![Euclid - Elements Commented]](https://static.fdocuments.net/doc/165x107/546d1c4fb4af9fd06d8b4579/euclid-elements-commented.jpg)
System Leadership Board – Meeting in Public – Agenda ... · ESSD Extend Early Supported Stroke...
129
NO ITEM LEAD FORMAT PURPOSE TIME 1. Welcome and apologies for absence RT Verbal To note 10.30 2. Declarations of Interest RT Verbal To note 3. Minutes of the last meeting held on 2 May 2019 RT Enc. To approve 4. Matters Arising and action log update DS Enc. To note OUR TEAMS 5. Presentation from our teams on delivering improvements in care: • Dementia Action Alliance film CD/PC Presentation/ Video To note 10.35 SYSTEM DEVELOPMENT 6. National & Regional – an update on developments • ICS Maturity matrix SE Verbal Enc. To note 11.00 7. Organisational Form Transaction - an update on the work between Cumbria Partnership NHS FT and North Cumbria University Hospitals NHS Trust SE Enc. To note 11.10 8. Stakeholder Engagement – an update on developments and key events in the future JR Enc. To note 11.15 9. Third Sector – an update on the work in support of the delivery of our Strategy CE Enc. To note 11.20 STRATEGY 10. Mental Health, Learning Disabilities & CAMHS SE Verbal To note 11.30 11. North Cumbria Health & Care Strategy 2019-2024 – an update on the development of our Strategy in line with the NHS Long Term Plan RD Encs. To note 11.35 12. Aligning System Strategies –updates on: 1. Population Health Framework & Plan 2. Cumbria Health & Wellbeing Strategy JH Enc Verbal To note 11.40 13. Primary Care Networks – update on the development in line with the NHS Long Term Plan NMcG/ MA Verbal To note 11.50 System Leadership Board – Meeting in Public – Agenda Thursday 4 July 2019 at 10.30 – 12.30 Venue: LEP Conference Centre, Redhills, Penrith, CA11 0DT
Transcript of System Leadership Board – Meeting in Public – Agenda ... · ESSD Extend Early Supported Stroke...

NO ITEM LEAD FORMAT PURPOSE TIME 1. Welcome and apologies for absence RT Verbal To note 10.30 2. Declarations of Interest RT Verbal To note
3. Minutes of the last meeting held on2 May 2019
RT Enc. To approve
4. Matters Arising and action log update DS Enc. To note
OUR TEAMS
5. Presentation from our teams on deliveringimprovements in care:• Dementia Action Alliance film CD/PC
Presentation/Video To note 10.35
SYSTEM DEVELOPMENT
6. National & Regional – an update ondevelopments• ICS Maturity matrix
SE Verbal
Enc.
To note 11.00
7. Organisational Form Transaction - anupdate on the work between CumbriaPartnership NHS FT and North CumbriaUniversity Hospitals NHS Trust
SE Enc. To note 11.10
8. Stakeholder Engagement – an update ondevelopments and key events in the future
JR Enc. To note 11.15
9. Third Sector – an update on the work insupport of the delivery of our Strategy
CE Enc. To note 11.20
STRATEGY
10. Mental Health, Learning Disabilities &CAMHS
SE Verbal To note 11.30
11. North Cumbria Health & Care Strategy2019-2024 – an update on the developmentof our Strategy in line with the NHS LongTerm Plan
RD Encs. To note 11.35
12. Aligning System Strategies –updates on:1. Population Health Framework & Plan2. Cumbria Health & Wellbeing Strategy
JH Enc Verbal
To note 11.40
13. Primary Care Networks – update on thedevelopment in line with the NHS LongTerm Plan
NMcG/MA
Verbal To note 11.50
System Leadership Board – Meeting in Public – Agenda Thursday 4 July 2019 at 10.30 – 12.30 Venue: LEP Conference Centre, Redhills, Penrith, CA11 0DT

DELIVERY 14. Learning Disability Services – an update
providing assurance on service provision VC Verbal To note 12.05
15. People Plan – an update on issues and delivery of the plan
JT Verbal To note 12.15
OTHER ISSUES 16. Questions from members of the public
relating to the agenda items RT Verbal For
discussion 12.25
17. Any Other Urgent Business FUTURE MEETINGS 2019/20: 10.30 – 12.30 5 September 2019 7 November 2019 (No meetings in January) 5 March 2020
Membership Organisations Role Name North Cumbria University NHS Trust
1 Chair [email protected] 2 Non-Executive Director [email protected] 3 Joint Chief Executive [email protected] 4 Deputy CEO [email protected]
Cumbria Partnership NHS FT
5 Chair [email protected] 6 Non-Executive Director [email protected] / Joint Chief Executive [email protected] / Deputy CEO [email protected]
NC CCG 7 Accountable Officer [email protected] 8 Chair [email protected] 9 Lay Member [email protected] 10 Chief Operating Officer [email protected]
Cumbria County Council* 11 Director of Public Health [email protected] 12 Assistant Director of
Adult Social Care [email protected]
13 Assistant Director – Integration & Partnerships
14* Cabinet Member for Public Health
15* Cabinet Member for Health & Care
General Practice 16 17
GP ICC Lead Representative(s) x 2
Niall McGreevy (NMG) ICC GP Lead, CCG Mark Alban (MA) ICC GP Lead, CCG
*Agenda and papers to be copied to 14,15 and [email protected] [email protected] Note: Other Directors and Officers may be required to attend for specific items

In attendance: Julian Auckland Lewis, Programme Director | Ramona Duguid, Executive Director of Strategy | Alison Smith, System Executive Chief Nurse | Judith Toland, System Executive Director of People & Digital | Mandy Nagra, System Executive Chief Operating Officer | Vince Connolly, System Medical Director | Daniel Scheffer, Joint Company Secretary CPFT & NCUHT | Julie Clayton, Head of Communications, NCCCG | Michael Smillie, Executive Director of Finance & Estates | Charles Welbourn, Chief Finance Officer, NCCCG | Clare Edwards, Health Partnerships Officer, Cumbria CVS | David Blacklock, Healthwatch Cumbria CEO | John Lawlor, NTW CEO | Francesca Bee, Corporate Governance Administrator, CPFT Presenters: Carol Desborough, Carer and Pauline Carlyle, OT, CPFT
GLOSSARY
Abbrev. In full AF Atrial Fibrillation AHP’s Approved Health Professionals CAMHS Child and Adolescent Mental Health Services CIC Cumberland Infirmary, Carlisle CT Computerised Tomography CVD Cardio Vascular Disease ESSD Extend Early Supported Stroke Discharge HASU Hyper Acute Stroke Unit IHCS Integrated Health and Care System JD Job Description LD Learning disabilities LOS Length Of Stay MDT Multi-Disciplinary Teams MH Mental Health MLU Midwife Led Unit MRI Magnetic Resonance Imaging MSK Muscular Skeletal RCPCH Royal College of Psychiatry SRO Senior Responsible Officer SSPAU Short Stay Paediatric Assessment Unit TOR Terms of Reference WCH West Cumberland Hospital, Whitehaven

UNCONFIRMED MINUTES OF SYSTEM LEADERSHIP BOARD PUBLIC MEETING HELD ON 2 MAY 2019
Members Present: NCUH CPFT NCCCG GP
Representatives CCC
Prof. Robin Talbot, Chair Mr Jon Rush, Chair
Dr Mark Alban, ICC GP Lead (NC CCG)
Mr Colin Cox, Director of Public Health
Prof. Stephen Eames, Chief Executive
Mr Peter Rooney, COO
Dr Niall McGreevy ICC GP Lead (NCCCG)
Prof. John Howarth, Deputy Chief Executive/ System Clinical Lead Mr Malcolm Cook, NED
Ms Heike Horsburgh, NED
In Attendance: Mrs Ramona Duguid, Director of Strategy (ICS)
Ms Julie Clayton, Head of Communications (NC CCG)
Ms Patricia Bell, Cabinet Member for Health & Care (CCC)
Mr Daniel Scheffer, Company Secretary (CPFT/NCUH)
Miss Fran Bee, Corporate Governance Admin (CPFT)
Mr Kevin Windebank, Lay Member (NCCCG)
Clare Edwards Health Partnerships Officer (CVS)
Helen Horne, Chair, (Healthwatch Cumbria)
Elspeth Desert, Consultant Clinical Psychologist (NCUH)
Joanna Manley, Network Manager, Physical Health & Rehab Psychology (CPFT)
Ruth O’Dowd, Consultant Anaesthetist (NCUH) Apologies: Ms Judith Toland, System Director of Workforce & OD
Ms Catherine Whalley, Assistant Director of ASC (CCC)
Mr David Rogers, AO (NCCCG)
Mr Julian Auckland-Lewis, Programme Director (NCUHT)
Ms Alison Smith, System Executive Chief Nurse
V1 Page 1 of 6 File Ref: SLB

Agenda No.
Minute
Action by
1. Welcome and Apologies for Absence Prof. Robin Talbot, Chair welcomed everyone to the public meeting of the System Leadership Board (SLB) and apologies were noted. There were a few members of the public in attendance.
2. Declarations of Interest There were no declarations of interest. Helen Horne, Chair Healthwatch Cumbria declared with regards to CQC. Helen is a member of Healthwatch England Committee and receives remuneration from CQC.
3. Minutes of the previous public meeting held on 7 March 2019 Minutes of the Public System Leadership Board meeting held on 7 March 2019 were approved.
4. Matters Arising and action log update Action Log SLB5 closed as Colin Cox providing an update at Item 12
OUR TEAMS 5. Presentation from our teams on delivery improvements in care:
‘Familiar Faces’ by Elspeth Desert, Consultant Clinical Psychologist Elspeth Desert talked about this new service ‘Familiar Faces’ which has been developed in north Cumbria to address the needs of patients with complex issues who are often termed ‘frequent attenders’. This service started 18 months ago and is embedded in three of the ICCs in north Cumbria. Priority for the 2019/20 is to embed into the remaining five ICCs offering equity of service and significant release of resource for the system. Malcolm Cook commented that this is a fantastic scheme in place looking at the whole system. Heike Horsburgh commented that Cumbria is benefiting from this service but wondered about young people in crisis and their repeat attendance plus their parents/carers repeat visits to GPs and what we might be doing about that. Patricia Bell commented that the results look really promising and how are we as a system supporting work at the lower levels Colin Cox commented that this approach works and proves that changes to restructuring our workforce to do things differently can work well. John Howarth commented that there are life changing interventions which we hope to sustain and raising awareness in the system. Peter Rooney commented that we need to get to psychological informed services everywhere so we need to educate our workforce to recognise stress and trauma and delivery appropriate intervention.
V1 Page 2 of 6 File Ref: SLB

Stephen Eames commented that within the new people plan there is a focus on mental health and wellbeing, connect with this and in public health that we need to consider how this can be taken forward. ACTION SLB6 – Judith Toland to be asked to talk about how public health and wellbeing could be taken forward in the People Plan at July meeting. Robin thanked Stephen for the action and thanked Elspeth, Joanna and team for all their good work.
SE/DS
6. Patient Safety Faculty/Stop the Line by Rod Harpin, Medical Director and Ruth O’Dowd, Consultant Anaesthetist Prof. Robin Talbot welcomed Rod Harpin and Ruth O’Dowd and congratulated Ruth on her appointment as a Generation Q Fellow of the Health Foundation. The presentation introduced the patient safety faculty who are championing safe, reliable and effective care across our healthcare system. The Stop the Line communication tool is about addressing something urgent that needs to be immediately resolved and is complimentary to ‘speak out safely’ and ‘freedom to speak up’. Staff are encouraged and supported to feel safe to report patient safety events, near misses or potential problems and managers must stop what they are doing to resolve the issue quickly. Staff are part of the improvement process and are recognised as such with feedback continuing to make things better. Heike Horsburgh asked how we manage the emotional safety of our patients on mental health wards and would this be part of the training. Rod Harpin acknowledged the point about patients and advised that Stop the line is currently about educating and supporting staff however the next step in coproduction would be to involve patients. Malcolm Cook commented that Stop the Line is a culture which needs to be embedded in the whole system. Stephen Eames commented that Stop the Line has started within the Acute Hospital setting but the SLB needs to understand the connectivity within the system to improve the quality of services and less incidents for patients. Patricia Bell commented that discharge pathways in social care need to consider this as a future development. Prof Robin Talbot thanked the presenters and would welcome them back to hear about future developments.
NATIONAL/REGIONAL/LOCAL DEVELOPMENT UPDATES The following items taken after Item 12 7. National and Regional Updates
Stephen Eames advised there was nothing significant to report at this time.
8. CPFT/NCUHT Organisational Form Update Stephen Eames referred to the paper circulated with the agenda and advised that the critical meeting with NHSI is due to take place mid-May
V1 Page 3 of 6 File Ref: SLB

and hopefully will allow us to continue to plan for October which aligns with the changes in providers for the mental health services. Helen Horne asked about the engagement activity of these plans with stakeholders and the public and would be keen to be involved. Daniel Scheffer commented that Sue Stevenson (Healthwatch Cumbria) has been involved in developing the survey which has helped and would welcome further involvement.
9. Stakeholder Engagement Update Jon Rush advised on 13 engagement events with stakeholders since the last meeting. Engagement within the third sector is encouraging although a lot still to do. We would like to map engagement over an annual basis which would be a good visual and help identify any gaps. Jon asked colleagues to drop a note to the CCG communications team to identify who, when and where so that this can be included in the map. The SLB agreed to do this. ACTION SLB7
ALL
10. Third Sector Programme Update Clare Edwards provided a report with the papers which shows the progress made since last report and highlighted a case study on the Lighthouse Project which is a calm, safe and comfortable place for people in Carlisle and Eden to visit when they are experiencing a mental health crisis, feeling unsafe and finding it hard to cope. The report also highlighted an additional issue on social prescribing and Clare put forward a recommendation that the north Cumbria system urgently needs to consider significant investment into the third sector to support the sector to meet the increased demands. In terms of Clare’s role it is coming to the end of the first 12 months of her post in operation and a range of priorities are currently to be agreed for the final year of her post. Patricia Bell commented that she was concerned about capacity in the third sector more widely and especially hoped this can be looked at again in the next few months. In all the communities the few constants are a church person, a politician and parish council; are we engaged with these people in the best possible way? There are local networks of people helping each other that are not know to us. Stephen Eames commented that there are significant opportunities to make stronger links. Capacity issues in the third sector is a priority issue and we have made a great start and further discussions are needed when Clare reports again at the July meeting. Prof Robin Talbot thanked Clare for her report and the discussion this has raised and offered if it would help, he can make contact with the Bishops office. A future presentation could show third sector/community groups that are working together.
V1 Page 4 of 6 File Ref: SLB

Strategy
11. Updating our strategy in line with the NHS Long Term Plan Ramona Duguid advised that work has been undertaken in the last 3 months to refresh our strategy in line with the NHS Long term plan and discussions have taken place with the provider boards and the CCG. A copy was circulated with the agenda. Ramona highlighted some key points and asked the SLB to endorse the engagement narrative. Engagement work will be undertaken with staff and key stakeholders starting next week. Patricia Bell liked the strategy but asked whether the community will commit to it. The ‘Wigan Deal’ is interesting and simple. There needs to be a culture change in the community to look at the NHS in a different way. Ramona responded that feedback so far has reiterated those comments and the strategy will be revised following engagement with and feedback from our local communities. The SLB endorsed the engagement narrative.
12 This item was taken after Item 6 to allow CC to leave the meeting. Aligning System Strategies 12.1 Cumbria Health & Wellbeing Strategy Colin Cox identified that this strategy is owned by Cumbria Health & Wellbeing Board and it is a requirement for the LA and CCGs to produce. This is a long term strategy aligning to the NHS Long term plans and was signed off by the Board on 18 April 2019. It is the intention that the North Cumbria System strategy will take into account and sign up to what is in the countywide strategy. Next steps are the development of an outcomes framework which will be monitored by the H&W Board. The SLB endorsed the strategy. 12.2 Population Health Update Colin Cox advised that now the H&W strategy is in place there are a number of other things that help take it forward. The population health framework will continue to be developed and brought back to the next meeting. Colin advised that an IT system due to be launched soon will support the population health management which again will be reported back to SLB. Helen Horne, Chair of Healthwatch Cumbria commented that she is uplifted by all the work being done on population health and prevention and can fully understand why North Cumbria is one of the 14 areas going forward to an ICS and having attended a recent meeting with staff, is impressed by the commitment of the staff working towards the same goal which she had not come across before and wanted to praise the work being done in public.
V1 Page 5 of 6 File Ref: SLB
Delivery
13. Annual Plan Delivery 2019/20 Ramona Duguid advised that discussions have taken place with the provider boards and the CCG. Important to note here that we have one system plan which endorses our system working. Our first quarter report will be presented at the July meeting. The SLB noted the plan.
RD
14. People Plan Due to family issues Judith has been unable to attend today and this will be brought back to the July meeting.
JT
15. Quality Metrics In Alison’s absence Daniel Scheffer advised that work continues and should be completed by the end of June and an update will be provided at the July meeting.
AS
16. MH/CAMHS/LD Update Stephen Eames advised that everyone will be aware of the changes to providers in the north and south Cumbria. All should be concluded by October 2019. In north Cumbria, Northumberland, Tyne and Wear FT will be a key partner and Chief Executive, John Lawlor will join the SLB.
Governance
17. Questions from the public relating to the agenda items Les Blacklock, Staff Governor CPFT raised awareness of the Delirium Reach Out Teams based in Carlisle and West Cumberland hospitals have been nominated for a national award. Les also raised concern about the third sector where in particular in north Copeland two day centres have closed and Age UK continues to retract their business. The impact is on health and wellbeing of patients and carers needing day care provision. Patricia Bell commented that she has been following this issue and asked to have a discussion outside of this forum.
18. Any Other Business None Raised.
Closing comments: Prof. Robin Talbot brought the Board’s awareness to the information items and the date of the next meeting and thanked everyone. Date, time and venue of next meeting in the LEP Conference Centre, Redhills, Penrith - 4 July 2019, 10.30 – 12.00
Confirmed minutes approved by: ………………………………………………………………… Date: ……………………………… Prof. Robin Talbot, Chair
V1 Page 6 of 6 File Ref: SLB

System Leadership Public Board North Cumbria Health Care
28/06/2019 File Ref: SLB
2018/19 SLB6 02/05/2019 5
How public health and wellbeing could be taken forward in the People Plan at July meeting.
Judith Toland to be asked to talk about how public health and wellbeing could be taken forward in the People Plan at July meeting.
ICS JT 04/07/201921/6/19 - The integrated workforce strategy is under development and this along with an action plan will be brought to the September meeting
2018/19 SLB7 02/05/2019 9
All engagement with stakeholders to be mapped on an annual basis.
All members of the SLB to contact the CCG Communicaitons Team to advise them who, when and where they have engaged throughout the coming year
CCG JR 30/04/2020
Issue to be addressed (why do we need an action?)
SYSTEM LEADERSHIP PUBLIC BOARD ACTION LOG
Update Report
Action Complete (Propose Yes/Yes/
No)
Action No Date of Meeting Agenda Item Action Lead Timescale
ISSUE ACTION
Org

Dementia Action Alliances –working creativelyPauline Carlyle and Carol Desborough

Memory & Later Life services
Memory MattersDementia Action Week 2019
Pauline Carlyle, Cumbria DEEP Project lead (Dementia Engagement & Empowerment Project)And
Carol Desborough, Carer Interventions Project lead
Collaboration and creativity
• Dementia Action Alliance
• A collaboration of NHS teams, local authority teams, third sector, community activists, service users and their carers.

The Carlisle Dementia Action Alliance involves CPFT Memory & Later Life service; Alzheimer’s Society, Carlisle City Council, Rotary and others• Pop up Shop in the Lanes in Carlisle - Dementia friends session,
memory concerns advice, 710 new contacts• Schools - Dementia awareness sessions• University of Cumbria- ‘Dementia Juke Box’Other activities in Cumbria include:• West Cumberland- Pigeon race & afternoon tea’s• South Lakes- ‘cha cha plank challenge’• Furness- awareness sessions throughout community & Walney
island• Allerdale- awareness sessions
Positive awareness supporting people to LIVE WELL

Understanding the person’s life history is key to supporting them to continue to live well and remain
connected to their past, present & future
Not understanding this life story- can lead to disconnection & fear
We need to see the PERSON
Understanding and empathy
Hide & Seek
• A Cumbrian film made by Cumbrian-based film makers in Cumbria - locally made in association with Carlisle Dementia Action Alliance & Tullie House Museum
• Seeing dementia differently
• NB: This film has been entered in international film festivals and can’t be shared on social media until the final festival

England
June 2019
Designing integrated care systems (ICSs) in EnglandAn overview on the arrangements needed to build strong health and care systems across the country
The NHS Long-Term Plan set the ambition that every part of the country should be an integrated care system by 2021.
It encourages all organisations in each health and care system to join forces, so they are better able to improve the health of their populations and offer well-coordinated efficient services to those who need them.
This overview is for all the health and care leaders working to make that ambition a reality, whether in NHS acute or primary care, physical or mental health, local government or the voluntary sector.
It sets out the different levels of management that make up an integrated care system, describing their core functions, the rationale behind them and how they will work together.

Introduction
Since 2016, health and care organisations have been working together in every part of England in sustainability and transformation partnerships (STPs). These are a pragmatic way to join up planning and service delivery across historical divides: primary and specialist care, physical and mental health, health and social care. They are also helping to prioritise self-care and prevention so that people can live healthier and more independent daily lives.
The partnerships have begun to agree shared priorities and to make practical improvements. For example, ensuring that people can get a wider range of treatments closer to where they live or work, at a time convenient for them. Or that those who regularly use different services feel like they are dealing with just one team, who make time to understand their full health or care needs and goals.
Integrated care systems (ICSs) accelerate this work. The first 14 were confirmed in 2018, including two areas with health devolution agreements (Greater Manchester and Surrey). They cover a range of urban and rural geographies, with wide variation in population size and system complexity.
The NHS Long-Term Plan confirmed that all STPs are expected to mature so that every part of England is covered by an integrated care system by 2021. NHS England and NHS Improvement have worked with local teams to develop a consistent approach to how systems are designed, and the NHS Long-Term Plan set this out, highlighting three important levels at which decisions are made:
• Neighbourhoods (populations circa 30,000 to 50,000 people) - served by groups of GP practices working with NHS community services, social care and other providers to deliver more coordinated and proactive services, including through primary care networks.
• Places (populations circa 250,000 to 500,000 people) - served by a set of health and care providers in a town or district, connecting primary care networks to broader services including those provided by local councils, community hospitals or voluntary organisations.
• Systems (populations circa 1 million to 3 million people) - in which the whole area’s health and care partners in different sectors come together to set strategic direction and to develop economies of scale.
Precise numbers will vary from area to area. In the earliest ICSs, they range from Gloucestershire, with a population of 528,000 and one recognised ‘place’, to the larger West Yorkshire & Harrogate with a population of 2.7 million and six recognised ‘places’. The exact shape of each system will depend on local factors such as demography and need, and reflect where effective local collaboration is already established.
This work follows years of partnership between NHS and council teams at different levels. Many of the earliest ICSs, and other areas that are making great progress joining up services, build on a long history of planning and providing person-centred care for residents, and on councils’ strategic plans to improve health and wellbeing.
They also incorporate learning from initiatives such as the 50 ‘vanguards’ that tested and refined new care models. In the most successful of these vanguards, NHS providers and commissioners, councils, care homes and others developed more preventive approaches to care and saw significant reductions in emergency admissions.
Effective, collaborative leadership – with clear, common purpose, drawing support from all parts of the system including different professional teams – has consistently been shown to be essential to developing the partnership culture needed to create and sustain systemwide improvement.
Each area is at a different stage in its journey, with even the earliest integrated care systems refining their approach as relationships and infrastructure mature. While some features are common to the most mature systems (such as behaviour that promotes collaboration at every level), priorities and solution will rightly vary between areas in reflection of different local geographies and histories of collaboration.
Systems work most effectively where functions at different levels are designed to support and complement each other – a truly interconnected approach. This overview is to help local leaders think through where functions should sit in their system; maximising resources, galvanising collective effort and systematically improving care for residents.
Overview of integrated care system and their priorities from the NHS Long-Term Plan
2 3
Level
Neighbourhood(c.30,000 to 50,000 people)
Place (c.250,000 to 500,000 people)
System(c.1 million to 3 million people
NHS England and NHS Improvement (regional)
NHS England and NHS Improvement (national)
Functions
• Integratedmulti-disciplinaryteams
•Strengthenedprimarycarethroughprimarycarenetworks – working across practices and health and social care
•Proactiveroleinpopulationheathandprevention
•Services(e.g.socialprescribing)drawingonresource across community, voluntary and independent sector, as well as other public services (e.g. housing teams).
•Typicallycouncil/boroughlevel
• Integrationofhospital,councilandprimarycareteams/services
•Developnewprovidermodelsfor‘anticipatory’care
•Modelsforout-of-hospitalcarearoundspecialtiesand for hospital discharge and admission avoidance
•Systemstrategyandplanning
•Developgovernanceandaccountabilityarrangements across system
• Implementstrategicchange
•Manageperformanceandcollectivefinancialresources
• Identifyandsharebestpracticeacrossthesystem,to reduce unwarranted variation in care and outcomes
•Agreesystemobjectives
•Holdsystemstoaccount
•Supportsystemdevelopment
• Improvementand,whererequired,intervention
•Continuetoprovidepolicypositionandnationalstrategy
•Developanddeliverpracticalsupporttosystems,throughregionalteams
•Continuetodrivenationalprogrammese.g.GettingItRightFirstTime(GIRFT)
•Providesupporttoregionsastheydevelopsystemtransformationteams
Priorities from the NHS Long-Term Plan
• Integrateprimaryandcommunityservices
• Implementintegratedcaremodels
•Embedandusepopulationhealthmanagementapproaches
•Rolloutprimarycarenetworkswithexpandedneighbourhood teams
•Embedprimarycarenetworkcontractandsharedsavingsscheme
•Appointnamedaccountableclinicaldirectorofeachnetwork
•Closerworkingwithlocalgovernmentandvoluntarysectorpartnersonpreventionandhealthinequalities
•Primarycarenetworkleadershiptoformpartofprovideralliances or other collaborative arrangements
• Implementintegratedcaremodels
•Embedpopulationhealthmanagementapproaches
•DeliverLong-TermPlancommitmentsoncaredeliveryand redesign
• ImplementEnhancedHealthinCareHomes(EHCH)model
•Streamlinecommissioningarrangements,withCCGstobecome leaner, more strategic organisations (typically one CCG for each system)
•Collaborationbetweenacuteprovidersandthedevelopment of group models
•Appointpartnershipboardandindependentchair
•Developsufficientclinicalandmanagerialcapacity
• Increasedautonomytosystems
•Revisedoversightandassurancemodel
•Regionaldirectorstoagreesystem-wideobjectiveswithsystems
•BespokedevelopmentplanforeachSTPtosupportachievement of ICS status

36 neighbourhoods with population of 30 - 50k. Atthislevel,primarycarewillbestrengthenedbyworking together in network.
Five places with populations between 250 - 500k. Atthistown/city/councillevel,healthandcarewill work together more closely.
One system with a population of 1.5m.Atthislevel,strategic planning and improvements can take place for the benefit of all as well as having an overview of system finance and performance.
What do these look like in a local system?
4 5
Joining up services from a range of professionals Anintegratedcare‘hub’inWeymouthbrings together a GP, community geriatrician, therapists, community nurses, social workers and mental health professionals to proactively support those at risk of hospitalisation. Early evaluation suggests a 10 per cent reduction in acute bed days for those treated, and improved staff experience. The ICS has supported the model to spread, with ten integrated care hubs now covering the whole county.
Improving care quality and experience with home visits InWestBerkshire,integratedparamedichome visiting gives residents rapid, one-stop care that takes account of their whole needs. Thanks to closer collaboration between primary care, social care and voluntary services, more are now treated at home. This hasimprovedcarequality,useofresourcesand staff experience, reduced deterioration and length of stay, and allowed the system to manage demand more evenly throughout the day. In the first seven months, 96 attendances were avoided, and 75 sessions of GP time saved.
Population health in Lancashire Lancashire neighbourhoods including Chorley and Skelmersdale are developing ‘population health management’ approaches, to improve local people’s health results, reduceinequalitiesandaddressthebroadrangeofindividual,socialandenvironmentalfactors that affect these. To do this, GPs, councils, community organisations and others are building shared information and understanding about how different groups of residents live their lives. For example, bringing different data sources together to identify how those with two or more long-term conditions can best be supported to prevent complications and live independently.
Neighbourhoods (populations circa 30,000 to 50,000 people)
‘Neighbourhoods’arethecornerstoneofintegratedcare.Basedonnaturalgeographies,population distribution and need, and previous work across different professional teams, these networks draw on a wide range of professional skills including: GPs, care homes and home care, pharmacists, community and mental health teams, and the voluntary sector.
They will give community-based care through urgent community response and recovery support, by helping residents to age well and by guaranteeing NHS support to those living in care homes. Byputtinginplaceseamlesscareforbothphysicalandmentalhealth,theywillallowtheNHSand its partners to give care (including secondary care) as close to people’s homes as possible.
Primary care networks, enabled by the new GP contract, are central to this. They will build on the experience of local partnerships already in place, and initiatives such as ‘Primary Care Home’, which have built locality-wide teams across organisational boundaries, often expanding what is offered in GP practices and other community settings.
Asaminimum,primarycarenetworkswillconsolidatethisworktoensureextendedhoursaccess to GPs and to reduce day-to-day pressures by allowing NHS and local government services to share functions or staff. More mature networks will use increasingly sophisticated data to identify and give more proactive care to those at risk of unnecessary hospital admission and will use new technology and tools such as social prescribing to help people to care for themselves where appropriate.
Barnsley
SheffieldRotherham
Doncaster
Bassetlaw
We will now consider the three levels – neighbourhood, place and system – in more detail.
South Yorkshire & Bassetlaw integrated care system

