syphilis ppt
72
Syphilis By Getahun K
-
Upload
getahunk -
Category
Health & Medicine
-
view
136 -
download
1
Transcript of syphilis ppt

Syphilis
By Getahun K

Contents
• Historical background• Introduction• Features & maof syphilis
-primary-Secondary-Tertiary syphilis
• Congenital syphilis• Syphilis in pregnancy• Tests for detecting syphilis

"syphilos" ---meaning crippled/heart victim.



• T. pallidum
• IP 21 days ….but 10-90days
• Mode of Transmission
-Sexual
direct contact with an infectious moist lesion.
treponemes pass through intact mucous membranes or abraded skin
– Vertical
Primary Syphilis
• Painless genital sore (chancre) on labia, vulva, vagina, cervix, anus, lips, or nipples.
• Painless, rubbery, regional lymphadenopathy followed by generalized lymphadenopathy in the third to sixth weeks.
• Dark-field microscopic findings.
• Positive serologic test in 70% of cases


Syphilis - Treponema pallidum

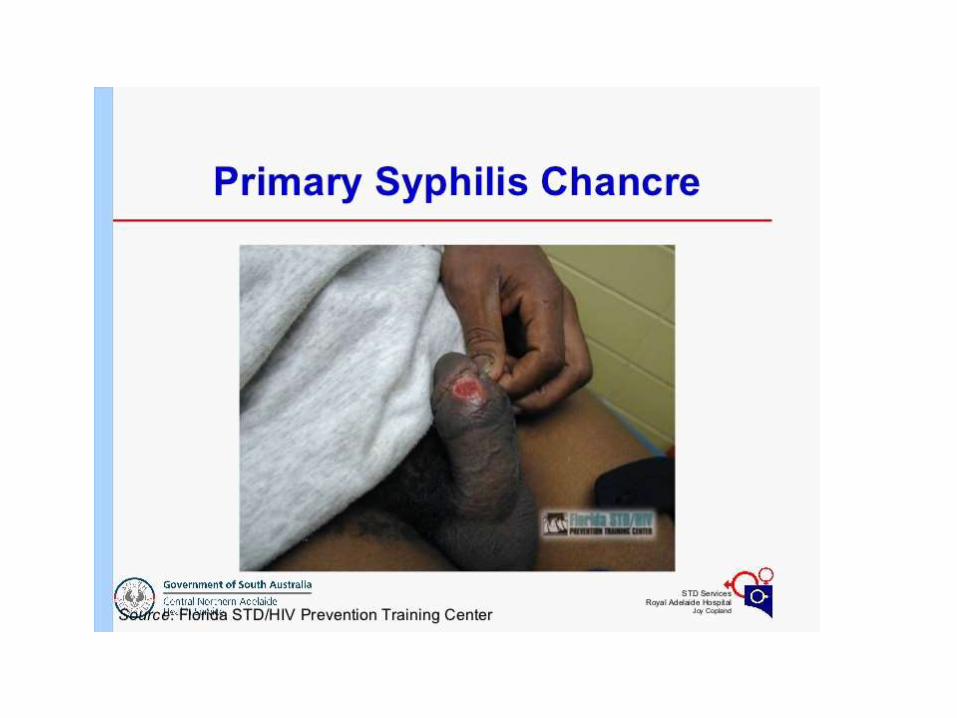
Primary syphilis-chancre
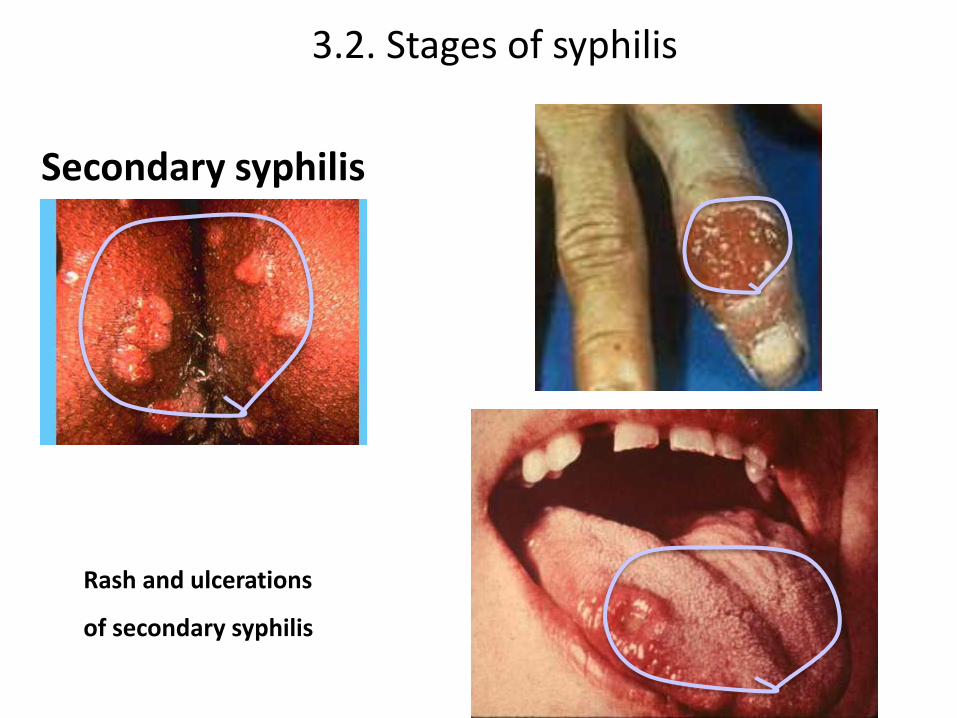
Secondary Syphilis
• Bilaterally symmetric extragenitalpapulosquamous eruption(6 weeks after primary lesion).
• Condyloma latum, mucous patches.
• Dark-field findings positive in moist lesions.
• Positive serologic test for syphilis.
• Lymphadenopathy

