Endoscopic endonasal cavernous sinus surgery: An Anatomic study

Neurosurg Focus / Volume 32 / June 2012
Neurosurg Focus 32 (6):E5, 2012
1
The endoscopic endonasal transpterygoid approach has been used to gain exposure for a variety of skull base lesions. This approach was first used
as an alternative to transfacial or sublabial approaches to access benign tumors in the PPF.20 However, with the rapid growth of endoscopic skull base surgery in the past decade through advances in imaging technology, instru-mentation, and surgical techniques, and with increased cooperation between neurosurgeons and otolaryngolo-gists, the number of lesions that are accessible using an endoscopic transpterygoid approach has increased con-siderably. Additionally, this procedure has now been reported to allow access to lesions in the infratemporal fossa, Meckel cave, petrous apex, and lateral sphenoid si-nus.2,7,16–18,28,37 One of the more well-defined applications of this approach is its use to access the lateral recess of the sphenoid sinus.1,3,5,6,11,21,34 Accessing the lateral sphe-
noid sinus and its recess may be necessary in the manage-ment of sinonasal tumors (both benign and malignant) as well as in the repair of spontaneous or congenital menin-goencephaloceles from this region.
Traditional microsurgical transsphenoidal approach-es may not adequately expose these so-called far-lateral encephaloceles located in the lateral recess of the sphe-noid sinus. This is due to the strictly midline nature of the exposure as well as the limited visibility and maneuver-ability restricted by an obstructing nasal speculum. Open frontotemporal transcranial approaches often require temporal lobe retraction, and transfacial approaches in-volve facial incisions and osteotomies to access these lateral sphenoid encephaloceles of the Sternberg canal. The primary advantage of the endoscopic endonasal transpterygoid approach is its ability to offer maximal exposure and panoramic visualization of encephaloceles in the far-lateral recesses of the sphenoid sinus without the risk of complications associated with brain retraction or facial osteotomies. The direct access given to these
Surgical nuances for the endoscopic endonasal transpterygoid approach to lateral sphenoid sinus encephaloceles
RichaRd F. Schmidt, B.a.,1 OSamah J. chOudhRy, B.a.,1 JOSeph Raviv, m.d.,2 SOly BaRedeS, m.d.,3 ROy R. caSianO, m.d.,4 Jean andeRSOn elOy, m.d.,1,3,5 and JameS K. liu, m.d.1,3,5
Departments of 1Neurological Surgery and 3Otolaryngology—Head & Neck Surgery, and 5Center for Skull Base and Pituitary Surgery, Neurological Institute of New Jersey, University of Medicine and Dentistry of New Jersey—New Jersey Medical School, Newark, New Jersey; 2Division of Otolaryngology, NorthShore University HealthSystem, Evanston Hospital, Evanston, Illinois; and 4Department of Otolaryngology—Head & Neck Surgery, Leonard Miller School of Medicine, University of Miami, Florida
Lateral sphenoid encephaloceles of the Sternberg canal are rare entities and usually present with spontaneous CSF rhinorrhea. Traditionally, these were treated via transcranial approaches, which can be challenging given the deep location of these lesions. However, with advancements in endoscopic skull base surgery, including improved surgical exposures, angled endoscopes and instruments, and novel repair techniques, these encephaloceles can be resected and successfully repaired with purely endoscopic endonasal approaches. In this report, the authors review the endoscopic endonasal transpterygoid approach to the lateral recess of the sphenoid sinus for repair of temporal lobe encephaloceles, including an overview of the surgical anatomy from an endoscopic perspective, and describe the technical operative nuances and surgical pearls for these cases. The authors also present 4 new cases of lateral sphenoid recess encephaloceles that were successfully treated using this approach.(http://thejns.org/doi/abs/10.3171/2012.3.FOCUS1267)
Key WORdS • endoscopic endonasal transpterygoid approach • lateral sphenoid encephalocele • Sternberg canal • nasoseptal flap • cerebrospinal fluid rhinorrhea • lateral sphenoid defect • lateral sphenoid recess • endoscopic skull base surgery
1
Abbreviations used in this paper: PNSF = pedicled nasoseptal flap; PPF = pterygopalatine fossa; SPA = sphenopalatine artery.
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

R. F. Schmidt et al.
2 Neurosurg Focus / Volume 32 / June 2012
laterally based encephaloceles through this approach also permits increased surgical maneuverability. Repair of CSF leaks arising from these encephaloceles can be safely and effectively performed with meticulous mul-tilayered reconstruction, with or without a vascularized PNSF. In this paper, we review the endoscopic endonasal transpterygoid approach for treatment of lateral sphenoid sinus encephaloceles, and describe the operative nuances and surgical pearls associated with this technique. The endoscopic surgical anatomy is illustrated, along with 4 additional cases that are new to the literature.
