
Table 1. Percent distribution of active physicians in patient care by specialty, 2007...
63
Emergency Medicine Intro Sarah Lewis MHS, PA-C
-
Upload
denis-booker -
Category
Documents
-
view
214 -
download
0
Transcript of Table 1. Percent distribution of active physicians in patient care by specialty, 2007...

Emergency Medicine Intro
Sarah Lewis MHS, PA-C

Emergency Medicine on TV

EM Intro Topics1. History and Stats
2. EMTALA
3. Personnel
4. General EM Principles
5. Timing and Schedule
6. Procedural Skills in EM
7. Social Considerations

EM History and Stats

Emergency Medicine History Emergency medicine as a medical specialty is relatively young.
Prior to the 1960’s and 70’s, hospital emergency departments were generally staffed by physicians on staff at the hospital on a rotating basis, among them general surgeons, internists, psychiatrists and dermatologists.
Physicians in training (interns and residents), foreign medical graduates and sometimes nurses also staffed the Emergency Department (ED)
EM was born as a specialty in order to fill the time commitment required by physicians on staff to work in the increasingly chaotic EDs all of the time.

Emergency Medicine HistoryThe first such groups were headed by 5 physicians at Alexandria
Hospital, VA
• established 24/7 year round emergency care which became known as the “Alexandria Plan”.
The first training program started at Cincinnati General Hospital in 1970. At this time it was not yet recognized as a specialty and hence no primary board certification exam.
It was not until 1979 that EM became a recognized medical specialty.

Stats• Number of visits: 136.1 million
• Number of injury-related visits: 45.4 million
• Number of visits per 100 persons: 45.1
• Percent of visits with patient seen in fewer than 15 minutes: 21.7%
• Percent of visits resulting in hospital admission: 12.6%

Table 1. Percent distribution of active physicians in patient care by specialty, 2007
Specialty PercentInternal medicine 20.1
Family medicine/general practice 12.4
Pediatrics 9.6
Obstetrics and gynecology 5.6
Anesthesiology 5.5Psychiatry 5.2General Surgery 5.0Emergency Medicine 4.1
SOURCE: American Medical Association, 2009 Physician Characteristic and Distribution in the US.

Bright future for PA’s employment in EM
The United States has nearly 40,000 clinically active emergency physicians, but these numbers are not adequate to treat the growing number of people who visit emergency departments each year. New emergency physicians are not being trained fast enough, and shortages are expected to continue for several decades, particularly in rural areas and the central part of the country.

Stats5,286 ED PA’s (practicing in 2008)
• 23% rural ED’s
• 41% Inner city ED’s
• 32% Suburban ED’s
• 1% Other
Residency programs for Docs and PA’s

"Millions more people each year are seeking emergency care, but emergency departments are continuing to close, often because so much care goes uncompensated, which is the real economic issue in emergency medicine today," said Dr. Linda Lawrence, president of the American College of Emergency Physicians. "This report is very troubling, because it shows that care is being delayed for everyone, including people in pain and with heart attacks. As policymakers debate proposals to reform the health care system, which focus on early treatment and prevention, it’s essential to remember that none of those reforms will be achieved for years to come. In the meantime, emergency departments are providing a health care safety net for everyone. That’s why any efforts to reform health care must include resources to strengthen the nation’s ERs, which are a critical, often life or death, part of our health care system."

ED’s are a safety net for people unable to obtain medical care elsewhere.
Crisis: hundreds of emergency departments have closed in the US in past 10 years while the number of ED visits increases dramatically.
Why?

EMTALA

EMTALAFederal law - 1986
• Emergency Medical Treatment and Labor Act.
Part of COBRA 1995
Requires "emergency" care to be provided to anyone who needs it, REGARDLESS of their ability to pay or insurance status.
• All pts must be screened (vitals, hx) and offered an evaluation from a provider

EMTALA Emergency Medical Condition
• "a condition manifesting itself by acute symptoms of sufficient severity (including severe pain) such that the absence of immediate medical attention could reasonably be expected to result in placing the individual's health [or the health of an unborn child] in serious jeopardy, serious impairment to bodily function or serious dysfunction of bodily organs."
BUT insurance co. & HMO determine payment by final diagnosis, not risk on entry of pt. to ED !

