
STRESS, SPIRITUALITY, COPING, & LIVING WITH HIV · STRESS & RELIGIOUS COPING AMONG PEOPLE LIVING...
24
1 STRESS & RELIGIOUS COPING STRESS & RELIGIOUS COPING AMONG PEOPLE LIVING WITH AMONG PEOPLE LIVING WITH HIV HIV Safiya George Dalmida, PhD Safiya George Dalmida, PhD Emory University Emory University Atlanta, Georgia Atlanta, Georgia OBJECTIVES OBJECTIVES Stress and Coping within PNI Framework Stress and Coping within PNI Framework Spirituality/religion as coping mechanisms Spirituality/religion as coping mechanisms Discuss research on Stress and Religious Discuss research on Stress and Religious Coping in persons with HIV Coping in persons with HIV
Transcript of STRESS, SPIRITUALITY, COPING, & LIVING WITH HIV · STRESS & RELIGIOUS COPING AMONG PEOPLE LIVING...
1
STRESS & RELIGIOUS COPING STRESS & RELIGIOUS COPING AMONG PEOPLE LIVING WITH AMONG PEOPLE LIVING WITH
HIVHIV
Safiya George Dalmida, PhDSafiya George Dalmida, PhDEmory UniversityEmory UniversityAtlanta, GeorgiaAtlanta, Georgia
OBJECTIVESOBJECTIVES
Stress and Coping within PNI FrameworkStress and Coping within PNI FrameworkSpirituality/religion as coping mechanismsSpirituality/religion as coping mechanismsDiscuss research on Stress and Religious Discuss research on Stress and Religious Coping in persons with HIVCoping in persons with HIV

2
Introduction: Introduction: StressStress
Common human experience Common human experience
Negative implications for healthy and Negative implications for healthy and chronically illchronically ill
Stress and HIVStress and HIV
HIV is viewed as a major life stressorHIV is viewed as a major life stressor
Psychosocial issuesPsychosocial issuesloss, bereavement, financial hardship, family or loss, bereavement, financial hardship, family or interpersonal discord, & social isolationinterpersonal discord, & social isolation
Physiological stressors Physiological stressors pain, infection, fever, hypoxia, sleep pain, infection, fever, hypoxia, sleep deprivation, & dehydrationdeprivation, & dehydration

3
Stress and Coping:Stress and Coping:Guiding FrameworksGuiding Frameworks
Lazaras & FolkmanLazaras & FolkmanStress and CopingStress and CopingTheory of psychological stress, building on the Theory of psychological stress, building on the concepts of cognitive appraisal and copingconcepts of cognitive appraisal and coping
Pargament Pargament Psychology of Religion & CopingPsychology of Religion & CopingIntersection of psychology and religionIntersection of psychology and religionRole of religion in copingRole of religion in copingPositive and negative religious coping Positive and negative religious coping
PsychoneuroImmunology (PNI)PsychoneuroImmunology (PNI)Stress and PsychoneuroStress and Psychoneuro--endocrineendocrine--immune processesimmune processes
PsychoNeuroImmunology (PNI)PsychoNeuroImmunology (PNI)
MindMind--Body connectionBody connectionRelationships between neuroendocrine Relationships between neuroendocrine and immune systemsand immune systemsExamines influence of psychosocial factors Examines influence of psychosocial factors on healthon healthStress, depression, social support & coping Stress, depression, social support & coping style can influence systemsstyle can influence systems

4
SpiritSpirit--MindMind--BodyBody& Coping Mechanisms& Coping Mechanisms
Spirituality/spiritual beliefs may function as a Spirituality/spiritual beliefs may function as a coping resource & buffer between stress & coping resource & buffer between stress & the immune system the immune system
Relaxation of an activated SNS may foster Relaxation of an activated SNS may foster enhancement of immune function. enhancement of immune function.
Enhanced ability to cope with stress, better Enhanced ability to cope with stress, better health practices, social support, & greater health practices, social support, & greater satisfaction with life satisfaction with life (Rabin, 1999)(Rabin, 1999)
Buffer between uncertainty & psychological Buffer between uncertainty & psychological wellwell--being being (Landis, 1996)(Landis, 1996)
Spirituality and Coping: Spirituality and Coping: MechanismsMechanisms
Provides feelings of happiness, greater Provides feelings of happiness, greater satisfaction with life, & fewer negative satisfaction with life, & fewer negative psychosocial consequences related to psychosocial consequences related to traumatic life events traumatic life events
Belief in God provides emotional Belief in God provides emotional assurance that results in favorable assurance that results in favorable autonomic responsesautonomic responses
Relaxation and reduction of SNS activity Relaxation and reduction of SNS activity (Rabin, 1999)(Rabin, 1999)
Less response to stressorLess response to stressor--induced catecholamines induced catecholamines

