Suboxone and the Opioid Epidemic · 9/10/2017 · (otherwise known as Narcan) which is a pure...
22
1| Page Suboxone and the Opioid Epidemic Jon Helander, Ph.D. September 10, 2017 Altum Research Revised Background Opium has been used for thousands of years, and extracts concentrated in morphine have been written about since the 1500’s. It was not until the early 1800’s when the morphine extract was isolated in high purity by Friedrich Sertürner, who immediately demonstrated the danger associated with opiates when used in high concentration. Sertürner injected four people, three boys and himself, all of which nearly died (Dahan, Aarts, and Smith 2010). Still, Sertürner was the first to market morphine, and ironically, did so for treatment of alcohol addiction. Today, opioids are typically prescribed in hospital care and are synthetic or semi-synthetic derivatives of morphine including heroin, and account for a significant percentage of addictions worldwide. The United States is experiencing an opioid epidemic caused by addictions, toxicity, misprescribing and overprescribing of opioid related treatments for pain management. In the U.S., the lead cause of accidental death is drug overdoses which accounted for approximately 55,403 deaths in 2015. Of those, 36% or 20,101 were due to prescription pain relievers. Heroin, by comparison, accounted for fewer deaths at 23.5% or 12,990 in the same year (Source: CDC Health Statistics, Figure 1A) Strikingly, drug overdose related deaths are increasing at an alarming rate. From 2000 to 2015, deaths from opioid overdoses increased by approximately 200% which includes prescription and illicit use (Figure 1B). These deaths have increased with increasing numbers of prescriptions being written; in 2012 there were over 250 million scripts written which is enough for every adult in the US to have an opiate pill bottle (CDC 2014). Further, the number of reported addiction cases and frequency of use has also dramatically risen (Han et al. 2015). These unfortunate trends are all in the face of the introduction of Suboxone, a mixture of two synthetic opioids, that was marketed and sold as a potential treatment to mitigate this very problem. However, as will be outlined here, the label of Suboxone and the respective marketing have not alleviated the opioid epidemic, and has may have made it substantially worse.
Transcript of Suboxone and the Opioid Epidemic · 9/10/2017 · (otherwise known as Narcan) which is a pure...

1|Page
Suboxone and the Opioid Epidemic JonHelander,Ph.D. September10,2017AltumResearchRevised
Background
Opiumhasbeenusedforthousandsofyears,andextractsconcentratedinmorphinehavebeenwrittenaboutsincethe1500’s.Itwasnotuntiltheearly1800’swhenthemorphineextractwas isolatedinhighpuritybyFriedrichSertürner,whoimmediatelydemonstratedthedangerassociatedwithopiateswhenusedinhighconcentration.Sertürnerinjectedfourpeople,threeboysandhimself,allofwhichnearlydied(Dahan,Aarts,andSmith2010).Still,Sertürnerwasthefirsttomarketmorphine,andironically,didsofortreatmentofalcoholaddiction.Today,opioidsare typically prescribed in hospital care and are synthetic or semi-synthetic derivatives ofmorphineincludingheroin,andaccountforasignificantpercentageofaddictionsworldwide.
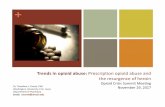
The United States is experiencing an opioid epidemic caused by addictions, toxicity,misprescribingandoverprescribingofopioid relatedtreatments forpainmanagement. In theU.S.,theleadcauseofaccidentaldeathisdrugoverdoseswhichaccountedforapproximately55,403deathsin2015.Ofthose,36%or20,101wereduetoprescriptionpainrelievers.Heroin,bycomparison,accountedforfewerdeathsat23.5%or12,990inthesameyear(Source:CDCHealthStatistics,Figure1A)
Strikingly,drugoverdoserelateddeathsareincreasingatanalarmingrate.From2000to2015, deaths from opioid overdoses increased by approximately 200% which includesprescriptionandillicituse(Figure1B).Thesedeathshaveincreasedwithincreasingnumbersofprescriptionsbeingwritten;in2012therewereover250millionscriptswrittenwhichisenoughforeveryadultintheUStohaveanopiatepillbottle(CDC2014).Further,thenumberofreportedaddiction cases and frequency of use has also dramatically risen (Han et al. 2015). TheseunfortunatetrendsareallinthefaceoftheintroductionofSuboxone,amixtureoftwosyntheticopioids, thatwasmarketed and sold as a potential treatment tomitigate this very problem.However,aswillbeoutlinedhere,thelabelofSuboxoneandtherespectivemarketinghavenotalleviatedtheopioidepidemic,andhasmayhavemadeitsubstantiallyworse.

2|Page
FIGURE1:U.S.DRUGOVERDOSEDEATHS
PanelA:55,403drugoverdosedeathsintheU.S.fromprescription,heroinorotheragentsin2015.PanelB:IncreaseindrugoverdosedeathsandopioidrelateddeathsintheU.S.fortheperiod2000to2014.
Thelethalityofopioiduseusuallystemsfromrespiratorydepression(Dahanetal.2001;Romberg et al. 2003). Reversal of this negative side effect can be quickly overcome byadministration of antagonists for the opioid receptors (Goodman, Le Bourdonnec, and Dolle2007).Whileadministrationofanopioidantagonistsuchasnaloxonecansavelives,thesituationmust be closely monitored due to its short half life. The short half life allows for an acutealleviationofrespiratorydepression,butaninitialheavydoseofopiatescanstillputthepatientatriskagain,evenwithoutsubsequentdosages(Sarton,Teppema,andDahan2008).
Inthisreport,wewilldiscussSuboxone,achemicalcombinationofopioidanalogs,andpresentdatathatsupportsourconclusionswhichinclude:
(a)Suboxone’scurrentlabeldoesnotadequatelydisclosure itshighlyaddictivenatureandcertainotherrisks;and,
(b)Suboxone’smarketingdoesnotadequatelytraindoctors(andpatients)astoproperdosing levels and certain other dangers, which has caused misprescriptions andoverprescriptions.
Furtherwewilldiscusscircumstancesunderwhich,webelieve,Suboxoneisdetrimentaltothetreatmentofopioidaddiction.GiventheriseofopioidrelateddeathssinceSuboxone’sapprovalin2002,webelievethereisnowadequatedatatosupporttheseconclusions.

