
STUDENT ENROLLMENT CHECK-SHEET - Amazon S3€¦ · It is not necessary to restart the series of any...
18
JUSTICE PUBLIC SCHOOL STUDENT ENROLLMENT CHECK-SHEET Student’s Name: (Last) (First) (Middle) Date of Enrollment:____ / ____ / ____ Grade Level: (M) (D) (Y) Please legibly initial the appropriate space beside each item in the appropriate column as it is completed. REQUIRED ITEMS Parent Initial Staff Initial 1. Student Enrollment/Information Sheet 2. Provide an up-to-date Immunization Record **See Current Immunization Schedule 3. Provide an original of the student’s Birth Certificate to copy 4. Provide the student’s Social Security Card to copy 5. Authorization to Administer Medicine (Form F) 6. Complete and sign Application for Computer and Network Use 7. Complete and sign Concussion and Head Injury Acknowledgement 8. Complete and sign Sudden Cardiac Arrest Acknowledgement REQUIRED ITEMS FOR AMERICAN INDIAN/ALASKA NATIVES 9. Provide an original of the student’s CDIB Card to copy 10. Title VI, 506 Indian Education Form (Form D) 11. Provide an original Tribal Enrollment Card to copy **If student has no tribal enrollment, a Tribal Enrollment Card for one (or both) parents listed on the original birth certificate is required for the child. REQUIRED ITEMS ACCORDING TO ENROLLMENT FORM INSTRUCTIONS 12. Initial Enrollment Prior Participation Form (Form A) 13. Vision Screening Form (Form B) 14. Home Language Survey (Form C) 15. Self-Administration of Asthma Medication (Form E) 16. Complete and sign for Receipt of Parent/Student Handbook Don’t forget to set up your FREE account on the Justice E-Notes portal.
Transcript of STUDENT ENROLLMENT CHECK-SHEET - Amazon S3€¦ · It is not necessary to restart the series of any...
JUSTICE PUBLIC SCHOOL STUDENT ENROLLMENT CHECK-SHEET
Student’s Name: (Last) (First) (Middle)
Date of Enrollment:____ / ____ / ____ Grade Level: (M) (D) (Y)
Please legibly initial the appropriate space beside each item in the appropriate column as it is completed.
REQUIRED ITEMS Parent Initial Staff Initial
1. Student Enrollment/Information Sheet
2. Provide an up-to-date Immunization Record**See Current Immunization Schedule
3. Provide an original of the student’s Birth Certificate to copy
4. Provide the student’s Social Security Card to copy
5. Authorization to Administer Medicine (Form F)
6. Complete and sign Application for Computer and Network Use
7. Complete and sign Concussion and Head Injury Acknowledgement
8. Complete and sign Sudden Cardiac Arrest Acknowledgement
REQUIRED ITEMS FOR AMERICAN INDIAN/ALASKA NATIVES
9. Provide an original of the student’s CDIB Card to copy
10. Title VI, 506 Indian Education Form (Form D)
11. Provide an original Tribal Enrollment Card to copy
**If student has no tribal enrollment, a Tribal Enrollment Card for one (or
both) parents listed on the original birth certificate is required for the child.
REQUIRED ITEMS ACCORDING TO ENROLLMENT FORM INSTRUCTIONS
12. Initial Enrollment Prior Participation Form (Form A)
13. Vision Screening Form (Form B)
14. Home Language Survey (Form C)
15. Self-Administration of Asthma Medication (Form E)
16. Complete and sign for Receipt of Parent/Student Handbook
Don’t forget to set up your FREE account on the Justice E-Notes portal.
JUSTICE PUBLIC SCHOOL STUDENT ENROLLMENT/INFORMATION SHEET
Student’s Name: Date of Enrollment: ____ / ____ / ____ (Last) (First) (Middle)
Date of Birth: Place of Birth: SS#: Grade Level: Gender: M / F Are you of Hispanic/Latino Origin (Circle One)? YES or NO
Race:
Form D & CDIB Required & Tribal
Enrollment if a member of a Tribe
(Circle All That Apply)
Black/ African American
American Indian/ Alaskan Native
Asian Native Hawaiian or
Pacific Islander White
Has the child being enrolled ever attended Justice Public School? Y / N Resident Address (Can not use P.O. Box): Mailing Address (if different from above—e.g., P.O. Box): Home Phone: Cell Phone(s): Last School Attended: Year: (School Name) (City / State)
Parent(s) or Guardian(s) with whom the student lives: (Must be listed with a valid phone number.) Name Relationship Place Employed Work Phone Cell Phone Email
Emergency Contacts: (Who to call if unable to locate the parents/guardians? Must be listed with a valid phone number.) Name Relationship Home Phone Cell Phone Other Phone
Please list all other parties authorized to pick up your child: (Must be listed with a valid phone number.) Name Relationship Home Phone Cell Phone Other Phone
Are you a resident of our district? Y / N (If not, in what district do you live?) Primary Transportation: By Parent: Bus: Other: Which available bus will your child ride? OAP / Country If Country, 911 #: YES - NO My student received the current Justice Parent/Student Handbook. YES - NO This is the first time my child has enrolled in school in Oklahoma OR my child is in the first grade or below.
(if yes, fill out Form A-Initial Enrollment)
Office Use Only
Student No.:_____________
Entry Code:_____________
Birth Auth.:______________
Immun. Records: Y / N
Spec. Svcs. Student: Y / N
YES - NO My child is enrolling in Kindergarten, First, or Third grade. (if yes, fill out Form B-SB1795 Vision Screening) YES - NO Is the custody of this child decreed by the courts?
If yes, who has primary custody? Relationship Current court documents declaring custody must be in this child’s school file.
YES - NO Does your child use a name other than his/her legal name? If so, what is it?
YES - NO Is either parent/guardian in the military or a civilian working on government property? If yes, who? Where?
