Pitfalls of CT Angiography for Acute Stroke Imaging Assessment

Stroke Mimics
Paul Guyler
Consultant Stroke Physician at Southend University Hospital
Clinical Lead for Acute Stroke – Essex Cardiac and Stroke Network
Aims • Why worry?
• Stroke Recognition Tools
• History, Examination and imaging
• Defining an approach to acute neurological symptoms
• FAST +ve Mimics
• FAST –ve Strokes
• FAST –ve Mimics
• Non-acute stroke presentations
Distinguishing stroke from mimics
Diagnostic inaccuracy approx 25%
Similar error rate for trained paramedics, A+E and GPs1
Risk of patient being inappropriately thrombolysed
Risk of patient not being given correct treatment promptly2
1Azzimondi et al Stroke 1997
2 Harbison et al Stroke 2003

Pathway activation by A+E
Age 8%
>3hrs 4%
No Time Line 10%
Non Stroke 23%
ICH/SAH 15%
Too severe 4%
Too Mild/TIA 15%
TPA 17%
Other Exclusion 4%
101 cases assessed in A+E, Leeds General Infirmary 1/7/2007-31/10/2008
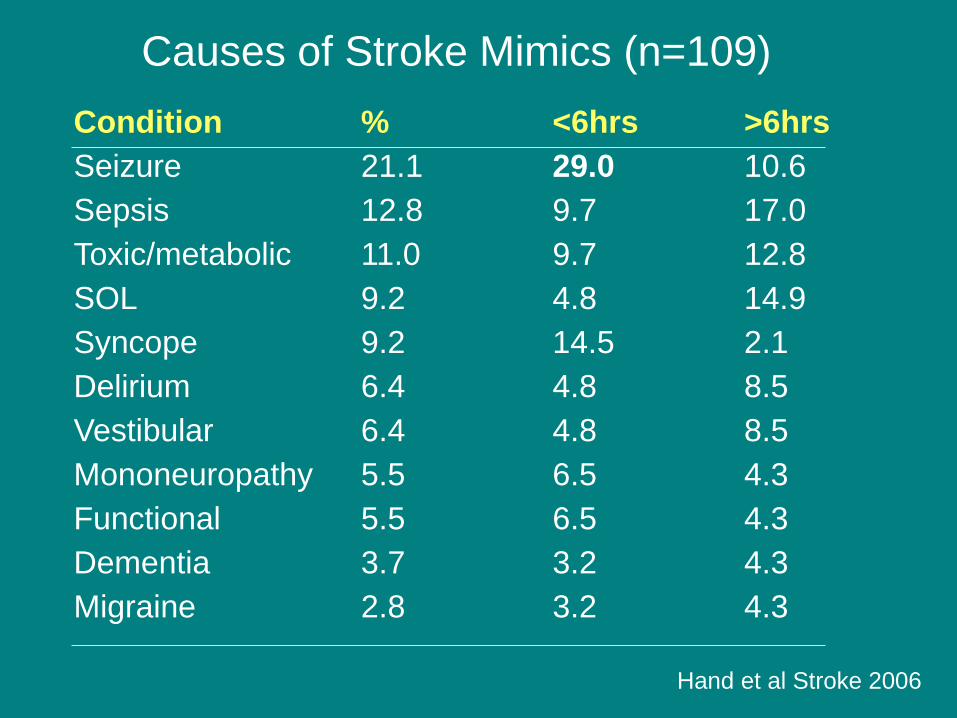
Causes of Stroke Mimics (n=109)
Condition % <6hrs >6hrs
Seizure 21.1 29.0 10.6
Sepsis 12.8 9.7 17.0
Toxic/metabolic 11.0 9.7 12.8
SOL 9.2 4.8 14.9
Syncope 9.2 14.5 2.1
Delirium 6.4 4.8 8.5
Vestibular 6.4 4.8 8.5
Mononeuropathy 5.5 6.5 4.3
Functional 5.5 6.5 4.3
Dementia 3.7 3.2 4.3
Migraine 2.8 3.2 4.3
Hand et al Stroke 2006

