
Supplementation of Mother’s Own Milk or Pooled Human Milk€¦ · Supplementation of Mother’s...
25
Supplementation of Mother’s Own Milk or Pooled Human Milk No supplement to human milk is usually needed if the infant is more than 1500 g at birth. The options for supplementing an infant’s own mother’s milk depend on need for additional vol- ume or for specific nutrients, especially protein, cal- cium, and phosphorus, based on birth weight and growth rates. 65, 66 538 Breastfeeding: A Guide for the Medical Profession
Transcript of Supplementation of Mother’s Own Milk or Pooled Human Milk€¦ · Supplementation of Mother’s...

Supplementation of Mother’s OwnMilk or Pooled Human Milk
No supplement to human milk is usually needed ifthe infant is more than 1500 g at birth.
The options for supplementing an infant’s ownmother’s milk depend on need for additional vol-ume or for speci�c nutrients, especially protein, cal-cium, and phosphorus, based on birth weight andgrowth rates.65,66
538 Breastfeeding: A Guide for the Medical Profession

BOX 15-10. Steps to Preserve the Nutrient Valueof Mother’s Milk
I. Most variable component: FatA. Lost in collection and storageB. Settles out on standingC. In one report fat content ranged from 2.2 to
4.7 g/dLD. Steps to enhance fat(1) Avoid separation of fat(2) Avoid continuous feeds(3)Utilize intermittent bolus feeds(4)Orient syringe of milk upward(5)Use short length of tubing(6) Empty syringe completely at end of
infusionE. Use hind milk preferentially if volume is
adequateII. Protein content declines from transitional to
mature milkA. Nutrient needs for premature are higher
III. Mineral content has increased bioavailability butcontent is lower than needs of premature infants.Vitamins A, C, and riboflavin levels decrease withcollection, storage, and delivery.
Premature Infants and Breastfeeding 539
The ideal supplementation is one using humanmilk nutrients and is referred to as lacto engineering,in which nutrient concentration is increased byadding specific nutrients derived from human milk.Techniques involve use of donor milk and separat-ing the cream and protein fractions, reducing thelactose content, and heat-treating the product witha high-temperature, short-time process of pasteur-ization. This completely human milk product pro-vides higher protein and energy needs so thatweight gains and nitrogen retention are similar tointrauterine rates.
Using a feeding prepared from human milk pro-tein andmedium-chain triglyceride supplementationof human milk for VLBW infants was reported byR€onnholm et al.119 Forty-four infants averaging30 weeks’ gestation with birth weights ranging from710 to 1510 g were nourished by one of four proto-cols: plain human milk, human milk and protein,human milk and triglycerides, or human milk andprotein and triglycerides. The triglycerides did notinfluence weight and length, but the two groupsreceiving added protein gained along a curve com-parable with the intrauterine growth for their birthweight, gaining faster from 4 to 6 weeks than theunsupplemented infants. The protein-supplementedgroups also grew more in length; however, head cir-cumference growth was similar in all groups.
Total protein is usually calculated by determin-ing the total nitrogen content (Kjeldahl method)and multiplying the number by the protein factor(6.25). Total protein corrected for nonproteinnitrogen, which is high in human milk, is true pro-tein.10 True protein is a heterogeneous mixture ofcasein and whey proteins. Whey proteins includelactoferrin, immunoglobulin, and lysozyme. Trueprotein minus those more or less indigestible pro-teins is called digestible protein. Analysis of pretermmilk by Beijers et al.10 demonstrated that nonpro-tein nitrogen was dependent on the degree of pre-maturity and averaged 20% to 25%, increasingduring the time of lactation. Only 30% to 60%of total protein is available for synthesis. However,in absolute amounts over lactation time, it remainsstable.
Schanler et al. compared plasma amino acidlevels in VLBW infants (mean age 16 days, meanbirth weight 1180 g, mean gestation 29 weeks)fed either human milk fortified with human milkor whey-dominant cow milk formula. The infantsreceived continuous enteral infusions of isonitrog-enous, isocaloric preparations. Taurine and cys-tine were significantly higher in the infants fedhuman milk, and threonine, valine, methionine,and lysine were significantly higher in the infantsfed formula.
Mother’s own milk shows a wide variability innutrient components when being pumped for a
hospitalized premature infant. Nutrient supplemen-tation is necessary to maintain adequate growthand good nutritional status. According to Hermanand Schanler,58 extraordinary efforts should bemade to use mother’s own milk because the advan-tages of nonnutrient components in human milk aresignificantly diminished by storage and heat pro-cessing. The most variable constituent is fat(Box 15-10). Protein does not meet the needs ofa small premature. Although levels of minerals(Ca, P) are stable, the needs of VLBW infantsrequire supplementation. Substantial benefits ofmother’s own milk include reduced infection,enhanced neurodevelopmental outcome, andhealthy postnatal growth. The minimum dose ofmother’s milk when given with various fortifica-tions has been found to be more than 50 mL/kg/day to protect against infection, especially late-onset sepsis.47 A systemic review looking at multi-nutrient fortification for human milk involved 10trials and a total of more than 600 infants weighingless than 1800 g.73 It clearly showed improvementin weight gain increments in length, head circum-ference, and BMC compared with unsupplementedmilk. Neurodevelopmental outcomes were signifi-cantly improved with mother’s milk. The magni-tude of the effect was seen as mother’s milkintake increased to 110 mL/kg/day; the develop-mental scales showed an increase of five points,an important gain for these ELBW infants. Preterminfants have lower energy expenditure when theyare fed breast milk than when they are fed preterminfant formula.

540 Breastfeeding: A Guide for the Medical Profession
Preterm infants with birth weights from 750 to1250 g were randomly assigned to a cream or con-trol group. The cream group received a humanmilk-derived cream supplement if the energy den-sity of the human milk tested below 20 kcal/oz,measured using a near infrared human milk ana-lyzer. The control group received their mother’sown milk or donor human milk with donor humanmilk-derived fortifier. Premature infants whoreceived human milk-derived cream as a fortifierhad improved weight and length compared to thecontrol group. Cream can be used as an adjunctivesupplement to an exclusive human milk-based dietto improve growth rates (see Figure 15-6 ProlactCRTM Human Milk Caloric Fortifier).
All preterm infants should receive human milkfortified with protein, minerals, and vitamins whenbirth weight is less than 1500 g according to theAmerican Academy of Pediatrics’ section onbreastfeeding.
Artificial Fortification ofHuman Milk
No longer is supplementing an infant’s ownmother’s milk with specially prepared formula sup-plements necessary. Available commercial prepara-tions for such supplementation were intended tocomplement human milk and not to be used as anexclusive formula. When multicomponent fortifiedhuman milk product for promoting growth in pre-term infants was examined in a Cochrane Review,74
the authors found short-term increases in weightgain, linear growth, and head circumference. Noeffect was seen on serum alkaline phosphataselevels, and the effect on BMC was unclear. Nitro-gen retention and blood urea levels were increased.Conclusions about long-term neurodevelopmentaland growth outcomes were limited by insufficientdata after 1 year. The significance of increasedblood urea nitrogen and blood pH levels wasunclear. Preparations are different and are used dif-ferently (Table 15-9). The powdered supplement isintended to add special nutrients to an adequatevolume of mother’s own milk (Enfamil humanmilk fortifier or Similac human milk fortifier), orit can be used to enhance pooled donor humanmilk. Neither fortifier contains fat. Milk fortifica-tion extends the mother’s milk and provides addi-tional nitrogen, calcium, phosphorus, andvitamins for an LBW infant. If an infant is fed themother’s milk, pooled donor milk, and a fortifier,the sum total should meet the infant’s daily require-ments (Table 15-10). Any addition of artificial for-mula interferes with the infection protectionqualities and other benefits of human milk so useof formula-based supplementation should be
avoided unless human milk-based formula is notavailable. Preventing one case of NEC saves$100,000.
Studies comparing fortified mother’s milk withpremature infant formulas have shown comparablegrowth in weight, length, and head circumference.This makes it possible to lose many advantages of amother’s milk, while providing the additional nutri-ents for appropriate accretion rates.127
When powdered fortifier was added to amother’s milk, the supplemented infants had signif-icantly greater weight gain, linear growth, and headcircumference growth than those not supplement-ed. The supplemented infants also had higherblood urea nitrogen levels (Table 15-11).53 Theloss of human milk benefits is of significantconcern.
When a preterm infant’s own mother’s milk wasfortified with protein (0.85 g/dL), calcium (90 mg/dL), and phosphorus (45 mg/dL), the rate of weightgain was greater than that of the unfortified groupand comparable with that of the Similac NaturalCare formula group.50–52 Bone mineralizationimproved during the 6 weeks of the study but didnot reach the intrauterine accretion rate of150 mg/kg/day. A relative phosphorus deficiencyoccurred in the human milk groups, both withand without supplementation. Fortifying pretermmother’s milk permits biochemically adequategrowth comparable with that provided by specialcare formula (Table 15-12).
The effect of calcium supplementation on fattyacid balance studies in LBW infants fed human milkor formula has been shown to be significant. Adecrease in total fatty acid absorption both inLBW infants fed their own mother’s milk and informula-fed infants was seen when calcium wasadded. Fecal output of fat and fatty acid excretionwas higher in the formula-fed infants. In mother’smilk-fed infants, the total fat absorption and thecoefficient of absorption were higher.
Preterm milk with routine multivitamin supple-mentation (providing 4.1 mg of tocopherol) uni-formly resulted in vitamin sufficiency in VLBWinfants in a control study by Gross and Gabriel.54
This was true when they received iron, as well aswhen they were not iron supplemented. VLBWinfants were fed preterm milk, bank milk, or for-mula, utilizing 2 mg/day of iron. Vitamin E contentof preterm milk does not differ significantly fromthat of term human milk from days 3 to 36.56
Jocson et al.68 studied the effects of nutrient for-tification and varying storage conditions on host-defense properties of human milk. Total bacterialcolony counts and immunoglobulin A (IgA) werenot affected by the addition of fortifier.
The effect of powdered human milk fortifiers onthe antibacterial actions of human milk were

TABLE 15-9 Composition of Infant Feeding Using Human Milk With and Without Various Supplements
PretermHuman Milk
SimilacNaturalCare
50:50 MixSimilac NaturalCare and PretermHuman Milk∗
EnfamilHuman MilkFortifier (fourpackets)
Enfamil HumanMilk Fortifier (fourpackets) Added toPreterm HumanMilk∗
Weeks postpartum 1 4 1 4 1 4
Kilocalories 67 70 81 72 76 14 81 84
Protein (g) 2.44 1.81 2.1 2.27 1.96 0.7 3.14 2.5
Carbohydrate (g) 6.05 6.95 8.6 7.3 7.8 2.7 8.75 9.65
Fat (g) 3.81 4.00 3.6 3.7 3.8 0.04 3.85 4.04
Vitamin A (IU)† 330 230 550 440 390 780 1110 1010
Vitamin E (mg)† 0.9 0.25 3 2.0 1.61 3.4 4.3 3.65
Vitamin K (mcg)† NA 1.5 10 NA 5.8 9.1 NA 10.6
Vitamin D (IU)† NA 2.5 120 NA 61 260 NA 262
Thiamin (mcg) 5.4 8.9 200 103 104 187 192 196
Riboflavin (mcg) 36.0 26.6 500 268 263 250 286 277
Niacin (mg) 0.11 0.21 4.0 2.1 2.1 3.1 3.2 3.3
Pyridoxine (mcg) 2.6 6.2 200 101 103 193 196 199
Folate (mcg) 2.1 3.1 30 16.1 16.6 23 25 26
Vitamin B12 (mcg) NA 0.1 0.45 NA 0.27 0.21 NA 0.3
Vitamin C (mg)† 7 5 30 19 18 24 31 29
Calcium (mg) 25 22 170 98 96 60 85 82
Phosphorus (mg) 14 14 85 50 50 33 47 47
Magnesium (mg) 3 2.5 10 6.5 6.3 4 7 6.5
Iron (mg) 0.1 0.1 0.3 0.2 0.2 0 0.1 0.1
Sodium (mEq) 2.2 1.3 1.7 2.0 1.5 0.3 2.5 1.6
Potassium (mEq) 1.8 1.7 2.9 2.4 2.3 0.4 2.2 2.1
Chloride (mEq) 2.5 1.6 2.0 2.3 1.8 0.5 3.0 2.1
Zinc (mg) 0.48 0.39 1.2 0.84 0.80 0.31 0.79 0.70
Copper (mg) 0.08 0.06 0.2 0.14 0.13 0.08 0.16 0.14
Manganese (mcg)† NA 0.4 NA NA NA 9 NA 9.4
Biotin (mcg) 0.15 0.54 NA NA NA 0.8 0.95 1.34
Pantothenic acid (mg) 0.16 0.23 1.5 0.83 0.87 0.79 0.95 1.02
Osmolality (mOsm/kg H2O)† 302 305 300 301 303 +60 362 365
*Volume 100 mL (1 dL).†Listed values for 1 and 4 weeks reflect reported values for full-term transitional and mature human milk, respectively.
IU, International units; NA, not available.
TABLE 15-10 Protein, Calcium, and SodiumRequirements by GrowingPremature Infants and Compositionof Banked Human Milk
Protein(g/100 kcal)
Calcium(mg/100 kcal)
Sodium(mEq/100 kcal)
Estimatedrequirements forhypothetic, growingpremature infants∗
2.54 132† 2.3
Composition ofbanked human milk
1.50 43 0.8
*Assumed body weight is 1200 g; weight gain, 20 g/day;energy intake, 120 kcal/kg/day. The basis for estimatingrequirements is described in the text.
†This estimate does not apply to infants fed formulas fromwhich calcium absorption is less than 65% of intake.
From Fomon SJ, Ziegler EE, VazquezHD:Humanmilk andthe small premature infant, Am J Dis Child 131:463, 1977.
TABLE 15-11 Fortified Versus UnfortifiedHuman Milk
Growth Fortified
13 studies, 596 infants; randomized∗Weight gain +3.7 g/kg/day
Length +0.13 cm/wk
Head circumference +0.12 cm/wk
Bone mineral content +8.3 mg/cm
Nitrogen balance +66 mg/kg/day
BUN +5.8 mg/dL
Necrotizing enterocolitis No significant difference
Feeding tolerance No significant difference
*Some comparisons with partial supplements.BUN, Blood urea nitrogen.From Kuschel CA, Harding JE: Multicomponent fortified
human milk for promoting growth in preterm infants(Cochrane Review). In The Cochrane Library, Issue 4,Chichester, 2004, John Wiley and Sons.

