Surgical anatomy of breasts
40
SURGICAL ANATOMY OF BREAST Dr. Ahmed Almumtin
-
Upload
ahmed-almumtin -
Category
Healthcare
-
view
262 -
download
11
Transcript of Surgical anatomy of breasts

S U R G I C A L A N A T O M Y O F B R E A S T
Dr. Ahmed Almumtin

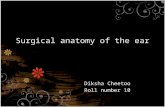
I N T R O D U C T I O N
• A modified sweat gland.
• Compartmentalized fat bounded by CT septa.
• Glandular lobules drained by 15-20 lactiferous ducts.
• Lactiferous ducts converge & open onto nipple.
• Areola surrounds nipple & conceals sebaceous glands • (i.e., produce lubrication for nipple).
Compartmentalisation Gland Lobules & Lac. Ducts

• lies over the 2nd - 6th rib.
• Two-thirds rests on pectoralis major.
• One-third lies on the serratus anterior.
• The lower medial edge overlaps the upper part of the rectus sheath.
• Medially from the sternal edge, to the mid-axillary line

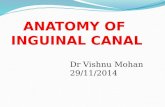
F O U R Q U A D R A N T S A N D A TA I L
• 4 quadrants.
• Majority of cancers develop in upper outer quadrant.
• Large amount of glandular tissue here.
• An axillary tail

R E T R O M A M M A R Y S PA C E
• Reteromammary space: is loose auroral tissue that separates then breast from the pectoralis major muscle.
• The retromammary space is often the site of of breast implantation due to its location away from key nerves and structure that support the breast.

S U R FA C E A N D A E S T H E T I C S
• The tail of Spencer.
• Determinants of aesthetics.

L I G A M E N T S
• Cooper’s ligament.
• Suspensory ligament of the breast.
• Fibrous septa anchor deep layer of skin to deep fascia.
• superfacial (avascular plane) separates the glandular portion and adipose portion.
Astley Cooper

I N F R A S T R U C T U R E
• Tumors may grow through retromammary space.
• Subsequently invade deep fascia & pec. major m.
• Leads to fixation of malignant breast lesion to chest wall.
• Shortens suspensory (Cooper’s) ligs.
• Leads to irregular dimpling of skin or retraction of nipple

A P P L I E D C L I N I C A L A N AT O M Y
• Skin dimpling.
• Nipple retraction.
• Peau d'orange
• Lymphoedema of ipsilateral upper limb post-mastectomy.

B L O O D S U P P LY
• Vessels of the Breast
• Enter from supr./med. & supr./lat. aspects
• Penetrate deep surface of breast.
• Exhibit extensive branches. & anastomoses.

A R T E R I A L S U P P LY T O T H E B R E A S T
• Lateral (mammary) thoracic a.
• Internal (mammary) thoracic a.
• Intercostal aa.
• Thoracoacromial a


V E N O U S D R A I N A G E
• Corresponds to arterial system.
• Cephalic vein


LY M P H AT I C S • Lat. drainage is via 5
groups of axillary nodes
• Supr. drainage is via 1 group of interpectoral nodes
• Med. drainage is via 1 group of parasternal nodes
• Ultimate drainage is via subclavian lymph trunk to vv. (i.e., jxn. of subclavian v. & IJV)

LY M P H AT I C S
• Pectoral nodes ( 4-5 nodes, most drainage).
• Subscapular (posterior) nodes (6-7),
• Lateral nodes (4-6).
• Central nodes (3-4), ?Neck?
• Apical nodes (6-12)
• Interpectoral (Rotter’s) nodes (1-4)
• Parasternal nodes

LY M P H AT I C S

LY M P H AT I C S I N A S S O C I AT I O N W I T H V E S S E L S
• Pectoral – lat. thoracic vessels
• Subscapular – subscapular vessels
• Humeral – distal (3rd) part of axillary v.
• Central – middle (2nd) part of axillary v.
• Apical – proximal (1st) part of axillary v.
• Interpectoral – pectoral vessels
• Parasternal – int. thoracic vessels

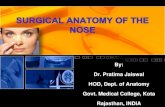
LY M P H N O D E L E V E L S ( B E R G ’ S )
• 3 Levels of surgical dissections relative to pec. minor.
• Level I – below (lateral to) pec. minor
• Level II – deep to pec. minor
• Level III – above (medial to) pec. minor

C L I N I C A L S I G N I F I C A N C E
• Cancer cells tend to spread along lymph passages
• Typical spread is supr./laterally to axillary lymph nodes
• Unilateral lymphatic blockage may occur
• Lymph (with cancer cells) can then drain to opposite side

N E R V E S U P P LY
• Cutaneous innervation.
• Medial pectoral n.
• Lateral pectoral n.
• Long thoracic n.

N E R V E S U P P LY

N E R V E S U P P LY
• Take care!:
• LTN
• Thoracodorsal
• lateral and medial pectoral nerve

T H E A X I L L A
• Axillary sheath (axillary a. & brachial plexus).
• Axillary v. & lymphatics (outside sheath).
• Fat & connective tissue
• Cutaneous nerves
The AxillaThe Axilla

T H E A X I L L A • very busy space.

S U R G I C A L A P P R O A C H T O A X I L L A
• In modified radical mastectomy
• Conservative breast surgery


M A S T E C T O M Y
• Radical Mastectomy.
• modified radical mastectomy
• Simple mastectomy
• skin sparing mastectomy
• Nipple-Areolar spaing mastectomy.

B O U N D R I E S F O R M A S T E C T O M Y
• Clavicle.
• inframammary fold (above rectus sheath)
• Sternum (midline).
• Latissimus dorsi (ant. border)

S I M P L E M A S T E C T O M Y
• Definition.
• frequency.

M O D I F I E D R A D I C A L M A S T E C T O M Y
• definition.
• indication

R A D I C A L M A S T E C T O M Y
• definition.
• success rates.

S K I N S PA R I N G M A S T E C T O M Y
• Definition.

N I P P L E - A R E O L A R S PA R I N G M A S T E C T O M Y
• Definition.
• Criteria

C H O I C E O F T H E P R O C E D U R E
• Radical mastectomy - No longer used.
• Lymph node status
• Desired time of reconstruction.
• Criteria of NSM.
• Prophylactic

I N C I S I O N S I N B R E A S T S U R G E R Y

I N C I S I O N S F O R M A S T E C T O M Y
• depends upon: location, size, reconstruction plans
• SSM.
• MRM
• NASM

Stewart!
* design according to tumour location

• The drains are left in place until the drainage of serous fluid has decreased to approximately 25 to 30 mL per 24-hour period