SYB Case 2
19
SYB Case 2 By: Amy
-
Upload
jermaine-huffman -
Category
Documents
-
view
50 -
download
0
description
SYB Case 2. By: Amy. History. 63 y/o female History of left breast infiltrating duct carcinoma s/p mastectom y in 1996 and chemotherapy ER negative, PR negative, HER-2/Neu negative. - PowerPoint PPT Presentation
Transcript of SYB Case 2
SYB Case 2
By: Amy
History
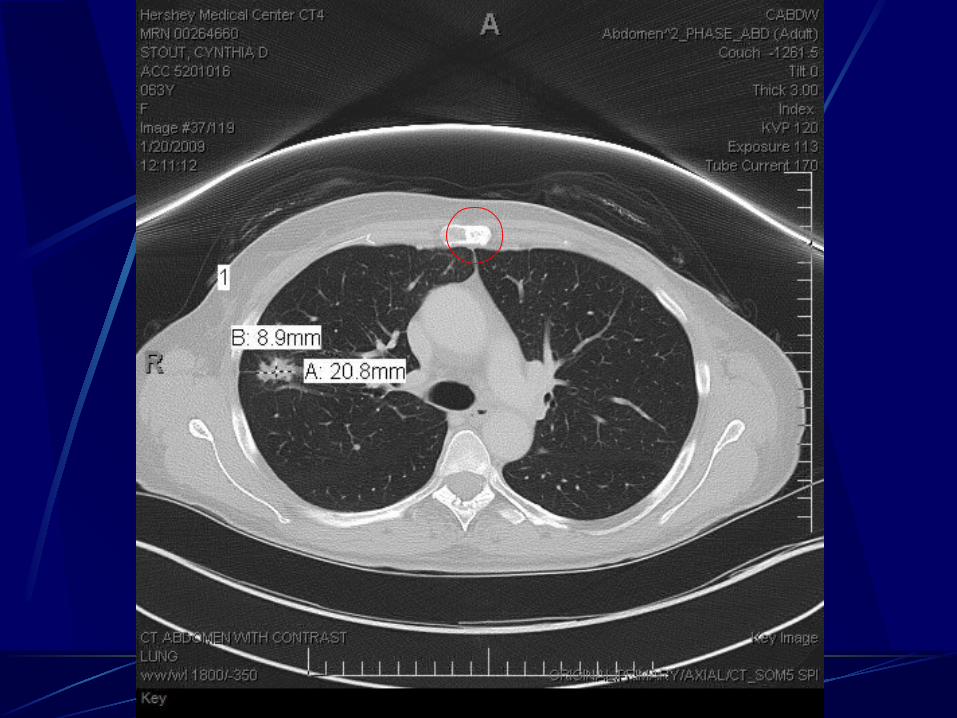
63 y/o female
History of left breast infiltrating duct carcinoma s/p mastectomy in 1996 and chemotherapyER negative, PR negative,
HER-2/Neu negative
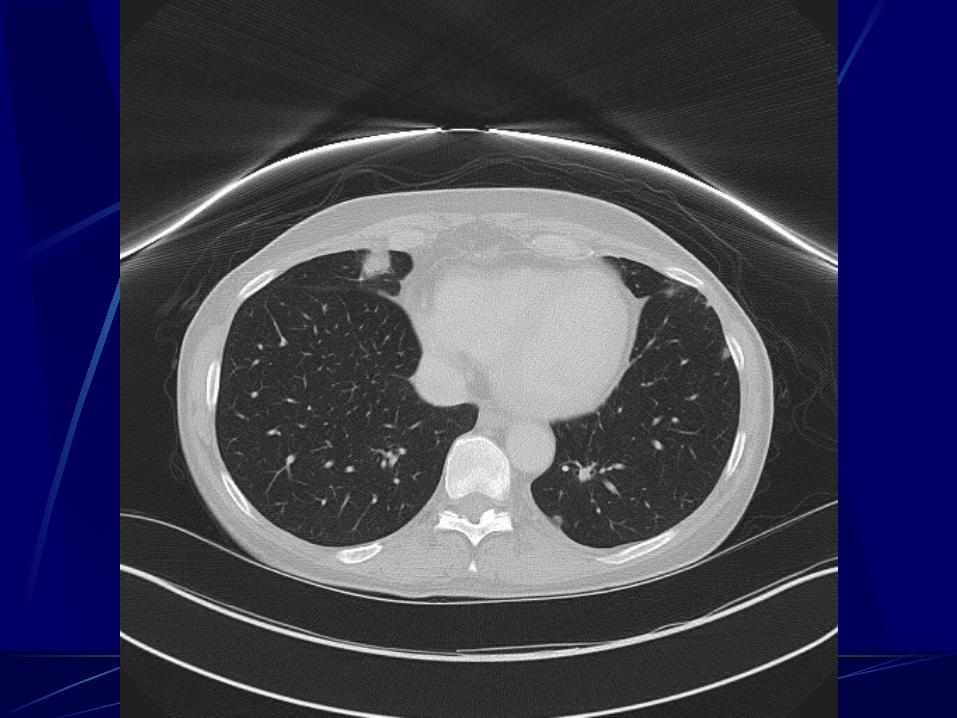
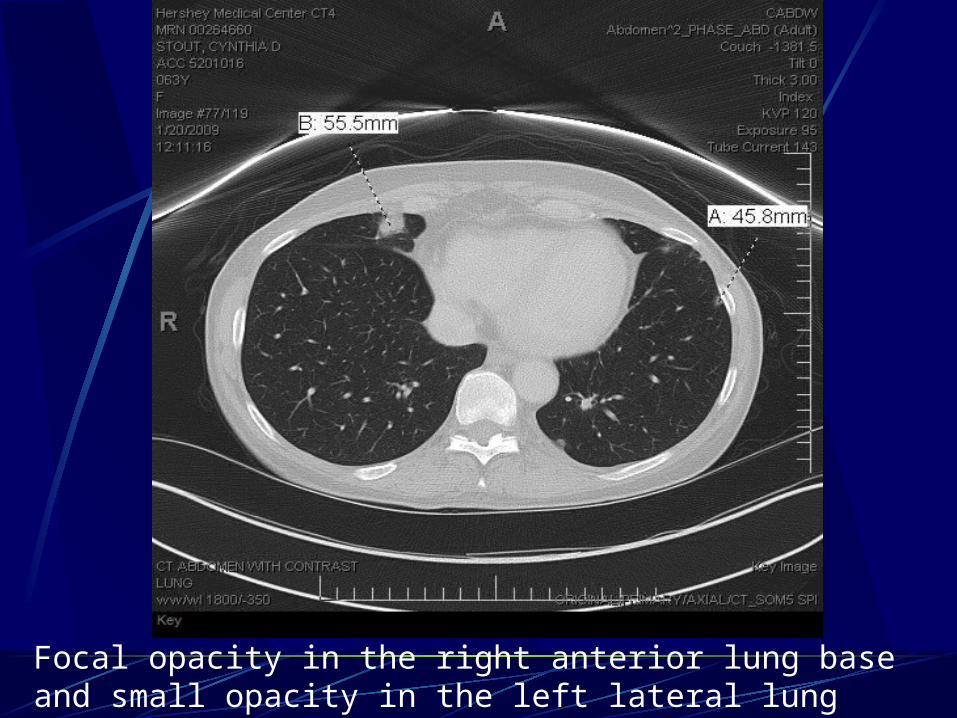
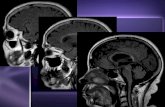