TABLE 15-12 Comparison of Selected Fortifiers for Human Milk (Prepared per 100 mL Milk)
Fortifier PrHM EHMF SNC Eoprotin∗ S-26/SMA HMF FM85† SHMF
Energy (kJ) (kcal) 298 (71) 357 (85) 319 (76) 357 (85) 361 (86) 374 (89) 357 (85)
Fat (g) 3.6 3.6{ 4.0 3.6{ 3.65 3.6 4.0
Carbohydrate (g) 7.0 9.7 7.8 9.8 9.4 10.6 8.8
Protein (g) 1.8 2.5 2.0 2.6 2.8 2.6 2.8
Calcium (mg) 22 112 97 72 112 73 139
Phosphorus (mg) 14 59 50 48 59 48 81
Magnesium (mg) 2.5 3.5 6.3 5.3 4.0 4.5 9.5
Sodium (mEq) 0.7 1.0 1.1 1.9 1.1 1.9 1.35
Zinc (mcg) 320 1030 760 320{ 450 320{ 1320
Copper (mcg) 60 122 1045 60{ 60{ 60{ 230
Vitamins Yes Multi} Multi} A, C, E, K Multi} Multi} Multi}
*Milupa, Friedrichsdorf, Germany.†Nestle, Vevey, Switzerland.{Nutrient not contained in fortifier.}Multivitamins: A, D, E, K, B1, B2, B6, C, B12, niacin, folate, pantothenate, and biotin.
EHMF, Enfamil Human Milk Fortifier (Mead Johnson Nutritionals, Evansville, Ind.); HMF, human milk-fed; PrHM, pretermhuman milk; S-26/SMA HMF, SMA Human Milk Fortifier (Wyeth Nutritionals, Philadelphia, Pa.); SHMF, Similac Human MilkFortifier (Ross Laboratories, Columbus, Ohio); SNC, Similac Natural Care (Ross Laboratories, Columbus, Ohio) mixed 1:1 (vol:vol) with PrHM.From Schanler RJ: The use of human milk for premature infants, Pediatr Clin North Am 48:207, 2001.
1001
2
3
4
200
300
400
40 90 120 180
Figure 15-7. WHO technical report on optimal feeding forLBW infants.
542 Breastfeeding: A Guide for the Medical Profession
explored by Chan.24 Human milk inhibited thegrowth of Escherichia coli, Staphylococcus aureus, Enter-obacter sakazakii, and group B Streptococcuswhen Enfa-mil and Similac human milk fortifiers were mixedwith humanmilk, along withmedium-chain triglyc-erides and 1.09 mg ferrous sulfate (in 25 mL milk).The fortifiers containing iron and the iron aloneinhibited the protective effect of human milkagainst the bacteria. The probable explanation isthe interference of iron with the protective actionof lactoferrin in human milk. The ferrous iron inthe fortifier is changed to a ferric state in humanmilk, which readily binds with lactoferrin.
Concerns over the nutrient content of supple-mented human milk have been expressed by manyauthors since the early work on premature infantsfrom the Houston group.125 After noting growthfailure in some premature infants, it was discoveredthat some mother’s milk was lower in calories than20 kcal/oz. This has been reported by Prolacta Bio-logicals, which tests the protein and caloric contentof all donations. This is a major issue for prematureinfants who have a restricted fluid intake inthe early months of life. Preterm infants fed acommercially prepared, bovine-based human milkfortifier receive less protein than they need, accord-ing to Arslanoglu et al.7 They tested the actualnutrient intakes observed in a previously reportedstudy, with assumed nutrient intakes based on theusual assumptions about the composition of humanmilk. Actual protein intakes were significantly andconsistently lower than the levels assumed based onthe standard protein content of human milk. Actual
intakes of protein by preterm infants fed bovine-fortified human milk were significantly lower, espe-cially after 3 weeks postpartum when the mother’smilk no longer had the higher protein contentof the milk of a mother who delivers prematurely.Calorie content was not significantly lower(Figure 15-7).
The Committee on Nutrition of the AAP hasoutlined requirements for the premature infantwho is less than 27 weeks’ gestation and less than1000 g at birth, regarding calcium and vitamin D.Bone mineral status should be started by 4 to5 weeks after birth. Alkaline phosphatase above800 to 1000 IU/L or clinical evidence of fracturesrequire radiographic evaluation. A persistent serumphosphorus concentration less than 4 mg/dLshould be monitored and supplementation withphosphorus considered. Postdischarge monitoring

BOX 15-11. Protein Recommendations
• Categorized by life stage and gender, becauseamong healthy individuals, these are the twoparameters responsible for variations in the body’sneed for protein� The Pediatrics Stage has been subdivided into sixgroupings: infancy, 0 to 6 months of age; infancy, 7to 12 months of age; toddlers, 1 to 3 years of age;early childhood, 4 to 8 years of age; puberty, 9 to13 years of age; and adolescence, 14 to 18 years ofage
• Optimal food for full-term infants is human milk� Recommended that it be the sole source ofnutrition for infants during the first 6 months oflife
� On average, infants to 6 months of age consume0.78 L of milk per day
• Average value of 11.7 g/L used to calculateadequate intake for protein
• Nonprotein nitrogen component of human milkcontains substantial quantities of taurine, which isvirtually absent from cow milk
• Human milk proteins have a high nutritionalquality and are digested and absorbed moreefficiently than cow milk proteins
• Breastfed infants’ protein intakes appear to satisfythe infant requirements for maintenance andgrowth without an amino acid or solute excess
Data from Rigo J, Senterre J: Nutritional needs of prematureinfants: current issues, J Pediatr 149:880, 2006; Kleinman RE,editor: Pediatric nutrition, ed 7, 2013, American Academy ofPediatrics; and World Health Organization: Protein and aminoacid requirements in human nutrition, Geneva, 2007, World HealthOrganization.
Premature Infants and Breastfeeding 543
is also necessary if exclusively breastfed. When theinfant reaches 1500 g, vitamin D intake should be400 IU/day minimum and up to a maximum of1000 IU/day. A mineral intake between 100 and166 mg/kg/day of highly absorbed calcium and60 to 75 mg/kg/day of phosphorus is recommendedto provide appropriate mineralization. Proteinrequirement is considered to be a matter of somedebate, as human milk protein is readily absorbed,and bovine protein is less well absorbed. Therevised recommendations for protein appear inBox 15-11. These adjustments were an effort toreduce metabolic stress from protein overloadand unbalanced amino acid supply. Human milkhas the ideal balance of casein and whey.
Fortification of Human Milk withHuman Milk
The problem of adding nutrients to mothers’ milkto meet the increased nutrient needs of prematureinfants, especially ELBW premature infants, has
challenged neonatologists for years. The commer-cial products developed from a bovine milk basehave been widely used and have improved thenutrient intake of these infants. The theoreticalconcern about the impact of bovine milk on theinfection protection properties of human milk hasbeen argued.62 A minimum of 50 mL/kg/day ofthe mother’s milk is deemed necessary to maintainthe protection provided by the mother’s milk. Anumber of investigators have explored the possibil-ity of a fortifier made out of human milk, so thefeeding would meet needs with entirely humanconstituents. The antibacterial activity inherent inhuman milk was inhibited when a bovine-based for-tifier containing added iron was mixed with humanmilk. Chan et al.25 tested the same antibacterialactivity when a newly derived human milk-basedproduct became available (Prolacta Bioscience,Monrovia, Calif.). Human milk samples from 10fully lactating mothers were utilized to test theeffect on the antimicrobial activity of human milk,milk plus bovine fortifier, and milk plus human milkfortifier against Ent. sakazakii, E. coli, Clostridium diffi-cile, and Shigella soneii. Human milk inhibited thegrowth of all the test organisms. The antibacterialactivity was almost completely inhibited by theaddition of the bovine-based fortifier. The activitywas unaffected by the addition of human milk-based fortifier. Further studies of human milk-basedfortifier (H2MF) have been conducted at nationaland international sites. The fortifier (H2MF) isavailable from Prolacta Bioscience. Preliminaryresults from University of Florida, Schneider’sChildren’s Hospital, Baylor College of Medicine,and Yale-New Haven Medical Center werereported on 207 extremely premature infants whosemothers intended to provide their milk. The infantswere randomized to one of three groups: mother’smilk plus (HUM40) or 100 mL/kg/day (HUM100);the third group received mother’s milk plus100 mL/kg/day of the bovine-based product(Table 15-13). The groups had similar lengths ofstay and rates of growth, chronic lung disease,and sepsis. However, significantly lower rates ofNEC, surgical NEC, and combined deaths wereobserved with the human-based fortifier. Furtherresults are available from other participating centersand all involved patients.
Long-Term Follow-Up of GrowthParameters in VLBW Infants
Weight gain and growth in length and head cir-cumference are similar in VLBW infants who arebreastfed or given standard formula after discharge.BMC was also followed at 10, 16, and 25 postnatal

TABLE 15-13 Use of Human Milk Fortifier Made from Human Milk
BOV HUM40 HUM100 p value∗
N 69 71 67
Gestation (wk)† 27.3�2.0 27.2�2.3 27.2�2.2 NS
Birth weight (g)† 922�197 921�188 945�202 NS
OMM consumed, mL(% of enteral intake){
5676 (82%) 4539 (70%) 4048 (73%) NS
Days of PN{ 22 20 20 NS
NEC, n (%) 11 (15.9) 5 (7.0) 3 (4.5) 0.05
Surgical NEC, n (%) 8 (11.6) 1 (1.4) 1 (1.5) 0.007
Death, n (%) 5 (7.2) 2 (2.8) 1 (1.5) NS
Death or NEC, n (%) 14 (20.3) 6 (8.5) 5 (7.5) 0.04
Results: The groups had similar lengths of stay and rates of growth, CLD, and sepsis. Other results are shown.BOV, Bovine; CLD, central line day; HUM40, human milk (mother’s milk) plus fortifier (Prolacta Bioscience); HUM100,
human milk (mother’s milk) 100 mL/kg/day; OMM, own mother’s milk; PN, parenteral nutrition; NEC, necrotizingenterocolitis.*Chi-square, Kruskal-Wallis, log-rank test.†Mean�SD.{Median.From Sullivan S, Schanler R, Abrams S, et al: Abstract at PAS 2009. #2155.1Neonatal nutrition and follow up 5/2/09. Sullivan
S, Schanler R, Abrams S, et al: A randomized controlled trial of human versus bovine-based human milk fortifier in extremelypreterm infants, Baltimore, Md., 2009, PAS Meetings.
544 Breastfeeding: A Guide for the Medical Profession
weeks in those graduates from the NICU who hadformerly received fortified human milk. At 16 and25 weeks, the breastfed infants had lower BMCand BMC/bone width ratio, as well as serum phos-phorus concentration and higher alkaline phos-phate activity than the formula-fed group. Thesedata suggest a need to carefully monitor this selectgroup of VLBW infants for suboptimal bone accre-tion while receiving their mother’s milk. However,human milk-based fortifier should solve thisproblem.57
Reduced bone mineralization is common in pre-term infants and has been associated with growthstunting at 18 months of age and dietary insuffi-ciency of calcium and phosphorus. Bishop et al.16
evaluated 54 children at a mean age of 5 yearswho were born prematurely and had been part ofa longitudinal dietary growth study. The dietsincluded were either banked donor milk or pretermformula as a supplement to the mothers’ own milk.Increased human milk intake was strongly associ-ated with better BMC. Those children who hadthe greater proportion of human milk had greaterBMC than children born at term. That is, supple-menting with donor milk produced a better out-come at age 5 years than supplementing withinfant formula, even though the nutrient contentof formula was greater. The later skeletal growthand mineralization of an infant can be calculatedand feeding adjusted to add necessary mineraliza-tion with human milk-based supplements.
Iron status has also been studied in LBW infantsat 6 months’ chronologic age. The incidence of irondeficiency was 86% in the breastfed group of LBW
infants and only 33% in those receiving iron-fortified formula.2 The breastfed group had signif-icantly lower serum ferritin and hemoglobin valuesat 4 months of age. Abouelfettoh et al.1 recom-mended that these special breastfed infants shouldreceive iron from 2 months of age, because theywere developed.
The AAP recommends that infants less than1500 g birth weight receive 4 mg/kg/day of iron.There were no studies to test this until Taylorand Kennedy compared the effect of 2 mg/kg/dayin a multivitamin on the hematocrit at 36 weeks’postmenstrual age. It was concluded that this irontherapy for infants under 1500 g at birth, in addi-tion to dietary intake, did not improve the hemat-ocrit or the number of transfusions requiredcompared to the controls who received noadditional iron.
The feeding of these special VLBW infants afterdischarge and for the next 6 to 9 months is animportant consideration. Breastfeeding with addedsupplementation has been studied. Some importantresults came from a randomized, double-blind trialof the effect of supplementary standard formulafeedings.84 Growth and clinical status of infantsreceiving nutrient-enriched “postdischarge” for-mula were significantly affected, without vomiting,gas, or stool problems. The group receiving theenriched formula ingested volumes similar to thosereceiving regular formula.
A large multicenter follow-up study of morethan 1000 ELBW infants who had extensive nutri-tional data collected was reported by Vohr et al.136
Birth weight, gestational age, intraventricular

