Surgery of Choledochal Cysts

of 15
-
Upload
intanpiana -
Category
Documents
-
view
229 -
download
0
Transcript of Surgery of Choledochal Cysts
-
8/2/2019 Surgery of Choledochal Cysts
1/15
Surgery of Choledochal CystsCystic enlargement of the bile ducts
Choledochal cysts are cystic enlargements of the bile ducts, which do not occur commonly.
Anatomy and Physiology
The gall bladder is a small pear shaped organ located beneath the liver in the right side of
the upper abdomen
The cystic duct carries bile from the gallbladder and joins the common hepatic duct,which carries bile from the liver) to form the common bile duct. The common bile duct
then empties into the duodenum, which is the beginning of the small intestine (Figure 1)
The main purpose of the gallbladder is to concentrate and store bile. It releases bile by
ejecting it through the common bile duct into the small intestine when fatty foods areeaten. The bile aids in the digestion of fatty foods.
The gall bladder may be congenitally absent
Figure 1 - Anatomy of the liver, duodenum,
gallbladder, hepatic ducts and common bile
duct. R. Walls
Pathology
The cause is not definitely known
It is more common in females and has a higher incidence in Japan
These cysts typically do not contain a normal biliary epithelium (lining cells of duct)
There are five main variants of choledochol cysts (Figure 2):1. Type I - fusiform (spindle shaped) dilation of the common bile duct and common
hepatic duct
2. Type II - a sac like duct off the side wall of a biliary duct3. Type III - cystic outpouching of the biliary duct into the duodenum4. Type IV - dilation of the hepatic ducts both inside and outside the liver5. Type V - dilation of the hepatic ducts inside the liver
-
8/2/2019 Surgery of Choledochal Cysts
2/15
Figure 2 - Types of choledochal cysts. See
text. R. Walls
History and Exam
These conditions present with jaundice (yellow skin), abdominal pain, fever associatedwith the jaundice and/or an abdominal mass
Clinical exam reveals the jaundice and often a tender mass in the upper abdomen on the
right side
These conditions are not always present in infancy
Tests
It may be diagnose before birth by ultrasound over the uterus as early as 20 weeks of
gestation
Laboratory tests show abnormal liver function
Multiple imaging tests help make the diagnosis:
1. Ultrasound of the abdomen usually makes the diagnosis2. Magnetic Resonance Imaging (MRI) demonstrates the cysts3. ERCP (See Endoscopic Retrograde CholangioPancreatography). An endoscope is
passed through the stomach into the duodenum and then through the ampulla of
Vater into the lower common bile duct. A dye is injected that shows up thehepatic ducts on X-ray. This test has some risk
4. Nuclear scanning. A compound, which is secreted by the liver into the hepaticducts and containing a medical nuclear isotope, is injected. Nuclear scanning of
the liver and bile ducts is then carried out and an image of the ducts produced
Indications for Surgery
Surgery is indicated to correct the abnormality and prevent progressive liver dysfunction
resulting in cholangitis (inflammation of the ducts) and biliary cirrhosis (chronic inflammation ofthe liver)
http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=67http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=67http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=67http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=67 -
8/2/2019 Surgery of Choledochal Cysts
3/15
Surgery
1. Regardless of the type of choledochal cyst surgery includes2. An initial exploration of the abdominal contents for other abnormalities3. An operative cholangiogram of the bile ducts, which is carried out by injection of
a dye that shows up on X-ray into the gall bladder or a hepatic duct outside the
liver4. Cholecystectomy (removal of the gall bladder -See Cholecystectomy) The type of defect determines the surgical procedure
1. Types I & II - In addition to the gallbladder, the hepatic duct cysts outside theliver are removed. This is followed with a hepaticojejunostomy in which the
hepatic duct is anastomosed (joined) to the jejunum using a Roux-en-Y jejunal
loop and end to side jejunum to jejunum anastomosis (Figure 3)2. Type III - The procedure varies with this type. Often there is excision of the cyst
along with sphincteroplasty, division of the sphincter of Oddi (muscle fibers at the
lower end of the common bile duct) which promotes bile drainage into duodenum
3. Type IV - This type of choledochal cyst may require total removal the hepatic
ducts lying outside the liver and partial removal of liver at the junction of thehepatic ducts from the right and left sides of the liver. This junction of ducts is
then anastomosed to a loop of bowel4. Type V - If the cysts are confined to a lobe of the liver then partial removal of the
involved sites is carried out. Extensive involvement may ultimately require a liver
transplant
Figure 3 - The gallbladder and the hepatic duct
cysts outside the liver are removed. This isfollowed with a hepaticojejunostomy in which
the hepatic duct is anastomosed to the jejunum
using a Roux-en-Y jejunal loop and end-to-side jejunum to jejunum anastomosis. R.