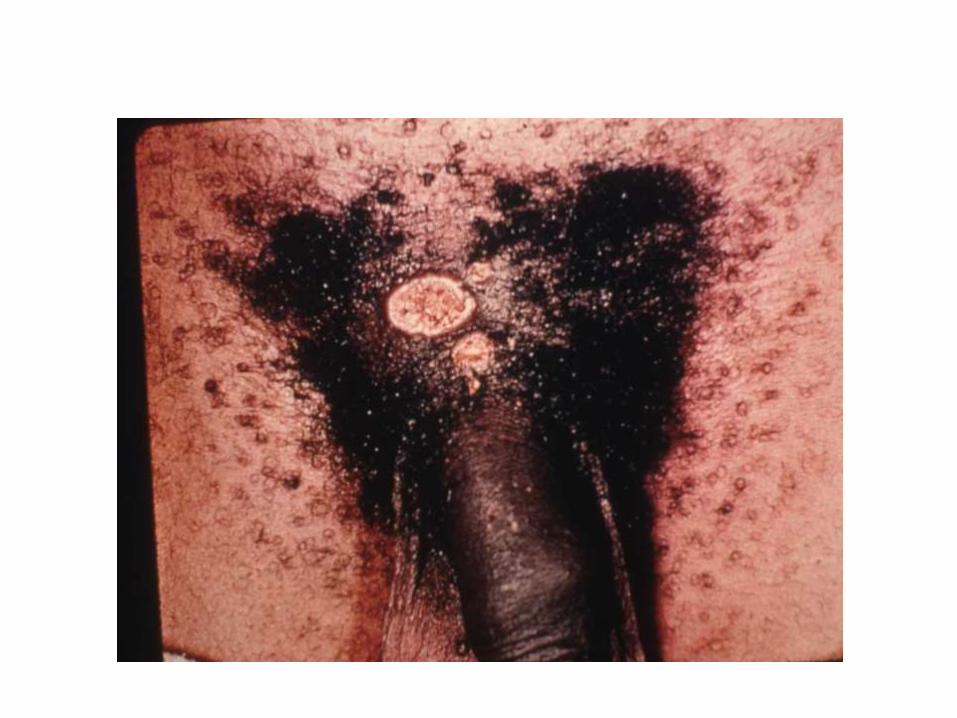
Secondary syphilis - papulosquamous rash


