
Summary of Benefits - Leon Medical Centers Health PlansSummary of Benefits. January 1st - December...
21
Summary of Benefits January 1st - December 31st H5410_20_77505_M LEON CARES MEDICARE For more information, please contact: Leon Medical Centers Health Plans Member Services at 1-866-393-5366 or 305-559-5366 (TTY: 711). We’re here from 8 a.m. to 8 p.m., seven days a week from October 1st through March 31st and Monday through Friday the rest of the year. You can also visit LMChealthplans.com. 2020
Transcript of Summary of Benefits - Leon Medical Centers Health PlansSummary of Benefits. January 1st - December...

Summaryof Benefits
January 1st - December 31st
H5410_20_77505_M
LEON CARES
MEDICARE
For more information, please contact: Leon Medical Centers Health Plans Member Services at 1-866-393-5366 or 305-559-5366 (TTY: 711). We’re here from 8 a.m. to 8 p.m., seven days a week from October 1st through March 31st and Monday through Friday the rest of the year. You can also visit LMChealthplans.com.
2020H5410_20_77505_M_Summary of Benefits.indd 1 9/3/19 2:42 PM

SUMMARY OF BENEFITS
Our service area only includes the following zip codes in Miami-Dade County, Florida:
Miami-Dade County, Florida: 33010, 33012, 33013, 33014, 33015, 33016, 33018, 33054, 33055, 33056, 33125, 33126, 33127,33128, 33129, 33130, 33131, 33132, 33133, 33134, 33135, 33136, 33137, 33138, 33139, 33140, 33141, 33142, 33143, 33144, 33145, 33146, 33147, 33150, 33155, 33156, 33157, 33158, 33161, 33165, 33166, 33167, 33168, 33169, 33170, 33172, 33173, 33174, 33175, 33176, 33177, 33178, 33182, 33183, 33184, 33185, 33186, 33187, 33189, 33190, 33192, 33193, 33194, 33196
20_S_H5410_001_A
Co
ve
rag
e
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) H54
10
-00
1
January 1, 2020 - December 31, 2020
Leon Medical Centers Health Plans – Leon Cares (HMO) H5410-001

INTRODUCTION TO SUMMARY OF BENEFITS
This Summary of Benefits gives you
a summary of what Leon Medical
Centers Health Plans – Leon Cares
(HMO) covers and what you pay. It
doesn’t list every service that we
cover or list every limitation or
exclusion. To get a complete list of
services we cover, refer to the plan’s
Evidence of Coverage (EOC) online at
LMChealthplans.com, or call us to
request a copy.
Tips for comparing your Medicare choices
• If you want to compare our plan
with other Medicare health plans,
ask the other plans for their
Summary of Benefits. Or, use the
Medicare Plan Finder on
www.medicare.gov.
• If you want to know more about the coverage and costs of Original Medicare, look
in your current “Medicare & You” handbook. View it online at www.medicare.gov
or get a copy by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day,
7 days a week. TTY users should call 1-877-486-2048.
Leon Medical Centers Health Plans – Leon Cares (HMO) Phone Numbers and Website
• If you’d you like to join our plan, call toll-free 1-866-393-5366 or 305-559-5366
(TTY 711). Licensed agents are available October 1 – March 31, 8 a.m. – 8 p.m. local
time, 7 days a week. From April 1 – September 30, Monday – Friday 8 a.m. – 8 p.m.
local time.
• If you are already a member of our plan, call toll-free 1-866-393-5366 or
305-559-5366 (TTY 711). Member Services is available October 1 – March 31,
8 a.m. – 8 p.m. local time, 7 days a week. Monday through Friday the rest of the
year.
• Our website: LMChealthplans.com
What’s Inside
1 About Leon Medical
Centers Health Plans –
Leon Cares (HMO)
2 Monthly Premium, Deductible
and Limits on How Much You
Pay for Covered Services
3 Covered Medical & Hospital
Benefits
4 Prescription Drug Benefits
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge
1 ABOUT LEON MEDICAL CENTERS HEALTH PLANS – LEON CARES (HMO)
Who can join?
