
Surgical Stabilization of Rib Fractures in Denver failure ... Surgical Stabilization of Rib...
29
Surgical Stabilization of Rib Fractures in Denver A Prospective Clinical Trial
Transcript of Surgical Stabilization of Rib Fractures in Denver failure ... Surgical Stabilization of Rib...

Surgical Stabilization of Rib Fractures in Denver
A Prospective Clinical Trial
Disclosures
• This work was supported by an investigator-initiated research grant from DePuy Synthes
• Paid faculty & consultant: – DePuy Synthes – Zimmer BioMet



Study Design
• Contributions – Prospective – Contemporary fixation system – Detailed fracture pattern information – Non flail chest fracture patterns – American
• Weaknesses
– Single center – Not truly randomized – Limited to acute period

• Surgical stabilization of severe rib fractures, as compared to best medical management, improves acute outcomes
Hypothesis
• Single institution, prospective, controlled evaluation
• Inclusion:
– Age ≥ 18 years – Severe rib fractures
1. Flail chest 2. ≥ 3 severely displaced fractures 3. ≥ 30% volume loss hemithorax 4. Failure of medical management
– Presentation within 72 hours of injury
Study Design

Denver Health Medical Center Algorithm for Non Operative Management of Rib Fractures
(Access response hourly)
Inadequate response defined as ≥ 1 of the following: Numeric pain score > 4 Spirometry < 75% predicted RR > 20 Poor cough/splinting/inability to clear secretions
Begin • Oral narcotics • Oral muscle relaxants • Oral/IV NSAIDs • “Rib blocks”
• Incentive spirometry • Upright position/ambulation • Cough and deep breathing
ANALGESIA
PULMONARY TOILET
Add • IV narcotics (PCA) • Continuous
intercostal nerve blockade
• Naso-tracheal suctioning
Add • Continuous thoracic
epidural catheter
• Cricothyroidotostomy tube (“mini-trach”)
• +/- Intubation/ mech ventilation
Routine therapies following intubation: Humidified O2 Positional changes E.T.T. suctioning CPAP
Inadequate response
Inadequate response
• 2013: Non-operative
• 2014: Operative
Study Design


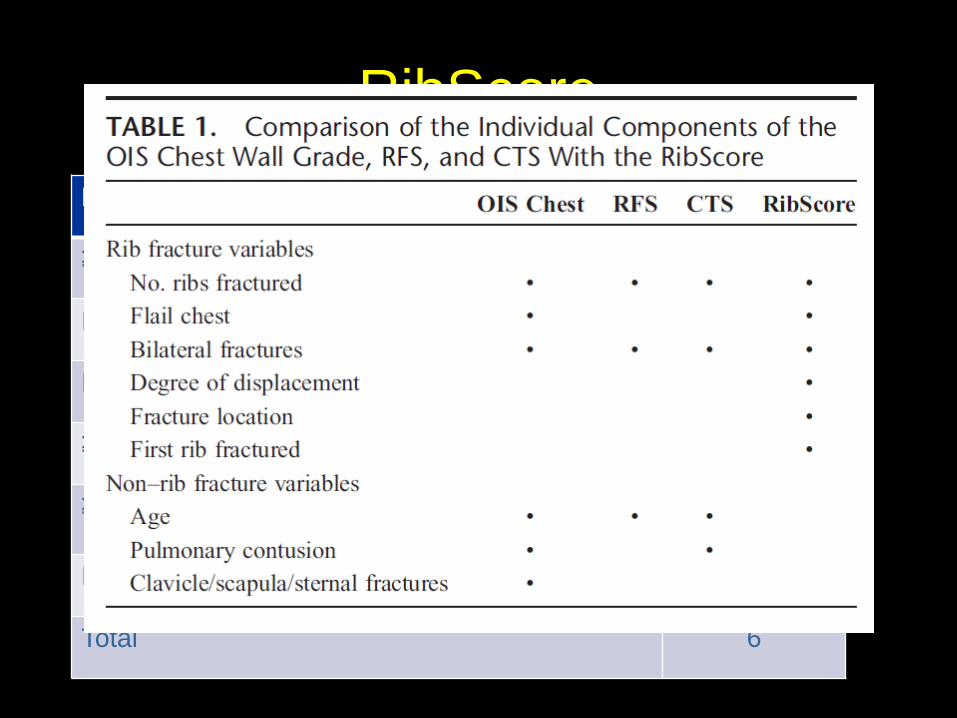
RibScore Parameter Points
≥ 6 fractures 1
Flail chest 1
Bilateral fractures 1
≥ 3 severely displaced fractures 1
≥ 1 anterior, lateral, and posterior fracture 1
First rib fracture 1
Total 6