Secondary syphilis

Secondary syphilis - condyloma lata

Secondary syphilis - alopecia
Secondary syphilis
Rash and ulcerations
of secondary syphilis
3.2. Stages of syphilis
Latent syphilis • no clinical signs but syphilis serology is
reactive……….?VDRL• without a history of therapy, a patient passes
into latency• History or serologic evidence of previous
infection1. Early latent = infection less than one year
2. Late latent= infection occur for over one year

Lumbar puncture should be done in latent syphilis of more than 1 year duration if:
• There are neurological symptoms
• Treatment fails
• Serological titer is 1:320 and higher
• Non penicillin therapy is planned
• There is concomitant HIV infection

Tertiary syphilis
- Gumma
- aortitis leading to valve incompetence and aneurysm
- Neuro-syphilis

Neurologic complications or neurosyphilis mayoccur earlier or progress more rapidly in HIV-positive patientsMeningitis, meningovascular, or parenchymatous
disease similar in HIV-uninfected patientsConcomitant uveitis and meningitis more common in
HIV-positive patients
Asymptomatic neurosyphilis (CSF with elevatedprotein, lymphocytosis, or positive serologic test, inabsence of symptoms): not a late complication ormanifestation
Neurosyphilis

• All patients require CSF sampling with laboratory testing for cell count, protein, VDRL, and FTA-ABS.
• FTA-ABS is less specific but very sensitive when diagnosing neurosyphilis.

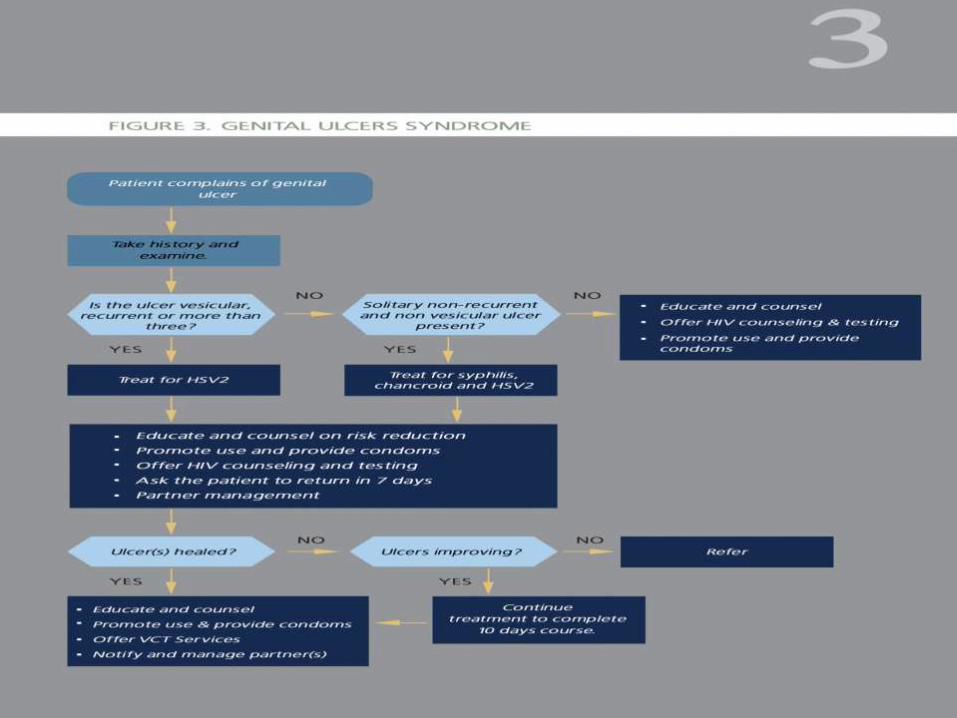
Management of ulcer
Benzathine penicillin 2.4 million units IM stat
Or (in penicillin allergy)
Doxycycline 100 mg bid for 14 days
Plus
Ciprofloxacin 500mg bid orally for 3 days.
Or
Erythromycin tablets 500 mg qid for 7 days