To join Leon Medical Centers Health Plans – Leon Cares (HMO), you must
be entitled to Medicare Part A, be enrolled in Medicare Part B and live in
our service area.
Our service area only includes the following zip codes in Miami-Dade County,
Florida:
Miami-Dade County, Florida: 33010, 33012, 33013, 33014, 33015, 33016, 33018,
33054, 33055, 33056, 33125, 33126, 33127,33128, 33129, 33130, 33131, 33132, 33133, 33134, 33135, 33136, 33137, 33138, 33139, 33140, 33141,
33142, 33143, 33144, 33145, 33146, 33147, 33150, 33155, 33156, 33157, 33158, 33161, 33165, 33166, 33167, 33168, 33169, 33170, 33172, 33173,
33174, 33175, 33176, 33177, 33178, 33182, 33183, 33184, 33185, 33186, 33187, 33189, 33190, 33192, 33193, 33194, 33196
Which doctors, hospitals and pharmacies can I use?
Leon Medical Centers Health Plans – Leon Cares (HMO) has a network of
doctors, hospitals, pharmacies and other providers. If you use the providers
that are not in our network, the plan may not pay for these services. Prior
authorization or a referral may be required to receive covered services.
You must generally use network pharmacies to fill your prescriptions for covered
Part D drugs. Some of our network pharmacies have preferred cost-sharing. You may pay less if you use these pharmacies.
• You can see our plan’s Provider and Pharmacy Directory on our website,LMChealthplans.com
• Or, call us and we will send you a copy of the Provider and Pharmacy Directory.
This is a Health Maintenance Organization (HMO) Medicare Advantage plan.
When you become a member of our plan, you must choose a primary care
provider (PCP) in the plan’s network to provide and oversee your medical care.
Your PCP will also “coordinate” the covered services you get as a member of our
plan. For example, in order for you to see a specialist, you may need to get a
referral from your PCP first.
Co
ve
rag
e
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)

What do we cover?
Like all Medicare Advantage plans, we cover everything that Original Medicare covers - and more.
• Our members get all of the benefits covered by Original Medicare.
• Our members also get more than what is covered by Original Medicare. Some of
the extra benefits are outlined in this Summary of Benefits.
We cover Part D drugs. In addition, we cover Part B drugs such as chemotherapy
and some drugs administered by your provider.
• You can see the plan’s complete Prescription Drug List (formulary) which lists the
Part D prescription drugs along with any restrictions on our website,LMChealthplans.com
• Or, call us and we will send you a copy of the plan’s Prescription Drug List
(formulary).
How will I determine my drug costs?
Our plan groups each medication into “tiers.” To locate the tier of your prescribed
drug, please refer to the Prescription Drug List (formulary). The amount you pay
depends on the tier of the drug you’re taking and what stage of coverage you have
reached. For information about the drug coverage stages that occur after you meet
your deductible, see the prescription drug section within this Summary of Benefits.
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

2 MONTHLY PREMIUM, DEDUCTIBLE & LIMITS
Benefit Leon Medical Centers Health Plans – Leon Cares (HMO)
Monthly Premium $0 per month. In addition, you must keep paying your Medicare Part B premium (unless your Part B premium is paid for you by Medicaid or another third party).
Medical Deductible This plan does not have a medical deductible.
Prescription Drug Deductible (Part D)
This plan does not have a prescription drug deductible.
Is there any limit on how much I will pay for my covered services?
Yes. Like all Medicare Advantage plans, our plan protects you by having yearly limits on your out-of-pocket costs for medical and hospital care.
Your maximum out-of-pocket limit in this plan is:
$3,400 for covered services you receive from in-network providers
This amount is the most you pay for copays, coinsurance and other costs for covered Medicare Part A (hospital) and Part B (medical) services for the year. Once you reach this limit, we will pay the full cost of your covered services in our plan for the rest of the year.