3|Page
SuboxoneIntroducedin2002
Inaseeminglybeneficialattempttocombatthisissue,Suboxone®,atradenameforthemixtureoftwoopioidderivatives,buprenorphineandnaloxone,wasapprovedbytheFDAin2002 for a treatment for opioid addiction. At that time, buprenorphine and SuboxoneweremanufacturedandmarketedbytheReckittBenckiserGroupplc(LSE:RB),aBritishmultinationalconsumergoodscompanythatmarketsbrandssuchasCalgon,LysolandFrench’smustard.In2010,theFDAapprovedapartnershipbetweenReckittBenckiserandMonosolRX,thedeveloperofPharmFilm-whichenablesthedeliveryofdrugsthroughadissolvablefilmplacedunderthetongue,tomarketaSuboxonesublingualfilmproducttopatients.
However, in December 2014, primarily due to mounting concerns about Suboxone’spotential liability from consumer or government litigation, Reckitt Benckiser spun off itspharmaceuticaldivisionwhichcontainedSuboxone,itsprimaryrevenuesource,andlistedthespinoffontheLondonStockExchange(LSE)underthenameIndiviorplc(LSE:INDV).
Buprenorphineisasemi-syntheticderivativeofthenaturallyoccurringopiatethebainewhichcanbefoundintheopiumpoppy(NymanandHall1976).Theotherconstituentisnaloxone(otherwiseknownasNarcan)whichisapureopioidantagonistandcanblockopioidanalgesiceffects(Sawynok,Pinsky,andLaBella2017).
Whilenaloxoneiseffectiveinthetreatmentofanacuteoverdoseofopioids,ithaslittlebenefitaloneinaddictiontreatment.Naloxoneisgenerallyregardedasarescuemedicationonly(vanDorp,Yassen,andDahan2007).Thecombinationofanactiveopioid(buprenorphine)andan opioid antagonist1 (naloxone) together, has thus been touted as a treatment for opioidaddiction.
WhileSuboxoneandbuprenorphinehaveshownbenefitsinsomeclinicaltrials,manyofthesebenefits areonly attributed to reduced “craving” foropiatesor retention in treatmentprograms.However,asoutlined inastudydonebyFudalaetal., for themost importantandrelevantfactor,reducingillicitdruguse,Suboxonedoesnotshowimprovement(Fudalaetal.2003).
Asoutlinedbelow,manytrialsutilizingbuprenorphineorSuboxonefailtoreduceopioiduse and consequently,may simply prolong, complicate, or even worsen the user’s opioidaddiction.
As such, we believe that the labeling for Suboxone does not adequately disclose its
1 Agonistsdefinedasactivatorsofreceptors.Antagonistsdefinedasdeactivatorsofreceptors.Antagonistscanblocktheeffectsofagonistssuchasopioids.

4|Page
dangersandeffectiveness.Further,webelievethatSuboxone’sadvertisingandmarketinghasfailedtoadequately
traindoctorsasto:I. ProperdiagnosismethodsII. Dosinglevels,whicharecouldoftenbeover-prescribedtopatientIII. Taperinganddiscontinuationregimen,whichisarguablythemostrelevantresult
foraddictiontreatment.
Note:TheissueswithSuboxonedescribedabovearesimilartothoseraisedbytheFDAin2007initslitigationagainstPurduePharma,aprivatelyheldcompanybasedinStamford,CT,andthemakersofOxyContin -anopioid-basedpainmedication.TheFDA’scaseresulted inasettlementconsistingof(a)a$600millionfinepaidbyPurduePharma,(b)theresignationofitstop 3 executives, including its CEO and (c) $34 million in fines paid personally by its top 3executives.AccordingtoaNYTimesarticle,the judgesoughtto imposejailtimeforthetop3executives,butwasunabletoincludethisinthesettlementterms.
In2015,ForbespublisheditslistofwealthiestfamiliesintheU.S.andincludedforthefirsttime,the100%ownersofPurduePharma,94yearoldRaymondandBeverlySacklerofGreenwich,CTwhosepersonalnetworthwasestimatedat$14billion.
HowdidtheSacklersbuildthe16thlargestfortuneintheU.S.edgingoutstoriedfamiliesliketheBusches,MellonsandRockefellers?Theshortanswerisbymakingthemostpopularandcontroversialopioidofthe21stcentury–OxyContin.ForbesestimatesthatPurduePharma’sOxyContinhasgeneratedover$35billioninrevenuethrough2015.Suboxone’sWeakData
ThestatisticspresentedinthisreportcoveroveradecadeofdatasincetheapprovalofSuboxone,adrugthathasrepresenteditselfasatreatmentforopioidrelatedaddictions.Tothebestofourknowledge,studiescommissionedbySuboxone’smanufacturer,ReckittBenckiser(orlater, by its spin off company, Indivior), have generally presented data from relatively shortperiodsoftime.
Oneofthelargestanalysesofmultiplestudiesconductedonopioid-addictiontreatmentsconsisted of over 5,400 participants across 31 trials. The analysis concluded that whilebuprenorphine used for the treatment of opioid addictionwas able to retain participants intreatment programs better than placebo,buprenorphine did not lower other opioid use asdeterminedbyurinalysis(Matticketal.1996).

5|Page
Inmanystudieswhereurineanalysiswasdeemedtoshownegativeresults,itshouldbenotedthatthesemi-syntheticorsynthetic2opioidswerenotscreened.Forinstance,ajournalclaiming significance in diminished opiate use with Suboxone via urinalysis tested only foropiates,notopioidssuchasoxycodone,fentanyl,ormeperidine(Fudalaetal.2003).Asimilarstudy, “didnotalways includea test foroxycodone” (Finch,Kamien,andAmass2007). Sincetheseopioidsaresomeofthemostwidelyusedillicitpainkillers,itisinconceivablewebelieve,thatsuchstudiescanclaimefficacy-ifitdoesnottestforthem.
Another study demonstrated a significance in keeping patients in treatment fromrelapsingat154 in-patientdays,butbuprenorphinehadonlya10%relapse-freerate,whichquestionsitseffectivenessoverthelongerterm(Schottenfeld,Chawarski,andMazlan2008).
Similarly,astudymeanttoassessthepositivebenefitsofSuboxoneormethadonefortreatmentofopioidusedeterminedthattherewasnodifferenceamongplacebo,methadone,or Suboxone for positive (finding employment, documented social/family improvement) ornegative(missed/positiveurinalysis,violationoftermsofprobation)events(Cradicketal.2014).
Inperhapsthemostobjectiveandreliablestudiesdonepost-Suboxone’sapproval,theNIH funded two studies (here and here) thatwere deemed “promising”. This “success”waslargelyattributedtoloweredopioiduseduringtreatmentinconjunctionwithgreatertreatmentretention.However,oncloserexamination,thesuccessisnotsoclearcut:
“ParticipantsassignedtoextendedSuboxonetreatmentweremuchlesslikelytoprovideopioid-positiveurinesamplesatweeks4and8,butnotatweek12(whenthedosehadtaperedoff)thanthoseinthestandarddetoxificationgroup.Follow-upevaluationsatmonths6,9and12showedincreasedratesofopioiduseinbothgroupscomparedtotheendofthetreatmentperiod”
Thisshouldbealarming,as thesearetheresults fromtheNIH,oneof the largestandforemost research institutions worldwide. This decline in efficacy after treatment ends ishighlightedstronglywhenlookingattheactualnumbers:
“Results showed that approximately 49 percent of participants reduced prescriptionpainkillerabuseduringextended(atleast12-week)Suboxonetreatment.Thissuccessratedroppedto8.6percentonceSuboxonewasdiscontinued.”
2Semi-syntheticreferstoopioidsthatarederivedfromtheirnaturalsource,butmodifiedwithsyntheticchemistry,such as oxycodone or heroin. Synthetic refers to opioids that are not derived from a natural source, and fullysynthesizedinthelab,suchasFentanyl.