Surgical TechniqueSurgical Considerations
For endoscopic endonasal skull base procedures, we prefer to use a dual-surgeon approach, with a skull base neurosurgeon and an otolaryngologist specializing in rhi-nology, sinus, and endoscopic skull base surgery. We use a bimanual binostril technique, permitting 3 to 4 instru-ments to be used simultaneously throughout the proce-dure. Furthermore, by using a dual-surgeon approach, one surgeon can provide continuous dynamic manipulation of the endoscope and appropriate retraction when necessary, while the other can perform traditional 2-handed micro-surgery in which endoscopic visualization of the surgical target is used. This strategy allows for maximal visualiza-tion throughout the entire procedure, improving depth of perception and permitting immediate reactionary changes in camera positioning that might be necessary throughout various components of the procedure.23–27 Using 2 sur-geons, as opposed to a single “one-handed” surgeon hold-ing the endoscope, also allows for more bimanual freedom of surgical maneuverability, which is of paramount impor-tance in performing fine microdissection in deep critical targets of the skull base.
After the induction of general anesthesia, the patient is given 10 mg of dexamethasone, 50 mg of diphenhydr-amine, and 1.5 mg of cefuroxime. For the treatment of spontaneous CSF leaks and encephaloceles, we place a lumbar drain at the start of the case and infuse intrathe-cal fluorescein through the drain according to a proto-col previously described by Tabaee and colleagues35 and Placantonakis et al.30 Ten milliliters of CSF is withdrawn from the lumbar drain and mixed with 25 mg of fluo-rescein (0.25 ml of injectable 10% solution; Akorn, Inc.), and then slowly injected back into the lumbar drain. This brilliant yellow indicator facilitates direct endoscopic vi-sualization and localization of the site of origin as well as the direction of flow of the CSF leak. It is important to inspect for multiple encephaloceles during endoscopic exploration. This technique is also useful for intraopera-tive assessment of adequate repair, because the absence of any further visible fluorescein correlates strongly with a low risk of postoperative CSF leak.35
Patient PositioningProper positioning of the patient is crucial to en-
abling this dual-surgeon approach. For combined endo-scopic endonasal skull base cases, we typically secure
the endotracheal tube on the patient’s left side, allowing both surgeons access to the patient from the right. The pa-tient’s head is stabilized using a 3-point Mayfield frame. The head is slightly rotated toward the right and laterally bent to the left shoulder so that the patient’s face is point-ing toward the surgeon standing on the right side. Image guidance using fine-cut CT scans is used for anatomical localization. We typically prepare the patient’s thigh and/or abdomen so that autologous fat or fascia lata can be harvested for graft reconstruction of the skull base defect, if needed.
The nose and nasal cavity are prepared with povi-done-iodine, followed by placement of Afrin-soaked pledgets to decongest the nasal passages. The uncinate process, sphenopalatine foramen region, and the tail and anterosuperior attachment of the middle turbinate are in-filtrated with 1% lidocaine with 1:100,000 of epinephrine solution for vasoconstriction.
Endoscopic Endonasal Approach to Sphenoid and Maxillary Sinuses
Using a 30° endoscope, the nostril ipsilateral to the encephalocele is explored. The middle turbinate is re-moved using a straight Thru Cut forceps. A posterior sep-tectomy or septotomy is then performed with endoscopic rongeurs and a microdebrider. These 2 steps enhance maximal maneuverability for the dual-surgeon, 4-instru-ment approach through binostril routes. Access through the contralateral nasal cavity allows a cross-court ap-proach that provides a direct path for straight instruments to the lateral sphenoid recess. If a high-flow CSF leak and/or a large skull base defect is being repaired, we prefer to harvest a unilateral vascularized PNSF during the initial exposure of the sphenoid sinus for later reconstruction of the skull base defect. The operative details of harvest-ing the PNSF are described elsewhere.14,19 The PNSF is stored in the nasopharynx throughout the procedure until later use. It is important not to violate or traumatize the PNSF and its vascular pedicle during the operation, to maximize its potential in preventing postoperative CSF fistula formation.13
The approach begins with resection of the uncinate process and identification of the natural ostium of the maxillary sinus. This is usually performed using a 30° rigid endoscope. The maxillary sinus ostium is subse-quently widened posteriorly in the region of the posterior fontanel of the maxillary sinus until its posterior wall is reached. A total ethmoidectomy is then performed by se-quentially resecting the ethmoid bulla, suprabullar cells, and the posterior ethmoid cells by transgressing the basal lamella (also called the third or ground lamella; this struc-ture separates the anterior ethmoid cells from the pos-terior ethmoid cells) of the ethmoid sinus. The sphenoid sinus is then entered via an inferomedial transethmoidal approach. The sphenoidotomy should be widely enlarged to allow maximal exposure and permit optimal maneu-verability within the sinus. If a PNSF has not yet been harvested at this point, care should be taken while enlarg-ing the sphenoid sinus inferiorly to prevent injury to the vascular pedicle of the flap, which courses just inferior to the sphenoid sinus ostium. Although we do not routinely
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

Neurosurg Focus / Volume 32 / June 2012
Endoscopic transpterygoid repair of lateral sphenoid encephalocele
3
use a PNSF for small defects, if a large defect is expected, an attempt is made to preserve the vascular pedicle of the PNSF. In cases in which the vascular pedicle cannot be preserved and a large defect is noted after the resection portion of the case, the contralateral PNSF may be an op-tion. If significant inferior pneumatization of the lateral sphenoid sinus recess into the pterygoid plates is noted, the inferior turbinate may be removed to allow maximal visualization of the posterior wall of the maxillary sinus and adequate inferolateral access to the recess (although this is rarely needed in our experience). Next, the mucosa of the posterior wall and roof of the maxillary sinus is elevated to permit access to the PPF through the postero-medial wall of the maxillary sinus.
