STROKE & TIA StR Teaching GIM
66
STROKE & TIA StR Teaching GIM Dr Ijaz M Anwar Stroke Consultant North Tees and Hartlepool NHS Foundation Trust Transforming our services Putting patients first Valuing our people Health and wellbeing
Transcript of STROKE & TIA StR Teaching GIM

STROKE & TIAStR Teaching GIMDr Ijaz M AnwarStroke ConsultantNorth Tees and HartlepoolNHS Foundation Trust
Transforming our services Putting patients first Valuing our people Health and wellbeing

• TIA
• Stroke
• Cases to Illustrate Treatment options
• Stroke Guidelines
Outline of the Talk

Transient Ischaemic AttackWHAT IS IT?
TIA is medical emergency characterised by a sudden onset of focal neurological symptoms and signs resolving rapidly (average of 15 minutes, most < 1 hour), including◦ Unilateral weakness or sensory loss in face or limb(s)◦ Speech disturbance◦ Unilateral visual loss
symptoms and signs have to be completely resolved to diagnose TIA
Loss of consciousness, pre-syncope and isolated dizziness are rarely due to TIA
Note – positive visual phenomena are NOT usually a TIA and suggest a migraine
Around 150,000 people/year have TIA

Risk Score - ABCD2
• Age > 59 years 1 point
• Blood pressure > 139/89 1 point
• Clinical features▫ Focal weakness 2 points▫ Speech disturbance (and no motor weakness) 1 point▫ Sensory or visual features only 0 points
• Duration▫ >59 minutes 2
points▫ 10-59 minutes 1 point▫ <10 minutes 0
points
• Diabetes 1 point


ABCD2 - pitfalls
• Prognostic information from ABCD2 should supplement, not replace -Clinical Judgement
▫ Ipsilateral carotid stenosis
▫ Heart failure and atrial fibrillation
▫ Smoking
▫ Recent MI, known peripheral vascular disease

Take home message
• Now all TIA pts. need to be assessed with in 24 hours
• Pts with AF need risk stratification
• Advise about driving

Stroke
• Facts
• Thrombolysis
• Complications


Blockages and bleeds
• 85% of stroke is due to a “blockage” (infarct)
• Atheroma
• +/- Thrombus
• 15% of stroke is due to a “bleed”
• Atheroma
• Aneurysm (less common)

Stroke- Brain Attack

Time is Brain
• Each minute you wait, you lose close to 1.9 million brain cells
• A pea sized piece of brain dies for every 12 minutes that treatment is delayed

Acute Medical Treatment of Stroke
• Restore Blood Flow– Thrombolytics
– Mechanical devices
• Stroke progression or recurrent thromboembolism
– Anticoagulants
– Antiplatelet agents

Evidence

Inclusion criteria
• Clinical S&S of definite acute stroke
• Clear time of onset
• Presentation within 4 ½ hrs. of acute onset
• Haemorrhage excluded by CT scan
• Age-
• NIHSS – NICE recommendations
• Consent to treat (every effort must be made to
contact next of kin)

Exclusion Criteria
• Rapidly improving or minor stroke symptoms
• Stroke or serious head injury 3 months
• Major surgery, external heart massage last 14 days,
• Seizure at onset of stroke
• Severe haemorrhage last 21/7
• Increase bleeding risk
• History of central nervous damage (neoplasm, haemorrhage, aneurysm, spinal or intracranial surgery or haemorrhagic retinopathy)

Risk Factors



BP• At least half of all heart attacks and strokes are caused by high blood
pressure• Every 10mmHg reduction in systolic blood pressure lowers risk of heart
attack and stroke by 20%• Blood pressure poorly controlled in about 1 out of 3 individuals

BP post stroke


AF and Stroke• AF - five-fold higher risk stroke
• Without preventive treatment, each year approximately 1 in 20 patients(5%) with AF will have a stroke
• The expected prevalence of AF in Northern England 2.65%
• Detected prevalence -1.63 %as at March 2015
• 29.8%of patients are currently undiagnosed.
• The prevalence of AF will likely double over the next few decades with an ageing population
• Over15,300 (20%) strokes per year are potentially attributable to AF
• AF related strokes are more severe than other strokes with an associated 70% increase in in-hospital mortality, 40% reduction in home discharge and 20% increase in length of in hospital stay