BOX 15-12. Feeding Schedule for Human Milk inLow-Birth-Weight Infants
1. Use refrigerated milk from the preterm infant’smother when it is available and has been collectedwithin 48 hours of feeding.
2. When fresh milk is not available, use frozen humanmilk from the infant’s mother. This milk should beprovided in the sequence that it was collected toprovide the greatest nutritional benefit.
3. When the preterm infant is tolerating human milkat greater than 100 mL/kg/day, supplementationusing a human milk fortifier is started.a. If it requires more than 1 week to reach
100 mL/kg/day intake, fortifier is addedeven though volume tolerance has notbeen achieved.
b. Milk volumes should increase to 150 butnot exceed 200 mL/kg/day. Weight gain isoptimally 15 g/kg/day and length increment1 cm/wk. Urinary excretion of calcium shouldbe less than 6 mg/kg/day and phosphorusgreater than 4 mg/kg/day.
c. If weight gain is less than 15 g/kg/day, hindmilk is used if mother’s milk productionexceeds the infant’s requirements by 30%.
4. If the mother’s milk supply is inadequate to meether infant’s feeding needs, an infant formuladesigned for preterm feeding is used as described.
5. Fortification of human milk is recommended untilthe infant is taking all feedings from the breastdirectly or weighs 1800 to 2000 g, depending onnursery policy on infant discharge weight. During
Premature Infants and Breastfeeding 545
hemorrhage status, sepsis, bronchopulmonary dys-plasia, and hospital stay were similar between thosenever receiving human milk and those for whomvariables of socioeconomic status, race, ethnicity,educational attainment, and parity were adjusted.Effects of human milk intake on mental and motordevelopment were significantly positive. Theimpact of receiving 110 mL/kg/day of human milkwas correlated with a 5-point increase on the Bay-ley scales. Human milk feedings affect scores evenwhen donor milk is used, compared with termformula.19
Infants fed breast milk were found to have fasterbrainstem maturation, compared to those infantswho received formula. This was determined by ananalysis of the rate of maturation of the BAERs(auditory evoked response). Components of humanmilk improved cognitive and neurological out-comes in a series of studies on VLBW infants. Lackof breastfeeding was a major predictor of poor cog-nitive outcome in very preterm infants, comparedto low social status and cerebral lesions byultrasound.
The association of human milk feedings with areduction in retinopathy of prematurity amongVLBW infants compared to formula-fed infants,after adjusting for confounding variables, is signif-icant. It can be considered as available intervention.
Box 15-12 lists recommendations modified fromthe work of Tsang et al.123a and Schanler andHurst.
the transition from feeding human milk by gavageor bottle and nipple to feeding at the breast, onlythose feedings given by gavage or bottle requirefortification.
6. Multivitamin supplementation is started oncefeeding tolerance has been established. Thissupplementation varies depending on thecomposition of human milk fortifier.
7. Iron supplementation providing 2 mg/kg/day isstarted by the time the infant has doubled birthweight.
Antimicrobial Properties of PretermBreast Milk
The infection-protective properties of human milkhave been considered to be a key reason to providehuman milk to high-risk infants who are prone todevastating infections such as NEC, sepsis, andmeningitis and viral infections such as respiratorysyncytial virus and rotavirus. The antimicrobialproperties of milk produced by mothers whodeliver preterm have been studied by severalinvestigators.
The antiinfective factors in preterm humancolostrum were studied by Mathur et al.,95 whocompared the colostrum values of a comparablegroup of postpartum mothers. The mean concen-trations of IgA, lysozyme, and lactoferrin were sig-nificantly higher than in full-term colostrum. IgGand IgM were similar in both groups. The absolutecounts of total cells, macrophages, lymphocytes,and neutrophils were significantly higher in pre-term colostrum. The mean percentage of IgA inthe premature colostrum was also significantlyhigher. The degree of prematurity had no effect,although the study group ranged in gestation from
28 to 36 weeks (mean 33�2.1 weeks), comparedwith the control infants, whowere at 38 to 40 weeks(mean 39.1�0.8 weeks). The colostrum of pretermmothers had an even greater potential for prevent-ing infection than term colostrum and are an addi-tional reason to begin early enteral feeds withhuman colostrum.95 Table 15-14 lists the specificantiinfective components.
The cells of preterm milk were compared withthose of termmilk and found to be similar in numberand in capacity to phagocytose and kill staphylo-cocci.108 The ability of the preterm cells to produceinterferon on stimulation with mitogens was mar-ginally better than that of term cells. The cells sur-vived 24 hours refrigerated at 4°C (39.2°F);
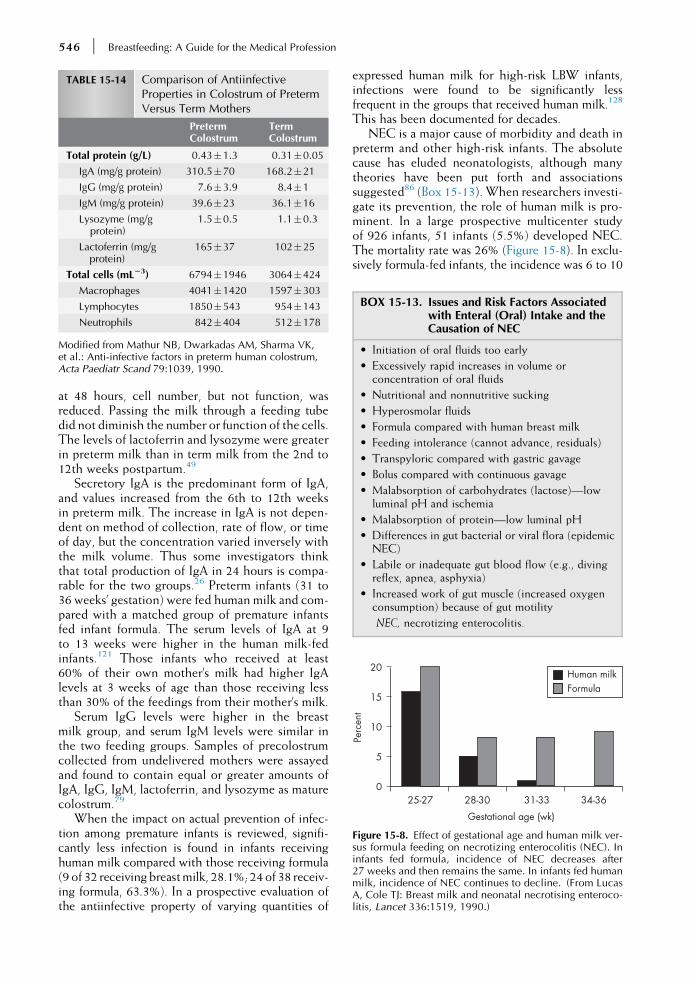
TABLE 15-14 Comparison of AntiinfectiveProperties in Colostrum of PretermVersus Term Mothers
PretermColostrum
TermColostrum
Total protein (g/L) 0.43�1.3 0.31�0.05
IgA (mg/g protein) 310.5�70 168.2�21
IgG (mg/g protein) 7.6�3.9 8.4�1
IgM (mg/g protein) 39.6�23 36.1�16
Lysozyme (mg/gprotein)
1.5�0.5 1.1�0.3
Lactoferrin (mg/gprotein)
165�37 102�25
Total cells (mL23) 6794�1946 3064�424
Macrophages 4041�1420 1597�303
Lymphocytes 1850�543 954�143
Neutrophils 842�404 512�178
Modified from Mathur NB, Dwarkadas AM, Sharma VK,et al.: Anti-infective factors in preterm human colostrum,Acta Paediatr Scand 79:1039, 1990.
BOX 15-13. Issues and Risk Factors Associatedwith Enteral (Oral) Intake and theCausation of NEC
• Initiation of oral fluids too early
• Excessively rapid increases in volume orconcentration of oral fluids
• Nutritional and nonnutritive sucking
• Hyperosmolar fluids
• Formula compared with human breast milk
• Feeding intolerance (cannot advance, residuals)
• Transpyloric compared with gastric gavage
• Bolus compared with continuous gavage
• Malabsorption of carbohydrates (lactose)—lowluminal pH and ischemia
• Malabsorption of protein—low luminal pH
• Differences in gut bacterial or viral flora (epidemicNEC)
• Labile or inadequate gut blood flow (e.g., divingreflex, apnea, asphyxia)
• Increased work of gut muscle (increased oxygenconsumption) because of gut motility
NEC, necrotizing enterocolitis.
Gestational age (wk)
20
15
10
5
0
Perc
ent
25-27 28-30 31-33 34-36
Human milkFormula
Figure 15-8. Effect of gestational age and human milk ver-sus formula feeding on necrotizing enterocolitis (NEC). Ininfants fed formula, incidence of NEC decreases after27 weeks and then remains the same. In infants fed humanmilk, incidence of NEC continues to decline. (From LucasA, Cole TJ: Breast milk and neonatal necrotising enteroco-litis, Lancet 336:1519, 1990.)
546 Breastfeeding: A Guide for the Medical Profession
at 48 hours, cell number, but not function, wasreduced. Passing the milk through a feeding tubedid not diminish the number or function of the cells.The levels of lactoferrin and lysozyme were greaterin preterm milk than in term milk from the 2nd to12th weeks postpartum.49
Secretory IgA is the predominant form of IgA,and values increased from the 6th to 12th weeksin preterm milk. The increase in IgA is not depen-dent on method of collection, rate of flow, or timeof day, but the concentration varied inversely withthe milk volume. Thus some investigators thinkthat total production of IgA in 24 hours is compa-rable for the two groups.26 Preterm infants (31 to36 weeks’ gestation) were fed human milk and com-pared with a matched group of premature infantsfed infant formula. The serum levels of IgA at 9to 13 weeks were higher in the human milk-fedinfants.121 Those infants who received at least60% of their own mother’s milk had higher IgAlevels at 3 weeks of age than those receiving lessthan 30% of the feedings from their mother’s milk.
Serum IgG levels were higher in the breastmilk group, and serum IgM levels were similar inthe two feeding groups. Samples of precolostrumcollected from undelivered mothers were assayedand found to contain equal or greater amounts ofIgA, IgG, IgM, lactoferrin, and lysozyme as maturecolostrum.79
When the impact on actual prevention of infec-tion among premature infants is reviewed, signifi-cantly less infection is found in infants receivinghuman milk compared with those receiving formula(9 of 32 receiving breastmilk, 28.1%; 24 of 38 receiv-ing formula, 63.3%). In a prospective evaluation ofthe antiinfective property of varying quantities of
expressed human milk for high-risk LBW infants,infections were found to be significantly lessfrequent in the groups that received human milk.128
This has been documented for decades.NEC is a major cause of morbidity and death in
preterm and other high-risk infants. The absolutecause has eluded neonatologists, although manytheories have been put forth and associationssuggested86 (Box 15-13). When researchers investi-gate its prevention, the role of human milk is pro-minent. In a large prospective multicenter studyof 926 infants, 51 infants (5.5%) developed NEC.The mortality rate was 26% (Figure 15-8). In exclu-sively formula-fed infants, the incidence was 6 to 10
Premature Infants and Breastfeeding 547
times more common than in those who receivedhuman milk exclusively. In those who receivedhuman milk and formula, it was three times morecommon than in the exclusively breastfed group.Pasteurization did not diminish the effect of humanmilk in these studies.86,128 The comparison wasmore dramatic at more than 30 weeks’ gestation,when formula-fed infants were 20 times more aptto develop NEC than human milk-fed infants. Earlyenteral feeding did not change the risk in thosereceiving breast milk, whereas delaying feedingsof formula did lower the rate of NEC.75 In a studyof the prevention of NEC in LBW infants, withfeedings higher in IgA and IgG, none of the infantsin the study group or the breastfeeding comparisongroup developed NEC. Six cases developed amongthe 91 infants in the untreated group.37
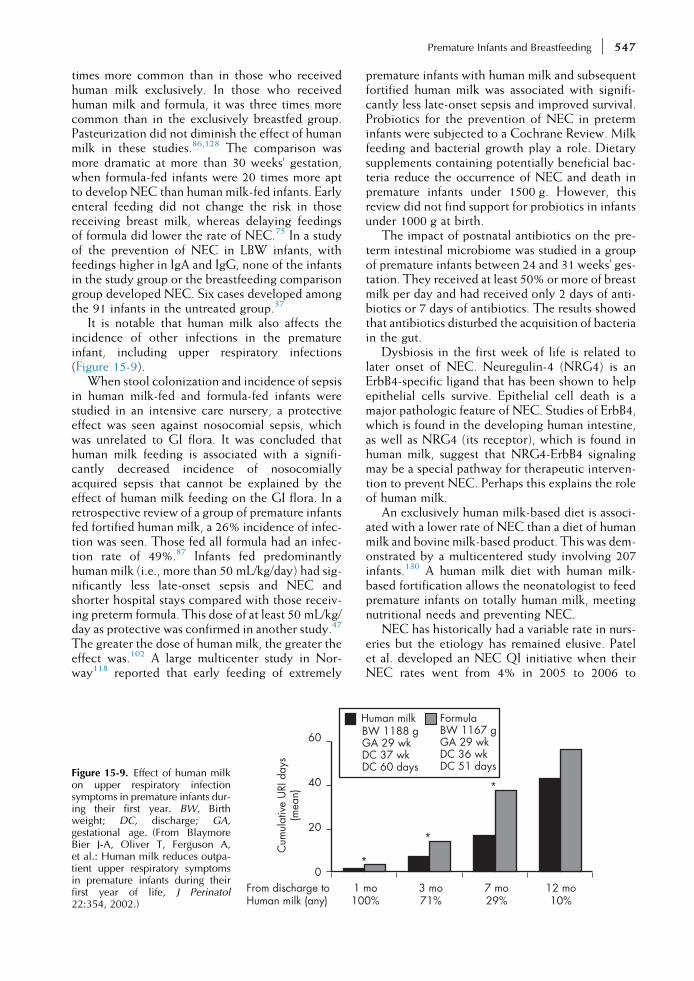
It is notable that human milk also affects theincidence of other infections in the prematureinfant, including upper respiratory infections(Figure 15-9).
When stool colonization and incidence of sepsisin human milk-fed and formula-fed infants werestudied in an intensive care nursery, a protectiveeffect was seen against nosocomial sepsis, whichwas unrelated to GI flora. It was concluded thathuman milk feeding is associated with a signifi-cantly decreased incidence of nosocomiallyacquired sepsis that cannot be explained by theeffect of human milk feeding on the GI flora. In aretrospective review of a group of premature infantsfed fortified human milk, a 26% incidence of infec-tion was seen. Those fed all formula had an infec-tion rate of 49%.87 Infants fed predominantlyhuman milk (i.e., more than 50 mL/kg/day) had sig-nificantly less late-onset sepsis and NEC andshorter hospital stays compared with those receiv-ing preterm formula. This dose of at least 50 mL/kg/day as protective was confirmed in another study.47
The greater the dose of human milk, the greater theeffect was.102 A large multicenter study in Nor-way118 reported that early feeding of extremely
*
60
40
20
0
Cum
ulat
ive
URI
day
s(m
ean)
1 10
H
From discharge toHuman milk (any)
Figure 15-9. Effect of human milkon upper respiratory infectionsymptoms in premature infants dur-ing their first year. BW, Birthweight; DC, discharge; GA,gestational age. (From BlaymoreBier J-A, Oliver T, Ferguson A,et al.: Human milk reduces outpa-tient upper respiratory symptomsin premature infants during theirfirst year of life, J Perinatol22:354, 2002.)
premature infants with human milk and subsequentfortified human milk was associated with signifi-cantly less late-onset sepsis and improved survival.Probiotics for the prevention of NEC in preterminfants were subjected to a Cochrane Review. Milkfeeding and bacterial growth play a role. Dietarysupplements containing potentially beneficial bac-teria reduce the occurrence of NEC and death inpremature infants under 1500 g. However, thisreview did not find support for probiotics in infantsunder 1000 g at birth.
The impact of postnatal antibiotics on the pre-term intestinal microbiome was studied in a groupof premature infants between 24 and 31 weeks’ ges-tation. They received at least 50% or more of breastmilk per day and had received only 2 days of anti-biotics or 7 days of antibiotics. The results showedthat antibiotics disturbed the acquisition of bacteriain the gut.
Dysbiosis in the first week of life is related tolater onset of NEC. Neuregulin-4 (NRG4) is anErbB4-specific ligand that has been shown to helpepithelial cells survive. Epithelial cell death is amajor pathologic feature of NEC. Studies of ErbB4,which is found in the developing human intestine,as well as NRG4 (its receptor), which is found inhuman milk, suggest that NRG4-ErbB4 signalingmay be a special pathway for therapeutic interven-tion to prevent NEC. Perhaps this explains the roleof human milk.
An exclusively human milk-based diet is associ-ated with a lower rate of NEC than a diet of humanmilk and bovine milk-based product. This was dem-onstrated by a multicentered study involving 207infants.130 A human milk diet with human milk-based fortification allows the neonatologist to feedpremature infants on totally human milk, meetingnutritional needs and preventing NEC.
NEC has historically had a variable rate in nurs-eries but the etiology has remained elusive. Patelet al. developed an NEC QI initiative when theirNEC rates went from 4% in 2005 to 2006 to
*
*
mo0%
3 mo71%
7 mo29%
12 mo10%
uman milkBW 1188 gGA 29 wkDC 37 wkDC 60 days
FormulaBW 1167 gGA 29 wkDC 36 wkDC 51 days