Transpterygoid Approach to the Lateral Sphenoid SinusTo obtain full visualization of the PPF and associ-
ated neurovascular structures, the orbital process of the palatine bone and the posteromedial wall of the maxil-lary sinus must be removed. The contents of the PPF in-clude the internal maxillary artery, which gives rise to the SPA (Fig. 1), the descending palatine artery, the pos-terosuperior alveolar artery, the pterygopalatine ganglion, and the infraorbital nerve. The anterior compartment of the PPF contains the vascular structures and fat, whereas the posterior compartment contains the neuronal struc-tures.12 The contents of the PPF must be retracted later-ally to allow exposure of the lateral wall of the sphenoid sinus and further bone dissection. The sphenoid process of the palatine bone must be removed, followed by the
medial pterygoid plate. This can be achieved using pow-ered instrumentation (such as a high-speed drill) or Ker-rison rongeurs. The vidian nerve may be identified and preserved by exposing it at the junction of the medial pterygoid plate and floor of the sphenoid sinus. This is best accomplished by limiting drilling to the inferior por-tion of the medial pterygoid plate. Although this nerve may be sacrificed, it can be used as a helpful tool in iden-tifying the internal carotid artery in more complex cases when followed posteriorly.37 With successful drilling of the pterygoid process, the lateral recesses of the sphenoid sinus should be widely exposed, with sufficient room to access and repair the skull base defect. While dissecting through the medial aspect of the PPF, the SPA will be encountered as it exits the sphenopalatine foramen. The SPA provides vascular supply to the ipsilateral PNSF. Often, this artery cannot be preserved while dissecting the PPF, which will make an ipsilateral nasoseptal flap avascular.
Resection of Encephalocele and Skull Base ReconstructionOnce the lateral recess of the sphenoid sinus is ex-
posed, the lateral sphenoid encephalocele is identified us-ing angled endoscopes, with the aid of image guidance. Active CSF egress can be identified by intraoperative visualization of fluorescein. Smaller encephaloceles can be shrunk with bipolar cautery, whereas larger enceph-aloceles presenting with neural masses in the sphenoid sinus may need to be debulked with a suction-rotation microdebrider. In the majority of cases, the encephalo-cele consists of nonfunctional neural tissue, which can be removed without neurological consequences. This is more true in cases with very small dural and bony defects (narrow-necked encephaloceles) despite the size of the in-tranasal encephalocele. Once the encephalocele is mini-mized down to the level of the bony skull base defect, he-mostasis is carefully obtained and the edges of the bony and dural defects are defined with an angled dissector or curette. It is important to denude the sphenoid sinus of all mucosa, especially around the bony skull base defect, to prevent intracranial entrapment of sinonasal mucosa, which can lead to late development of an intracranial mucocele.9 Removal of the sphenoid sinus mucosa also prevents mucosal secretions from separating the grafting material from the underlying bone (a phenomenon that can lead to repair failure). A small moist pledget is care-fully pushed into the defect by using a dull probe (frontal sinus probe or maxillary sinus seeker) to define the edges clearly and to provide enough space for placement of an underlay graft.
The method for closure of lateral sphenoid sinus en-cephaloceles largely depends on the size of the defect be-ing repaired. In general, this is accomplished with mul-tilayered free tissue grafts for smaller defects or a multi-layer method that includes a PNSF for larger defects with high-flow CSF leaks. In smaller defects (≤ 1 cm2), layers of Gelfoam (Pharmacia) or autologous fat buttressed by local rigid cartilaginous, bony, or synthetic grafts with an overlay of tissue sealant (Tisseel or Duraseal) have been reported, and should be sufficient to close the defect and prevent postoperative CSF leaks.17,36 Alternatively, an au-
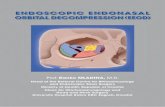
Fig. 1. A: Axial CT scan showing the PPF (yellow circle) with the lateral sphenoid recess posterolateral to the space. The red arrow depicts the trajectory through the PPF to get to the lateral sphenoid recess. B–D: Photographs of cadaveric dissections. B: The initial approach after a left maxillary antrostomy and left sphenoid sinus-otomy. Note the freer elevator dissecting the soft tissue overlying the medial pterygoid plate. C: After soft-tissue elevation medial to the medial pterygoid plate, the SPA and the sphenopalatine foramen (blue circular dotted line) are exposed. D: After drilling the pterygoid plates, the PPF contents are exposed as well as the contents of the infratem-poral fossa. Although the infratemporal fossa contents are dissected for demonstration purposes, this is not needed during the transpterygoid approach to the lateral sphenoid recess. IMA = internal maxillary ar-tery; V2 = maxillary division of trigeminal nerve.