6|Page
If the NIH has a problem finding efficacy, and demonstrates a clearweakness to thesuccess of the treatment after retention is no longer obligated, the perspective to supportSuboxoneasaneffectivetreatmentoptionforopioidaddictionissignificantlyweakened.
Whilethereductionistreasoningbehindtheuseofanopioidandanopioid-antagonistforan opioid addiction mitigation strategy is understandable, we believe it requires additionalextensive long-termstudies to truly identify itspotential impact indrugaddiction treatment.Thesestudiesshould includeassessmentforallopioiduse,treatment-programretention,andmost importantly, the ability toeventually stop all opioid use (including buprenorphine andnaloxone).Thecurrentstateofresearchonthesubject,inouropinion,indicatesthattheopioidaddictionproblemthatSuboxonerepresentsitissolving,doesinfact,continuetoexist-evenwhencombiningSuboxonewithpatienttreatmentprograms.
Webelievethemostlogicaltreatmentforopioidaddictionisnotanotheropioidsuchasbuprenorphine-whichisamerelyatransferofoneopioidrelatedaddictiontoanother.
Anoversimplifiedanalogyofthemisplacedlogicforprovidingbuprenorphinetoopioidaddicts,wouldbetoprovideshotsofJackDaniel’swhiskeyasatreatmenttoalcoholics.Further,byonly screening foropiates (andnotopioids)during treatment,and then,claima“negativeurinesample”-isanalogoustoscreeningalcoholicsforbeerconsumption,butforgettingtotestforliquor.
SuboxoneAntagonismandWithdrawals
Tounderstandwhywebelieve that Suboxone’swithdrawal symptoms are similar toheroin, ithelpstounderstand(i)theroleoftheopioidreceptorsinthehumanbrain,(ii)howvarious agents - buprenorphine, naloxone, morphine, and heroin affect the brain’s opioidreceptors,and(iii)theresultingeffectsonopioidaddicts.
Thereare3majoropioidreceptorsinthebrainthatareresponsibleforthetherapeuticeffectsofcommonlyusedopioids,μ(“mu”),κ(“kappa”),andδ(“delta”).
Below is a simplified table outlining the pharmacodynamic3 properties of opioids -buprenorphine,naloxone,morphine,andheroin,andtheireffectsonthe3opioidreceptorsin
3 Pharmacodynamics is thestudyof thebiochemicalandphysiologiceffectsofdrugs,especiallypharmaceuticaldrugs. The majority of drugs either (a) mimic or inhibit normal physiological/biochemical processes or inhibitpathologicalprocessesinanimalsor(b)inhibitvitalprocessesofendo-orectoparasitesandmicrobialorganisms.

7|Page
thehumanbrain.
Theterm“agonist”indicatesthatthedrugactivatesthereceptor’seffects,andtheterm“antagonist”means it inactives,orblocks, the receptor’s response. For thepurposesof thisreport,apartialagonistmeansitpartiallyactivatesthereceptor.
FIGURE2:OPIOIDACTIVATIONSONTHEBRAIN’S3OPIOIDRECEPTORS
OpioidReceptor Effects Bupenorphine Naloxone Morphine Heroin
μEuphoria
AnalgesiaPartialAgonist Antagonist Agonist Agonist
κDepression
SedationAntagonist Antagonist Agonist Agonist
δAnalgesia
AntidepressantAntagonist Antagonist Agonist Agonist
Ingeneral,theμ-(“mu”)receptorleadstotheeuphoriathatopioidaddictsseek.
As can be seen above, both morphine and heroin activate the μ receptor, whilebuprenorphineonlypartiallyactivates.Whilenotexceptionallyimportant,buprenorphinedoesshowsomeabilitytobeaninverseagonistwhenusedinconjunctionofopioids(Wang,Sun,andSadee2007).
Buprenorphine’spartialagonistactivityonμandantagonistactivityonκandδwasthebasisfortheviewthatitmayinhibitthebehaviorofanopioidaddict.Howeverthisalonedoesnotsupportaconclusionforitsuseinopioidaddiction.
RegardingNaloxone,itsoverdosetreatmenteffectsareduetoitsantagonistactivityonall the opioid receptors shown in Figure 2. Naloxone is able to bind very effectively to thereceptors which results in a displacement and essential inactivation of any opioid use. This