Causes of Stroke Mimics (n=109)
Condition % <6hrs >6hrs
Seizure 21.1 29.0 10.6
Sepsis 12.8 9.7 17.0
Toxic/metabolic 11.0 9.7 12.8
SOL 9.2 4.8 14.9
Syncope 9.2 14.5 2.1
Delirium 6.4 4.8 8.5
Vestibular 6.4 4.8 8.5
Mononeuropathy 5.5 6.5 4.3
Functional 5.5 6.5 4.3
Dementia 3.7 3.2 4.3
Migraine 2.8 3.2 4.3
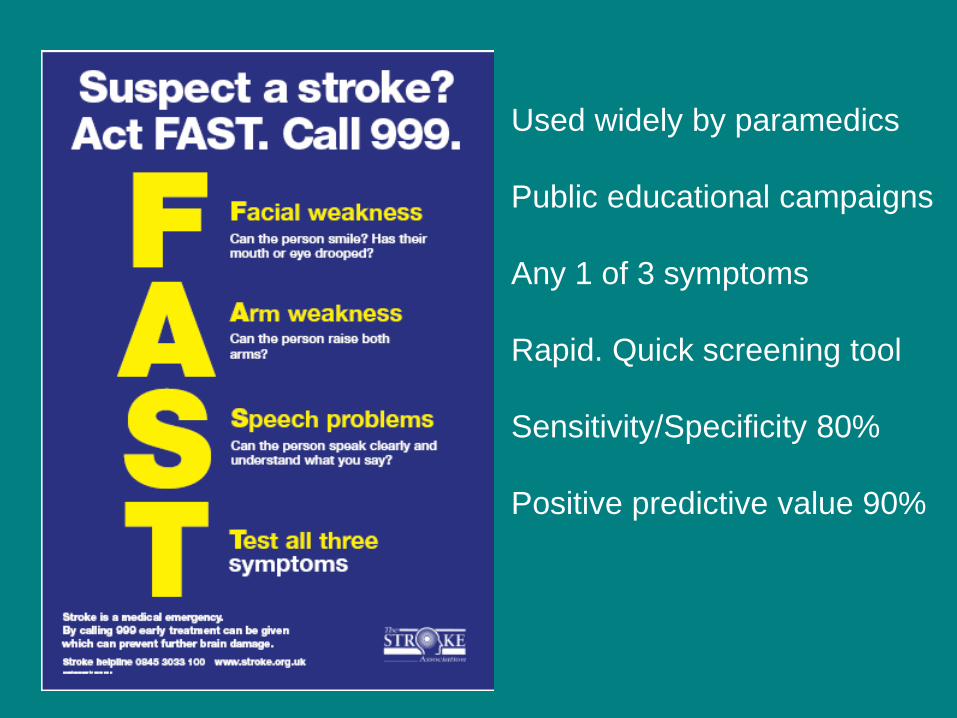
Used widely by paramedics
Public educational campaigns
Any 1 of 3 symptoms
Rapid. Quick screening tool
Sensitivity/Specificity 80%
Positive predictive value 90%
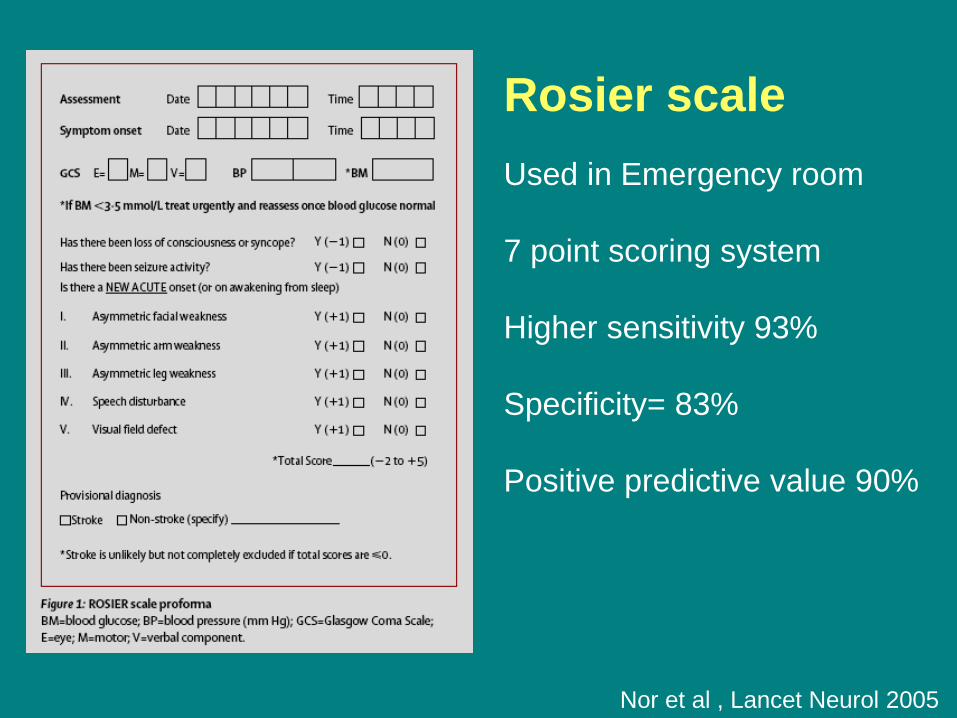
Rosier scale
Used in Emergency room
7 point scoring system
Higher sensitivity 93%
Specificity= 83%
Positive predictive value 90%
Nor et al , Lancet Neurol 2005
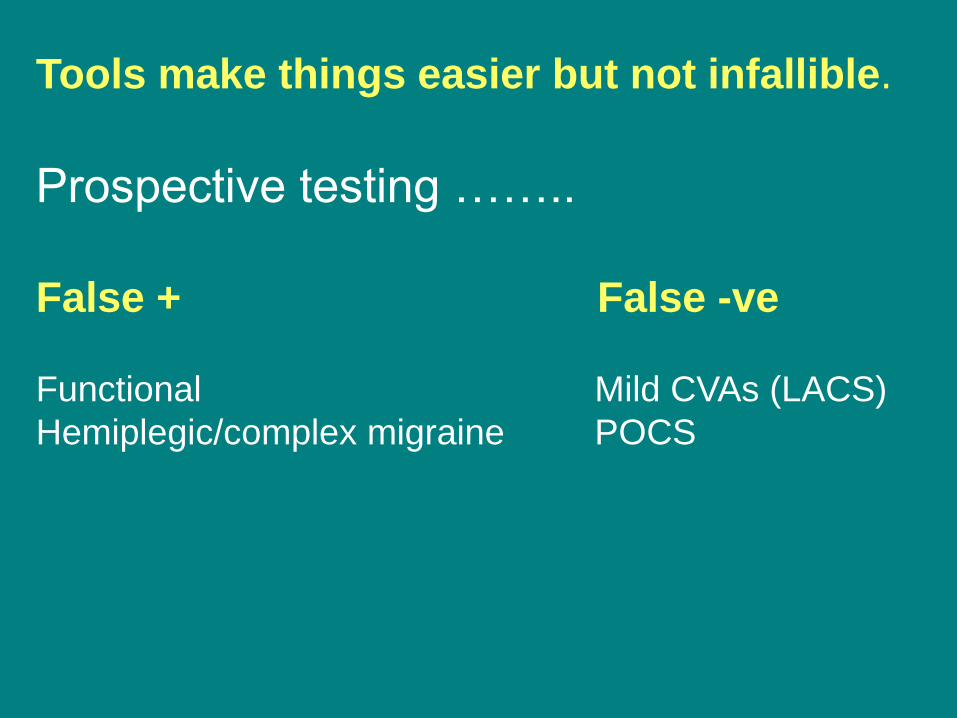
Tools make things easier but not infallible.
Prospective testing ……..
False + False -ve Functional Mild CVAs (LACS)
Hemiplegic/complex migraine POCS

Tools make things easier but not
infallible. FAST +
ve
FAST -
ve
The classic mimic
FALSE
POSITIVES
FAST –ve strokes
FALSE
NEGATIVES
Strokes Non-strokes
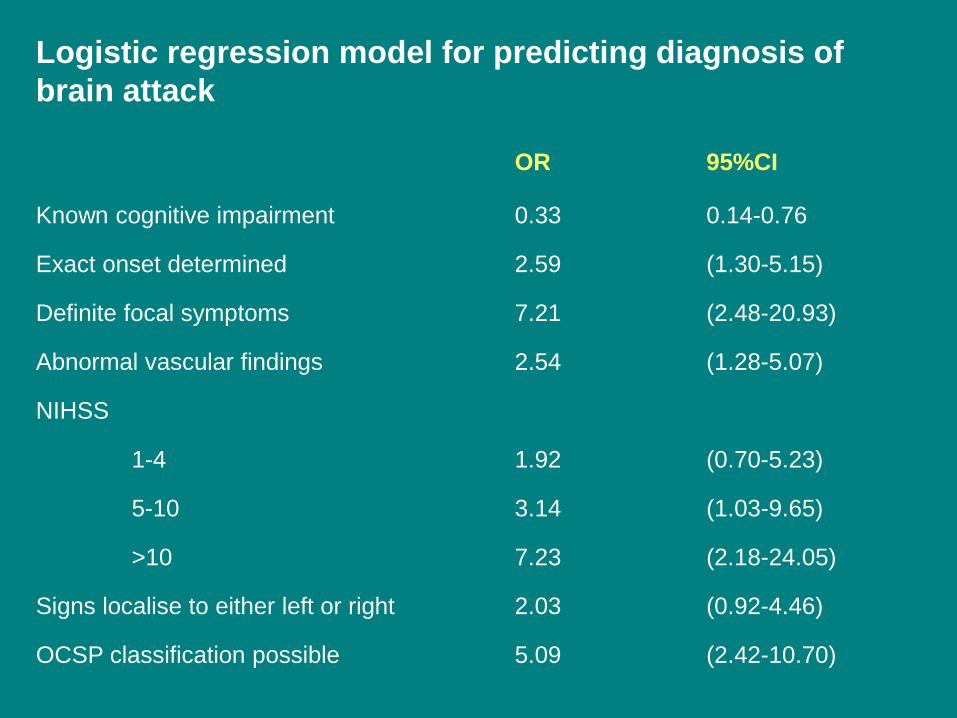
Logistic regression model for predicting diagnosis of
brain attack
OR 95%CI
Known cognitive impairment 0.33 0.14-0.76 Exact onset determined 2.59 (1.30-5.15) Definite focal symptoms 7.21 (2.48-20.93) Abnormal vascular findings 2.54 (1.28-5.07) NIHSS 1-4 1.92 (0.70-5.23) 5-10 3.14 (1.03-9.65) >10 7.23 (2.18-24.05) Signs localise to either left or right 2.03 (0.92-4.46) OCSP classification possible 5.09 (2.42-10.70)

