SuppressorCellActivityinaRandomizedTrialofPatientsReceivingActive...
8
(CANCER RESEARCH 50, 5358-5364. September 1, ]990| Suppressor Cell Activity in a Randomized Trial of Patients Receiving Active Specific Immunotherapy with Melanoma Cell Vaccine and Low Dosages of Cyclophosphamide1 Dave S. B. Hoon,2 Leland J. Foshag, Anne S. Nizze, Roger Bohman, and Donald L. Morton Division of Surgical Oncology, John Wayne Cancer Clinic, Armand Hammer Laboratories, Jonsson Cancer Center fD. S. B. H., L. J. F., A. S. N., D. L. M.], and Division ofNephrology [R. B.], University of California, Los Angeles School of Medicine, Los Angeles, California 90024 ABSTRACT Previous studies have shown that melanoma patients develop an im mune response to cell surface melanoma-associated antigens. The pres ence of this antibody response to cell surface antigens has been correlated with a better clinical outcome when melanoma patients are treated with an allogeneic melanoma cell vaccine (MCV) as an active immunotherapy protocol. It was hypothesized that the inability to consistently induce or enhance existing immune responses to melanoma-associated antigens was related to the downregulation by suppressor cells. Patients received treatments of MCV 3 times in a 4-week interval and then every fourth week. The biological response modifier cyclophosphamide (CYP) is an immunomodulator of suppressor T-cell function. In this study we set out to determine whether CYP given prior to MCV could reduce suppressor cell activity during vaccination. In a randomized trial stage II and III melanoma patients (n = 41) were given MCV alone or in conjunction with CYP at dosages of 300, 150, or 75 mg/m2. CYP was given 3 days prior to each MCV treatment. Suppressor cell activity in patients was monitored by a concanavalin A suppressor assay using peripheral blood lymphocytes from serial phlebotomies during a 12-week period of treat ment. In each trial group there were patients who had major reduction in suppressor cell activity (>50%). Overall, the greatest reduction in sup pressor cell activity occurred in patients receiving 300 mg/m2 CYP compared to the other CYP dosages or MCV alone. For the first two treatments at all CYP dosages there was a greater number of patients showing reduced suppressor cell activity compared to later treatments. In a comparison of patients receiving MCV alone to MCV + CYP 300 mg/m2 phenotypic analysis of lymphocyte subsets showed significant (/' = 0.03) reduction in the ( 1)X'( 1)11H* (suppressor) cells of the latter group. These studies suggest that CYP can be used at low dosages in conjunction with MCV to reduce suppressor cell activity. INTRODUCTION Human melanoma has been demonstrated to be immuno- genic in the host. Numerous reports have demonstrated hu moral and cellular immune responses that are specific to MAA3 (1-6). We have demonstrated that anti-melanoma antibodies in melanoma patients can substantiate clinical observations that host immune resistance influences the course of this disease as manifested by disease-free and overall survival (1,2). Although immunity is apparent in melanoma patients it is usually short term (1) which appears to be related to the downregulation of tumor-specific immune response(s) (3, 7). Melanoma is very difficult to manage once metastasis has occurred. Patients with métastasesto regional nodes (stage II) or distant organs (stage III) have a high risk of recurrence of disease within a short Received 10/17/89; revised 4/3/90. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1This study was supported by grant CA 12582 awarded by the National Cancer Institute. United States Department of Health and Human Services. ! To whom requests for reprints should be addressed, at Division of Surgery Oncology, CHS 54-140, UCLA School of Medicine, Los Angeles, CA 90024. 3The abbreviations used are: con A; concanavalin A, CYP; cyclophosphamide, MCV; melanoma cell vaccine, PBL; peripheral blood lymphocyte: TPBL. target PBL; PHA. phytohemagglutinin antigen: NED, no evidence of disease: AWD, alive with disease; Cn, day of CYP treatment: Vn, MCV treatment. period (8). It would seem logical that activating host immunity to MAA in such patients may provide control and protection against development of additional metastatic lesions that are not clinically detectable. In our clinic we have established an active specific immuno therapy protocol designed to enhance or induce immunity to MAA. This involves immunization of melanoma patients after surgery with an allogeneic MCV consisting of melanoma cell lines which were selected on the basis of expression of cell surface MAA to which melanoma patients have been shown to produce antibodies (1, 9). We have previously demonstrated that many patients receiving MCV have only a temporary or no elevation in antibody titers to melanoma-associated anti gens. It is believed that this lack of immune response after treatment with MCV may be due to immune suppression or downregulation by the immune system. In this study we sought to determine whether ¡mmunomo- dulation of the host immune system with the biological response modifier CYP given prior to vaccination could reduce suppres sor cell activity, thus enhancing responses to the MCV. CYP is an alkylating agent which is known to modulate immune re sponses in tumor-bearing animals and humans (10-15). Sup pressor T-cells are known to be very sensitive to this drug at concentrations that do not affect other subpopulations of lym phocytes (10, 16-18). The drug can enhance host cellular im mune recognition and responses against tumor cells (10, 13, 15). Higher dosages of CYP are known to have side effects on patients and be toxic to various immune cells, particularly B- cells (17, 19). We set up a randomized trial to investigate various low dosages of CYP (300, 150, and 75 mg/m2 body weight) given in conjunction with MCV. The immunomodula- tion of suppressor cell activity in melanoma patients receiving multiple treatments of MCV with various low dosages of CYP is presented in this report. MATERIALS AND METHODS Patients. Patients for this study were seen in the John Wayne Cancer Clinic of the Jonsson Cancer Center, UCLA. Those entered into the study were high risk stage II and stage III melanoma patients. Most patients had lymphadenectomy(s) and/or other surgery prior to ran domization and were entered into the MCV therapy protocol within several weeks of their surgery. The patients were randomized into four treatment groups: MCV alone (10 patients); MCV + 300 mg CYP/m2 (11 patients); MCV + 150 mg CYP/m2 (10 patients); and MCV + 75 mg CYP/m2 (10 patients). Patient eligibility criteria for high risk stage II were: (a) stage II melanoma with regional lymph node métastases (stratified for number of nodes involved for each treatment group); (b) within 2 months of lymphadenectomy surgery and clinically free of disease (NED); (c) no prior chemotherapy, radiation, or immunother apy; (d) no systemic métastases;and (e) age of 18-75 years. The eligibility criteria for stage III patients were: (a) stage III melanoma with s.c. or visceral métastases;(b) rendered disease-free prior to therapy (NED) or with objectively measurable disease (AWD); (c) must not have been receiving other prior treatments for a minimum of 30 5358 on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of SuppressorCellActivityinaRandomizedTrialofPatientsReceivingActive...

