systemic manifestations of skin disease
47
Skin Manifestations of Systemic Disease Dr Binita Guha-Niyogi ST6 Dermatology Email: [email protected]
Transcript of systemic manifestations of skin disease

Skin Manifestations of
Systemic Disease
Dr Binita Guha-Niyogi
ST6 Dermatology
Email: [email protected]

Aims
• To provide an overview of the dermatological manifestations associated with common systemic diseases
• To address some of competences outlined in the curriculum
• The trainee should be able to:
• Assess the patient
• Produce a valid differential diagnosis
• Investigate appropriately
• Consider when a biopsy is appropriate
• Formulate and implement a management plan for the acute period of care

Question 135 year old lady with a rash over her knees and elbows for a few years.
Improves with sunlight and worse with stress.
1. What is the diagnosis?2. List 2 nail signs associated with this condition? 3. Give 2 medical conditions associated with this diagnosis?

Psoriasis
• Well demarcated erythematous, scaly plaques
• Abnormal T cell activation, increased epidermal turnover, genetic (HLA)
Triggers• Trauma • Infection (Strep)• Stress• Medications
• Lithium, B-blockers, Antimalarial, ACEi, NSAIDS, Withdrawal of PO Steroids, G-CSF, INF

Psoriasis
Nail signs• Pitting
• Onycholysis
• Discolouration - Leukonychia
• Subungal hyperkeratosis
• Oil Spot
• Splinter haemorrhages
Medical Associations • Arthritis
• IBD
• Obesity
• Cardiovascular disease, HTN, Dyslipidaemia
Treatment• Topicals
• Steroids, Vit D3 analogue, calcineurin inhibitors
• Systemics
• Acitretin, MTX, Ciclosporin
• Phototherapy
• Biologics

Question 235 year old lady who is currently investigated for joint pains, develops a
photosensitive facial rash.
1. What is the likely diagnosis?
2. Name a blood test that you would like to perform.

Systemic lupus erythematosus (SLE)
Multiorgan (4/11)
•Malar erythema, DLE, oral ulcers
•Photosensitivity
•Haematological disorder
•Nephropathy
•Arthritis
•Serositis
•Neurologic disorder
•ANA, Immunologic (dsDNA ,anti- Sm)
Other bloods: FBC, C3,C4
•Other skin features:Alopecia, Raynaud’s, Livedo reticularis, Acrocyanosis, Urticarial vasculitis

SLE
Drug Induced SLE
• Hydralazine, Procainamide, INH, Quinidine, PUVA, Minocycline, D-Penicillamine
• Skin biopsy
– Lymphocytic infiltrate
– Dermal mucin
Treatment
•Top Steroid/calcineurin inhibitor
•Antimalarials – HCQ
•Steroid Sparing Agent
•Sun protection
Differentials for facial rash:•DLE•Rosacea•Seborrhoeic dermatitis•Dermatomyositis

Question 379 year old lady complains of tightening of her fingers and facial skin
for some years
1. What is the diagnosis? 2. Give two symptoms would you enquire about?

Systemic Sclerosis
• Scleroderma is a group of AI disorders: Morphoea, Systemic Sclerosis, CREST
• AI inflammatory condition
• Characterised by inflammation,
fibrosis and vasculopathy
• Underlying mechanisms are complex and largely unknown
• >Women (30-50yrs)
• African-Americans (early onset/ diffuse)

Systemic Sclerosis
Skin•Pruritus•Oedema of digits ->sclerosis, ulcers•‘Mask-like’ Face•Dyspigmentation•Calcinosis cutis
Vascular• Raynaud’s Phenomenon
Other•GI symptoms (reflux, dysphagia),•SOB (ILD, pulm HTN)•Cardiac•Renal•Synovitis (Symmetrical), migratory polyarthritis

Systemic Sclerosis
Investigations
• Bloods:
• ANA
• Anti-SCL-70
• Anti-Fibrillarin
• Anti-centromere
• Anti-RNA Polymerase
• Skin Biopsy
• Collagen deposition
• Loss of s/c fat
Treatment
• Raynauds: • Avoid cold temperatures,
Nifedipine, Low dose aspirin, PGE1
• Ulcers: Bosentan
• Prostacyclin
• Immunosuppressant
• D-penicillamine
• ACEi

