塗抹検査 - ecgo.jp•グラム染色(Gram Stain)とは、細菌等を染色液に よって紫色や赤色に染め分け、球菌か桿菌かの 分類を行う方法。 •前
Superbacteria with NDM-1
中華民國防疫學會
王任賢 秘書長
簡報者簡報註解This presentation will address the risk factors for and the prevention of surgical site infections.
New Delhi metallo-beta-lactamase (NDM-1): I NDM-1 is an enzyme that makes bacteria resistant
to a broad range of beta-lactam antibiotics. These include the antibiotics of the carbapenem family, which are a mainstay for the treatment of antibiotic-resistant bacterial infections. The gene for NDM-1 is one member of a large gene family that encodes beta-lactamase enzymes called carbapenemases. Bacteria that produce carbapenemases are often referred to in the news media as "superbugs" because infections caused by them are difficult to treat. Such bacteria are usually only susceptible to polymyxins and tigecycline.
New Delhi metallo-beta-lactamase (NDM-1): II NDM-1 was first identified in December 2009 in a
patient hospitalised in New Delhi with an infection caused by Klebsiella pneumoniae. It was later detected in bacteria in India, Pakistan, the United Kingdom, the United States, and Canada.The most common bacteria that make this enzyme are Gram negative such as Escherichia coli and Klebsiella pneumoniae, but the gene for NDM-1 can spread from one strain of bacteria to another by horizontal gene transfer
Klebsiella pneumoniaeThe bacterium in which NDM-1 was first identified
超級細菌NDM-1列第四類法定傳染病: I 超級細菌「NDM-1」在全球10多個國家傳出疫情,國
內雖然沒有偵測到相關感染個案,為了防範可能的傳播發生,衛生署疾病管制局公佈將NDM-1腸道菌感染症列為第四類法定傳染病,要求各醫療院所接到疑似個案,必須在24小時內通報,同時將菌株送到疾管局進行確認。
NDM-1基因之多重抗藥性腸道菌感染症,至少入侵全球16個國家或地區,包含鄰近的日本、香港都傳出病例,衛生署公告要求醫師在病患符合臨床、流行病學、檢驗等三大條件時,須於24小時內通報防疫單位。
超級細菌NDM-1列第四類法定傳染病: II 3大條件是:出現感染症狀,特別是曾接受侵入性或
外科手術且被懷疑「NDM-1腸道菌感染症」的病患;於6個月內曾有國外旅遊史,特別是印度、巴基斯坦等地區,或雖無國外醫療史,但在醫療照護過程中接觸疑似病例,臨床檢體分離出腸道菌具carbapenem抗藥性。
疾管局表示,NDM-1超級細菌並非空氣傳染,而是經由外科手術或醫療器械污染的「接觸傳染」,一般而言,患者不需強制隔離,各醫療院所可自行視需要,決定病患是否需要隔離,以落實院內感染管控措施。
NDM-1 Transmission NDM-1 is found in bacterial strains. Bacteria
can be transferred from one human being to another in a variety of different ways. It can be shared through human contact, improper food preparation, hospital procedures and surgeries and more. Proper hygiene including frequent hand washing can help to slow the spread of bacteria that may contain NDM-1
多重耐藥細菌之定義
目前沒有正確的定義
但由MDR-TB的定義中可看出端倪 MDR-TB=INH + RIF resistance
多重耐藥細菌之定義應該為----- 對現行治療準則的藥物均產生抗藥性之細菌
多重耐藥細菌有哪些? Gram-positive VRE GISA, GRSA
Gram-negative KPC Carbapenem resistant Acinetobacter NDM-1
Carbapenem resistance之種類
Carbapenems
Drug Route of Administration FDA Status
Imipenem IV Cleared
Meropenem IV Cleared
Ertapenem IM, IV Cleared
Doripenem IV Cleared
Spectrum of ActivityDrug Strep spp. & MSSA
Entero-bacteriaeae
Non-fermentors Anaerobes
Imipenem + + + +
Meropenem + + + +
Ertapenem + + Limited activity +
Doripenem + + + +
How are Carbapenems Used?Uses by Clinical
Syndrome Bacterial meningitis Hospital-associated
sinusitis Sepsis of unknown
origin Hospital-associated
pneumonia
Use by Clinical Isolate Acinetobacter spp. Pseudomonas
aeruginosa Alcaligenes spp. Enterobacteriaceae Mogenella spp. Serratia spp. Enterobacter spp. Citrobacter spp. ESBL or AmpC + E. coli
and Klebsiella spp.Reference: Sanford Guide
Emerging Carbapenem Resistance in Gram-Negative Bacilli
Significantly limits treatment options for life-threatening infections
No new drugs for gram-negative bacilli
Emerging resistance mechanisms, carbapenemases are mobile,
Detection of carbapenemases and implementation of infection control practices are necessary to limit spread
Carbapenem Resistance: MechanismsEnterobacteriaceae Cephalosporinase + porin loss
Carbapenemase
P. aeruginosa Porin loss
Up-regulated efflux
Carbapenemase
Acinetobacter spp. Cephalosporinase + porin loss
Carbapenemase
Carbapenemases
Classification Enzyme Most Common BacteriaClass A KPC, SME,
IMI, NMC, GES
Enterobacteriaceae(rare reports in P. aeruginosa)
Class B(metallo-β-lactamse)