(CANCER RESEARCH 50, 5358-5364. September 1, ]990|
Suppressor Cell Activity in a Randomized Trial of Patients Receiving ActiveSpecific Immunotherapy with Melanoma Cell Vaccine and Low Dosages ofCyclophosphamide1
Dave S. B. Hoon,2 Leland J. Foshag, Anne S. Nizze, Roger Bohman, and Donald L. Morton
Division of Surgical Oncology, John Wayne Cancer Clinic, Armand Hammer Laboratories, Jonsson Cancer Center fD. S. B. H., L. J. F., A. S. N., D. L. M.], and DivisionofNephrology [R. B.], University of California, Los Angeles School of Medicine, Los Angeles, California 90024
ABSTRACT
Previous studies have shown that melanoma patients develop an immune response to cell surface melanoma-associated antigens. The presence of this antibody response to cell surface antigens has been correlatedwith a better clinical outcome when melanoma patients are treated withan allogeneic melanoma cell vaccine (MCV) as an active immunotherapyprotocol. It was hypothesized that the inability to consistently induce orenhance existing immune responses to melanoma-associated antigens wasrelated to the downregulation by suppressor cells. Patients receivedtreatments of MCV 3 times in a 4-week interval and then every fourthweek. The biological response modifier cyclophosphamide (CYP) is animmunomodulator of suppressor T-cell function. In this study we set outto determine whether CYP given prior to MCV could reduce suppressorcell activity during vaccination. In a randomized trial stage II and IIImelanoma patients (n = 41) were given MCV alone or in conjunctionwith CYP at dosages of 300, 150, or 75 mg/m2. CYP was given 3 days
prior to each MCV treatment. Suppressor cell activity in patients wasmonitored by a concanavalin A suppressor assay using peripheral bloodlymphocytes from serial phlebotomies during a 12-week period of treatment. In each trial group there were patients who had major reduction insuppressor cell activity (>50%). Overall, the greatest reduction in suppressor cell activity occurred in patients receiving 300 mg/m2 CYP
compared to the other CYP dosages or MCV alone. For the first twotreatments at all CYP dosages there was a greater number of patientsshowing reduced suppressor cell activity compared to later treatments.In a comparison of patients receiving MCV alone to MCV + CYP 300mg/m2 phenotypic analysis of lymphocyte subsets showed significant (/'= 0.03) reduction in the ( 1)X'( 1)11H*(suppressor) cells of the latter
group. These studies suggest that CYP can be used at low dosages inconjunction with MCV to reduce suppressor cell activity.
INTRODUCTION
Human melanoma has been demonstrated to be immuno-genic in the host. Numerous reports have demonstrated humoral and cellular immune responses that are specific to MAA3(1-6). We have demonstrated that anti-melanoma antibodies inmelanoma patients can substantiate clinical observations thathost immune resistance influences the course of this disease asmanifested by disease-free and overall survival (1,2). Althoughimmunity is apparent in melanoma patients it is usually shortterm (1) which appears to be related to the downregulation oftumor-specific immune response(s) (3, 7). Melanoma is verydifficult to manage once metastasis has occurred. Patients withmétastasesto regional nodes (stage II) or distant organs (stageIII) have a high risk of recurrence of disease within a short
Received 10/17/89; revised 4/3/90.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This study was supported by grant CA 12582 awarded by the National CancerInstitute. United States Department of Health and Human Services.
! To whom requests for reprints should be addressed, at Division of SurgeryOncology, CHS 54-140, UCLA School of Medicine, Los Angeles, CA 90024.
3The abbreviations used are: con A; concanavalin A, CYP; cyclophosphamide,MCV; melanoma cell vaccine, PBL; peripheral blood lymphocyte: TPBL. targetPBL; PHA. phytohemagglutinin antigen: NED, no evidence of disease: AWD,alive with disease; Cn, day of CYP treatment: Vn, MCV treatment.
period (8). It would seem logical that activating host immunityto MAA in such patients may provide control and protectionagainst development of additional metastatic lesions that arenot clinically detectable.
In our clinic we have established an active specific immunotherapy protocol designed to enhance or induce immunity toMAA. This involves immunization of melanoma patients aftersurgery with an allogeneic MCV consisting of melanoma celllines which were selected on the basis of expression of cellsurface MAA to which melanoma patients have been shown toproduce antibodies (1, 9). We have previously demonstratedthat many patients receiving MCV have only a temporary orno elevation in antibody titers to melanoma-associated antigens. It is believed that this lack of immune response aftertreatment with MCV may be due to immune suppression ordownregulation by the immune system.
In this study we sought to determine whether ¡mmunomo-dulation of the host immune system with the biological responsemodifier CYP given prior to vaccination could reduce suppressor cell activity, thus enhancing responses to the MCV. CYP isan alkylating agent which is known to modulate immune responses in tumor-bearing animals and humans (10-15). Suppressor T-cells are known to be very sensitive to this drug atconcentrations that do not affect other subpopulations of lymphocytes (10, 16-18). The drug can enhance host cellular immune recognition and responses against tumor cells (10, 13,15). Higher dosages of CYP are known to have side effects onpatients and be toxic to various immune cells, particularly B-cells (17, 19). We set up a randomized trial to investigatevarious low dosages of CYP (300, 150, and 75 mg/m2 bodyweight) given in conjunction with MCV. The immunomodula-tion of suppressor cell activity in melanoma patients receivingmultiple treatments of MCV with various low dosages of CYPis presented in this report.
MATERIALS AND METHODS
Patients. Patients for this study were seen in the John Wayne CancerClinic of the Jonsson Cancer Center, UCLA. Those entered into thestudy were high risk stage II and stage III melanoma patients. Mostpatients had lymphadenectomy(s) and/or other surgery prior to randomization and were entered into the MCV therapy protocol withinseveral weeks of their surgery. The patients were randomized into fourtreatment groups: MCV alone (10 patients); MCV + 300 mg CYP/m2(11 patients); MCV + 150 mg CYP/m2 (10 patients); and MCV + 75mg CYP/m2 (10 patients). Patient eligibility criteria for high risk stage
II were: (a) stage II melanoma with regional lymph node métastases(stratified for number of nodes involved for each treatment group); (b)within 2 months of lymphadenectomy surgery and clinically free ofdisease (NED); (c) no prior chemotherapy, radiation, or immunotherapy; (d) no systemic métastases;and (e) age of 18-75 years. Theeligibility criteria for stage III patients were: (a) stage III melanomawith s.c. or visceral métastases;(b) rendered disease-free prior totherapy (NED) or with objectively measurable disease (AWD); (c) mustnot have been receiving other prior treatments for a minimum of 30
5358
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MELANOMA CELL VACCINE AND CYCLOPHOSPHAMIDE
days and no prior immunotherapy; (d) no brain métastases;(e) patientswith life expectancies of >4 months; and (/) age of 18-75 years.