You will still need to pay your monthly premiums and cost-sharing for your Part D prescription drugs.
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e
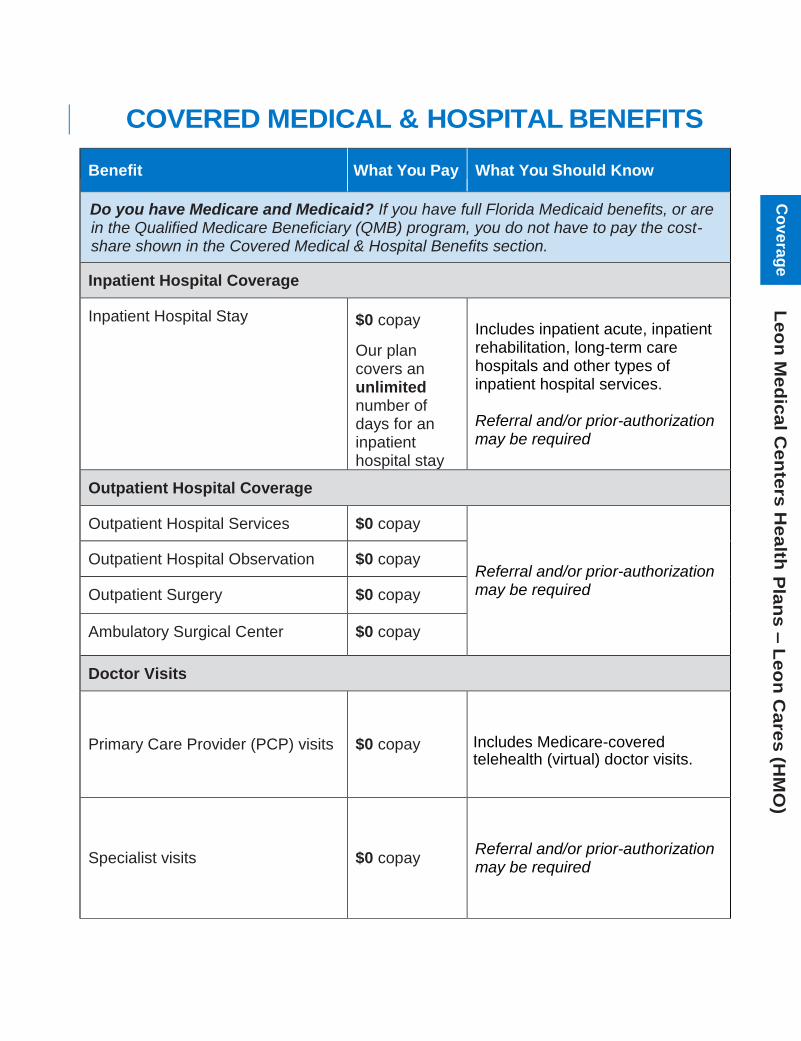
3 COVERED MEDICAL & HOSPITAL BENEFITS
Benefit What You Pay What You Should Know
Do you have Medicare and Medicaid? If you have full Florida Medicaid benefits, or are in the Qualified Medicare Beneficiary (QMB) program, you do not have to pay the cost-share shown in the Covered Medical & Hospital Benefits section.
Inpatient Hospital Coverage
Inpatient Hospital Stay $0 copay
Our plan covers an unlimited number of days for an inpatient hospital stay
Includes inpatient acute, inpatient rehabilitation, long-term care hospitals and other types of inpatient hospital services.
Referral and/or prior-authorization may be required
Outpatient Hospital Coverage
Outpatient Hospital Services $0 copay
Referral and/or prior-authorization may be required
Outpatient Hospital Observation $0 copay
Outpatient Surgery $0 copay
Ambulatory Surgical Center $0 copay
Doctor Visits
Primary Care Provider (PCP) visits $0 copay Includes Medicare-covered telehealth (virtual) doctor visits.