Results Study Flow
2013 (non-operative)
35 patients met criteria
35 analyzed
37 patients met criteria
2014 (operative)
35 analyzed
2 excluded (declined operation)
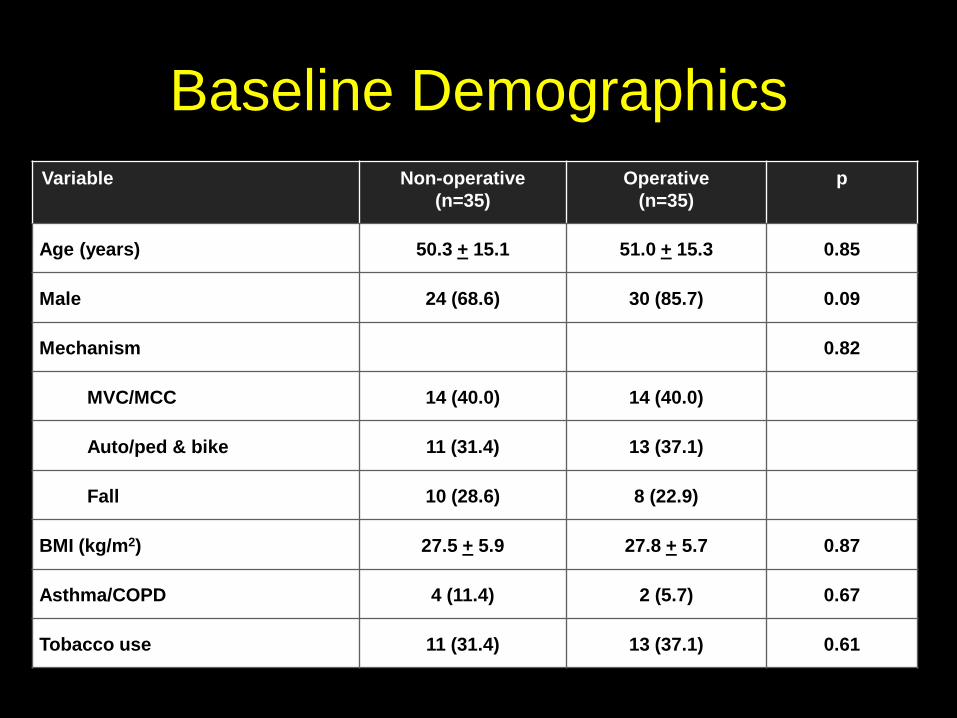
Baseline Demographics Variable Non-operative
(n=35) Operative
(n=35) p
Age (years) 50.3 + 15.1 51.0 + 15.3 0.85
Male 24 (68.6) 30 (85.7) 0.09
Mechanism 0.82
MVC/MCC 14 (40.0) 14 (40.0)
Auto/ped & bike 11 (31.4) 13 (37.1)
Fall 10 (28.6) 8 (22.9)
BMI (kg/m2) 27.5 + 5.9 27.8 + 5.7 0.87
