SYMMACS: Systematic monitoring of the voluntary · PDF fileKisumu, Kenya . Bailey ... Dickson,...
24
SYMMACS: Systematic Monitoring of the Voluntary Medical Male Circumcision Scale-up in Eastern and Southern Africa Jane T. Bertrand, PhD, MBA Jan. 13, 2014
Transcript of SYMMACS: Systematic monitoring of the voluntary · PDF fileKisumu, Kenya . Bailey ... Dickson,...
SYMMACS: Systematic Monitoring of the Voluntary Medical Male Circumcision Scale-up in
Eastern and Southern Africa
Jane T. Bertrand, PhD, MBA Jan. 13, 2014

Overview of presentation
• Background • Methodology • Selected results • Limitations • Dissemination
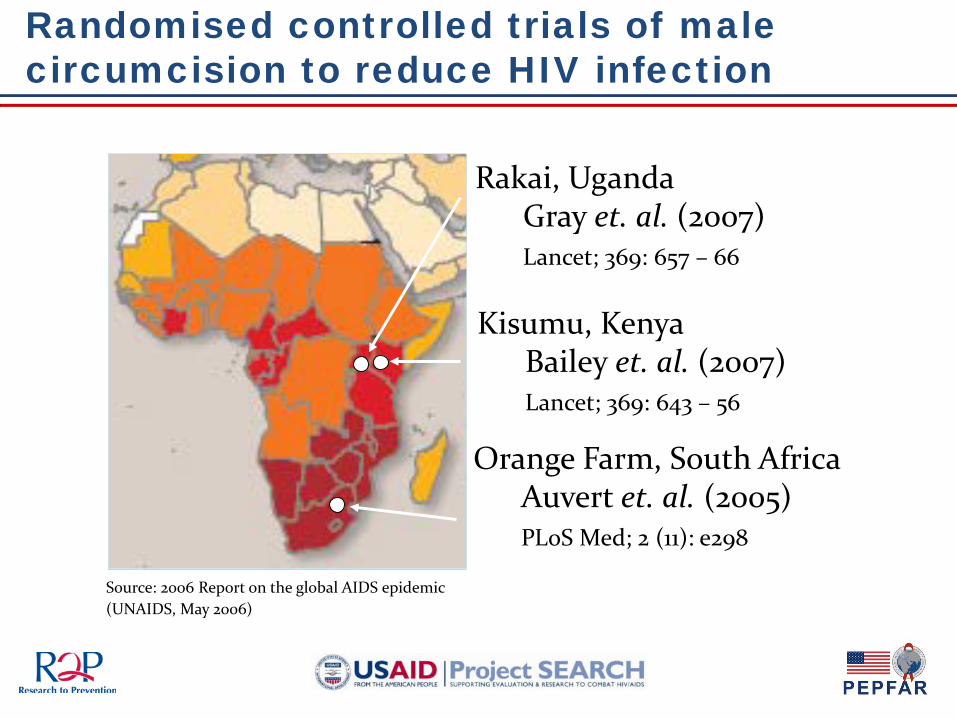
Source: 2006 Report on the global AIDS epidemic (UNAIDS, May 2006)
Rakai, Uganda Gray et. al. (2007) Lancet; 369: 657 – 66
Kisumu, Kenya Bailey et. al. (2007) Lancet; 369: 643 – 56
Orange Farm, South Africa Auvert et. al. (2005) PLoS Med; 2 (11): e298
Randomised controlled trials of male circumcision to reduce HIV infection

345,244
40,000 377,788
376,795
2,101,566
1,059,104
330,218
1,746,052
4,333,134
183,450
1,373,271
4,245,184
1,949,292 1,912,595
-
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000
4,500,000
5,000,000
Number of Adult 15-49 years male circumcision needed to reach 80% coverage in 5years
20,373,693M adult 15-49 years men to be circumcised across all 14 countries
WHO guidance (2010)
WHO convened a panel of experts to develop considerations for optimizing the volume and efficiency of VMMC services
Models for Optimizing the Volume and Efficiency of MC Services (2010)
“Considerations” to be adapted to local context Practitioners working on scale-up identified 6 elements of surgical efficiency that SYMMACS would monitor:
•Rotation among multiple bays in operating theatre •Pre-bundling of surgical supplies with disposable instruments •Task-shifting (use of non-medical providers to perform entire procedure) •Task-sharing (allowing non-medical providers to assist in certain aspects of the procedure) •Use of electrocautery/diathermy •Use of forceps-guided surgical method
6

Objectives of SYMMACS
1. Efficiency – Extent of adoption of 6 elements of efficiency – Factors that improve surgical efficiency
2. Quality – Assessment of VMMC facilities – Assessment of surgical technique during procedure – Effect of scale-up on quality of services (South Africa)
3. Provider perspectives on VMMC scale-up – Provider profile, experience, job satisfaction, burnout – Provider attitudes toward VMMC scale-up
7
SYMMACS methodology
• Process evaluation in four countries in southern and eastern Africa active in VMMC scale-up
– Kenya, South Africa, Tanzania, and Zimbabwe
• Two serial cross-sectional samples of VMMC service
delivery sites – Data collected in 2011 and 2012 using same instruments
• Included fixed, outreach and mobile sites (where they
existed) – Kenya: only country that had mobile sites
8

9
Kenya South Africa
Tanzania Zimbabwe
# sites visited 30 29
15 40
14 29
14 24
Types of sites: Fixed/outreach/ mobile
15/12/3 15/12/2
13/2/0
26/14/0
13/1/0 24/5/0
5/9/0
6/18/0
# providers interviewed
86 82
105 209
93 206
74 94
# VMMC procedures observed
151 218
120 361
133 251
140 204
Number of sites visited: 2011, 2012
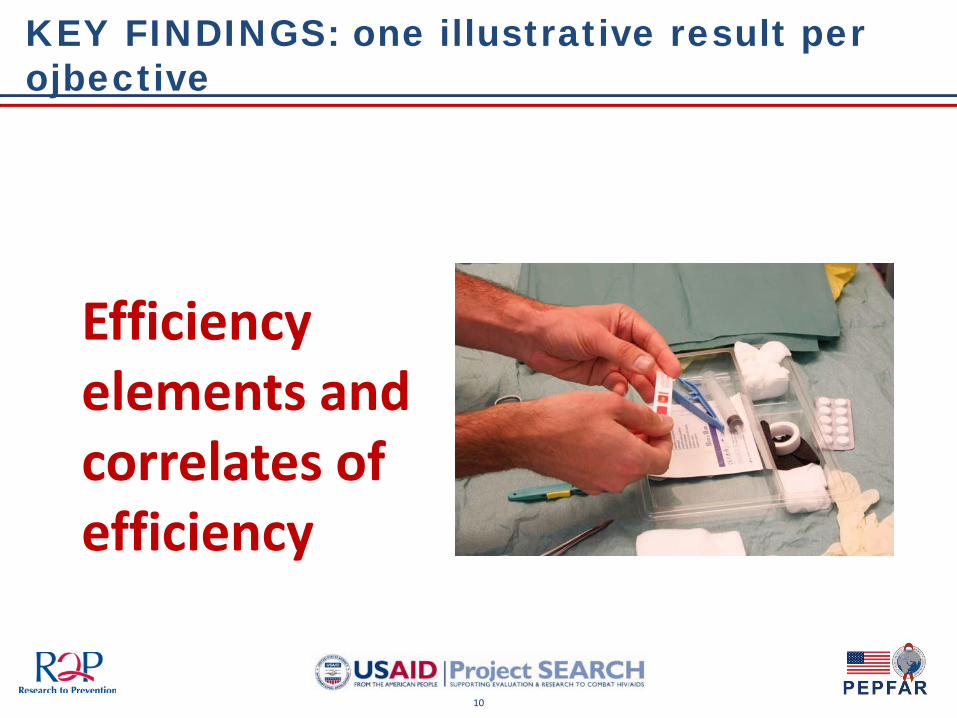
KEY FINDINGS: one illustrative result per ojbective
10
Efficiency elements and correlates of efficiency

Kenya South Africa Tanzania Zimbabwe
2011-2012 2011-2012 2011-2012 2011-2012
Multiple bays in operating theatre
X / X X / X X / X
Purchase of pre-bundled kits with disposable instruments
X / X X / X
Task-shifting X / X X / X
Task-sharing X / X X / X X / X X / X
Surgical method: forceps-guided X / X X / X X / X X / X