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

R. F. Schmidt et al.
4 Neurosurg Focus / Volume 32 / June 2012
tologous fat graft can also be used to pack the sphenoid sinus to buttress the defect repair. Larger defects (> 1 cm2) with high-flow CSF leaks may require multilayered watertight closure with a PNSF, or with a free mucosal overlay graft.
At our institution, for small defects we prefer to use an initial layer of thin acellular dermal allograft (Life-Cell Corp.) to plug the defect. The allograft is pushed into the defect by using a blunt angled probe, followed by gentle pressure exerted using a cottonoid pledget. At this juncture, no visible fluorescein-tinged CSF extravasation should be present. A second layer of thick implantable acellular dermal allograft is subsequently used to cover the initial graft. Gentamicin-soaked Gelfoam pledgets are then used to cover and buttress the grafts. For larger defects, we prefer to use an initial underlay graft using either autologous fascia lata or thick implantable acellu-lar dermal allograft. This initial layer is covered with a monolayer of Surgicel (Ethicon, Inc.). A second layer of fascia lata or acellular dermal allograft is used, followed by placement of the previously harvested PNSF. Details of proper placement of grafting materials have been well established.13,14,23,24 Although in our earlier cases we fre-quently used dural sealants over the PNSF at this junc-ture, we have found no significant advantage to their use in a recent retrospective study, and have discontinued this practice.8 The grafts are subsequently covered with multiple layers of gentamicin-soaked Gelfoam pledgets and bolstered and buttressed with a bacitracin-covered expandable Merocel nasal tampon, which is inflated with gentamicin solution.
Postoperative ManagementAs with all skull base defect repairs, limiting ac-
tivities that increase intracranial pressure is crucial to maintaining closure and preventing the formation of postoperative CSF fistulas. Patients are thus asked to avoid activities such as sneezing and straining, and are placed on stool softeners. In our practice, the patient is maintained on postoperative antibiotics (cephalosporin or b-lactamase–resistant penicillin) until the packing is re-moved approximately 10 days later in an outpatient visit. Last, the patient should be educated regarding the signs of postoperative CSF leak or infection, such as clear rhinor-rhea, postnasal drip, fever, nuchal rigidity, and purulent nasal discharge, and should be closely observed. We typi-cally remove the lumbar drain at the end of the surgery so that the patient is encouraged to mobilize earlier to avoid thromboembolic and pulmonary complications. The pa-tients are usually discharged on postoperative Day 1 or 2. Postoperative follow-up consists of clinical examina-tions and direct nasal endoscopy to assess for CSF leak and to ensure successful repair and mucosalization of the graft; visits are scheduled at approximately 1, 3, 8, and 12 weeks, and then every 6 months after surgery.
Illustrative CasesCase 1
This 52-year-old woman with a history of head trau-ma presented with recurrent right-sided CSF rhinorrhea
and was admitted to another hospital for meningitis. On nasal endoscopy, a gray, right-sided sinonasal mass sug-gestive of an encephalocele was found. A CT scan of the paranasal sinuses showed a right-sided sinonasal mass extending to the frontal sinus as well as an encephalocele in the left lateral sphenoid recess (Fig. 2). The patient un-derwent endoscopic resection of the encephaloceles and reconstruction of the skull base defects. The encephalo-cele in the left lateral sphenoid recess was repaired using a layer of thin acellular dermal allograft to tuck the small defect, followed by a layer of thick implantable dural al-lograft. The allografts were covered with gentamicin-soaked Gelfoam pledgets, and buttressed with Merocel nasal packing covered with bacitracin. The patients’ post-operative course was unremarkable. She was aymptom-atic and well healed at her 6-month follow-up and was lost to follow-up afterward.
Case 2This 58-year-old woman presented with spontaneous
CSF rhinorrhea from the left nostril. A CT and MRI ses-sion demonstrated a left lateral sphenoid encephalocele arising from the mesial temporal lobe and extravasat-ing through a skull base defect (Fig. 3). An endoscopic transpterygoid approach was performed to expose the lateral recess of the left sphenoid sinus (Fig. 4). A large encephalocele was identified and debulked down to the skull base defect with a rotation-suction microdebrider. Using a 30° and 70° endoscope, the defect was repaired with a small piece of thick implantable acellular dermal allograft tucked as an inlay graft, followed by a vascular-ized PNSF. There was no evidence of active fluorescein extravasation at the end of the repair. Postoperatively, the patient was neurologically intact, with no further evi-dence of CSF leakage after 14 months of follow-up.