IMP, VIM, GIM, SPM
P. aeruginosaEnterobacteriaceaAcinetobacter spp.
Class D OXA Acinetobacter spp.
Carbapenemases in the U.S.
Enzyme Bacteria
KPC Enterobacteriaceae
Metallo-β-lactamase P. aeruginosa
OXA Acinetobacter spp.
SME Serratia marcesens
KPC
β-lactams classificationBush-Jacoby-Medeiros system Major subgroups Ambler system Main attributes Group 1 cephalosporinases C (cephalosporinases) Usually chromosomal; resistance to all
β-lactams except carbapenems; not inhibited by clavulanate
Group 2 penicillinases (clavulanic acid susceptible)
2a 2b 2be 2br 2c 2e 2f 2d
A (serine β-lactamases) A A A A A A D (oxacillin hydrolyzing)
Staphylococcal penicillinases Broad-spectrum: TEM-1, TEM-2, SHV-1 Extended-spectrum: TEM and SHV
variants, predominantly Inhibitor-resistant TEM Carbenicillin hydrolyzing Cephalosporinases inhibited by clavulanate Carbapenemases inhibited by clavulanate Oxacillin-hydrolyzing (OXA)
Group 3 metallo-β-lactamase 3a 3b 3c
B (metalloenzymes) B B
Zinc-dependent carbapenemases
Group 4 Not classified Miscellaneous enzymes, most not yet sequenced
Manual of clinical microbiology 2007
Serine carbapenemases of Bush group 2f Hydrolyze imipenem but not resistant to clavulanic acid
inhibition, Include Sme-1, Sme-2, NCM-A, IMI-1, GES-2, KPC-1, KPC-2 and KPC-3 blaNMC-A and blaIMI-1
Chromosomal located genes in E. cloacae Induced by cefoxitin and imipenem
blaSme-1 Chromosomally located in E. cloacae and Serratia marcescens
blaGES-2 A plasmid carried β-Lactamases in P. aeruginosa A point mutation of clavulanic acid inhibited ESBL gene blaGES-1
Gly → Asp at position 170 in the Ω loop
Manual of clinical microbiology 2007
Serine carbapenemases of Bush group 2f
KPC (Klebsiella pneumonia carbapenemase) Also found in Salmonella enterica serotype Cubana,
Klebsiella oxytoca and enterobacter spp. blaKPC-1 Located on nonconjugative plasmid in K. pneumoniae
blaKPC-2 Conjugative plasmid in K. oxytoca and Salmonella spp.
blaKPC-3 Conjugative plasmid in K. pneumoniae
Manual of clinical microbiology 2007
EnterobacteriaceaeInterpretive standard for carbapenem
Antimicrobial Agent
MIC (µg/ml) Interpretive Standard
Susc Int Res
Ertapenem ≤2 4 ≥8
Imipenem ≤4 8 ≥16
Meropenem ≤4 8 ≥16
CLIS M100-S18, p. 100 (M7, MIC).