8|Page
antagonisticactivitycansavethelifeofsomeonewhooverdosesbydisplacing theoverdosedopioid,andhenceit’sinclusioninSuboxone.
However,anessentialaspecttoSuboxone’s inadequacyasatruetreatmentforopioidaddictionisthatitcanhavewithdrawalsymptomssimilartothatofheroin(Blumetal.2013).ThefactthatSuboxonecancausewithdrawalsrequiresittoactinasimilarmannerandprovidesimilareffectstotheopioidsitclaimstoprovidetreatmentfor!
The fact thatwithdrawal symptomsexistwith Suboxonediscontinuation is supportiveevidence that Suboxone displays serious addictive properties. This further complicatesSuboxoneasatreatmentsinceoneofthemostbeneficialaspectsSuboxoneclaimsinmostofitssponsored studies -was its increase in treatment program retention.However, this “successmarker”doesnotadequately take intoaccount (i) thedifficulties forpatients tostopuseofSuboxone,and(ii)thefactthatbuprenorphineitselfactsasanopioid.Givingpatientsanopioidthatelicitsopiate-likeeffects,andthenclaimingsuccesswhenpatientsuselessopioidsseemstobearedundantmeasureofefficacy.
Again,thelargestudycitedaboveshowedmoderateevidencethatwhileSuboxonewasabletokeepparticipantsintreatmentprogramslongerthanplacebo,urineanalysesindicatedthat opioid usewas similar between Suboxone users and placecbo. This could be partiallyexplained by the fact that buprenorphine does not directly treat addiction, but rather givespatientsaweakopioid“high”.
SuboxoneDangers
Buprenorphinealonecancauseopioideffectssuchaseuphoria,sedation,andanalgesia(Walshetal.1994).Thismaybeeffectiveinloweringthedependenceissuesofanopioidaddict,as the treatment partially fills the drug-seeking behavior, but the underlying neurologicalmechanismsofaddictionarenot treated inaneffectivemanner, and thepatient is stillusingopioids.
Based on the availability of “Suboxone addiction” treatment centers through internetsearches,andtheplethoraofforumswithpostsdealingwithdifficultiesinSuboxoneaddiction,itseemscommonthatpatientsfindthemselvesaddictedtoSuboxoneitself.Clearly,Suboxoneisnotanidealcandidateforaddictiontreatmentalone,asmanypatientsindicatetheiraddictionsimplychangesfromtheoriginalpainmedicationtotheSuboxoneaddictiontreatment.

9|Page
FIGURE3:CHEMICALSTRUCTURESOFBUPRENORPHINE,MORPHINE,ANDNALOXONE
OneaspectofSuboxonethatisdeceivinglyclaimedasbeneficialisthe“ceiling”effectofthe“high”.Thisceilingeffectcausesalimittothe“high”ausercanexperiencewithSuboxone.Therefore,patientswill findthat increasingtheSuboxonedoseactuallygeneratesdiminishingreturnsinitseuphoriceffects.
While seemingly beneficial, this ceiling hides a dangerous effect of the antagonisticnatureofthenaloxoneandbuprenorphineconstituents.ByincreasingtheSuboxonedose,thepatientactuallydecreasessensitivitytoallopioidswhileonSuboxone(Bowdle1998).
TheconcomitantuseofSuboxoneandanyillicitopioidsrequiresthepatienttoincreasetheirillicitdoseinordertoachievethesamelevelofeuphoriathatthepatientwasaccustomedtobeforetreatmentbegan.ThissimultaneoususeofSuboxoneandillicitopioidscouldcertainlyresultindosesthatwerepreviouslylethal,butduetoSuboxone’santagonisticeffects,arenownon-lethal.
The dangermay then be amplified if the patient stops Suboxone treatment for anyreason,butcontinuesusingotheropioids-astheopioiddosethresholdrequiredwithSuboxonemaynowprovelethalwithouttheSuboxonetreatment.
Thus,webelievethatSuboxonepatientsarenotproperlyinformedofthisdangerasitisnotdisclosedadequatelyonSuboxone’slabel.
Further,prescribingdirectionstodoctorswebelieve, lackanadequateexplanationofthisandotherrisksofSuboxone.
SuboxoneLabeling
Suboxonehasrepresented itselfasa treatment foropioidaddiction.ReckittBenckiser

10|Page
(andtoday,itsspinoff,Indivior)wasthemanufacturerofbuprenorphineandhasfundedmanyofthestudiesthatshowsupportforSuboxone.
However,acarefulreviewofrelevantscientificliteraturedemonstratesampleevidencethatwhileSuboxonemayshowsomebenefitsinopioidaddictionrecoveryovertheshortterm,thereissubstantial informationsupportingSuboxone’snegativeeffectswhichappearstobeeitherignoredorunknownbytheFDA.
FIGURE4:INCREASEINEMERGENCYROOMVISITSRESULTINGFROMSUBOXONE
Figure4source
TheFDAlabelsforSuboxonecanbeviewedhereandhereandhere.Astoundingly,verylittleonSuboxone’slabelspecificallyaddresses“addiction”andthedangers(whichincludetheriskofdeath)isminimallycovered.
Buprenorphine represents itself as a schedule III drug, indicating it has less abusepotentialthanmethadone(ScheduleII, isalsousedforopioidaddictiontreatment).However,buprenorphine’s label discloses the following dangerwarnings (which do not appear on theSuboxonelabels).
▪ Chronicadministrationproducesopioid-typephysicaldependence ▪ Abrupt discontinuation or rapid dose taper may result in opioid withdrawal
syndrome

11|Page
▪ Neonatalwithdrawalhasbeenreportedfollowinguseofbuprenorphinebythemotherduringpregnancy.
▪ A marked and intense withdrawal symptom is highly likely to occur withparenteral misuse of SUBOXONE sublingual film by individuals physicallydependent on full opioid agonists or by sublingual administration before theagonisteffectsofotheropioidshavesubsided.
We believe that buprenorphine’s opioid-type physical dependence, opioid-likewithdrawal,andneonatalwithdrawalsymptomsindicatethatReckittBenckiser(Indivior)havefalselyrepresentsbuprenorphineasaScheduleIIIdrug.Webelievebuprenorphineshouldbeclassified as a Schedule II drug, along with the other opioids such as morphine, codeine,hydrocodone,oxycodone,etc.
Further, thebuprenorphine label indicates that “mis-use” of buprenorphine leads toaddictivebehavior.However,“mis-use”isnotanaccuratedisclosuretermwebelieve-astheaddictivenatureofbuprenorphinehasclearlybeendocumented inpatientsunder treatmentwithprescribeddoses.
Additionally,ascitedearlier,buprenorphinehasa‘ceiling’doseeffectwhichwouldmakeSuboxonetreatmentoflittlebenefit.ThissupportsourbeliefthatSuboxoneactuallypromotesabuseandgreateraddiction.
Suboxone’s prescribing information is available online to view here, and is brieflyoutlinedbelow.
● Day1Onlyuponmoderatewithdrawalsymptomsshouldthefirstdosebetaken.
○ 8mg/2mgSuboxonesublingualfilmtotal.○ Startwithaninitialdoseof2mg/0.5mgor4mg/1mgbuprenorphine/naloxone.○ Titrateupwards in2or4mg incrementsofbuprenorphine,at2-hour intervals,
undersupervision,tototaldose
● Day2Singledailydoseofupto16mg/4mgSuboxone
● Day3+Maintenance:Incrementsof2mg/0.5mgor4mg/1mgbuprenorphine/naloxoneuntilwithdrawalceases,16mg/4mgperdayisrecommended
● Stopping&Tapering:Taperdosetoavoidwithdrawalsymptoms

