Systems Approaches to Colorectal Cancer Care
35
Systems Approaches to Colorectal Cancer Care Stephen D. Roberts Brian Denton Reha Uzsoy Edward P. Fitts Department of Industrial and Systems Engineering North Carolina State University Raleigh NC, USA 3rd Annual Cancer Care Engineering Retreat
description
3rd Annual Cancer Care Engineering Retreat. Systems Approaches to Colorectal Cancer Care. Stephen D. Roberts Brian Denton Reha Uzsoy Edward P. Fitts Department of Industrial and Systems Engineering North Carolina State University Raleigh NC, USA. About 150,000 people diagnosed each year. - PowerPoint PPT Presentation
Transcript of Systems Approaches to Colorectal Cancer Care

Systems Approaches to Colorectal Cancer Care
Stephen D. Roberts
Brian Denton
Reha UzsoyEdward P. Fitts Department of Industrial and Systems Engineering
North Carolina State University
Raleigh NC, USA
3rd Annual Cancer Care Engineering Retreat

Colorectal Cancer (CRC)
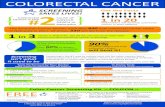
About 150,000 people diagnosed each yearSecond leading cause of cancer deathsAbout 90M people considered at risk

Key Characteristics
Cancer is a disease of the DNA Usually not symptomatic until advanced Deadly if not found early
Only 8.5% five-year survival if found late Over 90% five-year survival if found early
Risk factors include: Age, race, gender Personal or Family history Other related diseases Lifestyle (?) Diet (?)

Screening for CRC
Endoscopic Tests Colonoscopy Sigmoidoscopy
Non-Endoscopic Tests Fecal Occult Blood Test (FOBT) Double Contract Barium Enema (DCBE) Virtual Colonoscopy Fecal DNA

Treatment and Intervention Treatment
Surgery Resection: removal of “sections” of the colon
Ostomy
Chemotherapy Radiation Combination Therapy
Medical Screening Interventions Accepted Practice
Taught in Medical School (“experts”)
Stated in recognized Medical Literature
Recommended Guidelines American Cancer Society
American Gastroenterological Society

Systems Engineering for CRC Ongoing projects at NCSU Collaborations with
Vanderbilt University Medical Center and Health Services Research
University of North Carolina Chapel Hill ShepsCenter for Health Policy Research
Industry Medical Decision Modeling Inc.
Purdue CCE Project As of May 2008
Mayo Clinic
6

Work to date Focused on simulation models Effect of different screening policies on
population Population-level modeling of the natural history Cost-effectiveness of different screening policies
Effects of system design on the number of people seeking preventive screening Broader system including access to primary care
and screening facilities
Performance of endoscopy suites
7

Screening Decisions How “population-centric”?
age, gender, race, family history, compliance? What screening method?
Endoscopic and non-endoscopic When to start/stop screening? Protocol if screen is positive?
Verification and treatment Protocol if screen is negative?
Time to next screening When to stop screening

Evaluating medical decisions? Health burden
Mortality – life years Morbidity – quality-adjusted life years (QALY)
Cost burden Cost of intervention Cost of maintenance and surveillance
Value for cost Cost-effectiveness (CE): cost per QALY Cost-benefit (CB): net cost

Modeling Natural History Fundamentally stochastic Focus on the individual Intermediate relevant events
Start of disease (adenoma) Pathway and Progression
“Natural death” without the disease Marginal life expectancies Modify actuarial data (eliminating CRC)

Course of Disease (Natural History)
A1 – undetected first AdenomaA2 – undetected second Adenoma
C1 – invasive Cancer from A1C2 – invasive cancer from A2
CO – Colonoscopy/surgery to remove C1CD – Cancer DeathND – “Natural” Death
A10 A2 C1 CO CD ND C2
Medical TimelineBirth Death

Overall Software Design Strategy
Simulation Engine
User Interface
AccessDatabase
Results inExcel
Data Objects
Scenarios
CRC Variables
Report Writer
MedicalProtocolDesign
CRCExpertise

Sources of Data Cancer
National Cancer Institute (SEER) National Data
Centers for Disease Control (CDC) National Center for Health Statistics (NCHS) US Census Bureau Population Estimates Berkeley Mortality Statistics
Vanderbilt CRC Literature Database Validated based on Minnesota Colon cancer
Control Trial

Results Can be used to study a variety of aspects of
CRC progression and screening Health and cost burdens of CRC by population Effects of parameter uncertainty on the cost-
effectiveness of treatment options Cost-effectiveness of different screening
options based on willingness to pay for an additional QALY
14

Result: Health and Cost Burden of CRCGender Race Family history
Life Years Lost
QALYs Lost Costs of CRC
Female BlackNo Family
history10.83 (0.08) 10.24 (0.07) $123,714 (3736)
Female Black Family history 11.23 (0.06) 10.62 (0.05) $114,381 (2408)
Female WhiteNo Family
history11.68 (0.07) 10.99 (0.06) $124,875 (3320)
Female White Family history 12.15 (0.05) 11.45 (0.05) $118,188 (2283)
Male BlackNo Family
history10.19 (0.07) 9.74 (0.07) $110,460 (3188)
Male Black Family history 10.62 (0.05) 10.18 (0.05) $113,317 (2326)
Male WhiteNo Family
history 9.90 (0.06) 9.52 (0.06) $126,345 (3290)
Male White Family history 10.29 (0.05) 9.91 (0.04) $123,590 (2283)