Asthma/COPD 4 (11.4) 2 (5.7) 0.67
Tobacco use 11 (31.4) 13 (37.1) 0.61
Variable Non-operative (n=35)
Operative (n=35)
p
ISS 22.0 (17.0, 38.0) 21.5 (17.0, 26.0) 0.69
Intracranial hemorrhage 10 (28.6) 2 (5.7) 0.01
Admission GCS 14.0 (7.0, 15.0) 15.0 (14.0, 15.0) 0.03
Facial fracture 7 (20.0) 3 (8.6) 0.17
Pelvic fracture 12 (34.3) 8 (22.9) 0.19
Long bone fracture 0 1 (2.9) NA
Solid organ injury 11 (31.4) 9 (25.6) 0.60
BCVI 2 (5.7) 0 0.49
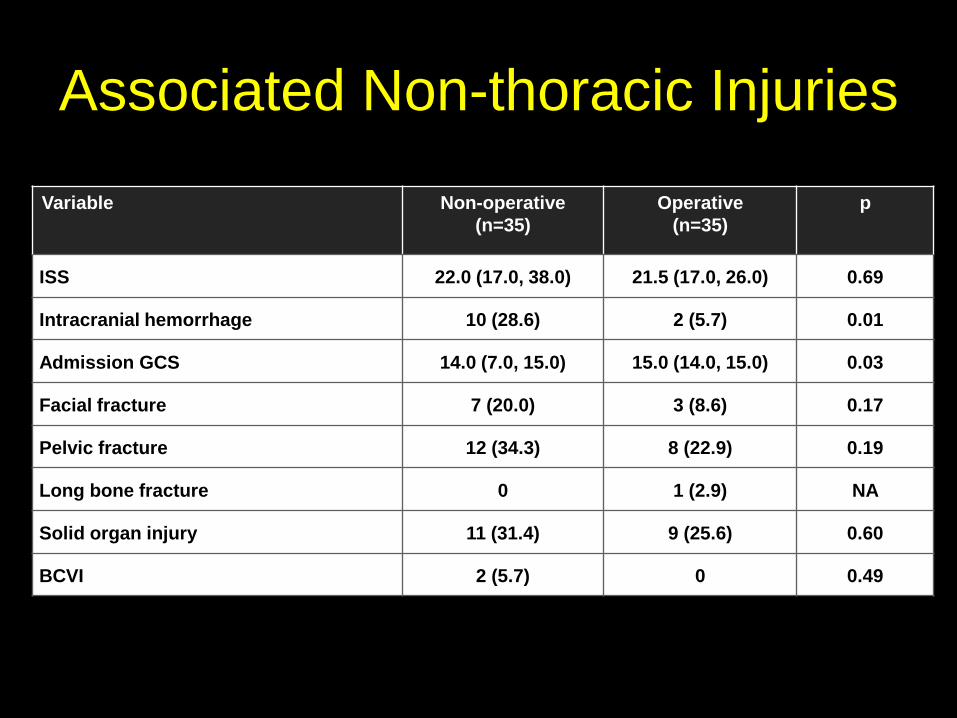
Associated Non-thoracic Injuries