548 Breastfeeding: A Guide for the Medical Profession
10% in 2007 to 2008. A change in feeding protocolhad no effect. However, NEC rates did change sig-nificantly when nasogastric tube management wasredesigned to include more frequent NG tubechanges, as well as reeducation of parents aboutpump cleaning and storage. This project demon-strated the need for ongoing evaluation of routinesand protocols.
Changing to an exclusively human milk diet forinfants under 33 weeks’ gestational age was testedto reduce the incidence of NEC. The diet was lim-ited to the mother’s milk and humanmilk-based for-tifier and excluded any trace of bovine protein. Itwas compared to the incidence of NEC duringthe years that formula was used, and human milkwas fortified with bovine-based supplements. Itreduced the incidence of NEC from 3.4% downto 1%.59
When donor milk was compared to themother’s own milk, it provided no short-termadvantage in infection rates over premature for-mula. The mother’s own milk appears to protectthe premature infant from infectious morbidity58
(Table 15-15). Further investigation into pasteur-ization techniques is important. High-temperatureshort-time techniques appear to protect moreinfectious protection properties than the Holtertechnique.
In South Africa, where mothers remain with andhelp care for their premature babies, a study com-pared feeding an infant its own mother’s milk withfeeding pooled pasteurized breast milk. Birthweights were between 1000 and 1500 g. Babieswho were not on ventilators began feedings by96 hours of age. Weight gain was significantlygreater using untreated mother’s milk, both forregaining birth weight and reaching 1800 g sooner.Both SGA and AGA infants did better on their ownmothers’ milk. This diet decreased hospital staysand decreased hospital-acquired infection. Theauthors attribute the advantages to the milk beingfed fresh, with early initiation of feeding at thebreast, compared to the pasteurization of the bankmilk.127
TABLE 15-15 Effects of Refrigeration Versus Freezing o
Component Refrigerate
Vitamin C 40%
Lysozyme 40% 20%
Lactoferrin 30% NC
Lipase 25%
Secretory IgA 40%
Specific IgH Variable ?
STHT, Short time high temperature.Modified with permission from Schanler RJ, Anderson D: The l
JB, Walker WA, editors: Nutrition in pediatrics, ed 4, Hamilton,
Kangaroo Care and Skin-to-SkinCare
Kangaroo care and skin-to-skin care are importantconstituents of the support program for milk pro-duction by mothers who are pumping to producemilk, without the benefit of the infant suckling atthe breast. The conduction of heat from parent toinfant is sufficiently high to compensate for theincrease in evaporative and conductive heat loss.
Extensive studies have been carried out to sub-stantiate not only the safety, but also the benefitsof the skin-to-skin contact for fragile prematures,including microprematures, at 24 weeks’ gestation.All the reports recommend initiation directlyafter birth, even when the infant requires ventilatorcare. Stability of heart rate, respirations, and oxygensaturation during skin-to-skin care is remarkablycalm.42 This technique was started initially inresource-poor countries but has been so effectivein calming stabilizing infants that it has become uni-versal. It is particularly effective when the mother isinitiating breastfeeding and pumping to start milkproduction. The Kangaroo Mother Care (KMC)method is a standardized, protocol-based systemfor preterm and/or LBW infants. The cardiorespira-tory instability seen in separated infants during thefirst hours is consistent with the mammalian “pro-test-despair” biology and with a hyperarousal anddissociation response.11 The aim is to empowerthe mother (and father, if possible) by graduallytransferring the skills and responsibility for becom-ing the child’s primary caregiver. It has been for-mally organized internationally.18,112 SeeBoxes 15-14 and 15-15.
Skin to skin has been evaluated by utilizing anumber of measurements to demonstrate the phys-iologic benefits of this close contactwith aparent forprematures. Measurements of salivary cortisolshowed that the infant’s cortisol reactivitydecreasedin response to handling. In addition, skin to skinimproves the symmetry between the mother’s andthe infant’s salivary cortisol levels.103 It also helps
n Pasturized STHT Milk
d 40°C Frozen Pasteurized STHT
0-65% 20-40%
0-65% 0-85%
100%
20-50% 0-20%
ow-birth weight infant in patient care. In Duggan C, Watkins2008, BC Decker.

BOX 15-14. Kangaroo Mother Care
There is sufficient evidence to make the followinggeneral statements about KMC:
• The kangaroo position provides a neutral thermalenvironment that provides immature infants withoptimal thermal regulation, which is the same orbetter than provided by an incubator.
• KMC enhances bonding and attachment, universalhuman needs that apply to all preterm and low-birth-weight infants, their parents, and families.
• Avoiding unwarranted mother-infant separationand initiating the kangaroo position as early aspossible helps repair a bonding process that isdisrupted by delivering a preterm or ill infant.
• KMChelps reduce maternal postpartum depressionsymptoms and increases parental sensitivity toinfant cues.
• Initiation of KMC as soon as possible is essential forthe establishment of breastfeeding and forincreasing the duration of exclusive and anybreastfeeding.
• KMC has positive effects on infant/parentpsychological development and the developmentof mutual communication, understanding, andsocial recognition; reduces parenting stress; andcontributes to anoptimal family homeenvironment.
KMC, Kangaroo Mother Care.
From Nyqvist KH, Anderson GC, Bergman N, et al.: Towardsuniversal Kangaroo Mother Care: recommendations andreport from the first European conference and SeventhInternational Workshop of Kangaroo Mother Care, ActaPaediatr 99:820, 2010.
BOX 15-15. Kangaroo Mother Care Principles
The following guiding principles should pervade allcomponents in KMC protocols:
• All intrapartum and postnatal care should adhere toa paradigm of nonseparation of infants and theirmothers/families.
• Preterm/low-birth-weight infants should beregarded as extero-gestational fetuses needingskin-to-skin contact to promote maturation.
• KMC should begin as soon as possible after birthand continue as often and for as long as appropriate(depending on circumstances).
KMC, Kangaroo Mother Care.
From Nyqvist KH, Anderson GC, Bergman N, et al.: Towardsuniversal Kangaroo Mother Care: recommendations andreport from the first European conference and SeventhInternational Workshop of Kangaroo Mother Care, ActaPaediatr 99:820, 2010.
Figure 15-10. Kangaroo care method.
Premature Infants and Breastfeeding 549
allay the father’s fears of spousal relationship prob-lems, as he feels abandoned when the mother istotally consumed by the infant’s needs. Breastfeed-ing was more common and more exclusive in theskin-to-skin group than in the control group at 1and 4 months (all 18 dyads vs. 16 of 19).103
KANGAROO CARE
Kangaroo care was first introduced in 1979 in a hos-pital in Bogota, Colombia, because of a shortage ofincubators, high death rate from infection, andabandonment of premature infants by theirmothers.Since that time, many investigators have carefullyevaluated kangaroocare and found it tobe beneficialto mother and infant.71 Dressed only in a diaper, aninfant is held skin to skin against the mother’s chestbetween her breasts, snug inside the mother’s cloth-ing, often for hours. The father can do the same.Many advantages have been noted, including morestable respirations, heart rates, and temperatures.The infants spend less time crying and more timein a quiet, alert state and deep sleep.82 Some studiessuggest better weight gain and earlier discharge.Hurst et al.61 also reported an increase in milk vol-ume during pumping (Figure 15-10).
Mothers who give kangaroo care breastfeed lon-ger and more frequently. They also report greaterconfidence in caring for their fragile infant thanthose who experience traditional care.6 NICUnurseries should encourage kangaroo care. All par-ents should be assisted in providing it wheneverthey are in the nursery to benefit both the motherand the infant. This skin-to-skin contact enhancesmilk production, especially when the infant is tooimmature to suckle.
Milk Production by Mothers ofPremature Infants
The Committee on Nutrition at the AAP28 pub-lished a handbook in 2014 that included a sectionon nutritional needs of LBW infants. They suggest

550 Breastfeeding: A Guide for the Medical Profession
that the mother’s own milk and new special formu-las for those babies who need breast milk substi-tutes are promising alternatives.
A joint effort of the AAP Committee on theFetus and Newborn and the American College ofObstetricians and Gynecologists Committee onObstetric Practice states that “human milk has anumber of special features that make its use desir-able in feeding preterm babies.”29
The production of milk by a mother who is notactively nursing her infant, as is frequently thecase in LBW infants and other neonates in NICUs,is a challenge to the resources of the NICU andthe postpartum staff. Insufficient milk productionis a common problem that becomes more criticalas time passes. As production continues to drop,an infant’s needs increase. Evaluation of variousprotocols has been undertaken by investigatorswho looked at onset of pumping postpartum, fre-quency of pumping, and duration in total minutesper day and length of time when no pumpingoccurred.
Hopkinson et al.60 enrolled 32 healthy mothers,19 of whom had no previous breastfeeding experi-ence, into a study protocol. Their infants were 28 to30 weeks’ gestation. All of the mothers initiatedpumping between days 2 and 6. The day of initia-tion was correlated with the volume of milk at2 weeks, but not at 4 weeks, with mothers whohad nursed previously and initiated pumpingsooner. Parity, gravidity, age, and previous nursingexperience were not correlated with volumes at2 weeks. Parity and previous nursing experiencewere associated with milk volume at 4 weeks, withmultiparas producing 60% greater volumes. Theinvestigators found no significant relationshipbetween 24-hour milk volume and frequency, dura-tion, or maximal night interval. The change in milkvolume from 2 to 4 weeks was correlated with fre-quency and duration of pumping but not to maxi-mal night intervals. The range in number ofpumpings per day was four to nine. The authors60
concluded that optimal milk production occurswith at least five expressions per day and pumpingdurations that exceed 100 min/day.
The frequency of milk expression was evaluatedby de Carvalho et al.32 in a crossover design studyof 25 mothers who delivered at 28 to 37 weeks’ ges-tation. Frequent expression of milk was signifi-cantly associated with greater milk production(342�229 mL) than with infrequent expression(221�141 mL). They compared three or fewerpumpings per day to four or more. The mean num-bers were 2.4 versus 5.7, neither equaling the fre-quency that a mother would usually feed herinfant in the first few weeks.
Minimum frequency and duration figures havebeen provided. However, it is advisable to increase
the frequency of pumping as the need to raise pro-duction increases and as the time for discharge andfeeding the infant exclusively at the breastapproaches. Consideration for increasing night-time pumpings is also important as dischargeapproaches. Some mothers experience a dread ofthe pump when demands are increased for “moremilk production.” The management of the motherproducing milk for her hospitalized infant shouldbe coordinated by a neonatologist and a primarycare physician. She should be assisted by a primarycare nurse and the unit’s lactation coordinator andlactation consultants to maximize support and min-imize stress.
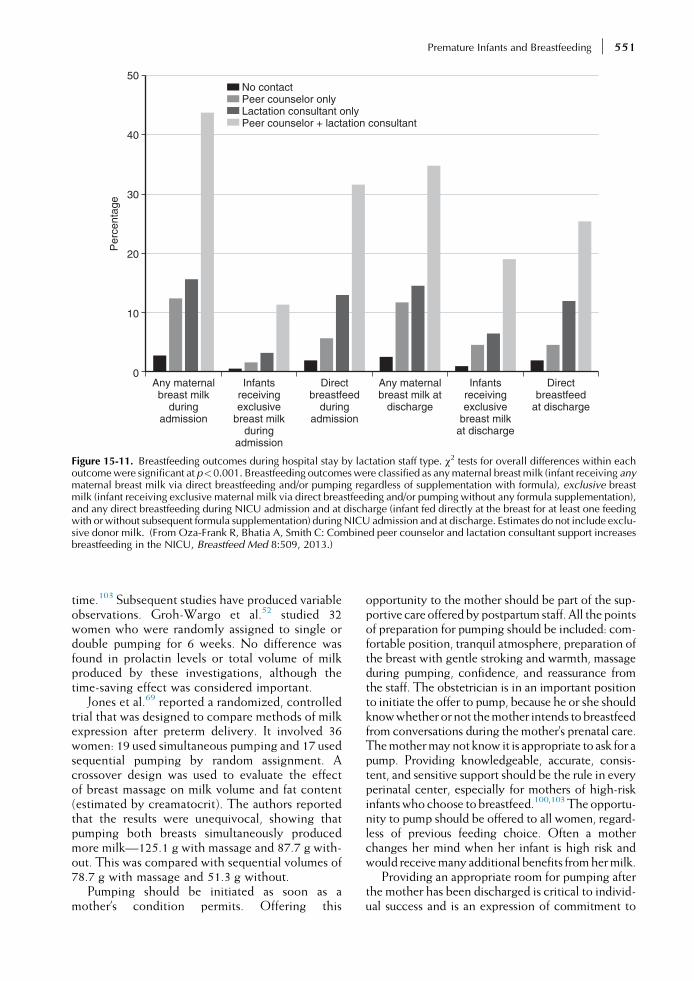
Peer counselors have become important mem-bers of the lactation support teams in the NICU,as they have been in birth centers and in the com-munity. Peer support was originated by theLaLeche League. Anthropologist Dana Raphaelcoined the expression “a friend from across thestreet.” Health departments and WIC programshave developed peer counselor programs, wherewomen (peers) with breastfeeding experienceare trained to provide support and counsel butnot practice medicine.114 Very successful pro-grams have been developed in NICUs. A combi-nation of a lactation consultant and a peercounselor provides the most effective breastfeed-ing support in the NICU100 (see Figure 15-11 andChapter 22).
The NICU at Rush University Medical Centerdeveloped a lactation support program thatincluded peer counselors who were former NICUparents.120 They work directly with NICUmothersand babies, in collaboration with the NICU nurses,to promote successful breastfeeding. The healthcare providers in a study of 17 university NICUsthought the peer counselors improved the care ofthe infants by empowering the mothers to providemilk and modeling good infant care for themothers.
When the physiology of lactation is applied tothe practical management of inducing milk supplywithout the benefit of an infant’s participation, it isapparent that mimicking natural breastfeeding ismore effective. The breast can be prepared withmassage and manual expression. Although somewomen succeed with manual expression alone, itis rare, and a good pump should be recommended.None of the hand pumps can truly duplicate themilking action of the infant, and all are essentiallyvacuum extractors. They should be used only as astopgap measure when the electric pump is unavail-able (see Chapter 21). A pump that can be used onboth breasts simultaneously saves time and gener-ates higher levels of prolactin. These pumps alsogenerate a greater total milk volume than pumpingeach breast separately for the same length of
Any maternalbreast milk
duringadmission
No contactPeer counselor onlyLactation consultant onlyPeer counselor + lactation consultant
0
10
20
30
40
50
Per
cent
age
Infantsreceivingexclusive
breast milkduring
admission
Directbreastfeed
duringadmission
Any maternalbreast milk at
discharge
Infantsreceivingexclusive
breast milkat discharge
Directbreastfeed
at discharge
Figure 15-11. Breastfeeding outcomes during hospital stay by lactation staff type. χ2 tests for overall differences within eachoutcomewere significant at p<0.001. Breastfeeding outcomeswere classified as anymaternal breast milk (infant receiving anymaternal breast milk via direct breastfeeding and/or pumping regardless of supplementation with formula), exclusive breastmilk (infant receiving exclusive maternal milk via direct breastfeeding and/or pumping without any formula supplementation),and any direct breastfeeding during NICU admission and at discharge (infant fed directly at the breast for at least one feedingwith or without subsequent formula supplementation) duringNICU admission and at discharge. Estimates do not include exclu-sive donor milk. (From Oza-Frank R, Bhatia A, Smith C: Combined peer counselor and lactation consultant support increasesbreastfeeding in the NICU, Breastfeed Med 8:509, 2013.)
Premature Infants and Breastfeeding 551
time.103 Subsequent studies have produced variableobservations. Groh-Wargo et al.52 studied 32women who were randomly assigned to single ordouble pumping for 6 weeks. No difference wasfound in prolactin levels or total volume of milkproduced by these investigations, although thetime-saving effect was considered important.
Jones et al.69 reported a randomized, controlledtrial that was designed to compare methods of milkexpression after preterm delivery. It involved 36women: 19 used simultaneous pumping and 17 usedsequential pumping by random assignment. Acrossover design was used to evaluate the effectof breast massage on milk volume and fat content(estimated by creamatocrit). The authors reportedthat the results were unequivocal, showing thatpumping both breasts simultaneously producedmore milk—125.1 g with massage and 87.7 g with-out. This was compared with sequential volumes of78.7 g with massage and 51.3 g without.
Pumping should be initiated as soon as amother’s condition permits. Offering this
opportunity to the mother should be part of the sup-portive careofferedbypostpartum staff. All the pointsof preparation for pumping should be included: com-fortable position, tranquil atmosphere, preparation ofthe breast with gentle stroking and warmth, massageduring pumping, confidence, and reassurance fromthe staff. The obstetrician is in an important positionto initiate the offer to pump, because he or she shouldknowwhetherornot themother intends tobreastfeedfrom conversations during themother’s prenatal care.Themothermaynot know it is appropriate to ask for apump. Providing knowledgeable, accurate, consis-tent, and sensitive support should be the rule in everyperinatal center, especially for mothers of high-riskinfantswho choose tobreastfeed.100,103Theopportu-nity to pump should be offered to all women, regard-less of previous feeding choice. Often a motherchanges her mind when her infant is high risk andwould receivemany additional benefits fromhermilk.
Providing an appropriate room for pumping afterthe mother has been discharged is critical to individ-ual success and is an expression of commitment to

