Stump the Experts- Interesting Cases · Treatment •HCs are first-line treatment in adolescents...
85
Stump the Experts- Interesting Cases Moderators: Dr Uday Thanawala Dr Anita Soni Experts: Dr Rama Vaidya Dr Gita Arjun Dr Sujata Mishra Dr Shobhana Patted Dr Sangeeta Agrawal
Transcript of Stump the Experts- Interesting Cases · Treatment •HCs are first-line treatment in adolescents...

Stump the Experts-Interesting Cases
Moderators Dr Uday Thanawala
Dr Anita Soni
Experts Dr Rama Vaidya
Dr Gita Arjun
Dr Sujata Mishra
Dr Shobhana Patted
Dr Sangeeta Agrawal
Case 1
bull 16 years old obese ( BMI 33 )
co -
bull Oligomenorrhea ( 45-60 days irregular scanty periods)
bull Acne
bull Excessive coarse hair on the face and over abdomen
bull Blackish velvety pigmentation at the neck
Do u think she is a PCOS
Guidelines of the Endocrine Society
Diagnosis
bull The diagnosis of PCOS in an adolescent girl be made based on
bull the presence of clinical andor biochemical evidence of hyperandrogenism (after exclusion of other pathologies)
bull in the presence of persistent oligomenorrhea
bull Anovulatory symptoms and PCO morphology are not sufficient to make a diagnosis in adolescents as they may be evident in normal stages in reproductive maturation
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Suspecting PCOS - What investigations
bull LHFSHbull TSHProlactinbull HbA1cbull Serum Insulin levels
-Fasting gt 20 mIUml- Glucose Insulin Ratio lt 45
DHEA-S Free TestosteroneUSG
Investigations
bull Sr Insulin FPP- 51271415 microIUml
bull TSH- 453 microIUml
bull HbA1c- 49
bull Vitamin D- 578 ngml
bull USG pelvis - Polycystic ovaries
Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
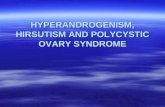
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Case 1
bull 16 years old obese ( BMI 33 )
co -
bull Oligomenorrhea ( 45-60 days irregular scanty periods)
bull Acne
bull Excessive coarse hair on the face and over abdomen
bull Blackish velvety pigmentation at the neck
Do u think she is a PCOS
Guidelines of the Endocrine Society
Diagnosis
bull The diagnosis of PCOS in an adolescent girl be made based on
bull the presence of clinical andor biochemical evidence of hyperandrogenism (after exclusion of other pathologies)
bull in the presence of persistent oligomenorrhea
bull Anovulatory symptoms and PCO morphology are not sufficient to make a diagnosis in adolescents as they may be evident in normal stages in reproductive maturation
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Suspecting PCOS - What investigations
bull LHFSHbull TSHProlactinbull HbA1cbull Serum Insulin levels
-Fasting gt 20 mIUml- Glucose Insulin Ratio lt 45
DHEA-S Free TestosteroneUSG
Investigations
bull Sr Insulin FPP- 51271415 microIUml
bull TSH- 453 microIUml
bull HbA1c- 49
bull Vitamin D- 578 ngml
bull USG pelvis - Polycystic ovaries
Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Do u think she is a PCOS
Guidelines of the Endocrine Society
Diagnosis
bull The diagnosis of PCOS in an adolescent girl be made based on