Focal opacity in the right anterior lung base and small opacity in the left lateral lung base - likely atelectasis but cannot r/o metastases
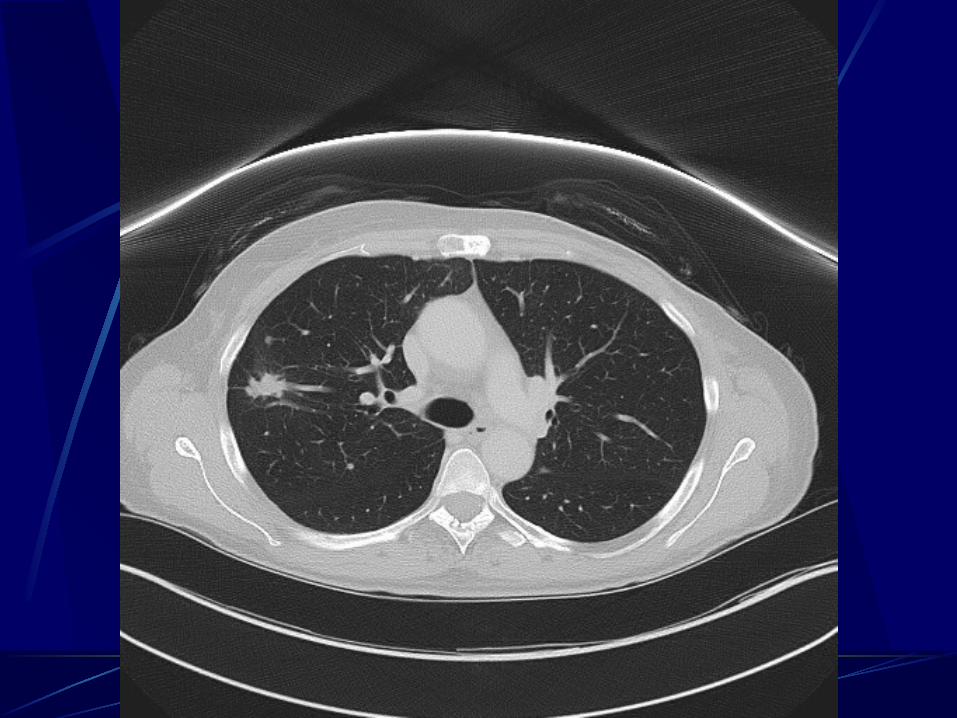
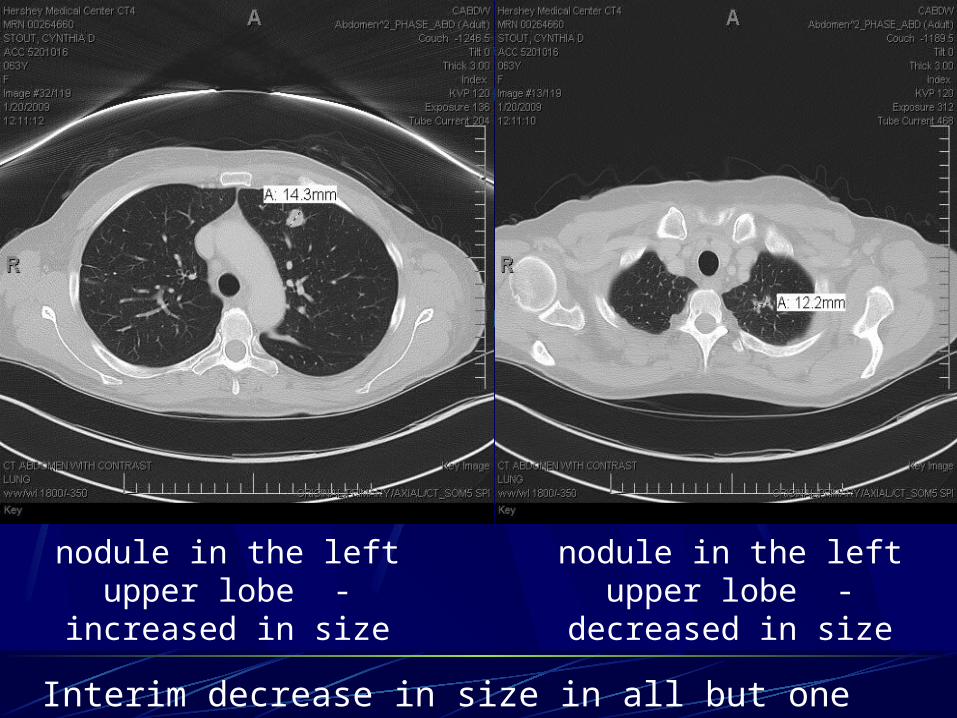
nodule in the left upper lobe - increased in size
Interim decrease in size in all but one metastatic lung nodules.