Fig. 2. Case 1. Axial (A) and coronal (B) CT scans demonstrating a left middle fossa skull base defect from an encephalocele in the left lateral sphenoid recess. There is opacification of the left sphenoid si-nus from the encephalocele. C: Intraoperative endoscopic view dem-onstrating a small defect in the left lateral sphenoid recess, with CSF extravasation of fluorescein dye. D: Intraoperative endoscopic view showing initial closure of the defect performed using a thin acellular dermal allograft.
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

Neurosurg Focus / Volume 32 / June 2012
Endoscopic transpterygoid repair of lateral sphenoid encephalocele
5
Case 3This 59-year-old woman presented with intermittent
CSF rhinorrhea from the left nostril shortly after having undergone a craniotomy on the left side for removal of an intracranial mucocele at another hospital. A left-sided lat-eral sphenoid encephalocele extruding through a medial middle fossa defect was confirmed on a CT cisternogram, which showed extravasation of dye into the left sphenoid encephalocele (Fig. 5). Testing of the CSF also confirmed positivity for b2-transferrin. The patient was referred to our center, where an endoscopic transpterygoid approach was performed. The encephalocele was identified with 30° and 70° endoscopes. The defect was repaired with acellular dermal allograft followed by an autologous fat graft in the sphenoid sinus. Postoperatively, the patient
was neurologically intact, with no further evidence of CSF leakage after 12 months of follow-up.
Case 4This 58-year-old, obese woman with a history of be-
nign intracranial hypertension presented with clear, in-termittent, right-sided CSF rhinorrhea that was positive for b2-transferrin. She had a long history of chronic head-aches and chronic sinusitis, with 3 previous endoscopic sinus surgeries. Interestingly, her headaches improved once the CSF leak began. The MRI studies demonstrated a lateral sphenoid encephalocele with opacification of the right sphenoid sinus. A partial empty sella was also identified, which was consistent with her history of be-nign intracranial hypertension. A CT cisternogram con-firmed the pathway of the CSF leak (Fig. 6). Because of the underlying intracranial hypertension, we thought that direct repair without long-term CSF diversion would pose a high risk of postoperative CSF leakage. We therefore performed an initial ventriculoperitoneal shunt insertion followed by endoscopic repair of the CSF leak and skull base defect via an endonasal transpterygoid approach. A small defect was identified, with a herniation of neural
Fig. 3. Case 2. Axial (A) and coronal (B) CT scans demonstrating a left middle fossa skull base defect from an encephalocele in the left lat-eral sphenoid recess. Axial (C) and coronal (D) T2-weighted MRI stud-ies demonstrating hyperintense opacification in the left sphenoid sinus.
Fig. 4. Case 2. Intraoperative views of the endoscopic transptery-goid approach. A: Extravasation of fluorescein-tinged CSF arising from the skull base defect in the lateral recess of the left sphenoid si-nus. B: A thick acellular dermal allograft is placed as an inlay graft to plug the defect initially. C: Panoramic endoscopic view demonstrating the left maxillary sinus, left sphenoid sinus, and drilled pterygoid pro-cess. D: The PNSF is rotated over the skull base repair.
Fig. 5. Case 3. Coronal (A) and axial (B) CT scans demonstrating a left middle fossa skull base defect from an encephalocele in the left lateral sphenoid recess. The CT cisternogram (A) demonstrates ex-travasation of contrast into the encephalocele. Coronal (C) and axial (D) T2-weighted MRI studies demonstrating hyperintense opacification in the left sphenoid sinus.
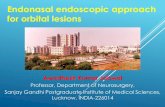
Fig. 6. Case 4. Coronal CT cisternogram (left) and axial T2-weight-ed MRI study (right) demonstrating a right middle fossa skull base de-fect (green arrow) from an encephalocele in the right lateral sphenoid recess (asterisk). LPP = lateral pterygoid plate; MPP = medial pterygoid plate.
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

R. F. Schmidt et al.
6 Neurosurg Focus / Volume 32 / June 2012
tissue extravasating CSF. The encephalocele was ampu-tated with a pituitary rongeur and the defect was repaired with a collagen-based dural allograft inlay, followed by Surgicel to plug the dural defect. A free mucosal graft was used as an overlay to cover the skull base defect, and was further buttressed with an autologous fat graft placed in the sphenoid sinus. Postoperatively, the patient was neurologically intact, with no further evidence of CSF leakage after 42 months of follow-up.