CHADS2 vs CHA2DS2VASc

CHADS2 vs CHA2DS2VASc
CHADS2
score
Patients
(n = 1733)
Adjusted
stroke
rate
%/year
0 120 1.9
1 463 2.8
2 523 4.0
3 337 5.9
4 220 8.5
5 65 12.5
6 5 18.2
CHA2DS2-
VASc
score
Patients (n
= 7329)
Adjusted
stroke
rate
(%/year)
0 1 0
1 422 1.3
2 1230 2.2
3 1730 3.2
4 1718 4.0
5 1159 6.7
6 679 9.8
7 294 9.6
8 82 6.7
9 14 15.2
From ESC AF Guidelines: http://www.escardio.org/guidelines-surveys/esc-
guidelines/GuidelinesDocuments/guidelines-afib-FT.pdf

HAS-BLED
26

CHADS VASc / HASBLED
Relation between risk scores and annual event rates of ischaemic stroke and ICH in relation to use of oral anticoagulation
in 159,013 Swedish AF patients followed up for 1.5±1.1 yrs (2005–2008)
CHA2DS2-VASc score
An
nu
al
eve
nt
rate
Score
0 1 2 3 4 5 6 7 8+
Stroke [no OAC]
Stroke [OAC]
ICH [OAC]ICH [no OAC]
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%HAS-BLED score
An
nu
al
eve
nt
rate
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Score
0 1 2 3 4 5+
Stroke [no OAC]
Stroke [OAC]
ICH [OAC]
ICH [no OAC]
*Except those with a very low risk of stroke
Adapted from Friberg et al. Circulation 2012;125:2298–307.

Warfarin (Vitamin K antagonist)• Rat poison!!-1948
• Approved in 1954
• Coumarin derivative -Wisconsin Alumni Research Foundation
• Narrow therapeutic window
28
20
15
10
5
1
Od
ds
Rat
io
1.0 INR2.0 3.0 4.0 5.0 6.0 7.0 8.0
Intracranial bleeding risk
Ischaemic stroke risk
Ischaemic stroke risk
Intracranial bleeding risk

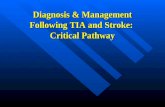
Poor INR control increases the risk of stroke in real-world practice
29
100
90
80
0 20 40 60 80 100
95
85
75
I I I I I I
< 30
31–40
41–50
51–60
61–70
> 70
%TTR
No warfarin
Months
% o
f p
atie
nts
wit
ho
ut
stro
ke
Stroke survival in 37,907 AF patients – UK General Practice Research Database
(27,458 warfarin users and 10,449 not treated with an antithrombotic)
Adapted from Gallagher et al. Thromb Haemost 2011;106:968–77.

NICE Guideline CG180 –Assessing anticoagulation control
• Time in therapeutic range (TTR) at each visit.
• Calculate TTR over a maintenance period of at least 6 months.
• Poor anticoagulation:
-2 INR values higher than 5 or 1 INR value higher
than 8 within the past 6 months
-2 INR values less than 1.5 within the past 6 months
-TTR less than 65%
• Discuss alternatives30

DOACs
• Standard dosing
• All recommended by NICE
• No routine blood tests/ monitoring
• Less Intracranial haemorrhage
• No bridging required
• ?Antidote- Is it needed? -------Idarucizumab
• Non valvular AF
• Not if CrCl <15

Dabigatran Apixaban Edoxaban * Rivaroxaban
Action
Direct
thrombin
inhibitor
Activated
factor Xa (FXa)
inhibitor
Activated factor
Xa (FXa)
inhibitor
Activated
factor Xa
(FXa) inhibitor
Dose150 mg BID
110 mg BID
5 mg BID
2.5 mg BID
60 mg QD
30 mg QD
15 mg QD
20 mg QD
15 mg QD
Phase III
clinical trialRE-LY 1
ARISTOTLE 2
AVERROES 3ENGAGE-AF 4 ROCKET-AF 5

Case - 1
• M,67yrs,
• No history from patient
• Found collapsed in the his house at 11.30AM
• Ambulance arrived at the seen at 11.50AM
• Found to have right sided dense weakness and patient was not speaking & drowsy.
• Brought into the A&E at 12.04 PM

On examination
• BP 165/78
• Pulse 82
• SpO2 100%on air
• BMs 7.3mmol
• CVS – S1 & S2 normal, no murmurs
• RS – Clear breath sounds

• CNS-
– CN- Rt.7th UMN Type Palsy
– Visual & sensory neglect on Rt.sided
– Motor – Right power 0/5
– Speech – expressive Dysphasia
– Plantar Rt.upgoing
• Had CT head at 12.47
• Bloods-Normal
• ECG – NSR
• NIHSS - 18


TPA -Infusion
• 0.9mg/kg/body weight, up to a maximum of 90mg
• Diluted with sterile water to 1mg/ml
• 10% of infusion as bolus
• 90% as infusion using syringe pump over 1 hour.