Places (populations circa 250,000 to 500,000 people)
This level may match local council boundaries or the natural geographies at which services are delivered. It will include clusters of primary care networks, linking these to care providers such as one or more acute hospital, care homes, mental health and community providers, local government and voluntary or community organisations.
Together, these will make a shared assessment of local need, plan how to use collective resources and to join up what they offer – including beyond traditional health and care services – to make best use of overall public and community resources.
Two crucial pieces of work are driven at ‘place’ level, both relying on collaboration and joint decision-making. These are clinical care redesign (simplifying and standardising care pathways across a whole area) and population health management (making better use of data to improve how health and care services address wider health determinants such as housing,environmentalqualityandaccesstogoodemploymentandtraining).
They may also be the level at which some local services are integrated and managed such as rapid response teams to support people with learning disabilities.
In the absence of a legal basis for statutory (NHS and local council) commissioners to form decision-making committees with statutory providers, the ‘board’ at place level will normally operate according to an NHS alliance agreement or initially with a lighter touch memorandum of understanding. ICSs will also be expected to work closely with health and wellbeing boards, the established statutory forum that brings together local leaders from different parts of the system, which will often coincide with place level.
Systems (populations circa 1 million to 3 million)
The ‘system’ level provides strategic leadership across the whole population of the ICS. This will include overseeing a single plan covering both operational and long-term transformation priorities (building on, and aligning place-level plans), and managing financial performance against a system control total that encompasses CCGs and NHS providers.
Itwilltakeresponsibilityfordeliveringhighqualityservicesandaccess,reducingunwarrantedclinicalvariationandaddressinghealthinequalities.Otherfunctionsthatwillbe undertaken at system-wide level include NHS workforce planning, agreeing how to make the best use of capital, estates and digital infrastructure, and spreading good practice that emerges at place level over a wider scale.
Clinical, managerial and support functions will be provided at system level when they can most efficiently and effectively be delivered once; for example, where analytical capacity or business intelligence capability is in short supply.
System leaders will take collective responsibility for financial and operational performance, typically through a systemwide board which includes all NHS partners. New governance arrangements will support this, enabling timely action on system-wide challenges.
6 7
Place-based commissioning in a combined authorityTen areas in Greater Manchester are moving to place-based joint commissioning betweenlocalgovernmentandCCGs,inlinewithlocalcouncil/healthandwellbeingboard boundaries. Together, these will join up health and care services at scale, drawing onrelationshipswithGreaterManchester’sMayorandCombinedAuthority,transportauthority, police, fire service, housing providers and the voluntary sector.
Sharing information and freeing staff to work across a countyDorsetICSdevelopedthe‘DorsetCareRecord’,asingle,confidentialsystemallowinghealth and care professionals across the whole county to see the same information about patients. Joining up information in this way means that people no longer need to repeat their story to different teams, and improves care by enabling a more comprehensive and up-to-date understanding of their whole needs.
The ICS has also introduced workforce ‘passports’ so staff can move freely between any organisation in the county. This allows people to develop different skills and perspectives and encourages them to stay in the system by providing a wider pool of career options.
Moving to a single accountable officer across commissionersFiveoftheearliestICSs(Dorset,SurreyHeartlands,NorthCumbria,GloucestershireandBedfordshire,LutonandMiltonKeynes)haveappointedjointaccountableofficersacross constituent CCGs. This has helped them to simplify commissioning arrangements, enabling a single set of system-wide decisions in line with agreed local needs and aspirations.
Joining up health and care in line with local council areasThesixplacesinWestYorkshire&Harrogate(BradfordDistrictandCraven,Calderdale,Harrogate,Kirklees,LeedsandWakefield)aredevelopingintegratedcareservices,scaled up as appropriate for differing population needs. For instance, partners in Wakefield (including NHS organisations, the council, housing providers, fire service and voluntary and community sector) are working together to keep residents safe and well in their own homes via two ‘connecting care’ hubs.
Improving productivity by better reflecting patients’ needsThe‘BetterTogether’allianceinMidNottinghamshire,whichincludesthecountycouncilalongside CCGs, NHS trusts and others, separates patients into different groups based on their risk levels. This has helped to improve care and timeliness for patients, avoiding unnecessary hospital admissions and bed days. Over time, it is expected to lead to all NHS providers in the area working through a single contract alliance.

NHS England and NHS Improvement – national and regional support and oversight
NHS England and NHS Improvement’s seven regional teams are responsible for holding systems to account, supporting their development and making interventions where necessary. ICSs will agree system-wide objectives with their regional director and be accountable for systemwide performance against these objectives.
National and regional teams will work together, steered by regional directors to encourage andsupportallsystemstotakeongreatercollaborativeresponsibilityforimprovingqualityof care, focusing on population health and improving their use of NHS resources.
Quality, safety and performance issues should be addressed as close to the system as possible.
The overall principles of this approach will be to:
• help to design the right support and intervention for local health systems, ensuring NHS England and NHS Improvement create maximum value and avoid unnecessary burden;
• decide when and how to intervene in systems, providers or CCGs in their region, or – wheretheseriousnessoftheinterventionrequiresanationaldecision–maketherelevantrecommendations to the decision-making group;
• be responsible for managing all interventions with – or seeking information or assurances from – systems, providers or CCGs;
• treat performance management and improvement as a continuum, rather than in terms of fixed check points;
• help develop standardised national approaches to improvement and performance, but have discretion to allow systems, providers or CCGs to depart from standardised approaches where they are performing well.
The regions continue to have a role in managing system development and performance; with this responsibility shifting to the system as it matures. Therefore, regional teams will need to adopt different approaches to regulating systems based on their maturity.
Some functions, such as ambulance services, specialised commissioning or emergency preparedness may be best arranged in line with scale of delivery or prevalence of need. This may sometimes be at a geography that is sub-regional but wider than system-wide.
In more mature systems, the regional role increasingly becomes that of a critical friend, providing the system with further autonomy regarding regulation, avoiding engaging with individual organisations without the knowledge of the system and reducing the number of formal meetings.
Over time, we envisage that NHS regional teams and overall operation will become leaner and more strategic, as systems take on more self-development and self-assurance as they progress to becoming thriving ICSs.
NHS England and NHS Improvement’s national team will remain the overall centre for policy and strategy development including overall health system strategy, the NHS provider landscape and heath commissioning strategy.
Maturity matrix for integrated care systems (ICSs)
The integrated care system maturity matrix has been developed to outline the core characteristics of systems as they develop. These were developed from observing and talking to the earliest ICSs, and from the objectives set out in the NHS Long-Term Plan.
ItisbasedonsimilartoolsusedbytheLocalGovernmentAssociationandothers,whohave experience in supporting system development and change. It provides a consistent framework for all regions and systems across the country.
The matrix outlines the core capabilities expected of emerging ICSs, developing ICSs, maturing ICSs and thriving ICSs. For a system to be formally named an ICS, they will need to meet the attributes of a maturing ICS.
It uses a progression model which shows a journey rather than a series of binary checklists, recognising that systems will not develop all domains at the same pace and will therefore havevaryinglevelsofmaturityacrosseachdomain.Bydoingthis,itseekstosupportmorenuanced and reflective discussions about system maturity.
System maturity matrix – five domains, four stages
8 9
System leadership, partnerships and change capability
System architecture and strong financial management and planning
Emerging DevelopingMaturing ICSSystem formally named an ICS and minimum level of maturity for all systems to reach by April 21
Thriving ICS
•Leadershipteamthatlacksauthority with no collectively-owned local narrative or sense of purpose.
•Lackoftransparencyinwaysof working.
•Littleprogressmadetofinalisesystem vision and objectives or embed these across the system and within individual organisations.
•Minimalmeaningfulengagement with primary care, local government, voluntary and community partners, service users and the public.
•Limitedunderstandingofsystem architecture across the footprint and limited plans to organise delivery around neighbourhood, place and system.
•Fragmentedcommissioninglandscape with few agreed plans to streamline arrangements.
•Systemnotinfinancialbalanceand unable to collectively agree recovery trajectory.
•Lackofsystemwideplansonworkforce, estates and digital.
•Allsystemleaderssigneduptoworking together with ability to carry out decisions that are made.
•Anearlysharedvisionandobjectives, starting to build common purpose and a collectively-owned narrative among the broader leadership community including primary care.
•Planstoincreasetheinvolvement of local government, voluntary and community partners, service users and the public in decision-making at system, place and neighbourhood.
•Clearplanstoorganisedeliveryaround neighbourhood, place and system.
•Planstostreamlinecommissioning, typically with one CCG that is leaner and more strategic.
•Goodunderstandingofsystemfinancial drivers and efficiency opportunities, with a shared plan to address issues.
•Systemwideplansbeingdeveloped to address workforce, estates and digital infrastructure.
•Collaborativeandinclusivemulti-professional system leadership and governance; including local government and the voluntary sector.
•Clearsharedvisionandobjectives, with steady progress made visible to stakeholders and staff.
•Dedicatedcapacityandsupporting infrastructure being developed to help drive change at system, place and neighbourhood level (through PCNs).
•Effectiveongoinginvolvementof voluntary and community partners, service users and the public in decision-making at system, place and neighbourhood levels.
•Acultureoflearningandsharing with system leaders solving problems together and drawing in the experiences of others.
•Systemisworkingwithregional teams to take on increased responsibility for oversight.
•Planstostreamlinecommissioning are underway.
•Systemhascredibleplansfor meeting system control total and, where not already achieved, for moving towards system financial balance
•Systemwideplansforworkforce, estates and digital infrastructure being implemented.
•Systemismanagingresourcescollectively and signed up to the ICS financial framework.
•Strongcollaborativeandinclusive system leadership, including local government and the voluntary sector, with a track record of delivery.
•Transparentandrobustgovernance, with multi-professional leadership aligned around the system and system working closely with health and wellbeing boards.
•Aproactiveapproachtothe identification and development of future system leaders at all levels.
•Dedicatedclinicalandmanagement capacity and infrastructure to execute system-wide plans.
•Anarrativethatiswellunderstood and strongly supported by the public and staff, outlining how integrated care is delivering on the ambitions of communities, with demonstrable impact on outcomes.
•Systemhasprogressedtothe most advanced stage of oversight progression – i.e. self-assurance, with clear communication and relationships with regional team.
•Streamlinedcommissioningarrangements fully embedded across all partners.
•Systemisinfinancialbalanceand is sharing financial risk using more sophisticated modelling of current and future population health and care needs.
•Incentivesandpaymentmechanisms support objectives and maximises impact for the local population.
•Improvementsinworkforce,estates and digital infrastructure being seen across the system.
•Systemismanagingresourcescollectively and signed up to the ICS financial framework.
System progression

Integrated care models Oversight
Finance
Planning
Support
Track record of delivery
Coherent and defined population
•Limiteduseofnationalandlocal data to understand population health and care needs.
•Limitedthinkingabouthowto scale up primary care and how to integrate services at neighbourhood or place
•Minimalcollaborationorengagement across providers.
•Systemscanprovideadviceand guidance on individual organisations within the system to support conversations
•NHSEIwilluseasingleperformance, oversight and assessment framework
•Organisationalfinancialrecovery plans will be developed with the system leaders to ensure consistency with five year system-level strategic plans, with system efficiency plans overseen by a system efficiency board
•NHSEIwillleadreviewandassurance of organisational and system operating plans.
•NHSEIwillworkwiththesystem to develop and strengthen these plans
•Intensesupport,regionallyledand nationally coordinated
•Slowprogresstowardsdelivering national priorities especially the 5 service changes set out in the LTP.
•Lackofrelativeprogressindelivering constitutional standards without system agreement to work together to support improvements.
•Weaksystemoperatingplandeveloped and system unable to make collective decisions around system funding.
•Ameaningfulgeographicalfootprint that respects patient flows
•Wherepossiblecontiguouswith local authority boundaries; where not practicable has clear arrangements for working across local authority boundaries
•CoversanexistingSTPofsufficient scale (~1m pop or more)
•Earlydevelopmentofthe5service changes within the LTP, and care models aiming to:
- address unwarranted clinical variation;
- integrate services around the needs of the population in neighbourhoods;
- integrate services vertically at place;
- collaborate horizontally across providers at the systemand/orplacelevel.
•PCNsdevelopingclearvisionfor integrated care models and transforming population health.
•Someunderstandingofcurrentand future population health and care needs using local and national data.
•Plansinplacetosupportinteroperable access to care records across health and social care providers.
•Systemswilldevelopandimplement a plan to support ICS development, which will be reviewed and agreed with NHSEI
•NHSEIwillinvitesystemleadership to attend and contribute to discussions relating to individual organisations within the system
•NHSEIwillconsultthesystemposition before any escalation action/interventionisapproved and enacted through a single identified lead
•NHSEIwillalignroleswithinthe regions to support systems
•STPswilldemonstratestrongfinancial leadership and governance for financial decision-making.
•NHSEIwillworkinpartnershipwith system leaders to review organisational and system operating plans
•Basedonneedsidentifiedindevelopment plan
•ICSAcceleratorProgrammeTBC
•Accesstoregionalandnationalsubject-matter expertise where required
•Evidenceofprogresstowardsdelivering national priorities especially the 5 service changes set out in the LTP.
•Improveddeliveryofconstitutional standards.
•Systemoperatingplaninplacethat demonstrates a shared set of principles to start to manage finances collectively.
•Ameaningfulgeographicalfootprint that respects patient flows
•Wherepossiblecontiguouswith local authority boundaries; where not practicable has clear arrangements for working across local authority boundaries
•CoversanexistingSTPofsufficient scale (~1m pop or more)
•PCNsimplementingnewor redesigned care models with partners to meet population need – that is enabling integrated provision of health and care within neighbourhoods.
•Integratedcareteamsoperating at neighbourhood and place bringing together PCNs, mental health, social care and hospital services as per the triple integration set out in the LTP.
•Startingtoimplementplansto:
- address unwarranted clinical variation;
- deliver the 5 service changes in the LTP;
- tackle the prevention agenda and address health inequalities.
•PHMcapabilitybeingimplemented including segmenting and stratifying population using local and national data to understand needs of key groups and resource use.
•ICSswillagreeandimplementsystem-wide objectives agreed with regional teams, coveringcarequalityandhealth outcomes, reductions in inequalities,implementationof integrated care models and improvements in financial and operational performance
•ICSswillconductandcontribute to the assurance and improvement of individual organisations performance
•NHSEIwillkeepadhocdatarequestsandroutinereportingoutside the performance framework and agreed ICS objectives to a minimum, and coordinate through an identified lead
•NHSEIwillnotengagewithindividual Trusts or CCGs without the knowledge of the ICS
•NHSEIwillco-locateregionalroles within the ICS to provide bespokesupportrequestedbythe ICS
•ICSswilltakeupthe19/20ICSfinancial framework
•ICSswillcommittodeliveringthe objectives of the relevant national programmes and report progress against this. Appropriategovernancearrangements to account for use of funds will be in place before any funds are released
•NHSEIwilldelegateauthority for the direction of transformation funding from national programmes to the system, where possible
•Organisationsthatareinfinancial surplus will play an active role in the development and delivery of financial recovery plans of organisations within their ICS
•NHSEIwillsupportsystem leaders to assure organisational plans, and will work in partnership with system leaders to ensure system operating plans are sufficiently robust.
•ICSDevelopmentProgramme
•Evidenceoftangibleprogresstowards delivering national priorities especially the 5 service changes set out in the LTP.
•Consistentlyimprovingdeliveryof constitutional standards with credible system plans to address risks.
•Robustsystemoperatingplan and system financial management in place, with a collective commitment to shared financial risk management.
•Robustapproachinplaceto support challenged organisations and address systemic issues.
•Ameaningfulgeographicalfootprint that respects patient flows
•Wherepossiblecontiguouswith local authority boundaries; where not practicable has clear arrangements for working across local authority boundaries
•CoversanexistingSTPofsufficient scale (~1m pop or more)
•Integratedteamsdemonstrating improvement in outcomes.
•FullymaturePCNsacrossthesystem delivering care with partners that meets population needs.
•Implementingprioritiesinprevention and reducing healthinequalitiesaspartof care model design and delivery.
•Fullpopulationhealthmanagement capability embedded at neighbourhood, place and system levels which supports the ongoing design and delivery of proactive care.
•Implementationofthe5service changes set out in the LTP demonstrating improvement in health outcomes.
•ICSswillleadtheassuranceofall individual organisations
•ICSswillagreeandcoordinateany trust or CCG intervention carried out by NHSEI, other than in exceptional circumstances
•ICSswillbeabletoleadandshape how gathering any data from individual organisations ismanagedwhererequired
•NHSEIwillagreeaminimumdataset with ICSs
•NHSEIwillembedregionalresources within the ICS to operate under the direction of the ICS
•NHSEIwillundertaketheleastnumber of formal assurance meetings possible with individual organisations
•ICSswilltakeupthe19/20ICSfinancial framework
•ICSswillleadassuranceoforganisational plans.
•Systemoperatingplanswillhave a light touch review by the NHSEI
•ICSDevelopmentProgramme
•Expectationtoworkalongsideregional and national teams to support less developed systems
•Evidenceofdeliveringnationalpriorities especially the 5 service changes set out in the LTP.
•Deliveryofconstitutionalstandards including working as a system to mitigate risks.
•Demonstratingearlyimpactonimproving population health outcomes.
•Consistentlydeliveringsystemcontrol total with resources being moved to address priorities.
•Asissuesemerge,leadersjoinforces to tackle them as a system including when under pressure.
•Ameaningfulgeographicfootprint that respects patient flows
•Wherepossiblecontiguouswith local authority boundaries; where not practicable has clear arrangements for working across local authority boundaries
•CoversanexistingSTPofsufficient scale (~1m pop or more)
10 11
Emerging
Emerging
Developing
Developing
Maturing ICSSystem formally named an ICS and minimum level of maturity for all systems to reach by April 21
Maturing ICSSystem formally named an ICS and minimum level of maturity for all systems to reach by April 21
Thriving ICS
Thriving ICS
System progression
System progression
KeyLTP – Long Term Plan; PCNs – Primary Care Networks; UEC – Urgent and Emergency Care; PHM – Population Health Management
ICS will drive forward five major practical service changes set out in the LTP – These are: (1) boost out-of-hospital care, and finally dissolve the historic divide between primary and community services; (2) re-design and reduce pressure on emergency hospital services; (3) give people more control over their own health, and more personalised care when they need it; (4) implement digitally-enabled primary and outpatient care; and (5) increasingly focus on population health and local partnerships with local authority-funded services.
Freedoms and Flexibilities for 2019-20

Find out more
Keep up to date on how health and care is changing: www.england.nhs.uk/integratedcare
Subscribe to NHS England’s fortnightly bulletin, Future Health and Care: www.england.nhs.uk/email-bulletins/future-health-and-care-update

PURPOSE The purpose of this report is to update System Leadership Board (SLB) on the progress being made with the organisational form transaction between North Cumbria University Hospitals NHS Trust (NCUH) and Cumbria Partnership NHS FT (CPFT). The aim of the transaction is to form a single NHS provider organisation in line with the North Cumbria Integrated Health & Care System strategy. KEY POINTS TO HIGHLIGHT • Full Business Case (FBC) has been developed in line with transaction guidance from NHS
Improvement (NHSI) as the regulator;• The FBC has been approved by both Boards of Directors and submitted to NHSI in order to
enable the necessary review and scrutiny;• Following this review, the FBC is scheduled to proceed to the approvals phase of the
process;• NHS North Cumbria CCG have provided a supporting letter for confirming the
commissioning provision under one provider organisation;• The timetable remains in place for the transaction to be enacted on the 1 October 2019
NEXT STEPS / AREAS OF WORK TO BE PROGRESSED Approvals stage with NHSI with view to enacting the merger on 1 October 2019.
RECOMMENDATION System Leadership Board is asked to note this paper for information.
System Leadership Board Public
4th July 2019 Enc:
Title: Organisational Form Transaction Update Author: Daniel Scheffer, Company Secretary CPFT & NCUH
1
7

Organisational Form Programme Update
4th July 2019
1. Introduction
At the meeting held on 24th May 2018, both boards agreed that the arrangements between Cumbria Partnership NHS Foundation Trust (CPFT) and North Cumbria Universities Hospital Trust (NCUH) as set out within the Memorandum of Understanding (MoU) needed to progress to the next stage. As a result, it was agreed to formally explore opportunities to merge in order to form one NHS Foundation Trust. This paper is provided to the System Leadership Board to update on progress with this work. Since May 2018, a small internal programme team has been in place which has been considering and developing options, engaging with internal and external stakeholders together with providing formal updates to the Boards. The work of the programme team has been undertaken in line with Transaction guidance published by NHS Improvement (NHSI). NHSI are the regulator with responsibility for such transactions. The Transaction guidance provides a clear framework and sets out three clear stages for approval by NHSI. The stages are: Stage 1: The development of a strategic case Stage 2: If the strategic case is approved, a Full Business Case (FBC) will be
developed by the Trusts which includes detailed plans on how the transaction will be delivered successfully;
Stage 3: Approvals – includes all the necessary regulatory and legal steps involved in completing the transaction.
The Strategic Case was considered and approved by the Board of Directors for CPFT and NCUH on the 20th December 2018 and formally submitted to NHSI on the 21st December 2018. After a full review and panel discussion NHSI issued a letter of approval to proceed to Stage 2 of the process in February 2019.
2. Programme Update
The programme has continued to move forward at pace with work streams under the leadership of executive directors working completing the content for the FBC whilst at the same time delivering on implementation plans. The FBC was submitted to both NCUH and CPFT Board of Directors on 27th June 2019 who approved its submission to NHSI to move forward with the next stage of the process during summer 2019.
2

The anticipated timeline and key activities for the next phase are identified below:
Business Case Development January – June 2019
Commissioning and submission of external opinions for Working Capital and Financial Reporting June – August 2019
Board Approval of Business Case June 2019
Business Case Submission to NHSI 1st July 2019
NHSI Approvals Engagement Process July – August 2019
Board to Board Meeting 23rd August 2019
CPFT & NCUH Boards Approve External Opinions if required Between 29th August & 6th September 2019
NHSI Risk Rating 10th September 2019
CPFT & NCUH Board Meeting to agree transaction 18th/19th September 2019
CPFT Governors Meeting to a approve transaction process 18th/19th September 2019
CPFT Formally apply to NHSI to dissolve NCUH & from North Cumbria NHS Foundation Trust 20th September 2019
NHSI Process to dissolve NCUH 20th September – 30th Sept
Formation of new Trust 1st October 2019
3. Conclusion The SLB is asked to note the information contained in the report and the associated timetable to enable the completion of the transaction by 1st October 2019.
3

PURPOSE
This report is an update on engagement activity for our North Cumbria Integrated Health and Care System which has taken place during May and June 2019.
KEY POINTS TO HIGHLIGHT
• Visits from senior NHS England leaders to talk to our staff and teams about progress inintegrating care.
• Events with community, third sector and local authority groups to seek feedback on oursix strategic aims for our system.
• Copeland Community Stroke Prevention Project event building an alliance of thirdsector, community and NHS teams with more events planned
• Successful People First Takeover day as part of Learning Disabilities AwarenessWeek.
• Allerdale and Copeland Local Committee engagement discussion on the developmentof our strategy.
• Work has commenced with key young people’s groups to engage and discuss thedevelopment of our strategy.
• Cumbria Chief Executive’s Group discussion on the development of our strategy.
NEXT STEPS / AREAS OF WORK TO BE PROGRESSED
• More work planned around engaging about the draft strategy• Engagement with district councils to be developed
RECOMMENDATION
To receive this update for information
System Leadership Board PUBLIC
4th July 2019 Enc: 8
Title: Engagement activity for the North Cumbria Health and Care System Author: Jon Rush – chair NHS North Cumbria CCG
1

Title: Engagement activity for the North Cumbria Health and Care System Author: Jon Rush – chair NHS North Cumbria CCG
Introduction
Engaging across our health and care system is important to developing the relationships which will ensure the successful delivery of our plans for future health and care services. Involving patients and our community in shaping those plans is one of our system’s key principles. Key stakeholder engagement highlights:
• In May we welcomed the Medical Director for NHS England, Professor Stephen Powis and Matthew Cripps, the NHS England Director for Sustainable Healthcare. They met frontline teams working on Hazel Ward and the Heart Centre at the Cumberland Infirmary; the hub at Maryport and Cockermouth ICC; and the teams in the Same Day Health Centre and Accident and Emergency at the West Cumberland Hospital.The pair heard about the challenges of running two district general hospitals in a remote area and saw first-hand the energy and enthusiasm of our teams. Both said they had enjoyed seeing the impact of integrating services in action.
• Our system leaders have been involved in national meetings to share our experiences and learn from others best practice.
• In June we supported the People First takeover which connected people with Learning
Disabilities with senior leaders in Cumbria as part of Learning Disabilities Week 2019. Nicky and her colleague Stef spent time with NHS North Cumbria Clinical Commissioning Group’s Director of Nursing and Quality Anna Stabler, along with Chairman Jon Rush, Chief Operating Officer Peter Rooney, and our Engagement Team.
• In June the newly formed Copeland Community Stroke Prevention Group held its first
event at the Cumbrian Trader’s Day in Whitehaven. The collaboration involved Rotary, the West Cumbrians’ Voices for Healthcare, the Stroke Association, Community Pharmacy Cumbria, Healthwatch Cumbria; public health, North west Ambulance Service, CVS Cumbria, the local NHS. More than 90- people had a free health check – all were offered information to help them make healthy life choices. More than 10 per cent were directed to extra monitoring and Dr John Howarth gave direct medical advice to 2 people.
• Other events we have been involved include the West Cumbria Community Forum and
a mental health focused Action 4 Health network meeting.
• We are also engaging with Healthwatch Cumbria which plans to expand a national feedback centre tool into Cumbria. We are linking with our patient engagement teams and other providers ahead of it being introduced.
2

Developing our Strategy Engagement There has been considerable work to support the engagement around the six strategic priorities we have published as the basis for our strategy for the future. The documents and survey have been promoted on social media and shared with staff at clinical forums, community groups, and others. We have also been talking to young people about their views of the NHS, their experience of services and what they would like to see in the future. We have linked with Cumbria County Council youth support workers in Carlisle, Eden, and west Cumbria and are grateful for the productive sessions they have supported. A series of staff drop-ins led by managers and execs are now underway and gathering feedback from staff across all sites, this has included the following
• Surgical & medical team • Carleton Clinic drop-in • Ward drop-in at Cumberland Infirmary Carlisle • Ward drop-in at West Cumberland Hospital • Joint Partnership Forum • Clinicians engagement event • ICCs steering and development group • Nursing and midwifery board
Further work with our staff is planned during July and will be an ongoing feature of bringing the strategy to life within our front line teams. A number of stakeholder engagement sessions have also taken place during the last two months, specifically focussed on the development of our strategy, they include:
• Working Together Group • Joint Scrutiny Panel at Cumbria County Council • Cumbria Health and Wellbeing Board • Eden and Carlisle youth councils • Whitehaven Traders day • Healthwatch engagement • Cumbria Chief Executive’s Group • Allerdale and Copeland Local Committee
The feedback to date is very supportive of the broad direction of travel. A summary of any changes made and how this has influenced the final version of the strategy refresh work will be included in the final document. Our approach has been supported by the NHS England national engagement team.
3

Democratic engagement Our teams also worked with all of the county’s MPs to support nominations for the 2019 Parliamentary Awards. Out of 10 categories we had 4 of the regional winners for the North East and Yorkshire region. Our winning local teams are: • Delirium Reach Out - The Excellence in Mental Health Care Award – nominated by
Rory Stewart; John Stevenson; Trudy Harrison • HAWCS – the County Council team - The Health Equalities Award [New for 2019] –
nominated by Rory Stewart; John Woodcock • Better Health at Work – The Wellbeing at Work Award [New for 2019] – nominated by
Rory Stewart; Sue Hayman • Familiar Faces - The Excellence in Primary Care Award – nominated by Rory Stewart,
John Stevenson, Trudy Harrison Recommendation
To note the report and plans to further engage on the developing future strategy for our system
4
PURPOSE This report updates SLB on progress with third sector working across the integrated health and care system.
KEY POINTS TO HIGHLIGHT
The regular update report on key activities and programmes of work is attached at Appendix 1.
• Progress with the integrating third sector into the ICC model continues to be made.• Work has commenced on gaining a greater understanding of financial investment and support
into the third sector.• The pilot to look at IG solutions is to be repeated due to capacity constraints.
In addition to the specific programmes of work, a meeting to discuss how the broader strategy for the third sector as part of the ICS could be developed in the future was held with the project team. It was recognised that linking the work to the County Council priority for improving third sector working and the thriving communities’ agenda was important. Equally, how the overarching strategic priorities are developed in conjunction with the Cumbria Compact is also important. Four broad themes have been identified which will form the basis of a collective discussion with third sector organisations and Cumbria CVS in developing the overarching strategy for third sector working across the system with clear priorities and opportunities (linked to the system plan development).
• A Strategic System Partner - bringing its expertise; strength and diversity to contribute on an equalbasis to the planning, shaping, decision making, and implementation of agreed local priorities.
• A Service Provider – improving health and wellbeing outcomes by responding to local and diversehealth and wellbeing needs.
• An Enabler of the Community Voice and Representation• A Source of support for volunteering, fund raising and using all assets in our communities.
NEXT STEPS / AREAS OF WORK TO BE PROGRESSED • The report attached at Appendix 1 is currently being updated into an OGIM for 19/20. This will
provide greater clarity on the specific initiatives which will be delivered this year. It will also allowfor greater connectivity between other programmes of work, for example ICCs.
• Scoping of the further discussions is required with Cumbria County Council and the Third Sector inshaping the work around the identified strategic themes of work.
RECOMMENDATION
The SLB is asked to note the report.
System Leadership Board 4 July 2019 Enc: 9
Title: Third Sector Update Report Author: Claire Edwards, Health Partnerships Officer
1