Specialist visits $0 copay Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Benefit What You Pay What You Should Know
Preventive Care
Our plan covers Medicare- covered preventive services, including:
Abdominal aortic aneurysmscreening
Alcohol misuse counseling
Annual wellness visit
Bone mass measurement Breast cancer screening
(mammogram) Cardiovascular disease risk
reduction
Cardiovascular disease testing Cervical and vaginal cancer
screening (pap test) Colorectal cancer screening
(colonoscopy, fecal occult bloodtest, flexible sigmoidoscopy)
Depression screening
Diabetes screenings
Diabetes self-managementtraining
Glaucoma screening
HIV screening Lung cancer screening with low
dose computed tomography(LDCT)
Medical nutrition therapy services
Medicare Diabetes PreventionProgram (MDPP)
Obesity screening and therapy
Prostate cancer screenings(PSA)
Sexually transmitted infectionsscreening and counseling
Smoking and tobacco usecessation counseling
Vaccines, including Flu shots,Hepatitis B shots andPneumonia shots
“Welcome to Medicare”preventive visit (one-time)
$0 copay Any additional preventive services approved by Medicare during the benefit year will be covered. Please see our Evidence of Coverage (EOC) for frequency of covered services.
Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e
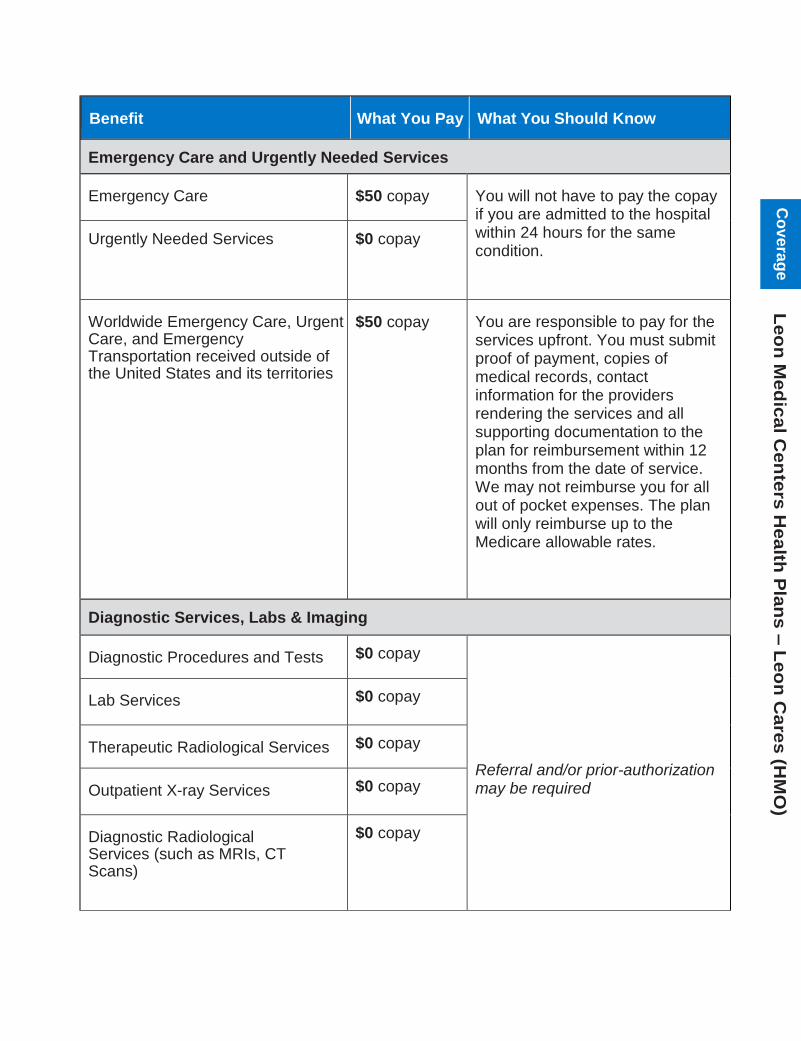
Benefit What You Pay What You Should Know
Emergency Care and Urgently Needed Services
Emergency Care $50 copay You will not have to pay the copay if you are admitted to the hospital within 24 hours for the same condition.