bull the presence of clinical andor biochemical evidence of hyperandrogenism (after exclusion of other pathologies)
bull in the presence of persistent oligomenorrhea
bull Anovulatory symptoms and PCO morphology are not sufficient to make a diagnosis in adolescents as they may be evident in normal stages in reproductive maturation
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Suspecting PCOS - What investigations
bull LHFSHbull TSHProlactinbull HbA1cbull Serum Insulin levels
-Fasting gt 20 mIUml- Glucose Insulin Ratio lt 45
DHEA-S Free TestosteroneUSG
Investigations
bull Sr Insulin FPP- 51271415 microIUml
bull TSH- 453 microIUml
bull HbA1c- 49
bull Vitamin D- 578 ngml
bull USG pelvis - Polycystic ovaries
Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Suspecting PCOS - What investigations
bull LHFSHbull TSHProlactinbull HbA1cbull Serum Insulin levels
-Fasting gt 20 mIUml- Glucose Insulin Ratio lt 45
DHEA-S Free TestosteroneUSG
Investigations
bull Sr Insulin FPP- 51271415 microIUml
bull TSH- 453 microIUml
bull HbA1c- 49
bull Vitamin D- 578 ngml
bull USG pelvis - Polycystic ovaries
Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Investigations
bull Sr Insulin FPP- 51271415 microIUml
bull TSH- 453 microIUml
bull HbA1c- 49
bull Vitamin D- 578 ngml
bull USG pelvis - Polycystic ovaries
Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Objectives of Treatment of Adolescent PCOS
bull Treatment of oligomenorrheaamenorrhea
bull Management of hirsutism and acne
bull Reducing the far reaching consequences of
insulin resistance and glucose intolerance
Singh R Yadav P Parveen R J South Asian Feder Obst Gynae 20124(3)123-125
Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Management
bull Diet
bull Exercise
bull Weight loss ndash goals
bull How to counsel the patient for all this
Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Weight loss
bull No time from school and classes
bull Now shy to take part in any games
bull Mother says ldquo very poor eaterrdquo
What practical advice to her and her mother
Decrease Screen time
Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Psychosocial support
bull Offering psychosocial support can be one of the most important aspects of managing this disease
bull This begins by
bull building positive supportive relationships with adolescent diagnosed PCOS
bull Such relationship will allow the adolescents to express their feelings and concerns regarding having a chronic disease whose signs and symptoms can greatly impact onersquos body image and self-esteem
Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Pharmacological management
What drugs will you advice
bull Drugs to regularize Periods ndash Only Progesterone or EP
bull Drugs to tackle hirsuitism
bull ( cyproterone acetate or drosperinone )
bull Drugs to bring down insulin resistance - Metformin or and Inositol
bull Drugs for weight loss ndash Orlistat (Xenical)
Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Insulin Sensitizers
Role of Metforminhellip
bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

