90% of subacute cutaneous lupus and vasculitis-associated SS. SS-A can also be found in lesser frequency in secondary SS associated with disease such as SLE, RA, PSS, myositis, or primary biliary cirrhosis. Circulating SS-A or SS-B antibodies in the mother can cause neonatal congenital heart block.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Ro Ab (SS-A)

46
715
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235 x 2
<20 Units
1 - 3 Days
The association of anti-Ro and Anti-La antibodies with symptoms of dry eyes, xerostomia and a positive Rose Bengal staining or Schirmer test, has a sensitivity and specificity of >90% for primary Sjogren’s syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Ro Ab (SS-A) & Anti-La Ab (SS-B) – Sjogren’s
644
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520 x 2
<20 Units
3 - 5 Days
ASCA aid in the diagnosis of patients with Crohn’s disease. They are also more prevalent in psoriasis and psoriatic arthritis. IgA antibodies should be used to complement but not to replace or to substitute for ASCA IgG antibody testing.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Saccharomyces Cerevisiae Ab, IgA & IgG (ASCA)
577
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
2 - 4 Days
If positive, reflexes to Immunodiffusion for confirmation, please add two days to turn around time.
Anti-Scl-70 antibodies are highly specific for scleroderma. They are present in about 20% of diffuse SSC and 10% of limited SSC. The antibodies are associate with digital ulcers, Raynauds, pulmonary fibrosis, renal crises and heart disease. EIA testing can yield false positive results, therefore, all EIA positive tests are confirmed with immunodiffusion.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Scl-70 Ab
57
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:10
2 - 4 Days
Skin antibodies are highly specific in patients with Pemphigus vulgaris and P. foliaceus. The titers correlate with disease activity and may be used to monitor therapy. Skin antibodies (inter-epithelial) are found in 90% of patients with Pemphigus vulgaris and P. foliaceus. Dermal-epidermal skin antibodies are found in 90% of patients with Bullous pemphigoid and 90% of Cicatricial pemphigoid.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Skin Ab, Pemphigus & Pemphigoid
47
579
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
1 - 3 Days
Anti-Sm antibodies offer a highly specific but relatively insensitive marker of SLE. Their overall prevalence ranges from approximately 20-30% in SLE. Anti-Sm reactivity is not described definitively in other diseases, although a few studies found SM antibodies in monoclonal gammopathies and uveitis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Sm Ab
30
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:20
1 - 3 Days
Smooth muscle antibodies (SMA) are classic serologic markers of autoimmune hepatitis (AIH) type 1. High titer SMA have a specificity of 96% with a sensitivity of 16%. Anti-Actin IgG is a type of smooth muscle antibody and has greater sensitivity and specificity for AIH type 1.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Smooth Muscle Ab
126
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
83520
<=20.0 Units
3 - 5 Days
Anti-SLA antibodies are highly specific for autoimmune hepatitis type 1, with a sensitivity of 10-30%. They can also be seen in autoimmune hepatitis type 2.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Soluble Liver Ag Ab
1602
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520
<=20.0 Units
4 - 7 Days
Primary Biliary Cirrhosis (PBC) is an organ-specific autoimmune disease characterized by chronic progressive destruction of intrahepatic bile ducts with portal inflammation resulting in chronic cholestasis and ultimately fibrosis. Serologic assays are important tools for the recognition and diagnosis of PBC, since many antibodies associated with PBC can be present years before symptoms become evident. Sp100 has a sensitivity of 21-39% and a specificity of 99% for PBC. Sp100, along with Gp210 can detect up to 70% of AMA negative PBC patients.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Sp-100 Ab
48
1252
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
86235
<20 Units
5 days
Anti-SS-A 52 kD antibodies have been reported in a variety of autoimmune diseases such as IIM, SLE, SS, SSc, PBC, AIH, MCTD and other overlap syndromes. They are found in about 30% of IIM; 27% of Anti-MDA5 positive patients; 40-58% of Anti-JO-1 positive patients. They are highly associated with ILD and are possibly associated with paraneoplastic syndromes.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-SS-A 52 kD Ab, IgG
311
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
86060
0 -250 UI/mL
1 - 3 Days
A marked rise in titer or a persistently elevated titer indicates that a Streptococcus infection or poststreptococcal sequelae are present. Increased ASO levels are observed in approximately 85% of the cases of rheumatic fever or pharyngitis associated with group A beta-hemolytic streptococcal infection. ASO titers rise as early as 1 week post onset and peak at 3-5 weeks. Values typically return to normal levels within 6- 12 months, with or without treatment.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Streptolysin O Ab, (ASO)
28
Requirements: 1 mL serum, ambient, refrigerated or frozen IFA
86256
<1:10
2 - 4 Days
Anti–striated muscle antibodies are present in about 80% of younger (<40 years old) myasthenia gravis (MG) patients who also have a thymoma, and are seen less frequently in MG patients without a thymoma.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Striated Muscle Ab
106
Requirements: 2 frozen plastic vials plasma,1 mL each, from sodium citrated (blue top) tubes
COAG
85300
75.6 - 122.4 % Activity
2 - 4 Days
Draw in sodium citrated (blue top) tubes. Mix by inverting 10 times. Check for fibrin clots using wooden applicator sticks. Clotted specimen is unsatisfactory. Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (by overnight express mail if out of the greater Los Angeles area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Please specify on the tubes if serum or plasma.
Low levels of antithrombin III activity are associated with an increased risk of thrombosis. Acquired deficiencies frequently occur due to consumption in DIC, following major operations, in cases of nephrosis, in liver disease and in contraceptive use with estrogen. Antithrombin III function deficiency can cause heparin resistance.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Antithrombin III Function (Activity)

49
1332
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86800
<60 U/mL
1 - 3 Days
Autoantibodies to thyroglobulin (TG) are often persent in patients with autoimmune thyroid disease. Approximately 5% of healthy individuals have TG autoantibodies at low levels; higher concentrations are found in 30% and 70% of patients with Graves’ disease and Hashimoto’s thyroiditis, respectively. Elevated levels of antibodies to thyroid peroxidase (TPO autoantibodies) occur more frequently than high anti-TG levels in these diseases.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Thyroglobulin Ab (TG)
1333
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86376
<60 U/mL
1 - 3 Days
Anti-TPO antibodies are the most common anti-thyroid autoantibody, present in about 90% of Hashimoto’s thyroiditis and 75% of Graves’ disease. 10-15% of normal individuals can have high levels of TPO antibodies, particularly if family members have an autoimmune thyroid disease. They can be infrequently found in thyroid carcinomas. Anti-TPO antibodies are present in 99% of cases where thyroglobulin antibodies are present, however only 35% of anti-TPO antibody positive cases also test positive for thyroglobulin antibodies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-Thyroid Microsomal Peroxidase Ab (TPO)
175
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
EIA
83520
<20
10 - 14 Days
Present in 15-38% of adult DM and 20-30% in JDM. Highly associated with malignancy which is found in 50-75% of positive adults patients; 89% specificity and 78% sensitivity for diagnosing cancer-associated DM; no cancer association in children.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Anti-TIF-1γ (P155/140 kD)
145
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86332
<4.4 uG Eq/mL
2 - 5 Days
Serum concentrations of C1q binding CIC by ELISA correlate with disease activity in SLE patients, especially with hypocomplementemia.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C1Q Circulating Immune Complex (C1Q CIC)

50
450
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
86160
87 - 200 mg/dl
1 - 3 Days
Measurement of C3 is used to detect an inborn deficiency of this factor or those with immunologic diseases in which complement is consumed at increased rates. These include lupus erythematosus, chronic active hepatitis, certain chronic infections, post streptococcal and membranoproliferative glomerulonephritis, etc.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C3 Complement
320
Requirements: 1 mL body fluid from red top tube, ambient, refrigerated or frozen. Should be tested along with serum sample.
TURB
86160
33% - 50% of patient’s serum C3 Complement level
1 - 3 Days
Measurement of C3 is used to detect an inborn deficiency of this factor or those with immunologic diseases in which complement is consumed at increased rates. These include lupus erythematosus, chronic active hepatitis, certain chronic infections, post streptococcal and membranoproliferative glomerulonephritis, etc.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C3 Complement, Body Fluid
460
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
86160
19 - 52 mg/dL
1 - 3 Days
Measurement of C4 is used to detect an inborn deficiency of this factor or those with immunologic diseases in which complement is consumed at increased rates. These include lupus erythematosus, chronic active hepatitis, certain chronic infections, post streptococcal and membranoproliferative glomerulonephritis, etc.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C4 Complement
322
Requirements: 1 mL body fluid from red top tube, ambient, refrigerated or frozen. Should be tested along with serum sample.
TURB
86160
33% - 50% of patient’s serum C4 Complement level
1 - 3 Days
Measurement of C4 is used to detect an inborn deficiency of this factor or those with immunologic diseases in which complement is consumed at increased rates. These include lupus erythematosus, chronic active hepatitis, certain chronic infections, post streptococcal and membranoproliferative glomerulonephritis, etc.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C4 Complement, Body Fluid