Urgently Needed Services $0 copay
Worldwide Emergency Care, Urgent Care, and Emergency Transportation received outside of the United States and its territories
$50 copay You are responsible to pay for the services upfront. You must submit proof of payment, copies of medical records, contact information for the providers rendering the services and all supporting documentation to the plan for reimbursement within 12 months from the date of service. We may not reimburse you for all out of pocket expenses. The plan will only reimburse up to the Medicare allowable rates.
Diagnostic Services, Labs & Imaging
Diagnostic Procedures and Tests $0 copay
Referral and/or prior-authorization may be required
Lab Services $0 copay
Therapeutic Radiological Services $0 copay
Outpatient X-ray Services $0 copay
Diagnostic Radiological Services (such as MRIs, CT Scans)
$0 copay
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Benefit What You Pay What You Should Know
Hearing Services
Non-routine Hearing Exams (Medicare-covered)
$0 copay Exam to diagnose and treat hearing and balance issues
Routine Hearing Exams
(one every year)
$0 copay
Hearing Aid Evaluation/Fitting
(up to two every three years) $0 copay
Hearing Aids
(one per ear every three years)
$0 copay You receive up to $1,050 per hearing aid per ear ($2,100 maximum benefit) every 3 years
Dental Services
Medicare-covered Dental Services $0 copay Limited dental services which does not include most dental care or procedures like cleanings, fillings, tooth extractions, dentures, or other dental devices.
Referral and/or prior-authorization may be required
Preventive Dental Services:
Cleaning (up to 2 every year)
Dental X-Ray(s) (1 every year)
Fluoride treatment (1 every year)
Oral exam (1 every year)
$0 copay
There is a combined maximum benefit of $2,300 per calendar year for preventive and comprehensive dental services.
For specific dental coverage, exclusions and limitations, please refer to the 2020 Dental Schedule of Services.
Referral and/or prior-authorization may be required
Comprehensive Dental Services:
Restorative services (Fillings)
Endodontics (Root Canals)
Periodontics (Gum and Bonetreatment)
Prosthodontics (Dentures)
Dental Implants
Oral and Maxillofacial Surgery(Extractions)
$0 copay
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e

Benefit What You Pay What You Should Know
Vision Services
Non-routine Eye Exam (Medicare-covered)
$0 copay Diagnosis and treatment of diseases and injuries of the eye, including treatment for age-related macular degeneration and Diabetic Retinopathy Screening
Referral and/or prior-authorization may be required
Routine Eye Exam
(one every year)
$0 copay
Non-routine Eyewear (Medicare-
covered)
$0 copay One pair of eyeglasses or contact lenses after each cataract surgery that includes insertion of an intraocular lens
Routine Eyewear
Eyeglasses (lenses and frames)(up to two every year)
Contact lenses
Upgrades
$0 copay Up to two (2) pairs of eyeglasses each year not to exceed $175 per pair of eyeglasses including upgrades for a maximum benefit of $350.
OR
Up to four (4) boxes of soft contact lenses each year not to exceed $35 per box of soft contact lenses for a maximum benefit of $140.
Vision services are only available at Leon Medical Centers’ on-site optical center
Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Benefit What You Pay What You Should Know
Mental Health Services
Inpatient Mental Health Care Days 1-90:
$0 copay
Days 91 and beyond:
$0 copay for each lifetime reserve day (up to 60 days per lifetime)
Our plan covers 90 days for an inpatient mental health hospital stay.
Our plan also covers 60 lifetime reserve days. The plan covers 190 days in a lifetime for inpatient mental health care in a psychiatric hospital.