Government properties that are eligible:
Federal Corrections Institution-FCI U.S. Postal Service Indian Health Services Tinker Air Force Base
Approved Indian Nation Casino Approved Community Hospitals Uniformed Services – (National Guard, Army, Air Force, Marines, Navy, Coast Guard, Reserves, etc.)
YES - NO Is the resident address owned by the Seminole (or other tribe) or Housing Authority or located on Indian Land?
Special Programs: Please circle all programs that your child has received. Gifted and Talented Speech OT/PT Special Education Reading Math
Other (describe):
YES - NO Do you use a language other than English in your home (this includes Native American Indian Languages)? If yes, what language? (and fill out Form C Home Language Survey)
YES - NO I give permission for my child to have access to the Justice School network and the Internet.
YES - NO I give permission for my child’s picture to be used in school publications. (yearbook, websites, newspaper, etc.)
YES - NO I give permission for my child to participate in school field trips. (Information will be sent home prior to each trip.)
YES - NO I give permission for my child to receive vision, hearing, and any other screening tests.
YES - NO Do you have any degree of American Indian ancestry or have a CDIB card? (if yes, fill out Form D-Title VI)
YES - NO Does this student take medication on a regular basis? If yes, list.
YES - NO Does this student have any health problems, asthma, or allergic reactions? Explain: (If asthma, fill out form E)
YES - NO I hereby authorize and give my consent to the employees of Justice Public School (Administration, Secretaries, homeroom teachers, etc.) to administer a non-aspirin medication, which the school will supply, in accordance with the instructions for administering such medication. (if yes, fill out Form F-Authorize to Dispense Medication)
I, the undersigned, do hereby authorize officials of Justice Public School to contact directly the persons named in this document, and do authorize the named physicians to render such treatment as may be deemed necessary in an emergency, for the health of said child. In the event physicians, other persons named in this document, or parents cannot be contacted, the school officials are hereby authorized to take whatever action is deemed necessary in their judgment for the health of the aforesaid child. I understand that Justice Public School will not be financially responsible for the emergency care and/or transportation for said child.
Physician (Doctor’s Name and Hospital Affiliation) 1st choice: Phone:
2nd choice: Phone: List other children in this household attending Justice Public School: Student’s Name Grade Student’s Name Grade
(Parent/Guardian’s Signature) (Date)
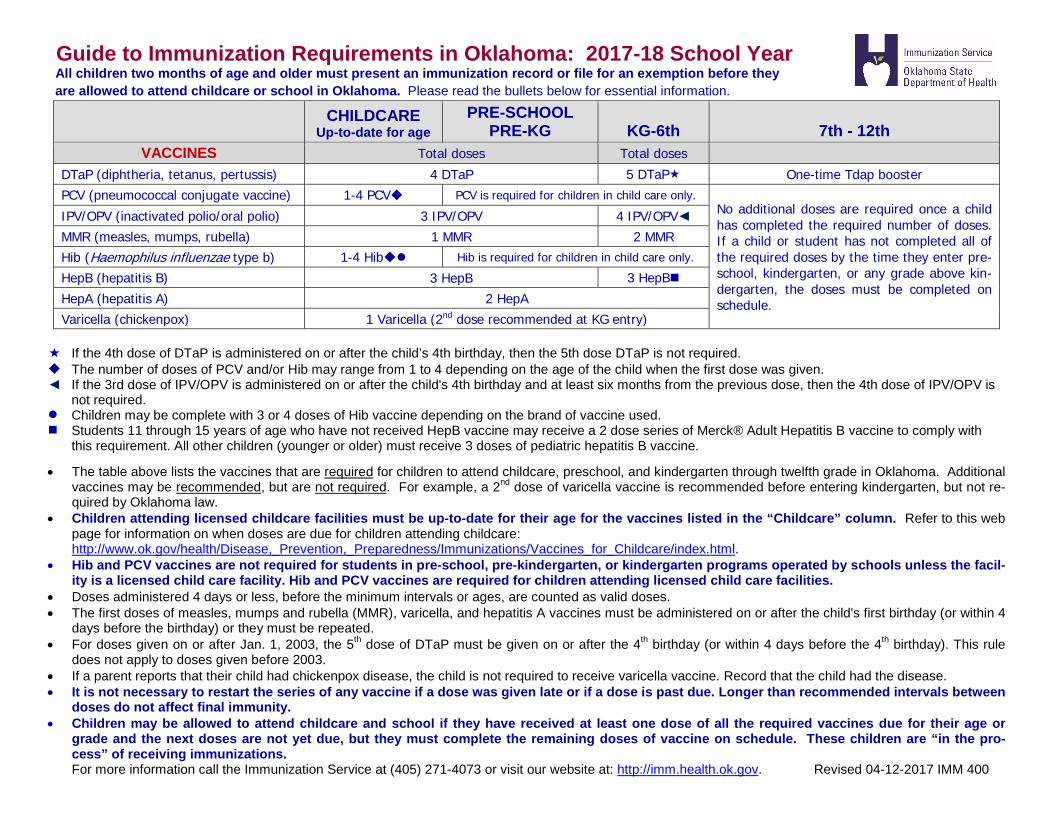
Guide to Immunization Requirements in Oklahoma: 2017-18 School Year All children two months of age and older must present an immunization record or file for an exemption before they are allowed to attend childcare or school in Oklahoma. Please read the bullets below for essential information.
CHILDCARE Up-to-date for age
PRE-SCHOOL PRE-KG KG-6th 7th - 12th
VACCINES Total doses Total doses
DTaP (diphtheria, tetanus, pertussis) 4 DTaP 5 DTaP One-time Tdap booster PCV (pneumococcal conjugate vaccine) 1-4 PCV PCV is required for children in child care only.