CREST
• Limited form of sclerosis
• Calcinosis
• Raynaud’s Phenomenon
• E oesphageal involvement
• S clerodactyly
• T elangiectasia
• Anticentromere Abs
• Rarely progresses to SSc
• Better prognosis than SSc

Question 422 year old woman presents with a sore throat and rash to her legs
1. What is this eruption?
2. Give two possible causes for this eruption?

Erythema Nodosum• >Women
• Tender red s/c nodules may ’bruise-like’
• >Symmetrical Pre-tibial areas
• +/- fever, arthralgia, malaise
Causes• Infection- viral, strep, salmonella,
campylobacter, TB, leprosy, fungi
• Drugs – OCP, sulphonamides, penicillin,NSAIDs
• Inflammatory – Crohn’s > UC, Behcet’s
• Sarcoidosis - (Good prognostic sign)
• Malignancy – lymphoma
• Pregnancy
• Idiopathic (30%)

Erythema Nodosum
Investigations• Skin biopsy: Septal
panniculitis
• Throat swabs
• FBC, CRP, ESR, ASOT
• CXR
• Quantiferon
Treatment
• Often self limiting
• If mild subsides 3-6 weeks
• Treat underlying cause
• Bed rest
• NSAIDs
• Doxycycline
• Prednisolone

Question 540 year old woman presents with a gradual history of skin changes over her
lower legs. She is otherwise well.
1. What is the diagnosis? 2. Give one investigation would you like to perform?

Necrobiosis lipoidica
• Well defined yellow/red-brown atrophic/indurated waxy plaques
• Surface telangiectasia +/-ulceration
• Pretibial areas
• 30-40% have DM
• Only 0.03-3% with DM present with NLD
• Check Blood glucose
• Skin biopsy: – Histiocytes encircle necrobiotic
collagen in dermis +/-sclerosis, granulomatous inflammation
Treatment
• Potent topical steroid: Dermovate + occlusion
• Others• IL Steroid, Aspirin
+Dipyridamole, Nicatinamide, Ciclosporin, Biologics, PUVA, PDT

Skin Manifestations in Diabetes
• Acanthosis Nigricans
• Bullous diabeticorum
• Diabetic dermopathy
• Disseminated GA
• Scleroedema of Buschke
• Eruptive xanthomas
• Ulcers
• Diabetic neuropathy

Question 640 year old man complains of increased appetite and skin changes over
lower legs
1. What is the diagnosis? 2. Where else would you like to examine? Give 2 other sites.

