Surgical Management of Chapter 12 Metastatic Bone...
9
BACKGROUND ■ The humerus is a common site of metastatic bone disease requiring surgery. A metastasis at that site, especially when it involves the dominant extremity, has an immediate and pro- found impact on the affected individual’s ability to perform activities of daily living. The quality of surgery, therefore, is an important factor in restoring vital function. ■ A detailed preoperative clinical and imaging evaluation is mandatory for defining the morphologic characteristics of the lesion and, in turn, establishing the indications for surgical in- tervention, as well as distinguishing between lesions that can be managed with curettage and cemented fixation and those that require resection with endoprosthetic reconstruction. 2,3,5,6 ■ Unlike primary sarcomas of the humerus, metastatic tumors usually have a small soft tissue component, even in the pres- ence of extensive bone destruction. This characteristic allows resection of bony elements only, permitting sparing of the ex- tracortical structures, such as the joint capsule, overlying mus- cles, and muscle attachments, and affords the opportunity to use them to reconstruct and preserve function (FIG 1A,B). To this end, exposure of the proximal humerus is done by split- ting the deltoid muscle rather using the deltopectoral interval, as is done in the case of a primary sarcoma of bone, which ne- cessitates en bloc resection of the deltoid muscle with the tumor. Moreover, a few centimeters of upper limb shortening following resection of bone segment has minimal impact on function, because a slight difference in positioning of that ex- tremity in space can easily compensate for such limb-length discrepancy. ■ In contrast, a similar discrepancy in the lower extremities, which require almost equal length for normal gait, would result in an inevitable limp, the extent of which would be pro- portional to the shortening of the operated extremity. 2 ■ Because of different anatomic and surgical considerations, surgeries around the proximal humerus (type I), humeral dia- physis (type II), and distal humerus (type III) are discussed separately (FIG 2). 1 ANATOMY Proximal Humerus: Type I Metastasis ■ The proximal humerus is covered anteriorly and laterally by the deltoid muscle. ■ The joint capsule encircles the humeral head and attaches to the base of the anatomic neck. ■ The proximal humerus is the attachment site for the rotator cuff muscles. The long head of the biceps muscle crosses the anterior aspect within the bicipital groove. Humeral Diaphysis: Type II Metastasis ■ The upper half is occupied by muscle insertions: ■ Medial aspect: teres major, latissimus dorsi, coraco- brachialis ■ Lateral aspect: pectoralis major, deltoid ■ The radial nerve curves at the back from medial to lateral at the mid-arm level. ■ The lower half is occupied by muscle origins: ■ Medial aspect: Brachialis ■ Lateral aspect: Brachioradialis ■ Neurovascular bundle along its medial aspect Distal Humerus: Type III Metastasis ■ The neurovascular bundle lies along its medial aspect be- tween the biceps and brachialis muscles. ■ The radial nerve lies along its lateral aspect between the brachialis and brachioradialis muscles. INDICATIONS ■ Pathological fracture ■ Impending pathological fracture ■ Intractable pain associated with locally progressive disease that has shown inadequate response to narcotics and preoper- ative radiation therapy ■ Solitary bone metastasis in selected patients IMAGING AND OTHER STAGING STUDIES ■ Plain radiographs of the entire humerus are mandatory to rule out synchronous metastases that may change the extent and technique of surgery. A CT scan of the lesion will clearly define the extents of bone destruction and soft tissue compo- nent. Total body bone scintigraphy is done to detect synchro- nous metastases elsewhere in the skeleton. At the conclusion of imaging, the surgeon should be able to answer the following questions: ■ Are there additional humeral metastases and, if there are, can they be managed by nonoperative techniques or do they require surgery? ■ Are there additional skeletal metastases and, if there are, can they be managed by nonoperative techniques or do they require surgery? ■ What is the appropriate surgery? As a rule, the tumor curettage and cemented fixation approach is used for lesions in which the remaining cortices allow containment of the fixation device; otherwise, surgery involves resection of the affected bone segment with prosthetic reconstruction. Chapter 12 Jacob Bickels and Martin M. Malawer Surgical Management of Metastatic Bone Disease: Humeral Lesions 1 13282_ON-12.qxd 3/22/09 9:37 AM Page 1
Transcript of Surgical Management of Chapter 12 Metastatic Bone...