Referral and/or prior-authorization may be required
Outpatient Mental Health Care $0 copay Individual or Group therapy visits
Referral and/or prior-authorization may be required
Outpatient Substance Abuse Services
$0 copay Covered services include substance abuse outpatient services, outpatient evaluation and treatment, outpatient individual or group therapy sessions and medication management for substance abuse related disorders
Referral and/or prior-authorization may be required
Partial Hospitalization Services $0 copay Structured program of active psychiatric treatment provided as a hospital outpatient service or by a community mental health center, that is more intense than the care received in your doctor’s or therapist’s office and is an alternative to inpatient hospitalization.
Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e

Benefit What You Pay What You Should Know
Skilled Nursing Facility
Skilled Nursing Facility (SNF) Care $0 copay You are covered for up to 100 days in a SNF.
Referral and/or prior-authorization may be required
Outpatient Rehabilitation Services
Physical Therapy $0 copay Outpatient rehabilitation services are provided in various outpatient settings, such as hospital outpatient departments, independent therapist offices, and Comprehensive Outpatient Rehabilitation Facilities (CORFs).
Occupational Therapy $0 copay Referral and/or prior-authorization may be required Speech Therapy $0 copay
Cardiac (heart) Rehab Services $0 copay Comprehensive programs of cardiac rehabilitation services that include exercise, education, and counseling
Referral and/or prior-authorization may be required
Pulmonary Rehab Services $0 copay Programs for moderate to very severe chronic obstructive pulmonary disease (COPD)
Referral and/or prior-authorization may be required
Supervised Exercise Therapy (SET) $0 copay Programs for symptomatic peripheral artery disease (PAD)
Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Benefit What You Pay What You Should Know
Ambulance
Ground Service (one-way trip) $0 copay Referral and/or prior-authorization may be required for non-emergency ambulance services.
Air Service (one-way trip) $0 copay
Transportation (non-emergency)
Routine Transportation Services (one-way trip)
$0 copay
Our plan covers unlimited one-way trips per year
Transportation services are provided from your home to your assigned PCP and Leon Medical Centers facility, or Leon Healthy Living Centers. Services are only available when using Leon Medical Centers transportation vehicles unless authorized by the plan. Transportation to network providers outside of Leon Medical Centers must be requested by a Leon Medical Centers physician and may require authorization by the plan.
Referral and/or prior-authorization may be required
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e

Benefit What You Pay What You Should Know
Medicare Part B Prescription Drugs
Medicare Part B Drugs $0 copay for Hyaluronate Sodium Injection, Inhalation drugs via Nebulizer, and Intravitreal Bevacizumab (Avastin) Injection
20% coinsurance for all other Part B drugs
Referral and/or prior-authorization may be required
This plan has Part D prescription drug coverage. See section 4 of this booklet for more details.
Chiropractic Care
Chiropractic Services (Medicare-covered)
$0 copay Manual manipulation of the spine to correct subluxation
Dialysis (Kidney Disease Services)
Outpatient/Inpatient Dialysis Treatments
$0 copay Referral and/or prior-authorization may be required
Self-dialysis Training $0 copay
Kidney Disease Education $0 copay
Fitness & Wellness Programs
Fitness Program $0 copay Leon Healthy Living Centers have strength and cardiovascular training equipment to help you reach your fitness goals
Health Education $0 copay Leon Healthy Living Centers offer information on a number of health-related topics, as well as programs to aid in personal development.
Enjoy health seminars on important issues that include: • Preventive Medicine• Diet and Nutrition• Diabetes• Fall prevention
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Benefit What You Pay What You Should Know
Home Health Agency Care
Home Health Services $0 copay Referral and/or prior-authorization may be required
Hospice Care
Medicare-certified Hospice Program
Your hospice services are paid for by Original Medicare, not our plan.
You may receive care from any Medicare-certified hospice program
Hospice Consultation Services $0 copay Our plan covers hospice consultation services (one-time only) before you select hospice
Meal Services
Meals $0 copay After a discharge from an acute inpatient hospital stay or skilled nursing facility, you may be eligible to receive 14 nutritious meals delivered to your home. You are eligible to receive this benefit up to three (3) times per year.