nodule in the left upper lobe - decreased in size
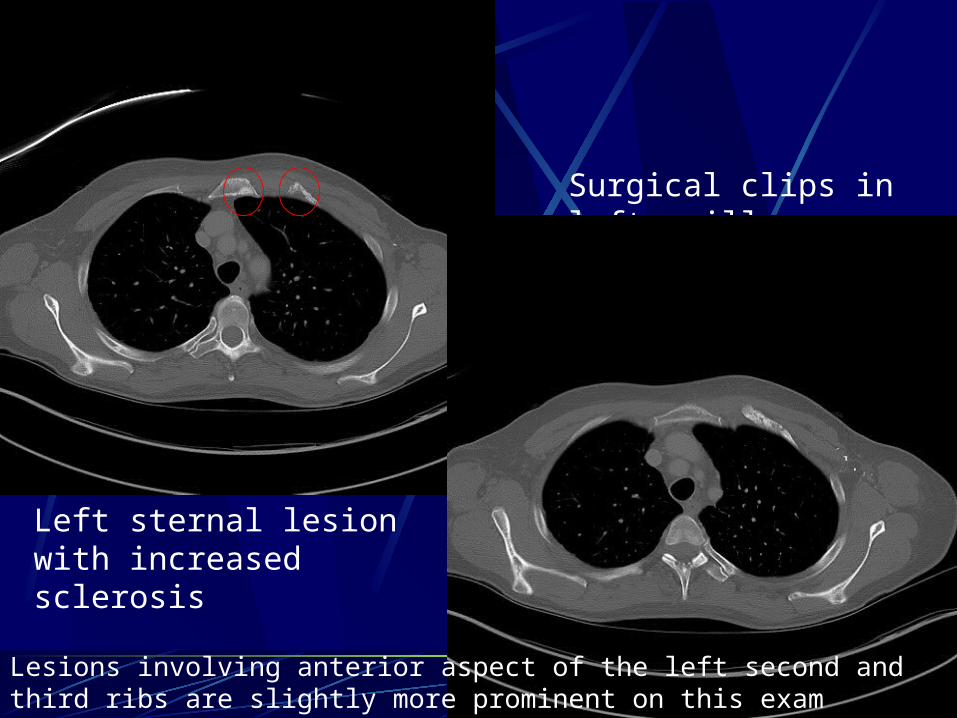
Left sternal lesion with increased sclerosis
Surgical clips in left axilla
Lesions involving anterior aspect of the left second and third ribs are slightly more prominent on this exam

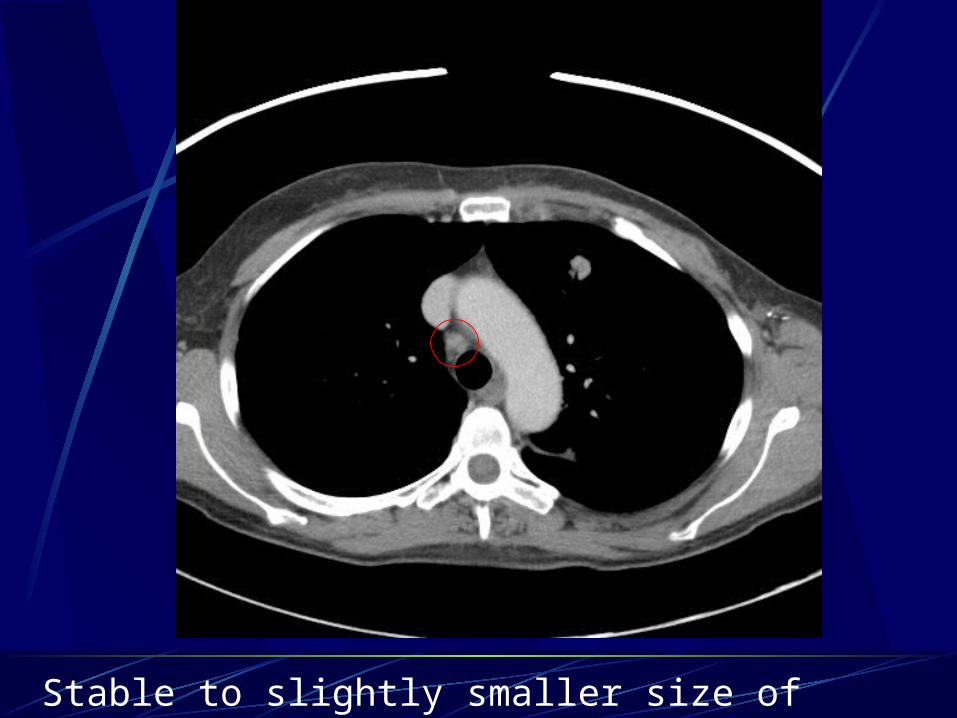
Stable to slightly smaller size of mediastinal lymph node
Breast Cancer
Most common female cancer in the U.S. Infiltrating ductal – most common type (70-
80%)
Second most common cause of cancer death in women
Main cause of death in women ages 45-55
Most common sites of metastasis
Bone – most common, particularly the spine, ribs, pelvis, proximal long bones, and skull
Liver
Lungs
Brain
Subcutaneous tissues
TNM Breast Cancer Staging
Primary tumor (T) TX — Primary tumor cannot be assessedT0 — No evidence of primary tumorTis — Carcinoma in situT1 — Tumor 2 cm or less in greatest dimensionT2 — Tumor more than 2 cm but not more than 5 cm in greatest dimensionT3 — Tumor more than 5 cm in greatest dimensionT4 — Tumor of any size with direct extension to (a) chest wall, (b) skin, (c) both chest wall and skin, or (d) inflammatory carcinoma
Regional lymph nodes (N): Clinical classification
NX — Regional lymph nodes cannot be assessed (eg, previously removed)N0 — No regional lymph node metastasesN1 — Metastasis to movable ipsilateral axillary lymph nodesN2 — Metastasis to ipsilateral axillary lymph nodes, or in clinically apparent ipsilateral internal mammary nodes in the absence of evident axillary node metastasesN3 — Metastasis to ipsilateral infraclavicular lymph nodes with or without clinically evident axillary lymph nodes, or in clinically apparent ipsilateral internal mammary lymph node(s) and in the presence of clinically evident axillary lymph node metastases, or metastasis in ipsilateral supraclavicular lymph nodes with or without axillary or internal mammary nodal involvement
TNM Staging contd.Regional lymph nodes: Pathologic classification (pN) - Classification is based
upon axillary lymph node dissection +/- sentinel lymph node dissection. pNX — Regional lymph nodes cannot be assessed (eg, previously removed, or not removed)pN0 — No regional lymph node metastasis; no additional examination for isolated tumor cells (i.e. single tumor cells or small clusters not greater than 0.2 mm, usually detected only by immunohistochemical or molecular methods but which may be verified on hematoxylin and eosin stains)pN1 — Metastasis in 1 - 3 ipsilateral axillary lymph nodes and/or in internal mammary nodes with microscopic disease detected by sentinal lymph node dissection but not clinically apparentpN2 — Metastasis in 4 - 9 axillary lymph nodes or in clinically apparent internal mammary lymph nodes in the absence of axillary lymph nodespN3 — Metastasis in 10 or more axillary lymph nodes, or in infraclavicular lymph nodes, or in clinically apparent ipsilateral internal mammary lymph nodes in the presence of one or more positive axillary nodes; or in more than three axillary lymph nodes with clinically negative microscopic metastasis in internal mammary lymph nodes; or in ipsilateral supraclavicular lymph nodes