Electrocautery to stop bleeding X / X (x)* / X
11
* Indicates partial adoption of efficiency element
Summary of adoption of 6 efficiency elements 2011-2012

12
KEY FINDINGS
Quality of services
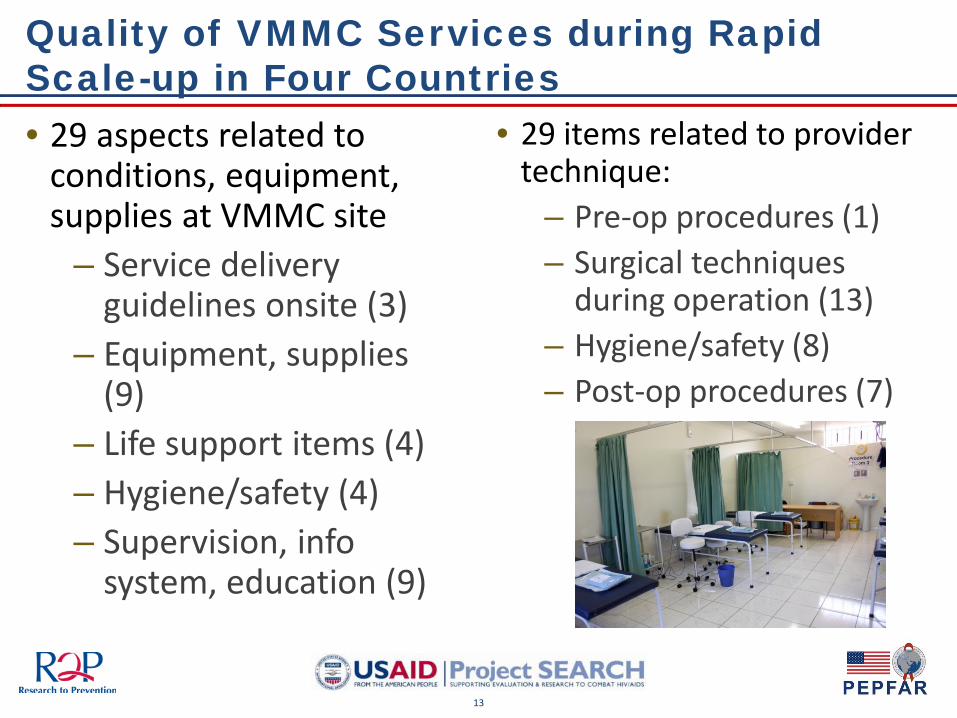
Quality of VMMC Services during Rapid Scale-up in Four Countries
13
• 29 aspects related to conditions, equipment, supplies at VMMC site
– Service delivery guidelines onsite (3)
– Equipment, supplies (9)
– Life support items (4) – Hygiene/safety (4) – Supervision, info
system, education (9)
• 29 items related to provider technique:
– Pre-op procedures (1) – Surgical techniques
during operation (13) – Hygiene/safety (8) – Post-op procedures (7)
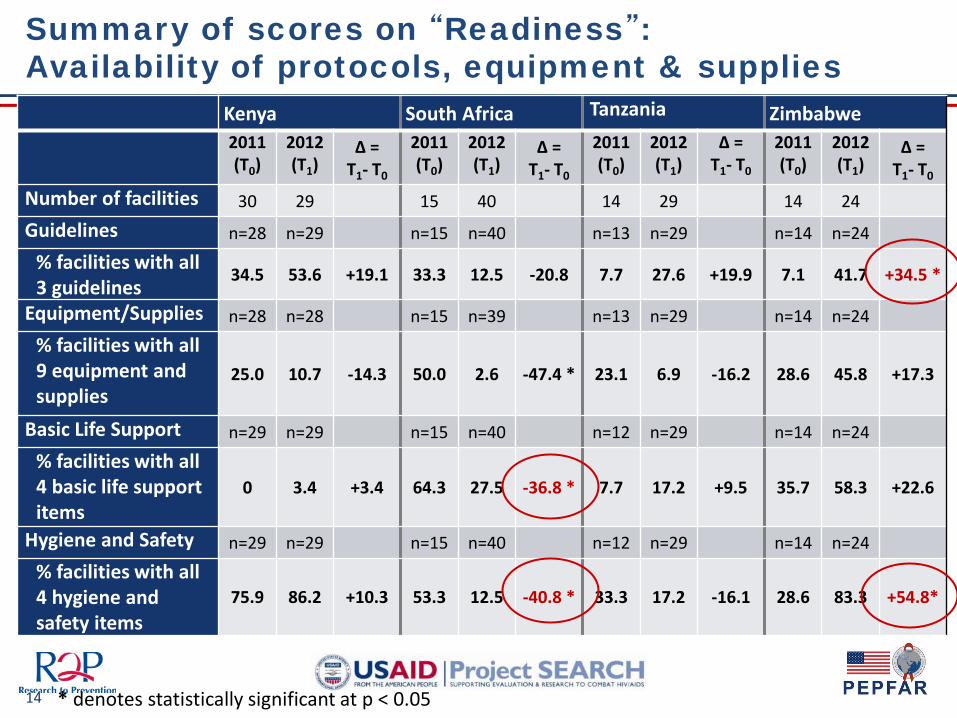
14
Kenya South Africa Tanzania Zimbabwe 2011
(T0) 2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
Number of facilities 30 29 15 40 14 29 14 24
Guidelines n=28 n=29 n=15 n=40 n=13 n=29 n=14 n=24
% facilities with all 3 guidelines
34.5 53.6 +19.1 33.3 12.5 -20.8 7.7 27.6 +19.9 7.1 41.7 +34.5 *
Equipment/Supplies n=28 n=28 n=15 n=39 n=13 n=29 n=14 n=24
% facilities with all 9 equipment and supplies
25.0 10.7 -14.3 50.0 2.6 -47.4 * 23.1 6.9 -16.2 28.6 45.8 +17.3
Basic Life Support n=29 n=29 n=15 n=40 n=12 n=29 n=14 n=24
% facilities with all 4 basic life support items
0 3.4 +3.4 64.3 27.5 -36.8 * 7.7 17.2 +9.5 35.7 58.3 +22.6
Hygiene and Safety n=29 n=29 n=15 n=40 n=12 n=29 n=14 n=24
% facilities with all 4 hygiene and safety items
75.9 86.2 +10.3 53.3 12.5 -40.8 * 33.3 17.2 -16.1 28.6 83.3 +54.8*
* denotes statistically significant at p < 0.05
Summary of scores on “Readiness”: Availability of protocols, equipment & supplies
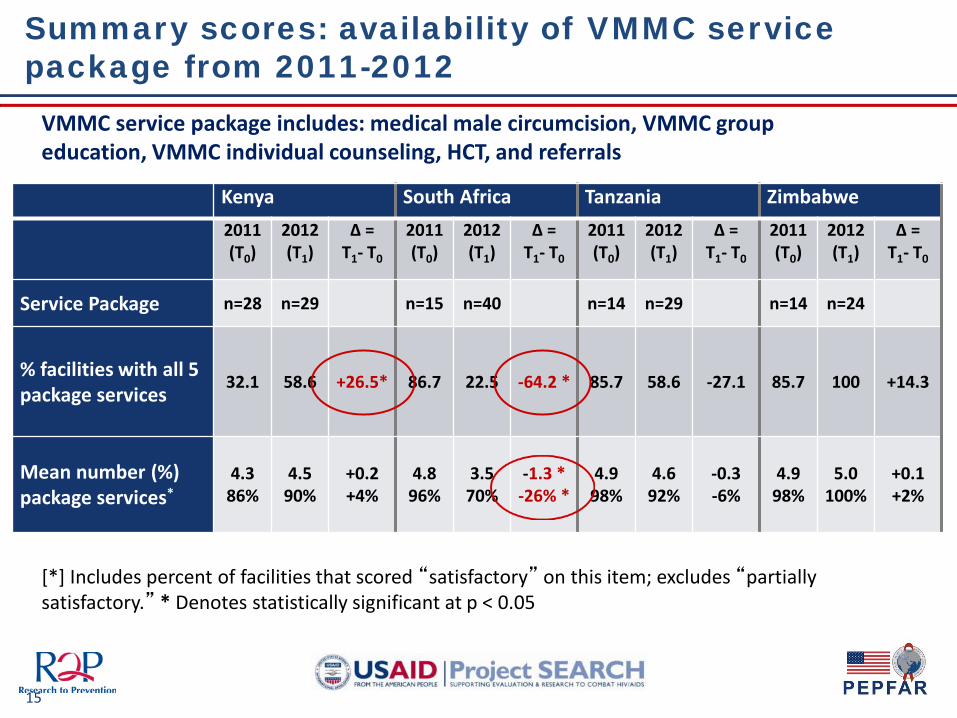
Summary scores: availability of VMMC service package from 2011-2012
15
Kenya South Africa Tanzania Zimbabwe