Referral and/or prior-authorization may be required
Medical Equipment & Supplies
Durable Medical Equipment (wheelchairs, oxygen, etc.)
$0 copay
Referral and/or prior-authorization may be required
Prosthetic Devices (braces, artificial limbs, etc.) and Related Medical Supplies
$0 copay
Diabetes Supplies & Services $0 copay
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e

Benefit What You Pay What You Should Know
Over-the-Counter (OTC) Items
OTC Items $0 copay You are eligible for a $150 per quarter benefit maximum of approved over-the-counter (OTC) items which include health and wellness products for your exclusive use. Items are only available at Leon Medical Centers’ on-site pharmacies and includes delivery to your home.
Unused amounts will not carry over to the next quarter.
Opioid Treatment Program Services
Opioid Use Treatment Services $0 copay Covered services include:
• FDA-approved opioidagonist and antagonisttreatment medicationsand the dispensing andadministration of suchmedications, if applicable
• Substance usecounseling
• Individual and grouptherapy
• Toxicology testing
Podiatry Services
Foot care (Medicare-covered) $0 copay Diagnosis and the medical or surgical treatment of injuries and diseases of the feet (such as hammer toe or heel spurs)
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

4 PRESCRIPTION DRUG BENEFITS
Benefit Leon Medical Centers Health Plans – Leon Cares (HMO)
Prescription Drug (Part D) Benefits
How do the prescription drug benefits work?
This plan includes prescription drug coverage. Our network includes pharmacies that offer standard cost-sharing and pharmacies that offer preferred cost-sharing. You may go to either type of network pharmacy to receive your covered prescription drugs. Your copay(s) may be less at pharmacies with preferred cost-sharing. To find a network pharmacy, you can look in our Provider & Pharmacy Directory, visit our website (LMCHealthPlans.com), or call us at the phone number in this booklet.
You can get your prescriptions from an out-of-network pharmacy, but may pay more than you would at an in-network pharmacy. If you reside in a long term care facility, you would pay the same cost-sharing as a standard network retail pharmacy.
The plan has a list of covered drugs known as a Formulary. We call it the “Drug List” for short. The term “covered drugs” means all of the Part D prescription drugs that are covered on the plan’s Drug List.
Additional Drug Coverage
We offer additional coverage on some prescription drugs that are not normally covered in a Medicare Prescription Drug Plan. Payments made for these drugs will not count towards your initial coverage limit or total out-of-pocket costs. To find out which drugs our plan covers, refer to your Formulary.
Are you currently getting help to pay for your drugs? If you are in a program, like Extra Help, that helps pay for your drugs, your costs may be lower than the cost-share in this section.
Drug Payment Stages As shown in the table below, there are “drug payment stages” for your prescription drug coverage. How much you pay for a drug depends on which of these stages you are in at the time you get a prescription filled or refilled.
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e

Initial Coverage Stage
You begin in this stage when you fill your first prescription of the year. During this stage, the plan pays its share of the cost of your drugs and you pay your share of the cost. You stay in this stage until your year-to-date “total drug costs” (your payments plus any Part D plan’s payments) total $7,000. If you reach this amount, you will leave the Initial Coverage Stage and move on to the Coverage Gap Stage.
Tier Preferred Retail Cost-Sharing Standard Retail Cost-Sharing
Tier 1: Generic Drugs $ 0 copay for 30-day supply. $ 0 copay for 90-day supply.
$ 5 copay for 30-day supply. $15 copay for 90-day supply.
Tier 2: Preferred Brand Drugs
$ 0 copay for 30-day supply. $ 0 copay for 90-day supply.
$10 copay for 30-day supply. $30 copay for 90-day supply.
Tier 3: Non-Preferred Drugs
$40 copay for 30-day supply. $80 copay for 90-day supply.
