Survival Outcomes Following Liver Transplantation (SOFT) Score: A Novel Method to Predict Patient...
10
American Journal of Transplantation 2008; 8: 2537–2546 Wiley Periodicals Inc. C 2008 The Authors Journal compilation C 2008 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2008.02400.x Survival Outcomes Following Liver Transplantation (SOFT) Score: A Novel Method to Predict Patient Survival Following Liver Transplantation A. Rana ∗ , M. A. Hardy, K. J. Halazun, D. C. Woodland, L. E. Ratner, B. Samstein, J. V. Guarrera, R. S. Brown Jr. and J. C. Emond Division of Abdominal Organ Transplantation, Columbia University College of Physicians and Surgeons, New York, NY ∗ Corresponding author: Abbas Rana, [email protected] It is critical to balance waitlist mortality against post- transplant mortality. Our objective was to devise a scoring system that predicts recipient survival at 3 months following liver transplantation to complement MELD-predicted wait- list mortality. Univariate and multivariate analysis on 21673 liver transplant recipients identified independent recipient and donor risk factors for posttransplant mortality. A retrospective analysis conducted on 30321 waitlisted candidates reevaluated the predictive ability of the Model for End-Stage Liver Disease (MELD) score. We identified 13 recipient factors, 4 donor factors and 2 operative factors (warm and cold ischemia) as signif- icant predictors of recipient mortality following liver transplantation at 3 months. The Survival Outcomes Following Liver Transplant (SOFT) Score utilized 18 risk factors (excluding warm ischemia) to successfully pre- dict 3-month recipient survival following liver trans- plantation. This analysis represents a study of waitlisted candi- dates and transplant recipients of liver allografts after the MELD score was implemented. Unlike MELD, the SOFT score can accurately predict 3-month survival fol- lowing liver transplantation. The most significant risk factors were previous transplantation and life support pretransplant. The SOFT score can help clinicians de- termine in real time which candidates should be trans- planted with which allografts. Combined with MELD, SOFT can better quantify survival benefit for individual transplant procedures. Key words: Liver transplantation, SOFT score, sur- vival outcomes following liver transplantation, post- transplant mortality, risk factors for post-transplant mortality, donor and recipient risk factors for death after liver transplant Received 14 April 2008, revised 30 June 2008 and accepted for publication 30 July 2008 Introduction The MELD (Model for End-Stage Liver Disease) scoring system (1,2) has transformed liver allograft allocation in the United States since it was implemented for prioritiza- tion of transplant candidates in 2002 (3). The MELD score is an accurate predictor of waitlist mortality, as demon- strated in the pioneering study by Wiesner et al. (4), with a c-statistic (5) of 0.83 when used to predict 3-month mor- tality of candidates on the waitlist. The score substituted effectively for candidate stratification based on subjective assessment. However, the MELD score is a poor predic- tor of mortality following transplantation (4,6,7). This ob- servation was confirmed by Desai et al. in their analysis, which reports a c-statistic of only 0.54 with the use of the MELD to predict 3-month recipient mortality following liver transplantation (7). When mortality of recipients on the waitlist is compared with the highest and the lowest MELD scores, there is a 300-fold difference, in contrast to the 2-fold difference in survival of patients after liver trans- plantation (8). Methods other than the MELD score, such as the Child–Pugh score, also had a poor ability to predict posttransplant survival (6). The inability of existing methods to predict posttransplant survival prevents clinicians from effectively selecting potential recipients for transplantation from MELD scores alone. Because candidate factors alone are not predictive of sur- vival following transplantation, a new model is required to accurately predict posttransplant survival. The lack of con- sideration of donor risk factors is one limitation of the exist- ing standard (transplanting patients with a MELD greater than 15) (8). Recently, the donor risk index (DRI) has been proposed as a method to stratify outcomes associated with graft selection (9). However, the lack of contribution from recipient factors gives the DRI alone a poor predictive value (c-statistic 0.53 based on its application to the United Net- work for Organ Sharing [UNOS] database). In the present analysis, we combined both donor and recipient risk fac- tors in constructing the Survival Outcomes Following Liver 2537
Transcript of Survival Outcomes Following Liver Transplantation (SOFT) Score: A Novel Method to Predict Patient...

American Journal of Transplantation 2008; 8: 2537–2546Wiley Periodicals Inc.
C© 2008 The AuthorsJournal compilation C© 2008 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2008.02400.x
Survival Outcomes Following Liver Transplantation(SOFT) Score: A Novel Method to Predict PatientSurvival Following Liver Transplantation
A. Rana∗, M. A. Hardy, K. J. Halazun, D. C.
Woodland, L. E. Ratner, B. Samstein, J. V.
Guarrera, R. S. Brown Jr. and J. C. Emond
Division of Abdominal Organ Transplantation, ColumbiaUniversity College of Physicians and Surgeons, New York,NY∗Corresponding author: Abbas Rana,[email protected]
It is critical to balance waitlist mortality against post-transplant mortality.
Our objective was to devise a scoring system thatpredicts recipient survival at 3 months following livertransplantation to complement MELD-predicted wait-list mortality.
Univariate and multivariate analysis on 21 673 livertransplant recipients identified independent recipientand donor risk factors for posttransplant mortality. Aretrospective analysis conducted on 30 321 waitlistedcandidates reevaluated the predictive ability of theModel for End-Stage Liver Disease (MELD) score.
