
Surgical Privileges Form Orthopedic Surgery - … · 10.Use of Hybrid External Fixator ......
10
Name of applicant……………… Page 1 of 10 Surgical Privileges Form Orthopedic Surgery CLINICAL PRIVILEGES REQUEST Applicant’s Name: …………………………….…… . Scope of Practice: ………………………. License No. (If Any): …………………………….…….. Facility:………………………… .......... Date: …………………………….………………………….. Place of Work: …………………................... Requested Recommended Not Privileges (To be completed (For committee use) Recommended by the applicant) (For committee use) CATEGORY I: CORE PRIVILEGES 1. Admitting Privileges 2. Admission history and physical examination 3. Interpretation of laboratory tests 4. Insertion of urinary catheters 5. Peripheral intravenous catheter insertion 6. Nasogastric tube insertion 7. Oropharyngeal airway insertion 8. Prescribing Oxygen therapy CATEGORY II: EMEREGENCY SURGERY 1.Application of Traction Pins 2.Closed manipulation of fractures / dislocations/splints/casts / splints / casts 3.Closed manipulation and Percutaneous wire / screw fixation 4.Open reduction with plate / screw fixation (MIPO + LISS) 5.Open reduction and tension wiring 6.Open reduction with intramedullary device 7.Closed reduction with intramedullary device 8.Open reduction and application of external fixation 9.Closed reduction and Application of external fixation 10.Use of Hybrid External Fixator (Illizarov) 11.Operative treatment of intra articular fractures 12.Operative treatment of Soft Tissue Injuries 13.Tendon / ligament repair 14.Fasciotomy 15.Wound debridement 16.Operative treatment of Acute bone, joint & Soft tissue infection
Transcript of Surgical Privileges Form Orthopedic Surgery - … · 10.Use of Hybrid External Fixator ......
Name of applicant………………
Page 1 of 10
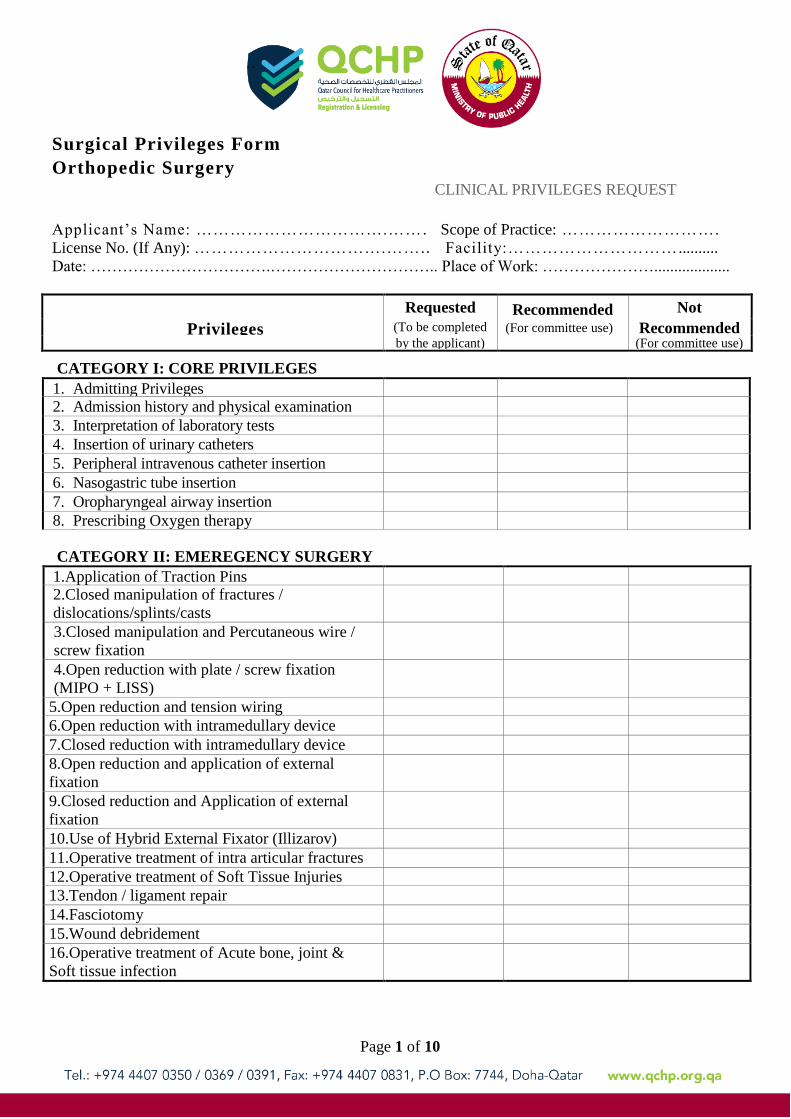
Surgical Privileges Form
Orthopedic Surgery
CLINICAL PRIVILEGES REQUEST
Applicant’s Name: …………………………….…… . Scope of Practice: ……………………….