5
Spirituality and Coping in HIVSpirituality and Coping in HIV
HIV disease may require coping beyond HIV disease may require coping beyond what individuals have used in the pastwhat individuals have used in the past
Spirituality provides practical, supportive Spirituality provides practical, supportive resources that facilitate psychological resources that facilitate psychological adaptation adaptation (Simoni et al., 2002; (Simoni et al., 2002; SomlaiSomlai et al., 1996)et al., 1996)
Many HIV+ women use spirituality to cope with Many HIV+ women use spirituality to cope with stress of HIV, mostly when usual coping stress of HIV, mostly when usual coping resources are ineffective resources are ineffective (McCormick et al., 2001; Powell et al., 2003; Sowell et al.,(McCormick et al., 2001; Powell et al., 2003; Sowell et al., 2000; Tuck et al., 2000; Tuck et al., 2000) 2000)
Religious Coping and HIV: Women Religious Coping and HIV: Women
Weaver et al. (2004)Weaver et al. (2004)90 HIV+ (minority) women on HAART 90 HIV+ (minority) women on HAART HIVHIV--specific coping strategies (cognitive specific coping strategies (cognitive coping strategies, denial, and coping strategies, denial, and religious religious copingcoping) and quality of life () and quality of life (QoLQoL))))
PradoPrado and colleagues (2004)and colleagues (2004)HIV+ mothersHIV+ mothersGreater religious involvement, inversely associated Greater religious involvement, inversely associated with psychological distresswith psychological distressSocial support and copingSocial support and coping

6
Religious Coping and HIV: MenReligious Coping and HIV: Men
Sample of gay HIV+ men used spirituality to Sample of gay HIV+ men used spirituality to help them cope with HIV help them cope with HIV Schwartzberg (1993)Schwartzberg (1993)
Woods, Antoni, Ironson, & Kling (1999)Woods, Antoni, Ironson, & Kling (1999)106 HIV+ gay men106 HIV+ gay menReligious copingReligious coping (e.g., placing trust in God, seeking (e.g., placing trust in God, seeking comfort in religion) was significantly associated with comfort in religion) was significantly associated with lower scores on the Beck lower scores on the Beck DepressionDepression Inventory Inventory Religious behaviorReligious behavior was significantly associated with was significantly associated with higher higher CD4CD4+ + countscounts & higher & higher CD4+ percentagesCD4+ percentagesR/t not mediated by selfR/t not mediated by self--efficacy or symptom severity efficacy or symptom severity
Spirituality, Stress, & Social Factors Spirituality, Stress, & Social Factors (SSS) Study: AIMS(SSS) Study: AIMS
CrossCross--sectional study designed to:sectional study designed to:Aim 1: To examine the relationships between Aim 1: To examine the relationships between religious coping (RC), depression, perceived religious coping (RC), depression, perceived stress, immune status, and CD4 count in HIVstress, immune status, and CD4 count in HIV--positive outpatients positive outpatients
Aim 2: To test the idea that religious coping Aim 2: To test the idea that religious coping (RC) explains a significant amount of the (RC) explains a significant amount of the variance in HRQOL and examine mediator variance in HRQOL and examine mediator relationshipsrelationships