BACKGROUND■ The humerus is a common site of metastatic bone diseaserequiring surgery. A metastasis at that site, especially when itinvolves the dominant extremity, has an immediate and pro-found impact on the affected individual’s ability to performactivities of daily living. The quality of surgery, therefore, is animportant factor in restoring vital function.■ A detailed preoperative clinical and imaging evaluation ismandatory for defining the morphologic characteristics of thelesion and, in turn, establishing the indications for surgical in-tervention, as well as distinguishing between lesions that canbe managed with curettage and cemented fixation and thosethat require resection with endoprosthetic reconstruction.2,3,5,6
■ Unlike primary sarcomas of the humerus, metastatic tumorsusually have a small soft tissue component, even in the pres-ence of extensive bone destruction. This characteristic allowsresection of bony elements only, permitting sparing of the ex-tracortical structures, such as the joint capsule, overlying mus-cles, and muscle attachments, and affords the opportunity touse them to reconstruct and preserve function (FIG 1A,B). Tothis end, exposure of the proximal humerus is done by split-ting the deltoid muscle rather using the deltopectoral interval,as is done in the case of a primary sarcoma of bone, which ne-cessitates en bloc resection of the deltoid muscle with thetumor. Moreover, a few centimeters of upper limb shorteningfollowing resection of bone segment has minimal impact onfunction, because a slight difference in positioning of that ex-tremity in space can easily compensate for such limb-lengthdiscrepancy.■ In contrast, a similar discrepancy in the lower extremities,which require almost equal length for normal gait, wouldresult in an inevitable limp, the extent of which would be pro-portional to the shortening of the operated extremity.2■ Because of different anatomic and surgical considerations,surgeries around the proximal humerus (type I), humeral dia-physis (type II), and distal humerus (type III) are discussedseparately (FIG 2).1
ANATOMYProximal Humerus: Type I Metastasis■ The proximal humerus is covered anteriorly and laterally bythe deltoid muscle.■ The joint capsule encircles the humeral head and attaches tothe base of the anatomic neck.■ The proximal humerus is the attachment site for the rotatorcuff muscles. The long head of the biceps muscle crosses theanterior aspect within the bicipital groove.
Humeral Diaphysis: Type II Metastasis■ The upper half is occupied by muscle insertions:
■ Medial aspect: teres major, latissimus dorsi, coraco-brachialis■ Lateral aspect: pectoralis major, deltoid
■ The radial nerve curves at the back from medial to lateral atthe mid-arm level.■ The lower half is occupied by muscle origins:
■ Medial aspect: Brachialis■ Lateral aspect: Brachioradialis■ Neurovascular bundle along its medial aspect
Distal Humerus: Type III Metastasis■ The neurovascular bundle lies along its medial aspect be-tween the biceps and brachialis muscles.■ The radial nerve lies along its lateral aspect between thebrachialis and brachioradialis muscles.
INDICATIONS■ Pathological fracture■ Impending pathological fracture■ Intractable pain associated with locally progressive diseasethat has shown inadequate response to narcotics and preoper-ative radiation therapy■ Solitary bone metastasis in selected patients
IMAGING AND OTHER STAGING STUDIES■ Plain radiographs of the entire humerus are mandatory torule out synchronous metastases that may change the extentand technique of surgery. A CT scan of the lesion will clearlydefine the extents of bone destruction and soft tissue compo-nent. Total body bone scintigraphy is done to detect synchro-nous metastases elsewhere in the skeleton. At the conclusion ofimaging, the surgeon should be able to answer the followingquestions:
■ Are there additional humeral metastases and, if there are,can they be managed by nonoperative techniques or do theyrequire surgery?■ Are there additional skeletal metastases and, if there are,can they be managed by nonoperative techniques or do theyrequire surgery?■ What is the appropriate surgery? As a rule, the tumorcurettage and cemented fixation approach is used for lesionsin which the remaining cortices allow containment of thefixation device; otherwise, surgery involves resection of theaffected bone segment with prosthetic reconstruction.