AGENDA ITEM: System Development 10:
THIRD SECTOR PROGRAMME REPORT - Health Partnerships Officer Report for SLB Board 04.07.2019
Subject Recommendation Progress Update Social Prescribing
• As Social Prescribing models develop in North Cumbria our system urgently needs to consider the investment requirements into the third sector to support the sector to meet increased demand
• Social prescribing workshop held with cross section of staff and partners.
• This will be linked with the process listed below on resourcing.
Capacity and resources
• There is a need to map current investment by North Cumbria Health and Care into the third sector including:
o In kind resources e.g. hot desking, office space, co-location, staff time
o Funding/grants o Contracts/SLA’s o Access to national funding pots (particularly where statutory sector
partnership is key) • A review of this investment needs to take place. The review should include:
the development of a better understanding of this investment’s fit for purpose in light of ICC development and the expectations the system has on the sector to support and deliver key elements of the ICC programme
• A need to develop a strategic investment plan for the sector in relation to ICC development programme
• There is a need to develop a better understanding of how in kind support to the sector is offered and to develop more effective systems to enable the growth of this area of support
• There is a need for partners to consider additional support for the proposed CCC Public Health investment into third sector ‘Fundraising’ capacity. Current plans indicate that post holders would be expected to work across health, care and third sector partners (and funders) to coordinate and write bids for funding (specifically focusing on prevention funding that requires
• A scoping exercise has commenced to clarify the current financial support into the third sector.
• This will require confirmation of statutory services provided and additional / over and above financial resource.
• Scoping work likely to take 3-6 months.
2

closer multi-sector collaboration) • There is a need for key staff to invest time to understand the principles
outlined in The Cumbria Compact* (a document supported by all partners that outlines the relationship between the public sector and the voluntary and community sector in Cumbria allowing them to work together more effectively to strengthen communities and improve people’s lives) and adhere to these in relation to issues relating to capacity and resource for the sector
*Copy of Compact available (Note: Compact refresh in progress): https://cumbriacvs.org.uk/compact/the-cumbria-compact/
Information Governance
• A solution needs to be found to issues relating to IG and the sharing of patient information with representatives of the third sector.
• 2 x ICC Hub based Third Sector Referral Co-ordinators now in post. Posts will be based in Eden ICC and Cockermouth & Maryport ICC. A third post will be advertised in September once CPFT Charitable Funds have been approved.
• Health Partnerships Officer and Head of Communications & Engagement for North Cumbria CCG to take part in national round table discussions organised by NHS Improvement & NHS Engagement 16.07.2019
Co-Production • To develop a system wide model for Co-Production processes. The model will need to have clear directions as to how to engage the third sector. This plan should include best use of third sector infrastructure bodies (e.g. Cumbria CVS, ACT and Cumbria Youth Alliance) and existing third networks (Cumbria Action for Health Network, Learning Disability Provider Forum, Children & Young People’s Voluntary Sector Reference Group, Churches Together, County Volunteering Network etc.)
• There is a need to consider how to effectively resource Co-Production. This is of particular reference to patients who have significant needs and may require support to attend and engage with Co-production activity and who may in addition be
3

• To develop a system wide model that ensures best use of outcomes from Co-Production processes. The model should include a model for the continued engagement of third sector organisations in the development planning and review of services developed as a result of Co-Production processes.
benefit dependent. In addition there is value in resourcing Co-production events to take place in community buildings. This will provide opportunities to support the community building’s sustainability and introduce patients, clinical staff and residents to a wealth of community based activity much of which could support health and wellbeing and ensure positive community engagement.
ICC referrals to & from third sector
• To develop a clear system wide pathway for referrals to and from the third sector using the Hub function
• The proposed pilot of the referral pathway has been largely unsuccessful due to staffing capacity issues in the two ICC Hubs engaged in the pilot; Copeland and Carlisle Network. The pilot will now be undertaken in the two ICC Hubs where Third Sector Referral Co-ordinators are hosted.
ICC multi-disciplinary meetings
• To develop a system wide model for the inclusion of third sector representation at multi-disciplinary team meetings
• Third Sector Referral Co-ordinators will commence attending MDT meetings in Eden and Cockermouth & Maryport ICCs from early July. There is still no opportunity for third sector organisations to be involved in the other 6 ICCs MDT meetings
Sector offer visibility in ICC Hub environment
• To develop a proposal that will enable system wide inclusion of third sector expertise in each ICC Hub.
See above Information Governance
4

Collaborative Case Study 3 An opportunity to show case examples of good practice where health professionals and staff from third sector organisations are working effectively to produce positive outcomes for patients and carers and where the health system or individual health professionals identify opportunities to work more effectively and efficiently. Hug a Mug (Ewanrigg Community Trust)
Hug a Mug operates a low key support and information session within Maryport Group Practice premises. It is supported by 15 volunteers from the local community and local businesses. During its first 18 months of operation the volunteers have supported 1441 client interactions. 93% of clients using the service have self referred 5% were referred by GPs the remaining referrals have come from nurses, local schools and the County Council’s Health & Wellbeing Coaches.
Hug a Mug provides a welcoming and social environment open to all, 9.30am to 11.30am five days per week. Clients do not need to make an appointment and can use the service as much as they require. Volunteers offer refreshments, information, sign posting, access to a phone and computer, support to contact other third sector and community resources and to navigate statutory sector services. Clients have been supported to access information about mental health issues and services including drug and alcohol, finance and employment including benefits, volunteering opportunities and support with loneliness and bereavement. 69% of support focuses around mental issues. Many of the clients using the service attend regularly with over 80% attending the service two or more times a week. Many of those who use the service two or more times a week are or have been patients who are very regular users of GP services. It is recognised that those patients using Hug a Mug appear to become less reliant on GP services and take up less GP consultation time.
Hug a Mug has worked closely with the practice manager to calculate accurate figures regarding GP time saved by the project. Patient usage of GP time has been plotted both before and after they have commenced attending Hug a Mug. The Practice Manager has calculated that on average the project has saved two days of GP time each month.
The following are just a few comments from Hug a Mug clients asked to explain what they get out of using the services.
‘Links to other organisations’ ‘A safe place’
‘Someone to talk to’ ‘Meeting new friends’
‘A less threatening place’
5
PURPOSE This report summarises the progress being made in development of the system strategy refresh work. This is linked directly to the recently published NHS Long Term Plan Implementation Framework which was published at the end of June. KEY POINTS TO HIGHLIGHT DEVELOPING OUR STRATEGY • Our strategy and priorities are well defined in terms of our high level strategic direction and
focus. • Significant engagement work on our strategic direction including our six strategic priorities
commenced in May 2019 (Appendix 1). The feedback from this engagement work with our staff, partners and community groups will help shape and finalise the key commitments we set out locally for delivery over the next 5 years. This will also include the work Healthwatch have been undertaking locally as part of the national programme of work.
• The delivery plan to support our strategy is where the key area of focus and work is required during July and August. Key leads from across the system have been identified for the key delivery plan areas, including clinical leads. The System Executive Group is overseeing the development of the plan and a small team has been established to lead on the production of the system plan.
• The technical material to support the activity, finance and workforce projections is also now a key area of focus. This links to the need to refresh our capacity modelling and demographic assumptions which we will do jointly with the business intelligence team from the NHS as well as Local Authority input. The capacity modelling work for the system is a critically important piece of work to support the assumptions and trajectories we will make in our five year plan submission.
• The commitments we set out will also need to cover the basic requirements of the NHS Long Term Plan which have been summarised in Appendix 2 of this report.
Timescales & Requirements • System plans for delivery through to 2023/24 are required, with an initial submission in
September 2019 and a final submission to follow by mid November 2019. Systems are asked to provide two elements at both the September and November milestones; - Strategy delivery plan: A document that sets out what the system plans to deliver
over the next five years. - Supporting technical material: Successful delivery will require systems plans to be
underpinned by realistic plans for workforce and activity, which must be delivered within the local financial allocation.
System Leadership Board
4 July 2019 Enc: 11
Title: Developing our Strategy and the NHS Long Term Plan Framework Author: Ramona Duguid, System Executive Director of Strategy
1

The System Leadership Board and the Cumbria Health and Wellbeing Board will consider the following draft documents in September: • Overarching Strategy for the North Cumbria Integrated Health and Care System • Strategic Delivery Plan 2019 – 2024
NEXT STEPS / AREAS OF WORK TO BE PROGRESSED • Complete the engagement work and collate feedback on changes / additions to our
strategic priorities & commitments. • Clinical & staff engagement – system and specialty specific. • Capacity modelling & activity projections. RECOMMENDATION The SLB is asked to note the report and associated appendices. Appendix 1 – Engagement Document on Developing our Strategy Appendix 2 – Summary of the NHS LTP Implementation Framework Appendix 2a – NHS Long Term Plan Implementation Framework
2

CARE
NORTH CUMBRIA
Developing our strategy For the next five years 2019-2024
Engagement Document Building Integrated Care: Happier, healthier communities

Shaping our plans for the futureOur NHS is constantly changing to meet the growing needs of our community and the increasing demand for services.
In January 2019, the NHS published its ‘Long Term Plan’ setting out how the NHS will meet the challenges it faces. This plan recognises that we need to change and do things differently because:
More people are living longer with a number of long term conditions, such as diabetes, heart disease and dementia – so we need to join up how we co-ordinate and deliver health and care.
The demand for urgent and emergency care is increasing – so we need to be better at identifying the things that affect your health and wellbeing much earlier to prevent you becoming more unwell. There is variation in health outcomes and experiences for our patients – so we need to close the gaps across communities where there are health inequalities.
We need to make better use of new technologies – so we can change the way we access and deliver care, particularly given our rural geography.
We need to improve the experience of our staff and the culture in which they work so we can recruit more staff and develop fulfilling new roles.
We have limited resources and we need to spend this wisely – so we need to reduce duplication and provide care in the right place, in the right way at the right time.
Here in North Cumbria our health and care providers and commissioners are working in partnership with the third sector and our community to develop an integrated care system. This means that instead of working just within our individual organisations, we are working together and collaborating across all parts of the health and care system to improve outcomes for our local population.
We want to hear your views on some of the plans we have for working together to build happier, healthier communities.
Our Vision – where do we want to be?
We want to build a new integrated health and care system together, using our collective capabilities for a healthier and happier population.
Building Integrated Care: Happier, healthier communities
Happier, healthier communities2 |

What does this mean for patients and carers?
We’ll help you to stay well and when you need us we will ensure you get the right care, in the right place at the right time when you need us.
We will help you to be more involved in managing your own health conditions. We will get better at sharing information so you don’t have to tell your story many times. We know ‘There’s No Place Like Home’. So health and care will work together to ensure you only have to go into hospital if absolutely necessary. You will be able to access advice from specialists and their teams more easily – this will include better use of technology, where appropriate.
We will listen to you and value your time so we can ensure you are at the heart of all we do and have a good patient experience.
What does this mean for our staff?We want to be a great place to work and develop
You will feel valued and empowered – as an individual and as a team.
Our shared values of - Kindness, Respect, Ambition, and Collaboration – will guide the way we work from ward to board.
You will have more opportunities to develop your skills and shape new roles to meet the multiple needs of our patients. We will build and develop services which allow our staff to provide treatment and care in a way which is manageable and rewarding. We will develop new services supporting patients with more complex conditions. We will help you to keep the patient at the heart of your care by making it easier to share information with other teams and organisations. We will listen and respond to your ideas and concerns in order to build a culture which is safe, open and forward thinking.
Building Integrated Care: Happier, healthier communities
KINDNESS RESPECT AMBITION COLLABORATION
Happier, healthier communities | 3
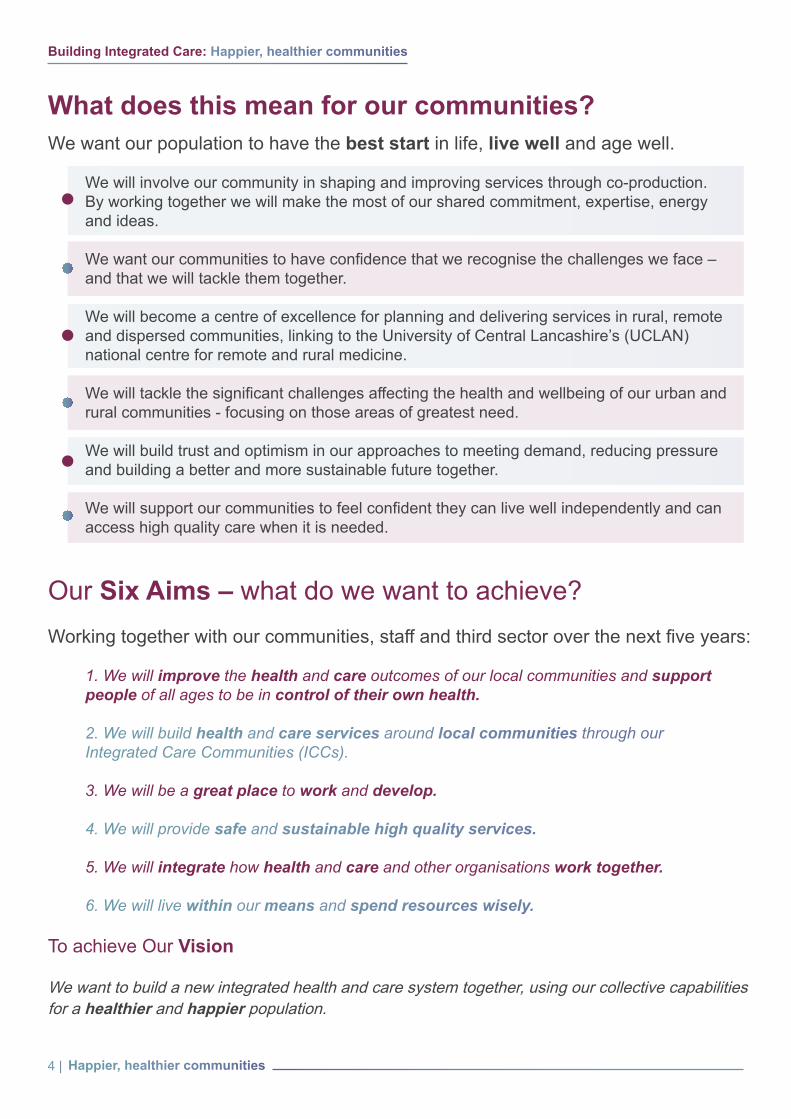
What does this mean for our communities?We want our population to have the best start in life, live well and age well.
We will involve our community in shaping and improving services through co-production. By working together we will make the most of our shared commitment, expertise, energy and ideas. We want our communities to have confidence that we recognise the challenges we face – and that we will tackle them together. We will become a centre of excellence for planning and delivering services in rural, remote and dispersed communities, linking to the University of Central Lancashire’s (UCLAN) national centre for remote and rural medicine. We will tackle the significant challenges affecting the health and wellbeing of our urban and rural communities - focusing on those areas of greatest need. We will build trust and optimism in our approaches to meeting demand, reducing pressure and building a better and more sustainable future together. We will support our communities to feel confident they can live well independently and can access high quality care when it is needed.
Our Six Aims – what do we want to achieve?Working together with our communities, staff and third sector over the next five years:
1. We will improve the health and care outcomes of our local communities and support people of all ages to be in control of their own health.
2. We will build health and care services around local communities through our Integrated Care Communities (ICCs).
3. We will be a great place to work and develop.
4. We will provide safe and sustainable high quality services.
5. We will integrate how health and care and other organisations work together.
6. We will live within our means and spend resources wisely.
To achieve Our Vision
We want to build a new integrated health and care system together, using our collective capabilities for a healthier and happier population.
Building Integrated Care: Happier, healthier communities
Happier, healthier communities4 |

We
need
to w
ork
hard
with
eve
ryon
e in
the
com
mun
ity to
mak
e th
is h
appe
n
Bui
ldin
g In
tegr
ated
Car
e: H
appi
er, h
ealth
ier c
omm
uniti
es
Prov
ide
safe
and
sus
tain
able
hi
gh q
ualit
y se
rvic
es.
Impr
ove
the
heal
th a
nd
care
out
com
es o
f our
lo
cal c
omm
uniti
es a
nd
supp
ort p
eopl
e of
all
ages
to b
e in
con
trol
of
thei
r ow
n he
alth
.
Live
with
in o
ur m
eans
and
sp
end
reso
urce
s w
isel
y.
Be a
gre
at p
lace
to
wor
k an
d de
velo
p.
Build
hea
lth a
nd c
are
serv
ices
aro
und
our
loca
l com
mun
ities
Inte
grat
e ho
w h
ealth
and
ca
re a
nd o
ther
org
anis
atio
ns
wor
k to
geth
er.

Improve the health and care outcomes of our local communities and support people of all ages to be in control of their own health.
• Reduce the health inequalities that exist across our communities.• Work together to address the wider determinants of health - recognising the things that affect a person’s health such as housing and income as well as lifestyle.• Support people to actively manage their own health and wellbeing on a daily basis.• Understand the issues affecting the health and wellbeing of our communities.• Work to provide fair access across our communities to improve outcomes for all, especially for major health conditions.
Things we have already achieved together include:• Developed a ‘starting well’ programme - Giving every child the best start in life - offering improved support e.g. breastfeeding, emotional wellbeing and mental health.• Improved personalised care through dedicated coaching posts (Living Well and Health and Wellbeing Coaches).• Fire and Rescue Service detecting Atrial Fibrillation, an irregular or fast heartbeat, in people’s own homes. • Training Health Walk leaders.• Identified the specific health needs of our local communities in order that we can target the provision of help and support to prevent people becoming ill.
Our focus for the future:• Improve how we use data so we can better target action to prevent people becoming ill, save lives and improve the quality of life, throughout the life course.• A unified approach to Healthy Weight for all ages.• Working together with you to address the wider determinants of health and wellbeing. • Develop social prescribing – enabling people to access appropriate local sources of support.• Introduce targeted stop smoking support.• Improve the detection and management of major health, including cancer as well as cardiovascular and respiratory illnesses.
Case Study26% of children aged 4-5, 35% of children aged 10-11 and 62% of adults in Cumbria are overweight or obese. A range of programmes to support healthy weight are planned during 2019/20. These include local activities such as volunteer-led health walks and increasing the number of breastfeeding peer support groups. We will also be improving support for obese adults. By ‘making every contact count’ we will positively promote healthy weight through the 1000s of conversations that take place every day.
Case Study20% of strokes are caused by Atrial Fibrillation (AF) - an irregular or fast heartbeat. To identify people who might have AF the Cumbria Fire & Rescue Service now carry out AF screening during their fire and safety home visits to the over 65s. Using a mobile screening device people who have a positive result for AF are referred to their local Integrated Care Community (ICC) and invited to visit their GP to discuss appropriate treatment options, potentially reducing their chances of having a stroke in the future.
Our Aim:Building Integrated Care
Happier, healthier communities6 |

• Health and care teams working together organised into eight Integrated Care Communities (ICCs) providing more care closer to home – in the right place at the right time. • Developing and supporting primary and community care services within each Integrated Care Community. • Begin to actively identify people at risk of becoming ill and support them to stay well.• Develop mental health services within our Integrated Care Communities. • Supporting children and families to thrive in communities.
Build health and care services around our local communities.
Things we have already achieved together include:• Developed eight Integrated Care Communities to support the delivery of primary and community care closer to home, reducing the need for admission to hospital and supporting people to return home quicker. • GP records accessible online. • GP online services means people can order repeat prescriptions and book appointments more easily.• Developed new roles within the primary care team including clinical pharmacists and frailty co-ordinators.• Intravenous (IV) and blood transfusions are now available at some community hospitals.• Captured the learning from our work with the community, and developed a co-production toolkit to support more people to help shape service improvements.• Developed our working arrangements with the third sector.• Developed the ‘No Place Like Home’ initiatives – supporting out of hospital care.
Our focus for the future:• Further develop Integrated Care Communities to include mental health, muscular treatment service and children’s services. • Involve the community in developing future services, using their experience and local knowledge. • Develop pathways of care for patients that join together primary, community and secondary care, improve quality and experience. • Improve the opportunities for clinical staff across primary/community and secondary care to work and learn together.• Expand of treatments available locally.• Utilise technology to monitor people’s health at home and develop interventions and target disease areas across communities. • Utilise technology to improve access and communication with our services and help reduce our environmental footprint. • Develop information to help you take control of your own care planning through ‘No Place Like Home.’ www.northcumbriahealthandcare.nhs.uk/projects/no-place-like-home/
Case StudyOur 8 Integrated Care Communities are where health and social care professionals, GPs, the 3rd sector and the community are working together as one team to support the health and wellbeing of local people (more than 90 staff having been appointed). Each Integrated Care Community has a hub which co-ordinates care for local people. The impact has been very positive, with evidence of people avoiding unnecessary hospital admissions by being supported at home and those that do need hospital care being helped to return home more quickly. People with long term conditions are also being supported to stay well. Each Integrated Care Community provides the same core services in addition to services specific to the health and care needs of local people.
Our Aim:Building Integrated Care
Happier, healthier communities | 7

• Live our values and improve the experience of our staff. • Work in a healthy & safe culture.• Staff will feel valued and to know their contribution counts.• Empower staff to improve their job and develop new ways of working through workforce innovation and introducing digital capabilities.• Develop our staff and leaders to work and learn together in networks and across pathways of care.
Building Integrated Care
Be a great place to work and develop.
Things we have already achieved together include:• Created ‘this is us’ our staff identity and engaged on our values. • Reduced vacancies rate and reliance on locums through successful overseas recruitment and almost full recruitment of A&E consultants.• A new GP retention scheme.• Successful and innovative recruitment - ‘is this you.’ • Award winning innovative workforce models.• Training developed with University of Central Lancashire & University of Cumbria. • Cumbria Learning Improvement Collaborative (CLIC) : 16,000 attendees on courses over the last 4 years.• Undertaken Rapid Process Improvement Workshops (RPIW).
Our focus for the future:• Develop our culture and live our values. • Listen and care for our staff and provide opportunities for them to have a rewarding career.• Develop a workforce with targeted plans to ensure we have the right people and skills to meet future needs.• Develop new primary care roles such as first contact physiotherapists, physician’s associates, social prescribing link workers and community paramedics. • Develop attractive career pathways and programmes.• Focus on Talent Management & Succession Planning. • Develop more confidence in involving patients, the community and third sector in service improvement.• Create more significant opportunities for research.• Develop innovative roles which will be more attractive/rewarding.
Case StudyWe continue to run the Step into Work programme, the latest programme helped five individuals who were unemployed to get the training and experience they needed to get work as health care assistants. Further programmes are planned.
Case StudyOur Cumbria Learning and Improvement Collaborative (CLIC) works with teams across our health and care system focusing on how frontline staff can make their service more efficient and successful. Rapid Process Improvement Workshops (RPIW) involve frontline staff and patients looking at ways of improving the way teams work and patient experience. e.g. Accident & Emergency Team at the Cumberland Infirmary Carlisle identified duplications and other efficiencies saving them 600 hours a year which is now spent on patient care.
Our Aim:
Happier, healthier communities8 |

• Develop innovative ways to address workforce supply and demand in key specialities. • Develop and support primary care. • Develop strong networks and partnerships with specialist centres.• Develop our two District General Hospitals to deliver safe and sustainable acute services across our remote and rural footprint.• Improve the quality of mental health services for both adults and children.• Deliver safe personalised services joined up for children and their families.• Improve the models of care and experience for patients with Learning Disability & Autism.
Building Integrated Care
Provide safe and sustainable high quality services.
Things we have already achieved together include:• Progressing the next phases of the West Cumberland Hospital development in Whitehaven.• GP appointments are now available 7 days a week.• In Copeland patients can access appointments at the ‘Same Day Health Centre’ at West Cumberland Hospital.• Training developed with University of Central Lancashire & University of Cumbria.• Developed new workforce models (Composite Workforce).• Introduced a link between Consultants and GPs offering timely advice for patients.• Developed Short Stay Paediatric Assessment Units at both the Cumberland Infirmary and West Cumberland Hospital. • Developed midwifery led care at both Cumberland Infirmary and West Cumberland Hospital. • Developed a mental health crisis support service with Lighthouse.• Developed practical ways of involving people and the community in shaping service developments.• Joint working on emotional wellbeing and mental health of children and young people.
Our focus for the future:• Achieve a Care Quality Commission (CQC) ‘good’ rating for our hospital services.• Develop clinical networks for specialist services. • Integrate emergency care services at both district general hospitals. • Build a new Cancer Centre at Cumberland Infirmary and develop cancer services at the West Cumberland Hospital in partnership with Newcastle Hospitals NHS Foundation Trust.• Improve electronic patient records at Cumberland Infirmary and West Cumberland Hospital. • Develop an integrated stroke service and a Hyper Acute Stroke Unit.• Complete the redevelopment of West Cumberland Hospital.• Improve Mental Health Services in partnership with specialist providers. • Develop and support wider social and independent care services.
Case StudyThe composite workforce is an innovative approach to delivering care where roles and functions traditionally performed by junior and middle grade doctors are performed by a range of appropriately qualified and experienced clinicians. For example we have Advanced Clinical Practitioners (ACPs) & Physician Associates (PAs) delivering care traditionally provided by trainee doctors. The model has been commended by the Care Quality Commission (CQC) for its beneficial effect on the care we provide, and has received a national award for workforce innovation.
Our Aim:
Happier, healthier communities | 9

• Create a single integrated health care organisation for the development and delivery of quality health care services across North Cumbria.• Work closely with social care at a local and strategic level.• Work with third sector partners on the design and delivery of services.• Develop joint commissioning arrangements between health and local authority.• Develop strong networks and partnerships with other NHS organisations to deliver services.• Supporting the development of General Practice services across networks - practices working together.• Develop good relationships across North Cumbria and the North East.
Building Integrated Care
Integrate how health and care organisations work together.
Things we have already achieved together include:• Become one of the first 14 Integrated Care Systems in England.• Enabled primary care, social care & community services to work together in Integrated Care Communities.• Appointed a partnerships officer to support joined up working and build relationships between health, care and the 3rd sector.• Co-ordinated approach to improving outcomes for health and care with our partners.• Established a joint single executive team that has saved £500,000.
Our focus for the future:• Merge the Acute Hospital & Community Trusts and evolve the clinical commissioning group functions as part of a new integrated organisation.• Integrate IT services to improve patient care and staff working. • Increase joint commissioning with the County Council and develop opportunities for commissioning within the Integrated Care System. • Improve mental health services in partnership with specialist providers. • Continue to develop Integrated Care Communities as our core building blocks for primary and community services in our places across north Cumbria,• Develop closer clinical service delivery links with the North East for specialist services. • Support GP Practices to work together creating a primary care provider network. • Involving and working with our communities at every stage.• Continue to develop the input of our NHS Foundation Trust Governors across services.
Case StudyNorth Cumbria University Hospitals NHS Trust & Cumbria Partnership NHS Foundation Trust have been working closer together for the past 18 months. We are now planning to merge these two organisations. This will enable us to work as a single team to provide more joined up care. With a focus on learning and continual improvement we will raise standards, enhance efficiency and better utilise our limited resources.
Our Aim:
Happier, healthier communities10 |

• Create a single North Cumbria health economy budget.• Work together to reduce waste and become more efficient.• Commission more services collectively in order to get better value for money.• Rebalance investment to support out of hospital care and prevention.
Building Integrated Care
Live within our means and spend resources wisely.
Things we have already achieved together include:• Across the NHS in North Cumbria our overall annual deficit has reduced from approx. £80m in 2015/16 to approx. £30m in 2018/19.• At the same time invested in mental health services and Integrated Care Communities to provide community alternatives to hospital stays and worked as a system to reduce the amount of time patients stay in hospital.• Undertaken significant work to ensure cost effective use of medicines.• Reduced waste and duplication across our services.
Our focus for the future:• Reduce our corporate footprint – our bureaucracy, estate, energy and overheads by working collaboratively.• Supporting patients to access services at a local level earlier to avoid becoming acutely unwell.• Securing resources for our system by consistently meeting quality and performance targets and attracting investment funds in innovative projects.• Work with our community, third sector and other partners to make the best use of our collective capabilities• Maximising our productivity and reducing waste.
Case StudyWe have invested in new local services to support patients manage chronic pain and muscular skeletal problems. This has reduced the amount previously spent on sending patients outside of Cumbria by £2.4m.
We have supported our GPs through a Quality Incentive scheme to focus on optimising prescribed medicines to focus on better prescribing of medicines reducing costs by around £1M in 2018/19. We have also saved similar amounts by moving hospital patients on to lower cost medicines without impacting on clinical quality.
We have standardised our approach to using locums and agency staff and have reduced our medical staffing vacancy rate from 31% in 2015 to 11.2% in 2019. We now spend £6m less on locum and agency costs than we did in 2015.
Our Aim:
Happier, healthier communities | 11
Building Integrated Care: Happier, healthier communitiesThere are also surveys you may want to take part in covering:What is important to you, your health and how care is provided | Long term conditions
If you would like to become more involved, you can become a member of our Trust - have your say to help improve and shape our services as well as receiving regular updates from us including our latest news. www.cumbriapartnership.nhs.uk/the-trust/members
You can access our questionaire here:www.northcumbriahealthandcare.nhs.uk/have-your-say/
Alternatively return your completed questionnaire to: Engagement at Rosehill | 4 Wavell Drive | Carlisle | Cumbria | CA1 2SE
We want your views...On the aims we have set out and our focus for the future.