Treatment Protocol. A polyvalent vaccine consisting of 3 humanmelanoma cell lines was chosen for immunization on the basis thatseveral melanoma-associated antigens are known to induce antibodyresponses in patients to autologous melanomas (1, 2). The cell lineswere chosen for their expression of antigens GM2 (20), GD2 (21) andM-TAA (22). One of the first two antigens are found to be present in>90% of melanoma biopsy specimens, whereas the latter is in >70%of melanoma biopsy specimens. The 3 melanoma cell lines were established in our laboratory. Cells were grown in RPMI 1640 medium(Flow Laboratories) supplemented with 10% fetal calf serum (heatinactivated) and antibiotics. After several passages cells were harvestedby trypsinization, washed 4 times, counted, adjusted to 25 x IO7cells
in freezing medium (RPMI 1640 + 10% human albumin + 10%dimethyl sulfoxide) and program freezed to be stored in liquid nitrogen.The vials contained equal amounts of each cell line. Before beingadministered to patients the cells were irradiated at 150 Gy. The vaccineis produced in large batches and carefully analyzed for antigen expression to determine variance from one lot to another. MCV is screenedfor hepatitis, bacteria, and Mycoplasma contamination by an outsidelaboratory before being considered for administration to patient.
Within several hours of patient arrival for treatment the MCV isthawed, washed 3 times in RPMI 1640 medium, and put into a syringefor intradermal inoculation. In the first 2 treatments the MCV is mixedwith one or one-half of a vial of Glaxo strain Bacille Calmette-Guérin(8-25 x IO6organisms/vial) (Glaxo, Greenford, England). In Fig. 1 a
diagram of the MCV protocol is given. Briefly, MCV is administeredby intradermal inoculation into 8 sites in the axilla and groin every 2weeks on 3 consecutive occasions and then at 4-week intervals for 1year. CYP (Cytoxan, Mead Johnson and Co., Evansville, IN) is given3 days prior to each MCV treatment (Fig. 1).
Lymphocyte Collection. Blood was collected in heparin-containingtubes from patients immediately prior to treatment. The PBLs wereseparated from blood by using a standard Ficoll-Hypaque gradientcentrifugation, washed twice, counted, aliquoted, and cryopreserved.For cryopreservation lymphocytes were resuspended in RPMI 1640,10% dimethyl sulfoxide (Sigma Chemical Co., St. Louis, MO), plus40% heat-inactivated agamma human AB serum (Biocell, Carson, CA).The cells were aliquoted in vials and frozen by time-controlled cryopreservation in liquid nitrogen. When cryopreserved cells were used alllymphocytes from serial phlebotomies were thawed at the same time.Cells were thawed rapidly, washed twice in RPMI 1640-supplemented10% human AB serum (Scientific, Irvine, CA), and treated with DNase(Sigma) for 20 min at 37°Cto remove DNA fragments from disrupted
cells. Cells were counted for viability. Viability was usually >95%. Ifthe viability of the cells was <80% the assay was not performed on thatparticular lymphocyte aliquot.
Con A-induced Suppressor Cell Assay. A con A-induced suppressorcell assay was used to assess suppressor cell activity on PBLs collectedfrom patients receiving therapy. Particularly important in assessingsuppressor cell activity of serially collected PBLs is the consistency andreproducibility of this assay system as previously reported (7, 15). In
MCV MCV + CYP
MCV I
MCV „
MCV III
DAY O
DAY 14
CYP IMCV I
DAY 0DAY 3
DAY 28M<=V III ---- ---- DAY 31
CYP IVMCV IV
DAY 56DAY 59MCV IV ----- DAY 56
REPEAT EVERY 4 WKS REPEAT EVERY 4 WKS
Fig. 1. Treatment schedule for MCV alone (left) and MCV + CYP (right).Blood was drawn for PBLs immediately prior to each treatment. For the MCVgroup after day 56 patients received MCV every 4 weeks. In the MCV + CYPgroup after day 59 patients received MCV + CYP every 4 weeks.
this assay suppressor cell activity of T-cells is measured (7, 23). Macrophages are removed during the 48-h incubation of the assay; therefore,they do not contribute directly to the suppression measured against thetarget PBLs.
The con A assay was performed as previously described. Culturemedium refers to RPMI 1640 containing 10% human AB serum(Scientific, Irvine) (heat inactivated), antibiotics, and 4-(2-hydroxy-ethyl)-l-piperazineethanesulfonic acid buffer (Gibco, New York).Briefly, PBLs from serial phlebotomies were incubated with 40 MgconA for 48 h at 2 x 106/ml in culture medium in 15-ml round-bottomed
culture tubes (Falcon). This duration of incubation was found to giveoptimal activation of existing suppressor cells (7). As a control PBLswere incubated in culture medium at the same concentration withoutcon A. After 48 h incubation con A-treated and control cells werewashed 3 times with a-D-mannose (5 jig/ml) in medium to competitivelyremove the con A from the cell surface membrane (7), resuspended inculture medium, and counted. Viability was >90% for con A-treatedand control PBLs.
TPBLs were obtained from donors 2-3 months before the assay,aliquoted, and cryopreserved. In the con A assay TPBLs were thawedrapidly, washed twice with culture medium, and assessed for viability.The TPBLs were then resuspended at 106/rnl in culture medium con
taining 0.5 Mg/ml PHA (Wellcome). One hundred M' of PBLs wasadded to each well in a 96-well microtiter plate (Costar). Control andcon A-treated PBLs were inactivated by mitomycin C (Sigma) treatmentand were washed 3 times in culture medium.
The assay was set up by adding 10' mitomycin C-treated controlPBLs or con A-treated cells to microwells containing TPBLs. Quadruplicate wells for both the control and con A-treated PBLs of eachphlebotomy point were set up. The cultures were incubated at 37°Cin
a humidified, 7% CO2 atmosphere incubator for 84 h. In the last 18 hthe cultures were pulsed with 1 ^Ci [3H]-thymidine. Cells were then
harvested with a PHD harvester (Cambridge, MA) and were countedin scintillation fluid using a Beckman LS-330 counter (Beckman Instruments, Inc., Fullerton, CA).
Suppressor cell activity was measured as the percentage of suppression of the PBL response to PHA. Data was calculated in cpm beforebeing expressed as percentage of suppression.