EMTALA
All pts. with similar medical conditions must be treated consistently.
Care cannot be delayed by questions about methods of payment or insurance coverage
Also to prevent hospitals from transferring those unable to pay to charity/county hospitals.

EMTALA Significant penalties for violation of EMTALA to the
hospital.
• Hospital: $25-50K / violation
• Physician: $50K / violation, excluded from medicare/aid programs
• Pt. can sue hospital for personal injury in a civil court
EMTALA is an unfunded mandate
Thus, ED’s are closing because of burden on the hospital.

Personnel

ED PersonnelProviders
• Staff physician, residents, APC’s (NP’s and PA’s), medical and PA students
Caregivers
• Charge nurse, primary RN supervisor, triage nurse, nurses, ED technicians, paramedics, respiratory therapists, nursing students, IV team, pastoral care
Clerks, secretary, administrators
Consultants, radiologists, PCP, specialists, non-physician therapists, social workers

ED Support PersonnelPre-hospital
• EMS
• Security
• Poison control
• Chaplains
In-hospital
• Unit clerks
• Social services
• Translators
Post hospital
• Chemical dependency units
• Psychiatric facilities
• Shelters

General ED Principles
I don’t know what they’ve got, but I don’t think it will kill them?

General ED PrinciplesIdentify and Stabilize a life-threatening condition
Find an explanation for the condition
Recognize coexistent pathology
Determine why the patient presented NOW rather than earlier or later
Address the patient’s symptoms
Consider the necessity to determine the diagnosis before the patient leaves the ED

General ED PrinciplesH&P
ED course/Plan
Medical Decision Making vs. DDx
Discuss the ED course and plan with the patient or family member.
Decide on the disposition
(Record the entire visit in the record)

Waiting….

The Clock is tickingTimer on every encounter
Door to triage
Door to EKG
Door to “Doc”
Door to CT
Door to Cath lab
ED consult till consultant arrives in ED
Admission orders till pt leaves ED (boarders)
Average LOS (Length of Stay)

Red Flags:LWOT= Left without treatment
AMA= against medical advice (form available to document specifically)

Lectures
Groups
Hands-On
BLS/ACLS
Schedule

EM topics in prior modules Infectious diseases
GYN emergencies
Urologic emergencies
Allergic reactions
Sickle cell, bleeding/clotting disorders
Renal disease, stones
Strokes, bleeds, seizures, CNS infections, delerium
ACS, arrhythmias, failure, etc
Ophtho emergencies
PE, respiratory failure, pneumonia, asthma/COPD
Suicide, psychoses, drug/EtOH
Gout, septic joint, Fractures, osteomyelitis, cauda equina
ENT emergencies
Hepatic failure, GI bleed, IBD, pancreatitis, ab pain, PUD
Surgery and complications

EM topics nowPre-hospital Care and Burns:
John Carroll
Procedures, Headaches: SKL
Chest Pain: Craig Ernst
ED Diagnostics, Access and Monitoring: Doc Freeman
Environmental Emergencies: John Leffort
Burns, Bites and Stings: WAE
Psych Clearance- Dr. Rigberg
Metabolic Emergencies: CG

EM/Trauma topics nowATLS: Dr. Armstrong
Peds Resucitation: Jen Bell
Head Trauma, Toxicology: Dr. Frailey
CBR Threats, ED Flow, Drugs of Abuse: Dr. Scott Goldstein
Penetrating Wounds, Thoracic and Spinal Trauma: Scott Nearhoof
OB-GYN Emergencies: AMS
Shock: Dr. Daniello

Hands-on: IV access
Airway control
BLS/ACLS

Small GroupsClinical scenarios to develop a plan
hands on trauma station
• CPR
• Airway
• Monitor/defibrillator
• IV access
• Foley cath
Discussion
BLS/ACLSOnline Course Completion
BLS hands on session
Optional Q&A
ACLS Mega Code Testing Stations

Emergency Medicine GradesComponent % of grade
EMed Module Exam 60%
Groups 10%
ACLS 10%
Semester Final 20%
TOTAL 100%

Blocks
Wound Care
I&D
Procedural Skills in EM

ProceduresRegional vs local blocks
Laceration repair
Abscess I&D
Joint aspiration
Corneal FB removal- slit lamp
Cerumen impaction
Peritonsillar Abscess I&D
Chest tube (during thoracic trauma lecture)
Nail avulsion
Urine catheterization
FAST exams
Dental repair
Deliveries! (Anna Mae will review)