51
641
Requirements: One EDTA (lavender top) tube whole blood at room temperature FC
86355
CD19%: 6 - 25%; CD19 Absolute: 90 - 660 cumm
2 - 4 Days
Do not spin, separate or refrigerate. Send by overnight express mail.
B activation/differentiation cells share CD19 and CD20 markers. Studies of the roles played by B cells and B cell depletion in autoimmune diseases have suggested that B cells contribute to the expression of autoimmunity and that antibodies targeting B cells (such as anti-CD20) may substantially suppress autoimmune disease. Our CD19 Detection assay is useful in monitoring the effectiveness of rituximab (anti-CD20 antibody) on B cell depletion.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
CD19 Detection
632
Requirements: One EDTA (lavender top) tube whole blood at room temperature FC
86355
CD20%: 5 - 26%, CD20 Absolute: 50 - 600 cumm
2 - 4 Days
Do not spin, separate or refrigerate. Send by overnight express mail.
B activation/differentiation cells share CD19 and CD20 markers. Studies of the roles played by B cells and B cell depletion in autoimmune diseases have suggested that B cells contribute to the expression of autoimmunity and that antibodies targeting B cells (such as anti-CD20) may substantially suppress autoimmune disease. Our CD20 Detection assay is useful in monitoring the effectiveness of rituximab (anti-CD20 antibody) on B cell depletion.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
CD20 Detection
626
Requirements: One EDTA (lavender top) tube whole blood at room temperature FC
86361
CD4%: 31-60%, CD4 Absolute: 410-1590 cumm
1 - 2 Days
Do not spin, separate or refrigerate. Send by overnight express mail.
Measures the CD4 Helper T-lymphocyte population.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
CD4 – Helper/Inducer Count
548
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
82390
18 - 58 mg/dL
2 - 5 Days
Measurement of ceruloplasmin aids in the diagnosis of copper metabolism disorders, such as Wilson’s disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Ceruloplasmin

52
323
Requirements: 1 mL serum, ambient, refrigerated or frozen ID
86635
NEGATIVE
4 - 6 Days
Coccidioidomycosis is a common fungal infection in the southwestern United States, increasing in incidence over the last decade. It is endemic to the San Joaquin Valley of California, southern Arizona, southern New Mexico, western Texas, and areas of Mexico as well as Central and South America. There have been numerous case reports of coccidioidomycosis in patients on TNF-alpha antagonists. One study showed that in endemic areas, patients with inflammatory arthritis who were undergoing anti-TNF-alpha treatment had a RR of 5.23, 95% CI 1.54-17.71 (P< 0.01) of developing symptomatic coccidioidomycosis as compared to those not on anti-TNF-alpha therapy.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Coccidioidomycosis, IgG & IgM
34
Requirements: One red top tube. DHA
86157
<1:64
3 - 5 Days
Do not use serum separator or barrier tube. Allow specimen to clot at +37 degrees C for 30 minutes. Centrifuge and separate serum immediately. After treatment, specimen can be refrigerated. Send by overnight express mail.
Cold agglutinins are autoantibodies that cause red blood cell clumping in low temperatures. They can be seen in some infections such as mycoplasma pneumonia, EBV and HIV. Lymphomas can produce cold agglutinins as well. Usually cold agglutinins do not cause clinical symptoms, however rarely they can cause tissue gangrene or autoimmune hemolytic anemia. Symptoms can be managed by warming the core temperature of the body to over 37° C.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Cold Agglutinins
314
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
86140
<1 mg/dL
1 - 3 Days
Measurements of CRP can aid in monitoring inflammatory states caused by autoimmune disease, infections, surgery or neoplasms. Elevated CRP levels predict erosions in Rheumatoid Arthritis and progression of disease in Ankylosing Spondylitis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
C-Reactive Protein (CRP)
340
Requirements: 1 mL serum, frozen COL
82550
30 - 223 U/L
1 - 3 Days
The specimen must be frozen within 24 hours. Send on dry ice by overnight express mail.
Measurements of total creatine kinase are used in the investigation of skeletal muscle disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Creatine Kinase (CPK)

53
1380
Requirements: One red top tube. Do not use SST or barrier tube. MAC
82595
Negative
2 - 8 Days
Immediately after collection, place into a water bath at 37 degrees C for 1 hour. Centrifuge and separate immediately, while still warm. Mark tube “Treated for Cryo”. Please note date and time of collection. Send by overnight express mail. Untreated whole blood cannot be accepted. Please Note: Cryos have to be read for 6 days to assure positivity. If it turns positive on the 6th day, 2 more days are needed to result it.
Cryoglobulinaemia is usually classified into three subgroups: type I is composed of single monoclonal immunoglobulins and is associated with lymphoproliferative disorders. Type II and III are composed of polyclonal IgG with either monoclonal IgM RF (type II) or polyclonal IgM RF (type III), and are associated with viral, bacterial or parastitic infections, especially Hepatitis C. Autoimmune diseases can be associated with both, Type II and III, but are more prevalent with type III.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Cryoglobulins
760
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86644
<=0.90 REV
3 - 5 Days
Seroprevalence for CMV infection worldwide ranges from about 60%-100%. Serologic studies indicating an acute CMV infection include the presence of positive IgM anti-CMV antibodies or a significant increase in the titer of IgG anti-CMV antibodies. CMV IgG antibodies will persist chronically post infection. CMV can cause severe disease in immunocompromised patients resulting in encephalitis, pneumonitis, hepatitis, uveitis, retinitis, colitis and graft rejection. In immunocompetent patients, primary CMV usually presents with a typical viral syndrome or a mononucleosis-like syndrome. However, there are case reports of severe illness from CMV in immunocompetent patients as well.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Cytomegalovirus (CMV) Ab, IgG
761
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86645
<=0.90 REV
3 - 5 Days
Seroprevalence for CMV infection worldwide ranges from about 60%-100%. Serologic studies indicating an acute CMV infection include the presence of positive IgM anti-CMV antibodies or a significant increase in the titer of IgG anti-CMV antibodies. CMV IgG antibodies will persist chronically post infection. CMV can cause severe disease in immunocompromised patients resulting in encephalitis, pneumonitis, hepatitis, uveitis, retinitis, colitis and graft rejection. In immunocompetent patients, primary CMV usually presents with a typical viral syndrome or a mononucleosis-like syndrome. However, there are case reports of severe illness from CMV in immunocompetent patients as well.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Cytomegalovirus (CMV) Ab, IgM
716
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86644, 86645
<=0.90 REV
3 - 5 Days
Seroprevalence for CMV infection worldwide ranges from about 60%-100%. Serologic studies indicating an acute CMV infection include the presence of positive IgM anti-CMV antibodies or a significant increase in the titer of IgG anti-CMV antibodies. CMV IgG antibodies will persist chronically post infection. CMV can cause severe disease in immunocompromised patients resulting in encephalitis, pneumonitis, hepatitis, uveitis, retinitis, colitis and graft rejection. In immunocompetent patients, primary CMV usually presents with a typical viral syndrome or a mononucleosis-like syndrome. However, there are case reports of severe illness from CMV in immunocompetent patients as well.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Cytomegalovirus (CMV), IgG & IgM

54
276
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-histidyl-tRNA synthetase autoantibodies are the most common Myositis Specific Antibodies, comprising 30-40% of Idiopathic Inflammatory Myopathies (IIM), although EJ specifically is seen in less than 5% of IIM. Anti-Synthetase antibodies can be found in polymyositis, dermatomyositis or overlap myositis. Symptoms associated with these antibodies include non-erosive arthritis, ILD, fever, mechanic’s hands and Raynaud’s.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
EJ
617
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86664
<=0.90 OD Ratio
3 - 5 Days
EBNA-1 IgG ELISA test system provides a means for the qualitative detection of IgG antibodies to the nuclear antigen-1 of Epstein-Barr virus (EBNA-1). Antibodies to EBNA are not seen in the acute phase of an EBV infection. These antibodies slowly appear 2 to 4 months after the onset of symptoms and persist indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Epstein Barr Nuclear Ag (EBNA) Ab, IgG
619
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86665
<=0.90 OD Ratio
3 - 5 Days
Anti-VCA IgG antibodies appear in the acute phase of an EBV infection, peak at 2 to 4 weeks after onset, decline slightly then persist indefinitely. Anti-VCA IgM antibodies appear early in an EBV infection and usually disappear within 4 to 6 weeks.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Epstein Barr Viral Capsid Ag (VCA) Ab, IgG
620
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86665
<=0.90 OD Ratio
3 - 5 Days
Anti-VCA IgM antibodies appear early in an EBV infection and usually disappear within 4 to 6 weeks. Anti-VCA IgG antibodies appear in the acute phase of an EBV infection, peak at 2 to 4 weeks after onset, decline slightly then persist indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Epstein Barr Viral Capsid Ag (VCA) Ab, IgM
55
618
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86665 x 2
<=0.90 OD Ratio
3 - 5 Days
Anti-VCA IgM antibodies appear early in an EBV infection and usually disappear within 4 to 6 weeks. Anti-VCA IgG antibodies appear in the acute phase of an EBV infection, peak at 2 to 4 weeks after onset, decline slightly then persist indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Epstein Barr Viral Capsid Ag (VCA) Abs, IgG & IgM
621
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86663
<=0.90 OD Ratio
3 - 5 Days
Anti-EA antibodies appear in the acute phase of an EBV infection and disappear after 3 to 6 months. The presence of antibodies to EA usually means an active infection, however, 20% of EA positivity will persist for years.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Epstein Barr Virus, Early Antigen (EA) Ab
1634
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
82728
Male Range: 22 - 322 ng/mL; Female Range: 10 - 291 ng/mL
2 - 4 Days
Ferritin is a major intracellular iron storage protein and reflects on biologically available iron stores. In addition, hyperferritinemia is associated with several inflammatory conditions such as sepsis, SIRS, macrophage activating syndrome, Still’s disease and catastrophic antiphospholipid syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Ferritin, Serum
232
Requirements: 1 mL serum, ambient, refrigerated or frozen RIPA
83516
Negative
10 - 14 Days
Anti-Fibrillarin (U3 RNP) antibodies are highly specific for diffuse SSc with a sensitivity of 4-10%. They are associated with isolated pulmonary arterial hypertension, myositis, renal and cardiac manifestations of SSc.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Fibrillarin (U3 RNP)
56
1345
Requirements: 2 frozen plastic vials plasma, 1 mL each, from 2 sodium citrated (blue top) tubes
COAG
85384
308 - 613 mg/dL
2 - 4 Days
Draw in sodium citrated (blue top) tubes. Mix by inverting 10 times. Check for fibrin clots using wooden applicator sticks. Clotted specimen is unsatisfactory. Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (by overnight express mail if out of the greater Los Angeles area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Please specify on the tubes if serum or plasma.
Fibrinogen is an acute phase reactant that can be elevated in numerous inflammatory conditions. It is also a risk factor for cardiovascular disease. Low fibrinogen levels can be seen in consumptive processes such as DIC, MAC (macrophage activating syndrome) and inherited deficiencies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Fibrinogen
241
Requirements: 1 mL serum, ambient (2 days), refrigerated (5 days) and frozen (6 months)
IFA
86780
Non-Reactive
7 Days
Comfirmatory test for syphilis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
FTA – Fluorescent Treponemal Ab, Absorbed
668
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
83010
44 - 215 mg/dL
2 - 5 Days
Haptoglobin may be low in hemolytic diseases related to the formation of hemoglobin-haptoglobin complexes, as well as certain liver diseases. Haptoglobin is also an acute-phase reactant that can be elevated in numerous inflammatory conditions.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Haptoglobin
1722
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86708
Negative
2 - 4 Days
Anti-HAV IgG antibodies are indicative of a past infection and can persist for years after viral clearance.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis A Virus Ab (HAV), IgG

