
Suicide Prevention Education › wp-content › uploads › 2020 › 01 › ... · 2020-01-13 ·...
48
Suicide Prevention Education Dental Healthcare Professionals Gregory L. Jantz, PhD
Transcript of Suicide Prevention Education › wp-content › uploads › 2020 › 01 › ... · 2020-01-13 ·...

Suicide Prevention Education
Dental Healthcare Professionals
Gregory L. Jantz, PhD
The Harsh Realities of Suicide
Since 2008, suicide has ranked as the 10th leading cause of death for all ages in the
United States.
Centers for Disease Control and Prevention. CDC WISQARS: Leading causes of death reports, 1981–2016 . https://www.cdc.gov/nchs/products/databriefs/db330.htm
In 2016, suicide became the second leading cause of death for ages 10–34 and the fourth leading cause for ages 35–54.

In 2017, there were 47,173 deaths by suicide. About one suicide every 11 minutes.
https://www.cdc.gov/niosh/topics/stress/suicide.html
It is estimated that for every suicide, there are almost thirty attempts.
https://afsp.org/about-suicide/suicide-statistics/

More than half who died by suicide did not have a known mental health condition
https://www.cdc.gov/media/releases/2018/p0607-suicide-prevention.html

From 2000 through 2016, suicide rates increased for both males and females, with Data from the National Vital Statistics System, Mortality
• From 1999 through 2017, the age-adjusted suicide rate increased 33% from 10.5 to 14.0 per 100,000.
• Suicide rates were significantly higher in 2017 compared with 1999 among females aged 10–14 (1.7 and 0.5, respectively), 15–24 (5.8 and 3.0), 25–44 (7.8 and 5.5), 45–64 (9.7 and 6.0), and 65–74 (6.2 and 4.1).
• Suicide rates were significantly higher in 2017 compared with 1999 among males aged 10–14 (3.3 and 1.9, respectively), 15–24 (22.7 and 16.8), 25–44 (27.5 and 21.6), 45–64 (30.1 and 20.8) and 65–74 (26.2 and 24.7).
• In 2017, the age-adjusted suicide rate for the most rural (noncore) counties was 1.8 times the rate for the most urban (large central metro) counties (20.0 and 11.1 per 100,000, respectively).
https://www.cdc.gov/nchs/products/databriefs/db330.htm
Suicide rates for males aged 10–74 were higher in 2017 than in 1999.
• Suicide rates for males were highest for those aged 75 and over in both 1999 (42.4 per 100,000) and 2017 (39.7).
• Suicide rates were significantly higher in 2017 compared with 1999 among males aged 10–14 (3.3 and 1.9, respectively), 15–24 (22.7 and 16.8), 25–44 (27.5 and 21.6), 45–64 (30.1 and 20.8), and 65–74 (26.2 and 24.7).
• The suicide rate in 2017 for males aged 75 and over (39.7) was significantly lower than the rate in 1999 (42.4).
https://www.cdc.gov/nchs/products/databriefs/db330.htm

Suicide rates for males, by
age group: United States, 2000 and 2017
NOTES: Suicides were identified using International Classification of Diseases, 10th Revision, underlying cause-of-death codes: U03, X60–X84, and Y87.0. SOURCE: NCHS, National Vital Statistics System, Mortality. https://www.cdc.gov/nchs/products/databriefs/db330.htm

Suicide rates for females aged 10–74 were higher in 2016 than in 2000.
• Suicide rates for females were highest among those aged 45–64 in both 2000 (6.2 per 100,000 females) and 2016 (9.9).
• Although based on a small number of deaths, the suicide rate for females aged 10–14 increased significantly, from 0.6 per 100,000 in 2000 to 1.7 in 2016.
• Suicide rates were significantly higher in 2016 compared with 2000 among females aged 15–24 (5.4 and 3.0, respectively), 25–44 (7.6 and 5.4), 45–64 (9.9 and 6.2), and 65–74 (6.2 and 4.0).
https://www.cdc.gov/nchs/products/databriefs/db309.htm