No additional doses are required once a child has completed the required number of doses. If a child or student has not completed all of the required doses by the time they enter pre-school, kindergarten, or any grade above kin-dergarten, the doses must be completed on schedule.
IPV/OPV (inactivated polio/oral polio) 3 IPV/OPV 4 IPV/OPV◄ MMR (measles, mumps, rubella) 1 MMR 2 MMR Hib (Haemophilus influenzae type b) 1-4 Hib Hib is required for children in child care only.
HepB (hepatitis B) 3 HepB 3 HepB
HepA (hepatitis A) 2 HepA Varicella (chickenpox) 1 Varicella (2nd dose recommended at KG entry)
If the 4th dose of DTaP is administered on or after the child’s 4th birthday, then the 5th dose DTaP is not required. The number of doses of PCV and/or Hib may range from 1 to 4 depending on the age of the child when the first dose was given.◄ If the 3rd dose of IPV/OPV is administered on or after the child's 4th birthday and at least six months from the previous dose, then the 4th dose of IPV/OPV is
not required. Children may be complete with 3 or 4 doses of Hib vaccine depending on the brand of vaccine used. Students 11 through 15 years of age who have not received HepB vaccine may receive a 2 dose series of Merck® Adult Hepatitis B vaccine to comply with
this requirement. All other children (younger or older) must receive 3 doses of pediatric hepatitis B vaccine.
• The table above lists the vaccines that are required for children to attend childcare, preschool, and kindergarten through twelfth grade in Oklahoma. Additionalvaccines may be recommended, but are not required. For example, a 2nd dose of varicella vaccine is recommended before entering kindergarten, but not re-quired by Oklahoma law.
• Children attending licensed childcare facilities must be up-to-date for their age for the vaccines listed in the “Childcare” column. Refer to this webpage for information on when doses are due for children attending childcare:http://www.ok.gov/health/Disease,_Prevention,_Preparedness/Immunizations/Vaccines_for_Childcare/index.html.
• Hib and PCV vaccines are not required for students in pre-school, pre-kindergarten, or kindergarten programs operated by schools unless the facil-ity is a licensed child care facility. Hib and PCV vaccines are required for children attending licensed child care facilities.
• Doses administered 4 days or less, before the minimum intervals or ages, are counted as valid doses.• The first doses of measles, mumps and rubella (MMR), varicella, and hepatitis A vaccines must be administered on or after the child's first birthday (or within 4
days before the birthday) or they must be repeated.• For doses given on or after Jan. 1, 2003, the 5th dose of DTaP must be given on or after the 4th birthday (or within 4 days before the 4th birthday). This rule
does not apply to doses given before 2003.• If a parent reports that their child had chickenpox disease, the child is not required to receive varicella vaccine. Record that the child had the disease.• It is not necessary to restart the series of any vaccine if a dose was given late or if a dose is past due. Longer than recommended intervals between
doses do not affect final immunity.• Children may be allowed to attend childcare and school if they have received at least one dose of all the required vaccines due for their age or
grade and the next doses are not yet due, but they must complete the remaining doses of vaccine on schedule. These children are “in the pro-cess” of receiving immunizations.For more information call the Immunization Service at (405) 271-4073 or visit our website at: http://imm.health.ok.gov. Revised 04-12-2017 IMM 400
Form A
Initial Enrollment Prior Participation Form Student Information
The following information should be completed by the parent or guardian of the student. This information is collected on a student’s initial enrollment into a school district. Please print legibly.
Student Legal Name: First Last
Student Date of Birth: Month Day Year
Student Gender – Please check one: Male Female
Did the student participate in any of the following programs? Please indicate by checking YES or NO for each statement.
PROGRAM YES NO A childcare program that is licensed pursuant to the tiered licensing system established by the Department of Human Services (a DHS licensed childcare program) The Sooner Start program operated by the State Department of Education
The Oklahoma Parents as Teachers (OPAT) program operated by the State Department of Education
The Children First program operated by the State Department of Health
Any child abuse prevention program operated by the State Department of Health
Any federally funded Head Start program
Form B
Vision Screening Form
Senate Bill 1795 became effective November 1, 2006. Beginning with the 2007-2008 school year, the parent or guardian of each student enrolled in Kindergarten, First, and Third grades at a public school must provide proof that their student passed a vision screening within the last twelve months.
Complete one of the following:
1. had a vision screening on . (Child’s Name) (Date)
The screening was administered by . (Screener’s Name)
was - was not referred for a comprehensive eye (Circle One)
examination by an eye care professional as a result of the above vision screening.
2. had a comprehensive eye exam on . (Child’s Name) (Date)
The comprehensive eye examination was administered by . (Eye Care Professional)
3. has not received a vision screening or (Child’s Name)
comprehensive eye examination in the past twelve months.