bull Inhibits hepatic glucose output insulin secretion
bull Metformin sensitises insulin receptors decreasing IR
bull Decreases androgen production by ovaries and adrenal glands
bull Significant improvement of metabolic parameters
Metformin
Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Metformin
OCPs
CC
1Hyperandrogenism
2Insulin resistance
3Ovulation amp Fertility
Benefits Treatment
Salt retention venous thromboembolism pregnancy impossible CI short stature depression
Multiple births breast tenderness flushing GI disturbances
Weakness numbness in extremitiestroubled breathingGI discomfort
Side effects
1 None
PCOS Gaps in treatment
2 3 Gap
Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Are there any real alternatives we can offer
NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

NEW KID ON THE BLOCK
Myoinositol with D Chiro Inositol
Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Myoinositola new insulin sensitiser
Six carbon sugar alcohol present abundantly in the
body
Synthesized by the cells in normal physiological
conditions
During periconceptional period requirement increases
A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

A newer approach for PCOS in young women
Increases action of insulin in PCOS patients
Improves ovulatory function
Decreases testosterone concentration
Restores spontaneous menstrual cycles
Improves endocrine metabolic and dermatological problems
Represents a simple and safe medication
18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

18
Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Growing evidence on emerging role of Myoinositol in PCOS
Myo-inositol showed a great improvement in
insulin sensitivity and ovarian functions
Myo-inositol besides improving hormonal
profile and restoring ovulation is also able
to induce regular menses in PCOS patients
Eur Rev Med Pharmacol Sci 2011 May15(5)509-14 Fertility and Sterility Vol 95 No 8 June 30 20112515-2516
Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Hyperinsulinemic
PCOS women
Metformin N= 123 Inositol N=506 month therapy
Significant improvement in the menstrual frequency
Reduction in insulin levels than Metformin
Better tolerability
Better patient complianceFertility and Sterility 2006 September 86( 3) Supplement 1S461
Superiority of Myoinositolover Metformin
Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Fifty patients with PCOS and signs of
hyperandrogenism (hirsutism andor acne)
Duration 3 months and 6 months
Parameter evaluated BMI LH FSH insulin HOMA
index testosterone free testosterone hirsutism and
acne
Gynecological Endocrinology August 2009 25(8) 508ndash513
Efficacy of myoinositol in the treatment of cutaneous disorders in young women with polycystic ovary syndromeZacchegrave MM Caputo L Filippis S Zacchegrave G Dindelli M Ferrari AGynecological-Obstetric Department IRCCS San Raffaele Hospital Vita-Salute University Milan Italy
significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

significaNT disappearance OF hirsutism and acne
-60
-50
-40
-30
-20
-10
0
-16
-30
-21
-53
Percent reduction
After 3 months
After 6 months
After 3 months
After 6 months2
AcneHirsutism
16-30 reduction in Hirsutism
21-53 reduction in Acne
Perc
ent
red
uct
ion
Gynecological Endocrinology August 2009 25(8) 508ndash513
Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Guidelines of the Endocrine Society Treatment
bull HCs are first-line treatment in adolescents with
suspected PCOS (if the therapeutic goal is to treat
acne hirsutism or anovulatory symptoms or to
prevent pregnancy)
bull lifestyle therapy (calorie-restricted diet and exercise)
with the objective of weight loss should also be first-
line treatment in the presence of overweightobesity
bull metformin as a possible treatment if the goal is to
treat IGTmetabolic syndrome
bull The optimal duration of HC or metformin use has
not yet been determinedJournal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Guidelines of the Endocrine Society Treatment
bull For premenarchal girls with clinical and
biochemical evidence of hyperandrogenism in
the presence of advanced pubertal
development (ie ge Tanner stage IV breast
development) start HCs
Journal of Clinical Endocrinology amp Metabolism December 2013 JCEM jc2013ndash2350
Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Clinical Situation 2
bull 26 year old diagnosed PCOS patient wants to conceive ndash what will be your advice and what all will you keep in mind for ovulation induction
bull BMI ndash 32 irregular periods Typical pcoovaries with thick stoma
bull OGGT ndash normal TSH ndash Normal
weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

weight loss
bull weight loss ndash how much before starting treatment what is practical
bull For weight loss when would you advice ndash
bull Lifestyle changes only
bull drugs
bull bariatic surgery
Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Ovulation Induction
bull ovulation induction ndash CC or Letrozole
bull FM with IUI better option
bull No response to CC or Letrozole hellip
bull Gonadotropin cycle ndash what will u start and what dose
bull Whatrsquos your take on chronic low dose protocol
bull When would you advice for IVF
Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Adjuvants
bull As an adjuvant to IVF ndash do insulin sensitizers have a effect on oocyte quality
bull Role of metformin inositols
lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

lsquoMyo-inositol is useful in treatment of PCOS
patients undergoing ovulation induction both for
its insulin sensitizing activity and its role in oocyte
maturationrsquo
Ciotta et al
Eur Rev med Pharmacol Sci 2007 11 347-354
Oocyte quality
bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

bull A study of 22 obese women with PCOS receiving D-chiro inositol (1200mg OD)
for 8 weeks versus 22 women receiving placebo
bull D chiro inositol supplementation resulted in
ndash Significantly higher reduction of waist- hip ratio
ndash Significantly early response to leuprolide for ovulation
ndash Decrease in plasma insulin levels
ndash serum testosterone and SHBG
19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