$50 copay for 30-day supply. $150 copay for 90-day supply.
Tier 4: Specialty Drugs
33% coinsurance – 30 Day Supply
33% coinsurance – 30 Day Supply
Coverage Gap Stage
Most Medicare prescription drug plans have a Coverage Gap (also called the “Donut Hole”). This means that there is a temporary change in what you will pay for your drugs.
You receive coverage for generic and some brand drugs while in the Coverage Gap. Only the amount you pay counts and moves you through the coverage gap. Many people do not reach the $7,000 limit for the Initial Coverage Stage and therefore not everyone will enter the coverage gap.
You stay in this stage until your year-to-date “out-of-pocket costs” (your payments) reach a total of $6,350. If you reach this amount, you will leave the Coverage Gap Stage and move on to the Catastrophic Coverage Stage.
Tier Preferred Retail Cost-Sharing
Standard Retail Cost-Sharing
Tier 1: Generic Drugs $ 0 copay for 30-day supply. $ 0 copay for 90-day supply.
$ 5 copay for 30-day supply. $15 copay for 90-day supply.
Tier 2: Preferred Brand Drugs
Tier 3: Non-Preferred Drugs
Tier 4: Specialty Drugs
For brand name drugs, you pay 25% of the price (plus a portion of the dispensing fee) and 25% of the price for generic drugs
Leo
n M
ed
ica
l Cen
ters
Hea
lth P
lan
s –
Leo
n C
are
s (H
MO
) C
ov
era
ge

Catastrophic Coverage Stage
After your yearly out-of-pocket drug costs (including drugs purchased through your retail pharmacy and through mail order) have reached $6,350, the plan will pay most of the cost for your drugs. Your share of the cost of covered drugs will be the greater of: 5% of the cost of the drug
— or —
$3.60 copay for generic drugs (including brand drugs treated as generic) and $8.95 copay for all other drugs.
All Cigna products and services are provided exclusively by or through operating subsidiaries of
Cigna Corporation, Cigna Health and Life Insurance Company, Cigna HealthCare of South Carolina,
Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare
of Arizona, Inc., Cigna HealthCare of St. Louis, Inc., HealthSpring Life & Health Insurance Company,
Inc., HealthSpring of Florida, Inc., Bravo Health Mid-Atlantic, Inc., and Bravo Health Pennsylvania,
Inc. HealthSpring of Florida, Inc. operates under the assumed name of “Leon Medical Centers
Health Plans” in the Miami-Dade service area. The Cigna name, logos, and other Cigna marks are
owned by Cigna Intellectual Property, Inc. “Leon Medical Centers” is a registered trademark of
Leon Medical Centers. Contact plan for details and availability of these services. Individuals may
enroll in a plan only during specific times of the year and must have Medicare Parts A and B.
Individuals must live in the plan service area. Benefits vary by plan. Prior authorization and / or
referrals are required for certain services. Leon Medical Centers Health Plans complies with
applicable Federal civil rights laws and does not discriminate on the basis of race, color,
national origin, age, disability, or sex. Leon Medical Centers Health Plans cumple con las leyes
federales de derechos civiles aplicables y no discrimina por motivos de raza, color, nacionalidad,
edad, discapacidad o sexo. ATTENTION: If you speak English, language assistance services,
free of charge, are available to you. Call 1-866-393-5366 (TTY 711). ATENCIÓN: Si habla
español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al
1-866-393-5366 (TTY 711). ATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou lang ki
disponib gratis pou ou. Rele 1-866-393-5366 (TTY 711). Leon Medical Centers Health Plans is an
HMO plan with a Medicare contract and a contract with the Florida Medicaid program. Enrollment in
Leon Medical Centers Health Plans depends on contract renewal. © 2020 Cigna
Leo
n M
ed
ica
l C
en
ters
Hea
lth
Pla
ns –
Leo
n C
are
s (
HM
O)
Co
ve
rag
e


