Hyperacute radiology for stroke mimic Non contrast CT widely available
Limited role, often normal
Early infarct signs confirm clinical suspicion of stroke
Rarely non stroke neurological mimics seen e.g. SOL
Rarely clarifies clinical picture, if diagnostic confusion
from outset (advanced imaging more useful)
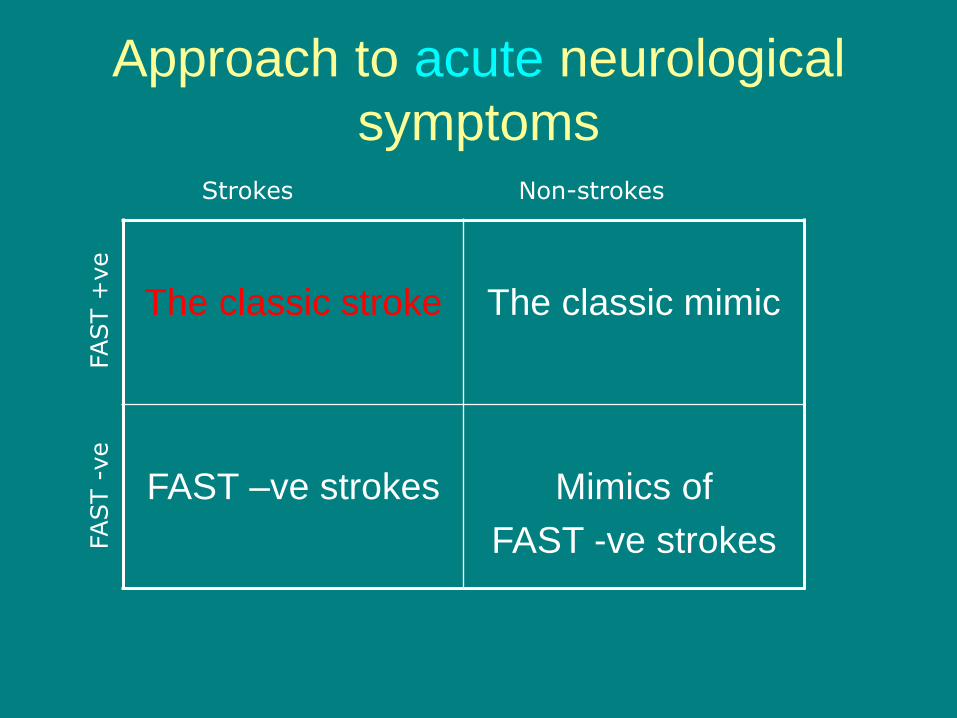
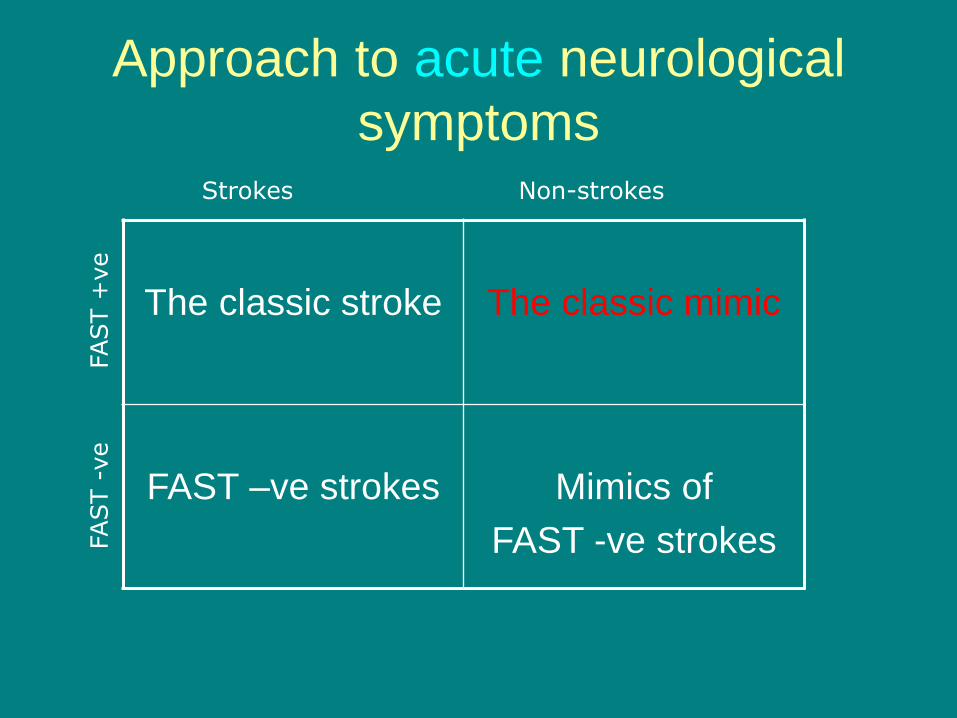
Approach to acute neurological
symptoms FAST +
ve
FAST -
ve
The classic stroke
The classic mimic
FAST –ve strokes
Mimics of
FAST -ve strokes
Strokes Non-strokes
61 M

Approach to acute neurological
symptoms FAST +
ve
FAST -
ve
The classic stroke
The classic mimic
FAST –ve strokes
Mimics of
FAST -ve strokes
Strokes Non-strokes

FAST +ve mimics
• Hypoglycemia
• Migraine with/without aura / Hemiplegic Migraine
• Post-ictal paralysis
• Brain Tumours
• Intracerebral haemorrhage
• Subarachnoid hemorrhage
• Subdural haemorrhage
• Cervical spondylotic myelopathy
• Venous infarction
• Hypertensive encephalopathy
• Functional hemiparesis
• Others!
Hypoglycemia
(Fast +ve mimic)
• Adrenergic symptoms/signs can be absent
• Neuroglycopenia
– Hemiplegia
– Quadreplegic
– brainstem signs
• Signs usually reverse after glucose
• Could lead to permanent neurological sequelae
Ravid JM: Transient insulin hypoglycemic hemiplegias. Am J Med Sci 1928;175:756-759

ROSIER SCALE
Migraine with/without aura
• 2.0-2.5 increase in stroke risk
• Strokes can mimic migraine!
• Neurological disturbance is almost always
transient.
Differentiating stroke/TIA from migraine
• Focal symptoms precede headache & are usually +ve
• Note headache seen in up to 50% of TIAs; seen at onset, usually ipsilateral & non-severe1
• Usually visual fortification spectra, hemianopia, perioral tingling & tingling in 1 arm, occ. dysphasia
• Often march over ~15 mins.
1. Chaturvedi et al. Transient ischaemic attacks. Blackwell, 2004

Hemiplegic Migraine
(FAST+ve mimic)
• Watch for the typical ‘march’ of symptoms
• Usual duration of neurological symptoms is 30 minutes to up to 2 hours
• Headaches could be ipsilateral or contralateral
• In this familial variety, neurological signs could become permanent – Frank hemiplegias
– ataxia and other cerebellar signs
– coma
Post-ictal paralysis (Fast +ve mimic)
• Lasts under 24 hours; rarely longer
• The residual neurology strongly points to the
origin of the epileptic focus
• In up to 15% of the epileptic attacks
– Mono or hemiplegia
– aphasia
– gaze deviation
– hemianopia
Brain Tumours
(FAST +ve mimic)
Tumours can cause transient neurological symptoms lasting minutes or indeed permanent There are symptoms which are acute by nature eg Dysphasia, diplopia, dysphagia Remember, without a contrast CT scan, metastasis and tumours can appear like infarcts Remember symptoms relating to the tumour oedema can resolve well with steroids (temporarily).