57
721
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86708, 86709
Negative
2 - 4 Days
Anti-HAV IgM antibodies appear 2-6 weeks after exposure and usually disappear within 6 months. Anti-HAV IgG antibodies are indicative of a past infection and can persist for years after viral clearance.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis A Virus Ab (HAV), IgG & IgM
1721
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86709
Negative
2 - 4 Days
During an acute phase of a HAV infection, IgM antibodies to the hepatitis A virus (anti-HAV IgM) appear in the patient’s serum 2-6 weeks after exposure and usually disappear within 6 months.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis A Virus Ab (HAV), IgM
1723
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86705
Negative
2 - 4 Days
Aids in the diagnosis of acute or recent (usually six months or less) hepatitis B viral infection.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Core Ab (HBc), IgM
1724
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86704
Negative
2 - 4 Days
Anti-HBV core antibodies appear at the onset of symptoms and persist lifelong. Their presence indicates a previous or ongoing infection in an undefined time frame.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Core Ab (HBc), Total

58
723
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86704, 86705
Negative
2 - 4 Days
Total anti-HBc (both IgM and IgG antibodies) are detected at the onset of symptoms. Anti-HBc IgM indicates an acute or recent infection (within 6 months). Anti-HBc IgG indicates an ongoing or previous infection and will persist indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Core Abs (HBc), Total & IgM
725
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
86706
Negative
2 - 4 Days
Presence of hepatitis B surface antibodies indicate recovery from an infection and immunity to the virus. Anti-HBs antibodies also develop after a successful vaccination against hepatitis B.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Surface Ab (HBsAb), Qualitative
726
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
87340
Negative
2 - 4 Days
If positive, reflexes to HBsAg Neutralization, Confirmation.
Presence of HBsAg indicates an acute or chronic active infection.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Surface Antigen (HBsAg)
727
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
87341
Negative
2 - 4 Days
Presence of HBsAg indicates an acute or chronic active infection.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis B Surface Antigen (HBsAg), Neutralization-Confirmation

59
730
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86803
Negative
2 - 4 Days
The Hepatitis Signal to Cutoff Ratio test is performed if the HCV is positive.
At least 170 million individuals worldwide are chronically infected with HCV. HCV infection is often asymptomatic, however, the majority (over 55-85%) of the individuals exposed to HCV become chronically infected. In 20% of these chronically infected individuals, the disease progresses to cirrhosis, liver failure, and possibly hepatocellular carcinoma or cholangiocarcinoma. Common modes of HCV transmission include blood transfusion, intravenous drug use, nosocomial exposure, during assisted reproductive techniques, and from mother-to-infant during pregnancy, delivery, or the postpartum period. A positive EIA HCV result should be confirmed with PCR testing. If the PCR is negative, then the patient either had a previous infection which cleared (spontaneously or with treatment) or there was an error in the EIA testing. A positive PCR confirms the HCV infection.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Hepatitis C Virus Ab (HCV), IgG
90
Requirements: One EDTA (lavender top) tube at room temperature Do not spin, separate or refrigerate.
FC
86812
Negative
1 - 3 Days
Do not spin, separate or refrigerate.
There is a strong association between the presence of the HLA-B27 antigen and an increased incidence of ankylosing spondylitis (AS), as well as several other disorders such as reactive arthritis, uveitis, JIA, psoriatic arthritis, and arthropathies associated with imflammatory bowel disease.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
HLA-B27
404
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
82784
66 - 433 mg/dL
1 - 3 Days
Measurement of immunoglobulin A aids in the diagnosis of abnormal protein metabolism, congenital deficiency and the body’s lack of ability to resist infectious agents.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
IgA, Immunoglobulin A
403
Requirements: 1 mL serum, ambient, refrigerated or frozen TURM
82784
635 - 1741 mg/dL
1 - 3 Days
The measurement of gammaglobulin in serum and other body fluids aids in the diagnosis of autoimmune diseases, sarcoidosis, chronic liver disease, chronic and recurrent infections, lymphoid malignancies, multiple myeloma and severe combined and variable immunodeficiencies.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
IgG, Immunoglobulin G

60
405
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
82784
45 - 281 mg/dL
1 - 3 Days
Measurement of immunoglobulin M aids in the diagnosis of abnormal protein metabolism, congenital deficiency, hyper IgM syndrome and the body’s lack of ability to resist infectious agents.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
IgM, Immunoglobulin M
115
Requirements: 1 mL serum, ambient, refrigerated or frozen EL
86334
Normal
3 - 5 Days
Immunofixation is used most frequently for the identification of monoclonal immunoglobulins.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Immunofixation Electrophoresis (IFE)
279
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Found in about 20% of IIM; associated with overlap syndromes such as PM/SSc (most common), SLE/PM and other autoimmune disorders such as PM, SS, SSc, SLE, UCTD, MCTD, RA; common clinical features include arthralgias/arthritis, myositis, Raynaud’s, esophageal dysmotility and ILD.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Ku
116
Requirements: 2 frozen plastic vials plasma, 1 mL each, from sodium citrated (blue top) tubes
DVVT
85613
<1.2 LAC Ratio
2 - 3 Days
Draw in sodium citrated (blue top) tubes. Mix by inverting 10 times. Check for fibrin clots using wooden applicator sticks. Clotted specimen is unsatisfactory. Centrifuge immediately for 15 minutes at 1500g. Pour into red top tube and centrifuge a second time. Do not let whole blood sit at room temperature for more than 20 minutes before centrifugation. Transfer plasma to two plastic vials, 1 mL each. Mark tube accordingly. Freeze immediately. Plasma must be separated from the red cells before freezing. Specimen must remain frozen throughout transport and shipped on dry ice (by overnight express mail if out of the greater Los Angeles area). For convenience, separated & spun serum for other tests can be frozen and sent along with the frozen plasma. Please specify on the tubes if serum or plasma.
The presence of lupus anticoagulant can cause hypercoagulable states, fetal loss and other manifestations of antiphospholipid antibody syndrome. Due to its heterogeneous nature, no single assay can absolutely identify the presence of LA.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Lupus Anticoagulant (LA)

61
764
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86618
Negative
3 - 7 Days
C6 peptide EIA has good sensitivity (>90%) and specificity, reacts with B. burgdorferi and other Borrelia spp. and is useful in patients who have been vaccinated with OspA Lyme vaccine for Lyme disease. In contrast to C6 EIA, all other Lyme antibody tests use either a sonicated or whole B. burgdorferi cell perparation as capture antigens and will be positive in vaccinated patients because of the strong OspA antibody reactions that are not common in Lyme disease with erythema migrans.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Lyme C6 Peptide Ag
710
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA, WB
86618, 86617 x 2
Negative
3 - 5 Days
The EIA results should only be used for patients with signs and symptoms that are consistent with Lyme disease. Equivocal or positive results must be confirmed by a standardized Western Blot procedure. Patients tested within the first few weeks of illness (<4wks) will often test negative, however, patients who have Lyme disease for longer than 4-6 weeks will almost always test positive. The CDC recommends a two-tiered testing system for Lyme disease. The first test should be EIA (or IFA), followed by Western Blot if the EIA is positive or equivocal.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Lyme Disease, EIA, Reflexive to Western Blot
792
Requirements: 2 mL serum, ambient, refrigerated or frozen WB
86617 x 2
Negative
3 - 5 Days
The Western Blot is useful for characterizing the specificity of the antibody response to B. burgdorferi. The Western Blot has greater specificity than either the IFA or EIA procedures. The CDC recommends a two-tiered testing system for Lyme disease. The first test should be EIA (or IFA), followed by Western Blot if the EIA is positive or equivocal.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Lyme Disease, Western Blot, IgG & IgM
237
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-Mi-2 antibodies are found in 10-20% of adult dermatomyositis (DM) and <10% of JDM. They are associated with classic DM features: mild to moderate weakness with shawl rash, heliotrope rash, V-sign, Gottron’s papules and have a good response to therapy, with lower incidence of cancer compared to Mi-2 negative DM.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
MI-2