We identified 13 recipient factors, 4 donor factors and2 operative factors (warm and cold ischemia) as signif-icant predictors of recipient mortality following livertransplantation at 3 months. The Survival OutcomesFollowing Liver Transplant (SOFT) Score utilized 18 riskfactors (excluding warm ischemia) to successfully pre-dict 3-month recipient survival following liver trans-plantation.
This analysis represents a study of waitlisted candi-dates and transplant recipients of liver allografts afterthe MELD score was implemented. Unlike MELD, theSOFT score can accurately predict 3-month survival fol-lowing liver transplantation. The most significant riskfactors were previous transplantation and life supportpretransplant. The SOFT score can help clinicians de-termine in real time which candidates should be trans-planted with which allografts. Combined with MELD,SOFT can better quantify survival benefit for individualtransplant procedures.
Key words: Liver transplantation, SOFT score, sur-vival outcomes following liver transplantation, post-transplant mortality, risk factors for post-transplant
mortality, donor and recipient risk factors for deathafter liver transplant
Received 14 April 2008, revised 30 June 2008 andaccepted for publication 30 July 2008
Introduction
The MELD (Model for End-Stage Liver Disease) scoringsystem (1,2) has transformed liver allograft allocation inthe United States since it was implemented for prioritiza-tion of transplant candidates in 2002 (3). The MELD scoreis an accurate predictor of waitlist mortality, as demon-strated in the pioneering study by Wiesner et al. (4), witha c-statistic (5) of 0.83 when used to predict 3-month mor-tality of candidates on the waitlist. The score substitutedeffectively for candidate stratification based on subjectiveassessment. However, the MELD score is a poor predic-tor of mortality following transplantation (4,6,7). This ob-servation was confirmed by Desai et al. in their analysis,which reports a c-statistic of only 0.54 with the use ofthe MELD to predict 3-month recipient mortality followingliver transplantation (7). When mortality of recipients onthe waitlist is compared with the highest and the lowestMELD scores, there is a 300-fold difference, in contrast tothe 2-fold difference in survival of patients after liver trans-plantation (8). Methods other than the MELD score, suchas the Child–Pugh score, also had a poor ability to predictposttransplant survival (6). The inability of existing methodsto predict posttransplant survival prevents clinicians fromeffectively selecting potential recipients for transplantationfrom MELD scores alone.
Because candidate factors alone are not predictive of sur-vival following transplantation, a new model is required toaccurately predict posttransplant survival. The lack of con-sideration of donor risk factors is one limitation of the exist-ing standard (transplanting patients with a MELD greaterthan 15) (8). Recently, the donor risk index (DRI) has beenproposed as a method to stratify outcomes associated withgraft selection (9). However, the lack of contribution fromrecipient factors gives the DRI alone a poor predictive value(c-statistic 0.53 based on its application to the United Net-work for Organ Sharing [UNOS] database). In the presentanalysis, we combined both donor and recipient risk fac-tors in constructing the Survival Outcomes Following Liver
2537

Rana et al.
Transplantation (SOFT) score to accurately predict recipientposttransplant survival at 3 months. This score would thenallow clinicians to balance waitlist mortality at 3 monthsas predicted by the MELD score against 3-month mortal-ity following liver transplantation as predicted by the SOFTscore to determine which candidates should undergo livertransplantation. Since MELD has been proven to be an ac-curate predictor of 3-month waitlist mortality (4), we con-structed the SOFT score to complement the MELD scoreby predicting 3-month posttransplant mortality. The SOFTscore along with the MELD score allows clinicians to makea real-time go or no-go decision on a particular allograft.
The SOFT score can also be used to avoid wasteful trans-plants where predicted survival is below acceptable stan-dards. Furthermore, as the critical liver allograft short-age fuels more aggressive practices to utilize increasinglymarginal donor allografts, the SOFT score can establishrisk limits for particular liver transplant candidates.
Methods
Study population
We performed a retrospective analysis of UNOS deidentified patient-leveldata of all recipients of liver transplantation between March 1, 2002, thedate of implementation of the MELD prioritization system, and August 1,2006. Our analysis employed the liver registry with data collected by the Or-gan Procurement and Transplantation Network. We included all transplantrecipients aged 18 years or older. Donor and recipient characteristics werereported at the time of transplant. Follow-up information was collected at6 months and then yearly after transplantation. Patients undergoing com-bined or multivisceral transplants (n = 1402) and recipients of a live-donortransplant (n = 1163) were excluded from the study. All patients were fol-lowed from the date of transplant until either death (n = 6004) or the dateof last known follow-up (n = 15 669); we analyzed 21 673 recipients.
We performed a retrospective analysis of waitlisted candidates to deter-mine their mortality rate at 3 months and to reassess the predictive valueof the MELD score. We excluded patients under the age of 18 years (n =2383). The analysis included patients with an initial date of registrationbetween March 1, 2002 and August 1, 2006. Patients who were trans-planted within 3 months upon registering on the waitlist were excluded (n =14 721). This exclusion was only used for our waitlist mortality analysis,since we needed 90 days at-risk to determine 3-month waitlist mortality.This was not an exclusion used in our analysis of posttransplant survival.The final analysis included 30 321 waitlisted candidates.