Topical
Local injected
Local vs Regional blocks

Field Block

Field Blocks
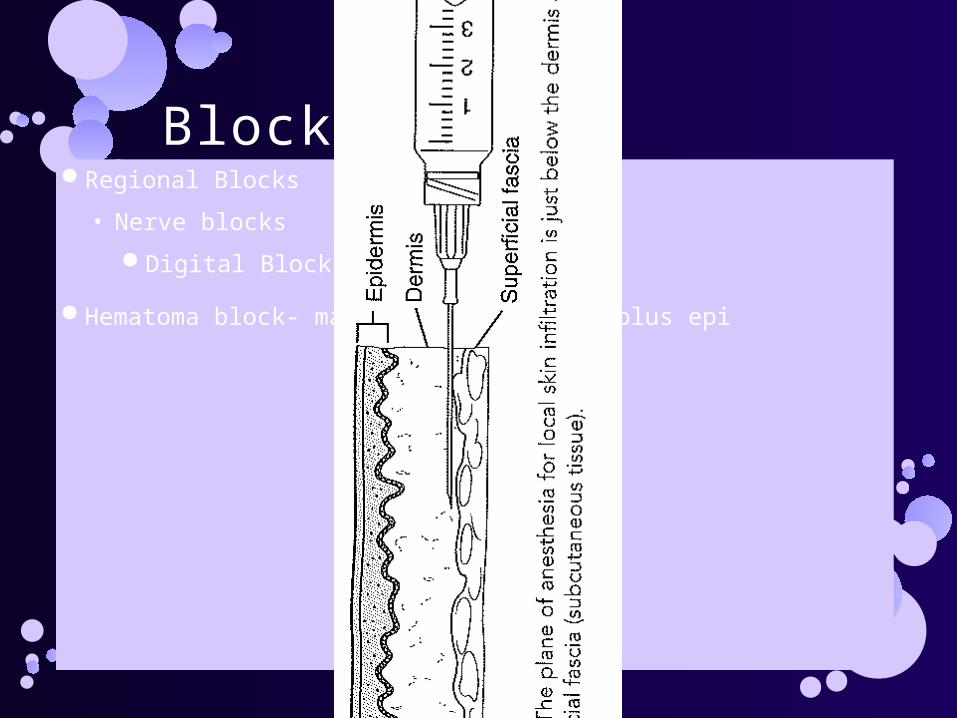
Blocks cont.Regional Blocks
• Nerve blocks
Digital Block- lidocaine
Hematoma block- marcaine/bupivicaine plus epi

Digital block

Irrigation

Laceration repairConsider cosmesis, consult plastics
Consider orthopedics for functional loss
Vascular surgeons?
Neurosurgery?
Another facility?

Nail avulsionSee PDF

http://lifeinthefastlane.com/2009/10/top-ten-foreign-bodies/
FB removal

Corneal FB removal- slit lampForeign body removal
• Alcaine
• Cotton swab needle/forcep
Rust ring removal– eye spud or burr
Fluoroscein

Joint aspirationMark
Sterile prep
Tube to lab for culture, crystals and gram stain- with cap on!

Abscess I&DAnesthetize
Incise and drain
• Septated lesions?
Culture!
Keep open how
• Packing
• Suture in a drain
Antibiotics?

Abscess- specialAsk consults before you I&D in certain areas
Consider imaging, labs