552 Breastfeeding: A Guide for the Medical Profession
breastfeeding by the NICU. This room should beclean, bright, and cheerful and accommodate morethan one mother and companion at a time, unlessseveral rooms are available. It should have a sinkfor washing hands and storage for equipment andsupplies. A nurse call button or other alarm systemis also essential. Additional features are soft music,a telephone, and reading material. The hospitalshould have a supply of approved electric pumpsand individual disposable attachment packets foreach mother. A place should be available to storeher properly labeled and dated milk in a freezer orrefrigerator. Sterile storage containers should bereadily available.
A mother should be encouraged to rent a pumpfor home use and around-the-clock pumping.These are available from medical supply stores,pharmacies, home care services, hospitals, andsome lactation consultants. Insurance companiesreimburse for the cost of the rental when the milkis prescribed for a high-risk infant. A neonatologistcan provide an appropriate letter of support. Thehospital support staff who are coordinating themother’s care or the NICU staff should be sure thatthe mother understands how to use the equipmenteffectively. Ideally, NICUs have at least one staffmember who is a licensed, certified lactation con-sultant who will coordinate this effort under thedirection of the obstetrician, pediatrician, and neo-natologist. One lactation consultant per 15 infantsin the NICU is ideal. The mother should not besubjected to pressures of pump equipment entre-preneurs and unsolicited advice. The best remedyis for the NICU to provide on-staff, up-to-dateexperience and support to the mother in her effortsto provide milk and breastfeed her high-risk infant.Box 15-16 outlines key strategies for successful
BOX 15-16. Guidelines for Initiating Milk SupplyWithout Infant Suckling
1. Begin as soon after delivery as maternal conditionpermits.
2. Initiate use of electric pump while in hospital.3. Begin slowly, increasing time over first week.4. Pump on more regular basis as soon as
engorgement is evident.5. Pump at least five times in 24 hours.6. Allow a rest period for uninterrupted sleep of at
least 6 hours.7. Pump a total of at least 100 min/day.8. Use “double” pump to pump both breasts
simultaneously, which can cut total timeproportionately.
9. Prepare breast with warm soaks, gentle stroking,and lightmassage tomaximizeproductionofmilk.
10. Encourage skin-to-skin care (kangaroo care).
pumping when an infant is unable to suckle thebreast. All neonatal nurses should be familiar withthe available pumps and their use and be supportiveof mothers who are pumping.100
Who Produces Milk for LBW orSGA Infants?
Nationwide, mothers who give birth to infants whoare admitted to special carenurseries are less likely toinitiate lactation than mothers of healthy terminfants, according to Meier.97 The profile ofmothers who give birth to these high-risk infantsincludes a higher percentage of low-income, low-education, young mothers, who do not breastfeedingreat numbers. PostpartumandNICUstaff shouldwork to encourage thesewomen to initiate lactation.
Maternal choice to breastfeed or provide milkfor an LBW infant is influenced by many factorsbeyond those that affect most feeding decisionsof normal full-term infants.92 Lucas et al.88,89
sought to answer two major questions in a studyof 925 mother-infant pairs in five hospitals. Dohealth care professionals in neonatal units exerta major influence on a mother’s feeding prefer-ence and availability of her milk for her infant?Are there population differences between motherswho do and do not provide their milk? In thisstudy of five centers, the demographic character-istics of the mother were important, not those ofthe staff. This study did not look at success rates,however.
Mothers in a study by Verronen135 had deliveredinfants at a mean of 31 weeks’ gestation; the infantsweighed less than 1850 g with a mean of 1370 g.More educated mothers provided their milk (98%)than uneducated (40%). Factors of higher socioeco-nomic class, lower parity or fewer living children,being married, and being older than 20 years ofage were associated with providing milk. Boys weremore apt to receive mother’s milk, as shown in otherstudies. Birth weight and extreme immaturity werenot a determinant, nor was transfer of the infant toanother center. The Rush Mother’s Milk Club,which is a breastfeeding intervention for mothersof VLBW infants in Chicago, was developed anddirected by Meier and colleagues.98,99 In the 52-bed urbanNICU, the staff provided facilitated learn-ing. Transportation was provided for mothers fromhome, as well as a weekly interactive social lun-cheon. They employ five peer counselors and pro-vide a 24-hour, toll-free pager information line.The peer counselors also contact mothers at home.Low milk supply is aggressively managed withrecord keeping, encouragement, and counseling.The lactation initiation rate among these predomi-nantly low-income African-American women was

Premature Infants and Breastfeeding 553
72.9%. Exclusive mother’s milk was attained by57.2% and some mother’s milk by 72.5%.101 Skin-to-skin and kangaroo care are important featuresof this program and many others.91
Feeding the Near-Term Infant (35 to37 Weeks’ Gestation) at the Breast
Near-term infants (i.e., 35 0/7 weeks to 36 6/7weeks) may be nursed at the breast if otherwise sta-ble. Breastfeeding should be initiated by one hour ofage if mother and infant are stable. Health care pro-fessionals should monitor to ensure that frequentongoing feedings are occurring “on demand” at least10-12 times a day. Communication among staff andwith the parents is key to success. Involvement oflactation-trained staff who are also skilled neonatalnurses mitigates confusion and conflictingmessagesto the family. Particular care should be given toassist a mother in getting the infant to suckle, espe-cially if the breast and nipples are large orengorged.107,110Weight should be followed closelyto prevent excessive weight loss. Infants whoreceive sugar water and formula supplements losemore weight than those who are nursed frequentlyat the breast without supplementation. If breast-feeding is goingwell, the infant could be dischargedwith the mother from the hospital as soon as theinfant begins to gain substantially, with closefollow-up at home. Poor weight gain, less than20 g/day, is usually the result of inadequate intake.Average weight gain should be 26 to 31 g/day (seeAppendix J). A mother may need to pump betweenfeedings if the infant does not stimulate the breastsadequately. The milk can be provided by cup or lac-tation aide device (see Appendix J and Figure 14-10). Difficulties with latch should be investigatedwith a careful examination of the infant’s mouthand the mother’s breast and nipples. Before dis-charge, the physician, as well as the nurse, shouldobserve the dyad.116 If a mother is a low producer,galactagogues can be considered. (See Chapter 11and Protocol #9 in Appendix J.) Follow-up shouldinclude frequent weighings and growth measure-ments (length and head circumference shouldincrease approximately 0.5 cm/wk). Home visitsor office checks are crucial to monitor progress.An extensive review of practice guidelines for thecare of the late preterm infant has been preparedby the National Perinatal Association.
Premature Infants of 28 6/7 Weeksto 32 6/7 Weeks
Infants of gestational age more than 28 weeks butless than 35 weeks are frequently breastfed in
NICUs, because the value of human milk has beenrecognized by most neonatologists.
Feeding at the breast when an infant is less than1500 g is considered too strenuous by many neona-tologists, even though it has been proved that ittakes less energy and less impact on vital signs tobreastfeed than bottle feed.81 When the feeding ofinfants of less than 1500 g was examined, however,the growth of those fed at the breast was comparablewith that of matched control infants fed expressedhuman milk by bottle.69 Breastfeeding was startedwhen sucking movements were observed. Initially,they received supplementary human milk by tubeplus 800 units of vitamin D and 60 mg of vitaminC daily. Unrestricted visiting of parents to the neo-natal unit, an optimistic and knowledgeable attitudeof the nursing staff toward breastfeeding, and theavoidance of a bottle for the infants are importantto success.93,94 Encouraging the expression ofmilkby the mothers early in the postpartum periodis essential. The main deterrent to successfulbreastfeeding was lack of maternal interest andcommitment.
Blaymore Bier et al.17 undertook a clinical studyof breast feeding and bottle feedings in ELBWinfants (birth weight 800 g or less) when they wereconsidered ready to bottle feed. This was at a meanage of 35 weeks since conception (correctedgestational age). One breastfeeding and one bottlefeeding were monitored each day for 10 days.Prefeeding and postfeeding weights, oxygen satura-tion, respiratory and heart rates, and axillary temper-ature were recorded. Higher oxygen saturation andhigher temperatures during breastfeeding and lesslikelihood of desaturation below 90% were notedin the breastfed infants. The weights reflectingintake were higher in the bottle-fed infants. Theauthors concluded that it was physiologically safeand less stressful for infants to breastfeed. The lowerintake requires monitoring, however.17
The ontogenic and temporal organization ofnonnutritive sucking during active sleep was stud-ied by Hack et al.55 in preterm infants. One ofthe six infants studied had recognizable rhythmicsucking bursts at 28 weeks, and all had bursts by31 to 32 weeks. The number of bursts increasedand the interval between bursts decreased as theinfants matured, with the earliest indications ofintrinsic rhythm beginning at 30 weeks.
Nonnutritive sucking has become a subject ofcontroversy in NICUs. Allowing premature infantsto suck on a pacifier during gavage feedings was ini-tially reported to be associated with increasedweight gain and shorter hospitalization. Whennutrient intake and other parameters were con-trolled, however, no advantages to nonnutritivesucking were observed in somatic growth, serumproteins, energy absorption, or feeding tolerance,nor was any increase in tropic hormones or growth

554 Breastfeeding: A Guide for the Medical Profession
promoters seen.33,40,93 Infants have been observedto have transcutaneous oxygen saturation measure-ments increase by 3% to 4% during nonnutritivesucking.32 Nonnutritive sucking does not appearto carry risk for infants destined for further bottlefeeding. However, it should be avoided for infantsdestined to breastfeed, in order to avoid interfer-ence with normal sucking. Unfortunately, moststudies have been done with bottles.35
Of greater significance is the value of havingthese infants placed at the “emptied” breast duringgavage tube feedings. When Narayanan et al.109
studied this practice, they found no change inweight gain or length of hospital stay. The practicedid, however, result in more successful and longerduration of breastfeeding after discharge. Thistechnique was originally designed in our nurseryto improve the mother’s milk production andencourage mothers who were becoming discour-aged. As the infant matures and begins swallowingwith sucking, it becomes unnecessary to pump thebreast “empty” before presenting it to the infant.This is because any milk provided could be suckledand swallowed. Suckling at the breast initiates aperistaltic action that also triggers swallowingand the physiologic response of the entire GI tract(see Chapter 8). Suckling the breast also improvesthe mother’s success when pumping. Readiness towean from tube feedings to oral feeding is poorlydefined and based on observations utilizing a bottleand/or a pacifier. Stable cardiopulmonary status at33 to 34 weeks is associated with sucking patternsthat resemble term infants (i.e., rhythmic alterationof suction and expression and the positive pressuregenerated by compression). Mature sucking patternis not necessary for safe, successful feeding at thebreast.76 Infants can feed orally without suction.The undulating motion of the tongue does triggerlet-down and the swallowing of fluid. An infant’sbehavioral state and organization during feeding,as well as the nursery environment (especially lightand sound), and a caretaker’s approach to oral feed-ing all affect an infant’s performance.76 This isanother point supportive of early breastfeeding.Avoidance of bottles during the establishment ofbreastfeeding in premature infants has been evalu-ated in a Cochrane Review.27 Small prematureinfants begin with tube feedings of their mother’smilk. As they mature, they have breastfeedingsadded. But in many nurseries, the bottle with themother’s milk is introduced. Its impact on successfulbreastfeeding is challenged. Five studies of 543infants were included in a Cochrane Review byCollins et al.27 Four of the studies substituted cupfeeding when mother was not available to breast-feed. The cup feedings increased the probabilityof successful breastfeeding and continuation ofbreastfeeding. Cup feedings, however, prolongedhospitalizations by 10 days. Noncompliance was
an issue as well. A study in Egypt, after this review,reported 30 cup-fed premature infants comparedwith 30 bottle-fed infants who were breastfed ondischarge because mothers did not provide theirmilk or breastfeed before discharge. The cup-fedinfants breastfed for longer durations and in greaternumbers.1 The crucial role of adequate nutrition tobrain growth, especially in the premature infant, isgenerally acknowledged. Although nutrition maynot overcome all the problems of extreme prematu-rity and its impact on the immature brain, it doesreduce infections and NEC and has immunomodu-latory properties when it includes over 50% humanmilk. The impact of humanmilk constituents on thewhite matter and its development is remarkable.This is being attributed to the gut-immune brainaxis.71 The nutritional adjustments to use humanmilk and human milk supplements are consideredsafe, inexpensive, cause few side effects, and areeasily implemented.
Breastfeeding the ExtremelyPremature Infant
Evaluations of feeding strategies are rarely con-ducted or published, in spite of rigid protocolsin some nurseries. Early initiation of feedingshas been thought valuable and safe. In a study of171 premature infants between 26 and 30 weeks’gestation, Schanler et al.124 tested the validity ofGI priming and continuous infusion, versus inter-mittent bolus tube feeding with human milk orpreterm formula. Infants were randomized to fourtreatment combinations in a balanced two-waydesign. Investigators compared the presence orabsence of GI priming for 10 days and continuousinfusion versus intermittent bolus tube feeding.Time to full feeding was similar in all groups.GI priming had no adverse effects and improvedcalcium/phosphorus retention and shorter in-tentional transient times. Bolus feeding was asso-ciated with less feeding intolerance and greaterweight gain than the continuous method. Themore human milk fed, the lower the morbidity ratewas. The authors concluded that early GI primingwith human milk and bolus feedings provided thebest advantage for premature infants. Very pre-term infants, born at 26 to 31 weeks’ gestation,have the capacity for the early development oforal motor competence that is sufficient for estab-lishment of full breastfeeding at a low postmen-strual age, according to Nyqvist.112 Using thePreterm Infant Breastfeeding Behavior Scale(Table 15-16), designed for use by mothers andprofessionals to observe levels of competence inoral motor behavior during breastfeeding, theauthor studied 15 infants born at 26 to 31 weeks’