33
Carbapenemases in Enterobacteriaceae including Klebsiella pneumoniae carbapenemases (KPC) and other
carbapenem-hydrolyzing beta-lactamases increasingly detected in clinical isolates of Enterobacteriaceae,
particularly K. pneumoniae, in some geographic regions Clinical isolates of Enterobacteriaceae harboring these
carbapenemases may be resistant to therapy with carbapenem agents, despite apparent in vitro susceptibility using current CLSI breakpoints
Enterobacteriaceae resistant to extended-spectrum cephalosporins and have carbapenem (meropenem, imipenem, ertapenem) MICs of 2 or 4 µg/mL may produce KPC-type or other carbapenemases
CLSI M100-S18, 2008
Klebsiella pneumoniae Carbapenemase (KPC) KPC confers resistance to all β-lactams including penicillins,
extended-spectrum cephalosporins, monobactams and carbapenems blaKPC gene located on plasmid often occurs with other resistent genes (e.g., ESBL,
fluoroquinolone-R, aminoglycoside-R) Potential for spread of plasmid and R factors Occurrence / Species
Common – Klebsiella pneumoniae Sporadic – Klebsiella oxytoca, Citrobacter freundii, Enterobacter spp.,
E. coli, Salmonella spp., Serratia spp. Also Pseudomonas aeruginosa
KPC Epidemiology First described 1996 in North Carolina
(Yigit et al. 2001. Antimicrob Agents Chemother. 45:1151) Early outbreak in NYC
8 ICU patients with previous exposure to imipenem 6/8 (75%) died
(Ahmad et al. 1999. Clin Infect Dis. 29:325) Highly endemic in NY-NJ area
Primarily ICUs Infections are healthcare associated Affects sickest patients (e.g., transplant) Noted outside the USA also
Geographical Distribution KPC-Producers
Frequent Occurrence
Sporadic Isolate(s)
Courtesy of J. Patel, PhD., CDC 1/0838
簡報者簡報註解Mixed; 29 reported Yes, they conducted some surveillance activity for MRSA; 23 had MRSA reportable in some form and all or selected area.
What might a KPC producer look like?
Amikacin >32 R
ampicillin >32 R
Amp-sulbactam >32 R
Aztreonam >32 R
Cefazolin >32 R
Cefepime >32 R
Cefoxitin >32 R
Ceftazidime >32 R
Ceftriaxone >32 R
Chloramphenicol >32 R
Ciprofloxacin >4 R
Ertapenem >8 R
Gentamicin >16 R
Imipenem >16 R
Levofloxacin >8 R
Meropenem >16 R
piper-tazo >128/4 R
Tetracycline >16 R
Tobramycin >16 R
trimeth-sulfa >4/76 R
MIC (µg/ml) MIC (µg/ml)
How do we detect KPCs? “I” or “R” to ertapenem, imipenem, and meropenem But not all KPC producers are “I” or “R” to all 3
carbapenems by reference methods Variability in results for ertapenem, imipenem, meropenem High sensitivity by ertapenem but lacks specificity Ertapenem also “I” or “R” for
- AmpC-type enzymes + porin loss- ESBLs + porin loss
Anderson et al. 2007. JCM. 45:2723.
How do we detect KPCs? MIC Low level resistance and elevated MICs but in “S” range Look for carbapenem “MIC ≥2 µg/ml”
Typical carbapenem MIC for (susceptible) Enterobacteriaceae is ≤0.5 µg/ml
Disk diffusion Look for carbapenem “I” or “R” Most give “I” or “R” result for ertapenem
Anderson et al. 2007. JCM. 45:2723.
KPC Detection by Carbapenem “I” or “R” Result
Sensitivity/specificity (%)
(K. pneumoniae: N = 31 KPC producers; 45 non-KPC producers)
MethodCarbapenem “I” or “R” result
Meropenem Imipenem Ertapenem
Reference BMD 94/98 94/93 97/89
Disk diffusion 71/96 42/96 97/87
Anderson et al. 2007. JCM. 45:2723.
KPC Detection by Carbapenem MIC of ≥2 µg/ml
Sensitivity/specificity (%)
(K. pneumoniae: N = 31 KPC producers; 45 non-KPC producers)NA, not applicable
MethodCarbapenem MIC of ≥2 µg/ml
Meropenem Imipenem Ertapenem
Reference BMD 100/93 100/93 100/89
Disk diffusion NA NA NA
Anderson et al. 2007. JCM. 45:2723.
If an isolate has an MIC ≥2 µg/ml (or an “I” or “R” zone) to ertapenem, imipenem, or meropenem, how can it be confirmed as a KPC producer?
KPC confirmation testing Best - PCR for blaKPC Alternative - Modified Hodge Test - phenotypic
test for “carbapenemase” activity 100% sensitivity in detecting KPC Variable specificity - detects other carbapenemases
Anderson et al. 2007. JCM. 45:2723.