DiscussionEncephaloceles of the lateral sphenoid sinus are rel-
atively rare. Large encephaloceles are commonly diag-nosed in utero or at birth as the product of a large neural tube defect in embryogenesis. However, smaller encepha-loceles may go unnoticed for years or spontaneously oc-cur as a result of trauma, iatrogenic injury, or skull base erosion from inflammatory and neoplastic processes. These disorders may also occur spontaneously as the result of increased intracranial pressure forcing neural tissue through a congenitally weakened portion of the sphenoid bone. Congenital defects causing a persistent craniopharyngeal tract in the lateral sphenoid sinus are exceedingly rare, but tend to be the result of incomplete fusion of the embryonic precursors to the sphenoid bone. This bone is formed from the fusion of 5 cartilaginous plates that undergo independent endochondral ossifica-tion during embryogenesis before fusing.31 Most com-monly, the presphenoid and basisphenoid fail to fuse with the greater wings of the sphenoid bone, which leads to a persistent lateral craniopharyngeal canal known as the Sternberg canal,4 after the physician who first described it in 1888.32,33 Patients with encephaloceles of the lateral sphenoid sinus may present with headache, imbalance or dizziness, unilateral clear rhinorrhea, diplopia, or menin-gitis.5 Additionally, patients with this defect may be com-pletely asymptomatic, and this lesion might go undiag-nosed until it appears as an incidental finding on imaging studies. Regardless, patients with lateral sphenoid sinus encephaloceles should be evaluated for surgical repair to relieve symptoms and reduce the risk for later complica-tions such as meningitis.
Due to their anatomical location deep within the skull base, encephaloceles of the lateral sphenoid sinuses can be challenging to reach with traditional microsurgi-cal transnasal and transfacial approaches. Traditionally, these lesions were accessed by more standard approaches, including the classic midline transseptal transsphenoidal approach, LeFort I transmaxillary approach, and the fron-totemporal–anterior middle cranial fossa approach.15,22 However, these approaches may result in more diffi-culty in accessing encephaloceles in patients who have far-lateral pneumatization of the sphenoid sinus, an ana-tomical variant seen in approximately 22%–40% of indi-viduals.22,29,38 Since this variant also carries an increased risk for encephalocele formation,36 the ability to access this region is a cornerstone of endoscopic management of sphenoid encephaloceles. Alternatively, an extradural frontotemporal approach (with or without intradural ex-ploration) with gentle brain retraction can be readily per-
formed for exposure of lateral sphenoid encephaloceles. The associated temporal encephalocele can be amputated and the dehiscent dura mater and skull base defect can be repaired with autologous tissue grafts.22
Initial attempts at repairing skull base defects in the lateral sphenoid sinus via a midline microsurgical trans-sphenoidal approach were associated with a high rate of failure because of poor visualization of these defects.22 In most cases, the laterally based defect of the Sternberg canal is situated beyond the line of sight of the speculum-based exposure. Wider exposures can be obtained with traditional extracranial transfacial approaches, such as the LeFort I osteotomy. However, these may be associ-ated with postoperative malocclusion or traction neura-praxia of the infraorbital nerves as well as injury to the hard palate and upper alveolar region affecting the neuro-vascular supply to the teeth.21 The endoscopic endonasal transpterygoid approach offers several advantages, in-cluding avoidance of a craniotomy and brain retraction, excellent panoramic visualization of the lateral sphenoid recess, improved illumination, and increased surgical freedom for maneuverability of surgical instruments by eliminating the traditional nasal speculum. Also, the use of angled endoscopes and instruments is helpful in vi-sualizing and accessing the far-lateral sphenoid sinus. Meticulous multilayered reconstruction is critical to suc-cessful repair of CSF leaks, and the aid of intraoperative fluorescein is vital to ensure that the repair is adequate. The advent of the vascularized PNSF is very effective in repairing larger defects with high-flow CSF leaks due to the robustness and vascularity of the tissue. In our experi-ence with the closure of skull base defects with a PNSF, we have found that the majority of these encephaloceles can be repaired successfully without postoperative CSF diversion, unless of course there is a history of benign intracranial hypertension (as in Case 4).10
ConclusionsThe endoscopic endonasal transpterygoid approach
enables excellent visualization and surgical access to en-cephaloceles arising from the lateral recess of the sphenoid sinus. These lesions can be safely resected and effective-ly repaired with a variety of multilayered reconstruction techniques, including the use of a vascularized PNSF if necessary. Although other transcranial and transfacial ap-proaches have been successfully performed in the past, the endoscopic endonasal transpterygoid approach offers direct access to these lesions with no brain retraction, de-creased operative risks, and improved cosmetic outcome.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript prepara-tion include the following. Conception and design: Liu, Eloy. Acquisition of data: Liu, Schmidt, Choudhry, Eloy. Analysis and interpretation of data: Liu, Schmidt, Raviv, Baredes, Casiano, Eloy. Drafting the article: Schmidt, Choudhry. Critically revising the article: all authors. Reviewed submitted version of manuscript: all
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

Neurosurg Focus / Volume 32 / June 2012
Endoscopic transpterygoid repair of lateral sphenoid encephalocele
7
authors. Approved the final version of the manuscript on behalf of all authors: Liu. Administrative/technical/material support: Liu, Choudhry, Eloy. Study supervision: Liu.