19 out of 22 women ovulated during treatment with D-chiro inositol
Authors observed an increase in insulin response to oral glucose following administration of D-chiro inositol in women of PCOS due to
improvement of peripheral insulin sensitivity
Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Combination Effect
Myo-inositol D-chiro-inositol
1 Eur Rev Med Pharmacol Sci 201216575-581
bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

bull Combination restores the ovulation in obese classic PCOS
bull Significant improvement in sex hormone levels following treatment
bull Compared to the MI group decrement of total T amp increase of SHBG was significantly higher in the MI+DCI group at both T1 (3months) and T2 (6months)
bull MI+DCI ndash First line treatment in obese PCOS women
Combination of Myoinositol andD Chiro Inositol
Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Clinical Situation 3
bull 26 year old Primi with a BMI of 23 ndash comes with a UPT positive
bull She has conceived on CC FM cycle
bull Told she was a PCO ndash had irregular cycles
bull Her routine investigations done 6 months earlier were all normal
bull Will you screen her for glucose intolerance
Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Advocates for Universal Testing
What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

What is a good time to screen her
When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

When - FIGO GUIDELINES Alternative strategies as currently used in
specified countries
Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Which test would you order
FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

FIGO GUIDELINES 2015
bull As per the recommendation of the IADPSG (2010) and WHO (2013) the diagnosis of GDM is made using a single-step 75-g OGTT when one or more of the following results are recorded during routine testing ndash
bull Fasting plasma glucose 51minus69 mmolL (92minus125 mgdL)
bull 1-hour post 75-g oral glucose load ge10 mmolL (180 mgdL)
bull 2-hour post 75-g oral glucose load 85ndash110 mmolL (153minus199 mgdL)
FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

FIGO also recognizes
bull Recommendations that are rigid and impractical in real-life settings are unlikely to be implemented and hence may produce little or no impact
bull On the other hand pragmatic but less than ideal recommendations may produce significant impact owing to more widespread implementation
Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Attitudes and practices differ in different settings in India
For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

For a pregnant women the request to attend fasting for a blood
test may not be realistic because of the long travel distance to
the clinic in many parts of the world and increased tendency to
nausea in the fasting state Consequently non-fasting testing
may be the only practical option
Strategies for Implementing the WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in
Pregnancy In Press
WHO Observations and Recommendations - 2013
OGTT is resource intensive and many health services especially in low
resource settings are not able to routinely perform an OGTT in
pregnant women In these circumstances many health services do not
test for hyperglycemia in pregnancy Therefore options which do not
involve an OGTT are required
WHO Recommendations - 2013
A ldquoSingle Step Procedurerdquo to diagnose GDMRef - WHONMHMND132
3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

3times more pick up than with two step
Suitable for Indian setting
Saves time
Saves cost
Avoids repeated visits
Reduces repeated invasive sampling
One step 75gm OGTT - Advantages
DIPSI Recommended method
Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Blood reports
GCT 178 mgdl
What next
HbA1C 112
Would you advice termination of pregnancy
How would you counsel her
44
Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Evaluation - Hb A1c ( NICE 2015)
bull Measure HbA1c levels in all women with gestational diabetes at the time of diagnosis to identify those who may have pre-existing type 2 diabetes
bull Pregnancy complications and risk of congenital malformations increase with an HbA1c level above 48 mmolmol (65)
bull Do not use HbA1c levels routinely to assess a womans blood glucose control in the second and third trimesters of pregnancy
Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Increase risk of congenital abnormalities sacral agenesis congenital heart diseaseamp neural tube defects
Hba1c level Risk
till 65 not increased
lt8 5
gt10 25
HbA1c amp congenital anomalies
Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Pregnancy Care
bull Scan for viability at 7 weeks
bull 11- 135 weeks scan ndash for anatomy and NT
bull Offer double marker ndash make sure to mention she is diabetic as it effects the results
bull Anomaly scan at 18- 20 weeks
bull Watch for Hypertension other maternal problems ndash retinopathy renal function
bull Frequent growth scans to pick up macrosomia IUGR
Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Monitoring sugars
bull How and How frequent
management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

management
Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Management
Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Pharmacological management
Glycemictargets
Weight gain
Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Insulin when
Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Planning delivery
bull 38- 39 weeks if sugars controlled with diet + exercise+ OHA
bull 38 weeks if on insulin earlier if sugars not controlled or signs of macrosomia
bull Neonatal backup
Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Includes recommendations for Postpartum care
Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Clinical Situation 4
bull 36 years old Gravida2 Para1 Living1
bull Weight 153 Kg BMI 575 Kgm2
bull Previous CS GDM mild preeclampsia
bull kco PCOD
What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