Statistical analysis
Data were analyzed using a standard statistical software package, Stata R©9 (Stata Corp, College Station, TX). Continuous variables were reported asa mean ± standard deviation and compared using the Student’s t-test. Con-tingency table analysis was used to compare categorical variables. Resultswere considered significant at a p-value of <0.05. All reported p-valueswere two-sided. The primary outcome measure was patient death. Time todeath was assessed as time from the date of transplantation to the date ofdeath. Kaplan–Meier analysis with log-rank test and logistic regression wereused for time-to-event analysis. Three-month survival was the dependentvariable and the risk factors were the independent variables in the logis-tic regression analysis. Patients lost to follow-up (n = 573) or alive (n =15 669) on October 7, 2007 were censored at the date of last knownfollow-up.
Risk factors
The recipient and donor risk factors considered in this analysis are listedin Table 1. The characteristics that were present in the plurality of trans-plants were used as the reference groups. Serum creatinine was utilizedinstead of calculated creatinine clearance because serum creatinine is read-ily accessible for rapid assessment of donor allograft quality. This analysisonly included recipients who were transplanted after the MELD scoringsystem was instituted for liver allocation in 2002, resulting in high entrycompletion (99.9%). Since MELD scores were analyzed as a recipient riskfactor, recipient creatinine, bilirubin and international normalized ratio (INR)were not included as individual predictors. Separately, the components ofthe MELD score were each significant predictors of 3-month posttrans-plant mortality: total recipient bilirubin ≥ 8 mg/dL (OR 1.2), INR ≥ 2.5 (OR1.2), creatinine between 1.5 and 2.0 mg/dL (OR 1.3) and creatinine ≥ 2.0mg/dL (OR 1.5). Patients with malignancy were known to have cancerprior to transplantation and did not reflect incidentally discovered cancer attransplantation.
Risk score
Logistic regression analysis determined the predictors of patient death at3 months posttransplantation. Donor and recipient variables were first an-alyzed with univariate analysis and are listed in Table 1. Variables foundto be significant in univariate analysis were then subjected to multivari-ate analysis. Points were assigned to each risk factor based on its oddsratio for patient death at 3 months. One point was awarded to each riskfactor for every 10% increase in risk for death at 3 months. Negativepoints were also awarded for every 10% decrease in risk for death at3 months.
We assigned four risk groups based on MELD-predicted 3-month waitlistmortality. We formulated two distinct scores: the preallocation score to pre-dict survival outcomes following liver transplantation (P-SOFT) designed toevaluate patients on the waitlist and the score to predict survival outcomesfollowing liver transplantation (SOFT) that includes both donor and recip-ient factors to evaluate transplants at the time of transplantation. Modeldiscrimination was assessed using the area under the receiver operatingcharacteristic (ROC) curve.
Results
Study population
The study population included 21 673 patients. Analysisincluded 41 504 years-at-risk for the liver transplant recip-ients. Mean graft survival was 4.2 years. Mean follow-upwas 2.0 years. Demographic and clinical characteristics aresummarized in Table 2.
Data entry rate
The data entry completion for variables that were signifi-cant in univariate analysis is listed in Table 3. A majority ofvariables are well populated. Exceptions include hepatitisC Virus (HCV, 87.1%), cold ischemia time (86.8%), warmischemia time (75.7%) and portal bleed 48 h pretrans-plant (50.7%). Recipients with missing entries were notdropped, but rather, added to the reference group underthe assumption that the missing reports were randomlydistributed. Given the large number of risk factors ana-lyzed, this was necessary to preserve the total number ofpatients studied.
2538 American Journal of Transplantation 2008; 8: 2537–2546

Survival Outcomes Following Liver Transplant Score
Table 1: Risk factors considered in univariate and multivariate analysis
Donor risk factors Recipient risk factors
Deceased donor after cardiac death∗ ABO incompatible transplant∗Age 0–10 years∗ Diagnosis—acute hepatic necrosis∗Age 10–20 years∗ Diagnosis—cholestatic liver disease∗Age 20–30 years∗ Diagnosis—metabolic liver disease∗Age 45–55 years∗ Diagnosis—malignancy∗Age 55–60 years∗ Diagnosis—other∗Age 60–70 years∗ Portal vein thrombosis at transplant∗Age > 70 years∗ Age 18–30∗Regional allocation∗ Age 30–40∗National allocation∗ Age 60–70∗Race—Asian∗ Age > 70∗Race—African American∗ Ascites pretransplant∗Race—Latino∗ Diabetes mellitus∗Race—multiracial, other∗ Height > 75th%tile∗Weight (>75th%tile)∗ Height < 25th%tile∗Weight (<25th%tile)∗ Female ∗Cause of death CNS tumor∗ Incidental tumor found at transplant∗Cause of death anoxia∗ Intensive care unit pretransplant∗Cause of death cerebral vascular accident∗ Admitted to hospital pretransplant∗Cause of death other∗ Life support pretransplant∗Cold