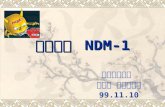
Modified Hodge Test Swab E. coli ATCC 25922
onto plate to create lawn (1:10 dilution of McF 0.5).
Place imipenem disk in center.
Streak test isolates from edge of disk to end of plate.
Incubate overnight. Look for growth of E. coli
around test isolate streak -indicates carbapenem-hydrolyzing enzyme.
negneg
neg
pos
neg
Photo courtesy of J. Patel
Modified Hodge Test
pospos pos
Meropenem ertapenem imipenem
Photo courtesy of J. Patel
Metalo-beta-lactamase
Etest for metallo-b-lactamase
Imipenem
Imipenem+
EDTA
Etest for metallo-b-lactamase
Imipenem
Imipenem+
EDTA
• TEM-1, SHV-1, ESBLs (Bush group 2, Ambler class A)Inhibited by CAS/ AMC 60
• AmpC: (Bush group 1, Ambler class C)Not inhibited by CA, inhibited by boronic acidR/ AMC 60 S/ FEP 10
• MBL: (Bush group 3, Ambler class B)Not inhibited by CA, inhibited by EDTAR/ AMC 60 R/ FEP 10
Common transferable (plasmid mediated) β-lactamases in coliforms
Inhibited by EDTA (Zinc molecule)IMP-4 (most common)VIM, SPM, GIM, SIM (P. aeruginosa)
Hydrolyses all beta-lactam (except aztreonam) Enterobacteriaceae
May have a zone > 6mm with IPM 10Pseudomonas aeruginosa
Highly resistant to all β-lactams => no zoneSusceptible only to aztreonam
Acquired Metallo-Beta-Lactamases Ambler class B or Bush group 3
Treatment
What other drugs can we test if isolate is “R” to all drugs that might be used for Enterobacteriaceae?
Colistin / polymyxin group MIC method No CLSI (or FDA) breakpoint for Enterobacteriaceae but
MIC ≤2 µg/ml likely susceptible
Tigecycline No CLSI breakpoints - use FDA breakpoints (µg/ml) from
pharmaceutical product labeling: ≤2 S; 4 I; ≥8 R
Fosfomycin
Increasing imipenem t>MIC for low level resistance by extended infusion
Polymyxin and Colistin Polymyxins (A-E) Discovered in 1947 Polymyxin B and polymyxin E (colistin
methanesulfate)in clinical use
Colistin Discovered in 1949 Bacillus polymyxa subspecies colistinus koyama
Falagas ME and Kasiakou SK. Clin Infect Dis 2005;40:1333-41.
Colistin
Colistimethate sodium(Colistin methanesulfate)
Chemical Structure
Falagas ME and Kasiakou SK. Clin Infect Dis 2005;40:1333-41.
Colistin (Polymyxin E) Cationic, cyclic decapeptide Target: the bacterial cell membrane
Binds with the anionic lipopolysaccharide (LPS) molecules in the outer membrane of GNB
Permeability change, leakage of cell content, and cell death
Potent anti-endotoxin activity
-- the endotoxin of GNB is the lipid A portion of LPS molecules, and colistin bind and neutrolizes LPS.
Falagas ME and Kasiakou SK. Clin Infect Dis 2005;40:1333-41.
Susceptibility of Colistin17 RCWs, Sputum & Urine Specimens
MIC (µg/mL) No. (%)
Bacteria Range 50% 90% susceptibility
K. pneumoniae –ESBL (n=45) 0.25-2 0.5 1 45 (100)
P. aeruginosa (n=275) 0.25-4 1 1 274 (99.7)
A. baumannii (n=88) 0.12-1 0.5 0.5 88 (100)
Anatomic site/Diagnosis/Modifying Circumstances
Etiologies(usual)
Suggested RegimensPrimary/Alternative
Adjunct Diagnostic or Therapeutic Measures and Comments
Lung/Klebsiella sp.--ESBL pos. & other coliforms
β-lactamase positive
IMP or MER;if resistant ,Polymyxin E (colistin) or B usually several weeks of therapy
ESBL inactivates all cephalosprins ,β-lactam/ β-lactamase inhibitor drug activ.not predicatable ;co-resistance to all FQS &often aminoglycoside
熱病 2007.p.37
SANFORD GUIDE TO ANTIMICROBIAL THERAPY
Intravenous dosage
2,000,000 IU q8h (1 vial q8h )(* 1. The dose is dissolved in 10ml of 0.9% sodium chloride solution or water for injections to form a clear solution.