Suicide rates for females, by age group: United States, 2000 and 2017
NOTES: Suicides were identified using International Classification of Diseases, 10th Revision, underlying cause-of-death codes: U03, X60–X84, and Y87.0. SOURCE: NCHS, National Vital Statistics System, Mortality. https://www.cdc.gov/nchs/products/databriefs/db330.htm
In 2016, the means of suicide among females varied by age group.•Among females aged 10–14, the most frequent means of suicide in 2016 was suffocation (119 of 171 deaths or 70%). (Suffocation can be by hanging or a plastic bag over the head.)•Nearly three-quarters of all suicides among females aged 15–24 involved either suffocation (509 of 1,148 deaths or 44%) or firearms (335 deaths or 29%).•Among females aged 25–44, 32% (1,035 of 3,215 deaths) of suicides involved firearms, 31% involved suffocation (1,004 deaths), and 28% involved poisoning (887 deaths).•Poisoning was the most frequent means of suicide among females aged 45 and over, accounting for 40% of suicides among those aged 45–64 (1,720 of 4,253 deaths), 41% among those aged 65–74 (381 of 940 deaths), and 37% among those aged 75 and over (188 of 510 deaths).•Firearms were the second most frequent means of suicide among females aged 45 and over, accounting for 32% of suicides among those aged 45–64 (1,361 of 4,253 deaths), 38% among those aged 65–74 (358 of 940 deaths), and 33% among those aged 75 and over (168 of 510 deaths).
https://www.cdc.gov/nchs/products/databriefs/db309.htm

Number of suicides for females, by age group and means of suicide: United States, 2016
NOTES: Suicides were identified using International Classification of Diseases, 10th Revision, underlying cause-of-death codes: U03, X60–X84, and Y87.0. Suicides were categorized by the means of suicide involved based on the underlying cause-of-death codes: firearm (X72–X74), suffocation (X70), poisoning (X60–X69), and other means (U03, X71, X75–X84, and Y87.0). SOURCE: NCHS, National Vital Statistics System, Mortality. https://www.cdc.gov/nchs/products/databriefs/db309.htm
In 2016, the means of suicide among males also varied by age group.
• In 2016, suffocation and firearms each accounted for about one-half (48%) of suicides among males aged 10–14 (128 and 126 of 265 deaths, respectively).
• For males aged 15–24, about one-half of all suicides (2,348 of 4,575 deaths or 51%) involved firearms while another one-third (1,591 deaths or 35%) involved suffocation.
• For males aged 25 and over, the percentage of suicides involving firearms increased with age, from 48% of suicides among those aged 25–44 (5,362 of 11,181 deaths), to 55% among those aged 45–64 (6,579 of 11,943 deaths), to 74% among those aged 65–74 (2,574 of 3,463 deaths), and to 81% among those aged 75 and over (2,656 of 3,291 deaths).
https://www.cdc.gov/nchs/products/databriefs/db309.htm
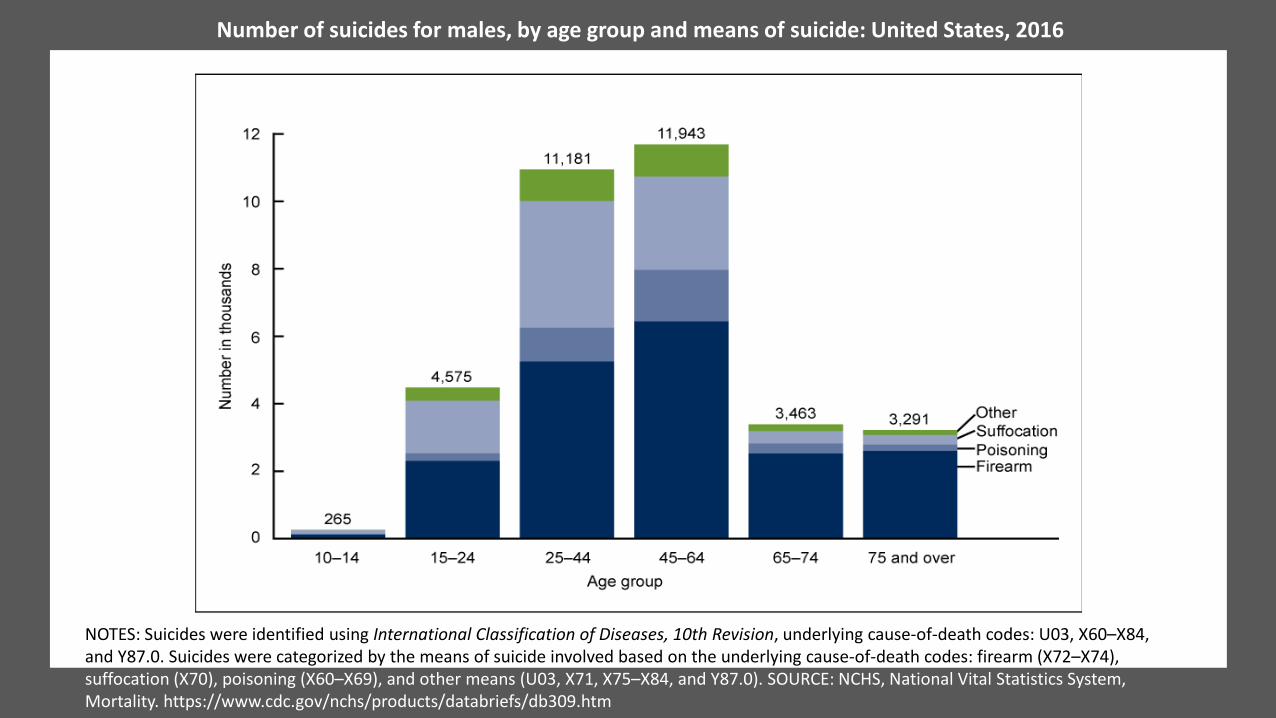
Number of suicides for males, by age group and means of suicide: United States, 2016
NOTES: Suicides were identified using International Classification of Diseases, 10th Revision, underlying cause-of-death codes: U03, X60–X84, and Y87.0. Suicides were categorized by the means of suicide involved based on the underlying cause-of-death codes: firearm (X72–X74), suffocation (X70), poisoning (X60–X69), and other means (U03, X71, X75–X84, and Y87.0). SOURCE: NCHS, National Vital Statistics System, Mortality. https://www.cdc.gov/nchs/products/databriefs/db309.htm