7
METHODOLOGYMETHODOLOGY
Data were collected via an audioData were collected via an audio--computer computer assisted interview (ACASI) assisted interview (ACASI) Measures used: Measures used:
Religious copingReligious copingdepressiondepressionhealthhealth--related quality of liferelated quality of lifeHIV medication adherence measure (AGAS)HIV medication adherence measure (AGAS)
Chart DataChart DataCD4 countCD4 countHIV Viral LoadHIV Viral Load
Demographic data were also used Demographic data were also used
MEASURESMEASURESDemographic questionnaireDemographic questionnaire
Center for Epidemiological Studies Depression scale (CESCenter for Epidemiological Studies Depression scale (CES--D)D)
Modified version Religious Coping Index (Koenig, 1994)Modified version Religious Coping Index (Koenig, 1994)
Adapted General Adherence Survey (Holstad et al., 2006)Adapted General Adherence Survey (Holstad et al., 2006)
A Modified version of the Brief Multidimensional Measure of A Modified version of the Brief Multidimensional Measure of Religiousness/Spirituality (BMMRS; Fetzer, 1999)Religiousness/Spirituality (BMMRS; Fetzer, 1999)
Social Support Questionnaire short form (Sarason et al., 1987)Social Support Questionnaire short form (Sarason et al., 1987)
Perceived Stress Scale (Cohen & Williamson,1988)Perceived Stress Scale (Cohen & Williamson,1988)
Short version of the Religious Coping Scale (RCOPE)Short version of the Religious Coping Scale (RCOPE)
Immune status measures: CD4 Cell Count, HIV Viral loadImmune status measures: CD4 Cell Count, HIV Viral load
8
HYPOTHESESHYPOTHESESH1a. There will be an inverse relationship between Positive H1a. There will be an inverse relationship between Positive RCOPE & stress RCOPE & stress H1b. There will be a positive relationship between Negative H1b. There will be a positive relationship between Negative RCOPE & stressRCOPE & stress
H2a. There will be an inverse relationship between Positive H2a. There will be an inverse relationship between Positive RCOPE & depression RCOPE & depression H2b. There will be a positive relationship between Negative H2b. There will be a positive relationship between Negative RCOPE & depression RCOPE & depression
H3.H3. There will be a positive relationship between RCOPE, There will be a positive relationship between RCOPE, and CD4 cell countsand CD4 cell counts
H4.H4. There will be an inverse relationship between depression There will be an inverse relationship between depression (CES(CES--D) and immune status (CD4 counts)D) and immune status (CD4 counts)
HYPOTHESESHYPOTHESES
H5. H5. Religious coping will contribute a significant amount Religious coping will contribute a significant amount of variance to of variance to physical physical HRQOL, beyond what is explained HRQOL, beyond what is explained by depression (CESby depression (CES--D), and immune status, controlling D), and immune status, controlling for med adherence, age and genderfor med adherence, age and gender
H6.H6. Religious coping will contribute a significant amount Religious coping will contribute a significant amount of the variance to of the variance to mental mental healthhealth--related QOLrelated QOL,, beyond beyond what is explained by depression (CESwhat is explained by depression (CES--D), and immune D), and immune status, controlling for medication adherence, age and status, controlling for medication adherence, age and gendergender
H7. H7. Social supportSocial support mediates the relationship between mediates the relationship between RCOPE and HRQOLRCOPE and HRQOL
9
SAMPLESAMPLE
N= 292 N= 292 HIV+ men and women at outpatient ID HIV+ men and women at outpatient ID clinics and AIDS Service organizations in clinics and AIDS Service organizations in Durham, North CarolinaDurham, North Carolina
SAMPLESAMPLE
Eligibility criteria Eligibility criteria HIV+HIV+18 years of age or older18 years of age or olderable to speak and understand Englishable to speak and understand EnglishMentally competent as determined by a health Mentally competent as determined by a health care provider and screening assessment care provider and screening assessment (MMSE)(MMSE)
10
RecruitmentRecruitment
Study flyersStudy flyersClinic nursesClinic nursesPhlebotomistPhlebotomistFront Desk ClerksFront Desk ClerksClinic ProvidersClinic ProvidersWordWord--ofof--mouthmouth
Data Analysis PlanData Analysis Plan
Descriptive statisticsDescriptive statisticsCorrelationsCorrelationsTT--tests/ Multivariate ANOVA test mean tests/ Multivariate ANOVA test mean differences on select measures between differences on select measures between men and women & racial/ethnic groupsmen and women & racial/ethnic groupsMultiple RegressionMultiple Regression
11
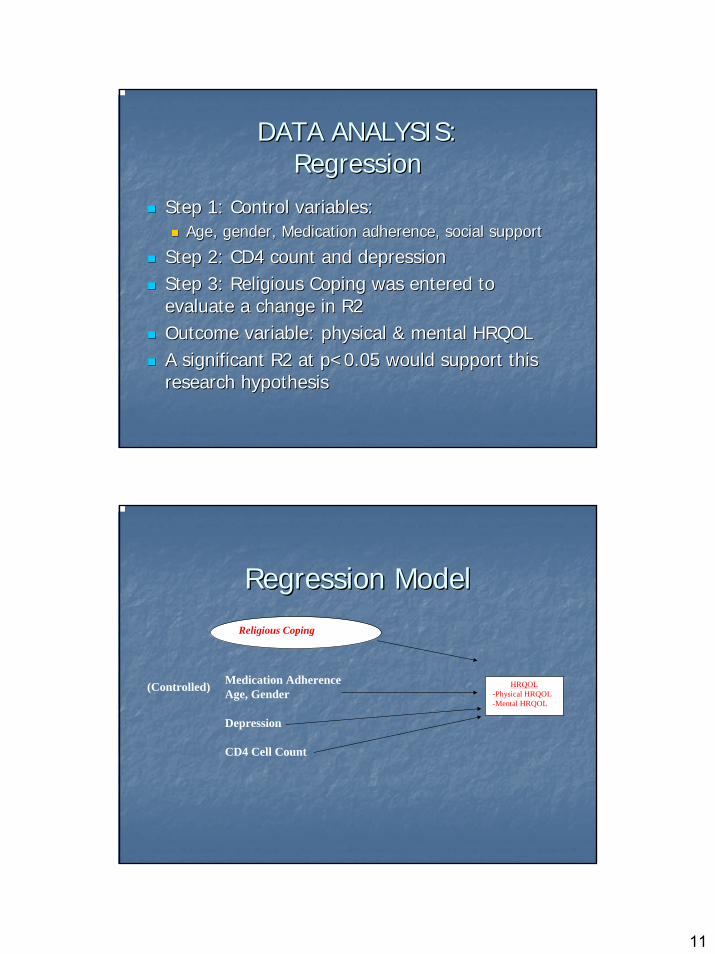
DATA ANALYSIS:DATA ANALYSIS:RegressionRegression
Step 1: Control variables: Step 1: Control variables: Age, gender, Medication adherence, social support Age, gender, Medication adherence, social support
Step 2: CD4 count and depression Step 2: CD4 count and depression Step 3: Religious Coping was entered to Step 3: Religious Coping was entered to evaluate a change in R2 evaluate a change in R2 Outcome variable: physical & mental HRQOLOutcome variable: physical & mental HRQOLA significant R2 at p<0.05 would support this A significant R2 at p<0.05 would support this research hypothesis research hypothesis
HRQOL -Physical HRQOL-Mental HRQOL
Religious Coping
Medication AdherenceAge, Gender
Depression
CD4 Cell Count
(Controlled)
Regression ModelRegression Model