NE CT
CE CT
67 M
NE CT
CE CT

55 F
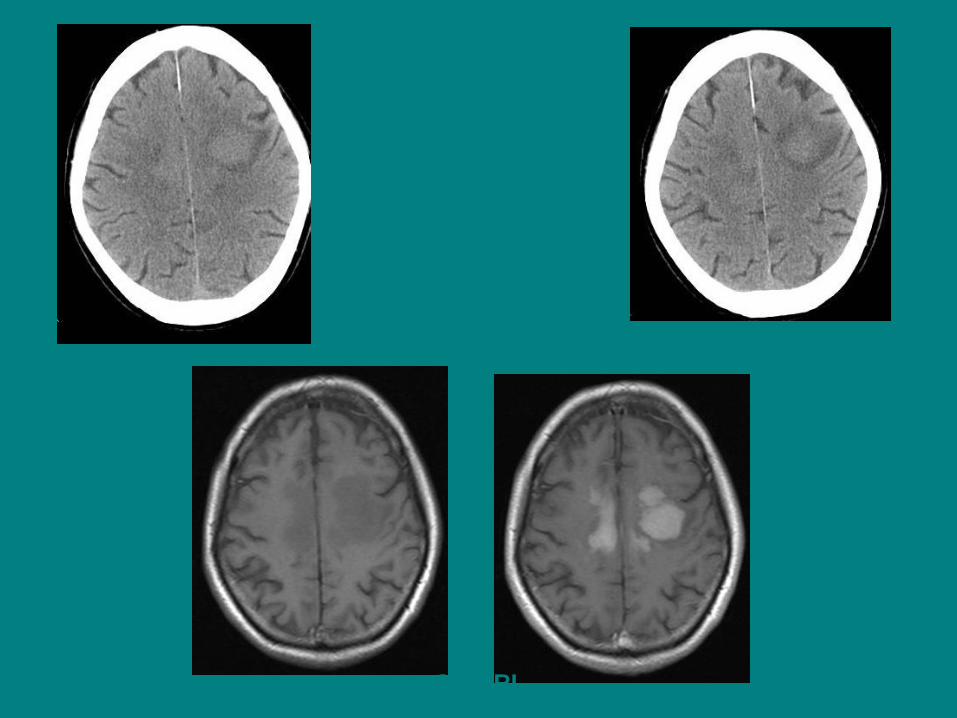
55 F
CE MRI
NE CT
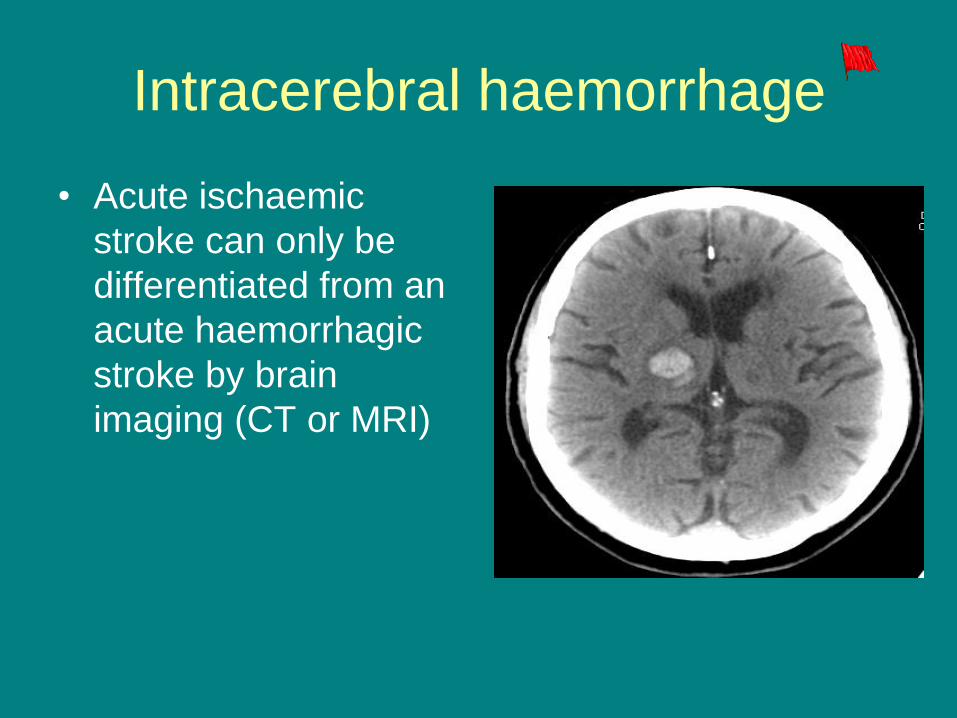
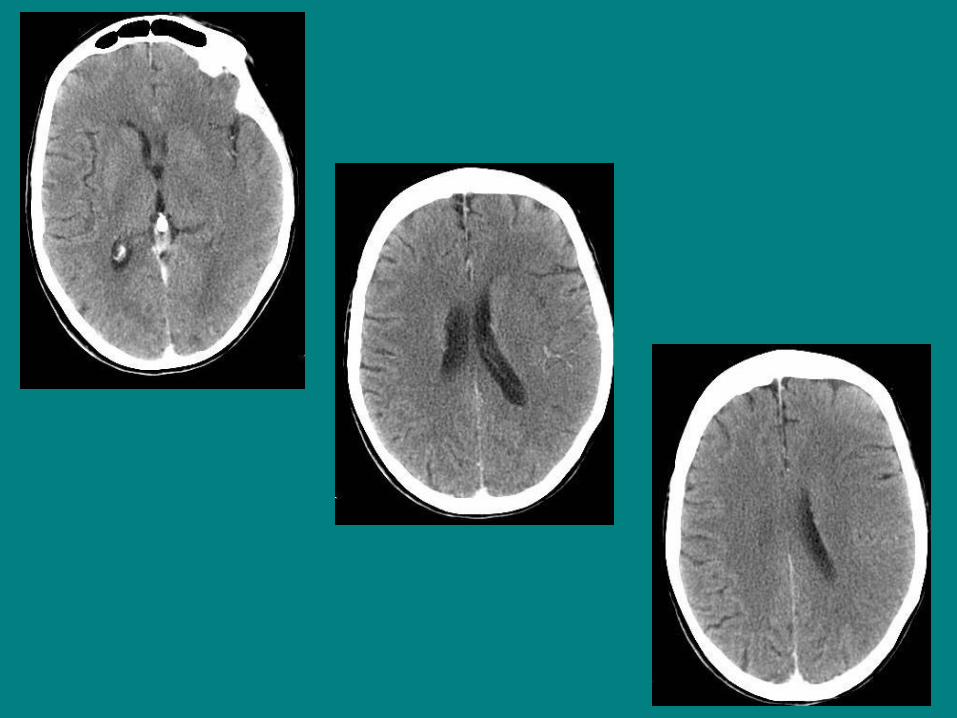
Intracerebral haemorrhage
• Acute ischaemic
stroke can only be
differentiated from an
acute haemorrhagic
stroke by brain
imaging (CT or MRI)
48 F
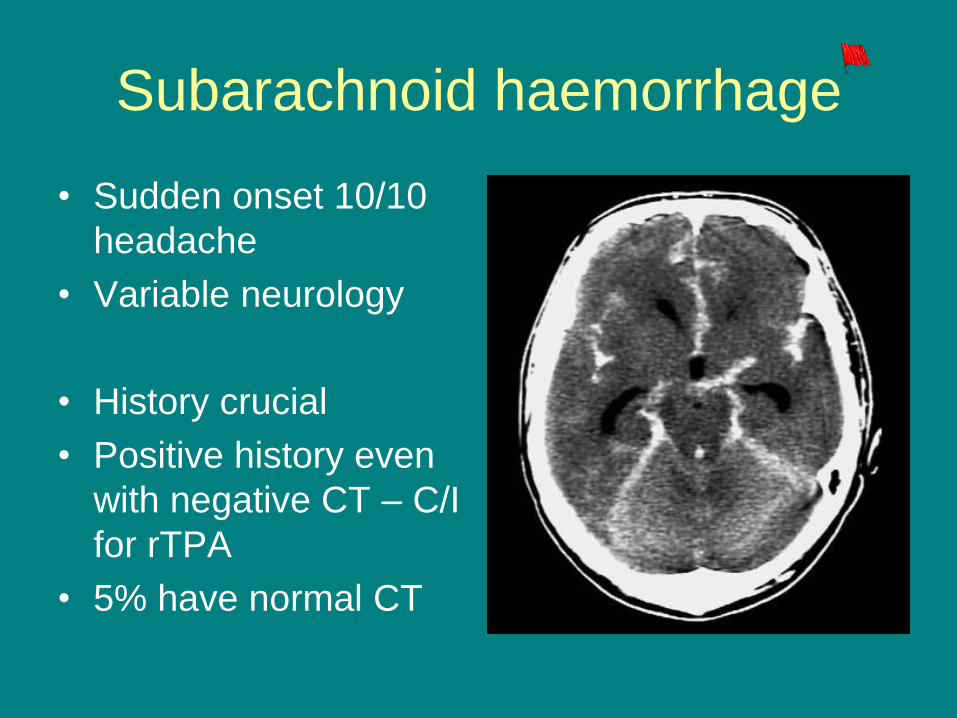
Subarachnoid haemorrhage
• Sudden onset 10/10
headache
• Variable neurology
• History crucial
• Positive history even
with negative CT – C/I
for rTPA
• 5% have normal CT