ischemia time 0–6 h∗ Previous abdominal surgery∗Cold ischemia time 12–16 h∗ Race—Asian∗Cold ischemia time 16–20 h∗ Race—African American∗Cold ischemia time >20 h∗ Race—Latino∗Partial or split liver∗ Race—multiracial, other∗Female Body mass index 30–35Creatinine > 1.5 mg/dL Body mass index > 35Creatinine > 2.0 mg/dL Hepatitis B (core Ab positive)Height (>75th%tile) Hepatitis C (positive serology)Height (<25th%tile) One previous transplantResuscitation following cardiac arrest Two previous transplantsAST or SGOT < 90 IU/L History of angina or coronary artery diseaseAST or SGOT > 140 IU/L HypertensionALT or SGPT < 60 IU/L ALT or SGPT > 100 IU/LALT or SGPT > 100 IU/L Albumin 2.0–2.5 g/dLDiabetes mellitus (type unspecified) Albumin < 2.0 g/dLInsulin-dependent diabetes mellitus Dialysis prior to transplantationHypertension—less than 10 yr duration UNOS status 1Hypertension—greater than 10 yr duration MELD score < 9History of alcohol dependency MELD score 10–19History of cigarette use > 20 pack years MELD score 20–29History of cocaine use in the past MELD score 30–39History of IV drug use MELD score > 40Tattoos Encephalopathy at transplantHepatitis B (core Ab positive) 1–2 yr on waitlistHepatitis C (positive serology) >2 yr on waitlistTotal bilirubin 1–1.8 mg/dL Transplant performed between 4-1-1994 to 1-1998Total bilirubin > 1.8 mg/dL Transplant performed between 1-1-1998 to 1-1-2002
Ventilator-dependent pretransplantDeceased donor—three or more inotropic agents Hx of peripheral vascular diseaseWarm ischemia time ≤30 min Hx of COPDWarm ischemia time 60–70 min Portal bleed 48 h pretransplantWarm ischemia time 70–80 min Any previous malignancyWarm ischemia time 80–90 min Variceal bleeding within 2 weeks of registrationWarm ischemia time >90 min Spontaneous bacterial peritonitis pretransplant
Pulmonary embolus within 6 months of registrationTIPS at transplant
CVA = cerebrovascular accident; AST = aspartate aminotransferase; SGOT = serum glutamic-oxaloacetic transaminase; ALT = alanineaminotransferase; SGPT = serum glutamate-pyruvate transaminase; UNOS = United Network of Organ Sharing; TIPS = transjugularintrahepatic portosytemic shunts; COPD = chronic obstructive pulmonary disease.∗Covariates from the SRTR 1-year patient survival model.
American Journal of Transplantation 2008; 8: 2537–2546 2539

Rana et al.
Table 2: Demographic characteristics of donors and recipients
Recipient Donor
Age (years) 52.0 ± 10.2 41.1 ± 17.6% Female 32.3% 40.9%% African American 8.8% 14.1%Height (cm) 172.4 ± 10.6 171.7 ± 11.0Weight (kg) 83.2 ± 19.5 77.9 ± 19.1INR 1.9 ± 1.8 NACreatinine (mg/dL) 1.4 ± 1.1 1.4 ± 1.5MELD 20.6 ± 9.6 NACause of liver failure
• Acute hepatic necrosis 7.00% NA• Cholestatic liver disease 9.20% NA• Metabolic liver disease 2.80% NA• Malignancy 10.70% NA• Hepatitis C 38.00% NA• Hepatitis B 18.90% NA• Alcoholic cirrhosis 17.90% NA
Cold ischemia time (hours) NA 7.7 ± 3.6Cause of death
• CVA NA 44.6%• Trauma NA 40.5%
NA = not applicable to this group of patients; CVA = cerebrovas-cular accident.
Univariate and multivariate analysis
Table 1 lists all of the risk factors that were considered. Riskfactors that were significant in univariate analysis werethen subjected to multivariate analysis. The significant riskfactors in multivariate analysis are presented in Table 3.The most significant risk factors were two previous trans-plants (OR 2.4, confidence interval (CI) 1.52–3.67), warmischemia time > 90 min (OR 2.3, CI 1.58–3.41), one previ-ous transplant (OR 1.9, CI 1.56–2.24), life support (OR 1.9,CI 1.54–2.35) and warm ischemia time 80–90 min (OR 1.8,CI 1.10–3.00).
Risk score
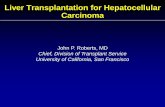
Table 3 summarizes donor and recipient risk factors andtheir assigned points. Table 4 presents two different riskscores: the preallocation score to predict survival out-comes following liver transplantation (P-SOFT) and thescore to predict survival outcomes following liver transplan-tation (SOFT). The SOFT score is formulated from combin-ing the recipient waitlist score in addition to donor factorsand cold ischemia times. Warm ischemia was excludedsince it cannot be reliably predicted prior to transplan-tation. Table 5 illustrates the population distribution andodds ratios based on the group with less than five points.The odds ratios for 3-month survival for groups with 6–15points, 16–35 points, 36–40 points and > 40 points were2.2, 5.8, 15.4 and 30.5 respectively. Figures 1 and 2 il-lustrate the Kaplan–Meier curves and life-table analysis ofimmediate patient survival post liver transplantation basedon risk point totals from the P-SOFT and SOFT scores.Using the SOFT score, the 3-month patient survival of re-cipients with <5 points was 97%, 6–15 points was 94%,16–35 points was 84%, 36–40 points was 62% and >40
points was 38%. These groups were then labeled accord-ing to 3-month mortality risk, with <5 points designatedlow risk, 6–15 points low-moderate risk, 16–35 points high-moderate risk and 36–40 points as high risk. Calculationsof area under the ROC curves for 3-month survival showedP-SOFT and SOFT score values of 0.69 (CI 0.67–0.70) and0.70 (CI 0.69–0.71), respectively.