Walls
http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=16http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=16http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=16http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=16 -
8/2/2019 Surgery of Choledochal Cysts
4/15
Complications
The complications associated with any major operation should be anticipated
Bleeding
Respiratory distress
Hypothermia (low body temperature) Low urine output
Infection in blood, urine, abdomen, lung and/or bile
Bowel obstruction
Anastomotic leak (fistula) at any anastomotic suture site (bowel, liver)
Stricture (narrowing) at bile duct anastomosis
Cholangitis - infection of bile ducts
Post Op Care
The child is cared for in an intensive care unit with:
1. Special monitoring to ensure adequate breathing since the child may requireventilator support2. Temperature monitoring3. Urine output monitoring
Fluids are given by vein until food is tolerated
A tube is placed through the nose into the stomach to keep the stomach decompressed
Antibiotics are given top prevent infection
Prolonged intensive care may be required
After Care
These children may be hospitalized for long periods and require special follow up The goal is a healthy baby able to eat, urinate, and eliminate stool at the time of discharge
without need for respiratory or special nutritional support
Follow up is determined by the complexity of the cyst formation
Physical activity is limited for 4-6 weeks
Follow up with surgeon in 7-10 days
Continued monitoring of liver function studies
-
8/2/2019 Surgery of Choledochal Cysts
5/15
Answer to Case of the Week: Jan 7-Jan 14, 2010
2 different patients with same diagnosis
-
8/2/2019 Surgery of Choledochal Cysts
6/15
Fusiform dilatation of common bile duct.
Diagnosis: Choledochal Cyst
-
8/2/2019 Surgery of Choledochal Cysts
7/15
Choledochal cysts are spectrum of
malformations of the extrahepatic and
intrahepatic bile ducts.
One in 100,000-150,000 live births in US versus
1 in 1,000 live births in Japan.
2/3 of all choledochal malformations are
diagnosed before 10 years of age.
More common in females 3 or 4:1
Cholangiocarcinoma is a worrisome long-term
complication, 2-18% and 5-35 increased risk.
Caroli disease and Caroli syndrome risk of
cholangicarcinoma at a rate of 100x that of
general population.
TRIAD:
Jaundice
Right upper quadrant pain
-
8/2/2019 Surgery of Choledochal Cysts
8/15
Palpable mass
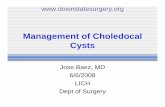
Classification:
Todani5 types ( See the figure)
Type I-(A)Segmental or fusiform dilatation of
the common bile duct-most common(75-95%)
Type II- (B) Diverticulum of the duct protrudingfrom the lateral wall
Type III- (C ) Choledochocele
Type IV-( D) Multiple extrahepatic bile ducts
alone(type IV B) or in association with Caroli-type (E)
Type V- (F) Cystic dilatation of intrahepatic bile
ducts equivalent to Caroli disease
Pathophysiology: Anomalous junction of thecommon biliary and pancreatic ducts with
provides conduit for mixing of pancreatic juice
and bile.
-
8/2/2019 Surgery of Choledochal Cysts
9/15
-
8/2/2019 Surgery of Choledochal Cysts
10/15
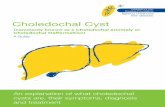
Residents Submitting Correct Diagnosis - Case of the Week
Radiology
Pediatrics
Choledochal cyst (type IV)
Added byWael Nemattallaon November 9, 2009 at 8:18am
View Images
http://www.radrounds.com/profile/WaelNemattallahttp://www.radrounds.com/profile/WaelNemattallahttp://www.radrounds.com/profile/WaelNemattallahttp://www.radrounds.com/photo/photo/listForContributor?screenName=15dftq1xwba7ahttp://www.radrounds.com/photo/photo/listForContributor?screenName=15dftq1xwba7ahttp://www.radiology.vcu.edu/facstaff/bio/dasnarla.htmlhttp://www.radiology.vcu.edu/facstaff/bio/dasnarla.htmlhttp://www.radrounds.com/photo/photo/listForContributor?screenName=15dftq1xwba7ahttp://www.radrounds.com/profile/WaelNemattalla -
8/2/2019 Surgery of Choledochal Cysts
11/15
Previous|Next
Choledochal cysts are congenital conditions associated with benign cystic dilatation of bileducts. They are uncommon in western countries but not as rare in East Asian nations like Japan
and China.