Chapter 12Jacob Bickels and Martin M. Malawer
Surgical Management ofMetastatic Bone Disease:Humeral Lesions
1
13282_ON-12.qxd 3/22/09 9:37 AM Page 1

2 Part 4 ONCOLOGY • Section I I SHOULDER GIRDLE AND UPPER EXTREMITIES
FIG 1 • A. Primary bone sarcomasusually have considerable extensioninto the soft tissues. Resection ofsuch tumors at the proximal humeruswould require en bloc removal of theoverlying deltoid muscle, rotator cufftendons, and the joint capsule.B. Bone metastases, however, usuallypresent with less soft tissue involve-ment, and their resection involves re-moval of bony elements with only athin layer of surrounding soft tissues.
FIG 2 • A,B. Type I humeral metastasis extend-ing across the anatomic neck to the humeralhead. C,D. Type II humeral metastasis involv-ing the humeral diaphysis between theanatomic neck and the supracondylar ridges ofthe humerus. E,F. Type III humeral metastasisextending to the humeral condyles below thesupracondylar ridges. (From Bickels J,Kollender Y, Wittig JC, et al. Function after re-section of numeral metastases. Analysis of 59consecutive patients. Clin Orthop Relat Res2005;437:201–208, with permission.)
A B
A B C D
E F
13282_ON-12.qxd 3/22/09 9:37 AM Page 2
Chapter 12 SURGICAL MANAGEMENT OF METASTATIC BONE DISEASE: HUMERAL LESIONS 3
TYPE I AND II METASTASES
Position and Incision■ The patient is placed in a semilateral position, and an an-
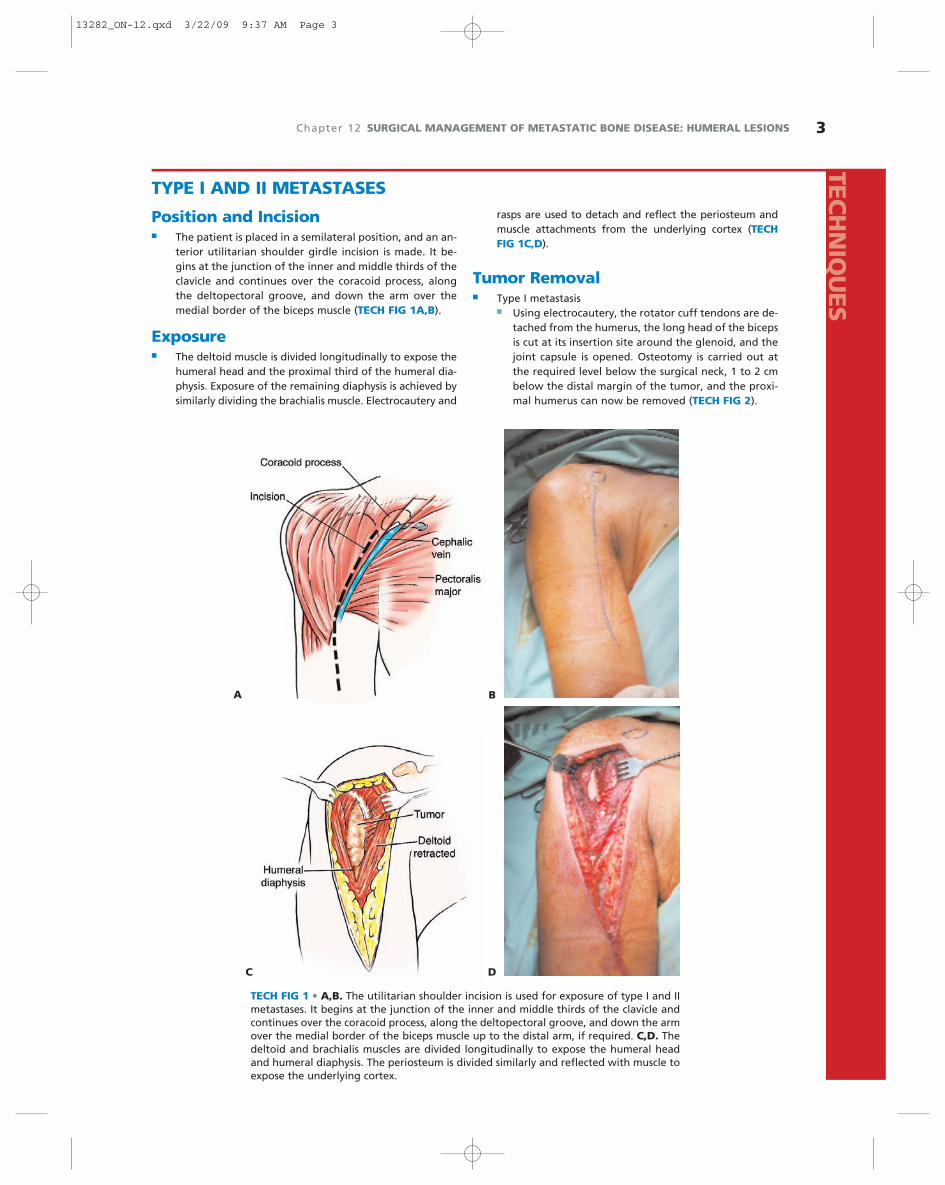
terior utilitarian shoulder girdle incision is made. It be-gins at the junction of the inner and middle thirds of theclavicle and continues over the coracoid process, alongthe deltopectoral groove, and down the arm over themedial border of the biceps muscle (TECH FIG 1A,B).
Exposure■ The deltoid muscle is divided longitudinally to expose the