Suicidal Thoughts and Behaviors Among U.S. Adults
4.3% of adults age 18 and older in the United States had thoughts about suicide in 2017.
• Among adults across all age groups, the prevalence of serious suicidal thoughts was highest among adults aged 18-25 (10.5%).
• Among adults reporting race/ethnicity, the prevalence of serious suicidal thoughts was highest among adults reporting two or more races (8.9%).
Based on data from the 2017 National Survey on Drug Use and Health (NSDUH)1 by the Substance Abuse and Mental Health Services Administration (SAMHSA). https://www.nimh.nih.gov/health/statistics/suicide.shtml#part_154973
Depression is the most common type of mental illness, affecting more than 26% of the U.S. adult population. It has been estimated that by the year 2020, depression will be the second leading cause of disability throughout the world, trailing only ischemic heart disease. (Centers for Disease Control & Prevention) https://www.cdc.gov/mentalhealth/basics.htm

Signs and Symptoms

According to the Mayo Clinic:Although depression may occur only once during your life, people typically have multiple episodes. During these episodes, symptoms occur most of the day, nearly every day and may include:• Feelings of sadness, tearfulness, emptiness or hopelessness• Angry outbursts, irritability or frustration, even over small matters• Loss of interest or pleasure in most or all normal activities, such as sex, hobbies or sports• Sleep disturbances, including insomnia or sleeping too much• Tiredness and lack of energy, so even small tasks take extra effort• Reduced appetite and weight loss or increased cravings for food and weight gain• Anxiety, agitation or restlessness• Slowed thinking, speaking or body movements• Feelings of worthlessness or guilt, fixating on past failures or self-blame• Trouble thinking, concentrating, making decisions and remembering things• Frequent or recurrent thoughts of death, suicidal thoughts, suicide attempts or suicide• Unexplained physical problems, such as back pain or headaches
https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007
Depression symptoms in children and teensCommon signs and symptoms of depression in children and teenagers are similar to those of adults, but there can be some differences.• In younger children, symptoms of depression may include sadness, irritability,
clinginess, worry, aches and pains, refusing to go to school, or being underweight.• In teens, symptoms may include sadness, irritability, feeling negative and
worthless, anger, poor performance or poor attendance at school, feeling misunderstood and extremely sensitive, using recreational drugs or alcohol, eating or sleeping too much, self-harm, loss of interest in normal activities, and avoidance of social interaction.
https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007