% suppression
/ cpm of con A PBL + TPBL + PHA cultures \~ \ cpm of control PBL + TPBL + PHA cultures/ X
Several specific T-cell subset populations of patients' PBLs were as
sessed using fluorochrome-conjugated monoclonal antibodies. Cellswere stained simultaneously with fluoroscein- and rhodamine-conju-gated monoclonal antibodies. The CD4 (T4) and TQ1 marker monoclonal antibodies were obtained from Coulter Electronics (Hialeah,FL). CDS (Leu2a) and CD1 IB (Leu 15) marker monoclonal antibodieswere obtained from Becton Dickinson (Mountain View, CA). Specificsubset populations were analyzed by dual color immunofluorescenceflow cytometry on an EPICS V cell sorter (Coulter). Respective isotype-matched fluorochrome-conjugated antibodies were used as controls.CD4+TQ1* are a T-suppressor inducer subpopulation (24, 25).CD4+TQ~ are a helper function for B-cell immunoglobulin production(24, 25). CD8*CD11B+ are a subpopulation of suppressor T-cells (26).CD8*CD11B~ are a subpopulation of cytotoxic precursor and effector
cells (26). The percentage of various marker combinations were determined using the MDADS computer software program (Coulter).
Data Evaluation. Statistical analysis of Cn-Vn couplets was evaluatedby analysis of variance (27). Comparison of T-cell subsets and percentage of reduction of suppressor cell activity was evaluated by Student's
t test (27). Correlation of clinical status to percentage of suppressionwas determined by x2 analysis (27).
RESULTS
Clinical Documentation of Patients. In Table 1 clinical documentation of the patients that were studied is given. The clinical
5359
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MELANOMA CELL VACCINE AND CYCLOPHOSPHAM1DE
Table 1 Clinical stratification of patients
MCV + CYPMCV (300mg/m2)SexMaleFemaleClinical
statusStage11Stage
IIIEntrystatusNEDAWDClark
levelIIII!IVVUnknownT346821Ì41173558212511MCV
+ CYP(150 mg/m2)6473912233MCV
+CYP(75mg/m2)7465922162
" Number of patients.
% Suppression
V3
MCV Treatments
Fig. 2. Serial analysis of suppressor cell activity of two representative patientsreceiving MCV therapy alone. Percentage of suppression refers to suppressor cellactivity as described in the "Materials and Methods." Vl-5 are the MCV
treatments given as shown in Fig. 1.
status is noted for each patient at the start of therapy. Overall,34 patients entered with NED (stage II and III) and 7 AWD(stage III). In the study there were 22 stage II and 19 stage IIIpatients. The Clark levels of the primary melanomas are documented for patients (Table 1). All patients had normal performance status. Through previous studies we have considered theimmune and clinical status at the 12th week of MCV treatmentas the reference point for evaluation of the patient's immediate
response to the MCV treatment (1). In the 12th week of theprotocol the patient will have received 4 MCV treatments.
Serial Analysis of Suppressor Cell Activity of MCV-treatedPatients. Blood samples from patients who received MCVtreatment alone were analyzed for suppressor cell activity.There was no significant pattern of suppressor cell activityobserved among the 10 patients. Some patients initially hadlow suppressor cell activity which eventually increased by the12th week, whereas in other patients the opposite effect wasobserved. In Fig. 2 examples of longitudinal analysis of suppressor cell activity are given. The mean (n = 10) suppressorcell activity at the first vaccine treatment was 25% suppressionand at the forth vaccine treatment the mean was 40.5%. Analysis of the differences of percentage of suppression between Vnand Vn + 1 indicated a trend of lesser inhibition of suppressorcell activity as the number of MCV treatments increased (Table2).
Serial Analysis of Suppressor Cell Activity for Patients Receiving MCV plus CYP. Suppressor cell activity was monitoredfrom serial blood samples obtained from patients receivingMCV plus different dosages of CYP. The activity was moni
tored on the day of administration of CYP and MCV treatment.In Fig. 3 representative examples of patients receiving 75, 150,and 300 mg CYP/m2 treatments are given. Individual patients
had variable responses to the different dosages of CYP asobserved in patients treated with MCV alone. To analyze suppressor cell activity during treatment percentage of suppressionwas determined on the day of CYP treatment (Cn) and 3 dayslater after MCV treatment (Vn). The reduction in percentageof suppression between Cn and Vn was considered a positiveeffect of CYP treatment, whereas no change in activity orincrease in activity was considered as no response. In analysis
100% Suppression
V2 C3
Treatments
so n
60-
40-
20 i
% Suppression
C1 V1 C2 V2 C3
TreatmentsV3 C4 V4
100 n
80-
60 -
% Suppression
40-
20-
V2 C3
TreatmentsFig. 3. Serial analysis of suppressor cell activity of 3 patients receiving MCV
+ CYP at different dosages. Percentage of suppression is as described in Fig. 2.CI-4 refer to CYP treatments. Vl-4 refer to MCV treatments. Patients received75 (A), 150 (A), and 300 (C) mg CYP/m2.
5360
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MELANOMA CELL VACCINE AND CYCLOPHOSPHAM1DE
of the couplets (Cn-Vn) of different serial blood samples therewas at least 1 patient in each CYP dosage group who had >50%reduction in suppressor cell activity after 3 days.
At the start of treatment for each CYP dose there wasvariability in individual patients' suppressor cell activities. The
mean suppressor cell activity at the initiation of treatment was32.3, 24.5, and 40% for 75, 150, and 300 mg CYP/m2, respec
tively. The mean suppressor cell activity at the fourth treatmentwas 28.4, 25.4, and 33.7% for patients treated with 75, 150,and 300 mg CYP/m2, respectively. In Table 2 a summary ofpercentage of suppression differences at the Cn-Vn intervalsfor each dose of CYP is given. For all CYP dosages the mostreduction (mean) in percentage of suppression occurred in thefirst 2 CYP treatments. The 300 mg CYP/m2 dose had the
highest overall mean reduction in suppressor cell activity. Incomparing the mean of reduction of percentage of suppressionof C1V1 + C2V2 versus C3V3 + C4V4 we found that only the300 mg CYP/m2 group had statistical significance (P < 0.01;Student's t test). In the MCV group there were no significant
differences between the couplets.To evaluate the percentage of patients having reduction of
suppression in response to CYP treatment Cn-Vn couplets forindividual patients were assessed. The patient is considered asresponding to CYP treatment if there is a reduction in suppressor cell activity after 3 days of treatment. For each Cn-Vncouplet the number of patients showing reduction in suppressorcell activity was determined for each CYP dose (Fig. 4). Thepattern of reduction of suppressor cell activity was similar forthe different CYP dosages. At the first and second treatmentsthe percentage of patients was the highest; thereafter the leveldeclined. Consistently, the 300 mg/m2 group had the highestpercentage of patients for each couplet (Cn-Vn) group. The 75and 150 mg/m2 treatment groups had similar responses, exceptat the 75 mg/m2 C2-V2 couplet there was a higher percentageof patients. The best response to CYP 300 and 75 mg/m2 groupwas at the C2-V2 couplet, whereas for CYP 150 mg/m2 it wasthe C1-VI couplet.