Warm ischemia times
Prolonged warm ischemia times may indicate surgicalinexperience or difficult operative circumstances and arelikely found only in exceptional cases. This factor was re-moved from the SOFT score since it cannot reliably bepredicted prior to transplantation.
Cancer
Eleven percent of the recipients had hepatocellular car-cinoma. Since this analysis only used calculated MELDscores, exceptional MELD points awarded for a cancer di-agnosis did not affect the analysis.
MELD as a predictor of posttransplant survival
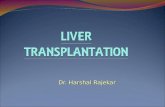
The MELD score is a poor predictor of posttransplant mor-tality as demonstrated in Figure 3. When the MELD scoreis used as a model to predict 3-month posttransplant sur-vival, the c-statistic was 0.63 (0.62–0.65).
One-year, 3-year and 5-year posttransplant survival
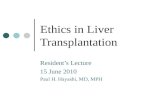
The SOFT score is also an accurate predictor of 1-year, 3-year and 5-year posttransplant survival as demonstrated inFigure 4.
Waitlist mortality
The 3-month posttransplant mortality for the SOFT scoreand the 3-month waitlist mortality for the MELD score arerepresented in Figure 5. The MELD score entry completionfor waitlisted patients was 99.9%. The c-statistic for 3-month waitlist survival is 0.83 (CI 0.82–0.83), consistentwith previous published studies (4).
Discussion
It is critical to balance pre- and post-transplant mortalityrates by considering graft, recipient and operative factorsto determine whether to accept a liver allograft for a par-ticular candidate. We report here the first model to fullyconsider the effect of graft selection, recipient factors andoperative impact with the highest reported c-statistic inthe literature. The MELD score has only proven to be anaccurate predictor of pretransplant mortality. Wiesner et al.analyzed 2 271 candidates on the waitlist before conclud-ing that the MELD score had a c-statistic of 0.83 whenused for predicting 3-month mortality while on the waitlist(4). Our analysis of 30 322 waitlisted candidates confirmedthis finding, with a c-statistic of 0.83 when only the MELDscore was used to predict 3-month mortality of candidates
2540 American Journal of Transplantation 2008; 8: 2537–2546

Survival Outcomes Following Liver Transplant Score
Table 3: Summary of donor and recipient risk factors
Donor factors
Percent entry Percent of p-Reference group Study group filled patients OR Value CI Points
Age 30–45 10–20 99.9% 15.5% 0.8 0.002 0.64–0.91 –2>70 99.9% 10.8% 1.3 0.002 1.09–1.51 3
Height > 25th%tile Height <25th%tile 100.0% 23.3% NS 0Weight > 25th%tile Weight <25th%tile 100.0% 21.2% NS 0COD (anoxia, trauma) COD CVA 99.9% 44.6% 1.2 0.003 1.06–1.34 2Cr < 1.5 Cr > 1.5 99.7% 10.4% 1.2 0.012 1.05–1.46 2No cocaine use Cocaine use 98.6% 11.8% NS 0Local procurement Regional 100.0% 22.8% NS 0
National 100.0% 6.9% 1.2 0.18 0.94–1.42 2CIT 6–12 h CIT < 6 h 86.8% 31.6% 0.7 0.00 0.63–0.81 –3WIT 30–60 min WIT 60–70 min 75.7% 4.9% 1.1 0.49 0.85–1.40 NA
WIT 70–80 min 75.7% 1.6% 1.5 0.023 1.06–2.19 NAWIT 80–90 min 75.7% 0.7% 1.8 0.022 1.09–3.00 NAWIT > 90 min 75.7% 1.1% 2.3 0.00 1.58–3.41 NA
Recipient factors
Age 40–60 Age > 70 100.0% 19.7% 1.4 0.00 1.26–1.63 4Male Female 100.0% 32.3% NS 0Height > 25th %tile Height < 25th %tile 99.2% 21.9% NS 0BMI < 30 BMI > 35 99.2% 12.2% 1.2 0.032 1.01–1.38 2All other diagnoses Acute hepatic necrosis 100.0% 7.0% NS 0
Cholestatic disease 100.0% 9.2% NS 0Malignancy 100.0% 10.7% NS 0HCV 87.1% 38.0% NS 0
No prior transplants 1 Previous transplant 100.0% 7.2% 1.9 0.00 1.56–2.24 92 Previous transplants 100.0% 0.7% 2.4 0.00 1.53–3.69 14
No previous abdominalsurgery
Previous abdominal surgery 100.0% 36.8% 1.2 0.002 1.07–1.36 2
Nondiabetic Diabetes mellitus 99.9% 23.0% NS 0ALT < 100 ALT > 100 97.1% 26.2% NS 0Albumin > 2.5 2.0 < Albumin < 2.5 99.9% 21.3% NS 0
Albumin < 2.0 99.9% 10.7% 1.2 0.023 1.03–1.42 2No dialysis Dialysis pretransplant 99.9% 6.1% 1.3 0.003 1.10–1.60 3Home pretransplant ICU pretransplant 100.0% 12.7% 1.6 0.00 1.34–1.99 6
Hospitalized pretransplant 100.0% 15.5% 1.3 0.001 1.12–1.53 3Non-UNOS status 1 UNOS Status 1 100.0% 6.4% NS 0MELD score: (10–19) MELD ≤ 9 99.9% 9.5% NS 0
MELD 30–39 99.9% 13.2% 1.4 0.00 1.19–1.62 4MELD ≥ 40 99.9% 5.1% 1.4 0.007 1.09–1.69 4