TABLE 15-16 The Preterm Infant Breastfeeding Behavior Scale (PIBBS)
Scale Items Levels of Competence
Rooting Did not root
Showed some rooting behavior (mouth opening, tongue extension, hand-to-mouth/facemovements, head turning)
Showed obvious rooting behavior (simultaneous mouth opening and head turning)
Areolar grasp (how muchof the breast was insidethe baby’s mouth)
None, the mouth only touched the nipple
Part of the nipple
The whole nipple, not the areola
The nipple and some of the areola
Latched on and fixed tothe breast
Did not latch on at all so the mother felt it
Latched on for <1 min
Latched on for 1-15 min or more, recorded by marking a cross along a line graded 1-15 min
Sucking No sucking or licking
Licking and tasting, but no sucking
Single sucks, occasional short sucking bursts (2-9 sucks)
Repeated (2 or more consecutive) short sucking bursts, occasional long bursts (10 sucks ormore before a pause)
Repeated long sucking bursts
Longest sucking bursts Maximum number of consecutive sucks, recorded by marking a cross along a line graded 1-30
Swallowing Swallowing was not noticed
Occasional swallowing was noticed
From Nyqvist KH: Early attainment of breastfeeding competence in very preterm infants, Acta Paediatr 97:776, 2008, p 778,Figure 1.
Premature Infants and Breastfeeding 555
gestational age. The author made daily assess-ments. Semidemand feeding was utilized with aprescribed total daily income volume. Breastfeed-ing was initiated at 29 weeks. Rooting, efficientareolar grasp, and repeated short sucking burstswere noted at 29 weeks. At 31 weeks, long suckingbursts and repeated swallowing were observed.Sucking rates ranged from 5 to 24 with a medianof 17. Full breastfeeding was reached between32 and 38 weeks with a median of 35 weeks.Weight gain was described as adequate. Alterna-tive techniques were described in a report froma nursery in Brazil,31 in which they placed infantsin groups trying techniques of relactation, trans-lactation, and breast-orogastric tubes. Theydescribed 432 infants who, at discharge, werebreastfeeding 85%, 100%, and 100% in eachgroup, respectively. All attained good weight gain,with only 1.6% feeding-related problems. Thedefinition of relactation and translactation resem-bles other nurseries’ use of lactation aide devicesfor additional nutrition.
Transpyloric tube feeding in VLBW infants withsuspected gastroesophageal reflux has been usedsuccessfully by Malcolm et al.92 They described72 VLBW infants with a median birth weight of870 g (a range of 365 to 1435 g) and a gestationalage of 26 weeks (range 23 to 31 weeks) whoreceived transpyloric feedings. They observed areduction in apneic episodes and a decrease in bra-dycardia. Five infants developed NEC, none of
whom were receiving human milk. The authorsconcluded that transpyloric feedings, when limitedto human milk, may safely reduce episodes of apneaand bradycardia in preterm infants suspected ofgastroesophageal reflux. They suggest confirma-tion of this work in other NICUs, with the potentialof changing hospital procedures.
SGA Infants
Infants who are below the 10th percentile (or 2SDs) in weight for their gestational age are termedSGA. These infants may also be shorter in lengthand have smaller heads, depending on when in ges-tational life the insult to their growth occurred. Themore general the growth failure is, the earlier theintrauterine effect appears. For example, rubellain the first trimester causes total growth retarda-tion, whereas hypertension in the mother in thethird trimester predominantly affects weight. Themore profound the growth retardation is, the moredifficult the nutritional problems are.
SGA infants are prone to be hypocalcemic; how-ever, if they can be provided with adequate breastmilk early, this complication may be avoided.This is because the calcium/phosphorus ratio ismore physiologic in human milk than formula.Other problems, including hypothermia and hypo-glycemia, which lead to a vicious circle of acidosisand associated problems, can be triggered by

556 Breastfeeding: A Guide for the Medical Profession
unmonitored exposure of an infant to thermal stressin the first hours of life and failure to identify thehypoglycemia early. Hypoglycemia in an SGAinfant cannot be ignored. The potential exists forsignificant stress to the nervous system, whichcan result in seizures that require aggressive therapyand a detailed diagnostic workup. SGA infants lackglycogen stores, so they cannot raise their ownblood sugar level by mobilizing stores.
Using human α-lactalbumin as a marker protein,Schanler et al.125 demonstrated that SGA infantswith intrauterine growth restriction have delayedpostnatal decrease in macromolecular absorptionand delayed intestinal maturation, even comparedwith premature infants of the same weight. Theirmanagement demands special care. The enzymesin human milk can facilitate catch-up maturationof the intestinal tract.
Thus perinatal nursery staff may appear to beobstructive to breastfeeding when they hover overthis infant or even insist on transfer to the nursery.Initial breastfeeding at delivery is permissible; how-ever, adequate external heat must be provided. Test-ing the blood sugar should be performed in thedelivery room recovery area. The infant should besent to the nursery if hypoglycemia or hypothermiacannot be controlled. Frequent breastfeeding can beinitiated unless the blood sugar level is too low (lessthan 30 mg/dL) or unresponsive to oral treatment. Itmay not be possible for even an actively lactatingmultipara to sustain an SGA infant initially, butthe infant should be put to breast at least every3 hours and given intravenous glucose as well.78
Term SGA infants often have a poor suck andpoor coordination with the swallow reflex. Theymayhave considerablemucus, with gagging and spit-ting. A simple lavage of the stomach with a No.8 feeding tube (orNo. 5, if the infantweighs less than2600 g) and warmed glucose water usually relievesthe gagging. Once this SGA infant begins to eat,he or she will do well and will require sufficient kilo-calories to meet the needs of an AGA infant. Themother may need to use a breast pump initially tostimulate lactation and increase the volume sheproduces.
Children born SGA are at a neurodevelopmentaldisadvantage. When these infants receive enrichedformula, it does improve their growth, but breastfedSGA infants grew best in a series of children fol-lowed by Morley et al.104 Three groups fed regularformula, enriched formula, or breast milk were fol-lowed: 147 were randomized to regular formula,152 received enriched formula, and 175 were inthe reference group of breastfeeding. The develop-mental scores using the Bayley Mental Develop-ment Index or the Psychomotor DevelopmentIndex at 18 months were measured. No differencebetween formula groups was seen. The breastfeed-ing infants had significantly higher Psychomotor
Development Index scores and a 6-point advantagein the Bayley Mental Development Index. Theauthors suggested that SGA infants clearlybenefited from being breastfed.104
Transitioning from Hospitalto Home
The transition from hospital to home is a stressfultime for all families, but when an infant is prematureand has been in the NICU for days, weeks, ormonths, transition can be extremely difficult. Thestress can be reduced by discharge planning. Themother should spend as much time as possible withher infant, breastfeeding when present. A lactationconsultant or trained staff member should observethese interactions. The presence of sucking andswallowing should be documented. If mothers havereceived adequate assistance in the days and weeksbefore discharge, then positioning and latch shouldbe perfected by discharge.
The Committee on Fetus and Newborn of theAAP has delineated three physiologic competen-cies that are recognized as essential before hospitaldischarge of the preterm infant:
• The ability to maintain body temperature in ahome environment
• Sufficiently mature respiratory control• Oral feeding sufficient to support appropriate
growth
Hospitals that have facilities to accommodatecare-by-parent overnight are helpful in the transi-tion. At minimum, parents should be given all themedications and treatments before discharge andbe breastfeeding. If a mother’s supply is not adequateyet, she should be instructed in the use of the lacta-tion supplementer before discharge, with a plan forthe amount and substance to be placed in the supple-menter. If she has stored milk available, it can beused. If not, the neonatologist will have to orderdonor milk, preferably from a milk bank. If not, aspecial care formula or special human milk supple-menter, which is designed to be used separately frommixing with mother’s milk as a feed, can be utilized.Mothers should be instructed to continue pumpinguntil the infants are exclusively breastfed and gainingweight adequately. Pumping three to four times perday to completely empty the breasts at home is crit-ical. Preterm infants usually do not completelyempty the breasts at first. They lack the suctionstrength and sustainable effective organization ofsucking until they approach 40 weeks’ corrected ges-tational age, according to Meier.97 To guaranteeadequate production and intake, these preterminfants need scheduling to ensure feeding every3 hours, although feeding on cue is more effectivein the long run.

Figure 15-12. 1100-g infant shown at 4 hours of life in a busyNICU. Infants in these situations require early intervention toensure successful breastfeeding.
Premature Infants and Breastfeeding 557
In Sweden, preterm infants who are less than32 weeks’ gestation are fed their mother’s milk or,if that is not available, donor milk. Twenty-sevenof 36 NICUs in Sweden that responded to a ques-tionnaire on breast milk handling had their ownmilk bank.113 The authors have established nationalguidelines for the hospital use of human milk. InNorth America, the Human Milk Banking Associa-tion of North America oversees volunteer milkbanking (see Chapter 21). Milk banks are listedin Appendix H.
Follow-up after discharge from the NICU isessential and should be involved as the dyad is pre-pared for discharge. Independent predictors ofhuman milk receipt at NICU discharge were deter-mined by Brownell et al.20 from analysis of the Ver-mont Oxford Network clinical data at a Level IVNICU in the inner city. They concluded that astrong NICU lactation program, in combinationwith a community-based peer counselor program,may increase rates of human milk consumptionamong VLBW infants of black/Hispanic mothers,as well as those with more complicated courses.
Community-based peer support programs arevery helpful in supporting postdischarge mothersto continue to provide their own milk.
Early discharge with tube feeding of preterminfants under close supervision by pediatric nursepractitioners in the Netherlands was done. Theeffect was an increase in the duration of breastfeed-ing.96 The finding continued for 6 months post-discharge. This approach needs confirmation butis important.
Not all premature infants will need supplemen-tation at home. Before and after weighings(Chapter 8) can be done while an infant is still inthe hospital to measure the infant’s intake at eachfeeding. Digital scales, accurate to 2 g, are availablein hospitals, and homemodels can be rented.Whenan infant is first discharged, it is helpful to both thephysician and the parents to know what intakeactually is.57 Some mothers produce large volumesof milk, but the infants do not gain weight. Pump-ing first to remove the foremilk (and freeze it) andhaving the infant suckle the hind milk can help thisproblem. A pediatrician plays a critical role in thesuccess of feeding after discharge. Monitoring ofprogress and knowledge of the unique concernsin breastfeeding premature infants are key. TheAcademy of Breastfeeding Medicine Protocol #12in Appendix J details the steps to follow.
Improving Milk Production
1. Begin pumping as soon postpartum as possible.2. Use hospital-grade double (two-breast) pumps.3. Pump 10 to 15 minutes every 3 hours until more
than a few drops are produced (72 hours).
4. When the amount increases, continue to pumpfor 2 minutes after the last drop is produced(total 20 to 30 minutes).
5. Keep a record of times pumped and volumesproduced.
6. Pump at babies’ bedside when possible.7. Start with kangaroo care.8. Stroke and massage breast during pumping.9. As soon as infant is able, place at emptied breast
to suckle or during gavage feedings.
Pump-dependent mothers are at risk for dimin-ishing milk supply. Mothers of preterm infantscan attain and sustain high production levels bycombining the use of electrical pumps with manualtechniques, including hand expression taught byan experienced nurse. This includes mothers ofnormal term babies. It is essential for mothers ofinfants in the NICU. Dr. Morton105 has developedseveral videotapes demonstrating these techniquesthat are excellent for mothers and staff alike.Chapter 8 discusses pharmacologic stimulation ofmilk volume.
Concluding Recommendations
Infants who weigh less than 1800 g at birth andhave to be gavage fed and infants of any weightwho are acutely ill present complex problems.A mother should be instructed to express her milkinitially and contribute any colostrum she pro-duces. This can be given by gastric tube spoon orcup. A hospital-grade electric pump is effective inhelping a mother increase the volume produced.When an infant is born at 1000 g, requires ventila-tor support for days, and is not discharged for8 weeks (Figure 15-12), it is difficult to maintain
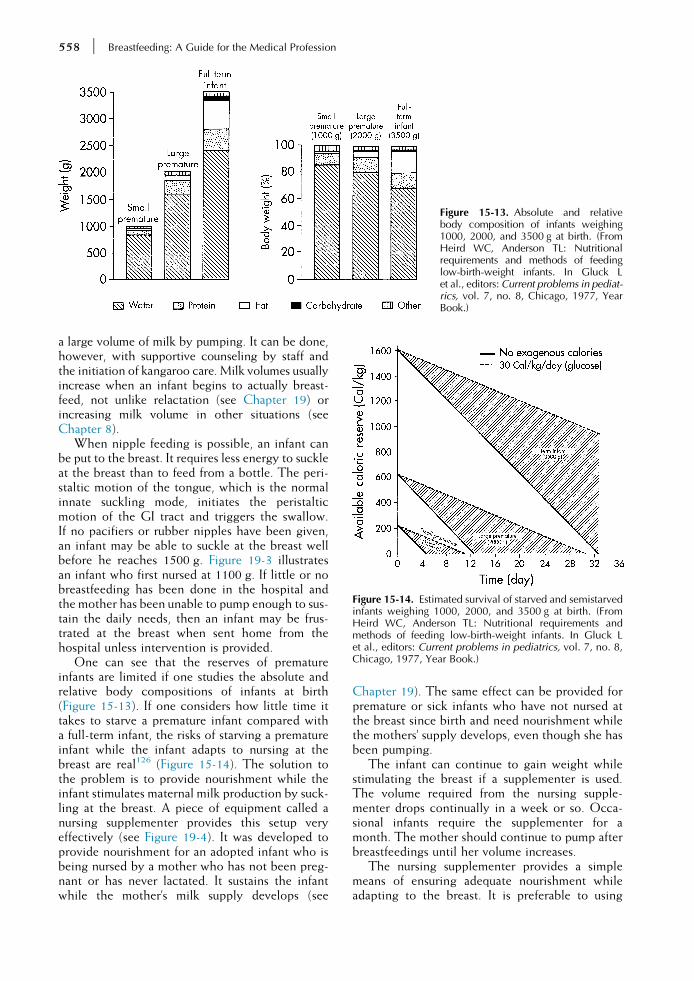
Figure 15-13. Absolute and relativebody composition of infants weighing1000, 2000, and 3500 g at birth. (FromHeird WC, Anderson TL: Nutritionalrequirements and methods of feedinglow-birth-weight infants. In Gluck Let al., editors: Current problems in pediat-rics, vol. 7, no. 8, Chicago, 1977, YearBook.)
Figure 15-14. Estimated survival of starved and semistarvedinfants weighing 1000, 2000, and 3500 g at birth. (FromHeird WC, Anderson TL: Nutritional requirements andmethods of feeding low-birth-weight infants. In Gluck Let al., editors: Current problems in pediatrics, vol. 7, no. 8,Chicago, 1977, Year Book.)
558 Breastfeeding: A Guide for the Medical Profession
a large volume of milk by pumping. It can be done,however, with supportive counseling by staff andthe initiation of kangaroo care. Milk volumes usuallyincrease when an infant begins to actually breast-feed, not unlike relactation (see Chapter 19) orincreasing milk volume in other situations (seeChapter 8).
When nipple feeding is possible, an infant canbe put to the breast. It requires less energy to suckleat the breast than to feed from a bottle. The peri-staltic motion of the tongue, which is the normalinnate suckling mode, initiates the peristalticmotion of the GI tract and triggers the swallow.If no pacifiers or rubber nipples have been given,an infant may be able to suckle at the breast wellbefore he reaches 1500 g. Figure 19-3 illustratesan infant who first nursed at 1100 g. If little or nobreastfeeding has been done in the hospital andthe mother has been unable to pump enough to sus-tain the daily needs, then an infant may be frus-trated at the breast when sent home from thehospital unless intervention is provided.
One can see that the reserves of prematureinfants are limited if one studies the absolute andrelative body compositions of infants at birth(Figure 15-13). If one considers how little time ittakes to starve a premature infant compared witha full-term infant, the risks of starving a prematureinfant while the infant adapts to nursing at thebreast are real126 (Figure 15-14). The solution tothe problem is to provide nourishment while theinfant stimulates maternal milk production by suck-ling at the breast. A piece of equipment called anursing supplementer provides this setup veryeffectively (see Figure 19-4). It was developed toprovide nourishment for an adopted infant who isbeing nursed by a mother who has not been preg-nant or has never lactated. It sustains the infantwhile the mother’s milk supply develops (see
Chapter 19). The same effect can be provided forpremature or sick infants who have not nursed atthe breast since birth and need nourishment whilethe mothers’ supply develops, even though she hasbeen pumping.
The infant can continue to gain weight whilestimulating the breast if a supplementer is used.The volume required from the nursing supple-menter drops continually in a week or so. Occa-sional infants require the supplementer for amonth. The mother should continue to pump afterbreastfeedings until her volume increases.
The nursing supplementer provides a simplemeans of ensuring adequate nourishment whileadapting to the breast. It is preferable to using