Acknowledgment
The authors gratefully thank Pratik A. Shukla, B.A., for his technical assistance.
References
1. Al-Nashar IS, Carrau RL, Herrera A, Snyderman CH: Endo-scopic transnasal transpterygopalatine fossa approach to the lateral recess of the sphenoid sinus. Laryngoscope 114:528–532, 2004
2. Al-Sheibani S, Zanation AM, Carrau RL, Prevedello DM, Prokopakis EP, McLaughlin N, et al: Endoscopic endona-sal transpterygoid nasopharyngectomy. Laryngoscope 121: 2081–2089, 2011
3. Bachmann-Harildstad G, Kloster R, Bajic R: Transptery-goid trans-sphenoid approach to the lateral extension of the sphenoid sinus to repair a spontaneous CSF leak. Skull Base 16:207–212, 2006
4. Bendersky DC, Landriel FA, Ajler PM, Hem SM, Carrizo AG: Sternberg’s canal as a cause of encephalocele within the lat-eral recess of the sphenoid sinus: a report of two cases. Surg Neurol Int 2:171, 2011
5. Bolger WE: Endoscopic transpterygoid approach to the lateral sphenoid recess: surgical approach and clinical experience. Otolaryngol Head Neck Surg 133:20–26, 2005
6. Castelnuovo P, Dallan I, Pistochini A, Battaglia P, Locatelli D, Bignami M: Endonasal endoscopic repair of Sternberg’s canal cerebrospinal fluid leaks. Laryngoscope 117:345–349, 2007
7. Cavallo LM, Messina A, Gardner P, Esposito F, Kassam AB, Cappabianca P, et al: Extended endoscopic endonasal ap-proach to the pterygopalatine fossa: anatomical study and clinical considerations. Neurosurg Focus 19(1):E5, 2005
8. Eloy JA, Choudhry OJ, Friedel ME, Kuperan AB, Liu JK: Endoscopic nasoseptal flap repair of skull base defects: Is ad-dition of a dural sealant necessary? Otolaryngol Head Neck Surg [epub ahead of print], 2012
9. Eloy JA, Fatterpekar GM, Bederson JB, Shohet MR: Intracra-nial mucocele: an unusual complication of cerebrospinal fluid leakage repair with middle turbinate mucosal graft. Otolar-yngol Head Neck Surg 137:350–352, 2007
10. Eloy JA, Kuperan AB, Choudhry OJ, Harirchian S, Liu JK: Efficacy of the pedicled nasoseptal flap without cerebrospinal fluid (CSF) diversion for repair of skull-base defects: inci-dence of postoperative CSF leaks. Int Forum Allergy Rhinol [epub ahead of print], 2012
11. Forer B, Sethi DS: Endoscopic repair of cerebrospinal fluid leaks in the lateral sphenoid sinus recess. Clinical article. J Neurosurg 112:444–448, 2010
12. Fortes FS, Sennes LU, Carrau RL, Brito R, Ribas GC, Yasuda A, et al: Endoscopic anatomy of the pterygopalatine fossa and the transpterygoid approach: development of a surgical in-struction model. Laryngoscope 118:44–49, 2008
13. Gardner P, Kassam A, Snyderman C, Mintz A, Carrau R, Moossy JJ: Endoscopic endonasal suturing of dural recon-struction grafts: a novel application of the U-Clip technology. Technical note. J Neurosurg 108:395–400, 2008
14. Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH, et al: A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope 116:1882–1886, 2006
15. Har-El G: Combined endoscopic transmaxillary-transnasal approach to the pterygoid region, lateral sphenoid sinus, and retrobulbar orbit. Ann Otol Rhinol Laryngol 114:439–442, 2005
16. Hofstetter CP, Singh A, Anand VK, Kacker A, Schwartz TH:
The endoscopic, endonasal, transmaxillary transpterygoid approach to the pterygopalatine fossa, infratemporal fossa, petrous apex, and the Meckel cave. Clinical article. J Neuro-surg 113:967–974, 2010
17. Hosseini SM, Razfar A, Carrau RL, Prevedello DM, Fernan-dez-Miranda J, Zanation A, et al: Endonasal transpterygoid approach to the infratemporal fossa: correlation of endoscopic and multiplanar CT anatomy. Head Neck 34:313–320, 2012
18. Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R: Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neuro-surg Focus 19(1):E6, 2005
19. Kassam AB, Thomas A, Carrau RL, Snyderman CH, Vescan A, Prevedello D, et al: Endoscopic reconstruction of the cra-nial base using a pedicled nasoseptal flap. Neurosurgery 63 (Suppl 1):ONS44–ONS52, 2008