Depression symptoms in older adultsDepression is not a normal part of growing older, and it should never be taken lightly. Unfortunately, depression often goes undiagnosed and untreated in older adults, and they may feel reluctant to seek help. Symptoms of depression may be different or less obvious in older adults, such as:• Memory difficulties or personality changes• Physical aches or pain• Fatigue, loss of appetite, sleep problems or loss of interest in sex — not
caused by a medical condition or medication• Often wanting to stay at home, rather than going out to socialize or doing new
things• Suicidal thinking or feelings, especially in older men

• Washington has the 10th highest overall rate of depression in the U.S.• From 2014-2018, Washington’s depression rate grew by 9.26%• Washington ranks 24th in the U.S. for access to mental healthcare.
https://quotewizard.com/news/posts/states-with-highest-depression-rates

Risk factors for suicide
Suicide is the 2nd leading cause of death in middle and high schoolers (ages 12-18)
Suicide is the 2nd leading cause of death in college age youth (ages 18-22)
Source: (2016 CDC WISQARS)

According to the National Institutes of Mental Health (NIMH),the main risk factors for suicide are:
• A prior suicide attempt• Depression and other mental health disorders• Substance abuse disorder• Family history of a mental health or substance abuse disorder• Family history of suicide• Family violence, including physical or sexual abuse• Having guns or other firearms in the home• Being in prison or jail• Being exposed to others’ suicidal behavior, such as a family member, peer, or
media figure• Medical illness• Being between the ages of 15 and 24 years or over age 60
https://www.nimh.nih.gov/health/publications/suicide-faq/index.shtml
CDC - Risk Factors for SuicideA combination of individual, relationship, community, and societal factors contribute to the risk of suicide. Risk factors are those characteristics associated with suicide—they might not be direct causes.• Family history of suicide• Family history of child maltreatment• Previous suicide attempt(s)• History of mental disorders, particularly clinical depression• History of alcohol and substance abuse• Feelings of hopelessness• Impulsive or aggressive tendencies• Cultural and religious beliefs (e.g., belief that suicide is noble resolution of a personal
dilemma)• Local epidemics of suicide• Isolation, a feeling of being cut off from other people• Barriers to accessing mental health treatment• Loss (relational, social, work, or financial)• Physical illness• Easy access to lethal methods• Unwillingness to seek help because of the stigma attached to mental health and substance
abuse disorders or to suicidal thoughtshttps://www.cdc.gov/violenceprevention/suicide/riskprotectivefactors.html
Warning Signs in Children:
• Changes in baseline behaviors, such as sleeping, eating, socializing with family and friends
• Psychosomatic symptoms, such as headaches, stomachaches, unexplained aches and pains
• Drop in academic performance• Decreased interaction with teachers and children at school• Lack of interest in school• Refusal to go to school• Loss of interest in daily activities, such as sports or extracurricular activities
https://www.psycom.net/children-and-suicide

Warning Signs in Children:
• Preoccupation with death, such as frequent questions or looking up ways to die• Statements about what would happen if the child dies (“You won’t miss me”)
(“I won’t bother you anymore”)• Statements of hopelessness• Giving away favorite possessions or telling who should get favorite possessions• Writing or drawing about death or suicide• Significant changes in mood
https://www.psycom.net/children-and-suicide

CDC Protective Factors for SuicideProtective factors buffer individuals from suicidal thoughts and behavior. To date, protective factors have not been studied as extensively or rigorously as risk factors. Identifying and understanding protective factors are, however,
equally as important as researching risk factors.• Effective clinical care for mental, physical, and substance abuse disorders• Easy access to a variety of clinical interventions and support for help seeking• Family and community support (connectedness)• Support from ongoing medical and mental health care relationships• Skills in problem solving, conflict resolution, and nonviolent ways of handling disputes• Cultural and religious beliefs that discourage suicide/support instincts for self-preservation