Associated Non-thoracic Injuries
Variable Non-operative (n=35)
Operative (n=35)
p
ISS 22.0 (17.0, 38.0) 21.5 (17.0, 26.0) 0.69
Intracranial hemorrhage 10 (28.6) 2 (5.7) 0.01
Admission GCS 14.0 (7.0, 15.0) 15.0 (14.0, 15.0) 0.03
Facial fracture 7 (20.0) 3 (8.6) 0.17
Pelvic fracture 12 (34.3) 8 (22.9) 0.19
Long bone fracture 0 1 (2.9) NA
Solid organ injury 11 (31.4) 9 (25.6) 0.60
BCVI 2 (5.7) 0 0.49

Associated Thoracic Injuries
Variable Non-operative (n=35)
Operative (n=35) p
BPC18 3.5 (2.0, 4.0) 4.0 (2.0, 5.0) 0.67
Pneumothorax 31 (88.6) 28 (80.0) 0.51
Hemothorax 10 (28.6) 18 (51.4) 0.09
Clavicle Fracture 5 (45.5) 6 (17.1) 0.74
Scapula fracture 5 (14.3) 8 (22.9) 0.36
Spine fracture 17 (48.6) 11 (31.4) 0.09
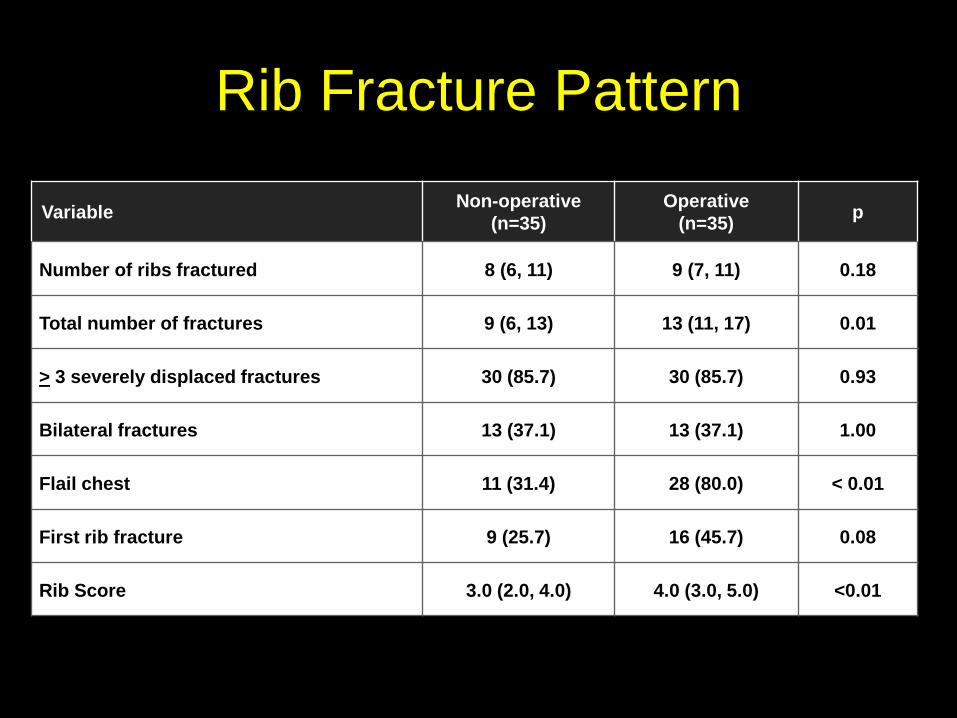
Rib Fracture Pattern
Variable Non-operative (n=35)
Operative (n=35) p
Number of ribs fractured 8 (6, 11) 9 (7, 11) 0.18
Total number of fractures 9 (6, 13) 13 (11, 17) 0.01
> 3 severely displaced fractures 30 (85.7) 30 (85.7) 0.93
Bilateral fractures 13 (37.1) 13 (37.1) 1.00
Flail chest 11 (31.4) 28 (80.0) < 0.01
First rib fracture 9 (25.7) 16 (45.7) 0.08
Rib Score 3.0 (2.0, 4.0) 4.0 (3.0, 5.0) <0.01

Rib Fracture Pattern
Variable Non-operative (n=35)
Operative (n=35) p
Number of ribs fractured 8 (6, 11) 9 (7, 11) 0.18
Total number of fractures 9 (6, 13) 13 (11, 17) 0.01
> 3 severely displaced fractures 30 (85.7) 30 (85.7) 0.93
Bilateral fractures 13 (37.1) 13 (37.1) 1.00
Flail chest 11 (31.4) 28 (80.0) < 0.01
First rib fracture 9 (25.7) 16 (45.7) 0.08
Rib Score 3.0 (2.0, 4.0) 4.0 (3.0, 5.0) <0.01

Unadjusted Outcomes
Variable Non-operative (n=35)
Operative (n=35) p
Respiratory Failure 25 (71.4) 17 (48.6) 0.04
Tracheostomy 16 (45.7) 5 (14.3) 0.01
Pneumonia 11 (31.4) 7 (20.0) 0.28
Days mechanical ventilation 5 (0,18) 0 (0,8) <0.01
Hospital length of stay (days) 16.0 (10.0, 23.0) 13.0 (9.0, 21.0) 0.11
ICU length of stay (days) 9.0 (4.0, 15.0) 6.0 (3.0, 10.0) 0.15