12|Page
We note that Suboxone’s prescribing instructions are very general. To illustrate,
Suboxone does not disclose when to begin the tapering process. Further, there are noinstructionsastohowtoexecutethetaperingprocess.Taperingcouldbethemostimportantstepforsuccessfuldiscontinuationofopioiduse,howeverSuboxone’slabelseemstoignorethisaspect of treatment.How, then, can an opioid-containing prescription drug be used for thetreatmentofopioid-basedaddiction, if there isno instructionsonhoworwhentodiscontinueuse?
As such, it is left to the patient to make important (and life threatening) taperingdecisionswhenusingSuboxone.WebelievesupportsouropinionthatSuboxone’strainingofdoctorsiswhollyinadequateandhasledtooverdosedeaths.
SuboxoneInvestigations,LitigationandContingentLiabilities
In connection with Suboxone, there are various pending investigations and litigationagainst Indivior (or Reckitt Benckiser) which has produced the following contingent liabilityreportsasofNovember2016.
Inouropinion,there is inadequatefinancialdisclosuresto investorsbypublicly listedReckittBenckiserand Indiviorastopotentialcontingent liabilities inconnectionwithpendingandexpectedlitigationwithSuboxone.
Webelievetheremaybematerialcontingentliabilitiestothesecompaniesinconnectionwith Suboxone and that investor protection agencies such as state attorneys general shouldinvestigatefurther.Thesearethecurrentcontingentliabilitiesthataredisclosedbythecompany.
DepartmentofJusticeInvestigation
▪ AfederalcriminalgrandjuryinvestigationofIndiviorinitiatedinDecember2013iscontinuing,andincludesmarketingandpromotionpractices,paediatricsafetyclaims, and overprescribing of medication by certain physicians. The U.S.Attorney's Office for theWestern District of Virginia has served a number ofsubpoenasrelatingtoSUBOXONE®Film,SUBOXONE®Tablet,SUBUTEX®Tablet,buprenorphineandourcompetitors,amongotherissues.Weareintheprocessofrespondingbyproducingdocumentsandotherinformationinconnectionwiththis on-going investigation, and in preliminary discussion about a possibleresolution of the investigation. We are cooperating fully with the relevantagenciesandprosecutorsandwillcontinuetodoso.

13|Page
FTCInvestigationandAntitrustLitigation
▪ The Judge overseeing the legal privilege dispute in the FTC investigation hasappointedaSpecialMaster(anindependentexternallawyer)toinvestigatetheclaimsoflegalprivilegeandprovidearecommendationtotheCourtonhowthedocuments at issue should be treated. An initial report and recommendationrelating to the first tranche of privileged documents reviewed by the SpecialMasterwasfinalizedinApril2016andadoptedbytheCourtonAugust1st,2016.PursuanttothisreportandtheCourt’sorder,Indiviorproducedcertainadditionaldocuments.A second trancheofdocuments remainsunder review. Followingthatreview,theCourt’sdecisionthenmaybesubjecttoappealbyeitherparty.
▪ FactdiscoveryiscontinuingintheantitrustclassactionlitigationdescribedonourAnnualReport (“ClassActionLitigation”).Plaintiffsallege,amongother things,that Indivior violated federal and state antitrust laws by attempting to delaygenericentryofalternativestoSUBOXONEtablets,andplaintiffsfurtherallegethat Indivior unlawfully acted to lower the market share of these genericproducts.
▪ Amneal Pharmaceuticals LLC, a manufacturer of generic buprenorphine /naloxonetablets,filedacomplaintagainsttheCompanyinDecember2015.ThiscasehasbeencoordinatedwiththeClassAction litigation.Amneal'scomplaintcontainsantitrustallegationssimilarinnaturetothosesetoutintheclassactioncomplaints,andAmnealhasalsoallegedviolationsoftheLanhamAct.
▪ OnSeptember22,2016,35statesandtheDistrictofColumbiafiledacomplaintagainst the Company in the samedistrictwhere the Class Action andAmneallitigation is pending. The States' complaint is similar to the other pendingcomplaints, andalleges violationsof stateand federal antitrust and consumerprotectionlaws.OnOctober25,2016,theCompanywasinformedthattheStatesplan to amend their complaint to add six additional states as plaintiffs. Thislawsuitrelatestotheinvestigationconductedbyvariousstates,asdiscussedinpreviousfilings.
▪ OnOctober12,2016,theCompanywasservedwithasubpoenaforrecordsfromthestateofConnecticutOfficeoftheAttorneyGeneralunderitsConnecticutcivilfalse claims act authority. The subpoena requests documents related to theCompany’s marketing and promotion of SUBOXONE® products and itsinteractions with a non-profit third party organization. The Company iscooperatinginthisinvestigation.

14|Page
ANDALitigation
▪ TherulingaftertrialagainstActavisandParinthelawsuitinvolvingtheOrangeBook-listedpatentsforSuboxone®FilmissuedonJune3rd,2016.Rulingfoundtheassertedclaimsofthe‘514patentvalidandinfringed;theassertedclaimsofthe‘150patentvalidbutnot infringed;and theassertedclaimsof the ‘832patentinvalid,butfoundthatcertainclaimswouldbeinfringediftheywerevalid.
▪ Basedontherulingastothe’514patent,ActavisandPararecurrentlyenjoinedfrom launchingagenericproduct.ParhasappealedandActavis isexpected toappealthisruling.ThegenericshavealsomovedtoreopenthejudgmentbasedonamorestringentclaimconstructionintheTevacase.Inlightofthemotionstoreopen,Par’s appealhasbeendeactivateduntil theDistrictCourt ruleson themotions, and the deadline for Actavis to file a notice of appeal has beenpostponed.
▪ Trial against Dr. Reddy’s, Actavis and Par in the lawsuits involving the processpatent(USPatentNo.8,900,497)scheduledforNovember16thand21st-23rd,2016.
▪ TrialagainstDr.Reddy’sinthelawsuitinvolvingtheOrangeBook-listedpatentsforSuboxone®Filmscheduled forNovember7th,16th ,and21st- -23rd,2016,withDr.Reddy’s30-monthstayofFDAapprovalonANDANo.20-5806expiringApril17th,2017.IndiviorbelievesDr.Reddy’s30-monthstayofFDAapprovalonANDANo.20-5299alsoexpiresonApril17th,2017,however,DrReddy’sdisputestheapplicabilityofthestaytothisANDA.
▪ TrialagainstAlvogeninthelawsuitinvolvingtheOrangeBook-listedpatentsandthe‘497processpatentforSuboxone®FilmoriginallyscheduledforApril2017isexpectedtoberescheduledtoadatelaterintheyear,withAlvogen’s30-monthstayofFDAapprovalexpiringOctober29th,2017.
▪ By a Court order dated August 22nd, 2016, Indivior’s Suboxone® Film patentlitigationagainstSandozhasbeendismissedwithoutprejudicebecauseSandozisno longer pursuing Paragraph IV certifications for its proposed genericformulationsofSuboxone®film.
▪ Trial againstMylan in the lawsuit involving theOrangeBook-listed patents forSuboxone®FilmisscheduledforSeptember25th,2017,withMylan’sstayexpiringMarch24,2018.
▪ IndiviorreceivedaParagraphIVnotificationfromTeva,datedFebruary8,2016,indicating that Teva had filed a 505(b)(2) New Drug Application (NDA) for a16mg/4mg strength of Buprenorphine/naloxone sublingual film. The Indivior