They were classified into 5 types by Todani in 1977.
Classification was based on site of the cyst or dilatation.
Type I: Most common variety involving sacular or fusiform dilatation of a portion or entirecommon bile duct (CBD) with normal intrahepatic duct.
Type II: Isolated diverticulum protruding from the CBD.Type III or Choledochocele: Arise from dilatation of duodenal portion of CBD or where
pancreatic duct meets.
http://www.radrounds.com/photo/photo/listForContributor?screenName=15dftq1xwba7ahttp://www.radrounds.com/photo/photo/listForContributor?screenName=15dftq1xwba7ahttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/prev?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/prev?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/next?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/next?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/next?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/next?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/next?context=userhttp://www.radrounds.com/photo/choledochal-cyst-type-iv-2/prev?context=user -
8/2/2019 Surgery of Choledochal Cysts
12/15
Type IV: Dilatation of both intrahepatic and extrahepatic biliary duct.
Type V or Caroli's disease: Cystic dilatation of intra hepatic biliary ducts.
Symptoms of Choledochal Cyst
Some newborns with cysts have symptoms right away. Others have good bile flow at first, butthey get symptoms soon after birth. Some children dont have symptoms for a couple of years or
longer. Some people live with a choledochal cyst for many years but dont know about it becausethey dont have symptoms until they are an adult.
Babies or children with a choledochal cyst may have these symptoms:
Yellow color to the eyes and skin (jaundice)
Pain in the upper right belly (upper right quadrant pain)
Soft mass that can be felt in the upper right belly
Pale or clay-colored stools (feces)
Fever, if they have an infection (cholangitis) If they have an inflamed pancreas (pancreatitis): belly pain that may come and go, nausea and
vomiting
Choledochal Cyst Diagnosis
Sometimes doctors can see a choledochal cyst on an ultrasound before a baby is born (prenatalultrasound). If this happens with your baby, doctors will plan the tests and treatment your baby
will need after birth. Its not always possible to see a cyst before birth.
If your childs cyst was not seen but your child has symptoms after they are born, your childs
doctor will ask for a detailed history of your childs illness. The doctor will do a thorough exam.
There is no blood test for choledochal cysts. But the doctor may do blood tests to check whether
your childs bile ducts are inflamed or infected and whether their liver is working well.
The doctor will do an ultrasound of your childs belly (abdomen) to see your childs bile ductsand other organs in the area. Imaging studies like ultrasound help the doctor know whether there
is a cyst, where it is and how it is shaped. These factors help your childs doctor plan surgery to
remove the cyst.
Your child may also need other imaging studies, like these:
Cholangiographyinjecting dye (contrast) into your childs bile ducts and then taking an X-ray.
This may be done in one of two ways. One way is to inject the dye through your childs skin and
liver into their ducts (percutaneous transhepatic cholangiography, PTC). The other way is to
inject the dye through a small tube placed into your childs mouth and down their throat into
their intestine (endoscopic retrograde cholangiopancreatography, ERCP).
Abdominal CT (computed tomography) scan.
Abdominal MRI (magnetic resonance imaging) scan.
-
8/2/2019 Surgery of Choledochal Cysts
13/15
HIDA scan (hepatobiliary iminodiacetic acid scan). A HIDA scan allows doctors to see whether a
special dye that collects in the liver can pass out of the liver through the bile
Click here to return to the Pediatric Surgery at Brown Home Page
Key words
What is a choledochal cyst?
Bilethat is produced in theliverflows through increasingly larger channels (ducts) within theliver and finally into even larger ducts that leave the liver, pass through the substance of the
pancreas, and then empty into theduodenum.