2011 (T0)
2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
2011 (T0)
2012 (T1)
∆ = T1- T0
Service Package n=28 n=29 n=15 n=40 n=14 n=29 n=14 n=24
% facilities with all 5 package services
32.1 58.6 +26.5* 86.7 22.5 -64.2 * 85.7 58.6 -27.1 85.7 100 +14.3
Mean number (%) package services*
4.3 86%
4.5 90%
+0.2 +4%
4.8 96%
3.5 70%
-1.3 * -26% *
4.9 98%
4.6 92%
-0.3 -6%
4.9 98%
5.0 100%
+0.1 +2%
[*] Includes percent of facilities that scored “satisfactory” on this item; excludes “partially satisfactory.” * Denotes statistically significant at p < 0.05
VMMC service package includes: medical male circumcision, VMMC group education, VMMC individual counseling, HCT, and referrals
Summary of changes – quality of services
16
Country specific QA trends (2011 versus 2012):
• South Africa: rapid expansion of sites led to decreased quality of services
• Zimbabwe showed improvement on multiple items
• Kenya and Tanzania – no significant change

17
KEY FINDINGS
Provider perspectives

Provider attitudes toward scale-up
• National policy dictates adoption (or not) of 6 elements of efficiency
• Compliance with practices and morale – related to provider attitudes toward these practices
18
• Findings: providers generally accepted the use of these 6 practices:
– Objected to lack of task shifting in South Africa and Zimbabwe
– Wanted training in methods other than forceps guided
– Wanted training in electrocautery (in Kenya – where not widespread)

KEY FINDINGS across 4 countries
Overall strengths of program • Group education on HIV prevention widely
available • Generally high marks on quality of surgical
procedure • Improvements in information systems by 2012
General areas for improvement • Inadequate recording of adverse events • Lack of emergency equipment on sites • Absence of guidelines on site
19
Limitations of the study