15|Page
GroupandTevaagreedthatinfringementbyTeva’s16mg/4mgdosagestrengthwillbegovernedby the infringement rulingontheaccused8mg/2mgdosagestrengthinitsANDAcurrentlyscheduledfortrialinNovember2016.
▪ TheUSPTOdeclined to institute Teva’s petitions for inter partes reviewof thethreeOrangeBook-listedpatentsonproceduralgrounds.
▪ Dr.Reddy’shasfiledaninterpartesreviewpetitiononeachofthethreeOrangeBookPatents.ThesepetitionsaresubstantivelysimilartothosefiledbyTeva.
▪ Certain claims of the ’832 patent were found invalid in an IPR proceeding, adecisionthathasbeenaffirmedbytheCourtofAppealsfortheFederalCircuit.
▪ Intheeventofarulinginthesemattersthatnoneoftheclaimsoftheassertedpatents are valid and infringed by the ANDA-filers, and should there be FDAapproval of one ormore of the ANDAs and subsequent commercial launch ofgenericSUBOXONE®film,andpipelineproductsfailtoobtainregulatoryapproval,there is the likelihoodthatrevenuesandoperatingprofitsof theCompanywilldecline.InthesecircumstancestheDirectorsbelievetheywouldbeabletotakethe required steps to reduce the cost base, however this would result in asignificantchangetothestructureofthebusiness.
SuboxoneAddictionCommentsfromOnlineForums
Theprobabilityofrelapseandcontinuedaddictionversussobrietyisnotwelldocumentedover longperiodsof time.Theprevalenceof socialmediaand forums thatdiscuss Suboxoneaddiction and relapse as ongoing major issues among recovering opioid addicts is a strongindicationthatSuboxonemaybecausingmoreharmthanbenefits.
Further,webelieveSuboxonemaybenomorebeneficialthansimpletapered-opioidregimes.
SinceitisdifficulttoobtainobjectivedataonthefulleffectsexperiencedbypatientswithSuboxonetreatment,ortheextentofprescriber-patientinteraction,selecteddiscussionsfromonline forums below describe the negative long-term and harmful results experienced bypatientsonprescribedSuboxonetreatment.
Of note, these discussions are only a small sample of themany discussions at onlineforums.While not peer-reviewed or independently investigated, the sheer number of thesecommentscannotbeignored.

16|Page
Hyperlink Drug Info
Drugs.com SuboxoneandRelapse MarriedmotheraddictedtoSuboxone
SuboxoneForum Relapseafter2years Doctorsays“YoucanonlygetoffSuboxoneonce”.
TheFix SuboxoneAddiction BlogstatesSuboxoneisnolessaddictivethanotheropioids
TheDailyBeast SuboxoneinPrison ClaimsSuboxonehasovertakenheroininamountssmuggledintoprisons.
AddictionRecoveryGuide Subutex(buprenorphine) Patientaddictedtobuprenorphinefor4years.
Drugs.com Suboxone PatientaddictedtoSuboxonefor2years.
Drugs-forum.com Suboxone Patientputonopiates,becameaddicted,putonSuboxone,becameaddicted.
Further, there are numerous other disturbing findings from opioid addiction online
forums.AbovearehighlightsofsomeofthemostcommonclaimsofpatientshavingtroublewithSuboxonetreatment.
SinceSuboxoneisanopioidinitselfanddoesnottreattheaddictionsymptomsonthe
neurological level, therapy and treatment programs are highly necessary in most cases foraddictiontobediminished.
InadequatePatientDiagnosisforSuboxoneTreatment
We’vereadextensively thatprescribingphysiciansdonotalwaysrequirepatientsto

17|Page
partakeinanytreatmentprograms,andthatSuboxonetreatmentmayonlyconsistofonein-officevisit.
FinancialIncentivestoOver-PrescribeSuboxone
Doctorsmayrequirepatientstopaythephysiciandirectlyat$10perpill (singledailydose).Patientshavereportedabeliefthatdoctorsdothisforprofit.
SeriousWithdrawalSymptomswithSuboxone
ManypatientsclaimthatSuboxoneishardertoquitthantheirprescriptionopioidsthatbroughtthemtoaddictiontreatmentinthefirstplace.
DangerousRespiratoryDepressionwithSuboxone
Suboxoneandotheropioidsmaycauserespiratorydepression.Manypatientsstatetheywere prescribed benzodiazepines in parallel with Suboxone. The combination ofbenzodiazepines and either Suboxoneor opioids can cause significant respiratory depressionwhich has been the cause ofmany deathswith patients using Suboxone.We believemanydoctorsarenotawareofthisdanger.
FinancialCostofTreatmentforSuboxoneandOpioidAddicts
DoctorsmaychargehundredsofdollarstoapatientforanappointmenttobetreatedforaSuboxoneaddiction.Then,doctorsareexpectedtowriteanewprescriptionorpersonallyhandoutSuboxonetothepatient.Thecostofsuchtreatmentmaycausepatientstoseekheroinorotherdrugsdue to financialproblems, increasing thechanceof relapseordeath. Further,dangers are associatedwith the lack of understanding of the ceiling effects and antagonismassociatedwithSuboxone“treatment”.
DoctorsNotCommittedtoGetPatientsOffSuboxoneorOtherMaintenanceDrugs
Therearemanypatients thatdiscussSuboxoneandmaintenancedrugs ingeneral,asonlyameansthatprolongaddiction,andthatmanymedicalprescribersarelargelyuninformedorhavelittleintentofhelpingpatientsoffSuboxoneorsuchmaintenancedrugs.Instead,patientsmust seek self-help online forums, private and non-medical treatment centers to get offSuboxoneandothermaintenancedrugs.
Suboxone’sImpactontheBrain’sReceptorsCausesCravingforOpioids
Due to the conflicting partial-agonist and antagonist effects of buprenorphine and