License No. (If Any): …………………………….…… .. Facility:………………………… ..........
Date: …………………………….………………………….. Place of Work: …………………...................
Requested Recommended Not
Privileges (To be completed (For committee use) Recommended by the applicant) (For committee use)
CATEGORY I: CORE PRIVILEGES
1. Admitting Privileges 2. Admission history and physical examination
3. Interpretation of laboratory tests
4. Insertion of urinary catheters
5. Peripheral intravenous catheter insertion
6. Nasogastric tube insertion
7. Oropharyngeal airway insertion
8. Prescribing Oxygen therapy
CATEGORY II: EMEREGENCY SURGERY
1.Application of Traction Pins 2.Closed manipulation of fractures /
dislocations/splints/casts
/ splints / casts
3.Closed manipulation and Percutaneous wire /
screw fixation
4.Open reduction with plate / screw fixation
(MIPO + LISS)
5.Open reduction and tension wiring
6.Open reduction with intramedullary device
7.Closed reduction with intramedullary device
8.Open reduction and application of external
fixation
9.Closed reduction and Application of external
fixation
10.Use of Hybrid External Fixator (Illizarov)
11.Operative treatment of intra articular fractures
12.Operative treatment of Soft Tissue Injuries
13.Tendon / ligament repair
14.Fasciotomy
15.Wound debridement
16.Operative treatment of Acute bone, joint &
Soft tissue infection

Name of applicant………………
Page 2 of 10
Requested Recommended Not
Privileges (To be completed (For committee use) Recommended by the applicant) (For committee use)
17.Bone grafting
18.Split thickness skin graft (STSG)
19.Hemi / Bipolar Arthroplasty of Hip Fractures
20.Operative fixation using DHS / DCS /
Cannulated screws
CATORGY III: PEDIATRIC SURGICAL PRCOEDURES
Upper Extremity
1.Correction of forearm deformities (e.g
hypoplasia of radius, Madelung’s deformity)
2.Correction of elbow deformities (e.g
congenital dislocation head of radius, Cubitus
Varus)
3.Correction of shoulder deformities (e.g
Sprengel’s Deformity)
4.Soft tissue release of the thumb or hand in CP
5.Tendon transfer to the elbow, hand or wrist
6.Release of congenital trigger fingers in
children
Hip Joint
1.Close reduction, spica for DDH 2.Arthrography of the hip
3.Percutaneous tenotomy, close reduction of the
hip
4.Extensive soft tissue release of the hip