48 F – Acute Headache,disoriented
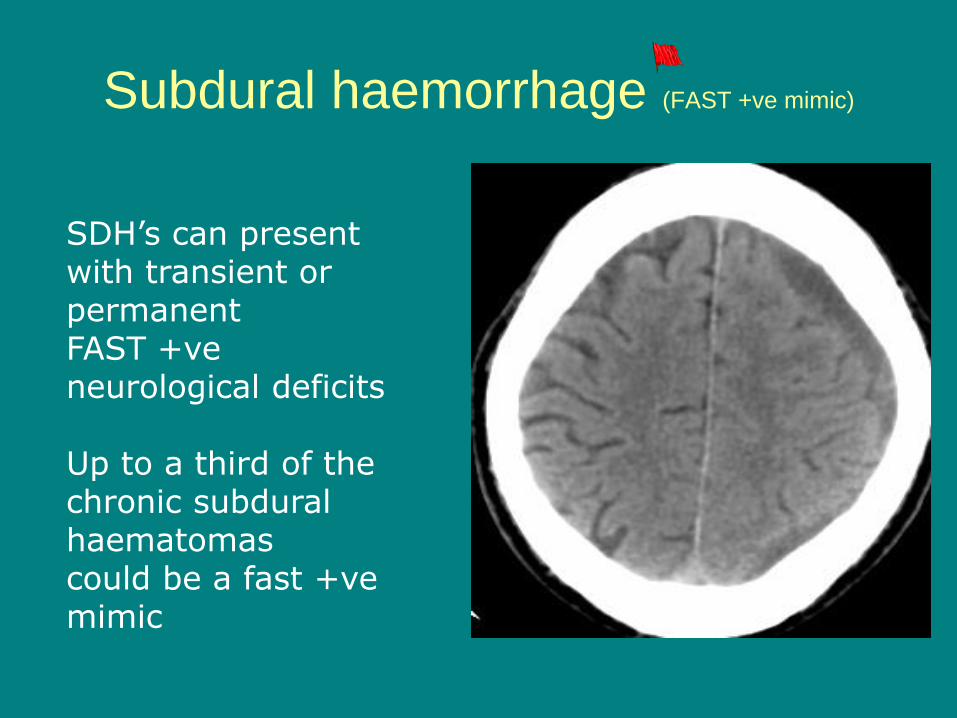
Subdural haemorrhage (FAST +ve mimic)
SDH’s can present with transient or permanent FAST +ve neurological deficits Up to a third of the chronic subdural haematomas could be a fast +ve mimic
73 YRS
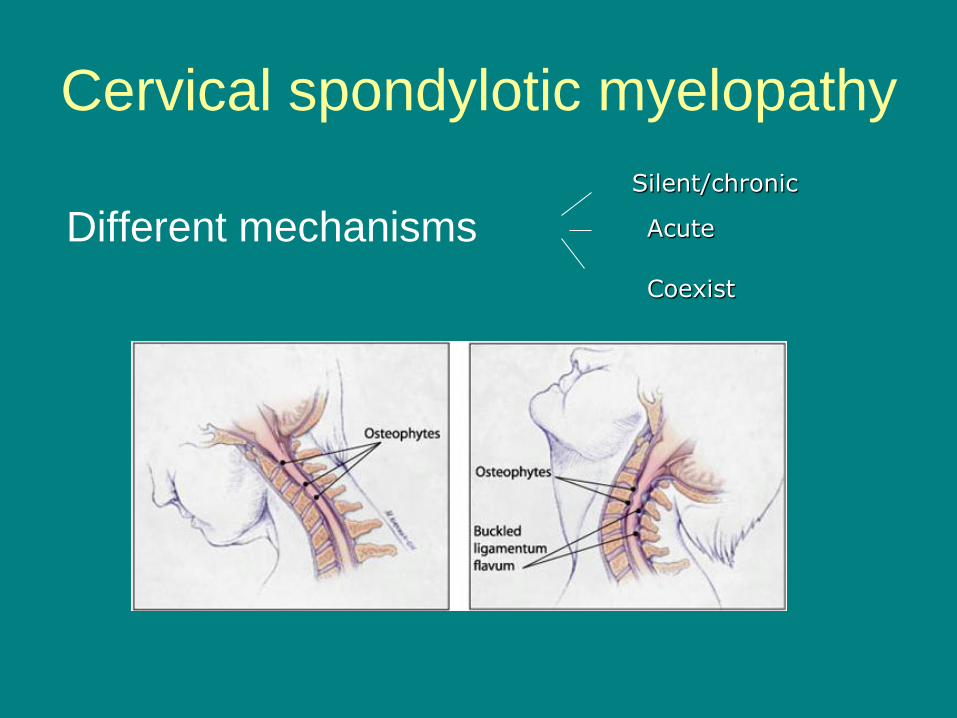
Cervical spondylotic myelopathy
Different mechanisms
Silent/chronic
Acute
Coexist
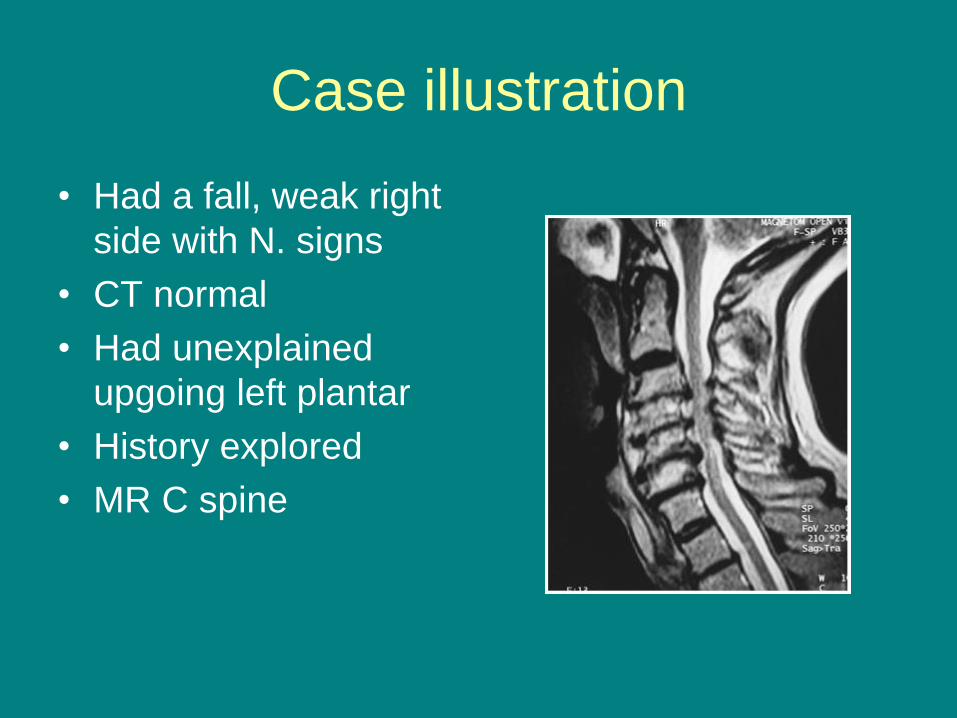
Case illustration
• Had a fall, weak right
side with N. signs
• CT normal
• Had unexplained
upgoing left plantar
• History explored