(Parent/Guardian Signature)
(Date)
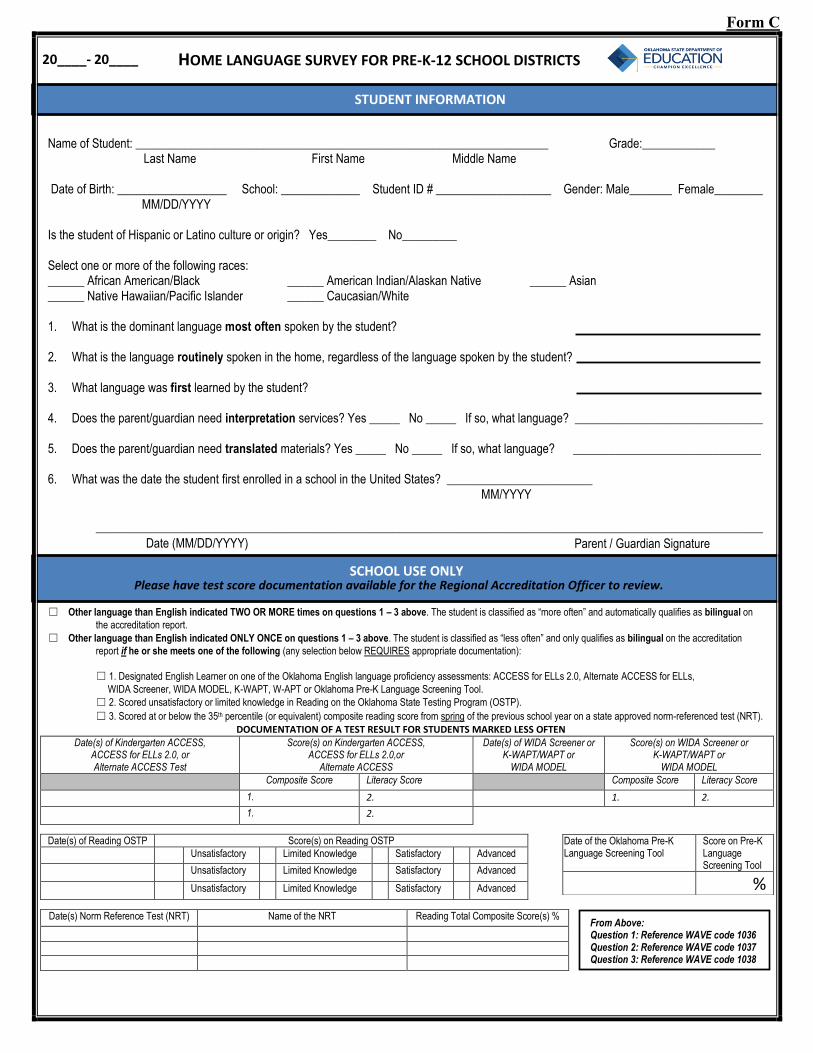
HOME LANGUAGE SURVEY FOR PRE-K-12 SCHOOL DISTRICTS
Name of Student: ____________________________________________________________________ Grade:____________ Last Name First Name Middle Name
Date of Birth: __________________ School: _____________ Student ID # ___________________ Gender: Male_______ Female________ MM/DD/YYYY
Is the student of Hispanic or Latino culture or origin? Yes________ No_________
Select one or more of the following races: ______ African American/Black ______ American Indian/Alaskan Native ______ Asian ______ Native Hawaiian/Pacific Islander ______ Caucasian/White
1. What is the dominant language most often spoken by the student?
2. What is the language routinely spoken in the home, regardless of the language spoken by the student?
3. What language was first learned by the student?
4. Does the parent/guardian need interpretation services? Yes _____ No _____ If so, what language? _______________________________
5. Does the parent/guardian need translated materials? Yes _____ No _____ If so, what language? _______________________________
6. What was the date the student first enrolled in a school in the United States? ________________________ MM/YYYY
______________________________________________________________________________________________________________
☐ Other language than English indicated TWO OR MORE times on questions 1 – 3 above. The student is classified as “more often” and automatically qualifies as bilingual on
the accreditation report.
☐ Other language than English indicated ONLY ONCE on questions 1 – 3 above. The student is classified as “less often” and only qualifies as bilingual on the accreditation
report if he or she meets one of the following (any selection below REQUIRES appropriate documentation):
☐ 1. Designated English Learner on one of the Oklahoma English language proficiency assessments: ACCESS for ELLs 2.0, Alternate ACCESS for ELLs,
WIDA Screener, WIDA MODEL, K-WAPT, W-APT or Oklahoma Pre-K Language Screening Tool.
☐ 2. Scored unsatisfactory or limited knowledge in Reading on the Oklahoma State Testing Program (OSTP).
☐ 3. Scored at or below the 35th percentile (or equivalent) composite reading score from spring of the previous school year on a state approved norm-referenced test (NRT).
DOCUMENTATION OF A TEST RESULT FOR STUDENTS MARKED LESS OFTEN
Date(s) of Kindergarten ACCESS, ACCESS for ELLs 2.0, or Alternate ACCESS Test
Score(s) on Kindergarten ACCESS, ACCESS for ELLs 2.0,or
Alternate ACCESS
Date(s) of WIDA Screener or K-WAPT/WAPT or
WIDA MODEL
Score(s) on WIDA Screener or K-WAPT/WAPT or
WIDA MODEL Composite Score Literacy Score Composite Score Literacy Score
1. 2. 1. 2.
1. 2.
Date(s) of Reading OSTP Score(s) on Reading OSTP
Unsatisfactory Limited Knowledge Satisfactory Advanced
Unsatisfactory Limited Knowledge Satisfactory Advanced
Unsatisfactory Limited Knowledge Satisfactory Advanced
Date(s) Norm Reference Test (NRT) Name of the NRT Reading Total Composite Score(s) %
Date of the Oklahoma Pre-K Language Screening Tool
Score on Pre-K Language Screening Tool
%
20____- 20____
SCHOOL USE ONLY Please have test score documentation available for the Regional Accreditation Officer to review.