humeral head and the proximal third of the humeral dia-physis. Exposure of the remaining diaphysis is achieved bysimilarly dividing the brachialis muscle. Electrocautery and
rasps are used to detach and reflect the periosteum andmuscle attachments from the underlying cortex (TECHFIG 1C,D).
Tumor Removal■ Type I metastasis
■ Using electrocautery, the rotator cuff tendons are de-tached from the humerus, the long head of the bicepsis cut at its insertion site around the glenoid, and thejoint capsule is opened. Osteotomy is carried out atthe required level below the surgical neck, 1 to 2 cmbelow the distal margin of the tumor, and the proxi-mal humerus can now be removed (TECH FIG 2).
TECH FIG 1 • A,B. The utilitarian shoulder incision is used for exposure of type I and IImetastases. It begins at the junction of the inner and middle thirds of the clavicle andcontinues over the coracoid process, along the deltopectoral groove, and down the armover the medial border of the biceps muscle up to the distal arm, if required. C,D. Thedeltoid and brachialis muscles are divided longitudinally to expose the humeral headand humeral diaphysis. The periosteum is divided similarly and reflected with muscle toexpose the underlying cortex.
A B
C D
TECH
NIQ
UES
13282_ON-12.qxd 3/22/09 9:37 AM Page 3

4 Part 4 ONCOLOGY • Section I I SHOULDER GIRDLE AND UPPER EXTREMITIES
■ Type II metastasis■ A longitudinal cortical window with oval edges is
made just above the lesion (TECH FIG 3A). Grosstumor is removed with hand curettes (TECH FIG 3B,C).Curettage should be meticulous and leave only micro-scopic disease in the tumor cavity. It is followed byhigh-speed burr drilling of walls of the tumor cavity(TECH FIG 3D–F). Occasionally, the cortices of the in-volved segment are completely destroyed, leaving nooption but an intercalary resection of the affected seg-ment. This is achieved by an osteotomy 1 to 2 cm aboveand below the segment (TECH FIG 3G–I).