Pretibial Myxoedema (Grave’s Disease)
• Elevated lesions on the skin
• Skin is shiny with ‘orange peel’ appearance
Other sites to examine
• Eyes - exopthalmos• Thyroid - enlargement, nodules• Nails - Thyroid acropachy onycholysis• Hair - diffuse thinning• Tremor
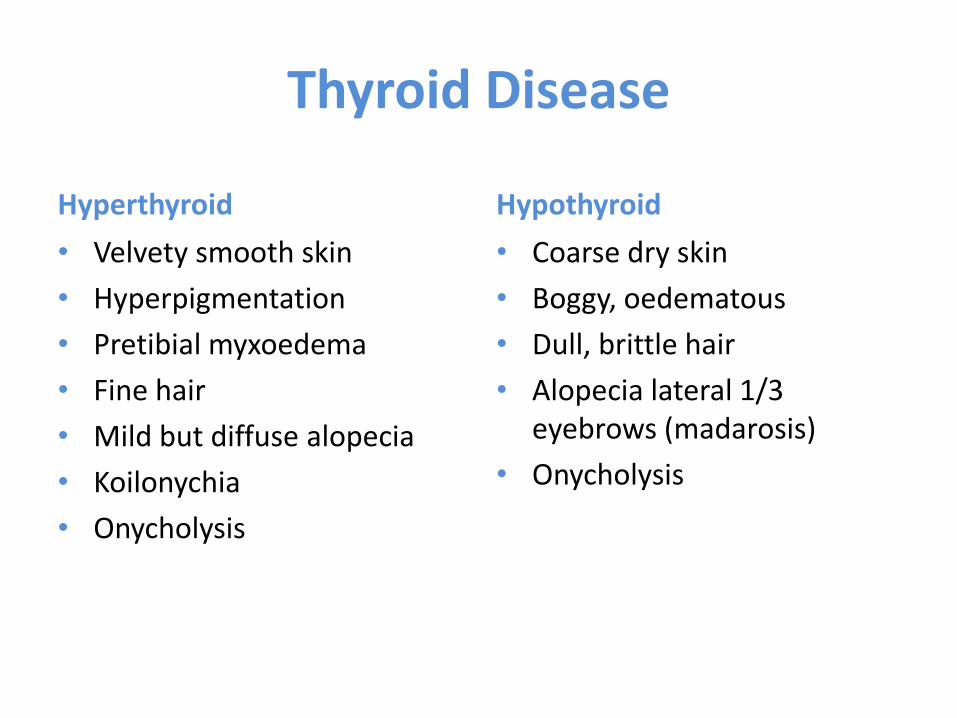
Thyroid Disease
Hyperthyroid
• Velvety smooth skin
• Hyperpigmentation
• Pretibial myxoedema
• Fine hair
• Mild but diffuse alopecia
• Koilonychia
• Onycholysis
Hypothyroid
• Coarse dry skin
• Boggy, oedematous
• Dull, brittle hair
• Alopecia lateral 1/3 eyebrows (madarosis)
• Onycholysis

Question 730 year old male with ulcerative colitis develops a painful ulcer on his lower
legs within the last few weeks
1. What is the diagnosis? 2. Give one condition which can be associated with this type of ulcer.

Pyoderma Gangrenosum
• Starts as papule/nodule
• Rapidly expanding ulceration with undermined border and violet/bluish edge
AssociationsIBDRA , Ankylosing spondylitisHaematological malignancyHepatitis, PBC NeoplasiaPost-trauma

Pyoderma Gangrenosum
Diagnosis• Clinical features • +ve pathergy test• Skin biopsy: Neutrophilic
inflammatory infiltrate -> Necrotic• May have +ve pANCA• Swabs
Treatment• Treat infection• Top Dermovate• PO Doxy • Dressings +/- compression• If larger: Po Steroids +/- steroid
sparing agent

Question 8An 80 year old man presented with chronic ulcers over the lower legs.
1. What is the cause of her leg ulcers? 2. How would you manage these ulcers?

Venous Insufficiency
• Itchy red, blistered, crusted plaques, dry, fissured
• Orange-brown macular pigmentation (Haemosiderin)
• Atrophie blanche• White irregular scars surrounded by red
spots
• “Champagne bottle”• Lipodermatosclerosis

Venous Insufficiency
Risk Factors
• Varicose veins/DVT
• Hx of cellulitis
• Chronic swelling aggravated by hot weather and prolonged standing
• Venous leg ulcers
Treatment
• Elevation
• Treat 2ry infection
• Topical Steroids/Emollients
• Potassium permangenate
• Compression (Need ABPIs)
• ?Need to treat veins
Complications:
• Infection, Secondary eczema, Contact allergy

Question 9A 65 year old woman presented with lethargy, pyrexia and a palpable rash.
1. Describe this rash? 2. Give a possible underlying cause.