APPENDIX 2 1. NHS LONG TERM PLAN IMPLEMENTATION FRAMEWORK The NHS Long Term Plan was published in January 2019. In June 2019 a framework to support its implementation was also published. The framework does not change the commitments and priorities set out in the NHS LTP but it provides guidance on the approach systems should be undertaking to create their five year strategic plans by November 2019. The key headlines from the implementation framework in the context of service provision and care are summarised below. A full copy of the framework is attached at Appendix 2a of this report. 1.1 New service model fit for 21st Century 1.1.1 Primary and Community Services As a minimum, system plans should focus on four things:
- meeting the new funding guarantees for primary medical and community health services;
- supporting the development of their PCN; - improving the responsiveness of community health crisis response services to
deliver the services within two hours of referral, and reablement care within two days of referral; and
- creating a phased plan of the specific service improvements and impacts they will enable primary and community services to achieve, year by year, taking account of the national phasing of the new five-year GP contract.
• For each of the four years from 2020/21 to 2023/24, system plans must set out,
indicatively, how they are going to meet the new primary medical and community health service funding guarantee of a £4.5 billion real terms increase in 2023/24 over 2018/19 planned spend.
• The four strategic priorities for community health services are: (i) delivering improved crisis response within two hours, and reablement care within two days; (ii) providing ‘anticipatory care’ jointly with primary care; (iii) supporting primary care to developed Enhanced Health in Care Homes; (iv) building capacity and workforce to do these three things, including by implementing the Carter report and using digital innovation. Of these, (ii) and (iii) are a joint enterprise with GP practices as part of PCN delivery.
1.1.2 Reducing pressure on emergency hospital services • System plans should show how local urgent and emergency care services will continue
to develop to provide an integrated network of community and hospital-based care. • The outcomes from the clinical review of standards (in particular A&E standards) will
need to be included in system plans.
1

1.1.3 Giving people more control over their health and more personalised care
• Systems will be expected to set out how they will use the funding available to them to
implement the six components of the NHS Comprehensive Model for Personalised Care:
- Shared decision making - Personalised care and support planning - Enabling choice, including legal rights to choice - Social prescribing and community-based support - Supported self-management - Personal health budgets and integrated personal budgets
1.1.4 Digitally-enabling primary care and outpatient care
• Systems should set out in their plans how they will increase the use of digital tools to transform how outpatient services are offered and provide more options for virtual outpatient appointments. As part of this, systems should identify which specialties they intend to prioritise as they work towards removing the need for up to a third of face-to-face outpatient visits.
• In General Practice – delivery of an online consultation offer in each practice by April 2020 and a video consultation offer to all patients by April 2021
1.1.5 Better care for major health conditions: Improving cancer outcomes Improving cancer outcomes including on early diagnosis and survival, while improving operational performance through interventions by: • Improving the one-year survival rate. • Improving bowel, breast and cervical screening uptake; • Roll-out of FIT for symptomatic and non-symptomatic populations in line with national
policy, and HPV as a primary screen in the cervical screening programme; • Improving GP referral practice; • Implementation of faster diagnosis pathways; • Improving access to high-quality treatment services, including through roll out of
Radiotherapy Networks, strengthening of Children and Young People’s Cancer Networks, and reform of Multi-Disciplinary Team meetings;
• Roll-out of personalised care interventions, including stratified follow-up pathways, to improve quality of life.
• Cancer Alliances will need to set out how the plans will address unwarranted variation, improve patient experience, and be supported by appropriate workforce.
2

1.1.6 Better care for major health conditions: Improving mental health services
Nationwide mental health priorities include:
• 345,000 additional children and young people (CYP) aged 0-25 will be able to access support via NHS-funded mental health services (in addition to the Five Year Forward View for Mental Health’s commitment to have 70,000 additional CYP accessing NHS Services by 2020/21);
• Expansion of access to specialist community perinatal mental health services in 2019/20;
• By 2020/21 there will be 100% coverage of 24/7 adult crisis resolution and home treatment teams operating in line with best practice;
• The continued expansion of CYP mental crisis services so that by 2023/24 there is 100% coverage of 24/7 crisis provision for CYP which combines crisis assessment, brief response and intensive home treatment functions;
• The development of local mental health crisis pathways including a range of alternative services so that by 2023/24 there is 100% roll out across the country.
System plans should clearly set out how the additional investment in mental health services will be applied.
1.1.7 Better care for major health conditions: Shorter waits for planned care
• Systems need to set out how they will expand the volume of planned surgery year-on-year, cut long waits, and reduce the size of waiting lists over the next five years.
• Systems will ensure that no patient will have to wait more than 52-weeks from referral to treatment (RTT). They will also need to implement a planned NHS-managed choice process across the country for all patients who reach a 26-week wait.
• By 2023/24, systems should have scaled their provision of First Contact Practitioners (FCP) so that all patients across England have access. This will provide faster access to diagnosis and treatment for people with MSK conditions and support more patients to effectively self-manage their conditions.
1.2 Increasing focus on Population Health – moving to integrated care systems
everywhere
• Delivering service transformation of the scale required will need a well-developed system and effective underpinning infrastructures. The ICS maturity matrix sets out the characteristics required in order to ensure all systems can reach a mature level by April 2021.
3

The characteristics of a mature ICS include: - Collaborative and inclusive multi-professional system leadership, partnerships and
change capability, with a shared vision and objectives including an independent chair; - An integrated local system, with population health management capabilities which
support the design of new integrated care models for different patient groups, with strong PCNs and integrated teams and clear plans to deliver the service changes set out in the Long Term Plan; improving patient experience, outcomes and addressing health inequalities;
- Developed system architecture, with clear arrangements for working effectively with all partners and involving communities as well as strong system financial management and planning (including a way forward for streamlining commissioning, and clear plans to meet the agreed system control total moving towards system financial balance);
- A track record in delivering nationally agreed outcomes and addressing unwarranted clinical variation and health inequalities;
- A coherent and defined population, where possible contiguous with local authority boundaries.
• Mature ICSs should also clearly set out how the provider and commissioner landscape is developing.
1.3 More NHS action on prevention
• Systems will need to work in close partnerships with regional and local Directors of
Public Health to set out how they and their local authority partners who have commissioning responsibility for many of these preventative services will develop and deliver prevention activities that respond to local health needs and deliver on the commitments in the Long Term Plan, including obesity, smoking, alcohol, sexual health, antimicrobial resistance and air pollution. Additional investment in these areas will also be targeted and need to be factored into system plans.
1.4 Delivering further progress on care quality and outcomes
A strong start in life for children and young people • Local Maternity Systems should set out how they will ensure that babies born
anywhere in England has the best possible start in life, consistent with the Long Term Plan commitments and the conclusions of Better Births.
• Local plans to improve outcomes for children and young people should:
- Establish local leadership – including named clinical and management
leaders, co-production with children, young people, families and carers and bringing together local leaders from across the NHS, local government, education and other partners to design and deliver transformation for the system;
- Show how they will improve performance of childhood screening and immunisation programmes and meet the base level standard in the NHS public health functions agreements;
4
Local plans should also outline how the Long Term Plan commitments will be dlivered for children and young people, with a specific focus on:
• Developing age-appropriate integrated care, integrating physical and mental health
services, enabling joint working between primary, community and acute services, and supporting transition to adult services;
• Improving care for children with long-term conditions, such as asthma, epilepsy, diabetes, and complex needs;
• Treating and managing childhood obesity; • Supporting the expansion of Children and Young People’s mental health services; • Improving outcomes for children and young people with cancer.
Learning Disabilities & Autism System plans should clearly set out: • Their share of the required further reduction inpatient usage and beds; • Learning disability and autism physical health checks for at least 75% of people
aged over 14 years; • how proposals for people with learning disabilities and/or autism align with their
plans for mental health, special educational needs and disability (SEND), children and young people’s services and health and justice;
• the local offer for autistic young people, people with a learning disability and their families;
• how NHS-led provider collaboratives will be developed locally and should ensure that digital plans use the reasonable adjustment ‘digital flag’ in the patient record or, where this is not available, use the Summary Care Record as an alternative.
• System investment should identify what community provision is in place for intensive, crisis and forensic community support. This includes seven-day specialist multidisciplinary services and crisis care and community teams for children and young people that can be built upon or strengthened with clear alignment with mental health and social care.
1.5 Improving care for major health conditions
• Cardiovascular Disease (CVD) - System plans should set out how they will, over the next five years, improve the prevention early detection and treatment of cardiovascular disease.
• Stroke Care - Systems are asked to ensure they have robust plans, and effective local clinical and system leadership to develop and improve stroke services, centred around delivering Integrated Stroke Delivery Networks (ISDNs), improving and configuring stroke services, to ensure that all patients who need it, receive mechanical thrombectomy and thrombolysis. Early Supported Discharge (ESD) should be routinely commissioned and available to all patients for whom it is appropriate, with systems developing plans to integrate ESD and community services.
• Diabetes - Systems are asked to set out their approach for delivering improved services in line with the Long Term Plan commitments for people with Type 1 and 2 diabetes.
5

• Respiratory Disease - System plans should set out how they will support local identification of respiratory disease and increase associated referrals to pulmonary rehabilitation services for those who will benefit, particularly for the most socio-economically disadvantaged people who are disproportionately represented in this patient cohort
1.6 Workforce, Digital and Finance
Workforce System plans will need to cover as a minimum its plans to address the workforce priorities on: • Making the NHS the best place to work: • Improving leadership culture: • Delivering a holistic approach to workforce transformation and workforce growth • Changing the workforce operating model Digital • Systems need to develop a comprehensive digital strategy and investment plan
consistent with the Tech Vision that describes how digital technology will underpin their local system’s wider transformation plans over the next five years. This includes, amongst other priorities, their approach to ensuring all secondary care providers are fully digitised by 2024 and that these are integrated with other parts of the health and care system.
• Digital transformation will require all NHS staff to make adjustments in how they work – from the receptionist who supports outpatient clinics to those on their Board. The interim NHS People Plan addresses the need for an increase in the technical skills of the NHS workforce for both specialist and non-specialist staff.
Finance • Central to the system planning process is the question of how resources allocated to
local health systems to meet population need will be deployed over a five-year period to deliver the commitments set out in the Long Term Plan, including delivery of the five financial tests.
- To meet financial Test 1 in the Long Term Plan plans must demonstrate how
organisations will return to, or maintain, financial balance including the impact on the financial performance of each provider and commissioner organisation.
- As part of this systems will need to work with providers so that, as a minimum, all providers deliver cash-releasing productivity growth of at least 1.1% a year in line with financial Test 2; and providers in deficit deliver an additional cash-releasing productivity benefit of at least 0.5% a year;
- Plans to incorporate system actions to maximise efficiencies and support appropriate reductions in the growth in demand for care, as required by financial Test 3.
- Financial Test 4 in the Long Term Plan requires the NHS to reduce variation across the health system, improving providers’ operational and financial performance
6

- Financial Test 5 in the Long Term Plan requires the NHS to make better use of capital investment and its existing assets to drive transformation.
1.7 Next steps and submission requirements Publication of the Implementation Framework begins the process of strategic system planning. System plans for delivery through to 2023/24 are required, with an initial submission in September 2019 and a final submission to follow by mid November 2019. Systems are asked to provide two elements at both the September and November milestones: • Strategy delivery plan: A document that sets out what the system plans to deliver
over the next five years. Whilst there is no template for this document, systems are encouraged to ensure that their plan covers all the elements set out in Chapter 1 of this Implementation Framework, including: a description of local need; what service changes will be taken forward and how; how the local system infrastructure will be developed – including workforce, digital and estates; how efficiency will be driven through all local activity, how local engagement has been undertaken to develop the plan and how financial balance will be delivered;
• Supporting technical material: Successful delivery will require systems plans to be underpinned by realistic plans for workforce and activity, which must be delivered within the local financial allocation. Templates and tools will be provided to support systems in this. Draft templates to support with modelling of finance, activity and key commitment metrics are provided in alongside this document. A full version of the finance and activity template will be provided in early July 2019
7

NHS Long Term PlanImplementation
Framework
June 2019
Appendix 2a

2 I NHS Long Term Plan Implementation Framework
Contents 1. Introduction to the NHS Long Term Plan Implementation Framework ............................ 3 2. Delivering a new service model for the 21st century ...................................................... 7
Transformed ‘out-of-hospital care’ and fully integrated community-based care .................. 7 Reducing pressure on emergency hospital services .......................................................... 9 Giving people more control over their own health and more personalised care ................. 9 Digitally-enabling primary care and outpatient care ......................................................... 10 Better care for major health conditions: Improving cancer outcomes ............................... 10 Better care for major health conditions: Improving mental health services ....................... 11 Better care for major health conditions: Shorter waits for planned care ........................... 13
3. Increasing the focus on population health ................................................................... 14 4. More NHS action on prevention .................................................................................. 15 5. Delivering Further progress on care quality and outcomes ........................................... 16
A strong start in life for children and young people .......................................................... 16 Learning disabilities and autism ....................................................................................... 17 Better care for major health conditions ............................................................................ 19
Cardiovascular disease ................................................................................................ 19 Stroke care .................................................................................................................. 19 Diabetes ...................................................................................................................... 20 Respiratory disease ..................................................................................................... 20
Research and innovation to drive future outcomes improvement ..................................... 21 Genomics ........................................................................................................................ 22 Volunteering .................................................................................................................... 22 Wider social impact ......................................................................................................... 22
6. Giving NHS staff the backing they need ....................................................................... 23 7. Delivering digitally-enabled care across the NHS ......................................................... 25 8. Using taxpayers’ investment to maximum effect........................................................... 28
Financial and planning assumptions for systems ............................................................. 28 Improving productivity ...................................................................................................... 29 Reducing variation across the health system ................................................................... 30
9. Next steps .................................................................................................................... 31 Annex A Funding the Long Term Plan ................................................................................ 33 Annex B: Financial assumptions for strategic plans ............................................................ 36 Annex C: LTP headline metrics ........................................................................................... 40 Annex D: Supporting wider social goals .............................................................................. 42
NHS Long Term Plan Implementation Framework I 3
Introduction to the NHS Long Term Plan Implementation Framework
1.1 The NHS Long Term Plan, published in January 2019, set out a 10-year practical programme of phased improvements to NHS services and outcomes, including a number of specific commitments to invest the agreed NHS five-year revenue settlement. This Implementation Framework sets out the approach Sustainability and Transformation Partnerships (STPs)/Integrated Care Systems (ICSs) are asked to take to create their five-year strategic plans by November 2019 covering the period 2019/20 to 2023/24. These plans should be based on realistic workforce assumptions and deliver all the commitments within the Long Term Plan. This document does not repeat the rationale and commitments set out in the Long Term Plan.
1.2 System plans will be aggregated, brought together with additional national activity and published as part of a national implementation plan by the end of the year so that we can properly take account of the Government Spending Review decisions on workforce education and training budgets, social care, councils’ public health service and NHS capital investment. The national implementation plan will set out initial performance trajectories and programme milestones to deliver Long Term Plan commitments.
1.3 Some of the commitments in the Plan are critical foundations to wider change. All systems must deliver on these foundational commitments for both service transformation (Chapter 2) and system development (Chapter 3) in line with nationally defined timetables or trajectories, including the Government’s five financial tests which are set out in Chapter 8, with proposed metrics included in Annex C.
1.4 Systems will also have substantial freedoms to respond to local need, prioritise, and define their pace of delivery for the majority of commitments (Chapters 4 and 5), but will need to plan to meet the end points the Long Term Plan has set.
1.5 Plans should prioritise actions that will help improve the quality of, and access to, care for their local populations, with a focus on reducing local health inequalities and unwarranted variation. Ensuring that we back our staff (Chapter 6) and develop a digitised NHS (Chapter 7) will also be at the heart of local plans.
1.6 The national and regional support that systems can draw on is signposted throughout this Implementation Framework alongside a number of nationally delivered activities to support local implementation. It aims to reflect our new national operating model. Our ambition is to better coordinate how national and regional teams are working together to provide support to systems, based on local needs.
1.7 The Implementation Framework has been developed and tested with many of the stakeholders that were involved in developing the Long Term Plan. We have sought views from systems across the country to inform the development of the Implementation Framework. We have also engaged with stakeholders, including the NHS Assembly and partners from Local Government Association, NHS Providers, the NHS Confederation, Academy of Royal Medical Colleges, government and VCSE organisations. Based on their feedback, we have focused this Implementation Framework on setting out what the NHS needs to deliver from 2020/21 through to 2023/24, including the national ‘must dos’, whilst leaving space for systems to set out
4 I NHS Long Term Plan Implementation Framework
how they will deliver and phase progress in line with local priorities. It does not repeat the asks of the 2019/20 Operational Planning and Contracting Guidance.
An integrated approach to strategic and operational planning
1.8 STPs/ICSs are expected to bring together members organisations and wider partners, adopting a common set of principles and leadership behaviours as they develop and deliver plans. In doing this, systems will be expected to ensure that their plans align with the following principles:
• Clinically-led: In practice this means that systems will need to identify and support senior clinicians to lead on the development of implementation proposals for all Long Term Plan commitments that have clinical implications and on the totality of their plan.
• Locally owned: Build on existing engagement with local communities to ensure they can meaningfully input into the development of local plans. Local government will be key partners to developing system plans and are asked to engage throughout the process. Similarly, the voluntary sector and other local partners, including representatives from the most marginalised communities who often experience the poorest health and greatest inequalities, should be involved. Support for this is available through the NHS Involvement Hub, the national resource pack and the nationally commissioned Healthwatch contract.
• Realistic workforce planning: The interim NHS People Plan sets out the national context. Systems should set out realistic workforce assumptions, matched to activity and their financial envelope. Plans should also show the steps to be taken locally to improve retention and recruitment.
• Financially balanced: The outline business rules for planning are set out in Chapter 8 of this Implementation Framework, with supporting assumptions and financial allocations set out in Annexes A and B. Systems need to show how they will deliver the commitments in the plans within the resources available. Local plans will need to include the financial recovery plans for individual organisations in deficit against specified deficit recovery trajectories (test 1), with actions to achieve cash releasing savings (test 2) including through the reduction of unwarranted variation (test 4) and how they will moderate growth demand (test 3). Plans should set out capital investment priorities for capital budgets being agreed through the forthcoming Spending Review (test 5).
• Delivery of all commitments in the Long Term Plan and national access standards: The Long Term Plan was based on an inclusive and thorough process that identified prioritised, costed interventions based on clinical evidence and patient and public views. The Long Term Plan will be implemented comprehensively, with system plans setting out what their contribution to this will be. Plans which will cover the four-year period April 2020 to March 2024 will also need to set out how systems will continue to maintain and improve performance for cancer treatment, mental health and A&E, to the point at which any new standards proposed by the Clinical Review and accepted by Government are implemented. They should also set out how elective care activity will be increased to reduce elective waiting lists and eliminate 52+ week waits.
• Phased based on local need: Whilst the Long Term Plan must be delivered in full, this does not mean that all initiatives should be implemented simultaneously everywhere. National requirements for some foundational requirements have been set out in Chapters 2 and 3. Beyond this, the scale and pace of local implementation should be based on local need and priorities.

NHS Long Term Plan Implementation Framework I 5
• Reducing local health inequalities and unwarranted variation: System plans should set out how they will use their allocated funding to deliver tangible improvements in health outcomes and patient experience and help reduce local health inequalities. System plans should also use available data to understand how their outcomes compare with their peers, identify and reduce unwarranted variation.
• Focussed on prevention: System plans must consider not just how to deliver health services but how to prevent ill health.
• Engaged with Local Authorities: System plans should expect to be developed in conjunction with Local Authorities and with consideration of the need to integrate with relevant Local Authority services.
• Driving innovation: All system plans must consider how to harness innovation locally.
1.9 All systems will be expected to agree their plans by mid-November 2019 and publish them shortly thereafter. These strategic plans will form the foundation of service and system change over the next five years. Whilst they will continue to evolve over that period, it is important that systems are transparent about their plans and ambitions. Annex C sets out the initial proposed headline measures against which the success of the NHS will be assessed. Views on the appropriateness of these measures are invited. These will then be finalised as part of the national Implementation Plan in the Autumn and used as the cornerstone of the mandate and planning guidance for the NHS for the next 5 years. Systems should therefore show how they plan to make progress against them. Further details on these measures will be published shortly.
1.10 As part of our new shared operating model, NHS England and NHS Improvement will work through our integrated regions with local systems as they develop and finalised their plans. For foundational elements as set out in Chapters 2 and 3 of this document, and for other Long Term Plan commitments where local need means rapid progress is required in the early years of implementation. Regions will seek greater levels of detail, including trajectories. National teams will work with regions to ensure that credible plans and trajectories (where applicable) exist to deliver Long Term Plan commitments and the five financial tests over the next five years. Further details on how national and regional teams will work together and support systems is set out in the Chapter 9.
A proactive approach to prevention and reducing health inequalities
1.11 Over the next five and ten years the NHS will progressively increase its focus on prevention and ensure that inequalities reduction is at the centre of all our plans. A Government’s forthcoming Prevention Green Paper should provide further opportunities for the NHS and Government to go further, faster, in prevention and inequality reduction and will feed into future iterations to system plans.
1.12 System plans should demonstrate the key areas of inequality they will tackle and how additional funding is targeted, for example actions that will address the health inequalities experienced by disadvantaged or vulnerable groups, such as people with disabilities, LGBT+, BME communities as well as others. Systems can draw on Public Health England’s (PHE) Place Based Approaches to Reducing Health Inequalities and the Menu of Evidence Based Interventions for reducing Health Inequalities being published in the summer as they develop their plans. Systems should complete an Equality Impact Assessment for their plans.

6 I NHS Long Term Plan Implementation Framework
Investment to support transformation
1.13 Systems already have five-year CCG allocations. This Implementation Framework also sets out where additional funding will be made available to support specific commitments and where activity will be paid for or commissioned nationally. Largely, additional funding will be provided in two ways:
• Where activity is expected to happen across the country and in every system, funding will generally be made available on a ‘fair share’ basis. Each system will be given an indicative additional allocation to reflect in their plans. Access to this service development funding will be conditional upon systems agreeing their strategic plans with NHS England/Improvement’s regional teams, who will be advised by the National Service Transformation Directors. More mature systems will have greater autonomy over how additional resources are deployed. Detail of the indicative additional allocation for each system will be communicated alongside this Implementation Framework.
• Some commitments within the Long Term Plan will of necessity have to be funded in a targeted way either because the whole country is not covered by the service based on specific needs, or to test implementation approaches as evidence is developed and service specifications finalised. The Implementation Framework identifies the commitments that will be funded in this way, and when funding will be available. Where there is a local ambition to act as a testing site for new approaches or interventions, and receive a share of the associated funding, systems should discuss and agree this with their region through the summer planning process. Individual national programme teams will also be able to share more information on how targeted funding can be accessed.
1.14 National aggregates for both the ‘fair share’ and targeted funding are set out at Annex A.

NHS Long Term Plan Implementation Framework I 7
Delivering a new service model for the 21st century
2.1 Delivering the fundamental service changes, set out in this chapter, along with the productivity ambitions set out in Chapter 8, are a prerequisite for being able to develop and improve other services based on local population health needs. Plans should set out how these foundational commitments within the Long Term Plan will be delivered and their five-year trajectories for doing so.
Transformed ‘out-of-hospital care’ and fully integrated community-based care
2.2 By July 2019 all of England will be covered by PCNs supported by significant investment (almost £1.8 billion by 2023/24) as set out in the five-year framework for GP contract reform. This investment is linked to a clear set of deliverables, laid out in the contract documents.
2.3 PCNs are encouraged to make early progress in the service specifications that commence from 2020/21 including the anticipatory care requirement (with community services); Enhanced Health in Care Homes; structured medication review requirements for priority groups; personalised care and early cancer diagnosis support. PCNs should also develop their partnerships with other health and care providers, particularly community and mental health services.
2.4 The GP contract guarantees funding to develop these multidisciplinary teams and will support the recruitment of 20,000 additional staff to work alongside doctors and nurses in PCNs over the next five years. The scheme will meet a recurrent 70% of employment costs for additional clinical pharmacists, physician associates, physiotherapists and community paramedics; and 100% of the costs of additional social prescribing link workers. Growth has been phased over the five-year period to align with supply and the developing maturity of PCNs. To effectively meet their diverse population’s needs, these staff will need to work alongside those from NHS, local authority and other organisations to provide integrated community care.
2.5 The Long Term Plan reconfirmed the commitment to ensure an increase of 5,000 full time equivalent doctors working in general practice as soon as possible. In addition to plans to recruit and retain more doctors and nurses – including additional fair shares funding for a two-year fellowship scheme for the newly qualified – growth in these roles will be supported through increased GP contract funding, which rises by £978 million a year by 2023/24 as a result of investment under the new contract. £12 million is also being invested in GP retention in 2019/20 and 2020/21 and will be allocated on a fair shares basis to STPs.
2.6 This workforce will be supported through a network of primary care and community training hubs that will deliver a set of core functions to educate, train and support the current and future workforce working as part of multidisciplinary teams. All STPs and ICSs will have access to the functions of a training hub by March 2020 and will receive a fair shares funding allocation from 2019/20 to 2023/24 to support this.
2.7 The framework for GP contract reform committed to the introduction of a new Investment and Impact fund for PCNs, which will start in 2020 and will support delivery of the Long Term Plan. Funding is expected to rise to £300 million in 2023/24.
2.8 The national PCN Development Programme will provide fair shares funding and support to local systems as they develop their PCNs including ensuring that each PCN

8 I NHS Long Term Plan Implementation Framework
Clinical Director is able to access leadership development support. Further details on the support available to systems is available here.
2.9 As a minimum, system plans should focus on four things:
i. meeting the new funding guarantees for primary medical and community health services;
ii. supporting the development of their PCN; iii. improving the responsiveness of community health crisis response
services to deliver the services within two hours of referral, and reablement care within two days of referral; and
iv. creating a phased plan of the specific service improvements and impacts they will enable primary and community services to achieve, year by year, taking account of the national phasing of the new five-year GP contract.
2.10 This part of the plan must involve and ideally be agreed with community providers, primary care providers, and the new Clinical Directors of Primary Care Networks. It should also be subject to dedicated discussion at all Health and Wellbeing Boards. The voluntary sector and Local Medical Committees should also be involved.
i. Meeting the new funding guarantee
2.11 For each of the four years from 2020/21 to 2023/24, system plans must set out, indicatively, how they are going to meet the new primary medical and community health service funding guarantee of a £4.5 billion real terms increase in 2023/24 over 2018/19 planned spend. This equates to a £7.1 billion cash increase and covers primary medical, community health and continuing health care (CHC) spend. Every region must meet its share from April 2020 onwards. That means every system has to agree what its share will be with its region and include that number in its system plan. Then, in 2023/24, the funding guarantee will directly apply to every ICS without exception.
2.12 As they do this, systems will need to ensure they honour the GP contract entitlements over and above existing baseline spend. They will need to show the distribution of funding across primary care, community health and CHC services.
ii. Supporting Primary Care Networks
2.13 System plans should show what development support will be provided. Systems should prioritise helping PCNs build excellent relationships with their community partners. The support they offer can only be designed with the full involvement of the Clinical Directors of the PCNs and their community health services partners. Dedicated national support funding is being provided as a “floor”, and a PCN development prospectus will be published in the summer.
iii. Improving the responsiveness of community health crisis response services to
deliver the services within two hours of referral and reablement care within two days of
referral
2.14 The four strategic priorities for community health services are: (i) delivering improved crisis response within two hours, and reablement care within two days; (ii) providing ‘anticipatory care’ jointly with primary care; (iii) supporting primary care to developed Enhanced Health in Care Homes; (iv) building capacity and workforce to do