* 2. Intravenous infusion over a period of 30 minutes )
Inhalation dosage 1,000,000 IU q12h
(*1. The dose is dissolved in 2-4 ml of 0.9% sodium chloride solution or water for injections and poured into the nebuliser.
2. Storing colistimethate aqueous solution for longer than 24 hours increases colistin concentration and increases the potential for lung toxicity.)
Clin Infect Dis 2005:40:1333-41.
Recommended dosage
Colistin loading dose is required
Plachouras D. AAC 2010
Pharmacoeconomic of Colimycin
藥品名 Colimycin Tygacil Tazocin Azactam Maxipime
Mepem Tienam
成分 Colistin Tigecycline Piperacillin+Tazobacta
m
Aztreonam
Cefepime Meropenem
Imipenem
劑量包裝
2M IU/vial 50mg/vial 2.25g/vial 1g/vial 1g/vial 500mg/vial
500mg/vial
價格 NT$138/vial
NT$1754/vial
NT$529/vial
NT$598/vial
NT$689/vial
NT$764/vial
NT$742/vial
使用劑量
2M IU q8h 50mg q12h 4.5g q8h 2g q8h 2g q8h 1g q8h 1g q6h
每日費用
NT$414 NT$3508 NT$3,174 NT$3,588 NT$4,137 NT$4,584 NT$5,936
每日節省2760~5522元,每個療程節省38640~77308元
G(-) in Vitro Data – TaiwanG(-) MIC No.(%) of isolates
Bacteria Range MIC50 MIC90 S* I* R*
E.coli (n=74) 0.12-1 0.25 0.5 74(100) 0(0) 0(0)
K. pneumoniae(n=74) 0.25-2 0.5 1 74(100) 0(0) 0(0)
E. cloacae(n=60) 0.25-2 0.5 1 60(100) 0(0) 0(0)
S. marcescens(n=49) 0.5-8 1 2 47(96) 1(2) 1(2)
C. freumdii(n=46) 0.25-2 0.5 1 46(100) 0(0) 0(0)
M. morgannii(n=56) 0.5-8 2 4 41(73) 11(20) 4(7)
P. Mirabilis(n=59) 2-32 8 8 2(3) 6(10) 51(86)
P. aeruginosa(n=74) 2-32 16 16 1(1) 2(3) 71(96)
A. baumannii(n=72) 0.12-4 1 2 70(97) 2(3) 0(0)
B. cepacia(n=21) 0.25-32 1 16 14(67) 1(5) 6(29)
B.fragilis (n=60) 0.25-16 1 8 46(77) 7(12) 7(12)
Peptococcus spp (n=60) 0.03-0.5
0.03 0.12 60(100) 0(0) 0(0)
Micro Drugs Resistance 2005; Winter 11(4):330-341.
* Provisional Breakpoints provided by Wyeth = “Negotiated Breakpoints” with FDA on June 13 for Enterobacteriaceae S ≤ 2 I = 4 R ≥ 8
Microbiological Spectrum: Taiwan705 Laboratory, unpublished data
Bacteria MIC90 (µg/mL) Susceptible Rate %
PDRAB 2 90
CRAB 2 93.3
Usual AB 2 96.7
Tigecycline and HAP Comparative trial for HAP/VAP of tigecycline vs.
imipenem failed to show non-inferiority Detailed data are not in the public domain
EMEA had concerned regarding the indication of CAP Based on the HAP study results CAP studies included many patients who did not require
hospitalization
The company withdrew the application for CAP as an indication
Doc. Ref. EMEA/245771/2008
管制
What else should we do if we think we have a carbapenem resistance? Inform MD and infection control (suggest ID consult) “Carbapenem-resistant Enterobacteriaceae (XDR
GNR) represent an Infection Control Emergency”(Paterson and Doi. 2007. Clin Infect Dis. 45:1179)
Protocols in regions where carbapenem resistanceare widespread may differ from those in regions where they are rare or have not been seen
Save the isolate!
Standard Precautions 應用於接觸到下列檢體:
BloodAll body fluids (secretions, excretions
(except sweat)) regardless of visible blood
Contact with non-intact skin, mucous membranes and intact skin visibly soiled with blood and body fluids
Standard Precautions Assumes every person/patient potentially infected or
colonized with a microorganism that could be transmitted and cause an infectious process
Hand hygiene programWaterless alcohol-based product or soap and water before and after patient contact, removal of gloves, contact with contaminated objects
Avoid artificial nails, extenders, etc.