neurosyphilis
• Aqueous bezylpenicillin 10-12 million IU IV, administered daily in doses of 2-4 million IU, every 4 hours for 14 days.
• Alternative regimen:
– Procain benzylpenicillin, 1.2 million IU IM, once daily, and probenecid, 500 mg orally, 4 times daily, both for 10-14 days.

3.2. Stages of syphilis
Primary Syphilis
Secondary Syphilis
Latent Syphilis
Tertiary Syphilis Persistent Asymptomatic
Relapse Trans placental Transmission
Congenital Syphilis
40%60%
Primary Chancre
Secondary lesions
Infection with T. pallidium
Gumma
(5 Yrs)
CardiovascularSyphilis(10-15Yrs)
Tabes Dorsalis(20 Yrs)

CONGENITAL SYPHILIS

• analogous to adult secondary disease, as the disease is systemic from onset due to transplacental hematogenous inoculation
• immunoglobulin (Ig)G (a reactive serologic test if the mother's test was reactive)
• may appear healthy at birth--A rising titerindicates congenital syphilis
Signs and symptoms of early congenital syphilis
• Rhinitis and serosanguinous discharge from nostrils
• Bullous skin lesions
• Periostitis with pseudo paralysis
• Hepatosplenomegaly
• Nephrotic syndrome
• Chorioretinitis




• Confirmed diagnosis
– spirochete on dark field microscopy from placenta or lesions from infant
• Presumptive
– Any infant whose mother had untreated syphilis
– Reactive specific treponemal tests with or without manifestation of congenital syphilis.
Treatment of early congenital syphilis
• Aqueous crystalline penicillin G 50,000 units/kg IV tid for 10 days
Or
• Procaine Penicillin G 50,000 units/kg IM daily for 10 days.
• Note: CSF should be examined with RPR to exclude involvement of the CNS

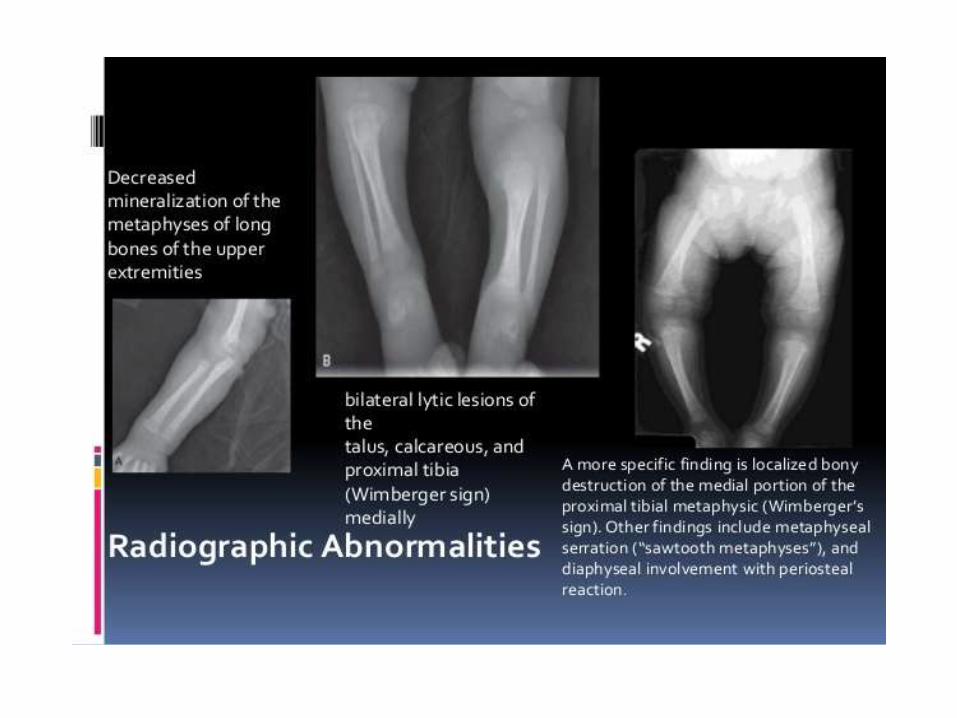
The late manifestations of congenital syphilis
• Deformity of long bones or nasal bridge
• Hutchinson’s triad consisting of deafness, keratitis and peg shaped incisor teeth.
• Hydrocephalus with evidence of mental retardation.
Treatment of late congenital syphilis
• Aqueous crystalline penicillin G 50,000 units/kg IV or IM QID for 10 days
• Alternative regimen for penicillin-allergic patients, after the first month of life
– Erythromycin 7.5-12.5 mg/kg orally, QID for 30 days