12
STUDY FINDINGS: STUDY FINDINGS: DemographicsDemographics
GenderGender %% (n)(n)
MalesMales 55.8 (163)55.8 (163)
FemalesFemales 43.5 (127)43.5 (127)
Race/ EthnicityRace/ Ethnicity %% (n)(n)Black/ AfricanBlack/ African--AmericanAmerican 90.190.1 (263)(263)WhiteWhite 6.2 6.2 (18)(18)Asian/Pacific Islander/IndianAsian/Pacific Islander/Indian 1.01.0 (3)(3)Hispanic/ Latino or LatinaHispanic/ Latino or Latina 1.01.0 (3)(3)OtherOther 1.4 1.4 (4)(4)
STUDY FINDINGS: STUDY FINDINGS: DemographicsDemographics
EducationEducation %% (n)(n)None, I have not had None, I have not had .3.3 (1)(1)any formal schoolingany formal schoolingPrimary or Elementary schoolPrimary or Elementary school 1.41.4 (4)(4)Junior High or Middle schoolJunior High or Middle school 12.012.0 (35)(35)High school or G.E.D.High school or G.E.D. 52.752.7 (154) (154) College/Technical SchoolCollege/Technical School 21.921.9 (85)(85)Graduate or Professional SchoolGraduate or Professional School 3.83.8 (11)(11)

13
STUDY FINDINGS: STUDY FINDINGS: DemographicsDemographics
Marital StatusMarital Status %% (n)(n)MarriedMarried 12.012.0 (35)(35)Separated/Divorced/Widowed 36.3 (106)Separated/Divorced/Widowed 36.3 (106)SingleSingle 51.451.4 (150)(150)
Committed relationshipCommitted relationship 15.115.1 (44)(44)
STUDY FINDINGS: STUDY FINDINGS: DemographicsDemographics
EmploymentEmployment %% (n)(n)Unemployed/ On disability Unemployed/ On disability 90.890.8 (265)(265)Employed partEmployed part--timetime 7.97.9 (23)(23)Employed fullEmployed full--timetime .3.3 (1)(1)
Annual IncomeAnnual Income %% (n)(n)Under $11,000Under $11,000 68.5 (200)68.5 (200)$11,000$11,000--20,99920,999 17.8 (52)17.8 (52)≥≥$21,000$21,000 7.6 (22)7.6 (22)

14
STUDY FINDINGS: STUDY FINDINGS: DemographicsDemographics
Mean age 45.11(SD) yearsMean age 45.11(SD) yearsMean (subjective) CD4 count 467.24 Mean (subjective) CD4 count 467.24 (SD222.03) cells/(SD222.03) cells/μμL L Mean (subjective) HIV viral load was 1.55 Mean (subjective) HIV viral load was 1.55 (SD) x 1000 copies/ml (copies/ml) (SD) x 1000 copies/ml (copies/ml)
STUDY FINDINGS: STUDY FINDINGS: Spiritual/ Religious PracticesSpiritual/ Religious Practices
Religious Affiliation/DenominationReligious Affiliation/Denomination %% (n)(n)BaptistBaptist 47.6 (139)47.6 (139)Christian (nonChristian (non--specific)specific) 13.4 (39)13.4 (39)NonNon--denominationaldenominational 6.2 (18)6.2 (18)Belief in God, but no affiliationBelief in God, but no affiliation 8.2 (24)8.2 (24)MuslimMuslim 2.4 (7)2.4 (7)BuddhistBuddhist 1.4 (4)1.4 (4)JewishJewish .7 (2).7 (2)No Belief in GodNo Belief in God 1.4 (4)1.4 (4)OtherOther 9.6 (28)9.6 (28)
JehovahJehovah’’s Witness (7), Paganism (1), Pantheism (1)s Witness (7), Paganism (1), Pantheism (1)
Religious Service AttendanceReligious Service Attendance %% (n)(n)Never or rarelyNever or rarely 8.68.6 (25)(25)Once or twice a yearOnce or twice a year 15.415.4 (48)(48)Once or twice a month/every mo or soOnce or twice a month/every mo or so 32.832.8 (96)(96)Once a week or more Once a week or more 42.542.5 (124)(124)