STUDENT INFORMATION
Date (MM/DD/YYYY) Parent / Guardian Signature
From Above: Question 1: Reference WAVE code 1036 Question 2: Reference WAVE code 1037 Question 3: Reference WAVE code 1038
Form C
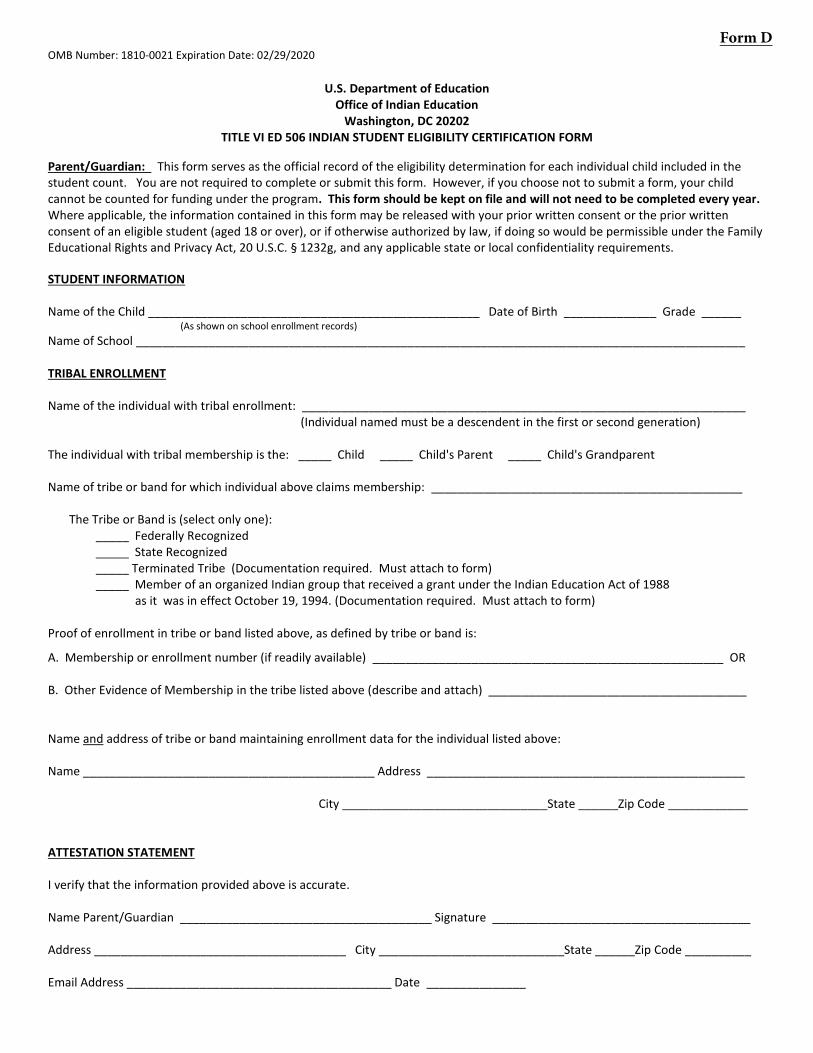
OMB Number: 1810-0021 Expiration Date: 02/29/2020
U.S. Department of Education Office of Indian Education
Washington, DC 20202 TITLE VI ED 506 INDIAN STUDENT ELIGIBILITY CERTIFICATION FORM
Parent/Guardian: This form serves as the official record of the eligibility determination for each individual child included in the student count. You are not required to complete or submit this form. However, if you choose not to submit a form, your child cannot be counted for funding under the program. This form should be kept on file and will not need to be completed every year. Where applicable, the information contained in this form may be released with your prior written consent or the prior written consent of an eligible student (aged 18 or over), or if otherwise authorized by law, if doing so would be permissible under the Family Educational Rights and Privacy Act, 20 U.S.C. § 1232g, and any applicable state or local confidentiality requirements.
STUDENT INFORMATION
Name of the Child __________________________________________________ Date of Birth ______________ Grade ______ (As shown on school enrollment records)
Name of School ____________________________________________________________________________________________
TRIBAL ENROLLMENT
Name of the individual with tribal enrollment: ___________________________________________________________________ (Individual named must be a descendent in the first or second generation)
The individual with tribal membership is the: _____ Child _____ Child's Parent _____ Child's Grandparent
Name of tribe or band for which individual above claims membership: _______________________________________________
The Tribe or Band is (select only one): _____ Federally Recognized _____ State Recognized _____ Terminated Tribe (Documentation required. Must attach to form) _____ Member of an organized Indian group that received a grant under the Indian Education Act of 1988
as it was in effect October 19, 1994. (Documentation required. Must attach to form)
Proof of enrollment in tribe or band listed above, as defined by tribe or band is:
A. Membership or enrollment number (if readily available) _____________________________________________________ OR
B. Other Evidence of Membership in the tribe listed above (describe and attach) _______________________________________
Name and address of tribe or band maintaining enrollment data for the individual listed above:
Name ____________________________________________ Address ________________________________________________
City _______________________________State ______Zip Code ____________
ATTESTATION STATEMENT
I verify that the information provided above is accurate.
Name Parent/Guardian ______________________________________ Signature _______________________________________
Address ______________________________________ City ____________________________State ______Zip Code __________
Email Address ________________________________________ Date _______________
Form D

OMB Number: 1810-0021 Expiration Date: 02/29/2020
INSTRUCTIONS FOR THE ED 506 FORM
FOR APPLICANTS:
PURPOSE: To comply with the requirements in 20 USC 7427(a), which provides that: “The Secretary shall require that, as part of an application for a grant under this subpart, each applicant shall maintain a file, with respect to each Indian child for whom the local educational agency provides a free public education, that contains a form that sets forth information establishing the status of the child as an Indian child eligible for assistance under this subpart, and that otherwise meets the requirements of subsection (b)”.
MAINTENANCE: A separate ED 506 form is required for each Indian child that was enrolled during the count period. A new ED 506 form does NOT have to be completed each year. All documentation must be maintained in a manner that allows the LEA to be able to discern, for any given year, which students were enrolled in the LEA’s school(s) and counted during the count period indicated in the application.
FOR PARENTS/GUARDIANS:
DEFINITION: Indian means an individual who is (1) A member of an Indian tribe or band, as membership is defined by the Indian tribe or band, including any tribe or band terminated since 1940, and any tribe or band recognized by the State in which the tribe or band resides; (2) A descendant of a parent or grandparent who meets the requirements described in paragraph (1) of this definition; (3) Considered by the Secretary of the Interior to be an Indian for any purpose; (4) An Eskimo, Aleut, or other Alaska Native; or (5) A member of an organized Indian group that received a grant under the Indian Education Act of 1988 as it was in effect on October 19, 1994.