(neuromuscular disorders)
5.Open reduction of the hip for DDH
6.Open reduction of the hip, femoral osteotomy
7.Pelvic osteotomies (Salter, Pemberton, Chiari,
etc.)
8.Fixation of slipped epiphysis
9. 3-plane intertrochanteric osteotomy of femur
Knee Joint
1.Manipulation, POP for congenital dislocation
of the knee
2.Soft tissue release for congenital dislocation of
the knee
3.Soft tissue release for fixed flexion deformity
(neuromuscular)
Name of applicant………………
Page 3 of 10
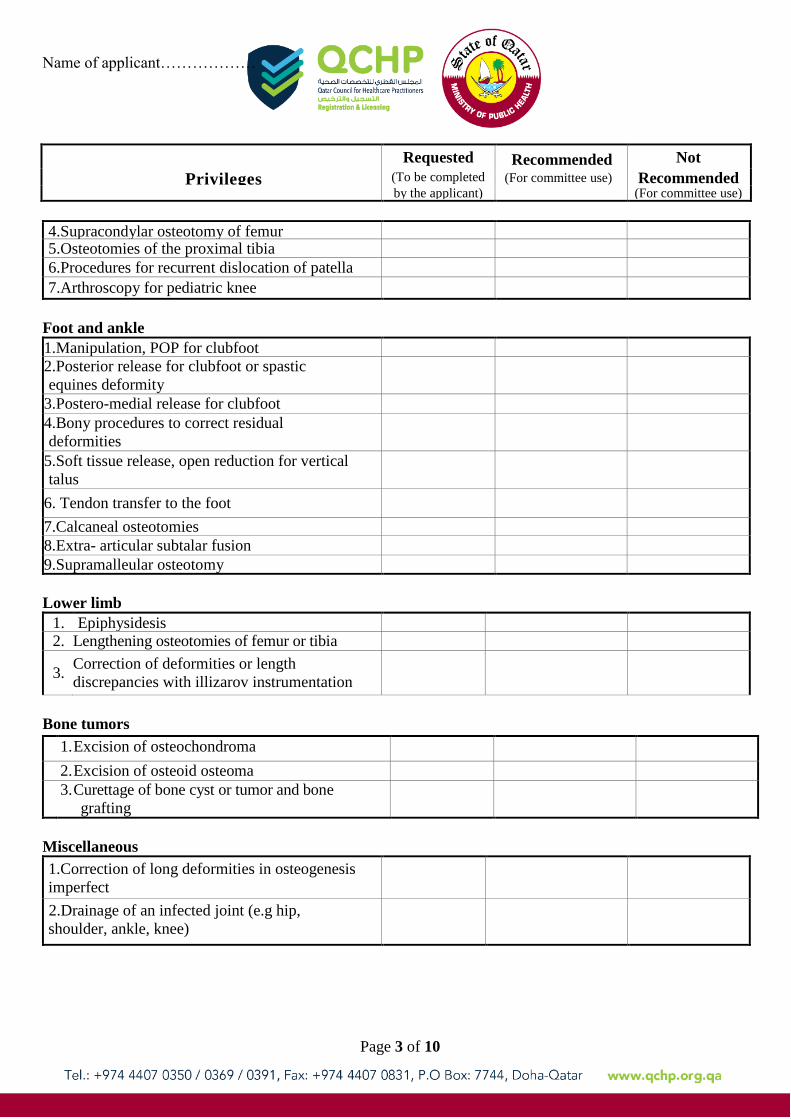
4.Supracondylar osteotomy of femur 5.Osteotomies of the proximal tibia
6.Procedures for recurrent dislocation of patella
7.Arthroscopy for pediatric knee
Foot and ankle
1.Manipulation, POP for clubfoot
2.Posterior release for clubfoot or spastic
equines deformity
3.Postero-medial release for clubfoot
4.Bony procedures to correct residual
deformities
5.Soft tissue release, open reduction for vertical
talus
6. Tendon transfer to the foot
7.Calcaneal osteotomies
8.Extra- articular subtalar fusion
9.Supramalleular osteotomy
Lower limb
1. Epiphysidesis
2. Lengthening osteotomies of femur or tibia
3. Correction of deformities or length
discrepancies with illizarov instrumentation
Bone tumors
1
.
1. Excision of osteochondroma
2
.
2. Excision of osteoid osteoma
3. Curettage of bone cyst or tumor and bone
grafting
Miscellaneous
1.Correction of long deformities in osteogenesis
imperfect
2.Drainage of an infected joint (e.g hip,
shoulder, ankle, knee)
Requested Recommended Not
Privileges (To be completed (For committee use) Recommended by the applicant) (For committee use)
Name of applicant……………
Page 4 of 10
Requested Recommended Not
Privileges (To be completed (For committee use) Recommended by the applicant) (For committee use)
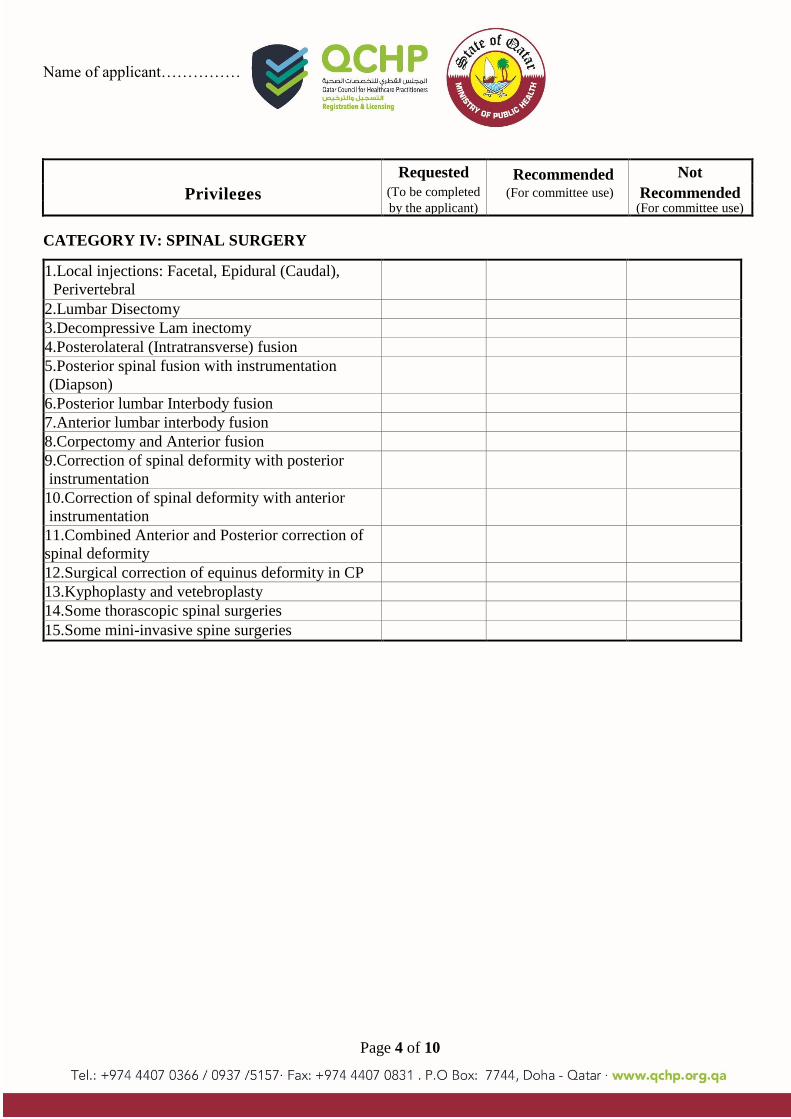
CATEGORY IV: SPINAL SURGERY
1.Local injections: Facetal, Epidural (Caudal),
Perivertebral
2.Lumbar Disectomy
3.Decompressive Lam inectomy
4.Posterolateral (Intratransverse) fusion
5.Posterior spinal fusion with instrumentation
(Diapson)
6.Posterior lumbar Interbody fusion
7.Anterior lumbar interbody fusion
8.Corpectomy and Anterior fusion
9.Correction of spinal deformity with posterior
instrumentation
10.Correction of spinal deformity with anterior
instrumentation