18|Page
naloxone,theingredientsinSuboxone,somepatientsclaimthattaperingwithSuboxoneactuallycauses an increase in the need for opioids , making the Suboxone taper actually counter-productiveforquittinganopioidaddiction.Conclusions
Together, the neurological understanding of opioids and the large studies done onSuboxonetreatmentindicatetousthat:
1. Suboxoneactivatestheopioidreceptors,induceseuphoriathatopioidaddicts
seek,andcancausewithdrawalssimilartoheroin.
2. Buprenorphine,anactiveingredientinSuboxonecancauserespiratorydepression(Naloxone,n.d.).
3. Suboxone’sefficacyhasbeenprematurelydeterminedbasedon(1)opioid
treatmentretentionand(2)negativeillicitopioidurinesamples-notsobrietyfromopioidsoverlongerperiods.
4. ManystudiesfundedbyIndiviorwereinadequatethatevaluatedSuboxone’s
efficacybasedonlimiteddatafromurinesamples-astheydidnotscreenforthesemi-syntheticorsyntheticagonistssuchasoxycodoneorfentanyl.
5. TheantagonistactivityofSuboxoneontheopioidbrainreceptorscould
potentiallyincreasethedangersofoverdoseanddeath.
6. ManyindependentstudiesonSuboxonehaveshownnodifferencebetweenplaceboandSuboxoneforillicitopioiduse.
Additionally,manypatienttestimonialsindicatethatSuboxonetreatmentmayprolong
theaddictionproblemandrequiresextensiveout-of-pocketpayments.
PrescriptionrequirementsanddiagnosisforSuboxonetreatmentseemtobeinformalatbest,andmanydoctorsappeartonotrequirepatientstojoinanaddictiontreatmentprogram.
Additionally,thereisnomaximumtimeframeforSuboxonetreatment,i.e.therearenocontrolledtrialsfordiscontinuationofuse,indicatingitwasnottheintentofthepharmaceutical

19|Page
producertocureopioidaddiction,buttoprovidemaintenanceindefinitely(whichcanbeseenasjustreplacement).
Yet, even in the face of substantial independent research showing little evidence forefficacy in actually treating opioid addiction, a substantial profit has been made by ReckittBenckiser and Indivior and this profit is being made in the face of rising deaths caused byprescriptiondrugoverdoses.
*Whileresearchingnaloxone/bupenorphinetreatmenttrials,itisessentialtoidentifythefunding source of the investigators. Multiple studies disclose funding sources as thepharmaceuticalcompanieswhoseproductseeksFDAapproval,whichcanbiasresults.
Alistofpharmaceutical-companyfundedresearch:http://www.sciencedirect.com/science/article/pii/S037687160900115Xhttp://onlinelibrary.wiley.com/doi/10.1111/j.1521-0391.2011.00186.x/fullhttp://www.sciencedirect.com/science/article/pii/S0140673603126001
References
Blum,Kenneth,MarleneOscar-Berman,JohnFemino,RogerL.Waite,LisaBenya,JohnGiordano,JoanBorsten, et al. 2013. “Withdrawal fromBuprenorphine/Naloxone andMaintenancewithaNaturalDopaminergicAgonist:ACautionaryNote.”JournalofAddictionResearch&Therapy4(2).doi:10.4172/2155-6105.1000146.
Bowdle,T.A.1998.“AdverseEffectsofOpioidAgonistsandAgonist-AntagonistsinAnaesthesia.”DrugSafety:AnInternationalJournalofMedicalToxicologyandDrugExperience19(3):173–89.
CDC. 2014. “CDC VitalSigns - Opioid Painkiller Prescribing.” Centers for Disease Control andPrevention.July1.http://www.cdc.gov/vitalsigns/opioid-prescribing/index.html.
Cradick,Mary, ShannonDeGrote, SpencerMarsall, and TerriWarholak. 2014. “Suboxone forMedically Assisted Treatment for Opioid Dependence.” The University of Arizona.http://arizona.openrepository.com/arizona/handle/10150/614151.
Dahan,Albert,LeonAarts,andTerryW.Smith.2010.“Incidence,Reversal,andPreventionofOpioid-InducedRespiratoryDepression.”Anesthesiology112(1):226–38.
Dahan, Albert, Elise Sarton, Luc Teppema, Cees Olievier, Diederik Nieuwenhuijs, HansW. D.Matthes,andBrigitteL.Kieffer.2001.“AnestheticPotencyandInfluenceofMorphineandSevofluraneonRespirationinμ-OpioidReceptorKnockoutMice.”Anesthesiology94(5).TheAmericanSocietyofAnesthesiologists:824–32.
Dorp,EvelineL.A.van,AshrafYassen,andAlbertDahan.2007.“NaloxoneTreatmentinOpioidAddiction:TheRisksandBenefits.”ExpertOpiniononDrugSafety6(2):125–32.