Preventing Suicide
Strategy Approach
Strengthen economic supports •Strengthen household financial security•Housing stabilization policies
Strengthen access and delivery of suicide care
•Coverage of mental health conditions in health insurance policies•Reduce provider shortages in under-served areas•Safer suicide care through systems change
Create protective environments
•Reduce access to lethal means among persons at risk of suicide•Organizational policies and culture•Community-based policies to reduce excessive alcohol use
Promote connectedness •Peer norm programs•Community engagement activities
Teach coping and problem-solving skills
•Social-emotional learning programs•Parenting skill and family relationship programs
Identify and support people at risk
•Gatekeeper training•Crisis intervention•Treatment for people at risk of suicide•Treatment to prevent re-attempts
Lessen harms and prevent future risk
•Postvention•Safe reporting and messaging about suicide
https://www.cdc.gov/violenceprevention/suicide/prevention.html

https://decisionsindentistry.com/article/identifying-risk-factors-suicide/
Use of a health history review:• Presence of history of depression
• Sadness• Loss of interest or pleasure in usual activities• Changes in appetite (increased or decreased)• Weight change• Disturbed sleep (insomnia or hypersomnia)• Psychomotor disturbances• Fatigue or loss of energy• Feelings of guilt or self-blame• Decreased ability to concentrate or make
decisions• Thinking about or planning suicide or suicidal
behavior

https://decisionsindentistry.com/article/identifying-risk-factors-suicide/https://afsp.org/about-suicide/suicide-statistics/
Use of a health history review:
• Presence of other mental health disorders• Presence of alcohol abuse• Presence of chronic pain• Lack of social support• Previous suicide attempt• Family history of suicide• Family history of violence• Access to guns• Medical illness