62
277
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-histidyl-tRNA synthetase autoantibodies are the most common MSA, comprising 30-40% of Idiopathic Inflammatory Myopathies (IIM), although OJ specifically is seen in less than 5% of IIM. Anti-Synthetase antibodies can be found in polymyositis, dermatomyositis or overlap myositis. Symptoms associated with these antibodies include non-erosive arthritis, ILD, fever, mechanic’s hands and Raynaud’s.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
OJ
2747
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86747
<0.9 I.V.
3 - 7 Days
Equivocal results are 0.8 - 1.2 I.V. Positive results are >1.2 I.V.
In adults, parvovirus B19 infection can be associated with arthritis/arthropathy, transient aplastic crisis, and rarely myocarditis, vasculitis, glomerulonephritis, encephalitis, ITP, HSP and HLH. IgG antibodies appear at 2 weeks and last indefinitely, while IgM antibodies are detected 10-12 days after inoculation and remain for months.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Parvovirus B-19 Ab, IgG
2748
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86747
<0.9 I.V.
3 - 7 Days
Equivocal results are 0.8 - 1.2 I.V. Positive results are >1.2 I.V.
In adults, parvovirus B19 infection can be associated with arthritis/arthropathy, transient aplastic crisis, and rarely myocarditis, vasculitis, glomerulonephritis, encephalitis, ITP, HSP and HLH. IgM antibodies are detected 10-12 days after inoculation and remain for months, while IgG antibodies appear at 2 weeks and last indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Parvovirus B-19 Ab, IgM
748
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
86747 x 2
<0.9. I.V.
3 - 7 Days
Equivocal results are 0.8 - 1.2 I.V. Positive results are >1.2 I.V.
In adults, parvovirus B19 infection can be associated with arthritis/arthropathy, transient aplastic crisis, and rarely myocarditis, vasculitis, glomerulonephritis, encephalitis, ITP, HSP and HLH. IgM antibodies are detected 10-12 days after inoculation and remain for months, while IgG antibodies appear at 2 weeks and last indefinitely.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Parvovirus B-19 Abs, IgG & IgM

63
239
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-histidyl-tRNA synthetase autoantibodies are the most common MSA, comprising 30-40% of Idiopathic Inflammatory Myopathies (IIM), although PL-12 specifically is seen in less than 5% of IIM. Anti-Synthetase antibodies can be found in polymyositis, dermatomyositis or overlap myositis. Symptoms associated with these antibodies include non-erosive arthritis, ILD, fever, mechanic’s hands and Raynaud’s.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
PL-12
238
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-histidyl-tRNA synthetase autoantibodies are the most common MSA, comprising 30-40% of Idiopathic Inflammatory Myopathies (IIM), although PL-7 specifically is seen in less than 5% of IIM. Anti-Synthetase antibodies can be found in polymyositis, dermatomyositis or overlap myositis. Symptoms associated with these antibodies include non-erosive arthritis, ILD, fever, mechanic’s hands and Raynaud’s.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
PL-7
113
Requirements: 2 mL serum, ambient, refrigerated or frozen EL
84165, 84155
Normal
2 - 6 Days
Please note: SPE is reflexive. 1) Monoclonal spike ->IFE & QIG. 2) Hypogammaglobulin -> QIG. If the SPE reflexes, the turn around time could be 6 days.
SPE is useful in the evaluation of myeloma, macroglobulinemia of Waldenstrom, collagen disease, monoclonal gammopathies, inflammatory states, low back pain, arthritis, amyloidosis, lymphoma, leukemia and anemia.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Protein Electrophoresis, Serum (SPE) – Reflexive
400
Requirements: 2 mL serum, ambient, refrigerated or frozen TURB
82784 x 3
IgG: 635-1741, IgA:66-433, IgM: 45-281 mg/dL
1 - 3 Days
Quantitation of serum immunoglobulins (IgG, IgA, and IgM) provide useful information for the evaluation of certain disease states. Increased concentrations of these proteins may occur in disorders such as monoclonal or polyclonal gammopathies. Decreased concentrations of immunoglobulins may indicate hypogammaglobulinemia as a result of primary or secondary immunodeficiency.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
QIG, Quantitative Immunoglobulins

64
317
Requirements: 1 mL body fluid from red top tube, ambient, refrigerated or frozen TURB
86431
=<14 IU/mL
1 - 3 Days
IgM-RF may be detected in body fluids of rheumatoid arthritis patients. About half of these patients will demonstrate RF in the synovial fluid. At times, the joint tissue will produce RF even if serum RF is negative. False-positive RF can result from several chronic inflammatory diseases.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor (Body Fluid) by Turbidimetry
615
Requirements: 1 mL serum, ambient, refrigerated or frozen TURB
86431
=<14 IU/mL
1 - 3 Days
IgM-RF is the main isotype identified by clinically available diagnostic assays for RF detection. In rheumatoid arthritis, the sensitivity of IgM-RF is 70-75%, with specificity of 85%. It can also be seen in other connective tissue diseases such as SLE, MCTD, Sjogren’s, psoriasis and liver disease, as well as infections such as SBE.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor (Serum), IgM by Turbidimetry
534
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86431
<=6 IU
3 - 5 Days
In rheumatoid arthritis, the sensitivity of IgA-RF is 50%, with specificity of 88%. The presence of this RF isotype is associated with a more severe disease course, worse prognosis and poor clinical response to treatment with anti-TNF-alpha inhibitors.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor, IgA by EIA
533
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86431
<=6 IU
3 - 5 Days
In rheumatoid arthritis, the sensitivity of IgG-RF is 44%, with specificity of 91%. The presence of this RF isotype is associated with RA vasculitis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor, IgG by EIA

65
555
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86431 x 3
<=6 IU
3 - 5 Days
EIA methods have the added advantage of being able to simultaneously detect RF of IgG and IgA subclasses in addition to RF IgM. The specificity and predictive value of the RF test is substantially increased by the detection of all three RF isotypes.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor, IgG, IgA, IgM by EIA
535
Requirements: 1 mL serum, ambient, refrigerated or frozen EIA
86431
<=6 IU
3 - 5 Days
IgM-RF is the main isotype identified by clinically available diagnostic assays for RF detection. In rheumatoid arthritis, the sensitivity of IgM-RF is 70-75%, with specificity of 85%. It can also be seen in other connective tissue diseases such as SLE, MCTD, Sjogren’s, psoriasis and liver disease, as well as infections such as SBE.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Rheumatoid Factor, IgM by EIA
7
Requirements: 1 mL serum, ambient, refrigerated or frozen FLOC
86592
Non-reactive
1 - 3 Days
The ASI RPR (rapid plasma reagin) Card Test for Syphilis is a qualitative and semiquantitative nontreponemal flocculation test for the detection of reagin antibodies in human serum and plasma as a screening test for syphilis. Also RPR can detect anti-nontreponemal antibodies (reagin). FTA is done as a confirmatory test for syphilis if the RPR is positive. A false positive RPR can be caused by antiphospholipid antibodies (specifically antibodies to cardiolipin).
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
RPR (Rapid Plasma Reagin)
104
Requirements: One EDTA (lavender top) tube whole blood at room temperature or refrigerated
WEST
85651
Child: 0 - 10 mm/hr; Male Range: 0 - 15 mm/hr; Female Range: 0 - 20 mm/hr
1 Day
Greater Los Angeles area only. Must be received within 8 hours of collection.
ESR is commonly used to monitor chronic inflammation, including disease severity in autoimmune and other disorders. ESR and C-reactive protein measurements are used most often by rheumatologists in monitoring response to treatment in inflammatory diseases.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Sedimentation Rate, Westergren

66
196
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Signal Recognition particle (SRP) is a myositis specific antibody that is found in 5-8% of adult IIM and <1% JM. It is closely associated with necrotizing myositis. Clinically it presents with acute onset, rapidly progressive, severe weakness, with high CPK levels, and commonly has cardiac and lung involvement. There is usually a poor response to therapy.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
SRP
200
Requirements: 1 red top tube plus one EDTA (lavender top) tube synovial fluid, ambient or refrigerated
MANUAL
89051, 89060, 83872, 85810
See separate components
1 - 3 Days
Must be sent by overnight express mail. Includes cell count with differential, crystal exam, mucin clot, viscosity and interpretation. Do not spin or freeze.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Synovial Fluid Analysis, Complete
Complete analysis consists of the following: appearance and volume, cell count and differential, crystal examination, mucin and viscosity.
201
Requirements: One EDTA (lavender top) tube synovial fluid, ambient or refrigerated MANUAL
89051
WBC :<200 cells/mm3, RBC: <200 cells/mm3, diff: <25% neutrophils
1 - 3 Days
Must be sent by overnight express mail. Do not spin or freeze.
Normal synovial fluid should be colorless, with high viscosity, good mucin clotting, <200 WBCs with <25% neutrophils. Inflammatory (non-infected) fluid is typically white, gray, yellow, green or cloudy/turbid with absent viscosity, poor mucin clotting, <100,000 of WBCs with >50% neutrophils.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Synovial Fluid, Cell Count & Differential
202
Requirements: 1 red top tube synovial fluid, ambient or refrigerated MANUAL
89060
None seen
1 - 3 Days
Must be sent by overnight express mail. Do not contaminate with glove powder. Do not spin, separate or freeze.
A gout diagnosis can be made by the presence of monosodium urate crystals (MSU). MSU crystals are usually thin, needle-like crystals that polarize light and are negatively birefringent. MSU crystals are yellow when aligned with the compensator filter (in parallel). Calcium pyrophosphate dehydrate (CPPD) crystals are present in pseudogout. Compared to MSU, the CPPD crystals are smaller, rod or rhomboid like, and are positive birefringent. Crystals aligned with the compensator filter are blue.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Synovial Fluid, Crystal Exam