20
• Sampling: impossible to know the “universe” of sites at start of data collection
• Timing of data collection: did not correspond to “high volume” periods (except Zimbabwe, 2011; South Africa, 2012)
• Observations of sites and VMMC procedures were by definition subjective
– But based on pre-established written criteria
• Provider data were self reported
Dissemination of findings
• Presented at international conferences – IAS, Malaysia, 2012 – ICASA, Cape Town, 2013
• Dissemination of SYMMACS Final report
– Posted on the R2P website (www.jhsph.edu/r2p) and announced via social media
– Posted on front page of Clearinghouse on Male Circumcision for HIV Prevention (http://www.malecircumcision.org/)
• Publication of VMMC journal supplement in PLoS One – Six papers on SYMMACS, publication dates starting in December 2013
21

Acknowledgment to country teams
Kenya South Africa Tanzania Zimbabwe Implementing Agency
FHI360/Kenya CHAPS MCHIP Jhpiego/Tanzania PSI/Zimbabwe, with ZAPP-UZ as subcontractor
Co-investigator Dr. Nicholas Muraguri, Dr. Peter Cherutich, Dr. Kawango Agot, Dr. Walter Obiero, Dr. Jackson Kioko
Dr. Dirk Taljaard,
Dr. James McIntyre
Dr. Bennet Fimbo, Dr. Eleuter Samky
Dr. Karin Hatzold, Christopher Samkange
Country Coordinator
Dr. Mores Loolpapit, Mathews Onyango Sasha Frade Michael D. Machaku Webster Mavhu
Clinician (data collection)
Omondi Dickens,
Nicolas Pule
Mulashi Biola, Daniel Shabangu, Sindiswe Zwane, Sindiswe Maseko
Dr. Sifuni Koshuma, Milton Kabiligi
Dr. Tendai Mutwirah Dr. Eric Nyazika Dr. Kelvin Nemayire
Social Scientist for data collection
Rosemary Owigar, Dr. Violet Naanyu n/a n/a n/a
Data Manager Omondi Dickens Alexandra Spyrelis Flora Hezwa, Dr. Obadia Venance Nyongole Dudzai Mureyi
USAID Mission Anne Murphy Wendy Benzerga, Rebecca Fertziger
Duncan Onditi, Seth Greenberg,