Overall Effect of CYP on Suppressor Cell Activity. The overallcumulative effect of CYP on reduction of suppressor cell activitywas analyzed by taking the initial treatment value at Cl andsubtracting the mean of suppressor cell activity for C2, C3, andC4 in each patient [Cl - (mean of C2 + C3 + C4)]. This
derived value represented overall mean reduction, if any, in
Table 2 Suppressor cell activity reduction after each CYP treatment% Reduction in suppressor cell activity"
Interval
3 day Vnc Mean ±SEM" MedianCYP 75mg/m2CYP
150mg/m2CYP
300mg/m2MCVC1-V1C2-V2C3-V3C4-V4C1-V1C2-V2C3-V3C4-V4C1-V1C2-V2C3-V3C4-V4VI
-V2V2-V3V3-V45.7
±9.817.4±13.5-6.6±8.5-7.4±9.46.5±8.2-4.9±5.9-14.8
±8.3-13.7±10.219.8±8.219.2±9.0-3.2±5.5-6.0±14.40.2±12.3-8.2±14.9-25.3±16.615.740.4-8.5-9.42.1-5.7-8.60.713.315.5-7.9-9.0-7.5-0.1-9.0
' The values represent the differences of % suppression between Cn and Vn inpatients treated with MCV + CYP. —,no inhibition of suppression.
* Overall value for individual patient differences between % suppression of Cn
and Vn in each trial group.' Difference of % suppression between Vn and Vn + 1.
100
80
60
% Patients Responding
C1-V1 C2-V2 C3-V3
Treatment Interval
C4-V4
Fig. 4. Effect of CYP 3 days after treatment on reduction of suppressor cellactivity. Columns, % of patients with reduction in suppressor cell activity. Thereduction in suppressor cell activity is determined by Cn % suppression —Vn %suppression. Patients are divided according to CYP treatment dose: D, 75 mg/m2; ^, 150 mg/m2; •300 mg/m2.
Patients(%) with reduction of suppressor cell activity80
60
TreatmentFig. 5. Cumulative effect of MCV and MCV + CYP treatment on suppressor
cell activity. The % of patients having overall reduction in suppressor cell activityfor each treatment group is given. Overall effect of treatment on % suppressionin individual patients is calculated by subtracting the % suppression at Cl fromthe mean of % suppression of C2 + C3 + C4. Columns, % of patients having acumulative reduction in % suppression relative to pretreatment (CI).
suppressor cell activity from the initiation of treatment. In Fig.5 the percentage of patients having reduction in suppressor cellactivity for the individual CYP treatments is presented. Thepercentage of patients having an overall reduction in suppression was significantly greater in the 300 mg CYP group (P <0.05; analysis of variance) compared to MCV alone or the 75mg CYP group. There were no significant differences in thereduction of suppressor activity between MCV alone and 150or 75 mg CYP/m2 treatments. When patients were compared
with regard to their entry status (AWD, NED) into differenttreatment groups there were no significant differences.
Relation of Suppressor Cell Activity to Clinical Status. Clinicalstatus of patients at 12 months of therapy was correlated tosuppressor cell activity (Table 3). Correlation of overall clinicalresponse to suppressor activity was higher for CYP treatmentgroups MCV + CYP 300 and 150 mg/m2 (80%) than for MCV+ CYP 75 mg/m2 or MCV alone (45.5 and 40%, respectively).
Statistical analysis of the correlation of clinical status to overallsuppressor cell activity in the MCV + CYP treatment groups(all CYP groups) was significant (P < 0.05; x2)- An evaluation
of positive clinical status to positive suppressor cell activityshowed a trend favoring the MCV + CYP groups, especiallyfor MCV + CYP 300 mg/m2 compared to MCV alone (Table
3).Lymphocyte Subset Analysis of Patients Receiving Therapy.
Lymphocyte subsets were analyzed from serial PBL samples5361
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MELANOMA CELL VACCINE AND CYCLOPHOSPHAMIDE
Table 3 Relation of suppressor cell activity to clinical status"
Treatment group
Correlation of (+)Overall correlation of clinical response to
clinical response to (+) suppressor cellsuppressor cell activity activity
MCVMCV+ CYP (75 mg)
MCV + CYP (150mg)MCV + CYP (300 mg)4/10
(40%)5/11 (45.5%)8/10(80%)8/10(80%)2/4
(50%)2/4 (50%)3/5 (60%)4/6 (66.7%)
" Correlation of patients suppressor cell activity to clinical status at 12 months
of therapy. Suppressor cell activity was then categorized as positive or negative:a positive was patients with low overall suppression during treatment (mean<30%) or cumulative reduction in suppression as described in Fig. 5; a negativewas high overall suppression during treatment (>30%) or no cumulative reductionin % suppression after CYP. Clinical status of patients at start of treatment and12 months after treatment was evaluated as follows: a positive response wasconsidered to be when patients had no change in clinical status (NED to NED,AWD to AWD); a negative response was considered to be when patients hadprogression of disease (NED to recurrence of death. AWD to death). Correlationrefers to congruence in clinical course and suppressor activity, i.e., if suppressorcell activity was not reduced, the clinical course was adverse or. if clinical coursewas favorable, the suppressor cell activity was reduced.
from 4 patients in the MCV and MCV plus 300 mg CYP/m2
groups. A summary of 6 serial lymphocyte samples analyzedby dual color flow cytometry is given in Table 4. PBLs wereanalyzed at the time of each vaccine (VI-V5) treatment. Thecell subset having the highest positive staining was theCd4+TQl~ (helper cells). The CD4~TQ1+ cells at pre- andMCV treatments were significantly (Student's / test) lower than
the MCV + CYP group (P < 0.02 and = 0.03, respectively).The CD8+CD11B+ (suppressor) cell subset at pre- and MCVtreatments was significantly higher than MCV + CYP (P =0.03 and < 0.05, respectively). All other subset comparisons ofeither pretreatment or MCV compared to MCV + CYP werenot significant. The analysis of individual subsets for eachvaccine treatment is given in Table 5. When the two treatmentgroups were compared, only the CD8+CD11B+ subset had
significant (P < 0.05 for VI, V3, and V5) differences for morethan one cycle of MCV treatment.
DISCUSSION
In this study we set out to determine whether CYP as animmunomodulator could reduce suppressor cell activity in patients receiving MCV. We sought a drug dosage which wouldnot inhibit positive immune effector mechanisms toward melanoma, such as antibody production to tumor-associated antigen. The effect of CYP on enhancement or inhibition of antibody production to melanoma-associated antigen has been previously assessed (1). We reviewed the literature and to the bestof our knowledge this is the largest clinical trial in whichsuppressor cell activity of various low dosages of CYP <300mg/m2 as an immunomodulator was assessed in a significant
series of patients with normal performance status and a singlehistológica! type of cancer (28-30). Our study is unique compared to other published trials in that the patients: (a) all hadthe same neoplasm, (b) all had normal performance status, (c)did not have any chemo-, immuno-, or radiotherapy(s) prior to
receiving CYP, (d) did not receive any other therapies duringtreatment, and (e) were randomized to receive low dosages ofCYP and MCV or MCV alone. When analyzing immunologicalparameters these criteria are very important. The effect oftherapy on the human immune system may either be immediateor delayed for several months. Therefore, to analyze cellularfunctions such as suppressor cell activity it is important thatpatients entering the randomized trial be as homogeneous aspossible.