• MR C spine
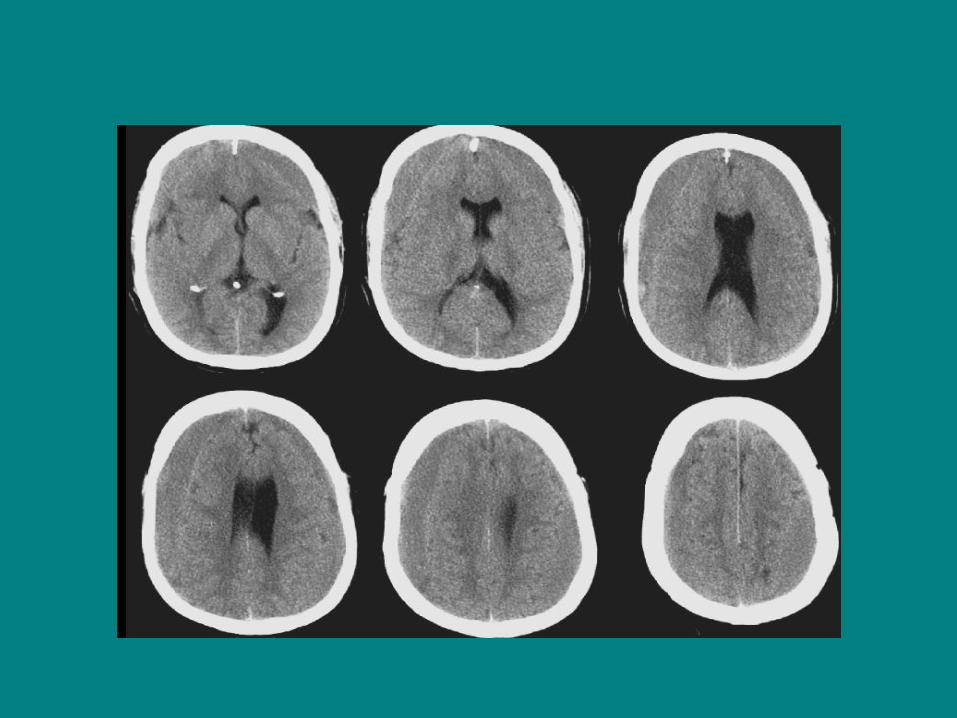
VENOUS INFARCTION
• Think about it!
• On CT be suspicious if see bilateral low
densities or low density in non-arterial
distribution. NB temporal lobe.
• Look for high attenuation thrombus on non
contrast CT scan
• Can confirm with enhanced scan or
preferably CTV
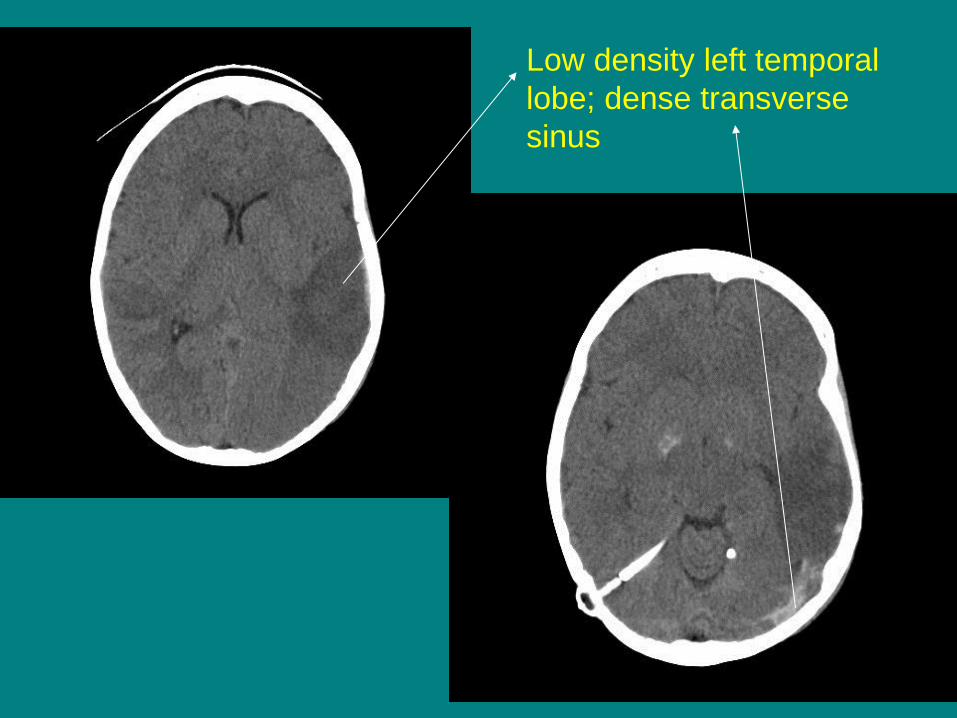
Low density left temporal
lobe; dense transverse
sinus
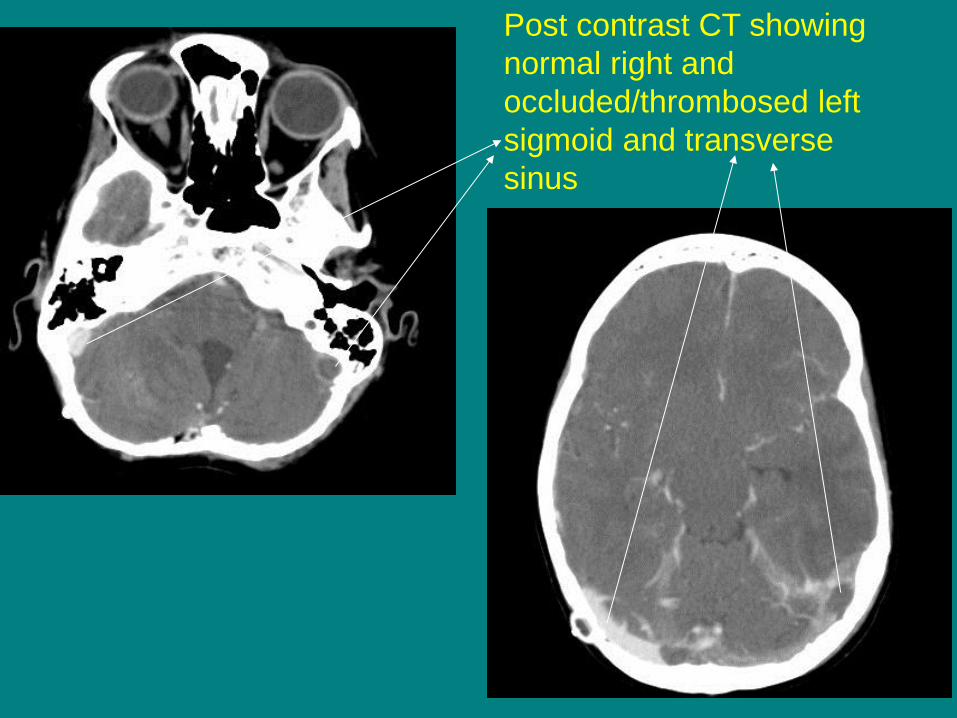
Post contrast CT showing
normal right and
occluded/thrombosed left
sigmoid and transverse
sinus