Multivariable Logistic Regression
Variable Adjusted OR¥ 95% CI p
Mechanical ventilation 0.24 0.06-0.93 0.03
Tracheostomy 0.18 0.04-0.78 0.03
Pneumonia 0.53 0.14-2.00 0.62
¥Adjusted for RibScore, ISS and ICH
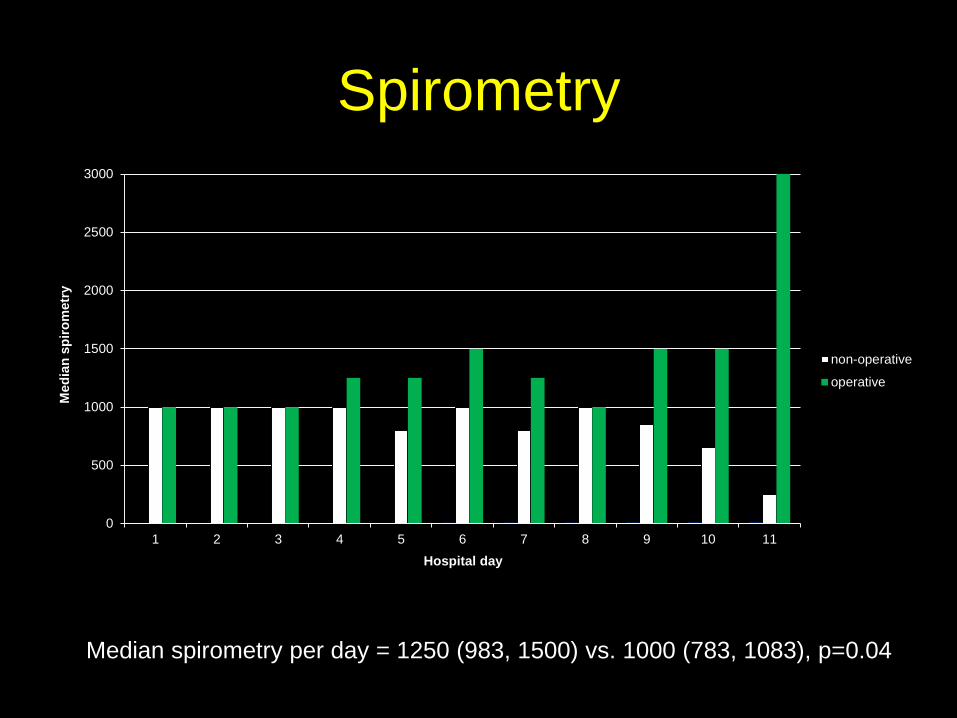
Spirometry
0
500
1000
1500
2000
2500
3000
1 2 3 4 5 6 7 8 9 10 11
Med
ian
spiro
met
ry
Hospital day
non-operative
operative
Median spirometry per day = 1250 (983, 1500) vs. 1000 (783, 1083), p=0.04

Narcotic Requirements
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Med
ian
Req
uire
men
ts
Hospital Days
non-operative
operative
Median narcotic requirement per day = 9 (3,17) vs. 12 (7,25), p=0.15
• Surgical stabilization independently improved pulmonary outcomes: – Respiratory failure – Tracheostomy – Duration of mechanical ventilation – Spirometry
• Recommendation: Consideration of surgical
stabilization in all trauma patients who meet ≥ 1 inclusion criteria
Conclusion

• Do we need another RCT showing efficacy?
• Which RCTs do we need?
• How best to develop an international RCT group (e.g., ARDSnet)
Critical Next Steps

Surgical Stabilization of Rib Fractures in Denver
A Prospective Clinical Trial

• Respiratory Failure • Pneumonia • Tracheostomy
• Ventilator Days • ICU LOS • Hospital LOS
• Spirometry • Narcotic Requirements
Methods Outcomes

Results Operative Details
Variable Outcome
Ribs fractured: ribs plated 2.0 (1.0, 2.0)
Ribs plated 5 (4, 6)
Time to surgery from injury (days) 2.4 + 0.78
Surgery length (hours) 1.5 + 1.2
Number of surgeons 4
Hardware failure 1 (2.9)
Hardware infection 1 (2.9)


