TABLE 15-17 Postdischarge NutritionalScreening Assessment
Action Values
Growth
Weight gain <20 g/day
Length growth <0.5 cm/wk
Head circumference <0.5 cm/wk
Biochemical test
Phosphorus <4.5 mg/dL
Alkaline phosphatase >450 IU/L
Urea nitrogen <5 mg/dL
IU, International units.Modified from Hall, RT: Nutritional follow-up of the
breastfeeding premature infant after hospital discharge,Pediatr Clin North Am 48:435, 2001.
Premature Infants and Breastfeeding 559
supplemental bottles because the infant is not con-fused by the rubber nipple, which requires a differ-ent mechanism of sucking than the human nipple.Furthermore, the suckling of the breast provides thecontinued stimulus necessary for increasing milkproduction. Cup feeding is an alternative to thebottle if the infant needs additional nourishment.
The parameters that are to be met before dis-charge home from the hospital include sustainedweight gain, growth in length and head circum-ference, and stable biochemical parameters49
(Table 15-17). After discharge from the hospital,these same parameters should be met. If falteringis persistent, fortifying breastfeeding may be indi-cated. This can be accomplished without interfer-ing with the breastfeeding process again by usinga lactation supplementer containing enrichedbreast milk that had been previously pumped ordonor milk, which is preferable to formula.
Posthospitalization breastfeeding patterns ofmoderately preterm infants (30 to 35 weeks) werestudied by Wooldridge and Hall138 using dailyfeeding diaries in 55 women for the first monthafter discharge. Those women who were able toexclusively breastfeed before the end of the firstweek at home were able to maintain their supply.In general, those women who did not have an ade-quate supply during the first week were unlikely toachieve it by week 4. The proportion of breastfeedsincreased during the 4 weeks of observation, butonly 56% achieved exclusive breastfeeds by 4weeksin this study. Proper preparation prior to dischargeand adequate support at home assures success.
REFERENCES
1. Abouelfettoh AM, Dowling DA, Elguindy SR, et al: Cupversus bottle feeding for hospitalized late preterm infantsin Egypt: a quasi-experimental study, Neonatal Intensive Care22:33–38, 2009.
2. Abrahms SA, Schanler RJ, Garza C: Bone mineralization informer very low birth weight infants fed either human milkor commercial formula, J Pediatr 112:956, 1988.
3. Alfaleh K, Anabrees J: Probiotics for prevention of necro-tizing enterocolitis in preterm infants (review),Cochrane Libr(4)2014.
4. American Academy of Pediatrics, Section onBreastfeeding: Breastfeeding and the use of human milk,Pediatrics 129:e527–e544, 2012.
5. Anderson DM, William FH, Merkatz RB, et al: Length ofgestation and nutritional composition of human milk, AmJ Clin Nutr 37:810, 1983.
6. Anderson GC: Touch and the kangaroo care method.In Field TM, editor: Touch in early development, Mahwah,N.J., 1995, Erlbaum Associates.
7. Arslanoglu S, Moro GE, Ziegler EE: Preterm infants fedfortified human milk receive less protein than they need,J Perinatol 29:489–492, 2009.
8. Atkinson SA, Anderson GH, Bryan MH: Human milk:comparison of the nitrogen composition in milk frommothers of premature and full-term infants, Am J Clin Nutr33:811, 1980.
9. Atkinson SA, Radde IC, Chance GW, et al: Macromineralcontent of milk obtained during early lactation frommothers of premature infants, Early Hum Dev 4:5, 1980.
10. Beijers RJW, Graaf FVD, Schaafsma A, et al: Compositionof premature breast milk during lactation: constant digest-ible protein content (as in full term milk), Early Hum Dev29:351, 1992.
11. BergmanNJ, Linley LL, Faucus SR: Randomized controlledtrial of skin-to-skin contact from birth versus conventionalincubator for physiological stabilization in 1200 to 2199gram newborns, Acta Paediatr 93:779–785, 2004.
12. Berseth CL: Gastrointestinal motility in the neonate, ClinPerinatol 23:179, 1996.
13. Bigger HR, Fogg LJ, Patel A, et al: Quality indicators forhuman milk use in very low-birthweight infants; are wemeasuring what we should be measuring? J Perinatol34:287–291, 2014.
14. Billeaud C, Senterre J, Rigo J: Osmolality of the gastricand duodenal contents in low birth weight infants fedhuman milk or various formulae, Acta Paediatr Scand71:799, 1982.
15. Birch DG, Birch EE, Hoffman DR, et al: Retinal develop-ment in very-low-birth-weight infants fed diets differingin omega-3 fatty acids, Invest Ophthalmol Vis Sci 33:2365,1992.
16. Bishop NJ, Dahlenburg SL, Fewtrell MS, et al: Early diet ofpreterm infants and bone mineralization at age five years,Acta Paediatr 85:230, 1996.
17. Blaymore Bier JA, Oliver T, Ferguson AE, et al: Humanmilk improves cognitive and motor development of prema-ture infants during infancy, J Hum Lact 18:361, 2002.
18. Blomovist YT, Ewald V, Grandin M, et al: Initiation andextent of skin-to-skin at two Swedish neonatal intensivecare units, Acta Paediatr 102:22–28, 2013.
19. Boyd CA, Quigley MA, Brocklehurst P: Donor breast milkversus infant formula for preterm infants: a systematicreview and meta analysis, Arch Dis Child Fetal Neonatal Ed92:F169, 2006.
20. Brownell EA, Lussier MM, Hagadorn JI, et al: Independentpredictors of human milk receipt at NICU discharge, Am JPerinatol 31(10):891–898, 2014.
21. Brumberg H, LaGamma EF: Perspectives on nutrition:enhance outcomes for premature infants, Pediatr Ann 32(9):617, 2003.
22. Carey DE, Rowe JC, Goetz CA, et al: Growth and phos-phorus metabolism in premature infants fed human milk,fortified human milk, or special premature formula, Am JDis Child 141:511, 1987.
560 Breastfeeding: A Guide for the Medical Profession
23. Cavell B: Gastric emptying in preterm infants, Acta PaediatrScand 68:725, 1979.
24. Chan GM: Effects of powdered human milk fortifiers onanti bacterial actions of human milk, J Perinatol23:620–623, 2002.
25. Chan GM, LeeML, Rechtman DJ: Effects of a humanmilk-derived human milk fortifier on the antibacterial actions ofhuman milk, Breastfeed Med 2(2):205–208, 2007.
26. Chandra RK: Immunoglobulin and protein levels in breastmilk produced by mothers of preterm infants, Nutr Res2:27, 1982.
27. Collins CT, Makrides M, Gillis J, et al: Avoidance of bot-tles during the establishment of breastfeeds in preterminfants, Cochrane Database Syst Rev 1, 2004.
28. Committee on Nutrition, American Academy of Pediatrics:Nutritional needs of the preterm infant, Pediatric nutritionhandbook, ed 7, Elk Grove, Ill., 2014, American Academyof Pediatrics.
29. Committee on Obstetric Practice, American College ofObstetricians and Gynecologists, Committee on the Fetusand Newborn, et al: Guidelines for perinatal care, ed 4, ElkGrove, Ill., 2007, American Academy of Pediatrics.
30. Davey AM, Wagner CL, Phelps DL, et al: Do prematureinfants with umbilical artery catheters tolerate oral feeds?Pediatr Res 31:199A, 1992.
31. de Aquino RR, OsorioMM: Relactation, translactation andbreast-orogastric tube as transition methods in feeding pre-term babies, J Hum Lact 25:420, 2009.
32. de Carvalho M, Anderson DM, Giangreco A, et al:Frequency of milk expression and milk production bymothers of non-nursing premature neonates, Am J Dis Child139:483–485, 1985.
33. DeCurtis M, McIntosh N, Ventura V, et al: Effect of non-nutritive suckling on nutrient retention in preterm infants,J Pediatr 109:888, 1986.
34. Domany KA, Mandel D, Kedem MH, et al: Breast milk fatcontent of mothers to small-for-gestational-age infants,J Perinatol 34:1–3, 2014.
35. Dowling (deMonterice) D: Physiologic responses ofbreastfeeding and bottle feeding, Nurs Res 48:78, 1999.
36. Edmond K, Bahl R: Optimal feeding of low-birth-weight infants:technical review, Geneva, 2006, WHO Library.
37. Eibl MM,Wolf HM, FurnkranzH, et al: Prevention of nec-rotizing enterocolitis in low-birth-weight infants byIgA-IgG feeding, N Engl J Med 319:1, 1988.
38. Eidelmann AI, Hoffman NW, Kaitz M: Cognitive deficitsin women after childbirth, Obstet Gynecol 81:764, 1993.
39. El-Mohaneles AE, Picard MB, Simmens SJ, et al: Useof human milk in the intensive care nursery decreas-es the incidence of nosocomial sepsis, J Perinatol 17:130,1997.
40. Ernst JA, Rickard KA, Neal PR, et al: Lack of improvedgrowth outcome related to non-nutritive sucking in verylow birth weight premature infants fed a controlled nutri-ent, Pediatrics 83:706, 1989.
41. Feldman R, Eidelman AI: Direct and indirect effectsof breast milk on the neurobehavioral and cognitive de-velopment of premature infants, Dev Psychobiol 43:109,2003.
42. Fischer CB, Sontheimer D, Scheffer F, et al: Cardiorespira-tory stability of premature boys and girls during kangaroocare, Early Hum Dev 52:145–153, 1998.
43. Forbes GB: Nutritional adequacy of human breast milk forpremature infants. In Lebenthal E, editor: Textbook of gastro-enterology and nutrition, New York, 1981, Raven.
44. Forbes GB: Human milk and the small baby, Am J Dis Child136:577, 1982.
45. Forbes GB: Fetal growth and body composition: implica-tions for the premature infant, J Pediatr Gastroenterol Nutr 2(Suppl):552, 1983.
46. Ford JE, Zechalko A, Murphy J, et al: Comparison of the Bvitamin composition of milk from mothers of preterm andterm babies, Arch Dis Child 58:367, 1983.
47. Furman L, Taylor G,MinichN, et al: The effect of maternalmilk on neonatal morbidity of very low-birth-weightinfants, Arch Pediatr Adolesc Med 157:66–71, 2003.
48. Goldman AS, Chheda S, Keeney SE, et al: Immunologicprotection of the premature newborn by human milk, SeminPerinatol 18:495, 1994.
49. Goldman AS, Garza C, Nichols B, et al: Effects of prema-turity on the immunologic system in human milk, J Pediatr101:901, 1982.
50. Greer FR, McCormick A: Improved bone mineralizationand growth in premature infants fed fortified own mother’smilk, J Pediatr 112:961, 1988.
51. Greer FR, Tsang RC: Calcium, phosphorus, magnesium,and vitamin D requirements for preterm infants.In Tsang RC, editor: Vitamin and mineral requirements for preterminfants, New York, 1985, Marcel Dekker.
52. Groh-Wargo S, Toth A, Mahoney K: The utility of a bilat-eral breast pumping system for mothers of prematureinfants, Neonatal Netw 14:31, 1995.
53. Gross SJ: Bonemineralization in preterm infants fed humanmilk with and without mineral supplementation, J Pediatr111:450, 1987.
54. Gross SJ, Gabriel E: Vitamin E status in preterm infants fedhuman milk or infant formula, J Pediatr 106:635, 1985.
55. Hack M, Estabrook MM, Robertson SS: Development ofsucking rhythm in preterm infants, Early Hum Dev 11:133,1985.
56. Haug M, Laubach C, Burke M, et al: Vitamin E in humanmilk from mothers of preterm and term infants, J PediatrGastroenterol Nutr 6:605, 1987.
57. Heine W: Is mother’s milk the most suitable food for lowbirth weight infants? Early Hum Dev 29:345, 1992.
58. Herman H, Schanler RJ: Benefits of maternal and donorhuman milk for premature infants, Early Hum Dev 82:781,2006.
59. Herrmann K, Carroll K: An exclusively human milk dietreduces necrotizing enterocolitis, Breastfeed Med 9(4):184–190, 2014.
60. Hopkinson JM, Schanler RJ, Garza C: Milk production bymothers of premature infants, Pediatrics 81:815, 1988.
61. Hurst NM, Valentine CJ, Renfro L, et al: Skin-to-skin hold-ing in the neonatal intensive care unit influences maternalmilk volume, J Perinatol 17:213, 1997.
62. Hylander MA, Strobino DM, Dhanireddy R: Human milkfeedings and infection among very low birth weightinfants, Pediatrics 102e:38, 1998.
63. Itabashi K, Hayashi T, Tsugoshi T, et al: Fortified pretermhumanmilk for very low birth weight infants, Early Hum Dev29:339, 1992.