Hypertensive encephalopathy
(FAST +ve mimic)
• Neurological deficits
– Hemiplegia
– Bilateral clumsiness
– Drowsiness
– Coma
– Bilateral upgoing plantars
• Usually occurs in longstanding
HT
• Imaging may show
abnormalities which disappear
after treatment
• Cautious BP control –
overzealous treatment or
undertreatment can cause
strokes!
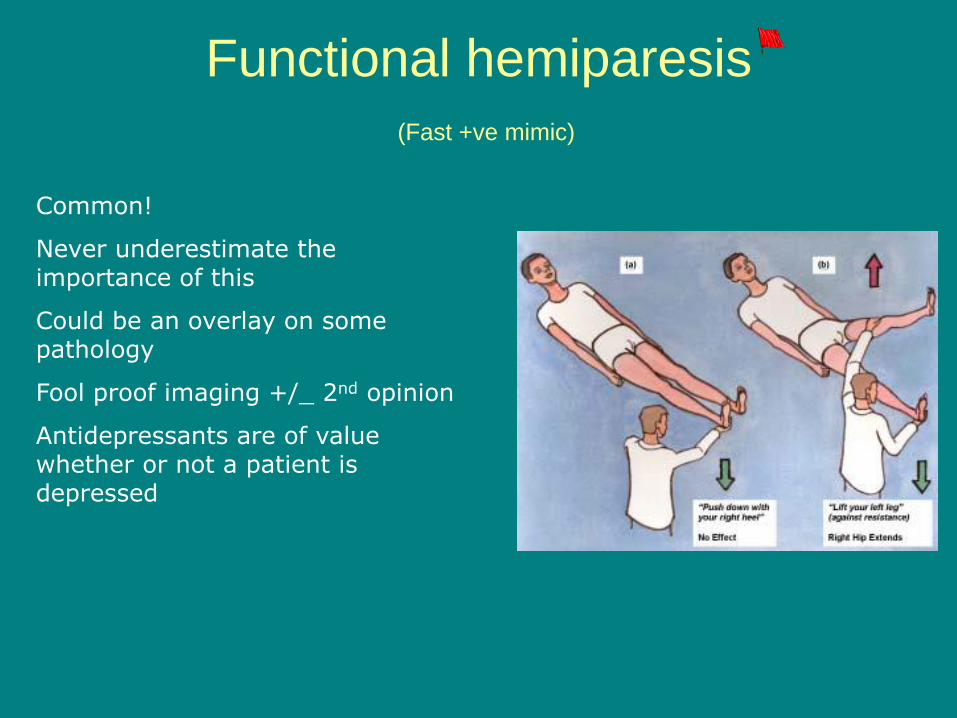
Functional hemiparesis
(Fast +ve mimic)
Common!
Never underestimate the importance of this
Could be an overlay on some pathology
Fool proof imaging +/_ 2nd opinion
Antidepressants are of value whether or not a patient is depressed
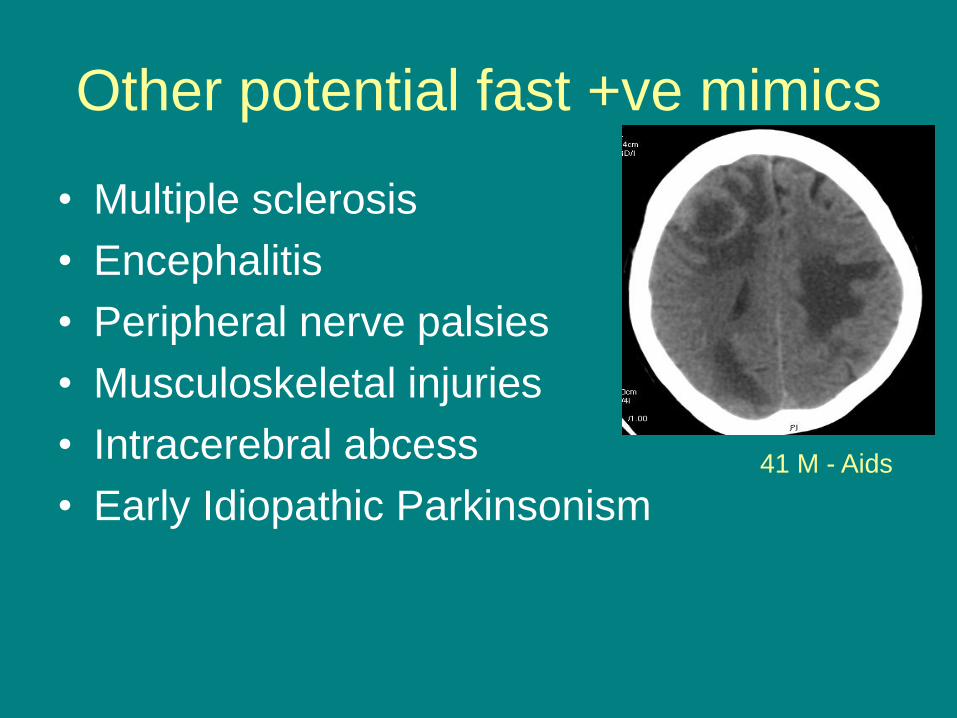
Other potential fast +ve mimics
• Multiple sclerosis
• Encephalitis
• Peripheral nerve palsies
• Musculoskeletal injuries
• Intracerebral abcess
• Early Idiopathic Parkinsonism
41 M - Aids