Peritonsillar Abscess I&DAspirate culture
Suction!
Incision- watch this done if possible
(wear a mask)
http://www.entusa.com/surgery_videos_flash/quinsy-drainage-2/quinsy-drainage_flv0.htm
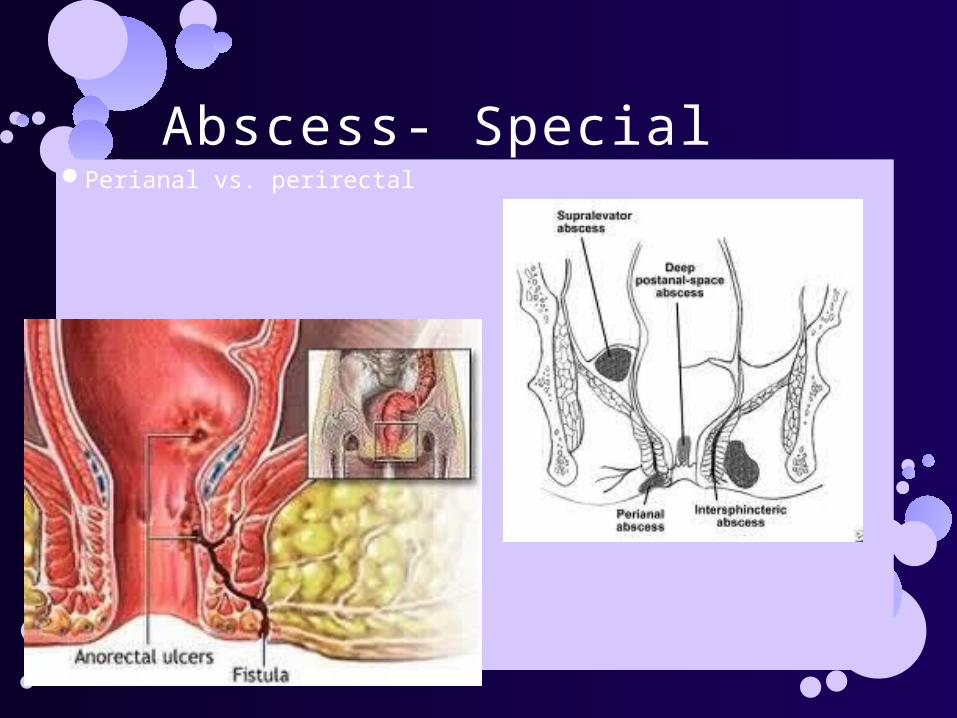
Abscess- SpecialPerianal vs. perirectal

Cerumen impaction Wet vs. Dry
Soften first:
• Water/peroxide 50/50 mix
• Debrox OTC
• Liquid Colase
Irrigate with large soft tipped syringe
• Body temp water
• Can add an astringent
Scoops and hooks vs. dynamite
Cortisporin Otic suspension?

Urine catheterization Tool as well for post void residual, multiports irrigation for
bleeding
Nurses will ask for your help if tricky!
Sterile technique, Use urojet or other numbing lubricant
Consider small catheter vs larger catheter
If foley coming out overinflate the balloon
If can’t get past the prostate try a larger (smaller # french) catheter (more rigid) or a coude tipped catheter
Call Urology

Be open, receptive, non-judgmental
Social Aspects of the ER

Sharing Personal InformationBeliefs
Culture
Religion
Work issues
Relationship/Marital issues
Family situation

Awkwardpeople have trouble asking for help:
• note off work
• request for pain meds
disclosing embarrassing stuff
• H&P
• Financial including lack of insurance
• employment issues
• social/family issues
Language barriers

EmbarassingYou will see and hear jaw-dropping stuff
• history/ mechanism
• PE
Financial constraints
Sexual preference and practice
Infidelity
Get out your Poker Faces!

ExpensiveTests recommended may equal $$$ to the patient
• Some patients even with insurance are responsible for at %, or initial amount for the year
• Unplanned expense
Cost may have delayed their care, or limited them to the ER
• Low collection rates from ERs

FrustrationMay have seen other providers
May have a timing issue outside of this visit
• Work, childcare, travel
May leave with no answer, or little understanding
Hard to get feedback later to new questions
WaitingDid you make an appointment to visit the ER?
Would you like fries with that?
Do you see that person dying over there, with a team working frantically around them- that’s the delay. We’ll see you and your stubbed toe after they die!

Still Waiting . . .Patients with the lowest level of visit, document the most
frustration with wait times on surveys!
• Fast tracks/ quick care/ urgent care centers
Update patients of delays
Tell them the expected process and timing.

Lack of Privacy

Good luck and Enjoy!


![[SAMPLE] Specialty Physicians Discuss Their Opinions of the U.S. Biosimilars Market](https://static.fdocuments.net/doc/165x107/554b9490b4c905463d8b4a5c/sample-specialty-physicians-discuss-their-opinions-of-the-us-biosimilars-market.jpg)










![[SAMPLE] Specialty Physicians Discuss Their Opinions of the United States Biosimilars Market](https://static.fdocuments.net/doc/165x107/55d53372bb61ebfa548b461a/sample-specialty-physicians-discuss-their-opinions-of-the-united-states-biosimilars.jpg)