Vasculitis
• Palpable Purpura, papules, vesicles, macules -> Necrotic, ulcers, oedema
• > Dependent sites
• +/- fever, arthralgia, myalgia, weight loss
Causes •Infection•Drugs-Penicillin, NSAIDs,
COX2-inhibitors, ACEi, Allopurinol, furosemide
•Inflammatory – IBD, AI
•Malignancy•50% Idiopathic

Vasculitis
• Prognosis depends on systemic involvement
• Vasculitis screen
• ANA, ANCA, Ig and electrophoresis, complement, haematinics, Cryoglobulins, FBC, U&Es, LFTs
• Urine Dip/PCR
• BP
• Skin biopsy
Treatment
• Remove trigger
• Supportive therapy
• 90% Spontaneously resolve
• Top Dermovate
• Prednisolone
• Immunosuppressant
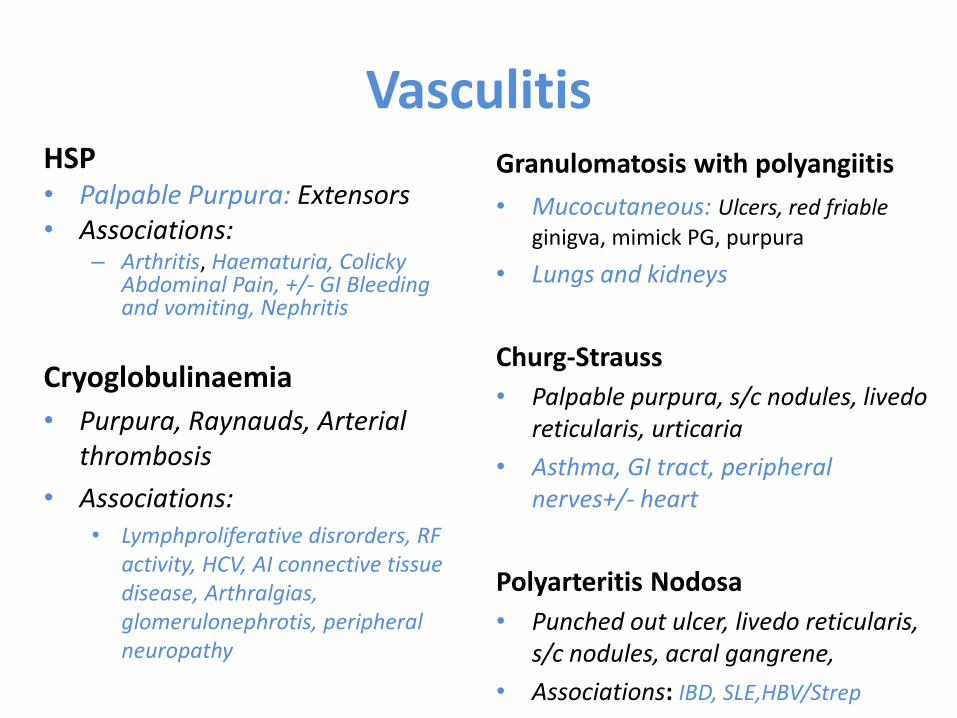
VasculitisHSP• Palpable Purpura: Extensors• Associations:
– Arthritis, Haematuria, Colicky Abdominal Pain, +/- GI Bleeding and vomiting, Nephritis
Cryoglobulinaemia
• Purpura, Raynauds, Arterial thrombosis
• Associations:• Lymphproliferative disrorders, RF
activity, HCV, AI connective tissue disease, Arthralgias, glomerulonephrotis, peripheral neuropathy
Granulomatosis with polyangiitis
• Mucocutaneous: Ulcers, red friable
ginigva, mimick PG, purpura
• Lungs and kidneys
Churg-Strauss
• Palpable purpura, s/c nodules, livedoreticularis, urticaria
• Asthma, GI tract, peripheral nerves+/- heart
Polyarteritis Nodosa
• Punched out ulcer, livedo reticularis, s/c nodules, acral gangrene,
• Associations: IBD, SLE,HBV/Strep

Question 1050 year old woman is under the respiratory team with SOB, joint pains and
general fatigue. A rash is noted:
1. What is the likely diagnosis?
2. What tests would you like to perform?