64. Iwai Y, Takanashi T, Nakao Y, et al: Iron status in low birthweight infants on breast and formula feeding, Eur J Pediatr145:63, 1986.
65. Javenpaa AL: Feeding the low-birth-weight infant. IV. Fatabsorption as a function of diet and duodenal bile acids,Pediatrics 72:684, 1983.
66. Javenpaa AL, Raiha NCR, Rassin DK, et al: Preterm infantsfed humanmilk attain intrauterine weight gain,Acta PaediatrScand 72:239, 1983.
67. Jensen RG, Jensen GL: Specialty lipids for infant nutrition.I milks and formulas, J Pediatr Gastroenterol Nutr 15:232–245,1992.
68. Jocson MAL, Mason EO, Schanler RJ: The effects of nutri-ent fortification and varying storage conditions onhost defense properties of human milk, Pediatrics 100:240,1997.
69. Jones E, Dimmock PW, Spencer SA: A randomised con-trolled trial to compare methods of milk expression after
Premature Infants and Breastfeeding 561
preterm delivery, Arch Dis Child Fetal Neonatal Ed 85:F91,2001.
70. Kelly EJ, Newell SJ: Gastric ontogeny: clinical implica-tions, Arch Dis Child 71:F136, 1994.
71. Keunen K, VanElburg RM, VanBel F, et al: Impact of nutri-tion on brain development and its neuroprotectiveimplications following preterm birth (review), Pediatr Res77(1):148–155, 2015.
72. Klein CJ: Nutrient requirements for preterm infant formu-las, J Nutr 132:1395S–1577S, 2002.
73. Kuschel CA, Harding JE: Multicomponent fortified humanmilk for promoting growth in preterm infants, CochraneDatabase Syst Rev 8(4)2004.
74. Kuschel CA, Harding JE: Multicomponent fortified humanmilk for promoting growth in preterm infants (Cochranereview). In The Cochrane Library, issue 4, Chichester, 2004,John Wiley and Sons.
75. LaGamma EF, Browne LE: Feeding practices for infantsweighing less than 1500 g at birth and the pathogenesisof failure of delayed oral feedings to prevent necrotizingenterocolitis, Clin Perinatol 21:271–306, 1994.
76. Lau C: Oral feeding in the preterm infant, Neoreviews 7:e19–e27, 2006.
77. Lebenthal E, Leung YK: The impact of development of thegut on infant nutrition, Pediatr Ann 16:211, 1987.
78. Letarte J, Guyda H, Dussault JH, et al: Lack of protectiveeffect of breastfeeding in congenital hypothyroidism:report of 12 cases, Pediatrics 65:703, 1980.
79. Lewis-Jones DI, Reynolds GI: A suggested role for preco-lostrum in preterm and sick newborn infants, Acta PaediatrScand 72:13, 1983.
80. Lubetsky R, Mandel D, Mimouni FB, et al: Diurnal varia-tions in creamatocrits from expressed breast milk of pre-term infants. Neonatal Fetal Nutr Metab abstract no.644, Pediatr Res 55:644, 2003.
81. Lubetsky R, Vaisman N, Mimouni FB, et al: Energy expen-diture in human milk versus formula-fed preterm infants, JPediatr 143:750–753, 2003.
82. Lubit EC: Cleft palate orthodontics: why, when, how?Am JOrthod 69:562, 1976.
83. Lucas A: Enteral nutrition. In Tsang RC, Lucas A, Uauy R,et al, editors: Nutritional needs of the preterm infant, Baltimore,1993, Williams & Wilkins.
84. Lucas A, Bishop NJ, King FL, et al: Randomized trial ofnutrition for preterm infants after discharge, Arch Dis Child67:324, 1992.
85. Lucas A, Bloom SR, Aynsley-Green A: Gut hormones and“minimal enteral feeding,” Acta Paediatr Scand 75:719, 1986.
86. Lucas A, Cole TJ: Breast milk and neonatal necrotisingenterocolitis, Lancet 336:1519, 1990.
87. Lucas A, Fewtrell MS, Morley R, et al: Randomizedoutcome trial of human milk fortification and develop-mental outcome in preterm infants, Am J Clin Nutr64:142, 1996.
88. Lucas A, Morley R, Cole TJ, et al: Early diet in pretermbabies and developmental status in infancy, Arch Dis Child64:1570, 1989.
89. Lucas A, Morley R, Cole TJ, et al: Early diet in pretermbabies and developmental status at 18 months, Lancet335:1477, 1990.
90. Lucas A, Morley R, Cole TJ, et al: Breast milk and subse-quent intelligence quotient in children born premature,Lancet 339:261, 1992.
91. Maastrup R, Greisen G: Extremely preterm infants tolerateskin-to-skin contact during first weeks of life, Acta Paediatr99:1145–1149, 2010.
92. Malcolm WF, Smith PB, Mears S, et al: Transpyloric tubefeeding in very low birth weight infants with suspected gas-tro esophageal reflux: impact on apnea and bradycardia, JPerinatol 29:372–375, 2009.
93. Mathew OP: Science of bottle feeding, J Pediatr 119:511,1991.
94. Mathew OP, Bhatia J: Sucking and breathing patternsduring breast- and bottle-feeding in term neonates: effectsof nutrient delivery and composition, Am J Dis Child143:588, 1989.
95. Mathur NB, Dwarkadas AM, Sharma VK, et al: Anti-infective factors in preterm human colostrum, Acta PaediatrScand 79:1039, 1990.
96. Meerlo-Habing ZE, Koster-Boes EA, Klip H, et al: Earlydischarge with tube feeding at home for preterm infantsis associated with longer duration of breast feeding, ArchDis Child Fetal Neonatal Ed 94:F294–F297, 2009.
97. Meier PP: Supporting lactation in mothers with very lowbirth weight infants, Pediatr Ann 32:317–325, 2003.
98. Meier PP, Brown LP, Hurst NM: Breastfeeding the preterminfants. In Riordan J, Auerbach K, editors: Breastfeeding andhuman lactation, ed 4, Boston, 2014, Jones & Bartlett, p 449.
99. Meier PP, Brown LP, Hurst NM, et al: Nipple shields forpreterm infants: effects on milk transfer and duration ofbreastfeeding, J Hum Lact 10:63–68, 1994.
100. Meir PP, Engstrom JL, Rossman B: Breastfeeding peercounselors as direct lactation care providers in the neonatalintensive care unit, J Hum Lact 29:313–322, 2013.
101. Meier PP, Engstrom JL, Spanier S, et al: The RushMothers’Milk Club: breastfeeding interventions for mothers withvery-low-birth weight infants, J Obstet Gynecol Neonatal Nurs33:164–174, 2004.
102. Meinzen-Derr J, Poindexter BB, Donovan EF, et al: Therole of human milk feedings in risk of late onset sepsis,Pediatr Res 55:393A, 2004.
103. Morelius E, Ortenstrand A, Theodoresson E, et al: A ran-domized trial of continuous skin-to-skin contact after pre-term birth and the effects on salivary cortisol, parentalstress, depression and breastfeeding, Early Hum Dev91:63–70, 2015.
104. Morley R, Fewtrell MS, Abbott RA, et al: Neurodevelop-ment in children born small for gestational age: a random-ized trial of nutrient-enriched versus standard formula andcomparison with a reference breastfed group, Pediatrics113:515, 2004.
105. Morton J, Hall JY, Wong RJ, et al: Combining hand tech-niques with electric pumping increases milk productioninmothers of preterm infants, JPerinatol289:757–764, 2009.
106. Mortensen EL, Michaelsen KF, Sanders SA, et al: The asso-ciation between duration of breastfeeding and adult intel-ligence, JAMA 287:2365, 2002.
107. Morton JA: The role of the pediatrician in extended breast-feeding of the preterm infant, Pediatr Ann 32:308, 2003.
108. Murphy JF, Neale ML, Matthews N: Antimicrobial proper-ties of preterm breast milk cells, Arch Dis Child 58:198,1983.
109. Narayanan I, Mehta R, Choudhury DK, et al: Sucking onthe “emptied” breast: non-nutritive sucking with a differ-ence, Arch Dis Child 66:241, 1991.
110. Neifert MR, Seacat JM: Practical aspects of breastfeedingthe premature infant, Perinat Neonatal 12:24, 1988.
111. Newell SJ: Enteral feeding of the micro preemie, Clin Peri-natol 27:221, 2000.
112. Nyqvist KH: Early attainmentof breastfeedingcompetencein very preterm infants, Acta Paediatr 97:776–781, 2008.
113. Omarsduttir S, Casper C, Akerman A, et al: Breast milkhandling routines for preterm infants in Sweden: a nationalcross-sectional study, Breastfeed Med 3:165–170, 2008.
114. Orza-Frank R, Bhatia A, Smith C: Combined peer coun-selor and lactation consultant support increases breastfeed-ing in the NICU, Breastfeed Med 8(6):509–510, 2013.
115. Oski FA: Iron requirements of the premature infant.In Tsang RC, editor: Vitamin and mineral requirements in preterminfants, New York, 1985, Marcel Dekker.
1
562 Breastfeeding: A Guide for the Medical Profession
116. Phillips RM, Goldstein M, Houglan K, et al: Multidisci-plinary guidelines for the care of the late preterm infants,J Perinatol 33:S5–S22, 2013.
117. Picciano MF: Nutrient composition of human milk, PediatrClin North Am 48:53, 2001.
118. Ronnestad A, Abrahamsen TG, Medbo S, et al: Late-onsetsepticemia in a Norwegian national cohort of extremelypremature infants receiving very early full human milkfeeding, Pediatrics 115:269–276, 2006.
119. R€onnholm KAR, Perheentupa J, Siimes MA: Supplementa-tion with human milk protein improves growth of smallpremature infants fed human milk, Pediatrics 77:649, 1986.
120. Rossman B, Engstrom JL, Meier PP: Healthcare providers’perceptions of breastfeeding peer counselors in theneonatal intensive care unit, Res Nurs Health 35(5):460–474, 2012.
121. Savilahti E, Jarvenpaa A-L, Raiha NCR: Serum immuno-globulin in preterm infants: comparison of human milkand formula feeding, Pediatrics 72:312, 1983.
122. Schanler RJ, Abrams SA: Postnatal attainment of intrauter-ine macro mineral accretion rates in low birth weightinfants fed fortified human milk, J Pediatr 126:441, 1995.
123. Schanler RJ, Anderson D: The low-birth weight infant.In Duggan C, Watkins JB, Walker WA, editors: Nutritionin pediatrics, ed 4, Hamilton, 2008, BC Decker.
23a. Schanler RJ, Hurst NM: Semin Perinatol, 18:476, 1994.124. Schanler RJ, Shulman RJ, Lau C, et al: Feeding strategies
for premature infants: randomized trial of gastroin-testinal priming and tube-feeding method, Pediatrics 103:434–439, 1999.
125. Schanler RJ, Shulman RN, Lau C, et al: Feeding strateg-ies for premature infants: randomized trial of gastroin-testinal priming and tube-feeding method, Pediatrics103:434–439, 1999.
126. Senterre J, Patel G, Salle B, et al: Beneficial outcomes offeeding fortified human milk versus preterm formula,J Pediatr 103:1150–1157, 1983.
127. Stein H, Cohen D, Herman AAB, et al: Pooled pasteurizedbreast milk and untreated own mother’s milk in the feedingof very low birth weight babies: a randomized controlledtrial, J Pediatr Gastroenterol Nutr 5:242, 1986.
128. Stevenson DK, Yang C, Kerner JA, et al: Intestinal flora inthe second week of life in hospitalized preterm infants fedstored frozen breast milk or a proprietary formula, ClinPediatr (Phila) 24:338, 1985.
129. Sturman JA, Rassin DK, Gaull GE: Amini review: taurine indevelopment, Life Sci 21:1, 1977.
130. Schanler RJ, et al: Subcommittee on Nutrition during Lac-tation, Institute of Medicine: Nutrition during lactation,Washington, D.C., 1991, National Academies Press.
131. Taylor SN, Basile LA, Ebeling M, et al: Intestinal perme-ability in preterm infants by feeding type: mother’s milkversus formula, Breastfeed Med 4:11–15, 2009.
132. Tsang RC, Lucas A, Uauy R, et al: Nutritional needs of the pre-term infant, Baltimore, 1993, Williams & Wilkins.
133. Tyson JE,KennedyKA:Trophic feedings forparenterally fedinfants, Cochrane Database Syst Rev 2005, http://dx.doi.org/10.1002/14651858.CD000504. Art. No.: CD000504.
134. Uauy RD, Birch DG, Birch EE: Effect of dietary omega-3fatty acids on retinal function of very low birth weight neo-nates, Pediatr Res 28:245, 1990.
135. Verronen P: Breastfeeding of low birth weight infants, ActaPaediatr Scand 74:495, 1985.
136. Vohr BR, Poindexter BB, Dusick AM, et al: Beneficialeffects of breast milk in the neonatal intensive care uniton the developmental outcome of extremely low birthweight infants at 18 months, Pediatrics 118:115–123, 2006.
137. Wagner CL, Greer FR, AAP Section on Breastfeeding andCommittee on Nutrition: Prevention of rickets and vitaminD deficiency in infants, children, and adolescents, Pediatrics122:1142–1152, 2008.
138. Wooldridge J, HallWA: Post hospitalization breastfeedingpatterns of moderately preterm infants, J Perinat NeonatalNurs 17:50, 2003.


