In melanoma patients there is considerable heterogeneity inimmunological status, tumor burden, immunogenicity of tumor, and duration of tumor presence. Analysis within a patients' serial bleed by comparison of pre- to posttreatment is
often the most informative to evaluate the effect of the drug. Incomparing all 3 dosages of CYP the 300-mg/m2 dose consist
ently gave the most reduction in suppressor cell activity withinindividual patients as well as the highest number of respondingpatients. There were, however, patients who had very significantreductions (>50%) in suppressor cell activity with the otherdosages of CYP. The assessment of suppressor cell activity atindividual couplet points (Cn-Vn) and during a 12-week periodindicated that 300 mg CYP/m2 was consistently effective. Much
to our surprise in patients receiving MCV treatment alone,>40% had an overall reduction in suppressor cell activity duringthe course of 4 treatments. This may be related to activation ofthe patients' immune responses during therapy. These results
led us to investigate lymphocyte phenotype subsets to comparepatients receiving MCV with or without 300 mg CYP/m2.
The data from the subset analysis supported the functionalsuppressor data from the con A assay. There was significantreduction in the suppressor cell subset CD8*CD11B+ in patients receiving 300 mg CYP/m2 + MCV versus MCV alone or
pretreatment. At 4 of 5 individual Vn points, a significantreduction in CD8+CD11B+ cells occurred. CYP treatment didnot significantly affect the number of CD4+TQ1+ (suppressorinducer) cells. There was a significant increase in CD4~TQ1 +
cells in the CYP treatment group compared to MCV alone orpretreatment. Although this subset has not been clearly defined,it is likely to be part of the CDS* cell subset (30, 31). The TQ1
antigen is found on about 50% of PBLs, with distribution of70-85% on CD4 cells and 30-60% on CDS cells (24, 25, 32).CYP did not significantly alter the cytotoxic T-cell subsetCD8+CD11B~. Our studies indicate that the percentage ofCD4+ and CD8+ cells overall are not altered after treatmentwith 300 mg CYP/m2, although subsets expressing these major
markers may vary in numbers.Studies by Bast et al. (28) have shown that treatment with
CYP dosages of 200-600 mg/m2 gave selective reduction ofcirculating CD8+ cells in patients with melanoma. Our studiesindicated no overall reduction of CD8+ cells after treatment but
reduction in a specific subset. Berd and Mastrangelo (29) havereported that there were no significant changes in theCD8+CD1 IB* cell subset in advanced stage melanoma patientsreceiving vaccine plus 300 mg CYP/m2. One of the major
Table 4 Phenotypic analysis of lymphocyte subsets
Positive staining lymphocytes
Treatment"Pretreatment
MCVMCV + 300 mg CYP/m2CD4*TQ1*19.0
±3.8*
19.2 ±1.619.7 ±2.4CD4*TQ1-35.7
±4.030.8 ±1.531.1 ±1.5CD4-TQT10.8
±2.113.2 ±1.918.6 ±1.8CD8*CD11B*9.1
±1.29.6 ±1.26.4
±0.5CD8*CD11B-15.5±
1.915.6 ±1.716.9 ±2CDS-CD
1IB*9.4
±1.512.9 + 0.811.1 ±0.8
" In each treatment group 4 patients were analyzed. Pretreatment represents the mean values of 8 patients prior to treatment (VO). The values in the treatmentgroups represent the mean of 4 patients; for each patient the mean of 5 points (Vl-5) was taken.
6 Mean ±SEM.
5362
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MELANOMA CELL VACCINE AND CYCLOPHOSPHAMIDE
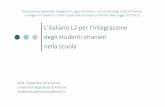
Table 5 Phenotypic analysis of lymphocyte subsets at each MCV treatment
Treatment"
>Positive staining cells
Vaccination CD4*TQ1* CD4*TQ1~ CD8*CD1IB* CD8*CD11B-
MCVMCV
+ 300 mg CYP/m2VIV'2V3V4vsVIV2V3V4V516.9±19.2
±20.5±18.2±18.5
±25.6±19.3±17.6±22.6
±17.8±5.9*1.34.64.15.612.64.83.48.89.838.3
±6.732.6±3.127.4±1.631.631.936.931.137.822.740.95.315.56.830.0
0.19.8
±1.68.8±3.48.9±0.912.518.54.85.06.011.46.16.61.20.91.65.45.2
0.312.7±16.3
±15.5±16.8±22.2±11.0±12.9±12.6±23.2
±13.4±5.83.83.96.211.32.33.26.26.98.8
°In each treatment group there are 4 patients. The value given for each vaccination treatment represents the mean of 4 patients. The pretreatment analysis of
phenoljpic subsets is given in Table 4.* Mean ±SEM.
differences in our protocol is that by day 56 (8 weeks) thepatients have received 4 CYP treatments, whereas in their trialonly 3 CYP treatments have been given. The reduction in theCD8+CD11B+ cell subset were consistent at multiple vaccine
(V) points therefore, supporting the validity of the overallevaluation. Also in the study by Berd and Mastrangelo (29) amodest reduction in the CD4*2H4H" (suppressor inducer) cells
occurred after 7 weeks of CYP and vaccine treatment. Thesuppressor inducer subset CD4+TQ1* we analyzed showed nosignificant changes. The CD4+TQ1+ and CD4+2H4* are not
the same but are believed to overlap. Comparison of the trialsmay not be appropriate since the extent of disease was notsimilar, different melanoma vaccines were administered, thenumber of CYP treatments were not the same, and the scheduling of treatments differed.
Patients consistently gave a similar pattern of response toCYP, regardless of dose, for the first 2 treatments. This type ofresponse may be predicted, since suppressor cells sensitive toCYP will be removed or inhibited early in treatment. This doesnot imply that suppressor cell activity would be abrogatedcompletely, since there are suppressor cells that are not sensitiveto CYP.4 The efficiency of CYP as a suppressor cell immuno-modulator may be limited to the number of CYP-sensitivesuppressor cells. There is question as to what phenotype(s) theCYP-sensitive population might be. The CD8+CD11B+ may
possibly be included as a CYP-sensitive cell population sincethere was a reduction during 300 mg CYP/m2 treatment. An
important question that needs to be addressed is to what extentmelanoma tumor burden induces CYP-sensitive suppressorcells in patients? It may be that only patients with melanomasexpressing certain tumor and/or particular tumor burden havehigh levels of these cell types. Also CYP treatment effect isrelated to the extent of immune suppression the patient has atthe start of the study. Due to the limitation of CYP effect oncertain subsets of suppressor cells other drugs which modulatesuppressor cell activity should be investigated for possiblegreater efficacy. One such drug, cimetidine, is currenty beinginvestigated. Preliminary results suggest that this drug can alsomodulate suppressor cell activity and immunological responsesin melanoma patients (1).