STUDENT INFORMATION: Write the name of the child, date of birth and school name and grade level.
TRIBAL ENROLLMENT INFORMATION: Write the name of the individual with the tribal membership. Only one name is needed for this section, even though multiple persons may have tribal membership. Select only one name: either the child, child’s parent or grandparent, for whom you can provide membership information.
Write the name of the tribe or band of Indians to which the child claims membership. The name does not need to be the official name as it appears exactly on the Department of Interior’s list of federally-recognized tribes, but the name must be recognizable and be of sufficient detail to permit verification of the eligibility of the tribe. Check only one box indicated whether it is a Federally Recognized, State Recognized, Terminated Tribe or Organized Indian Group. If Terminated Tribe or Organized Indian Group is elected, additional documentation is required and must be attached to this form.
Federally Recognized- an American Indian or Alaska Native tribal entity limited to those indigenous to the U.S. The Department ofInterior maintains a list of federally-recognized tribes, which OIE can provide you upon request.
State Recognized- an American Indian or Alaska Native tribal entity that has recognized status by a State. The U.S. Department ofEducation does not maintain a master list. It is recommended that you use official state websites only.
Terminated Tribe-a tribal entity that once had a federally recognized status from the United States Department of Interiorand had that designation terminated.
Organized Indian Group- Member of an organized Indian group that received a grant under the Indian Education Act of 1988as it was in effect October 19, 1994.
Write the enrollment number establishing the membership of the child, if readily available, or other evidence of membership. If the child is not a member of the tribe and the child’s eligibility is through a parent or grandparent, either write the enrollment number of the parent or grandparent, or provide other proof of membership. Some examples of other proof of membership may include: affidavit from tribe, CDIB card or birth certificate. Write the name and address of the organization that maintains updated and accurate membership data for such tribe or band of Indians.
ATTESTATION STATEMENT: Provide the name, address and email of the parent or guardian of the child. The signature of the parent or guardian of the child verifies the accuracy of the information supplied.
The Department of Education will safeguard personal privacy in its collection, maintenance, use and dissemination of information about individuals and make such information available to the individual in accordance with the requirements of the Privacy Act.
PAPERWORK BURDEN STATEMENT According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of
information unless such collection displays a valid OMB control number. The valid OMB control number for this information collection is 1810-0021.
The time required to complete this portion of the information collection per type of respondent is estimated to average: 15 minutes per Indian
student certification (ED 506) form; including the time to review instructions, search existing data resources, gather the data needed, and complete
and review the information collection. If you have any comments concerning the accuracy of the time estimate(s) or suggestions for improving this
form, please write to: U.S. Department of Education, Washington, D.C. 20202-4651. If you have comments or concerns regarding the status of your
individual submission of this form, write directly to: Office of Indian Education, U.S. Department of Education, 400 Maryland Avenue, S.W.,
LBJ/Room 3W203, Washington, D.C. 20202-6335. OMB Number: 1810-0021 Expiration Date: 02/29/2020.
Form E REGULATION
PARENTAL AUTHORIZATION FOR STUDENT SELF-ADMINISTRATION OF
INHALED ASTHMA MEDICATION
The undersigned, , (“Parent”) is the parent or legal guardian of , (“Student”) who attends Justice Public School.
By Parent’s signature below, Parent understands and agrees to the following:
1. Parent hereby authorizes Student to self-administer inhaled asthma medication pursuantto the guidelines set forth in District Policy.
2. Parent has read, understands and agrees to the provisions and regulations of DistrictPolicy, Student Self-Administration of Inhaled Asthma Medication, and understands thatviolation of the terms and conditions set forth in that Policy by either Student or Parentmay result in revocation of Student’s permission to self-administer Inhaled asthmamedication at school.
3. Parent has provided to the District a written statement from Student’s physicianindicating that Student has asthma and is capable of, and has been instructed in the propermethod of self-administration of inhaled asthma medication.
4. Parent acknowledges the following statement:
“The District, its employees and agents shall incur no liability as a result of any injury arising from the self-administration of medication by the student.”
5. Parent has read, understands and agrees to the provisions and regulations of DistrictPolicy, Dispensing Medications, and understands that violation of the terms andconditions set forth in that Policy by either Student or Parent may result in revocation ofStudent’s permission to self-administer inhaled asthma medication at school.
6. Parent has been given a copy of District Policy, Student Self-Administration of InhaledAsthma Medication; and a copy of this Parental Authorization form.
(Signature of Parent or Legal Guardian)
(Date)
No medicine shall be administered to students by school personnel unless a form authorizing to administer medicine has been signed by the parent or legal guardian.
Form F
PARENTAL AUTHORIZATION TO ADMINISTER MEDICATION
To: (Principal)
Justice Public School (School)
I am the parent with legal custody or legal guardian of , a student attending this school. This student requires or may require medication at intervals during the school day.
I hereby authorize and give my consent to the employees of Justice Public School (Principal, secretary, homeroom teacher, etc.) to:
Administer a non-aspirin medication which the school will supply, in accordance with the instructions for administering such medication as stated on the original container’s directions.
Administer , a non-prescription medication which I am hereby supplying you or will supply in the original container when required, in accordance with the instructions for administering such medication as stated on the original container’s directions.
Administer , a filled prescription medication which I am hereby supplying you or will supply when required, in accordance with directions for administering the medication as listed on the label on the vial or according to any written instructions of the physician prescribing the medication.
I understand that under state law the Board of Education, the School District, or employees of the District shall not be liable for personal injuries to the student which results from acts or omissions of school employees in administering the medicine I have hereby authorized.