15
STUDY FINDINGS:STUDY FINDINGS:Spiritual/Religious PracticesSpiritual/Religious Practices
Prayer or MeditationPrayer or Meditation __%% (n)_(n)_Once a day or moreOnce a day or more 44.144.1 (129)(129)Once a week/ a few times a weekOnce a week/ a few times a week 17.117.1 (50)(50)A few times a monthA few times a month 6.86.8 (20)(20)Once a month Once a month 4.54.5 (13)(13)Less than once a month Less than once a month 6.86.8 (20)(20)NeverNever 19.519.5 (57)(57)
Reading Religious/Spiritual MaterialsReading Religious/Spiritual Materials %% (n) (n) Once a day or moreOnce a day or more 32.532.5 (95)(95)A few times a weekA few times a week 21.221.2 (62)(62)Once a monthOnce a month 6.56.5 (19)(19)Less than once a monthLess than once a month 14.414.4 (42)(42)NeverNever 9.2 9.2 (27)(27)
STUDY FINDINGS:STUDY FINDINGS:Coping PracticesCoping Practices
““How do you manage to cope with your situation?How do you manage to cope with your situation?”” How How do you keep yourself from getting depressed, sad, or do you keep yourself from getting depressed, sad, or discouraged, despite your current situation, health or discouraged, despite your current situation, health or stressors ?stressors ?
Religious Coping (RCI)Religious Coping (RCI)Religious ways of coping: Religious ways of coping: 43.8% (128)43.8% (128)NonNon--religious coping:religious coping: 55.1% (161)55.1% (161)
Extent Religious ways of coping used (1Extent Religious ways of coping used (1--10)10)Mean= 8.1; Median=9.0Mean= 8.1; Median=9.0
Proportion of coping time on religious copingProportion of coping time on religious copingMean=66.6%; Median= 80%Mean=66.6%; Median= 80%

16
STUDY FINDINGS:STUDY FINDINGS:Spiritual/Religious ExperiencesSpiritual/Religious Experiences
Spiritual/Religious LifeSpiritual/Religious Life--Changing ExperienceChanging Experience76% (222)76% (222)Average age= 29 yrs, Median age= 28 yrsAverage age= 29 yrs, Median age= 28 yrs
Gain in FaithGain in Faith81.8 % (239)81.8 % (239)Average Age= 30.25 yrs, Median= 30 yrsAverage Age= 30.25 yrs, Median= 30 yrs
Loss in FaithLoss in Faith36% (105)36% (105)Average Age= 29.3 yrs, Median= 30 yrsAverage Age= 29.3 yrs, Median= 30 yrs
STUDY FINDINGS: STUDY FINDINGS: Mean ScoresMean Scores
MeanMean (SD)(SD)
CESCES--D score D score 19.319.3 (12.8)(12.8)
Religious copingReligious copingNegative RCOPENegative RCOPE 4.864.86 (5.34)(5.34)Positive RCOPEPositive RCOPE 16.616.6 (5.06)(5.06)
AGAS AGAS 24.324.3 (5.87)(5.87)
17
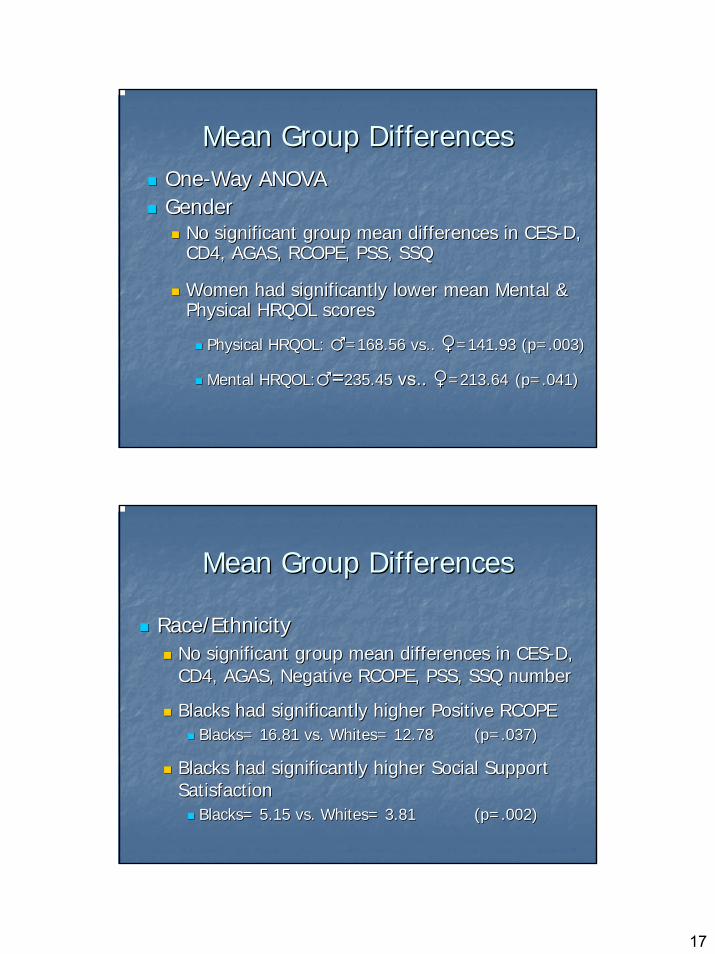
Mean Group DifferencesMean Group DifferencesOneOne--Way ANOVAWay ANOVAGenderGender
No significant group mean differences in CESNo significant group mean differences in CES--D, D, CD4, AGAS, RCOPE, PSS, SSQCD4, AGAS, RCOPE, PSS, SSQ
Women had significantly lower mean Mental & Women had significantly lower mean Mental & Physical HRQOL scores Physical HRQOL scores
Physical HRQOL: Physical HRQOL: ♂♂=168.56 vs.. =168.56 vs.. ♀♀=141.93 (p=.003)=141.93 (p=.003)
Mental HRQOL:Mental HRQOL:♂♂==235.45235.45 vs..vs.. ♀♀=213.64=213.64 (p=.041)(p=.041)
Mean Group DifferencesMean Group Differences
Race/EthnicityRace/EthnicityNo significant group mean differences in CESNo significant group mean differences in CES--D, D, CD4, AGAS, Negative RCOPE, PSS, SSQ numberCD4, AGAS, Negative RCOPE, PSS, SSQ number
Blacks had significantly higher Positive RCOPEBlacks had significantly higher Positive RCOPEBlacks= 16.81 vs. Whites= 12.78 Blacks= 16.81 vs. Whites= 12.78 (p=.037)(p=.037)
Blacks had significantly higher Social Support Blacks had significantly higher Social Support SatisfactionSatisfaction
Blacks= 5.15 vs. Whites= 3.81 Blacks= 5.15 vs. Whites= 3.81 (p=.002) (p=.002)