Approach to acute neurological
symptoms FAST +
ve
FAST -
ve
The classic stroke
The classic mimic
FAST –ve strokes
Mimics of
FAST -ve strokes
Strokes Non-strokes
Fast –ve strokes • Cerebellar strokes
• Occipital infarcts
• Non-dominant parietal lesions
• Sensory strokes
• Frontal infarcts causing just leg weakness
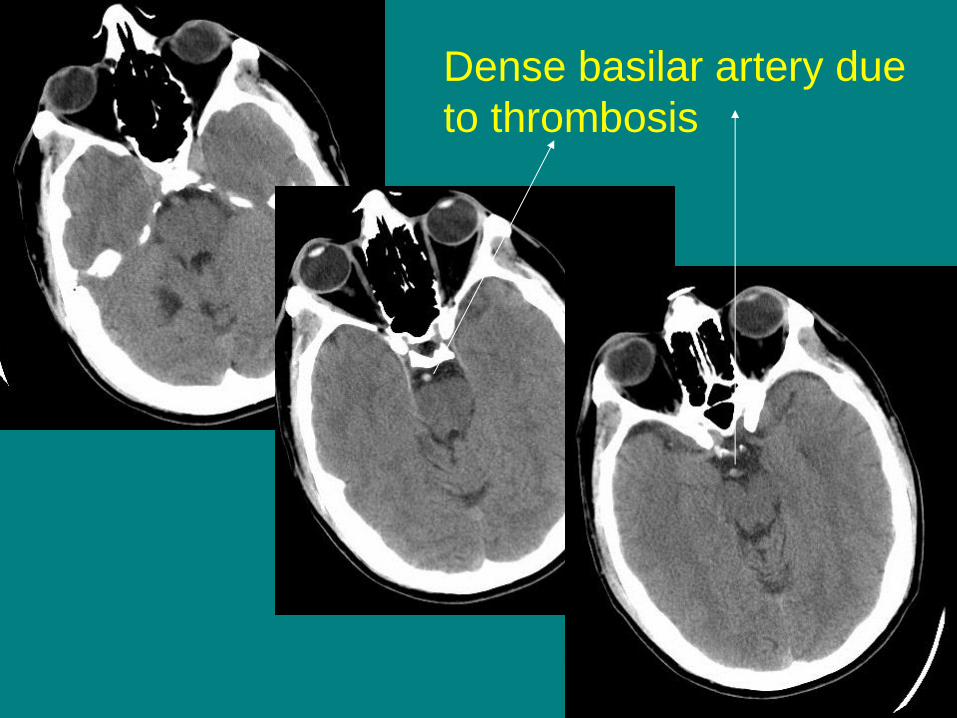
Dense basilar artery due
to thrombosis
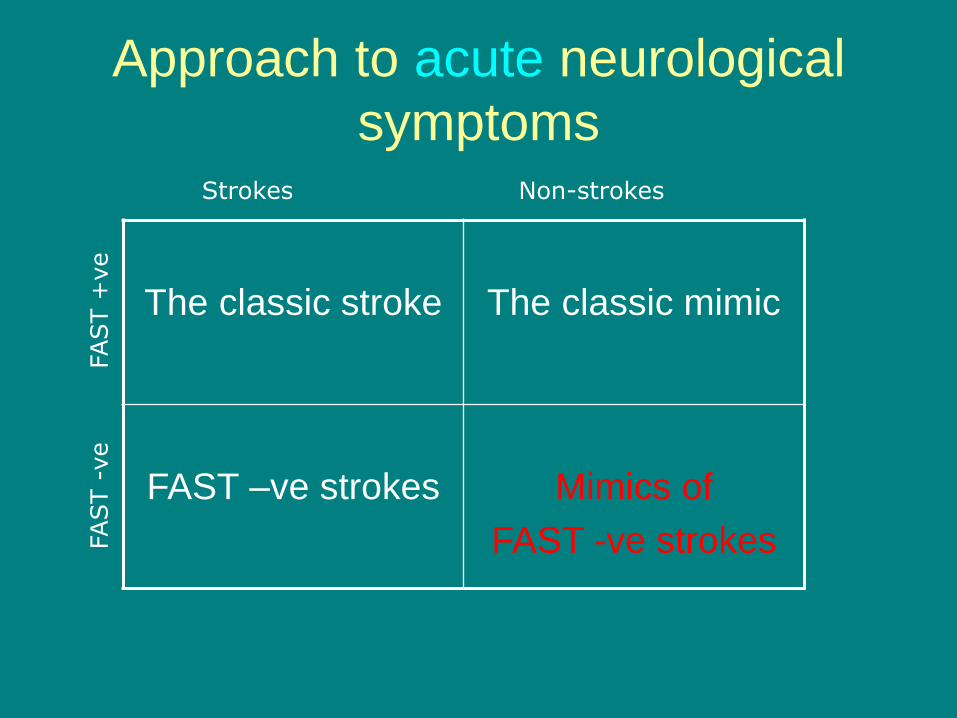
Approach to acute neurological
symptoms FAST +
ve
FAST -
ve
The classic stroke
The classic mimic
FAST –ve strokes
Mimics of
FAST -ve strokes
Strokes Non-strokes
Mimics for FAST-ve strokes
• Vestibular neuronitis
• Falls (ataxia)
• Transient Global amnesia

Transient global amnesia
• Sudden onset, loss of ‘registration’ of events
during the attack and associated loss of
retrograde memory.
• Repetitive questioning a hallmark
• Patients appear confused but personal identity
and intellect preserved

Non-acute stroke presentations • Stuttering/progressive symptoms
Non-acute stroke presentations
• Patient who has a stroke and refuses or
unable to accept it!
• Wrong diagnosis due to pitfalls in
investigations
SUMMARY
• Try and have a logical approach to acute neurological symptoms
• FAST +ve vs FAST –ve
• Good luck!!