Result: Effect of Colonoscopy Screening
ΔCost
ΔLifeYears(0,0)
$500
.100.040
.160
(F,B,N - $8,342)
(F,W,N - $4,008)
(M,B,N - $7,329)
(M,W,N - $2,571)
Higher (Poorer) Cost-Effectiveness
(F,B,F – Cost-Saving)
(F,W,F – Cost-Saving)(M,B,F – Cost-Saving)
(M,W,F – Cost-Saving)

Acceptability Curves
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 10 20 30 40 50 60 70 80
ThousandsCeiling Ratio
Pro
ba
bili
ty C
os
t-E
ffe
cti
ve
A: No Screening B: FOBT C: Sig D: Sig & FOBT E: Colon 10
A
E
DC
B
No Screening FOBT Colon 10
4.1 25.3
WTP (λ)

A broader view… Effective screening significantly reduces the
risks of CRC However, not all patients who could benefit
from screening receive it Estimate an additional 30,000 lives could be
saved annually if people would get screened How to improve the number of people who get
screened?
18

Combined simulation model Combines discrete event and continuous
(system dynamics) aspects Continuous variables change continuously
over time Level of awareness of CRC risk
Other variables change at discrete points in time Number of screening facilities
Used ARENA 7.0 software
19

Continuous component Uses causal loop representation to capture
relationships between quantities of interest Sterman(2000); Forester(1962)
Nodes represent variables, arcs causal relationships
Signs on arcs represent positive or negative correlation between variables
20

21

Results
22

Simulation of Endoscopy Suites Collaboration with Brian Denton of NCSU-ISE
and Mayo Clinic Examine the operational and design aspects
of endoscopy suites Clear relevance to the level of screening in the
population, cost of providing care
23

Endoscopy Process Patient Intake: patient checks-in,
administrative activities, gowning, patient roomed
Procedure: endoscopist enters room, patient sedated, colonoscopy starts, polyps removed, patient extubated
Recovery: post anesthesia care unit (PACU), patient discharged
Intake Procedure Recovery

Complicating Factors
Many types of resources: endoscopists, nurses, equipment, materials
High cost of resources and fixed time to complete activities
Large number of activities to be coordinated in a highly constrained environment
Uncertainty in duration of activities Many competing criteria

ModelP
atie
nt C
hec
k-in
W
aitin
g A
rea
PreoperativeWaiting Area
Procedure Rooms
Recovery Area
Pat
ient
Arr
ival
s
Pat
ient
Dis
char
ge
Intake Area
Dependent (Waiting)
Independent (Process)
Dependent (Waiting)
Independent (Process)
Dependent (Waiting)
Independent (Process)

General Insights
Economies of Scale: No observed efficiencies in patient throughput due to increasing the number of Ors. Some benefits for up and down stream resources.
Turn-over Times: The impact of reducing turnover times for ORs on all performance measures is limited to staffing scenarios is which endoscopists have 1 or 1.5 ORs.
Utilization: The maximum achievable endoscopist utilization is 90% and the maximum achievable OR utilization is 67%.

Some conclusions Systems engineering techniques can be
deployed effectively to support the CRC care cycle (continuum)
Effective collaboration with health care providers and health services researchers is critical
Data collection to parameterize and validate models is a major effort
Increased networking among researchers will allow us to leverage each others’ efforts
28

Future directions Continue to develop and enhance simulation
models Treatment pathways?
Extend from simulation to optimization models Determine number and location of CRC
screening facilities Explicitly consider demographics, queueing
effects of capacity on wait times, travel distances affecting demand
Build on work in supply chain network design with lead time aspects
29

Validation Overall Characteristics
SEER Data, Life-Table, Prior Model Screening Validation: Minnesota Colon
Cancer Control Study Use FOBT relative to no screening (from 1975
through 1977 and followed until 1991 Randomized trial of three groups: annual
screening, biennial screening, and no screening Simulated population fit to Minnesota trial
population Some parameters had to be modified to be consistent
with the inputs reported


Graphical Interpretation:Cost-Effectiveness Plane
ΔCost
ΔEffect(0,0)
Greater Cost, Greater Effect
Less Cost, Greater Effect
Greater Cost, Less Effect
Less Cost, Less Effect
Unacceptable
Cost Saving
CE > 0

Results
Willingness to Pay (λ) Screening Method
λ≤ $4,100/QALY No Screening
$4,100/QALY <λ
λ≤ $25,300/QALYFOBT
λ> $25,300/QALY Colon 10

34

Why Simulation Not readily Markovian
No geometric or exponential state occupancy State explosion to achieve memorylessproperty
(due to age, gender, race, family history)
Concurrent multiple precursors to CRC Multivariate and time-dependent processes
(depend on person and adenoma state) Discrete-Event System (variable time
updating) Object-Oriented