Not on life support Pretransplant
Life support pretransplant 100.0% 7.1% 1.9 0.00 1.54–2.35 9
Nonencephalopathic Encephalopathy at transplant 100.0% 19.7% 1.2 0.026 1.02–1.33 2No portal vein
thrombosisPortal vein thrombosis at transplant 93.9% 3.9% 1.5 0.001 1.16–1.84 5
No incidental tumors Incidental tumor found at transplant 99.9% 4.0% NS 0< 1 year on waitlist 1–2 years on waitlist 99.9% 9.6% NS 0ABO compatible ABO incompatible 100.0% 0.5% NS 0Not ventilator
dependentVentilator-dependent pretransplant 100.0% 3.9% NS 0
No portal bleed within48 h pretransplant
Portal bleed within 48 h pretransplant 50.7% 3.1% 1.5 0.001 1.18–1.89 6
No variceal bleedingwithin 2 weeks ofregistration
Variceal bleeding within 2 weeks of registration 92.9% 5.4% NS 0
No ascitespretransplant
Ascites pretransplant 100.0% 83.9% 1.3 0.004 1.08–1.51 3
No SBP pretransplant SBP pretransplant 94.8% 6.7% NS 0No PE within 6 months
of registrationPE within 6 months of registration 93.4% 0.3% NS 0
COD = cause of death; Cr = serum creatinine; CIT = cold ischemia time; WIT = warm ischemia time; CVA = cerebrovascular accident;%tile = percentile; BMI = body mass index; HCV = hepatitis C Virus; ALT = alanine aminotransferase; ICU = intensive care unit; UNOS =United Network for Organ Sharing; MELD = model for end-stage liver disease.
American Journal of Transplantation 2008; 8: 2537–2546 2541

Rana et al.
Actuarial Survival for Liver Allograft Recipients Divided According to SOFT Score 6 3 1 htnoM
Low Risk 99% 97% 96%Low-Moderate 97% 94% 92% High-Moderate 90% 84% 80%
High 72% 62% 56% Futile 46% 38% 37%
* All groups p<0.01 compared to Low Risk
0.00
0.25
0.50
0.75
1.00
Survival
0 2 4 6Months
Low Low-Moderate
High-Moderate High
Futile
Patient Survival by SOFT Score
Figure 1: Kaplan–Meier curve of
recipient survival by the Survival
Outcomes Following Liver Trans-
plantation (SOFT) score. The y-axisis the percentage recipient survivalof total recipients and the x-axisis the months post liver transplant.p < 0.001 for each group by log-ranktest with reference to low SOFT riskgroup.
on the waitlist. Attempts to employ the MELD score aloneto predict posttransplant mortality have yielded inaccurateresults (6,7). In the present analysis, the MELD score aloneyielded a c-statistic of 0.63 when used to predict 3-monthsurvival following transplantation. The Kaplan–Meier sur-vival curves, stratified by the MELD score in Figure 3, illus-trate the poor predictive value of the MELD score. In themodel proposed by Desai et al., retransplantation, recipi-ent age, mechanical ventilation and dialysis were used topredict posttransplant recipient survival at 3 months andyielded a c-statistic of 0.65 (7). Our newly formulated sur-vival outcomes following liver transplantation (SOFT) scorethat combined donor and recipient risk factors resulted in ac-statistic of 0.70 as a predictor of 3-month posttransplantsurvival. The SOFT score is therefore the most accuratepredictor to date of 3-month recipient survival followingliver transplantation.
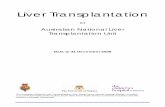
The preallocation score to predict survival following livertransplantation (P-SOFT) differs from the SOFT score sinceit utilizes only 14 out of 19 risk factors that are availablewhen the candidate is on the waitlist. It is designed toevaluate a candidate prior to liver allograft allocation andresults in a c-statistic of 0.69 as a predictor of 3-monthrecipient survival following liver transplantation. The SOFT
score includes donor and recipient factors but is dominatedby recipient factors, which comprise 14 out of 18 includedrisk factors. Seven donor factors, cold ischemic timesand portal bleeds are also considered in the SOFT score(Table 4). The SOFT score does not correlate with theMELD score as shown in Figure 6. Although cold ischemictimes are determined in the course of transplantation, wepropose that they may be estimated when a donor allo-graft is offered. The overall result of the SOFT score mayultimately guide the clinician to either accept or declinethe offer based on the projected risk group into which therecipient is placed. The DRI is inadequate in this respectsince there is no consideration for recipient risk factors.