Suicide Screening Tools
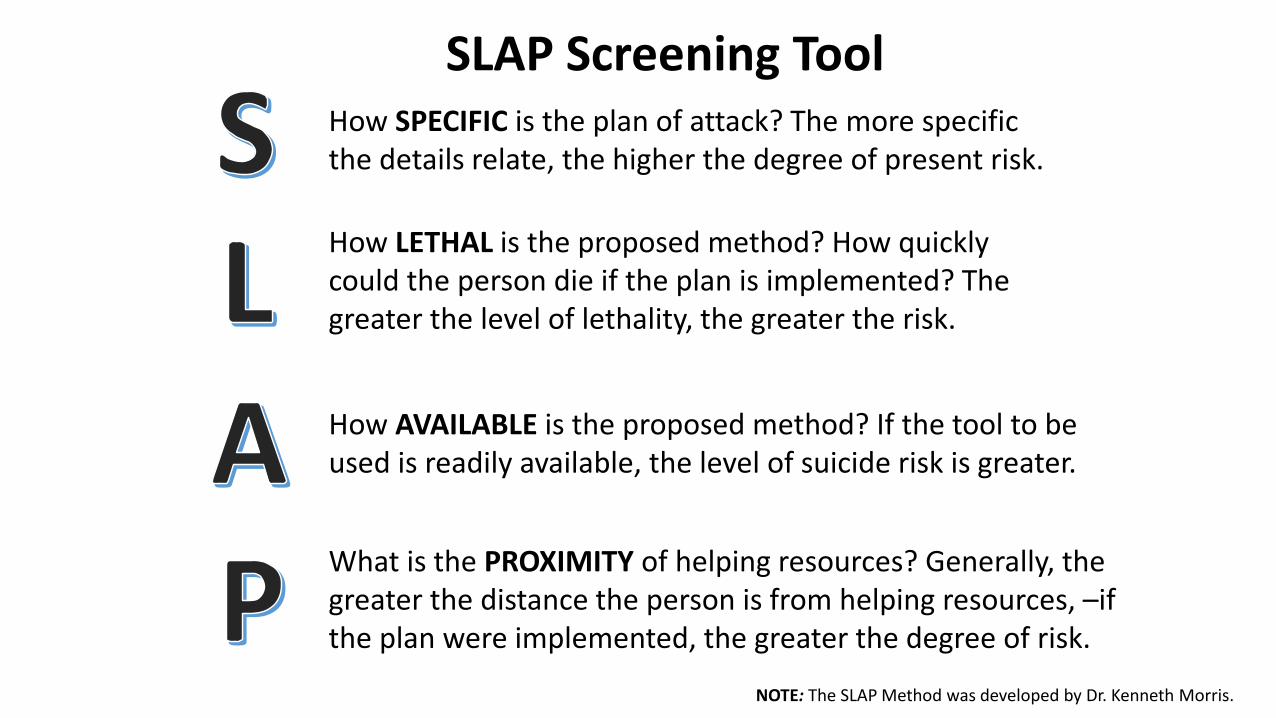
SLAP Screening ToolHow SPECIFIC is the plan of attack? The more specific the details relate, the higher the degree of present risk.
How LETHAL is the proposed method? How quickly could the person die if the plan is implemented? The greater the level of lethality, the greater the risk.
How AVAILABLE is the proposed method? If the tool to be used is readily available, the level of suicide risk is greater.
What is the PROXIMITY of helping resources? Generally, the greater the distance the person is from helping resources, –if the plan were implemented, the greater the degree of risk.
NOTE: The SLAP Method was developed by Dr. Kenneth Morris.
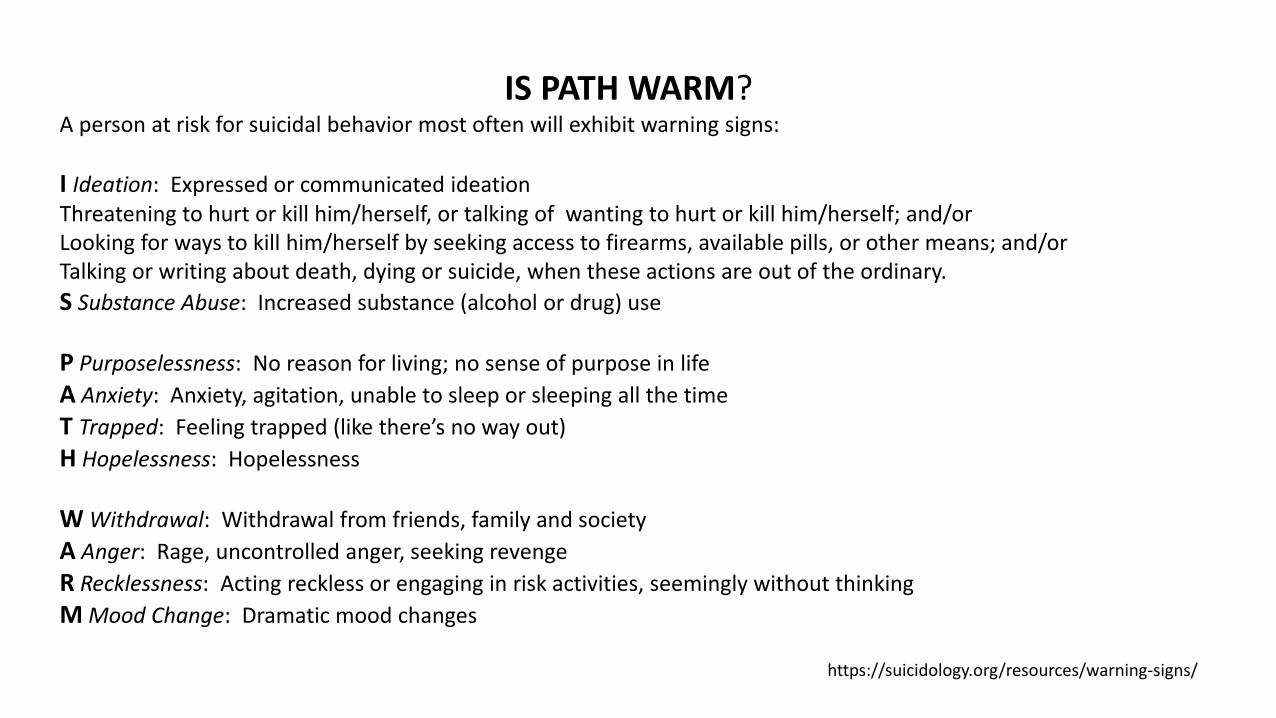
IS PATH WARM?A person at risk for suicidal behavior most often will exhibit warning signs:
I Ideation: Expressed or communicated ideationThreatening to hurt or kill him/herself, or talking of wanting to hurt or kill him/herself; and/orLooking for ways to kill him/herself by seeking access to firearms, available pills, or other means; and/orTalking or writing about death, dying or suicide, when these actions are out of the ordinary.S Substance Abuse: Increased substance (alcohol or drug) use
P Purposelessness: No reason for living; no sense of purpose in lifeA Anxiety: Anxiety, agitation, unable to sleep or sleeping all the timeT Trapped: Feeling trapped (like there’s no way out)H Hopelessness: Hopelessness
W Withdrawal: Withdrawal from friends, family and societyA Anger: Rage, uncontrolled anger, seeking revengeR Recklessness: Acting reckless or engaging in risk activities, seemingly without thinkingM Mood Change: Dramatic mood changes
https://suicidology.org/resources/warning-signs/