SYPHILIS IN PREGNANCY

Syphilis in Pregnancy
• 2.7%
• RPR positivity rate of > 5% indicates high prevalence
• course of syphilis is unaltered by pregnancy
• Treponemes may cross the placenta at all stages of pregnancy, but fetal involvement is rare before 18 weeks because of fetal immunoincompetence
• Grossly, the placenta looks hydropic --pale yellow, waxy, and enlarged.
• Adverse outcomes
– miscarriage or stillbirth
– congenital syphilis in the newborn
– progression of latent syphilis in the mother
• RPR test should be routinely done on pregnant mothers in their first trimester and treatment if shows strong reactivity
• Weak reactivity--specific serologic tests before treatment .

Management
• If primary syphilis, secondary syphilis, or/& history of non-reactive RPR test within the past 2 years:
– Benzathine penicillin G 2.4 million units IM
OR
– If allergic to penicillin, ceftriaxone 1 gm IM daily x 8 – 10 days

reactive RPR test in pregnancy
• If infected more than two years OR no prior history of non-reactive RPR test:– Benzathine penicillin G 2.4 million units IM x weekly
for 3 weeks
OR– If allergic to penicillin, erythromycin 500 mg PO QID
x 30 days
– Repeat RPR in the 3rd trimester or delivery

In all aspects of syphilis
• H/E-safer sexual practice, partner notification & tracing…..
• Condom promotion & use
• Screening for HIV,PREGNANCY
• Looking for complications is needed
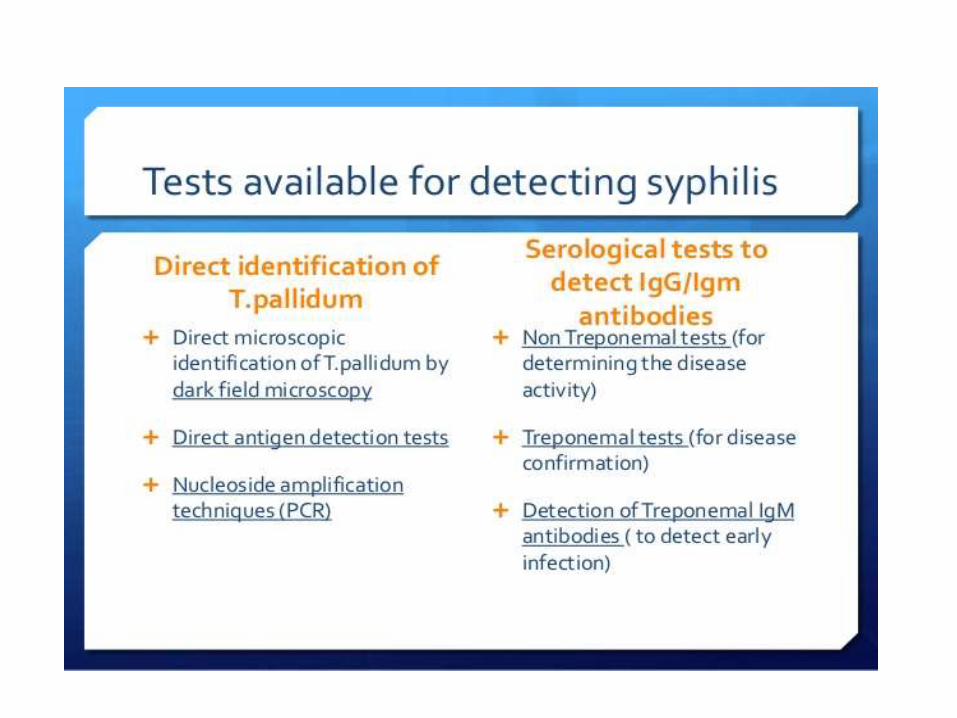