11.Combined Anterior and Posterior correction of
spinal deformity
spinal deformity
12.Surgical correction of equinus deformity in CP
13.Kyphoplasty and vetebroplasty
14.Some thorascopic spinal surgeries
15.Some mini-invasive spine surgeries

Name of applicant……………
Page 5 of 10
CATEGORY V: SHOULDER SURGERIES
1.Manipulation of frozen shoulders 2.Subacromial and Intraarticular injections
3.Scapular bursa injection: excision – open
4.Scapular bursa injection: arthroscopic
5.Shoulder arthroscopy: diagnostic
6.Shoulder arthroscopy: synovial biopsy
7.Shoulder arthroscopy: lose bodies
8.Shoulder arthroscopy: slap lesions
9.Subacromial decompression: open
10.Subacromial decompression: arthroscopic
11.A/C joint resection: acromioplasty open
12.A/C joint resection: arthroscopic
13.Anterior shoulder stabilization procedures:
open
14.Anterior shoulder stabilization procedures:
arthroscopic
15.Posterior shoulder stabilization: open
16.Shoulder replacement
17.Rotator cuff repair: open
18.Rotator cuff repair: arthroscopic
19.Biceps tendon tenodesis open
20.Subscapular Nerve entrapment release
21.Soft tissue / Bony tumors around shoulder:
excision
22.Soft tissue / Bony tumors around shoulder:
Biopsy
23.Shoulder Arthrodesis
24.ORIF of fractures of scapula
25.ORIF of fractures of humeral head / humeral
shaft
Requested Recommended Not
Privileges (To be completed
by (For committee use) Recommended
the applicant) (For committee use)

Page 6 of 10
CATEGORY VI: WRIST AND HAND SURGERY
1.Arthrodesis of the Wrist
2.Arthroscopy of the Wrist
3.Tendon Repair Basic Techniques
4.Nerve Entrapment surgery (Medial Nerve,
Ulnar nerve)
5.Surgical treatment of Tenosynovitis
6.Surgical treatment of special hand infections
(Palmer spaces, web spaces … etc)
7.Surgical treatment of tendon sheets infection
8.Carpal ligament instability (repair &
reconstruction)
9.Surgical treatment of Carpal bones non union
10.Surgical treatment of Arthritic Wrist and
hand(proximal) row carpectomy, radial & ulnar
shortening and lengthening Savue – Kapandji,
limited Arthrodesis triscaphoid, STT)
11.Stabilization of the DRUJ
12.Surgery for the TFCC Pathology
13.Trigger finger, Mallet Finger, Dequarvian
(stenosing tenosynovitis)
(stenosing Tenosynvoitis)
14.Dupuytren Release
15.CM CJ, M CPJ, IPJ Replacement, and ligament
repair.