The variation in responses of patients to the various lowdosages may be related to in vivo activation of CYP. CYPrequires activation to a metabolic form by enzymes from theliver (33). Since the patient population is very heterogeneousthe concentration of the final activated form to which theimmune cells are exposed would vary from patient to patientreceiving the same CYP dose. This may in part explain why
4 D. Hoon and D. Martin, unpublished results.
there is variation in patient responses. The results that havebeen observed from tumor-bearing animals receiving CYP areoften more uniform since the animals used in those studies areinbred.
In this study, and others, overall suppressor cell activity hasbeen measured by the con A assay and flow cytometry ofindividual T-cell subsets which can be either nonspecific orspecific. The immune system is constantly regulating multipleantigen stimulations via antigen-specific and nonspecific suppressor cells. Analysis of the effect of immunomodulating drugssuch as CYP may be much more informative if antigen-specific(related to the disease) T-cell subsets could be assessed. However, this is a difficult task, since only recently melanoma-associated antigens that induce autologous serological responses have been characterized (1). The question of which ismore important, antigen-specific or nonspecific suppressorcells, will remain unsolved until more antigen-specific cellularresponses toward tumors are well characterized.
In previous studies we found that 300 mg CYP/m2 enhancedtumor necrosis factor-like production from monocytes, whereasat the lower dosages of 75 and 150 mg/m2 production of this
factor was unaltered or diminished (34). Our studies indicatethat CYP at 300 mg/m2 has multiple effects on the cellular
immune functions which control eradication of tumor burden.Cytokines released from monocytes can effect T-cell subsetfunctions (35). The effect of CYP on T-suppressor cell activitymay be indirect through modulation of monocyte activity.
One of the objectives of using CYP was to downregulatesuppressor cell activity prior to MCV treatment. The studysuggests that low dose CYP can be used for this purpose inconjunction with MCV. Analysis of the clinical response (12months) with overall suppressor cell activity reduction indicateda significant correlation for the MCV + CYP groups. Thepatients receiving the 300 mg CYP/m2 had the most favorable
clinical response in 12 months as well as the best overallreduction in suppressor cell activity. Although 300 mg/m2 was
consistently most effective, lower dosages were effective forboth clinical and overall suppression in some patients. Sinceeven 300 mg/m2 of the drug can have toxic effects on some
patients a method is needed for determining the lowest effectivedose for a given patient. Designing alternative treatment schedules may maximize the effect of CYP. From our study it issuggested that the initial two treatments have the major effectand that subsequent treatments may be delayed until suppressorcell activity rises. Melanoma patients have varying levels ofsuppressor cell activity including some that have low activity.Suppressor cell activity was not significantly affected by CYPin these particular patients. This strongly suggests that pretreatment analysis before CYP administration may be very impor-
5363
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MELANOMA CELL VACCINE AND CYCLOPHOSPHAMIDE
tant. Future studies should be focused in this direction in orderto predict which patients are likely to respond so that unnecessary treatment of nonresponders can be avoided.
ACKNOWLEDGMENTS
We wish to thank the nursing staff of the John Wayne Cancer Clinicand the technical staff, E. Famitiga, J. Naungayan, L. Ordonez, andM. Siene, for their help in the study.
REFERENCES
1. Morton. D. L., Hoon, D. S. B., Gupta, R. G.. Nizze, A. J., Farmitiga, E.,Foshag. L. J., Furutani, S., and Irie, R. F. Treatment of malignant melanomaby active specific immunotherapy in combination with biological responsemodifiers. In: M. Torisu and T. Yoshida (eds.). New Horizons in TumorImmunotherapy. pp. 665-683. Fukuoka, Japan: Elsevier, 1989.
2. Jones, P. C., Sze. L. L., Liu, P. Y., Morton, D. L., and Irie, R. F. Prolongedsurvival for melanoma patients with elevated IgM antibody to oncofetalantigen. J. Nati. Cancer. Inst.. 66: 249-254. 1981.
3. Mukherji, B.. Wilhelm, S. A., Guha. A., and Ergin, M. T. Regulation ofcellular immune response against autologous human melanoma. I. Evidencefor cell-mediated suppression of in vitro cytotoxic immune response. J.Immunol.. 136: 1888-1892, 1986.
4. Parmiani, G., Fossati, G., and Tarmelli. D. Autologous cellular immune toprimary and metastatic human melanomas and its regulation by Dr antigensexpressed on tumor cells. Cancer Metastatis Rev., 4: 7-26, 1985.
5. Tai, T.. Cahan. L. D., Tsuchida. T., Saxton, R. E., Irie, R. F., and Morton,D. L. Immunogenicity of melanoma-associated gangliosides in cancer patients. Int. J. Cancer, 35: 607-612, 1985.
6. Slingluff. C. L., Jr.. Darrow, T., Vervaert, C.. Quin-Allen, M. A., and Seigler,H. F. Human cytotoxic T cells specific for autologous melanoma cells:successful generation from lymph node cells in seven consecutive cases. J.Nati. Cancer. Inst., SO: 1016-1026, 1988.
7. Hoon, D. S. B., Bowker, R. J., and Cochran. A. J. Suppressor cell activity inmelanoma-draining lymph nodes. Cancer Res., 47: 1529-1533, 1987.
8. Morton. D. L. Adjuvant immunotherapy of malignant melanoma: status ofclinical trials at UCLA. Int. J. Immunother., //: 31-36. 1986.
9. Morton, D. L., Nizze, A. J., Gupta, R. K., Famatiga, E., Hoon, D. S. B., andIrie. R. F. Active specific immunotherapy of malignant melanoma. In: J. P.Kim, B. S. Kim, and J-G. Park (eds.). Current Status of Cancer Control andImmunobiology. pp. 152-161, Seoul, Korea: Seoul Press. 1987.
10. Hoon, D. S. B., and Ramshaw, I. A. Chemoimmunotherapeutic effect ofcyclophosphamide on the highly metastatic MAT 13762 tumor. CancerImmunol. Immunother., 20: 175-178, 1985.
11. Hengst, J. C. D., Mokyr. M. B., and Dray, S. Correlation between cyclophosphamide tumoricidal activity and host antitumor immunity in the cureof mice bearing large MOPC-315 tumors. Cancer Res.. 41:1163-2167, 1981.