Mechanical Reconstruction■ Type I metastasis
■ A cemented prosthesis is used for reconstruction (TECHFIG 4). The prosthetic design should allow the reat-tachment of rotator cuff tendons.
■ Type II metastasis■ An intramedullary nail is introduced. After proper po-
sition and length are verified, the nail is partiallypulled back, and the entire tumor cavity is filledwith cement (TECH FIG 5A,B). The nail is then pushed
back into the medullary canal and fixed with inter-locking screws. Alternatively, a side plate can be usedfor reinforcement (TECH FIG 5C,D). If an intercalaryresection has been done, the remaining bone defectis filled with cement (TECH FIG 5E–G).
Soft Tissue Reconstruction andWound Closure■ Type I metastasis
■ The rotator cuff tendons are attached to the prosthetichead using 3-mm Dacron tapes (Deknatel, Falls River,MA) or no. 5 Ethibond sutures (Ethicon, Somerville, NJ;TECH FIG 6). The pectoralis major, teres major, latis-simus dorsi, and coracobrachialis muscles are similarlyattached. Using the same technique, the prosthetichead also is secured to the drill holes within the bonyelements around the shoulder joint, acromion, clavicle,and glenoid. The second, overlying muscular layer in-cludes the deltoid and brachialis muscles, which are su-tured to cover the implant.
■ Type II metastasis■ The deltoid and brachialis muscles are sutured to
cover the humeral diaphysis.
TECH FIG 2 • A–C. Resection of the type I metastatic renal cellcarcinoma seen in the plain radiograph in Figure 1C is exe-cuted by detaching the rotator cuff tendons and the long headof the biceps and opening the joint capsule. An osteotomy isperformed and the proximal humeral segment is removed.D. Surgical specimen.
A B C
D
TYPE III METASTASES■ Type III metastases extend to the humeral condyles
below the supracondylar ridges. In most of thesecases, the extent of bone destruction allows tumorcurettage and reconstruction with cemented hard-
ware (the technique is described in the following sec-tion). Rarely will extensive destruction of the distalhumerus necessitate formal resection with endopros-thetic reconstruction.
TEC
HN
IQU
ES
13282_ON-12.qxd 3/22/09 9:37 AM Page 4

Chapter 12 SURGICAL MANAGEMENT OF METASTATIC BONE DISEASE: HUMERAL LESIONS 5
TECH FIG 3 • A. A longitudinal cortical window with oval edges is made just above the lesion. B,C. Gross tumor is removed withhand curettes. Curettage should be meticulous and should leave only microscopic disease in the tumor cavity. D,E. Curettage isfollowed by high-speed burr drilling of walls of the tumor cavity. F. Tumor cavity following curettage and burr drilling. G. Plainradiograph of type II thyroid carcinoma metastases. The extent of cortical destruction may does not allow curettage and burrdrilling and so intercalary resection of the affected segment is indicated. H–J. Intercalary resection is achieved by proximal anddistal osteotomies 1 to 2 cm above and below the tumor margin.
A B C
D E F
G H I J
TECH
NIQ
UES
13282_ON-12.qxd 3/22/09 9:37 AM Page 5

6 Part 4 ONCOLOGY • Section I I SHOULDER GIRDLE AND UPPER EXTREMITIES
TECH FIG 4 • Intraoperative photograph (A) and plain radiograph (B) show-ing a proximal humeral tumor prosthesis used for reconstruction after resec-tion of a type I metastasis.