18
Correlations:Correlations:Stress and CopingStress and Coping
H1 Supported:H1 Supported: Religious coping scores Religious coping scores were correlated with stresswere correlated with stress
More positive forms of religious coping More positive forms of religious coping associated with lower perceived stressassociated with lower perceived stress
Positive RCOPE & Perceived stress Positive RCOPE & Perceived stress ((--.16) p=.005.16) p=.005
More negative forms of religious coping More negative forms of religious coping associated with higher perceived stress scoresassociated with higher perceived stress scores
Negative RCOPE & Perceived stress Negative RCOPE & Perceived stress (.45) p=.000(.45) p=.000
STUDY FINDINGS: STUDY FINDINGS: CorrelationsCorrelations
22ndnd Hypotheses supported: Religious coping Hypotheses supported: Religious coping scores were correlated with depression scoresscores were correlated with depression scores
H2a. Inverse relationship H2a. Inverse relationship Positive RCOPE and depressionPositive RCOPE and depression ((--.20).20) p<.01p<.01
H2b. Positive relationshipH2b. Positive relationshipNegative RCOPE and depressionNegative RCOPE and depression ( .54)( .54) p<.01p<.01

19
STUDY FINDINGS: STUDY FINDINGS: CorrelationsCorrelations
H3 Not supportedH3 Not supportedReligious coping scores not correlated with CD4 countReligious coping scores not correlated with CD4 count
(+) religious coping & CD4 count (.04) p=.64(+) religious coping & CD4 count (.04) p=.64((--) religious coping & CD4 count () religious coping & CD4 count (--.09) p=.36.09) p=.36
CD4 count only correlated with:CD4 count only correlated with:Depression Depression ((--.25) p=.016.25) p=.016Mental HRQOLMental HRQOL ( .23) p=.027( .23) p=.027Physical HRQOL Physical HRQOL ( .25) p=.015( .25) p=.015
STUDY FINDINGS: STUDY FINDINGS: CorrelationsCorrelations
H4 supportedH4 supportedCESCES--D scores were significantly inversely D scores were significantly inversely correlated with CD4 countcorrelated with CD4 count
CESCES--D and CD4 count D and CD4 count ((--.25).25) p=.016p=.016