Ask the Patient:
1. In the past few weeks, have you wished you were dead? YES NO2. In the past few weeks, have you felt that you or your family
would be better off if you were dead? YES NO3. In the past week, have you had thoughts of killing yourself? YES NO4. Have you ever tried to kill yourself?
If yes, how?If yes, when?
(If the patient answers YES to any of the above questions, ask the following acuity question:
5. Are you having thoughts of killing yourself right now? YES NOIf yes, please describe.

Next Steps:If person answers “NO” to all questions 1-4, the screening is complete (not necessary to ask question #5). No intervention is necessary. (Note: clinical judgment can always override a negative screen.)
If patient answers “YES” to any questions 1-4, or refuses to answer, they are considered a Positive Screen. Ask question #5 to access acuity.
□ Yes to question #5 = acute positive screen (imminent risk identified)• Patient requires a STAT safety/full mental health evaluation.
Patient cannot leave until evaluated for safety. • Keep patient in sight. Remove all dangerous objects from room. Alert physician or clinician
responsible for patient’s care.□ No to question #5 = non-acute positive screen (potential risk identified)
• Patient requires a brief suicide safety assessment to determine if a full mental health evaluation is needed. Patient cannot leave until evaluated for safety.
• Alert physician or clinician responsible for patient’s care.
Provide resources for all patients: • 24/7 National Suicide Prevention Lifelife: 1-800-273-TALK (8255). En Español: 1-888-628-9454• 24/7 Crisis Text Line: Text “HOME” to 741-741.

https://www.integration.samhsa.gov/clinical-practice/screening-tools#suicide

https://www.integration.samhsa.gov/clinical-practice/screening-tools#suicide

Be sure to document any warning signs reported or observed and be prepared to make documentation available to mental health referrals, as needed.

Identifying an
appropriate referral
• 24/7 National Suicide Prevention Lifelife: 1-800-273-TALK (8255). (Use that number and press "1" to reach the Veterans Crisis Line.)En Español: 1-888-628-9454
• 24/7 Crisis Text Line: Text “HOME” to 741-741.
• Suicide Prevention Resource Centerwww.sprc.org
• National Institute of Mental Healthwww.nimh.nih.org
• Substance Abuse and Mental Health Services Administrationwww.samhsa.gov

Create Local Resource ListNearest Hospital Emergency Room• King Mental Health Services
• 206-263-8997• 1-800-790-8049• https://kingcounty.gov/depts/community-human-services/mental-
health-substance-abuse/services/mental-health.aspx• Snohomish County Community Mental Health
• 2-1-1• Care Crisis Line 1-800-584-3578 (Triage Center, Involuntary Mental
Health, Mental Health Voluntary outreach team and outpatient treatment services)
• https://snohomishcountywa.gov/427/Community-Mental-Health
National Resources Related to Suicide Prevention• A Voice at the Table: vimeo.com/92330799• American Association of Suicidology: suicidology.org• preventyouthsuicide.org• The Centers for Disease Control: cdc.gov• The Coalition to Stop Gun Violence: csgv.org/issues/preventing-suicide• Live Through This: livethroughthis.org/the-project• National Action Alliance for Suicide Prevention: actionallianceforsuicideprevention.org• Zero Suicide Toolkit• The Way Forward • National Council for Behavioral Health: thenationalcouncil.org• National Council for Suicide Prevention: ncsponline.org• National Institute of Mental Health: nimh.nih.gov• National Suicide Prevention Lifeline: suicidepreventionlifeline.org• The Safety Plan Intervention: suicidesafetyplan.com• Substance Abuse Mental Health Services Administration: samhsa.gov• Suicide Prevention Resource Center: sprc.org

Connecting a client or patient to a referral –maintaining patient safety

Resources by Dr. Gregory Jantz
www.aplaceofhope.com www.drgregoryjantz.com


