20. Klossek JM, Ferrie JC, Goujon JM, Fontanel JP: Endoscopic approach of the pterygopalatine fossa: report of one case. Rhinology 32:208–210, 1994
21. Lai SY, Kennedy DW, Bolger WE: Sphenoid encephaloceles: disease management and identification of lesions within the lateral recess of the sphenoid sinus. Laryngoscope 112:1800–1805, 2002
22. Landreneau FE, Mickey B, Coimbra C: Surgical treatment of cerebrospinal fluid fistulae involving lateral extension of the sphenoid sinus. Neurosurgery 42:1101–1105, 1998
23. Liu JK, Christiano LD, Patel SK, Eloy JA: Surgical nuances for removal of retrochiasmatic craniopharyngioma via the endoscopic endonasal extended transsphenoidal transplanum transtuberculum approach. Neurosurg Focus 30(4):E14, 2011
24. Liu JK, Christiano LD, Patel SK, Tubbs RS, Eloy JA: Surgical nuances for removal of olfactory groove meningiomas using the endoscopic endonasal transcribriform approach. Neuro-surg Focus 30(5):E3, 2011
25. Liu JK, Christiano LD, Patel SK, Tubbs RS, Eloy JA: Surgi-cal nuances for removal of tuberculum sellae meningiomas with optic canal involvement using the endoscopic endonasal extended transsphenoidal transplanum transtuberculum ap-proach. Neurosurg Focus 30(5):E2, 2011
26. Liu JK, Eloy JA: Endoscopic endonasal transplanum trans-tuberculum approach for resection of retrochiasmatic cranio-pharyngioma. Neurosurg Focus (Suppl) 32(1):Video 2, 2012
27. Liu JK, Eloy JA: Expanded endoscopic endonasal transcrib-riform approach for resection of anterior skull base olfactory schwannoma. Neurosurg Focus (Suppl) 32(1):Video 3, 2012
28. McLaughlin N, Bresson D, Ditzel Filho LF, Carrau RL, Kelly DF, Prevedello DM, et al: Vidian nerve neurofibroma removed via a transpterygoid approach. Minim Invasive Neurosurg 54:250–252, 2011
29. Morley TP, Wortzman G: The importance of the lateral exten-sions of the sphenoidal sinus in post-traumatic cerebrospinal rhinorrhoea and meningitis: clinical and radiological aspects. J Neurosurg 22:326–332, 1965
30. Placantonakis DG, Tabaee A, Anand VK, Hiltzik D, Schwartz TH: Safety of low-dose intrathecal fluorescein in endoscopic cranial base surgery. Neurosurgery 61 (3 Suppl):161–166, 2007
31. Ricciardelli EJ: Embryology and anatomy of the cranial base. Clin Plast Surg 22:361–372, 1995
32. Schick B, Brors D, Prescher A: Sternberg’s canal—cause of congenital sphenoidal meningocele. Eur Arch Otorhinolar-yngol 257:430–432, 2000
33. Sternberg M: Ein bisher noch nicht beschriebener Kanal im Keilbein des Menschen. Anat Anz 3:784–785, 1888
34. Tabaee A, Anand VK, Cappabianca P, Stamm A, Esposito F, Schwartz TH: Endoscopic management of spontaneous me-ningoencephalocele of the lateral sphenoid sinus. Clinical ar-ticle. J Neurosurg 112:1070–1077, 2010
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC

R. F. Schmidt et al.
8 Neurosurg Focus / Volume 32 / June 2012
35. Tabaee A, Placantonakis DG, Schwartz TH, Anand VK: Intra-thecal fluorescein in endoscopic skull base surgery. Otolar-yngol Head Neck Surg 137:316–320, 2007
36. Van Alyea OE: Sphenoid sinus: anatomic study, with consid-eration of the clinical significance of the structural character-istics of the sphenoid sinus. Arch Otolaryngol 34:225–253, 1941
37. Vescan AD, Snyderman CH, Carrau RL, Mintz A, Gardner P, Branstetter B IV, et al: Vidian canal: analysis and relationship to the internal carotid artery. Laryngoscope 117:1338–1342, 2007
38. Vidić B: The postnatal development of the sphenoidal sinus and its spread into the dorsum sellae and posterior clinoid pro-
cesses. Am J Roentgenol Radium Ther Nucl Med 104:177–183, 1968
Manuscript submitted February 15, 2012.Accepted March 28, 2012.Please include this information when citing this paper: DOI:
10.3171/2012.3.FOCUS1267. Address correspondence to: James K. Liu, M.D., Department of
Neurological Surgery, Neurological Institute of New Jersey, Univer-sity of Medicine and Dentistry of New Jersey—New Jersey Medical School, 90 Bergen Street, Suite 8100, Newark, New Jersey 07101. email: [email protected].
Unauthenticated | Downloaded 05/24/20 04:42 AM UTC