Nontreponemal Tests
• measure reaginic antibody
• rapidly, relatively easily, and inexpensively
• syphilis screening
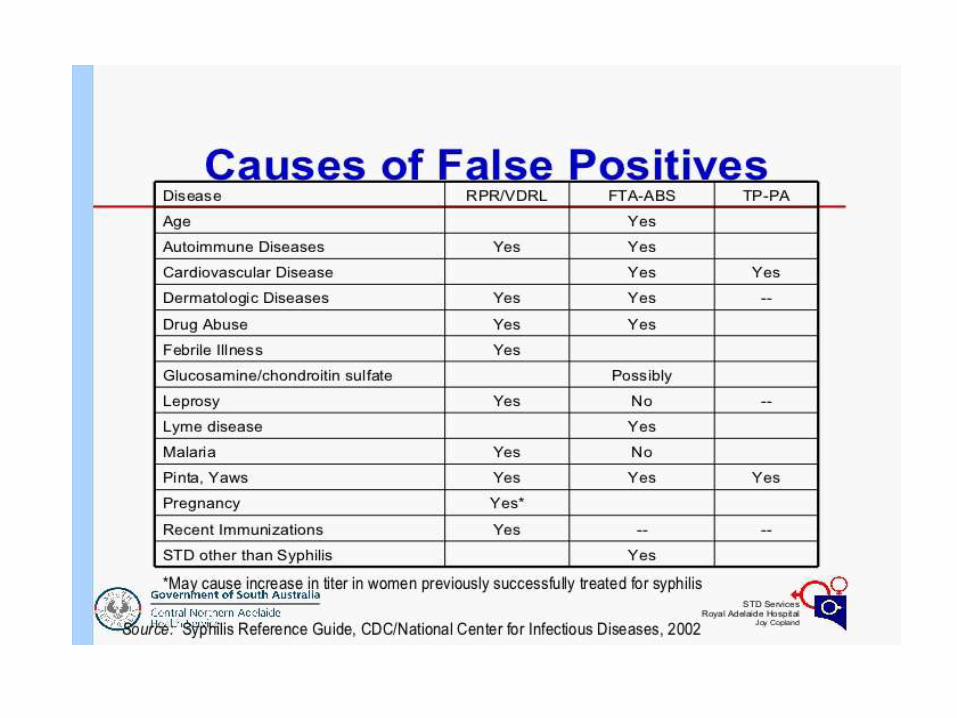
• false-positive reactions
• VDRL slide test(more specific-measure the degree of reactivity), rapid reagin test, and automated reagin

The VDRL test
• positive 3–6 weeks after infection, or 2–3 weeks after the appearance of the primary lesion;
• positive in the secondary stage
• titer is usually lower or even nil in late forms of syphilis




• a falling or stable titer in latent or late syphilis
False-positive serologic reactions • collagen diseases• infectious mononucleosis• Malaria• many febrile diseases• leprosy, vaccination• drug addiction• old age• possibly pregnancy


Treponemal Antibody Tests
• FTA-ABS test and MHA-TP
• detect antibody against Treponema spirochetes.
• Both tests are more sensitive and specific than nontreponemal tests
• except the MHA-TP test with primary disease
• remain positive despite therapy (so they are not given in titers or used to follow serologic response to treatment).