Repair
CATEGORY VII: PELVIS AND HIP SURGERY
1.Closed reduction with clamp / Fix Pelvic Ring
disruptions
2. Fixation of Pelvic Ring Disruptions with S.I.
Screws / Plates
3.Fixation of Acetabular fracture through
inoinguinal Approach
4.Fixation of Acetabular fracture through
Kocher – Lanenaeck Approach
5.Fixation of A cetabular fracture through
extensile iliofermal approach
6.Periacetabular osteotom y (Adult)
7.Proximal femoral osteotomy (Adult)
8.Arthrodesis of hip joint
9.Cemented total Arthroplasty of Hip
10.Cementless total Arthroplasty of Hip
11.Surface Replacement / Hybrid Athroplasty of
Hip
Requested Recommended Not
Privileges (To be completed
by (For committee use) Recommended
the applicant) (For committee use)
Name of applicant……………
Page 7 of 10
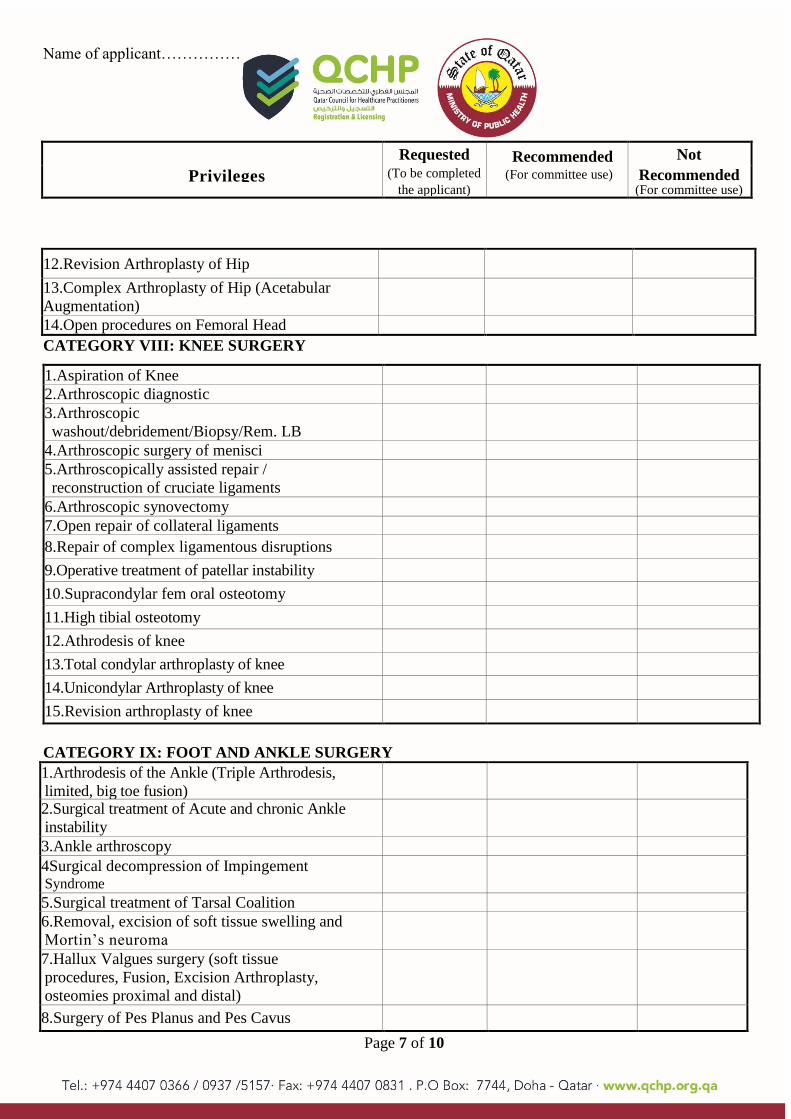
CATEGORY VIII: KNEE SURGERY
1.Aspiration of Knee
2.Arthroscopic diagnostic
3.Arthroscopic
washout/debridement/Biopsy/Rem. LB
4.Arthroscopic surgery of menisci
5.Arthroscopically assisted repair /
reconstruction of cruciate ligaments
6.Arthroscopic synovectomy
7.Open repair of collateral ligaments
8.Repair of complex ligamentous disruptions
9.Operative treatment of patellar instability
10.Supracondylar fem oral osteotomy
11.High tibial osteotomy
12.Athrodesis of knee
13.Total condylar arthroplasty of knee
14.Unicondylar Arthroplasty of knee
15.Revision arthroplasty of knee
CATEGORY IX: FOOT AND ANKLE SURGERY
1.Arthrodesis of the Ankle (Triple Arthrodesis,
limited, big toe fusion)
2.Surgical treatment of Acute and chronic Ankle
instability
3.Ankle arthroscopy
4Surgical decompression of Impingement Syndrome
5.Surgical treatment of Tarsal Coalition
6.Removal, excision of soft tissue swelling and
Mortin’s neuroma
7.Hallux Valgues surgery (soft tissue
procedures, Fusion, Excision Arthroplasty,
osteomies proximal and distal)
8.Surgery of Pes Planus and Pes Cavus
12.Revision Arthroplasty of Hip
13.Complex Arthroplasty of Hip (Acetabular
Augmentation)
14.Open procedures on Femoral Head
Requested Recommended Not
Privileges (To be completed
by (For committee use) Recommended
the applicant) (For committee use)

Page 8 of 10
9.Surgery of Hammer toes, claw Toes and
mallet toes, soft tissue and bony procedure
10.Surgical treatment of Ankle Tendons and
fascia (Posterior and anterior Tibial, Peroneal
and Achilles Tendon, planter fascia pathology)
11.Ingrown toenail operation
12.Lesser toe fusion 13.Calcaneal spur excision
14.Steidler operation for foot
CATEGORY X: Amputations
Upper Extremity
1. Disarticulation at Shoulder
2.Transarticular Amputation of Elbow 3.Amputation of Elbow
4.Amputation of Wrist 5.Amputation of Hand