Lupus Pernio - Sarcoidosis
• Chronic multisystem granulomatous disease
• 30-40% present with skin findings
Specific
• Skin coloured-red/brown annular papules/plaques
• Lupus pernio
• S/C nodules
• Infiltration of old scars
Non-Specific
• EN, EM, nummular eczema, calcinosis cutis, pruritus, Hypopigmentation, scarring alopecia, ulcers, ichthyosis

Sarcoidosis
• Lung function tests
• Exclude TB
• ECG
• CXR
Treatment
• Top/IL/PO steroids
• HCQ
• MTX/steroid sparing agents
Can affect other organs:
• Eye 20-30%
• Liver 30-40%
• Heart 5-25%
• Nervous system 1-5%
• Musculoskeletal 2-38%
Investigation
• Raised ACE, calcium, ESR
• Skin biopsy– Non-caseating granulomas
– Asteroid bodies and Schaumannbodies in giant cells

Question 11 A 60 year old woman presented with itching, burning rash on the face,
recently had difficulty combing her hair and walking up the stairs
1. What is the cause of her symptoms? 2. What’s associated with this condition?

Dermatomyositis
• Chronic Inflammatory dermatomyopathy
• Skin changes usually 2-3 months before muscle weakness (proximal symmetrical)
• +/- fever, malaise
• Can get cardiac and respiratory involvement
• 15–50% have an underlying malignancy• Lung/GI >Men• Ovaries/Breast > Women
Heliotrope Rash
Gottron’s papules
Gottron’s sign
Samitz Sign
Poikiloderma
Mechanic’s Hands
Calcinosis Cutis

Dermatomyositis
Investigations
• Bloods:– Myositis screen
– ANA (60%), CK (90%) aldolase, ESR, transaminases (AST), LDH
• Skin biopsy: – Atrophic epidermis, mucin,
lymphocytic infiltrate (Lupus picture), dermal sclerosis
• Muscle Biopsy, EMG, MRI
• Screen for malignancy
Treatment
• PO Steroids
• +/- Steroid sparing agent
• HCQ and Sun protection
• Diltiazem/Colchicine
• Bed rest/Physio
• Resolves in 1/5

Question 12 60 year old lady with ESRF has regular dialysis, she’s recently noticed tender
lesions developing on her legs
1. What is the skin condition?

Calciphylaxis
• Rare
• >ESRF on HD
• Post renal Tx with elevated Ca-Phosphate product
• Systemic calcification of small/medium vessels
• Ischaemic necrosis of skin and soft tissue
• Skin
• Painful violaceous mottling (reticulated)
• >Lower limbs
• Purpura with central necrosis +/- bulla
• Necrosis and ulceration
• High mortality associated with gangrene and sepsis

Calciphylaxis
Treatment
• Normalise Calcium and phosphate product (low calcium dialysis)
• Sodium thiosulfate (increase solubility of Calcium deposits)
• Bisphosphonates
• Calcimimetics
• Parathyroidectomy

End Stage Renal Disease
• Pruritus
• Uremic Frost
• Acquired perforating disorder
• Nephrogenic Systemic Fibrosis

Question 13A 70 year old gentleman has been itchy for over a year.
1. What investigations would you like to do?
Pruritus
• Localised or Generalised
Localised
Skin (Primary rash)• Eczema, seborrhoeic eczema,
contact dermatitis• Head lice, scabies, candida, tinea• Lichen planus, Lichen sclerosus• Bullous Pemphigoid
Nerves• Hypersensitive nerves• (+/- reduced/absent sweating)
Often present
• Excoriations
• Lichenification
• Lichen simplex
• Prurigo Nodularis

Pruritus
Investigations• Review medications• Lymph nodes• Bloods:
• FBC, U&Es, Extended LFTs• TFTs, glucose• ?BBV screen• Ig and electrophoresis• Haematinics• Skin autoantibodies
• Urine dip
Treatment
• Depends on cause
Skin
• Treat primary skin rash
• Cooling cream:
• Menthol in aqueous
• Emollients
• Antihistamines
• Topical steroids
• Amitryptylline/Gabapentin

Outcomes
• Recognise the dermatological manifestations associated with common systemic diseases
• How to assess the patient
• Consider differential diagnoses
• Investigate appropriately
• Known when a biopsy is appropriate
• Formulate and implement a management plan for acute period of care

Questions?