NHS Long Term Plan Implementation Framework I 9
these three things, including by implementing the Carter report and using digital innovation. Of these, (ii) and (iii) are a joint enterprise with GP practices as part of PCN delivery. Nationally, we will develop standard service specifications that take into account the phasing of funding increases.
iv. Implementing service improvements and achieving impact
2.15 The funding guarantee, primary care network support, and focusing on community services transformation are necessary means - but they are not the ends.
2.16 System plans should set out an initial view of what services improvements they realistically are aiming to achieve when, demonstrably phased over the next four years. As they do this, they will need to take into account of the phasing of the new GP contract including the seven new national service specifications and full implementation of the final years of the pre-existing GP Forward View commitments, recognise that community services will need a major capacity boost to deliver Long Term Plan goals, and that primary care faces major workforce and workload challenges. The schedule of improvements must be agreed with community providers and Clinical Directors of Primary Care Networks and be linked to meeting the new funding guarantee.
2.17 Linked to phased improvements, system plans will ultimately need to set out the quantified impacts expected on “downstream” hospital NHS utilisation, as well as better outcomes. Realistically, for a challenged system this exercise is likely to be best undertaken in the next 12-24 months in the light of planned improvements, rather than now. Equally, leading systems will be able to include more detail in their plans now and show the way forward for the rest of the country.
2.18 The Long Term Plan set out the steps that will be taken to build a more carer-friendly NHS. Local plans should set out how carer identification and support is being addressed locally, to help improve outcomes for carers. More information on the support the national carers team will provide to systems can be found here.
2.19 National support for systems as they develop their plans can be found here.
Reducing pressure on emergency hospital services 2.20 System plans should show how local urgent and emergency care services will
continue to develop to provide an integrated network of community and hospital-based care. Where systems can reduce the pressure on their emergency services they will benefit from an upside financial, capacity and staffing ‘dividend’ that can be reinvested in their local priorities. Field testing for the Clinical Review of Standards has now begun; learning from this will be considered before any changes are recommended for wider roll out. In the interim, systems should continue ongoing service improvement work so that performance is maintained and improved for A&E, to the point at which any new standards, proposed by the Clinical Review and accepted by Government, are implemented.
2.21 Support available to systems as they develop their emergency care services can be found here.
Giving people more control over their own health and more personalised care
2.22 Systems will be expected to set out how they will use the funding available to them to implement the six components of the NHS Comprehensive Model for Personalised

10 I NHS Long Term Plan Implementation Framework
Care as set out in Universal Personalised Care. Regional teams will support systems to develop local trajectories in line with the national ambition in the Long Term Plan, including their shares of social prescribing activity and personal health budget take up.
2.23 Funding to support the delivery of Universal Personalised Care is available as follows:
• Through the Network Contact Direct Enhanced Services (DES) from 2019/20, for employment of social prescribing link workers;
• Targeted funding to deliver the NHS Comprehensive Model for Personalised Care from 2019/20 to 2021/22;
• Targeted funding from 2019/20 to 2021/22 to CCG champions to support other local areas to deliver components of the Comprehensive Model;
• NHS England and NHS Improvement has committed to increase its contribution to funding both children’s hospices and children’s palliative and end of life care services. More detail will be set out shortly, including arrangements for match-funding CCGs where they commit to increase their local investment. System plans should reflect this local increase in investment.
2.24 Additional support for developing and delivering system plans will be available through the national personalised care team and can be found here.
Digitally-enabling primary care and outpatient care 2.25 Systems should set out in their plans how they will increase the use of digital tools to
transform how outpatient services are offered and provide more options for virtual outpatient appointments. As part of this, systems should identify which specialties they intend to prioritise as they work towards removing the need for up to a third of face-to-face outpatient visits, reducing outpatient visits by 30 million a year nationally, and reducing the need for unnecessary patient and staff travel. Systems should also demonstrate in their plans how they will work with their CCGs and GP practices to deliver the commitments relevant to digital primary care set out in the NHS Operational Planning and Contracting Guidance 2019/20, GMS contract for 2019/20 and GMS contract framework. This includes the delivery of an online consultation offer in each practice by April 2020 and a video consultation offer to all patients by April 2021. The programme of work to deliver digital first primary care is being finalised and by the end of July 2019, we will confirm the programme arrangements and process for managing targeted funding for health systems. Selected sites in each region will test and validate the approach to digital first primary care.
2.26 Together with NHSX we will support systems to develop and deliver their plans. Further information can be found here.
Better care for major health conditions: Improving cancer outcomes
2.27 Local systems should engage with their Cancer Alliances to set out practically how they will deliver the Long Term Plan commitments for cancer over the next five years including on early diagnosis and survival, while improving operational performance through interventions by:
• Improving the one-year survival rate. • Improving bowel, breast and cervical screening uptake; • Roll-out of FIT for symptomatic and non-symptomatic populations in line with
national policy, and HPV as a primary screen in the cervical screening programme;

NHS Long Term Plan Implementation Framework I 11
• Improving GP referral practice; • Implementation of faster diagnosis pathways; • Improving access to high-quality treatment services, including through roll out
of Radiotherapy Networks, strengthening of Children and Young People’s Cancer Networks, and reform of Multi-Disciplinary Team meetings;
• Roll-out of personalised care interventions, including stratified follow-up pathways, to improve quality of life.
• Cancer Alliances will need to set out how the plans will address unwarranted variation, improve patient experience, and be supported by appropriate workforce.
2.28 By 2023/24 over £400 million of additional funding will have been distributed to Cancer Alliances on a fair shares basis to support delivery of the Long Term Plan ambitions for cancer. Targeted funding will also be available to support the development and spread of innovative models of early identification of cancer:
• We are already establishing lung health checks in ten areas of the country with some of the worst mortality rates from lung cancer. From April 2020, we will continue to roll these out, based on the evidence gathered, in areas with higher mortality rates.
• In 2019/20, Cancer Alliances are working to implement the first round of Rapid Diagnostic Centres (RDCs). RDC rollout will be agreed as part of LTP implementation planning in the Autumn.
• Alongside lung health checks and RDCs, we will also support new innovations in healthcare for early diagnosis. Based on identification of promising new technologies and service models by an expert clinical group, we will drive the rapid take-up and spread of innovation across the country led by the Cancer Alliances.
2.29 National and regional teams will work to support Cancer Alliances and systems, details of this support can be found here.
Better care for major health conditions: Improving mental health services
2.30 The Long Term Plan committed that investment in mental health services will grow faster than the NHS budget overall for each of the next five years, creating a new ringfenced local investment fund worth at least £2.3 billion a year by 2023/24. In addition, children and young people’s mental health services will grow faster than both overall NHS funding and total mental health spending. Funding to deliver the full suite of Five Year Forward View for Mental Health (FYFVMH) and NHS Long Term Plan mental health commitments will be available via a mix of CCG baseline allocations and transformation funding available over the five-year period. System plans must now set out how they will meet this mental health investment standard and use the investment and the additional funding set out in this document to deliver the commitments in the Long Term Plan and the Five Year Forward view for Mental Health including taking account of the patient and carers race equality framework we are developing.
2.31 Where appropriate, specialised mental health services and learning disability and autism services will be managed through NHS-led provider collaboratives over the next five years. NHS-led provider collaboratives will become the vehicle for rolling-out specialist community forensic care. The specialised commissioning mental health budget will be increasingly devolved directly to lead providers for adult low and medium secure mental health services, CAMHS Tier 4 services and adult eating

12 I NHS Long Term Plan Implementation Framework
disorder inpatient services. NHS-led provider collaboratives will be able to reinvest savings they make on improving local services and pathways.
2.32 Growing CCG allocations across the five-year period are available to systems to deliver the plan including stabilising and expanding core community teams for adults and older adults with severe mental health illnesses. This includes testing and rolling out adult community access standards once agreed, services for people with specific and complex needs for people with a diagnosis of ‘personality disorder’, Early Intervention in Psychosis (EIP), adult eating disorders, and mental health community rehabilitation. In addition, all areas will receive a fair share of transformation funding from 2021/22 to 2023/24 to deliver these services in new models of care integrated with primary care networks
2.33 In addition to CCG baseline funding all local areas will receive an additional fair share funding allocation to support the delivery of these nationwide mental health priorities:
• 345,000 additional children and young people (CYP) aged 0-25 will be able to access support via NHS-funded mental health services (in addition to the Five Year Forward View for Mental Health’s commitment to have 70,000 additional CYP accessing NHS Services by 2020/21);
• Expansion of access to specialist community perinatal mental health services in 2019/20;
• By 2020/21 there will be 100% coverage of 24/7 adult crisis resolution and home treatment teams operating in line with best practice;
• The continued expansion of CYP mental crisis services so that by 2023/24 there is 100% coverage of 24/7 crisis provision for CYP which combines crisis assessment, brief response and intensive home treatment functions;
• The development of local mental health crisis pathways including a range of alternative services so that by 2023/24 there is 100% roll out across the country.
2.34 Further funding allocations will be made to individual systems in consultation with NHS England/Improvement regions as follows:
• Salary support for IAPT trainees (approximately 60% of salary) will be available from 2019/20 to all areas in accordance with the number of trainees recruited;
• Development of school or college-based Mental Health Support Teams (MHSTs) in all regions (in line with the previous Green Paper commitments), which will contribute to the additional 345,000 CYP access figure.
Detail of the funding available for each of these initiatives and allocations to individual systems will be decided through the five-year planning process.
2.35 Targeted funding will also be available to specific sites for a range of smaller initiatives and pilots, including:
• Funding for the development and testing of maternity outreach clinics in 2020/21 and 2021/22 ahead of national roll-out;
• Funding to pilot new models of integrated primary and community care for adults and older adults with severe mental illnesses in 2019/20 and 2020/21.
• Continuation of funding for mental health liaison services to achieve 70% coverage of ‘core 24’ services by 2023/24;
• Continuation of the Individual Placement Support wave funding in 2019/20 and 2020/21;

NHS Long Term Plan Implementation Framework I 13
• Testing of clinical review of standards in 2019/20; • Developing a hub and spoke model for problem gambling from 2019/20, with
central clinics which have satellite clinics in neighbouring populations; • Completing the piloting of Specialist Community Forensic Care and women’s
secure blended services by 2020/21; • Implementation of enhanced suicide prevention initiatives and bereavement
support services; • Developing new mental health services to support rough sleepers, to meet the
ambition of the Government’s rough sleeping strategy for the NHS to invest up to £30 million over the next five years in this area.
2.36 Systems will be able to access support from national and regional teams, details of which can be found here.
Better care for major health conditions: Shorter waits for planned care
2.37 Systems need to set out how they will expand the volume of planned surgery year-on-year, cut long waits, and reduce the size of waiting lists over the next five years. Systems should confirm they are continuing to provide patients with a wide choice of options for quick elective care, including expanding provision of digital and online services.
2.38 Systems will ensure that no patient will have to wait more than 52-weeks from referral to treatment (RTT). They will also need to implement a planned NHS-managed choice process across the country for all patients who reach a 26-week wait, starting in areas with the longest waits and rolling out best practice through a combination of locally established targeted initiatives and nationally-driven pilots.
2.39 By 2023/24, systems should have scaled their provision of First Contact Practitioners (FCP) so that all patients across England have access. This will provide faster access to diagnosis and treatment for people with MSK conditions and support more patients to effectively self-manage their conditions. Mature systems will be expected to achieve a faster pace of mobilisation. An updated FCP specification has been developed and was published in May 2019. Systems should also set out how they will expand access to other MSK support services, including via digital and online routes.
2.40 The data, tools and practical support offered by the national improvement and clinical improvement programmes, including GIRFT and NHS RightCare, will support systems in identifying and addressing unwarranted variation and support the delivery of shorter waits for planned care.

14 I NHS Long Term Plan Implementation Framework
Increasing the focus on population health – moving to Integrated Care Systems everywhere
3.1 Delivering service transformation of this scale requires a well-developed system and effective underpinning infrastructures. Plans must therefore set out how STPs will develop to become an ICS by April 2021. We published an ICS maturity matrix to guide systems on the characteristics we expect of Integrated Care Systems. We anticipate systems to show how they will reach the ‘mature’ level by April 2021.
3.2 The characteristics of a mature ICS include:
• Collaborative and inclusive multi-professional system leadership, partnerships and change capability, with a shared vision and objectives including an independent chair;
• An integrated local system, with population health management capabilities which support the design of new integrated care models for different patient groups, with strong PCNs and integrated teams and clear plans to deliver the service changes set out in the Long Term Plan; improving patient experience, outcomes and addressing health inequalities;
• Developed system architecture, with clear arrangements for working effectively with all partners and involving communities as well as strong system financial management and planning (including a way forward for streamlining commissioning, and clear plans to meet the agreed system control total moving towards system financial balance);
• A track record in delivering nationally agreed outcomes and addressing unwarranted clinical variation and health inequalities;
• A coherent and defined population, where possible contiguous with local authority boundaries. Most systems are working within their existing footprint. However, if there are any systems who wish to propose an adjustment to their current geography, then the STP or Local Authority should formally notify NHS England and NHS Improvement via their Regional Director by 31 July 2019 of their requested change.
3.3 Further information about ICSs, including examples from existing ICSs, is available to systems.
3.4 We expect systems to set out how they see the provider and commissioner landscape developing, for example to overcome challenges faced by providers in rural or remote locations. Proposals may include developing group structures or new approaches to collective decision-making. Guidance for aspirant provider groups will be published later in 2019, followed by the new ‘fast-track’ approach to assessing transactions for groups. We intend to publish the Integrated Care Provider Contract during summer 2019. This will offer an opportunity for greater integration of care through contractual integration of primary medical services with other services.
3.5 We have developed guidance that further details the growing freedoms and flexibilities that will be available to ICS as they increasingly mature and demonstrate strong system performance. We expect this to evolve over time as systems and regional team work together. Further details on the support available to systems can be found here.

NHS Long Term Plan Implementation Framework I 15
More NHS action on prevention
4.1 In previous chapters we have set out foundational elements of the Long Term Plan where additional detail, trajectories, and expectations of progress in the early years of Long Term Plan implementation are expected. The wider service transformations described in chapters 4 and 5 are also key elements of Long Term Plan delivery. However, they include areas where systems will want to phase activity to reflect local priorities, varying starting points or where national enabling actions are required before they can be implemented at scale across the NHS. Regions will agree trajectories for delivery of these commitments that take account of this flexibility.
4.2 In developing their plans, systems will need to work in close partnerships with regional and local Directors of Public Health to set out how they and their local authority partners who have commissioning responsibility for many of these preventative services will develop and deliver prevention activities that respond to local health needs and deliver on the commitments in the Long Term Plan, including obesity, smoking, alcohol, sexual health, antimicrobial resistance and air pollution. At a national level, we will develop indicators and datasets to monitor the impact of these prevention activities on health inequalities.
4.3 Further details of the prevention programme support can be found here. To support the delivery of prevention activities additional funding will be made available:
• Smoking: o Targeted investment to develop NHS-funded smoking cessation services
in selected sites in 2020/21; o Additional indicative allocations for all STPs and ICSs, from 2021/22, for
the phased implementation of NHS smoking cessation services for all inpatients who smoke, pregnant women and users of high-risk outpatient services (as a complement not a substitute for local authority’s own responsibility to fund smoking cessation).
• Obesity: o The Diabetes Prevention Programme (DPP) is a nationally-funded and
commissioned programme. Systems should set out local referral trajectories that will contribute to the national DPP uptake;
o Targeted funding for 2020/21 and 2021/22 for a small number of sites to test and refine an enhanced weight management support offer for those with a BMI of 30+ with Type 2 diabetes or hypertension and enhanced Tier 3 services for people with more severe obesity and comorbidities.
• Alcohol: o Targeted funding available from 2020/21 to support the development and
improvement of optimal Alcohol Care Teams in hospitals with the highest rates of alcohol dependence-related admissions.
• Air pollution: o Targeted support from the NHS Sustainable Development Unit to spread
best practice in sustainable development, including improving air quality, plastics and carbon reduction.
• Antimicrobial resistance: o Targeted support available to regions to drive progress in implementing
the Government’s five-year national action plan, Tackling Antimicrobial Resistance, to reduce overall antibiotic use and drug-resistant infections.

16 I NHS Long Term Plan Implementation Framework
Delivering further progress on care quality and outcomes
5.1 Chapter 5 sets out wider service transformations that are key elements of Long Term Plan delivery where systems will want to phase activity to reflect local priority, varying starting points or where national enabling actions are required before they can be implemented at scale across the NHS. Regions will agree trajectories for delivery of these commitments that take account of this flexibility.
A strong start in life for children and young people
5.2 Local Maternity Systems should set out how they will ensure that babies born anywhere in England has the best possible start in life, consistent with the Long Term Plan commitments and the conclusions of Better Births. The national Maternity Transformation Programme and Children and Young People’s Transformation Programme will work together in supporting systems. LMS plans should be integrated into broader local system plans. Further support is set out here.
Maternity and neonatal services
5.3 There will be fair shares funding for LMSs to 2020/21 to support the implementation of Better Births. Additional funding will be provided to all systems to support the delivery of the following Long Term Plan commitments:
• Continuity of Carer: Targeted funding will go to LMSs in 2021/22 to 2023/24 to support the most deprived areas, to address health inequalities.
• Saving Babies’ Lives Care Bundle (v2): Funding will be available on a fair shares basis from 2021/22 to optimise implementation, particularly the new element on reducing pre-term births.
• UNICEF Baby Friendly Initiative: Targeted funding will be available from 2019/20 to 2023/24.
• Neonatal Critical Care services: Targeted funding will be available from 2021/22 to support the expansion and improvement of neonatal critical care services and to develop allied health professional (AHP) support. A finalised neonatal critical care services tariff will be in place by March 2022.
• Integrated support for families during neonatal care: Targeted funding will be available from 2020/21 to ensure that there are care coordinators within each of the clinical neonatal networks across England to support families to become more involved in the care of their baby.
• Postnatal physiotherapy and multidisciplinary pelvic health clinics: Targeted funding will be available to support the roll out of these clinics in some sites from 2020/21 to 2022/23, followed by fair shares funding for all systems in 2023/24.
5.4 Local Maternity Systems will also continue to receive financial support for the release of senior clinicians for local leadership and LMS implementation capacity up to 2023/24.
Services for children and young people
5.5 In April 2019 we established the national Children and Young People’s Transformation Programme to support the delivery of service improvements set out in the Long Term Plan. Local plans to improve outcomes for children and young people should:

NHS Long Term Plan Implementation Framework I 17
• Establish local leadership – including named clinical and management leaders, co-production with children, young people, families and carers and bringing together local leaders from across the NHS, local government, education and other partners to design and deliver transformation for the system;
• Show how they will improve performance of childhood screening and immunisation programmes and meet the base level standard in the NHS public health functions agreements;
• Develop plans that will deliver Long Term Plan commitments, with a specific focus on: o Developing age-appropriate integrated care, integrating physical and
mental health services, enabling joint working between primary, community and acute services, and supporting transition to adult services;
o Improving care for children with long-term conditions, such as asthma, epilepsy, diabetes, and complex needs;
o Treating and managing childhood obesity; o Supporting the expansion of Children and Young People’s mental health
services; o Improving outcomes for children and young people with cancer.
5.6 Additional funding will be available to systems as follows:
• From 2021/22 to 2022/23, there will be targeted investment to support the integration and improvement of Children and Young People’s services, with additional indicative funding distributed to all systems in 2023/24 to support these integrated services;
• Targeted funding will be available from 2021/22 to increase the capacity to treat obese children and the severe health complications related to their obesity (ie increasing access to Tier 3 services).
5.7 The Children and Young People’s Transformation Programme support to systems can be found here.
Learning disabilities and autism
5.8 System plans should set out how they will deliver the Long Term Plan commitments to improve services and outcomes for people with learning disabilities, autism or both, reducing the reliance on inpatient provision and increasing community capacity. To do this effectively, systems must ensure that they understand their local unmet need, gaps in care, including local health inequalities. It is expected that all STPs and ICSs will have a named senior responsible officer to oversee local implementation of Long Term Plan ambitions for individuals with learning disabilities, autism or both, and their families.
5.9 Systems should involve people with lived experience and their families in checking the quality of care, support and treatment, and set out how they will ensure all local services make reasonable adjustments for people with learning disabilities, autism or both when they need it.
5.10 System plans should clearly set out:
• their share of the required further reduction inpatient usage and beds; • learning disability and autism physical health checks for at least 75% of people
aged over 14 years;

18 I NHS Long Term Plan Implementation Framework
• how proposals for people with learning disabilities and/or autism align with their plans for mental health, special educational needs and disability (SEND), children and young people’s services and health and justice;
• the local offer for autistic young people, people with a learning disability and their families;
• how NHS-led provider collaboratives will be developed locally and should ensure that digital plans use the reasonable adjustment ‘digital flag’ in the patient record or, where this is not available, use the Summary Care Record as an alternative.
5.11 System investment should identify what community provision is in place for intensive, crisis and forensic community support. This includes seven-day specialist multidisciplinary services and crisis care and community teams for children and young people that can be built upon or strengthened with clear alignment with mental health and social care.
5.12 Funding to deliver the improvements set out in the Long Term Plan will be provided through CCG allocations and additional service development funding, distributed to all systems, which includes agreed transfers to cover specialised services, community service investment and for Transforming Care Partnerships.
5.13 Targeted funding will be available to:
• Support pilot work for community services for both adults and children and young people from 2020/21. Indicative additional funding allocations have been made to support the roll out of these services in 2023/24;
• Develop keyworkers for children and young people with the most complex needs and their carers/families from 2020/21. Initial funding will focus on supporting children and young people who are in mental health inpatient units. Indicative additional funding allocations have then been made to support roll out of these services in 2023/24;
• Further ‘catch up’ in the number of Learning Disabilities Mortality Reviews (LeDeR) in 2019/20. Systems plans should ensure that LeDeR reviews are undertaken within six months of the notification of death, and that completed LeDeR reviews are analysed and address the themes and recommendations published through local LeDeR reports and the national Action from Learning report, to reduce health inequalities taking account of forthcoming guidance;
• Roll out, as part of new PCN arrangements the Stopping Over Medication of People with a learning disability or autism and Supporting Treatment and Appropriate Medication in Paediatrics (STOMP-STAMP) programmes – available from 2020/21;
• Test the model for taking eye, hearing and dental services to children and young people in residential schools from 2021/22;
• Provide capital investment for 2019/20 and 2020/21 to support the development of new housing options and suitable accommodation in the community.
5.14 The national Learning Disability and Autism team will provide support to systems in developing and delivering their plans, details of that support can be found here. When drawing up plans, systems can draw on the Ask Listen Do Framework to learn from, and improve the experiences of people with a learning disability, autism or both.
NHS Long Term Plan Implementation Framework I 19
Better care for major health conditions
Cardiovascular disease
5.15 System plans should set out how they will, over the next five years, improve the prevention early detection and treatment of cardiovascular disease (CVD). Funding to deliver improved treatment for CVD is included in indicative additional allocations, with additional ‘fair share’ funding for systems from 2020/21 to increase the number of people with CVD who are treated for the cardiac high-risk conditions; Atrial Fibrillation, high blood pressure and high cholesterol. Additional targeted funding will be made available for:
• Increasing the numbers of people at risk of heart attack and stroke who are treated for the cardiovascular high risk conditions; Atrial Fibrillation, high blood pressure and high cholesterol. This will be supported by the roll-out in 2020 of the CVDPREVENT audit. From 2020/21 funding will be included in fair shares allocations to systems.
• Testing the use of technology to increase referral and uptake of cardiac rehabilitation from 2021/22. In 2023/24, funding for wider roll out will be included in fair shares allocations to systems;
• Pilot schemes in 2020/21 and 2021/22 to increase access to echocardiography and improve the investigation of those with breathlessness and the early detection of heart failure and valve disease. From 2022/23 funding for wider roll out will be included in fair shares allocations to systems.
5.16 The national CVD and respiratory programme will provide additional support to help systems deliver improved outcomes for CVD as set out here.
Stroke care
5.17 Systems are asked to ensure they have robust plans, and effective local clinical and system leadership to develop and improve stroke services, centred around delivering Integrated Stroke Delivery Networks (ISDNs), improving and configuring stroke services, to ensure that all patients who need it, receive mechanical thrombectomy and thrombolysis. Early Supported Discharge (ESD) should be routinely commissioned and available to all patients for whom it is appropriate, with systems developing plans to integrate ESD and community services.
5.18 Additional funding to support implementation of stroke commitments will be available as follows:
• Targeted funding to support roll out of ISDNs will be available from 2021/22; • Targeted funding for developing and testing improved post-hospital
rehabilitation models available 2020/21 and 2021/22. Fair shares funding will be available for wider roll out from 2022/23;
5.19 Plans should identify proposed capital investment to reconfigure stroke services via the STP capital bids process. To support this, all ISDNs should be established across between one and four ICSs or STPs, and have an accountable ISDN governance structure in place by April 2020. This should include all relevant providers from pre-hospital care through to post-acute rehabilitation. Regions will assure cross-boundary coordination of ISDN footprints and provide improvement support.
5.20 National support to help systems deliver these improvements can be found here.

20 I NHS Long Term Plan Implementation Framework
Diabetes
5.21 Systems are asked to set out their approach for delivering improved services in line with the Long Term Plan commitments for people with Type 1 and 2 diabetes, including:
• Support for more people living with diabetes to achieve the three recommended treatment targets;
• Targeting variation in the achievement of diabetes management, treatment and care processes;
• Addressing health inequalities through the commissioning and provision of services;
• Expanded provision of access to digital and face-to-face structured education and self-management support tools for people with Type 1 and Type 2 diabetes;
• Providing access for those living with Type 2 diabetes to the national HeLP Diabetes online self-management platform, which will commence phased roll out in 2019/20;
• Ensuring universal coverage of multidisciplinary footcare teams (MDFTs) and diabetes inpatient specialist nurses (DISN) teams, for those who require support in secondary care.
5.22 To support systems to deliver these improvements additional funding is available as follows:
• Central reimbursement arrangements are in place for 2019/20 and 2020/21 to enable up to 20% of people living with Type 1 diabetes who are eligible under the clinical criteria for that funding, to access flash glucose monitoring devices;
• There will be targeted funding for MDFTs and DISNs transformation projects. In the first instance, continued funding will be provided in 2019/20 for currently established MDFTs and DISN transformation projects, supporting them to become sustainable from 2020/21 onwards. Thereafter, targeted funding will be available for systems that have not had access to MDFTs and DISNs by this point, to help improve equality of access and ensure universal coverage;
• Targeted funding from 2019/20 to 2023/24 to support delivery of the three recommended treatment targets and to continue funding for existing structured education projects. This funding is tapered to reduce across the period as improvements are embedded;
• Targeted funding to test low calorie diets for obese people with Type 2 diabetes, working with demonstrator sites covering up to 5,000 people from 2019/20;
• Ensuring that pregnant women with Type 1 diabetes are offered continuous glucose monitoring from April 2020, where clinically appropriate. Funding arrangements will be confirmed later in 2019/20.
5.23 Details of the support available to systems can be found here.
Respiratory disease
5.24 System plans should set out how they will support local identification of respiratory disease and increase associated referrals to pulmonary rehabilitation services for those who will benefit, particularly for the most socio-economically disadvantaged people who are disproportionately represented in this patient cohort.

NHS Long Term Plan Implementation Framework I 21
5.25 Funding to deliver improvements in respiratory care in line with Long Term Plan commitments is available as follows:
• Targeted funding for a number of sites in 2020/21 and 2021/22 to expand pulmonary rehabilitation services and test new models of care for breathlessness management in patients with either cardiac or respiratory disease. From 2022/23 fair shares funding will be available to all systems to support wider roll out;
• Targeted funding available to increase spirometry training via new Primary Care Training Hubs from 2020/21.
5.26 National support for improving outcomes for people with respiratory disease can be found here.
Research and innovation to drive future outcomes improvement
5.27 The Long Term Plan recognised the importance of research and innovation as drivers of improved outcomes and efficiency in the NHS. Over the coming five years, we will work with systems to increase participation in research and accelerate the development and uptake of innovation that addresses the needs of the NHS, based on input from patients and staff. We will further support this by working with innovators to test promising innovations that meet systems’ local needs. System plans should set out how they will:
• Contribute to the national ambitions to increase public and patient participation in research;
• Work with innovators to test innovations that meet the NHS’s needs in real-world settings;
• Ensure local adoption and spread of proven innovations, working with Academic Health Science Networks (AHSNs) where appropriate.
5.28 Locally, AHSNs and National Institute for Health Research (NIHR) Applied Research Collaboratives will work with systems to ensure that their research and innovation needs are communicated effectively to academic partners and innovators.
5.29 National support for innovation will be enhanced and better coordinated. Key partners across government, the NHS, Arms’ Length Bodies, industry, charities and patient groups have been brought together to form the Accelerated Access Collaborative (AAC), tasked with streamlining the process of bringing innovations into the NHS. The role of the AAC was substantially expanded in May 2019, with the AAC now responsible for delivering a number of key priorities across the NHS and government, further details can be found here.
5.30 Following the production of system plans, we will select a small number of exemplar systems at the end of 2019/20 with which to undertake more detailed co-design of how the research and innovation commitments in the LTP can be delivered locally. The outputs of this work will be published during 2020/21 to support more detailed implementation plans in all systems.
5.31 National support to increase participation in research can be found here.