Dated this day of , .
Signature of Parent with Legal Custody or Legal Guardian
Address Signature of Witness

JUSTICE BOARD OF EDUCATION EFBCA-E
Adoption Date: Effective July 1, 2014 Revision Date(s): Page 1 of 1
APPLICATION FOR USE OF INTERNET AND OTHER COMPUTER NETWORKS
The Justice Public School district is pleased to make available to students access to interconnected computer systems within the district and to the Internet, the worldwide network that provides various means of accessing significant educational materials and opportunities. This application must be completed and returned for all personnel, students, and/or guests before access will be granted.
User’s Full Name (Please Print)
Home Address
Home Phone Work Phone
Login I.D. Grade Level/Status
(Will be assigned by network administrator)
I am a: Administrator Teacher Parent
Guest/District Patron Justice Student
Student or Guest Users: I understand and will abide by the above terms and conditions for computer and Internet access. I further understand that any violation of the Justice policy for computer and internet use is unethical and may constitute a criminal offense. Should I commit any violation, my access privileges may be revoked, school and disciplinary and/or appropriate legal action may be taken.
Student/Guest User Signature Date
Parent or Guardian: As the parent or guardian of this student, I have read the terms and conditions for computer and Internet access. I understand that this access is designed for educational purposes and Justice School District and the Oklahoma State Department of Education have taken available precautions to eliminate controversial material. However, I also recognize it is impossible for Justice School District and the Oklahoma State Department of Education to restrict access to all controversial materials and I will not hold Justice School District and the Oklahoma State Department of Education responsible for materials acquired on the network. Further, I accept full responsibility for supervision if and when my child’s use is not in a school setting. I hereby give my permission to grant access for my child and certify that the information contained on the application form is correct.
Parent or Guardian Name (Please Print)
Parent or Guardian Signature Date
Teacher/Employee: I have read the terms and conditions for computer and Internet access. I understand the policy and law regarding computer and Internet use. I agree to instruct the students on acceptable use of the network and proper network etiquette.
Teacher/Employee Signature Date

“Justice Public School: Where Children Think, Dream, Believe and Achieve.”
Concussion and Head Injury Acknowledgement
In compliance with Oklahoma Statute Section 24-155 of Title 70, this acknowledgement form is to confirm that you have read and understand the CONCUSSION FACT SHEET provided to you by Justice Public School related to potential concussions and head injuries during participation in athletics.
I, , as a student-athlete who participates in Justice Public (Student athlete’s name)
School athletics and I, , as the parent/legal guardian, have (Parent/Guardian’s name)
read the information material provided to us by Justice Public School related to concussions and head
injuries occurring during participation in athletic programs and understand the content and warnings.
Signature of Student-Athlete Date
Signature of Parent/Legal Guardian Date
This form should be completed annually prior to the athlete’s first practice and/or competition and be kept on file for one year beyond the date of signature in the principal’s office or the office designated by the principal.

“Justice Public School: Where Children Think, Dream, Believe and Achieve.”
CONCUSSION/HEAD INJURY FACT SHEET FOR PARENTS/GUARDIANS
WHAT IS A CONCUSSION?
A concussion is a brain injury. Concussions are caused by a bump or blow to the head. Even a “ding”, “getting your bell rung” or what seems to be a mild bump or blow to the head can be serious. You cannot see a concussion. Signs and symptoms of a concussion can show up right after the injury or may not appear to be noticed until days or weeks after the injury. If your child reports any symptoms of a concussion or if you notice any symptoms yourself, seek medical attention right away.
WHAT ARE THE SYMPTOMS REPORTED BY ATHLETES? Headache or “pressure” in head Nausea or vomiting Balance problems or dizziness Sensitivity to light Sensitivity to noise Feeling sluggish, hazy, foggy or groggy Concentration or memory problems Confusion Does not “feel right”
WHAT ARE THE SIGNS OBSERVED BY PARENTS/GUARDIANS? Appears dazed or stunned Is confused about assignment or position Forgets an instruction Is unsure of game, score or opponent Moves clumsily Answers questions slowly Loses consciousness (even briefly) Shows behavior or personality changes Cannot recall events prior to hit or fall Cannot recall events after hit or fall
HOW CAN I HELP MY CHILD PREVENT A CONCUSSION? Ensure they follow their coach’s rules for safety and the rules of the sport. Make sure they use the proper equipment, including personal protective equipment (such as helmets, padding, shin
guards and eye and mouth guards----IN ORDER FOR EQUIPMENT TO PROTECT YOU, it must be the rightequipment for the game, position and activity; it must be worn correctly and used every time you play.)
Learn the signs and symptoms of a concussion.
FOR MORE INFORMATION VISIT: www.cdc.gov/TraumaticBrainInjury/ www.oata.net www.ossaa.com www.nfhslearn.com
IT’S BETTER TO MISS ONE GAME THAN THE WHOLE SEASON!
“Justice Public School: Where Children Think, Dream, Believe and Achieve.”
CONCUSSION/HEAD INJURY FACT SHEET FOR STUDENT-ATHLETES
WHAT IS A CONCUSSION? A concussion is a brain injury Is caused by a bump or blow to the head Can change the way your brain normally works Can occur during practice or games in any sport Can happen even if you have not been knocked out Can be serious even if you have just been “dinged”
WHAT ARE THE SYMPTOMS REPORTED BY ATHLETES? Headache or “pressure” in head Nausea or vomiting Balance problems or dizziness Sensitivity to light Sensitivity to noise Feeling sluggish, hazy, foggy or groggy Concentration or memory problems Confusion Does not “feel right”
WHAT SHOULD I DO IF I THINK I HAVE A CONCUSSION? Tell you coaches or parents. Never ignore a bump or blow to the head even if you feel fine. Also, tell your coach if
one of your teammates may have a concussion. Get a medical checkup. A doctor or health care professional can tell you if you have a concussion and when you are
OK to return to play. Give yourself time to get better. If you have had a concussion, your brain needs time to heal. While your brain is
still healing, you are much more likely to have a second concussion. Additional concussions can cause damage toyour brain. It is important to rest until you get approval from a doctor or health care professional to return to play.