67
203
Requirements: 1 red top tube synovial fluid, ambient or refrigerated MANUAL
83872
Firm
1 - 3 Days
Must be sent by overnight express mail. Do not contaminate with glove powder. Do not spin, separate or freeze.
Normal synovial fluid should be colorless, with high viscosity, good mucin clotting, <200 WBCs with <25% neutrophils. Inflammatory (non-infected) fluid is typically white, gray, yellow, green or cloudy/turbid with absent viscosity, poor mucin clotting, <100,000 of WBCs with >50% neutrophils.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Synovial Fluid, Mucin Clot
204
Requirements: 1 red top tube synovial fluid, ambient or refrigerated MANUAL
85810
High
1 - 3 Days
Must be sent by overnight express mail. Do not contaminate with glove powder. Do not spin, separate or freeze.
Normal synovial fluid should be colorless, with high viscosity, good mucin clotting, <200 WBCs with <25% neutrophils. Inflammatory (non-infected) fluid is typically white, gray, yellow, green or cloudy/turbid with absent viscosity, poor mucin clotting, <100,000 of WBCs with >50% neutrophils.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Synovial Fluid, Viscosity
1635
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
84481
2.3 - 4.2 pg/mL
2 - 3 Days
Used to evaluate thyroid function and binding protein status. In hyperthyroidism, if TSH levels are low but the Free T4 level is normal, a T3 measurement should be performed, since the serum T3 concentration is often elevated earlier in the course of hyperthyroidism, and to a greater degree than is the T4 concentration.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
T3, Free
1644
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
84479
22 - 37 %
2 - 3 Days
The thyroid uptake test is ordinarily used in conjunction with an immunoassay for total T4 to correct for the influence which alterations in the levels of circulating thyroid hormone-binding proteins have on the total T4 level.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
T3, Uptake

68
1636
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
84439
0.9 - 1.8 ng/dL
2 - 3 Days
Since abnormal T4 levels may signify either abnormal thyroid function or carrier protein variation (physiological or pathological), free T4 measurements more highly correlate with thyroid status than total T4 measurements.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
T4, Free
1641
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
84436
4.5 - 10.9 ug/dL
2 - 3 Days
T4 (total) is the primary secretory product of the normal thyroid gland. Total T4 undergoes peripheral deiodination of the outer ring at the 5’ position to yield T3. The total T4 assay is used to evaluate thyroid function, independent of binding protein status.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
T4, Thyroxine (Total)
233
Requirements: 1 mL serum, ambient, refrigerated or frozen, or EDTA (lavender top) plasma can be used
RIPA
83516
Negative
10 - 14 Days
Anti-Th/To antibodies are present in 2-6% of patients with limited SSc and are rarely found in diffuse SSc. They have a high specificity and are associated with isolated pulmonary arterial HTN, pulmonary fibrosis, and renal crisis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Th/To Ab
1643
Requirements: 1 mL serum, ambient, refrigerated or frozen CH
84443
0.35 -5.50 uIU/mL
2 - 3 Days
Measurements of circulating TSH have been used as a primary test for the diagnosis of hypothyroidism, and as an aid in monitoring the adequacy of thyroid hormone replacement therapy.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Thyroid Stimulating Hormone (TSH), 3rd Generation

69
266
Requirements: 2 mL serum, ambient, refrigerated or frozen EIA
83520
<20 ng/mL
3 - 5 Days
Tissue transglutaminase (tTG), human IgA has a 85-98% sensitivity with a 95-99% specificity for Celiac disease. tTG can decrease or disappear in patients compliant with a gluten free diet.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Tissue Transglutaminase Ab, Human IgA (tTG)
37
Requirements: 1 mL serum, frozen, in plastic vial from SST tube EIA
86162
63 - 145 CAE Units
2 - 5 Days
Centrifuge specimen and transfer to a plastic vial. Freeze serum immediately and send on dry ice by overnight express mail.
Deficient or decreased levels of serum complement activity of the classical pathway are associated with a number of diseases. A normal CH50 assay indicates that C1 through C9 are present and functional. Although CH50 can be used to assess the integrity of the classical pathway, it must not be used as a sensitive test for in vivo complement fixation. In vitro degradation can also cause low CH50 activity.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Total Hemolytic Complement (CH50)
412
Requirements: 1 mL serum, ambient, refrigerated or frozen COL
84155
6.4 - 8.9 g/dL
1 - 3 Days
Total serum protein measures the total amount of blood protein.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Total Protein, Serum
288
Requirements: 2 Lithium Heparin (green top), 6 mL each at room temperature. ELISPOT
86481
Negative
3 Days
Patients can only be drawn Monday – Thursday. Please do not draw on Friday (except for clients in the greater Los Angeles area). Before drawing, call RDL for special supplies with gel pack. 1. Draw two lithium heparin [green top] tubes [6 mL each]. Invert ten times to mix. Do not centrifuge. Time of draw must be written on both tubes. Keep them at room temperature. NEVER REFRIGERATE OR FREEZE. 2. Keep the specimen ambient, at room temperature until the RDL courier or FEDEX courier picks it up. The specimen must be picked up the same day of draw.
Testing for latent TB is done via the T-Spot TB assay, which is an FDA approved Interferon Gamma Release Assay (IGRA). When compared to the QuantiFERON-TB Gold, multiple studies show a more favorable sensitivity, similar specificity and less indeterminate results with the T-Spot TB test.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
T-Spot TB Test

70
234
Requirements: 1 mL serum, ambient, refrigerated or frozen RIPA
83516
Negative
10 - 14 Days
U2 snRNP autoantibodies are myositis associated autoantibodies (MAA) found in less than 5% of idiopathic inflammatory myopathies. Clinically they are associated with the scleroderma/myositis overlap syndrome.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
U2 snRNP
384
Requirements: 2 mL serum, ambient, refrigerated or frozen COL
84550
2.3 - 7.6 mg/dL
1 - 3 Days
Uric acid is the end product of purine metabolism, can be elevated in serum and is associated with gout. Other possible causes of increased uric acid may be renal failure, hereditary diseases, and nondiabetic ketosis.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Uric Acid
1148
Requirements: 1 mL serum (preferred) or plasma from EDTA (lavender top) tube or heparin (green top) tube, refrigerated or frozen
CHEM
82306
30 - 100 ng/mL
2 - 5 Days
Send serum or plasma by overnight express mail, on an ice pack if refrigerated or on dry ice if frozen.
Serum concentration of 25-OH D is considered to be the most reliable measure of overall vitamin D status and thus can be used to determine whether a patient is vitamin D sufficient.
Method:
CPT Codes:
Normal:
Turnaround Time:
Utilities:
Instructions:
Vitamin D, 25-Hydroxy (Calcifediol)

71

72

73
Index of Test Combinations and Individual Tests
By Test Name

74
Test # Test Name Page
Index of Test Combinations By Test Name
1228 ANA 12 Plus Profile ....................................................... 18
1785 ANA 12 Plus Profile with RPR ........................................ 18
1201 ANA 12 Profile ............................................................... 18
1100 ANA Profile I .................................................................. 18
1020 ANA Profile II ................................................................. 19
994 ANCA Panel .................................................................. 19
1811 Antiphospholipid Ab Panel I ........................................... 19
1850 Antiphospholipid Ab Panel II .......................................... 19
1292 Anti-Synthetase Panel ................................................... 20
996 Arthritis Panel ................................................................ 20
265 Autoimmune Inner Ear Disease Panel (AIED Panel) ........ 20
558 Autoimmune Liver Disease Panel, Comprehensive ........ 20
1044 Celiac Disease Ab Panel ............................................... 21
1390 Cryoglobulins Characterization Panel ............................ 21
564 Epstein Barr Viral Panel ................................................. 21
1079 Glomerulonephritis Panel (GNP) .................................... 21
349 Gluten Free Dietary Compliance Panel .......................... 22
704 Hepatitis Panel I – Acute ............................................... 22
705 Hepatitis Panel II ........................................................... 22
1277 Implant Failure Panel ..................................................... 22
1265 Inflammatory Bowel Disease Panel II ............................. 23
475 Interstitial Lung Disease Panel I ..................................... 23
354 Interstitial Lung Disease Panel II .................................... 23
1065 Lupus Activity Panel ..................................................... 23
342 Lupus Renal Activity Panel ............................................ 24
628 Lymphocyte Immunophenotyping Panel: ...................... 24 Helper/Suppressor Panel
634 Lymphocyte Immunophenotyping Panel: ...................... 24 T & B Cell Panel
629 Lymphocyte Immunophenotyping Panel: ...................... 24 T, B & NK Cell Panel
633 Lymphocyte Immunophenotyping: ................................ 25 Natural Killer Cell 56/16