6.Amputation of Digits
Lower
1. Disarticulation at Hip
2. Transarticular Amputation of Knee 3. Fore / Hind Quarter Amputation
4.Above Knee Amputation
5.Below Knee Amputation
6.Amputations around Ankle
7.Amputations through Tarsus
8.Amputations through Metacarpals /
Metatarsals
9.Ray Amputations
10.Amputations/ Terminalisations through
Phalanges
11.Soft tissue release around hip, knee, ankle and
foot in CP
12.Graf method for diagnosis of DDH with USG
Requested Recommended Not
Privileges (To be completed
by (For committee use) Recommended
the applicant) (For committee use)
Name of applicant……………
Page 9 of 10
CATEGORY XI: ADDITIONAL PRIVILEGES (not included above)
Note: If additional privilege(s) are desired, please indicate this in the space provided above. You must submit
along with this application a necessary document(s) to support your request. If documentation is incomplete,
your request will not be accepted.
By signing below, I acknowledge that I have read, understand, and agree to abide by QCHP standards for
privileging. I have requested only those privileges for which by education, training, current experience and
demonstrated performance I am qualified to perform and wish to exercise, and I understand that:
a) In exercising any clinical privileges granted, I am constrained by QCHP's policies and rules applicable
generally and any applicable to the particular situation.
b) Any restriction on the clinical privileges granted to me is waived in an emergency situation and in such
situation my actions are governed by the recognized policies and rules.
………………………………………………….. …………………………
Applicant’s signature (Stamp if any) Date
………………………………………………….. …………………………
1. Medical Director (of the facility the applicant Date will perform surgeries in) Stamp & Signature
………………………………………………….. …………………………
2. Medical Director (of the facility the applicant Date will perform surgeries in) Stamp & Signature
………………………………………………….. …………………………
3. Medical Director (of the facility the applicant Date will perform surgeries in) Stamp & Signature
Requested Recommended Not
Privileges (To be completed
by (For committee use) Recommended
the applicant) (For committee use)

Page 10 of 10
Name of applicant……………
For Committee use only
Evaluation Committee Chairman:
I have reviewed the requested clinical privileges and supporting documentation for the above-named applicant and
I have made the above-noted recommendation(s).
………………………………………………….. …………………………
Chairperson’s Stamp & signature Date
Other Committee Members:
………………………………………………….. …………………………
1) Name Date
………………………………………………….. …………………………
2) Name Date


