22 I NHS Long Term Plan Implementation Framework
Genomics
5.32 Delivery of the Long Term Plan ambitions for genomics will be supported by the new national genomic medicine service, which will consolidate existing infrastructure into seven Genomic Laboratory Hubs working with clinical genetics and NHS Genomic medicine centres in alignment with the Cancer Alliances and pathology networks. This will provide patients with consistent and equitable access to testing in line with the new national genomic test directory.
5.33 For local systems, implementation of these commitments will mean working with the relevant Genomic Laboratory Hub and the NHS Genomic Medicine Centres to ensure clinical pathways are in place, operating to national standards and protocols. This should ensure that all eligible patients receive access to appropriate genomic testing and that requests for genomic testing are consistent with the national genomic test directory and delivered by the designated providers.
Volunteering
5.34 Volunteering is already being supported in acute NHS Trusts through the nationally-funded Helpforce programme. A national volunteering programme is being established to provide further support to systems in developing volunteering across the NHS, building on the excellent work already taking place in voluntary and community organisations. Systems should seek to increase the appropriate use of volunteering across local health and care services.
5.35 Funding to facilitate the expansion of volunteering is available as follows:
• Additional funding allocated to STPs and ICSs, on a fair shares basis in 2019/20, to support the identification, integration and growth of volunteering, especially in areas of deprivation;
• Further targeted funding to develop volunteering in selected sites in 2020/21 and 2021/22.
5.36 Details of the support available to systems can be found here.
Wider social impact
5.37 The Long Term Plan set out how the NHS is supporting wider social impact across England including support focused on health and the justice system, veterans and the armed forces, health and the environment, health and employment and anchor institutions. Much of this work will be driven by national programme teams but will require engagement and partnership working with systems to deliver improved outcomes and services for local communities. Further details on the support available to deliver these commitments can be found in Annex D.

NHS Long Term Plan Implementation Framework I 23
Giving NHS staff the backing they need
6.1 As set out in the interim NHS People Plan, we need more staff working in the NHS and NHS-commissioned services over the next five years, both to address existing shortages and to deliver the improvements set out in the Long Term Plan. But more of the same will not be enough on its own. We need a broader range of people in different professions, working in different ways, supported by more effective use of existing technologies and faster application of scientific and technological innovation. We need a widescale set of cultural changes to build the diverse workforce that is required for a world-class 21st century healthcare system. We must take action to capitalise on the role of the NHS as a ‘system anchor’. This includes improving access for marginalised groups to the good quality jobs offered by the NHS, promoting positive cultures, building a pipeline of compassionate and engaging leaders, and making the NHS an agile, inclusive and modern employer, if we are to attract and retain the people we need to deliver our plans.
6.2 Workforce planning needs to be central to our overall planning processes and should cover workforce growth and workforce transformation for all areas of NHS-funded care including primary care, community, mental health and acute services.
6.3 In line with the themes of the interim NHS People Plan, system plans will need to set out specific action to:
• Make the NHS the best place to work: Delivering the themes set out in the interim NHS People Plan, including setting targets for BME representation across its leadership team and broader workforce by 2021/22, improving mental and physical health and wellbeing and enabling flexible working. This includes responding to the requirements of the new Workforce Disability Equality Standard, introduced in April 2019;
• Improve leadership culture: Establishing the cultural values and behaviours we expect from our senior leaders, implementing system-wide processes for managing and supporting talent, and developing strategies to support all staff to work in compassionate and inclusive leadership cultures;
• Deliver a holistic approach to workforce transformation and workforce growth (‘more people, working differently’), including: o Setting out (after taking account of these efficiency plans) the workforce
growth planned for different groups; o Show the action that will be taken locally to improve retention,
international recruitment and maximise use of the Apprenticeship Levy; o Ensuring that overall efficiency and productivity plans (Chapter 8) include
practical, system-wide action to improve workforce efficiency and release greater time for care, including changes in skill mix, new ways of working, better use of scientific and technological innovation, and reductions in sickness absence.
• Change the workforce operating model: Describing – as part of broader ICS development – plans to develop the capacity (including prioritising urgent action on nursing shortages), capability, governance and ways of working. This will enable ICSs to take on growing responsibility for workforce and people activities, informed by the capacity building diagnostic and tool that we have developed with local systems.
6.4 In partnership with Health Education England, we will work with systems to share existing data, analysis and insights that may support them in designing workforce

24 I NHS Long Term Plan Implementation Framework
models to deliver Long Term Plan service priorities. STPs/ICSs will need to work with trusts, primary care networks and other partners to develop optimal workforce models for their local health system, informed by national work but taking account of local context.

NHS Long Term Plan Implementation Framework I 25
Delivering digitally-enabled care across the NHS
7.1 Systems need to develop a comprehensive digital strategy and investment plan consistent with the Tech Vision that describes how digital technology will underpin their local system’s wider transformation plans over the next five years. This includes, amongst other priorities, their approach to ensuring all secondary care providers are fully digitised by 2024 and that these are integrated with other parts of the health and care system, for example through a local shared health and care record platform. These strategies should describe:
• How and when each organisation will achieve a defined minimum level of digital maturity;
• How they will adopt Global Digital Exemplar (GDE) Blueprints and an approach based on IT system convergence to reduce unnecessary duplication and costs;
• How they will adhere to controls and use approved commercial vehicles such as the Health System Support Framework to ensure technology vendors and platforms comply with national standards for the capture, storage and sharing of data.
7.2 Systems are expected to set out plans for how they will significantly improve the provision of services and information though digital routes aligned to national standards and requirements. The newly created NHSX will ensure that the NHS has clear guidance and support to accelerate progress in this area. Systems can draw on a range of national platforms, such as the NHS App and NHS Login and nationally led support and programmes to develop and deliver their plans, such as the Provider Digitisation programme. Local systems should drive forward digitisation focussed on the user need and engage staff and patients in its development.
7.3 The priority for NHSX will be defining and mandating technology standards for all systems and platforms used in the NHS and ensuring all publicly funded source code is open by default. Details of the mechanisms that will be used to support and drive the implementation of these universally across the NHS will be published later this year. Following this, systems will need to ensure any locally developed or procured services meet these standards, ensuring full interoperability with the national infrastructure and other local services.
7.4 The security of data within the NHS is critical. By summer 2021, we expect 100% compliance with mandated cyber security standards across all NHS organisations. Work to deliver on this commitment will be overseen by NHSX and includes:
• Support for the implementation of Microsoft Advanced Threat Protection and the migration to Windows 10 by June 2021, with 85% of NHS estate migrated by Q1 2020;
• Access to the Cyber Security Support Model programme to support organisations progress towards achieving Cyber Essential Plus, including specialist support for improving cyber resilience;
• Access to the Cyber Risk and Operations support package, which provides on-the-ground specialist support and services to support organisations to improve their cyber resilience;
• Enhancements to the national Cyber Security Operations Centre (CSOC) to uplift its capability to detect and remediate cyber threats across the NHS.
7.5 Digital transformation will require all NHS staff to make adjustments in how they work – from the receptionist who supports outpatient clinics to those on their Board. The interim NHS People Plan addresses the need for an increase in the technical skills of the NHS workforce for both specialist and non-specialist staff. The NHS Digital

26 I NHS Long Term Plan Implementation Framework
Academy will support an increase in capability among senior technology and digital leadership enabling further cohorts of NHS staff to become digital change leaders. By 2021/22, all NHS organisations will have a CCIO or CIO on the Board.
7.6 On top of significantly higher local investment in technology, central funding (revenue and capital) will support the delivery of these strategies. Access to this will be managed and coordinated by our regional teams who will support ICS/STPs in establishing an affordable and realistic pipeline of digital investment in each region within the funding envelope available.
7.7 Regional CCIOs and their Regional Directors of Digital Transformation will work with the national provider digitisation team to ensure investment is directed towards strategic programmes that deliver the expected level of digitisation among providers, in a way that minimises unnecessary variation in systems and meets the principles defined in the Tech Vision relating to open standards and user needs. They will also ensure that these programmes make a direct contribution to the delivery of wider system transformation objectives and specific priorities such as improved cancer care and mental health services
7.8 We will support NHS organisations to digitise to core standards supported by a robust IT infrastructure by 2024 through:
• Local capability: NHSX will drive a standards-based approach to provider digitisation to deliver a core level of digitisation across the system and local sharing of records to support integrated care by 2024
• Core services: Nationally-provided services such as the electronic prescriptions and electronic referrals will continue;
• Access to mobile digital services: By 2021/22 all staff working in the community will have access to mobile digital services to help them perform their role, with ambulance services having access to digital services that reduce avoidable conveyance;
• Integrated child protection system: By 2022 a new system will replace dozens of legacy systems;
• Fax machines: NHSX will monitor progress against the Secretary of state's commitment to cease the use of fax machines for communication between NHS organisations and with patients.
7.9 Several nationally-delivered services are available to develop core digital services:
• The transformed NHS.uk website continues to provide high quality information about conditions and treatments, keeping well and NHS services and acts as a platform for other tools, providing Application Programming Interfaces (APIs) that enable partners to provide consistent and coherent information to users of NHS services. The NHS Login provides a single way for patients to identify themselves to a range of services;
• The NHS App, acts as a platform, providing APIs so that third parties can provide their own digital tools and services, and ensures that tools and services can be integrated into it. It also provides a digital front door to primary care, symptom checking, the ability to register as an organ donor and to 111. Two-thirds of GP practices are already connected to the NHS App with 96% expected to be connected by July 2019. The NHS App Roadmap is available here;
• To support the faster uptake of proven digital tools and services, NHSX will be updating the Digital Assessment Questions and the associated assurance process to help local systems to identify digital tools for use within the NHS.

NHS Long Term Plan Implementation Framework I 27
Version 2 will be published in 2019. Further work to improve NHS procurement of technology will be delivered by NHSX.
7.10 National work is supporting the development of locally-delivered digital personal healthcare records so that patients, or their authorised carer, can access and provide contributions to their care record. This includes:
• Patient access: By 2020, every patient with a long-term condition will have access to their care plan via the NHS App, enabled by the Summary Care Record (SCR). By 2023 the SCR functionality will be moved to the local shared health and care record systems and be able to send reminders and alerts directly to the patient;
• Personal Health Records (PHRs): These will be delivered through local health and care records that will also hold care plans, which incorporate information added by the patient themselves, or their authorised carer, and additional information (such as from monitoring devices) which the patient chooses to provide. The PHR adoption service provides advice and guidance for systems developing PHRs and other public-facing health tools;
• Digital maternity records: 55,000 women across 11 areas are already accessing their records digitally. This will be increased to 100,000 across 22 areas by the end of 2019/20. We will continue to build on this work to meet the ambition that all women have their own digital maternity record by 2023/24;
• Digital Redbook for children’s immunisation records and growth: By 2021 all parents will have a choice of a paper or digital Redbook for their new babies. To support this, a core specification will be developed nationally, which suppliers will be expected to work within.

28 I NHS Long Term Plan Implementation Framework
Using taxpayers’ investment to maximum effect
Financial and planning assumptions for systems
8.1 Central to the system planning process is the question of how resources allocated to local health systems to meet population need will be deployed over a five-year period to deliver the commitments set out in the Long Term Plan, including delivery of the five financial tests.
8.2 Five-year CCG allocations covering the period to 2023/24 were published in January, along with the updated 2019/20 planning guidance. This is the starting point for system planning and will be complemented with:
• An additional funding allocation distributed to all systems on an indicative, fair shares basis (national totals are set out in Annex A and system allocations set out alongside this document);
• An indication of targeted funding which will be deployed subsequently against specific Long Term Plan commitments through regions and national programmes (see Annex A);
• Indicative provider-level figures for specialised commissioning funding, over a five-year period, which will be shared with local systems for planning purposes by regional teams in July;
• A set of indicative planning assumptions for pay, non-pay and drugs costs and the indicative tariff uplift;
• Over the coming months we will work with the NHS and set out further detail on the Financial Framework for 2020/21 and beyond. Until this point systems should plan on the basis of the existing framework.
8.3 System plans will need to set out how this resource will be deployed to deliver the commitments within their plans and the government’s financial tests set out in the Long Term Plan:
• To meet financial Test 1 in the Long Term Plan plans must demonstrate how organisations will return to, or maintain, financial balance including the impact on the financial performance of each provider and commissioner organisation. As part of this systems will need to work with providers so that, as a minimum, all providers deliver cash-releasing productivity growth of at least 1.1% a year in line with financial Test 2; and providers in deficit deliver an additional cash-releasing productivity benefit of at least 0.5% a year;
• Regional teams will work with each system to agree what a realistic and stretching bottom line position is (and corresponding allocations from the Financial Recovery Fund) in each year. Financial recovery plans, consistent with the local system plan, will be required for each provider organisation and CCG not in financial balance;
• Plans to incorporate system actions to maximise efficiencies and support appropriate reductions in the growth in demand for care, as required by financial Test 3. National programmes and resource available to support this are set out below.
8.4 Spending plans will need to be consistent with the commitments in the Long Term Plan to increase investment in mental health, and in primary medical and community health services, as a share of total local NHS revenue spend across the five years from 2019/20 to 2023/24. Further detail on what these commitments mean for local systems (including relevant baselines) will provided through regional teams.

NHS Long Term Plan Implementation Framework I 29
8.5 For planning purposes, employers should assume that there is no impact on employer pension contributions as a result of the recent revaluation of the NHS pension scheme, that Marginal Rate Emergency Tariff (MRET) funding is available on a flat cash basis with the same distribution as in 2019/20, and that price relativities in the national tariff remain unchanged.
Improving productivity
8.6 The second financial test in the Long Term Plan requires the NHS to achieve cash releasing productivity growth of at least 1.1% a year, with all savings reinvested in frontline care. Systems are responsible for agreeing and delivering actions to deliver financial recovery and improve productivity. As part of this, national support is available to help systems plan and deliver improvements in productivity in each of the ten priority areas from the Long Term Plan where there are proven efficiency opportunities. The asks of the NHS includes:
i. Improving clinical productivity and releasing more time for patient care forms an integral part of the interim NHS People Plan and the NHS Long Term Plan. To support all systems to be using electronic tools (including e-rostering and e-job planning) by 2021 and evidence-based approaches to staffing by 2023, support available from the national team can be found here.
ii. Maximising the buying power of the NHS, including through the use of the Purchase Price Index and Benchmarking Tool (PPIB), GIRFT clinically led procurement work and Support Supply Chain Coordination Limited (SCLL). Support to deliver this can be found here.
iii. Supporting the development of pathology networks across England by 2021 and of diagnostic imaging networks across England by 2023. Support to deliver this can be found here.
iv. Supporting pharmacy staff to take on increased patient facing clinical roles and, through the Medicines Value Programme, help the NHS deliver better value from the £16 billion annual spend on medicines The Pharmacy and Medicines Optimisation Team will continue to work with systems to support this and further details can be found here.
v. System plans set out how they will collectively deliver an additional £700m savings in administration costs by 2023/24 (£290 million, commissioners; over £400 million, providers). Systems should plan on the basis that total running costs across CCGs and system-level bodies are reduced or held flat in cash terms from 2020/21 onwards. National support for this can be found here.
vi. Financial Test 5 in the Long Term Plan requires the NHS to make better use of capital investment and its existing assets to drive transformation. Capital budgets will only be confirmed at the upcoming Spending Review. Planning assumptions for the current provider self-financed capital spend and nationally-funded capital schemes will be provided by regions in July 2019. We will provide an initial baseline for each area in July and ask systems to identify their priorities within that and prioritise investments above that should the funding be available. National support for estates and facilities can be found here.
vii. The national Evidence-Based Interventions Programme (EBI) published statutory commissioning guidance for 17 interventions in November 2018 to reduce harm and free up resource. As they implement the guidance to free up

30 I NHS Long Term Plan Implementation Framework
capacity through the reduction of 128,000 interventions, systems can draw on national support that can be found here.
viii. The national Patient Safety Strategy will be published in summer 2019, setting out how we will continue to improve patient safety, preventing harm and the substantial costs associated with it. Systems will be expected to set out how they will contribute to the improvements described within the upcoming national strategy, to the agreed timetable within their local plan. Support from the national team can be found here.
Reducing variation across the health system
8.7 Financial Test 4 in the Long Term Plan requires the NHS to reduce variation across the health system, improving providers’ operational and financial performance. A number of different national programmes are focused on supporting the NHS reduce variation in quality, access and outcomes. Systems should draw on these resources as they develop local plans that will tackle variation in service provision and address health inequalities within their local population. Further details be found here.

NHS Long Term Plan Implementation Framework I 31
Next steps
9.1 Publication of this Implementation Framework begins the process of strategic system planning. System plans for delivery through to 2023/24 are required, with an initial submission in September 2019 and a final submission to follow by mid November 2019. Plans should fully align across the organisations within each system so that they can subsequently be translated into organisational plans for 2020/21, which will be required in early 2020. The collection process, support offer, and timescales are set out here.
Milestone Date
Interim People Plan published 3 June 2019
Publication of the Long Term Plan Implementation Framework June 2019
Main technical and supporting guidance issued July 2019
Initial system planning submission End of September 2019
System plans agreed with system leads and regional teams Mid November 2019
Further operational and technical guidance issued December 2019
Publication of the national implementation programme for the Long Term Plan December 2019
First submission of draft operational plans Early February 2020
Final submission of operational plans By end March 2020
9.2 Systems are asked to provide two elements at both the September and November milestones:
• Strategy delivery plan: A document that sets out what the system plans to deliver over the next five years. Whilst there is no template for this document, systems are encouraged to ensure that their plan covers all the elements set out in Chapter 1 of this Implementation Framework, including: a description of local need; what service changes will be taken forward and how; how the local system infrastructure will be developed – including workforce, digital and estates; how efficiency will be driven through all local activity, how local engagement has been undertaken to develop the plan and how financial balance will be delivered;
• Supporting technical material: Successful delivery will require systems plans to be underpinned by realistic plans for workforce and activity, which must be delivered within the local financial allocation. Templates and tools will be provided to support systems in this. Draft templates to support with modelling of finance, activity and key commitment metrics are provided in alongside this document. A full version of the finance and activity template will be provided in early July 2019.
9.3 In 2019/20, systems should continue with ongoing service improvement work to maintain and improve performance for cancer treatment and A&E until any new

32 I NHS Long Term Plan Implementation Framework
standards, proposed by the Clinical Review and accepted by Government, are implemented. Systems should also work to reduce elective waiting lists and eliminate 52+ week waits, setting the foundations for future improvements.
9.4 A list of published resources and supporting materials for planning can be found here. In addition, over the summer, there will be a programme of national and regional opportunities for systems to understand the support and resources that will be available to them over the planning period, and over the next five years.
9.5 In line with the new operating model, systems should work with their regional teams to set out what additional support they need to develop their local plans and should seek to develop these in house. Where additional help is needed, regions will coordinate input from national teams and CSUs. Regions will also encourage and enable facilitated peer review, and provide feedback to systems following their submissions:
• By 27 September 2019: Systems are asked to share a draft of their plans, including detail on clinical priorities and trajectories. Regions, working with central teams, will use this information to build a national picture against our overall outcome goals, feeding back where adjustments are needed.
• By 15 November 2019: System plans should be agreed with system leads and regional teams, in consultation with National Programme Directors. Packages of future support from central teams to support delivery will also be agreed.
9.6 As outlined in Chapter 1 system plans need to be clinically-led and developed with full local engagement of stakeholders. When system leaders are finalising their plans for submission, they will be expected to demonstrate how this has been achieved and how they have secured support from key stakeholders.
9.7 System plans will be aggregated, along with wider national action, to develop a detailed national implementation programme for the Long Term Plan in December 2019. This will also take account of the Spending Review, planned for later this year.

NHS Long Term Plan Implementation Framework I 33
Annex A: Funding the Long Term Plan
A1 Annex A sets out the funding which has been allocated to support the commitments in the Long Term Plan and previous requirements from the Five Year Forward View, in addition to the published five-year CCG allocations. For system planning purposes this funding is best understood in two parts.
Indicative funding allocations available to systems A2 Additional indicative funding will be made available to all systems for commitments in
the Long Term Plan which apply across the country, with funding distributed on a fair shares basis. An indicative allocation for each system will be communicated alongside this document.
A3 The Long Term Plan commitments to be delivered within these funding allocations are set out for information in the Table 1. Systems will need to make local decisions on how to deploy funding to meet the Long Term Plan commitments which may involve a different distribution or phasing of expenditure.1
A4 This indicative funding is intended to support the elements of the Long Term Plan outlined in Table 2.
Table 2. Commitments to be delivered through system funding allocations
Mental Health
The expansion of community mental health services for Children and Young People aged 0-25; funding for new models of integrated primary and community care for people with SMI from 2021/22 onwards; and specific elements of developments of the mental health crisis pathways. See 2.27.
Primary Care
This funding includes the continuation of funding already available non-recurrently to support Extended Access and GP Forward View funding streams, (eg practice resilience programme), and associated commitments must be met. Additional funding is also included to support the development of Primary Care Networks.
Ageing Well Deployment of home-based and bed-based elements of the Urgent Community Response model, Community Teams, and Enhanced Health in Care Homes.
1 Note that additional funding allocated for mental health is required to be spent on mental health services, in line with the commitments made in the Long Term Plan.
Table 1. Additional indicative funding allocations England 2019/20 2020/21 2021/22 2022/23 2023/24 £m £m £m £m £m Total 538 560 814 1,219 1,779 Of which: 1. Mental Health 60 65 220 441 592 2. Primary Medical and Community Services (a) Primary Care 321 335 359 369 364 (b) Ageing Well 0 30 70 204 343 3. Cancer 118 89 71 68 68 4. Other 39 41 94 137 412

34 I NHS Long Term Plan Implementation Framework
Cancer
Rapid Diagnostic Centres funding in 2019/20 only; Cancer Alliance funding to support screening uptake delivery of the Faster Diagnosis Standard and timed pathways, implementation of personalised care interventions, including personalised follow up pathways and Cancer Alliance core teams.
CVD, Stroke and Respiratory
Increased prescribing of statins, warfarin and antihypertensive drugs; Increased rates of cardiac, stroke and pulmonary rehabilitation services; increased thrombolysis rates; and early detection of heart failure and valve disease.
CYP & Maternity
Local Maternity Systems funding; Saving Babies Lives Care Bundle funding from 2021/22; postnatal physio funding from 2023/24; funding for integrated CYP services from 2023/24.
LD Autism Funding for rollout of community services for adults and children and keyworkers from 2023/24.
Prevention Tobacco addiction - inpatient, outpatient/day case and Smoke Free pregnancy smoking cessation interventions.
A5 This funding should be reflected in plans in addition to published five-year CCG funding allocations and any other locally assumed income.
A6 Our regional teams, who will be advised by National Service Transformation Directors, will jointly approve the release of funding based on assurance of plans to ensure that they deliver the commitments made in the Long Term Plan. ICS areas will have a higher degree of autonomy over deployment of this funding.
Targeted funding available to systems A7 In addition to the indicative funding available to all systems (outlined in Tables 1 and
Table 2), budgets have been allocated to fund targeted schemes and for specific investments, where a general distribution is not appropriate. These are outlined in Table 3. The process for accessing this funding and detailed distributions will be provided to systems at a future date, with some elements expected to be notified during the planning process.
A8 This targeted funding is intended to support the elements of the Long Term Plan outlined in Table 4.
Table 3. Targeted funding available to systems England 2019/20 2020/21 2021/22 2022/23 2023/24 £m £m £m £m £m Total 418 939 1,101 1,249 1,481 Of which: 1. Mental Health 182 251 190 234 292 2. Primary Medical and Community Services
(a) Primary Care 100 208 303 381 475 (b) Ageing Well 6 40 40 24 24 3. Cancer 46 121 198 186 398 4. Technology 26 238 199 192 179 5. Other 58 82 172 231 114

NHS Long Term Plan Implementation Framework I 35
Table 4. Commitments to be delivered through targeted funding allocations
Mental Health
Includes: - funding for continuation of previous waves such as mental health liaison
or Individual placement support funding; pilots as part of the clinical review of standards, and other pilots such as rough sleeping.
- funding to be distributed in phases in consultation with regional teams including: funding for testing new models of integrated primary and community care for adults and older adults with severe mental illness, community based integrated care, rolling out mental health teams in schools and salary support for IAPT trainees. See2.28.
Primary Care Digital First Primary Care support funding; the Investment and Impact Fund; and Estates and Technology Transformation Programme.
Ageing Well Targeted funding to accelerator STPs to rollout the Ageing Well models.
Cancer Development and roll out of innovative models of early identification of cancer (starting with lung health checks); funding for the development of Rapid Diagnostic Centres from 2020/21 onwards; support for further innovations to support early diagnosis.
Technology Revenue funding for Provider Digitisation and Local Health and Care Records.
Cardiovascular Disease, Stroke and Respiratory
Pilots for improving access to cardiac, stroke and pulmonary rehabilitation services and early detection of heart failure and valve disease.
Maternity and Neonates
Continuity of carer for BME and disadvantaged women from 2021/22; funding to support the UNICEF Baby Friendly Initiative; funding to support the expansion and improvement of neonatal critical care services from 2021/22; funding from 2020/21 for Family Integrated Care; funding to support the rollout of postnatal physiotherapy and multidisciplinary pelvic health clinics from 2021/22 to 2022/23.
Diabetes Funding to pilot the use of low calorie diets from 2019/20 until 2022/23; funding to support delivery of recommended treatment targets; funding for multi-disciplinary footcare teams and diabetes inpatient specialist nurses (see 4.31).
Learning Disabilities and Autism
Funding to pilot and develop community services for adults and children and keyworkers from 2020/21 to 2022/23; piloting of models to expand Stopping Treatment and Appropriate Medication in Paediatrics (STOMP-STAMP) programmes from 2020/21 to 2023/24; testing the model for ophthalmology, hearing and dental services to children and young people in residential schools from 2021/22; funding to reduce the backlog of the Learning Disabilities Mortality Review Programme (LeDeR).
Personalised Care Targeted transformation funding to deliver the NHS Comprehensive Model for Personalised Care from 2019/20–2021/22.
Prevention Alcohol Care Teams from 2020/21 to 2023/24; Tobacco addiction services early implementer sites from 2020/21; targeted support for weight management service improvements from 2020/21.
36 I NHS Long Term Plan Implementation Framework
Annex B: Financial assumptions for strategic plans
B1 This annex provides a set of national assumptions which systems may wish to
consider when developing their strategic plans. B2 They are not intended to be definitive and plans will need to be resilient to alternative
outcomes. Systems should consider using locally generated assumptions where these are more reflective of the actual impacts at a local level.
Funding allocations B3 CCG programme allocations for the period 2019/20 to 2023/24 are available on the
NHS England/Improvement allocations website (www.england.nhs.uk/allocations). These allocations are indicative for the period 2022/23 to 2023/24.
B4 Primary care allocations for the period 2019/20 to 2023/24 (as revised post the agreement of the new GP contract) are available on the NHS England/ Improvement allocations website. These allocations are indicative for the period 2022/23 to 2023/24.
B5 CCG running cost allowances have been published for 2019/20 and 2020/21 on the NHS England/Improvement allocations website. For strategic planning purposes, CCGs should assume allocations are maintained at a flat cash level in future years. Before 2021/22 these allocations will need to reviewed and may be changed to reflect changes in population.
B6 Specialised commissioning indicative allocations will be issued to regions for the period 2020/21 to 2023/24 in June. Specialised commissioners have been asked to produce indicative funding at provider level in July to inform system plans.
B7 Additional Long Term Plan indicative allocations are being issued alongside this document. These allocations are additional to core CCG and primary care allocations, but may include recurrent funding for commitments which were supported on a non-recurrent basis in 2019/20.
Prices and income Tariff
B8 The table below sets out core assumptions on prices, income and other relevant factors. Further detail is provided in the notes below.
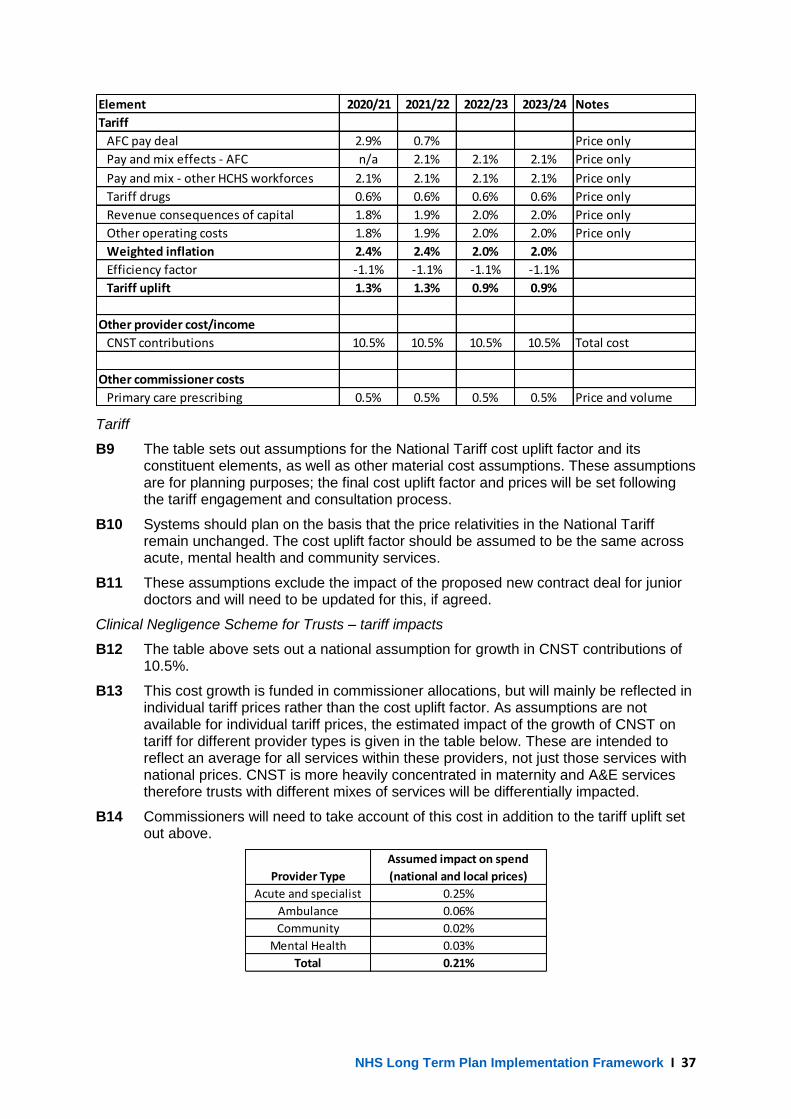
NHS Long Term Plan Implementation Framework I 37
Tariff
B9 The table sets out assumptions for the National Tariff cost uplift factor and its constituent elements, as well as other material cost assumptions. These assumptions are for planning purposes; the final cost uplift factor and prices will be set following the tariff engagement and consultation process.
B10 Systems should plan on the basis that the price relativities in the National Tariff remain unchanged. The cost uplift factor should be assumed to be the same across acute, mental health and community services.
B11 These assumptions exclude the impact of the proposed new contract deal for junior doctors and will need to be updated for this, if agreed.
Clinical Negligence Scheme for Trusts – tariff impacts
B12 The table above sets out a national assumption for growth in CNST contributions of 10.5%.
B13 This cost growth is funded in commissioner allocations, but will mainly be reflected in individual tariff prices rather than the cost uplift factor. As assumptions are not available for individual tariff prices, the estimated impact of the growth of CNST on tariff for different provider types is given in the table below. These are intended to reflect an average for all services within these providers, not just those services with national prices. CNST is more heavily concentrated in maternity and A&E services therefore trusts with different mixes of services will be differentially impacted.
B14 Commissioners will need to take account of this cost in addition to the tariff uplift set out above.
Element 2020/21 2021/22 2022/23 2023/24 Notes
Tariff
AFC pay deal 2.9% 0.7% Price only
Pay and mix effects - AFC n/a 2.1% 2.1% 2.1% Price only
Pay and mix - other HCHS workforces 2.1% 2.1% 2.1% 2.1% Price only
Tariff drugs 0.6% 0.6% 0.6% 0.6% Price only
Revenue consequences of capital 1.8% 1.9% 2.0% 2.0% Price only
Other operating costs 1.8% 1.9% 2.0% 2.0% Price only
Weighted inflation 2.4% 2.4% 2.0% 2.0%
Efficiency factor -1.1% -1.1% -1.1% -1.1%
Tariff uplift 1.3% 1.3% 0.9% 0.9%
Other provider cost/income
CNST contributions 10.5% 10.5% 10.5% 10.5% Total cost
Other commissioner costs
Primary care prescribing 0.5% 0.5% 0.5% 0.5% Price and volume
Provider Type
Assumed impact on spend
(national and local prices)
Acute and specialist 0.25%
Ambulance 0.06%
Community 0.02%
Mental Health 0.03%
Total 0.21%