75
Test # Test Name Page
Index of Test Combinations By Test Name
1377 MyoMarker™ Panel 1 ................................................... 25
245 MyoMarker™ Panel 2 ................................................... 25
1222 MyoMarker™ Panel 3 ................................................... 25
655 Pre-Biologic Therapy Assessment Panel ....................... 26
822 Pre-Biologic Therapy Assessment Panel + .................... 26 ANA, dsDNA & Histone
788 Pre-Biologic Therapy Assessment Panel ....................... 26 with Coccidioidomycosis
1600 Primary Biliary Cirrhosis Panel (PBC) ............................. 26
1789 Recurrent Pregnancy Loss Panel .................................. 27
1041 Reflexive Systemic Vasculitis Panel I (RSVP I) ................ 27
1085 Reflexive Systemic Vasculitis Panel II (RSVP II) .............. 27
1030 Rheumatoid Arthritis Ab Panel ...................................... 27
1836 Rheumatoid Arthritis Autoantibody Panel, ..................... 28 Comprehensive
1686 Scleroderma Panel, Comprehensive ............................. 28
1257 Seronegative Arthritis Panel I ........................................ 28
1438 Spondyloarthropathy Panel ........................................... 28
1717 Thyroid Autoantibody Panel .......................................... 29
1661 Thyroid Function Panel ................................................. 29
1070 Vasculitis Panel I ........................................................... 29

76
Test # Test Name Page
Index of Individual Tests By Test Name
272 Aldolase ....................................................................... 32
465 Alpha 1-Antitrypsin ....................................................... 32
147 Angiotensin Converting Enzyme (ACE) .......................... 32
105 Anti-Actin Ab, IgG ......................................................... 32
10 Anti-Adrenal Ab ............................................................ 33
185 Anti-Alpha Fodrin Ab, IgA ............................................. 33
184 Anti-Alpha Fodrin Ab, IgG ............................................. 33
6 Anti-Beta-2-Glycoprotein I Abs, IgG, IgA & IgM ............. 33
458 Anti-C1Q Ab, IgG ......................................................... 34
9 Anticardiolipin Abs, IgG, IgA & IgM ................................ 34
12 Anti-Centromere Ab ...................................................... 34
578 Anti-Chromatin Ab, IgG ................................................ 34
165 Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP), IgG ...... 35
14 Anti-DNA Ab (Single Stranded) ..................................... 35
38 Anti-dsDNA Ab (Crithidia) .............................................. 35
13 Anti-dsDNA Ab (Farr Assay, Double Stranded) .............. 35
136 Anti-dsDNA Ab by Elisa ................................................ 36
914 Anti-ENA Abs (Anti-SM & Anti-RNP) ............................. 36
52 Anti-Endomysial Ab, IgA ............................................... 36
575 Anti-F Actin Ab, IgA ...................................................... 36
452 Anti-Gliadin II (DGP) Ab, IgG & IgA ................................ 37
956 Anti-Glomerular Basement Membrane Ab (Anti-GBM) ... 37
1601 Anti-Gp-210 Ab ............................................................ 37
15 Anti-Histone Ab ............................................................ 37
1809 Anti-HMGCR IgG Ab .................................................... 38
260 Anti-Human Heat Shock Protein 70-kd Ab, IgG ............ 38 (HSP-70), EIA
559 Anti-Human Heat Shock Protein 70-kd Ab, IgG ............ 38 (HSP-70), WB
259 Anti-Inner Ear Membrane Ab, IgG ................................. 38
53 Anti-Islet Cell Ab ........................................................... 39
434 Anti-JO 1 Ab ................................................................. 39
576 Anti-LA Ab (SS-B) ......................................................... 39

77
Test # Test Name Page
Index of Individual Tests By Test Name
129 Anti-Liver/Kidney Microsomal Ab .................................. 39
173 Anti-MDA5 (part of P140 kD) AKA CADM-140 .............. 40
18 Anti-Mitochondrial Ab by IFA ......................................... 40
428 Anti-Mitochondrial M2 EP Ab by EIA ............................. 40
230 Anti-Mup44 (cN1A) Ab .................................................. 40
88 Anti-Myeloperoxidase Ab (Anti-MPO) ............................ 41
19 Anti-Myocardial Ab ....................................................... 41
156 Anti-Neuronal Ab, IgG ................................................... 41
990 Anti-Neutrophil Cytoplasmic Ab (ANCA) ........................ 41
20 Anti-Nuclear Ab (ANA) .................................................. 42
205 Anti-Nuclear Ab (ANA), Body Fluid ................................ 42
287 Anti-Nuclear Ab, CSF ................................................... 42
174 Anti-NXP-2 (MJ) (part of P140 kD) ................................ 42
55 Anti-Ovary Ab ............................................................... 43
645 Anti-Pancreatic Ab ........................................................ 43
21 Anti-Parietal Cell Ab ...................................................... 43
1888 Anti-Phosphatidylserine Abs, IgG, IgA & IgM ................. 43
531 Anti-phosphatidylserine/prothrombin antibodies ........... 44 (aPS/PT) Abs, IgG & IgM
69 Anti-PM/Scl Ab ............................................................. 44
73 Anti-Proliferating Cell Nuclear Ab (Anti-PCNA) ............... 44
89 Anti-Proteinase 3 Ab (PR-3) .......................................... 44
572 Anti-Ribosomal P Protein Ab ........................................ 45
449 Anti-RNA Polymerase III IgG Ab .................................... 45
574 Anti-RNP Ab (U1 snRNP) .............................................. 45
570 Anti-Ro Ab (SS-A) ......................................................... 45
715 Anti-Ro Ab (SS-A) & Anti-La Ab (SS-B) – Sjogren’s ....... 46
644 Anti-Saccharomyces Cerevisiae Ab, IgA & IgG (ASCA) .. 46
577 Anti-Scl-70 Ab .............................................................. 46
57 Anti-Skin Ab, Pemphigus & Pemphigoid ....................... 46
579 Anti-Sm Ab ................................................................... 47
30 Anti-Smooth Muscle Ab ................................................ 47

78
Test # Test Name Page
Index of Individual Tests By Test Name
126 Anti-Soluble Liver Ag Ab ............................................... 47
1602 Anti-Sp-100 Ab ............................................................ 47
1252 Anti-SS-A 52 kD Ab, IgG .............................................. 48
311 Anti-Streptolysin O Ab, (ASO) ....................................... 48
28 Anti-Striated Muscle Ab ................................................ 48
106 Antithrombin III Function (Activity) .................................. 48
1332 Anti-Thyroglobulin Ab (TG) ............................................ 49
1333 Anti-Thyroid Microsomal Peroxidase Ab (TPO) .............. 49
175 Anti-TIF-1γ (P155/140 kD) ............................................ 49
145 C1Q Circulating Immune Complex (C1Q CIC) ............... 49
450 C3 Complement ........................................................... 50
320 C3 Complement, Body Fluid ......................................... 50
460 C4 Complement ........................................................... 50
322 C4 Complement, Body Fluid ......................................... 50
641 CD19 Detection ............................................................ 51
632 CD20 Detection ............................................................ 51
626 CD4 – Helper/Inducer Count ........................................ 51
548 Ceruloplasmin ............................................................... 51
323 Coccidioidomycosis, IgG & IgM .................................... 52
34 Cold Agglutinins ........................................................... 52
314 C-Reactive Protein (CRP) .............................................. 52
340 Creatine Kinase (CPK) .................................................. 52
1380 Cryoglobulins ................................................................ 53
760 Cytomegalovirus (CMV) Ab, IgG .................................... 53
761 Cytomegalovirus (CMV) Ab, IgM ................................... 53
716 Cytomegalovirus (CMV), IgG & IgM ............................... 53
276 EJ ................................................................................. 54
617 Epstein Barr Nuclear Ag (EBNA) Ab, IgG ....................... 54
619 Epstein Barr Viral Capsid Ag (VCA) Ab, IgG .................. 54
620 Epstein Barr Viral Capsid Ag (VCA) Ab, IgM .................. 54
618 Epstein Barr Viral Capsid Ag (VCA) Abs, IgG & IgM ....... 55
621 Epstein Barr Virus, Early Antigen (EA) Ab ...................... 55

79
Test # Test Name Page
Index of Individual Tests By Test Name
1634 Ferritin, Serum .............................................................. 55
232 Fibrillarin (U3 RNP) ........................................................ 55
1345 Fibrinogen .................................................................... 56
241 FTA – Fluorescent Treponemal Ab, Absorbed ............... 56
668 Haptoglobin .................................................................. 56
1722 Hepatitis A Virus Ab (HAV), IgG ..................................... 56
721 Hepatitis A Virus Ab (HAV), IgG & IgM ........................... 57
1721 Hepatitis A Virus Ab (HAV), IgM ..................................... 57
1723 Hepatitis B Core Ab (HBc), IgM ..................................... 57
1724 Hepatitis B Core Ab (HBc), Total ................................... 57
723 Hepatitis B Core Abs (HBc), Total & IgM ....................... 58
725 Hepatitis B Surface Ab (HBsAb), Qualitative .................. 58
726 Hepatitis B Surface Antigen (HBsAg) ............................ 58
727 Hepatitis B Surface Antigen (HBsAg), ........................... 58 Neutralization-Confirmation
730 Hepatitis C Virus Ab (HCV), IgG .................................... 59
90 HLA-B27 ...................................................................... 59
404 IgA, Immunoglobulin A .................................................. 59
403 IgG, Immunoglobulin G ................................................. 59
405 IgM, Immunoglobulin M ................................................ 60
115 Immunofixation Electrophoresis (IFE) ............................. 60
279 Ku ................................................................................ 60
116 Lupus Anticoagulant (LA) .............................................. 60
764 Lyme C6 Peptide Ag ..................................................... 61
710 Lyme Disease, EIA, Reflexive to Western Blot ............... 61
792 Lyme Disease, Western Blot, IgG & IgM ........................ 61
237 MI-2 ............................................................................. 61
277 OJ ................................................................................ 62
2747 Parvovirus B-19 Ab, IgG ............................................... 62
2748 Parvovirus B-19 Ab, IgM ............................................... 62
748 Parvovirus B-19 Abs, IgG & IgM ................................... 62
239 PL-12 ........................................................................... 63