Position and Exposure■ The patient is placed supine on the operating table with
the ipsilateral arm lying across the chest. A slightly curvedincision is made on the lateral aspect of the arm over thesupracondylar ridge of the elbow (TECH FIG 7A).
■ The distal humerus is exposed using the plane betweenthe brachioradialis and triceps muscles. The brachioradialisis reflected anteriorly and the triceps posteriorly. Furtherposterior reflection of the anconeus muscle combinedwith detachment and anterior reflection of the commonextensor origin exposes the radial head (TECH FIG 7B).
Tumor Removal and MechanicalReconstruction■ A longitudinal cortical window with oval edges is made
just above the lesion. Gross tumor is removed with handcurettes (TECH FIG 8A), and this is followed by high-speed burr drilling (TECH FIG 8B).
■ An intramedullary rod is introduced through the tumorcavity, which is then filled with cement. A reconstructionplate along the lateral supracondylar ridge is used toreinforce the reconstruction (TECH FIG 8C).
BA
A B C
TECH FIG 5 • A. An intramedullary nail is introduced. B. After proper position and length are verified, the nail ispartially pulled back, and the entire tumor cavity is filled with cement. The nail is then pushed back into themedullary canal and fixed with interlocking screws. Intraoperative photograph (C) and plain radiograph (continued)
TEC
HN
IQU
ES
13282_ON-12.qxd 3/22/09 9:37 AM Page 6

Chapter 12 SURGICAL MANAGEMENT OF METASTATIC BONE DISEASE: HUMERAL LESIONS 7
TECH FIG 5 • (continued) (D) show-ing side plate reinforcement of a ce-mented intramedullary humeralnail. Plain radiograph (E) and intra-operative photographs (F,G) show-ing side plate reinforcement of a ce-mented intramedullary humeralnail following intercalary resectionof a type II metastasis. The remain-ing bone defect is filled with ce-ment.
D E
F G
A B C
TECH FIG 6 • 3-mm Dacron tapes (A) or no. 5 Ethibond sutures (B) are used for securing the prosthetic head to the neighbor-ing acromion, clavicle, and glenoid and for reattachment of the rotator cuff tendons. C. Rotator cuff tendons are sutured tothe prosthetic head.
TECH
NIQ
UES
13282_ON-12.qxd 3/22/09 9:37 AM Page 7

8 Part 4 ONCOLOGY • Section I I SHOULDER GIRDLE AND UPPER EXTREMITIES
TECH FIG 7 • A. To expose a lesion at the distal humerus, the patient is placed supine on the operating tablewith the ipsilateral arm lying across the chest. A slightly curved incision is made on the lateral aspect of thearm over the supracondylar ridge of the elbow. B. The distal humerus and radial head are exposed using theplane between the brachioradialis and triceps muscles.
TECH FIG 8 • A. Gross tumor is removed with hand curettes. B. Curettage isfollowed by high-speed burr drilling. C. A cemented intramedullary rod thatis reinforced by a reconstruction plate along the supracondylar ridge is usedfor reconstruction.
BA
A B
C
TEC
HN
IQU
ES
13282_ON-12.qxd 3/22/09 9:37 AM Page 8

Chapter 12 SURGICAL MANAGEMENT OF METASTATIC BONE DISEASE: HUMERAL LESIONS 9
POSTOPERATIVE CAREType I and II Metastases■ Continuous suction is required for 3 to 5 days, and perioper-ative intravenous antibiotics are continued until the drainagetubes are removed. If endoprosthetic reconstruction was done,the shoulder is immobilized in a sling for 3 weeks. During thattime, the rehabilitation program emphasizes range of motion(ROM) of the elbow, wrist, and fingers with gravity assistance.Gradual passive and active ROM of the shoulder is then started,with emphasis on forward flexion, abduction, and shrugging.■ If tumor curettage has been carried out, ROM exercisesshould be practiced without delay. Once the wound has healed,usually 3 to 4 weeks after surgery, patients are referred to adju-vant radiation therapy. Radiation therapy usually is not re-quired in patients who have undergone proximal humerusresection with endoprosthetic reconstruction.