20
STUDY FINDINGS: STUDY FINDINGS: RegressionRegression
H5 Supported H5 Supported The full model The full model (F=6.15, p=.000)(F=6.15, p=.000) explained 37% explained 37% of the variance of the variance (Adjusted R(Adjusted R--square=.373)square=.373) in in physical HRQOLphysical HRQOLPositive RCOPE explained 2.3% significant Positive RCOPE explained 2.3% significant additional variance in the physical HRQOL additional variance in the physical HRQOL (Adjusted R(Adjusted R--square .373 square .373 -- .350).350)
Predictors of Physical HRQOLPredictors of Physical HRQOL
Positive RCOPE Positive RCOPE (B= 3.09) p=.036(B= 3.09) p=.036Age Age (B=(B=--3.175) p=.0043.175) p=.004GenderGender (B=(B=--42.77) p=.01642.77) p=.016Depression Depression (B=(B=--2.35) p=.0022.35) p=.002
21
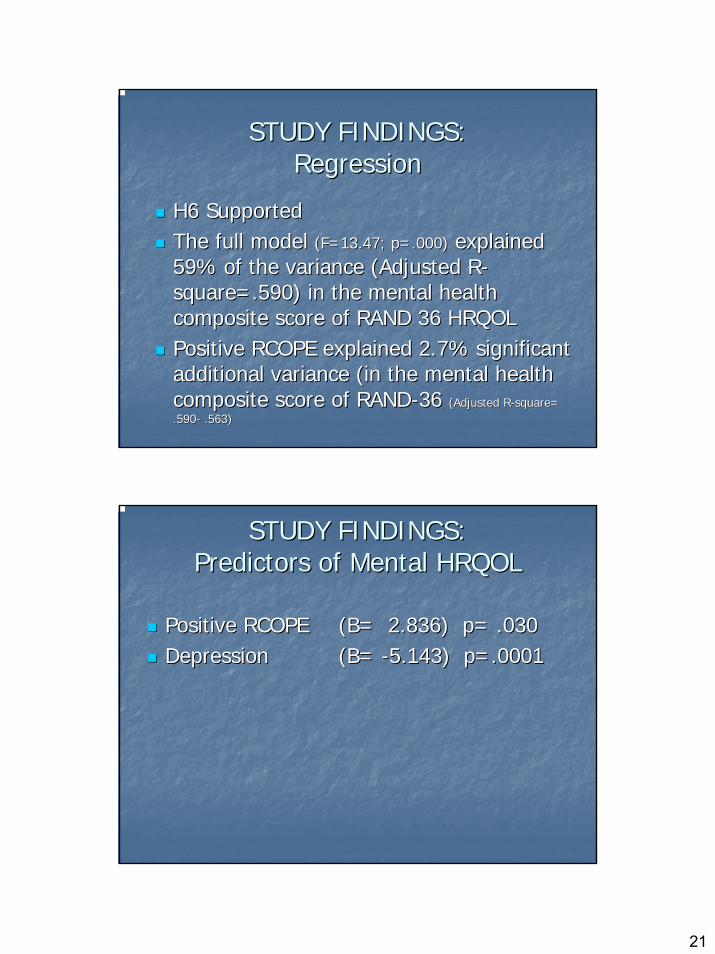
STUDY FINDINGS: STUDY FINDINGS: RegressionRegression
H6 Supported H6 Supported The full model The full model (F=13.47; p=.000)(F=13.47; p=.000) explained explained 59% of the variance (Adjusted R59% of the variance (Adjusted R--square=.590) in the mental health square=.590) in the mental health composite score of RAND 36 HRQOLcomposite score of RAND 36 HRQOLPositive RCOPE explained 2.7% significant Positive RCOPE explained 2.7% significant additional variance (in the mental health additional variance (in the mental health composite score of RANDcomposite score of RAND--36 36 (Adjusted R(Adjusted R--square= square= .590.590-- .563) .563)
STUDY FINDINGS: STUDY FINDINGS: Predictors of Mental HRQOLPredictors of Mental HRQOL
Positive RCOPE Positive RCOPE (B= 2.836) p= .030(B= 2.836) p= .030Depression Depression (B= (B= --5.143) p=.00015.143) p=.0001
22
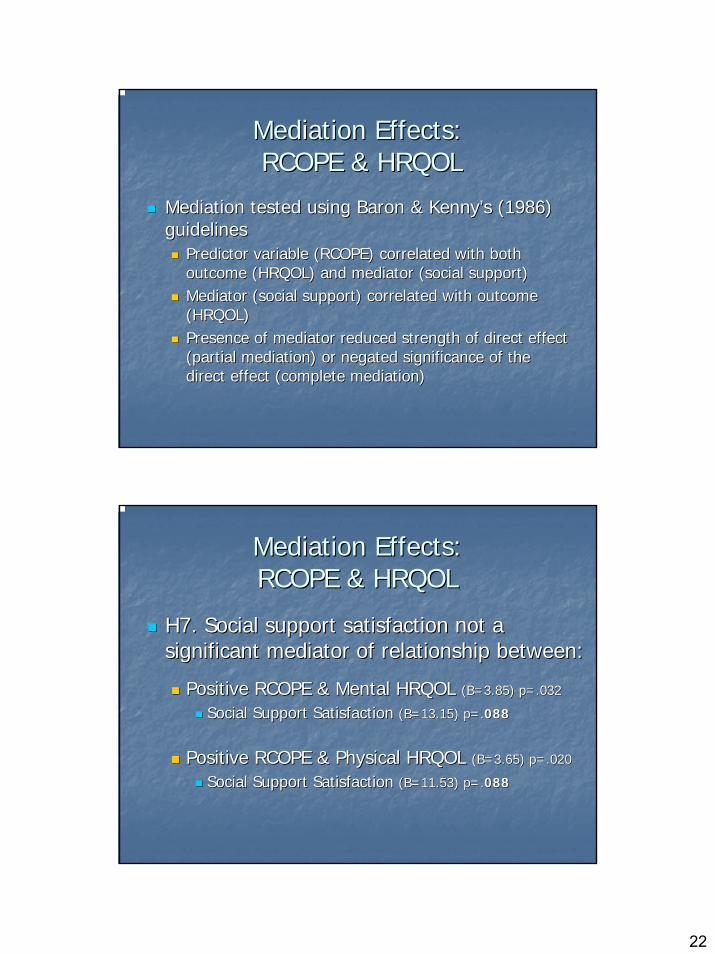
Mediation Effects:Mediation Effects:RCOPE & HRQOLRCOPE & HRQOL
Mediation tested using Baron & KennyMediation tested using Baron & Kenny’’s (1986) s (1986) guidelinesguidelines
Predictor variable (RCOPE) correlated with both Predictor variable (RCOPE) correlated with both outcome (HRQOL) and mediator (social support)outcome (HRQOL) and mediator (social support)Mediator (social support) correlated with outcome Mediator (social support) correlated with outcome (HRQOL)(HRQOL)Presence of mediator reduced strength of direct effect Presence of mediator reduced strength of direct effect (partial mediation) or negated significance of the (partial mediation) or negated significance of the direct effect (complete mediation)direct effect (complete mediation)
Mediation Effects:Mediation Effects:RCOPE & HRQOLRCOPE & HRQOL
H7. Social support satisfaction not a H7. Social support satisfaction not a significant mediator of relationship between:significant mediator of relationship between:
Positive RCOPE & Mental HRQOL Positive RCOPE & Mental HRQOL (B=3.85) p=.032(B=3.85) p=.032
Social Support Satisfaction Social Support Satisfaction (B=13.15) p=.(B=13.15) p=.088088
Positive RCOPE & Physical HRQOL Positive RCOPE & Physical HRQOL (B=3.65) p=.020(B=3.65) p=.020
Social Support Satisfaction Social Support Satisfaction (B=11.53) p=.(B=11.53) p=.088088