20|Page
Finch, James W., Jonathan B. Kamien, and Leslie Amass. 2007. “Two-Year Experience withBuprenorphine-Naloxone (Suboxone) forMaintenance Treatment ofOpioidDependenceWithinaPrivatePracticeSetting.”JournalofAddictionMedicine1(2):104–10.
Fudala,PaulJ.,T.PeterBridge,SusanHerbert,WilliamO.Williford,C.NoraChiang,KarenJones,JosephCollins,etal.2003.“Office-BasedTreatmentofOpiateAddictionwithaSublingual-TabletFormulationofBuprenorphineandNaloxone.”TheNewEnglandJournalofMedicine349(10):949–58.
Goodman,AllanJ.,BertrandLeBourdonnec,andRolandE.Dolle.2007.“MuOpioidReceptorAntagonists:RecentDevelopments.”ChemMedChem2(11):1552–70.
Han, Beth, Wilson M. Compton, Christopher M. Jones, and Rong Cai. 2015. “NonmedicalPrescriptionOpioidUseandUseDisordersAmongAdultsAged18Through64YearsintheUnitedStates,2003-2013.”JAMA:TheJournaloftheAmericanMedicalAssociation314(14):1468–78.
Mattick, Richard P., Courtney Breen, Jo Kimber, and Marina Davoli. 1996. “BuprenorphineMaintenance versus Placebo or Methadone Maintenance for Opioid Dependence.” InCochraneDatabaseofSystematicReviews.JohnWiley&Sons,Ltd.
Naloxone,StructuralFormulaO.F.n.d.“NaloxoneHydrochlorideIsaWhitetoSlightlyoff-WhitePowderandIsSolubleinWater,inDiluteAcidsandinStrongAlkali.Chemically,NaloxoneIs17-Allyl-4, 5 α -Epoxy-3, 14- Dihydroxymorphinan-6-One Hydrochloride. NaloxoneHydrochlorideHas theMolecular Formula CHNOHCl .2HO and theMolecularWeight Is399.87.”https://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM191529.pdf.
Nyman, U., and O. Hall. 1976. “Some Varieties of Papaver Somniferum L. with ChangedMorphinaneAlkaloidContent.”Hereditas84(1):69–78.
Romberg, R., E. Sarton, L. Teppema, H. W. D. Matthes, B. L. Kieffer, and A. Dahan. 2003.“Comparison of Morphine-6-Glucuronide and Morphine on Respiratory Depressant andAntinociceptiveResponses inWildTypeandMu-OpioidReceptorDeficientMice.”BritishJournalofAnaesthesia91(6):862–70.
Sarton, Elise, Luc Teppema, and Albert Dahan. 2008. “Naloxone Reversal of Opioid-InducedRespiratory Depression with Special Emphasis on the Partial Agonist/antagonistBuprenorphine.”AdvancesinExperimentalMedicineandBiology605:486–91.
Sawynok, J., C. Pinsky, and F. S. LaBella. 2017. “On the Specificity of Naloxone as anOpiateAntagonist - ScienceDirect.” Accessed January 23.http://www.sciencedirect.com/science/article/pii/002432057990403X.
Schottenfeld, Richard S., Marek C. Chawarski, and Mahmud Mazlan. 2008. “MaintenanceTreatment with Buprenorphine and Naltrexone for Heroin Dependence in Malaysia: ARandomised,Double-Blind,Placebo-ControlledTrial.”TheLancet371(9631):2192–2200.
Walsh,S.L.,K.L.Preston,M.L.Stitzer,E.J.Cone,andG.E.Bigelow.1994.“ClinicalPharmacologyofBuprenorphine:CeilingEffectsatHighDoses.”ClinicalPharmacologyandTherapeutics55(5):569–80.
Wang,Danxin,XiaochunSun,andWolfgangSadee.2007.“DifferentEffectsofOpioidAntagonists

21|Page
onMu-,Delta-,andKappa-OpioidReceptorswithandwithoutAgonistPretreatment.”TheJournalofPharmacologyandExperimentalTherapeutics321(2):544–52.
AppendixofMediaonSuboxoneandtheOpioidEpidemic
Suboxone:TheNewDrugEpidemic?“Thisisinsanity,”saysPercyMenzies,apharmacistandaddictionexpert.“Buprenorphineisoneofthemostabusedpharmaceuticalsintheworld.“Wetookanabuseddrugandwesaidlet’suseittotreataddictiontoheroinandopiates.”
EmergencyDepartmentVisitsInvolvingBuprenorphine● Emergencydepartment(ED)visitsinvolvingbuprenorphineincreasedsubstantiallyfrom
3,161in2005to30,135visitsin2010,asavailabilityofthedrugincreased● In 2010, most buprenorphine-related ED visits were classified as nonmedical use of
pharmaceuticals(52percent,or15,778visits),followedbypatientsseekingdetoxificationor substance abuse treatment (24 percent, or 7,372 visits) and adverse reactions (13percent,or4,017visits)
● Buprenorphine-relatedEDvisitsinvolvingnonmedicaluseofpharmaceuticalsincreased255percentfrom4,440visitsin2006to15,778visitsin2010
● Additionaldrugswereinvolvedin59percentofbuprenorphine-relatedEDvisitsinvolvingnonmedicaluseofpharmaceuticalsin2010
DrugOverdosesSpurRiseinAccidentalDeaths,SaysReport
Oneobviousplacetoreducedeathsisbydrugoverdoses.Morethan2millionAmericansabuseprescriptiondrugs,thereportsays,withheroinuseontheupswingagain.
Recoveringheroinaddictexplainswhysomanypeoplefailoutofrehabafterafewdays"WhenIwasonSuboxone[abrandnameversionofbuprenorphine],IfeltlikeIcoulddoit,"Petersonsaid."EverytimeIcameoffofit,IwantedtogethighandIcouldn'tgetthatthoughtoutofmyheadlongenoughtofocusonanythingelse.Itwasaconstant,'Ineedtouserightnow.'"
ForOpioid-AddictedInfants,aNewTreatmentOptionTheDangersofLongTermSuboxoneUse
Patients being prescribed Suboxonewere told this prescribedmedicinewould be thesolutiontotheirproblemofdrugaddiction.Inadditiontothefactthatapatientisstill

22|Page
physicallydependentonasubstancetofunction,thereareseveraldisturbingeffectsofSuboxonethatarerarelydiscussed.
TheSuboxoneProblemNoOneIsTalkingAbout
The act suggested that buprenorphine treatment be combined with regular urinescreenings and counseling. The key word here is suggested, and it's a terrible flaw.
Suboxone:ConcernsBehindtheMiracleWhenusedintheshortterm,SuboxoneisthebestdetoxdrugIhaveeverseen-itcanimmediatelystabilizeapatient'slife,andthiscanbedoneinanoutpatientsetting.Whenusedlong-term,though,it isthehardestmedicationIhaveeverdealtwithintermsofdetoxingapatientfromit.
AddictionTreatmentWithaDarkSideSuboxonedidnotsaveMilesMalone,20;itkilledhim.In2010,afriendtextedMr.Maloneaninvitationtousethedrugrecreationally—“wecandothesuboxinsassoonasIgivethem to u, right, dude?” — and he died that night in South Berwick, Me., ofbuprenorphinepoisoning.Thefriend,ShawnVerrill,wassentencedthissummerto71monthsinprison.AbouttheAuthorJonHelander,Ph.D.isapartneratAltumResearch,whoseresearchanalystsspecializeinscience-relatedduediligencereviewsofbiotechcompanies.www.altum-research.com