Type III Metastases■ The wound is closed over suction drains. Continuous suc-tion is required for 3 to 5 days, and perioperative intravenousantibiotics are continued until the drainage tubes are removed.■ Passive and active ROM exercises of the elbow joint are ini-tiated when the suction drains are removed.■ Once the wound has healed, usually 3 to 4 weeks aftersurgery, the patient is referred to adjuvant radiation therapy.Radiation therapy usually is not required, however, for pa-tients who have undergone distal humerus resection with en-doprosthetic reconstruction.
OUTCOMES■ Most patients who undergo resection of a humeral metas-tasis experience immediate relief of their metastasis-relatedpain. Patients who had a type II metastasis and who have un-dergone either curettage or intercalary resection have betterROMs and superior functional outcome than those who un-derwent proximal or distal humeral resection with endopros-thetic reconstruction.
■ Bickels et al.2 reported that overall total function in their56 patients (95%) who had undergone resection of a humeralmetastasis was over 68% of full normal upper extremity func-tion, which is the mean functional outcome score after recon-struction of the upper extremity.4
COMPLICATIONS■ Thromboembolic complications, deep wound infections,and prosthetic loosening (rare)■ Proximal humeral prosthetic dislocation, from poor secur-ing to the adjacent bones and inadequate soft tissue coverage■ Decreased ROM around the shoulder, due to poor attach-ment of the rotator cuff tendons to the prosthesis■ Decreased elbow ROM after surgery around distal humeruslesions■ Local tumor recurrence of less than 5% if adjuvant tumorremoval was done adequately and adjuvant radiation therapywas administered.
REFERENCES1. Bickels J, Kollender Y, Wittig JC, et al. Function after resection of
humeral metastases. Analysis of 59 consecutive patients. Clin OrthopRelat Res 2005;137:201–208.
2. Bickels J, Wittig JC, Kollender Y, et al. Limb-sparing resections of theshoulder girdle. J Am Coll Surg 2002;194:422–435.
3. Eckardt JJ, Kabo JM, Kelly CM, et al. Endoprosthetic reconstructionsfor bone metastases. Clin Orthop Relat Res 2003;415(Suppl):s254–262.
4. Enneking WF, Dunham W, Gebhardt MC, et al. A system for func-tional evaluation of reconstructive procedures after surgical treat-ment of tumors of the musculoskeletal system. Clin Orthop Relat Res1993;286:241–246.
5. Flemming JE, Beals RK. Pathologic fractures of the humerus. ClinOrthop Relat Res 1986;203:258–260.
6. Harrington KD, Sim FH, Enis JE, et al. Methylmethacrylate as an ad-juvant in internal fixation of pathological fractures: Experience withthree hundred and seventy-five cases. J Bone Joint Surg Am 1976;58A:1047–1055.
PEARLS AND PITFALLSType I and II MetastasesPreoperative ■ Adequate imaging of the entire humerus—decision on tumor curettage, intercalary resection, or
resection with endoprosthetic reconstruction
Intraoperative ■ Use the utilitarian shoulder incision.■ Wide exposure of the tumor cavity using properly positioned and large cortical window■ Meticulous curettage and burr drilling■ Reconstruction with cemented hardware■ If endoprosthetic reconstruction was done: (1) secure the prosthetic head to the surrounding bony ele-
ments to ensure shoulder stability; and (2) reattach the rotator cuff tendons to the prosthetic head toallow shoulder function
Postoperative ■ Immobilize the shoulder for 3 weeks and only then allow range of motion exercises
Type III Metastases■ Adequate exposure of the distal humerus■ Meticulous curettage and burr drilling■ Reconstruction with cemented hardware■ Early postoperative mobilization of the elbow joint
13282_ON-12.qxd 3/22/09 9:37 AM Page 9