80
Test # Test Name Page
Index of Individual Tests By Test Name
238 PL-7 ............................................................................. 63
113 Protein Electrophoresis, Serum (SPE) – Reflexive .......... 63
400 QIG, Quantitative Immunoglobulins ............................... 63
317 Rheumatoid Factor (Body Fluid) by Turbidimetry ........... 64
615 Rheumatoid Factor (Serum), IgM by Turbidimetry .......... 64
534 Rheumatoid Factor, IgA by EIA ..................................... 64
533 Rheumatoid Factor, IgG by EIA ..................................... 64
555 Rheumatoid Factor, IgG, IgA, IgM by EIA ...................... 65
535 Rheumatoid Factor, IgM by EIA ..................................... 65
7 RPR (Rapid Plasma Reagin) .......................................... 65
104 Sedimentation Rate, Westergren .................................. 65
196 SRP .............................................................................. 66
200 Synovial Fluid Analysis, Complete ................................. 66
201 Synovial Fluid, Cell Count & Differential ......................... 66
202 Synovial Fluid, Crystal Exam ......................................... 66
203 Synovial Fluid, Mucin Clot ............................................. 67
204 Synovial Fluid, Viscosity ................................................ 67
1635 T3, Free ........................................................................ 67
1644 T3, Uptake ................................................................... 67
1636 T4, Free ........................................................................ 68
1641 T4, Thyroxine (Total) ...................................................... 68
233 Th/To Ab ....................................................................... 68
1643 Thyroid Stimulating Hormone (TSH), 3rd Generation ..... 68
266 Tissue Transglutaminase Ab, Human IgA (tTG) .............. 69
37 Total Hemolytic Complement (CH50) ............................ 69
412 Total Protein, Serum ..................................................... 69
288 T-Spot TB Test .............................................................. 69
234 U2 snRNP .................................................................... 70
384 Uric Acid ....................................................................... 70
1148 Vitamin D, 25-Hydroxy (Calcifediol) ............................... 70

81
Index of Test Combinations and Individual Tests
By Test Number

82
Test # Test Name Page
Index of Test Combinations By Test Number
245 MyoMarker™ Panel 2 ................................................... 25
265 Autoimmune Inner Ear Disease Panel (AIED Panel) ....... 20
342 Lupus Renal Activity Panel ............................................ 24
349 Gluten Free Dietary Compliance Panel .......................... 22
354 Interstitial Lung Disease Panel II .................................... 23
475 Interstitial Lung Disease Panel I ..................................... 23
558 Autoimmune Liver Disease Panel, Comprehensive ........ 20
564 Epstein Barr Viral Panel ................................................. 21
628 Lymphocyte Immunophenotyping Panel: ...................... 24 Helper/Suppressor Panel
629 Lymphocyte Immunophenotyping Panel: ...................... 24 T, B & NK Cell Panel
633 Lymphocyte Immunophenotyping: ................................ 25 Natural Killer Cell 56/16
634 Lymphocyte Immunophenotyping Panel: ...................... 24 T & B Cell Panel
655 Pre-Biologic Therapy Assessment Panel ....................... 26
704 Hepatitis Panel I – Acute ............................................... 22
705 Hepatitis Panel II ........................................................... 22
788 Pre-Biologic Therapy Assessment Panel ....................... 26 with Coccidioidomycosis
822 Pre-Biologic Therapy Assessment Panel + .................... 26 ANA, dsDNA & Histone
994 ANCA Panel ................................................................. 19
996 Arthritis Panel ............................................................... 20
1020 ANA Profile II ................................................................ 19
1030 Rheumatoid Arthritis Ab Panel ...................................... 27
1041 Reflexive Systemic Vasculitis Panel I (RSVP I) ................ 27
1044 Celiac Disease Ab Panel ............................................... 21
1065 Lupus Activity Panel ..................................................... 23
1070 Vasculitis Panel I ........................................................... 29
1079 Glomerulonephritis Panel (GNP) .................................... 21
1085 Reflexive Systemic Vasculitis Panel II (RSVP II) .............. 27
1100 ANA Profile I ................................................................. 18

83
Test # Test Name Page
Index of Test Combinations By Test Number
1201 ANA 12 Profile .............................................................. 18
1222 MyoMarker™ Panel 3 ................................................... 25
1228 ANA 12 Plus Profile ...................................................... 18
1257 Seronegative Arthritis Panel I ........................................ 28
1265 Inflammatory Bowel Disease Panel ............................... 23
1277 Implant Failure Panel ..................................................... 22
1292 Anti-Synthetase Panel .................................................. 20
1377 MyoMarker™ Panel 1 ................................................... 25
1390 Cryoglobulins Characterization Panel ............................ 21
1438 Spondyloarthropathy Panel ........................................... 28
1600 Primary Biliary Cirrhosis Panel (PBC) ............................. 26
1661 Thyroid Function Panel ................................................. 29
1686 Scleroderma Panel, Comprehensive ............................. 28
1717 Thyroid Autoantibody Panel .......................................... 29
1785 ANA 12 Plus Profile with RPR ....................................... 18
1789 Recurrent Pregnancy Loss Panel .................................. 27
1811 Antiphospholipid Ab Panel I .......................................... 19
1836 Rheumatoid Arthritis Autoantibody Panel, ..................... 28 Comprehensive
1850 Antiphospholipid Ab Panel II ......................................... 19

84
Test # Test Name Page
Index of Individual Tests By Test Number
6 Anti-Beta-2-Glycoprotein I Abs, IgG, IgA & IgM ............. 33
7 RPR (Rapid Plasma Reagin) .......................................... 65
9 Anticardiolipin Abs, IgG, IgA & IgM ................................ 34
10 Anti-Adrenal Ab ............................................................ 33
12 Anti-Centromere Ab ...................................................... 34
13 Anti-dsDNA Ab (Farr Assay, Double Stranded) .............. 35
14 Anti-DNA Ab (Single Stranded) ..................................... 35
15 Anti-Histone Ab ............................................................ 37
18 Anti-Mitochondrial Ab by IFA ......................................... 40
19 Anti-Myocardial Ab ....................................................... 41
20 Anti-Nuclear Ab (ANA) .................................................. 42
21 Anti-Parietal Cell Ab ...................................................... 43
28 Anti-Striated Muscle Ab ................................................ 48
30 Anti-Smooth Muscle Ab ................................................ 47
34 Cold Agglutinins ........................................................... 52
37 Total Hemolytic Complement (CH50) ............................ 69
38 Anti-dsDNA Ab (Crithidia) .............................................. 35
52 Anti-Endomysial Ab, IgA ............................................... 36
53 Anti-Islet Cell Ab ........................................................... 39
55 Anti-Ovary Ab ............................................................... 42
57 Anti-Skin Ab, Pemphigus & Pemphigoid ....................... 46
69 Anti-PM/Scl Ab ............................................................. 44
73 Anti-Proliferating Cell Nuclear Ab (Anti-PCNA) ............... 44
88 Anti-Myeloperoxidase Ab (Anti-MPO) ............................ 41
89 Anti-Proteinase 3 Ab (PR-3) .......................................... 44
90 HLA-B27 ...................................................................... 59
104 Sedimentation Rate, Westergren .................................. 65
105 Anti-Actin Ab, IgG ......................................................... 32
106 Antithrombin III Function (Activity) .................................. 48
113 Protein Electrophoresis, Serum (SPE) – Reflexive .......... 63
115 Immunofixation Electrophoresis (IFE) ............................. 60
116 Lupus Anticoagulant (LA) .............................................. 60

85
Test # Test Name Page
Index of Individual Tests By Test Number
126 Anti-Soluble Liver Ag Ab ............................................... 47
129 Anti-Liver/Kidney Microsomal Ab .................................. 39
136 Anti-dsDNA Ab by Elisa ................................................ 36
145 C1Q Circulating Immune Complex (C1Q CIC) ............... 49
147 Angiotensin Converting Enzyme (ACE) .......................... 32
156 Anti-Neuronal Ab, IgG ................................................... 41
165 Anti-Cyclic Citrullinated Peptide Ab (Anti-CCP), IgG ...... 35
173 Anti-MDA5 (part of P140 kD) AKA CADM-140 .............. 40
174 Anti-NXP-2 (MJ) (part of P140 kD) ................................ 42
175 Anti-TIF-1γ (P155/140 kD) ............................................ 49
184 Anti-Alpha Fodrin Ab, IgG ............................................. 33
185 Anti-Alpha Fodrin Ab, IgA ............................................. 33
196 SRP .............................................................................. 65
200 Synovial Fluid Analysis, Complete ................................. 66
201 Synovial Fluid, Cell Count & Differential ......................... 66
202 Synovial Fluid, Crystal Exam ......................................... 66
203 Synovial Fluid, Mucin Clot ............................................. 67
204 Synovial Fluid, Viscosity ................................................ 67
205 Anti-Nuclear Ab (FANA), Body Fluid .............................. 42
230 Anti-Mup44 (cN1A) Ab .................................................. 40
232 Fibrillarin (U3 RNP) ........................................................ 55
233 Th/To Ab ....................................................................... 68
234 U2 snRNP .................................................................... 70
237 MI-2 ............................................................................. 61
238 PL-7 ............................................................................. 63
239 PL-12 ........................................................................... 63
241 FTA – Fluorescent Treponemal Ab, Absorbed ............... 56
259 Anti-Inner Ear Membrane Ab, IgG ................................. 38
260 Anti-Human Heat Shock Protein 70-kd Ab, .................. 38 IgG (HSP-70), EIA
266 Tissue Transglutaminase Ab, Human IgA (tTG) .............. 69
272 Aldolase ....................................................................... 32