In order to determine which recipients, defined by MELDrisk score, should be transplanted, we compared waitlistmortality predicted by the MELD score to posttransplantmortality defined by the SOFT score (Figure 5). On thebasis of these results, we suggest that candidates with aMELD score ranging from 17 to 19 points should only re-ceive low-risk SOFT transplants; candidates with a MELDscore of 20–29 points should receive low or low-moderaterisk SOFT transplants; candidates with a MELD score of30–39 points should receive low, low-moderate or high-moderate risk SOFT transplants; and candidates with the
2542 American Journal of Transplantation 2008; 8: 2537–2546

Survival Outcomes Following Liver Transplant Score
Actuarial Survival for Liver Allograft Recipients Divided According to p-SOFT Score
Month 1 3 6 Low Risk 98% 97% 95%
Low-Moderate 97% 94% 91% High-Moderate 88% 82% 78%
High 60% 53% 50% Futile 50% 41% 38%
* All groups p<0.01 compared to Low Risk
0.00
0.25
0.50
0.75
1.00
Survival
0 2 4 6Months
Low Low-Moderate
High-Moderate High
Futile
Patient Survival by p-SOFT Score
Figure 2: Kaplan–Meier curve of recipi-
ent survival by the preallocation score
to predict survival following liver trans-
plantation (P-SOFT). The y-axis is the per-centage recipient survival of total recip-ients and the x-axis is the months postliver transplant. p < 0.001 for each groupby log-rank test with reference to low riskgroup.
Actuarial Survival for Liver Allograft Recipients Divided by MELD Score Categories 6 3 1 htnoM
MELD < 9 98% 97% 95%10-19 98% 96% 94% 20-29 96% 93% 90% 30-39 93% 88% 84% ≥ 40 90% 85% 83%
* All Groups p<0.05 compared to MELD < 9
0.00
0.25
0.50
0.75
1.00
Survival
0 2 4 6months
<9 10-19
20-29 30-39
>40
Patient Survival by Meld Score Alone
Figure 3: Kaplan–Meier curve of recip-
ient survival by the MELD score alone.
The y-axis is the percentage recipient sur-vival of total recipients and the x-axis isthe months post liver transplant. p < 0.05for each group by log-rank test with refer-ence to the group with a MELD score ofless than 9.
American Journal of Transplantation 2008; 8: 2537–2546 2543

Rana et al.
Actuarial Survival for Liver Allograft Recipients Divided According to SOFT Score Month 12 36 60
Low Risk 93% 85% 77%Low-Moderate 87% 78% 71% High-Moderate 75% 67% 57%
High 53% 42% 38% Futile 35% 26% --
* All groups p<0.01 compared to Low Risk
0.00
0.25
0.50
0.75
1.00
Survival
0 20 40 60Months
Low Low-Moderate
High-Moderate High
Futile
Patient Survival by SOFT Score
Figure 4: Kaplan–Meier curve of
recipient survival by the Survival
Outcomes Following Liver Trans-
plantation (SOFT) score. The y-axisis the percentage recipient survivalof total recipients and the x-axisis the months post liver transplant.p <0.001 for each group by log-ranktest with reference to low SOFT riskgroup.
highest waitlist mortality risk with a MELD score of greaterthan 40 should receive low, low-moderate, high-moderateor high-risk SOFT transplants. These recommendationslikely do not apply to patients with hepatic cancers sincethe benefit of early removal of tumor must also be consid-ered in addition to the MELD and SOFT scores.
This study emphasizes that transplants in patients with aSOFT score of >40 are likely futile since the predicted post-transplant mortality is greater than any waitlist mortality aspredicted by the MELD score. Since patients with acutehepatic failure have an exceptionally high waitlist mortal-ity, which is not accurately predicted by the MELD scorealone, the futility of a SOFT score >40 does not apply tothis group of patients.
The Scientific Registry for Transplant Recipients (SRTR) of-fers a risk-adjusted model to project patient survival afterliver transplantation. The model combines an extensive listof donor and recipient covariates and is an effective audit-ing tool since a transplant program’s observed outcomescan be compared to expected outcomes (10,11). Unlike theSRTR risk-adjusted model, the proposed SOFT risk scorecan be used to predict outcomes for a particular recipi-ent and donor allograft prior to transplantation in order to
compare against waitlist mortality predicted by the MELDscore. The multivariate analysis in this study included all ofthe variables considered in the SRTR risk-adjusted model.
Figure 5: Waitlist mortality as predicted by the MELD score
compared to mortality following liver transplantation as pre-
dicted by the SOFT score. The y-axis is the mortality percent-age at 3 months and the x-axis presents MELD and SOFT scoregroups. Each pair of compared groups were significantly differentwith a p-value of <0.05 using the chi-square test. Only the SOFTscore had a significant p-value for Group B (<0.05).
2544 American Journal of Transplantation 2008; 8: 2537–2546

Survival Outcomes Following Liver Transplant Score
Table 4: P-SOFT and SOFT scores
Risk factor Points allotted
Preallocation score to predict survival outcomes following liver
transplantation (P-SOFT)
• Age > 60 4• BMI > 35 2• One previous transplant 9• Two previous transplants 14• Previous abdominal
surgery2
• Albumin < 2.0 g/dL 2• Dialysis prior to
transplantation3
• Intensive care unitpretransplant
6
• Admitted to hospitalpretransplant
3
• MELD score >30 4• Life support pretransplant 9• Encephalopathy 2• Portal vein thrombosis 5• Ascites pretransplant 3
Score to predict survival outcomes following liver
transplantation (SOFT)
• P-SOFT score Total from above• Portal bleed 48 h
pretransplant6
• Donor age 10–20 years –2• Donor age > 60 years 3• Donor cause of death from
cerebral vascular accident2
• Donor creatinine > 1.5mg/dL
2
• National allocation 2• Cold ischemia time 0–6 h –3
BMI = body mass index; MELD = model for end-stage liverdisease.