38 I NHS Long Term Plan Implementation Framework
MRET funding adjustments
B15 For planning purposes, systems should assume that the replacement funding for MRET is available on the same basis and with the same financial distribution as in the agreed 2017/18 values used for 2019/20 payments. As for 2019/20, this will be taken into account in setting financial recovery expectations. The distribution mechanism for this funding in 2020/21 will be notified at a later date.
Provider and commissioner sustainability funding
B16 As set out in the 2019/20 Planning and Contracting Guidance, funding will be available from the Financial Recovery Fund and Commissioner Sustainability Fund where an agreed financial recovery plan is in place, developed as part of the planning process. Regional teams will work with each system to agree what a realistic and stretching bottom line position is (and corresponding allocations from the Financial Recovery Fund) in each year.
Other provider income
B17 Funding for Health Education England, research and development, and the local authority public health grant is subject to decisions in the Spending Review and subsequent DHSC budget setting. We suggest that systems use net tariff as a price assumption for planning purposes.
Pension revaluation costs
B18 For planning purposes, systems should assume that there is no pressure on employer pension contributions as a result of the increase from 14.38% to 20.68% in April 2019. This cost is being funded centrally in 2019/20 and arrangements for future years will be notified in advance of operational planning.
Activity B19 Systems should develop and agree realistic local assumptions which should be
based on local trends derived from recent activity within a system. B20 This should take account of the expectation set out in the Implementation Framework
that systems should:
• set out how they will use the increase in their allocations to improve the volume of elective treatments year-on-year, cut long waits, and reduce the size of waiting lists.
• set out how they will transform outpatients, increasing use of digital tools to redesign how services are offered, and remove up to a third of face-to-face outpatient visits.
B21 In respect of emergency care, STPs/ICSs, commissioners and providers should review assumptions for demand growth to ensure they reflect recent local trends, adjusting as appropriate for demand management and other efficiency schemes that have been agreed within the system, and to reflect delivery of national priorities. In 2019-20, the planning guidance requires systems to continue with ongoing service improvement work to maintain and improve performance for cancer treatment and A&E until any new standards, proposed by the Clinical Review and accepted by Government, are implemented.
Investment commitments Mental health
B22 The Long Term Plan commits that mental health services will grow faster than the overall NHS budget, creating a new ringfenced local investment fund worth at least £2.3 billion a year in real terms by 2023/24, and a new commitment that funding for children and young people’s mental health services will grow faster than both overall NHS funding and total mental health spending. As part of this commitment, systems

NHS Long Term Plan Implementation Framework I 39
should plan on growth in CCG programme spending on mental health in line with the Mental Health Investment Standard (MHIS). In 2020/21 the standard will require an increase in spend by at least the overall CCG programme allocation growth plus an additional percentage increment to reflect the additional mental health funding included in CCG allocations. For 2021/22 and later years, spending should increase by at least the overall CCG programme allocation growth. The strategic planning tool will calculate achievement of the MHIS in each year.
B23 Additional funding from the LTP allocation for mental health will also need to be spent on mental health on top of this growth in core CCG programme spending.
Primary medical and community services
B24 The Long Term Plan commits to an increase of £4.5 billion in real terms expenditure on primary medical and community health services. To support this, systems should plan to:
• Spend the primary care (GP) allocation in full • Increase overall spending from CCG programme allocations on primary medical
care, community services and Continuing Healthcare services above overall CCG allocation growth, together with additional LTP allocations, in order to deliver on the commitment. This includes meeting the new commitment to provide £1.50 per registered patient to PCNs.
B25 Further detail will be provided separately on the required increase by system by 2023/24 and interim requirements in order to contribute to delivering this commitment.
Capital B26 Indicative capital assumptions will be produced at system level to support planning.
Revenue plans and financial improvement trajectories should be consistent with these assumptions. Systems may also wish to produce a well prioritised list of further capital investments beyond this envelope, and exemplify for each the impact these investments would have on the revenue position and on LTP delivery.
B27 For the purposes of system planning, we are asking systems to contain and prioritise capital spending across their ICS/STP and region within an affordable envelope covering all expenditure that scores within capital limits set by the Treasury. We are also asking systems to plan within the envelope for all capital needs across their patch, including both routine and backlog maintenance, depreciation and other self-financed investments, loan-financed schemes and more significant transformational schemes. Systems will need to take account of capital requirements across all care settings, including primary care and mental health, and for digital transformation. Again, both the approach and the quantum are indicative at this stage, and are in particular subject to the outcome of any forthcoming Spending Review; no decisions have been made about the future capital and financing regime, and we are committed to engaging the sector in the development of any future reforms.

40 I NHS Long Term Plan Implementation Framework
Annex C: LTP headline metrics
A new service model for the 21st century 1. Primary and community services (extra £4.5 billion): annual implementation milestones
for 5-year GP contract – more detail to be agreed: new community services response times and teams.
2. Comprehensive ICS coverage including a partnership board, drawn from and representing commissioners, trusts, primary care networks, and – with the clear expectation that they will wish to participate – local authorities, the voluntary and community sector and other partners.
3. Emergency care: on agreed trajectory for Same Day Emergency Care (SDEC) and Integrated Urgent Care Services (IUCS).
More NHS action on prevention and health inequalities 4. Prevention (1): increase uptake of screening and immunisation 5. Inequalities: inequalities reduction trajectory 6. Prevention (2): alcohol care teams, tobacco treatment services, and diabetes prevention
programme Further progress on care quality, access and outcomes 7. Maternal and children’s health: on agreed trajectory for 50% reduction in stillbirth,
neonatal and maternal deaths and brain injury by 2025 8. Improve cancer survival: Improve one and five-year cancer survival; on agreed trajectory
so that 75% of cancer patients diagnosed at stage 1 or 2 by 2028 9. Learning disability and autism: on agreed trajectory for halving inpatient rate by 2023/24
and increasing learning disability physical health checks to 75% of people aged over 14 10. Mental health: on track for locally agreed service expansion, and increase in investment
for mental health services as a share of the NHS budget over the next five years, worth in real terms at least a further £2.3 billion a year by 2023/24
11. Implementation of agreed waiting times/clinical standards for urgent and emergency care, elective care, cancer and mental health, from April 2020, and the maintenance and improvement of performance for cancer treatment and A&E until that point.
NHS staff will get the backing they need 12. Workforce metrics will be agreed through development of the NHS People Plan but will
include: o Staff retention: retention rate to improve by at least 2% o Leadership: CQC well led indicator, and staff engagement indicator o Diversity/inclusion: BME representation, gender, bullying/harassment
Digitally enabled care will go mainstream across the NHS 13. Outpatient reform: 30% reduction trajectory, outpatient digital role out 14. Empowering people: Summary care record roll out. 15. Access to online/telephone consultations in primary care. Taxpayers’ investment will be used to maximum effect 16. Test 1: The NHS will return to financial balance
o proportion of NHS organisations in financial balance. 17. Test 2: The NHS will achieve cash-releasing productivity growth of at least 1.1% per year

NHS Long Term Plan Implementation Framework I 41
o Annual cash releasing productivity growth of at least 1.1% 18. Test 3: The NHS will reduce growth in demand for care through better integration and
prevention o With population health management delivering demand growth moderation in line
with LTP activity model 19. Test 4: The NHS will reduce variation in performance across the health system
o GIRFT/RightCare metric to be confirmed 20. Test 5: The NHS will make better use of capital investment and its existing assets to
drive transformation o Metrics to support this test will be confirmed following the Spending Review and
development of the new NHS capital regime

42 I NHS Long Term Plan Implementation Framework
Annex D: Supporting wider social goals
Health and the justice system
D1 System plans should set out how they will engage with nationally commissioned services to improve outcomes for people engaged in the health and justice systems. Alongside this, the national team will support delivery of the improvements set out in the Long Term Plan as set out below.
D2 By 2020/21: ▪ Roll out of the Health and Justice digital patient record Information System
(HJIS) will begin across all adult prisons, immigration removal centres and secure training centres for children and young people, to enable digital transfer of patient records before custody, in custody and on release;
▪ Targeted roll out of the care after custody service, RECONNECT, will begin by focusing on areas identified through the pilot sites;
▪ Provision of support for survivors of sexual assault will be expanded so they can access integrated therapeutic mental health support, both immediately after an incident and to provide continuity of care where needed. This will include provision of Sexual Assault Referral Centres (SARCs) across England and seamless referral into mental health and other specialist support services.
D3 By 2023/24: ▪ Roll-out of the Community Service Treatment Requirement (CSTR)
programme, will cover a targeted population in England. This will be supported by a national evaluation of the CSTR test sites and will develop an assurance framework to ensure implementation of subsequent sites is iteratively improved;
▪ The CSTR programme will be expanded to cover more women offenders, short-term offenders, offenders with a learning disability and those with mental health and additional requirements;
▪ The development of a trauma-informed framework for integrated care for the most high-risk, high-harm and highly vulnerable children and young people in the community with complex needs. Funding will be made available over the five-year period to set up this offer in partnership with Health and Justice Commissioners.
Veterans and the Armed Forces
D4 The NHS will expand support for all veterans and their families as they transition out of the armed forces, regardless of when people left the service. Local systems are asked to work with the national team to deliver on the Long Term Plan commitments so that by 2023/24: ▪ We have a better understanding of the mental health needs of the veteran
population; ▪ Improved recovery will be defined and achieved in 50% of patients accessing
Transition, Intervention and Liaison Service (TILs) and Complex Treatment Service (CTS);
▪ We have reduced A&E attendances and crisis calls from veterans.
D5 The national team will support this by: ▪ Working in conjunction with Health and Justice Regional Commissioners, who
will ensure that targeted prisons are enabled to support the Veterans Criminal Justice pathway;

NHS Long Term Plan Implementation Framework I 43
▪ Continuing to roll out the Veteran’s Trauma Network and Veteran Aware Hospitals;
▪ Rolling out a Military Veteran Aware Accreditation scheme in conjunction with the RCGP.
Health and the environment
D6 To support the NHS to reduce its carbon footprint in line with the Climate Change Act (34% by 2020, 51% by 2025 compared with the 2007 baseline) we are working with national partners to review opportunities to reduce carbon, waste and water use in line with these targets. In the first instance, they will develop national programmes to drive progress in three key areas: ▪ Shifting to appropriate use of lower carbon inhalers across the NHS; ▪ Reducing the use of high carbon anaesthetics, where it is clinically safe to do
so; ▪ Reducing use of single-use plastic, based on best practice.
D7 Additional information to support systems to respond to the sustainable development targets for carbon reduction, air pollution and reduction in use of single-use plastic will be published later in 2019. Additional support for driving sustainable development across the NHS estate is also set out in Chapter 8.
D8 In summer 2019, the Healthy New Town Principles, Putting Health Into Place, will be published. Any geography with planned housing growth should use these principles as a guide for collaboration between local authorities, NHS services and developers in ensuring that new developments plan, design and build healthier environments. A Healthy New Towns Standard will be developed in 2019/20, as further incentive to build health and wellbeing into developments.
Health and employment
D9 The national health and work team is continuing to work in partnership with the Government’s Health and Work unit to develop and test best practice in supporting people with health conditions and disabilities to get and stay in appropriate work. Systems identifying employment as a local priority can draw on expertise from the national team, via their region, to develop local plans.
Anchor institutions
D10 The national team is continuing to identify, test and spread existing good work where NHS organisations are working as ‘system anchors’ to create wider social value for their local community, specifically relating to procurement or employment. The national team is looking to work with any system delivering, or considering, initiatives with these ambitions so that we can map, test and spread action that will help tackle health inequalities and wider social determinants.

44 I NHS Long Term Plan Implementation Framework
Contact us: NHS England This publication can be made available in a number of other formats on request. Please call 0300 311 22 33 or email [email protected]. NHS Improvement [email protected] improvement.nhs.uk #NHSworkforce NHS Improvement publication code: Corp 04/19 NHS England Publishing Approval Reference: 000801
PURPOSE
The purpose of this Population Health Framework and Plan is to clearly articulate the North
Cumbria Health & Care system’s population health priorities and initiatives for the next three
years. This plan has been developed under guidance from the North Cumbria Population
Health Steering Group, jointly chaired by Colin Cox and Prof. John Howarth.
KEY POINTS TO HIGHLIGHT
• The Framework aligns to the Cumbria Health and Wellbeing Strategy 2019-2029
• It includes suggested action across all tiers of the system; Integrated Care Community,
Network/Pathway and System
• The plan includes the following six key priority areas, each of which is supported by an
OGIM plan:
o Leadership and workforce development
o Protecting the health of the population as a whole
o Tackling the wider determinants of health and wellbeing
o Providing high quality person-centred care
o Improving health and wellbeing throughout the life course
o Population Health Management
NEXT STEPS / AREAS OF WORK TO BE PROGRESSED
• Initiatives that are being taken forward at pace during 19/20 are highlighted in red in the
OGIMs
• Each Integrated Care Community Delivery Group is being asked to use the plan to inform
their own population health developments
• An population health outcomes framework is under development
RECOMMENDATION
Members of the System Leadership Board are asked to approve the North Cumbria
Population Health Framework and Plan 2019-2022.
System Leadership Board PUBLIC
4th July 2019 Enc: 12.1
Title: North Cumbria Population Health Framework and Plan 2019-2022 Author: Colin Cox, Director of Public Health
1
North Cumbria Health & Care Population Health
Framework and Plan 2019 – 2022
1

North Cumbria Health & Care: Population Health
Framework and Plan 2019 – 2022
1. What is population health?
NHS England, NHS Improvement and Public Health England have jointly agreed the following definition of population health: “Population Health is an approach aimed at improving the health of an entire population. It is about improving the physical and mental health outcomes and wellbeing of people, whilst reducing health inequalities within and across a defined population. It includes action to reduce the occurrence of ill-health, including addressing wider determinants of health, and requires working with communities and partner agencies.” 2. What is our Vision?
Our vision aligns to those of the Cumbria Joint Health and Wellbeing Strategy 2019-2029 and North Cumbria Integrated Care System: Cumbria Joint Health and Wellbeing Strategy 2019-2029
Enable Cumbrian communities to be healthy and to tackle health inequalities.
North Cumbria Integrated Care System
To build a new integrated health and care system together, using our collective capabilities for a healthier and happier population. We are our communities; the health and care of our people run with our people for our people.”
3. How are we defining success?
High level measures of success will be monitored through changes to:
• life expectancy • healthy life expectancy • the life expectancy / healthy life expectancy gap between the most and least
deprived communities It is difficult to measure changes to these indicators on a regular basis (and at a very local level), so we have put in place a number of other objectives (linked to factors we know impact on life expectancy and healthy life expectancy). We have also defined the actual actions we need to take to achieve these objectives. 4. How have we structured these objectives and actions?
Using the following framework. Each numbered priority is the theme for an action plan called an OGIM (which stands for Objectives, Goals, Initiatives and Metrics). Action at all three levels of the system have been considered where appropriate
2

(ICS, clinical network and ICC). We also recognise that there is significant inter-connections between each area of the framework and it is important to consider this as part of an integrated health and care system.
The ‘Improving health and wellbeing throughout the life-course’ priority has been further broken down into individual OGIM’s for the following life course periods; ‘starting well’, ‘living well’, ‘ageing well’ and ‘dying well’. The OGIMs can be found in section 5.
1) Enabler: Local system leadership and workforce development
Care Health Improvement
Population Focus
2) Protecting the health of the population as a whole
3) Tackling the wider determinants of health and wellbeing
Individual Focus 4) Providing high quality person-centred care
5) Improving health and wellbeing throughout the life-course
6) Enabler: Population Health Management
3

5. Detailed Population Health OGIMs for North Cumbria Health & Care 2019 - 2022
Created: November 2018 Reviewed: June 2019
Initiatives highlighted in red are priorities within the 19/20 North Cumbria Health and Care System Plan
1) Enabler: Local System Leadership and Workforce Development
Objectives Goals Initiatives Metric Lead
Develop a population health system that: • Distributes focus across
all priority areas within the framework
• supports connections between the priority areas within the framework
• Strong population health leadership at all levels of the system
• A workforce aligned to population health priorities
• Activated individuals and
communities championing wellbeing and self-care
• Population Health/Population Health Management leadership programme established and delivered
• Organisational/Workforce development programme established and implemented
• Population Health
Comms and Engagement plan developed and implemented
Number of individuals across the system supported to champion/lead a population health approach: • Number of Training opportunities • Number of Development sessions • Comms and Engagement Plan
developed. • Level of Comms activity
NHS North East Leadership Academy developing a population health leadership programme for the North East and North Cumbria. CLIC Leadership Group developing a local ‘place-based’ leadership offer. Comms and Engagement Plan: North Cumbria Health & Care System Comms
2) Protecting the health of the population as a whole OGIM 4

Objectives Goals Initiatives Metric Lead
Increase vaccination uptake across eligible populations (including workforce)
• Reduce variation in uptake between practices, ICCs and socio-economic groups
• Support those who find it
most challenging to attend vaccination/screening appointments/clinics
• Use data and intelligence more effectively to target individuals who have missed vaccinations/screens
• Utilise the primary care workforce and local health volunteers to proactively follow-up those with missed vaccinations/screens
• Adopt evidence-based approaches to support uptake (e.g. sending set-time appointment invitations)
• % change in uptake rates (population level)
• % change in uptake rates (target
groups)
• ICC delivery/action groups supported by NECSU, Public Health and NHS England
Reduce the difference in uptake of screening programmes between ICCs
Support a reduction in the number of gram negative bloodstream infections
• Reduce number of community acquired urinary tract infections (UTIs)
• Catheter passport for all patients having a catheter inserted
• To dip or not to dip – use of UTI assessment tool following clinical assessment
• Use of aseptic non-touch technique when dealing with catheter care
• Encouraging use of red top bottles to obtain lab result. Only prescribing appropriate antibiotics following a positive lab result
• Reduction in incidence of UTIs • Reduction in number of gram
negative e-coli infections specifically linked to UTIs
• Integrated Care Communities with support from Cumbria County Council’s Health Protection Team
3) Tackling the wider determinants of health and wellbeing OGIM
5

Objectives Goals Initiatives/Metric Lead
Planet: Cumbria’s natural environment, from the Lake District World Heritage Site to the centre of our towns, will be protected and enhanced. Sustainability will be at the heart of future development, and Cumbria will reduce its ecological footprint even as it develops economically. People: Everyone in Cumbria will have the opportunity to develop and use their skills and talents in a way that recognises the value they bring to society, and to enjoy a varied and fulfilling life. Participation: Cumbrian communities will be strong, resilient and inclusive, with well-developed social networks and widespread engagement with community life. Place: Cumbria’s physical infrastructure will promote health and wellbeing, with good quality housing, a high quality urban environment, and good access to the services needed for a healthy lifestyle. Prosperity: Cumbria’s economy will develop sustainably, with growth particularly focused on tackling poverty and providing quality employment for all.
- Green and blue spaces are protected, and where possible enhanced. Usage is maximised. Air quality is improved. Fuel poverty is reduced.
- Reduce disparities in educational attainment and
increase the proportion of the workforce with higher level skills and qualifications, halving the current gap by 2028
- Ensure people have access to informal social
activities, and feel connected to their local community. Ensure that Cumbria’s communities and community organisations have access to the support they need to flourish.
- Prioritise active transport, ensure there is access
to a diverse range of food (to purchase and grow). Community and health infrastructure meet’s local needs, maximising the potential for redevelopment, while also making use of empty premises and spaces and encouraging opportunities for co-location.
- Reduce the proportion of households living in
poverty. Reduce the rate of children in poverty.
• ICCs, clinical networks and the Health and Care System are asked to support the implementation of this strategy
• Your local public
health locality manager or consultant in public health can advise on how to do this. An initial example is Eden ICC are supporting reductions in Fuel Poverty.
• Metrics are being
defined and monitored via the Joint Public Health Strategy.
• Health and Wellbeing Forums in conjunction with ICC Delivery/Action groups.
4) Providing high quality person-centred care OGIM
6

Objectives Goals Initiatives Metric Lead
In line with the NHS Personalised Care Plan, develop a North Cumbria approach to social prescribing, which in turn supports people’s ability to self-care and connect to support within their communities
- Improved social prescribing pathways in place by March 2020
- Improved digital support for social prescribing
- Clear mechanism in place for resourcing third sector capacity
- Social prescribing programme, including Link Worker Funding (NHSE)
- Third Sector coordinator posts - Living Well - Fundraiser Posts (funded by
Public Health, employed by CVS)
• Number of link workers in post
• Number of people referred via social prescribing approach
• Amount of external funding secured
• Personalised Care Lead: Caroline Rea
• Fundraising Lead: Jozi
Brown - CVS
Improved long term condition pathways that support: • self-care • early intervention • optimised secondary
prevention
- Prevention, early detection and patient activation fully integrated into long term condition pathways.
- Suggested areas – multi-morbidity, CVD, Falls and fragility, fractures, stroke, diabetes, COPD
- Making Every Contact Count (MECC)
- Population Health High Impact Actions (see appendix 1): 1) Weight Management 2) Stop Smoking initiatives 3) Physical Activity pathway 4) Optimise NHS Health Checks 5) CVD prevention through
detection and management of AF, Blood Pressure and Cholesterol
• Number of staff trained – MECC
• Outputs from AF
optimisation programme • Data from Copeland Stroke
Prevention Community Events
• MECC: Public Health • AF optimisation
programme: Helen Horton/Emma Graham
• Copeland Stroke
Prevention: Project Steering Group facilitated by Julie Clayton
5a) Improving health and wellbeing throughout the life-course
7

Starting Well OGIM (Preconception, Maternity and 0-3 age range)
Objectives Goals Initiatives Metric Lead
Increase the number of children who are breastfed at birth and continue to be breastfed two months later in North Cumbria
Achieve a 2% increase year-on-year in the initiation and continuation at 6-8 weeks of breastfeeding across North Cumbria
- Baby Friendly Initiative - Actions outlined in the ‘Starting Well’ Breastfeeding Action Plan* (March 2018), including improving peer support provision
• 100% relevant settings (including neonatal) to have achieved Baby Friendly Initiative stage 3 accreditation by 2020/2021
• Number of breastfeeding peer
support groups available across North Cumbria
• Cumbria Breastfeeding Friendly Initiative and Infant Feeding Steering Group
Increase the number of professionals, volunteers and residents who are aware of and champion clear consistent ‘Making Every Contact Count’ (MECC) approaches to wellbeing before, during and after pregnancy
Making Every Contact Count resources developed and shared by the end of March 2020
- MECC guides produced for each of the Starting Well priority areas:
• Breastfeeding • Stop smoking • Alcohol • Healthy weight • Vaccinations • Safe spacing
between pregnancies
• Domestic violence • Mental wellbeing • Cold weather
risks/planning
• Number/% of guides approved by the Better Births Board
• Denise Lightfoot, Public Health Lead Midwife, NCUH
5b) Improving health and wellbeing throughout the life-course
Starting Well OGIM (4-19 Years age range)
8

Objectives Goals Initiatives Metric Lead
Halt the increase in overweight and obesity amongst children and young people in North Cumbria. Be aspirational and aim to reduce prevalence in each district/ICC.
Reception (4-5 year-olds) Minimum: For each district/ICC, there should be no increase in the percentage of overweight and obese children in reception year. Aspirant: Reduce prevalence of overweight and obesity in reception years to 22% (current national average) by 2020/21. Year 6: Minimum: For each district/ICC, there should be no increase in the percentage of overweight and obese children in year 6. Aspirant: Progress should be made to bring down the levels of overweight and obesity in year 6 down to the best district rate in Cumbria (29%).
- ICC reference/delivery groups to define their own healthy weight plans
- Community Initiatives could include physical activity events such as ‘Mile a day’ and Park Run and healthy eating activities such as cookery clubs.
- Develop and commission an
agreed pathway for tier 2-4 healthy weight services for children and young people
• Number of ICC Healthy Weight Plans developed during 2019
• Pathway agreed by
March 2020 (as phase two of the adult pathway being developed during 2019/20)
• ICC delivery/action groups in partnership with local people & e.g. VCS orgs/groups public health, schools, colleges, district councils, Active Cumbria, leisure providers
• Public Health
(Claire King)/NCCCG (Helen Horton)
Reduce the number of physically inactive children and young people and support them to develop positive attitudes to physical activity.
To increase the take up of PE, school sport and community based physical activity and sport opportunities to tackle inactivity. To support children and young people to develop positive attitudes to physical activity. To reduce current ‘Less Active’ (less than an average of 30 minutes a day) rates for children and young people in year groups 1-11: • Allerdale: 30.7% • Carlisle: 34.3% • Copeland: 36% • Eden: 18.9% (Active Lives Survey Children and Young People 1)
ICCs to work with Active Cumbria, education partners, school sport networks and local third sector/leisure providers to: • Develop a range of needs led
activity opportunities through the delivery of programmes such as 100 Mile Challenge / Daily Mile, Satellite Clubs and after school clubs to help tackle inactivity and develop positive attitudes to physical activity.
• Influence schools to adopt
whole school approaches to physical activity in order to improve pupils’ health and wellbeing.
• Outcome: Increased physical activity has contributed to improved health and wellbeing of the people of Cumbria
• Output: Numbers of CYP moving out of ‘Less Active’ (less than an average of 30 minutes/day) into ‘Fairly Active’ (an average of 30-59 minutes/day minutes/week) or ‘Active Across the Week’ (an average of 60 minutes or more a day but not every day) or ‘Active Every Day’ (60 minutes or
• ICC delivery/action groups in conjunction with Active Cumbria and education partners
9

• Apply for/source funding in order to increase physical activity provision that helps to improve the health and wellbeing of children and young people.
more every day) • Measure: Active Lives
Survey Children and Young People
Support children and young people to: • achieve and maintain
good levels of mental wellbeing
• be smoke free (by not smoking themselves or being exposed to second-hand smoke)
ICC delivery/action groups to consider how best to measure improvements in mental wellbeing amongst children and young people and attitudes towards smoking/exposure to second-hand smoke (based on outputs and outcomes from the initiatives developed locally). (Consider National Tobacco Control Plan Target - reduce the number of 15 year olds who regularly smoke from 8% to 3% or less)
To be determined by individual ICCs, but may include • Peer support and education programmes (5-19 Public
Health Team can support) on topics such as resilience, digital wellbeing and adverse experiences/trauma
• Awareness campaigns co-produced with young people • Promoting and enforcing smokefree environments and
estates Also: • See Cumbria Children’s Trust Board strategy re: ‘Getting
advice’ as part of the Thrive model and actions under the ‘resilience’ priority
• Consider ways to support the recommendations within the 2018 Director of Public Health’s Annual report on Adverse Childhood Experiences (due to be published Dec 2018)
• ICC delivery/action groups supported by Public Health Locality Managers and Consultant in Public Health
5c) Improving health and wellbeing throughout the life-course
Living Well/Ageing Well OGIM (20+ years) (1/3)
Objectives Goals Initiatives Metric Lead
10