What maternal complications should we be on look out for
Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Obesity
Increased chances of
bull spontaneous abortion
bull chromosomal abnormality
bull PIH IUGR macrosomia
bull Operative deliveries anesthesia risk post op complications like DVT
Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Is the fetus also at risk
Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Risks and Complications
Increased fetal risk of
bull Congenital malformation (16 fold)
bull Fetal macrosomia (21-31 fold)
bull Shoulder dystocia
bull Stillbirth (21 fold)
bull Neonatal death (26 fold)
bull Neonatal morbidity ie NICU admission
bull Reduced rates of breast feeding
antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

antenatal care
bull More frequent ultrasounds to monitor growth
bull Screen for PIH GDM
bull Diet advice
bull Exercise Advice
PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

PROBLEMS OF LABOUR
Ist and IInd stages are prolonged
The median dose and duration of predelivery oxytocin
is significantly greater among obese patients
(26 units and 65 hours) vs (50 units and 85 hours)
Pevzner (2009) Obstet Gynecol
PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

PROBLEMS OF LABOUR
o Increased rates of operative deliveries [forceps] due to
early maternal exhaustion
poor bearing down efforts
malpresentations
o IIIrd stage post partum hemorrhage
o LACTATION FAILURE
Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Cesarean Section in OBESE Women Difficulty in delivery
bull Anticipation
bull High floating head
bull Simpsonrsquos Obstetric Forceps
Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Cesarean Section in OBESE Women A Challenge
bull Team of doctors
bull Additional helping hands
bull Difficult pfannenstielincision due to large panniculus
bull Panniculus should be retracted by an assistant
Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Difficulties with Spinal Anaesthesia
Difficulty in identification of space (l4l5) due to obscured landmarks difficult positioning layers of adipose tissue
Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Cesarean Section in OBESE Women Suturing of uterine incision
bull Difficult suturing in depth
bull Bleeding from uterine incision difficult to tackle
Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Cesarean Section in OBESE Women Subcutaneous drain
Mini Vac subcutaneous
drain no 8 or 10- Prevents
wound infection
Leg Compression Heparin
prophylaxis
ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

ACOG 2013 Recommendations
bull Preconceptional assessment and counselling
bull Monitoring and guidance regarding appropriate weight gain during pregnancy
bull Nutrition and exercise counselling
bull Women who have undergone bariatric surgery should be evaluated for nutritional deficiences and supplementation should be done
ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

ACOG 2013 Recommendations
bull Individual risk assessment and Thromboprophylaxis in the form of pneumatic compression pumps and LMW Heparin
bull Consider using higher dose of pre-operative antibiotics
bull Suturing subcutaneous layer prevents any disruption of wound
bull Anesthesiology consultation early in labour
ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

ACOG 2013 Recommendations
bull Consultation with a weight reduction specialist should be encouraged post delivery
Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Outcome
bull Elective repeat CS at 38 weeks
bull Obstetric forceps 44 Kg baby
Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Clinical Situation 5
bull 45 yrs old obesebull BMI 35bull Abnormal uterine bleeding since 6 monthsbull HO PCOS with irregular periods bull 2 FTNDsbull kco diabetes mellitusbull No hypertensionbull USG so Bulky uterus with ET- 20 mm
bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