Standard Precautions Personal Protective Equipment (PPE)
HCW/patient interaction dictates when and what type of PPE to be worn
Gloves – anticipated contact with blood, body fluids, soiled skin, mucous membranes, non-intact skin
Remove gloves immediately after terminating contact with patient/contaminated environment contact and perform hand hygiene
Gloves should be durable and fit properly
Standard Precautions Gowns
Long-sleeve gown or apron depends on extent of blood or body fluid exposure
Protects skin and prevents soiling of clothing
Fluid or moisture proof or repelling
Standard Precautions Mouth, nose, eye protection
Surgical mask, eye protection (goggles) or face shield when splashing or spraying of blood, body fluids anticipated-Suctioning and wound irrigation or patient’s cough productive, spontaneous
Remove PPE immediately when no longer needed and perform hand hygiene
Standard Precautions Patient Placement
Assess patient for uncontained and excessive secretions, excretions, wound drainage
Semi-private or multiple bed room; no or small amount secretions, etc.
Single bed room if poor hygiene or excessive secretions, excretions or wound drainage
Patient Care EquipmentIf used on multiple patients, clean after each use
(alcohol or disinfectant impregnated disposable wipe)
Standard Precautions Environment
Routine daily and discharge cleaningClean surfaces in close proximity to patient if
blood or body fluids contaminate environmental objects (bed side rails, tables)
EPA-approved disinfectant Laundry
No special precautions, bag securely All hospital soiled laundry considered infectious
Contact Precautions In addition to Standard Precautions
Used by some healthcare facilities to isolate patients with epidemiologically important microorganisms (MRSA, VRE)Patient placementStratified by availability of private rooms and ability to contain blood and body fluids
Contact Precautions Gloves
When touching patient’s skin or inanimate objects in vicinity of patient
GownsDirect contact with patient or environmental objects
Patient EquipmentDedicate or disposable; avoid sharing
懇請賜教
Superbacteria with NDM-1New Delhi metallo-beta-lactamase (NDM-1): INew Delhi metallo-beta-lactamase (NDM-1): IIKlebsiella pneumoniae �The bacterium in which NDM-1 was first identified投影片編號 5超級細菌NDM-1列第四類法定傳染病: I超級細菌NDM-1列第四類法定傳染病: IINDM-1 Transmission多重耐藥細菌之定義多重耐藥細菌有哪些?Carbapenem resistance�之種類CarbapenemsSpectrum of ActivityHow are Carbapenems Used?Emerging Carbapenem Resistance in Gram-Negative BacilliCarbapenem Resistance: MechanismsCarbapenemasesCarbapenemases in the U.S.KPCβ-lactams classificationSerine carbapenemases of Bush group 2f�Serine carbapenemases of Bush group 2fEnterobacteriaceae�Interpretive standard for carbapenemCarbapenemases in Enterobacteriaceae Klebsiella pneumoniae Carbapenemase (KPC)KPC Epidemiology投影片編號 27What might a KPC producer �look like?How do we detect KPCs? How do we detect KPCs?KPC Detection by �Carbapenem “I” or “R” Result KPC Detection by �Carbapenem MIC of 2 µg/mlIf an isolate has an MIC 2 µg/ml (or an “I” or “R” zone) to ertapenem, imipenem, or meropenem, how can it be confirmed as a KPC producer?Modified Hodge TestModified Hodge TestMetalo-beta-lactamase投影片編號 37投影片編號 38投影片編號 39投影片編號 40TreatmentWhat other drugs can we test if isolate is “R” to all drugs that might be used for Enterobacteriaceae?Increasing imipenem t>MIC for low level resistance by extended infusionPolymyxin and Colistin投影片編號 45Colistin (Polymyxin E)Susceptibility of Colistin� 17 RCWs, Sputum & Urine Specimens投影片編號 48Recommended dosageColistin loading dose is required投影片編號 51G(-) in Vitro Data – TaiwanMicrobiological Spectrum: Taiwan�705 Laboratory, unpublished data投影片編號 54管制What else should we do if we think we have a carbapenem resistance?Standard PrecautionsStandard PrecautionsStandard PrecautionsStandard PrecautionsStandard PrecautionsStandard PrecautionsStandard PrecautionsContact PrecautionsContact Precautions懇請賜教