In comparison, the SRTR model for 1-month posttransplantsurvival had an index of concordance of 0.66.
Limitations
Since the passage of the National Transplantation Act of1984, data entry has been mandatory for all US trans-
Table 5: Risk groups generated from P-SOFT and SOFT scores
Risk group Point range Percentage of patients Odds ratio (CI)(low risk is Ref) p-Value
SOFT Score Low 0–5 35.8Low-moderate 6–15 46.8 2.16 (1.86–2.51) <0.001High-moderate 16–35 16.3 5.82 (4.98–6.81) <0.001
High 36–40 0.72 15.44 (10.81–22.04) <0.001Futile > 40 0.41 30.48 (19.73–47.08) <0.001
P-SOFT score Low 0–5 40.29Low-moderate 6–15 44.13 1.97 (1.71–2.26) <0.001High-moderate 16–35 14.54 5.30 (4.57–6.14) <0.001
High 36–40 0.68 12.68 (8.81–18.26) <0.001Futile > 40 0.36 26.56 (16.75– 42.11) <0.001
Figure 6: Scatter plot of MELD score and SOFT score for liver
transplant recipients. The y-axis is the score range for the SOFTscore and the x-axis is the score range for the MELD score.
plant centers. Nevertheless, all patient registries oftensuffer from variability in data entry. Findings from thisstudy use large cohorts of patients and are unlikely tobe significantly impacted by small amount of missingdata. Fields contained within this data base were gener-ally well populated with a 95–99% data entry rate for themajority of variables. The fact that center-specific factorscould not be appropriately accounted for is a significantlimitation.
Conclusion
This analysis represents the largest study of waitlisted can-didates and transplant recipients of liver allografts afterthe MELD Score was implemented for allocation in 2002.Survival after liver transplantation must be greater thansurvival on the waitlist to justify liver transplantation. TheSOFT score, newly formulated from the same cohort ofpatients, can accurately predict 3-month survival followingliver transplantation. It can then be compared with MELD-predicted waitlist mortality to determine which patientsshould be transplanted. The SOFT score can also be usedto improve donor–recipient matching.
American Journal of Transplantation 2008; 8: 2537–2546 2545

Rana et al.
Acknowledgment
This study was funded by National Institutes of Health training grantT32HL07854–11 (AR) and by Health Resources and Services Administrationcontract 231–00-0115.
References
1. Malinchoc M, Kamath PS, Gordon FD et al. A model to predictpoor survival in patients undergoing transjugular intrahepatic por-tosystemic shunts. Hepatology 2000; 31: 864–871.
2. Kamath PS, Wiesner RH, Malinchoc M et al. A model to predictsurvival in patients with end-stage liver disease. Hepatology 2001;33: 464–470.
3. Freeman RB, Wiesner RH, Edwards E, Harper A, Merion R, WolfeR. United Network for Organ Sharing Organ Procurement andTransplantation Network Liver and Transplantation Committee. Re-sults of the first year of the new liver allocation plan. Liver Transpl2004; 10: 7–15.
4. Wiesner R, Edwards E, Freeman R et al. United Network for Or-gan Sharing Liver Disease Severity Score Committee. Model forend-stage liver disease (MELD) and allocation of donor livers. Gas-troenterology 2003; 124: 91–96.
5. Hanley JA, McNeil BJ. The meaning and use of the area undera receiver operating characteristic (ROC) curve. Radiology 1982;143: 29–36.
6. Brown RS Jr., Kumar KS, Russo MW et al. Model for end-stageliver disease and Child-Turcotte-Pugh score as predictors of pre-transplantation disease severity, posttransplantation outcome, andresource utilization in United Network for Organ Sharing status 2Apatients. Liver Transpl 2002; 8: 278–284.
7. Desai NM, Mange KC, Crawford MD et al. Predicting outcome afterliver transplantation: Utility of the model for end-stage liver diseaseand a newly derived discrimination function. Transplantation 2004;77: 99–106.
8. Merion RM, Schaubel DE, Dykstra DM, Freeman RB, Port FK,Wolfe RA. The survival benefit of liver transplantation. Am J Trans-plant 2005; 5: 307–313.
9. Feng S, Goodrich NP, Bragg-Gresham JL et al. Characteristics as-sociated with liver graft failure: The concept of a donor risk index.Am J Transplant 2006; 6:783–790.
10. Levine GN, McCullough KP, Rodgers AM, Dickinson DM, AshbyVB, Schaubel DE. Analytical methods and database design: Impli-cations for transplant researchers, 2005. Am J Transplant 2006; 6:1229–1242.
11. Dickinson DM, Shearon TH, O’Keefe J et al. SRTR center-specificreporting tools: Posttransplant outcomes. Am J Transplant 2006;6: 1199–1211.
2546 American Journal of Transplantation 2008; 8: 2537–2546