12. North, R. J. Cyclophosphamide-facilitated adoptive immunotherapy of anestablished tumor depends on elimination of tumor-induced suppressor Tcells. J. Exp. Med., 155: 1063-1074, 1982.
13. Reissmann, T., Voegeli, R., Pohl, J., and Hilgard, P. Augmentation of hostimmunity by low doses of cyclophosphamide and mafosfamide in two animaltumor models. Cancer Immunol. Immunother., 28: 179-184. 1989.
14. Livingston, P. O., Deleo, A. B., Jones, M., and Oettgen, H. F. Comparisonof approaches for augmenting the serologie response to the individuallyspecific methyl-cholanthracene-induced sarcoma-Meth A: pretreatment withcyclophosphamide is most effective. J. Immunol., 31: 2601-2606. 1983.
15. Berd, D., Danna, V., McGuire, H. C.. Jr., and Mastrangelo, M. J. Induction
of cell-mediated immunity to autologous melanoma cells and regression ofmétastasesafter treatment with melanoma cell vaccine preceded by cyclophosphamide. Cancer Res., 46: 2572-2577, 1986.
16. Ozer, H., Cowens, J. W., Colvin, M., Nussbaum-Blumenson, A., and Sheedy,D. In vitro effects of 4-hydroperoxyclophosphamide on human regulatory Tsubset function. I. Selective effects on lymphocyte function in T-B collaboration. J. Exp. Med.. 155: 276-290, 1982.
17. Askenase, P. W., Hayden, B. J., and Gershon, R. K. Augmention of delayed-type hypersensitivity by doses of cyclophosphamide which do not affectantibody responses. J. Exp. Med., 141:697-701, 1975.
18. Rollinghoff, M., Starzin-Powitz, A., Pfizenmaier, K., and Wagner, H. Cyclo-phosphamide-sensitive T lymphocytes suppress the in vitro generation ofantigen-specific cytotoxic T lymphocytes. J. Exp. Med., 145:455-459, 1977.
19. Cupps, T. R., Edgar, L. C., and Fauci, A. S. Suppression of human Blymphocyte function by cyclophosphamide. J. Immunol., 126: 2453-2457,1982.
20. Tai, T., Paulson, J. C., Cahan. L. D., and Irie, R. F. Ganglioside GM2 as atumor antigen (OFA-I-1). Proc. Nati. Acad. Sci. USA, 80: 5392-5396, 1983.
21. Tsuchida, T., Saxton, R. E., Morton, D. L., and Irie, R. F. Gangliosides ofhuman melanoma. J. Nati. Cancer. Inst., 78: 45-54, 1987.
22. Gupta. R. K., and Morton, D. L. Studies of melanoma tumor-associatedantigen detected in the spent culture medium of human melanoma cell linesby allogeneic antibody I. Purification and development of a radioimmuno-assay. J. Nati. Cancer. Inst., 72: 67-74, 1984.
23. Oh-Ishi, T., Goldman, C. K., Misiti, J., and Waldmann, T. A. Blockade ofthe interleukin-2 receptor of anti-Tac antibody inhibits the generation ofantigen-nonspecific suppressor T cells in vitro. Proc. Nati. Acad. Sci. USA,«5:6478-6482, 1988.
24. Reinherz, E. C., Morimoto, K. A., Fitzgerald, R. E., Hussey, J. F., Daley,and Schlossman, S. F. Heterogeneity of human T4+ inducer T cells definedby a monoclonal antibody that delineates two functional subpopulations. J.Immunol., 128: 463-468, 1982.
25. Nicholson, J. K. A., McDougal, J. S., Spira, T. J., Cross, G. D., Jones, B.M., and Reinherz, E. L. Immunoregulatory subsets of the T helper and Tsuppressor cell populations in homosexual men with chronic unexplainedlymphadenopathy. J. Clin. Invest., 73: 191-201, 1984.
26. Landay, A., Gartland, L., and Clement. A. T. Characterization of a pheno-typically distinct subpopulation of Leu-2-t- cells which suppresses T cellproliferative responses. J. Immunol., 131: 2757-2761, 1983.
27. Colton, T. Statistics in Medicine. Boston: Little, Brown and Company, 1974.28. Bast, R. C., Jr., Reinherz, E. L., Maver, C., Lavin, P., and Schlossman, S.
F. Contrasting effects of cyclophosphamide and prednisolone on the pheno-type of human peripheral blood leukocytes. Clin. Immunol. Immunopathol.,28: 101-114, 1983.
29. Berd, D., and Mastrangelo, M. J. Effect of low dose cyclophosphamide onthe immune system of cancer patients: depletion of CD4*, 2H4* suppressor-inducer T-cells. Cancer Res., 48: 1671-1675, 1988.
30. Livingston, P. O., Cunningham-Rundles, S., Marfleet, G., Gnecco, C., Wong,G. Y., Schiffman, G., Enker, W. E., and Hoffman, M. K. Inhibition ofsuppressor-cell activity by cyclophosphamide in patients with malignantmelanoma. J. Biol. Response Modif., 6: 392-403, 1987.
31. Kansas, G. S., and Engleman, E. G. Phenotypic identification of suppressor-effector, suppressor-amplifier and suppressor-inducer T cells of B cell differentiation in man. Eur. J. Immunol., 17: 453-457, 1987.
32. Reinherz, E. L., Meuer, S. C., and Schlossman, S. F. The human T cellreceptor: analysis with cytotoxic T cell clones. Immunol. Rev., 74: 83-112,1983.
33. Brock, N. Oxazaphosphorine cytostatics: past-present-future. Seventh CainMemorial Award Lecture. Cancer Res., 49: 1-7, 1989.
34. McBride, W. H., Hoon, D. B., Jung, T., Naungayan, J., Nizze, A., andMorton, D. L. Cyclophosphamide-induced alterations in human monocytefunctions. J. Leuk. Biol., 42: 659-666. 1987.
35. Balkwill. F. R., and Burke, F. The cytokine network. Immunol. Today, 10:299-304, 1989.
5364
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1990;50:5358-5364. Cancer Res Dave S. B. Hoon, Leland J. Foshag, Anne S. Nizze, et al. Vaccine and Low Dosages of CyclophosphamideReceiving Active Specific Immunotherapy with Melanoma Cell Suppressor Cell Activity in a Randomized Trial of Patients
Updated version
http://cancerres.aacrjournals.org/content/50/17/5358
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/50/17/5358To request permission to re-use all or part of this article, use this link
on June 5, 2018. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
![M-COM 5358 [PDF, 3.18MB]](https://static.fdocuments.net/doc/165x107/58904e9b1a28ab77318c04cf/m-com-5358-pdf-318mb.jpg)