Distant metastasis (M)
MX — Distant metastasis cannot be assessedM0 — No distant metastasisM1 — Distant metastasis
Stage Groupings by TNM Classification
Stage 0 — Tis N0 M0
Stage I — T1 N0 M0 (including T1mic)
Stage IIA — T0 N1 M0; T1 N1 M0; T2 N0 M0
Stage IIB — T2 N1 M0; T3 N0 M0
Stage IIIA — T0 N2 M0; T1 N2 M0; T2 N2 M0; T3 N1 M0; T3 N2 M0
Stage IIIB — T4 Any N M0
Stage IIIC — Any T N3 M0
Stage IV — Any T Any N M1
Metastatic work-up
Physical Exam - skin, breasts, lymph nodes, and abdomenDiagnostic bilateral mammography (+/- ultrasound)Blood tests – CBC, LFT’sChest imaging CT scanning of the liver and pelvis and radionuclide bone scans
have a low diagnostic yield in women with early stage (TI-II; N0-I) breast cancer and are not routinely necessary
Chest CT is performed for radiation planning in women, but is not necessary for routine staging of the thorax in women with early stage disease
Staging CT of the abdomen and pelvis and a radionuclide bone scan is more likely to influence therapy in patients with stage III disease and are therefore recommended in these patients
Management of Metastatic Breast Cancer
Relapses are most common in the initial 5 years after treatment for early stage disease, but can occur up to 30 years later Prognostic factors include the interval between initial therapy and
relapse, number of metastatic sites, presence/absence of visceral involvement, age and stage at diagnosis, and hormone receptor status
Patients with metastases are unlikely to be cured of their disease by any means Complete remissions from chemo are uncommon Serial plain radiographs, CT scans, or MRI allow assessment of
tumor response Plain radiographs showing sclerosis of previously lytic lesions is
highly indicative of response, while enlargement of the lytic area suggests progression
In pts with mainly sclerotic lesions, serial plain films are less helpful because the healing cannot be observed
References
UpToDate; all accessed 1/25/09 Hirsch, A., et al. Management of locoregional recurrence
of breast cancer after breast conserving therapy. Bleiweiss, I. Pathology of breast cancer: The invasive
carcinomas. Esserman, L., and Joe, B. Diagnostic evaluation and
initial staging work-up of women with suspected breast cancer.
Hurria, A., and Come, S. Follow-up for breast cancer survivors: Recommendations for surveillance after therapy.
Hayes, D. General principles of management of metastatic breast cancer.