bull Burden of AUB in the peri-menopausal age group
bull Impact on quality of life
Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Burden of HMB in India
Excessive bleeding has been reported in about 8-9 women from India and neighboring countries1
42-53 of women aged lt 21 years and those gt 21 years complained of excessive bleeding2
15 of all gynecology OPD visits and 25 of all gynaecological surgeries3
1 Harlow SD Campbell OM BJOG 20041116ndash 16 2 Omidvar S Begum K J Nat Sci Biol Med 20112174ndash93 Chattopdhyay B Nigam A Goswami S Eur Rev Medi Pharmacol Sci 201115764ndash768
8ndash9
42ndash53
15
Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Impact of AUB on Quality of life (QoL)
Major impact on a womanrsquos quality of life
Over 60 of women diagnosed with HMB ended up having a hysterectomy within 5 years from the diagnosis4
About 13rd of hysterectomies for HMB result in removal of anatomically normal uterus5
Impact of HMB
Anxiety
Decreases work
productivity2
Iron deficiency anaemia 1
Discomfort1
Negative impact on
relationship with
partners3
Decreased QOL1
1 Ghazizadeh S Int J Womenrsquos Health 20113 207ndash21 2 Magon N J Midlife Health 20134(1)8ndash15 3 Bitzer JOpen Access J Contracep 2013 21ndash28 4 NICE 2007 can be accessed at httpswwwniceorgukguidancecg44 5Roy SN Bhattacharya S Drug safety 2004
AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

AUB - E
bull Endometrial pathology is not of AUB ndash E is not
a structural concept but a functional concept
bull Biochemical or endocrine variation
bull The DUB of yesteryears
Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Investigations and Management
Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Algorithm for the Diagnosis of AUB
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

GCPR- Endometrial Assessment and Biopsy
recommended in all women with AUB
Older than 40 years of age (Grade A Level 2)
Less than 40 years who are at risk of endometrial cancer (Grade A Level 2)
Risk factors of endometrial cancerbull Irregular bleedingbull Obesity associated with hypertensionbull Endometrial thickness gt 12 mmbull Polycystic Ovarian syndrome (PCOS)bull Diabetes Mellitusbull History of malignancy of ovarybreast
endometriumcolonbull Use of Tamoxifen for HRT or breast cancerbull AUB-unresponsive to medical managementbull HNPCC syndrome (hereditary nonpolyposis
colorectal cancer or Lynch Syndrome)
Endometrial assessment (EA)
Endometrial histopathology Dilatation and curettage Hysteroscopy
Performed if endometrium is thick on imaging but HPE is inadequate to rule out polyps(Grade A Level 2)
Not be a procedure of choice for EA (Grade A Level 3)
Endometrial aspiration should be the
preferred procedure for obtaining
endometrial sample for histopathology
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations
for AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Treatment Options
Medical
Non-hormonal
Non-steroidal
Surgical
Certain clinical
situationsHormonal
Depends on
bull Clinical condition
bull Overall acuity
bull Suspected aetiology
bull Desire for future fertility and
bull Underlying medical problem
Preferred
Depends on
bull Clinical stability
bull Severity of bleeding
bull Contraindications lack of
response to medication
bull Desire for future fertility
1 ACOG Obstet Gynecol 2013121(4)891-6
Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Too many hysterectomies
bull One in five women will have a hysterectomy
before the age of 60
bull 46 of hysterectomies are performed for AUB
bull Over half the uteri that are removed are
structurally normalMaresh MJ et al The VALUE study BJOG 2002
National Evidence Based Guidelines UK 2003
NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

NICE Guidelines
Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Management of AUB-COEIN
Key recommendations for Treatment of AUB-COEIN
AUB-C Nor-hormonal is primary treatment Tranexmic acid Hormonal treatment secondary treatment LNG IUSCOCs
AUB-O Women not desirous of fertility COCs for 1st 6 months If COCs are contraindicated then LNG IUS is preferred as 1st line treatment
Surgical treatment not a choice of treatment unless failure of medical management
AUB-E Similar to AUB-O
AUB-I LNG IUS is preferred choice of treatment
AUB-N Women not desirous of contraception LNG IUS is 1st line of treatment If medical and surgical treatment fails or is contraindicated GnRH agonists are
preferred
The Federation of Obstetric and Gynecological Societies of India Good clinical practice recommendations for
AUB Available at httpwwwfogsiorgwp-contentuploads201602gcpr-on-aubpdf Last accessed at 24
February 2016
Thank you

Thank you