Eric Mlanga
William Jansen
Technical assistance and/or sampling
Dr. Kate McIntyre, Zebedee Mwandi
Carlos Toledo, Lisa Mulwenga Koku Kasaura n/a
Manuscript review n/a n/a Hally Mahler Dr Karin Hatzold 22
Principal investigators Jane T. Bertrand (PI), Dino Rech (co-PI)
Co-investigators Emmanuel Njeuhmeli, Delivette Castor, Jason Reed
Technical Advisory Group to the R2P Project for VMMC (convened in 2010)
Bertran Auvert, Stella Babalola, Robert Bailey, Kelly Curran, Kim Eva Dickson, Timothy Farley, Ron Gray, Jason Reed, Caroline Ryan; also present from USAID: Benny Kottiri, David Stanton, Alison Cheng, Timothy Mah, Emmanuel Njeuhmeli.
USAID/Washington: Emmanuel Njeuhmeli, Delivette Castor, Alison Cheng, Benny Kottiri, Sarah Sandison, Timothy Mah
PEPFAR/CDC/Atlanta: Jason Reed (at the time of initiation of the study)
Center for Communication Programs (CCP), Johns Hopkins Bloomberg School of Public Health:
Susan Krenn, William Glass, and Mark Beisser; and from R2P staff (CCP): Deanna Kerrigan, Caitlin Kennedy, Brandon Howard, Emily Hurley, Heena Brahmbhatt, Andrea Vazzano,‘Kuor Kumoji, Erica Layer, Jessica Spielman and Margie Wild
Technical and administrative support / Tulane SPTHM
Alan Czaplicki, Bobbie Garner-Coffie, Frances Mather, Christopher Swalm.
Research support / Tulane SPTHM
Linnea Perry, Margaret Farrell, Nicholas Thomas
Acknowledgement - other collaborators
24
The USAID | Project SEARCH, Task Order No.2, is funded by the U.S. Agency for International Development under Contract No. GHH-I-00-07-00032-00, beginning September 30, 2008, and supported by the President’s Emergency Plan for AIDS Relief. The Research to Prevention (R2P) Project is led by the Johns Hopkins Center for Global Health and managed by the Johns Hopkins Bloomberg School of Public Health Center for Communication Programs (CCP).