Reduce smoking rates in communities in North Cumbria.
National Tobacco Control Plan target: Reduce smoking prevalence to 12% Current prevalence: • Allerdale: 17.2% • Carlisle: 13.9% • Copeland: 19.7% • Eden: 14.7%
- Individual ICCs to develop plans. Public Health Locality Managers to support ICCs around best evidence-based approaches
- Improve provision of specialist
stop smoking support to target groups e.g. those in hospital, people living severe and enduring mental health conditions and pregnant women (see high impact change 1)
• Outputs and outcomes links to ICC plans
• Numbers receiving
intensive support (referrals, completers, smoking status) through the stop smoking pilot being developed and delivered at CiC during 2019/20
ICC delivery/action groups • Public Health
(Claire King) and Respiratory Consultant – Matthew Lane
Reduce the prevalence of overweight and obesity amongst the adult population
Minimum: Aim to have no further increase in the rate of adults who are overweight or obese within ICCs. Aspirant: reduce rates in the ICCs with the highest levels in line with the North Cumbria average by 2020/21. Highly Aspirant: Reduce adult obesity prevalence to 20%
- Whole systems approach. ICCs can ask their Public Health Locality Manager to advise them on this
- Develop a weight
management pathway for North Cumbria. Link to other clinical pathways (see high impact change 1)
• Outcome measure: Obesity prevalence and % body weight lost
• Output measures: dependent on initiatives developed e.g. number of initiatives, initiative attendance, customer/patient surveys, relevant training completion
• ICC delivery/action groups
• Public Health/NCCCG
Living Well/Ageing Well OGIM (20+ years) continued (2/3) Objectives Goals Initiatives Metric Lead
Reduce the number of physically inactive adults, specifically older adults and those from low socio
To create new local sustainable community based introductory style physical activity interventions to tackle inactivity focusing upon behaviour change.
ICCs to work with Active Cumbria and local third sector/leisure providers to: - Explore opportunities to improve
• Outcome: Increased physical activity has contributed to improved health and
• ICC delivery/action groups in conjunction with
11

economic groups to change their behaviour and become regularly active.
To reduce current ‘Inactive’ (less than 30 minutes/week moderate intensity physical activity) rates for adults aged 16+: • Allerdale: 23.2% • Carlisle: 23% • Copeland: 27.2% • Eden: 23.4% (Active Lives Survey 4)
links between health and care services and physical activity programmes, such as the Cumbria Walking for Health Scheme, Activate and GLL’s ‘Healthwise’ programme.
- Pathway: Apply for/source funding in
order to increase physical activity provision that helps to prevent as well as manage long term conditions (see high impact change 3).
wellbeing of the people of Cumbria
• Output: Numbers of people moving out of ‘Inactive’ (less than 30 minutes/week) into ‘Fairly Active’ (30-149 minutes/week) or ‘Active’ (150+ minutes/week)
• Measure: Active Lives Survey
Active Cumbria • Pathway: Public
Health (Claire King) and Active Cumbria (Bruce Lawson)
Reduce the number of people developing long term conditions such as diabetes, respiratory illness, CVD and dementia. Reduce the burden of multi-morbidity on health & care services Increase the age at which people develop long term conditions
Shift the curve – reduce the inequalities gap between the number of 50 year olds who have developed one or more LTC: e.g. most deprived 50 year olds approx. 40% have one or more LTC. Least deprived = approx. 18%. Reduce this 22% gap
- High Impact Changes (see appendix 1)
- Use population health management approach – RAIDR to risk stratify ICC and GP practice populations
- Improve integration of prevention (including NHS Health Checks and National Diabetes Programme) into Long Term Condition pathways
• Outcome: prevalence of long term conditions, multi- morbidity and related health inequalities gap
• Outcomes: Number of pathways redesigned to include greater emphasis on population health and prevention
• High Impact Changes: Public Health (Claire King)
• RAIDR – NECSU
• Prevention within clinical pathways: Public health (Claire King)
5d) Improving health and wellbeing throughout the life-course Living Well/Ageing Well OGIM (20+ years) continued (3/3) Objectives Goals Initiatives Metric Lead
Whilst we do not currently have a reliable measure of loneliness levels in our community (an indicator is
North Cumbria Social Prescribing approach to be designed and implemented during 19/20
- Community/third-sector groups and activities, such as ‘Hug a Mug’ (Maryport)
- Living well programme
• Outcome: changes in self-report levels of loneliness
• Output: Number of referrals made via social prescribing
• Third sector (ACTion for Cumbria have developed a
12

being developed nationally as part of the Government’s new loneliness strategy) we will: Increase the number of locally developed initiatives that support social connection and reduce isolation
ICCs to develop approaches to reducing social isolation across its communities. Plans developed by March 2021
(Keswick & Solway, Eden) - Initiatives aimed specifically at
groups at higher risk of loneliness e.g.
o New mums (baby and toddler groups)
o Young single men e.g. Men in Sheds initiative (Carlisle)
o Those with long term disabilities
- Community connectors (e.g. link workers based in coordination hubs, volunteers/health champions)
- Marketing campaign – celebrating Neighbourliness
platform, number of initiatives, numbers attending, coverage/accessibility
Neighbourliness forum)
• ICC delivery/action groups
• CCC Public Health/Area Teams
5e) Improving health and wellbeing throughout the life-course Dying Well OGIM Objectives Goals Initiatives Metric Lead
North Cumbria Health and Care should actively promote the model of person-centred care as being at the heart of the new approach to delivering health
The data on place of death should be actively monitored and consideration given to setting a goal of increasing the proportion of people dying at home or in a hospice setting
- Promote a ‘café conversation’ approach to discussing death and encourage people to feel comfortable talking about their wishes and planning for the end of their lives
• Outcome: Number of local people with an end of life care plan in place
• Outputs: Number of initiatives/events held. Self-
• ICC reference/ delivery groups in partnership with the third sector
13

and cares services in the County (see the Cumbria Director of Public Health’ Annual Report 2017 for more detail)
Community approaches are developed to engage the public more in local action through community development approaches, particularly in partnership with third sector organisations.
reported changes in people’s attitudes and beliefs about the end of life
6) Enabler: Population Health Management (PHM) Approach Objectives Goals Initiatives Metric Lead
Develop the capability of the North Cumbria Health & Care System to manage population health effectively
Develop and implement a population health management plan
- Continued involvement in national NHSE Communities of Practice
- ICS RAIDR platform – continued
development
• Number/% of Community of Practice events attended by representatives from the North Cumbria System
• RAIDR ICS platform launched • Number/% of ICCs who have used
RAIDR to risk stratify their population
• CoP: John Howarth
• RAIDR Development: Holly Marshall (NCCCG)
14

Utilise business intelligence tools (such as RAIDR) to inform pathway development
Initial focus areas: - COPD - CVD
• RAIDR Lung Health tool rolled out • Lung health tool used by ICCs to
support patients with most need • RAIDR CVD risk stratification
developed for use by practices • CVD risk stratification used by
ICCs to target at risk patients
• Holly Marshall (NCCCG) and NECSU (Ian Nicholson)
ICCs to have utilised Business Intelligence tools (such as RAIDR) to risk stratify/segment their populations to better manage population health
- Risk Strat: COPD, Diabetes - Segmentation: Long Term Conditions - Trust employed practice pharmacist to
use RAIDR to identify and reduce inappropriate use of medicines of low clinical value, review COPD prescribing/ inhaler choice and review and improve CVD prescribing.
• RAIDR population segmentation, sub-segmentation and forecasting tool in place
• ICCs and practices supported to develop plans to use population segmentation tool for providing focused interventions for cohorts of patients
• Epact reports will used to track performance and progress will be reported to Medicines Optimisation Committee
• Holly Marshall (NCCCG) and NECSU (Ian Nicholson)
• Pharmacy Initiative: Andrea Loudon
15

Appendix 1:
North Cumbria Health & Care: Population Health Identifying High Impact Actions
Introduction 2019/20 will be an exciting year for population health developments in North Cumbria. At a system level, population health is an identified priority for development across Health & Care Integration. Our clinical networks will be defining how, as a system, we develop effective person-centred pathways that prevent, as well as manage, long-term conditions. Our eight Integrated Care Communities (ICCs) will also be identifying their population health approaches that build on local assets and mobilise communities at scale to achieve the best wellbeing possible for the people of Cumbria. In order to support this, a North Cumbria population health plan for 2019 – 2022 has already been drafted. Informed by our Joint Strategic Needs Assessment and the Cumbria Health and Wellbeing Strategy 2019 – 2029, the plan identifies a number of priority areas for improving the population’s health (and should be used in conjunction with Business Intelligence tools such as the ICC Health Profiles). The plan clearly tells us ‘what’ we need to do. What it does not tell us is the ‘how’ and this is because the ‘how’ needs to be co-produced between all partners, including local people. Co-production will be even more powerful if partners feel informed to make effective decisions. The aim of this paper is to provide a summary of the extensive research and policy that is currently shaping population health approaches in England. It is hoped this information will be a useful tool in helping to identify activity that can significantly impact on our population health ambitions; to increase Healthy Life Expectancy and reduce health inequalities. Methodology The following approach has been used to identify the high impact areas outlined in this paper:
Step 1: Identify conditions that
have the greatest impact on morbidity
and mortality
Step 2: Identify the preventative (modifiable) factors that
have the greatest impact on these conditions
Step 3: Identify the actions that
have been shown to significantly modify the
factors identified through step 2
16

Step 1: Identifying conditions that have the greatest impact on morbidity and mortality in the UK 1a. What causes the most premature deaths? Top 10 causes of years of life lost (YLL) in 2017 and percent change, 2007-2017,
all-age numbers (1)
Rank 2007 2017 % change between 2007 - 2017
1 Ischemic Heart Disease
Ischemic heart disease -16.8%
2 Lung Cancer
Lung Cancer 1.7%
3 Stroke
Stroke -12.0%
4 COPD
Alzheimer’s Disease 25.8%
5 Alzheimer’s disease
COPD 7.1%
6 Lower respiratory infections
Lower respiratory infections 6.5%
7 Colorectal Cancer
Colorectal cancer 5.1%
8 Breast Cancer
Breast cancer -3.0%
9 Self-harm
Cirrhosis 6.5%
10 Cirrhosis
Self-harm 1.8%
17

1b. What health problems cause the most disability? Top 10 causes of years lived with a disability (YLDs) in 2017 and percent change, 2007-2017, all-age numbers (1)
Rank 2007 2017 % change between
2007 - 2017 1 Low back pain
Low back pain 10.2%
2 Headache disorders
Headache disorders 5.7%
3 Depressive disorders
Depressive disorders 7.6%
4 Neck pain
Neck pain 8.3%
5 Falls
Diabetes 42.8%
6 COPD
Falls 16.5%
7 Age related hearing loss
Age-related hearing loss 14.9%
8 Diabetes
COPD 10.0%
9 Anxiety disorders
Anxiety disorders 5.6%
10 Asthma
Other musculoskeletal 5.4%
18

1c. What causes the most death and disability combined? Top 10 causes of disability-adjusted life years (DALYs) in 2017 and percent change, 2007-2017, all-age numbers (1)
Rank 2007 2017 % change between
2007 - 2017 1 Ischemic Heart Disease
Ischemic heart disease -15%
2 Low back pain Low back pain
10%
3 COPD
COPD 8%
4 Lung cancer
Lung cancer 2%
5 Stroke
Stroke -7%
6 Alzheimer’s disease Alzheimer’s disease
24%
7 Headache disorders
Headache disorders 5%
8 Depressive disorders Depressive disorders
7%
9 Diabetes Diabetes
31%
10 Falls
Falls 15%
19

Step 2a: What risk factors drive the most death and disability combined in the UK? Top 10 risks contributing to DALYs in 2017 and percent change, 2007-2017, all ages, numbers (1)
Rank 2007 2017 % change between
2007 - 2017 1 Tobacco
Tobacco -9.2%
2 Dietary risks
Dietary risks -6.7%
3 High blood pressure
High body mass index 7.6%
4 High body mass index
High blood pressure -12.6%
5 High fasting plasma glucose
High fasting plasma glucose 21.5%
6 High LDL
Alcohol use 2.0%
7 Alcohol use
High LDL -15.8%
8 Occupational risks
Occupational risks 4.7%
9 Air pollution
Air pollution -8.4%
10 Drug use
Drug use 13.0%
20

Step 2b: Mapping top ten 2017 risk factors and approaches across the ‘prevent’ ‘detect’ and ‘protect’ elements of clinical pathways (please note this mapping assumes that the wider determinants of health and primary care mental health will
be considered through other workstreams)
Risk Factor Prevent (for consideration by ICCs and maternity services)
(not including wider determinants)
Detect (optimise evidence-based approach and embed in clinical
pathways)
Protect (fund high quality services, embed in pathways
and optimise medical management)
Tobacco - Starting well - Tackling smoking (preconception and in pregnancy)
- Education programmes in schools and community settings (preventing smoking & e-cig
use) - Reducing second-hand smoke exposure in
homes, vehicles and public spaces
- CO monitoring by midwives/BabyClear
programme - Asking smoking status –
Making Every Contact Count - NHS Health Checks
- Brief advice in health & care settings
- Specialist Programme (Behavioural/addiction support + access to NRT/medication - including e-cigarettes where
appropriate) Dietary risks - Starting well - Promoting healthy diet
(preconception and during pregnancy) - Education programmes in schools and
community settings - 5-a-day/swap campaigns
- Asking about diet – Making every contact count
- Blood tests (for conditions such as anaemia)
- Brief advice/social prescribing - Dietician input
- Very low calorie diets (potential to be introduced via National Diabetes Prevention
Programme) High body mass index
- Whole systems approach to healthy weight - Starting well - Promoting healthy diet
(preconception and during pregnancy) - Physical activity initiatives - Healthy diet – campaigns
- National Child Measurement Programme
- Measuring BMI – Making Every Contact Count
- NHS Health Checks
- Brief advice/social prescribing - Weight Management pathway
- Physical activity pathway - Medical management
High blood pressure
- Starting well - Lifestyle advice (preconception and during pregnancy)
- Physical activity initiatives - Preventing smoking (educational campaigns)
- Preventing poor diet (e.g. salt intake) - Maintaining healthy weight (see above)
- Alcohol consumption within recommended levels
- NHS Health Checks - Testing during pregnancy
- Targeted community-based testing (in agreement with
primary care)
- Medical management - Brief advice/Social Prescribing
- Physical activity pathway - Weight management pathway
- Specialist stop smoking support
21
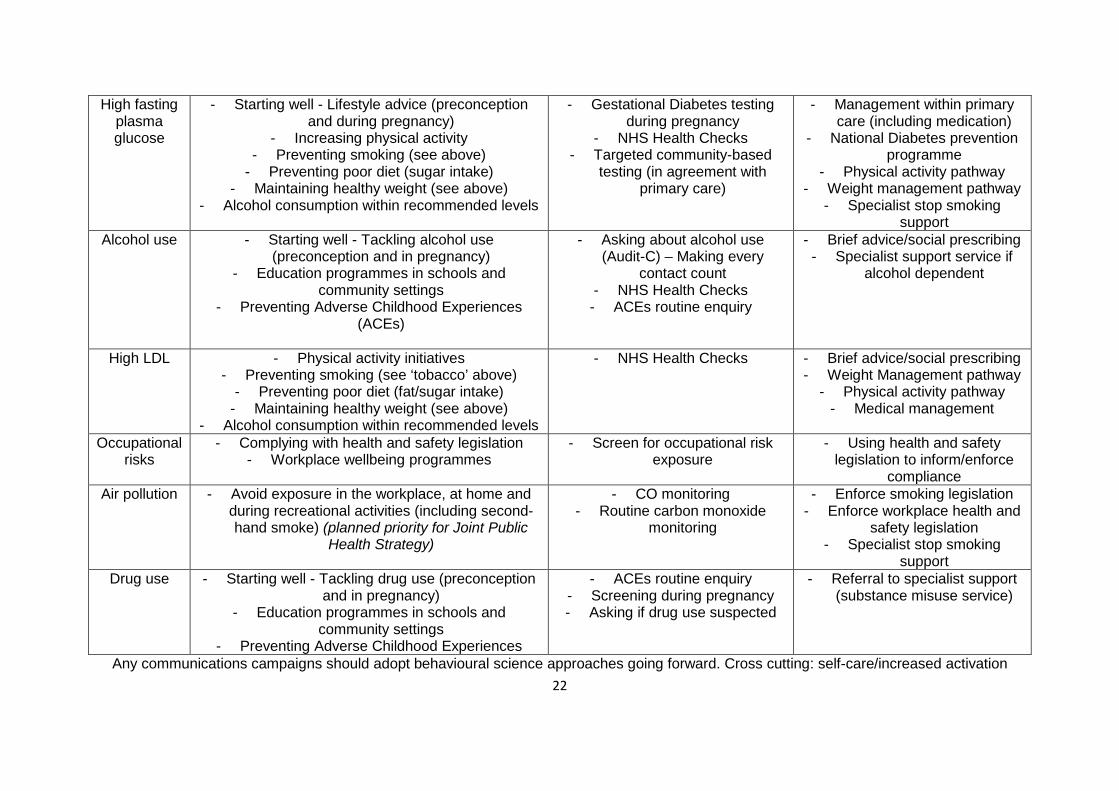
High fasting plasma glucose
- Starting well - Lifestyle advice (preconception and during pregnancy)
- Increasing physical activity - Preventing smoking (see above)
- Preventing poor diet (sugar intake) - Maintaining healthy weight (see above)
- Alcohol consumption within recommended levels
- Gestational Diabetes testing during pregnancy
- NHS Health Checks - Targeted community-based
testing (in agreement with primary care)
- Management within primary care (including medication)
- National Diabetes prevention programme
- Physical activity pathway - Weight management pathway
- Specialist stop smoking support
Alcohol use - Starting well - Tackling alcohol use (preconception and in pregnancy)
- Education programmes in schools and community settings
- Preventing Adverse Childhood Experiences (ACEs)
- Asking about alcohol use (Audit-C) – Making every
contact count - NHS Health Checks - ACEs routine enquiry
- Brief advice/social prescribing - Specialist support service if
alcohol dependent
High LDL - Physical activity initiatives - Preventing smoking (see ‘tobacco’ above)
- Preventing poor diet (fat/sugar intake) - Maintaining healthy weight (see above)
- Alcohol consumption within recommended levels
- NHS Health Checks - Brief advice/social prescribing - Weight Management pathway
- Physical activity pathway - Medical management
Occupational risks
- Complying with health and safety legislation - Workplace wellbeing programmes
- Screen for occupational risk exposure
- Using health and safety legislation to inform/enforce
compliance Air pollution - Avoid exposure in the workplace, at home and
during recreational activities (including second-hand smoke) (planned priority for Joint Public
Health Strategy)
- CO monitoring - Routine carbon monoxide
monitoring
- Enforce smoking legislation - Enforce workplace health and
safety legislation - Specialist stop smoking
support Drug use - Starting well - Tackling drug use (preconception
and in pregnancy) - Education programmes in schools and
community settings - Preventing Adverse Childhood Experiences
- ACEs routine enquiry - Screening during pregnancy - Asking if drug use suspected
- Referral to specialist support (substance misuse service)
Any communications campaigns should adopt behavioural science approaches going forward. Cross cutting: self-care/increased activation22

Section 3:
Tackling the risk factors:
5 High Impact Population Health Actions
23

1. Prevent (primary prevention): Develop a robust weight management pathway for both adults and children
Description: Cumbria is facing an obesity epidemic. By the time children enter primary school, 1 in 4 is already overweight or obese and, by the time they leave primary school, that figure increases to 1 in 3. In adults, an estimated 62% of the population is overweight or obese. Tackling obesity and its causes is high on the public health agenda and it is clear that there is no simple solution. Public Health recognises that cross-sector, system-wide action is required to change the status quo and the County Council is supporting the development of a whole-systems approach to healthy weight, which aims to coordinate action across a life-course and place-based approach. The approach will ultimately need to include the local delivery of evidence-based, effective and sustainable tier 2 and 3 weight management (WM) services, as recommended by the National Institute for Health and Care Excellence (NICE), which individuals and families can access if they are above a healthy weight. The National Institute for Health and Care Excellence (NICE) recommends that WM services are provided for adults with a body mass index (BMI) of >25, and for children, >91st centile, as part of a tiered approach to WM services. Health Inequalities Considerations • People living with learning disabilities, mental ill-health and in deprived areas are more
likely to be overweight or obese. • 12.8% of children in reception age in Cumbria from the most deprived areas are obese
compared to 5.7% in the least deprived. • 20% of people accessing the current adult Tier 2 service are from the most deprived
decile. • Men are less likely to access the current tier two programme in Cumbria (but 18% males
access the Cumbria Slimming World compared to 10% elsewhere). Alternative pathway (e.g. physical activity) would be beneficial for men
• Current analysis shows the tier 2 weight management programme supports people with disabilities (carers can access the programme for free when accompanying the person they care for)
What could next steps look like? Development of a business case to support the development of a weight management pathway (children and adults).
Timescales for Impact: Weight management interventions aim to have lifelong impact and are unlikely to manifest as high savings in the short term. Tier 2/3 interventions could be cost saving to the health and care system by year 2.
24

2. Prevent (primary prevention): Increase the provision of targeted specialist stop smoking support
Description: Smoking accounts for an estimated 22 percent of adult hospital admission costs and remains the leading cause of preventable ill health in England and a major cause of health inequalities. Currently in Cumbria we do not have a specialist stop smoking service (however self-referred support is available through many pharmacies). As a result, the successful quit rates in Cumbria are understandably low. We therefore need to invest in increased specialist stop smoking support. This should be targeted at specific groups (as listed under the evidence section below). Evidence of Effectiveness: Specialist treatment within secondary care: The CURE project at Wythenshawe Hospital is a treatment programme for tobacco addiction. The costs and predicted savings are outlined here (note: Wythenshawe provides tertiary services): http://www.innovationagencyexchange.org.uk/sites/default/files/CURE%20Summary%20-Treating%20Tobacco%20Addiction.pdf Smoking in Pregnancy: Implementing the ‘BabyClear’ Programme: https://www.ncl.ac.uk/press/articles/archive/2017/02/schemessuccessatstoppingmums-to-besmoking/ Specialist support for those with severe mental health issues: Smoking Cessation Intervention for Severe Mental Ill Health (SCIMITAR) Trial: Gilbody S, Peckham E, Man MS, et al (2015) Bespoke smoking cessation for people with severe mental ill health (SCIMITAR): A pilot randomised controlled trial. The Lancet [Abstract] Health Inequalities Considerations? People with severe mental health issues are more likely to start smoking earlier, smoke more cigarettes per day and find it more difficult to quit. Evidence suggests that smoking rates are reducing in most population groups, except those from our most deprived communities. Timescales for Impact: The biggest short-term savings opportunity lies in helping smokers who are in contact with the NHS; the greatest long-term savings would come from preventing people from ever smoking altogether
25
3. Prevent (primary prevention): Increase the provision of Physical Activity opportunities for those at risk of/diagnosed with a long term health condition (including falls and mental health problems)
Description: It is estimated that the health cost of physical inactivity in Cumbria amounts to £9,100,000 every year, with additional costs to wider society. The UK Chief Medical Officers (CMOs) recommend adults undertake at least 150 minutes per week of moderate intensity or 75 minutes per week of vigorous intensity physical activity or a combination of both, plus building strength and improving balance activities on two days per week as well as minimise extended periods of sitting. Current evidence shows that 23.8% of men and 26.4% of women are doing less than 30 minutes activity per week, and 50.4% of those with 3 or more limiting impairments are inactive. Physical inactivity is responsible for 1 in 6 UK deaths and up to 40% of long term medical conditions. An inactive person has 38% higher hospital bed days, 5.5% higher GP visits and 13% higher use of specialist services. Physical activity can reduce the risk and help the management of over 20 long-term conditions. Evidence of Effectiveness: A number of programmes are endorsed by Public Health England as a result of having a strong evidence-base. Specific to Health & Care are the following: • Healthcare professionals to deliver effective brief advice on the benefits of physical activity.
Invest in raising skills and knowledge of healthcare professionals. • Invest in evidence-based exercise programmes for patients. For example, providing exercise
referral schemes where patients receive supervised support by trained professionals. • Invest/resource in local low-level introductory physical activities for example the Cumbria
Walking for Health Scheme and socially prescribe such activities to patients. Health Inequalities Considerations? Results from the Active Lives Survey demonstrate that people living in deprived areas of North Cumbria are less likely to achieve the recommended physical activity levels. Older adults and people living with disabilities and mental health problems are also less likely to be active. Any weight management referral programme should be targeted at those that are least likely to be physically active. What could the next steps look like? Further work required to assess the feasibility of investing in targeted physical activity programmes. Timescales for Impact: PHE estimates member of staff training healthcare professionals to provide brief advice could deliver a minimum of £308,000 of direct savings to the local NHS over 5 years, through the four modelled conditions alone and potential savings within the financial year. Health Walks - 11p cost per head of a health walk compared to £8.40 prescription (Source: Sheffield Public Health Service)
26

4. Detect (secondary prevention): Optimising the NHS Health Check and follow-up
Description: The NHS Health Check is a health check-up for adults in England aged 40-74. It's designed to spot early signs of stroke, kidney disease, heart disease, type 2 diabetes or dementia. Once someone has had their NHS Health Check, a healthcare professional should discuss the results with the patient. They should be given advice on ow to lower their risk of CVD disease. Evidence suggests that a) not all the recommended tests are routinely completed as part of the NHS Health Check (e.g. the Audit-C to check alcohol consumption levels may not be being asked) and b) follow up does not take place or is of a poor quality (ideally there should be robust arrangements in place to ‘advise’ and ‘signpost/refer’ where appropriate following the checks. Evidence of Effectiveness: The University of Cambridge recently published an evidence synthesis on the NHS Health Check. The study shows there is robust evidence of the effectiveness of NHS Health Checks in improving risk factor identification and in referral and uptake of evidenced based lifestyle and clinical interventions. The study showed that the following actions would maximise the effectiveness of the programme: • Increase statin and anti-hypertensive prescribing • Increase referrals to smoking cessation services • Increase referrals to effective weight management services • Prioritise Invitations Health inequalities considerations? The University of Cambridge study showed that the NHS Health Check can actively reduce health inequalities allaying concerns that the programme would be taken up only by the “worried well”. Furthermore, that it can successfully engage people with the greatest health needs, actively reducing health inequalities, and that individuals having a check are more likely to be diagnosed with a disease and to receive lifestyle or clinical management to help them reduce that risk or manage the health condition. A local Health Equity Audit completed in 2017 showed that there was good uptake across most groups (slightly lower in working-age males). What could next steps look like? Service Development programme supported by CLIC? Possible use of processes such as RPIW (Rapid Process Improvement Workshops).
Timescales for Impact: Impact would be seen in less than five years. Further Information: https://www.healthcheck.nhs.uk/commissioners_and_providers/evidence/
27

5. Protect (secondary prevention): Intervening Early and optimising pathways/medication
Description: Systematically detecting the early stages of disease (see High Impact Action – NHS Health Checks) and intervening before full symptoms develop – for example, prescribing statins to reduce cholesterol and taking measures to reduce high blood pressure. Why is it important? • Secondary prevention is based on a range of interventions that are often highly cost-effective
and that, if implemented at scale, would rapidly have an impact on life expectancy. • There is substantial variation between practices in the systematic implementation of approaches
towards secondary prevention – for example, use of disease registers. Only a minority of patients receive all recommended interventions.
• Evidence suggests that this is an area where the 'inverse care law' applies and those in greatest need are least likely to receive beneficial services.
• Identifying those at risk and intervening appropriately is one of the most effective ways in which GPs can reduce the widening gaps in life expectancy and health outcomes (Marmot Review 2010).
Evidence of Effectiveness: • Successful secondary prevention would have a major impact on health outcomes, in terms of
improvement in life expectancy and reduction in complications. • The National Audit Office (2010) suggests that improving cholesterol levels and hypertension
control have not been adopted at a sufficient scale. If they were, they would have a significant impact on inequalities.
Health Inequalities Considerations? Modelling by the Department of Health (2009) has shown that systematic and scaled-up secondary prevention is a cost-effective, clinically significant and fast way to tackle inequalities in health in local areas. What could next steps look like? Where not already known, development of a population health management approach at ICC/GP practice level to
• ensure appropriate coverage of key secondary preventive interventions and processes including managing disease registers systematically by modelling expected versus actual prevalence and incidence, and thereby identifying practices where improvement is needed
• ensuring systematic control of hypertension, cholesterol and diabetes among ICC populations (resource accordingly)
Timescales for Impact: • Cost savings are likely to accrue over the medium term, as patients are prevented from
experiencing a wide range of adverse events as their life expectancy lengthens.
Further Information: https://www.kingsfund.org.uk/publications/articles/transforming-our-health-care-system-ten-priorities-commissioners/summary
References
1. The Institute for Health Metrics and Evaluation (IHME) (2018) [online] Global Burden of Disease – Data for the United Kingdom. Available from: http://www.healthdata.org/united-kingdom Accessed: 11/02/2019
28


