23
STUDY LIMITATIONSSTUDY LIMITATIONS
Inability to identify causal relationships Inability to identify causal relationships or make causal inferences with crossor make causal inferences with cross--sectional study design. sectional study design. Limited generalizability of the study Limited generalizability of the study findings to clients other than low to findings to clients other than low to moderate income HIVmoderate income HIV--infected men and infected men and women.women.SelfSelf--reported CD4 count used in current reported CD4 count used in current analysisanalysis
SUMMARYSUMMARYSpirituality is an important factor in health Spirituality is an important factor in health & well& well--being among people with HIV being among people with HIV Religious coping is associated with stress, Religious coping is associated with stress, depression, and HRQOL components depression, and HRQOL components Depression is inversely associated with Depression is inversely associated with immune status (CD4 count)immune status (CD4 count)Positive RCOPE explains a significant Positive RCOPE explains a significant amount of the variance in physical & amount of the variance in physical & mental HRQOLmental HRQOL

24
Implications for PracticeImplications for Practice
Acknowledging and supporting patient Acknowledging and supporting patient spirituality may enhance overall patient care spirituality may enhance overall patient care (Mueller, Plevak & Rummans, 2001)(Mueller, Plevak & Rummans, 2001)
Routine assessment of patientsRoutine assessment of patients’’ spiritual needs spiritual needs Assess if HIVAssess if HIV--positive people rely on spiritual positive people rely on spiritual resources or coping to adjust to having a liferesources or coping to adjust to having a life--threatening illness. threatening illness. Help HIV+ people find meaning and purpose to Help HIV+ people find meaning and purpose to facilitate improvements in HRQOL.facilitate improvements in HRQOL.
QUESTIONS?QUESTIONS?
SafiyaSafiya George George [email protected]@emory.edu
(404) 712(404) 712--8449 (Office)8449 (Office)
1520 Clifton Rd1520 Clifton RdEmory UniversityEmory University
Atlanta, GA 30322Atlanta, GA 30322


