HOW CAN I PREVENT A CONCUSSION? Follow your coach’s rules for safety and the rules of the sport. Practice good sportsmanship. Use the proper equipment, including personal protective equipment (such as helmets, padding, shin guards and eye
and mouth guards----IN ORDER FOR EQUIPMENT TO PROTECT YOU, it must be the right equipment for thegame, position and activity; it must be worn correctly and used every time you play.)
FOR MORE INFORMATION VISIT: www.cdc.gov/TraumaticBrainInjury/ www.oata.net www.ossaa.com www.nfhslearn.com
IT’S BETTER TO MISS ONE GAME THAN THE WHOLE SEASON!
OK State Department of Health and OK State Department of Education: Sudden Cardiac Arrest Symptoms and Warning Signs Information Sheet and Acknowledgement of Receipt and Review Form. 7/1/2015
Athlete/Parent/Guardian Sudden Cardiac Arrest Symptoms and Warning Signs Information Sheet and
Acknowledgement of Receipt and Review Form
What is sudden cardiac arrest?
Sudden cardiac arrest (SCA) is when the heart stops beating, suddenly and unexpectedly. When this happens, blood stops flowing to the brain and other vital organs. SCA doesn’t just happen to adults; it takes the lives of students, too. However, the causes of sudden cardiac arrest in students and adults can be different. A student’s SCA will likely result from an inherited condition, while an adult’s SCA may be caused by either inherited or lifestyle issues.
SCA is NOT a heart attack. A heart attack may cause SCA, but they are not the same. A heart attack is caused by a blockage that stops the flow of blood to the heart. SCA is a malfunction in the heart’s electrical system, causing the heart to suddenly stop beating.
How common is sudden cardiac arrest in the United States?
While studies have shown sudden cardiac death among young athletes is very uncommon, SCA is the #1 cause of death for student athletes.
Are there warning signs?
Although SCA happens unexpectedly, some people may have signs or symptoms, such as:
fainting or seizures during exercise;
unexplained shortness of breath;
a racing heart;
dizziness;
chest pain with exercise; or
extreme fatigue.
These symptoms can be unclear in athletes, since people often confuse these warning signs with physical exhaustion. SCA can be prevented if the underlying causes can be diagnosed and treated.
What are the risks of practicing or playing after experiencing these symptoms?
There are risks associated with continuing to practice or play after experiencing these symptoms. When the heart stops, so does the blood that flows to the brain and other vital organs. Death or permanent brain damage can occur in just a few minutes. Most people who experience SCA die from it.
OK State Department of Health and OK State Department of Education: Sudden Cardiac Arrest Symptoms and Warning Signs Information Sheet and Acknowledgement of Receipt and Review Form. 7/1/2015
2
Can you screen for cardiac abnormalities?
The annual sports preparticipation physical examination includes a personal and family health history to screen for symptoms or warning signs of SCA.
An electrocardiogram (ECG) and echocardiogram (ECHO) are noninvasive and painless options. However, these procedures are not currently advised by the American Academy of Pediatrics and the American College of Cardiology unless the preparticipation examination reveals an indication for these tests.
Senate Bill 239 – The Chase Morris Sudden Cardiac Arrest Prevention Act (the Act)
The Act is intended to address any sport sanctioned and offered in grades 7 through 12 by a school district in order to keep student-athletes safe while practicing or playing. The requirements of the act are:
All student-athletes and their parents or guardians must read and sign this form. It mustbe returned to the school before participation in any athletic activity. A new form must besigned and returned each school year.
Schools may also hold informational meetings. The meetings can occur before eachathletic season. Meetings may include student-athletes, parents, coaches and schoolofficials. Schools may also want to include doctors, pediatric cardiologists and athletictrainers.
In order to coach an athletic activity, coaches are required once each year to completean approved SCA training course offered by a provider approved by the Oklahoma StateDepartment of Health.
Removal from play/return to play
Any student who collapses or faints without a concurrent head injury while participatingin an athletic activity shall be removed by the coach from participation at that time.
Any student who is removed or prevented from participating in an athletic activity shallnot return to participation until the student is evaluated and cleared for return toparticipation in writing by a health care provider. Health care provider is defined as aperson who is licensed, certified, or otherwise authorized by the laws of this state topractice a health care or healing arts profession or who administers health care in theordinary course of business (such as a physician, physician assistant, advanced practicenurse, or cardiologist).
OK State Department of Health and OK State Department of Education: Sudden Cardiac Arrest Symptoms and Warning Signs Information Sheet and Acknowledgement of Receipt and Review Form. 7/1/2015
Athlete/Parent/Guardian Sudden Cardiac Arrest Symptoms and Warning Signs
___________________________________________ (NAME OF SCHOOL)
I have reviewed the Athlete/Parent/Guardian Sudden Cardiac Arrest Symptoms (SCA) and
Warning Signs informational material jointly developed by Oklahoma State Department of
Health and the Oklahoma State Department of Education and understand the symptoms and
warning signs of SCA related to participation in athletic programs.
______________________________ ______________________________ ____________ Signature of Student-Athlete Print Student-Athlete’s Name Date
______________________________ ______________________________ ____________ Signature of Parent/Guardian Print Parent/Guardian’s Name Date
This form is required to be completed annually prior to the athlete’s first practice and/or competition and be kept on file for one year beyond the date of signature in the principal’s office or the office designated by the principal.
JUSTICE PUBLIC SCHOOL


