86
Test # Test Name Page
Index of Individual Tests By Test Number
276 EJ ................................................................................. 54
277 OJ ................................................................................ 62
279 Ku ................................................................................ 60
287 Anti-Nuclear Ab, CSF ................................................... 42
288 T-Spot TB Test .............................................................. 69
311 Anti-Streptolysin O Ab, (ASO) ....................................... 48
314 C-Reactive Protein (CRP) .............................................. 52
317 Rheumatoid Factor (Body Fluid) by Turbidimetry ........... 64
320 C3 Complement, Body Fluid ......................................... 50
322 C4 Complement, Body Fluid ......................................... 50
323 Coccidioidomycosis, IgG & IgM .................................... 52
340 Creatine Kinase (CPK) .................................................. 52
384 Uric Acid ....................................................................... 70
400 QIG, Quantitative Immunoglobulins ............................... 63
403 IgG, Immunoglobulin G ................................................. 59
404 IgA, Immunoglobulin A .................................................. 59
405 IgM, Immunoglobulin M ................................................ 60
412 Total Protein, Serum ..................................................... 69
428 Anti-Mitochondrial M2 EP (MIT3) Ab ............................. 40
434 Anti-JO 1 Ab ................................................................. 39
449 Anti-RNA Polymerase III IgG Ab .................................... 45
450 C3 Complement ........................................................... 50
452 Anti-Gliadin II (DGP) Ab, IgG & IgA ................................ 37
458 Anti-C1Q Ab, IgG ......................................................... 34
460 C4 Complement ........................................................... 50
465 Alpha 1-Antitrypsin ....................................................... 32
531 Anti-phosphatidylserine/prothrombin antibodies ........... 44 (aPS/PT) Abs, IgG & IgM
533 Rheumatoid Factor, IgG by EIA ..................................... 64
534 Rheumatoid Factor, IgA by EIA ..................................... 64
535 Rheumatoid Factor, IgM by EIA ..................................... 65
548 Ceruloplasmin ............................................................... 51

87
Test # Test Name Page
Index of Individual Tests By Test Number
555 Rheumatoid Factor, IgG, IgA, IgM by EIA ...................... 65
559 Anti-Human Heat Shock Protein 70-kd Ab, .................. 38 IgG (HSP-70), WB
570 Anti-Ro Ab (SS-A) ......................................................... 45
572 Anti-Ribosomal P Protein Ab ........................................ 45
574 Anti-RNP Ab (U1 snRNP) .............................................. 45
575 Anti-F Actin Ab, IgA ...................................................... 36
576 Anti-LA Ab (SS-B) ......................................................... 39
577 Anti-Scl-70 Ab .............................................................. 46
578 Anti-Chromatin Ab, IgG ................................................ 34
579 Anti-Sm Ab ................................................................... 47
615 Rheumatoid Factor (Serum), IgM by Turbidimetry .......... 64
617 Epstein Barr Nuclear Ag (EBNA) Ab, IgG ....................... 54
618 Epstein Barr Viral Capsid Ag (VCA) Abs, IgG & IgM ....... 55
619 Epstein Barr Viral Capsid Ag (VCA) Ab, IgG .................. 54
620 Epstein Barr Viral Capsid Ag (VCA) Ab, IgM .................. 54
621 Epstein Barr Virus, Early Antigen (EA) Ab ...................... 55
626 CD4 – Helper/Inducer Count ........................................ 51
632 CD20 Detection ............................................................ 51
641 CD19 Detection ............................................................ 51
644 Anti-Saccharomyces Cerevisiae Ab, IgA & IgG (ASCA) .. 46
645 Anti-Pancreatic Ab ........................................................ 43
668 Haptoglobin .................................................................. 56
710 Lyme Disease, EIA, Reflexive to Western Blot ............... 61
715 Anti-Ro Ab (SS-A) & Anti-La Ab (SS-B) – Sjogren’s ....... 46
716 Cytomegalovirus (CMV), IgG & IgM ............................... 53
721 Hepatitis A Virus Ab (HAV), IgG & IgM ........................... 57
723 Hepatitis B Core Abs (HBc), Total & IgM ....................... 58
725 Hepatitis B Surface Ab (HBsAb), Qualitative .................. 58
726 Hepatitis B Surface Antigen (HBsAg) ............................ 58
727 Hepatitis B Surface Antigen (HBsAg), ........................... 58 Neutralization-Confirmation
730 Hepatitis C Virus Ab (HCV), IgG .................................... 59
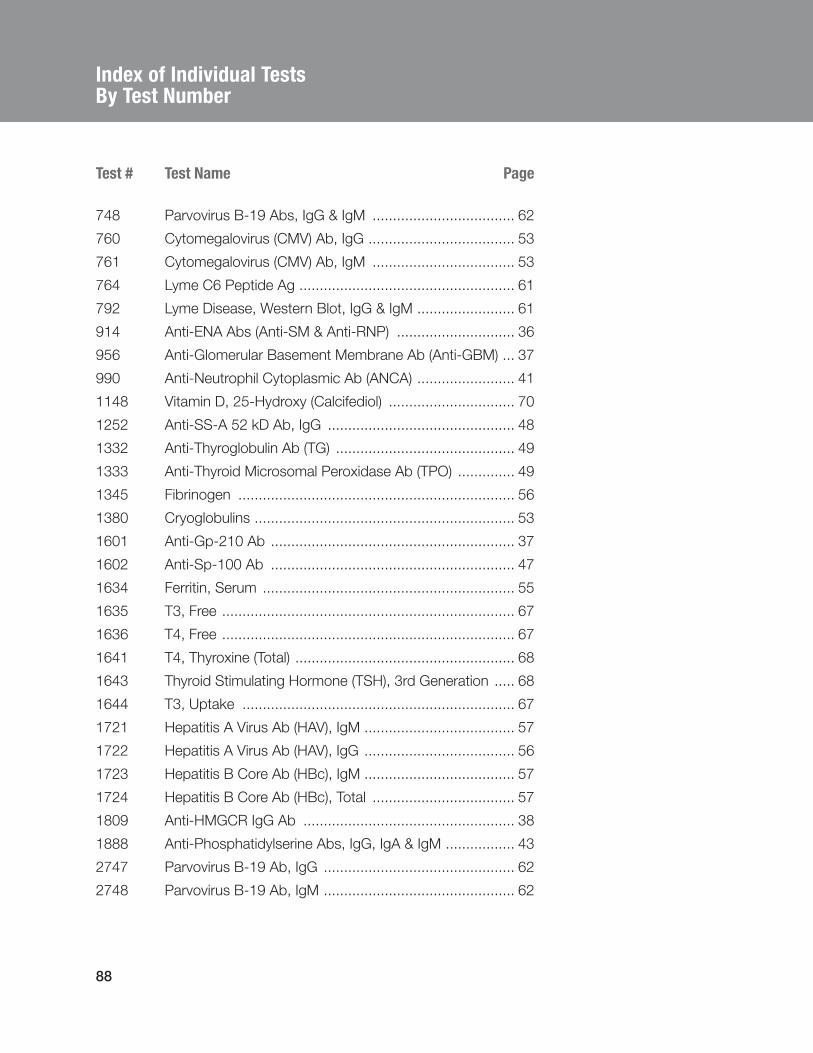
88
Test # Test Name Page
Index of Individual Tests By Test Number
748 Parvovirus B-19 Abs, IgG & IgM ................................... 62
760 Cytomegalovirus (CMV) Ab, IgG .................................... 53
761 Cytomegalovirus (CMV) Ab, IgM ................................... 53
764 Lyme C6 Peptide Ag ..................................................... 61
792 Lyme Disease, Western Blot, IgG & IgM ........................ 61
914 Anti-ENA Abs (Anti-SM & Anti-RNP) ............................. 36
956 Anti-Glomerular Basement Membrane Ab (Anti-GBM) ... 37
990 Anti-Neutrophil Cytoplasmic Ab (ANCA) ........................ 41
1148 Vitamin D, 25-Hydroxy (Calcifediol) ............................... 70
1252 Anti-SS-A 52 kD Ab, IgG .............................................. 48
1332 Anti-Thyroglobulin Ab (TG) ............................................ 49
1333 Anti-Thyroid Microsomal Peroxidase Ab (TPO) .............. 49
1345 Fibrinogen .................................................................... 56
1380 Cryoglobulins ................................................................ 53
1601 Anti-Gp-210 Ab ............................................................ 37
1602 Anti-Sp-100 Ab ............................................................ 47
1634 Ferritin, Serum .............................................................. 55
1635 T3, Free ........................................................................ 67
1636 T4, Free ........................................................................ 67
1641 T4, Thyroxine (Total) ...................................................... 68
1643 Thyroid Stimulating Hormone (TSH), 3rd Generation ..... 68
1644 T3, Uptake ................................................................... 67
1721 Hepatitis A Virus Ab (HAV), IgM ..................................... 57
1722 Hepatitis A Virus Ab (HAV), IgG ..................................... 56
1723 Hepatitis B Core Ab (HBc), IgM ..................................... 57
1724 Hepatitis B Core Ab (HBc), Total ................................... 57
1809 Anti-HMGCR IgG Ab .................................................... 38
1888 Anti-Phosphatidylserine Abs, IgG, IgA & IgM ................. 43
2747 Parvovirus B-19 Ab, IgG ............................................... 62
2748 Parvovirus B-19 Ab, IgM ............................................... 62



