Effectiveness of Thrombolysis• 10% get significantly better
• 20% receive some benefit
• 10% have IC haemorrhage (variable)
• 3% get worse with significant bleed

RCP Guidelines 2016
• 3.5.1 Recommendations• A Patients with acute ischaemic stroke, regardless of age or stroke severity, in whom treatment• can be started within 3 hours of known onset should be considered for treatment with• alteplase.• B Patients with acute ischaemic stroke under the age of 80 years in whom treatment can be• started between 3 and 4.5 hours of known onset should be considered for treatment with• alteplase.• C Patients with acute ischaemic stroke over 80 years in whom treatment can be started• between 3 and 4.5 hours of known onset should be considered for treatment with alteplase• on an individual basis. In doing so, treating clinicians should recognise that the benefits of• treatment are smaller than if treated earlier, but that the risks of a worse outcome, including• death, will on average not be increased.• D Patients with acute ischaemic stroke otherwise eligible for treatment with alteplase should have
BP<185

Post Thrombolysis

Progress
• Discharged home after 8 days
• Normal swallow
• Mild expressive dysphasia
• Walking with one stick and one
• ADLs with assistance
• Continent
• Note:7% risk of bleeding, Some times life threatening

Case 2
• 25 Years M
• Found collapsed on Christmas day
• Drowsy
• Left weakness, Inattention
• High NIHSS

CT at 18.35

Thrombolysis
• No improvement
• More drowsy
• Struggling to breath
• ITU involved

CT at 00.25


Malignant MCA Syndrome
• Rapid neurological deterioration due to the effects of space occupying cerebral oedema following middle cerebral artery (MCA) territory stroke.
• Neurological decline is early
• Symptoms usually headache and vomiting
• Radiological evidence of cerebral oedema and mass effect
• The prognosis is generally poor, and death usually occurs as a result of transtentorial herniation and brainstem compression.

Indications for-Decompressive hemicraniectomy
People with middle cerebral artery (MCA) infarctionwho meet all of the criteria should be considered fordecompressive hemicraniectomy. They should bereferred within 24 hours of onset of symptoms andtreated within a maximum of 48 hours

Decompressive Hemicraniectomy for Malignant MCA Syndrome
• Age-
• Stroke in MCA territory
• Severe stroke - NIHSS >15
• Fall in conscious level to drowsy
• Large infarcts on CT(>50%of MCA territory)
-Referral with in 24hr of stroke onset
-Surgery no later than 48hrs of stroke


Case 3
• 67 years Male
• Sudden onset Left sided weakness at 830
• Fit & well on Ramipril for hypertension
• NIHSS 7



Thrombolysis
• CT Showed Dense MCA on the right side
• Thrombolysis started in the meantime
• CTA
• Decision for IA
• Catheter Angio-Right MCA-M1 Clot
• Mechanical Thrombectomy

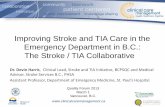
Micro catheter Run Solitaire-AB in position

NIHSS improved from 15 to 3

PRE AND POST

THROMBUS

Progress
• Stroke symptoms resolved
• 24 hour CT-no bleed
• Carotid –no stenosis
• Discharged home day 2
• Back to Normal

• 7 RCTs
• Show increased alive & independent with treatment (but only improvement in mRS)
• Mr CLEAN, ESCAPE, EXTEND IA, SWIFT PRIME, THRACE, REVASCAT, THERAPY
• With & without IV thrombolysis
• Would need service redesign
• Issues re number of interventional neuroradiologists
Intra-arterial thrombectomy

RCP 2016 Guidelines
• 3.4.1 Recommendations• A Patients with suspected acute stroke should be admitted directly to a hyperacute stroke unit• and be assessed for emergency stroke treatments by a specialist physician without delay.• B Patients with suspected acute stroke should receive brain imaging urgently and at most• within 1 hour of arrival at hospital.• C Interpretation of acute stroke imaging for thrombolysis decisions should only be made by• healthcare professionals who have received appropriate training.• D Patients with ischaemic stroke who are eligible for endovascular therapy should have a CT• angiogram from aortic arch to skull vertex immediately. This should not delay the• administration of intravenous thrombolysis.• E MRI with stroke-specific sequences (diffusion-weighted imaging, T2*) should be performed in• patients with suspected acute stroke when there is diagnostic uncertainty

Stroke due to bleed


RCP Recommendation on ICH
• 1-Blood pressure control
• 2 Reversal of anticoagulation

Summary
• Stroke is common
• Recent development are exciting
• Treat TIA early to prevent stroke
• Need to train more interventionists
• Driving advice

Question
Questions?