A choledochal cyst is a cyst (hollow outpouching) of the bile ducts. Choledochal cysts have been
classified into several different types depending on where they are located and whether they can
be seen as separate structures from the ducts (diverticulum-like); or whether they can be seen asa localized dilation (enlargement) of the ducts. Choledochal cysts are rare, occurring in less than
1% of individuals. The cause of choledochal cysts is unknown, but they are congenital, that is,
present from birth, and, therefore, represent developmental abnormalities of the bile ducts in thefetus.
http://med.brown.edu/pedisurg/index.htmlhttp://med.brown.edu/pedisurg/index.htmlhttp://www.medicinenet.com/script/main/art.asp?articlekey=2459http://www.medicinenet.com/script/main/art.asp?articlekey=2459http://www.medicinenet.com/script/main/art.asp?articlekey=4179http://www.medicinenet.com/script/main/art.asp?articlekey=4179http://www.medicinenet.com/script/main/art.asp?articlekey=4179http://www.medicinenet.com/script/main/art.asp?articlekey=4743http://www.medicinenet.com/script/main/art.asp?articlekey=4743http://www.medicinenet.com/script/main/art.asp?articlekey=3132http://www.medicinenet.com/script/main/art.asp?articlekey=3132http://www.medicinenet.com/script/main/art.asp?articlekey=3132http://www.medicinenet.com/script/main/art.asp?articlekey=15599http://www.medicinenet.com/script/main/art.asp?articlekey=15599http://www.medicinenet.com/script/main/art.asp?articlekey=15599http://www.medicinenet.com/script/main/art.asp?articlekey=3424http://www.medicinenet.com/script/main/art.asp?articlekey=3424http://www.medicinenet.com/script/main/art.asp?articlekey=3424http://www.medicinenet.com/script/main/art.asp?articlekey=15599http://www.medicinenet.com/script/main/art.asp?articlekey=3132http://www.medicinenet.com/script/main/art.asp?articlekey=4743http://www.medicinenet.com/script/main/art.asp?articlekey=4179http://www.medicinenet.com/script/main/art.asp?articlekey=2459http://med.brown.edu/pedisurg/index.html -
8/2/2019 Surgery of Choledochal Cysts
14/15
What are the symptoms and complications of choledochal cysts?
In infants, choledochal cysts usually lead to obstruction of the bile ducts and retention of bile.This leads tojaundiceand an enlarged liver. If the obstruction is not relieved, permanent damage
may occur to the liver - scarring and cirrhosis - with the signs ofportal hypertension(obstructionto the flow of blood through the liver) andascites(fluid accumulation in the abdomen). There is
an increased risk ofcancerin the wall of the cyst.
In older individuals, choledochal cysts are more likely to causeabdominal painand intermittent
episodes of jaundice and occasionallycholangitis(inflammation within the bile ducts caused by
the spread of bacteria from the intestine into the bile ducts). Pancreatitisalso may occur. Thecause of these complications may be related to either abnormal flow of bile within the ducts or
the presence ofgallstones.
http://www.medicinenet.com/script/main/art.asp?articlekey=1899http://www.medicinenet.com/script/main/art.asp?articlekey=1899http://www.medicinenet.com/script/main/art.asp?articlekey=1899http://www.medicinenet.com/script/main/art.asp?articlekey=41912http://www.medicinenet.com/script/main/art.asp?articlekey=41912http://www.medicinenet.com/script/main/art.asp?articlekey=41912http://www.medicinenet.com/script/main/art.asp?articlekey=103748http://www.medicinenet.com/script/main/art.asp?articlekey=103748http://www.medicinenet.com/script/main/art.asp?articlekey=103748http://www.medicinenet.com/script/main/art.asp?articlekey=13931http://www.medicinenet.com/script/main/art.asp?articlekey=13931http://www.medicinenet.com/script/main/art.asp?articlekey=13931http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=22935http://www.medicinenet.com/script/main/art.asp?articlekey=22935http://www.medicinenet.com/script/main/art.asp?articlekey=22935http://www.medicinenet.com/script/main/art.asp?articlekey=439http://www.medicinenet.com/script/main/art.asp?articlekey=439http://www.medicinenet.com/script/main/art.asp?articlekey=439http://www.medicinenet.com/script/main/art.asp?articlekey=368http://www.medicinenet.com/script/main/art.asp?articlekey=368http://www.medicinenet.com/script/main/art.asp?articlekey=368http://www.medicinenet.com/script/main/art.asp?articlekey=368http://www.medicinenet.com/script/main/art.asp?articlekey=439http://www.medicinenet.com/script/main/art.asp?articlekey=22935http://www.medicinenet.com/script/main/art.asp?articlekey=1908http://www.medicinenet.com/script/main/art.asp?articlekey=13931http://www.medicinenet.com/script/main/art.asp?articlekey=103748http://www.medicinenet.com/script/main/art.asp?articlekey=41912http://www.medicinenet.com/script/main/art.asp?articlekey=1899 -
8/2/2019 Surgery of Choledochal Cysts
15/15